
Submitted:
06 April 2025
Posted:
07 April 2025
You are already at the latest version
Abstract
Background/Objectives: Adolescence is a pivotal stage marked by physiological and behavioral shifts that shape dietary habits and health outcomes. Methods: This cross-sectional study analyzed 662 questionnaire responses to explore associations between socio-demographic variables, dietary behaviors, and health practices among school-aged children and adolescents. Results: The analysis reveals significant gender differences in body mass index (BMI), weight-loss behaviors, and family structure. Female adolescents were more likely to be underweight (18.27%) compared to male adolescents (10.82%), while overweight prevalence was higher among male adolescents (18.66%) than female adolescents (11.68%) (χ² = 11.457, p = 0.009). Dietary patterns varied significantly across age groups, with high school-aged children demonstrating lower vegetable consumption and increased autonomy over food choices. Primary school children exhibited higher intake of carbonated beverages (OR = 0.185, p = 0.002 for high school; OR = 0.116, p < 0.001 for middle school), whereas teenagers showed a preference for structured meals and lower fast-food intake. Meat consumption frequency correlated with greater diversity in protein sources (χ² = 48.77, p < 0.001), while chaotic eating behaviors were more prevalent among middle and high school-aged children (OR = 2.291, p = 0.032 for middle school; OR = 2.225, p = 0.030 for high school). Hydration habits played an essential role in dietary quality, with school-age children consuming ≥3 liters of water daily exhibiting healthier eating patterns (OR = 7.146, p = 0.001). Additionally, psychological factors such as fatigue and stress were significantly associated with unhealthy dietary choice. Conclusions: These findings highlight the need for targeted nutritional education, school-based interventions, and family-focused strategies to improve adolescent health behaviors.
Keywords:
adolescent nutrition
; dietary habits
; gender differences
; socio-demographic factors
; health behaviors
; nutritional interventions
1. Introduction
Adolescence is a critical period of physical and psychological development, during which nutrition and lifestyle choices play a fundamental role in mental well-being. A balanced diet rich in essential nutrients, such as omega-3 fatty acids, vitamins B and D, calcium and antioxidants, supports brain function, emotional regulation, cognitive performance and bone health [1-3]. Conversely, diets high in processed foods, sugar, and unhealthy fats have been linked to an increased risk of anxiety, depression, and mood instability [4,5]. In addition to diet, lifestyle factors such as physical activity, sleep quality, and screen time significantly impact adolescents’ psychological health. Regular exercise promotes the release of endorphins and reduces stress, while insufficient sleep and excessive screen exposure contribute to irritability, poor concentration, and emotional distress. Understanding the complex interaction between nutrition, lifestyle, and mental health is essential for developing effective strategies to promote psychological resilience and overall well-being in adolescents [6].
Proper nutrition during childhood and adolescence is fundamental to the development of physical, cognitive, and emotional well-being. During these critical growth stages, the body requires essential nutrients, including proteins, vitamins, minerals, and healthy fats, to support the rapid growth and development of tissues, organs, and the brain. Adequate nutrition also plays a pivotal role in strengthening the immune system, ensuring optimal energy levels, and fostering healthy bone development. Moreover, a balanced diet influences behavior, mood, and academic performance, ultimately shaping long-term health outcomes. Establishing healthy eating habits early in life can reduce the risk of developing chronic conditions such as obesity, diabetes, and cardiovascular diseases, while contributing to the formation of lifelong patterns of health and wellness. Therefore, prioritizing nutrition in childhood and adolescence is key to promoting a healthier, more prosperous future [7,8].
Balanced nutrition in children and adolescents is influenced by a variety of factors, including socioeconomic status, cultural practices, access to nutritious foods, and the influence of family and peers. Socioeconomic constraints often limit access to fresh, nutrient-dense foods, leading to a reliance on processed, calorie-dense options that are lower in essential nutrients. Cultural and familial dietary traditions also play a significant role in shaping eating habits, which may either promote or hinder balanced nutrition depending on the emphasis placed on nutrient-rich foods [9-12]. Additionally, the increasing prevalence of sedentary behaviors, such as excessive screen time, alongside a lack of physical activity, can contribute to poor dietary choices and unhealthy weight gain. The role of schools and community environments is also critical, as these institutions often serve as primary sources of nutrition education and meal options for adolescents. Thus, achieving balanced nutrition requires addressing these multifaceted influences through education, policy interventions, and improving access to healthy foods across different settings [13-15].
An unbalanced diet during childhood and adolescence can have significant medium- and long-term consequences on physical, cognitive, and emotional health. In the medium term, poor dietary habits can lead to issues such as nutrient deficiencies, which may impair growth, immune function, and cognitive development. Conditions such as anemia, poor bone health, and stunted growth are common among children with inadequate nutrition [16,17]. In the long term, the cumulative effects of an unbalanced diet can increase the risk of chronic health conditions, including obesity, type 2 diabetes, cardiovascular diseases, and certain types of cancer [18,19]. Moreover, poor nutrition during these critical developmental stages can negatively affect academic performance, behavior, and mental health, contributing to lower self-esteem and increased risk of mental health disorders like depression and anxiety [20-22]. These long-term health implications underscore the importance of promoting balanced nutrition early in life to mitigate future health risks and support optimal development and well-being.
Recent data indicates a significant increase in the prevalence of metabolic pathologies among children and adolescents globally and within Europe. According to a study published in The Lancet in March 2025, projections suggest that by 2050, over half of adults and nearly a third of children and adolescents worldwide will be overweight or obese, totaling more than 3.8 billion adults and 746 million youths. This study highlights a "monumental societal failure" to address the rising obesity rates, emphasizing the urgent need for effective public health interventions [23].
In the European context, the World Health Organization's European Childhood Obesity Surveillance Initiative (COSI) provides valuable insights. Data from the fifth round of COSI, conducted between 2018 and 2020 across 33 countries, revealed that approximately 25% of children aged 6–9 years were overweight or obese. Notably, countries such as Spain reported that in 2019, about 40.6% of children in this age group were overweight, with 17.3% classified as obese [24].
Looking ahead, the World Obesity Atlas 2023 projects that childhood obesity will more than double from 2020 levels by 2035, with a 100% increase in boys to 208 million and a 125% increase in girls to 175 million. These trends are particularly concerning given the associated health risks, including type 2 diabetes, cardiovascular diseases, and certain cancers [25].
These findings underscore the critical need for comprehensive public health strategies aimed at promoting healthy diets, increasing physical activity, and implementing policies that create supportive environments for children and adolescents. Addressing the root causes of these rising obesity rates is essential to mitigate future health risks and ensure the well-being of future generations.
Recent data on the prevalence of metabolic pathologies among children and adolescents in Romania is limited. A study conducted in Bucharest in 2015 involving 866 participants aged 6–18 years found a significant prevalence of obesity and unhealthy behaviors among Romanian youth. The age group of 6–10.9 years exhibited a higher prevalence (40.7%) of overweight compared to the 11–17.9 age group (26.6%). However, more recent national data is scarce, highlighting the need for updated research to accurately assess current trends and inform public health strategies [26].
Another Romanian study indicate a significant prevalence of overweight and obesity among children and adolescents, with variations based on measurement standards and age groups. A pooled analysis of studies conducted between 2006 and 2015 revealed that 34.7% of 8-year-old children were overweight, with 16.2% classified as obese [27].
Similarly, the World Health Organization's Childhood Obesity Surveillance Initiative (COSI) reported that between 2018 and 2020, 8-year-old children in Romania had an overweight prevalence of 25.2% and an obesity prevalence of 10%, based on WHO standards [28]. Gender differences are evident, with boys exhibiting higher rates of overweight and obesity compared to girls. Additionally, the incidence of obesity varies across different age groups, highlighting the need for targeted interventions. These findings underscore the urgency for comprehensive public health strategies in Romania to address the growing concerns of childhood and adolescent obesity. Such strategies should focus on promoting healthy eating habits, increasing physical activity, and implementing policies aimed at creating supportive environments for youth health.
Assessing the impact of behavioral and nutritional risk factors in children is essential for understanding their long-term health outcomes, particularly regarding the development of metabolic pathologies. Early identification of unhealthy eating habits, sedentary behaviors, and other risk factors enables timely interventions to prevent the onset of conditions such as obesity, type 2 diabetes, and cardiovascular diseases. Since childhood is a critical period for physical and metabolic development, the effects of poor nutrition and lifestyle choices can have lasting consequences, influencing not only immediate health but also the trajectory of health throughout adulthood. By evaluating these risk factors, healthcare professionals can better understand the complex relationship between diet, behavior, and disease onset, leading to more targeted and effective preventive strategies. Furthermore, such assessments provide valuable insights into the broader public health landscape, informing policies and interventions aimed at reducing the prevalence of metabolic disorders among future generations.
The aim of this study is to analyze the dietary habits, socio-demographic influences, and health-related behaviors of school-aged children and adolescents to identify key patterns and risk factors associated with unhealthy eating behaviors. By assessing the impact of gender, age, family structure, and psychological factors on food choices, this study seeks to provide evidence-based recommendations for targeted nutritional interventions and educational programs aimed at promoting healthier eating habits and preventing diet-related health issues among young populations.
Despite growing concerns regarding adolescent nutrition, limited studies comprehensively explore the interplay between socio-demographic characteristics, psychological well-being, and dietary patterns in school-aged children. Existing research often focuses on isolated dietary components rather than the holistic assessment of eating behaviors in relation to gender, age, and family environment. This study fills a critical gap by integrating these variables and providing a nuanced understanding of how socio-demographic factors shape adolescent food choices. The findings contribute to public health strategies by offering insights for the development of school-based nutrition programs, personalized dietary guidelines, and policies that foster healthier food environments for adolescents.
2. Materials and Methods
This cross-sectional study aimed to assess the dietary habits, health behaviors, and socio-demographic characteristics of school-aged children and adolescents. Data collection was conducted using a structured, self-administered questionnaire distributed across several educational institutions. The questionnaire was designed to gather comprehensive information on participants’ nutritional intake, meal patterns, psychological well-being, and lifestyle factors, including physical activity and screen time.
A total of 662 valid responses were collected from students aged between 6 and 18 years. Participants were stratified by gender, educational level (primary, middle, or high school), residence (urban or rural), family structure, and body mass index (BMI), which was calculated based on self-reported weight and height using standard WHO z-score classifications.
Study Design
This study employs a cross-sectional observational design to assess the dietary behaviors and nutritional preferences of school-aged children in relation to socio-demographic determinants. Data collection is conducted using validated dietary assessment questionnaires [29,30] and socio-economic surveys administered to both children and their parents. The study is conducted in multiple educational institutions across urban and rural areas to ensure a representative sample. Inclusion criteria: children attending school regularly. Exclusion criteria: children with diagnosed metabolic disorders affecting diet (e.g., diabetes, celiac disease). Incomplete responses to the survey instruments.
The questionnaire included both closed and multiple-choice items covering food frequency, type of meals consumed (e.g., home-cooked, fast food), hydration habits, and perceptions of health. Psychological well-being was assessed through items measuring fatigue, stress, mood fluctuations, and sleep quality. The tool was piloted for clarity and relevance prior to distribution. Validated Food Frequency Questionnaire (FFQ): used to assess the frequency and types of foods consumed. Dietary Diversity Score (DDS): calculated based on food group consumption to assess nutritional balance.
Statistical Analysis
Statistical analyses were conducted using SPSS software (version 30.0.0). Descriptive statistics were used to characterize the sample. Chi-square tests assessed associations between categorical variables. Multinomial logistic regression was applied to examine the influence of socio-demographic and behavioral factors on educational level and dietary outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated, with a significance level set at p < 0.05.
All data were collected anonymously, and participation was voluntary. Parental consent was obtained for participants under 18 years of age. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Commission of the Carol Davila University of Medicine and Pharmacy from Bucharest, no. 4201/16.02.2024.
3. Results
Following the dissemination of the questionnaire, 662 responses were collected (Table 1), with 59.52% of respondents being female adolescents and 40.48% male adolescents. The respondents were categorized based on various socio-demographic and anthropometric factors, including BMI, residence area, education level, family structure, weight-loss behaviors, and family history of excessive weight.
A significant association was observed between BMI and gender (χ² = 11.457, p = 0.009). Most respondents fell within the normal BMI range (66.61%), with minimal gender differences (66.75% females vs. 66.42% males). However, notable discrepancies were present in the underweight and overweight categories.
Educational level distribution was significantly associated with gender (χ² = 32.425, p < 0.001). A higher percentage of female adolescents were high school students (45.94%) compared to male adolescents (28.36%), whereas a greater proportion of male adolescents were in primary school (42.91%) compared to female adolescents (23.35%).
Weight-loss behaviors demonstrated a highly significant association with gender (χ² = 21.300, p < 0.001).
Family structure also showed significant gender differences (χ² = 13.727, p = 0.008). Male adolescents were more likely to be only children (35.82%) compared to female adolescents (25.63%), while female adolescents were more likely to have three siblings (5.08%) compared to males (1.12%). The family structure may play a role in shaping health behaviors, as children from larger families may have different social dynamics, dietary habits, and physical activity patterns compared to only children.
No significant gender differences were observed regarding the presence of excessive weight in the family (χ² = 2.947, p = 0.400). Most respondents reported no family history of excessive weight (73.57%), with slight variations between female adolescents (71.83%) and male adolescents (76.12%). This suggests that familial weight issues may not differ substantially between genders within this cohort.
3.1. The Influence of Sociodemographic Factors on Adolescent Nutritional Patterns
Table 2 presents the results of the multinomial logistic regression analysis, evaluating the association between educational level (high school and middle school vs. primary school) and socio-demographic factors, BMI, and dietary habits. Odds ratios (OR) and 95% confidence intervals (CI) are calculated to identify significant trends in adolescents' dietary behaviors. High school students who consume vegetables two or three times per week have significantly higher odds of being in high school compared to primary school students (OR = 1.603, p = 0.082), but this effect weakens in middle school students (OR = 1.290, p = 0.373). These findings suggest that higher vegetable consumption may correlate with higher educational attainment, though the relationship is not strongly defined. Adolescents who consume fast food less frequently (less than once a week) are more likely to be in high school. The odds ratio for those eating fast food 2–3 times a week is significantly lower in high school adolescents (OR = 0.121, p = 0.018). This suggests that reducing fast food consumption could have a positive association with academic outcomes, as adolescents in high school tend to have healthier eating habits regarding fast food.
3.2. Dietary Habits Among Adolescents
Figure 1 illustrates how the frequency of vegetable consumption correlates with the diversity of plant-based food categories consumed. The categories examined include grains and pseudo-grains (e.g., rice, corn, wheat, quinoa), various vegetables (e.g., broccoli, mush-rooms, zucchini), legumes (e.g., beans, lentils, soy), root vegetables (e.g., carrots, beets, potatoes), leafy greens (e.g., spinach, leeks, parsley), and a miscellaneous category labeled as other plant-based foods. The Chi-square test results (χ² = 55.07, p < 0.001) indicate a statistically significant association between the frequency of vegetable consumption and the diversity of plant-based products in respondents' diets.
Figure 2 presents the distribution of fruit categories consumed by respondents based on the frequency of their fruit consumption. The fruit categories analyzed include citrus fruits (e.g., oranges, lemons, grapefruits), berries (e.g., blueberries, strawberries, raspber-ries), exotic fruits (e.g., kiwi, bananas, pineapples), indigenous fruits (e.g., apples, pears, grapes), and nuts (e.g., walnuts, almonds, hazelnuts). The "Other" category encompasses less common fruits or unspecified types.
The Chi-square test reveals a statistically significant association between the fre-quency of fruit consumption and the diversity of fruit categories consumed (χ² = 51.08, p < 0.001). This suggests that individuals who consume fruits more frequently incorporate a broader variety of fruit types into their diet.
Figure 3 illustrates the distribution of various meat types consumed by respondents in relation to the frequency of their meat consumption. The analyzed meat categories include poultry (such as chicken, duck, and turkey), fish, pork, game meat, beef, lamb, and a miscellaneous category labeled as "Other."
The Chi-square test result (χ² = 48.77, p < 0.001) indicates a statistically significant association between the frequency of meat consumption and the types of meat incorporated into the diet. This suggests that individuals who consume meat more frequently tend to diversify their meat choices compared to those who consume it infrequently.
3.3. The Impact of Dietary Patterns and Lifestyle on Adolescent Well-Being
The analysis of dietary habits among adolescents, particularly as they transition from primary to middle and high school, reveals significant changes in food consumption pat-terns that can impact their health outcomes. The data presented in Table 3 highlights var-ious factors influencing dietary choices, including the type of food consumed, cooking methods, and the overall assessment of eating behaviors.
Adolescence is a stage characterized by psychological and behavioral shifts that in-fluence overall well-being. To explore how these factors shape health-related behaviors, a multinomial logistic regression analysis was performed. Table 4 displays the findings, highlighting the relationships between stress, fatigue, mental health symptoms, and life-style habits across different educational levels. For high school students, there is a significant negative association with daily exercise for less than an hour (OR = 0.231, p = 0.008), indicating they are less likely to engage in this level of physical activity compared to primary school students.
For middle school, there were no significant associations with physical activity levels across the different exercise categories compared to primary school.
This suggests that High school students might be more sedentary or engage in shorter periods of physical activity than Primary school students.
4. Discussion
Proper nutrition during childhood and adolescence plays an essential role in shaping long-term health outcomes, influencing growth, cognitive development, and the prevention of chronic diseases. However, modern dietary habits are increasingly shifting toward processed and nutrient-poor foods, driven by socio-economic factors, cultural influences, and food availability. Understanding the dietary patterns of school-aged children is essential for developing targeted interventions that promote balanced nutrition. This study explores the complex interplay between socio-demographic factors and dietary behaviors, aiming to identify key determinants that influence food choices among children. By addressing these factors, the research seeks to provide valuable insights for policymakers, educators, and healthcare professionals striving to enhance nutritional education and food accessibility in school environments.
Female adolescents were more likely to be underweight (18.27%) compared to male adolescents (10.82%), possibly reflecting societal pressures on girls to maintain a slimmer physique (Table 1). Conversely, overweight prevalence was higher among male adolescents (18.66%) than female adolescents (11.68%) [31].
Female adolescents reported engaging in weight-loss diets more frequently, with 8.38% indicating they do so very often and 26.65% sometimes, compared to only 3.73% and 15.30% of male adolescents, respectively. Male adolescents were more likely to report not engaging in weight-loss behaviors at all (69.40% vs. 53.55% for female adolescents). These findings are consistent with previous studies that highlight the prevalence of dieting behaviors among adolescent girls, often driven by body image concerns and societal expectations [32].
As it concerns dietary habits of adolescents one significant trend is the association between the frequency of vegetable consumption and educational level. High school students who rarely or never consume vegetables have a significantly increased risk of unhealthy dietary behaviors (OR = 0.418, p = 0.023) compared to primary school students (Table 2). Similarly, middle school students show a tendency toward reduced vegetable intake, though this is not statistically significant. This reduction may reflect the growing inde-pendence of older students and their increased exposure to less nutritious food options outside the home [33]. Studies have shown that adolescents often replace vegetables with energy-dense, nutrient-poor foods as they gain more autonomy over their dietary choices [34].
The consumption of carbonated or sweetened drinks also highlights critical differences. Both high school and middle school students show a substantially lower likelihood of frequent consumption compared to primary school students (OR = 0.185, p = 0.002 for high school; OR = 0.116, p < 0.001 for middle school). This suggests that younger students are more exposed to these sugary beverages, possibly due to parental influence or school policies that limit access to such drinks in older age groups. However, this trend may vary depending on socio-economic factors and regional dietary norms [35]. For example, adolescents in rural areas may have less access to sugary drinks due to limited availability, while urban adolescents may face greater exposure to marketing and convenience stores.
The analysis of meat consumption patterns (Table 2) reveals that middle school students who consume meat very rarely or not at all have a significantly increased risk of unhealthy dietary behaviors (OR = 6.578, p = 0.039). This could indicate a shift toward imbalanced diets lacking essential proteins and nutrients, possibly influenced by dietary fads, misinformation, or the adoption of plant-based diets without proper nutritional guidance [36]. The lack of meat in the diet may lead to deficiencies in iron, vitamin B12, and other essential nutrients, particularly if not replaced with adequate plant-based protein sources.
Interestingly, the frequency of fast food consumption did not show a strong association with unhealthy dietary habits among high school students but indicated a risk among middle school students. This aligns with findings from global studies on the impact of fast food marketing targeting younger demographics [37]. Middle school students may be more susceptible to fast food advertising and peer influence, leading to higher consumption rates. However, high school students may have greater awareness of the health risks associated with fast food or may have developed more stable dietary habits.
The frequency of water consumption also highlights a critical shift. Middle school students who consume 3 liters of water daily have a significantly higher likelihood of healthy dietary habits (OR = 7.146, p = 0.001), suggesting that hydration plays an essential role in overall health and dietary behavior (Table 2). This aligns with research indicating the importance of adequate hydration in maintaining cognitive and physical performance in adolescents [38]. Proper hydration is also associated with better appetite regulation and reduced consumption of sugary beverages.
The results indicate a significant association between the frequency of vegetable consumption and the diversity of plant-based products in respondents' diets (Figure 1). This suggests that individuals who consume vegetables more frequently tend to have a more varied and nutritionally balanced diet, incorporating a wider range of plant-based food categories. This finding is consistent with previous research indicating that higher vegetable intake is associated with improved diet quality and better health outcomes, particularly in adolescents [39]. Respondents who reported very rare or no vegetable consumption predominantly relied on grains and pseudo-grains, which constituted 27.71% of their intake, while their consumption of vegetables and leafy greens remained minimal at 7.72% and 9.81%, respectively. This dietary pattern suggests a preference for processed or grain-based foods, which may contribute to less balanced nutritional profiles. In contrast, participants consuming one or two categories of vegetables exhibited a more diverse plant-based intake, with higher proportions of root vegetables and general vegetables, indicating a transitional stage towards healthier eating patterns [40]. A notable dietary shift occurs among respondents consuming three or more vegetable categories. In these groups, vegetable intake significantly increases, with vegetables comprising 18.56% for those consuming three categories and 28.60% for those consuming more than three.
The analysis of fruit consumption patterns among respondents reveals significant in-sights into dietary diversity and health-related behaviors (Figure 2). Individuals who reported consuming fruits very rarely or not at all (24.10%) predominantly relied on items categorized as "Other" (40.40%). Their intake of indigenous fruits (8.84%) and citrus fruits (8.65%) was notably lower compared to those with higher fruit consumption. This pattern suggests a limited variety of fruits and possibly a higher reliance on processed or non-fresh fruit options, which may negatively impact their overall nutritional intake [41]. In the moderate fruit consumption category, participants consuming one (18.56%) or two (23.97%) types of fruits demonstrated an increased intake of diverse fruit categories. For instance, those consuming two types of fruits had higher proportions of berries (26.28%) and citrus fruits (18.86%). This indicates a transition towards more balanced fruit consumption patterns, which is essential for achieving recommended dietary guide-lines. A substantial shift is evident in respondents who consume three (18.61%) or more than three (19.51%) types of fruits. These groups showed a marked increase in the consumption of indigenous fruits (16.98% for three types; 15.58% for more than three) and nuts (18.61% for three types; 15.59% for more than three). Conversely, the proportion of "Other" fruits declined to 19.17% and 24.13%, indicating a stronger focus on nutrient-rich, commonly consumed fruits. This shift aligns with findings that suggest higher fruit and nut consumption is associated with improved overall diet quality and better health out-comes, including reduced risk of chronic diseases and enhanced immune function [42,43]. The data reveal that increased frequency of fruit consumption is associated with greater dietary diversity and a shift towards nutrient-rich fruit categories, such as berries, nuts, and indigenous fruits. This aligns with existing literature indicating that higher fruit consumption contributes to better overall diet quality and improved health outcomes, including reduced risk of chronic diseases and enhanced immune function [42,44]. The promotion of indigenous fruits and nuts is particularly noteworthy, as these foods are often rich in essential nutrients and can play a significant role in addressing dietary deficiencies in various populations [43,44]. Furthermore, the integration of indigenous foods into diets has been shown to enhance nutritional security and improve health outcomes, particularly in communities that traditionally rely on these foods [43].
Respondents who reported consuming meat very rarely or not at all predominantly fall into the "Other" category, with 88.56% likely indicating vegetarian or plant-based preferences (Figure 3). Only 7.40% of these individuals consume poultry, with negligible consumption of other meat types. This suggests a minimal reliance on meat, potentially driven by dietary restrictions, health considerations, or personal preferences. In Romania, the adoption of vegetarian or plant-based diets has been growing, particularly among younger populations, influenced by global health trends and environmental concerns [45]. However, without proper nutritional guidance, such diets may lead to deficiencies in essential nutrients like iron, vitamin B12, and protein [46].
In contrast, respondents who consume meat 2-3 times a month exhibit a broader variety of meat types. Poultry accounts for 18.57% of their consumption, while fish constitutes 15.44%. Pork represents 11.94%, indicating a gradual incorporation of diverse meats into their diet as consumption frequency increases.
A notable shift is observed among respondents who consume meat once a week or more frequently. Those who eat meat once a week show higher consumption of poultry (37.85%) and fish (15.44%), with a moderate intake of pork (6.83%). As meat consumption frequency increases to 2-3 times a week, pork becomes the dominant choice, representing 38.08% of meat intake, followed by poultry (12.97%) and beef (8.32%). This group also shows a notable increase in game meat consumption (13.58%), suggesting a preference for richer, more diverse meat options
Respondents who consume meat daily exhibit the greatest diversity in meat choices. Poultry remains significant at 20.16%, while beef (19.64%), pork (20.44%), and fish (6.37%) also feature prominently. Game meat and lamb are more frequently consumed by daily meat eaters, at 13.44% each, indicating a well-rounded, varied meat diet among this group. For example, red meats like beef and lamb are rich in iron and zinc, while poultry and fish provide lean protein and omega-3 fatty acids.
The data demonstrate a clear trend linking increased meat consumption frequency with greater diversity in meat types. Individuals who consume meat infrequently tend to rely predominantly on poultry or avoid meat altogether, whereas frequent meat consumers incorporate a wide variety of meat types, including pork, beef, fish, and game meat.
Primary school students generally exhibit healthier and more structured eating patterns compared to their older counterparts. This is likely due to the strong influence of parental supervision, school meal programs, and the absence of significant exposure to external food environments. In contrast, as children transition to middle and high school, their dietary habits tend to become less structured and more influenced by external factors such as peer pressure, academic stress, and increased independence.
One of the most notable trends is the shift toward chaotic and excessive eating among middle and high school students (Table 3). Compared to primary school students, both middle and high school students are significantly more likely to report chaotic eating patterns (OR = 2.291, p = 0.032 for middle school; OR = 2.225, p = 0.030 for high school). This aligns with global studies showing that adolescents often skip meals, snack irregularly, and consume energy-dense, nutrient-poor foods [47]. This trend is exacerbated by the increasing availability of fast food and the decline of traditional family meals, which are more common among primary school students [48].
Another key finding is the growing consumption of fast food and processed products among middle and high school students. While primary school students are more likely to consume home-cooked meals or meals provided by school canteens, older students show a tendency to-ward fast food consumption (OR = 3.712, p = 0.166 for middle school). This reflects a broader global trend where adolescents are increasingly exposed to fast-food outlets and marketing campaigns targeting their age group (Smith et al., 2020). Urbanization and the proliferation of fast-food chains have contributed to this shift, particularly in urban areas [49].
The role of family meals also diminishes as children grow older. Both middle and high school students are less likely to eat meals with their families compared to primary school students (OR = 0.587, p = 0.029 for middle school; OR = 0.438, p < 0.001 for high school). Family meals are a cornerstone of healthy eating habits, providing an opportunity for parents to model balanced diets and monitor their children’s food intake. The decline in family meals among older students may contribute to the adoption of less healthy eating behaviors, such as increased consumption of snacks and fast food [50].
Receptivity to new foods also decreases as children transition from primary school to adolescence. Both middle and high school students are less likely to try new foods compared to primary school students (OR = 0.370, p < 0.001 for middle school; OR = 0.200, p < 0.001 for high school). This may reflect a natural tendency toward food neophobia during adolescence, as well as the influence of peer preferences and the desire to conform to social norms.
The shift from structured, family-centered eating patterns in primary school to chaotic, fast-food-oriented diets in middle and high school has significant implications for adolescent health. Chaotic eating and excessive consumption of fast food are associated with an increased risk of obesity, cardiovascular diseases, and other chronic conditions [51]. Additionally, the decline in family meals and reduced receptivity to new foods may limit adolescents’ exposure to essential nutrients, further compromising their long-term health.
Recent studies have highlighted the need for targeted interventions to promote healthy eating habits among adolescents [45], including strengthening nutritional education, regulating the availability of unhealthy foods in schools, and encouraging family meals.
Based on the multinomial logistic regression analysis of dietary patterns and eating behaviors associated with educational level (high school and middle school vs. primary school), the findings reveal several important insights that reflect the complex relationship between educational level and food consumption behaviors. High school students are significantly less likely to consume home-cooked meals compared to primary school students, which may reflect a trend towards increased reliance on fast foods and restaurant-cooked meals as students grow older. This shift could be driven by factors such as greater autonomy, changing lifestyles, and a shift towards convenience foods as adolescents navigate academic and social demands. The consumption of oven-cooked foods is notably lower among middle school students compared to primary school students, suggesting a potential trend toward less healthy cooking methods. Although the difference is not marked in all cooking methods, these findings may point to broader shifts in food preparation styles as children grow older and have greater exposure to processed and fast foods. There is no significant difference between high school and middle school students for many food types, including vegetables, cereals, pasta, and fish, but high school students tend to be less receptive to new foods compared to their primary school counterparts. This reluctance towards trying new foods may be linked to established preferences and a resistance to unfamiliar tastes or textures, which could have implications for their long-term health outcomes. Despite the lack of significant differences for some categories, fast food products (such as burgers, shawarma, and fries) show a tendency to be consumed more frequently among high school students. This highlights the growing influence of the fast food industry and peer influence in adolescence, contributing to less healthy dietary habits. Both high school and middle school students are more likely to report chaotic, excessive eating patterns compared to primary school students. This finding emphasizes the importance of addressing disordered eating behaviors early on, particularly as children transition into adolescence. Hormonal changes specific to adolescence significantly influence eating behaviors through complex mechanisms, in which leptin and ghrelin regulate hunger and satiety, insulin influences carbohydrate metabolism, and cortisol, the stress hormone, can stimulate appetite for foods rich in sugar and fat; at the same time, fluctuations in estrogen and progesterone at adolescent girls, as well as increased testosterone levels at adolescent boys, can determine specific food preferences and changes in energy metabolism, being also influenced by circadian rhythm and sleep quality. Excessive eating habits at these stages can contribute to weight gain and poor nutritional health in the long run.
Interestingly, middle school students are more likely than primary school students to monitor their weight, suggesting an increased awareness of body image and health at a younger age. This could reflect growing societal pressures related to appearance and health that influence dietary choices. School stress and anxiety profoundly influence adolescents' eating behaviors, as elevated cortisol levels can stimulate appetite for high-calorie, sugary foods, while academic pressure, heavy homework, and exams can promote either compulsive eating as a stress management mechanism or food restriction due to decreased appetite or excessive weight concerns, with these effects exacerbated by lack of sleep and an unbalanced daily routine.
Social media and peer influence play a key role in shaping adolescents' eating behaviors, with the promotion of unrealistic body standards and extreme diets by influencers and celebrities contributing to the adoption of unhealthy eating habits, increased body image concerns, and, in some cases, the development of eating disorders, such as anorexia or bulimia, especially in the context of constant exposure to idealized content.
However, the relationship between weight monitoring and actual healthy eating behaviors remains complex and warrants further exploration. High school students tend to eat less frequently with family compared to primary school students. This trend suggests a shift towards more independent meal habits as adolescents seek autonomy in their dietary choices. The reduced family involvement during meals may have implications for social and emotional eating habits, potentially leading to unhealthy eating behaviors if not addressed. The family is a determining factor in the development of adolescents' eating habits, with regular family meals, a balanced parenting style and emotional support contributing to the formation of healthy eating behavior, while lack of parental involvement or a tense family environment can favor chaotic eating or excessive consumption of unhealthy foods, and well-structured educational interventions in schools can play an essential role in preventing unbalanced eating behaviors by promoting a balanced diet and stress management strategies.
Both high school and middle school students exhibit significant resistance to accepting new foods, with high school students being especially reluctant. This could be attributed to the development of more ingrained food preferences and a desire for comfort and familiarity, which may hinder the adoption of healthier food choices. The findings regarding eating pace and multitasking during meals show that while high school students are not significantly different from middle school students in terms of eating speed or doing other activities while eating, these behaviors are common across age groups. Such habits may contribute to overeating or poor digestion, signaling a need for more mindful eating interventions in school settings.
Fatigue is a significant issue among middle and high school students, with both groups reporting higher levels compared to primary school students (Table 4). High school students are particularly affected, with those experiencing frequent fatigue showing a significantly higher risk of unhealthy behaviors (OR = 2.330, p = 0.013). Alarmingly, students who are almost always fatigued exhibit an extremely high risk (OR = 14.592, p < 0.001). This aligns with recent research indicating that academic pressure, poor sleep hygiene, and increased screen time contribute to chronic fatigue among adolescents (Owens et al., 2020). Similarly, stress levels escalate as student advance through the educational sys-tem. High school students frequently report stress (OR = 2.574, p = 0.011), which can be attributed to academic demands, social pressures, and the transition to adulthood. This trend is consistent with findings from the World Health Organization, which highlights stress as a critical issue affecting adolescent mental health [52].
Conflictual relationships with peers become more prevalent in older students. High school students who report conflicts with peers have a significantly higher risk of adverse health outcomes (OR = 2.752, p = 0.025), with middle school students showing an even higher risk (OR = 3.428, p = 0.006). These findings suggest that peer relationships play a pivotal role in adolescents' psychological well-being. Peer conflicts are strongly associated with anxiety, depression, and poor academic performance, as supported by recent studies [53]. Mental health concerns, particularly depressive states, also show a marked increase in high school students. Those frequently experiencing depressive symptoms have a significantly reduced likelihood of maintaining healthy behaviors (OR = 0.121, p = 0.005), and those almost always in depressive states exhibit similar risks (OR = 0.160, p = 0.045). This trend highlights the urgent need for mental health interventions in schools, echoing global calls for increased mental health resources for adolescents [54].
Fatigue and irritability are closely linked, with high school students showing higher prevalence rates. Frequent fatigue (OR = 2.330, p = 0.013) and irritability contribute to un-healthy lifestyle choices, as adolescents may resort to comfort foods, skip meals, or engage in irregular eating patterns. This is supported by literature linking psychological stress and fatigue to disordered eating behaviors in adolescents [55]. Interestingly, immune system perceptions also differ across educational levels. High school students who believe they have a weakened immune system are nearly twice as likely to report unhealthy behaviors (OR = 1.999, p = 0.092).
Physical activity levels decline as student progress through school, with high school students who engage in daily physical activity for less than an hour showing a signifi-cantly higher likelihood of healthy behaviors (OR = 0.231, p = 0.008). This highlights the importance of regular physical activity in promoting overall health. Conversely, excessive screen time is associated with unhealthy behaviors. Students who spend less time in front of screens are more likely to maintain healthy dietary habits (OR = 0.195, p = 0.001 for middle school; OR = 0.245, p = 0.004 for high school). This aligns with studies linking ex-cessive screen time to sedentary behavior and poor dietary choices [56].
For both high school and middle school students, there is a negative association with the amount of time spent in front of screens compared to primary school students (Tale 4). Specifically:
- high school and middle school students are less likely to spend more than 1 hour, 2-3 hours, or 4-5 hours daily in front of screens than primary school students;
- in both groups, students who spend a few hours 2-3 times a week in front of screens also show a significant negative association, indicating they are less likely to engage in this behavior compared to primary school students.
These findings suggest that primary school students tend to spend more time in front of screens across various categories compared to high school and middle school students.
The multinomial logistic regression analysis underscores that sociodemographic factors such as residence area and dietary habits, particularly related to the consumption of vegetables, fruits, sweetened drinks, fast food, and water, significantly influence the educational attainment of adolescents. Rural adolescents tend to be overrepresented in middle school, while dietary habits, such as regular vegetable consumption, reduced intake of fast food, and increased water consumption, are associated with higher odds of being in higher educational levels (high school). These findings suggest the need for interventions that promote healthier eating habits, particularly focusing on improving the availability and consumption of nutritious foods and beverages to enhance the educational outcomes of adolescents. The results indicate also a significant evolution in dietary behaviors and eating patterns as student transition from primary school to middle and high school. While there are some commonalities, such as a tendency toward chaotic eating and reluctance to try new foods, there are also critical shifts, such as decreased consumption of home-cooked meals and increased consumption of fast food, particularly in high school students. These changes highlight the need for targeted interventions to promote healthy eating habits, mindful consumption, and family engagement in meal times during adolescence, a critical period for establishing long-term health behaviors. Moreover, the resistance to new foods and chaotic eating patterns suggest that educational programs focusing on healthy eating, cooking skills, and family meal practices could be important in mitigating the rise in unhealthy dietary trends among adolescents.
Limitations of the Study
This study has several limitations that should be considered when interpreting the findings. First, the reliance on self-reported dietary data may introduce recall bias and social desirability bias, potentially affecting the accuracy of responses. Second, the cross-sectional design of the study limits the ability to establish causal relationships between socio-demographic factors and dietary behaviors. Longitudinal studies would be necessary to examine changes in eating habits over time and their long-term health implications.
Additionally, while the study considers key socio-demographic and psychological variables, other potential influences such as cultural differences, economic constraints, and peer influence on dietary choices are not fully explored. The sample may also not be entirely representative of all school-aged children, particularly those from rural or marginalized communities with different food access conditions. Lastly, the study does not account for biochemical markers of nutritional status, which could provide more objective insights into the impact of dietary patterns on health outcomes. Future research should address these limitations by incorporating more diverse populations, longitudinal approaches, and biochemical assessments to strengthen the validity and applicability of the findings.
5. Conclusions
This study highlights the significant influence of socio-demographic factors on the dietary behaviors of school-aged children, emphasizing the need for targeted nutritional interventions to promote healthier eating habits. The findings suggest that parental education, economic status, and urban versus rural living environments play crucial roles in shaping children's food choices and nutritional intake. Understanding these determinants is essential for developing effective policies and educational programs that encourage balanced diets and long-term health benefits.
Moreover, the study underscores the importance of integrating tailored nutritional guidance into school curricula and public health initiatives, ensuring that children from diverse backgrounds have access to appropriate dietary resources. While acknowledging its limitations, this research provides a foundation for future longitudinal studies and interventions aimed at bridging nutritional gaps and mitigating diet-related health risks in young populations.
Author Contributions
Conceptualization, C.E.L., A.S.U., S.R.M. and M.M.; methodology, C.E.L., A.S.U., S.R.M. and M.M.; software, G.S., F.H., A.M. and S.L.; validation, M.L., T.I.S. and M.M.; formal analysis, G.S., F.H., A.M. and S.L.; investigation, R.E., R.E.C., S.C.B., O.B. and A.C.; resources, O.B. and A.C.; data curation, R.E.C.; writing—original draft preparation, M.L., T.I.S. and M.M.; writing—review and editing, M.L., T.I.S. and M.M.; visualization, S.C.B.; supervision, R.E.; project administration, C.E.L., A.S.U., S.R.M. and M.M.; funding acquisition, R.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Commission of the Carol Davila University of Medicine and Pharmacy from Bucharest, no. 4201/16.02.2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Acknowledgments
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grajek, M.; Krupa-Kotara, K.; Białek-Dratwa, A.; Sobczyk, K.; Grot, M.; Kowalski, O.; Staśkiewicz, W. Nutrition and mental health: A review of current knowledge about the impact of diet on mental health. Front Nutr. 2022; 9:943998. [CrossRef]
- Lange, K.W. Omega-3 fatty acids and mental health, Global Health Journal, 2020, 4(1):18-30. [CrossRef]
- Pop, A.L.; Henteș, P.; Pali, M.-A.; Oșanu, L.; Ciobanu, A.; Nasui, B.A.; Mititelu, M.; Crișan, S.; Peneș, O.N. Study regarding a new extended-release calcium ascorbate and hesperidin solid oral formulation. Farmacia, 2022, 70(1):151-157. [CrossRef]
- Zhang, L.; Sun, H.; Liu, Z.; Yang, J.; Liu, Y. Association between dietary sugar intake and depression in US adults: a cross-sectional study using data from the National Health and Nutrition Examination Survey 2011-2018. BMC Psychiatry. 2024; 24(1):110. [CrossRef]
- Chen, H.; Cao, Z.; Hou, Y.; Wang, X.; Xu, C. The associations of dietary patterns with depressive and anxiety symptoms: a prospective study. BMC Med 2023, 21, 307. [CrossRef]
- Xu, Q.; Hu, Z.; Zeng, M.; Su, Y.; Jiang, K.; Li, S.; Li, Z.; Fu, L.; Shi, Z.; Sharma, M.; et al. Relationships among Sleep Time, Physical Activity Time, Screen Time, and Nutrition Literacy of Adolescents: A Cross-Sectional Study in Chongqing, China. Nutrients 2024, 16, 1314. [CrossRef]
- Saavedra, J.M.; Prentice, A.M. Nutrition in school-age children: a rationale for revisiting priorities. Nutr Rev. 2023; 81(7):823-843. [CrossRef]
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the "First 1000 Days". J Pediatr. 2016; 175:16-21. [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [CrossRef]
- Gyawali, B.; Mkoma, G.F.; Harsch, S. Social Determinants Influencing Nutrition Behaviors and Cardiometabolic Health in Indigenous Populations: A Scoping Review of the Literature. Nutrients 2024, 16, 2750. [CrossRef]
- Mititelu, M.; Udeanu, D.I.; Docea, A.O.; Tsatsakis, A.; Calina, D.; Arsene, A.L.; Nedelescu, M.; Neacsu, S.M.; Velescu, B.S.; Ghica, M. New method for risk assessment in environmental health: The paradigm of heavy metals in honey, Environmental Research, 2023, 236 part 1, 115194. [CrossRef]
- Ioniță-Mîndrican, C.-B.; Mititelu, M.; Musuc, A.M.; Oprea, E.; Ziani, K.; Neacșu, S.M.; Grigore, N.D.; Negrei, C.; Dumitrescu, D.-E.; Mireșan, H.; Roncea, F.N.; Ozon, E.A.; Măru, N.; Drăgănescu, D.; Ghica, M. Honey and Other Beekeeping Products Intake among the Romanian Population and Their Therapeutic Use. Appl. Sci. 2022, 12, 9649. [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu Rev Clin Psychol. 2020; 16:351-378. [CrossRef]
- Haghjoo, P.; Siri, G.; Soleimani, E.; Farhangi, M.A.; Alesaeidi, S. Screen time increases overweight and obesity risk among adolescents: a systematic review and dose-response meta-analysis. BMC Prim. Care 2022, 23, 161. [CrossRef]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Richard Larouche, Rachel C Colley, Gary Goldfield & Sarah Connor Gorber. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act 2011, 8, 98. [CrossRef]
- Abdoli, M.; Scotto Rosato, M.; Cipriano, A.; Napolano, R.; Cotrufo, P.; Barberis, N.; Cella, S. Affect, Body, and Eating Habits in Children: A Systematic Review. Nutrients 2023, 15, 3343. [CrossRef]
- Morales, F.; Montserrat-de la Paz, S.; Leon, M.J.; Rivero-Pino, F. Effects of Malnutrition on the Immune System and Infection and the Role of Nutritional Strategies Regarding Improvements in Children’s Health Status: A Literature Review. Nutrients 2024, 16, 1. [CrossRef]
- Al-Jawaldeh, A.; Abbass, M.M.S. Unhealthy Dietary Habits and Obesity: The Major Risk Factors Beyond Non-Communicable Diseases in the Eastern Mediterranean Region. Front Nutr. 2022; 9:817808. [CrossRef]
- Fruh, S.M. Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J Am Assoc Nurse Pract. 2017; 29(S1):S3-S14. [CrossRef]
- O'Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship between diet and mental health in children and adolescents: a systematic review. Am J Public Health. 2014 Oct;104(10):e31-42. [CrossRef]
- Muscaritoli, M. The Impact of Nutrients on Mental Health and Well-Being: Insights From the Literature. Front Nutr. 2021; 8:656290. [CrossRef]
- Colizzi, M.; Lasalvia, A.; Ruggeri, M. Prevention and early intervention in youth mental health: is it time for a multidisciplinary and trans-diagnostic model for care? Int J Ment Health Syst 2020, 14, 23. [CrossRef]
- https://www.healthdata.org/news-events/newsroom/news-releases/lancet-more-half-adults-and-third-children-and-adolescents (accessed on 22 February 2025).
- https://www.who.int/europe/news-room/03-03-2023-childhood-obesity--five-facts-about-the-who-european-region (accessed on 22 February 2025).
- https://www.cieh.org/ehn/public-health-and-protection/2023/march/childhood-obesity-set-to-more-than-double-from-2020-levels/ (accessed on 22 February 2025).
- Barbu, C.G.; Teleman, M.D.; Albu, A.I.; Sirbu, A.E.; Martin, S.C.; Bancescu, A.; Fica, S.V. Obesity and eating behaviors in school children and adolescents –data from a cross sectional study from Bucharest, Romania. BMC Public Health 2015, 15, 206. [CrossRef]
- Chirita-Emandi, A.; Barbu, C.G.; Cinteza, E.E.; Chesaru, B.I.; Gafencu, M.; Mocanu, V.; Pascanu, I.M.; Tatar, S.A.; Balgradean, M.; Dobre, M.; Fica, S.V.; Ichim, G.E.; Pop, R.; Puiu, M. Overweight and Underweight Prevalence Trends in Children from Romania - Pooled Analysis of Cross-Sectional Studies between 2006 and 2015. Obes Facts. 2016; 9(3):206-20. [CrossRef]
- https://data.worldobesity.org/country/romania (accessed on 22 February 2025).
- Mititelu, M.; Oancea, C.-N.; Neacșu, S.M.; Musuc, A.M.; Gheonea, T.C.; Stanciu, T.I.; Rogoveanu, I.; Hashemi, F.; Stanciu, G.; Ioniță-Mîndrican, C.-B.; Belu, I.; Măru, N.; Olteanu, G.; Cîrțu, A.-T.; Stoicescu, I.; Lupu, C.E. Evaluation of Junk Food Consumption and the Risk Related to Consumer Health among the Romanian Population. Nutrients 2023, 15, 3591. [CrossRef]
- Mititelu, M.; Oancea, C.-N.; Neacșu, S.M.; Olteanu, G.; Cîrțu, A.-T.; Hîncu, L.; Gheonea, T.C.; Stanciu, T.I.; Rogoveanu, I.; Hashemi, F.; Stanciu, G.; Ionită-Mîndrican, C.-B.; Caunii, A.; Măru, N.; Lupu, S.; Lupu, C.E. Evaluation of Non-Alcoholic Beverages and the Risk Related to Consumer Health among the Romanian Population. Nutrients 2023, 15, 3841. [CrossRef]
- Yoon, C.; Mason, S.M.; Hooper, L.; Eisenberg, M.E.; Neumark-Sztainer, D. Disordered Eating Behaviors and 15-year Trajectories in Body Mass Index: Findings From Project Eating and Activity in Teens and Young Adults (EAT). J. Adolesc. Health 2020, 66, 181-188. [CrossRef]
- Zamfir, A.-M.; Aldea, A.B.; Molea, R.-M. Stratification and Inequality in the Secondary Education System in Romania. Systems 2024, 12, 15. [CrossRef]
- Costa, A.; Oliveira, A. Parental Feeding Practices and Children’s Eating Behaviours: An Overview of Their Complex Relationship. Healthcare 2023, 11, 400. https://doi.org/10.3390/healthcare11030400 (2021). The influence of parental practices on children’s vegetable consumption: A systematic review. Appetite, 157, 104987. [CrossRef]
- Sinai, T.; Axelrod, R.; Shimony, T.; Boaz, M.; Kaufman-Shriqui, V. Dietary Patterns among Adolescents Are Associated with Growth, Socioeconomic Features, and Health-Related Behaviors. Foods 2021, 10, 3054. [CrossRef]
- Bleich, S.N.; Vercammen, K.A.; Koma, J.W.; Li, Z. Trends in Beverage Consumption among Children and Adults, 2003–2014. Obesity 2018, 26(2), 432-441. [CrossRef]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2022, 14, 29. [CrossRef]
- Smith, R.; Kelly, B.; Yeatman, H.; Boyland, E. Food Marketing Influences Children’s Attitudes, Preferences and Consumption: A Systematic Critical Review. Nutrients 2019, 11, 875. [CrossRef]
- Perrier, E.T.; Armstrong, L.E.; Bottin, J.H.; Clark, W.F.; Dolci, A.; Guelinckx, I.; Iroz, A.; Kavouras, S.A.; Lang, F.; Lieberman, H.R.; Melander, O.; Morin, C.; Seksek, I.; Stookey, J.D.; Tack, I.; Vanhaecke, T.; Vecchio, M.; Péronnet, F. Hydration for health hypothesis: A narrative review of supporting evidence. Eur. J. Nutr. 2021, 60, 1167–1180. [CrossRef]
- Outzen, M.; Thorsen, A.-V.; Davydova, A.; Thyregod, C.; Christensen, T.; Grønborg, I.; Trolle, E.; Sabinsky, M.; Ravn-Haren, G. Effect of School-Based Educational Intervention on Promoting Healthy Dietary Habits in Danish Schoolchildren: The FOODcamp Case Study. Nutrients 2023, 15, 2735. [CrossRef]
- Oja, L.; Slapšinskaitė, A.; Piksööt, J.; Šmigelskas, K. Baltic Adolescents’ Health Behaviour: An International Comparison. Int. J. Environ. Res. Public Health 2020, 17, 8609. [CrossRef]
- Alkazemi, D.; Salmean, Y. Fruit and Vegetable Intake and Barriers to Their Consumption Among University Students in Kuwait: A Cross-Sectional Survey. J. Environ. Public Health 2021, 2021, 9920270. [CrossRef]
- Gervasi, T.; Barreca, D.; Laganà, G.; Mandalari, G. Health Benefits Related to Tree Nut Consumption and Their Bio-Active Compounds. Int. J. Mol. Sci. 2021, 22, 5960. [CrossRef]
- Ghosh-Jerath, S.; Kapoor, R.; Bandhu, A.; Singh, A.; Downs, S.; Fanzo, J. Indigenous Foods to Address Malnutrition: An Inquiry into the Diets and Nutritional Status of Women in the Indigenous Community of Munda Tribes of Jharkhand, India. Curr. Dev. Nutr. 2022, 6, nzac102. [CrossRef]
- Osunu, P.; Nwose, E. Advancing Indigenous Fruits Consumption to Promote Self-Management in Ill-Health: A Critical Narrative Review. Int. J. Basic Clin. Pharmacol. 2021, 10, 738. [CrossRef]
- Mititelu, M.; Stanciu, G.; Licu, M.; Neacșu, S.M.; Călin, M.F.; Roșca, A.C.; Stanciu, T.I.; Busnatu, Ș.S.; Olteanu, G.; Boroghină, S.C.; et al. Evaluation of the Consumption of Junk Food Products and Lifestyle among Teenagers and Young Population from Romania. Nutrients 2024, 16, 1769. [CrossRef]
- Johnson, S.S.; Paiva, A.L.; Cummins, C.O.; Johnson, J.L.; Dyment, S.J.; Wright, J.A.; Prochaska, J.O.; Prochaska, J.M. Transtheoretical model-based multiple behavior intervention for weight management: Effectiveness on a population basis. Prev. Med. 2008, 46, 238–246. [CrossRef]
- Bîlbîie, A.; Druică, E.; Dumitrescu, R.; Aducovschi, D.; Sakizlian, R.; Sakizlian, M. Determinants of Fast-Food Consumption in Romania: An Application of the Theory of Planned Behavior. Foods 2021, 10, 1877. [CrossRef]
- Smith, K.J.; Gall, S.L.; McNaughton, S.A.; Blizzard, L.; Dwyer, T.; Venn, A.J. Skipping breakfast: Longi-tudinal associations with cardiometabolic risk factors in the Childhood Determinants of Adult Health Study. Am. J. Clin. Nutr. 2010, 92, 1316–1325. [CrossRef]
- Dunn, R.A.; Nayga, R.M.; Thomsen, M.R.; Rouse, H.L. A Longitudinal Analysis of Fast-Food Exposure on Child Weight Outcomes: Identifying Causality through School Transitions. Q Open 2021, 1, qoaa007. [CrossRef]
- Hammons, A.J.; Fiese, B.H. Is frequency of shared family meals related to the nutritional health of children and adolescents? A meta-analysis. Pediatrics 2011, 127, e1565–e1574. [CrossRef]
- Wang, Y.; Wang, L.; Xue, H.; Qu, W. A Review of the Growth of the Fast Food Industry in China and Its Potential Impact on Obesity. Int. J. Environ. Res. Public Health 2016, 13, 1112. [CrossRef]
- World Health Organization (WHO). Adolescent Mental Health. WHO Fact Sheets 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescent-mental-health (accessed at 14 February 2024).
- Rueger, S.Y.; Malecki, C.K.; Pyun, Y.; Aycock, C.; Coyle, S. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol. Bull. 2016, 142, 1017–1067. [CrossRef]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: evidence for action. Lancet 2011, 378, 1515–1525. [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Larson, N.I.; Eisenberg, M.E.; Loth, K. Dieting and Disordered Eating Behaviors from Adolescence to Young Adulthood: Findings from a 10-Year Longitudinal Study. J. Am. Diet. Assoc. 2018, 111, 1004–1011. [CrossRef]
- Twenge, J.M.; Campbell, W.K. Associations between screen time and lower psychological well-being among children and adolescents: Evidence from a population-based study. Prev. Med. Rep. 2018, 12, 271–283. [CrossRef]
Figure 1.
Distribution of plant-based food categories by frequency of vegetable consumption among respondents (χ2 = 55.07, p < 0.001).
Figure 1.
Distribution of plant-based food categories by frequency of vegetable consumption among respondents (χ2 = 55.07, p < 0.001).
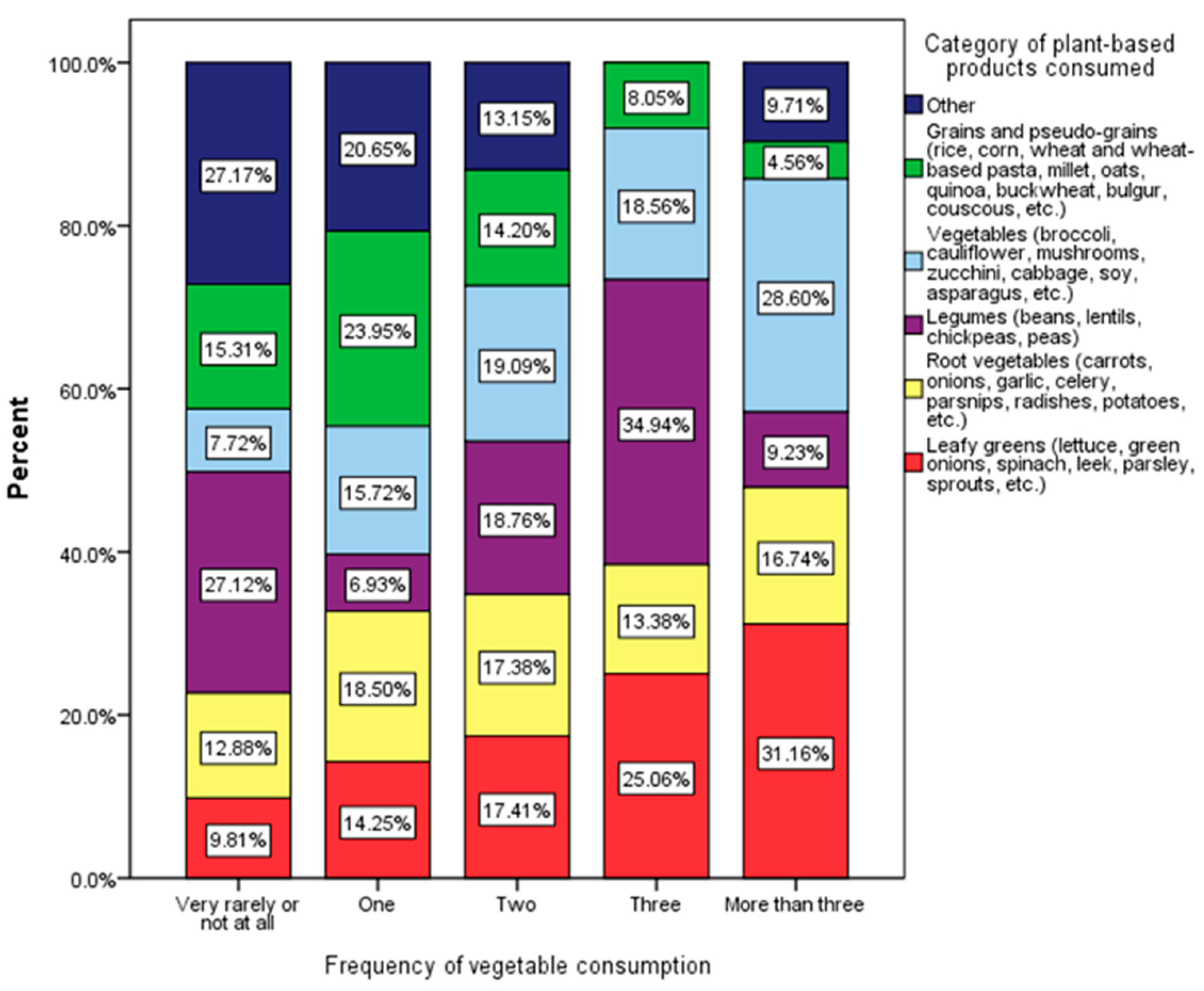
Figure 2.
Distribution of fruit categories by frequency of fruit consumption among respondents (χ2 = 51.08, p < 0.001).
Figure 2.
Distribution of fruit categories by frequency of fruit consumption among respondents (χ2 = 51.08, p < 0.001).
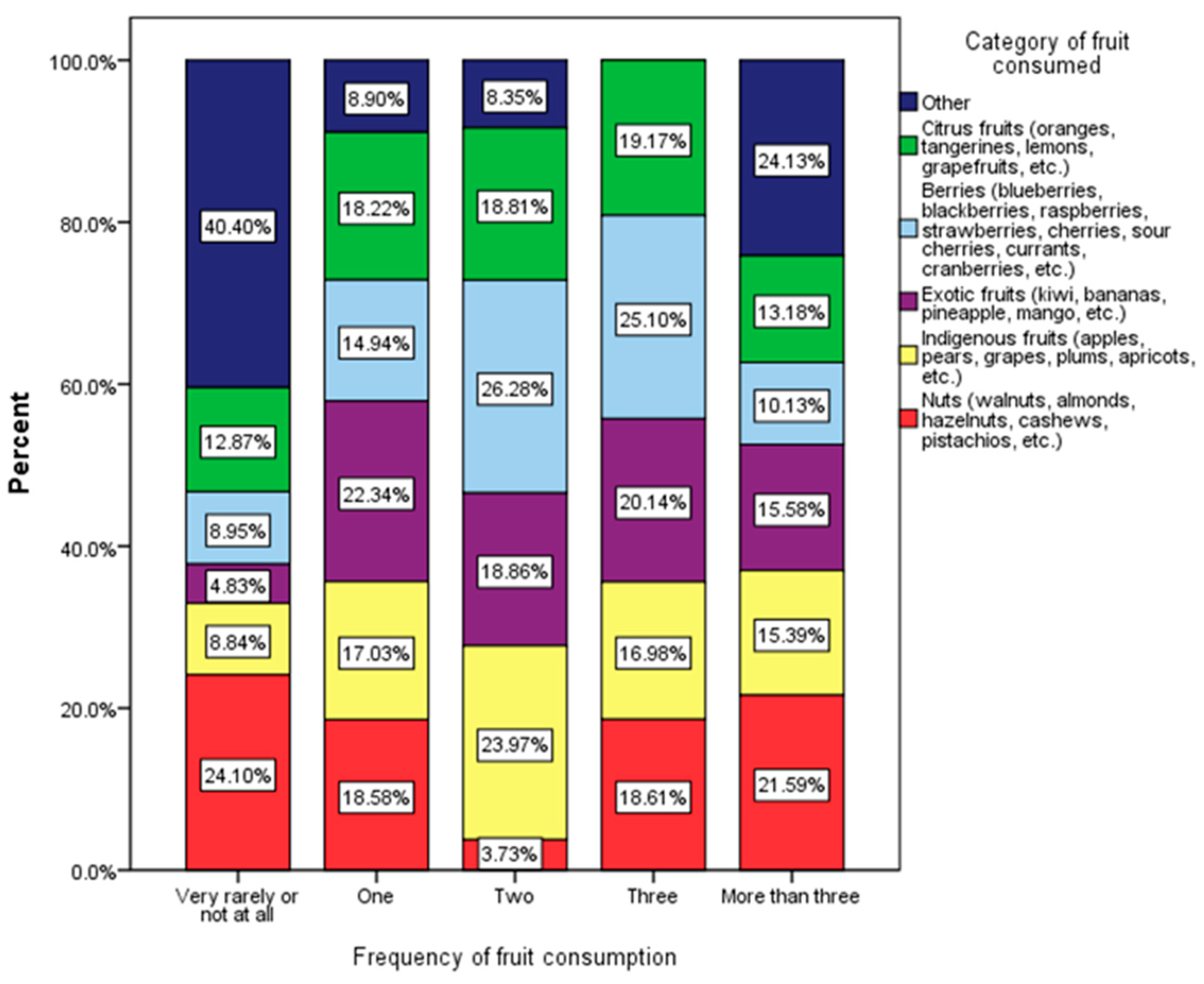
Figure 3.
Distribution of meat types by frequency of meat consumption among respondents (χ2 = 48.77, p < 0.001).
Figure 3.
Distribution of meat types by frequency of meat consumption among respondents (χ2 = 48.77, p < 0.001).
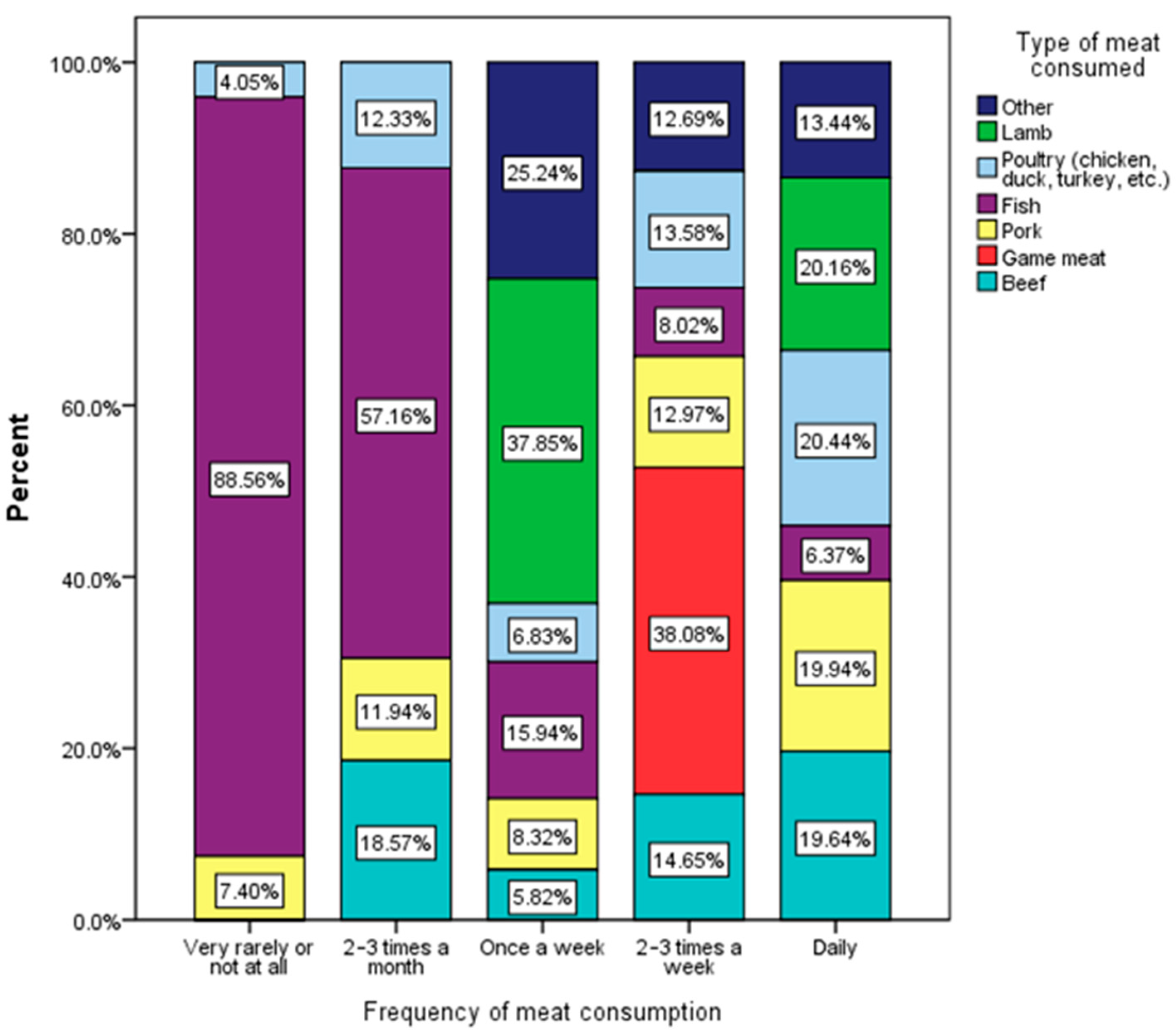

Table 1.
Socio-demographic and anthropometric characteristics of the respondents with z-scores.
| Total Population | Female adolescents (A) |
Male adolescents (B) |
||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| 662 | 100 | 394 | 59.52 | 268 | 48.48 | |
| Body Mass index (BMI) (χ2 = 11.457, p = 0.009) | ||||||
| Normal | 441 | 66.61 | 263 | 66.75 | 178 | 66.42 |
| Obese | 24 | 3.63 | 13 | 3.30 | 11 | 4.10 |
| Overweight | 96 | 14.50 | 46 | 11.68 | 50 | 18.66A |
| Underweight | 101 | 15.26 | 72 | 18.27B | 29 | 10.82 |
| Residence area (χ2 = 0.006, p = 0.937) | ||||||
| Urban area | 441 | 66.62 | 262 | 66.50 | 179 | 66.79 |
| Rural area | 221 | 33.38 | 132 | 33.50 | 89 | 33.21 |
| Level of education (χ2 = 32.425, p < 0.001) | ||||||
| High school | 257 | 38.82 | 181 | 45.94B | 76 | 28.36 |
| Middle school | 198 | 29.91 | 121 | 30.71 | 77 | 28.73 |
| General/primary school | 207 | 31.27 | 92 | 23.35 | 115 | 42.91A |
| Siblings (χ2 = 13.727, p = 0.008) | ||||||
| Only child | 197 | 29.76 | 101 | 25.63 | 96 | 35.82A |
| One sibling | 355 | 53.63 | 219 | 55.58 | 136 | 50.75 |
| Two siblings | 67 | 10.12 | 42 | 10.66 | 25 | 9.33 |
| Three siblings | 23 | 3.47 | 20 | 5.08A | 3 | 1.12 |
| More than three siblings | 20 | 3.02 | 12 | 3.00 | 8 | 3.00 |
| Weight-loss diet (χ2 = 21.300, p < 0.001) | ||||||
| Yes, very often | 43 | 6.5 | 33 | 8.38 | 10 | 3.73 |
| Yes, sometimes | 146 | 22.05 | 105 | 26.65B | 41 | 15.30 |
| Very rarely | 76 | 11.48 | 45 | 11.42 | 31 | 11.57 |
| Not at all | 397 | 59.97 | 211 | 53.55 | 186 | 69.40A |
| Excessive weight in family (χ2 = 2.947, p = 0.400) | ||||||
| Yes, both parents | 44 | 6.64 | 28 | 7.11 | 16 | 5.97 |
| Yes, one parent | 122 | 18.43 | 79 | 20.05 | 43 | 16.04 |
| Yes, the whole family | 9 | 1.36 | 4 | 1.02 | 5 | 1.87 |
| Not at all | 487 | 73.57 | 283 | 71.83 | 204 | 76.12 |
The Chi-square statistic is significant at the 0.05 level.
Table 2.
Multinomial logistic regression analysis of educational ettainment (high school and middle school vs. primary school) in relation to sociodemographic factors, body mass index (BMI) and dietary habits.
Table 2.
Multinomial logistic regression analysis of educational ettainment (high school and middle school vs. primary school) in relation to sociodemographic factors, body mass index (BMI) and dietary habits.
| Independent Variables | High school | Middle school | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Gender | ||||||
| Male adolescents | 1 | 1 | ||||
| Female adolescents | 0.619 | (0.363–1.055) | 0.078 | 0.822 | (0.538–1.256) | 0.365 |
| Residence area | ||||||
| Urban area | 1 | 1 | ||||
| Rural area | 0.889 | (0.601–1.314) | 0.554 | 1.849 | (1.037–2.922) | 0.008 |
| Body mass index (BMI) | ||||||
| Underweight (<18.5) | 1 | 1 | ||||
| Normal (18.5–24.9) | 0.715 | (0.389-1.315) | 0.281 | 1.211 | (0.630-2.327) | 0.566 |
| Overweight (25–29.9) | 0.865 | (0.383–1.954) | 0.728 | 1.570 | (0.658–3.747) | 0.309 |
| Obese (≥30) | 0.996 | (0.307–3.233) | 0.995 | 1.197 | (0.296–4.847) | 0.801 |
| Frequency of vegetables consumption | ||||||
| Very rarely or not at all | 0.418 | (0.198–0.888) | 0.023 | 0.635 | (0.295–1.366) | 0.245 |
| One | 1 | 1 | ||||
| Two | 1.603 | (0.942–2.727) | 0.082 | 1.290 | (0.737–2.257) | 0.373 |
| Three | 2.447 | (0.980-6.112) | 0.055 | 1.481 | (0.536-4.095) | 0.449 |
| More than three | 1.865 | (0.626-5.558) | 0.263 | 1.225 | (0.406–3.695) | 0.719 |
| Frequency of fruits consumption | ||||||
| Very rarely or not at all | 1.328 | (0.628-2.809) | 0.458 | 1.425 | (0.640-3.175) | 0.386 |
| One | 1 | 1 | ||||
| Two | 0.925 | (0.536-1.596) | 0.779 | 1.473 | (0.821-2.641) | 0.194 |
| Three | 0.741 | (0.328-1.675) | 0.471 | 2.125 | (0.925-4.879) | 0.076 |
| More than three | 0.421 | (0.171-1.038) | 0.060 | 1.602 | (0.667-3.849) | 0.292 |
| Frequency of meat consumption | ||||||
| Very rarely or not at all | 4.518 | (0.748-27.290) | 0.100 | 6.578 | (1.105-39.165) | 0.039 |
| 2 – 3 times a month | 1.369 | (0.322-5.812) | 0.670 | 6.857 | (1.799-26.126) | 0.005 |
| Once a week | 0.917 | (0.425-1.981) | 0.826 | 1.246 | (0.559-2.777) | 0.591 |
| 2 – 3 times a week | 0.993 | (0.609-1.618) | 0.977 | 0.903 | (0.5371.518) | 0.701 |
| Daily | 1 | 1 | ||||
| Frequency of carbonated or sweetened drinks consumption | ||||||
| Very rarely or not at all | 0.185 | (0.064-0.532) | 0.002 | 0.116 | (0.040-0.334) | <0.001 |
| 2 – 3 times a month | 0.372 | (0.122-1.131) | 0.081 | 0.089 | (0.027-0.289) | <0.001 |
| Once a week | 0.255 | (0.088-0.736) | 0.012 | 0.147 | (0.051-0.426) | <0.001 |
| 2 – 3 times a week | 0.555 | (0.192-1.605) | 0.277 | 0.323 | (0.113-0.929) | 0.036 |
| Daily, more than one serving | 0.423 | (0.129-1.392) | 0.157 | 0.303 | (0.092-0.994) | 0.049 |
| Daily, one serving | 1 | 1 | ||||
| Frequency of fresh juices or smoothies consumption | ||||||
| Very rarely or not at all | 0.458 | (0.124-1.685) | 0.240 | 1.305 | (0.306-5.560) | 0.719 |
| 2 – 3 times a month | 0.689 | (0.185-2.567 | 0.579 | 1.447 | (0.334-6.265) | 0.621 |
| Once a week | 0.755 | (0.195-2.924) | 0.684 | 0.799 | (0.174-3.664) | 0.772 |
| 2 – 3 times a week | 1.120 | (0.277-4.529) | 0.873 | 1.190 | (0.249-5.692) | 0.828 |
| Daily, one serving | 1 | 1 | ||||
| Frequency of fish or seafood consumption | ||||||
| Very rarely or not at all | 1.602 | (0.650-3.950) | 0.306 | 2.013 | (0.775-5.232) | 0.151 |
| 2 – 3 times a month | 1.218 | (0.513-2.892) | 0.655 | 1.871 | (0.751-4.661) | 0.179 |
| Once a week | 1 | 1 | ||||
| 2 – 3 times a week | 2.118 | (0.872-5.147) | 0.097 | 1.738 | (0.678-4.458) | 0.250 |
| Frequency of sweets/pastries consumption | ||||||
| Very rarely or not at all | 1.827 | (0.708-4.710) | 0.213 | 1.391 | (0.510-3.792) | 0.519 |
| 2 – 3 times a month | 3.392 | (1.378-8.354) | 0.008 | 2.845 | (1.055-7.677) | 0.039 |
| Once a week | 1.152 | (0.585-2.267) | 0.682 | 1.172 | (0560-2.454) | 0674 |
| 2 – 3 times a week | 1.409 | (0.819-2.424) | 0.216 | 2.080 | (1.180-3.667) | 0.011 |
| Daily | 1 | 1 | ||||
| Frequency of pasta, rice or cereals consumption | ||||||
| Very rarely or not at all | 3.200 | (0.942-10.876) | 0.062 | 0.885 | (0.251-3.128) | 0.850 |
| 2 – 3 times a month | 3.872 | (1.462-10.254) | 0.006 | 1.382 | (0.536-3.561) | 0.503 |
| Once a week | 1.841 | (0.768-4.414) | 0.172 | 0.604 | (0.260-1.402) | 0.241 |
| 2 – 3 times a week | 1.817 | (0.800-4.130) | 0.154 | 0.807 | (0.377-1.729) | 0.807 |
| Daily | 1 | 1 | ||||
| Bread daily consumption | ||||||
| More than 12 slices | 1 | 1 | ||||
| 8 – 12 slices | 1.811 | (0.133-24.555) | 0.655 | 2.727 | (0.175-42.469) | 0.474 |
| 5 – 7 slices | 0.315 | (0.032-3.115) | 0.323 | 0.597 | (0.053-6.762) | 0.677 |
| 1 – 4 slices | 0.249 | (0.026-2.349) | 0.225 | 0.514 | (0.048-5.551) | 0.583 |
| Very rarely or not at all | 0.514 | (0.052-5.035) | 0.567 | 0.801 | (0.071-9.059) | 0.858 |
| Frequency of fast food consumption | ||||||
| Very rarely or not at all | 0.643 | (0.112-3.689) | 0.620 | 1.174 | (0.190-7.242) | 0.862 |
| 2 – 3 times a month | 0.323 | (0.058-1.788) | 0.196 | 0.482 | (0.081-2.853) | 0.421 |
| Once a week | 0.272 | (0.050-1.496) | 0.134 | 0.364 | (0.062-2.141) | 0.264 |
| 2 – 3 times a week | 0.121 | (0.021-0.691) | 0.018 | 0.224 | (0.036-1.380) | 0.107 |
| Daily | 1 | |||||
| Frequency of dairy consumption | ||||||
| Very rarely or not at all | 0.861 | (0.308-2.403) | 0.774 | 0.801 | (0.269-2.384) | 0.690 |
| 2 – 3 times a month | 0.803 | (0.326-1.977) | 0.633 | 0.505 | (0.182-1.402) | 0.190 |
| Once a week | 1.935 | (0.935-4.007) | 0.025 | 1.796 | (0.833-3.873) | 0.136 |
| 2 – 3 times a week | 1.052 | (0.622-1.779) | 0.851 | 1.308 | (0.760-2.252) | 0.332 |
| Daily | 1 | 1 | ||||
| Frequency of eggs weekly consumption | ||||||
| Very rarely or not at all | 0.316 | (0.053-1.891) | 0.207 | 0.525 | (0.076-3.617) | 0.513 |
| 1 – 2 eggs | 0.304 | (0.054-1.706) | 0.176 | 0.544 | (0.085-3.494) | 0.521 |
| 3 – 4 eggs | 0.169 | (0.030-0.951) | 0.044 | 0.331 | (0.051-2.136) | 0.245 |
| 5 – 7 eggs | 0.298 | (0.048-1.829) | 0.191 | 0.563 | (0.079-4.002) | 0.566 |
| More than 7 eggs | 1 | 1 | ||||
| Frequency of water drink per day consumption | ||||||
| Less than 1 L | 1 | 1 | ||||
| 1 L | 1.026 | (0.439-2.402) | 0.952 | 2.755 | (1.039-7.300) | 0.042 |
| 2 L | 1.574 | (0.683-3.629) | 0.287 | 3.015 | (1.148-7.300) | 0.025 |
| 3 L | 3.732 | (1.277-10.907) | 0.016 | 7.146 | (2.176-23.468) | 0.001 |
| More than 3 L | 2.353 | (0.672-8.242) | 0.181 | 2.076 | (0.487-8.853) | 0.323 |
The reference category is: Primary School.
Table 3.
Multinomial logistic regression analysis of dietary patterns and eating behaviors associated with educational level (High school and Middle school vs. Primary school).
Table 3.
Multinomial logistic regression analysis of dietary patterns and eating behaviors associated with educational level (High school and Middle school vs. Primary school).
| Independent Variables | High school | Middle school | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Type of food most often cunsumed | ||||||
| Fast food products | 0.546 | (0.116-2.562) | 0.443 | 3.712 | (0.581-23.715) | 0.166 |
| Pizza, snacks, pastries, sweets | 0.457 | (0.125-1.674) | 0.237 | 1.860 | (0.354-9.772) | 0.464 |
| Processed meats and canned products | 1 | 1 | ||||
| Restaurant-cooked meals | 0.265 | (0.063-1.110) | 0.069 | 1.040 | (0.168-6.433) | 0.967 |
| Home-cooked meals | 0.211 | (0.067-0.665) | 0.008 | 1.159 | (0.250-5.370) | 0.851 |
| Type of cooked food most often consumed | ||||||
| Fried food | 0.799 | (0.330-1.934) | 0.618 | 0.947 | (0.397-2.259) | 0.902 |
| Wood/charcoal-grilled food | 1.577 | (0.445-5.582) | 0.480 | 0.710 | (0.177-2.845) | 0.628 |
| Grilled food | 1.175 | (0.466-2.958) | 0.733 | 0.621 | (0.240-1.609) | 0.327 |
| Oven-cooked food | 0.711 | (0.326-1.552) | 0.392 | 0.449 | (0.205-0.981) | 0.045 |
| Boiled or steamed food | 0.507 | (0.214-1.203) | 0.123 | 0.547 | (0.234-1.276) | 0.163 |
| Other | 1 | 1 | ||||
| Type of food products in daily diet | ||||||
| Vegetables and fruits | 0.945 | (0.418-2.135) | 0.891 | 0.577 | (0.259-1.282) | 0.177 |
| Cereals and pasta | 0.752 | (0.296-1.911) | 0.549 | 0.577 | (0.231-1.445) | 0.240 |
| Dairy products | 1 | 1 | ||||
| Fish and seafood dishes | 1.656 | (0.359-7.632) | 0.517 | 0.352 | (0.051-2.415) | 0.288 |
| Meat | 1.024 | (0.463-2.267) | 0.953 | 0.619 | (0.285-1.346) | 0.227 |
| Eggs | 0.341 | (0.073-1.592) | 0.171 | 0.435 | (0.108-1.758) | 0.243 |
| Meat-based products (cold cuts, minced meat, canned food, etc.) |
2.138 | (0.762-6.000) | 0.149 | 1.153 | (0.408-3.259) | 0.788 |
| Pizza, sweets, and pastries | 1.187 | (0.227-6.215) | 0.839 | 1.047 | (0.214-5.118) | 0.955 |
| Foods rich in fats (lard, bacon, fatty meat, etc.) |
1.007 | (0.135-7.519) | 0.994 | 0.402 | (0.042-3.881) | 0.431 |
| Fast food products (burgers, shawarma, chicken nuggets, french fries, etc.) | 1.723 | (0.448-6.626) | 0.429 | 0.796 | (0.204-3.101) | 0.742 |
| Assessment of the amount of food consumed daily | ||||||
| Chaotic, excessive | 2.225 | (1.079-4.587) | 0.030 | 2.291 | (1.075-4.884) | 0.032 |
| Chaotic, insufficient | 1.517 | (0.833-2.763) | 0.173 | 1.693 | (0.910-3.147) | 0.096 |
| Moderate, without excess | 1 | 1 | ||||
| According to the body’s needs, monitoring the weight | 1.396 | (0.807-2.413) | 0.233 | 1.935 | (1.105-3.386) | 0.021 |
| According to a plan set by a specialist | 0.627 | (0.170-2.303) | 0.481 | 1.753 | (0.525-5.849) | 0.361 |
| Assessing receptivity to new foods introduced into their diet | ||||||
| Generally accepts them easily and is receptive to new foods | 1 | 1 | ||||
| Generally finds it difficult to accept and is reluctant to new foods | 0.200 | (0.120-0.334) | <0.001 | 0.370 | (0.223-0.615) | <0.001 |
| It is difficult to assess | 0.672 | (0.373-1.208) | 0.184 | 0.865 | (0.470-1.592) | 0.641 |
| How do they eat their meals | ||||||
| Generally eats in a hurry | 0.805 | (0.451-1.435) | 0.462 | 0.764 | (0.420-1.391) | 0.379 |
| Often does other activities during meals | 0.655 | (0.403-1.065) | 0.088 | 0.612 | (0.368-1.018) | 0.059 |
| Eats calmly and without rushing | 1 | 1 | ||||
| How do they eat their meals at home | ||||||
| Alone | 1 | 1 | ||||
| With siblings or friends | 1.049 | (0.477-2.309) | 0.905 | 1.326 | (0.577-3.047) | 0.506 |
| With siblings, possibly friends, and parents | 0.438 | (0.278-0.689) | <0.001 | 0.587 | (0.364-0.946) | 0.029 |
The reference category is: Primary School.
Table 4.
Multinomial logistic regression analysis of psychological and behavioral factors associated with educational level (High school and Middle school vs. Primary school).
Table 4.
Multinomial logistic regression analysis of psychological and behavioral factors associated with educational level (High school and Middle school vs. Primary school).
| Independent Variables | High school | Middle school | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Evaluation of the child's immune system | ||||||
| I believe they have a strong immune system | 1 | 1 | ||||
| I believe they have a weakened or unbalanced immune system | 1.999 | (0.893-4.475) | 0.092 | 1.706 | (0.748-3.891) | 0.204 |
| Periodically uses methods to strengthen the immune system | 0.675 | (0.371-1.230) | 0.199 | 0.638 | (0.338-1.205) | 0.166 |
| Experiencing periods of irritability | ||||||
| Never | 1.293 | (0.671-2.194) | 0.443 | 1.595 | (0.826-3.081) | 0.164 |
| Sometimes | 1 | 1 | ||||
| Frequently | 0.808 | (0.418-1.560) | 0.525 | 0.879 | (0.447-1.729) | 0.709 |
| Almost always | 0.465 | (0.156-1.382) | 0.168 | 0.742 | (0.247-2.229) | 0.595 |
| Suffering from fatigue | ||||||
| Never | 0.490 | (0.250-0.959) | 0.037 | 0.275 | (0.132-0.576) | 0.275 |
| Sometimes | 1 | 1 | ||||
| Frequently | 2.330 | (1.197-4.536) | 0.013 | 2.131 | (1.069-4.246) | 0.032 |
| Almost always | 14.592 | (3.563-59.769) | <0.001 | 8.735 | (2.063-36.986) | 0.003 |
| Suffering from anxiety or panic attacks | ||||||
| Never | 0.749 | (0.418-3.110) | 0.797 | 1.101 | (0.608-1.993) | 0.752 |
| Sometimes | 1 | 1 | ||||
| Frequently | 1.141 | (0.418-3.110) | 0.797 | 1.008 | (0.356-2.855) | 0.988 |
| Almost always | 1.234 | (0.224-6.799) | 0.809 | 0.266 | (0.030-2.329) | 0.266 |
| Stress Experience | ||||||
| Never | 0.640 | (0.339-1.207) | 0.168 | 0.793 | (0.420-1.499) | 0.476 |
| Sometimes | 1 | 1 | ||||
| Frequently | 2.574 | (1.245-5.319) | 0.011 | 1.101 | (0.496-2.442) | 0.814 |
| Almost always | 1.478 | (0.488-4.474) | 0.489 | 0.839 | (0.267-2.639) | 0.764 |
| Experiencing concentration issues | ||||||
| Never | 1.046 | (0.632-1.732) | 0.862 | 0.885 | (0.526-1.487) | 0.644 |
| Sometimes | 1 | 1 | ||||
| Frequently | 1.400 | (0.510-3.844) | 0.514 | 1.750 | (0.641-4.777) | 0.274 |
| Almost always | 0.637 | (0.180-2.259) | 0.485 | 1.249 | (0.370-4.221) | 0.720 |
| Dealing with insomnia | ||||||
| Never | 1.282 | (0.758-2.168) | 0.354 | 1.064 | (0.624-1.814) | 0.818 |
| Sometimes | 1 | 1 | ||||
| Frequently | 1.055 | (0.347-3.203) | 0.925 | 0.694 | (0.212-2.273) | 0.546 |
| Almost always | 0.776 | (0.158-3.821) | 0.755 | 0.339 | (0.057-2.025) | 0.235 |
| Experiencing depressive states | ||||||
| Never | 1.243 | (0.654-2.361) | 0.507 | 1.059 | (0.540-2.075) | 0.868 |
| Sometimes | 1 | 1 | ||||
| Frequently | 0.121 | (0.027-0.535) | 0.005 | 0.527 | (0.129-2.154) | 0.373 |
| Almost always | 0.160 | (0.027-0.958) | 0.045 | 0.142 | (0.020-1.026) | 0.053 |
| Sociability and communication | ||||||
| Yes | 1.896 | (0.881-4.083) | 0.102 | 1.023 | (0.482-2.169) | 0.954 |
| No | 1 | 1 | ||||
| Conflictuality with peers | ||||||
| Yes | 2.752 | (1.136-6.670) | 0.025 | 3.428 | (1.418-8.290) | 0.006 |
| No | 1 | 1 | ||||
| Practicing exercises/sports | ||||||
| No | 1 | 1 | ||||
| Yes, very rarely | 0.965 | (0.394-2.363) | 0.938 | 0.634 | (0.247-1.626) | 0.343 |
| Yes, 2-3 times a week | 0.482 | (0.200-1.158) | 0.103 | 0.561 | (0.226-1.391) | 0.212 |
| Yes, daily for under an hour | 0.231 | (0.078-0.684) | 0.008 | 0.487 | (0.168-1.410) | 0.184 |
| Yes, daily for at least an hour | 0.590 | (0.230-1.512) | 0.272 | 0.915 | (0.349-2.400) | 0.856 |
| Number of hours spent in front of the TV, tablet, computer, or phone | ||||||
| Daily, a maximum of 1 hour | 0.245 | (0.093-0.645) | 0.004 | 0.195 | (0.073-0.519) | 0.001 |
| Daily, 2-3 hours | 0.324 | (0.144-0.727) | 0.006 | 0.261 | (0.114-0.597) | 0.001 |
| Daily, 4-5 hours | 0.415 | (0.180-0.954) | 0.038 | 0.388 | (0.166-0.907) | 0.029 |
| Daily, 6-7 hours | 0.613 | (0.237-1.585) | 0.313 | 0.714 | (0.276-1.850) | 0.488 |
| Daily, more than 8 hours | 1 | 1 | ||||
| A few hours 2-3 times a week | 0.116 | (0.026-0.512) | 0.004 | 0.108 | (0.022-0.534) | 0.006 |
| Very rarely has access to these devices | 0.423 | (0.073-2.435) | 0.335 | 0.304 | (0.045-2.066) | 0.223 |
| Does not have access to these devices | 0.617 | (0.064-5.915) | 0.675 | 0.278 | (0.019-4.019) | 0.347 |
Dependent variable: healthy diet as the reference category.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



