
Submitted:
27 April 2025
Posted:
28 April 2025
You are already at the latest version
Abstract
Orthodontic treatment applies mechanical forces that induce oxidative stress and inflammatory response within the periodontal tissue, potentially affecting oral health. Non-invasive diagnostic method through saliva offering a promising medium for evaluating oxidative stress biomarkers and gene expression profiles. This cross-sectional study assessed salivary biomarkers and the expression of the IL-1β and IL-8 genes in patients with orthodontic appliances, as these factors are crucial in inflammation, bone resorption, and remodeling during orthodontic treatment. Thirty orthodontic patients with fixed metallic appliances (≥6 months) and thirty matched healthy controls, ages 18 to 35, participated in this cross-sectional study. Salivary biomarkers, such as total protein concentration and oxidative stress markers were measured using standard assays. The expression of target genes was determined through Quantitative Reverse Transcription-PCR and the results were presented as fold change values. Oxidative stress markers demonstrated significant differences between groups, with the case group exhibiting notably higher levels of 8-OHdG (p = 0.0067), MDA (p = 0.0031), TAC (p = 0.0074), and TBARS (p < 0.0001). Orthodontic patients also displayed significantly elevated mean fold changes in IL-1β (p < 0.0001; 4.4) and IL-8 (p < 0.0001; 5.45) gene expression relative to controls. Furthermore, positive correlations were reported between the target genes and oxidative stress indicators, particularly MDA and 8-OHdG.A significant increase in oxidative stress levels and changes in salivary Interleukin-1 beta and Interleukin-8 gene expression have been observed during orthodontic treatment.
Keywords:
IL-1β
; IL-8
; Bone remodeling
; Gene expression
; Inflammation
; Orthodontic forces
; Oxidative stress
; Saliva biomarkers
1. Introduction
The main objective of orthodontic treatment, a crucial area of modern dentistry, is to enhance the function and appearance of the oral cavity by correcting dental malocclusions and craniofacial abnormalities [1,2]. Over time, much progress has been made in both technique and material [1]. However, the application of orthodontic forces can introduce biological stress which has implications for both tissue remodeling and periodontal health [3,4]. The oral ecosystem is a complex environment where various factors interact, and saliva serves as a key biological indicator of its condition, with orthodontic treatment often inducing inflammation and oxidative stress in response to applied forces [5].
The mechanical stresses applied during orthodontic treatment induce structural and physiological modifications in the periodontal ligament, including shifts in cellular activity, vascular dynamics, and fluid flow, as well as alterations to collagen fibers and extracellular matrix tension [6]. Oxidative stress, which damages cellular structures by peroxidatively damaging lipids, proteins, and genetic material, due to an imbalance between the host total antioxidant capacity and reactive oxygen species [7]. In the periodontal ligament, orthodontic stresses cause the release of inflammatory mediators, which results in tissue remodeling, inflammation, and an increase in ROS generation [8]. Biomolecules such as interleukin, TNF-α, macrophage colony-stimulating factor, prostaglandins, growth factors, enzymes, and vasoactive neurotransmitters are released as a result of this process [6]. Important modulators of bone remodeling in response to mechanical pressures include IL-1B (Interleukin-1 beta), IL-6 (Interleukin-6), TNF-α (Tumor necrosis factor),and IL-8 (Interleukin-8), and [9,10]. Additionally, orthodontic materials, such as metals and plastics, can release elements that further increase ROS levels, influencing both the oral environment and tissue remodeling [7,11]. Fixed orthodontic appliances induce oxidative stress by releasing metal ions through corrosion and friction, triggering ROS production and associated health risks [12]. Laboratory-based research has demonstrated that orthodontic appliances, including brackets and arch wires, can trigger oxidative stress by releasing heavy metal ions [13,14]. In vivo studies on salivary and gingival crevicular fluid biomarkers report mixed results [5,15,16].
Research has indicated that oxidative stress biomarkers temporarily rise immediately following the placement of orthodontic devices but normalize to pre-treatment levels within days or weeks [5,15]. In contrast, one investigation revealed no statistically significant alterations in these biomarkers after one and six months of orthodontic therapy [16]. Saliva serves as a useful medium for evaluating oxidative stress biomarkers associated with local oral conditions and, as a noninvasive diagnostic method indicate the changes caused on by medical conditions [17,18]. The activity of genes involved in inflammation during orthodontic treatment linked to bone resorption and periodontal disease [19,20]. IL-1β is released by various cells including connective tissue fibroblasts, gingival epithelium, macrophages, neutrophils, and dendritic cells, it promotes inflammation, bone resorption, and tissue degradation [21]. In reaction to IL-1 and TNF-α, different cells release IL-8, which draw neutrophils and leukocytes to inflammatory areas. Orthodontic forces raise IL-8 levels, which may also be a factor in bone resorption [22,23,24].
In dental medicine, specific biomarkers are utilized to evaluate oxidative stress and cellular damage within oral tissues [25]. Key indicators include Total Protein Concentration, markers of lipid peroxidation (MDA, AND TBARS); Total Antioxidant Capacity (TAC) which quantifying systemic antioxidant responses in host; and the marker of DNA alterations (8-Hydroxy-2'-Deoxyguanosine) [4,26]. These biomarkers play a critical role in identifying and managing conditions such as periodontal disease, offering insights into pathological mechanisms and therapeutic monitoring for oral health disorders during orthodontic therapy [27,28]. This study therefore aimed to evaluate salivary expression of IL-8 and IL-1B genes, as well as salivary markers in patients with orthodontic bracket and their corresponding healthy adults.
2. Materials and Methods
2.1. Study Design
This cross-sectional study was carried out in Erbil-Iraq, from February to April 2025. Thirty individuals undergoing orthodontic treatment, fixed metallic bracket, for over six months and thirty age-matched controls without orthodontic interventions, systemic illnesses, or oral health issues (ages 18–35). Demographic and baseline data were gathered using structured interviews. To reduce confounding factors, saliva samples were collected in the morning between 10:00 and 12:00 AM. Collections occurred in pre-labeled sterile containers prior to any clinical interventions. The levels of oxidative stress biomarkers were determined using standardized laboratory procedures. Furthermore, the gene expression levels of inflammatory, bone resorption, and remodeling biomarkers like (IL-1β) and (IL-8) were evaluated through the qRT-PCR. Descriptive methods of statistics were employed to calculate the data, and SPSS version 25 (IBM Corp., Armonk, NY, USA) was chosen for statistical evaluation, with an acceptable level of significance of p < 0.05.
2.2. Sample Collection
The method suggested by Henson et al. [29], was utilized as collecting saliva. Subjects refrained from oral intake, dental hygiene practices, tobacco use, or gum consumption for a minimum one-hour period preceding specimen collection. Ten minutes prior to collecting, the mouth was rinsed with tap water. The saliva was then expectorated into sterile tubes, chilled on ice packs, centrifuged at °C (5 minutes, 5000 gravitational force) in the laboratory, and stored at -20°C for subsequent biochemical and molecular analysis.
2.3. Total Protein Concentration
Saliva was tested for total protein using a commercial kit (Biuret technique, PROTBIU-600). This technique uses alkaline conditions to cause cupric ions and proteins to form a purple-blue complex. The results were expressed as g/dL, and the intensity was reported at 560 and 520 nm. The concentration of total protein was directly proportional to the color intensity [30].
2.4. Total Antioxidant Capacity
The Abbexa Kit (abx295022), which is based on the FRAP (Ferric Reducing Antioxidant Power) analysis method, was used to determine the concentration of total antioxidant capacity (TAC) in saliva. To separate the supernatant, saliva samples were centrifuged at 4°C (10 minutes, 10000 rpm). The buffer solution, tripyridyltriazine (TPTZ) solution, and substrate (sample) were combined to create the working solution (FRAP). An iron sulfate (FeSO4) solution containing 100 mmol/L was used to create standards with known values (0–2.5 mmol/L). 180 µL of the FRAP was applied to the samples and standard solution (5 µL) [31]. The absorbance was reported at 593 nm following a 5-minute incubation period at 37°C. A standard curve was used to calculate the concentrations of TAC (mmol/L).
2.5. Measurement of Malondialdehyde (MDA)
Malondialdehyde (MDA) was quantified using the thiobarbituric acid reactive substances (TBARS) method, which produces a chromogenic pink complex when MDA and thiobarbituric acid react. At a wavelength of 532 nm, the optical density of this chemical was measured using spectrophotometry, and concentrations were expressed as micromoles per liter (µmol/L) [32].
2.6. Measurement of Salivary 8-OHdG Levels by ELISA
The concentration of salivary 8-OHdG was assessed via a commercially available ELISA kit utilizing a monoclonal antibody with high specificity. The procedure was conducted in a 96-well microplate (Thermo Fisher Scientific), and absorbance was recorded spectrophotometrically at 450 nm within a 15-minute window following the addition of the stop reagent. The assay demonstrated a detection threshold spanning 0.125 to 225 nanograms per milliliter (ng/mL) [33].
2.7. Measurement of Thiobarbituric Acid Reactive Substances (TBARS)
A spectrofluorometric technique was used for quantifying the amounts of TBARS following derivatization with 0.67% thiobarbituric acid in phosphoric acid (100°C, 45 min). N-butanol was used to extract colored products, which was then centrifuged for 12 minutes at 3000 rpm and compared against a standardized (1,1,3,3-tetrametoxypropan). After measuring each sample's absorbance at 532 nm, the findings were calculated with a constructed standard curve and the results expressed as µmol/L [34].
2.8. Extraction of Salivary RNA
RNA isolation was performed with the available saliva mini-extraction Kit (Qiagen, Germany), adhering to the supplier’s instructions. The kit employs a silica membrane-based methodology engineered to isolate >100 µg of RNA, optimizing yield for downstream RT-qPCR applications. Enzymatic treatment with DNase and protease ensured elimination of genomic DNA and protein contaminants, respectively. Purified RNA (~10 µL) was eluted and preserved at -20°C until subsequent processing. RNA integrity and quantification were determined using a NanoDrop spectrophotometer (Lantech, Korea), with nucleic acid purity quantified via A260/A280 absorbance ratios.
2.9. Quantitative Gene Expression (qRT-PCR)
For cDNA synthesis, Reverse Transcription Kit (Thermo Fisher, USA) was used, with a total volume of 10.0 µL per reaction. The reaction mixture contained 10X Buffer (2.0 µL), 25X dNTP Mix (0.8 µL, 100 mM), 10X Random Primers (2.0 µL), Reverse Transcriptase enzyme (1.0 µL), RNase Inhibitor (1.0 µL), and nuclease-free H2O (3.2 µL). Following synthesis, the cDNA was immediately used in quantitative PCR applications. IL-1β and IL-8 gene expressions were evaluated using quantitative real-time PCR based on SYBR.
Ten µL of GoTaq® qPCR Master Mix (Promega, USA), two µL of salivary cDNA, and ten µmol of each primer were included in the reaction mixture. For IL-8, the primers were F: GAGGGTTGTGGAGAAGTTTTTG and R: CTGGCATCTTCACTGATTCTTG, whereas for IL-1β, they were F: GTGCTGAATGTGGACTCAATCC and R: ACCCTAAGGCAGGCAGTTG. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as a reference for gene expression, and the forward and reverse primers were TGAAGGTCGGAGTCAACGGATTTGGT and CATGTGGGCCATGAGGTCCACCAC, respectively. Table 1 displays the PCR primer set sequences (in the 5'–3' orientation). A Real-Time PCR machine (Thermo Fisher Scientific) was used to accomplish relative quantification. Each sample's relative expression for each particular product was assessed in triplicate. The target gene expression was determined using the 2−ΔΔCt methods based on threshold cycle (CT) for both the reference gene GAPDH and the target genes (ΔCt = Ct (target genes) - Ct (reference gene), ΔΔCt = ΔCt (target group) - ΔCt (control group).

Table 1.
used primers in this study.
| Gene Symbol | Sequence | Gene ID | Amplicon Size (bp) | References |
|---|---|---|---|---|
| IL-8 | F1: GAGGGTTGTGGAGAAGTTTTTG R1: CTGGCATCTTCACTGATTCTTG |
NM_000584 | 88bp | [35,36,37] |
| IL-1β | F2: GTGCTGAATGTGGACTCAATCC R2: ACCCTAAGGCAGGCAGTTG |
M15330 | 120bp | |
| GAPDH | F3: TGAAGGTCGGAGTCAACGGATTTGGT R3: CATGTGGGCCATGAGGTCCACCAC |
NM_002046.7 | 983bp | [37,38,39]. |
3. Results
A control group of thirty healthy adults and a case group of thirty orthodontic patients with fixed appliances made up a total of sixty participants. Table 2 showed no significant differences between two groups; the p values for gender, age, and smoking status were 0.79, 0.94, and 0.59, respectively.
Table 2.
Baseline characteristics.
| Gender Distribution | Control (n=30) Frequency, % |
Case (n=30) Frequency, % |
P value | |
|---|---|---|---|---|
| Male | 14 (46.7) | 13 (43.3) | 0.79 | |
| Female | 16 (53.3) | 17 (56.7) | ||
| Age (Mean ± SD) | 26.0 (5.33) | 26.1 (5.12) | 0.94 | |
| Smoking status | Smoker | 10 (33.3) | 12 (40) | 0.59 |
| Nonsmoker | 20 (66.7) | 18 (60) | ||
Salivary biomarker concentrations were evaluated for each participant following unstimulated salivary samples collection which were taken from both groups, Table 3. Salivary total protein level was not significantly different between the groups (control: mean = 1.71 g/dl, SD = 0.12; case: mean = 2.25 g/dl, SD = 1.82, P = 0.1103). Salivary oxidative stress biomarkers were significantly greater in the case group than in the controls. In particular, the mean TBARS concentration in the case group was 1.40 μmol/l (SD = 0.87), while for the control group was 0.48 μmol/l (SD = 0.24; P < 0.0001). The case group also had higher levels of TAC, MDA, and 8-OHdG, with respective means of 0.57, 0.59, and 0.83.
Table 3.
Salivary total protein concentration and levels of oxidative stress biomarkers in study groups.
Table 3.
Salivary total protein concentration and levels of oxidative stress biomarkers in study groups.
| Parameters | Control (n=30) Frequency, % |
Case (n=30) Frequency, % |
P value | |
|---|---|---|---|---|
|
Total Protein g/dl |
Mean ± SD | 1.71 (0.12) | 2.25 (1.82) | P = 0.1103 |
|
TBARS μmol/l |
0.48 (0.24) | 1.40 (0.87) | P < 0.0001 | |
|
TAC mmol/l |
0.34 (0.11) | 0.57 (0.44) | P = 0.0074 | |
|
MDA μmol/l |
0.31 (0.08) | 0.59 (0.49) | P = 0.0031 | |
|
8-OHdG ng/ml |
0.49 (0.05) | 0.83 (0.66) | P = 0.0067 | |
Table 4, Figure 1, and Figure 2 represent the mean fold change values for the salivary relative gene expression levels of IL-1β (IL1) and IL-8 (IL8) for both groups. The expression levels of both target genes were significantly elevated in case group (P < 0.0001, t-statistic = 4.678). The mean fold change for IL-1β was 4.4 (SD = 3.31) in case group, while for controls was 1.3 (SD = 1.49). Additionally, IL-8 showed a significant difference (P < 0.0001, t-statistic = 4.421); the mean fold changes were 5.45 (SD = 4.79) and 1.41 (SD = 1.45) for case and controls, respectively. Overall, in both groups, IL8 had a greater mean fold change than IL1.
Age, gender, and smoking status did not significantly correlate with the target gene expression, according to Table 5. Salivary IL1 expression and MDA levels (ρ = 0.575, P < 0.0001) and 8-OHdG levels (ρ = 0.416, P = 0.001) showed a strong positive significant relationship. The expression level of IL1 was also observed to have a moderate association with TAC levels (ρ = 0.318, P = 0.013) and total protein concentration (ρ = 0.264, P = 0.041). Similar findings were made by salivary IL8 expression, which was strongly correlated with both MDA (ρ = 0.479, P < 0.0001) and 8-OHdG (ρ = 0.467, P < 0.0001). Furthermore, Figure 3 shows a strong positive significant association between the levels of IL1 and IL8 expression (ρ = 0.821, P < 0.0001).
4. Discussion
This investigation focused on salivary total protein, oxidative stress biomarkers, and inflammatory cytokines (IL-1β and IL-8) during orthodontic treatment for over six months. Sixty participants (aged 18-35) were included, thirty orthodontic patients in the case group and thirty healthy adults.
Age (p = 0.94), smoking status (p = 0.59), and gender (p = 0.79) did not significantly differ between the groups. The results of the study were therefore unaffected by these factors. According to previous studies, it is more appropriate to collect and evaluate salivary oxidative stress biomarkers, particularly 8-OHGua, in the morning [40]. Another study also reported higher salivary TAC concentrations during the early morning hours [41]. A longitudinal pilot study aimed at determining the variability of oxidative stress biomarkers in healthy adults (mean age 38.73 ± 5.18 years) found no significant day-to-day differences but observed significant variations in the concentration of biomarkers (GPX, TAC, and MDA) between morning and afternoon [42]. Base on the study by Kamodyová and Celec [43], stimulated saliva collection techniques changes the concentration of oxidative stress biomarkers (AGEs and TBARS) compare to unstimulated saliva collection. Therefore, in this study, unstimulated saliva samples (1 mL) were collected from both groups during the same time frame (10:00-12:00 AM) after rinsing with tap water.
The findings showed no noticeable difference in the concentration of salivary total protein across the groups (P = 0.1103). A previous study reported salivary total protein levels before the placement of fixed metallic appliances (T0, 405.6 mmol/L), one month after placement (T1, 347.0 mmol/L), and nine months after placement (T2, 371.0 mmol/L) in patients aged 10 to 20 years. Their results showed a statistically significant difference in total protein levels between T0 and T1, but no significant differences were observed between T0 and T2 [44]. This finding is consistent with the results of our study, as in this study salivary total protein levels compared between patients with fixed metallic appliances for more than 6 months and control group. Another study also reported no significant differences (p = 0.83) of salivary total protein concentration in patients currently under fixed orthodontic treatment (n=25) compared to control group (n=25), aged between 15.8 to 25.2 years old [45].
The study found statistically significant differences (p = 0.0001, 0.0074, 0.0031, and 0.0067, respectively) between the orthodontic patient group and controls in terms of mean concentrations of oxidative stress biomarkers. Additionally, previous study revealed notable increases in TBARS and total oxidant status (TOS) in both stimulated and unstimulated saliva samples one week following orthodontic appliance placement, as observed in a subgroup of 37 participants aged 21.2 to 24.5 years [5]. A study measured the mean salivary total antioxidant capacity (TAC) at different stages in 10 patients (mean age: 26.8 years), same study concluded a significant increase in TAC at the at the beginning of orthodontic treatments in case group compare to their controls, and a progressive decrease in TAC values approaching baseline levels after sixty days [46]. The findings of our study is not aligned with the finding of previous studies in term of salivary MDA levels. For instance, a study reported no significant changes in the MDA levels after orthodontic treatments (foxed metallic appliance) at different stages [44]. Similarly, previous study concluded that the concentration of lipid peroxidase biomarker (MDA) and DNA alteration biomarker (8-OHdG) during orthodontic treatment with fixed appliances showed no significant changes after (6 or 12 months) in patients aged between 15-18 years old [47]. On other hand, other reported an increase of 8-OHdG after 9 months of treatment, but the difference were not significant [48]. While findings of present study agree with other findings, level of salivary MDA start to increase in patients undergo fixed orthodontic treatment, especially at first 24 hours and start to but yet not reaching to the base values at after 3 months due to the metal ions release from appliances [49]. Other study, reported two-fold increase of 8-OHdG concentration in oral epithelial cells of 51 patients (aged between 12 and 36 years old) after placement of fixed orthodontic treatment [50]. Moreover, invitro study confirmed that, all types of orthodontic brackets increase oxidative stress biomarkers especially full metal and polyurethane brackets [13]. With considerably greater levels of TBARS, TAC, MDA, and 8-OHdG in the case group, therefore these results are in line with earlier studies that suggest fixed orthodontic appliances can contribute to increase oxidative stress. The level of oral reactive oxygen species is known to rise when metal ions are released from orthodontic appliances, which could explain the increase in oxidative stress markers. As highlighted in earlier studies, the presence of metal in the mouth can lead to corrosion, disrupting the balance between antioxidant capacity and ROS production, ultimately leading to oxidative stress [14,51]. Additionally, other external factors, such as the oxidative potential of dental materials, may further exacerbate the generation of ROS during orthodontic treatment [52].
Few studies have examined salivary pro-inflammatory markers during orthodontic tooth movement in humans. This present study aimed to compare the expression of IL-1β and IL-8 genes in patients with fixed metallic appliances and a control group using a PCR based method. According to the results of quantitative real-time PCR, the mean fold change of IL-1β, and IL-8 was significantly higher in case group compared to controls, p value was 0.0001 for both genes. This results agree with results of previous study, the mechanical forces orthodontic appliance cause a rapid release of TNF-α, IL-1β, and IL-8 in the process of treatment [53]. In contrast, others reported the significant elevation of salivary level of IL-1α, and IL-8 at early stages of orthodontic treatments [24]. The difference in results may be due to varying methodologies, as previous studies used enzyme-linked immunosorbent assay (ELISA), while this study employed quantitative real-time PCR for determining the expression levels of salivary IL-1β and IL-8.
The correlation between salivary IL-1β, IL-8, and other biomarker expression levels was also evaluated in this analysis. The data for fold change values of IL-1β and IL-8 were not normally distributed, as confirmed by the Kolmogorov-Smirnov and Shapiro-Wilk tests (P = 0.000). Therefore, a non-parametric Spearman’s rank correlation test was applied to analyze the relationships between various parameters. No significant correlations were found between gene expression levels and age, gender, or smoking status. However, a strong positive correlation was observed between IL-1β expression and MDA levels (ρ = 0.575, P < 0.0001), as well as with 8-OHdG levels (ρ = 0.416, P = 0.001). Additionally, moderate correlations were found between IL-1β expression and total protein concentration (ρ = 0.264, P = 0.041) and TAC levels (ρ = 0.318, P = 0.013). Similarly, IL-8 expression showed significant correlations with MDA (ρ = 0.479, P < 0.0001) and 8-OHdG (ρ = 0.467, P < 0.0001). Furthermore, a strong positive correlation between IL-1β and IL-8 expression levels was observed (ρ = 0.821, P < 0.0001). Few studies have thoroughly explored the relationship between salivary IL-1β and IL-8 expression levels, particularly in the context of orthodontic treatments. Thus, the results of our study have primarily compared in terms of the association of target genes. In orthodontic patients, there is a positive correlation between the salivary IL-1β level and the oral bacterial load [54]. The local host reaction to orthodontic stresses causes an increase in IL-8 and neutrophil buildup, which in turn sets off processes of bone resorption and remodeling [53]. IL-6 and 8-OHdG levels in the serum of patients with TMJ disorders were found to be strongly correlated in another investigation [55].
5. Conclusions
According to the results, fixed metallic orthodontic equipment changes the expression of salivary IL-1β and IL-8 genes and dramatically enhance oxidative stress (TBARS, TAC, MDA, and 8-OHdG). These biological changes indicate that orthodontic therapy may cause oxidative and inflammatory reactions that could affect periodontal health. The study design as a cross-sectional, sample collection at a single point, and the small sample size of 30 participants per group may limit the generalizability of the results.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of Hawler Medical University College of Dentistry (protocol code 2425161 at 2\2\2025).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting the results of this study are available within the manuscript itself. All relevant datasets and information generated during the study are included in the published article.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviation | Full Term |
| 8-OHdG | 8-Hydroxy-2'-Deoxyguanosine |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| GAPDH | Glyceraldehyde-3-Phosphate Dehydrogenase |
| IL-1β | Interleukin-1 beta |
| IL-6 | Interleukin-6 |
| IL-8 | Interleukin-8 |
| MDA | Malondialdehyde |
| qRT-PCR | Quantitative Reverse Transcription-Polymerase Chain Reaction |
| TAC | Total Antioxidant Capacity |
| TBARS | Thiobarbituric Acid Reactive Substances |
| TNF-α | Tumor Necrosis Factor-alpha |
References
- Inchingolo F, Inchingolo AM, Latini G, Ferrante L, Trilli I, Del Vecchio G; et al. Oxidative stress and Natural products in Orthodontic Treatment: a systematic review. 2023, 16, 113. [CrossRef]
- Bazarova KM, Zhartybaev RA, Salymbekov BB, Iskakova MK, editors. Orthodontic problems in the treatment of patients with dental defects. Science and education: problems and innovations; 2021. [CrossRef]
- Yan M, Zhang Y, Niu W, Liu K, Xue L, Zhou KJMR; et al. Reactive oxygen species-mediated endoplasmic reticulum stress contributes to osteocyte death induced by orthodontic compressive force. 2023, 86, 1529–41. [CrossRef]
- GEÇER RBJH, -II S. OXIDATIVE STRESS AND ORTHODONTIC TREATMENT. 2024:137.
- Buczko, P.; Knaś, M.; Grycz, M.; Szarmach, I.; Zalewska, A.J.A.i.M.S. Orthodontic treatment modifies the oxidant–antioxidant balance in saliva of clinically healthy subjects. 2017, 62, 129-35. [CrossRef]
- Li Y, Jacox LA, Little SH, Ko C-CJTKjoms. Orthodontic tooth movement: The biology and clinical implications. 2018, 34, 207–14. [CrossRef]
- Menéndez López-Mateos C, Menéndez López-Mateos ML, Aguilar-Salvatierra A, Gómez-Moreno G, Carreño JC, Khaldy H; et al. Salivary Markers of Oxidative Stress in Patients Undergoing Orthodontic Treatment with Clear Aligners versus Self-Ligating Brackets: A Non-Randomized Clinical Trial. 2022, 11, 3531. [CrossRef]
- Tóthová Lu, Celec PJFip. Oxidative stress and antioxidants in the diagnosis and therapy of periodontitis. 2017, 8, 1055. [CrossRef]
- Ren Y, Hazemeijer H, de Haan B, Qu N, de Vos PJJop. Cytokine profiles in crevicular fluid during orthodontic tooth movement of short and long durations. 2007, 78, 453–8. [CrossRef]
- Karimi-Afshar, M.; Torabi, M.; Abdollahi, S.; Safarian, M.S.; Farsinejad, A.J.J.o.K.U.o.M.S. A comparative study on the IL-8 expression in gingival crevicular fluid during early alignment stage of orthodontic treatment in adults and adolescents. 2021, 28, 367-73. [CrossRef]
- Rodrigues R, Mesquita CM, ALVES HBdN, Silva FG, VIEIRA WdA, AGUIAR PCSd; et al. Changes in salivary biomarkers of pain, anxiety, stress, and inflammation related to tooth movement during orthodontic treatment: a systematic review. 2024, 29, e242436. [CrossRef]
- Primožič, J.; Poljšak, B.; Jamnik, P.; Kovač, V.; Čanadi Jurešić, G.; Spalj, S.J.A. Risk assessment of oxidative stress induced by metal ions released from fixed orthodontic appliances during treatment and indications for supportive antioxidant therapy: A narrative review. 2021, 10, 1359. [CrossRef]
- Buljan, Z.I.; Ribaric, S.P.; Abram, M.; Ivankovic, A.; Spalj, S.J.T.A.O. In vitro oxidative stress induced by conventional and self-ligating brackets. 2012, 82, 340-5. [CrossRef]
- Spalj S, Zrinski MM, Spalj VT, Buljan ZIJAjoo, orthopedics d. In-vitro assessment of oxidative stress generated by orthodontic archwires. 2012, 141, 583–9. [CrossRef]
- Olteanu C, Muresan A, Daicoviciu D, Tarmure V, Olteanu I, Keularts IMJPF. VARIATIONS OF SOME SALIVA MARKERS OF THE OXIDATIVE STRESS IN PATIENTS WITH ORTHODONTIC APPLIANCES. 2009, 19.
- Atuğ Özcan SS, Ceylan İ, Özcan E, Kurt N, Dağsuyu İM, Çanakçi CFJDm. Evaluation of oxidative stress biomarkers in patients with fixed orthodontic appliances. 2014, 2014, 597892. [CrossRef]
- Vlková B, Stanko P, Minárik G, Tóthová Ľ, Szemes T, Baňasová L; et al. Salivary markers of oxidative stress in patients with oral premalignant lesions. 2012, 57, 1651–6. [CrossRef]
- Cazzolla AP, Brescia V, Lovero R, Fontana A, Giustino A, Dioguardi M; et al. Evaluation of Biomarkers of Bone Metabolism on Salivary Matrix in the Remodeling of Periodontal Tissue during Orthodontic Treatment. 2024, 12, 209. [CrossRef]
- Chairatnathrongporn, R.; Tansriratanawong, K.; Santiprabhob, J.; Boriboonhirunsarn, C.; Promsudthi, A.J.J.o.I.S.o.P.; Dentistry, C. Salivary gene expression of RANK, RANKL, and OPG in type 1 diabetes mellitus and periodontal disease patients. 2022, 12, 603-11. [CrossRef]
- Ismah, N.; Bachtiar, E.W.; Purwanegara, M.K.; Tanti, I.; Mardiati, E.J.J.o.I.S.o.P.; Dentistry, C. Evaluation of IL-1β and CRP mRNA expression levels by RT-PCR in postorthodontic treatment patients with temporomandibular joint disorders: a cross-sectional Study. 2024, 14, 98-104. [CrossRef]
- Guarnieri R, Reda R, Di Nardo D, Miccoli G, Pagnoni F, Zanza A; et al. Expression of IL-1β, IL-6, TNF-α, and a-MMP-8 in sites with healthy conditions and with periodontal and peri-implant diseases: A case-control study. 2024, 18, 135. [CrossRef]
- Alhashimi, N.; Frithiof, L.; Brudvik, P.; Bakhiet, M.J.A.J.o.O.; Orthopedics, D. Orthodontic tooth movement and de novo synthesis of proinflammatory cytokines. 2001, 119, 307-12. [CrossRef]
- Başaran, G.; Özer, T.; Kaya, F.A.; Hamamci, O.J.A.J.o.O.; Orthopedics, D. Interleukins 2, 6, and 8 levels in human gingival sulcus during orthodontic treatment. 2006, 130, 7. e1-7. e6. [CrossRef]
- Saloom, H.F. Evaluation of Salivary Levels of Proinflammatory Cytokines (IL-1α, IL-8 and GM-CSF) in Adult Orthodontic Patients. 2018.
- de Sousa Né YG, Lima WF, Mendes PFS, Baia-da-Silva DC, Bittencourt LO, Nascimento PC; et al. Dental caries and salivary oxidative stress: global scientific research landscape. 2023, 12, 330. [CrossRef]
- Demirci-Çekiç S, Özkan G, Avan AN, Uzunboy S, Çapanoğlu E, Apak RJJop; et al. Biomarkers of oxidative stress and antioxidant defense. 2022, 209, 114477. [CrossRef]
- Khajuria AK, Thalquotra M, Singh P, Agarwal GJEJoM, Medicine C. ASSESSMENT OF OXIDATIVE STRESS GENERATED BY ORTHODONTIC ARCHWIRES-AN IN VITRO STUDY. 2022, 9, 2092–7.
- Syed IB, Khalid S, Abbas A, Faisal Z, Abbas H, Azeem MJJOKCOD. IN-VIVO ANALYSIS OF OXIDATIVE STRESS IN AESTHETIC COATED ORTHODONTIC ARCH-WIRES & BRACKETS. 2025, 15, 44–51. [CrossRef]
- Henson, B.S.; Wong, D.T. Collection, storage, and processing of saliva samples for downstream molecular applications. Oral biology: molecular techniques and applications: Springer; 2010. p. 21-30. [CrossRef]
- Akbarnejad, A.A.; Mahjoub, S.; Tamaddoni, A.; Masrour-Roudsari, J.; Seyedmajidi, S.A.; Ghasempour, M.J.J.o.D. Salivary oxidative stress, total protein, iron and ph in children with β-thalassemia major and their correlation with dental caries. 2022, 23, 266. [CrossRef]
- Benzie IF, Strain JJJAb. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: the FRAP assay. 1996, 239, 70–6. [CrossRef]
- De Leon, J.A.D.; Borges, C.R.J.J.o.v.e.J. Evaluation of oxidative stress in biological samples using the thiobarbituric acid reactive substances assay. 2020(159):10.3791/61122.
- Arunachalam, R.; Reshma, A.P.; Rajeev, V.; Kurra, S.B.; Prince, M.R.J.; Syam, N.J.T.S.J.f.D.R. Salivary 8-Hydroxydeoxyguanosine–a valuable indicator for oxidative DNA damage in periodontal disease. 2015, 6, 15-20. [CrossRef]
- Celec P, Hodosy J, Celecová V, Vodrážka J, Červenka T, Halčák L; et al. Salivary thiobarbituric acid reacting substances and malondialdehyde–their relationship to reported smoking and to parodontal status described by the papillary bleeding index. 2005, 21, 133–7. [CrossRef]
- Li Y, St. John MA, Zhou X; et al. Salivary transcriptome diagnostics for oral cancer detection. 2004, 10, 8442-50. [CrossRef]
- Park NJ, Zhou X, Yu T, Brinkman BM, Zimmermann BG, Palanisamy V; et al. Characterization of salivary RNA by cDNA library analysis. 2007, 52, 30–5. [CrossRef]
- Senevirathna K, Mahakapuge TAN, Jayawardana NU, Rajapakse J, Gamage CU, Seneviratne B; et al. Diagnostic potential of salivary IL-1β, IL-8, SAT, S100P, and OAZ1 in oral squamous cell carcinoma, oral submucous fibrosis, and oral lichen planus based on findings from a Sri Lankan cohort. 2024, 14, 27226. [CrossRef]
- Uehara A, Sugawara S, Watanabe K, Echigo S, Sato M, Yamaguchi T; et al. Constitutive expression of a bacterial pattern recognition receptor, CD14, in human salivary glands and secretion as a soluble form in saliva. 2003, 10, 286–92. [CrossRef]
- Feng, P.; Tong, C.; Li, Y.; Liu, L.J.A.R. LncRNA HOTAIR: A Novel Biomarker for the Diagnosis of Asymptomatic Carotid Artery Stenosis and Prediction of the Onset of Cerebral Ischemic Events. 2024, 30, 5. [CrossRef]
- Watanabe S, Kawasaki Y, Kawai KJG, Environment. Diurnal variation of salivary oxidative stress marker 8-hydroxyguanine. 2019, 41, 1–4. [CrossRef]
- Borisenkov, M.; Erunova, L.; Lyuseva, E.; Pozdeeva, N.J.H.P. Diurnal changes in the total antioxidant activity of human saliva. 2007, 33, 375-6. [CrossRef]
- Alajbeg IZ, Lapić I, Rogić D, Vuletić L, Andabak Rogulj A, Illeš D; et al. Within-subject reliability and between-subject variability of oxidative stress markers in saliva of healthy subjects: A longitudinal pilot study. 2017, 2017, 2697464. [CrossRef]
- Kamodyová, N.; Celec, P.J.C.C.; Medicine, L. Salivary markers of oxidative stress and Salivette collection systems. 2011, 49, 1887-90.
- Dallel I, Salem IB, Merghni A, Bellalah W, Neffati F, Tobji S; et al. Influence of orthodontic appliance type on salivary parameters during treatment. 2020, 90, 532. [CrossRef]
- Teixeira, H.S.; Kaulfuss, S.M.O.; Ribeiro, J.S.; Pereira, B.d.R.; Brancher, J.A.; Camargo, E.S.J.D.P.J.o.O. Calcium, amylase, glucose, total protein concentrations, flow rate, pH and buffering capacity of saliva in patients undergoing orthodontic treatment with fixed appliances. 2012, 17, 157-61. [CrossRef]
- ANA-MĀDĀLINAR, *!!! REPLACE !!!*; Sebastian, M.; Aureliana, C.; Victoria, B. ANA-MĀDĀLINAR; Sebastian, M.; Aureliana, C.; Victoria, B. Studies regarding salivary total antioxidant activity in different types of orthodontic treatement. 2019. [CrossRef]
- Shamaa, M.S.; Mansour, M.M.J.E.D.J. Long-term assessment of the salivary oxidative stress status during orthodontic treatment with fixed appliances. 2019;65:3151-7. [CrossRef]
- Ángeles-Estrada, L.; Pérez-Soto, E.; Pérez-Vielma, N.M.; Gómez-López, M.; Sánchez-Monroy, V. Oxidative stress and genotoxicity in oral epithelial cells of subjects undergoing Fixed Orthodontic Appliances. 2023. [CrossRef]
- Yamyar, S.; Daokar, S.J.O.J.o.N. Oxidative Stress Levels in Orthodontic Patients and Efficacy of Antioxidant Supplements in Combating Its Effects-A Randomized Clinical Study. 2019, 9, 29-34.
- Pérez-Vielma, N.M.; Domínguez-Rojas, M.; Mendoza-Tapia, S.V.; Angeles-Estrada, L.; Sánchez-Monroy, V.J.R.O.M. Genotoxicity of Fixed Orthodontic Treatment. 2023, 27, 3-11. [CrossRef]
- Kovac V, Poljsak B, Perinetti G, Primozic JJBri. Systemic level of oxidative stress during orthodontic treatment with fixed appliances. 2019, 2019, 5063565. [CrossRef]
- Żukowski P, Maciejczyk M, Waszkiel DJAoOB. Sources of free radicals and oxidative stress in the oral cavity. 2018, 92, 8–17. [CrossRef]
- Kaya FA, Hamamci N, Basaran G, Dogru M, Yildirim TTJJoID, Research M. TNF-α, IL-1β AND IL-8 LEVELS IN TOOTH EARLY LEVELLING MOVEMENT ORTHODONTIC TREATMENT. 2010, 3.
- Chen, Y.; Wong, W.K.; Seneviratne, J.C.; Huang, S.; McGrath, C.; Hagg, U.J.M. Associations between salivary cytokines and periodontal and microbiological parameters in orthodontic patients. 2021, 100, e24924. [CrossRef]
- Kazan, D.; BAŞ, B.; Aksoy, A.; Atmaca, E.J.T.J.o.M.S. The evaluation of oxidative stress and inflammation markers in serum and saliva of the patients with temporomandibular disorders. 2023, 53, 1690-6. [CrossRef]
Figure 1.
Fold change value of salivary IL-1β (IL1) gene expression.
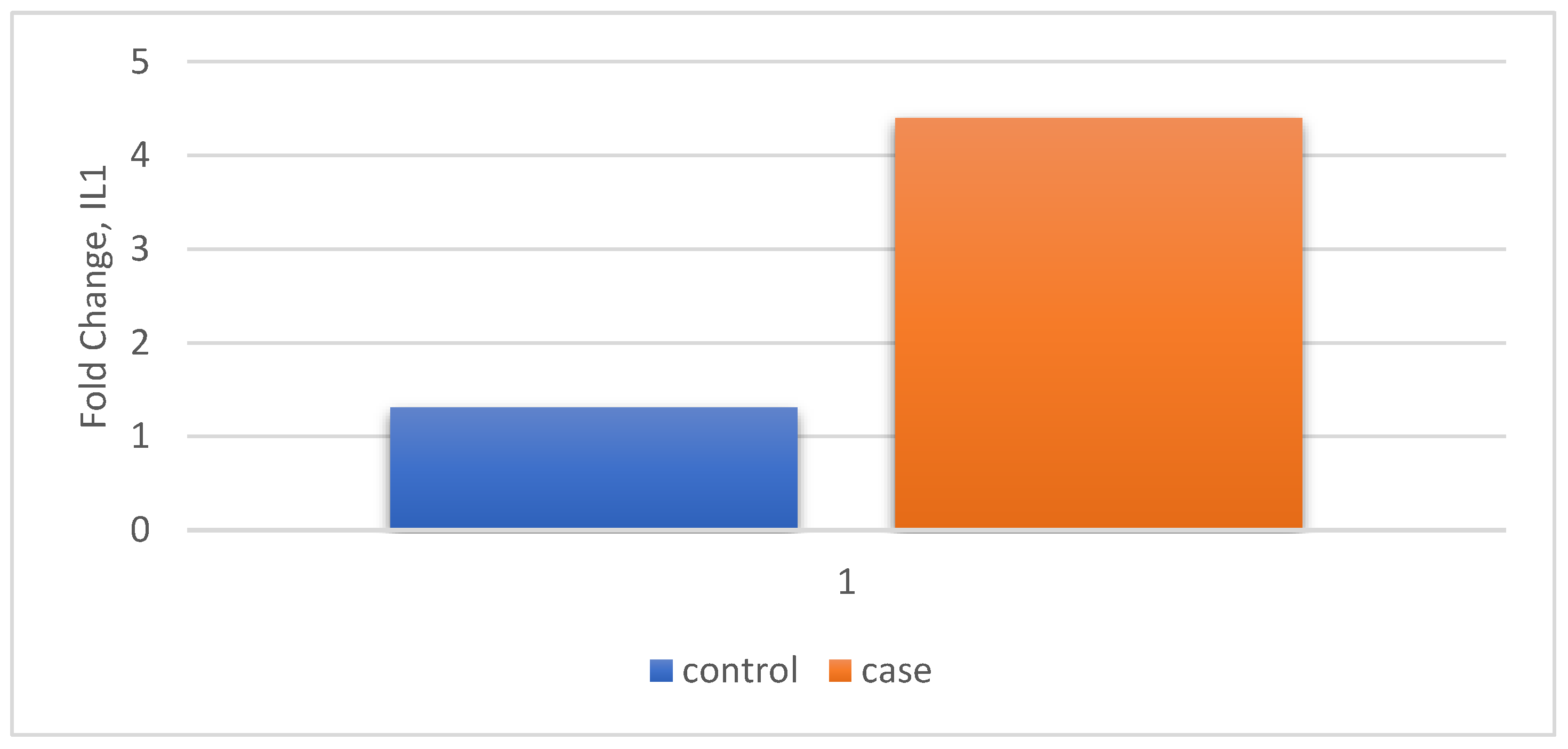
Figure 2.
Fold change value of IL-8 (IL8) gene expression in case and control.
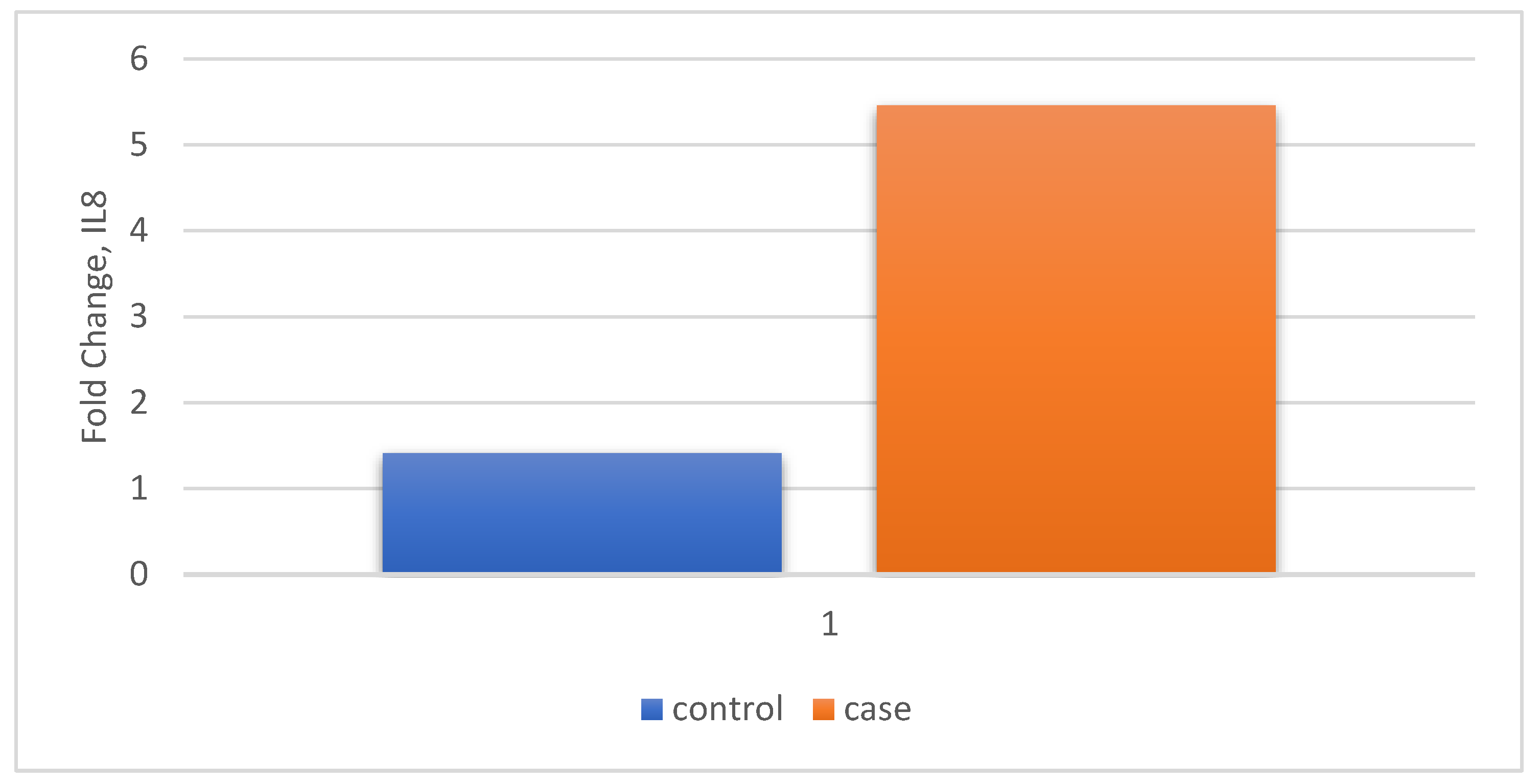
Figure 3.
Correlation between target genes.
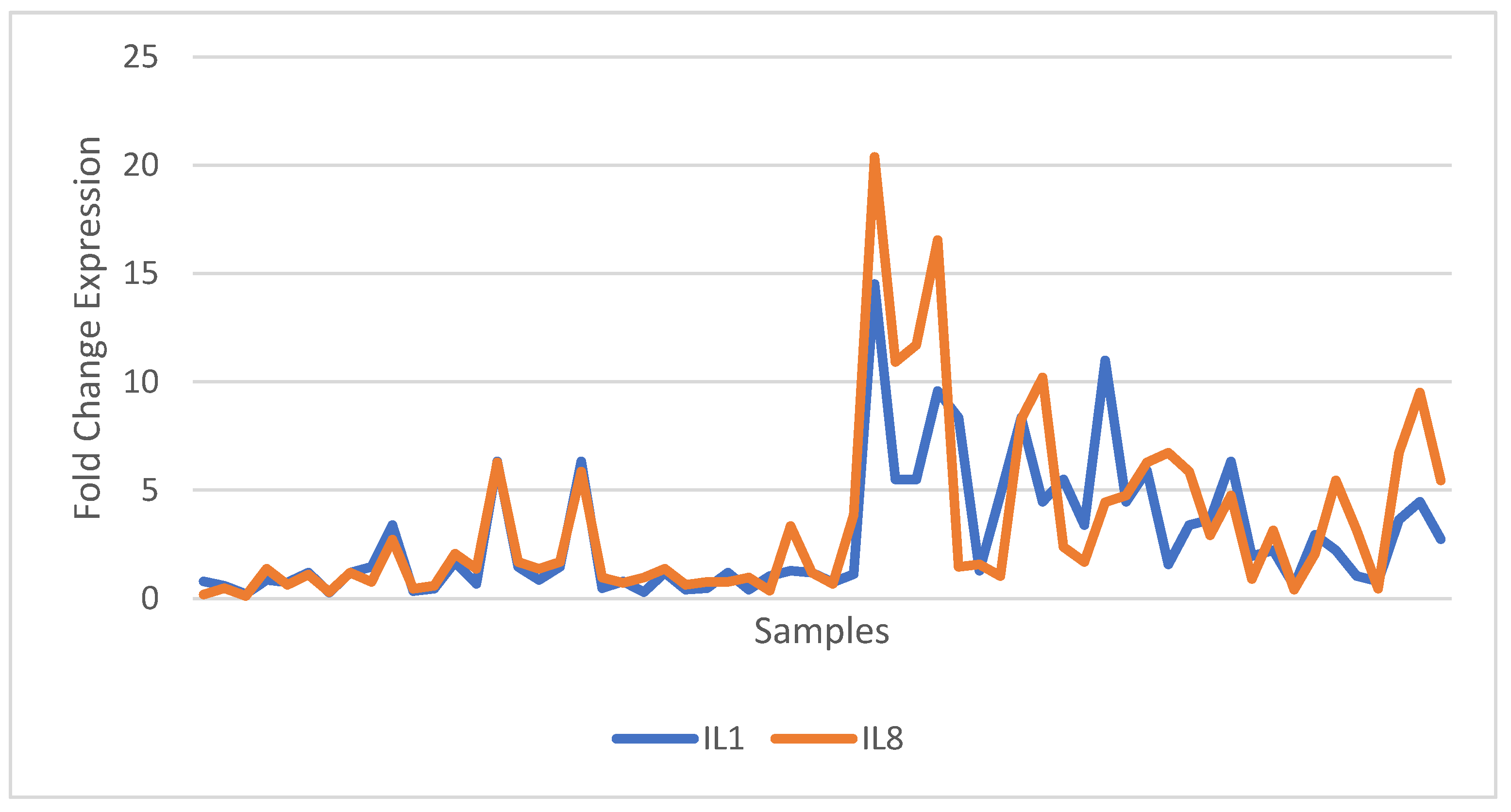
Table 4.
Fold change value of salivary IL-1β (IL1) and IL-8 (IL8).
| Relative Gene Expression | Control n=30 |
Case n=30 |
P value | |
|---|---|---|---|---|
| IL1 | Fold Change (Mean ± SD) |
1.3 (1.49) | 4.4 (3.31) | P < 0.0001 t-statistic =4.678 |
| IL8 | Fold Change (Mean ± SD) |
1.41 (1.45) | 5.45 (4.79) | P < 0.0001 t-statistic =4.421 |
Table 5.
Correlation between relative gene expression of salivary IL-1β (IL1) and IL-8 (IL8) with demographic variables and salivary biomarkers.
Table 5.
Correlation between relative gene expression of salivary IL-1β (IL1) and IL-8 (IL8) with demographic variables and salivary biomarkers.
| Variable | Relative gene expression IL1 |
Relative gene expression IL8 |
||
| r | p | r | p | |
| Age | 0.021 | 0.873 | 0.088 | 0.503 |
| Gender | 0.086 | 0.513 | 0.010 | 0.942 |
| Smoking | 0.027 | 0.838 | 0.080 | 0.544 |
| Total Protein concentration (g/dL) | 0.264 | 0.041 | 0.234 | 0.072 |
| MDA (μmol/l) | 0.575 | 0.000 | 0.479 | 0.000 |
| TAC (mmol/l) | 0.318 | 0.013 | 0.194 | 0.138 |
| 8-OHdG (ng/ml) | 0.416 | 0.001 | 0.467 | 0.000 |
| IL1 | 1.000 | - | 0.821 | 0.000 |
| IL8 | 0.821 | 0.000 | 1.000 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



