Submitted:
05 April 2025
Posted:
08 April 2025
Read the latest preprint version here
Abstract
Small intestinal bacterial overgrowth (SIBO) has recently garnered significant attention from both medical professionals and the general public, likely due to its increasing prevalence and advancements in testing technology. However, the accuracy of breath tests in clinical practice for diagnosing SIBO still requires thorough validation. This review compiles the definition, etiology, influencing factors, novel testing methods, and the determination and interpretation of SIBO results. We particularly discuss the various controversies and limitations associated with these tests. By comparing and evaluating the advantages and disadvantages of different diagnostic methods for SIBO, we aim to enhance the understanding of its clinical diagnosis and promote future research focused on accurate detection methods.
Keywords:
Small intestinal bacterial overgrowth
; Breath test
; Methane
; Lactulose Breath Test
; Glucose Breath Test
1. Introduction
The gut microbiota in the human body consists of approximately 1014 microbial monomers, which is more than tenfold the number of cells in the human body, and plays a crucial role in regulating host health. As one of the most diverse ecosystems, the gut microbiota may encompass up to 1,500 different species, each as individual and unique as a fingerprint [1,2]. Recent advancements in molecular techniques have revealed that the gene content of microorganisms inhabiting our gastrointestinal tract (GIT)—including bacteria, archaea, viruses, fungi, and eukaryotic parasites—is more extensive than that of their human host [3]. The microbiota plays a pivotal role in overall host health and disease susceptibility [4], as it is essential for vital functions such as digestion, immune system regulation, and the production of nutrients and metabolites in the human body [5,6].
The oral and salivary microbiomes of a healthy individual harbor millions of microbes that are ingested daily through food. However, duodenal aspirates reveal a microbial abundance that is a thousandfold lower than that of oral samples, a phenomenon attributed to the acidity of gastric juice, the activity of digestive enzymes, the production of bile acids (BAs) both within the duodenum, and the presence of antimicrobial proteins [7]. Furthermore, various dynamic conditions, such as rapid transit times ranging from 2 to 5 hours in the small intestine and exceeding 10 hours in the colon, a broad pH spectrum, bodily secretions, and relatively high oxygen levels that diminish from the duodenum to the ileum, contribute to an oxygen gradient between the mucosa and the lumen. This gradient, along with the modulation of facultative anaerobes on oxygen availability in conjunction with dietary nutrients, fosters unique and specialized niches for microbial communities. From the duodenum to the large intestine, microbial concentrations escalate from 103 CFU/mL to 1011 CFU/mL, with the highest density observed in the colon [8,9,10].
In recent years, ethical restrictions have led to a disproportionately high proportion of samples being collected from patients with intestinal disorders rather than from healthy individuals. This has resulted in significant heterogeneity in the taxonomic composition of the current microbiome; however, general trends can still be observed [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25].
Microorganisms exhibit differences at the phylum level across various sections of the digestive tract. The Firmicutes phylum dominates the stomach and duodenum, constituting 50% to 56% of the total bacterial population. In contrast, the Proteobacteria phylum is the most prevalent in the ileum, accounting for 48% of the bacterial community. Furthermore, the Bacteroidetes phylum demonstrates greater abundance within the lower GIT, compared to the stomach and duodenum [26]. Nonetheless, the application of next-generation sequencing technology has significantly advanced our understanding of the small intestinal microbiota (SIM) to the level of genus classification. The core constituents of the microbiota, such as Streptococcus, Veillonella, Prevotella, Fusobacterium, and Haemophilus, can be identified by their inherent characteristics in the small intestine, regardless of the specific section sampled [17,18,27].
The microbiota is intricately linked to the overall health and susceptibility to disease of the host [28,29]. The gut microbiome enhances the immune function of the entire body by hindering the colonization and growth of pathogens through competitive exclusion mechanisms [30]. Furthermore, the microbiota improves intestinal barrier function by upregulating the activity of pattern recognition receptors (e.g., NOD2 and NLRP6), which increases the secretion of antimicrobial peptides and mucus. It also strengthens mucosal barriers and suppresses excessive inflammation by enhancing cytokine secretion (e.g., IL-22) through innate lymphoid cells (ILCs), thereby maintaining immune homeostasis [6,31]. Additionally, the gut microbiota promotes carbohydrate degradation and short-chain fatty acid (SCFA) production by upregulating carbohydrate-active enzymes (CAZymes), thus enhancing energy acquisition [13,23]. In terms of amino acid metabolism, the microbiota increases the availability of essential amino acids through degradation and synthesis [32]. In lipid metabolism, it regulates bile acid metabolism to promote fat storage (e.g., via L-lactate produced by Lactobacillus) and enhance fat oxidation (e.g., via acetate produced by Escherichia coli), thereby modulating host energy balance [33,34].
SIBO is primarily characterized by the overgrowth of Gram-negative aerobic and anaerobic bacteria [35]. This condition is closely linked to dysfunction of the ileocecal valve, impaired motility of the small intestine, and reduced secretion of gastric acid [36]. Studies have shown that low ileocecal valve pressure (< 54.5 mmHg) is significantly correlated with SIBO, suggesting that dysfunction of the ileocecal valve leads to reflux of colonic contents into small intestinal, thereby promoting bacterial overgrowth [37].Additionally, prolonged small bowel transit time (> 6.75 hours) is independently associated with SIBO, indicating that delayed clearance of intestinal contents provides a favorable environment for bacterial proliferation [38]. Finally, an elevated gastric pH (> 2.05) is linked to SIBO, implying that insufficient gastric acid secretion diminishes the stomach's antimicrobial function, thereby increasing the risk of bacterial colonization in the small intestine [39]. Collectively, these mechanisms contribute to the development of SIBO.
This paper summarizes the etiology, clinical manifestations, and effective diagnostic strategies of SIBO and its impact on the human body. Additionally, it provides a brief overview of the interrelationships between related diseases and the development of SIBO, aiming to identify new directions for microbiological research that may enhance our understanding of gastrointestinal diseases and facilitate the development of new treatment strategies.
2. Pathophysiology and Influence on SIBO
2.1. The Pathophysiology of SIBO
The gut microbiota exists in a state of dynamic equilibrium, influenced by a multitude of internal and external factors [2]. Any perturbation to the structure or function of the intestines can disrupt this normal balance, potentially leading to the emergence of SIBO [28]. (Figure A1).
2.1.1. Abnormalities in GI Structure and Motility
Alterations or disruptions in the structure or motility of the small intestine can lead to increased bacterial colonization, thereby predisposing individuals to certain conditions. Bani et al. found that the mean small bowel transit time (SBTT) was 6.6 hours in the lactulose breath test (LBT) positive group, with 47.6% experiencing prolonged SBTT (≥ 6 hours). In contrast, the mean SBTT was 4.2 hours in the LBT negative group, where only 7.7% experienced prolonged SBTT (≥ 6 hours) [40]. This confirms that the occurrence of SIBO is associated with decreased small intestinal motility. Numerous studies have also demonstrated that diabetes and connective tissue diseases are significantly linked to gastrointestinal motility disorders, which can induce SIBO [41,42]. Research indicates that approximately 90% of patients with systemic sclerosis exhibit symptoms of gastrointestinal involvement. The elevated levels of serum anti-muscarinic type 3 receptor blocking antibodies contribute to reduced gastrointestinal motility, resulting in a SIBO prevalence rate of about 39% in this population [43,44,45].
A recent investigation involving individuals diagnosed with type 1 diabetes mellitus, both with normal and abnormal cardiovascular autonomy, revealed that SIBO was present in 2 (8%) patients with normal cardiovascular autonomy and 11 (44%) patients with abnormal cardiovascular autonomy. This suggests that diabetic autonomic neuropathy may play a significant role in the increased prevalence of SIBO [42]. Furthermore, it has been confirmed that several systemic conditions, including hypothyroidism [46], chronic renal failure [47], and various myoneuropathies [48,49], as well as certain collagen diseases such as systemic lupus erythematosus and parkinsonism [50,51], may be associated with reduced intestinal motility.
In addition to the association between delayed gastrointestinal motility and SIBO, abnormal gastrointestinal structure is also related to the occurrence of SIBO. Studies have shown that a history of abdominal surgery is significantly associated with SIBO. A retrospective study found that the positive rate of SIBO in patients after abdominal surgery was significantly higher than that of the control group (84% vs 20%, p < 0.01). Compared to healthy individuals, the prevalence of SIBO after gastrectomy was significantly increased (77.6% vs 6.7%, p < 0.01) [52]. According to current research, changes in gastrointestinal structure, intestinal dysmotility, and microbial imbalance are responsible for the development of SIBO. For instance, the loss of ileocecal valve function, as observed in Crohn's disease (CD) or ileal resection, facilitates the migration of colonic bacteria to the small intestine, and the retention of undigested nutrients promotes the abnormal growth of bacterial groups such as Proteobacteria, which can also lead to the occurrence of SIBO. Additionally, the prevalence of SIBO in patients with CD was found to be 25.3%, with a significantly higher daily frequency of defecation compared to patients without SIBO (5.9 vs 3.7, p = 0.003) [53]. Interestingly, among patients who underwent Roux-en-Y gastric bypass surgery (RYGBS), 72% were found to have thiamine deficiency accompanied by elevated folate levels, while only 34% had elevated folate levels without thiamine deficiency. This indicates a significant association between thiamine deficiency and elevated folate levels in this patient population. Notably, after antibiotic treatment, the thiamine levels of all 21 patients diagnosed with SIBO returned to normal, suggesting that thiamine deficiency caused by anatomical changes may be a key driver of SIBO [54].
2.1.2. Dysfunction of Gut Defense and Immunity Regulation
The occurrence of SIBO is closely linked to dysfunctions in intestinal defense mechanisms and immune regulation. On one hand, dysfunction of the intestinal mucosal barrier, characterized by increased intestinal permeability due to weakened protection by the mucus layer, destruction of tight junction proteins, and insufficient secretion of antimicrobial peptides by Paneth cells, facilitates bacterial adhesion and invasion of the intestinal mucosa [55]. On the other hand, immune dysregulation, which includes abnormal immunoglobulin A (IgA) secretion [56,57], alterations in neutrophil and macrophage activity, and an imbalance between Th17 cells and regulatory T cells (Tregs), results in a decreased capacity for bacterial clearance [58]. Notably, studies have shown that 41% of immunodeficient patients exhibit SIBO, with significantly higher lactulose/L-rhamnose urinary excretion ratios compared to control subjects (0.216 vs 0.029, p < 0.001), indicating that abnormal intestinal permeability predisposes individuals to bacterial overgrowth [59].
2.1.3. Drug, Diseases and Other
Research indicates that the use of proton pump inhibitors (PPIs) or colonization with Helicobacter pylori (HP) is significantly associated with an increased risk of SIBO. Specifically, the risk of SIBO in PPI users is 7.587 times higher than that in non-users (95% CI: 1.805-31.894) [60]. This association may be attributed to the disruption of the gastric acid barrier, alterations in gastrointestinal motility, and immune dysregulation. However, no significant association was found between immunomodulatory drugs (such as thiopurines and biologics) and SIBO, despite the potential for these drugs to influence SIBO development through immune suppression and microbial dysbiosis [61]. These findings suggest that long-term PPI use should be carefully evaluated concerning the risk of SIBO, while the impact of immunomodulatory drugs on SIBO may be overshadowed by other factors [62].
In addition to PPIs, recent studies suggest that probiotics may colonize the small intestine, increasing the susceptibility of patients to SIBO [63]. This finding highlights the complex interplay between exogenous interventions, gut microbiota, and the development of SIBO. The incidence of SIBO in patients with cirrhosis can be as high as 51.1%, with a significant increase in the abundance of Firmicutes and Fusobacteria phyla, while the Bacteroidetes phylum decreases in SIBO patients. This microbial shift is primarily driven by an increase in the genus Blautia of the Lachnospiraceae family, which may influence gut microbiota composition by converting primary BAs into secondary BAs, thereby inducing SIBO [64].
Similarly, the incidence of SIBO in patients with chronic pancreatitis (CP) is significantly higher than that in the general population, estimated to be around 36% (95% CI: 17%-60%). The underlying mechanisms may be related to factors such as fat malabsorption, surgical history, the use of PPIs, motility disorders, and diabetic neuropathy in patients with CP [65]. Beyond these conditions, SIBO is significantly associated with various gastrointestinal, hepatic, endocrine, and systemic diseases. Its prevalence is notably high in patients with functional dyspepsia (FD) (34.7%) [66], irritable bowel syndrome (IBS) (36.7%) [67], celiac disease (18.3%) [68], CD (25.3%) [53], ulcerative colitis (UC) (14.3%) [69], and metabolic-associated fatty liver disease (MAFLD) (35.0%) [70].
Moreover, the severity of SIBO often correlates with disease progression, as observed in conditions such as cirrhosis, Metabolic Associated Fatty Liver Disease (MAFLD), diabetes, and pancreatitis. Worsened symptoms are associated with increased bacterial overgrowth.
These findings emphasize the multifactorial nature of SIBO, which is influenced by underlying diseases, medication use, alterations in gut microbiota, and immune modulation. A comprehensive approach is essential for assessing SIBO risk factors and optimizing management strategies for affected patients.
2.2. The Influence of SIBO on Human Body
The clinical manifestations of SIBO exhibit significant variability. Initially, SIBO was regarded as a potential contributor to maldigestion and malabsorption [28,30,71]. Furthermore, patients with SIBO often present with IBS-like symptoms, which encompass a range of nonspecific gastrointestinal (GI) complaints, including weight loss, bloating, flatulence, diarrhea, abdominal pain, and distension, particularly in cases of carbohydrate malabsorption [35,72].
Chronic bloating and diarrhea are the most frequently reported symptoms in SIBO, believed to result from the enhanced deconjugation of BAs by intestinal bacteria. This process leads to malabsorption of fats, bacterial metabolism that produces osmotically active substances such as SCFAs, and an increased level of bacterial fermentation, all of which contribute to postprandial bloating [73]. Additionally, SIBO can lead to the production of inactive analogues of vitamins that compete with normal vitamin B12 for binding and absorption, ultimately resulting in vitamin B12 deficiency [74]. Following the nausea and discomfort associated with bloating, patients may begin to avoid eating to prevent these symptoms, which can ultimately lead to poor nutritional intake and weight loss [75].
Previously, experts believed that the dysfunction and symptoms induced by SIBO were confined to the GIT, encompassing conditions such as IBS [76], CD [77], UC, celiac disease [78], liver cirrhosis [79], pancreatitis [65], and non-alcoholic fatty liver disease (NAFLD) [70]. However, an increasing number of hypotheses have emphasized the association of SIBO with a wide range of other diseases, including autoimmune disorders [80,81,82,83,84], cardiovascular diseases [85], metabolic disorders [86], endocrine disorders [87], kidney disease [88,89], dermatological issues [90,91], neurological diseases [92], and mental disorders [93,94,95,96]. Furthermore, genetic diseases and gastrointestinal cancers [97] have also been linked to SIBO. Thus, SIBO emerges as a risk factor that complicates the progression of these diseases and potentially plays a pathogenic role in the manifestation of their symptoms (Figure A2; Table A1 and Table A2).
The table presents data on disease types, average patient age, sample size, diagnostic test methods, diagnostic criteria, and prevalence rates. The findings indicate that the prevalence rates of SIBO across different diseases range from 3% to 73.4%, highlighting substantial variability in the prevalence of SIBO among various conditions. This variability may be attributed to the types of diseases, regional differences, and discrepancies in diagnostic methods and criteria.
3. The Diagnosis of SIBO and Current Challenges
3.1. Duodenal/Jejunal Fluid Aspirate Culture
Currently, there is no definitive diagnostic method for SIBO. The duodenal/jejunal fluid aspiration culture is an invasive testing procedure that necessitates sample acquisition via intubation. The general protocol involves the insertion of an endoscope into the duodenum or jejunum, followed by the introduction of a sterile catheter through the endoscope's biopsy channel. Subsequently, 2-5 mL of duodenal/jejunal fluid is aspirated and transferred to a sterile container or transport medium. The aspirate is then inoculated onto appropriate culture media (e.g., blood agar, MacConkey agar) and incubated under both aerobic and anaerobic conditions. Finally, the colony-forming units (CFU/mL) of bacteria in the aspirate are quantified. In contrast to breath tests (e.g., hydrogen and methane breath tests), which are less invasive but also less specific, the duodenal/jejunal aspirate culture provides direct evidence of bacterial overgrowth and can identify specific pathogens. Therefore, the duodenal/jejunal aspirate culture is regarded as the accepted gold standard for diagnosing SIBO, with cut-off levels reported as > 10³ or ≥ 10⁵ CFU/mL for the definition of SIBO [35,98,99,100,101,102,103,104,105]. A systematic review and meta-analysis indicated that the combined prevalence of SIBO in diabetic patients is 29% (95% CI 20–39%). Notably, the prevalence of SIBO in diabetic patients was higher in studies utilizing jejunal aspiration cultures (39%, 95% CI 12-66%) and lower in studies employing the LBT (31%, 95% CI 18-43%) or glucose breath test (GBT) (29%, 95% CI 14-43%) [106].
However, significant drawbacks of this invasive examination include considerable pain for patients, high costs, time consumption, poor reproducibility, lack of standardization, and high technical requirements, all of which limit its clinical applicability [107,108,109,110,111]. More importantly, the unreliability of this method stems from the fact that only 30% of intestinal bacteria can be cultured, primarily due to unavoidable contamination from oral bacteria. This method is unsuitable for detecting SIBO in the distal small intestine, as the aspirate is typically collected from the proximal duodenum or jejunum, while many SIBO cases are caused by the displacement of colonic bacteria into the distal small intestine. Duodenal/jejunal aspirate culture remains the gold standard for diagnosing SIBO due to its high diagnostic accuracy and capability to identify specific pathogens [107,112,113,114,115,116]. In complex cases, such as those involving cystic fibrosis or diabetes, duodenal/jejunal aspirate culture is invaluable for guiding targeted treatment [106]. However, its invasiveness and cost limit its widespread use, making breath tests a more practical initial screening tool.
3.2. Hydrogen Breath Tests
Recently, breath test methods (GBT and/or LBT) for detecting SIBO have garnered increasing attention. These breath tests are proposed as sensitive and straightforward diagnostic tools for bacterial overgrowth, offering a non-invasive and cost-effective alternative to the gold standard, which involves the culture of intestinal aspirates [35,36,98,105,113,117].
The standardized testing process is crucial for ensuring the accuracy and reliability of test results. Determining the correct substrate dosage is essential for optimizing the sensitivity and specificity of the experiment. In 2005 and 2009, expert groups from Germany and Italy developed recommendations for breath tests and reached a consensus on hydrogen breath tests [117]. In 2017, the North American consensus on breath tests recommended that patients discontinue antibiotics for at least four weeks and avoid laxatives for at least one week prior to undergoing a breath test. Patients should follow a light diet and refrain from consuming fermented foods one day before the test. Additionally, patients must fast for 8 to 12 hours before the breath test. On the day of the test, smoking and vigorous activities should be minimized. The recommended dosage for the breath test is 10 grams of lactulose in the LBT and 75 grams of glucose in the hydrogen breath test (HBT), mixed with a glass of water or taken sequentially. During the breath test, the carbohydrates ingested by the patient are metabolized by the gastrointestinal microbiota, producing hydrogen and methane. Some of these gases are absorbed into the bloodstream through the digestive tract and are ultimately exhaled through the alveoli. Therefore, analyzing the changes in gas metabolites in exhaled samples after carbohydrate intake can indirectly detect SIBO. Hydrogen, methane, and carbon dioxide should be measured simultaneously during the breath test [113]. (Figure A3).
The standardization of breath test result interpretations can significantly enhance diagnostic accuracy. In the conducted experiment, an increase in hydrogen concentration of ≥ 20 ppm from baseline within 90 minutes is indicative of a positive detection of SIBO. When the bacterial level threshold for SIBO was set at 10⁵ CFU/mL, the sensitivity of the breath test was found to be 64% at 12 ppm and 48% at 20 ppm, while the specificity was 78% and 86%, respectively. Notably, the breath test demonstrated lower sensitivity but higher specificity for SIBO detection at 20 ppm compared to 12 ppm [35,98,113].
According to a systematic review, the sensitivity of the LBT for SIBO ranges from 31% to 68%, with specificity ranging from 44% to 100%. In contrast, the sensitivity of the GBT varies from 20% to 93%, and its specificity ranges from 30% to 86%, when compared to cultures obtained from small bowel aspirates [6,14]. Lactulose, a non-absorbable synthetic sugar, traverses the entire small intestine and reaches distal regions where bacterial overgrowth may occur, thereby enhancing sensitivity to approximately 60% for detecting SIBO in both proximal and distal segments. However, lactulose can also ferment in the colon, which may lead to lower specificity. In contrast, glucose is rapidly absorbed in the proximal small intestine, improving specificity to approximately 70%, but it may miss distal cases, resulting in lower sensitivity [35,98,113,117,118,119].
Numerous studies have demonstrated that breath tests, such as LBT and GBT, are less invasive and more accessible alternatives for diagnosing SIBO. However, these tests exhibit lower sensitivity and specificity when compared to duodenal or jejunal aspirate culture. For instance, one study reported that GBT achieved a sensitivity of 71.4% and a specificity of 92.3% relative to jejunal aspirate culture [120]. Furthermore, the hydrogen breath test serves as a non-invasive and cost-effective diagnostic tool for SIBO; however, it necessitates strict adherence to established protocols to enhance accuracy. Clinical correlation with patient symptoms and risk factors is crucial for accurate interpretation of results. Consequently, in cases of ambiguity, additional testing or empirical treatment may be necessary [121].
3.3. Methane Breath Tests
Apart from HBT, methane breath testing (MBT) serves as a non-invasive and accessible alternative, currently recognized as the clinical standard for diagnosing SIBO [122,123]. Methane is produced by anaerobic methanogens in the large intestine, with its production influenced by factors such as race, diet, gut microbiota, and intestinal transit time. High-fiber diets are associated with increased methane output, whereas diets rich in animal protein or fat may reduce the availability of fermentable substrates, consequently lowering methane production. Extended colonic transit time provides more opportunity for microbial fermentation, which correlates with increased methane production; thus, constipation is often associated with elevated methane levels. Some studies indicate a higher prevalence of methane in specific populations, although these variations likely reflect differences in dietary patterns, cultural practices, or environmental exposures [124,125,126,127,128,129,130,131,132,133].
In breath tests, an increase in methane concentration of 5 ppm within 90 minutes following the oral ingestion of either 75 g of glucose or 10 g of lactulose is considered to have the same biological significance as an increase in hydrogen concentration of 20 ppm, which is the widely accepted diagnostic criterion for an abnormal breath test [113]. In clinical practice, however, cutoff values of ≥ 5 ppm and ≥ 10 ppm are used to predict excessive methanogenesis for the diagnosis of SIBO, with specificities of 99.7% and 100%, and sensitivities of 96.1% and 86.4%, respectively. Despite this, there is currently insufficient research to clearly establish whether methane levels ≥ 3 ppm should be classified as abnormal. Therefore, clinicians must judiciously assess the significance of methane levels ≥ 3 ppm based on the individual circumstances of their patients [35,113,134,135].
Simultaneous detection of hydrogen and methane levels in exhaled breath can enhance the accuracy of SIBO diagnosis in breath tests [136,137,138,139]. In a study cohort comprising 1,461 patients, 484 (33.1%) were diagnosed as SIBO positive. Among these SIBO positive patients, 241 (49.8%) produced only hydrogen (H2), 188 (38.8%) produced only methane (CH4), and 55 (11.4%) produced both hydrogen and methane simultaneously [20]. Additionally, total gas production was positively correlated with age in CH4-SIBO positive patients; however, a higher proportion of patients with diabetes exhibited elevated levels of hydrogen [130,140].
The characteristic of intestinal methane-producing bacteria overgrowth (IMO) is the excessive presence of methane-producing bacteria in the intestine. Methanogenic bacteria belong to the archaeal domain and can also proliferate in the colon, not just in the small intestine. A concentration of 10 ppm of methane at any time during the testing period indicates the colonization of methanogenic bacteria. Currently, the diagnosis of small intestinal IMO is typically conducted using a 2-hour breath test. According to the 2020 ACG guidelines, a positive diagnosis for IMO is defined as an increase in hydrogen gas exceeding the baseline value by ≥ 20 ppm for 90 minutes, alongside an increase in methane by ≥ 10 ppm [35]. The North American Consensus states that supplementing the measurement of respiratory methane concentration can enhance the sensitivity of the test; a methane level of ≥ 10 ppm during a fasting breath test is considered diagnostic for IMO. This method demonstrates a sensitivity of 86.4% and a specificity of 100% when compared to the standard GBT or LBT, which are more complex and time-consuming [113]. A single fasting methane breath measurement (SMM) streamlines the diagnostic process, eliminating the need for lengthy tests like LBT and GBT, thereby making it more suitable for clinical applications. IMO is characterized by the overgrowth of methane-producing archaea, which slows intestinal transit and is often associated with constipation-predominant symptoms. This approach is particularly beneficial for differentiating IMO from other conditions such as SIBO, which necessitates distinct diagnostic and treatment strategies [28,99,123,129,132,135,141,142,143].
However, due to the varying sugar substrates (glucose and lactulose) and evaluation indicators (hydrogen and methane) employed in breath tests, the sensitivity and specificity of these tests differ significantly. This variability poses substantial challenges for clinical application, necessitating a unified and standardized approach.
3.4. More New Testing Methods of SIBO
The Smart Capsule Bacteria Detection System (SCBDS) is equipped with targeted sampling technology and an on-board detection method specifically designed for identifying metabolically active bacteria in the duodenum. A study involving 66 patients collected and analyzed duodenal aspirates to determine total bacterial count (TBC) and assess SCBDS detection efficacy. The overall agreement between the two detection methods was found to be between 82% and 92%. Additionally, the sensitivity of SCBDS detection ranged from 67% to 100%, while specificity was reported to be between 90% and 97%, utilizing cutoff values of ≥ 10³ or 10⁵ CFU/ml. Thus, SCBDS has demonstrated its potential as a simple and non-invasive tool for aiding in the diagnosis of SIBO, warranting further clinical validation [144].
It has been reported that gas-sensing capsules are telemetric swallowable devices that successfully evaluate the gastric, small, and large intestinal transit times of solid food. These capsules can sense oxygen, hydrogen, and carbon dioxide, measuring concentrations of hydrogen that are over 3000 times higher than those obtained from breath tests [145,146,147,148,149]. Research indicates that the gas-sensing capsule exhibits a sensitivity of 83% and 79%, specificity of 96% and 84%, and accuracy of 94% and 82% when using the standard cutoff values for delayed gastric emptying (> 5 hours) and colonic transit (> 9 hours) [150]. The gas-sensing capsules can pinpoint early H2 spikes in the small intestine, effectively distinguishing SIBO from normal colonic fermentation. The simultaneous detection of O2, CO2, and H2 aids in differentiating gastrointestinal regions; for instance, an early rise in H2 levels may indicate SIBO. CO2 levels can reflect metabolic activity or neutralization processes, which further assists in identifying motility delays. Unlike breath tests that conflate signals from the entire GI tract, gas-sensing capsules provide location-specific data (e.g., small or large intestine) [111,129,151,152]. Moreover, the smart capsule bacterial detection system can sample fluid in the small or large bowel and conduct microbiome analysis to detect SIBO or fungal overgrowth as well [154]. Overall, gas-sensing capsules represent a significant advancement in gastrointestinal diagnostics, offering precise, non-invasive evaluations of transit times across different gut regions, with the potential to revolutionize diagnostics for disorders such as IBS, gastroparesis, and SIBO.
16S rRNA gene sequencing is a technique of amplicon sequencing that targets specific regions of the genome. The core principle involves utilizing the genetic information from the 16S rRNA gene to identify and classify bacterial and archaeal species. This process encompasses five key steps: collecting microbial samples, extracting microbial DNA, performing PCR and library construction, sequencing via high-throughput platforms, and conducting data analysis [155,156,157,158,159]. Some researchers have defined SIBO using high-throughput sequencing. Analysis of duodenal aspirates through 16S rRNA gene sequencing demonstrates high sensitivity and specificity [160,161]. Suspected SIBO cases were evaluated through quantitative culture of duodenal aspirates, and a glucose hydrogen breath test was conducted on the same day. The positive rates for the hydrogen breath test and quantitative culture of duodenal aspirates were 50% and 62%, respectively. Patients diagnosed with SIBO exhibited significantly reduced α-diversity compared to non-SIBO patients, while β-diversity analysis revealed distinct distribution patterns between the two groups. Notably, there was an increased relative abundance of Streptococcus and a decreased relative abundance of Bacteroides [104,162,163,164,165,166]. The bacterial compositions of the mucosal samples from the duodenum, ileum, and sigmoid colon in SIBO-positive subjects were significantly different from those in SIBO-negative subjects (p = 0.039, 0.002, and 0.007, respectively) [167]. Additionally, microbial network connectivity across different SIBO thresholds and predicted microbial metabolic functions were assessed [64,104]. The advantages of 16S rRNA gene sequencing include its universality, conservation, and the fact that it does not require culturing. This method enables effective identification of microbial species and quantification of bacteria and archaea in specific environments, as well as monitoring the presence of probiotics, conditional pathogens, and certain food-borne pathogens within the intestinal tract [64,159].
Recent studies have demonstrated that the scintigraphy-lactulose hydrogen breath test (ScLBT) is an accurate and reproducible diagnostic tool for SIBO[168,169,170]. However, it has been established that the less expensive and radiation-free nutrient challenge test (NCT) cannot replace ScLBT in diagnosing SIBO. In a cohort of 81 patients, SIBO was diagnosed in 32 patients (39.5%) through NCT, while 51 patients (63.0%) were diagnosed through ScLBT, using the diagnostic criterion of a hydrogen increase of more than 10 ppm compared to baseline within 20-90 minutes after the intake of the testing substance [168]. No studies have confirmed the equivalence of NCT and ScLBT in diagnosing SIBO, which may be attributed to the differing testing substances that entail varying orocecal transit times (OCTT). Therefore, further prospective and multicenter studies are warranted to validate the results of the ScLBT [168,169,170,171,172].
4. Diverse Influences Associated with SIBO
4.1. Dietary Standards Vary Before the Methane-Hydrogen Breath Test
The dietary standards prior to conducting a methane or hydrogen breath test are crucial for ensuring accurate results, as certain foods, medications, and activities can interfere with gas production measurements. Smoking can lead to a 3 to 137-fold increase in hydrogen concentrations above baseline levels due to exhaled cigarette smoke; however, most subjects typically return to baseline values within 10 to 15 minutes after smoking [173,174,175,176]. Additionally, excessive ventilation resulting from exercise or overexertion has been recognized as having a significant impact on breath test results [177]. Both physical activity and smoking can alter gut motility and breath gas levels, potentially affecting the outcomes of the tests.
Aside from lifestyle factors such as smoking, exercise, and daily routines, diet is generally considered to be closely linked to the development of digestive system diseases, including IBS. The North American consensus recommends that patients undergo a fasting period of at least 12 hours, with no restrictions on water intake, prior to a breath test. This is to ensure that baseline hydrogen levels accurately reflect fasting conditions and minimize fermentation from undigested food [113]. Evidence from several studies indicates that fasting hydrogen levels in patients with conditions like IBS are significantly elevated compared to healthy individuals (10.1 ± 6.5 ppm vs 5.5 ± 6.2 ppm, p < 0.0001), underscoring the necessity for strict adherence to fasting protocols [178,179,180].
Additional requirements for the HBT include avoiding complex carbohydrates and dairy products the day before the test, as well as fasting for 8 to 12 hours [113]. Similar guidelines are outlined in the 2022 European recommendations, which advise avoiding difficult-to-absorb foods, fermentable carbohydrates, and dietary fiber at least one day prior to the test, along with a fasting period of at least 8 hours [142]. It has been confirmed that fiber and fermentable foods can elevate baseline hydrogen and methane levels (p < 0.01), with a positive correlation observed between hydrogen production in healthy adults and dietary fiber intake from rye [174]. Therefore, a strictly restrictive diet is recommended to enhance the diagnostic quality of the GBT [174]. In addition to dietary restrictions, antibiotics should be discontinued at least 4 weeks before the test, as they can alter gut microbiota. Probiotics, laxatives, stool softeners, PPIs, non-steroidal anti-inflammatory drugs (NSAIDs), and motility agents should all be restricted for 1 week prior to the test [113,181,182,183,184,185]. If baseline hydrogen levels exceed 16 to 20 ppm, the test may be deemed invalid due to improper dietary adherence, necessitating retesting after stricter preparation [113,138].
Therefore, it is recommended to strictly adhere to a low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet. Additionally, the use of antibiotics, probiotics, laxatives, stool softeners, PPIs, NSAIDs, and motility agents should be prohibited. It is also advised to refrain from smoking, drinking alcohol, and excessive ventilation prior to the examination, as well as to maintain a sedentary state during the test to enhance the diagnostic quality of the breath test [186].
4.2. No Standard Diagnostic Methods
The breath test is a simple, non-invasive, and patient-friendly method for diagnosing SIBO. The practicality and low cost of the test make it the preferred diagnostic tool in clinical practice [105]. However, the definition of a positive test about GBT is still not reach a consensus. A rise of ≥ 20 ppm above baseline within 90—180 minutes post-substrate ingestion is widely accepted. But some authors believe that being positive is an increase of > 10 ppm above the baseline value [187,188], or a value of > 20 ppm is independently of the baseline value.
Certain diseases, such as lactose intolerance, IBS, carbohydrate malabsorption, and the use of antibiotics, can significantly influence baseline hydrogen breath test values. Notably, lactose intolerance typically does not elevate baseline hydrogen levels unless the patient has recently ingested lactose or other fermentable carbohydrates. However, if bacterial fermentation occurs due to undigested lactose in the colon, baseline levels may be slightly elevated [189,190,191,192,193,194,195,196,197]. Another consideration is secondary lactose intolerance resulting from celiac disease, which can cause intestinal damage and potentially raise baseline hydrogen levels [198,199,200]. Comorbid conditions, such as carbohydrate malabsorption, which are prevalent among patients with IBS-D, may also lead to elevated baseline levels [201]. Furthermore, chronic malabsorption can result in higher baseline levels due to bacterial adaptation. In contrast to IBS-D, rapid transit may facilitate the early delivery of carbohydrates to the colon, where a higher concentration of bacteria can lead to elevated baseline hydrogen levels [202,203,204]. Additionally, colonic bacterial overgrowth and constipation can increase baseline hydrogen levels due to the ongoing fermentation of residual carbohydrates and the prolonged retention of fermentable substrates [205,206,207,208,209]. Antibiotics exert dual regulatory effects on gut microbiota abundance, potentially decreasing baseline hydrogen levels through bactericidal and bacteriostatic actions, while also promoting the overgrowth of hydrogen-producing bacteria, thereby elevating baseline levels through disruption of the microbiome [210]. In summary, diseases that affect gastrointestinal motility, carbohydrate malabsorption, and gut microbiota abundance can alter baseline hydrogen levels in breath tests, ultimately impacting measurement accuracy.
To ensure accurate baseline measurements, patients must fast and avoid fermentable carbohydrates for at least 12 hours prior to the test [211]. Additionally, patients should refrain from smoking and brushing their teeth, as well as avoid certain medications (e.g., antibiotics, probiotics) before the test to prevent interference with oral bacterial activity and alterations in gut bacteria.
An increase in hydrogen concentrations in breath samples facilitates the diagnosis of SIBO. The North American consensus recommends that the presence of methane levels ≥ 10 ppm is diagnostic of methanogenic overgrowth [211]. Different cutoff times influence the positive rate of breath tests for diagnosing SIBO. According to the North American consensus, 34.5% of patients tested positive at 180 minutes, whereas the positive rate was 28% at 120 minutes [211]. However, another study suggests that the best sensitivity and specificity are achieved at 120 minutes using the lactulose-[13C]urea breath test for diagnosing SIBO [212]. This indicates that further research is needed to determine the optimal cutoff time for SIBO diagnosis. Additionally, the site of bacterial overgrowth in the GIT and the speed of substrate transit also impose limitations on breath tests. Since glucose is readily absorbed in the upper GIT, bacterial overgrowth in the lower GIT may lead to false-negative results [213].
In the detection of SIBO through small intestinal fluid aspiration culture, it is crucial to implement standardized aseptic procedures during sampling to minimize cross-contamination. A sterile catheter, guided by a wire under endoscopic visualization, should be employed for aspiration, which must be confirmed via fluorescence microscopy. The specimen should be promptly sent to the microbiology laboratory for both aerobic and anaerobic bacterial cultures [214]. Multiple systematic reviews of published research indicate substantial heterogeneity in duodenal and jejunal fluid aspirate culture methods, including aspects such as the placement of liquid aspiration, specific locations and quantities of aspirates, sample processing and culture techniques, as well as the interpretation of culture results. For example, duodenal samples from SIBO patients have shown counts that were 4 × 103-fold higher than those from non-SIBO patients when cultured on MacConkey agar (p < 0.0001), and 3.8-fold higher when cultured on blood agar (p < 0.0001) [215,216]. Further limitations of small intestinal aspiration culture for SIBO diagnosis include its cost, invasiveness, time requirements, potential for sample contamination, insufficient validation, culture accuracy, and the possible absence of distal SIBO [211,217]. Consequently, the culture of unwashed endoscopic jejunal mucosal biopsy presents an effective and straightforward alternative to jejunal fluid culture for evaluating jejunal microflora, with sensitivity, specificity, positive predictive value, and negative predictive value in diagnosing SIBO reported as 83.5%, 97.2%, 94.7%, and 91.6%, respectively [218].
The incidence rate of SIBO appears to be influenced by both race and the types of diseases present. In the Japanese population, the incidence of SIBO among patients with FD is reported to be 7.1%, which is significantly lower than the 72.5% observed in the United States (p < 0.05) [219,220]. However, when standardized diagnostic tests and cutoff values are applied, the incidence of SIBO in Functional Gastrointestinal Disorders (FGIDs) within the German population is 34.9%, also lower than that in the United States (p < 0.05) [219,221]. Furthermore, among patients with Inflammatory Bowel Disease (IBD), the incidence of SIBO in the German population is 14.1%, markedly lower than the 46.6% reported in China (p < 0.05) [222,223]. Consistently applying diagnostic criteria reveals that the incidence of SIBO in the Australian population with IBD is 15.2%, which is lower than the 32.6% seen in Brazil (p < 0.05) [224,225]. Additionally, the incidence of SIBO in the Indian population stands at 6.7%, significantly lower than the 33.3% found in China among patients suffering from constipation (p < 0.05) [226,227]. (Table A3)
Table A3 illustrates that the detection rates of SIBO prevalence in IBS, cirrhosis, and chronic pancreatitis vary depending on the diagnostic test employed. The prevalence rates of SIBO, as determined by small bowel aspirate culture, GBT, and LBT, are 33.5%, 20.7%, and 62.3% for IBS; 48.0%, 35.9%, and 52.7% for cirrhosis; and 50%, 26.7%, and 65.3% for chronic pancreatitis, respectively. Notably, the detection rates from jejunal aspirate culture and LBT were significantly higher than those from GBT.
Consequently, it appears challenging to establish a uniform diagnostic method for SIBO across different diseases, necessitating the use of various diagnostic approaches due to factors such as differing races, dietary habits, gut microbiota composition, transit times, examination equipment, and conditions.
4.3. Sensitivity and Specificity of Diagnosis
Typically, LBT yield a higher positive rate compared to GBT, primarily due to the occurrence of false positives resulting from lactulose fermentation in the cecum rather than the small intestine [228,229]. The sensitivity of GBT and LBT varies significantly, ranging from 20% to 93% and 31% to 68%, respectively, while their specificity ranges from 30% to 86% and 44% to 100%, respectively [226]. In a comparative study involving 80 cases of IBS based on the ROME III criteria, duodenal aspirate cultures were positive in 15 IBS patients. Subsequently, breath tests were performed on these 15 positive cases, revealing a positive GBT with a sensitivity of 27% and specificity of 100%, double peaks on LBT with a sensitivity of 0% and specificity of 98%, an early peak on LBT with a sensitivity of 33% and specificity of 65%, and high methane levels on LBT with a sensitivity of 13.3% and specificity of 58.7% [226]. The low sensitivity of GBT may be attributed to the rapid absorption of glucose in the proximal small intestine, which limits its availability as a substrate, or potentially due to a lower bacterial concentration [230]. Despite the low sensitivity and specificity of breath tests, multiple guidelines recommend glucose over lactulose as the substrate for testing, highlighting that LBT cannot be used as a standard for early peaks since the oral delivery time of lactulose typically occurs in less than 90 minutes. Although studies have indicated that the sensitivity of hydrogen sulfide breath tests is superior to that of hydrogen breath tests (93.6% vs. 46.0%) [231], the current limitations of available gas chromatography equipment, which cannot detect hydrogen sulfide, pose a significant challenge to this diagnostic method.
The diagnosis of SIBO typically necessitates the measurement of hydrogen production in the small intestine. This process requires patients to ingest a substantial amount of lactulose or glucose within a short timeframe, followed by monitoring hydrogen levels over the subsequent hours [232]. Furthermore, the LBT primarily reflects intestinal transit time, rather than providing an accurate assessment of bacterial counts in the small intestine, exhibiting low specificity and sensitivity [233]. Additionally, despite the widespread use of these tests, current evidence indicates that their diagnostic value in conditions such as IBS is limited, potentially leading to unnecessary antibiotic usage, which may result in adverse effects and economic burdens [234].
Sensitivity and specificity are critical indicators for evaluating the accuracy of diagnostic tests. In the context of SIBO diagnosis, these metrics are influenced by various factors. An early breath test conducted for diagnosing SIBO in patients with IBS reported a specificity of 100% for the GBT, albeit with a sensitivity of merely 27%. Conversely, the LBT exhibited low sensitivity and specificity, particularly with the double peak and early peak standards [235]. Khoshini's review identified 11 studies that assessed the accuracy of LBT for SIBO, revealing sensitivities ranging from 31% to 68% and specificities from 44% to 100%. The sensitivity of GBT varied from 20% to 93%, while specificity ranged between 30% and 86% [236]. Additionally, research indicates that a fasting level of ≥ 10 ppm can predict excessive methane production, achieving a specificity of 100% and a sensitivity of 86.4%. However, current studies have yet to establish that a positive MBT is attributable to anaerobic methanogenic bacteria in the colon as opposed to the small intestine. This evidence suggests that GBT is superior to LBT for detecting SIBO. Nonetheless, some researchers argue that despite the low sensitivity of glucose hydrogen breath testing, it does not lead to false over-diagnosis of SIBO until a more reliable diagnostic method becomes available [237]. This perspective aligns with the positions of the European Society of Neurogastroenterology and Motility (ESNM) and the American Neurogastroenterology and Motility Society (ANMS) [232].
In summary, HBT and MBT are widely utilized for the non-invasive diagnosis of SIBO due to their simplicity, repeatability, and cost-effectiveness, particularly in patients who are intolerant to invasive procedures. However, their clinical utility is limited by several factors, including the potential for false-positive results in patients with intestinal motility disorders or recent antibiotic use, as well as false-negative outcomes in those with ileal strictures or following proton pump inhibitor therapy. Furthermore, inconsistent standardized protocols for test preparation (e.g., fasting duration, dietary restrictions) and result interpretation (e.g., threshold values for hydrogen and methane levels) across institutions affect inter-study comparability. Notably, breath tests may fail to detect regional bacterial dysbiosis in patients with structural abnormalities, necessitating complementary imaging or invasive procedures for a definitive diagnosis.
The future of breath testing lies in the integration of innovative technologies to enhance accuracy and applicability. The development of portable real-time monitoring devices and machine learning algorithms for analyzing breath curve dynamics could improve test sensitivity and reduce patient burden. Additionally, exploring novel substrates (e.g., mannitol) combined with HBT may provide insights into both bacterial overgrowth and small intestinal absorption dysfunction. Meanwhile, standardized international guidelines for breath test protocols and cutoff values are critical for optimizing clinical implementation. For patients with indeterminate results, a multidisciplinary approach that combines endoscopy, jejunal aspirate culture, and metagenomic sequencing may be warranted. Ultimately, integrating breath testing with host genetics, metabolic profiling, and microbiome analysis could enable personalized management of SIBO, advancing early detection and targeted therapies.
Author Contributions
Yuanyuan Zhang and Pengchun Yang performed most of the review, data analysis and wrote the manuscript;Caihua Yan, Jing Wang and Xue Ran provided partial literature inquiry assistance; Xiaoyan Gao, Gang Lei, Chunmei Ran provided partial literature inquiry and data analysis.Tao Bai,Xiaohua Hou and Chibing Dai performed Writing designed and guidance.All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Health Commission of Hubei Provincial , grant number WJ2021F060.
Institutional Review Board Statement
Ethical review and approval were waived for this study because it utilized publicly available/anonymized data with no identifiable human/animal involvement.
Informed Consent Statement
Not applicable.
Acknowledgments
We sincerely thank Professor Gengqing Song for critical review and revision of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SIBO | small intestinal bacterial overgrowth |
| GIT | gastrointestinal tract |
| BAs | bile acids |
| ILCs | lymphoid cells |
| SCFA | short-chain fatty acid |
| CAZymes | carbohydrate-active enzymes |
| SBTT | small bowel transit time |
| LBT | lactulose breath test |
| GBT | glucose breathtest |
| CD | Crohn's disease |
| RYGBS | Roux-en-Y gastric bypass surgery |
| PPIs | proton pump inhibitors |
| HP | Helicobacter pylori |
| CP | chronic pancreatitis |
| FD | functional dyspepsia |
| IBS | irritable bowel syndrome |
| UC | ulcerative colitis |
| MAFLD | metabolic-associated fatty liver |
| NAFLD | non-alcoholic fatty liver disease |
| DM | diabetes mellitus |
| MBT | methane breath testing |
| HBT | hydrogen breath test |
| IMO | intestinal methane producing bacteria overgrowth |
| SMM | single fasting breath methane measurement |
| SCBDS | Smart Capsule Bacteria Detection System |
| TBC | total bacterial count |
| ScLBT | scintigraphy-lactulose hydrogen breath test |
| OCTT | orocecal transit times |
| NCT | radiation-free nutrient challenge test |
| FODMAP | fermentable oligosaccharides, disaccharides, monosaccharides, and polyols |
References
- de Vos, W.M.; Tilg, H.; Van Hul, M.; Cani, P.D. Gut microbiome and health: mechanistic insights. Gut 2022, 71, 1020–1032. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, C.; Hendry, C.; Farley, A.; McLafferty, E. The digestive system: part 1. Nurs. Stand. 2014, 28, 37–45. [Google Scholar] [CrossRef]
- Hooper, L.V.; Gordon, J.I. Commensal Host-Bacterial Relationships in the Gut. Science 2001, 292, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Vijay, A.; Valdes, A.M. RETRACTED ARTICLE: Role of the gut microbiome in chronic diseases: a narrative review. Eur. J. Clin. Nutr. 2021, 76, 489–501. [Google Scholar] [CrossRef]
- Gentile, C.L.; Weir, T.L. The gut microbiota at the intersection of diet and human health. Science 2018, 362, 776–780. [Google Scholar] [CrossRef]
- Thaiss, C.A.; et al. The microbiome and innate immunity. Nature 2016, 535, 65–74. [Google Scholar] [CrossRef]
- Barlow, J.T.; Leite, G.; Romano, A.E.; Sedighi, R.; Chang, C.; Celly, S.; Rezaie, A.; Mathur, R.; Pimentel, M.; Ismagilov, R.F. Quantitative sequencing clarifies the role of disruptor taxa, oral microbiota, and strict anaerobes in the human small-intestine microbiome. Microbiome 2021, 9, 214. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.M.; Schellekens, R.C.A.; van Rieke, H.M.; Wanke, C.; Iordanov, V.; Stellaard, F.; Wutzke, K.D.; Dijkstra, G.; van der Zee, M.; Woerdenbag, H.J.; et al. Gastrointestinal pH and Transit Time Profiling in Healthy Volunteers Using the IntelliCap System Confirms Ileo-Colonic Release of ColoPulse Tablets. PLOS ONE 2015, 10, e0129076. [Google Scholar] [CrossRef]
- Kiela, P.R.; Ghishan, F.K. Physiology of Intestinal Absorption and Secretion. Best Pr. Res. Clin. Gastroenterol. 2016, 30, 145–159. [Google Scholar] [CrossRef]
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLOS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef]
- Fukui, A.; Takagi, T.; Okayama, T.; Katada, K.; Uchiyama, K.; Ishikawa, T.; Handa, O.; Itoh, Y.; Nakagawa, M.; Naito, Y.; et al. Higher Levels of Streptococcus in Upper Gastrointestinal Mucosa Associated with Symptoms in Patients with Functional Dyspepsia. Digestion 2020, 101, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Seekatz, A.M.; Schnizlein, M.K.; Koenigsknecht, M.J.; Baker, J.R.; Hasler, W.L.; Bleske, B.E.; Young, V.B.; Sun, D. Spatial and Temporal Analysis of the Stomach and Small-Intestinal Microbiota in Fasted Healthy Humans. mSphere 2019, 4, e00126-19. [Google Scholar] [CrossRef] [PubMed]
- Shalon, D.; Culver, R.N.; Grembi, J.A.; Folz, J.; Treit, P.V.; Shi, H.; Rosenberger, F.A.; Dethlefsen, L.; Meng, X.; Yaffe, E.; et al. Profiling the human intestinal environment under physiological conditions. Nature 2023, 617, 581–591. [Google Scholar] [CrossRef]
- Xia, K.; Gao, R.; Wu, X.; Sun, J.; Wan, J.; Wu, T.; Fichna, J.; Yin, L.; Chen, C. Characterization of Specific Signatures of the Oral Cavity, Sputum, and Ileum Microbiota in Patients With Crohn’s Disease. Front. Cell. Infect. Microbiol. 2022, 12, 864944. [Google Scholar] [CrossRef]
- Zheng, Y.-F.; Liang, S.-P.; Zhong, Z.-S.; Zhang, W.; Wu, Y.-Y.; Liu, J.-B.; Huang, S.-P. Duodenal microbiota makes an important impact in functional dyspepsia. Microb. Pathog. 2021, 162, 105297. [Google Scholar] [CrossRef] [PubMed]
- Zmora, N.; Zilberman-Schapira, G.; Suez, J.; Mor, U.; Dori-Bachash, M.; Bashiardes, S.; Kotler, E.; Zur, M.; Regev-Lehavi, D.; Brik, R.B.-Z.; et al. Personalized Gut Mucosal Colonization Resistance to Empiric Probiotics Is Associated with Unique Host and Microbiome Features. Cell 2018, 174, 1388–1405.e21. [Google Scholar] [CrossRef]
- Yang, M.; Zhang, L.; Hong, G.; Li, Y.; Li, G.; Qian, W.; Xiong, H.; Bai, T.; Song, J.; Hou, X. Duodenal and rectal mucosal microbiota related to small intestinal bacterial overgrowth in diarrhea-predominant irritable bowel syndrome. J. Gastroenterol. Hepatol. 2019, 35, 795–805. [Google Scholar] [CrossRef]
- Mei, Q.-X.; Huang, C.-L.; Luo, S.-Z.; Zhang, X.-M.; Zeng, Y.; Lu, Y.-Y. Characterization of the duodenal bacterial microbiota in patients with pancreatic head cancer vs. healthy controls. Pancreatology 2018, 18, 438–445. [Google Scholar] [CrossRef]
- Maeda, T.; Zai, H.; Fukui, Y.; Kato, Y.; Kumade, E.; Watanabe, T.; Furusyo, N.; Nakajima, H.; Arai, K.; Ishii, Y.; et al. Impact of Helicobacter pylori infection on fluid duodenal microbial community structure and microbial metabolic pathways. BMC Microbiol. 2022, 22, 27. [Google Scholar] [CrossRef]
- Schiepatti, A.; Bacchi, S.; Biagi, F.; Panelli, S.; Betti, E.; Corazza, G.R.; Capelli, E.; Ciccocioppo, R. Relationship between duodenal microbiota composition, clinical features at diagnosis, and persistent symptoms in adult Coeliac disease. Dig. Liver Dis. 2021, 53, 972–979. [Google Scholar] [CrossRef]
- Panelli, S.; Capelli, E.; Lupo, G.F.D.; Schiepatti, A.; Betti, E.; Sauta, E.; Marini, S.; Bellazzi, R.; Vanoli, A.; Pasi, A.; et al. Comparative Study of Salivary, Duodenal, and Fecal Microbiota Composition Across Adult Celiac Disease. J. Clin. Med. 2020, 9, 1109. [Google Scholar] [CrossRef]
- Yilmaz, B.; Fuhrer, T.; Morgenthaler, D.; Krupka, N.; Wang, D.; Spari, D.; Candinas, D.; Misselwitz, B.; Beldi, G.; Sauer, U.; et al. Plasticity of the adult human small intestinal stoma microbiota. Cell Host Microbe 2022, 30, 1773–1787.e6. [Google Scholar] [CrossRef]
- Zoetendal, E.G.; Raes, J.; van den Bogert, B.; Arumugam, M.; Booijink, C.C.G.M.; Troost, F.J.; Bork, P.; Wels, M.; De Vos, W.M.; Kleerebezem, M. The human small intestinal microbiota is driven by rapid uptake and conversion of simple carbohydrates. ISME J. 2012, 6, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Repiso, C.; Moreno-Indias, I.; Martín-Núñez, G.M.; Ho-Plágaro, A.; Rodríguez-Cañete, A.; Gonzalo, M.; García-Fuentes, E.; Tinahones, F.J. Mucosa-associated microbiota in the jejunum of patients with morbid obesity: alterations in states of insulin resistance and metformin treatment. Surg. Obes. Relat. Dis. 2020, 16, 1575–1585. [Google Scholar] [CrossRef]
- Vonaesch, P.; Araújo, J.R.; Gody, J.-C.; Mbecko, J.-R.; Sanke, H.; Andrianonimiadana, L.; Naharimanananirina, T.; Ningatoloum, S.N.; Vondo, S.S.; Gondje, P.B.; et al. Stunted children display ectopic small intestinal colonization by oral bacteria, which cause lipid malabsorption in experimental models. Proc. Natl. Acad. Sci. 2022, 119. [Google Scholar] [CrossRef] [PubMed]
- Leite, G.G.S.; Weitsman, S.; Parodi, G.; Celly, S.; Sedighi, R.; Sanchez, M.; Morales, W.; Villanueva-Millan, M.J.; Barlow, G.M.; Mathur, R.; et al. Mapping the Segmental Microbiomes in the Human Small Bowel in Comparison with Stool: A REIMAGINE Study. Dig. Dis. Sci. 2020, 65, 2595–2604. [Google Scholar] [CrossRef]
- Agamennone, V.; Abuja, P.M.; Basic, M.; De Angelis, M.; Gessner, A.; Keijser, B.; Larsen, M.; Pinart, M.; Nimptsch, K.; Pujos-Guillot, E.; et al. HDHL-INTIMIC: A European Knowledge Platform on Food, Diet, Intestinal Microbiomics, and Human Health. Nutrients 2022, 14, 1881. [Google Scholar] [CrossRef] [PubMed]
- Bushyhead, D.; Quigley, E.M. Small Intestinal Bacterial Overgrowth—Pathophysiology and Its Implications for Definition and Management. Gastroenterology 2022, 163, 593–607. [Google Scholar] [CrossRef]
- Sittipo, P.; Shim, J.-W.; Lee, Y.K. Microbial Metabolites Determine Host Health and the Status of Some Diseases. Int. J. Mol. Sci. 2019, 20, 5296. [Google Scholar] [CrossRef]
- Yersin, S.; Vonaesch, P. Small intestinal microbiota: from taxonomic composition to metabolism. Trends Microbiol. 2024, 32, 970–983. [Google Scholar] [CrossRef]
- Hooper, L.V.; Wong, M.H.; Thelin, A.; Hansson, L.; Falk, P.G.; Gordon, J.I. Molecular Analysis of Commensal Host-Microbial Relationships in the Intestine. Science 2001, 291, 881–884. [Google Scholar] [CrossRef] [PubMed]
- Folz, J.; Culver, R.N.; Morales, J.M.; Grembi, J.; Triadafilopoulos, G.; Relman, D.A.; Huang, K.C.; Shalon, D.; Fiehn, O. Human metabolome variation along the upper intestinal tract. Nat. Metab. 2023, 5, 777–788. [Google Scholar] [CrossRef]
- Martinez-Guryn, K.; Hubert, N.; Frazier, K.; Urlass, S.; Musch, M.W.; Ojeda, P.; Pierre, J.F.; Miyoshi, J.; Sontag, T.J.; Cham, C.M.; et al. Small Intestine Microbiota Regulate Host Digestive and Absorptive Adaptive Responses to Dietary Lipids. Cell Host Microbe 2018, 23, 458–469.e5. [Google Scholar] [CrossRef]
- Araújo, J.R.; Tazi, A.; Burlen-Defranoux, O.; Vichier-Guerre, S.; Nigro, G.; Licandro, H.; Demignot, S.; Sansonetti, P.J. Fermentation Products of Commensal Bacteria Alter Enterocyte Lipid Metabolism. Cell Host Microbe 2020, 27, 358–375.e7. [Google Scholar] [CrossRef]
- Pimentel, M.; Saad, R.J.; Long, M.D.; Rao, S.S.C. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am. J. Gastroenterol. 2020, 115, 165–178. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Lauritano, E.C.; Gabrielli, M.; Scarpellini, E.; Lupascu, A.; Ojetti, V.; Gasbarrini, G. Small Intestinal Bacterial Overgrowth: Diagnosis and Treatment. Dig. Dis. 2007, 25, 237–240. [Google Scholar] [CrossRef]
- Miller, L.S. Ileocecal valve dysfunction in small intestinal bacterial overgrowth: A pilot study. World J. Gastroenterol. 2012, 18, 6801–6808. [Google Scholar] [CrossRef] [PubMed]
- Vantrappen, G.; Janssens, J.; Hellemans, J.; Ghoos, Y. The Interdigestive Motor Complex of Normal Subjects and Patients with Bacterial Overgrowth of the Small Intestine. J. Clin. Investig. 1977, 59, 1158–1166. [Google Scholar] [CrossRef] [PubMed]
- Husebye, E.; Skar, V.; Høverstad, T.; Iversen, T.; Melby, K. Abnormal intestinal motor patterns explain enteric colonization with gram-negative bacilli in late radiation enteropathy. Gastroenterology 1995, 109, 1078–1089. [Google Scholar] [CrossRef]
- Roland, B.C.; Ciarleglio, M.M.; Clarke, J.O.; Semler, J.R.; Tomakin, E.; Mullin, G.E.; Pasricha, P.J. Small Intestinal Transit Time Is Delayed in Small Intestinal Bacterial Overgrowth. J. Clin. Gastroenterol. 2015, 49, 571–576. [Google Scholar] [CrossRef]
- Marie, I.; Ducrotté, P.; Denis, P.; Menard, J.-F.; Levesque, H. Small intestinal bacterial overgrowth in systemic sclerosis. Rheumatology 2009, 48, 1314–1319. [Google Scholar] [CrossRef]
- Ojetti, V.; Pitocco, D.; Scarpellini, E.; Zaccardi, F.; Scaldaferri, F.; Gigante, G.; Gasbarrini, G.; Ghirlanda, G.; Gasbarrini, A. Small bowel bacterial overgrowth and type 1 diabetes. . 2010, 13, 419–423. [Google Scholar]
- Singh, J.; Cohen, S.; Mehendiratta, V.; Mendoza, F.; Jimenez, S.A.; Dimarino, A.J.; Rattan, S. Effects of Scleroderma Antibodies and Pooled Human Immunoglobulin on Anal Sphincter and Colonic Smooth Muscle Function. Gastroenterology 2012, 143, 1308–1318. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Haberberger, R.V.; Gordon, T.P.; Jackson, M.W. Antibodies interfering with the type 3 muscarinic receptor pathway inhibit gastrointestinal motility and cholinergic neurotransmission in Sjögren's syndrome. Arthritis Rheum. 2011, 63, 1426–1434. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Nakamura, Y.; Matsumoto, I.; Nishimagi, E.; Satoh, T.; Kuwana, M.; Sumida, T.; Hara, M. Muscarinic-3 acetylcholine receptor autoantibody in patients with systemic sclerosis: contribution to severe gastrointestinal tract dysmotility. Ann. Rheum. Dis. 2009, 68, 710–714. [Google Scholar] [CrossRef]
- Lauritano, E.C.; Bilotta, A.L.; Gabrielli, M.; Scarpellini, E.; Lupascu, A.; Laginestra, A.; Novi, M.; Sottili, S.; Serricchio, M.; Cammarota, G.; et al. Association between Hypothyroidism and Small Intestinal Bacterial Overgrowth. J. Clin. Endocrinol. Metab. 2007, 92, 4180–4184. [Google Scholar] [CrossRef] [PubMed]
- Strid, H.; Simrén, M.; Stotzer, P.-O.; Ringström, G.; Abrahamsson, H.; Björnsson, E.S. Patients with Chronic Renal Failure Have Abnormal Small Intestinal Motility and a High Prevalence of Small Intestinal Bacterial Overgrowth. Digestion 2003, 67, 129–137. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; et al. Jejunal diverticulosis. A heterogenous disorder caused by a variety of abnormalities of smooth muscle or myenteric plexus. Gastroenterology 1983, 85, 538–547. [Google Scholar] [CrossRef]
- Pimentel, M.; Wallace, D.; Hallegua, D.; Chow, E.; Kong, Y.; Park, S.; Lin, H.C. A link between irritable bowel syndrome and fibromyalgia may be related to findings on lactulose breath testing. Ann. Rheum. Dis. 2004, 63, 450–452. [Google Scholar] [CrossRef]
- Tan, A.H.; Mahadeva, S.; Thalha, A.M.; Gibson, P.R.; Kiew, C.K.; Yeat, C.M.; Ng, S.W.; Ang, S.P.; Chow, S.K.; Tan, C.T.; et al. Small intestinal bacterial overgrowth in Parkinson's disease. Park. Relat. Disord. 2014, 20, 535–540. [Google Scholar] [CrossRef]
- Barboza, J.L.; Okun, M.S.; Moshiree, B. The treatment of gastroparesis, constipation and small intestinal bacterial overgrowth syndrome in patients with Parkinson's disease. Expert Opin Pharmacother, 2015, 16, 2449–2464. [Google Scholar] [CrossRef] [PubMed]
- Petrone, P.; Sarkisyan, G.; Coloma, E.; Akopian, G.; Ortega, A.; Kaufman, H.S. Small Intestinal Bacterial Overgrowth in Patients With Lower Gastrointestinal Symptoms and a History of Previous Abdominal Surgery. Arch. Surg. 2011, 146, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Klaus, J.; Spaniol, U.; Adler, G.; A Mason, R.; Reinshagen, M.; C, C.v.T. Small intestinal bacterial overgrowth mimicking acute flare as a pitfall in patients with Crohn's Disease. BMC Gastroenterol. 2009, 9, 61. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, S.V.; Shah, H.N.; Alexander, K.; Finelli, F.C.; Kirkpatrick, J.R.; Koch, T.R. Small intestinal bacterial overgrowth and thiamine deficiency after Roux-en-Y gastric bypass surgery in obese patients. Nutr. Res. 2008, 28, 293–298. [Google Scholar] [CrossRef]
- Salzman, N.H. Paneth cell defensins and the regulation of the microbiome: detente at mucosal surfaces. Gut Microbes 2010, 1, 401–406. [Google Scholar] [CrossRef]
- Mantis, N.J.; Forbes, S.J. Secretory IgA: Arresting Microbial Pathogens at Epithelial Borders. Immunol. Investig. 2010, 39, 383–406. [Google Scholar] [CrossRef]
- Mo, J.; Gao, L.; Zhang, N.; Xie, J.; Li, D.; Shan, T.; Fan, L. Structural and quantitative alterations of gut microbiota in experimental small bowel obstruction. PLOS ONE 2021, 16, e0255651. [Google Scholar] [CrossRef]
- Jones, R.M.; Neish, A.S. Recognition of bacterial pathogens and mucosal immunity. Cell. Microbiol. 2011, 13, 670–676. [Google Scholar] [CrossRef]
- Pignata, C.; Budillon, G.; Monaco, G.; Nani, E.; Cuomo, R.; Parrilli, G.; Ciccimarra, F. Jejunal bacterial overgrowth and intestinal permeability in children with immunodeficiency syndromes. . Gut 1990, 31, 879–882. [Google Scholar] [CrossRef]
- Lo, W.; Chan, W.W. Proton Pump Inhibitor Use and the Risk of Small Intestinal Bacterial Overgrowth: A Meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 11, 483–490. [Google Scholar] [CrossRef]
- Shah, A.; Morrison, M.; Burger, D.; Martin, N.; Rich, J.; Jones, M.; Koloski, N.; Walker, M.M.; Talley, N.J.; Holtmann, G.J. Systematic review with meta-analysis: the prevalence of small intestinal bacterial overgrowth in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2019, 49, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, L.; Foti, M.; Ruggia, O.; Chiecchio, A. Increased Incidence of Small Intestinal Bacterial Overgrowth During Proton Pump Inhibitor Therapy. Clin. Gastroenterol. Hepatol. 2010, 8, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.S.C.; Rehman, A.; Yu, S.; de Andino, N.M. Brain fogginess, gas and bloating: a link between SIBO, probiotics and metabolic acidosis. Clin. Transl. Gastroenterol. 2018, 9, e162. [Google Scholar] [CrossRef]
- Maslennikov, R.; Ivashkin, V.; Efremova, I.; Poluektova, E.; Kudryavtseva, A.; Krasnov, G. Gut dysbiosis and small intestinal bacterial overgrowth as independent forms of gut microbiota disorders in cirrhosis. World J. Gastroenterol. 2022, 28, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Capurso, G.; Signoretti, M.; Archibugi, L.; Stigliano, S.; Fave, G.D. Systematic review and meta-analysis: Small intestinal bacterial overgrowth in chronic pancreatitis. United Eur. Gastroenterol. J. 2016, 4, 697–705. [Google Scholar] [CrossRef]
- Kucheryavyy, Y.A.; Andreev, D.N.; Maev, I.V.; Александрoвич, К.Ю. Prevalence of small bowel bacterial overgrowth in patients with functional dyspepsia: a meta-analysis. Ter. arkhiv 2020, 92, 53–58. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Nehra, A.; Mathur, A.; Rai, S. A meta-analysis on small intestinal bacterial overgrowth in patients with different subtypes of irritable bowel syndrome. J. Gastroenterol. Hepatol. 2019, 35, 922–931. [Google Scholar] [CrossRef]
- Shah, A.; Thite, P.; Hansen, T.; Kendall, B.J.; Sanders, D.S.; Morrison, M.; Jones, M.P.; Holtmann, G. Links between celiac disease and small intestinal bacterial overgrowth: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2022, 37, 1844–1852. [Google Scholar] [CrossRef]
- Gandhi, A.; Shah, A.; Jones, M.P.; Koloski, N.; Talley, N.J.; Morrison, M.; Holtmann, G. Methane positive small intestinal bacterial overgrowth in inflammatory bowel disease and irritable bowel syndrome: A systematic review and meta-analysis. Gut Microbes 2021, 13, 1933313. [Google Scholar] [CrossRef]
- Gudan, A.; Jamioł-Milc, D.; Hawryłkowicz, V.; Skonieczna-Żydecka, K.; Stachowska, E. The Prevalence of Small Intestinal Bacterial Overgrowth in Patients with Non-Alcoholic Liver Diseases: NAFLD, NASH, Fibrosis, Cirrhosis—A Systematic Review, Meta-Analysis and Meta-Regression. Nutrients 2022, 14, 5261. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Ghoshal, U. Small Intestinal Bacterial Overgrowth and Other Intestinal Disorders. Gastroenterol Clin North Am 2017, 46, 103–120. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, A.H.; Pimentel, M. Gastrointestinal bacterial overgrowth: pathogenesis and clinical significance. Ther. Adv. Chronic Dis. 2013, 4, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Zaidel, O.; Hum, S. Intestinal transit of fat depends on accelerating effect of cholecystokinin and slowing effect of an opioid pathway. Dig. Dis. Sci. 2002, 47, 2217–2221. [Google Scholar] [CrossRef]
- Giannella, R.A.; Broitman, S.A.; Zamcheck, N. Influence of Gastric Acidity on Bacterial and Parasitic Enteric Infections. Ann. Intern. Med. 1973, 78, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Roland, B.C.; Mullin, G.E.; Passi, M.; Zheng, X.; Salem, A.; Yolken, R.; Pasricha, P.J. A Prospective Evaluation of Ileocecal Valve Dysfunction and Intestinal Motility Derangements in Small Intestinal Bacterial Overgrowth. Dig. Dis. Sci. 2017, 62, 3525–3535. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Shukla, R.; Ghoshal, U. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome: A Bridge between Functional Organic Dichotomy. Gut Liver 2017, 11, 196–208. [Google Scholar] [CrossRef]
- Rana, S.V.; Sharma, S.; Malik, A.; Kaur, J.; Prasad, K.K.; Sinha, S.K.; Singh, K. Small Intestinal Bacterial Overgrowth and Orocecal Transit Time in Patients of Inflammatory Bowel Disease. Dig. Dis. Sci. 2013, 58, 2594–2598. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Giorgetti, G. High prevalence of small intestinal bacterial overgrowth in celiac patients with persistence of gastrointestinal symptoms after gluten withdrawal. Am J Gastroenterol 2003, 98, 839–843. [Google Scholar] [CrossRef]
- Kapil, S.; Duseja, A.; Sharma, B.K.; Singla, B.; Chakraborti, A.; Das, A.; Ray, P.; Dhiman, R.K.; Chawla, Y. Small intestinal bacterial overgrowth and toll-like receptor signaling in patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2015, 31, 213–221. [Google Scholar] [CrossRef]
- Gyger, G.; Baron, M. Gastrointestinal Manifestations of Scleroderma: Recent Progress in Evaluation, Pathogenesis, and Management. Curr. Rheumatol. Rep. 2011, 14, 22–29. [Google Scholar] [CrossRef]
- Sjogren, R.W. Gastrointestinal motility disorders in scleroderma. Arthritis Rheum. 1994, 37, 1265–1282. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, S.; Tandon, P.; Gohel, T.; Corrigan, M.L.; Coughlin, K.L.; Shatnawei, A.; Chatterjee, S.; Kirby, D.F. Gastrointestinal Manifestations, Malnutrition, and Role of Enteral and Parenteral Nutrition in Patients With Scleroderma. J. Clin. Gastroenterol. 2015, 49, 559–564. [Google Scholar] [CrossRef]
- Sawadpanich, K.; Soison, P.; Chunlertrith, K.; Mairiang, P.; Sukeepaisarnjaroen, W.; Sangchan, A.; Suttichaimongkol, T.; Foocharoen, C. Prevalence and associated factors of small intestinal bacterial overgrowth among systemic sclerosis patients. Int. J. Rheum. Dis. 2019, 22, 695–699. [Google Scholar] [CrossRef]
- Levin, D.; De Palma, G.; Zou, H.; Bazzaz, A.H.Z.; Verdu, E.; Baker, B.; Pinto-Sanchez, M.I.; Khalidi, N.; Larché, M.J.; Beattie, K.A.; et al. Fecal microbiome differs between patients with systemic sclerosis with and without small intestinal bacterial overgrowth. J. Scleroderma Relat. Disord. 2021, 6, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chu, M.; Wang, D.; Luo, Y.; Liu, Z.; Zhao, J. Risk factors for small intestinal bacterial overgrowth in patients with acute ischaemic stroke. J. Med Microbiol. 2023, 72, 001666. [Google Scholar] [CrossRef] [PubMed]
- Kvit, K.B.; Kharchenko, N.V.; Kharchenko, V.V.; Chornenka, O.I.; Chornovus, R.I.; Dorofeeva, U.S.; Draganchuk, O.B.; Slaba, O.M. THE ROLE OF SMALL INTESTINAL BACTERIAL OVERGROWTH IN THE PATHOGENESIS OF HYPERLIPIDEMIA. Wiadomosci Lek. (Warsaw, Pol. : 1960) 2019, 72, 645–649. [Google Scholar] [CrossRef]
- Ciobanu, L.; Dumitrascu, D.L. Gastrointestinal motility disorders in endocrine diseases. Pol. Arch. Intern. Med. 2011, 121, 129–136. [Google Scholar] [CrossRef]
- Yang, J.; Kim, C.J.; Go, Y.S.; Lee, H.Y.; Kim, M.-G.; Oh, S.W.; Cho, W.Y.; Im, S.-H.; Jo, S.K. Intestinal microbiota control acute kidney injury severity by immune modulation. Kidney Int. 2020, 98, 932–946. [Google Scholar] [CrossRef]
- Mahmoodpoor, F.; Rahbar Saadat, Y.; Barzegari, A.; Ardalan, M.; Zununi Vahed, S. The impact of gut microbiota on kidney function and pathogenesis. Biomed. Pharmacother. 2017, 93, 412–419. [Google Scholar] [CrossRef]
- Drago, F.; et al. Oral psoriasis and SIBO: is there a link? J Eur Acad Dermatol Venereol 2018, 32, e368–e369. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Indemini, E.; Savarino, V.; Parodi, A. Psoriasis and small intestine bacterial overgrowth. Int. J. Dermatol. 2018, 57, 112–113. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Feng, X.; Jiang, Z.; Jiang, Z. Association of small intestinal bacterial overgrowth with Parkinson’s disease: a systematic review and meta-analysis. Gut Pathog. 2021, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Zhou, L.; Wang, Q.; Zheng, G.; Su, S. Effect of Compound Lactic Acid Bacteria Capsules on the Small Intestinal Bacterial Overgrowth in Patients with Depression and Diabetes: A Blinded Randomized Controlled Clinical Trial. Dis. Markers 2022, 2022, 6721695. [Google Scholar] [CrossRef] [PubMed]
- Kossewska, J.; Bierlit, K.; Trajkovski, V. Personality, Anxiety, and Stress in Patients with Small Intestine Bacterial Overgrowth Syndrome. The Polish Preliminary Study. Int. J. Environ. Res. Public Heal. 2022, 20, 93. [Google Scholar] [CrossRef]
- Chojnacki, C.; Konrad, P.; Błońska, A.; Medrek-Socha, M.; Przybylowska-Sygut, K.; Chojnacki, J.; Poplawski, T. Altered Tryptophan Metabolism on the Kynurenine Pathway in Depressive Patients with Small Intestinal Bacterial Overgrowth. Nutrients 2022, 14, 3217. [Google Scholar] [CrossRef]
- Chojnacki, C.; Popławski, T.; Konrad, P.; Fila, M.; Błasiak, J.; Chojnacki, J. Antimicrobial treatment improves tryptophan metabolism and mood of patients with small intestinal bacterial overgrowth. Nutr. Metab. 2022, 19, 66. [Google Scholar] [CrossRef]
- Liang, S.; Xu, L.; Zhang, D.; Wu, Z. Effect of probiotics on small intestinal bacterial overgrowth in patients with gastric and colorectal cancer. Turk. J. Gastroenterol. 2016, 27, 227–232. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; et al. Asian-Pacific consensus on small intestinal bacterial overgrowth in gastrointestinal disorders: An initiative of the Indian Neurogastroenterology and Motility Association. Indian J Gastroenterol 2022, 41, 483–507. [Google Scholar] [CrossRef]
- Khoshini, R.; Dai, S.-C.; Lezcano, S.; Pimentel, M. A Systematic Review of Diagnostic Tests for Small Intestinal Bacterial Overgrowth. Dig. Dis. Sci. 2007, 53, 1443–1454. [Google Scholar] [CrossRef]
- Vanner, S. The small intestinal bacterial overgrowth. Irritable bowel syndrome hypothesis: implications for treatment. Gut 2008, 57, 1315–1321. [Google Scholar] [CrossRef]
- Siniewicz-Luzenczyk, K.; et al. Small intestinal bacterial overgrowth syndrome in children. Prz Gastroenterol 2015, 10, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Cangemi, D.J.; Lacy, B.E.; Wise, J. Diagnosing Small Intestinal Bacterial Overgrowth: A Comparison of Lactulose Breath Tests to Small Bowel Aspirates. Dig. Dis. Sci. 2020, 66, 2042–2050. [Google Scholar] [CrossRef] [PubMed]
- Leite, G.; Morales, W.; Weitsman, S.; Celly, S.; Parodi, G.; Mathur, R.; Barlow, G.M.; Sedighi, R.; Millan, M.J.V.; Rezaie, A.; et al. The duodenal microbiome is altered in small intestinal bacterial overgrowth. PLOS ONE 2020, 15, e0234906. [Google Scholar] [CrossRef]
- Bamba, S.; Imai, T.; Sasaki, M.; Ohno, M.; Yoshida, S.; Nishida, A.; Takahashi, K.; Inatomi, O.; Andoh, A. Altered gut microbiota in patients with small intestinal bacterial overgrowth. J. Gastroenterol. Hepatol. 2022, 38, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Achufusi, T.G.; Sharma, A.; A Zamora, E.; Manocha, D. Small Intestinal Bacterial Overgrowth: Comprehensive Review of Diagnosis, Prevention, and Treatment Methods. Cureus 2020, 12, e8860. [Google Scholar] [CrossRef]
- Feng, X.; Li, X.-Q. The prevalence of small intestinal bacterial overgrowth in diabetes mellitus: a systematic review and meta-analysis. Aging 2022, 14, 975–988. [Google Scholar] [CrossRef]
- Franco, D.L.; Disbrow, M.B.; Kahn, A.; Koepke, L.M.; Harris, L.A.; Harrison, M.E.; Crowell, M.D.; Ramirez, F.C. Duodenal Aspirates for Small Intestine Bacterial Overgrowth: Yield, PPIs, and Outcomes after Treatment at a Tertiary Academic Medical Center. Gastroenterol. Res. Pr. 2015, 2015, 971582. [Google Scholar] [CrossRef]
- Gabrielli, M.; D'Angelo, G.; Di Rienzo, T.; Scarpellini, E.; Ojetti, V. Diagnosis of small intestinal bacterial overgrowth in the clinical practice. Eur Rev Med Pharmacol Sci. 2013, 30–35. [Google Scholar]
- Sundin, O.H.; Mendoza-Ladd, A.; Zeng, M.; Diaz-Arévalo, D.; Morales, E.; Fagan, B.M.; Ordoñez, J.; Velez, P.; Antony, N.; McCallum, R.W. The human jejunum has an endogenous microbiota that differs from those in the oral cavity and colon. BMC Microbiol. 2017, 17, 160. [Google Scholar] [CrossRef]
- Rao, S.S.C.; Bhagatwala, J. Small Intestinal Bacterial Overgrowth: Clinical Features and Therapeutic Management. Clin. Transl. Gastroenterol. 2019, 10, e00078. [Google Scholar] [CrossRef]
- Ginnebaugh, B.; Chey, W.D.; Saad, R. Small Intestinal Bacterial Overgrowth How to Diagnose and Treat (and Then Treat Again). Gastroenterol. Clin. North Am. 2020, 49, 571. [Google Scholar] [CrossRef]
- Sroka, N.; Rydzewska-Rosołowska, A.; Kakareko, K.; Rosołowski, M.; Głowińska, I.; Hryszko, T. Show Me What You Have Inside—The Complex Interplay between SIBO and Multiple Medical Conditions—A Systematic Review. Nutrients 2022, 15, 90. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef]
- Shah, A.; Talley, N.J.; Jones, M.; Kendall, B.J.; Koloski, N.; Walker, M.M.; Morrison, M.; Holtmann, G.J. Small Intestinal Bacterial Overgrowth in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. Am. J. Gastroenterol. 2020, 115, 190–201. [Google Scholar] [CrossRef]
- Suarez Teran, J. and F. Guarner Aguilar, Small Intestinal Bacterial Overgrowth (SIBO), a clinically overdiagnosed entity? Gastroenterol Hepatol 2024, 47, 502190. [Google Scholar] [PubMed]
- Maeda, Y.; Murakami, T. Diagnosis by Microbial Culture, Breath Tests and Urinary Excretion Tests, and Treatments of Small Intestinal Bacterial Overgrowth. Antibiotics 2023, 12, 263. [Google Scholar] [CrossRef] [PubMed]
- Gasbarrini, A.; Corazza, G.R.; Gasbarrini, G.B.; Montalto, M.; di Stefano, M.; Basilisco, G.; Parodi, A.; Usai-Satta, P.; Satta, P.U.; Vernia, P.; et al. Methodology and Indications of H2-Breath Testing in Gastrointestinal Diseases: The Rome Consensus Conference. Aliment. Pharmacol. Ther. 2009, 29 (Suppl. 1), 1–49. [Google Scholar] [CrossRef]
- Lin, E.C.; Massey, B.T. Scintigraphy Demonstrates High Rate of False-positive Results From Glucose Breath Tests for Small Bowel Bacterial Overgrowth. Clin. Gastroenterol. Hepatol. 2016, 14, 203–208. [Google Scholar] [CrossRef]
- Saad, R.J.; Chey, W.D. Breath Testing for Small Intestinal Bacterial Overgrowth: Maximizing Test Accuracy. Clin. Gastroenterol. Hepatol. 2014, 12, 1964–1972. [Google Scholar] [CrossRef]
- Tang, S.; Li, J.; Ma, J.; Li, Y.; Li, Y.; Wan, J.; Zhang, R. Comparison of jejunal aspirate culture and methane and hydrogen breath test in the diagnosis of small intestinal bacterial overgrowth. Ir. J. Med Sci. (1971 -) 2023, 193, 699–703. [Google Scholar] [CrossRef]
- Romagnuolo, J.; Schiller, D.; Bailey, R.J. Using breath tests wisely in a gastroenterology practice: an evidence-based review of indications and pitfalls in interpretation. Am J Gastroenterol 2002, 97, 1113–1126. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, A.; Pimentel, M.; Rao, S.S. How to Test and Treat Small Intestinal Bacterial Overgrowth: an Evidence-Based Approach. Curr. Gastroenterol. Rep. 2016, 18, 8. [Google Scholar] [CrossRef]
- Costello, B.P.J.d.L.; Ledochowski, M.; Ratcliffe, N.M. The importance of methane breath testing: a review. J. Breath Res. 2013, 7, 024001. [Google Scholar] [CrossRef]
- Tuteja, A.K.; Talley, N.J.; Stoddard, G.J.; Samore, M.H.; Verne, G.N. Risk factors for upper and lower functional gastrointestinal disorders in Persian Gulf War Veterans during and post-deployment. Neurogastroenterol. Motil. 2019, 31, e13533. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.Z.; Lyu, R.; McMichael, J.; Gabbard, S. Chronic Intestinal Pseudo-Obstruction Is Associated with Intestinal Methanogen Overgrowth. Dig. Dis. Sci. 2022, 67, 4834–4840. [Google Scholar] [CrossRef]
- Pyleris, E.; Giamarellos-Bourboulis, E.J.; Tzivras, D.; Koussoulas, V.; Barbatzas, C.; Pimentel, M. The Prevalence of Overgrowth by Aerobic Bacteria in the Small Intestine by Small Bowel Culture: Relationship with Irritable Bowel Syndrome. Dig. Dis. Sci. 2012, 57, 1321–1329. [Google Scholar] [CrossRef]
- Wielgosz-Grochowska, J.P.; Domanski, N.; Drywień, M.E. Efficacy of an Irritable Bowel Syndrome Diet in the Treatment of Small Intestinal Bacterial Overgrowth: A Narrative Review. Nutrients 2022, 14, 3382. [Google Scholar] [CrossRef] [PubMed]
- Takakura, W.; Pimentel, M. Small Intestinal Bacterial Overgrowth and Irritable Bowel Syndrome – An Update. Front. Psychiatry 2020, 11, 664. [Google Scholar] [CrossRef]
- Kashyap, P.; Moayyedi, P.; Quigley, E.M.M.; Simren, M.; Vanner, S. Critical appraisal of the SIBO hypothesis and breath testing: A clinical practice update endorsed by the European society of neurogastroenterology and motility (ESNM) and the American neurogastroenterology and motility society (ANMS). Neurogastroenterol. Motil. 2024, 36, e14817. [Google Scholar] [CrossRef]
- Madigan, K.E.; Bundy, R.; Weinberg, R.B. Distinctive Clinical Correlates of Small Intestinal Bacterial Overgrowth with Methanogens. Clin. Gastroenterol. Hepatol. 2022, 20, 1598–1605.e2. [Google Scholar] [CrossRef]
- Hoegenauer, C.; Hammer, H.F.; Mahnert, A.; Moissl-Eichinger, C. Methanogenic archaea in the human gastrointestinal tract. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Takakura, W.; Pimentel, M.; Rao, S.; Villanueva-Millan, M.J.; Chang, C.; Morales, W.; Sanchez, M.; Torosyan, J.; Rashid, M.; Hosseini, A.; et al. A Single Fasting Exhaled Methane Level Correlates With Fecal Methanogen Load, Clinical Symptoms and Accurately Detects Intestinal Methanogen Overgrowth. Am. J. Gastroenterol. 2022, 117, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Efremova, I.; Maslennikov, R.; Poluektova, E.; Vasilieva, E.; Zharikov, Y.; Suslov, A.; Letyagina, Y.; Kozlov, E.; Levshina, A.; Ivashkin, V. Epidemiology of small intestinal bacterial overgrowth. World J. Gastroenterol. 2023, 29, 3400–3421. [Google Scholar] [CrossRef]
- Khoshini, R.; Dai, S.-C.; Lezcano, S.; Pimentel, M. A Systematic Review of Diagnostic Tests for Small Intestinal Bacterial Overgrowth. Dig. Dis. Sci. 2007, 53, 1443–1454. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; et al. Evaluation of small intestinal bacterial overgrowth. Expert Rev Gastroenterol Hepatol 2023, 17, 461–467. [Google Scholar] [CrossRef]
- Chuah, K.H.; Wong, M.S.; Tan, P.O.; Lim, S.Z.; Beh, K.H.; Chong, S.C.S.; Zulkifli, K.K.; Thalha, A.M.; Mahadeva, S.; Lee, Y.Y. Small Intestinal Bacterial Overgrowth In Various Functional Gastrointestinal Disorders: A Case–Control Study. Dig. Dis. Sci. 2021, 67, 3881–3889. [Google Scholar] [CrossRef]
- Gurusamy, S.R.; Shah, A.; Talley, N.J.; Koloski, N.; Jones, M.P.; Walker, M.M.; Morrison, M.; Holtmann, G. Small Intestinal Bacterial Overgrowth in Functional Dyspepsia: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2021, 116, 935–942. [Google Scholar] [CrossRef]
- Pitcher, C.K.; Farmer, A.D.; Haworth, J.J.; Treadway, S.; Hobson, A.R. Performance and Interpretation of Hydrogen and Methane Breath Testing Impact of North American Consensus Guidelines. Dig. Dis. Sci. 2022, 67, 5571–5579. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, M.; Mayer, A.G.; Park, S.; Chow, E.J.; Hasan, A.; Kong, Y. Methane Production During Lactulose Breath Test Is Associated with Gastrointestinal Disease Presentation. Dig. Dis. Sci. 2003, 48, 86–92. [Google Scholar] [CrossRef]
- Mihajlovski, A.; Doré, J.; Levenez, F.; Alric, M.; Brugère, J. Molecular evaluation of the human gut methanogenic archaeal microbiota reveals an age-associated increase of the diversity. Environ. Microbiol. Rep. 2010, 2, 272–280. [Google Scholar] [CrossRef]
- Houben, E.; et al. Additional Value of CH(4) Measurement in a Combined (13)C/H(2) Lactose Malabsorption Breath Test: A Retrospective Analysis. Nutrients 2015, 7, 7469–85. [Google Scholar] [CrossRef] [PubMed]
- Hammer, H.F.; Fox, M.R.; Keller, J.; Salvatore, S.; Basilisco, G.; Hammer, J.; Lopetuso, L.; Benninga, M.; Borrelli, O.; Dumitrascu, D.; et al. European guideline on indications, performance, and clinical impact of hydrogen and methane breath tests in adult and pediatric patients: European Association for Gastroenterology, Endoscopy and Nutrition, European Society of Neurogastroenterology and Motility, and European Society for Paediatric Gastroenterology Hepatology and Nutrition consensus. United Eur. Gastroenterol. J. 2021, 10, 15–40. [Google Scholar] [CrossRef]
- Mion, F.; et al. Does Single Fasting Methane Levels Really Detect Intestinal Methanogen Overgrowth? Am J Gastroenterol 2023, 118, 1299–1300. [Google Scholar] [CrossRef]
- Lee, S.N.; Rahimian, P.; Stork, C.; Moshiree, B.; Jones, M.; Chuang, E.; Wahl, C.; Singh, S.; Rao, S.S.C. Evaluation of a Novel Smart Capsule Bacterial Detection System Device for Diagnosis of Small Intestinal Bacterial Overgrowth. Neurogastroenterol. Motil. 2024, 37, e14965. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.Z.; Yao, C.; Rotbart, A.; Muir, J.G.; Gibson, P.R.; Kalantar-Zadeh, K. Human intestinal gas measurement systems: in vitro fermentation and gas capsules. Trends Biotechnol. 2015, 33, 208–213. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Yao, C.K.; Berean, K.J.; Ha, N.; Ou, J.Z.; Ward, S.A.; Pillai, N.; Hill, J.; Cottrell, J.J.; Dunshea, F.R.; et al. Intestinal Gas Capsules: A Proof-of-Concept Demonstration. Gastroenterology 2016, 150, 37–39. [Google Scholar] [CrossRef]
- Rehan, M.; Al-Bahadly, I.; Thomas, D.G.; Young, W.; Cheng, L.K.; Avci, E. Smart capsules for sensing and sampling the gut: status, challenges and prospects. Gut 2023, 73, 186–202. [Google Scholar] [CrossRef]
- Thwaites, P.A.; Yao, C.K.; Maggo, J.; John, J.; Chrimes, A.F.; Burgell, R.E.; Muir, J.G.; Parker, F.C.; So, D.; Kalantar-Zadeh, K.; et al. Comparison of gastrointestinal landmarks using the gas-sensing capsule and wireless motility capsule. Aliment. Pharmacol. Ther. 2022, 56, 1337–1348. [Google Scholar] [CrossRef]
- Spiller, R. Editorial: Interaction between fibre and colonic fermentation assessed with a novel gas-sensing capsule. Aliment. Pharmacol. Ther. 2023, 58, 828–829. [Google Scholar] [CrossRef]
- Zhou, J.; A Thwaites, P.; Gibson, P.R.; Burgell, R.; Ho, V. Comparison of Gas-sensing Capsule With Wireless Motility Capsule in Motility Disorder Patients. J. Neurogastroenterol. Motil. 2024, 30, 303–312. [Google Scholar] [CrossRef]
- A Thwaites, P.; Slater, R.; Probert, C.; Gibson, P.R. Recent advances in measuring the effects of diet on gastrointestinal physiology: Sniffing luminal gases and fecal volatile organic compounds. JGH Open 2024, 8, e70006. [Google Scholar] [CrossRef] [PubMed]
- So, D.; Yao, C.K.; Gill, P.A.; Thwaites, P.A.; Ardalan, Z.S.; McSweeney, C.S.; Denman, S.E.; Chrimes, A.F.; Muir, J.G.; Berean, K.J.; et al. Detection of changes in regional colonic fermentation in response to supplementing a low FODMAP diet with dietary fibres by hydrogen concentrations, but not by luminal pH. Aliment. Pharmacol. Ther. 2023, 58, 417–428. [Google Scholar] [CrossRef]
- Sonu, I.; Oh, S.J.; Rao, S.S.C. Capsules for the Diagnosis and Treatment of Gastrointestinal Motility Disorders- A Game Changer. Curr. Gastroenterol. Rep. 2024, 26, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Yao, C.K.; Berean, K.J.; Ha, N.; Ou, J.Z.; Ward, S.A.; Pillai, N.; Hill, J.; Cottrell, J.J.; Dunshea, F.R.; et al. Intestinal Gas Capsules: A Proof-of-Concept Demonstration. Gastroenterology 2016, 150, 37–39. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of General 16S Ribosomal RNA Gene PCR Primers for Classical and Next-Generation Sequencing-Based Diversity Studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Fan, X.; Shi, H.; Li, J.; Zhang, M.; Zhao, J.; Su, X. Comprehensive Assessment of 16S rRNA Gene Amplicon Sequencing for Microbiome Profiling across Multiple Habitats. Microbiol. Spectr. 2023, 11, e0056323. [Google Scholar] [CrossRef]
- Matsuo, Y. Full-Length 16S rRNA Gene Analysis Using Long-Read Nanopore Sequencing for Rapid Identification of Bacteria from Clinical Specimens. Methods Mol Biol 2023, 2632, 193–213. [Google Scholar]
- Moorlag, S.J.C.F.M.; Coolen, J.P.M.; Bosch, B.v.D.; Jin, E.H.-M.; Buil, J.B.; Wertheim, H.F.L.; Melchers, W.J.G. Targeting the 16S rRNA Gene by Reverse Complement PCR Next-Generation Sequencing: Specific and Sensitive Detection and Identification of Microbes Directly in Clinical Samples. Microbiol. Spectr. 2023, 11, e0448322. [Google Scholar] [CrossRef]
- Johnson, J.S.; Spakowicz, D.J.; Hong, B.-Y.; Petersen, L.M.; Demkowicz, P.; Chen, L.; Leopold, S.R.; Hanson, B.M.; Agresta, H.O.; Gerstein, M.; et al. Evaluation of 16S rRNA gene sequencing for species and strain-level microbiome analysis. Nat. Commun. 2019, 10, 5029. [Google Scholar] [CrossRef]
- Quigley, E.M. Exploring the Small Intestinal Microbiome: Relationships to Symptoms and Small Intestinal Bacterial Overgrowth. Clin. Gastroenterol. Hepatol. 2023, 22, 241–242. [Google Scholar] [CrossRef]
- Leite, G.; Rezaie, A.; Mathur, R.; Barlow, G.M.; Rashid, M.; Hosseini, A.; Wang, J.; Parodi, G.; Villanueva-Millan, M.J.; Sanchez, M.; et al. Defining Small Intestinal Bacterial Overgrowth by Culture and High Throughput Sequencing. Clin. Gastroenterol. Hepatol. 2023, 22, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Maslennikov, R.; Ivashkin, V.; Efremova, I.; Poluektova, E.; Kudryavtseva, A.; Krasnov, G. Gut dysbiosis and small intestinal bacterial overgrowth as independent forms of gut microbiota disorders in cirrhosis. World J. Gastroenterol. 2022, 28, 1067–1077. [Google Scholar] [CrossRef]
- Yang, M.; Zhang, L.; Hong, G.; Li, Y.; Li, G.; Qian, W.; Xiong, H.; Bai, T.; Song, J.; Hou, X. Duodenal and rectal mucosal microbiota related to small intestinal bacterial overgrowth in diarrhea-predominant irritable bowel syndrome. J. Gastroenterol. Hepatol. 2019, 35, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Sundin, J.; Aziz, I.; Nordlander, S.; Polster, A.; Hu, Y.O.O.; Hugerth, L.W.; Pennhag, A.A.L.; Engstrand, L.; Törnblom, H.; Simrén, M.; et al. Evidence of altered mucosa-associated and fecal microbiota composition in patients with Irritable Bowel Syndrome. Sci. Rep. 2020, 10, 593. [Google Scholar] [CrossRef]
- Shin, A.S.; Gao, X.; Bohm, M.; Lin, H.; Gupta, A.; Nelson, D.E.; Toh, E.; Teagarden, S.; Siwiec, R.; Dong, Q.; et al. Characterization of Proximal Small Intestinal Microbiota in Patients With Suspected Small Intestinal Bacterial Overgrowth: A Cross-Sectional Study. Clin. Transl. Gastroenterol. 2019, 10, e00073. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, R.; Ma, J.; Tang, S.; Li, Y.; Li, Y.; Wan, J. Mucosa-Associated Microbial Profile Is Altered in Small Intestinal Bacterial Overgrowth. Front. Microbiol. 2021, 12. [Google Scholar] [CrossRef]
- Guo, H.; Chen, Y.; Dong, W.; Lu, S.; Du, Y.; Duan, L. Fecal Coprococcus, hidden behind abdominal symptoms in patients with small intestinal bacterial overgrowth. J. Transl. Med. 2024, 22, 496. [Google Scholar] [CrossRef]
- Schindler, V.; Huellner, M.; Murray, F.; Schnurre, L.; Becker, A.S.; Bordier, V.; Pohl, D. Nutrient Challenge Testing Is Not Equivalent to Scintigraphy−Lactulose Hydrogen Breath Testing in Diagnosing Small Intestinal Bacterial Overgrowth. J. Neurogastroenterol. Motil. 2020, 26, 514–520. [Google Scholar] [CrossRef]
- Zhao, J.; Zheng, X.; Chu, H.; Cong, Y.; Fried, M.; Fox, M.; Dai, N. A study of the methodological and clinical validity of the combined lactulose hydrogen breath test with scintigraphic oro-cecal transit test for diagnosing small intestinal bacterial overgrowth in IBS patients. Neurogastroenterol. Motil. 2014, 26, 794–802. [Google Scholar] [CrossRef]
- Miller, M.A.; Parkman, H.P.; Urbain, J.-L.C.; Brown, K.L.; Donahue, D.J.; Knight, L.C.; Maurer, A.H.; Fisher, R.S. Comparison of Scintigraphy and Lactulose Breath Hydrogen Test for Assessment of Orocecal Transit (Lactulose Accelerates Small Bowel Transit). Dig. Dis. Sci. 1997, 42, 10–18. [Google Scholar] [CrossRef]
- Esposito, I. Breath test for differential diagnosis between small intestinal bacterial overgrowth and irritable bowel disease: An observation on non-absorbable antibiotics. World J. Gastroenterol. 2007, 13. [Google Scholar] [CrossRef]
- Yu, D.; Cheeseman, F.; Vanner, S. Combined oro-caecal scintigraphy and lactulose hydrogen breath testing demonstrate that breath testing detects oro-caecal transit, not small intestinal bacterial overgrowth in patients with IBS. Gut 2010, 60, 334–340. [Google Scholar] [CrossRef]
- Rosenthal, A.; Solomons, N.W. Time-course of cigarette smoke contamination of clinical hydrogen breath-analysis tests. Clin. Chem. 1983, 29, 1980–1981. [Google Scholar] [CrossRef]
- Mattio, N.; Pradat, P.; Machon, C.; Mialon, A.; Roman, S.; Cuerq, C.; Mion, F. Glucose breath test for the detection of small intestine bacterial overgrowth: Impact of diet prior to the test. Neurogastroenterol. Motil. 2024, 36, e14801. [Google Scholar] [CrossRef] [PubMed]
- Tadesse, K.; Eastwood, M. BREATH-HYDROGEN TEST AND SMOKING. Lancet 1977, 310, 91. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, A.; Solomons, N.W. Time-course of cigarette smoke contamination of clinical hydrogen breath-analysis tests. Clin. Chem. 1983, 29, 1980–1981. [Google Scholar] [CrossRef]
- Perman, J.; Modler, S.; Engel, R.; Heldt, G. Effect of ventilation on breath hydrogen measurements. J Lab Clin Med 1985, 105, 436–439. [Google Scholar]
- Le Nevé, B.; Derrien, M.; Tap, J.; Brazeilles, R.; Portier, S.C.; Guyonnet, D.; Ohman, L.; Störsrud, S.; Törnblom, H.; Simrén, M. Fasting breath H2 and gut microbiota metabolic potential are associated with the response to a fermented milk product in irritable bowel syndrome. PLOS ONE 2019, 14, e0214273. [Google Scholar] [CrossRef]
- Korterink, J.J.; Benninga, M.A.; van Wering, H.M.; Deckers-Kocken, J.M. Glucose Hydrogen Breath Test for Small Intestinal Bacterial Overgrowth in Children With Abdominal Pain–Related Functional Gastrointestinal Disorders. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 498–502. [Google Scholar] [CrossRef]
- Kumar, S.; Misra, A.; Ghoshal, U.C. Patients With Irritable Bowel Syndrome Exhale More Hydrogen Than Healthy Subjects in Fasting State. J. Neurogastroenterol. Motil. 2010, 16, 299–305. [Google Scholar] [CrossRef]
- Lombardo, L.; Foti, M.; Ruggia, O.; Chiecchio, A. Increased Incidence of Small Intestinal Bacterial Overgrowth During Proton Pump Inhibitor Therapy. Clin. Gastroenterol. Hepatol. 2010, 8, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Su, T.; Lai, S.; Lee, A.; He, X.; Chen, S. Meta-analysis: proton pump inhibitors moderately increase the risk of small intestinal bacterial overgrowth. J. Gastroenterol. 2017, 53, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Revaiah, P.C.; Kochhar, R.; Rana, S.V.; Berry, N.; Ashat, M.; Dhaka, N.; Reddy, Y.R.; Sinha, S.K. Risk of small intestinal bacterial overgrowth in patients receiving proton pump inhibitors versus proton pump inhibitors plus prokinetics. JGH Open 2018, 2, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Li, Y.; Ma, J.X.; Tang, S.; Li, C.M.; Wan, J. [The effects of continuous proton pump inhibitor therapy on small intestinal bacterial overgrowth in elderly]. . 2020, 59, 706–710. [Google Scholar]
- Muraki, M.; Fujiwara, Y.; Machida, H.; Okazaki, H.; Sogawa, M.; Yamagami, H.; Tanigawa, T.; Shiba, M.; Watanabe, K.; Tominaga, K.; et al. Role of small intestinal bacterial overgrowth in severe small intestinal damage in chronic non-steroidal anti-inflammatory drug users. Scand. J. Gastroenterol. 2013, 49, 267–273. [Google Scholar] [CrossRef]
- Kumar, S.; Misra, A.; Ghoshal, U.C. Patients With Irritable Bowel Syndrome Exhale More Hydrogen Than Healthy Subjects in Fasting State. J. Neurogastroenterol. Motil. 2010, 16, 299–305. [Google Scholar] [CrossRef]
- Mac Mahon, M.; et al. Are hydrogen breath tests valid in the elderly? Gerontology 1996, 42, 40–45. [Google Scholar] [CrossRef]
- Flourie, B.; Turk, J.; Lemann, M.; Florent, C.; Colimon, R.; Rambaud, J. Breath hydrogen in bacterial overgrowth. Gastroenterology 1989, 96, 1225–1226. [Google Scholar] [CrossRef]
- Sendino, T.; Sandúa, A.; Calleja, S.; González, Á.; Alegre, E. Lactose tolerance test as an alternative to hydrogen breath test in the study of lactose malabsorption. Adv. Lab. Med. / Av. en Med. de Lab. 2020, 1, 20200102. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Kumar, S.; Chourasia, D.; Misra, A. Lactose hydrogen breath test versus lactose tolerance test in the tropics: does positive lactose tolerance test reflect more severe lactose malabsorption? Trop Gastroenterol 2009, 30, 86–90. [Google Scholar]
- Pimentel, M.; Kong, Y.; Park, S. Breath testing to evaluate lactose intolerance in irritable bowel syndrome correlates with lactulose testing and may not reflect true lactose malabsorption. Am J Gastroenterol 2003, 98, 2700–2704. [Google Scholar] [CrossRef] [PubMed]
- Misselwitz, B.; et al. Lactose malabsorption and intolerance: pathogenesis, diagnosis and treatment. United European Gastroenterol J 2013, 1, 151–159. [Google Scholar]
- Newcomer, A.D.; McGill, D.B.; Thomas, P.J.; Hofmann, A.F. Prospective Comparison of Indirect Methods for Detecting Lactase Deficiency. New Engl. J. Med. 1975, 293, 1232–1236. [Google Scholar] [CrossRef]
- Rana, S.V.; Malik, A. Hydrogen Breath Tests in Gastrointestinal Diseases. Indian J. Clin. Biochem. 2014, 29, 398–405. [Google Scholar] [CrossRef]
- Beyerlein, L.; et al. Correlation between symptoms developed after the oral ingestion of 50 g lactose and results of hydrogen breath testing for lactose intolerance. Aliment Pharmacol Ther 2008, 27, 659–65. [Google Scholar] [CrossRef]
- Bond, J.H.; Levitt, M.D. Quantitative Measurement of Lactose Absorption. Gastroenterology 1976, 70, 1058–1062. [Google Scholar] [CrossRef]
- Robles, L.; Priefer, R. Lactose Intolerance: What Your Breath Can Tell You. Diagnostics 2020, 10, 412. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, M.; et al. Mixing of the intestinal content and variations of fermentation capacity do not affect the results of hydrogen breath test. Am J Gastroenterol 2003, 98, 1584–1587. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Strocchi, A.; Gasbarrini, G. Fasting breath hydrogen in celiac disease. Gastroenterology 1987, 93, 53–58. [Google Scholar] [CrossRef]
- Ansaldi-Balocco, N.; Malorgio, E.; Faussone, D.; Dell'Olio, D.; Morra, I.; Forni, M.; Oderda, G. [Hydrogen breath test in celiac disease: relationship to histological changes in jejunal mucosa]. Minerva Pediatr. 1994, 46, 569–574. [Google Scholar]
- Villanueva-Millan, M.J.; Leite, G.; Wang, J.; Morales, W.; Parodi, G.; Pimentel, M.L.; Barlow, G.M.; Mathur, R.; Rezaie, A.; Sanchez, M.; et al. Methanogens and Hydrogen Sulfide Producing Bacteria Guide Distinct Gut Microbe Profiles and Irritable Bowel Syndrome Subtypes. Am. J. Gastroenterol. 2022, 117, 2055–2066. [Google Scholar] [CrossRef]
- Schneider, C.; Wutzke, K.D.; Däbritz, J. Methane breath tests and blood sugar tests in children with suspected carbohydrate malabsorption. Sci. Rep. 2020, 10, 18972. [Google Scholar] [CrossRef] [PubMed]
- Casellas, F.; Guarner, L.; Antolín, M.; Malagelada, J.-R. Hydrogen Breath Test With Low-Dose Rice Flour for Assessment of Exocrine Pancreatic Insufficiency. Pancreas 2004, 29, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Hassan, N.A.; Al-Ani, M.R.; Lafta, A.M.; Kassir, Z.A. Value of breath hydrogen test in detection of hypolactasia in patients with chronic diarrhoea. J. Chromatogr. B: Biomed. Sci. Appl. 1990, 530, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Lee, K.; Chung, Y.Y.; Lee, Y.W.; Kim, D.B.; Sung, H.J.; Chung, W.C.; Paik, C. Clinical significance of the glucose breath test in patients with inflammatory bowel disease. J. Gastroenterol. Hepatol. 2015, 30, 990–994. [Google Scholar] [CrossRef]
- Mishkin, D.; Boston, F.M.; Blank, D.; Yalovsky, M.; Mishkin, S. The Glucose Breath Test: A Diagnostic Test for Small Bowel Stricture(s) in Crohn's Disease. Dig. Dis. Sci. 2002, 47, 489–494. [Google Scholar] [CrossRef]
- Tsuji, K.; Shimizu, M.; Nishimura, Y.; Nakagawa, Y.; Ichikawa, T. Simultaneous Determination of Hydrogen, Methane and Carbon Dioxide of Breath Using Gas-Solid Chromatography. J. Nutr. Sci. Vitaminol. 1992, 38, 103–109. [Google Scholar] [CrossRef]
- Di Stefano, M.; Mengoli, C.; Bergonzi, M.; Miceli, E.; Pagani, E.; Corazza, G.R. Hydrogen breath test in patients with severe constipation: the interference of the mixing of intestinal content. Neurogastroenterol. Motil. 2014, 26, 1754–1760. [Google Scholar] [CrossRef]
- Wolf, P.G.; Parthasarathy, G.; Chen, J.; O'Connor, H.M.; Chia, N.; Bharucha, A.E.; Gaskins, H.R. Assessing the colonic microbiome, hydrogenogenic and hydrogenotrophic genes, transit and breath methane in constipation. Neurogastroenterol. Motil. 2017, 29, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Rezaie, A. Pros and Cons of Breath Testing for Small Intestinal Bacterial Overgrowth and Intestinal Methanogen Overgrowth. Gastroenterol Hepatol (N Y) 2023, 19, 140–146. [Google Scholar]
- Rezaie, A.; Buresi, M.; Lembo, A.; Lin, H.; McCallum, R.; Rao, S.; Schmulson, M.; Valdovinos, M.; Zakko, S.; Pimentel, M. Hydrogen and Methane-Based Breath Testing in Gastrointestinal Disorders: The North American Consensus. Am. J. Gastroenterol. 2017, 112, 775–784. [Google Scholar] [CrossRef]
- Berthold, H.K.; Schober, P.; Scheurlen, C.; Marklein, G.; Horré, R.; Gouni-Berthold, I.; Sauerbruch, T. Use of the lactose-[13C]ureide breath test for diagnosis of small bowel bacterial overgrowth: comparison to the glucose hydrogen breath test. J. Gastroenterol. 2009, 44, 944–951. [Google Scholar] [CrossRef]
- Sundin, O.H.; et al. Does a glucose-based hydrogen and methane breath test detect bacterial overgrowth in the jejunum? Neurogastroenterol Motil 2018, 30, e13350. [Google Scholar] [CrossRef] [PubMed]
- Stotzer, P.; Brandberg, A.; Kilander, A.F. Diagnosis of small intestinal bacterial overgrowth in clinical praxis: a comparison of the culture of small bowel aspirate, duodenal biopsies and gastric aspirate. Hepatogastroenterology 1998, 45, 1018–1022. [Google Scholar]
- Leite, G.; Morales, W.; Weitsman, S.; Celly, S.; Parodi, G.; Mathur, R.; Barlow, G.M.; Sedighi, R.; Millan, M.J.V.; Rezaie, A.; et al. The duodenal microbiome is altered in small intestinal bacterial overgrowth. PLOS ONE 2020, 15, e0234906. [Google Scholar] [CrossRef]
- Maeda, Y. and T. Murakami, Diagnosis by Microbial Culture, Breath Tests and Urinary Excretion Tests, and Treatments of Small Intestinal Bacterial Overgrowth. Antibiotics 2023, 12, 263. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Talley, N.J.; Holtmann, G. Current and Future Approaches for Diagnosing Small Intestinal Dysbiosis in Patients With Symptoms of Functional Dyspepsia. Front. Neurosci. 2022, 16, 830356. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Dutta, U.; Noor, M.T.; Taneja, N.; Kochhar, R.; Sharma, M.; Singh, K. Endoscopic jejunal biopsy culture: a simple and effective method to study jejunal microflora. Indian J. Gastroenterol. 2010, 29, 226–230. [Google Scholar] [CrossRef]
- Tuteja, A.K.; Talley, N.J.; Stoddard, G.J.; Samore, M.H.; Verne, G.N. Risk factors for upper and lower functional gastrointestinal disorders in Persian Gulf War Veterans during and post-deployment. Neurogastroenterol. Motil. 2019, 31, e13533. [Google Scholar] [CrossRef]
- Shimura, S.; Ishimura, N.; Mikami, H.; Okimoto, E.; Uno, G.; Tamagawa, Y.; Aimi, M.; Oshima, N.; Sato, S.; Ishihara, S.; et al. Small Intestinal Bacterial Overgrowth in Patients with Refractory Functional Gastrointestinal Disorders. J. Neurogastroenterol. Motil. 2015, 22, 60–68. [Google Scholar] [CrossRef]
- Petzold, G.; Amanzada, A.; Gress, T.M.; Ellenrieder, V.; Neesse, A.; Kunsch, S. High Prevalence of Pathological Hydrogen Breath Tests in Patients with Functional Dyspepsia. Digestion 2018, 100, 186–191. [Google Scholar] [CrossRef]
- Wanzl, J.; Gröhl, K.; Kafel, A.; Nagl, S.; Muzalyova, A.; Gölder, S.K.; Ebigbo, A.; Messmann, H.; Schnoy, E. Impact of Small Intestinal Bacterial Overgrowth in Patients with Inflammatory Bowel Disease and Other Gastrointestinal Disorders—A Retrospective Analysis in a Tertiary Single Center and Review of the Literature. J. Clin. Med. 2023, 12, 935. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Feng, J.; Chen, L.; Yang, Z.; Tao, H.; Li, L.; Xuan, J.; Wang, F. Small intestinal bacterial overgrowth is associated with clinical relapse in patients with quiescent Crohn’s disease: a retrospective cohort study. Ann. Transl. Med. 2022, 10, 784–784. [Google Scholar] [CrossRef]
- Shah, A.; Talley, N.J.; Koloski, N.; Macdonald, G.A.; Kendall, B.J.; Shanahan, E.R.; Walker, M.M.; Keely, S.; Jones, M.P.; Morrison, M.; et al. Duodenal bacterial load as determined by quantitative polymerase chain reaction in asymptomatic controls, functional gastrointestinal disorders and inflammatory bowel disease. Aliment. Pharmacol. Ther. 2020, 52, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Ricci, J.E.; Chebli, L.A.; Ribeiro, T.C.; Castro, A.C.; Gaburri, P.D.; Pace, F.H.; Barbosa, K.V.; Ferreira, L.E.; Passos, M.D.; Malaguti, C.; et al. Small-Intestinal Bacterial Overgrowth is Associated With Concurrent Intestinal Inflammation But Not With Systemic Inflammation in Crohn’s Disease Patients. J. Clin. Gastroenterol. 2018, 52, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; et al. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur J Gastroenterol Hepatol 2014, 26, 753–60. [Google Scholar] [CrossRef]
- Zhao, J.; Zheng, X.; Chu, H.; Cong, Y.; Fried, M.; Fox, M.; Dai, N. A study of the methodological and clinical validity of the combined lactulose hydrogen breath test with scintigraphic oro-cecal transit test for diagnosing small intestinal bacterial overgrowth in IBS patients. Neurogastroenterol. Motil. 2014, 26, 794–802. [Google Scholar] [CrossRef]
- Rana, S.; Sharma, S.; Kaur, J.; Sinha, S.; Singh, K. Comparison of Lactulose and Glucose Breath Test for Diagnosis of Small Intestinal Bacterial Overgrowth in Patients with Irritable Bowel Syndrome. Digestion 2012, 85, 243–247. [Google Scholar] [CrossRef]
- Ghoshal, U.C. How to Interpret Hydrogen Breath Tests. J. Neurogastroenterol. Motil. 2011, 17, 312–317. [Google Scholar] [CrossRef]
- Lin, H.C. Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome. JAMA 2004, 292, 852–858. [Google Scholar] [CrossRef]
- Banik, G.D.; De, A.; Som, S.; Jana, S.; Daschakraborty, S.B.; Chaudhuri, S.; Pradhan, M. Hydrogen sulphide in exhaled breath: a potential biomarker for small intestinal bacterial overgrowth in IBS. J. Breath Res. 2016, 10, 026010. [Google Scholar] [CrossRef]
- Kashyap, P.; Moayyedi, P.; Quigley, E.M.M.; Simren, M.; Vanner, S. Critical appraisal of the SIBO hypothesis and breath testing: A clinical practice update endorsed by the European society of neurogastroenterology and motility (ESNM) and the American neurogastroenterology and motility society (ANMS). Neurogastroenterol. Motil. 2024, 36, e14817. [Google Scholar] [CrossRef]
- Chen, B.; Kim, J.J.-W.; Zhang, Y.; Du, L.; Dai, N. Prevalence and predictors of small intestinal bacterial overgrowth in irritable bowel syndrome: a systematic review and meta-analysis. J. Gastroenterol. 2018, 53, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Moraru, I.G.; Portincasa, P.; Moraru, A.G.; Diculescu, M.; Dumitraşcu, D.L. Small intestinal bacterial overgrowth produces symptoms in irritable bowel syndrome which are improved by rifaximin. A pilot study.. 2014, 51, 143–147. [Google Scholar]
- Ghoshal, U.C.; et al. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur J Gastroenterol Hepatol. 2014, 26, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Khoshini, R.; Dai, S.-C.; Lezcano, S.; Pimentel, M. A Systematic Review of Diagnostic Tests for Small Intestinal Bacterial Overgrowth. Dig. Dis. Sci. 2007, 53, 1443–1454. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; et al. Evaluation of small intestinal bacterial overgrowth. Expert Rev Gastroenterol Hepatol 2023, 17, 461–467. [Google Scholar] [CrossRef]
- Jo, I.H.; Paik, C.-N.; Kim, Y.-J.; Lee, J.M.; Choi, S.Y.; Hong, K.P. Lactase Deficiency Diagnosed by Endoscopic Biopsy-based Method is Associated With Positivity to Glucose Breath Test. J. Neurogastroenterol. Motil. 2023, 29, 85–93. [Google Scholar] [CrossRef]
- Zhou, D.X.; Ma, Y.J.; Chen, G.Y.; Gao, X.; Yang, L. [Relationship of TLR2 and TLR4 expressions on the surface of peripheral blood mononuclear cells to small intestinal bacteria overgrowth in patients with hepatocellular carcinoma]. Zhonghua Gan Zang Bing Za Zhi 2019, 27, 286–290. [Google Scholar]
- Gkolfakis, P.; Tziatzios, G.; Leite, G.; Papanikolaou, I.S.; Xirouchakis, E.; Panayiotides, I.G.; Karageorgos, A.; Millan, M.J.; Mathur, R.; Weitsman, S.; et al. Prevalence of Small Intestinal Bacterial Overgrowth Syndrome in Patients with Non-Alcoholic Fatty Liver Disease/Non-Alcoholic Steatohepatitis: A Cross-Sectional Study. Microorganisms 2023, 11, 723. [Google Scholar] [CrossRef]
- Fitriakusumah, Y.; Lesmana, C.R.A.; Bastian, W.P.; Jasirwan, C.O.M.; Hasan, I.; Simadibrata, M.; Kurniawan, J.; Sulaiman, A.S.; Gani, R.A. The role of Small Intestinal Bacterial Overgrowth (SIBO) in Non-alcoholic Fatty Liver Disease (NAFLD) patients evaluated using Controlled Attenuation Parameter (CAP) Transient Elastography (TE): a tertiary referral center experience. BMC Gastroenterol. 2019, 19, 43. [Google Scholar] [CrossRef]
- Shi, H.; Mao, L.; Wang, L.; Quan, X.; Xu, X.; Cheng, Y.; Zhu, S.; Dai, F. Small intestinal bacterial overgrowth and orocecal transit time in patients of nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2021, 33, e535–e539. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; Baker, J.; Harer, K.; Lee, A.; Hasler, W.; Saad, R.; Schulman, A.R. Small Intestinal Bacterial Overgrowth: Clinical Presentation in Patients with Roux-en-Y Gastric Bypass. Obes. Surg. 2020, 31, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.B.; Paik, C.-N.; Kim, Y.J.; Lee, J.M.; Jun, K.-H.; Chung, W.C.; Lee, K.-M.; Yang, J.-M.; Choi, M.-G. Positive Glucose Breath Tests in Patients with Hysterectomy, Gastrectomy, and Cholecystectomy. Gut Liver 2017, 11, 237–242. [Google Scholar] [CrossRef]
- Larsen, H.M.; Krogh, K.; Borre, M.; Gregersen, T.; Hansen, M.M.; Arveschoug, A.K.; Christensen, P.; Drewes, A.M.; Emmertsen, K.J.; Laurberg, S.; et al. Chronic loose stools following right-sided hemicolectomy for colon cancer and the association with bile acid malabsorption and small intestinal bacterial overgrowth. Color. Dis. 2022, 25, 600–607. [Google Scholar] [CrossRef]
- Zhu, D.; et al. Influence of Helicobacter pylori infection and its eradication treatment on small intestinal bacterial overgrowth. Zhonghua Yi Xue Za Zhi 2022, 102, 3382–3387. [Google Scholar]
- George, N.S.; Sankineni, A.; Parkman, H.P. Small Intestinal Bacterial Overgrowth in Gastroparesis. Dig. Dis. Sci. 2012, 59, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Xu, Y.; Hou, X.; Li, J.; Cai, Y.; Hao, Y.; Ouyang, Q.; Wu, B.; Sun, Z.; Zhang, M.; et al. Small Intestinal Bacterial Overgrowth in Subclinical Hypothyroidism of Pregnant Women. Front. Endocrinol. 2021, 12. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, G.; Duan, Y.; Han, X.; Dong, H.; Geng, J. Prevalence of Small Intestinal Bacterial Overgrowth in Multiple Sclerosis: a Case-Control Study from China. J. Neuroimmunol. 2016, 301, 83–87. [Google Scholar] [CrossRef]
- Hasuike, Y.; Endo, T.; Koroyasu, M.; Matsui, M.; Mori, C.; Yamadera, M.; Fujimura, H.; Sakoda, S. Bile acid abnormality induced by intestinal dysbiosis might explain lipid metabolism in Parkinson’s disease. Med Hypotheses 2020, 134, 109436. [Google Scholar] [CrossRef]
- Jo, J.H.; Park, S.J.; Cheon, J.H.; Kim, T.I.; Kim, W.H. Rediscover the clinical value of small intestinal bacterial overgrowth in patients with intestinal Behçet's disease. J. Gastroenterol. Hepatol. 2018, 33, 375–379. [Google Scholar] [CrossRef]
- Naletov, A.V.; Svistunova, N.A. Assessment of the state of the small intestine microbiota in children on a long-term dairy-free diet. Probl. Nutr. 2022, 91, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Durán-Rosas, C.; Priego-Parra, B.A.; Morel-Cerda, E.; Mercado-Jauregui, L.A.; Aquino-Ruiz, C.A.; Triana-Romero, A.; Amieva-Balmori, M.; Velasco, J.A.V.-R.; Remes-Troche, J.M. Incidence of Small Intestinal Bacterial Overgrowth and Symptoms After 7 Days of Proton Pump Inhibitor Use: A Study on Healthy Volunteers. Dig. Dis. Sci. 2023, 69, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Muraki, M.; Fujiwara, Y.; Machida, H.; Okazaki, H.; Sogawa, M.; Yamagami, H.; Tanigawa, T.; Shiba, M.; Watanabe, K.; Tominaga, K.; et al. Role of small intestinal bacterial overgrowth in severe small intestinal damage in chronic non-steroidal anti-inflammatory drug users. Scand. J. Gastroenterol. 2013, 49, 267–273. [Google Scholar] [CrossRef]
- Shah, A.; Talley, N.J.; Jones, M.; Kendall, B.J.; Koloski, N.; Walker, M.M.; Morrison, M.; Holtmann, G.J. Small Intestinal Bacterial Overgrowth in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Case-Control Studies. Am. J. Gastroenterol. 2020, 115, 190–201. [Google Scholar] [CrossRef]
- Shah, A.; Thite, P.; Hansen, T.; Kendall, B.J.; Sanders, D.S.; Morrison, M.; Jones, M.P.; Holtmann, G. Links between celiac disease and small intestinal bacterial overgrowth: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2022, 37, 1844–1852. [Google Scholar] [CrossRef]
- Maslennikov, R.; Pavlov, C.; Ivashkin, V. Small intestinal bacterial overgrowth in cirrhosis: systematic review and meta-analysis. Hepatol. Int. 2018, 12, 567–576. [Google Scholar] [CrossRef] [PubMed]
- El Kurdi, B.; Babar, S.; El Iskandarani, M.; Bataineh, A.; Lerch, M.M.; Young, M.; Singh, V.P. Factors That Affect Prevalence of Small Intestinal Bacterial Overgrowth in Chronic Pancreatitis: A Systematic Review, Meta-Analysis, and Meta-Regression. Clin. Transl. Gastroenterol. 2019, 10, e00072. [Google Scholar] [CrossRef]
- Feng, X.; Li, X.-Q. The prevalence of small intestinal bacterial overgrowth in diabetes mellitus: a systematic review and meta-analysis. Aging 2022, 14, 975–988. [Google Scholar] [CrossRef]
- Shah, A.; Pakeerathan, V.; Jones, M.P.; Kashyap, P.C.; Virgo, K.; Fairlie, T.; Morrison, M.; Ghoshal, U.C.; Holtmann, G.J. Small Intestinal Bacterial Overgrowth Complicating Gastrointestinal Manifestations of Systemic Sclerosis: A Systematic Review and Meta-analysis. J. Neurogastroenterol. Motil. 2023, 29, 132–144. [Google Scholar] [CrossRef]
- Shimura, S.; Ishimura, N.; Mikami, H.; Okimoto, E.; Uno, G.; Tamagawa, Y.; Aimi, M.; Oshima, N.; Sato, S.; Ishihara, S.; et al. Small Intestinal Bacterial Overgrowth in Patients with Refractory Functional Gastrointestinal Disorders. J. Neurogastroenterol. Motil. 2015, 22, 60–68. [Google Scholar] [CrossRef]
- Petzold, G.; Amanzada, A.; Gress, T.M.; Ellenrieder, V.; Neesse, A.; Kunsch, S. High Prevalence of Pathological Hydrogen Breath Tests in Patients with Functional Dyspepsia. Digestion 2018, 100, 186–191. [Google Scholar] [CrossRef]
- Chojnacki, C.; Konrad, P.; Błońska, A.; Chojnacki, J.; Mędrek-Socha, M. Usefulness of the hydrogen breath test in patients with functional dyspepsia. Gastroenterol. Rev. 2020, 15, 338–342. [Google Scholar] [CrossRef]
- Tziatzios, G.; Gkolfakis, P.; Papanikolaou, I.S.; Mathur, R.; Pimentel, M.; Damoraki, G.; Giamarellos-Bourboulis, E.J.; Dimitriadis, G.; Triantafyllou, K. High Prevalence of Small Intestinal Bacterial Overgrowth among Functional Dyspepsia Patients. Dig. Dis. 2020, 39, 382–390. [Google Scholar] [CrossRef]
- Chuah, K.H.; Wong, M.S.; Tan, P.O.; Lim, S.Z.; Beh, K.H.; Chong, S.C.S.; Zulkifli, K.K.; Thalha, A.M.; Mahadeva, S.; Lee, Y.Y. Small Intestinal Bacterial Overgrowth In Various Functional Gastrointestinal Disorders: A Case–Control Study. Dig. Dis. Sci. 2021, 67, 3881–3889. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Lee, K.; Chung, Y.Y.; Lee, Y.W.; Kim, D.B.; Sung, H.J.; Chung, W.C.; Paik, C. Clinical significance of the glucose breath test in patients with inflammatory bowel disease. J. Gastroenterol. Hepatol. 2015, 30, 990–994. [Google Scholar] [CrossRef]
- Greco, A.; Caviglia, G.P.; Brignolo, P.; Ribaldone, D.G.; Reggiani, S.; Sguazzini, C.; Smedile, A.; Pellicano, R.; Resegotti, A.; Astegiano, M.; et al. Glucose breath test and Crohn’s disease: Diagnosis of small intestinal bacterial overgrowth and evaluation of therapeutic response. Scand. J. Gastroenterol. 2015, 50, 1376–1381. [Google Scholar] [CrossRef] [PubMed]
- Andrei, M.; Gologan, S.; Stoicescu, A.; Ionescu, M.; Nicolaie, T.; Diculescu, M. Small Intestinal Bacterial Overgrowth Syndrome Prevalence in Romanian Patients with Inflammatory Bowel Disease. Curr Health Sci J 2016, 42, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Ricci, J.E.; Chebli, L.A.; Ribeiro, T.C.; Castro, A.C.; Gaburri, P.D.; Pace, F.H.; Barbosa, K.V.; Ferreira, L.E.; Passos, M.D.; Malaguti, C.; et al. Small-Intestinal Bacterial Overgrowth is Associated With Concurrent Intestinal Inflammation But Not With Systemic Inflammation in Crohn’s Disease Patients. J. Clin. Gastroenterol. 2018, 52, 530–536. [Google Scholar] [CrossRef]
- Shah, A.; Talley, N.J.; Koloski, N.; Macdonald, G.A.; Kendall, B.J.; Shanahan, E.R.; Walker, M.M.; Keely, S.; Jones, M.P.; Morrison, M.; et al. Duodenal bacterial load as determined by quantitative polymerase chain reaction in asymptomatic controls, functional gastrointestinal disorders and inflammatory bowel disease. Aliment. Pharmacol. Ther. 2020, 52, 155–167. [Google Scholar] [CrossRef]
- Ghoshal, U.C.; Yadav, A.; Fatima, B.; Agrahari, A.P.; Misra, A. Small intestinal bacterial overgrowth in patients with inflammatory bowel disease: A case-control study. Indian J. Gastroenterol. 2021, 41, 96–103. [Google Scholar] [CrossRef]
- Wei, J.; Feng, J.; Chen, L.; Yang, Z.; Tao, H.; Li, L.; Xuan, J.; Wang, F. Small intestinal bacterial overgrowth is associated with clinical relapse in patients with quiescent Crohn’s disease: a retrospective cohort study. Ann. Transl. Med. 2022, 10, 784–784. [Google Scholar] [CrossRef] [PubMed]
- Wanzl, J.; Gröhl, K.; Kafel, A.; Nagl, S.; Muzalyova, A.; Gölder, S.K.; Ebigbo, A.; Messmann, H.; Schnoy, E. Impact of Small Intestinal Bacterial Overgrowth in Patients with Inflammatory Bowel Disease and Other Gastrointestinal Disorders—A Retrospective Analysis in a Tertiary Single Center and Review of the Literature. J. Clin. Med. 2023, 12, 935. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, U.C.; et al. Breath tests in the diagnosis of small intestinal bacterial overgrowth in patients with irritable bowel syndrome in comparison with quantitative upper gut aspirate culture. Eur J Gastroenterol Hepatol 2014, 26, 753–60. [Google Scholar] [CrossRef] [PubMed]
- Moraru, I.G.; Moraru, A.G.; Andrei, M.; Iordache, T.; Drug, V.; Diculescu, M.; Portincasa, P.; Dumitrascu, D.L. Small intestinal bacterial overgrowth is associated to symptoms in irritable bowel syndrome. Evidence from a multicentre study in Romania. Rom J Intern Med. 2014, 52, 143–150. [Google Scholar]
- Abbasi, M.H.; et al. Small bowel bacterial overgrowth in patients with irritable bowel syndrome: the first study in iran. Middle East J Dig Dis 2015, 7, 36–40. [Google Scholar]
- Chuah, K.H.; Wong, M.S.; Tan, P.O.; Lim, S.Z.; Beh, K.H.; Chong, S.C.S.; Zulkifli, K.K.; Thalha, A.M.; Mahadeva, S.; Lee, Y.Y. Small Intestinal Bacterial Overgrowth In Various Functional Gastrointestinal Disorders: A Case–Control Study. Dig. Dis. Sci. 2021, 67, 3881–3889. [Google Scholar] [CrossRef]
Figure A1.
The primary risk factors for SIBO include neurological disorders, immune-related diseases, hepatobiliary and pancreatic diseases, gastrointestinal disorders, endocrine and metabolic diseases, surgical interventions, aging, Helicobacter pylori infection, dietary factors, and medication use.
Figure A1.
The primary risk factors for SIBO include neurological disorders, immune-related diseases, hepatobiliary and pancreatic diseases, gastrointestinal disorders, endocrine and metabolic diseases, surgical interventions, aging, Helicobacter pylori infection, dietary factors, and medication use.
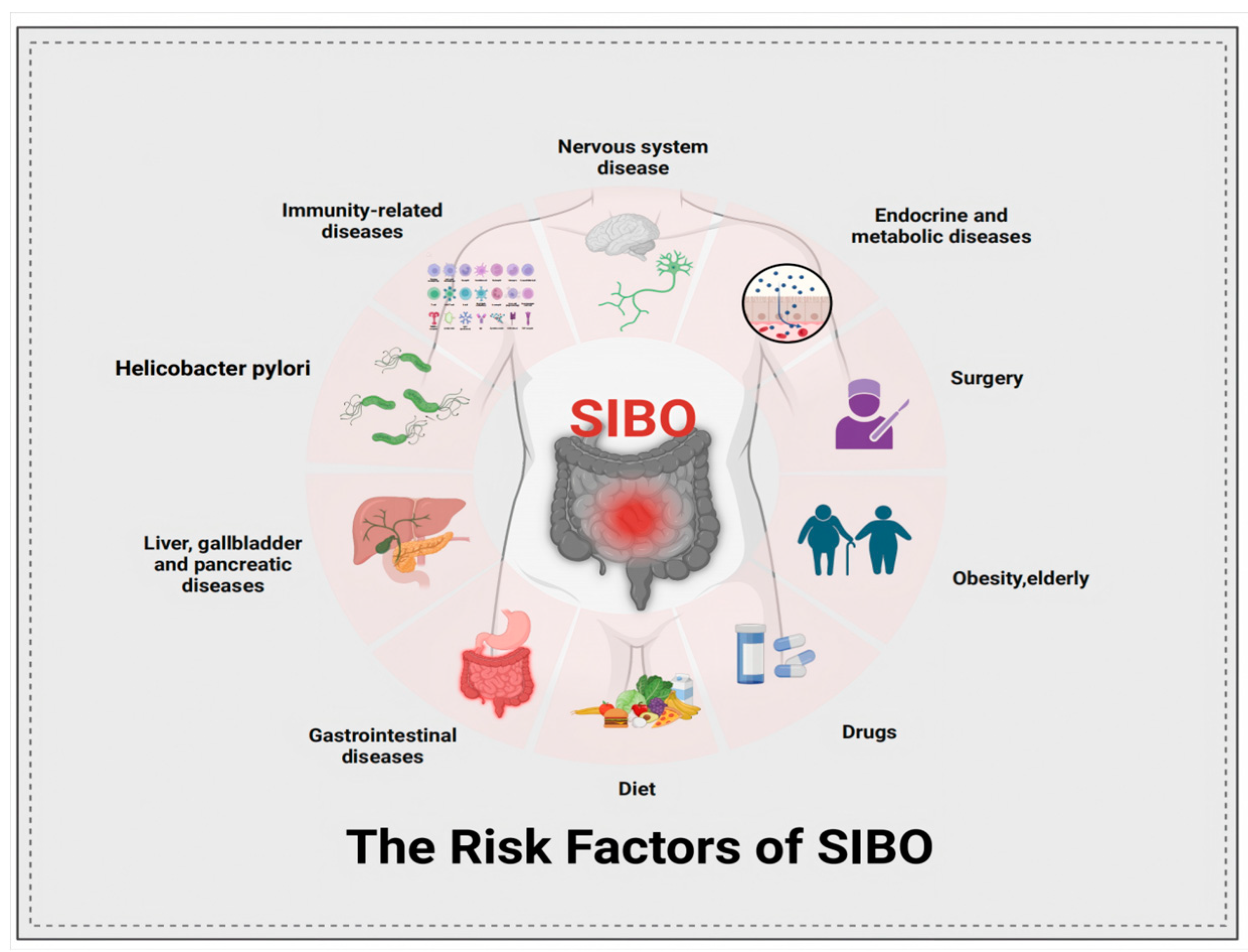
Figure A2.
The influence of SIBO on the human body encompasses a range of gastrointestinal disorders, including IBS, CD, UC, celiac disease, liver cirrhosis, pancreatitis, and NAFLD. Furthermore, SIBO is linked to various extra-GIT diseases, such as autoimmune disorders (e.g., rheumatoid arthritis, lupus), cardiovascular diseases (e.g., atherosclerosis, hypertension), metabolic disorders (e.g., obesity, type 2 diabetes), endocrine disorders (e.g., thyroid dysfunction), kidney disease, dermatological issues (e.g., acne, psoriasis), neurological diseases (e.g., migraine, Parkinson's disease), and mental health disorders (e.g., anxiety, depression). Additionally, SIBO has been associated with genetic predispositions and gastrointestinal cancers, including gastric cancer and colorectal cancer.
Figure A2.
The influence of SIBO on the human body encompasses a range of gastrointestinal disorders, including IBS, CD, UC, celiac disease, liver cirrhosis, pancreatitis, and NAFLD. Furthermore, SIBO is linked to various extra-GIT diseases, such as autoimmune disorders (e.g., rheumatoid arthritis, lupus), cardiovascular diseases (e.g., atherosclerosis, hypertension), metabolic disorders (e.g., obesity, type 2 diabetes), endocrine disorders (e.g., thyroid dysfunction), kidney disease, dermatological issues (e.g., acne, psoriasis), neurological diseases (e.g., migraine, Parkinson's disease), and mental health disorders (e.g., anxiety, depression). Additionally, SIBO has been associated with genetic predispositions and gastrointestinal cancers, including gastric cancer and colorectal cancer.
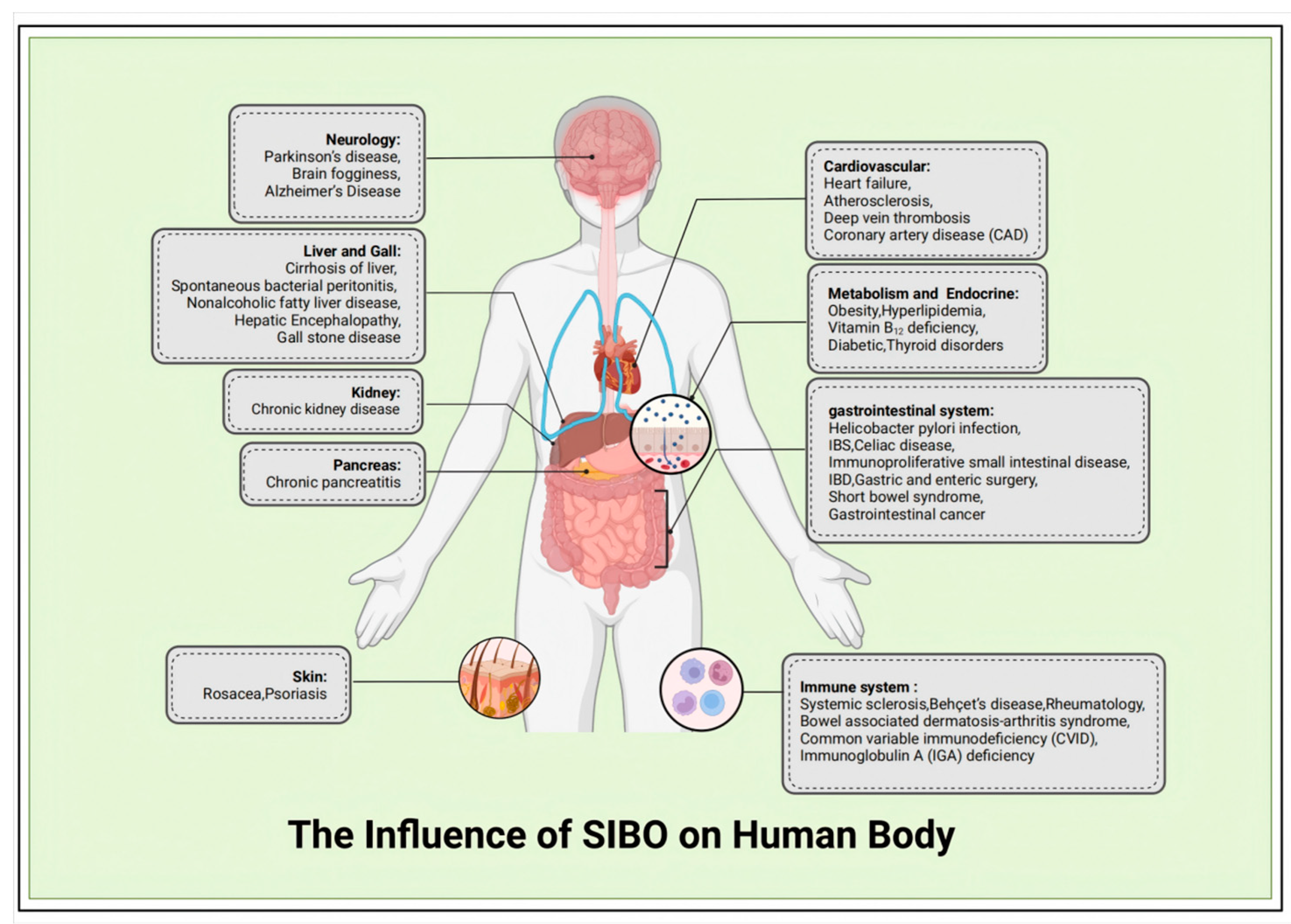
Figure A3.
Diagram of the breath test machine. a. The human body does not produce hydrogen and methane molecules through its own metabolism; instead, all hydrogen and methane molecules in the body originate from the fermentation of carbohydrates by bacteria in the digestive tract. These gases are reabsorbed and subsequently expelled through the respiratory tract, allowing for the evaluation of small intestinal bacterial levels using appropriate instruments. b. Schematic diagram of gas generation. c. Schematic representation of the early rise in hydrogen and methane levels during breath tests for both healthy individuals and patients with SIBO. d. Breath test results in a SIBO patient, displaying a double peak that represents the early rise observed in the small intestine, followed by a brief decline in hydrogen levels before the anticipated increase in hydrogen occurs in the large bowel.
Figure A3.
Diagram of the breath test machine. a. The human body does not produce hydrogen and methane molecules through its own metabolism; instead, all hydrogen and methane molecules in the body originate from the fermentation of carbohydrates by bacteria in the digestive tract. These gases are reabsorbed and subsequently expelled through the respiratory tract, allowing for the evaluation of small intestinal bacterial levels using appropriate instruments. b. Schematic diagram of gas generation. c. Schematic representation of the early rise in hydrogen and methane levels during breath tests for both healthy individuals and patients with SIBO. d. Breath test results in a SIBO patient, displaying a double peak that represents the early rise observed in the small intestine, followed by a brief decline in hydrogen levels before the anticipated increase in hydrogen occurs in the large bowel.
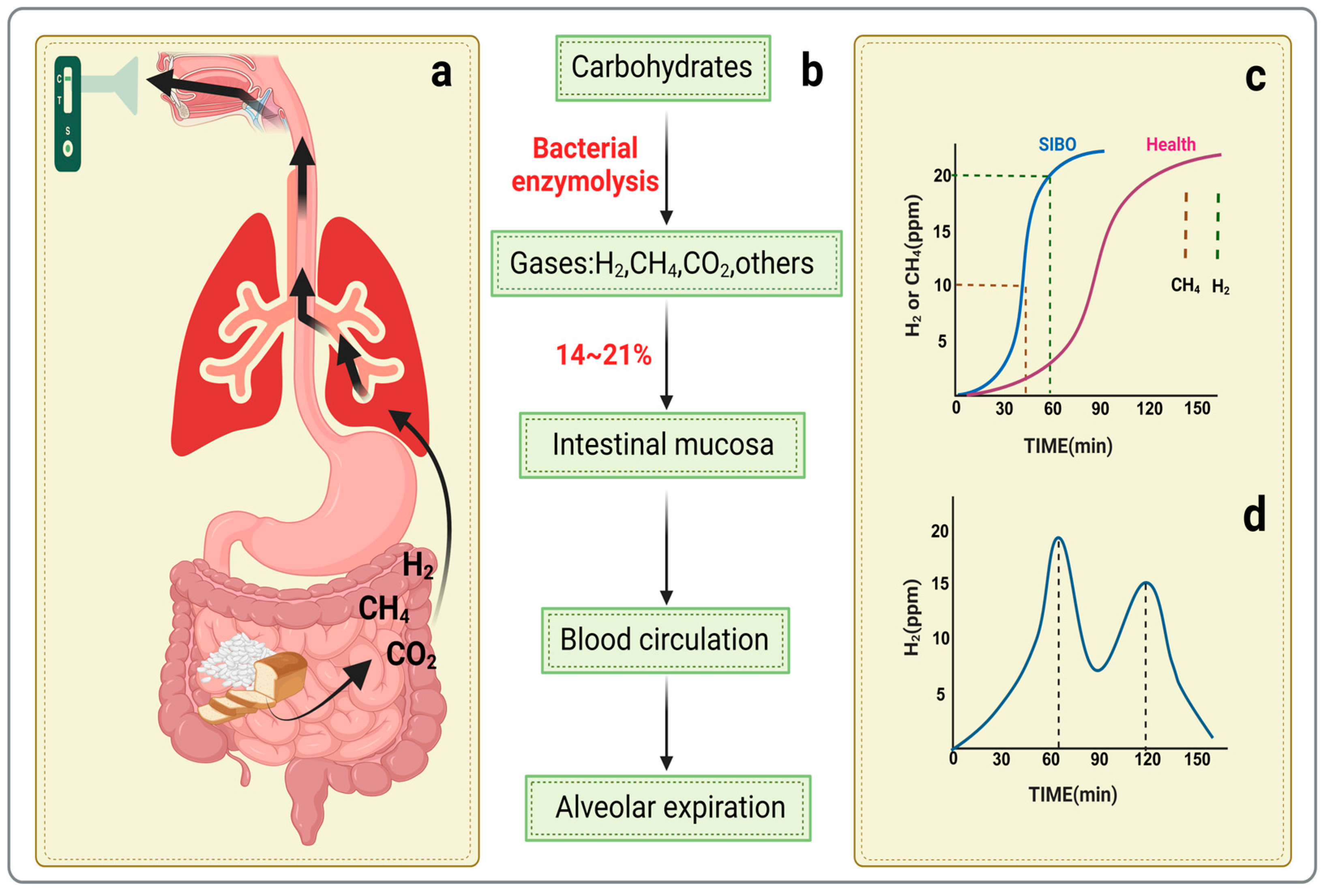

Table A1.
Prevalence of SIBO in Various Diseases.
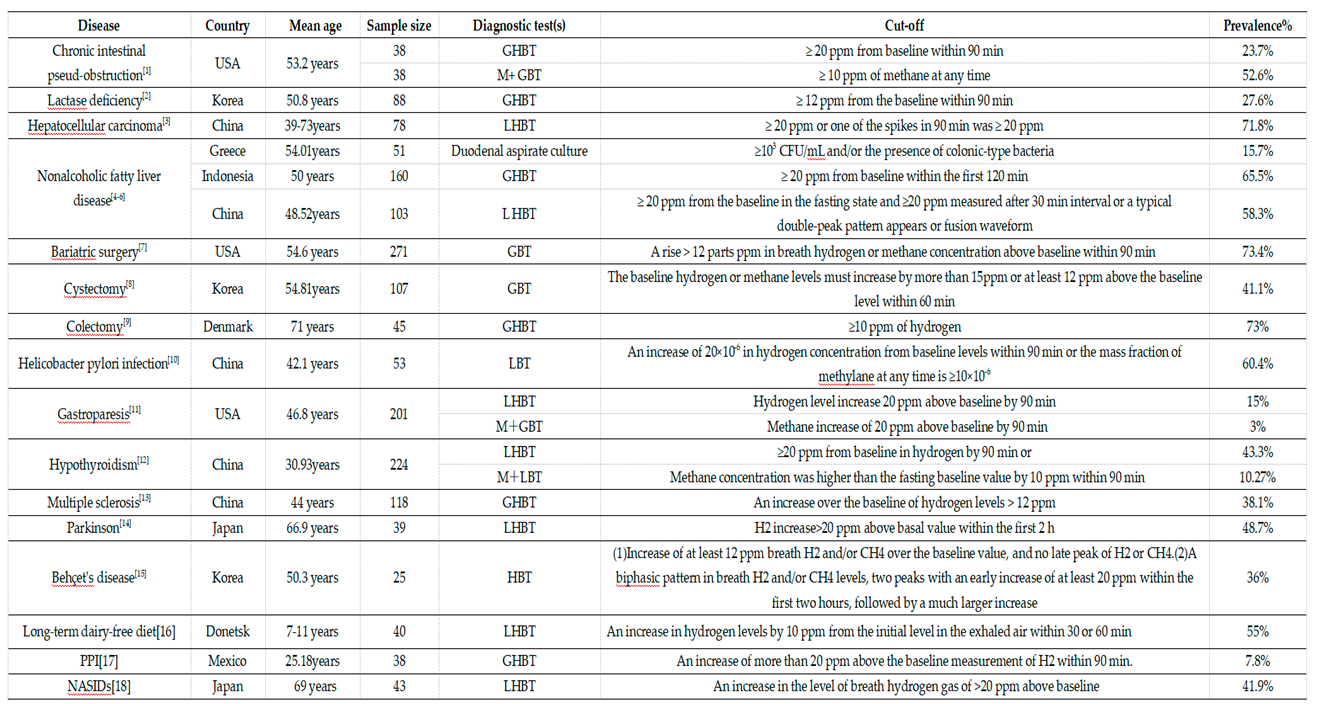 |
Table A2.
Meta-analysis of SIBO prevalence in various diseases.
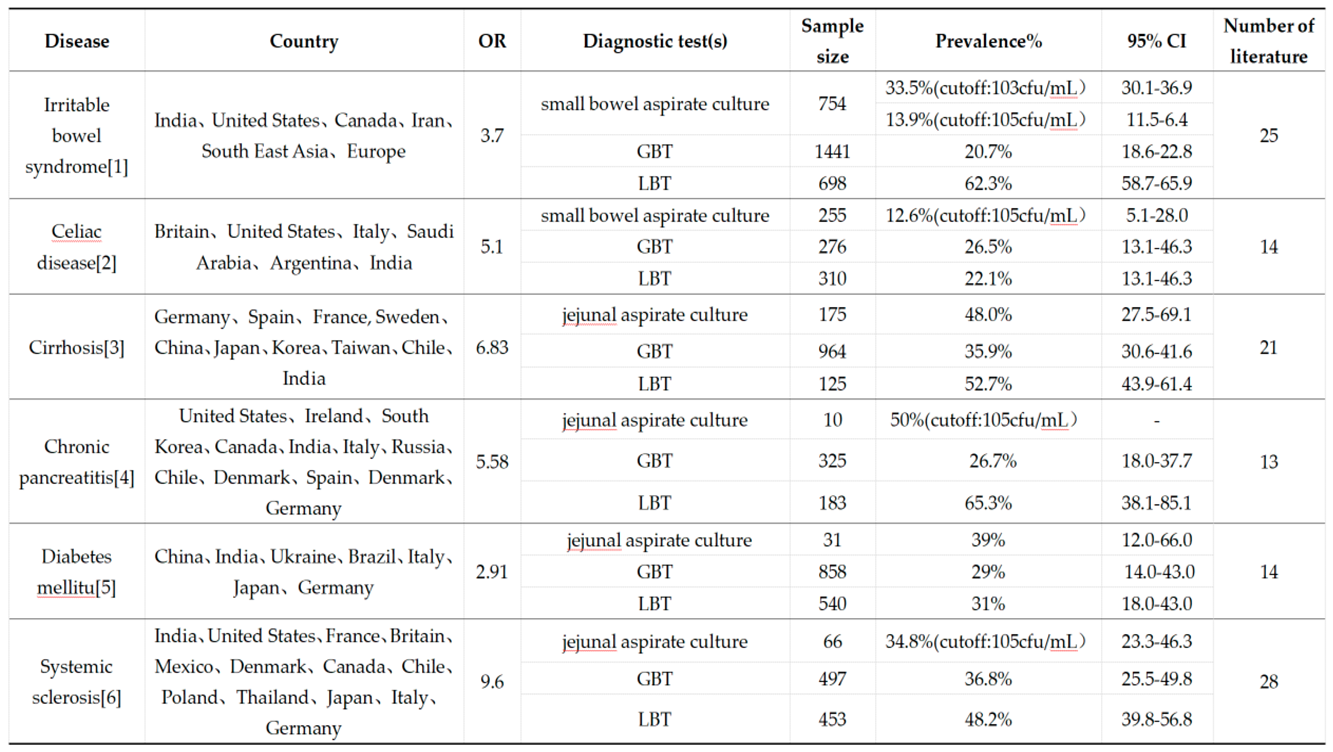 |
The table summarizes the results of a meta-analysis concerning the prevalence of SIBO across various diseases, as reported in previous literature. It includes information on the countries involved, sample sizes, diagnostic testing methods, odds ratios, 95% confidence intervals, and the number of studies included in each analysis. 2) Furthermore, an odds ratio (OR) greater than 1 indicates a higher risk of SIBO in individuals with the specified diseases. The 95% confidence interval (CI) suggests that there is a 95% probability that the true prevalence of SIBO falls within this specified range.
Table A3.
Comparative analysis of SIBO in FD, inflammatory bowel disease, and constipation.
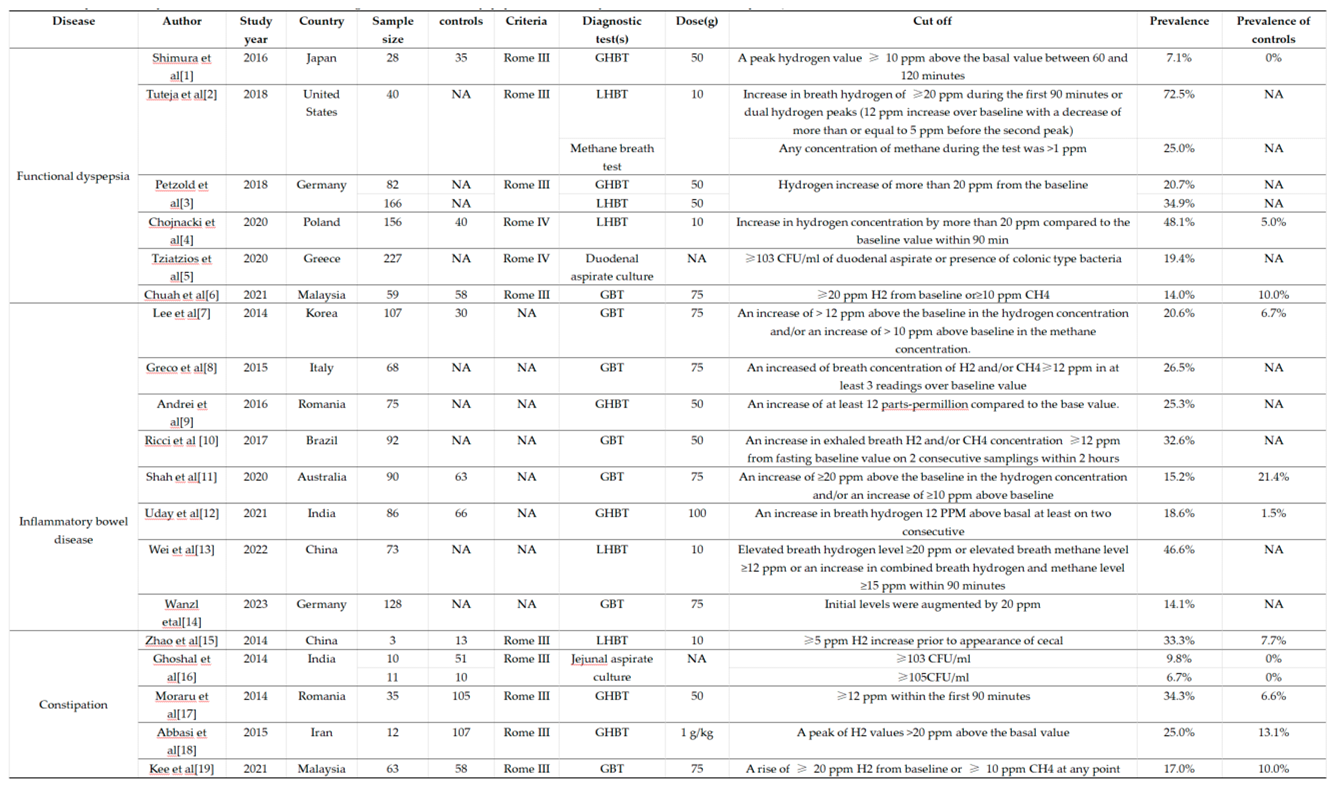 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



