
Submitted:
11 April 2025
Posted:
14 April 2025
You are already at the latest version
Abstract
Early biomarkers are needed to predict the long-term persistence of rheumatic symptoms in patients infected with chikungunya virus (CHIKV). This nested case-control study aimed to assess immunological factors during the early phases of CHIKV infection to pre-dict the risk of post-CHIK chronic rheumatism (pCHIK-CR) in adult patients of two pro-spective cohorts. We evaluated 46 febrile patients (median age: 33.5 years, IQR:19 years; women: 50.0%) with CHIKV infection confirmed during the 2014-2015 outbreak in San-tander, Colombia. Participants were classified by a rheumatologist as either cases (pCHIK-CR) or controls (WoRM, without rheumatic manifestations). We quantified serum levels of IL-4, IL-6, IL-8/CXCL-8, IL-27, CCL-2, CXCL-9, CXCL-10 and IgG using Luminex and ELISA assays during the acute and subacute phases of infection. Then, we evaluated the association of these immune factors with the case-control status using piecewise lo-gistic regression adjusted for age and sex. There were non-linear associations between IL-8/CXCL-8, CXCL-9 and CXCL-10 with pCHIK-CR. Elevated levels of IL-8/CXCL-8 (< 35.7 pg/mL), CXCL-9 (≥2,000 pg/mL), CXCL-10 (≥36,800 pg/mL), significantly reduced the risk of pCHIK-CR (adjusted ORs: 0.85, 0.96 and 0.94, respectively). These results suggest that higher levels of IL-8/CXCL-8, CXCL-9 and CXCL-10, measured in the early stages of CHIKV infection, may predict chronic disease risk. This suggests that an early and strong immune response may enhance CHIKV control and reduce the risk of persistent joint symptoms. Given their expression patterns and timing, these three immune factors may be considered promising biomarker candidates for assessing the risk of chronic rheuma-tism. These findings should be validated in additional cohort studies.
Keywords:
chikungunya fever
; chronic rheumatism
; biomarkers
; cytokines
; chemokines
1. Introduction
Chikungunya fever (CHIKF) is caused by the Chikungunya virus (CHIKV), an RNA virus member of the Togaviridae family, Alphavirus genus [1,2]. CHIKV genome contains two open reading frames (ORFs). The first ORF encodes a polyprotein that is cleaved by viral proteases into four non-structural proteins: nsP1, nsP2 (protease), nsP3, and nsP4 (RNA-dependent RNA polymerase), which are involved in viral genome replication and evasion of host immune response [3]. The second ORF encodes a polyprotein, which is processed by both viral and cellular proteases to produce six structural proteins: capsid (C), envelope (E3, E2, 6K, and E1), and transfer-enhancing protein (TF). These structural proteins are essential for assembling and generating new viral particles [1,2]. CHIKV is classified into three main genotypes: Asian, West Africa (WA), and East/Central/South Africa (ECSA) [4].
CHIKV infection progresses through three clinical phases: acute, subacute, and chronic [5]. The acute phase is characterized by an abrupt onset of fever and joint pain, which may be accompanied by myalgia, headache, nausea, vomiting, conjunctivitis, and skin rashes, lasting 5 to 7 days [6,7]. While most patients recover during this phase, some progress to the subacute phase, characterized by persistent joint pain, fatigue, and weakness, lasting from 10 days to 3 months [5]. The chronic phase begins after three months and can persist for years, manifesting as rheumatic symptoms [5,8,9,10].
During the chronic phase, some cases develop post-chikungunya chronic rheumatism (pCHIK-CR), defined by the persistence of joint and extra-articular symptoms for more than three months after disease onset or by the emergence of specific immune-mediated inflammatory pathology during follow-up [11,12]. This condition is frequently associated with a reduction in quality of life and chronic fatigue [13,14,15,16,17,18,19,20,21]. Several patients’ characteristics, such as age over 45 years, female sex, a history of joint pain, and elevated IgG antibody levels have been proposed as prognostic factors for progression to chronicity [22,23]. However, the understanding of the pathogenesis and the identification of prognostic biomarkers for pCHIK-CR remain limited.
After the bite of an infected Aedes mosquito, CHIKV infects and replicates in monocytes, macrophages, fibroblasts, and endothelial cells in the skin [7,24,25]. The virus then spreads to lymph nodes and, through the lymphatic and bloodstream circulation, distributes to various tissues, including the synovial tissue [26]. In the joints, it has been suggested that the virus may persist and evade the immune response by establishing immune-privileged niches, contributing to tissue damage [27]. This hypothesis is supported by the detection of viral RNA in synovial macrophages 18 months after infection [27]. While some studies have not confirmed the persistence of viral RNA, a study has found the CHIKV glycoprotein E1 in synovial tissue between 22-24 months post-infection, suggesting that specific viral antigens may remain in the affected tissue [28].
Viral persistence leads to the continuous recruitment and activation of monocytes, macrophages, effector T cells, and natural killer (NK) cells, which release pro-inflammatory cytokines (IL-6, IL-8/CXCL-8, CCL-2, and IFNs) that promote fibroblast apoptosis and cartilage destruction [27,29]. Compared to healthy controls, during the acute phase of CHIKV infection, patients show an immune profile characterized by elevated levels of pro-inflammatory cytokines (IFN-α, IFN-γ, IL-2R, IL-6, IL-7, IL-8/CXCL-8, and IL-27), anti-inflammatory cytokines (IL-1Ra and IL-4), chemokines (CCL-2, CXCL-9, and CXCL-10), and growth factors (VEGF, G-CSF, and GM-CSF) in the blood [30]. Given the apparent role of these inflammatory factors in CHIKV progression, further studies are needed to assess their potential as prognostic biomarkers to help stratify the risk of long-term complications. In this context, our study aimed to quantify serum levels of a set of inflammatory factors to identify potential candidate early in the course of CHIKF that could serve as immunological biomarkers for predicting progression to pCHIK-CR.
2. Materials and Methods
We conducted a nested case-control study within two cohorts to quantify immune factors in the serum of patients during the acute and subacute phases of CHIKV infection, to identify immunological biomarkers potentially associated with the development of pCHIK-CR. This section describes each cohort, eligibility criteria, case and control definitions, the procedure for immunological factors quantification, and the data analysis plan.
2.1. Description of Cohorts
Cases of CHIKV infection were identified in two prospective cohorts assembled during the outbreak that occurred between 2014 and 2015 in the municipalities of Capitanejo and Piedecuesta, Colombia, as detailed below:
Capitanejo cohort: Established in 2015 as part of the response to the CHIKV outbreak in the municipality of Capitanejo [9], this cohort included 105 patients aged 5 to 95 years who sought health care due to persistent joint pain. During the baseline visit (subacute phase), patients underwent a physical examination, and a blood sample was collected to confirm CHIKV infection. In 2017, a subsample of adult patients with confirmed infection was followed and evaluated by a rheumatologist to determine the presence of pCHIK-CR.
Piedecuesta cohort: This study was assembled by merging two cohorts conducted in Piedecuesta. One is based on passive surveillance, and the other on active surveillance. The passive surveillance sub-cohort was assembled in 2014 and recruited 839 participants (aged 1 to 55 years) who sought care for acute febrile syndrome at two healthcare institutions [31]. The active surveillance sub-cohort was assembled in 2015 and recruited 2,400 healthy participants from the community [32]. This sub-cohort was followed through biweekly phone calls for 3.5 years to identify cases of acute febrile illness. In both sub-cohorts, participants with febrile illness were clinically assessed within 7 days of symptoms’ onset (baseline visit) and followed up 7 to 14 days later to conduct a clinical evaluation and collect a blood sample. In total, the Piedecuesta cohort identified 219 cases of CHIKV infection during the acute phase of the disease. In 2022, adult participants with confirmed CHIKV infection were followed to undergo a physical examination that included an musculoskeletal screening using the GALS methodology (gait, upper extremities, lower extremities) conducted by a physician [33,34] . Additionally, a rheumatologist evaluated those patients with an abnormal GALS screening (unrelated to trauma) to determine the presence of pCHIK-CR.
In both Capitanejo and Piedecuesta cohorts, CHIKV infection was diagnosed based on a positive result in the NovaLisa® ELISA IgG or IgM tests (NOVATEC Inmunodiagnostica GmbH, Dietzenbach, Germany) or the reverse transcription quantitative polymerase chain reaction (RT-qPCR) test [35]. This diagnostic approach was adopted because the virus was newly introduced to the population during the study period.
2.2. Eligibility Criteria
We included adults over 18 years old with confirmed CHIKV infection who attended a follow-up evaluation during the chronic phase of the disease. We excluded participants with a history of rheumatic disease before CHIKV infection, as well as those diagnosed with non-inflammatory pain likely degenerative (NIP-LD) during the follow-up evaluation. We also excluded individuals who did not consent to using their biological samples for future research, as requested in the original cohorts, and those who had no samples collected at baseline for the quantification of immunological factors.
2.3. Case-Control Definition
The case-control status was determined based on the clinical evaluation results conducted during the follow-up visit of the cohorts. The median follow-up was 2.2 years for patients recruited in the Capitanejo cohort, and 7.7 years for those recruited in the Piedecuesta cohort. The cases of pCHIK-CR were defined as patients experiencing persistent joint and extra-articular symptoms lasting more than three months after the onset of CHIKV infection; or patients with a specific immune-mediated inflammatory pathology at follow-up [11,12]. Further, pCHIK-CR patients were classified as cases of rheumatoid arthritis [36], spondylarthritis [37], systemic lupus erythematosus [38], post-viral arthritis [39], post-viral arthralgia [39], and soft tissue rheumatism (tenosynovitis, bursitis, fasciitis, noninflammatory localized pain, enthesitis, or fibromyalgia) [40]. Participants without rheumatic manifestations (Wo-RM) at follow-up were classified as controls.
2.4. Immunological Factor Assays
We quantified immunological factors in the samples collected during the baseline visit stored at –80°C. The serum concentrations of IL-4, IL-6, IL-8/CXCL-8, IL-27, CCL-2, CXCL-9, and CXCL-10 were quantified using the Milliplex® Human Cytokine/Chemokine/Growth Factor Panel A (HCYTA-60K, Millipore, MA, USA) kit on the Luminex MAGPIX® system (XMAP Technology, MAGPIX, TX, USA), following the manufacturer's instructions. Specific IgG antibodies against CHIKV were quantified using the NovaLisa® IgG capture ELISA kit (NOVATEC Inmunodiagnostica GmbH, Dietzenbach, Germany). This assay measures NovaTec Units (NTU), and the results are classified as negative (<9 NTU), positive (>11 NTU), or indeterminate (9-11 NTU).
2.5. Ethical Considerations
The Ethics Committees of the Universidad Industrial de Santander (Acta No. 07, 23 April 2021, and Acta No. 04, 18 March 2023) and the Centro de Atención y Diagnóstico de Enfermedades Infecciosas—C.D.I. (Acta 293, 9 July 2022) approved the study protocol. Informed consent was obtained from all participants before inclusion in the original cohorts and their authorization for future use of biological samples.
2.6. Data Analysis
We described continuous variables using the mean and standard deviation (SD), or the median and interquartile range [IQR] for those not normally distributed, according to the Shapiro-Wilk test. We calculated their absolute and relative frequencies (percentages) for discrete variables. We compared the means and medians between groups using Student’s T-test and the Kruskal-Wallis test, respectively. We assessed differences in proportions using the chi-square test and, alternatively, the Fisher’s exact test whenever the expected counts in contingency tables were less than five. We assessed partial correlations among immunological factors concentrations using Spearman's rank correlation coefficient (rs), adjusting for age at baseline and sex. We explored the shape of the functional relationship between each immunological factor and the case-control status using locally weighted regression to identify inflection points. Then, we performed multiple logistic regression both with and without piecewise modelling (using previously determined cut-points), and estimated odds ratios (ORs) with 95% confidence intervals (95%CI), forcing the adjustment for age but conditioning it by age, sex, and disease duration at baseline visit, only if these covariates were associated to the case-control status at a significance level of ≤10% in the bivariate analysis. We evaluated the model fit using the Hosmer-Lemeshow (HL) test and their assessed discriminatory accuracy by estimating the area under the receiver operating characteristic (ROC) curve. Data analysis was conducted using the statistical software Stata/MP version 12.0 (Stata Corp. TX, USA).
3. Results
3.1. Population Characteristics
The analysis included 11 cases of pCHIK-CR and 35 controls from the Piedecuesta cohort, and 14 cases and 20 controls from the Capitanejo cohort (Figure 1). Patients from both cohorts differed in the disease duration at which the immune factors were measured, the length of follow-up, and their demographic and clinical characteristics (Table 1). The samples used for the immune factor quantification were collected earlier in the illness course in the Piedecuesta cohort compared to the Capitanejo cohort (2.8 versus 40.5 days, respectively); however, follow-up for pCHIK-CR determination was longer in the Piedecuesta cohort (7.7 versus 2.2 years, respectively). Additionally, the Capitanejo cohort had a higher median age (54.0 versus 33.5 years), a greater proportion of women (73.5% versus 50.0%), and a higher prevalence of cardiovascular disease (20.6% versus 0.0%) and diabetes (7.1% versus 2.2%) than the Piedecuesta cohort. Furthermore, cases were older and more likely to be women than controls; however, these differences were statistically significant only in the Piedecuesta cohort.
3.2. Quantification and correlation of immunological factors
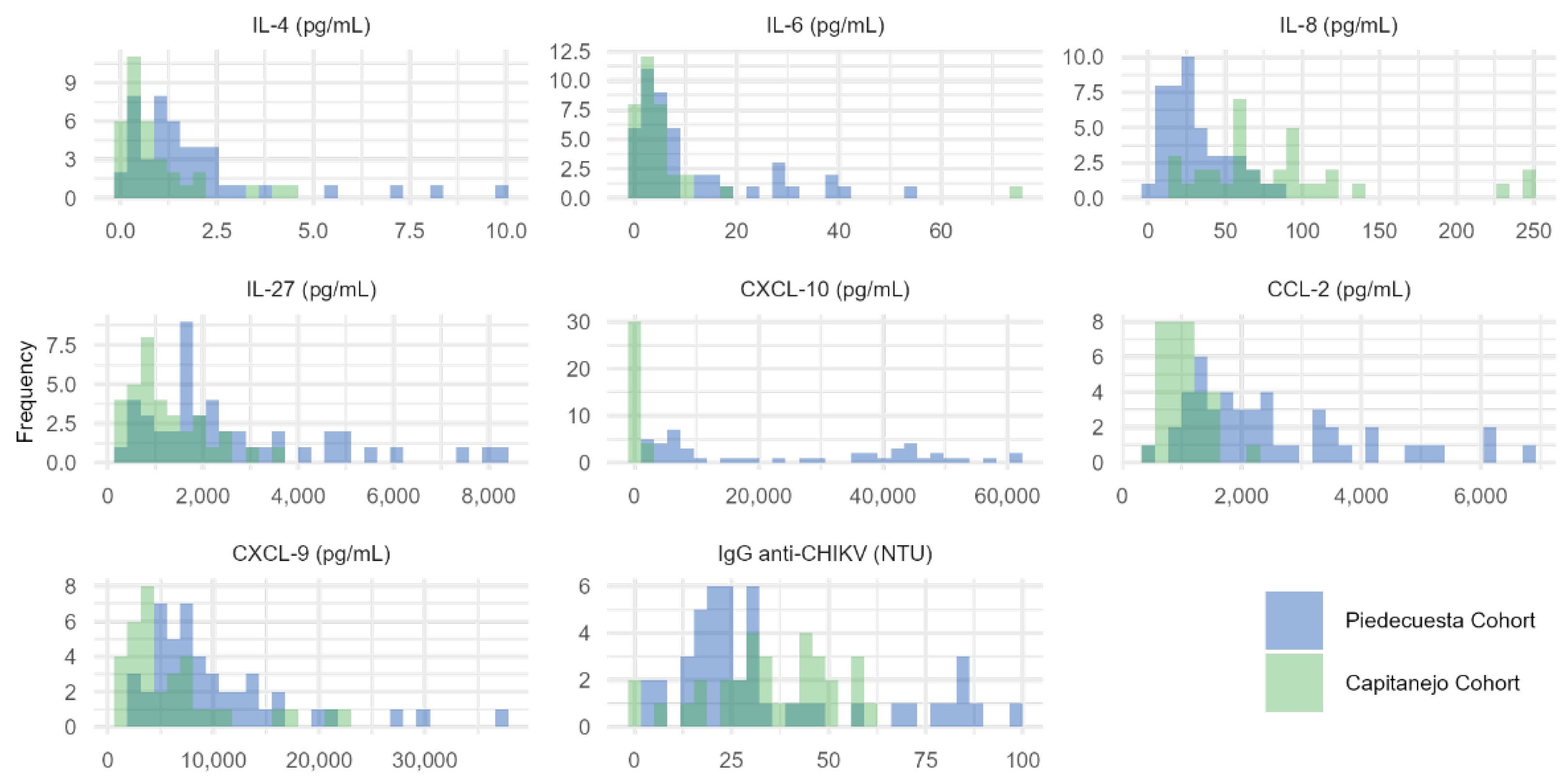
The levels of IL-4, IL-6, IL-27, CCL-2, CXCL-9, and CXCL-10 were higher in the Piedecuesta than in the Capitanejo cohort (Table 2, Appendix A.1). In contrast, IL-8/CXCL-8 had higher concentrations in Capitanejo compared to the Piedecuesta cohort. On the other hand, the pattern of partial correlations between immunological factors differed across cohorts (Figure 2). In the Piedecuesta cohort, CXCL-10 was positively correlated with IL-27 (rs=0.358, p=0.017) but negatively correlated with IL-4 (rs=-0.313, p=0.039). Additionally, we observed positive correlations between IL-6 and CCL-2 (rs=0.403, p=0.007), and between IL-8/CXCL-8 and IgG (rs=0.391, p=0.009, Figure 2A). In the Capitanejo cohort, we observed statistically significant negative correlations between IL-4 and CXCL-10 (rs=-0.425, p=0.019) and CCL-2 (rs=-0.379, p=0.039) and positive correlations between CXCL-10 and CCL-2 (rs=0.409, p=0.025) and CXCL-9 (rs=0.548, p=0.002, Figure 2B).
3.3. Quantification of immunological factors by case-control status
In both cohorts, the baseline concentrations of IL-8/CXCL-8, CXCL-9, and CXCL-10 were non-statistically lower in cases than in controls, while the opposite was observed for IgG (Table 2, Figure 3). In addition, IL-6 and CCL-2 concentrations were higher in samples collected during the acute phase of cases than in controls (Piedecuesta cohort), whereas IL-4 and IL-27 concentrations were higher in samples collected during the subacute phase of cases than in controls (Capitanejo cohort); however, none of these differences reached statistical significance.
In the multivariate analysis, we found non-linear associations between IL-8/CXCL-8 and CXCL-10 concentrations – measured in samples collected during the acute phase of CHIKV infection (Piedecuesta cohort) – and the likelihood of developing pCHIK-CR (Table 3, Appendix A.2). The threshold concentrations were determined as 35.7 pg/mL for IL-8/CXCL-8 and 36,800 pg/mL for CXCL-10. For IL-8/CXCL-8, concentrations below the threshold indicated that a 1.0 pg/mL increase was associated with a 15% lower likelihood of pCHIK-CR (adjusted OR = 0.85, 95%CI: 0.74 - 0.99). On the other hand, for CXCL-10, a 100 pg/mL increase above the threshold was associated with a 6% lower likelihood of pCHIK-CR (adjusted OR = 0.94, 95%CI: 0.90 - 0.99). Additionally, we observed a non-linear association between CXCL-9 concentration – measured in samples collected during the subacute phase of CHIKV infection (Capitanejo cohort) – and the likelihood of pCHIK-CR. Here, a 100 pg/mL increase above the threshold (2,000 pg/mL) was associated with a 4% lower likelihood of pCHIK-CR (adjusted OR = 0.96, 95%CI: 0.93 - 0.99). No statistically significant associations, whether linear or non-linear, were observed for any other immunological factors.
4. Discussion
In this study, we observed that the concentrations of IL-8/CXCL-8, CXCL-9, and CXCL-10 were lower in the cases of pCHIK-CR compared to the controls; however, these differences were not statistically significant, regardless of whether the samples were collected during the acute or subacute phases. In contrast, the concentrations of IL-6 and CCL-2 were higher in samples collected during the acute phase of the cases of pCHIK-CR compared to the controls. Additionally, IL-4 and IL-27 concentrations were elevated in cases compared to controls, during the subacute phase. Multivariate analysis indicated that in samples from the acute phase of CHIKV infection, levels of CXCL-10 (≥36,800 pg/mL) and IL-8/CXCL-8 (≤35.7 pg/mL) were associated with a lower likelihood of developing pCHIK-CR seven years after symptom onset. Further, CXCL-9 (≥2,000 pg/mL) levels were associated with a reduced risk of pCHIK-CR after two years of follow-up in samples from the subacute phase.
We evaluated the hypothesis that immune factors are associated with the development of pCHIK-CR by analyzing data from two cohorts assembled during the CHIKV epidemic in Santander, Colombia, between 2014 and 2015. These cohorts differed in several aspects, including the duration of the disease when immune factors were measured, the length of follow-up, and their baseline demographic and clinical characteristics. These differences help explain the varying incidence of pCHIK-CR between cohorts [21,22,23,41], as indicated by their case-control ratios. This variation allowed us to explore the role of the immune response to CHIKV infection during the early stages of the disease, namely the acute and subacute phases.
During the acute phase of CHIKV, IL-8/CXCL-8 and CXCL-10 seem to play a significant role in predicting the development of pCHIK-CR. Higher IL-8/CXCL-8 levels below the threshold of 35.7 pg/mL were associated with a lower likelihood of the outcome. In terms of CXCL-10, higher levels (above 36,800 pg/mL) during the acute phase were associated with a lower probability of developing pCHIK-CR after seven years of follow-up. Similarly, in the subacute phase, higher levels of CXCL-9 above 2,000 pg/mL were negatively associated with the likelihood of developing pCHIK-CR two years after symptoms onset. CXCL-9 and CXCL-10 are STAT1-dependent inflammatory factors induced by different cell populations in response to interferons and IL-27 [42], and their expression correlates with the induction of interferon-stimulated genes (ISGs) which promote antiviral state to control viral infections [24,42]. Additionally, both chemokines play a role in the recruitment of T cells and monocytes to infection sites, contributing to virus clearance and inflammatory response [26,43,44]. Therefore, our findings suggest that the induction of early and strong IFN-STAT1-dependent inflammatory factors may enhance CHIKV control and prevent persistent joint symptoms.
In response to viral infections, the host induces an antiviral response characterized by the production of type I interferons (IFN-α, IFN-β), type III interferons (IFN-λ), and IL-27 (IFN-V) [43,45]. These interferons activate the JAK-STAT signaling pathway, triggering the transcription of ISGs that encode antiviral proteins (AVPs), cytokines, and chemokines essential for viral control and clearance [26,46]. Furthermore, type II IFN (IFN-γ), produced by NK cells, CD4+ T cells (Th1), and cytotoxic CD8+ T cells; or IL-27 from macrophages, induces the expression of IL-7, IL-15, CXCL-9, CXCL-10, and AVPs, contributing to the establishment of the antiviral state and control CHIKV replication [26,43]. Type I IFNs play a crucial role in controlling acute CHIKV infection, as mice lacking the type I IFN receptor exhibit higher viremia and increased susceptibility to severe CHIKV disease [47,48,49]. Additionally, CHIKV infection in human monocytes promotes robust IFN-I-dependent antiviral response involved in control viral replication [50]. Considering this, if an efficient immune response for viral clearance occurs during the early days of CHIKV infection, the likelihood of progressing to the chronic phase of the disease could decrease, as well as the persistence of residual viral antigens in the synovial tissue and associated inflammation.
In this study, the findings for CXCL-9 and CXCL-10, along with the absence of an IL-27 signal during the early stage of the disease, suggest that this response may be primarily mediated by the interferon signaling pathway rather than IL-27. Although IL-27 may activate the JAK-STAT signaling pathway independently of interferons and contribute to the CCL-2, CXCL-9, and CXCL-10 production [24,26,43]. We did not find significant differences in IL-27 levels between cases and controls in our cohorts. Some studies have indicated that IL-27 serum levels positively correlate with the number of painful joints during the chronic phase of CHIKF (8.5 and 29 weeks), suggesting a potential role in later inflammatory stages [51].
The absence of an association between early CCL-2 and IL-6 levels and the development of pCHIK-CR suggests that these factors are not differentially regulated in acute CHIKV infection based on case-control status. Their release may be stimulated by signaling pathways other than JAK-STAT, such as the NF-kB pathway [52,53]. Moreover, their contribution to the disease pathogenesis may become evident during the chronic phase, potentially through the perpetuation of inflammation and tissue damage [52,54,55,56]. Previous studies assessing the relationship between IL-6 levels during the acute phase and joint pain at 12 and 20 months of follow-up found no significant association [27,57]. CCL-2 has not yet been evaluated using the methodology applied in our study.
We did not observe a significant signal for IL-4, which contrasts with the findings of Chan et al, who reported that a strong immune response during the acute phase, including TNF-α, IL-4, IL-2, and IL-13, reduced the likelihood of persistent joint pain after 20 months [57]. This discrepancy may be partially explained on the one hand, due to insufficient statistical power in our study, and on the other, by the use of a different definition of the outcome (joint pain versus pCHIK-CR). Additionally, IL-4 plays a key role in adaptive immunity, primarily by promoting B-cell proliferation and differentiation, which are essential for antibody production. Since humoral responses develop later in the disease's natural history, IL-4 levels during the acute phase may not exhibit a distinct pattern based on the case-control status.
This study has some strengths worth mentioning. First, it is a nested case-control study within two cohorts that given their differences in design (duration of the disease when immune factors were measured and length of follow-up) allowed us to explore the role of the immune response to CHIKV infection during the early stages of the disease, namely the acute and subacute phases. Further, the Piedecuesta cohort is among the studies conducted in Latin America with the most extended follow-up to assess pCHIK-CR, and additional follow-up visits could be conducted in this population. Second, the nested case-control approach minimized the risk of selection bias, considering that controls were selected from the same population as cases. Third, outcome adjudication was conducted by certified rheumatologists who were unaware of the results from immunological factor quantification, which, on the one hand, ensures the validity of pCHIK-CR determination, and on the other, minimizes the risk of information bias. Fourth, we adjusted the associations under study for biologically and clinically relevant confounders which minimized the risk of spurious findings. This study also has limitations. First, we only measured immunological factors at the baseline visit of each cohort, which precluded the evaluation of their dynamic interplay throughout disease progression to the chronic phase of the disease. Second, due to the differences in the cohorts’ designs, we decided to test our hypothesis within each cohort separately, which limited the statistical power to detect associations between some immunological factors and pCHIK-CR. Third, using serological for CHIKV diagnosis in a single sample may carry a risk of false positives; however, the original cohorts were conducted during the early introduction of CHIKV in these municipalities, when prior immunity was unlikely. Finally, the CHIKV cases were identified in two municipalities in Colombia, which could limit the generalizability of the findings to other populations and epidemiological context.
Considering the limitations of this study and the still incomplete understanding of the immunopathogenesis of chronic CHIKV-related disease, future research could benefit from additional follow-up visits to evaluate potential changes in the frequency of pCHIK-CR over time. Furthermore, the collection of serum, peripheral blood cells and synovial membrane biopsies during the chronic phase could yield valuable insights into the expression of the immunological factors evaluated. Longitudinal studies with repeated measurements of these immune factors would also provide a better understanding of disease pathogenesis.
5. Conclusions
Our results suggest that higher concentrations of IL-8/CXCL-8 and CXCL-10, and CXCL-9 measured during the acute and subacute phases of CHIKV infection, respectively, are associated with a reduced likelihood of developing pCHIK-CR, suggesting that induction of early and strong immune responses may enhance CHIKV control and prevent persistent joint symptoms. Furthermore, these chemokines could be considered as potential biomarkers for stratifying the risk of developing chronic sequels of CHIKV. These could enable timely symptoms management and improve the quality of life of the patients. Validation in more extensive studies is necessary to confirm their clinical utility and guide early intervention strategies to improve patient outcomes.
Author Contributions
A.L.P.: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft preparation, writing—review and editing. V.H.: Conceptualization, formal analysis, methodology, writing—original draft preparation, writing—review and editing. L.A.V.: Conceptualization, investigation, writing—review and editing. S.U-I.: Investigation, writing—review and editing. J.F.V-L.: Investigation, writing—review and editing. E.M.R.G.: Conceptualization, investigation, methodology, supervision, writing—review and editing, funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported by Centro de Atención y Diagnóstico de Enfermedades Infecciosas (CDI), Fundación INFOVIDA, Programa de beneficios tributarios I+D+i de Colombia, MINCIENCIAS (Agreement N. 9895-913-93197) and Universidad Industrial de Santander.
Institutional Review Board Statement
The Ethics Committees of the Universidad Industrial de Santander (Acta No. 07, 23 April 2021, and Acta No. 04, 18 March 2023) and the Centro de Atención y Diagnóstico de Enfermedades Infecciosas—C.D.I. (Acta 293, 9 July 2022) approved the study protocol.
Informed Consent Statement
Informed consent was obtained from each participant prior to inclusion in the initial cohorts, and authorization for the use of the samples in future studies was confirmed.
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request. Due to privacy and ethical restrictions, the data cannot be made publicly available.
Acknowledgments
We thank the members of CER Project in the Centro de Atención y Diagnóstico de Enfermedades Infecciosas—C.D.I. for their work in data collection and their support in establishing of case-control status.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Appendix A.1. Histograms of the concentration of immunological factors quantified in each cohort.
Appendix A.2. Exploration of the functional relationship between IL-8/CXCL-8, CXCL-9, and CXCL-10 and the case-control status.
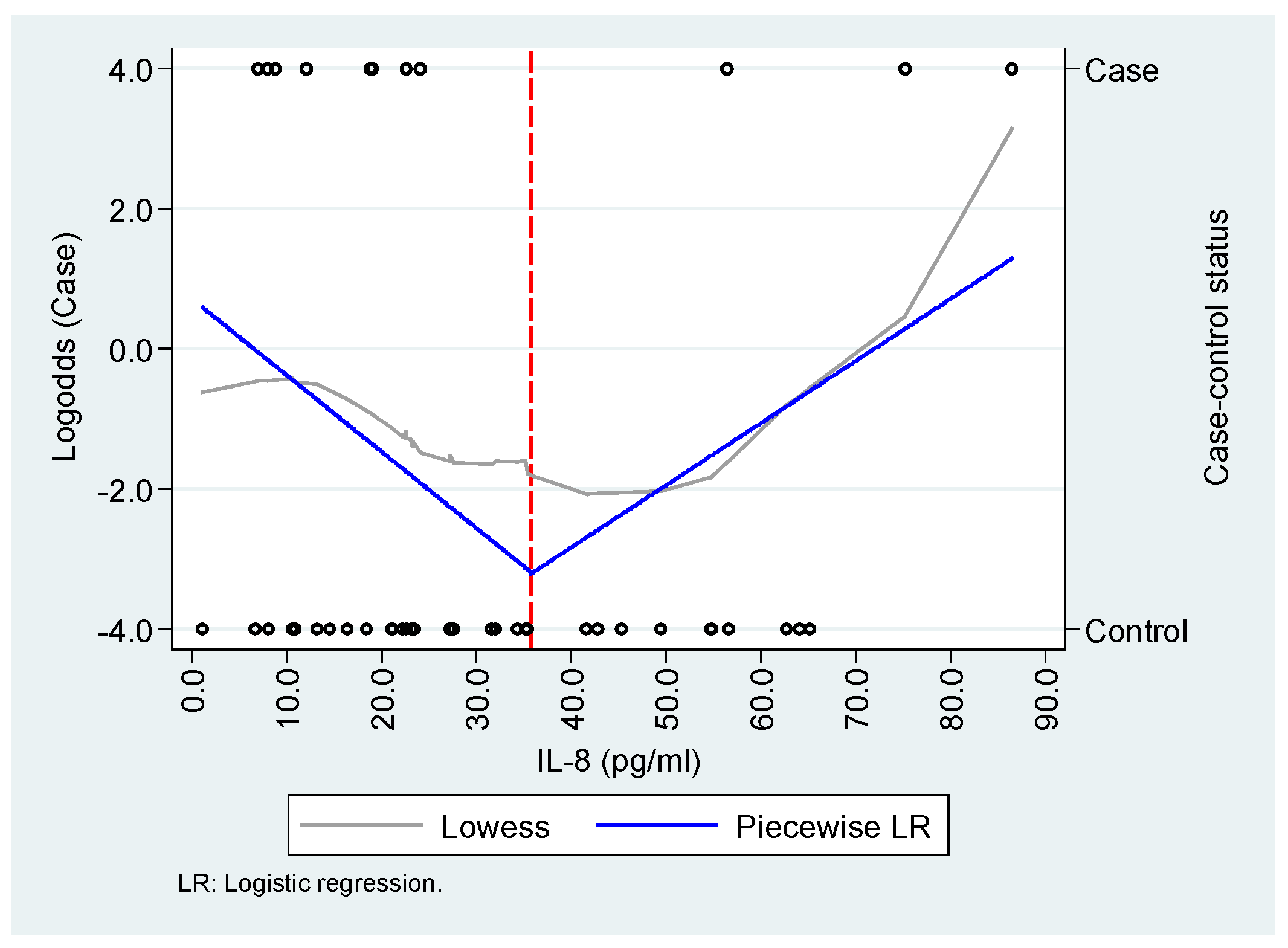
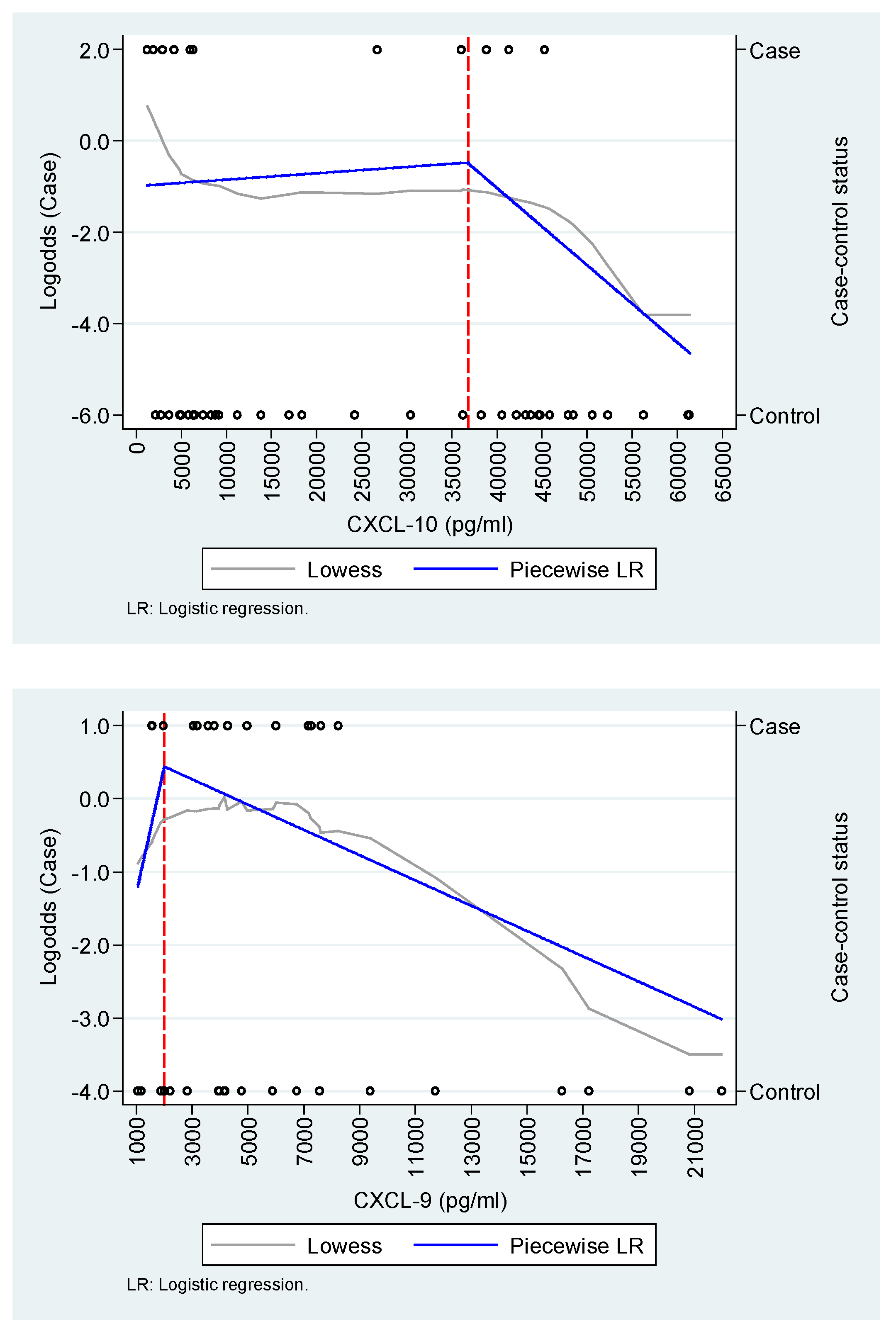
The Capitanejo cohort includes 14 cases (chronic post-CHIKV rheumatism, pCHIK-CR) and 20 controls (without rheumatic manifestations, Wo-RM), whereas the Piedecuesta cohort includes 11 cases of pCHIK-CR and 35 controls Wo-RM. The exploration of IL-8/CXCL-8 and CXCL-10 was conducted in the Piedecuesta cohort, while the exploration of CXCL-9 was performed in the Capitanejo cohort.
References
- Valdés López, J.F.; Velilla, P.A.; Urcuqui-Inchima, S. Chikungunya Virus and Zika Virus, Two Different Viruses Examined with a Common Aim: Role of Pattern Recognition Receptors on the Inflammatory Response. Journal of Interferon & Cytokine Research 2019. [CrossRef]
- Constant, L.E.C.; Rajsfus, B.F.; Carneiro, P.H.; Sisnande, T.; Mohana-Borges, R.; Allonso, D. Overview on Chikungunya Virus Infection: From Epidemiology to State-of-the-Art Experimental Models. Front Microbiol 2021, 12, 2873. [Google Scholar] [CrossRef] [PubMed]
- Akhrymuk, I.; Kulemzin, S. V.; Frolova, E.I. Evasion of the Innate Immune Response: The Old World Alphavirus NsP2 Protein Induces Rapid Degradation of Rpb1, a Catalytic Subunit of RNA Polymerase II. J Virol 2012, 86, 7180–7191. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.A.; Dermody, T.S. Chikungunya Virus: Epidemiology, Replication, Disease Mechanisms, and Prospective Intervention Strategies. J Clin Invest 2017, 127, 737–749. [Google Scholar] [CrossRef]
- Organización Panamericana de la Salud Preparación y Respuesta Ante La Eventual Introducción Del Virus Chikungunya En Las Américas 2011.
- Organización Mundial de la Salud Chikungunya. Nota Descriptiva. Available online: http://www.who.int/mediacentre/factsheets/fs327/es/ (accessed on 8 September 2024).
- Tanabe, I.S.B.; Tanabe, E.L.L.; Santos, E.C.; Martins, W. V.; Araújo, I.M.T.C.; Cavalcante, M.C.A.; Lima, A.R. V.; Câmara, N.O.S.; Anderson, L.; Yunusov, D.; et al. Cellular and Molecular Immune Response to Chikungunya Virus Infection. Front Cell Infect Microbiol 2018, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kucharz, E.J.; Cebula-Byrska, I. Chikungunya Fever. Eur J Intern Med 2012, 23, 325–329. [Google Scholar] [CrossRef]
- López Rodríguez, M.A. Evaluación de Las Manifestaciones Reumatológicas y Las Alteraciones Paraclínicas Luego de Dos Años de La Presentación de La Infección Por Virus de Chikungunya En Un Brote En El Municipio de Capitanejo, Santander. [Tesis de Especialización En Medicina Interna], Universidad Industrial de Santander, 2018.
- Thiberville, S.D.; Moyen, N.; Dupuis-Maguiraga, L.; Nougairede, A.; Gould, E.A.; Roques, P.; de Lamballerie, X. Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis and Therapy. Antiviral Res 2013, 99, 345–370. [Google Scholar] [CrossRef]
- Simon, F.; Javelle, E.; Cabie, A.; Bouquillard, E.; Troisgros, O.; Gentile, G.; Leparc-Goffart, I.; Hoen, B.; Gandjbakhch, F.; Rene-Corail, P.; et al. French Guidelines for the Management of Chikungunya (Acute and Persistent Presentations). November 2014. Med Mal Infect 2015, 45, 243–263. [Google Scholar] [CrossRef]
- Segura-Charry, J.S.; Parada-Martinez, M.A.; Segura-Puello, H.R.; Muñoz-Forero, D.M.; Nieto-Mosquera, D.L.; Villamil-Ballesteros, A.C.; Cortés-Muñoz, A.J. Musculoskeletal Disorders Due to Chikungunya Virus: A Real Experience in a Rheumatology Department in Neiva, Huila. Reumatol Clin 2021, 17, 456–460. [Google Scholar] [CrossRef]
- Soumahoro, M.K.; Gérardin, P.; Boëlle, P.Y.; Perrau, J.; Fianu, A.; Pouchot, J.; Malvy, D.; Flahault, A.; Favier, F.; Hanslik, T. Impact of Chikungunya Virus Infection on Health Status and Quality of Life: A Retrospective Cohort Study. PLoS One 2009, 4, e7800. [Google Scholar] [CrossRef]
- Ramachandran, V.; Malaisamy, M.; Ponnaiah, M.; Kaliaperuaml, K.; Vadivoo, S.; Gupte, M.D. Impact of Chikungunya on Health Related Quality of Life Chennai, South India. PLoS One 2012, 7, e51519. [Google Scholar] [CrossRef]
- Couturier, E.; Guillemin, F.; Mura, M.; Léon, L.; Virion, J.M.; Letort, M.J.; De valk, H.; Simon, F.; Vaillant, V. Impaired Quality of Life after Chikungunya Virus Infection: A 2-Year Follow-up Study. Rheumatology (United Kingdom) 2012, 51, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Elsinga, J.; Gerstenbluth, I.; Van Der Ploeg, S.; Halabi, Y.; Lourents, N.T.; Burgerhof, J.G.; Van Der Veen, H.T.; Bailey, A.; Grobusch, M.P.; Tami, A. Long-Term Chikungunya Sequelae in Curaçao: Burden, Determinants, and a Novel Classification Tool. Journal of Infectious Diseases 2017, 216, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Marimoutou, C.; Ferraro, J.; Javelle, E.; Deparis, X.; Simon, F. Chikungunya Infection: Self-Reported Rheumatic Morbidity and Impaired Quality of Life Persist 6 Years Later. Clinical Microbiology and Infection 2015, 21, 688–693. [Google Scholar] [CrossRef]
- Duvignaud, A.; Fianu, A.; Bertolotti, A.; Jaubert, J.; Michault, A.; Poubeau, P.; Fred, A.; Méchain, M.; Gaüzère, B.A.; Favier, F.; et al. Rheumatism and Chronic Fatigue, the Two Facets of Post-Chikungunya Disease: The TELECHIK Cohort Study on Reunion Island. Epidemiol Infect 2018, 146, 633–641. [Google Scholar] [CrossRef]
- Gérardin, P.; Fianu, A.; Malvy, D.; Mussard, C.; Boussaïd, K.; Rollot, O.; Michault, A.; Gaüzere, B.A.; Bréart, G.; Favier, F. Perceived Morbidity and Community Burden after a Chikungunya Outbreak: The TELECHIK Survey, a Population-Based Cohort Study. BMC Med 2011, 9. [Google Scholar] [CrossRef] [PubMed]
- Manimunda, S.P.; Vijayachari, P.; Uppoor, R.; Sugunan, A.P.; Singh, S.S.; Rai, S.K.; Sudeep, A.B.; Muruganandam, N.; Chaitanya, I.K.; Guruprasad, D.R. Clinical Progression of Chikungunya Fever during Acute and Chronic Arthritic Stages and the Changes in Joint Morphology as Revealed by Imaging. Trans R Soc Trop Med Hyg 2010, 104, 392–399. [Google Scholar] [CrossRef]
- Lozano-Parra, A.; Herrera, V.; Calderón, C.; Badillo, R.; Gélvez Ramírez, R.M.; Estupiñán Cárdenas, M.I.; Lozano Jiménez, J.F.; Villar, L.Á.; Rojas Garrido, E.M. Chronic Rheumatologic Disease in Chikungunya Virus Fever: Results from a Cohort Study Conducted in Piedecuesta, Colombia. Tropical Medicine and Infectious Disease 2024, Vol. 9, Page 247 2024, 9, 247. [Google Scholar] [CrossRef]
- Moro, M.L.; Grilli, E.; Corvetta, A.; Silvi, G.; Angelini, R.; Mascella, F.; Miserocchi, F.; Sambo, P.; Finarelli, A.C.; Sambri, V.; et al. Long-Term Chikungunya Infection Clinical Manifestations after an Outbreak in Italy: A Prognostic Cohort Study. Journal of Infection 2012, 65, 165–172. [Google Scholar] [CrossRef]
- Gérardin, P.; Fianu, A.; Michault, A.; Mussard, C.; Boussaïd, K.; Rollot, O.; Grivard, P.; Kassab, S.; Bouquillard, E.; Borgherini, G.; et al. Predictors of Chikungunya Rheumatism: A Prognostic Survey Ancillary to the TELECHIK Cohort Study. Arthritis Res Ther 2013, 15, R9. [Google Scholar] [CrossRef]
- Valdés-López, J.F.; Fernandez, G.J.; Urcuqui-Inchima, S. Synergistic Effects of Toll-Like Receptor 1/2 and Toll-Like Receptor 3 Signaling Triggering Interleukin 27 Gene Expression in Chikungunya Virus-Infected Macrophages. Front Cell Dev Biol 2022, 10, 812110. [Google Scholar] [CrossRef]
- Schwartz, O.; Albert, M.L. Biology and Pathogenesis of Chikungunya Virus. Nature Reviews Microbiology 2010 8:7 2010, 8, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Valdés-López, J.F.; Fernandez, G.J.; Urcuqui-Inchima, S. Interleukin 27 as an Inducer of Antiviral Response against Chikungunya Virus Infection in Human Macrophages. Cell Immunol 2021, 367. [Google Scholar] [CrossRef] [PubMed]
- Hoarau, J.J.; Jaffar Bandjee, M.C.; Krejbich Trotot, P.; Das, T.; Li-Pat-Yuen, G.; Dassa, B.; Denizot, M.; Guichard, E.; Ribera, A.; Henni, T.; et al. Persistent Chronic Inflammation and Infection by Chikungunya Arthritogenic Alphavirus in Spite of a Robust Host Immune Response. The Journal of Immunology 2010, 184, 5914–5927. [Google Scholar] [CrossRef] [PubMed]
- de Brito, M.S.A.G.; de Marchi, M.S.; Perin, M.Y.; Côsso, I. da S.; Bumlai, R.U.M.; Júnior, W.V. da S.; Prado, A.Y.M.; da Cruz, T.C.D.; Avila, E.T.P.; Damazo, A.S.; et al. Inflammation, Fibrosis and E1 Glycoprotein Persistence in Joint Tissue of Patients with Post-Chikungunya Chronic Articular Disease. Rev Soc Bras Med Trop 2023, 56, e0278-2023. [Google Scholar] [CrossRef]
- Dupuis-Maguiraga, L.; Noret, M.; Brun, S.; Le Grand, R.; Gras, G.; Roques, P. Chikungunya Disease: Infection-Associated Markers from the Acute to the Chronic Phase of Arbovirus-Induced Arthralgia. PLoS Negl Trop Dis 2012, 6. [Google Scholar] [CrossRef]
- Lozano-Parra, A.; Herrera, V.; Urcuqui-Inchima, S.; Ramírez, R.M.G.; Villar, L.Á. Acute Immunological Profile and Prognostic Biomarkers of Persistent Joint Pain in Chikungunya Fever: A Systematic Review. Yale J Biol Med 2024, 97, 473. [Google Scholar] [CrossRef]
- Carabali, M.; Lim, J.K.; Palencia, D.C.; Lozano-Parra, A.; Gelvez, R.M.; Lee, K.S.; Florez, J.P.; Herrera, V.M.; Kaufman, J.S.; Rojas, E.M.; et al. Burden of Dengue among Febrile Patients at the Time of Chikungunya Introduction in Piedecuesta, Colombia. Tropical Medicine & International Health 2018, 23, 1231–1241. [Google Scholar] [CrossRef]
- Estupiñán Cardenas, M.I.; Rodriguez-Barraquer, I.; Gélvez, R.M.; Herrera, V.; Lozano, A.; Vanhomwegen, J.; Salje, H.; Manuguerra, J.-C.; Cummings, D.A.; Miranda, M.C.; et al. Endemicity and Emergence of Arboviruses in Piedecuesta, Colombia. Am J Trop Med Hyg 2018, 99, 512–512. [Google Scholar]
- Riel, P.L.C.M. van.; Gestel, A.M. van.; Scott, D.L. Eular Handbook of Clinical Assessments in Rheumatoid Arthritis. 2000.
- Dacre, J. The GALS Screen: The Rapid Rheumatological Exam. Medical Journal of Australia 2019, 210, 396–397.e1. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Real Time RT-PCR for Detection of Chikungunya Virus (SOP); Molecular Diagnostics and Research Laboratory, Division of Vector-Borne Diseases, CDC Dengue Branch: San Juan, Puerto Rico, 2014.
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Rudwaleit, M.; Van Der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The Assessment of Spondyloarthritis International Society Classification Criteria for Peripheral Spondyloarthritis and for Spondyloarthritis in General. Ann Rheum Dis 2011, 70, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Ann Rheum Dis 2019, 78, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- van Riel, P.L.C.M.; van Gestel, A.M.; Scott, D.L. EULAR Handbook of Clinical Assessments in Rheumatoid Arthritis: On Behalf of the EULAR Standing Committee for International Clinical Studies Including Therapeutic Trials -ESCISIT, 3rd ed.; Van Zuiden Communications B.V: Alphen aan den Rijn, Netherlands, 2004; ISBN 9789075141900. [Google Scholar]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia Criteria and Severity Scales for Clinical and Epidemiological Studies: A Modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Guillot, X.; Ribera, A.; Gasque, P. Chikungunya-Induced Arthritis in Reunion Island: A Long-Term Observational Follow-up Study Showing Frequently Persistent Joint Symptoms, Some Cases of Persistent Chikungunya Immunoglobulin M Positivity, and No Anticyclic Citrullinated Peptide Seroconversion after 13 Years. The Journal of Infectious Diseases ® 2020, 222, 1740–1744. [Google Scholar] [CrossRef]
- Valdés-López, J.F.; Hernández-Sarmiento, L.J.; Tamayo-Molina, Y.S.; Velilla-Hernández, P.A.; Rodenhuis-Zybert, I.A.; Urcuqui-Inchima, S. Interleukin 27, like Interferons, Activates JAK-STAT Signaling and Promotes pro-Inflammatory and Antiviral States That Interfere with Dengue and Chikungunya Viruses Replication in Human Macrophages. Front Immunol 2024, 15. [Google Scholar] [CrossRef]
- Valdés-López, J.F.; Hernández-Sarmiento, L.J.; Tamayo-Molina, Y.S.; Velilla-Hernández, P.A.; Rodenhuis-Zybert, I.A.; Urcuqui-Inchima, S. Interleukin 27, like Interferons, Activates JAK-STAT Signaling and Promotes pro-Inflammatory and Antiviral States That Interfere with Dengue and Chikungunya Viruses Replication in Human Macrophages. Front Immunol 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Matsushima, K.; Yang, D.; Oppenheim, J.J. Interleukin-8: An Evolving Chemokine. Cytokine 2022, 153, 155828. [Google Scholar] [CrossRef]
- Teo, T.H.; Lum, F.M.; Lee, W.W.L.; Ng, L.F.P. Mouse Models for Chikungunya Virus: Deciphering Immune Mechanisms Responsible for Disease and Pathology. Immunol Res 2012, 53, 136–147. [Google Scholar] [CrossRef]
- Henderson Sousa, F.; Ghaisani Komarudin, A.; Findlay-Greene, F.; Bowolaksono, A.; Sasmono, R.T.; Stevens, C.; Barlow, P.G. Evolution and Immunopathology of Chikungunya Virus Informs Therapeutic Development. Dis Model Mech 2023, 16. [Google Scholar] [CrossRef]
- Lum, F.M.; Ng, L.F.P. Cellular and Molecular Mechanisms of Chikungunya Pathogenesis. Antiviral Res 2015, 120, 165–174. [Google Scholar] [CrossRef]
- Locke, M.C.; Fox, L.E.; Dunlap, B.F.; Young, A.R.; Monte, K.; Lenschow, D.J. Interferon Alpha, but Not Interferon Beta, Acts Early To Control Chronic Chikungunya Virus Pathogenesis. J Virol 2022, 96. [Google Scholar] [CrossRef] [PubMed]
- Cook, L.E.; Locke, M.C.; Young, A.R.; Monte, K.; Hedberg, M.L.; Shimak, R.M.; Sheehan, K.C.F.; Veis, D.J.; Diamond, M.S.; Lenschow, D.J. Distinct Roles of Interferon Alpha and Beta in Controlling Chikungunya Virus Replication and Modulating Neutrophil-Mediated Inflammation. J Virol 2019, 94. [Google Scholar] [CrossRef]
- Felipe, V.L.J.; Paula A, V.; Silvio, U.I. Chikungunya Virus Infection Induces Differential Inflammatory and Antiviral Responses in Human Monocytes and Monocyte-Derived Macrophages. Acta Trop 2020, 211. [Google Scholar] [CrossRef]
- Gualberto Cavalcanti, N.; MeloVilar, K.; Branco Pinto Duarte, A.L.; Jesus Barreto de Melo Rêgo, M.; Cristiny Pereira, M.; da Rocha Pitta, I.; Diniz Lopes Marques, C.; Galdino da Rocha Pitta, M. IL-27 in Patients with Chikungunya Fever: A Possible Chronicity Biomarker? Acta Trop 2019, 196, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Anshita, D.; Ravichandiran, V. MCP-1: Function, Regulation, and Involvement in Disease. Int Immunopharmacol 2021, 101, 107598. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb Perspect Biol 2014, 6, a016295. [Google Scholar] [CrossRef]
- Jones, S.A.; Takeuchi, T.; Aletaha, D.; Smolen, J.; Choy, E.H.; McInnes, I. Interleukin 6: The Biology behind the Therapy. Considerations in Medicine 2018, 2, 2–6. [Google Scholar] [CrossRef]
- Chen, W.; Foo, S.S.; Sims, N.A.; Herrero, L.J.; Walsh, N.C.; Mahalingam, S. Arthritogenic Alphaviruses: New Insights into Arthritis and Bone Pathology. Trends Microbiol 2015, 23, 35–43. [Google Scholar] [CrossRef]
- Avila-Trejo, A.M.; Rodríguez-Páez, L.I.; Alcántara-Farfán, V.; Aguilar-Faisal, J.L. Multiple Factors Involved in Bone Damage Caused by Chikungunya Virus Infection. Int J Mol Sci 2023, 24, 13087. [Google Scholar] [CrossRef]
- Chang, A.; Tritsch, S.; Reid, St.; Martins, K.; Encinales, L.; Pacheco, N.; Amdur, R.; Porras-Ramirez, A.; Rico-Mendoza, A.; Li, G.; et al. The Cytokine Profile in Acute Chikungunya Infection Is Predictive of Chronic Arthritis 20 Months Post Infection. Diseases 2018, 6, 95. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the case-control selection.
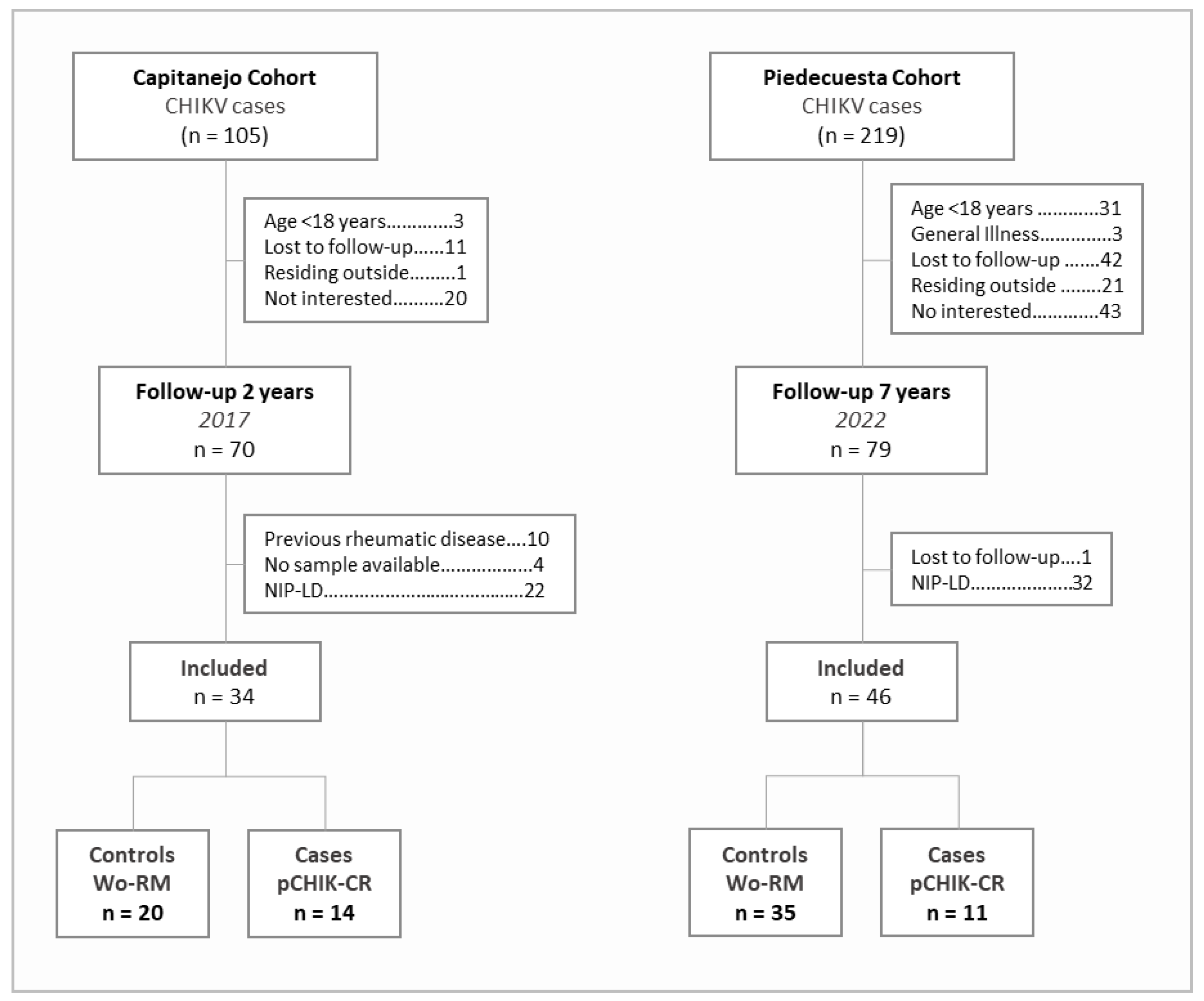
Figure 2.
Heatmap of partial correlations (adjusted for age and sex) between the immunological factors quantified at the baseline visit. * p<0.05.
Figure 2.
Heatmap of partial correlations (adjusted for age and sex) between the immunological factors quantified at the baseline visit. * p<0.05.
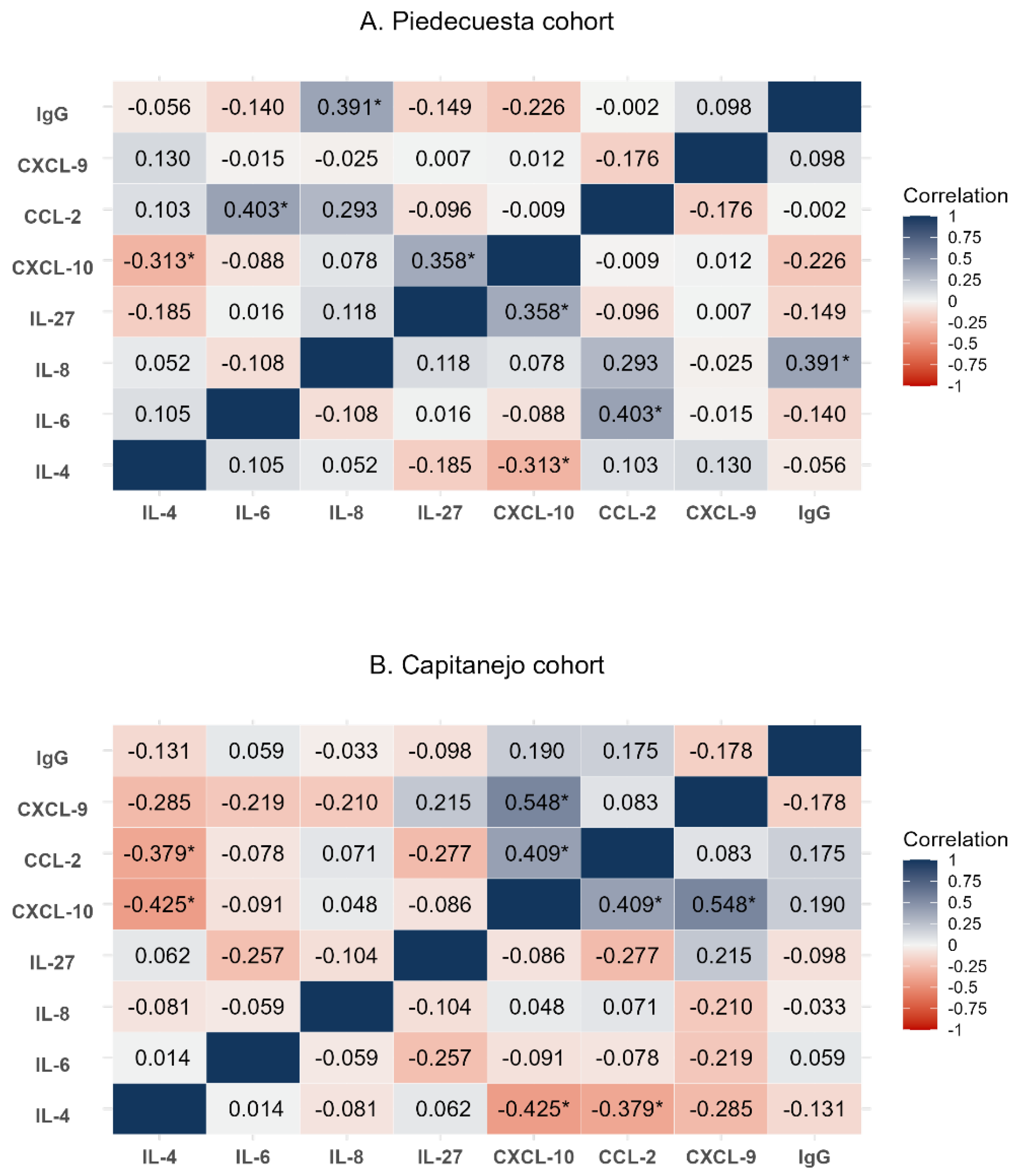
Figure 3.
Scatter plot of immunological factors concentrations quantified at the baseline visit, stratified by case-control status and cohort. The Capitanejo cohort included 14 cases (pCHIK-CR) and 20 controls (Wo-RM), while the Piedecuesta cohort included 11 cases of pCHIK-CR and 35 controls Wo-RM. Horizontal red lines represent median concentrations.
Figure 3.
Scatter plot of immunological factors concentrations quantified at the baseline visit, stratified by case-control status and cohort. The Capitanejo cohort included 14 cases (pCHIK-CR) and 20 controls (Wo-RM), while the Piedecuesta cohort included 11 cases of pCHIK-CR and 35 controls Wo-RM. Horizontal red lines represent median concentrations.
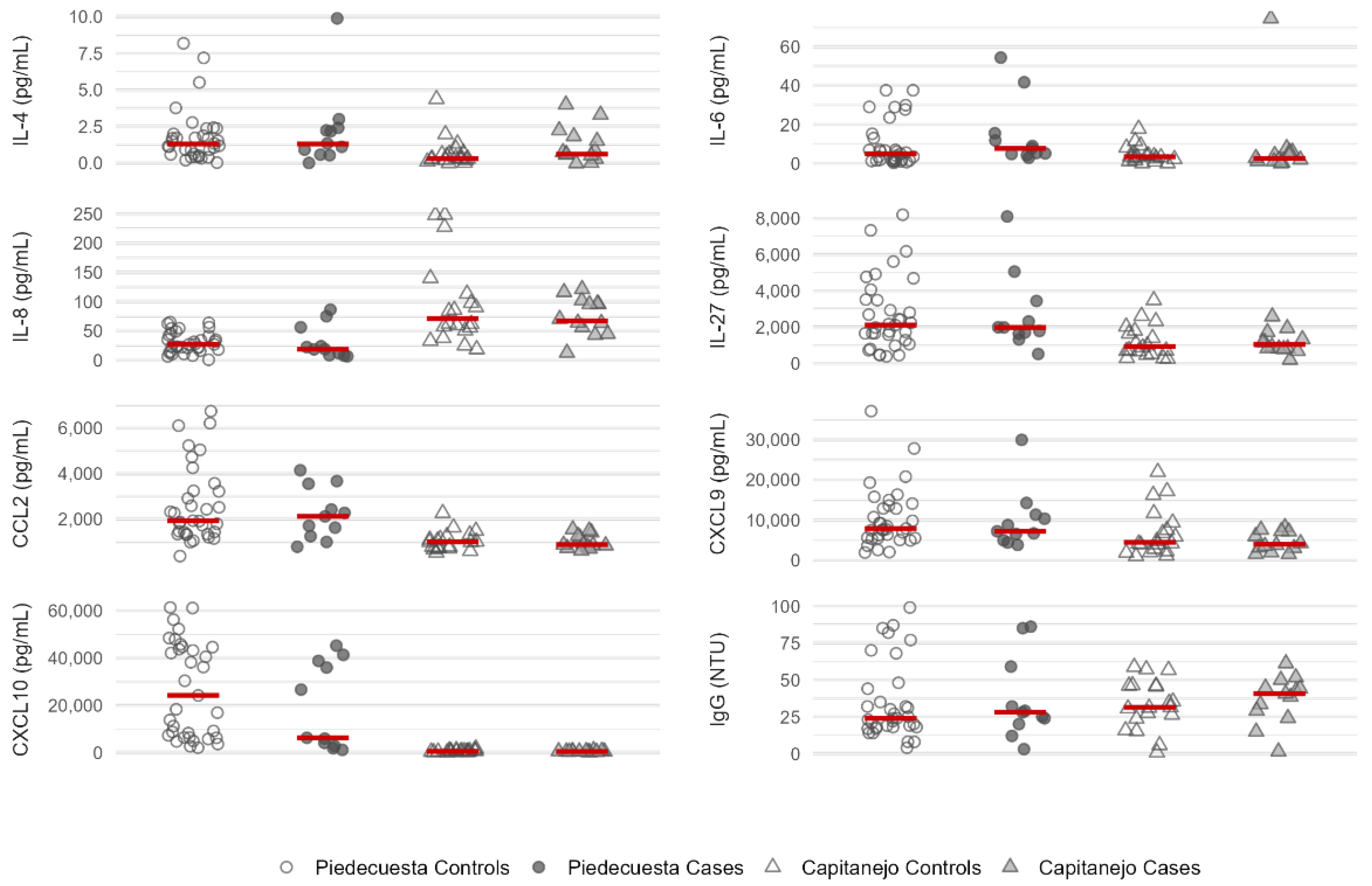

Table 1.
Demographic characteristics of CHIKV cases at the baseline visit, by case-control status.
| Characteristic, n (%) | Cases | Controls | Total | p |
|---|---|---|---|---|
| Piedecuesta cohort | ||||
| Female | 9 (81.2) | 14 (40.0) | 23 (50.0) | 0.035 |
| Age (years) | 45.0 [15.0] | 30.0 [20.0] | 33.5 [19.0] | 0.001 |
| Medical history | ||||
| Diabetes mellitus | 0 (0.0) | 1 (2.9) | 1 (2.2) | 1.000 |
| Cardiovascular disease | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| Articular disease | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| No medical history | 11 (100.0) | 34 (97.1) | 45 (97.8) | 1.000 |
| Capitanejo cohort | ||||
| Female | 12 (85.7) | 13 (65.0) | 25 (73.5) | 0.250 |
| Age (years) | 60.2 [13.3] | 48.8 [27.3] | 54.0 [25.5] | 0.150 |
| Medical history | ||||
| Diabetes mellitus | 0 (0.0) | 1 (10.0) | 1 (7.1) | 1.000 |
| Cardiovascular disease | 1 (25.0) | 3 (27.3) | 4 (20.6) | 1.000 |
| Articular disease | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| No medical history | 13 (92.9) | 17 (85.0) | 30 (88.2) | 1.000 |
The Capitanejo cohort included 14 cases (post-CHIKV chronic rheumatism, pCHIK-CR) and 20 controls (without rheumatic manifestations, Wo-RM), while the Piedecuesta cohort included 11 cases of pCHIK-CR and 35 controls Wo-RM. Figures in each cell represent medians [first and third quartiles] and absolute (relative) frequencies.
Table 2.
Immunological factors quantified during the baseline visit by case-control status.
| Biomarker (pg/mL) | Cases | Controls | Total | p | Median Difference | ||
|---|---|---|---|---|---|---|---|
| Absolute | Relative (%) | ||||||
| Piedecuesta cohort | |||||||
| IL-4 | 1.3 [0.6 - 2.4] | 1.3 [0.6 - 2.0] | 1.3 [0.6 -2.2] | 0.661 | 0.0 | 0.0 | |
| IL-6 | 7.7 [4.8 - 15.5] | 4.9 [1.5 - 15.2] | 5.4 [1.9 – 15.2] | 0.102 | 2.8 | 57.1 | |
| IL-8/CXCL-8 | 19.1 [8.8 - 56.4] | 27.3 [18.4 – 42.8] | 23.4 [16.4 – 42.8] | 0.421 | -8.1 | -29.9 | |
| IL-27 | 1,978.0 [1,631.9 - 3,435.9] | 2,104.3 [1,052.3 - 3,513.3] | 1,981.8 [1,307.3 – 3,481.2] | 0.867 | -126.3 | -6.0 | |
| CCL-2 | 2,119.3 [1,246.8 - 3,552.7] | 1,929.9 [1,339.7 - 3,290.0] | 2,024 [1,339.7 – 3,290.0] | 0.598 | 189.4 | 9.8 | |
| CXCL-9 | 7,230.7 [4,974.4 - 11,349.4] | 7,926.7 [5,518.5 - 13,596.0] | 7,836.9 [5,518.5 – 12,908.3] | 0.709 | -696.0 | -8.8 | |
| CXCL-10 | 6,333.5 [2,862.6 - 38,829.6] | 24,223.1 [6,484.3 - 44,777.8] | 21,293.3 [6,329.2 – 43,769.0] | 0.082 | -17,889.6 | -73.9 | |
| IgG* | 28.0 [20.0 - 59.0] | 24.0 [18.0 - 44.0] | 25.0 [18.0 – 44.0] | 0.699 | 4.0 | 16.7 | |
| Capitanejo cohort | |||||||
| IL-4 | 0.6 [0.3 - 1.8] | 0.3 [0.2 - 0.9] | 0.6 [0.2 – 1.0] | 0.268 | 0.3 | 116.7 | |
| IL-6 | 2.6 [1.2 - 5.9] | 3.4 [1.8 - 5.6] | 3.2 [1.4 – 5.9] | 0.674 | -0.8 | -23.5 | |
| IL-8/CXCL-8 | 67.4 [45.2 - 96.9] | 71.2 [53.4 - 105.8] | 67.4 [50.9 – 97.9] | 0.806 | -3.8 | -5.3 | |
| IL-27 | 1,036.4 [814.7 - 1,379.1] | 927.7 [579.2 - 1,907.2] | 951.7 [680.6 – 1,715.5] | 0.834 | 108.7 | 11.7 | |
| CCL-2 | 878.9 [771.2 - 1,259.6] | 1,002.8 [733.9 - 1,187.1] | 991.0 [737.7 – 1,248.1] | 0.944 | -124.0 | -12.4 | |
| CXCL-9 | 4,032.6 [3,046.9 - 7,170.6] | 4,479.4 [2,518.5 - 10,558.0] | 4,226.0 [2,813.5 – 7,558.3] | 0.441 | -446.8 | -10.0 | |
| CXCL-10 | 522.9 [390.8 - 631.6] | 589.0 [373.0 - 858.4] | 536.4 [388.2 – 733.3] | 0.382 | -66.1 | -11.2 | |
| IgG* | 40.7 [29.1 – 44.7] | 31.4 [23.7 - 46.1] | 34.9 [25.2 – 46.0] | 0.632 | 9.3 | 29.6 | |
The Capitanejo cohort included 14 cases (post-CHIKV chronic rheumatism, pCHIK-CR) and 20 controls (without rheumatic manifestations, Wo-RM), while the Piedecuesta cohort included 11 cases of pCHIK-CR and 35 controls Wo-RM. Figures in each cell represent medians [first and third quartiles]. * Expressed in NovaTec Units (NTU).
Table 3.
Association between pro-inflammatory factors and post-CHIKV chronic rheumatism.
| Biomarker | Crude OR (CI 95%) | Adjusted OR (CI 95%) |
|---|---|---|
| IL-8/CXCL-8 (pg/mL) * | ||
| <35.7 | 0.90 (0.81 – 0.98) | 0.85 (0.74 - 0.99) |
| ≥35.7 | 1.09 (1.01 – 1.18) | 1.09 (0.97 - 1.22) |
| Age | - | 1.13 (1.01 - 1.27) |
| Sex | - | 0.13 (0.14 - 1.07) |
| Disease onset | - | 0.47 (0.21 - 1.05) |
| HL | 0.634 | 0.875 |
| AUC | 0.75 (IC95%: 0.59 - 0.91) | 0.92 (IC95%: 0.85 - 1.00) |
| CXCL-10 (100 pg/mL) * | ||
| <36,800 | 1.00 (0.99 - 1.01) | 1.01 (0.99 - 1.02) |
| ≥36,800 | 0.98 (0.96 - 1.01) | 0.94 (0.90 - 0.99) |
| Age | - | 1.18 (1.03 - 1.35) |
| Sex | - | 0.13 (0.02 - 1.14) |
| HL | 0.502 | 0.830 |
| AUC | 0.57 (IC95%: 0.38 - 0.75) | 0.90 (IC95%: 0.80 - 0.99) |
| CXCL-9 (100 pg/mL) † | ||
| <2,000 | 1.19 (0.84 - 1.69) | 0.95 (0.60 - 1.50) |
| ≥2,000 | 0.98 (0.96 - 1.00) | 0.96 (0.93 - 0.99) |
| Age | - | 1.11 (1.01 - 1.22) |
| Sex | - | 0.21 (0.01 - 2.90) |
| Disease onset | - | 0.96 (0.91 - 1.02) |
| HL | 0.439 | 0.408 |
| AUC | 0.61 (0.42 - 0.80) | 0.84 (0.70 - 0.97) |
* Piedecuesta cohort: 11 cases of pCHIK-CR and 35 controls of Wo-RM. † Capitanejo cohort: 14 cases of pCHIK-CR and 20 controls Wo-RM. HL: p-value corresponding to the Hosmer-Lemeshow goodness-of-fit test. AUC: Area under the curve.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



