
Submitted:
18 September 2024
Posted:
19 September 2024
You are already at the latest version
Abstract
This study aimed to determine the incidence of post-chikungunya chronic rheumatism (pCHIK-CR) its impact on quality of life (QoL) and chronic fatigue in adult seven years after the 2014-2015 CHIKV outbreak in Piedecuesta, Colombia. We evaluated 78 adults (median age: 30 years, IQR: 21.0; women 60.3%) with confirmed CHIKV infection. In 2022, participants underwent a GALS examination and completed surveys on disability, stiffness, health status, and fatigue. A rheumatologist evaluated patients who reported arthralgia, morning stiffness, and abnormal GALS examination. Chronic fatigue was defined as fatigue persisting for over six months. Seven years after infection, 14.1% of participants were classified as pCHIK-CR cases, 41.0% as having non-inflammatory pain likely degenerative (NIP-LD), and 44.9% without rheumatic disease (Wo-RM). Patients with pCHIK-CR and NIP-LD exhibited significantly worse QoL compared to Wo-RM cases. Chronic fatigue prevalence increased from 8.6% in Wo-RM patients to 25.0% in NIP-LD and 54.6% in pCHIK-CR cases. This study implemented a comprehensive clinical as-sessment to objectively estimate and characterize the incidence of chronic rheumatological disease attributed to CHIKV infection. One in seven cases with CHIKV infection develops pCHIK-CR, which impacts both QoL and chronic fatigue. This study contributes to understanding the burden of these arboviruses in the medium term.
Keywords:
Chikungunya
; chronic rheumatism
; rheumatic disease
; fatigue
; quality of life
1. Introduction
The emergence of chikungunya virus (CHIKV) in the Americas is recent, causing about 3.7 million cases of infection between December 2013 and June 2023 [1]. In 2015, Colombia reported the highest number of infections in the Americas, with 275,907 cases [2]. However, a study conducted in 2017 in five Colombian cities found that CHIKV seroprevalence ranged from 9.0% to 73.0%, highlighting the heterogeneity in virus attack rates and susceptibility in specific populations to its reemergence [3,4].
Chikungunya fever is characterized by joint pain, which can sometimes be long-lasting and incapacitating. In addition to fever and joint pain, symptoms such as myalgia, headache, nausea, fatigue, and rash may appear during the acute stage (5-7 days) of the disease [5,6]. While most patients recover, some experience musculoskeletal pain, disabling joint pain, and fatigue for more than three months and even years [7]. Different studies have found that post-CHIKV rheumatologic manifestations occur in 17.0% to 53.7% of cases, with variations reflecting differences in follow-up periods and the definitions for these complications [8,9,10]. Factors such as age over 45 years [11], female sex [12], history of joint pain [12], and high levels of IgG anti-CHIKV antibodies [11,12] predispose patients to the chronic form of the disease.
Post-CHIKV chronic rheumatism (pCHIK-CR) was first described in 1979 [13]. However, even after 10 years of CHIKV emergence in America and the efforts to characterize symptoms during the chronic phase of the disease, there is still no standardized and reproducible definition of pCHIK-CR. A proposed definition of pCHIK-CR is the persistence of joint and extra-articular symptoms for more than three months after the onset of CHIKV disease or the development of specific immune-mediated inflammatory pathology during follow-up [14,15].
The persistence of joint symptoms could impact the quality of life (QoL) [16,17,18,19]. This impact appears to be long-lasting and affects both mental and physical aspects of health, particularly concerning rheumatological manifestations [20]. Additionally, patients who recover from CHIKV tend to have a better quality of life compared to those with persistent symptoms [19]. Chronic fatigue is increasingly recognized as a symptom accompanying post-chikungunya rheumatic findings [21,22,23]. It has even been suggested that a significant proportion of musculoskeletal pain may be due to chronic fatigue rather than the primary rheumatic disease [21].
Considering the above, this study aimed to estimate the incidence of pCHIK-CR in adult patients seven years after the 2014-2015 CHIKV outbreak in Piedecuesta, Colombia. Additionally, we sought to determine the impact on quality of life and the presence of chronic fatigue associated with pCHIK-CR. Finally, we evaluated the effectiveness of the Health Assessment Questionnaire disability index (HAQ-DI) and the handgrip strength test for identifying pCHIK-CR in the chronic phase.
2. Materials and Methods
We used clinical and epidemiological data from two prospective cohort studies to identify cases of CHIKV infection, assessed the incidence of post-chikungunya chronic rheumatism (pCHIK-CR), and evaluated its impact on the quality of life and its association with chronic fatigue. These cohorts were initially designed to determine the etiology of acute febrile syndrome. This section describes both source studies, the procedure for data harmonization, the eligibility criteria, the recontacting protocol, participants' follow-up, outcome definitions, and the analytical approach.
2.1. Source Studies
We identified acute CHIKV infection cases from two prospective cohorts conducted during the 2014-2015 outbreak in Piedecuesta, Colombia, as described below:
Passive surveillance cohort: This study was assembled in 2014 and included 839 patients aged 1-55 years who sought health care due to an unspecified acute febrile syndrome of less than or equal to a week of duration. The syndrome’s etiology was determined upon inclusion, and participants underwent a follow-up evaluation 7-14 days afterward [24].
Active surveillance cohort: This study was assembled in 2015 and included 2,000 healthy children aged 2-15 years and 400 healthy adults who were identified through a convenience sampling from the community [4]. Participants underwent biweekly telephone follow-ups over 3.5 years to identify cases of acute febrile illness. They were evaluated within a week of the disease’s onset to determine etiology and followed 7-14 days later.
In both studies, the diagnosis of CHIKV infection was determined by a positive result in the NovaLisa® IgG or IgM ELISA tests or the reverse transcription polymerase chain reaction (RT-qPCR) test [25]. We adopted this diagnostic approach because the virus was newly introduced to the population during the study period. We identified a total of 219 CHIKV infection cases: 188 from the passive surveillance cohort and 31 from the active surveillance cohort.
2.2. Data Harmonization
To harmonize the data from both cohorts, we initially reviewed their data dictionaries to assess the availability of relevant variables and their definitions. This process aimed to evaluate semantic reconciliation between the dictionaries and to establish harmonization rules. Finally, we syntactically transformed demographic and clinical variables to ensure they were suitable for data analysis.
2.3. Eligibility and Re-Contact
In this analysis, we included adult participants (over 18 years old) who experienced an acute febrile illness and had a confirmed diagnosis of CHIKV infection. We excluded individuals with a history of any general physical or mental illness, those with any rheumatic disease diagnosed before the CHIKV infection, as well as those who did not consent to share their data or samples for future studies as per the informed consent obtained by the source cohorts. Eligible participants underwent a comprehensive re-contact protocol that included at least three phone calls (two on weekdays and one on weekends) made to every available telephone number in the databases, text messages through a short message service (SMS), a search on social networks (Facebook and Instagram), and at least an attempt to establish direct contact at their address of residency. After re-contacting and updating residency information, we excluded participants who resided outside the Metropolitan Area of Bucaramanga and those not interested in further evaluation.
2.4. Follow-Up
We invited eligible participants who were successfully re-contacted to attend a follow-up visit between September and December 2022. During this visit, participants provided informed consent and underwent a comprehensive physical examination focused on musculoskeletal health using the GALS methodology (Gait, Arm, Legs, Spine) [26,27], conducted by a physician who had been trained by a rheumatologist. Participants also performed a handgrip strength test following the guidelines of Roberts et al. [28] and answered the following self-reported questionnaires to assess their health status: the Health Assessment Questionnaire Disability Index (HAQ-DI) [29], the Musculoskeletal Stiffness Questionnaire (MSQ) [30], the SF-36v2 Health and Wellness Questionnaire [31], and the Fatigue Severity Scale (FSS) [32].
A certified rheumatologist conducted a second, independent evaluation on those participants who had any of the following findings in the first visit (median time between visits=10 days): a report of arthralgia in one or more joints or morning stiffness lasting more than 30 minutes, an abnormal GALS examination, signs of joint swelling, enthesopathy or spondyloarthropathy non-trauma-related. The rheumatologist also evaluated a random sample of the participants with a normal first examination to estimate the rate of false negative results. Finally, we determined the rheumatoid factor (RF), C-reactive protein (CRP), antinuclear antibodies (ANAs), anti-cyclic citrullinated peptide (anti-CCP), and HLA-27, as well as performed magnetic resonance imaging, bilateral neuro conduction, and electromyography tests in selected patients per request of the rheumatologist.
2.5. Outcomes
2.5.1. Post-CHIK Chronic Rheumatism (pCHIK-CR)
Post-CHIK chronic rheumatism (pCHIK-CR) was defined as an abnormal GALS examination with persistence of joint and extra-articular symptoms for more than three months after the onset of CHIKV disease or the development of a specific immune-mediated inflammatory pathology during follow-up [14,15]. We categorized patients with pCHIK-CR based on the following definitions: rheumatoid arthritis (according to ECR/EULAR 2010 criteria) [33], axial or peripheral spondylarthritis (based on ASAS 2011 criteria) [34], systemic lupus erythematosus (following ACR/EULAR 2019 criteria) [35], post-viral arthritis (confirmed by joint pain and fluctuation of joint margins in one or more joints) [36], post-viral arthralgia (documented by joint pain at the margin level without swelling) [36], and soft tissue rheumatism (identified by the presence of tenosynovitis, bursitis, fasciitis, noninflammatory localized pain, enthesitis, or fibromyalgia based on ACR 2011 criteria) [37]. We classified participants with an abnormal GALS examination but not meeting the pCHIK-CR criteria as non-inflammatory pain likely degenerative (NIP-LD) cases. Participants with a normal GALS examination who did not meet the pCHIK-CR criteria were classified as cases without rheumatic manifestations (Wo-RM).
2.5.2. Quality of Life (QoL)
We evaluated the QoL using the SF-36v2™ questionnaire [38]. This questionnaire includes 36 items assessing eight domains of health status: physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role, and mental health. These domains are classified into two main components: mental and physical [39,40,41]. The SF-36 score ranges from 0 to 100, with higher scores indicating better quality of life. We categorized the scores for each domain and component into three levels based on standardized data from the general US population [42]: ≤40 as “Well Below”; between 40 and 44 as “Below”; and ≥45 as “Same or Better” than the mean population score [42]. We used the PROCoRE Smart Measurement® System software for data analysis and defined impaired QoL if any component (mental or physical) was classified into the “Well Below” category.
2.5.3. Chronic Fatigue (CF)
We used the Fatigue Severity Scale (FSS) to evaluate fatigue [32,43]. This scale uses a Likert-type format with seven levels to assess physical, social, and motivational dimensions of fatigue, where higher scores indicate greater severity. We defined fatigue as a total FSS score greater or equal to 36 points [44], and chronic fatigue (CF) in participants reporting fatigue lasting for more than 6 months [21].
2.6. Data Analysis
We described continuous variables by estimating the mean and standard deviation (SD) or the median and interquartile range [IQR] for those not normally distributed, according to the Shapiro-Wilk test. We calculated their absolute and relative frequencies (percentages) for discrete variables. We contrasted means and medians between groups using a student’s t-test or analysis of variance (ANOVA) and the sum of ranks test, respectively, and differences in proportions by using the chi-square test and, alternatively, the Fisher's exact test whenever the expected counts in contingency tables were less than five. We adjusted for multiple comparisons using the Bonferroni correction. The GALS examination's positive and negative predictive values and 95% confidence intervals (95%CI) for pCHIK-CR, as determined by the rheumatologist, were estimated using the exact binomial method. We estimated the correlation between the HAQ-DI and MSQ scales using Spearman's correlation coefficient (rs) and their agreement (dichotomized around their medians) with patients’ classification (the extreme classes: pCHIK-CR versus Wo-RM) using Cohen’s Kappa. Finally, we evaluated the association between QoL and chronic fatigue with joint involvement (pCHIK-CR and NIP-LD versus Wo-RM) by using multinomial logistic regression, adjusting for age, sex, and comorbidities. The analyses were conducted using Stata version 12.0 (Stata Corp.).
3. Results
We identified 219 cases of CHIKV infection from both data sources that occurred between November 2014 and December 2015, of which 185 (85.5%) were eligible for re-contacting (Figure 1). Upon completing the protocol of re-contact, 42 (22.7%) patients could not be reached, 21 (11.4%) reported residing outside the Metropolitan Area of Bucaramanga, and 43 (23.2%) declined the invitation to participate. Only one of the enrolled participants declined to attend the follow-up evaluation; therefore, the study's final sample consisted of 78 individuals. Not enrolled participants were younger than those who could be contacted and accepted to participate (24.0 versus 35.0, p=0.001), but the sex distribution was comparable (p=0.114). The median age of the sample at CHIKV symptoms’ onset was 30.0 years (IQR=21.0 years) and included 47 women (60.3%). The mean duration of the symptoms during the acute phase of the infection was 2.8 days (SD=1.5 days): 92.3% and 97.5% of the cases reported arthralgia and fatigue, respectively. None of the participants reported a medical history of articular disease before the CHIKV infection; however, 1.3% and 3.9% had prevalent diagnoses of diabetes and cardiovascular disease, respectively (Table 1).
The median time between the disease’s onset and the follow-up evaluation was 7.7 years, at which 14.1% (95%CI: 7.3 – 23.8) of participants were classified as cases of pCHIK-CR, 41.0% (95%CI: 30.0 – 52.7) as cases of NIP-LD, and 44.9% (95%CI: 33.6 - 56.6) did not have any clinical manifestation of rheumatic disease (Wo-RM; Table 2). Among pCHIK-CR patients, the three most frequent clinical patterns that the rheumatologist identified were post-viral oligo/polyarthritis (36.4%), post-viral arthralgia (27.2%), and fibromyalgia (18.2%). Most pCHIK-CR cases reported arthralgia (72.7%), with a median pain scale score of 7.0 (IQR=2.5). The knees (62.5%), hands (50.0%), and feet (37.5%) were the most affected joints. Additionally, 27.3% of pCHIK-CR cases reported stiffness, with a median MSQ score of 8.0 (IQR=5.0). The GALS screening evaluation's estimated positive and negative predictive values were 25.6% (95% CI: 13.5 – 41.2) and 100.0% (95% CI: 47.8 – 100.0), respectively, compared to the rheumatologist’s criterion.
Patients with pCHIK-CR and NIP-LD were younger and predominantly female compared to Wo-RM cases (Table 3). Joint stiffness and swelling were more often reported by cases of pCHIK-CR than NIP-LD and Wo-RM; however, cases of NIP-LD showed the highest frequency of gait limitation. There was no difference between groups in terms of comorbidities or obesity. Still, patients with pCHIK-CR reported higher dexamethasone use (at any time post-CHIKV infection) than cases of NIP-LD and Wo-RM: 18.2% versus 3.1% and 0.0%, respectively. Although the grip strength was similar in patients with pCHIK-CR and NIP-LD, it was significantly lower compared to Wo-RM cases: 19.1 kg, 18.1 kg, and 32.1 kg, respectively. The median MSQ and HAQ-DI scores showed statistically significant gradients across groups (with the lowest values observed among Wo-RM cases) and a positive correlation (rs=0.69, p<0.001). Once dichotomized around their medians, the HAQ-DI scale showed a stronger concordance with the study outcome (considering the extreme classes: pCHIK-CR versus Wo-RM) than the MSQ scale (kappa=0.54, p<0.001; and kappa=0.32, p=0.013, respectively).
Figure 2 illustrates the quality of life (QoL) assessed with the SF-36 questionnaire across groups of participants according to the pattern of chronic rheumatism. Patients with pCHIK-CR and NIP-LD showed significantly lower median scores across the eight domains of the SF-36 compared to Wo-RM cases (Table 2). Participants with affected QoL were significantly more likely to have pCHIK-CR than Wo-RM (adjusted OR=11.4, 95%CI: 1.8 – 73.7). Similarly, affected QoL was associated with increased odds of being a NIP-LD case than Wo-RM (adjusted OR=6.8, 95% CI: 1.8 – 25.3). The prevalence of chronic fatigue gradually increased from 8.6% in patients Wo-RM to 25.0% and 54.6% among NIP-LD and pCHIK-CR cases, respectively. Chronic fatigue was significantly associated with pCHIK-CR (adjusted OR=19.0, 95% CI: 2.46 – 146.42) but not with NIP-LD (adjusted OR=2.92, 95% CI: 0.62 – 13.65) considering Wo-RM as the reference group.

Table 4.
Quality of life and fatigue assessed during the follow-up evaluation, by clinical pattern of chronic rheumatism.
Table 4.
Quality of life and fatigue assessed during the follow-up evaluation, by clinical pattern of chronic rheumatism.
| Assessment | pCHIK-CR (n=11) |
NIP-LD (n=32) |
Wo-RM (n=35) |
p |
|---|---|---|---|---|
| SF-36 | ||||
| Physical component | 46.1 [16.1] a | 43.5 [17.2] b | 56.7 [7.8] | 0.001 |
| Physical functioning | 46.1 [19.1] a | 44.2 [19.1] b | 55.6 [3.8] | 0.000 |
| Physical role | 45.9 [27.0] | 43.7 [18.0] b | 54.9 [13.5] | 0.004 |
| Bodily pain | 42.2 [21.0] a | 38.2 [17.0] b | 55.6 [6.5] | 0.000 |
| General health | 41.3 [19.0] a | 42.0 [20.7] b | 55.6 [11.9] | 0.003 |
| Mental component | 39.8 [16.0] a | 43.2 [13.8] b | 53.0 [13.0] | 0.043 |
| Vitality | 46.7 [8.9] a | 46.7 [8.9] b | 55.6 [11.9] | 0.000 |
| Social functioning | 42.3 [15.0] a | 39.8 [15.0] b | 52.3 [10.0] | 0.006 |
| Emotional role | 35.3 [24.4] a | 38.8 [20.9] b | 56.2 [13.9] | 0.006 |
| Mental health | 45.6 [18.3] a | 43.0 [15.7] | 53.5 [15.7] | 0.014 |
| Impaired QoL, n (%) | 6 (54.6) a | 19 (59.4) b | 5 (14.3) | 0.000 |
| FSS score | 44.0 [21.0] a | 35.5 [33.0] b | 15.0 [22.0] | 0.002 |
| Chronic Fatigue, n (%) | 6 (54.6) a | 8 (25.0) | 3 (8.6) | 0.005 |
The values in square brackets denote the interquartile range [IQR]. pCHIK-CR: Post-CHIK Chronic Rheumatism; NIP-LD: Non-inflammatory pain likely degenerative; Wo-RM: Without rheumatic manifestations. Chronic fatigue was defined as an FSS score ≥ 36 lasting over six months. Quality of life (QoL) impairment was defined as a score ≤ 40 in any component of the SF-36 questionnaire. a P<0.050 for the comparison between pCHIK-CR and Wo-RM. b P<0.050 for the comparison between NIP-LD and Wo-RM. c P<0.050 for the comparison between pCHIK-CR and NIP-LD.
4. Discussion
Based on the harmonization and extension of follow-up of two cohorts of patients diagnosed with CHIKV infection between 2014-2015, we estimated a 14.1% incidence of post-chikungunya chronic rheumatism (pCHIK-CR) after 7.7 years from symptoms onset. The rheumatological evaluation showed a predominance of the post-viral oligo/polyarthritis pattern among pCHIK-CR cases. Additionally, 41.0% and 44.9% of all participants were classified as non-inflammatory pain likely degenerative (NIP-LD) cases and without rheumatic manifestations (Wo-RM), respectively, and no patient fulfilled criteria for rheumatoid arthritis, lupus, or spondyloarthropathy. The Health Assessment Questionnaire-Disability Index (HAQ-DI) and the Musculoskeletal Stiffness Questionnaire (MSQ) were positively correlated; however, the first showed a higher concordance with the pCHIK-CR status than the first. Patients with impaired quality of life (QoL) or chronic fatigue were more likely classified as cases of pCHIK-CR than Wo-RM. Finally, the Gait, Arms, Legs, and Spine (GALS) screening used to identify pCHIK-CR cases by general physicians demonstrated positive and negative predictive values of 25.6% and 100.0%, respectively.
Multiple cohorts have studied the degree of long-term joint involvement in patients with CHIKV infection. Our analysis, based on harmonized data from two of the lengthiest follow-up studies conducted in Latin America, revealed that about one out of seven patients experience pCHIK-CR up to 7.7 years after the acute phase of CHIKV infection; however, comparing this estimate to those from other cohorts is challenging due to methodological heterogeneity across studies and the tendency for these symptoms to fade over time. The latest could be attributable among other reasons to the natural progression of the disease, the susceptibility of the exposed population or the use of treatments aimed at modulating the inflammatory response. For example, in the Reunion Island cohort, which also had a long-term follow-up, the prevalence of chronic inflammatory rheumatism decreased from 45.9% to 10.7% at 3 and 13 years post-CHIKV infection [11,45].
Previous studies conducted in Colombia documented a high prevalence of joint pain or pCHIK-CR within the first and second years after CHIKV infection, with rathes of 58.5% and 25.4%, respectively [46,47]. However, these studies relied on retrospective data or self-reporting through telephone surveys. Similarly, a cohort study conducted in Capitanejo, Colombia, found a 25.0% (95%CI: 14.4 – 38.4) incidence of pCHIK-CR, diagnosed by a rheumatologist, two years post-infection [10]. Despite using the same definition of pCHIK-CR, the incidences could not be directly compared because of the length of follow-up (two years versus seven years).
In addition, a survey conducted in 2017 across five Colombian cities estimated CHIKV seroprevalence rates ranged from 9% to 73% during the outbreak [3,4]. Extrapolating from our results, which indicate a 14.1% incidence of chronic rheumatism seven years after acute infection, we estimate that between 412,872 and 3,356,959 Colombians could be affected by this condition, using the 2015 estimate of 32,614,000 Colombian adults as reference [48].
The clinical characterization of pCHIK-CR cases by trained rheumatologists could help more reliably identify chronic chikungunya disease. Our study showed that the most common clinical patterns of pCHIK-CR were post-viral oligo/polyarthritis, post-viral arthralgia, and fibromyalgia. In the Reunion Island cohort, patients with pCHIK-CR exhibited more severe clinical patterns, such as rheumatoid arthritis, spondylarthritis, and psoriatic arthritis in 64.7%, 23.5%, and 11.8% of the cases, respectively [45]. These differences in patterns and severity across studies could be partially attributed to differences in the CHIKV genotypes that circulated during the outbreaks in Reunion Island and the Americas [49,50]. Studies in animal models had showed that the Asian genotype, which circulated in the Americas, has weaker replication or competitive fitness, and induces moderate joint edema and swelling, with a weaker proinflammatory Th1 response and natural killer cell activity compared to the ECSA genotype [51,52]. These differences should be taken into account, as they might contribute to variations in the clinical evolution observed during the chronic phase in humans. Furthermore, the prevalence of symptoms, chronic inflammatory rheumatism, and other pathologic outcomes may differ in Western, African, or Asian cohorts.
Another factor that could influence rheumatologic findings' incidence and clinical patterns is the baseline susceptibility to inflammatory/autoimmune disorders in different populations. According to epidemiological studies, the prevalence of rheumatologic diseases by the time of the introduction of Chikungunya in Colombia was lower compared to other populations like Europeans, Asians, and even other native American people [53,54]. We should highlight that in our cohorts, none of the cases that met the criteria for pCHIK-CR have undergone treatment with disease-modifying anti-rheumatic drugs (DMARDs). This observation could be due to several reasons. One possibility is that the inflammation shown by these patients after the acute phase is less severe compared to other cohorts with the same diagnosis. On the other hand, we cannot dismiss the possibility that the low use of DMARDs is due to limited access to healthcare services in this population or the lack of evidence-based guidelines for using these types of therapies in this disease.
The involvement of joints, as indicated by higher HAQ-DI scores, showed agreement with pCHIK-CIR when contrasted against Wo-RM cases. This is consistent with previous findings from a cohort of CHIKV-infected patients who did not use DMARDs during 24-month follow-up [55]. Additionally, Watson et al. [56] reported elevated HAQ-DI scores in patients experiencing chronic arthralgia, with a strong correlation between this index and the degree of joint pain and tenderness after three years of follow-up. These findings suggest significant impairment among patients with pCHIK-CR, potentially affecting their ability to perform daily life activities such as dressing, arising, walking, reaching, self-hygiene, and handling objects.
Patients with chronic articular symptoms not only experienced impaired quality of life (QoL) as measured by the SF-36v2 questionnaire but also chronic fatigue. Compared to Wo-RM cases, patients with pCHIK-CR and NIP-LD had lower SF-36 physical and mental component scores; however, there were no significant differences in QoL between pCHIK-CR and NIP-LD cases. An impaired QoL was associated with the outcomes of pCHIK-CR and NIP-LD, when Wo-RM cases were taken as a reference. This finding suggests that CHIKV-induced rheumatologic involvement could lead to disease burden like other non-inflammatory rheumatologic diseases. Previous studies have also shown that patients exposed to CHIKV reported lower SF-36 scores compared with those not exposed, with the impairment of QoL persisting even at 30 and 72 months of follow-up [20,57]. Furthermore, it was reported that CHIKV cases who recovered from rheumatologic symptoms showed a higher SF-36 scores compared to those with persistent joint involvement two years post-infection [18,19].
In our harmonized cohorts of CHIKV-exposed patients, we found that 21.8% of them experienced chronic fatigue during the follow-up examination, with a higher frequency among pCHIK-CR cases. After adjusting for age, sex, and comorbidities, we observed a significant association between chronic fatigue and pCHIK-CR. The literature supports the relationship between acute infections and chronic fatigue in cases such as dengue, Ross River virus, Epstein-Barr virus, and cytomegalovirus, among other [44,58,59]. In addition to the rheumatologic involvement in chronic CHIKV disease, chronic fatigue could reflect other persistent symptoms accompanying this condition [21,22]. Manimunda et al. [22] reported fatigue in 34% of CHIKV infection cases at one month and in 13% at ten month of follow-up, while in the TELECHIK cohort, 34.3% of patients presented idiopathic chronic fatigue [21].
The rheumatologic characterization of patients with chronic CHIKV infection involved two stages. First, a physician trained in musculoskeletal semiology performed an evaluation using the GALS assessment. Then, a trained rheumatologist conducted a second assessment, mimicking typical healthcare pathways. This approach aimed to provide valuable information to identify patients needing specialized assessment rather than just a primary care. Our findings suggest that a primary healthcare approach based on the GALS assessment could effectively rule out most patients without joint involvement, while correctly identifying just one out of four pCHIK-CR cases. Currently, comprehensive healthcare pathways for infectious diseases such as chikungunya succinctly address the management of chronic cases [60]. Therefore, our results could shape recommendations for disease management and improve timely access to therapeutic interventions among patients with CHIKV infection. This is particularly relevant in countries such as Colombia where exclusively circulated the Asian genotype [50,61] with a wide range of attack rates observed during the 2014-2015 outbreak [3,4]. Furthermore, the recent increase in CHIKV cases in the Americas, particularly in Brazil and Paraguay, has been associated with a higher number of deaths attributable to the virus, mainly due to the ECSA genotype [1,62,63].
Our study has some strengths worth mentioning. Firstly, the extended follow-up period allowed us to observe the long-term progression of post-chikungunya chronic rheumatism (pCHIK-CR), Secondly, the involvement of trained rheumatologists in clinical evaluations enhance the accuracy of diagnosing clinical patterns of chronic rheumatism. Thirdly, we assessed the performance of the GALS screening tool, highlighting its potential utility for initial assessments in primary care during the chronic phase of the disease. Our study also has limitations. Firstly, the cases of chikungunya infection were identified in a single municipality in Colombia, which could limit the generalizability of the findings to other populations and epidemiological contexts. Secondly, the fact that the eligible patients were younger than those included might have overestimated the incidence of pCHIK-CR. Thirdly, the total sample size reached, even after harmonizing data from two cohorts, might have limited the power to detect associations and the accuracy of our estimates. Finally, we did not assess the quality of life and chronic fatigue during the acute phase of CHIKV infection, so our findings can only be considered correlational.
5. Conclusions
Our results showed that about one out of seven patients with CHIKV infection developed symptoms and signs compatible with chronic rheumatism (pCHIK-CR) almost eight years post-disease onset. This condition leads to a significant impairment of QoL and a high prevalence of chronic fatigue, comparable to that observed in non-inflammatory rheumatic diseases. The comprehensive approach we implemented for characterizing CHIKV cases could be a valuable tool for assessing the disease burden, facilitating the design of clinical trials, and developing patient management strategies; however, these findings require further replication in the context of larger cohorts.
Author Contributions
A.L.P.: Conceptualization, data curation, formal analysis, investigation, methodology, writing—original draft preparation, writing—review and editing. V.H.: Conceptualization, formal analysis, methodology, writing—original draft preparation, writing—review and editing. C.C.: Methodology. R.B.: Methodology and writing—review and editing. R.M.G.R.: Conceptualization, investigation, methodology, writing—review and editing. M.I.E.C.: Conceptualization, investigation, methodology, writing—review and editing. J.F.L.J.: Investigation, methodology, writing—review and editing. L.A.V.: Conceptualization, investigation, writing—review and editing. E.M.R.G.: Conceptualization, investigation, methodology, supervision, writing—original draft preparation, writing—review and editing, funding acquisition. All authors have read and agreed to the published version of the manuscript.
Funding
The work was supported by Centro de Atención y Diagnóstico de Enfermedades Infecciosas (CDI), Fundación INFOVIDA, Programa de beneficios tributarios I+D+i de Colombia, MINCIENCIAS (Agreement N. 9895-913-93197) and Universidad Industrial de Santander.
Institutional Review Board Statement
The Ethics Committees of the Universidad Industrial de Santander (Acta No. 07, April 23, 2021, and Acta No. 04, March 18, 2023) and the Centro de Atención y Diagnóstico de Enfermedades Infecciosas – C.D.I (Acta 293, July 9, 2022) approved the study protocol.
Informed Consent Statement
Informed consent was obtained from all participants before their inclusion in the study.
Data Availability Statement
The data supporting the findings of this study are available upon reasonable request. Due to privacy and ethical restrictions, the data cannot be made publicly available.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- de Souza, W.M.; Ribeiro, G.S.; S de Lima, S.T.; de Jesus, R.; R Moreira, F.R.; Whittaker, C.; Anice Sallum, M.M.; F Carrington, C. V; Sabino, E.C.; Kitron, U.; et al. Chikungunya: A Decade of Burden in the Americas. The Lancet Regional Health - Americas 2024, 30, 100673. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization; World Health Organization Data - Weekly Report. Available online: https://www3.paho.org/data/index.php/en/mnu-topics/chikv-en/550-chikv-weekly-en.html (accessed on 6 June 2024).
- Cucunubá, Z.M.; Rodriguez-Barraquer, I.; Montoya, M.C.M.; Trujillo Correa, A.; Camacho, E.; Estupiñan, M.I.; Lozano, A.; Gelvez, R.M.; Herrera, V.M.; Villar, L.Á. Characterization of Population Exposure (Seroprevalence) to Arboviruses after Recent Outbreaks in Colombia: Dengue, Chikungunya and Zika. Journal of Tropical Medicine and Hygiene 2018, 99, 296–296. [Google Scholar]
- Estupiñán Cardenas, M.I.; Rodriguez-Barraquer, I.; Gélvez, R.M.; Herrera, V.; Lozano, A.; Vanhomwegen, J.; Salje, H.; Manuguerra, J.-C.; Cummings, D.A.; Miranda, M.C.; et al. Endemicity and Emergence of Arboviruses in Piedecuesta, Colombia. Am J Trop Med Hyg 2018, 99, 512–512. [Google Scholar]
- Organización Mundial de la Salud Chikungunya. Nota Descriptiva. Available online: http://www.who.int/mediacentre/factsheets/fs327/es/ (accessed on 8 September 2024).
- Tanabe, I.S.B.; Tanabe, E.L.L.; Santos, E.C.; Martins, W. V.; Araújo, I.M.T.C.; Cavalcante, M.C.A.; Lima, A.R. V.; Câmara, N.O.S.; Anderson, L.; Yunusov, D.; et al. Cellular and Molecular Immune Response to Chikungunya Virus Infection. Front Cell Infect Microbiol 2018, 8, 1–15. [Google Scholar] [CrossRef]
- Thiberville, S.D.; Moyen, N.; Dupuis-Maguiraga, L.; Nougairede, A.; Gould, E.A.; Roques, P.; de Lamballerie, X. Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis and Therapy. Antiviral Res 2013, 99, 345–370. [Google Scholar] [CrossRef]
- Edington, F.; Varjão, D.; Melo, P. Incidence of Articular Pain and Arthritis after Chikungunya Fever in the Americas: A Systematic Review of the Literature and Meta-Analysis. Joint Bone Spine 2018, 85, 669–678. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Gil-Restrepo, A.F.; Ramírez-Jaramillo, V.; Montoya-Arias, C.P.; Acevedo-Mendoza, W.F.; Bedoya-Arias, J.E.; Chica-Quintero, L.A.; Murillo-García, D.R.; García-Robledo, J.E.; Castrillón-Spitia, J.D.; et al. Post-Chikungunya Chronic Inflammatory Rheumatism: Results from a Retrospective Follow-up Study of 283 Adult and Child Cases in La Virginia, Risaralda, Colombia. F1000Res 2016.
- López Rodríguez, M.A. Evaluación de Las Manifestaciones Reumatológicas y Las Alteraciones Paraclínicas Luego de Dos Años de La Presentación de La Infección Por Virus de Chikungunya En Un Brote En El Municipio de Capitanejo, Santander. [Tesis de Especialización En Medicina Interna], Universidad Industrial de Santander, 2018.
- Gérardin, P.; Fianu, A.; Michault, A.; Mussard, C.; Boussaïd, K.; Rollot, O.; Grivard, P.; Kassab, S.; Bouquillard, E.; Borgherini, G.; et al. Predictors of Chikungunya Rheumatism: A Prognostic Survey Ancillary to the TELECHIK Cohort Study. Arthritis Res Ther 2013, 15, R9. [Google Scholar] [CrossRef]
- Moro, M.L.; Grilli, E.; Corvetta, A.; Silvi, G.; Angelini, R.; Mascella, F.; Miserocchi, F.; Sambo, P.; Finarelli, A.C.; Sambri, V.; et al. Long-Term Chikungunya Infection Clinical Manifestations after an Outbreak in Italy: A Prognostic Cohort Study. Journal of Infection 2012, 65, 165–172. [Google Scholar] [CrossRef]
- Fourie, E.; Morrison, J. Rheumatoid Arthritic Syndrome after Chikungunya Fever. S Afr Med J. 1979, 56, 130–132. [Google Scholar]
- Simon, F.; Javelle, E.; Cabie, A.; Bouquillard, E.; Troisgros, O.; Gentile, G.; Leparc-Goffart, I.; Hoen, B.; Gandjbakhch, F.; Rene-Corail, P.; et al. French Guidelines for the Management of Chikungunya (Acute and Persistent Presentations). November 2014. Med Mal Infect 2015, 45, 243–263. [Google Scholar] [CrossRef]
- Segura-Charry, J.S.; Parada-Martinez, M.A.; Segura-Puello, H.R.; Muñoz-Forero, D.M.; Nieto-Mosquera, D.L.; Villamil-Ballesteros, A.C.; Cortés-Muñoz, A.J. Musculoskeletal Disorders Due to Chikungunya Virus: A Real Experience in a Rheumatology Department in Neiva, Huila. Reumatol Clin 2021, 17, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Soumahoro, M.K.; Gérardin, P.; Boëlle, P.Y.; Perrau, J.; Fianu, A.; Pouchot, J.; Malvy, D.; Flahault, A.; Favier, F.; Hanslik, T. Impact of Chikungunya Virus Infection on Health Status and Quality of Life: A Retrospective Cohort Study. PLoS One 2009, 4, e7800. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, V.; Malaisamy, M.; Ponnaiah, M.; Kaliaperuaml, K.; Vadivoo, S.; Gupte, M.D. Impact of Chikungunya on Health Related Quality of Life Chennai, South India. PLoS One 2012, 7, e51519. [Google Scholar] [CrossRef] [PubMed]
- Couturier, E.; Guillemin, F.; Mura, M.; Léon, L.; Virion, J.M.; Letort, M.J.; De valk, H.; Simon, F.; Vaillant, V. Impaired Quality of Life after Chikungunya Virus Infection: A 2-Year Follow-up Study. Rheumatology (United Kingdom) 2012, 51, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Elsinga, J.; Gerstenbluth, I.; Van Der Ploeg, S.; Halabi, Y.; Lourents, N.T.; Burgerhof, J.G.; Van Der Veen, H.T.; Bailey, A.; Grobusch, M.P.; Tami, A. Long-Term Chikungunya Sequelae in Curaçao: Burden, Determinants, and a Novel Classification Tool. Journal of Infectious Diseases 2017, 216, 573–581. [Google Scholar] [CrossRef]
- Marimoutou, C.; Ferraro, J.; Javelle, E.; Deparis, X.; Simon, F. Chikungunya Infection: Self-Reported Rheumatic Morbidity and Impaired Quality of Life Persist 6 Years Later. Clinical Microbiology and Infection 2015, 21, 688–693. [Google Scholar] [CrossRef]
- Duvignaud, A.; Fianu, A.; Bertolotti, A.; Jaubert, J.; Michault, A.; Poubeau, P.; Fred, A.; Méchain, M.; Gaüzère, B.A.; Favier, F.; et al. Rheumatism and Chronic Fatigue, the Two Facets of Post-Chikungunya Disease: The TELECHIK Cohort Study on Reunion Island. Epidemiol Infect 2018, 146, 633–641. [Google Scholar] [CrossRef]
- Manimunda, S.P.; Vijayachari, P.; Uppoor, R.; Sugunan, A.P.; Singh, S.S.; Rai, S.K.; Sudeep, A.B.; Muruganandam, N.; Chaitanya, I.K.; Guruprasad, D.R. Clinical Progression of Chikungunya Fever during Acute and Chronic Arthritic Stages and the Changes in Joint Morphology as Revealed by Imaging. Trans R Soc Trop Med Hyg 2010, 104, 392–399. [Google Scholar] [CrossRef]
- Gérardin, P.; Fianu, A.; Malvy, D.; Mussard, C.; Boussaïd, K.; Rollot, O.; Michault, A.; Gaüzere, B.A.; Bréart, G.; Favier, F. Perceived Morbidity and Community Burden after a Chikungunya Outbreak: The TELECHIK Survey, a Population-Based Cohort Study. BMC Med 2011, 9. [Google Scholar] [CrossRef]
- Carabali, M.; Lim, J.K.; Palencia, D.C.; Lozano-Parra, A.; Gelvez, R.M.; Lee, K.S.; Florez, J.P.; Herrera, V.M.; Kaufman, J.S.; Rojas, E.M.; et al. Burden of Dengue among Febrile Patients at the Time of Chikungunya Introduction in Piedecuesta, Colombia. Tropical Medicine & International Health 2018, 23, 1231–1241. [Google Scholar] [CrossRef]
- CDC Real Time RT-PCR for Detection of Chikungunya Virus; 2014.
- Riel, P.L.C.M. van.; Gestel, A.M. van.; Scott, D.L. Eular Handbook of Clinical Assessments in Rheumatoid Arthritis. 2000.
- Dacre, J. The GALS Screen: The Rapid Rheumatological Exam. Medical Journal of Australia 2019, 210, 396–397.e1. [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A Review of the Measurement of Grip Strength in Clinical and Epidemiological Studies: Towards a Standardised Approach. 2011. [CrossRef]
- Maska, L.; Anderson, J.; Michaud, K. Measures of Functional Status and Quality of Life in Rheumatoid Arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Improved Health Assessment Questionnaire (Improved HAQ), and Rheumatoid Arthritis Quality of Life (RAQoL). Arthritis Care Res (Hoboken) 2011, 63. [Google Scholar] [CrossRef]
- Halls, S.; Sinnathurai, P.; Hewlett, S.; Mackie, S.L.; March, L.; Bartlett, S.J.; Bingham, C.O.; Alten, R.; Campbell, I.; Hill, C.L.; et al. Stiffness Is the Cardinal Symptom of Inflammatory Musculoskeletal Diseases, yet Still Variably Measured: Report from the OMERACT 2016 Stiffness Special Interest Group. J Rheumatol 2017, 44, 1904–1910. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.; Ware, J.J.; Raczek, AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and Clinical Tests of Validity in Measuring Physical and Mental Health Constructs. Med Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Larocca, N.G.; Muir Nash, J.; Steinberg, A.D. The Fatigue Severity Scale: Application to Patients with Multiple Sclerosis and Systemic Lupus Erythematosus. Arch Neurol 1989. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid Arthritis Classification Criteria: An American College of Rheumatology/European League Against Rheumatism Collaborative Initiative. Arthritis Rheum 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Rudwaleit, M.; Van Der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The Assessment of Spondyloarthritis International Society Classification Criteria for Peripheral Spondyloarthritis and for Spondyloarthritis in General. Ann Rheum Dis 2011, 70, 25–31. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Ann Rheum Dis 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- van Riel, P.L.; van Gestel, A.M.; Scott, D.L. EULAR Handbook of Clinical Assessments in Rheumatoid Arthritis: On Behalf of the EULAR Standing Committee for International Clinical Studies Including Therapeutic Trials -ESCISIT; Van Zuiden, A. aan den R., Ed.; 3rd ed.; 2004; ISBN 9789075141900.
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia Criteria and Severity Scales for Clinical and Epidemiological Studies: A Modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Bullinger, M.; Alonso, J.; Apolone, G.; Leplège, A.; Sullivan, M.; Wood-Dauphinee, S.; Gandek, B.; Wagner, A.; Aaronson, N.; Bech, P.; et al. Translating Health Status Questionnaires and Evaluating Their Quality: The IQOLA Project Approach. J Clin Epidemiol 1998, 51, 913–923. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. El Cuestionario de Salud SF-36 Español: Una Década de Experiencia y Nuevos Desarrollos Por Los Investigadores de La Red-IRYSS*. Gac Sanit 2005, 19. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Anto, J. La Versión Española Del SF-36 Health Survey (Cuestionario de Salud SF-36): Un Instrumento Para La Medida de Los Resultados Clínicos. Med Clin (Barc) 1995, 104, 771–776. [Google Scholar] [PubMed]
- Díaz, J.A.; Dávila, F.A.; Quintana López, G.; Brown, P. Evaluación de La Fiabilidad Del SF-36 En Pacientes Colombianos Con Artritis Reumatoide. Rehabilitacion (Madr) 2017, 51, 79–85. [Google Scholar] [CrossRef]
- Maruish, M.E. (Ed. ) User’s Manual for the Sf-36v2 Health Survey.; 3rd ed.; Lincoln, RI: QualityMetric Incorporated., 2011; ISBN 1-891810-28-6.
- Bernal-Vargas, L.; Riveros, F.; Vinaccia, S.; Qulceno, J. Estructura Factorial y Consistencia Interna de La Escala de Severidad de Fatiga En Población Colombiana Con Enfermedades Crónicas. Enfermeria Global 2017, 16, 37–43. [Google Scholar] [CrossRef]
- Ayala Sierra, E.F.; Rojas, E.M.; Villar-centeno, L.A. Post Infectious Fatigue in Patients with Dengue 2015-2016. [Tesis de Especialización En Medicina Interna], Universidad Industrial de Santander, 2017.
- Guillot, X.; Ribera, A.; Gasque, P. Chikungunya-Induced Arthritis in Reunion Island: A Long-Term Observational Follow-up Study Showing Frequently Persistent Joint Symptoms, Some Cases of Persistent Chikungunya Immunoglobulin M Positivity, and No Anticyclic Citrullinated Peptide Seroconversion after 13 Years. The Journal of Infectious Diseases ® 2020, 222, 1740–1744. [Google Scholar] [CrossRef] [PubMed]
- Consuegra-Rodríguez, M.P.; Hidalgo-Zambrano, D.M.; Vásquez-Serna, H.; Jimenez-Canizales, C.E.; Parra-Valencia, E.; Rodriguez-Morales, A.J. Post-Chikungunya Chronic Inflammatory Rheumatism: Follow-up of Cases after 1 Year of Infection in Tolima, Colombia. Travel Med Infect Dis 2018, 21, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Encinales, L.; Porras, A.; Pacheco, N.; Reid, S.P.; Martins, K.A.O.; Pacheco, S.; Bravo, E.; Navarno, M.; Rico Mendoza, A.; et al. Frequency of Chronic Coint Pain Following Chikungunya Virus Infection: A Colombian Cohort Study. Arthritis Rheumatol 2018, 70, 578–584. [Google Scholar] [CrossRef]
- Colombia - Encuesta de Cultura Política - ECP - 2015. Available online: https://microdatos.dane.gov.co/index.php/catalog/406 (accessed on 9 September 2024).
- Gérardin, P.; Guernier, V.; Perrau, J.; Fianu, A.; Le Roux, K.; Grivard, P.; Michault, A.; de Lamballerie, X.; Flahault, A.; Favier, F. Estimating Chikungunya Prevalence in La Réunion Island Outbreak by Serosurveys: Two Methods for Two Critical Times of the Epidemic. BMC Infect Dis 2008, 8, 99. [Google Scholar] [CrossRef]
- Laiton-Donato, K.; Usme-Ciro, J.A.; Rico, A.; Pardo, L.; Martínez, C.; Salas, D.; Ardila, S.; Páez, A. Análisis Filogenético Del Virus Del Chikungunya En Colombia: Evidencia de Selección Purificadora En El Gen E1. Biomédica 2015. [Google Scholar] [CrossRef]
- Gardner, J.; Anraku, I.; Le, T.T.; Larcher, T.; Major, L.; Roques, P.; Schroder, W.A.; Higgs, S.; Suhrbier, A. Chikungunya Virus Arthritis in Adult Wild-Type Mice. J Virol 2010, 84, 8021–8032. [Google Scholar] [CrossRef]
- Teo, T.-H.; Her, Z.; Tan, J.J.L.; Lum, F.-M.; Lee, W.W.L.; Chan, Y.-H.; Ong, R.-Y.; Kam, Y.-W.; Leparc-Goffart, I.; Gallian, P.; et al. Caribbean and La Réunion Chikungunya Virus Isolates Differ in Their Capacity to Induce Proinflammatory Th1 and NK Cell Responses and Acute Joint Pathology. J Virol 2015. [Google Scholar] [CrossRef]
- Londoño, J.; Peláez Ballestas, I.; Cuervo, F.; Angarita, I.; Giraldo, R.; Rueda, J.C.; Ballesteros, J.G.; Baquero, R.; Forero, E.; Cardiel, M.; et al. Prevalencia de La Enfermedad Reumática En Colombia, Según Estrategia COPCORD-Asociación Colombiana de Reumatología. Estudio de Prevalencia de Enfermedad Reumática En Población Colombiana Mayor de 18 Años. Revista Colombiana de Reumatología 2018, 25, 245–256. [Google Scholar] [CrossRef]
- Venetsanopoulou, A.I.; Alamanos, Y.; Voulgari, P. V.; Drosos, A.A. Epidemiology and Risk Factors for Rheumatoid Arthritis Development. Mediterr J Rheumatol 2023, 34, 404–413. [Google Scholar] [CrossRef] [PubMed]
- Medina-Cintron, N.; Martinez, I.; Perez-Rios, N.; Berrios-Lopez, Y.; Vila, L.M. Clinical Manifestations and Outcomes in Disease-Modifying Antirheumatic Drug-Naive Adult Patients with Chronic Chikungunya Arthritis. Am J Trop Med Hyg 2021, 104, 1741. [Google Scholar] [CrossRef] [PubMed]
- Watson, H.; Tritsch, S.R.; Encinales, L.; Cadena, A.; Cure, C.; Ramirez, A.P.; Mendoza, A.R.; Chang, A.Y. Stiffness, Pain, and Joint Counts in Chronic Chikungunya Disease: Relevance to Disability and Quality of Life. Clin Rheumatol 2020, 39, 1679. [Google Scholar] [CrossRef] [PubMed]
- Marimoutou, C.; Vivier, E.; Oliver, M.; Boutin, J.P.; Simon, F. Morbidity and Impaired Quality of Life 30 Months after Chikungunya Infection: Comparative Cohort of Infected and Uninfected French Military Policemen in Reunion Island. Medicine (United States) 2012, 91, 212–219. [Google Scholar] [CrossRef]
- Carruthers, B.M.; Van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.P.; Speight, N.; Vallings, R.; et al. Myalgic Encephalomyelitis: International Consensus Criteria. J Intern Med 2011, 270, 327–338. [Google Scholar] [CrossRef]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A.; Schluederberg, A.; Jones, J.F.; Lloyd, A.R.; Wessely, S.; et al. The Chronic Fatigue Syndrome - A Comprehensive Approach to Its Definition and Study. Ann Intern Med 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Ministerio de Salud y Protección Social Rutas Integrales de Atención En Salud (RIAS). Available online: https://www.minsalud.gov.co/Paginas/rutas-integrales-de-atencion-en-salud.aspx (accessed on 19 June 2024).
- Mattar, S.; Miranda, J.; Pinzon, H.; Tique, V.; Bolaños, A.; Aponte, J.; Arrieta, G.; Gonzalez, M.; Barrios, K.; Contreras, H.; et al. Outbreak of Chikungunya Virus in the North Caribbean Area of Colombia: Clinical Presentation and Phylogenetic Analysis. J Infect Dev Ctries 2015. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization Epidemiological Alert: Increase in Cases and Deaths from Chikungunya in the Region of the Americas. 8 March 2023; 2023.
- Torales, M.; Beeson, A.; Grau, L.; Galeano, M.; Ojeda, A.; Bq, D.; Bettiana Martinez, ; León, N.; Cabello, A.; Rojas, F.; et al. Notes from the Field: Chikungunya Outbreak — Paraguay, 2022–2023. Morbidity and Mortality Weekly Report; 2023.
Figure 1.
Flowchart of the re-contact and enrolment processes.
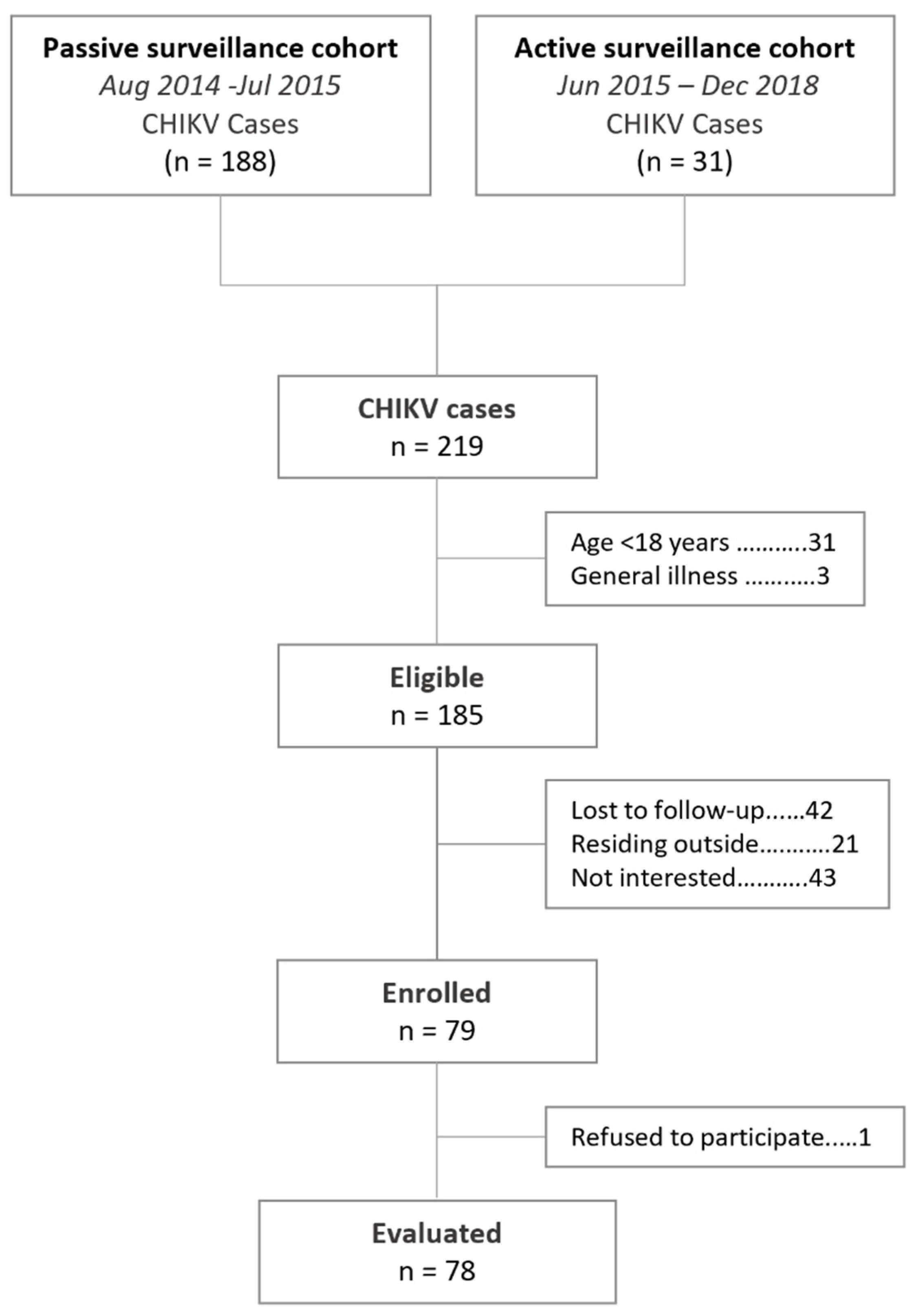
Figure 2.
Quality of life assessed using the SF-36 questionnaire during the follow-up evaluation, by clinical pattern of post-CHIK chronic rheumatism.
Figure 2.
Quality of life assessed using the SF-36 questionnaire during the follow-up evaluation, by clinical pattern of post-CHIK chronic rheumatism.
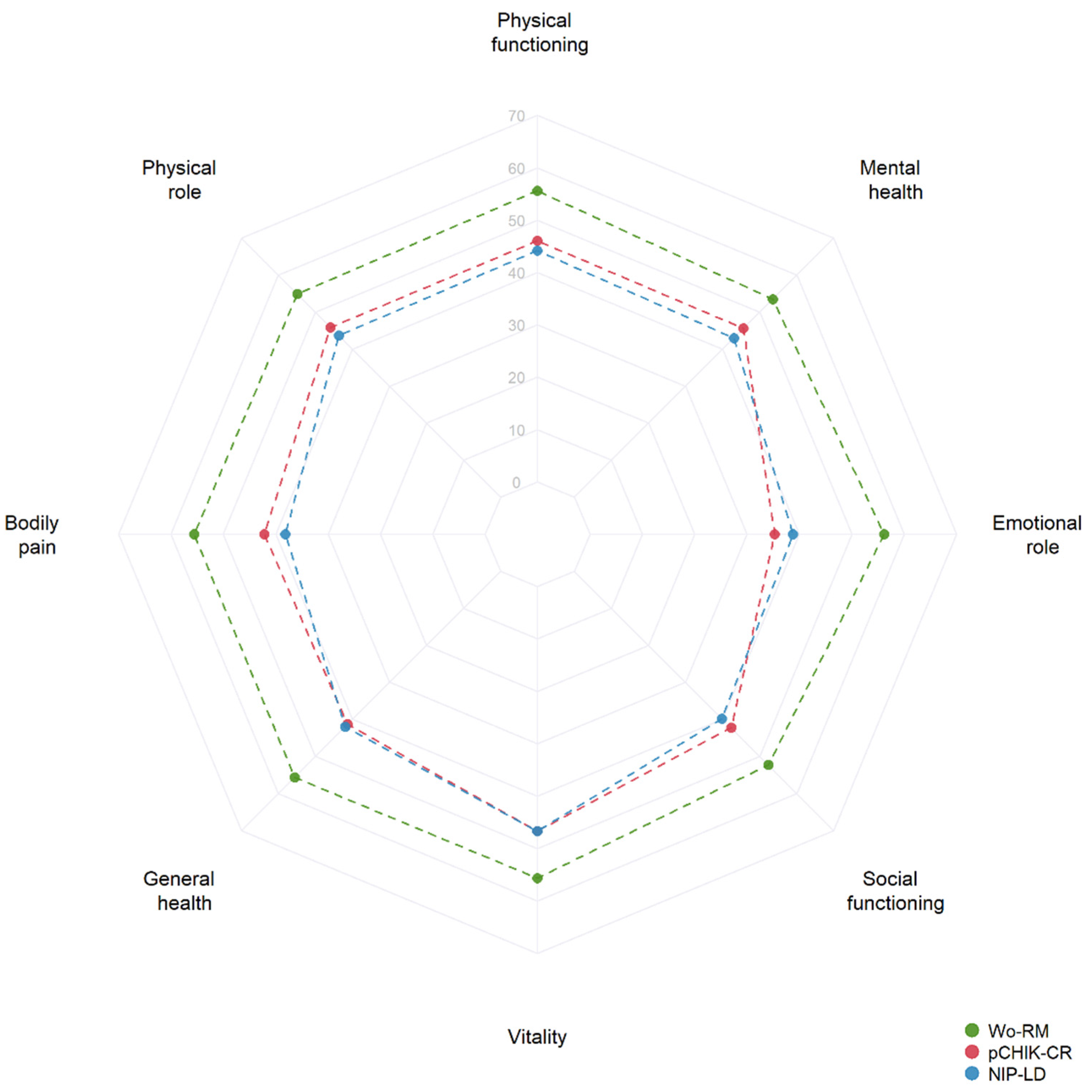
Table 1.
Characteristics of patients during the acute phase of CHIKV infection (2014-2015), categorized by the source of information.
Table 1.
Characteristics of patients during the acute phase of CHIKV infection (2014-2015), categorized by the source of information.
| Characteristic, n (%) |
Passive surveillance cohort (n=65) |
Active surveillance cohort (n=13) |
All (n=78) |
|---|---|---|---|
| Sex | |||
| Male | 23 (35.4) | 8 (61.5) | 31 (39.7) |
| Female | 42 (64.6) | 5 (38.5) | 47 (60.3) |
| Age (years) | |||
| < 18 | 9 (13.8) | 8 (61.5) | 16 (20.5) |
| 18 – 30 | 21 (32.3) | 0 (0.0) | 22 (28.2) |
| 31 – 45 | 25 (38.5) | 5 (38.5) | 30 (38.5) |
| ≥ 46 | 10 (15.4) | 0 (0.0) | 10 (12.8) |
| Days of illness, Mean (SD) | 2.8 (1.6) | 3.0 (1.2) | 2.8 (1.5) |
| Symptoms | |||
| Arthralgia | 62 (95.4) | 10 (76.9) | 72 (92.3) |
| Myalgia | 54 (83.1) | 11 (84.6) | 65 (83.3) |
| Fatigue | 65 (100.0) | 11 (84.6) | 76 (97.4) |
| Skin rash | 53 (81.5) | 10 (76.9) | 63 (80.8) |
| Headache | 62 (95.4) | 11 (84.6) | 73 (93.6) |
| Nauseas | 36 (55.4) | 3 (23.1) | 39 (50.0) |
| Medical history | |||
| Diabetes mellitus | 1 (1.5) | 0 (0.0) | 1 (1.3) |
| Renal disease | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Liver disease | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Cardiovascular disease | 3 (4.6) | 0 (0.0) | 3 (3.9) |
| Articular disease | 0 (0.0) | 0 (0.0) | 0 (0.0) |
Table 2.
Clinical patterns of chronic rheumatism during the follow-up evaluation.
| Clinical Patterns | n (%) |
|---|---|
| Post-CHIK Chronic Rheumatism | 11 (14.1) |
| Rheumatoid arthritis | 0 (0.0) |
| Post-viral oligo/polyarthritis | 4 (36.4) |
| Post-viral arthralgia | 3 (27.2) |
| Soft tissue rheumatism | |
| Tenosynovitis | 0 (0.0) |
| Fibromyalgia | 2 (18.2) |
| Fasciitis | 1 (9.1) |
| Enthesitis | 1 (9.1) |
| Non-inflammatory pain likely degenerative | 32 (41.0) |
| Without rheumatic manifestations | 35 (44.9) |
Table 3.
Characteristics of participants during the follow-up evaluation, categorized by clinical pattern of chronic rheumatism.
Table 3.
Characteristics of participants during the follow-up evaluation, categorized by clinical pattern of chronic rheumatism.
| Characteristic | pCHIK-CR (n=11) |
NIP-LD (n=32) | Wo-RM (n=35) |
p |
|---|---|---|---|---|
| Female, n (%) | 9 (81.2) | 24 (75.0) b | 14 (40.0) | 0.004 |
| Age (years) | 45.0 [15.0] a | 40.5 [16.5] b | 30.0 [20.0] | 0.004 |
| Symptoms, n (%) | ||||
| Myalgia | 5 (45.5) | 20 (62.5) | 13 (37.1) | 0.113 |
| Paresthesia | 8 (72.7) | 21 (65.6) | 14 (40.0) | 0.059 |
| Stiffness | 2 (18.2) | 1 (3.1) | 0 (0.0) | 0.025 |
| Limitation of gait | 4 (36.4) a | 18 (56.3) b | 2 (5.7) | 0.000 |
| Joint swelling | 7 (63.4) a | 13 (40.6) b | 1 (2.9) | 0.000 |
| Medical history, n (%) | ||||
| Arthritis | 1 (9.1) | 1 (3.1) | 0 (0.0) | 0.136 |
| Osteoarthrosis | 1 (9.1) | 1 (3.1) | 0 (0.0) | 0.136 |
| Hypertension | 3 (27.3) | 5 (15.6) | 3 (8.6) | 0.239 |
| Diabetes | 1 (9.1) | 1 (3.1) | 1 (2.9) | 0.522 |
| Chronic renal disease | 1 (9.1) | 0 (0.0) | 0 (0.0) | 0.141 |
| Liver disease | 0 (0.0) | 1 (3.1) | 0 (0.0) | 0.551 |
| Medication use, n (%) | ||||
| Dexamethasone | 2 (18.2) | 1 (3.1) | 0 (0.0) | 0.025 |
| Prednisolone | 0 (0.0) | 2 (6.3) | 0 (0.0) | 0.429 |
| Methotrexate | 0 (0.0) | 1 (3.1) | 0 (0.0) | 0.551 |
| Body mass index (kg/m2) | 31.0 [9.8] | 26.7 [8.7] | 27.0 [6.5] | 0.584 |
| Handgrip (kg) | 19.1 [16.5] a | 18.1 [14.2] b | 32.1 [22.0] | 0.043 |
| HAQ-DI score | 0.6 [1.5] a | 0.5 [0.6] b | 0.0 [0.1] | 0.000 |
| HAQ-DI categories | ||||
| Dressing and grooming | 0.0 [1.0] a | 0.0 [0.0] | 0.0 [0.0] | 0.039 |
| Arising | 1.0 [1.0] a | 0.5 [1.0] b | 0.0 [0.0] | 0.000 |
| Eating | 0.0 [0.0] | 0.0 [0.5] | 0.0 [0.0] | 0.195 |
| Walking | 0.0 [2.0] a | 1.0 [1.0] b | 0.0 [0.0] | 0.000 |
| Hygiene | 0.0 [1.0] a | 0.0 [0.0] | 0.0 [0.0] | 0.008 |
| Reaching | 1.0 [1.0] a | 0.0 [1.0] b | 0.0 [0.0] | 0.001 |
| Grip | 0.0 [1.0] a | 0.0 [1.0] b | 0.0 [0.0] | 0.012 |
| Usual activities | 0.0 [2.0] a | 0.0 [1.0] b | 0.0 [0.0] | 0.002 |
| MSQ score (%) | 22.8 [40.3] a | 30.1 [26.9] b | 0.0 [5.0] | 0.000 |
The values in square brackets denote the interquartile range [IQR]. pCHIK-CR: Post-CHIK Chronic Rheumatism; NIP-LD: Non-inflammatory pain likely degenerative; Wo-RM: Without rheumatic manifestations. a p<0.050 for the comparison between pCHIK-CR and Wo-RM. b p<0.050 for the comparison between NIP-LD and Wo-RM. c Pp<0.050 for the comparison between pCHIK-CR and NIP-LD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



