
Submitted:
10 April 2025
Posted:
16 April 2025
You are already at the latest version
Abstract
Identifying prognostic markers in colorectal cancer (CRC) is crucial for improving treatment outcomes. Although carcinoembryonic antigen (CEA) is recommended in the guidelines of the National Comprehensive Cancer Network, its sensitivity and specificity are inconsistent, limiting its utility in patients with normal CEA levels. Circulating tumor cells (CTCs), including those expressing CD133—a cancer stem cell marker involved in tumor progression and therapy resistance—are associated with metastasis and survival outcomes. This study evaluated the prognostic significance of CD133-positive CTCs, and their combined effect with CEA, in patients with CRC. Peripheral blood samples from 195 patients with CRC (stages I–IV) were analyzed. CTCs were isolated using OncoQuick tubes and CD133 mRNA expression was detected by reverse transcription polymerase chain reaction. In clinicopathological analysis, CD133-positive CTCs were detected in 27.2% of cases, correlating with serosal invasion (P=0.016). Multivariate Cox analysis showed that CD133-positive CTCs were associated with worse disease-specific survival (P=0.001). Patients with CD133-positive CTCs and CEA ≥5 ng/mL (high CEA) had a significantly poorer prognosis (P<0.001), whereas those with CD133-negative CTCs and CEA <5 ng/mL (low CEA) had a better prognosis (P=0.039). CD133 expression in CTCs, especially in combination with CEA, may serve as a valuable prognostic marker in CRC.
Keywords:
colorectal adenocarcinoma
; CD133
; cancer stem cells
; circulating tumor cells
; tumor marker
1. Introduction
Colorectal cancer (CRC) is the third most diagnosed cancer worldwide, with approximately 1.9 million new cases and 903,859 deaths annually [1]. CRC accounts for a significant proportion of cancer-related mortality, with recurrence and metastasis being the primary contributors to poor outcomes [2]. Although recent advancements in molecular targeted therapies and immunotherapies have improved survival rates, these treatments are often associated with substantial financial costs, adverse effects, and limited availability [3]. These challenges underscore the urgent need for reliable biomarkers that can predict recurrence, assess prognosis, and optimize treatment strategies. Carcinoembryonic antigen (CEA) is one of the most widely used tumor markers in CRC, and is recommended in the guidelines of the National Comprehensive Cancer Network (NCCN) for prognostic assessment and disease monitoring [4,5,6,7,8,9]. Elevated preoperative CEA levels have been consistently associated with poor prognosis and an increased risk of recurrence. Despite its utility, the clinical application of CEA levels is limited by inconsistent cutoff values, sensitivity, and specificity, which result in false positives and negatives in certain patient populations [10,11,12,13]. This variability highlights the need for novel biomarkers that can complement or surpass the prognostic accuracy of CEA. Metastasis, the leading cause of CRC-related mortality, is a complex process involving multiple steps, including tumor cell detachment, intravasation into the bloodstream, survival as circulating tumor cells (CTCs), and colonization of distant organs [14]. Elevated CTC counts have been associated with worse progression-free survival (PFS) and overall survival (OS) in patients with CRC, suggesting their potential as independent prognostic markers [15,16,17]. Furthermore, dynamic changes in CTC counts during treatment have been proposed as early indicators of therapeutic efficacy, particularly in metastatic CRC [18]. However, the clinical utility of CTC enumeration is limited by the phenomenon of “metastatic inefficiency,” wherein only a small fraction of CTCs possess the capacity to form metastatic lesions [19]. Understanding the biological properties of these rare, metastasis-competent CTCs is critical for improving prognostic and therapeutic strategies. Emerging evidence suggests that a subpopulation of CTCs, with cancer stem cell (CSC)-like properties, play a pivotal role in metastasis, recurrence, and resistance to therapy [20,21,22]. CSCs are a small subset of tumor cells, and possess stem cell-like features that include self-renewal, differentiation, and enhanced resistance to conventional therapies. In CRC, several CSC-specific markers, such as leucine-rich repeat-containing G-protein-coupled receptor 5 (LGR5), CD44, and CD133, have been identified as indicators of tumor aggressiveness and poor clinical outcomes [23,24,25]. Among these, CD133 has emerged as one of the most promising markers due to its association with tumorigenicity, chemoresistance, and metastatic potential [26]. CD133, also known as Prominin-1, is a transmembrane glycoprotein predominantly expressed on the apical membrane protrusions of embryonic epithelial cells and various stem-like cancer cells [21,27]. CD133-positive CRC cells exhibit enhanced self-renewal, invasive capacity, and chemoresistance compared to CD133-negative CRC cells [28,29,30]. These properties are mediated through the activation of critical signaling pathways, such as Wnt, Notch, and Hedgehog, which are essential for maintaining CSC characteristics and promoting tumor progression [28,29,30]. Additionally, under hypoxic conditions, CD133 expression has been linked to the upregulation of hypoxia-inducible factor-1α (HIF-1α) and epithelial-mesenchymal transition (EMT) markers, such as N-cadherin and vimentin, facilitating metastatic dissemination [31,32]. Clinical studies have consistently reported that high CD133 expression in primary CRC tumors is associated with advanced disease stages, increased recurrence rates, and poor survival outcomes [33,34,35]. However, the prognostic role of CD133 expression in CTCs is underexplored. While CTC enumeration has demonstrated potential as a prognostic tool, integrating CD133 expression in CTCs with established markers like CEA may provide a more comprehensive understanding of disease progression and patient prognosis. To date, no studies have investigated the synergistic prognostic value of CD133 expression in CTCs and CEA levels in patients with CRC.
In this study, we aimed to evaluate the prognostic significance of CD133 expression in CTCs for disease-specific survival (DSS) in patients with CRC. Secondary objectives included assessing the combined utility of CD133 expression in CTCs and CEA levels for prognostic evaluation, and exploring the associations between CD133-positive CTCs and clinicopathological factors, such as tumor stage, grade, and metastatic potential. By addressing these gaps, this study aims to provide novel insights into the biology of CSCs in CRC and highlight the potential of CD133-positive CTCs as a robust biomarker for improving prognostic accuracy and guiding personalized treatment strategies.
2. Materials and Methods
2.1. Patients and Sample Collection
A total of 195 patients who underwent CRC resection at our institution from 2010 to 2020 were included in the study. Patients with synchronous or metachronous cancers were excluded from the analysis. Additionally, 10 healthy donors were recruited as controls. Blood samples were drawn prior to primary tumor resection to assess preoperative CEA and CTC levels, with or without CD133 expression. The reference value for CEA was set at 5 ng/mL.
To minimize the risk of skin cell contamination, the first 5 mL of blood was discarded. Subsequently, 20 mL of blood was collected and processed using the OncoQuick density gradient system (Greiner Bio-One GmbH, Frickenhausen, Germany) following the manufacturer’s protocol. Tumor cells were then isolated through density gradient centrifugation, and resuspended in 400 μL of phosphate-buffered saline.
For the negative controls, blood from healthy volunteers, devoid of epithelial cells, was also processed using the OncoQuick system. This study was approved by the Research Ethics Committee of the University of Fukui (Approval No. 20200058). Written informed consent was obtained from all participants for the publication of this research.
2.2. Reverse Transcription-Polymerase Chain Reaction
Total RNA was extracted from tumor cells using the ISOGEN reagent (Nippon Gene, Tokyo, Japan) and reverse-transcribed into cDNA with the PrimeScript RT reagent kit (Takara Bio Inc., Otsu, Japan). The coding region of CD133 was amplified by polymerase chain reaction (PCR) using the following primers: forward primer CAGAGTACAACGCCAAACCA and reverse primer AAATCACGATGAGGGTCAGC [36]. The thermal cycling conditions were as follows: 35 cycles of denaturation at 94°C for 1 minute, annealing at 55°C for 1 minute, and extension at 72°C for 2 minutes. Amplification was conducted using a PTC-100 Programmable Thermal Controller (MJ Research Inc., Manahawkin, NJ, USA). The resulting PCR products were purified using the QIAquick PCR Purification Kit (Qiagen, Hilden, Germany) and analyzed through gel electrophoresis on a 1.2% agarose gel. The purified products were sequenced to confirm the presence of CD133. For semi-quantitative mRNA analysis, CD133 bands on the gels were visualized using ethidium bromide staining. To ensure reliability, all PCR amplifications were performed in duplicate.
2.3. Clinical Assessment
Data on patient demographics (age, sex), tumor characteristics (size, location, histological type, depth of invasion), metastasis status (lymph node and distant metastasis), cancer stage, CEA levels, and DSS were collected from patients with CRC. DSS was defined as the period from the date of CRC surgery to death due to CRC, with deaths from other causes censored at the time of occurrence. Tumor histopathology and clinical staging were determined according to the TNM classification system. All the patients underwent regular follow-up evaluations, including blood tests for tumor markers every 3 months, contrast-enhanced abdominal computed tomography every 6 months, and colonoscopy every 3 years.
2.4. Statistical Analysis
The Kaplan–Meier method was used to evaluate DSS, with group comparisons conducted using the log-rank test. The Cox regression model was utilized to calculate hazard ratios (HRs). Other characteristics between the two groups were analyzed using the chi-square test for categorical variables and logistic regression for multivariate analysis. All statistical analyses were conducted using IBM SPSS Statistics software version 21.0 (IBM Japan, Ltd., Tokyo, Japan). Statistical significance was defined as P < 0.05.
3. Results
3.1. Associations between CD133 Expression and Clinicopathologic Features
The baseline demographic and clinicopathologic data of all the patients with CRC are summarized in Table 1. The median age was 71 years (range: 38–91 years). Of the 195 total patients, 44, 64, 54, and 33 were classified as stages I, II, III, and IV, respectively. CD133-positive CTCs were detected in 53 of the 195 cases (27.2%; Figure 1), whereas none of the healthy donors had CD133-positive CTCs. In analysis stratified by stage, CD133-positive CTCs were detected in 5 stage I, 25 stage II, 17 stage III, and 6 stage IV CRC cases. Univariate analysis revealed no correlations between CD133-positive CTCs and tumor size, histological type, lymph node metastasis, distant metastasis, or stage. However, a significant positive correlation was observed between CD133-positive CTCs and serosal involvement. No association was found between serum CEA levels and CD133 expression (Table 1). Multivariate logistic regression analysis showed that CD133-positive CTCs were significantly associated with serosal involvement (odds ratio [OR] = 3.000, 95% confidence interval [CI] = 1.225–7.345, P = 0.016). However, no significant relationship was observed with other pathological characteristics (Table 2).
3.2. Association between CD133 Expression in CTCs and Survival Rate
The median observation period for the 195 patients was 44.9 months, during which 31 patients died of the primary disease. The 5-year DSS rate for CD133-positive cases in stages I–III was 85.3%, whereas it was 95.0% for CD133-negative cases (Figure 2). This indicates that CD133-positive cases had a significantly poorer prognosis (P = 0.018). In the analysis for each stage, however, no significant relationship was observed between CD133 expression and the 5-year DSS rate in stages I and II, nor between CD133 expression and the 2-year DSS rate in stage IV (P = 0.128, 0.721, and 0.275, respectively) (Figures S1a, S1b, and S1c). In stage III CRC cases, the 5-year DSS rate was 73.8% for CD133-positive cases and 96.3% for CD133-negative cases, indicating that CD133-positive cases had a significantly poorer prognosis (P = 0.021; Figure S1d).
3.3. Multivariate Cox Analysis for DSS, Incorporating CD133 Expression
Table 3 presents the results of the multivariate Cox analysis evaluating age, sex, distant metastasis, and CD133 expression in all the patients. The analysis revealed significant associations between DSS and both distant metastasis and CD133 expression (both P < 0.05).
3.4. Association between CEA Levels and Survival Rates
A total of 70 cases with CEA ≥ 5 ng/mL (high CEA) were identified, including 7, 23, 19, and 21 cases in stages I, II, III, and IV, respectively. The 5-year survival rate for stage I–III cases with high CEA levels was 76.1%, whereas those for cases with CEA < 5 ng/mL (low CEA) was 98.5%, indicating a significantly poorer prognosis for cases with high CEA levels (P < 0.001; Figure 3). Correlation analysis revealed no significant associations between CEA levels and the 5-year DSS rate in stage I patients or the 2-year DSS rate in stage IV patients (P = 0.270 and 0.488, respectively) (Figures S2a and S2b). However, for stage II cases, the 5-year DSS rate was 78.4% for those with high CEA levels and 100% for those with low CEA levels (Figure S2c). Similarly, the 5-year DSS rate for stage III patients with CRC and high CEA levels was 72.8%, whereas it was 100% for those with low CEA levels (Figure S2d). These results indicate that elevated CEA levels are a poorer prognostic factor for stage II and III cases (P = 0.033 and 0.005, respectively).
3.5. Multivariate Cox Analysis for DSS, Incorporating CEA Levels
Table 4 presents the results of the multivariate Cox analysis evaluating age, sex, distant metastasis, and CEA levels for DSS in all patients. The analysis revealed significant associations between DSS and both distant metastasis and elevated CEA levels (both P < 0.05).
3.6. Impact of Combined CD133 Expression and CEA Levels on DSS in Stage I–III Cases
Among the patients, 83 cases had CD133-negative CTCs with low CEA levels, 32 had CD133-negative CTCs with high CEA levels, 30 had CD133-positive CTCs with low CEA levels, and 17 had CD133-positive CTCs and high CEA levels. The 5-year survival rates for these groups were 100%, 80.0%, 94.4%, and 68.0%, respectively. The differences were significant (P < 0.001; Figure 4).
3.7. Comparison of DSS between Cases with CD133-Positive CTCs and High CEA Levels and Other Cases
CD133-positive CTCs and high CEA levels were observed in 0 of 44 stage I cases, 11 of 64 stage II cases, 6 of 54 stage III cases, and 3 of 33 stage IV cases. A comparison of 5-year survival rates across all the CRC stages revealed that cases with CD133-positive CTCs and high CEA levels had worse 5-year DSS than did other cases (60.4% vs. 80.7%, P = 0.014; Figure 5). No significant difference was observed in 5-year DSS between cases with CD133-positive CTCs and high CEA levels and other stage II cases (88.9% vs. 94.7%, P = 0.127) (Figure S3a). However, stage III cases with CD133-positive CTCs and high CEA levels showed a significantly worse 5-year DSS (40.0% vs. 96.8%, P < 0.001) (Figure S3b). Cox regression analysis revealed that distant metastasis and CD133-positive CTCs with high CEA levels were significantly associated with poorer prognosis (P < 0.001 for both; Table 5).
3.8. Comparison of DSS between Cases with CD133-Negative CTCs and Low CEA, and Other Cases
CD133-negative CTCs with low CEA levels were observed in 32 of 44 stage I cases, 27 of 64 stage II cases, 24 of 54 stage III cases, and 9 of 33 stage IV cases. A comparison of 5-year survival rates across all the CRC stages revealed that cases with CD133-negative CTCs and low CEA levels had better 5-year DSS than did other cases (91.1% vs. 66.9%, P < 0.001; Figure 6). A significantly better 5-year DSS was observed in stage I and III cases with CD133-negative CTCs and low CEA levels than in other cases (100% vs. 77.8%, P = 0.042, and 100% vs. 80.5%, P = 0.043, respectively; Figure S4a, S4b). In contrast, the 5-year DSS for stage II cases and the 2-year DSS for stage IV cases with CD133-negative CTCs and low CEA levels did not differ significantly from those of other cases (100% vs. 87.9%, P = 0.201, and 88.9% vs. 60.7%, P = 0.129, respectively; Figure S4c, S4d). Cox regression analysis revealed that the absence of distant metastasis and presence of CD133-negative CTCs with low CEA levels were significantly associated with a better prognosis (P = 0.039 in all cases; Table 6).
4. Discussion
In this study, we investigated the association between CD133 mRNA expression in CTCs and the prognosis of CRC. Our results revealed that patients with CD133-positive CTCs had a significantly poorer prognosis. Furthermore, cases with CD133-negative CTCs and low CEA levels showed a significantly better prognosis compared to that of other cases. In contrast, patients with CD133-positive CTCs and high CEA levels exhibited significantly poorer prognosis. Additionally, the prevalence of CD133-positive CTCs was significantly higher in cases with serosal invasion, suggesting their potential role in tumor infiltration. CTCs are cancer cells that detach from the primary tumor and enter the bloodstream [37]. Previous studies have reported that higher CTC counts are associated with poorer prognosis [15,16,17]. However, only approximately one in 10,000 CTCs is estimated to be capable of initiating metastasis. This phenomenon, termed “metastatic inefficiency,” indicates that while CTCs are necessary for metastasis, they are not sufficient for metastatic progression [19]. Furthermore, CSCs constitute a subset of the CTCs [38,39,40,41]. CSCs possess the capacity for self-renewal and play a crucial role in tumor initiation and progression. They are also implicated in chemoresistance and can differentiate into most tumor cells, which lack tumorigenic potential [42,43,44]. Chun et al. reported that among patients with breast cancer, cases with high expression of CSC markers, including CD133 in CTCs, exhibited poor treatment response and worse OS and PFS [45]. Similarly, Yang et al. demonstrated that among patients with metastatic castration-sensitive prostate cancer, CD133 expression in CTCs was associated with poorer PFS [46]. We have previously reported that among patients with CRC, the expression of CD44 variant exon 9 (CD44v9), a known CSC marker, in CTCs serves as a reliable prognostic marker for poor outcomes [47]. CD133 is considered a prominent CSC marker in CRC, but its functional role remains unclear. It has been reported that CD133-positive cancer cells exhibit a higher proliferative capacity than do CD133-negative cancer cells [28]. Furthermore, CD133 has been implicated in hypoxic adaptation, EMT, and mesenchymal-epithelial transition, which are crucial for cancer metastasis, and in the suppression of apoptosis.
As solid tumors grow, they experience insufficient blood supply, leading to a hypoxic environment. To adapt to this condition, tumors undergo angiogenesis and disseminate through the bloodstream to more favorable environments [48]. A central factor in this process is HIF-1α [32]. HIF-1α not only promotes angiogenesis and cell proliferation but also enhances cancer cell survival and migration, ultimately accelerating tumor invasion and metastasis [49]. Okada et al. reported that in CRC, CD133-positive cells exhibit significantly higher HIF-1α expression under hypoxic conditions than do CD133-negative cells [31]. Consequently, hypoxia is thought to promote EMT in CD133-positive cells. Additionally, in CD133-positive cells, E-cadherin expression, which is downregulated during EMT, has been shown to return to baseline levels within 24 hours upon reoxygenation, leading to mesenchymal-epithelial transition and subsequent metastatic formation [31].
Moreover, HIF-1α is known to activate autophagy in CD133-positive cells [50,51]. Autophagy plays a critical role in maintaining cellular homeostasis by removing damaged organelles and proteins, thus preventing stress-induced apoptosis. Additionally, by recycling intracellular components, autophagy supplies nutrients and energy, enabling CD133-positive cells to survive in nutrient-deprived conditions. CD133-positive cells are also known to secrete interleukin-4, an immunomodulatory factor that further suppresses apoptosis [52]. These findings suggest that CD133-positive CSCs may serve as a prognostic marker of poor outcomes in CRC. In studies examining CD133 expression in primary CRC tissues, using immunohistochemistry to assess its association with OS, Kojima et al. analyzed 160 patients with stage I–IV CRC and reported that CD133 expression was associated with poor prognosis [53]. Similarly, Jao et al. conducted a study with 233 patients and reported that CD133 expression was associated with poorer prognosis [54]. Additionally, meta-analyses conducted by Chen and Wang reported similar findings [34,35]. Conversely, Choi et al., in a study of 523 cases, found no significant association between CD133 expression in primary CRC tissues and OS. Regarding CD133-positive CTCs and prognosis, Pilati et al. analyzed 50 CRC cases with liver metastases and reported that CD133-positive cases had a poorer prognosis than did CD133-negative cases [55]. Similarly, Lin et al. investigated 100 patients with CRC and found that CD133-positive CTCs were a reliable predictor of recurrence and were associated with a shorter median OS [56]. However, Iinuma et al., in a study of 735 CRC cases, reported that CD133-positive CTCs alone were not significantly associated with OS [11].
The discrepancies in these findings may be due to differences in patient cohorts, study designs, CTC isolation methods, evaluation techniques, and cutoff values used in the analyses. Moreover, Zhou et al. reported that CTCs can be classified into epithelial and mesenchymal CTCs, and that in CRC patients with elevated levels of CD133-positive mesenchymal CTCs were more prone to distant metastases and exhibited poorer PFS [57]. These findings suggest that the proportion of mesenchymal CTCs may also influence prognosis. Despite these variations, all reports indicate that CD133-positive CTCs are associated with prognosis to some extent. In our study, using the OncoQuick density gradient system to analyze 195 cases, we demonstrated a strong association between CD133-positive CTCs and prognosis. Furthermore, Ren et al. reported that CD133-positive CTCs were a particularly reliable prognostic marker in middle-stage CRC. Consistent with this, our study also found a significant association between CD133-positive CTCs and prognosis in stage III cases (Figure S1d).
CEA is recommended as a tumor marker for CRC in the NCCN guidelines [4,5,6,7,8,9]. Elevated CEA levels have been reported to be associated with poor prognosis [58]. Chu et al. demonstrated that the combination of CTC count and CEA levels serves as a reliable prognostic indicator. Specifically, cases with high CTC counts (≥4 CTCs per 2 mL of blood) and high CEA levels were associated with poor prognosis [59]. In our study, CEA levels were confirmed to be a reliable prognostic marker. However, there was no significant association between CEA levels and CD133 expression in CTCs, suggesting that they are independent prognostic factors. We further investigated the prognostic value of combining these independent predictors. Patients with both CD133-positive CTCs and high CEA levels had significantly poorer prognoses than did those without these factors. The HR for DSS was higher when both CD133-positive CTCs and high CEA levels were considered together than when either factor was considered alone, suggesting that their combination enhances prognostic accuracy. Conversely, patients with CD133-negative CTCs and low CEA levels exhibited favorable prognoses. Since there are limited reports on favorable prognostic factors, this finding may have implications for the selection of candidates for adjuvant chemotherapy. Several studies have reported that the combination of CD133-positive CTCs with other prognostic markers improves prognostic accuracy. Zahran et al. reported that patients with both CD133-positive and CD44-positive CTCs had significantly poorer OS [60]. Similarly, Iinuma et al. demonstrated that the combination of CEA, cytokeratin, and CD133 was a reliable prognostic marker for poor outcomes in Dukes’ stage B and C CRC cases [11]. Additionally, in patients with CRC and liver metastases, concurrent positivity for CD133, CD44, and CD54 was associated with poorer prognosis [61]. In our analysis of clinicopathological factors in primary CRC tumors, we found that CD133-positive CTCs were significantly associated with serosal involvement. Since CD133-positive cells are believed to originate exclusively from CD133-positive tumor cells, the presence of CD133-positive CTCs likely reflects CD133 expression in the primary tumor [28]. Numerous studies have reported that CD133 positivity in primary CRC is associated with tumor depth [21,34,62,63,64,65]. In vitro [66] and in vivo [67] studies have shown that CD133-positive CRC cells exhibit greater invasiveness than do CD133-negative cells. Chao et al. further demonstrated that CD133-positive CRC cells enhance their interaction with surrounding fibroblasts, which may contribute to their increased invasiveness relative to CD133-negative cells [30].
However, no significant correlation was found between distant metastasis and CD133-positive CTCs. Okada et al. highlighted differences in CD133 expression based on the metastatic site. They reported that CD133 expression levels in liver metastases were significantly higher than those in the corresponding primary tumors, whereas CD133 expression levels in peritoneal metastases were significantly lower than those in primary tumors [31]. Liver metastases are thought to occur because of the high EMT capacity of CD133-positive cells under hypoxic conditions. In contrast, peritoneal metastases are believed to result from the high expression of β1-integrin in CD133-negative cells [67]. Similarly, Gao et al. reported that different stem cell markers are involved in liver and lung metastases of CRC, indicating that chemoattraction and adhesion mechanisms differ according to the metastatic organ [68]. This study has several limitations. First, in stage II and III cases, the number of deaths was low, which limited the feasibility of multivariate analysis to evaluate the impact of CD133-positive CTCs on prognosis in these cases. However, in univariate analysis for stage III cases, CD133-positive CTCs appeared to be a potential risk factor for poor prognosis. Second, in this study, the assessment of CD133 expression in the blood relied solely on its presence or absence, without considering expression intensity. This may have contributed to discrepancies between our results and those of previous reports. Nonetheless, many studies have reported associations between CD133 expression and prognosis in various contexts, which aligns with our findings.
5. Conclusions
Our study confirmed that CD133 expression in CTCs is a reliable prognostic marker in CRC. Furthermore, combining CD133 expression in CTCs with the established tumor marker CEA effectively stratified patients into groups with favorable and unfavorable prognoses. This approach may aid treatment decisions, including the selection of candidates for postoperative adjuvant chemotherapy.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Formal analysis, K.S. and Y.K.; Investigation, K.S.; Data curation, K.S.; Writing—original draft, K.S.; Supervision, K.K.; Project administration, T.G. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare that this study received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Research Ethics Committee of the University of Fukui (approval No. 20200058 and approval date 1 April 2017).
Informed Consent Statement
Written informed consent was obtained from participants prior to the study.
Data Availability Statement
All data included in this study are available upon request from the corresponding author.
Acknowledgments
The authors thank Masae Saitoh for assistance in patient data collection and administrative support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Iinuma, H.; Watanabe, T.; Mimori, K.; Adachi, M.; Hayashi, N.; Tamura, J.; Matsuda, K.; Fukushima, R.; Okinaga, K.; Sasako, M.; et al. Clinical significance of circulating tumor cells, including cancer stem-like cells, in peripheral blood for recurrence and prognosis in patients with dukes’ stage b and c colorectal cancer. J. Clin. Oncol. 2011, 29, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; van Dalen, A.; Haglund, C.; Hansson, L.; Holinski-Feder, E.; Klapdor, R.; Lamerz, R.; Peltomaki, P.; Sturgeon, C.; Topolcan, O. Tumour markers in colorectal cancer: European group on tumour markers (egtm) guidelines for clinical use. Eur. J. Cancer 2007, 43, 1348–1360. [Google Scholar] [CrossRef]
- Locker, G.Y.; Hamilton, S.; Harris, J.; Jessup, J.M.; Kemeny, N.; Macdonald, J.S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C. Asco 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J. Clin. Oncol. 2006, 24, 5313–5327. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon cancer, version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Ward, U.; Primrose, J.N.; Finan, P.J.; Perren, T.J.; Selby, P.; Purves, D.A.; Cooper, E.H. The use of tumour markers cea, ca-195 and ca-242 in evaluating the response to chemotherapy in patients with advanced colorectal cancer. Br. J. Cancer 1993, 67, 1132–1135. [Google Scholar] [CrossRef]
- Preketes, A.P.; King, J.; Caplehorn, J.R.M.; Clingan, P.R.; Ross, W.B.; Morris, D.L. Cea reduction after cryotherapy for liver metastases from colon-cancer predicts survival. Aust. N. Z. J. Surg. 1994, 64, 612–614. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the united states, National Cancer Institute of canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef]
- Kim, G.; Jung, E.J.; Ryu, C.G.; Hwang, D.Y. Usefulness of carcinoembryonic antigen for monitoring tumor progression during palliative chemotherapy in metastatic colorectal cancer. Yonsei Med. J. 2013, 54, 116–122. [Google Scholar] [CrossRef]
- Hisae Iinuma, T.W.; Mimori, K.; Adachi, M.; Hayashi, N.; Tamura, J.; Matsuda, R.F.K.; Okinaga, K.; Sasako, M.; Mori, M. Clinical Significance of Circulating Tumor Cells, Including Cancer Stem-Like Cells, in Peripheral Blood for Recurrence and Prognosis in Patients with Dukes’ Stage b and c Colorectal Cancer.
- Kim, I.H.; Lee, J.E.; Yang, J.H.; Jeong, J.W.; Ro, S.; Oh, S.T.; Kim, J.G.; Choi, M.H.; Lee, M.A. Clinical significance of discordance between carcinoembryonic antigen levels and recist in metastatic colorectal cancer. Cancer Res. Treat. 2018, 50, 283–292. [Google Scholar] [CrossRef]
- de Haas, R.J.; Wicherts, D.A.; Flores, E.; Ducreux, M.; Lévi, F.; Paule, B.; Azoulay, D.; Castaing, D.; Lemoine, A.; Adam, R. Tumor marker evolution: Comparison with imaging for assessment of response to chemotherapy in patients with colorectal liver metastases. Ann. Surg. Oncol. 2010, 17, 1010–1023. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol. 2019, 16, 409–424. [Google Scholar] [CrossRef]
- Aggarwal, C. Relationship among circulating tumor cells, cea and overall survival in patients with metastatic colorectal cancer. Ann. Oncol. 2013, 24, 2708–2710. [Google Scholar] [CrossRef] [PubMed]
- Bork, U.; Rahbari, N.N.; Schölch, S.; Reissfelder, C.; Kahlert, C.; Büchler, M.W.; Weitz, J.; Koch, M. Circulating tumour cells and outcome in non-metastatic colorectal cancer: A prospective study. Br. J. Cancer 2015, 112, 1306–1313. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Punt, C.J.A.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.A.; Mitchell, E.; Miller, M.C.; et al. Prognostic significance of circulating tumor cells in patients with metastatic colorectal cancer. Ann. Oncol. 2009, 20, 1223–1229. [Google Scholar] [CrossRef]
- Netterberg, I.; Karlsson, M.O.; Terstappen, L.W.M.M.; Koopman, M.; Punt, C.J.A.; Friberg, L.E. Comparing circulating tumor cell counts with dynamic tumor size changes as predictor of overall survival: A quantitative modeling framework. Clin. Cancer Res. 2020, 26, 4892–4900. [Google Scholar] [CrossRef]
- Weiss, L. Metastatic inefficiency. Adv. Cancer Res. 1990, 54, 159–211. [Google Scholar] [CrossRef]
- Sipos, F.; Műzes, G. Interconnection of CD133 stem cell marker with autophagy and apoptosis in colorectal cancer. Int. J. Mol. Sci. 2024, 25, 11201. [Google Scholar] [CrossRef]
- Zhou, F.; Mu, Y.D.; Liang, J.; Liu, Z.X.; Chen, H.S.; Zhang, J.F. Expression and prognostic value of tumor stem cell markers aldh1 and CD133 in colorectal carcinoma. Oncol. Lett. 2014, 7, 507–512. [Google Scholar] [CrossRef]
- Abdul Khalek, F.J.; Gallicano, G.I.; Mishra, L. Colon cancer stem cells. Gastrointest. Cancer Res. 2010, (Supplement 1), S16–23. [Google Scholar]
- Dalerba, P.; Dylla, S.J.; Park, I.K.; Liu, R.; Wang, X.H.; Cho, R.W.; Hoey, T.; Gurney, A.; Huang, E.H.; Simeone, D.M.; et al. Phenotypic characterization of human colorectal cancer stem cells. Proc. Natl. Acad. Sci. U S A 2007, 104, 10158–10163. [Google Scholar] [CrossRef]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Barker, N.; Ridgway, R.A.; van Es, J.H.; van de Wetering, M.; Begthel, H.; van den Born, M.; Danenberg, E.; Clarke, A.R.; Sansom, O.J.; Clevers, H. Crypt stem cells as the cells-of-origin of intestinal cancer. Nature 2009, 457, 608–611-U119. [Google Scholar] [CrossRef]
- Kazama, S.; Kishikawa, J.; Kiyomatsu, T.; Kawai, K.; Nozawa, H.; Ishihara, S.; Watanabe, T. Expression of the stem cell marker CD133 is related to tumor development in colorectal carcinogenesis. Asian J. Surg. 2018, 41, 274–278. [Google Scholar] [CrossRef]
- Corbeil, D.; Röper, K.; Hellwig, A.; Tavian, M.; Miraglia, S.; Watt, S.M.; Simmons, P.J.; Peault, B.; Buck, D.W.; Huttner, W.B. The human ac133 hematopoietic stem cell antigen is also expressed in epithelial cells and targeted to plasma membrane protrusions. J. Biol. Chem. 2000, 275, 5512–5520. [Google Scholar] [CrossRef]
- Ren, F.; Sheng, W.Q.; Du, X. CD133: A cancer stem cells marker, is used in colorectal cancers. World J. Gastroenterol. 2013, 19, 2603–2611. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Ohuchida, K.; Mizumoto, K.; Moriyama, T.; Onimaru, M.; Nakata, K.; Nabae, T.; Ueki, T.; Sato, N.; Tominaga, Y.; et al. Prospectively isolated cancer-associated CD10(+) fibroblasts have stronger interactions with CD133(+) colon cancer cells than with CD133(-) cancer cells. PLoS ONE 2010, 5, e12121. [Google Scholar] [CrossRef]
- Chao, C.; Carmical, J.R.; Ives, K.L.; Wood, T.G.; Aronson, J.F.; Gomez, G.A.; Djukom, C.D.; Hellmich, M.R. CD133+ colon cancer cells are more interactive with the tumor microenvironment than CD133- cells. Lab. Invest. 2012, 92, 420–436. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Kawai, K.; Sonoda, H.; Shiratori, H.; Kishikawa, J.; Nagata, H.; Nozawa, H.; Sasaki, K.; Kaneko, M.; Murono, K.; et al. Epithelial-mesenchymal transition and metastatic ability of CD133+ colorectal cancer stem-like cells under hypoxia. Oncol. Lett. 2021, 21, 19. [Google Scholar] [CrossRef]
- Semenza, G.L.; Wang, G.L. A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Mol. Cell Biol. 1992, 12, 5447–5454. [Google Scholar] [CrossRef]
- Huang, R.; Mo, D.; Wu, J.; Ai, H.; Lu, Y. CD133 expression correlates with clinicopathologic features and poor prognosis of colorectal cancer patients an updated meta-analysis of 37 studies. Medicine 2018, 97, e10446. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Song, X.; Chen, Z.; Li, X.; Li, M.; Liu, H.; Li, J. CD133 expression and the prognosis of colorectal cancer: A systematic review and meta-analysis. PLoS ONE 2013, 8, e56380. [Google Scholar] [CrossRef]
- Wang, K.; Xu, J.; Zhang, J.; Huang, J. Prognostic role of CD133 expression in colorectal cancer: A meta-analysis. BMC Cancer 2012, 12, 573. [Google Scholar] [CrossRef]
- Akbari, M.; Shanehbandi, D.; Asadi, M.; Shomali, N.; Faraji, A.; Khaze, V.; Pakdel, A.; Mokhtarzadeh, A.; Ebrahimi, A.A.; Shabani, A.; et al. Effects of CD133 silencing on survival and migration of ht-29 colorectal cancer cells. Iran. J. Immunol. 2019, 16, 246–257. [Google Scholar] [CrossRef]
- Masuda, T.; Hayashi, N.; Iguchi, T.; Ito, S.; Eguchi, H.; Mimori, K. Clinical and biological significance of circulating tumor cells in cancer. Mol. Oncol. 2016, 10, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Mocellin, S.; Del Fiore, P.; Guarnieri, L.; Scalerta, R.; Foletto, M.; Chiarion, V.; Pilati, P.; Nitti, D.; Lise, M.; Rossi, C.R. Molecular detection of circulating tumor cells is an independent prognostic factor in patients with high-risk cutaneous melanoma. Int. J. Cancer 2004, 111, 741–745. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative pcr and the 2(-delta c(t)) method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer New York: New York, NY, 2000. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Siskind, V. Quantification of completeness of follow-up. In Lancet 2002, 360, 724. [Google Scholar] [CrossRef]
- Harel, O.; Zhou, X.H. Multiple imputation: Review of theory, implementation and software. Stat. Med. 2007, 26, 3057–3077. [Google Scholar] [CrossRef] [PubMed]
- Hebbar, M.; Pruvot, F.R.; Romano, O.; Triboulet, J.P.; de Gramont, A. Integration of neoadjuvant and adjuvant chemotherapy in patients with resectable liver metastases from colorectal cancer. Cancer Treat. Rev. 2009, 35, 668–675. [Google Scholar] [CrossRef]
- Lee, C.H.; Hsieh, J.C.H.; Wu, T.M.H.; Yeh, T.S.; Wang, H.M.; Lin, Y.C.; Chen, J.S.; Lee, C.L.; Huang, W.K.; Hung, T.M.; et al. Baseline circulating stem-like cells predict survival in patients with metastatic breast cancer. BMC Cancer 2019, 19, 1167. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, Z.; Wang, Q.; Chang, K.; Zhang, J.; Ye, D.; Kong, Y.; Dai, B. Presence of CD133-positive circulating tumor cells predicts worse progression-free survival in patients with metastatic castration-sensitive prostate cancer. Int. J. Urol. 2022, 29, 383–389. [Google Scholar] [CrossRef]
- Sawai, K.; Goi, T.; Kimura, Y.; Koneri, K. Presence of cd44v9-expressing cancer stem cells in circulating tumor cells and effects of carcinoembryonic antigen levels on the prognosis of colorectal cancer. Cancers 2024, 16, 1556. [Google Scholar] [CrossRef]
- Pennacchietti, S.; Michieli, P.; Galluzzo, M.; Mazzone, M.; Giordano, S.; Comoglio, P.M. Hypoxia promotes invasive growth by transcriptional activation of the met protooncogene. Cancer Cell 2003, 3, 347–361. [Google Scholar] [CrossRef]
- Semenza, G.L. Targeting hif-1 for cancer therapy. Nat. Rev. Cancer 2003, 3, 721–732. [Google Scholar] [CrossRef]
- Petrova, V.; Annicchiarico-Petruzzelli, M.; Melino, G.; Amelio, I. The hypoxic tumour microenvironment. Oncogenesis 2018, 7, 10. [Google Scholar] [CrossRef]
- Yun, Z.; Lin, Q. Hypoxia and regulation of cancer cell stemness. Adv. Exp. Med. Biol. 2014, 772, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.L.; Oshi, M.; Endo, I.; Takabe, K. Clinical relevance of stem cell surface markers CD133, CD24, and CD44 in colorectal cancer. Am. J. Cancer Res. 2021, 11, 5141–5154. [Google Scholar] [PubMed]
- Kojima, M.; Ishii, G.; Atsumi, N.; Fujii, S.; Saito, N.; Ochiai, A. Immunohistochemical detection of CD133 expression in colorectal cancer: A clinicopathological study. Cancer Sci. 2008, 99, 1578–1583. [Google Scholar] [CrossRef]
- Jao, S.W.; Chen, S.F.; Lin, Y.S.; Chang, Y.C.; Lee, T.Y.; Wu, C.C.; Jin, J.S.; Nieh, S. Cytoplasmic CD133 expression is a reliable prognostic indicator of tumor regression after neoadjuvant concurrent chemoradiotherapy in patients with rectal cancer. Ann. Surg. Oncol. 2012, 19, 3432–3440. [Google Scholar] [CrossRef]
- Pilati, P.; Mocellin, S.; Bertazza, L.; Galdi, F.; Briarava, M.; Mammano, E.; Tessari, E.; Zavagno, G.; Nitti, D. Prognostic value of putative circulating cancer stem cells in patients undergoing hepatic resection for colorectal liver metastasis. Ann. Surg. Oncol. 2012, 19, 402–408. [Google Scholar] [CrossRef]
- Lin, E.H.; Hassan, M.; Li, Y.N.; Zhao, H.; Nooka, A.; Sorenson, E.; Xie, K.P.; Champlin, R.; Wu, X.F.; Li, D.H. Elevated circulating endothelial progenitor marker CD133 messenger RNA levels predict colon cancer recurrence. Cancer 2007, 110, 534–542. [Google Scholar] [CrossRef]
- Zhou, H.; Shen, H.; Xiang, F.; Yang, X.; Li, R.; Zeng, Y.; Liu, Z. Correlation analysis of the expression of mesenchymal circulating tumor cells and CD133 with the prognosis of colorectal cancer. Am. J. Transl. Res. 2023, 15, 3489–3499. [Google Scholar]
- Konishi, T.; Shimada, Y.; Hsu, M.; Tufts, L.; Jimenez-Rodriguez, R.; Cercek, A.; Yaeger, R.; Saltz, L.; Smith, J.J.; Nash, G.M.; et al. Association of preoperative and postoperative serum carcinoembryonic antigen and colon cancer outcome. JAMA Oncol. 2018, 4, 309–315. [Google Scholar] [CrossRef]
- Chu, H.Y.; Lu, L.S.; Cho, W.; Wu, S.Y.; Chang, Y.C.; Lin, C.P.; Yang, C.Y.; Lin, C.H.; Jiang, J.K.; Tseng, F.G. Enumerating circulating tumor cells with a self-assembled cell array (saca) chip: A feasibility study in patients with colorectal cancer. Cancers (Basel) 2019, 11, 56. [Google Scholar] [CrossRef]
- Zahran, A.M.; Rayan, A.; Fakhry, H.; Attia, A.M.; Ashmawy, A.M.; Soliman, A.; Elkady, A.; Hetta, H.F. Pretreatment detection of circulating and tissue CD133(+) CD44(+) cancer stem cells as a prognostic factor affecting the outcomes in Egyptian patients with colorectal cancer. Cancer Manag. Res. 2019, 11, 1237–1248. [Google Scholar] [CrossRef]
- Fang, C.; Fan, C.W.; Wang, C.; Huang, Q.R.; Meng, W.T.; Yu, Y.Y.; Yang, L.; Hu, J.K.; Li, Y.; Mo, X.M.; et al. Prognostic value of CD133+cd54+cd44+ circulating tumor cells in colorectal cancer with liver metastasis. Cancer Med. 2017, 6, 2850–2857. [Google Scholar] [CrossRef]
- Wu, X.S.; Xi, H.Q.; Chen, L. Lgr5 is a potential marker of colorectal carcinoma stem cells that correlates with patient survival. World J. Surg. Oncol. 2012, 10, 244. [Google Scholar] [CrossRef]
- Chen, Q.; Zhang, X.; Li, W.M.; Ji, Y.Q.; Cao, H.Z.; Zheng, P. Prognostic value of lgr5 in colorectal cancer: A meta-analysis. PLoS ONE 2014, 9, e107013. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Xue, X.; Jiang, M.; Guo, X.; Li, P.; Liu, F.; Yuan, B.; Shen, Y.; Guo, X.; Zhi, Q.; et al. Lgr5, a relevant marker of cancer stem cells, indicates a poor prognosis in colorectal cancer patients: A meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2015, 39, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Hongo, K.; Kazama, S.; Sunami, E.; Tsuno, N.H.; Takahashi, K.; Nagawa, H.; Kitayama, J. Immunohistochemical detection of CD133 is associated with tumor regression grade after chemoradiotherapy in rectal cancer. Med. Oncol. 2012, 29, 2849–2857. [Google Scholar] [CrossRef] [PubMed]
- Ieta, K.; Tanaka, F.; Haraguchi, N.; Kita, Y.; Sakashita, H.; Mimori, K.; Matsumoto, T.; Inoue, H.; Kuwano, H.; Mori, M. Biological and genetic characteristics of tumor-initiating cells in colon cancer. Ann. Surg. Oncol. 2008, 15, 638–648. [Google Scholar] [CrossRef]
- Li, G.; Liu, C.; Yuan, J.; Xiao, X.; Tang, N.; Hao, J.; Wang, H.; Bian, X.; Deng, Y.; Ding, Y. CD133(+) single cell-derived progenies of colorectal cancer cell line sw480 with different invasive and metastatic potential. Clin. Exp. Metastasis 2010, 27, 517–527. [Google Scholar] [CrossRef]
- Gao, W.; Chen, L.; Ma, Z.; Du, Z.; Zhao, Z.; Hu, Z.; Li, Q. Isolation and phenotypic characterization of colorectal cancer stem cells with organ-specific metastatic potential. Gastroenterology 2013, 145, 636–46.e5. [Google Scholar] [CrossRef]
Figure 1.
Representative image of CD133 mRNA expression. Lane 3, negative expression of CD133 mRNA; lanes 1 and 2, positive expression of CD133; M, DNA size marker.
Figure 1.
Representative image of CD133 mRNA expression. Lane 3, negative expression of CD133 mRNA; lanes 1 and 2, positive expression of CD133; M, DNA size marker.
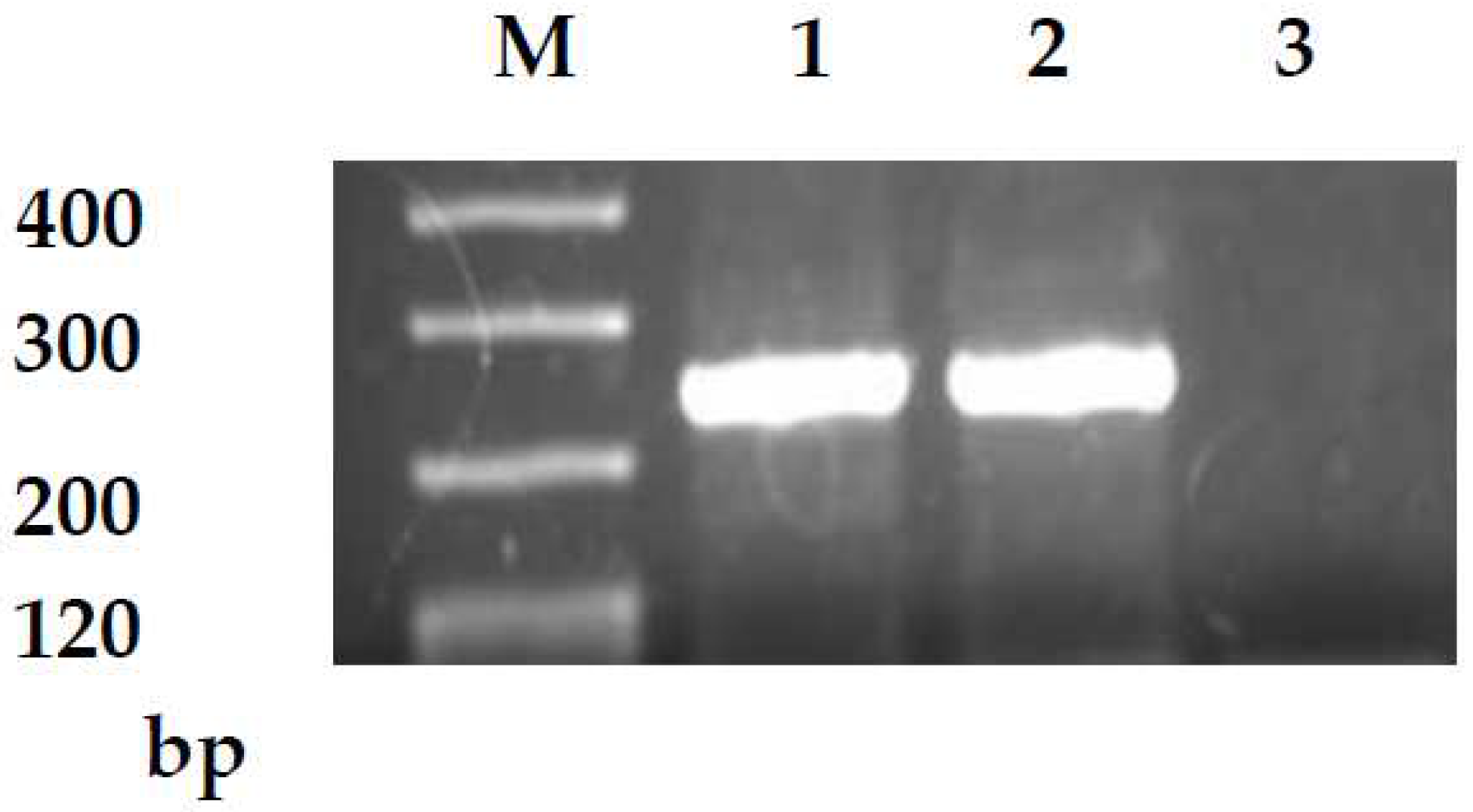
Figure 2.
5-year DSS for CD133-positive and CD133-negative cases.
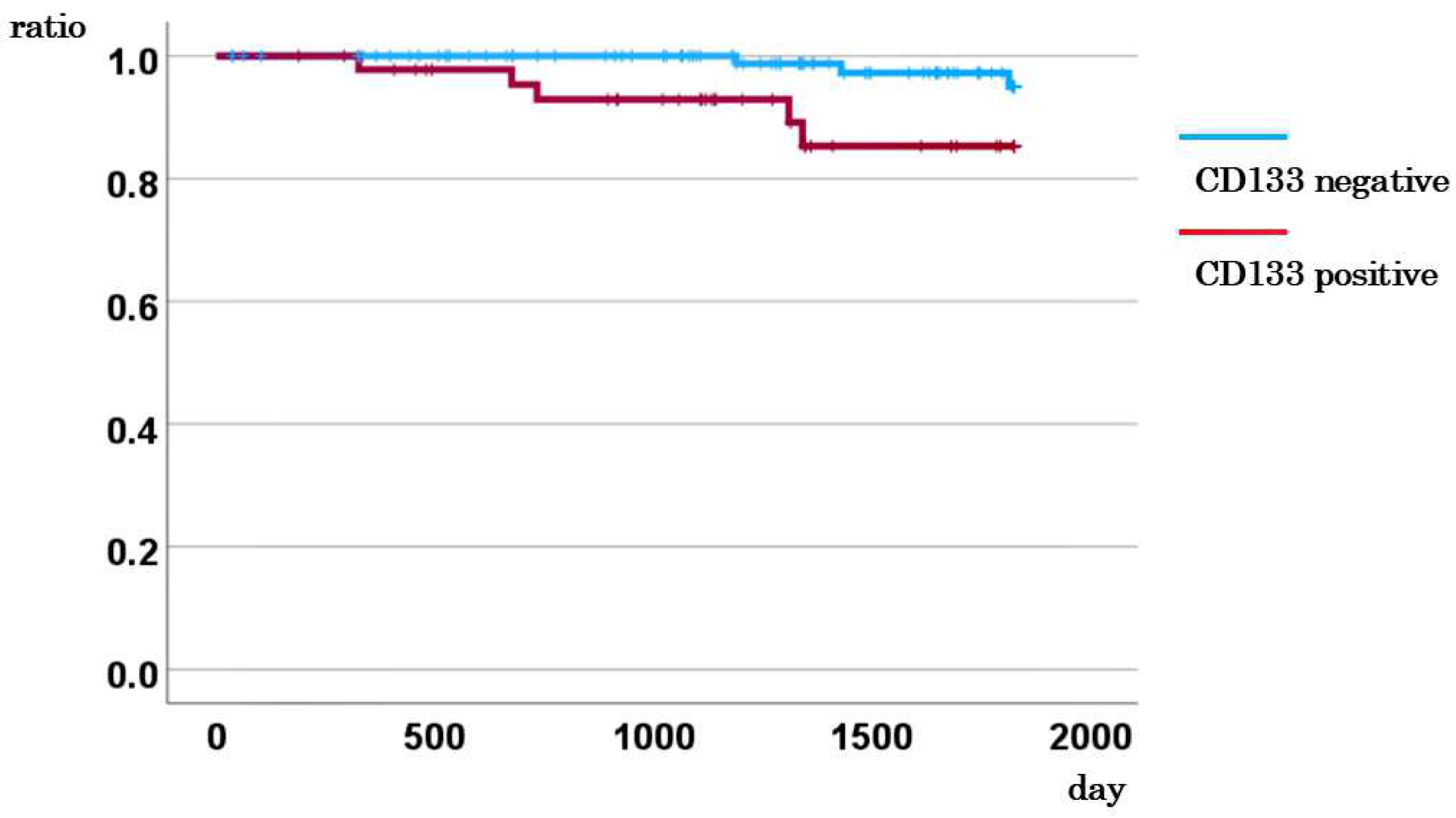
Figure 3.
5-year DSS for cases with low and high CEA levels.
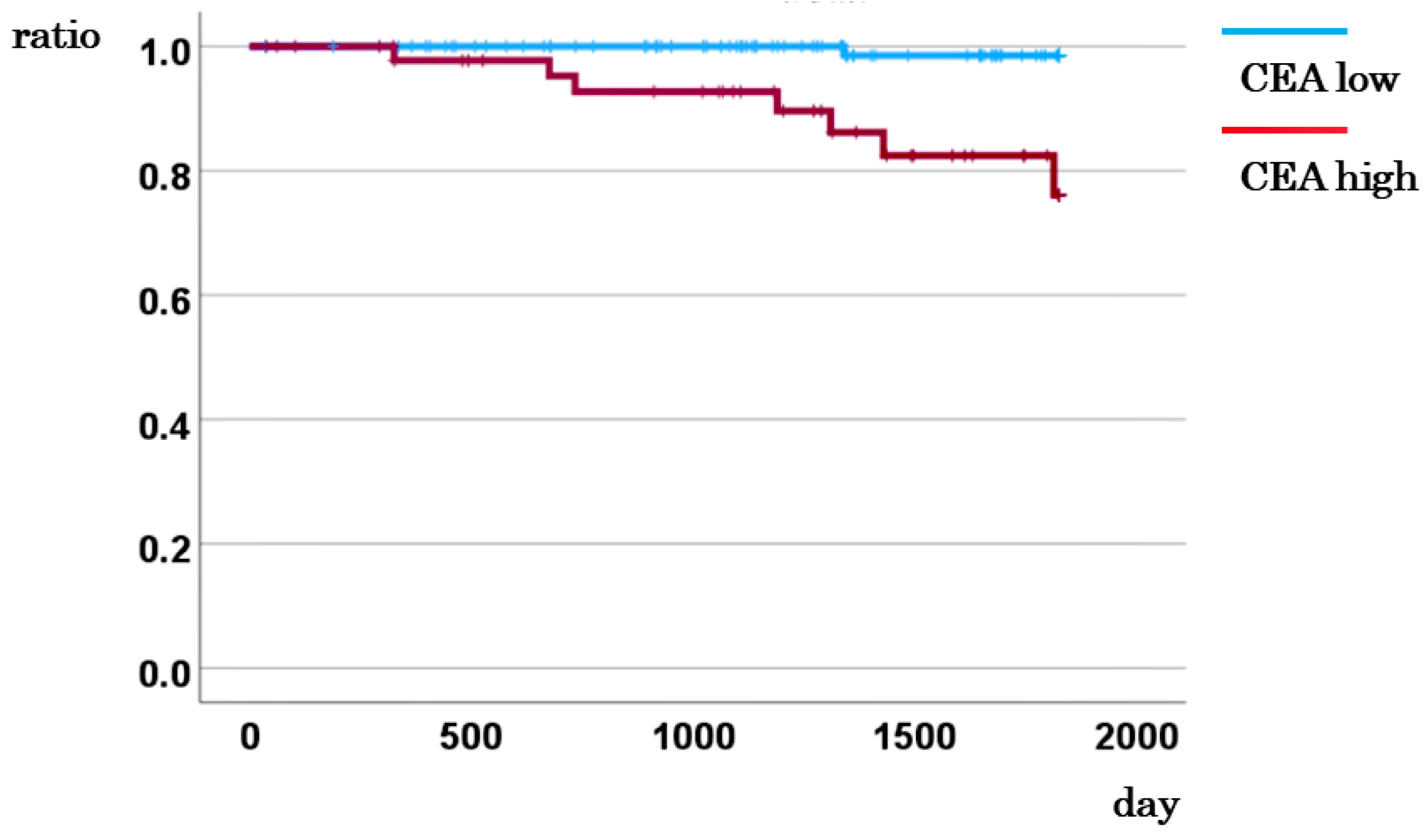
Figure 4.
5-year DSS based on the combination of CD133 and CEA.
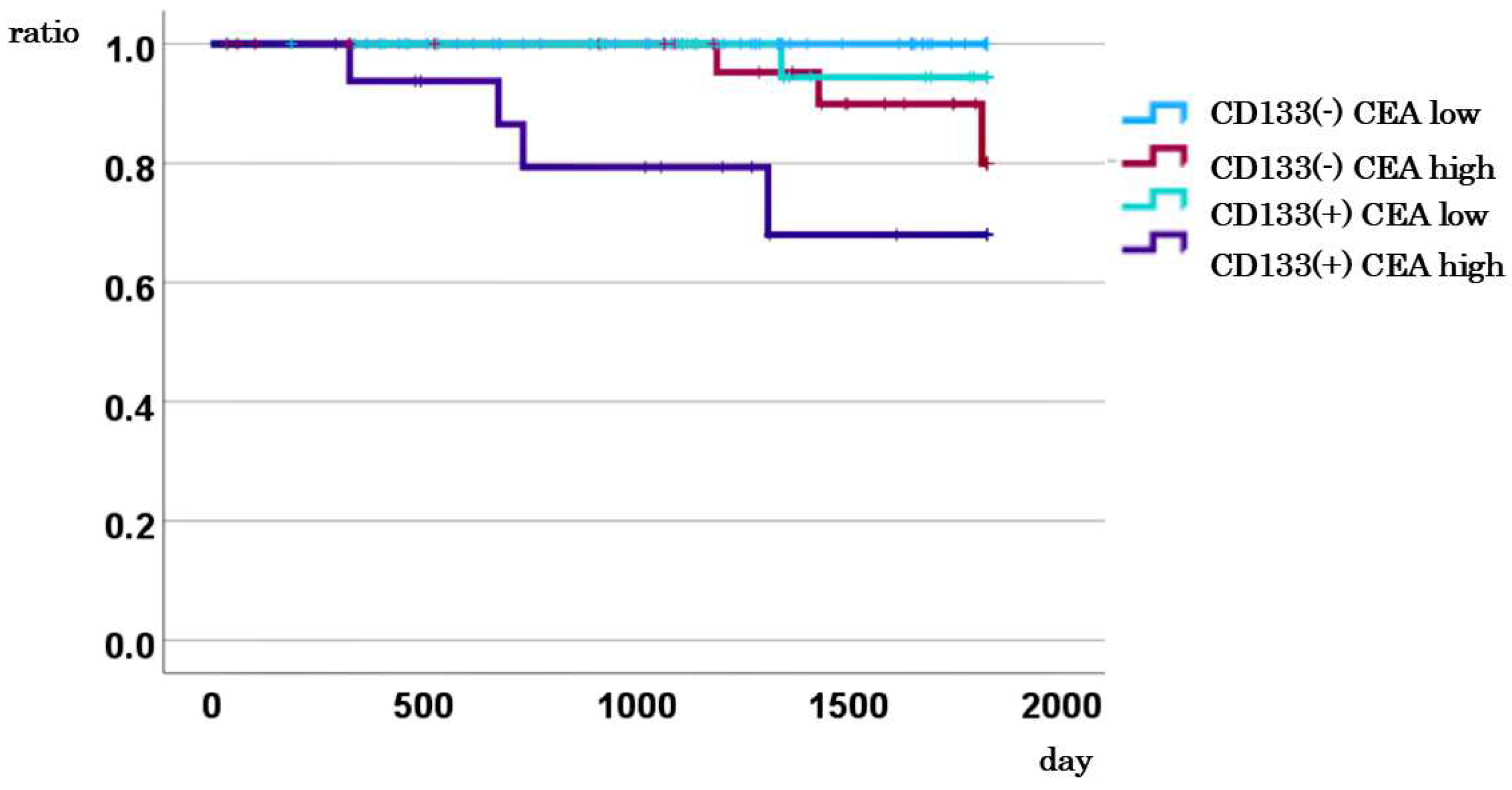
Figure 5.
Comparison of the 5-year DSS between cases with CD133-positive CTCs and high CEA levels and other cases.
Figure 5.
Comparison of the 5-year DSS between cases with CD133-positive CTCs and high CEA levels and other cases.
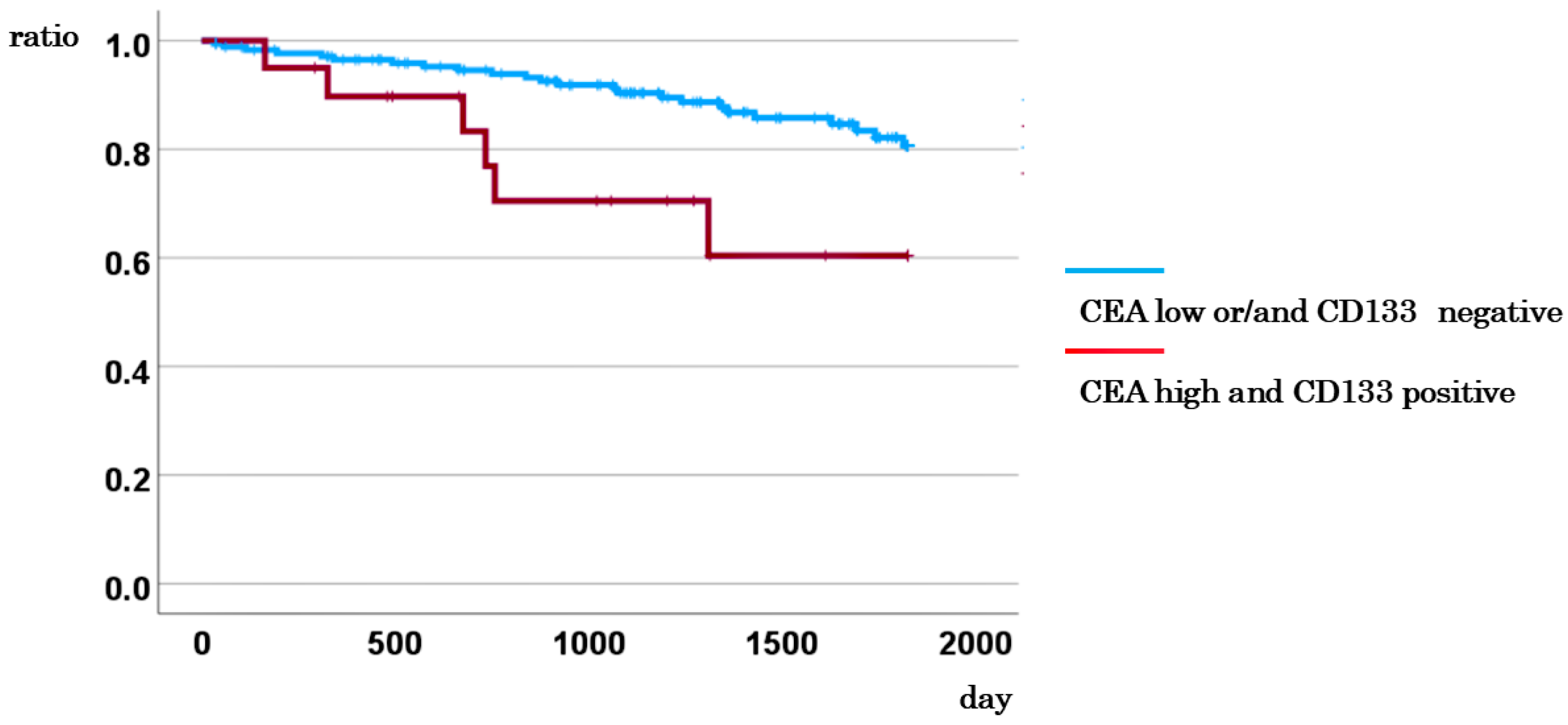
Figure 6.
Comparison of the 5-year DSS between cases with CD133-negative CTCs and low CEA levels, and other cases.
Figure 6.
Comparison of the 5-year DSS between cases with CD133-negative CTCs and low CEA levels, and other cases.
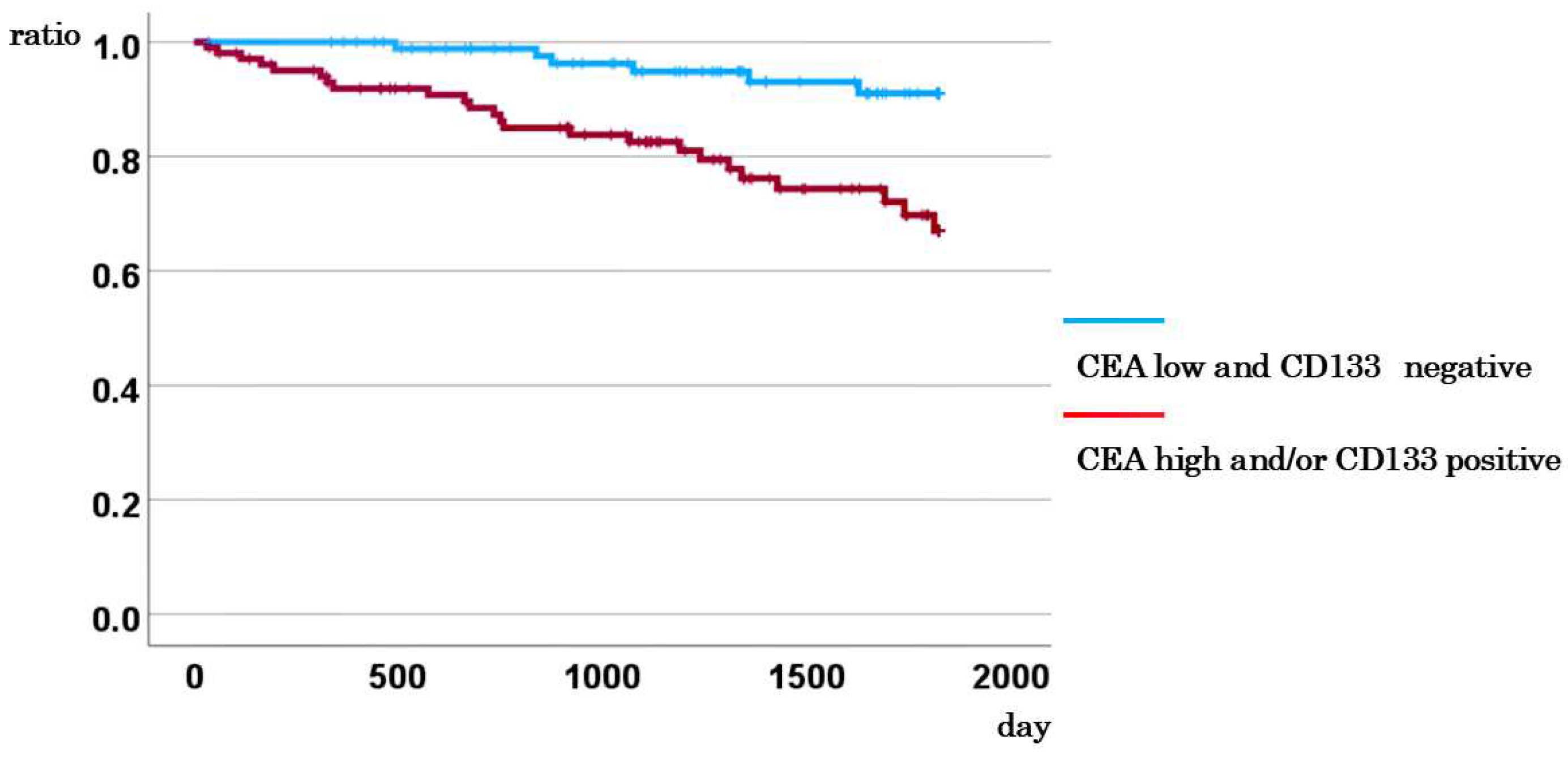

Table 1.
CD133 expression and clinicopathological factors on univariate analysis.
| CD133 mRNA | |||||
| No. of cases | Negative cases (%) | Positive cases (%) | P-value | ||
| All cases (%) | 195 | 142 (72.8) | 53 (27.2) | ||
| Age (median years) | 71.0 | 70.0 | 0.900 | ||
| Sex | Male | 105 | 76 (72.4) | 29 (27.6) | 0.882 |
| Female | 90 | 66 (73.3) | 24 (26.7) | ||
| Location | Right colon | 74 | 53 (71.6) | 21 (28.4) | 0.769 |
| Left colon | 121 | 89 (73.6) | 32 (26.4) | ||
| Size (average mm) | < 50 | 113 | 88(77.9) | 25(22.1) | 0.062 |
| ≧50 | 82 | 54(65.9) | 28(34.1) | ||
| Histological type | Differentiated | 184 | 135 (73.4) | 49 (26.6) | 0.481 |
| Undifferentiated | 11 | 7 (63.6) | 4 (36.4) | ||
| Serosal involvement | Negative | 52 | 44 (84.6) | 8 (15.4) | 0.026 |
| Positive | 143 | 98 (68.5) | 45 (31.5) | ||
| Lymph node metastasis | Negative | 113 | 82 (72.6) | 31 (27.4) | 0.925 |
| Positive | 82 | 60 (73.2) | 22 (26.8) | ||
| Distant metastasis | Negative | 163 | 116 (71.2) | 47 (28.8) | 0.241 |
| Positive | 32 | 26 (81.2) | 6(18.8) | ||
| Stage | I, II | 108 | 78 (72.2) | 30 (27.8) | 0.834 |
| III, IV | 87 | 64 (73.6) | 23 (26.4) | ||
| CEA | 5.0> | 125 | 92 (73.6) | 33 (26.4) | 0.744 |
| 5.0≦ | 70 | 50 (71.4) | 20 (28.6) | ||
Table 2.
CD133 expression and clinicopathological factors on multivariate analysis.
| Multivariate | ||||
| Variable | Odds ration | 95% CI | P-value | |
| Age | 0.997 | 0.967-1.028 | 0.847 | |
| Sex | Male vs Female | 0.961 | 0.493-1.874 | 0.907 |
| Serosal invasion | Negative vs Positive | 3.000 | 1.225-7.345 | 0.016 |
| Lymph node metastasis | Negative vs Positive | 0.850 | 0.412-1.754 | 0.660 |
| Distant metastasis | Negative vs Positive | 0.472 | 0.165-1.353 | 0.162 |
| CEA | 5.0> vs 5.0≦ | 1.074 | 0.532-2.167 | 0.842 |
Table 3.
Multivariate Cox analysis for DSS incorporating CD133 Expression.
| Multivariate | ||||
| Variable | HR | 95% CI | P-value | |
| Distant metastasis | Negative vs. Positive | 35.713 | 14.520-87.838 | < 0.001 |
| CD133 expression | Negative vs. Positive | 3.057 | 1.298-7.196 | 0.011 |
Table 4.
Multivariate Cox analysis for DSS incorporating CEA levels.
| Multivariate | ||||
| Variable | HR | 95% CI | P-value | |
| Distant metastasis | Negative vs. Positive | 19.715 | 8.296-46.853 | < 0.001 |
| CEA level | CEA< 5 vs. CEA≧5 | 2.309 | 1.017-5.244 | 0.046 |
Table 5.
Multivariate Cox analysis for DSS incorporating positive CD133 mRNA expression and high CEA levels.
Table 5.
Multivariate Cox analysis for DSS incorporating positive CD133 mRNA expression and high CEA levels.
| Multivariate | ||||
| Variable | HR | 95% CI | P-value | |
| Distant metastasis | Negative vs. Positive | 33.112 | 13.797-79.468 | < 0.001 |
| CD133 and CEA | Others vs. CD133 (positive) and CEA≧5 | 5.948 | 2.210-16.007 | <0.001 |
Table 6.
Multivariate Cox analysis for DSS incorporating negative CD133 mRNA expression and low CEA levels.
Table 6.
Multivariate Cox analysis for DSS incorporating negative CD133 mRNA expression and low CEA levels.
| Multivariate | ||||
| Variable | HR | 95% CI | P-value | |
| Distant metastasis | Negative vs. Positive | 22.126 | 9.549-51.266 | < 0.001 |
| CD133 and CEA | CD133 (negative) and CEA<5 vs. others | 2.600 | 1.049-6.441 | 0.039 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



