
Submitted:
09 April 2025
Posted:
10 April 2025
You are already at the latest version
Abstract
Background/Objectives. The study aims to observe and compare the real-world total costs of hospitalization in patients with chronic heart failure (CHF) and metabolic syndrome (MetS) from an upper-middle-income European country. Methods. Data were electronically retrieved from three different internal medicine departments of university hospitals in Bucharest, Romania, including all admissions from December 2023 to June 2024. Collected data included demographics, cost of hospitalization (€), and discharge diagnoses (ICD10 codes, used to calculate the Charleston comorbidity index - CCI and to define a MetS surrogate definition). Results. Database query retrieved 4732 hospitalizations (median duration of 4 days; median cost of 1002€) of unique patients (53.9% women, average age of 68.7 years), of whom 48.0% had CHF and 11.0% classified as MetS. Compared to men, women were significantly older, with significantly higher prevalence of CHF, but similar median hospitalization duration and costs. Compared to patients without CHF or MetS, those with CHF or MetS were significantly older, with more comorbidities (CCI) and with higher median hospitalization duration, total cost and cost/day of hospitalization. The total cost of hospitalization increases steadily from a minimum in patients without CHF or Met to a maximum in patients with both conditions. Conclusions. CHF is highly prevalent among patients admitted to internal medicine wards and it is more prevalent among hospitalized women, without significant hospitalization cost differences compared to men. CHF and MetS incrementally increased the total costs of hospitalization in a DRG-based reimbursement systems.
Keywords:
cost
; chronic heart failure
; metabolic syndrome
; hospitalization
1. Introduction
Chronic heart failure (CHF) is a progressive clinical syndrome which arises most commonly from structural or functional cardiac abnormalities, often secondary to ischemic heart disease, arterial hypertension, valvular disorders, or cardiomyopathies. Pathophysiologically, CHF involves neurohormonal activation, leading to maladaptive compensatory mechanisms such as sympathetic nervous system overactivation and renin-angiotensin-aldosterone system upregulation [1,2]. These processes contribute to fluid retention, ventricular remodeling, and progressive myocardial dysfunction. Clinically, CHF manifests as dyspnea, fatigue, fluid overload, and exercise intolerance, significantly impairing quality of life. Management strategies include pharmacological interventions (such as beta-blockers, renin-angiotensin system inhibitors, sodium-glucose cotransporter-2 inhibitors and mineralocorticoid receptor antagonists), alongside non-pharmacological measures, including lifestyle modifications and device-based therapies [3,4,5,6]. Despite advances in treatment, CHF remains a major cause of morbidity and mortality worldwide, necessitating ongoing research into novel therapeutic approaches [7,8].
Consequently, CHF entails a substantial economic burden on healthcare systems worldwide due to its high prevalence, frequent hospitalizations, and long-term management requirements [7,9,10,11,12]. The costs associated with CHF are primarily driven by hospital admissions [13], pharmacological therapies, outpatient care, and the need for advanced interventions such as implantable devices [14] or heart transplantation [15]. Indirect costs, including loss of productivity and caregiver burden, further contribute to the financial impact. In developed countries, CHF accounts for a significant proportion of total healthcare expenditures [16], with costs projected to rise due to aging populations and increasing disease prevalence [17]. Strategies to reduce the economic burden of CHF include optimizing medical therapy, promoting early diagnosis, and implementing preventive measures to reduce hospital readmissions and disease progression [18,19,20].
The metabolic syndrome (MetS) has a high prevalence among CHF patients [21]. The International Diabetes Foundation (IDF) defined MetS as the co-occurrence of central obesity and any two of the following: elevated triglycerides, reduced HDL-cholesterol, elevated blood pressure, elevated fasting plasma glucose [22]. The interplay between MetS and CHF) is multifaceted, involving both the contribution of MetS to CHF development and its influence on patient outcomes. On one hand, the MetS can act as a risk factor for CHF through visceral adiposity, which initiates chronic inflammation and insulin resistance, which can lead to myocardial dysfunction and subsequent heart failure [23]. Additionally, CHF and the MetS share biomarkers and pathways relating to obesity, lipid metabolism and chronic inflammation, such as leptin, fatty acid-binding protein 4, interleukin-1 receptor antagonist, tumor necrosis factor receptors, proto-oncogene tyrosine-protein kinase receptor Ret [24], C-reactive protein (CRP) [25] and hormonal deficiency [26]. In this context, their association has been rightly named the cardiometabolic syndrome [27,28], as opposed to the cardiorenal syndrome [29,30]. On the other hand, the presence of the MetS may cause negative prognostic implications for CHF patients [31,32], an observation which still needs investigation. Last but not least, the MetS significantly increases healthcare costs [33].
In this context, the current study aims to observe and compare the real-world total costs of hospitalization in patients with CHF and MetS from an upper-middle-income European country.
2. Materials and Methods
2.1. Data
Data were electronically retrieved from three different internal medicine departments of university hospitals in Bucharest, Romania, covering an admission timeframe from December 2023 to June 2024. All patients admitted to the hospital in the specified period were included, and the first admission form each unique patient was retained for analysis. On admission, all patients gave written informed consent for the scientific use of personal and medical data. Collected data included sex, age, admission and discharge dates, cost of hospitalization (reported at an approximate exchange rate of 5 Romanian leu for 1 €uro), discharge diagnoses coded with the 10th version of the International Classification of Diseases (ICD10). The retrospective design and missing data did not allow for quantitative measurement retrieval of definition criteria, ICD10 codes were used to identify diagnoses included in the Charleston comorbidity index (CCI; Table 1) [34] and in the definition of the MetS (defined as either: E66 + I10 + E11, or E66 + I10 + E78.0-5, or E66 + E11 + E78.0-5).
2.2. Hospitalization Costs
Since 2003, in Romania, public hospital financing is primarily managed through a system based on Diagnosis-Related Groups (DRGs), using initially the Australian Refined DRG (AR-DRG) version 5 for hospital reimbursement [35], which was modified in 2010, when Romania developed its own DRG variant (RO-DRG), incorporating new definitions for comorbidities and complications, and adjusting grouping limits for certain cases. This system undergoes periodic updates to enhance its applicability to the Romanian healthcare context. The financial mechanism of hospital reimbursement consists of prospective payments comprising a mix of methods, including DRG-based case payments, day tariffs, lump sums for national health programs, and fee-for-service payments for outpatient services. The DRG component is central, determining reimbursement based on the complexity and resource needs of treated cases.
2.3. Statistics
Data distribution normality was assessed using descriptive statistics, normality, stem-and-leaf plots and the Lillefors corrected Kolmogorov-Smirnov tests. Continuous variables are reported as “mean ± standard deviation” (SD) if normally distributed, or as “median (interquartile range)” (IQR) if non-normally distributed, while nominal variables are reported as “absolute frequency (percentage of group or subgroup)”. The difference of continuous variables among subgroups were assessed by independent-sample t tests (for normally distributed continuous variables among groups of dichotomous nominal variables) or Mann Whitney and Kruskal Wallis tests (for non-normally distributed continuous variables among groups of nominal variables with two or more states), while associations of dichotomous categorical variables were assessed using χ2 tests. All tests were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., released 2019, Armonk, NY).
3. Results
Database query retrieved 4732 admissions of unique patients within the timeframe. The patients included in the lot were more frequently women (53.9%) and they had an average age of 68.7 years (Table 2).
Regarding the diagnoses included in the CCI, CHF was highly prevalent in the sample (48.0%), followed by diabetes mellitus (30.5%), chronic kidney disease (19.8%), myocardial infarction (18.8%) and cirrhosis (17.3%; Table 3). Approximately 11,1% of patients were categorized as having the MetS. Regarding the diagnoses included in the definition of the MetS, arterial hypertension was the most prevalent (50.0%), followed by dyslipidemia (38.5%), diabetes mellitus (30.5%) and obesity (19.8%; Table 3). In terms of costs, the median hospitalization duration was 4 days and the median cost of hospitalization reached 1002 € (Table 2).
Compared to men, women were significantly older (average age of 70.0 ± 13.7 years versus 67.3 ± 13.1 years; p < 0.001) and they had a significantly higher prevalence of CHF (49.4% versus 46.4%; p = 0.042; Figure 1A), but similar median hospitalization durations (4 (6) days versus 4 (6) days; p = 0.087), similar median total hospitalization costs (1002 (7346) € versus 1002 (7338) €; p = 0.938), similar median costs per day of hospitalization (305 (1479) € versus 322 (1474) €; p = 0.214) and similar median CCI scores (5 (3) versus 5 (3); p = 0.635).
Compared to patients without CHF, those with CHF were significantly older (average age of 72.2 ± 11.7 years versus 65.4 ± 14.1 years; p < 0.001; Figure 2A), they had significantly longer median hospitalization durations (5 (7) days versus 3 (6) days; p < 0.001; Figure 2B), significantly higher median total hospitalization costs (1014 (7198) € versus 728 (7384) €; p < 0.001; Figure 2C), significantly higher median costs per day of hospitalization (327 (1479) € versus 312 (1476) €; p = 0.044) and significantly higher median CCI scores without including CHF itself (5 (3) versus 4 (3); p < 0.001; Figure 2D).
Compared to patients without the MetS, patients with the MetS were more frequently women (46.9% versus 39.2%; p < 0.001), were significantly older (68.8 ± 13.7 years versus 67.5 ± 11.1 years; p = 0.029) and they had a significantly higher prevalence of CHF (55.7% versus 47.1%; p = 0.042; Figure 1B), similar median hospitalization durations (4 (5) days versus 4 (6) days; p = 0.552), but significantly higher median total hospitalization costs (6552 (7197) € versus 951 (7350) €; p < 0.001), significantly higher median costs per day of hospitalization (906 (2500) € versus 285 (1215) €; p < 0.001) and significantly higher median CCI scores (5 (3) versus 4 (3); p < 0.001).
The total cost of hospitalization increases steadily from a minimum in patients without CHF or Met to a maximum in patients with both conditions (Figure 3).
4. Discussion
The first observation of the current study is the higher prevalence of CHF among women (who were also significantly older than men), without significant hospitalization cost differences compared to men. This difference emerges in pre-diagnosis period since men and women exhibit different risk profiles for CHF [36,37]: men are more likely to develop CHF heart failure with reduced ejection fraction, often resulting from ischemic heart disease, whereas women more frequently exhibit preserved ejection fraction, which is commonly associated with arterial hypertension, obesity, and MetS [38,39]. Additionally, hormonal factors, particularly estrogens, may provide some cardioprotective effects in premenopausal women, potentially delaying the onset of CHF compared to men. Men with CHF typically show greater ventricular dilation and systolic dysfunction, whereas women often have preserved systolic function but exhibit diastolic dysfunction. Women with CHF are more likely to experience symptoms such as dyspnea and fatigue (which prone them to seek hospitalization), and consequently lower quality of life [40,41], while men may present with more overt signs of volume overload, such as peripheral edema [42,43]. Furthermore, women tend to have a heightened inflammatory response [44], which may contribute to differences in disease progression and prognosis [45,46]. Diagnosis of CHF in women is often delayed due to atypical symptoms and under-recognition of preserved ejection fraction [47,48,49]. Despite these differences, women generally have better survival rates than men with CHF [50,51], particularly in cases of preserved ejection fraction. The reasons for this survival advantage are not fully understood [52], but may be related to differences in ventricular remodeling, hormonal influences, and healthcare-seeking behaviors. Social factors, including disparities in access to care and adherence to treatment, may also play a role in gender differences in CHF outcomes. Studies have also identified gender differences in healthcare costs among patients with CHF: men with CHF often incur higher healthcare expenses compared to women [53,54], an observation which was not replicated by the current study. These disparities may be attributed to several factors, including differences in disease severity, comorbidities, and treatment approaches between sexes.
Apart from prevalence differences among sexes, another observation of the current study is the high prevalence of CHF (48.0%) among patients admitted to internal medicine wards. The literature confirms that CHF is a significant contributor to hospital admissions globally. While the exact proportion of CHF among hospitalized patients varies by region and study, several studies provide insight into its prevalence. For example, a nationwide analysis in Thailand between 2008 and 2013 reported that heart failure in adult patients accounted for approximately 1.7% of all adult hospitalizations during that period [55]. Another relevant report comes from Spain, where the Basque Health Service, analyzing data from 2011-2015, reported that 36% of unplanned admissions were due to heart failure [56]. These findings highlight the substantial impact of CHF on hospital admissions and underscore the importance of effective management strategies to reduce hospitalization rates among CHF patients. In parallel with the high prevalence of CHF, the study observed a relatively low prevalence of MetS (11.1%) among hospitalized patients (while the literature consistently reports high prevalence rates among hospitalized patients, regardless of their primary diagnoses and profiles [57,58,59]), which is probably caused by under-reporting of relevant ICD codes and which underlines on the weaknesses of the DRG system: concentration on ICD10 codes which increase the case’s complexity.
The main observation of the study is the confirmation in a particular medical and financial environment that CHF and MetS increase costs of hospitalization. There are multiple mechanisms through which CHF significantly increases hospitalization costs, including prolonged hospital stays, frequent readmissions, intensive treatments, use of specialized hospital units, the management of comorbidities and end-of-life care needs. The point that the current study raises is that hospitalizations account for a significant portion of CHF-related healthcare expenditures: some studies report that approximately 75% to 80% of direct costs for heart failure are attributable to inpatient hospital stays [9]. Therefore, further research should aim at reducing CHF hospitalization costs, which most likely requires a complex approach, including preventing hospital admissions with better outpatient care [60], shortening hospital stays with standardized management protocols, preventing readmissions with post-discharge monitoring [61] and using advanced therapies and technologies to reduce long-term costs. This issue should be more relevantly addressed in the specific nation-based medical system, especially in emergent economies, where saving unnecessary costs may increase healthcare accessibility.
There are several limitations of this study which may impact the interpretation of its results. First, the descriptive retrospective design does not establish cause-and-effect relationships between CHF and hospitalization costs (for example, higher costs may be due to disease severity, comorbidities, or hospital policies) and does not allow for the evaluation of long-term outcomes (e.g., readmission expenses, medication adherence costs, home healthcare and rehabilitation expenses). Second, indirect costs (e.g., lost productivity, caregiver burden) were not recorded, underestimating the total economic impact. Third, a selection bias may have not allowed for the study to capture all CHF patients, especially those treated in outpatient settings and those who avoid hospitalization due to financial or geographic barriers. Since the data are collected from a single city, findings may not be generalizable to other healthcare settings or populations. Lastly, since the study relied on hospital records, errors in coding or missing data may affect the accuracy of cost estimates.
5. Conclusions
CHF is highly prevalent (48.0%) among patients admitted to internal medicine wards and it is more prevalent among hospitalized women, without significant hospitalization cost differences compared to men. CHF and MetS incrementally increased the total costs of hospitalization in a DRG-based reimbursement systems. Addressing CHF-related costs requires early disease management, optimized outpatient care, and reducing preventable hospital admissions.
Author Contributions
Conceptualization, A.M. and D.-I.M.; methodology, A.-L.C., D.G.M.; software, C.-C.P., D.-I.M.; validation, A.M., C.-C.P. and ; formal analysis, C.-C.P., D-.I.M.; investigation, A.-L. C., A.C.; resources, A.C.; data curation, A.M.; writing—original draft preparation, A.M., C.-C. P.; writing—review and editing, A.C., D.-I.M., A.-L.C., V.G., D.G.M.; visualization, V.G.; supervision, D.-G. M., V.G.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of “Prof. Dr. Agrippa Ionescu” Clinical Hospital (protocol code 292318/April 18th 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila through the institutional program “Publish not Perish”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AIDS | acquired immune-deficiency syndrome |
| CCI | Charleston comorbidity index |
| CHF | chronic heart failure |
| CRP | C-reactive protein |
| DRG | Diagnosis-Related Groups |
| HDL | high density lipoproteins |
| ICD | International Classification of Diseases |
| IDF | International Diabetes Foundation |
| IQR | interquartile range |
| MetS | metabolic syndrome |
| SD | standard deviation |
References
- Brake R, Jones ID. Chronic heart failure part 1: pathophysiology, signs and symptoms. Nurs Stand. 2017;31(19):54-63. [CrossRef]
- Elendu C, Amaechi DC, Elendu TC, Fiemotonghan BE, Okoye OK, Agu-Ben CM, et al. A comprehensive review of heart failure: Unraveling the etiology, decoding pathophysiological mechanisms, navigating diagnostic modalities, exploring pharmacological interventions, advocating lifestyle modifications, and charting the horizon of emerging therapies in the complex landscape of chronic cardiac dysfunction. Medicine (Baltimore). 2024;103(3):e36895. [CrossRef]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-726. [CrossRef]
- Tomasoni D, Fonarow GC, Adamo M, Anker SD, Butler J, Coats AJS, et al. Sodium-glucose co-transporter 2 inhibitors as an early, first-line therapy in patients with heart failure and reduced ejection fraction. Eur J Heart Fail. 2022;24(3):431-41. [CrossRef]
- Cunningham JW, Vaduganathan M, Claggett BL, Kulac IJ, Desai AS, Jhund PS, et al. Dapagliflozin in Patients Recently Hospitalized With Heart Failure and Mildly Reduced or Preserved Ejection Fraction. J Am Coll Cardiol. 2022;80(14):1302-10. [CrossRef]
- Bhatt DL, Szarek M, Steg PG, Cannon CP, Leiter LA, McGuire DK, et al. Sotagliflozin in Patients with Diabetes and Recent Worsening Heart Failure. N Engl J Med. 2021;384(2):117-28. [CrossRef]
- Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;118(17):3272-87. [CrossRef]
- Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Kober L, Squire IB, et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34(19):1404-13. [CrossRef]
- Heidenreich PA, Fonarow GC, Opsha Y, Sandhu AT, Sweitzer NK, Warraich HJ, Chair HSSCM. Economic Issues in Heart Failure in the United States. J Card Fail. 2022;28(3):453-66. [CrossRef]
- Tran DT, Ohinmaa A, Thanh NX, Howlett JG, Ezekowitz JA, McAlister FA, Kaul P. The current and future financial burden of hospital admissions for heart failure in Canada: a cost analysis. CMAJ Open. 2016;4(3):E365-E70. [CrossRef]
- Khan SU, Khan MZ, Alkhouli M. Trends of Clinical Outcomes and Health Care Resource Use in Heart Failure in the United States. J Am Heart Assoc. 2020;9(14):e016782. [CrossRef]
- Rosano GMC, Seferovic P, Savarese G, Spoletini I, Lopatin Y, Gustafsson F, et al. Impact analysis of heart failure across European countries: an ESC-HFA position paper. ESC Heart Fail. 2022;9(5):2767-78. [CrossRef]
- Norhammar A, Bodegard J, Vanderheyden M, Tangri N, Karasik A, Maggioni AP, et al. Prevalence, outcomes and costs of a contemporary, multinational population with heart failure. Heart. 2023;109(7):548-56. [CrossRef]
- Baras Shreibati J, Goldhaber-Fiebert JD, Banerjee D, Owens DK, Hlatky MA. Cost-Effectiveness of Left Ventricular Assist Devices in Ambulatory Patients With Advanced Heart Failure. JACC Heart Fail. 2017;5(2):110-9. [CrossRef]
- Urbich M, Globe G, Pantiri K, Heisen M, Bennison C, Wirtz HS, Di Tanna GL. A Systematic Review of Medical Costs Associated with Heart Failure in the USA (2014-2020). Pharmacoeconomics. 2020;38(11):1219-36. [CrossRef]
- Berry C, Murdoch DR, McMurray JJ. Economics of chronic heart failure. Eur J Heart Fail. 2001;3(3):283-91. [CrossRef]
- Khan MS, Shahid I, Bennis A, Rakisheva A, Metra M, Butler J. Global epidemiology of heart failure. Nat Rev Cardiol. 2024;21(10):717-34. [CrossRef]
- Koutlas A, Jenkins P. Reducing Hospital Admissions for Patients with Heart Failure by Implementing the Chronic Care Management Framework: A Cost, Quality and Satisfaction Improvement Project. J Dr Nurs Pract. 2022. [CrossRef]
- Leon-Justel A, Morgado Garcia-Polavieja JI, Alvarez-Rios AI, Caro Fernandez FJ, Merino PAP, Galvez Rios E, et al. Biomarkers-based personalized follow-up in chronic heart failure improves patient’s outcomes and reduces care associate cost. Health Qual Life Outcomes. 2021;19(1):142. [CrossRef]
- Maru S, Byrnes J, Carrington MJ, Chan YK, Thompson DR, Stewart S, et al. Cost-effectiveness of home versus clinic-based management of chronic heart failure: Extended follow-up of a pragmatic, multicentre randomized trial cohort - The WHICH? study (Which Heart Failure Intervention Is Most Cost-Effective & Consumer Friendly in Reducing Hospital Care). Int J Cardiol. 2015;201:368-75. [CrossRef]
- Miura Y, Fukumoto Y, Shiba N, Miura T, Shimada K, Iwama Y, et al. Prevalence and clinical implication of metabolic syndrome in chronic heart failure. Circ J. 2010;74(12):2612-21. [CrossRef]
- Alberti KG, Zimmet P, Shaw J. Metabolic syndrome--a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med. 2006;23(5):469-80. [CrossRef]
- Purwowiyoto SL, Prawara AS. Metabolic syndrome and heart failure: mechanism and management. Med Pharm Rep. 2021;94(1):15-21. [CrossRef]
- van der Hoef CCS, Boorsma EM, Emmens JE, van Essen BJ, Metra M, Ng LL, et al. Biomarker signature and pathophysiological pathways in patients with chronic heart failure and metabolic syndrome. Eur J Heart Fail. 2023;25(2):163-73. [CrossRef]
- Roytman AP, Sedova NA, Godkov MA. Laboratory indicators of pathological changes in patients with chronic heart failure with metabolic syndrome. Klin Lab Diagn. 2021;66(2):75-9. [CrossRef]
- Bossone E, Arcopinto M, Iacoviello M, Triggiani V, Cacciatore F, Maiello C, et al. Multiple hormonal and metabolic deficiency syndrome in chronic heart failure: rationale, design, and demographic characteristics of the T.O.S.CA. Registry. Intern Emerg Med. 2018;13(5):661-71. [CrossRef]
- Kearney MT. Chronic heart failure: a missing component of the metabolic syndrome? Diab Vasc Dis Res. 2009;6(3):145. [CrossRef]
- Nichols GA, Amitay EL, Chatterjee S, Steubl D. The Bidirectional Association of Chronic Kidney Disease, Type 2 Diabetes, Atherosclerotic Cardiovascular Disease, and Heart Failure: The Cardio-Renal-Metabolic Syndrome. Metab Syndr Relat Disord. 2023;21(5):261-6. [CrossRef]
- Leon-Roman J, Azancot MA, Marouco C, Patricio-Liebana M, Zamora JI, Ramos Terrades N, et al. A New Era in the Management of Cardiorenal Syndrome: The Importance of Cardiorenal Units. Cardiorenal Med. 2025;15(1):174-83. [CrossRef]
- Yaqoob N, Khalid F, Khan MF, Anwar W, Khan MF, Iqbal MH. Prevalence Of Cardiorenal Syndrome In Patients Admitted For Acute Decompensated Heart Failure And Its Correlation With In-Hospital Outcomes. J Ayub Med Coll Abbottabad. 2024;36(4):773-7. [CrossRef]
- Perrone-Filardi P, Savarese G, Scarano M, Cavazzina R, Trimarco B, Minneci S, et al. Prognostic impact of metabolic syndrome in patients with chronic heart failure: data from GISSI-HF trial. Int J Cardiol. 2015;178:85-90. [CrossRef]
- Tadaki S, Sakata Y, Miura Y, Miyata S, Asakura M, Shimada K, et al. Prognostic Impacts of Metabolic Syndrome in Patients With Chronic Heart Failure - A Multicenter Prospective Cohort Study. Circ J. 2016;80(3):677-88. [CrossRef]
- Ricardo SJ, Araujo MYC, Santos LLD, Romanzini M, Fernandes RA, Turi-Lynch BC, Codogno JS. Burden of metabolic syndrome on primary healthcare costs among older adults: A cross-sectional study. Sao Paulo Med J. 2024;142(6):e2023215. [CrossRef]
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373-83. [CrossRef]
- Radu CP, Chiriac DN, Vladescu C. Changing patient classification system for hospital reimbursement in Romania. Croat Med J. 2010;51(3):250-8. [CrossRef]
- Bonapace S, Mantovani A. Do Sex and Gender-Related Differences Account to Different Risk of Developing Heart Failure in Middle-Aged People with Metabolic Syndrome? Metabolites. 2024;14(10). [CrossRef]
- Chandra A, Skali H, Claggett B, Solomon SD, Rossi JS, Russell SD, et al. Race- and Gender-Based Differences in Cardiac Structure and Function and Risk of Heart Failure. J Am Coll Cardiol. 2022;79(4):355-68. [CrossRef]
- Ciutac AM, Pana T, Dawson D, Myint PK. Sex-related differences in heart failure patients: physiological mechanisms of cardiovascular ageing and evidence-based sex-specific medical therapies. Ther Adv Cardiovasc Dis. 2025;19:17539447241309673. [CrossRef]
- Kim TE, Kim DY, Kim H, Kim SH. Sex and Age Differences in the Impact of Metabolic Syndrome on Heart Failure Development. Metabolites. 2024;14(12). [CrossRef]
- Yang X, Wen Y, Peng H, Zhu H, Wang WE, Zhou J. Gender Differences in Anxiety, Depression, Insomnia, and Quality of Life in Heart Failure With Preserved Ejection Fraction: A Multicenter, Cross-sectional Study. J Cardiovasc Nurs. 2023;38(5):425-32. [CrossRef]
- Tapia J, Basalo M, Enjuanes C, Calero E, Jose N, Ruiz M, et al. Psychosocial factors partially explain gender differences in health-related quality of life in heart failure patients. ESC Heart Fail. 2023;10(2):1090-102. [CrossRef]
- Lim A, Benjasirisan C, Tebay J, Liu X, Badawi S, Himmelfarb CD, et al. Gender Differences in Disease Burden, Symptom Burden, and Quality of Life Among People Living With Heart Failure and Multimorbidity: Cross-Sectional Study. J Adv Nurs. 2025. [CrossRef]
- Shi K, Zhang G, Fu H, Li XM, Jiang L, Gao Y, et al. Sex differences in clinical profile, left ventricular remodeling and cardiovascular outcomes among diabetic patients with heart failure and reduced ejection fraction: a cardiac-MRI-based study. Cardiovasc Diabetol. 2024;23(1):266. [CrossRef]
- Tang WHW. Targeting Inflammation in Heart Failure Prevention: Are There Sex Differences? JACC Heart Fail. 2025;13(3):450-2. [CrossRef]
- Fluschnik N, Strangl F, Kondziella C, Gossling A, Becher PM, Schrage B, et al. Gender differences in characteristics and outcomes in heart failure patients referred for end-stage treatment. ESC Heart Fail. 2021;8(6):5031-9. [CrossRef]
- Saldarriaga C, Garcia-Arango M, Valentina Lopez L, Contreras J. Sex Differences in Worsening Heart Failure: Learning From Real-world Evidence. J Card Fail. 2024;30(8):991-3. [CrossRef]
- Kocabas U, Kivrak T, Yilmaz Oztekin GM, Tanik VO, Ozdemir I, Kaya E, et al. Gender-related clinical and management differences in patients with chronic heart failure with reduced ejection fraction. Int J Clin Pract. 2021;75(3):e13765. [CrossRef]
- Cediel G, Codina P, Spitaleri G, Domingo M, Santiago-Vacas E, Lupon J, Bayes-Genis A. Gender-Related Differences in Heart Failure Biomarkers. Front Cardiovasc Med. 2020;7:617705. [CrossRef]
- Lee SY, Park SM. Sex differences in diagnosis and treatment of heart failure: toward precision medicine. Korean J Intern Med. 2025;40(2):196-207. [CrossRef]
- Qiu W, Cai A, Wu S, Zhu Y, Zheng H, Feng Y. Sex- and age-specific differences in the associations between comorbidity and incident heart failure. QJM. 2025. [CrossRef]
- Qiu W, Wang W, Wu S, Zhu Y, Zheng H, Feng Y. Sex differences in long-term heart failure prognosis: a comprehensive meta-analysis. Eur J Prev Cardiol. 2024;31(17):2013-23. [CrossRef]
- Chen CC, Chiu CC, Hao WR, Hsu MH, Liu JC, Lin JL. Sex differences in clinical characteristics and long-term clinical outcomes in Asian hospitalized heart failure patients. ESC Heart Fail. 2024;11(5):3095-104. [CrossRef]
- Salem K, ElKhateeb O. Gender-adjusted and age-adjusted economic inpatient burden of congestive heart failure: cost and disability-adjusted life-year analysis. ESC Heart Fail. 2017;4(3):259-65. [CrossRef]
- Cremers HP, Theunissen LJHJ, Essers PPM, van de Ven ART, Spee R, Verbunt R, et al. Gender differences in Heart Failure; Data on Outcomes and Costs. European Society of Cardiology (Virtual Journal). 2020. DOI:.
- Janwanishstaporn S, Karaketklang K, Krittayaphong R. National trend in heart failure hospitalization and outcome under public health insurance system in Thailand 2008-2013. BMC Cardiovasc Disord. 2022;22(1):203. [CrossRef]
- Aizpuru F, Millan E, Garmendia I, Mateos M, Librero J. Hospitalizations for heart failure: Epidemiology and health system burden based on data gathered in routine practice. Medicina Clínica Práctica. 2020;3(4-5):100140. [CrossRef]
- Alosaimi FD, Abalhassan M, Alhaddad B, Alzain N, Fallata E, Alhabbad A, Alassiry MZ. Prevalence of metabolic syndrome and its components among patients with various psychiatric diagnoses and treatments: A cross-sectional study. Gen Hosp Psychiatry. 2017;45:62-9. [CrossRef]
- Nguyen NT, Nguyen TN, Nguyen KM, Tran HPN, Huynh KLA, Hoang SV. Prevalence and impact of metabolic syndrome on in-hospital outcomes in patients with acute myocardial infarction: A perspective from a developing country. Medicine (Baltimore). 2023;102(45):e35924. [CrossRef]
- Park HJ, Jung JH, Han K, Shin J, Lee Y, Chang Y, et al. Association between metabolic syndrome and mortality in patients with COVID-19: A nationwide cohort study. Obes Res Clin Pract. 2022;16(6):484-90. [CrossRef]
- Checa C, Canelo-Aybar C, Suclupe S, Ginesta-Lopez D, Berenguera A, Castells X, et al. Effectiveness and Cost-Effectiveness of Case Management in Advanced Heart Failure Patients Attended in Primary Care: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022;19(21). [CrossRef]
- Wang C, Ba Y, Ni J, Huang R, Du X. Role of Telemedicine Intervention in the Treatment of Patients with Chronic Heart Failure: A Systematic Review and Meta-analysis. Anatol J Cardiol. 2024;28(4):177-86. [CrossRef]
Figure 1.
The prevalence of chronic heart failure (CHF) among sexes (A: 2552 women and 2180 men; p = 0.042) and among patients with or without the metabolic syndrome (B: n = 526 and n = 4206 respectively; p < 0.001).
Figure 1.
The prevalence of chronic heart failure (CHF) among sexes (A: 2552 women and 2180 men; p = 0.042) and among patients with or without the metabolic syndrome (B: n = 526 and n = 4206 respectively; p < 0.001).
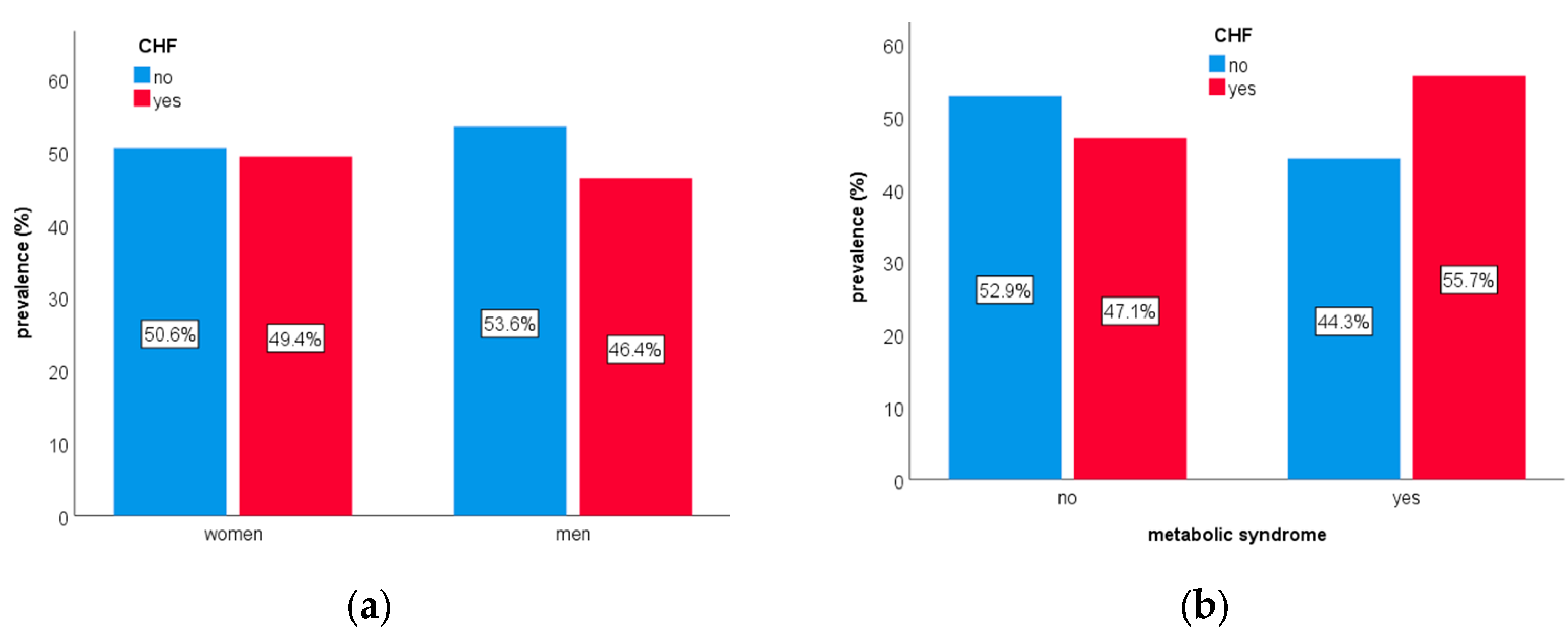
Figure 2.
Differences among patients with or without chronic heart failure (CHF) in terms of age (A; p = 0.042), hospitalization duration (B; p < 0.001), cost of hospitalization (C; p < 0.001) and CCI score without including CHF (D; p < 0.001). Note: hospitalization duration and cost of hospitalization are reported as natural logarithms.
Figure 2.
Differences among patients with or without chronic heart failure (CHF) in terms of age (A; p = 0.042), hospitalization duration (B; p < 0.001), cost of hospitalization (C; p < 0.001) and CCI score without including CHF (D; p < 0.001). Note: hospitalization duration and cost of hospitalization are reported as natural logarithms.
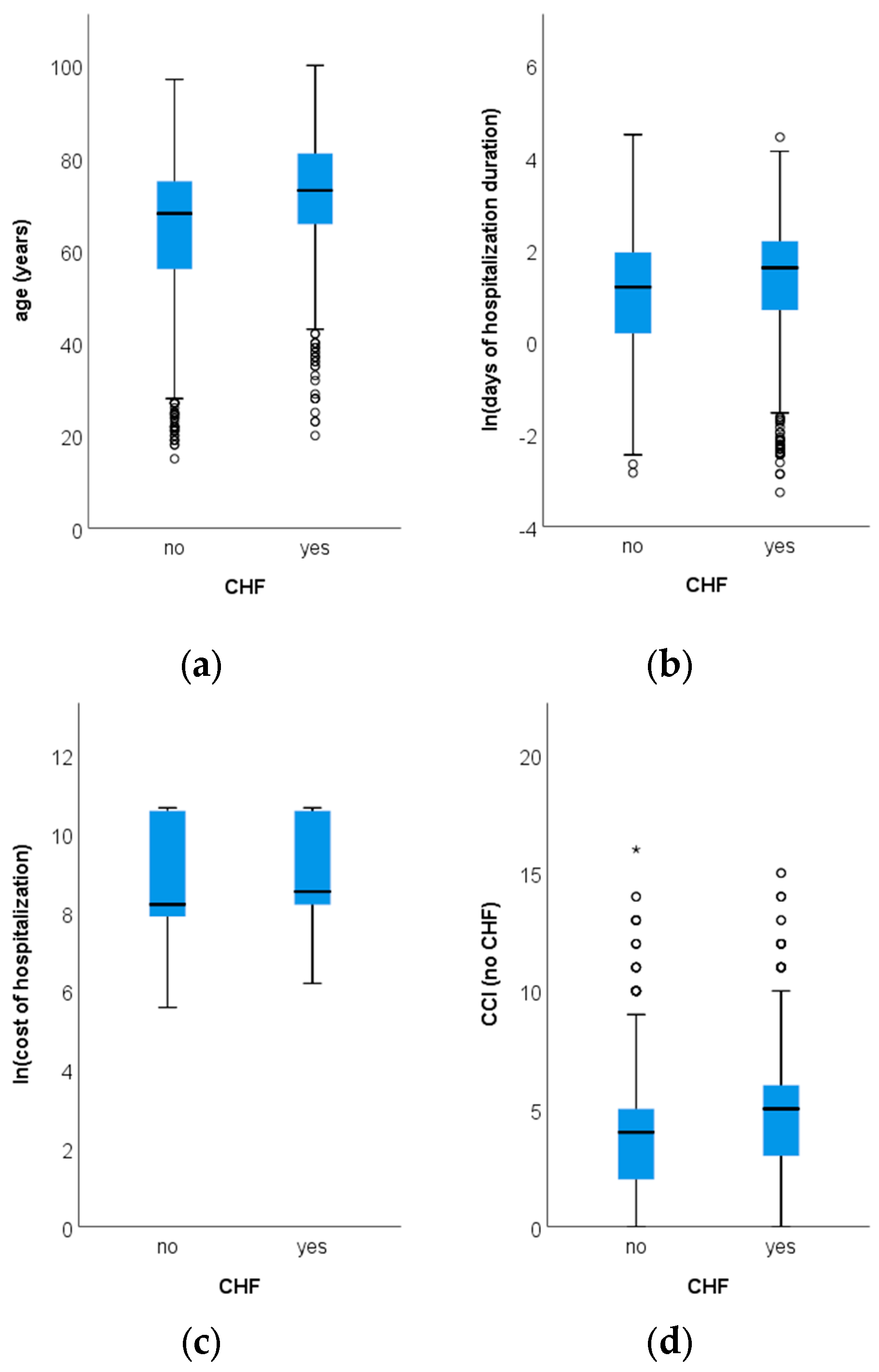
Figure 3.
The median total hospitalization cost (€) in patients with or without chronic heart failure (CHF), metabolic syndrome (MetS) and their combinations (Mann Whitney H = 162 (3), p < 0.001).
Figure 3.
The median total hospitalization cost (€) in patients with or without chronic heart failure (CHF), metabolic syndrome (MetS) and their combinations (Mann Whitney H = 162 (3), p < 0.001).
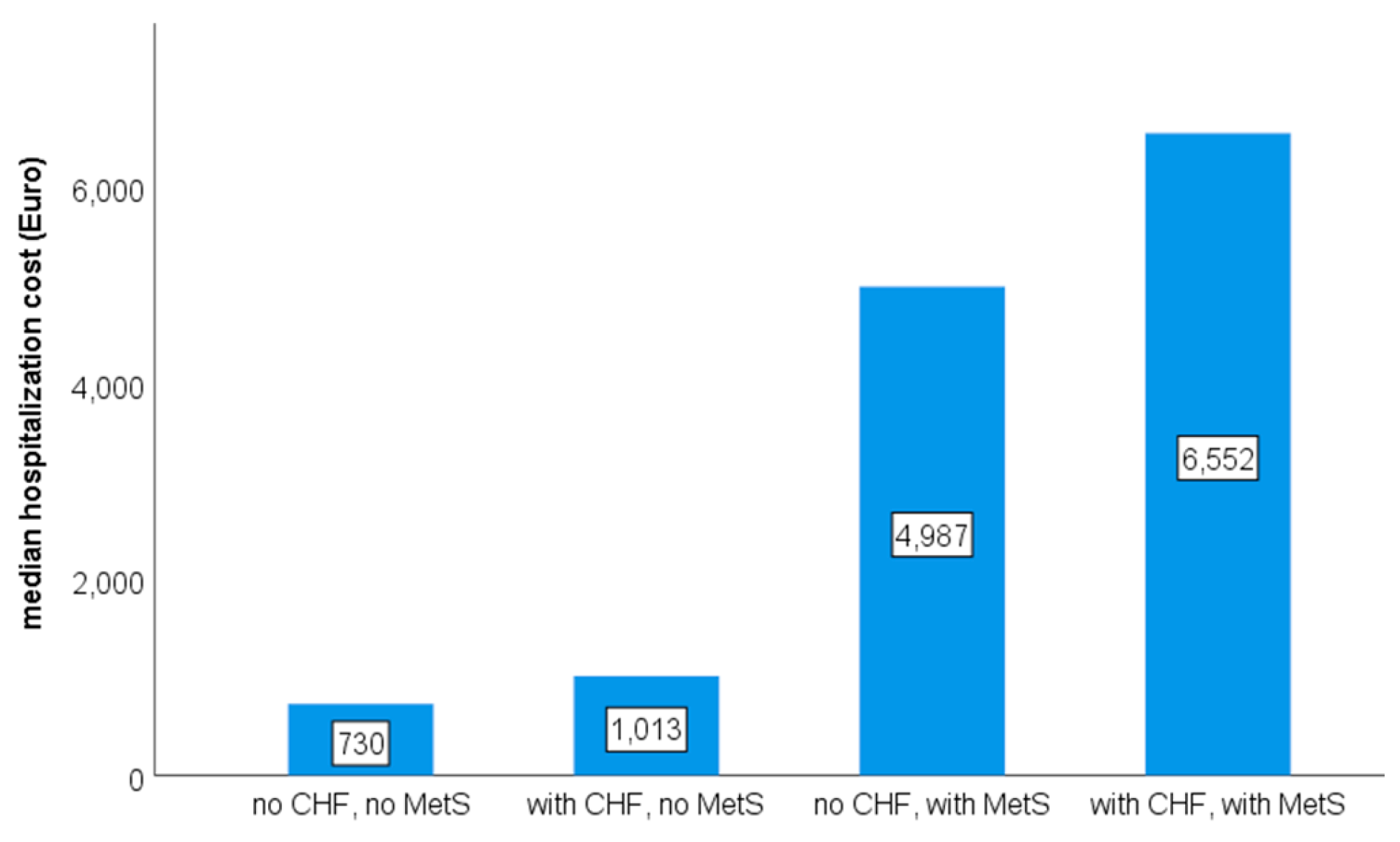

Table 1.
ICD10 codes for the studied diagnoses.
| diagnosis | ICD10 code |
|---|---|
| chronic heart failure | I50 |
| myocardial infarction | I21, I25 |
| peripheral vascular disease | I73 |
| cerebrovascular disease | I60, I61, I63, I64, I67, G45.8, G45.9 |
| dementia | F00, F01, F03 |
| chronic pulmonary disease | J44 |
| rheumatic disease | M05, M06, M45, L40.5, M07, M32, M33, M34, M35 |
| peptic ulcer disease | K27 |
| cirrhosis | K70, K71, K74, K76 |
| variceal bleeding | I85.0, I98.3 |
| diabetes mellitus | E10, E11, E12, E13, E14 |
| hemiplegia | G81 |
| chronic kidney disease | N18 |
| solid tumor | C |
| metastatic cancer | C78, C79, C80 |
| leukemia | C90, C91, C92, C93, C94, C95 |
| lymphoma | C81, C82, C83, C84, C85, C86, C88 |
| AIDS | B20, B21, B22, B23, B24 |
| obesity | E66 |
| arterial hypertension | I10 |
| dyslipidemia | E78 |
Abbreviations: AIDS - acquired immune-deficiency syndrome; ICD10 – International Classification of Diseases version 10.
Table 2.
General characteristics (n = 4732).
| variable | observed |
|---|---|
| women | 53.9% |
| men | 46.1% |
| age (years, average ± SD) | 68.7 ± 13.4 |
| hospitalization duration (days, median (IQR) | 4.0 (5.9) |
| total cost of hospitalization (€, median (IQR)* | 1002 (7338) |
| cost per day of hospitalization (€, median (IQR)* | 322 (1477) |
| Charlson Comorbidity Index (average ± SD) | 4.8 ± 2.5 |
Notes: * approximate exchange rate of 5 Romanian leu for 1 €; IQR - interquartile range; SD - standard deviation.
Table 3.
Prevalence of diagnoses included in the CCI and metabolic syndrome definition (n = 4732).
| diagnosis | prevalence | diagnosis | prevalence |
| chronic heart failure | 48.0% | hemiplegia | 0.4% |
| myocardial infarction | 18.8% | chronic kidney disease | 19.8% |
| peripheral vascular disease | 0.9% | solid tumor | 8.7% |
| cerebrovascular disease | 6.5% | metastatic cancer | 2.8% |
| dementia | 4.8% | leukemia | 0.5% |
| chronic pulmonary disease | 9.6% | lymphoma | 0.3% |
| rheumatic disease | 2.9% | AIDS | 0.1% |
| peptic ulcer disease | 0.0% | obesity | 19.8% |
| cirrhosis | 17.3% | arterial hypertension | 50.0% |
| variceal bleeding | 0.0% | dyslipidemia | 38.5% |
| diabetes mellitus | 30.5% | metabolic syndrome | 11.1% |
Abbreviations: AIDS - acquired immune-deficiency syndrome; CCI - Charlson Comorbidity Index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



