Submitted:
28 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
Understanding the diagnostic landscape prior to developing novel diagnostic strategies is key to managing expectations and authenticating results. In considering the possibility of developing alternate diagnostic approaches for coeliac disease based on duodenal biopsies, we audited 18 months’ worth of duodenal biopsies received in our centre to determine the exact proportions of different diagnoses. A total of 6245 duodenal biopsies were audited, of which 73.76% were normal and 8.84% fell within the spectrum of coeliac disease. Additionally, 6.47% were classified as showing non-specific inflammation, 1.86% were adenomas, 0.42% were carcinomas, and 0.06% were neuroendocrine tumours. Rarer diagnoses included ulceration, Helicobacter pylori infection, Giardiasis, lymphangiectasia, transplant rejection, and lymphoma. Furthermore, 227 biopsies (3.63%) showed isolated intraepithelial lymphocytosis, of which 24 cases eventually received a definitive diagnosis of coeliac disease. We present the first long-term audit of all endoscopic duodenal biopsies received by the histopathology department of a tertiary care facility. The results indicate that a fully automated system that could identify normal duodenal biopsies and biopsies within the spectrum of coeliac disease-associated enteropathy could decrease pathologists’ endoscopic duodenal biopsy workload by up to 80%.
Keywords:
coeliac disease
; audit
; duodenal biopsy
; gluten sensitivity
1. Introduction
Global Shortage of Pathologists
There exists a well-documented global shortage of pathologists resulting from a demand-supply mismatch. [1,2,3,4,5] A worldwide audit encompassing 162 countries averaged the number of pathologists per million population at 14. [6] Only 3% of histopathology departments in the United Kingdom had sufficient staff to meet clinical demand in 2018 [7] and in 2021, 10.8% of histopathology consultant posts were vacant. [8] Developing countries, for example in sub-Saharan Africa, have a disproportionately low number of trained pathologists dealing with a growing burden of cancer diagnosis, [9] while resource-rich countries like the United States of America are seeing a steadily declining pool of pathologists in active clinical practice. [4]
Effect on Endoscopic Duodenal Biopsies
With the existing workforce, endoscopic duodenal biopsies are frequently subject to delays as they are a relatively “low risk” sample type. As demonstrated in this study, only a minor proportion of the biopsies contain cancer. Backlogs in biopsy diagnosis can adversely impact patient care by prolonging decisions on management, delaying treatment initiation, and potentially extending hospital stays.
Diagnosing Coeliac Disease in Endoscopic Duodenal Biopsies
The most frequent specific diagnosis made on duodenal biopsies is gluten-sensitivity or coeliac disease. Coeliac disease is an autoimmune disorder characterised by an adverse reaction to gluten, a protein found in wheat, barley, and rye, leading to small intestinal mucosal inflammation and malabsorption. The population prevalence of coeliac disease is estimated to be around 1%, yet only about one-third of these cases have been officially diagnosed [10,11]. Accurate diagnosis is particularly important for gluten-sensitive patients, as false negative or equivocal results may leave them with chronic debilitating symptoms, including abdominal pain, diarrhoea, vomiting, malaise, fatigue, mouth ulcers and itchy skin rashes, as well as long-term complications, including cancer, lymphoma, vitamin deficiency, anaemia, osteoporosis and infertility [12,13].
Pathologists’ Discordance in Biopsy-Based Coeliac Disease Diagnosis
While a 3-6% discrepancy in agreement among histopathologists exists across all biopsy specimens, [14,15,16] this discrepancy is notably higher for coeliac disease biopsies, as demonstrated by a recent study involving 17 histopathologists from the UK and Norway. [17] Disagreement between any two pathologists regarding the categorisation of a biopsy as histologically normal, containing coeliac disease, or showing indeterminate enteropathy occurred 20% of the time (Cohen’s kappa of 0.59, considered “fair agreement”), [17] aligning with findings from other published studies [18,19,20,21,22,23].
Isolated intraepithelial lymphocytosis further complicates histology-based diagnosis of coeliac disease. While a lymphocyte count of more than 25 per 100 epithelial cells [24] is commonly recognised as indicative of coeliac disease, [25,26] it lacks specificity in isolation without appropriate clinical context, as similar elevations occur in so-called non-coeliac gluten intolerance, wheat and milk allergies, autoimmune diseases or, uncommonly, as a reaction to certain medications [12,27,28]. The persistence of inaccurate and inconclusive diagnoses contributes significantly to the average period from symptom onset to a diagnosis of coeliac disease being 13.2 years in the UK [29,30]. This underscores the need for more rapid and accurate diagnostic approaches for duodenal biopsies.
Digital Pathology
With growing utilisation of artificial intelligence in medical disciplines such as oncology, radiology and dermatology [31,32,33] and its increasing application within histopathology, [34,35] studies are under way to evaluate the practical implementation of computational diagnostic classifiers within routine clinical practice [36]. Our team is currently developing an artificial intelligence system for automating specific tasks associated with histopathological evaluation of duodenal biopsies to improve diagnostic accuracy and workflow [37,38,39].
Rationale for Audit
When developing a new diagnostic approach, it is crucial to understand what the expected results might look like following real-life deployment. Accordingly, we audited 18 months’ worth of duodenal biopsies received at Cambridge University Hospitals NHS Foundation Trust to determine the exact proportions of different diagnoses. Furthermore, pathologists’ diagnoses are frequently used as training data for AI models. Consequently, we analysed cases initially classified as showing isolated intraepithelial lymphocytosis, to determine how many eventually receive a CeD diagnosis. These cases should be reclassified as CeD in the AI dataset, despite the initial pathologist’s report.
2. Materials and Methods
Retrospective review of the histological diagnoses of all endoscopic duodenal biopsies received by the Department of Histopathology, Addenbrooke’s Hospital, Cambridge, UK, was undertaken over a period of 18 months from 01 January 2018 to 30 June 2019. The full text of the anonymised histopathology report was retrieved for each patient and the text of the final diagnosis, clinical details and microscopy sections was used to determine the diagnostic category for each biopsy.
For rare or more serious conditions that may not be safely assessed in an automated way in the near future (e.g., refractory coeliac disease, dysplasia, malignancy and ulceration), the clinical details accompanying the specimen were examined in order to determine key words that could be used to exclude such cases from a potential AI-based automated diagnostic tool. For biopsies with isolated intraepithelial lymphocytosis, we determined how many patients in this cohort were subsequently clinically diagnosed with coeliac disease using follow-up data at CUH. Finally, we compared the at-risk HLA genotypes for coeliac disease in this audit subgroup with that of the genome-wide genotyping dataset from the UK Biobank’s anonymized database available at their Research Analysis Platform [55] (RAP).
We obtained HLA typing data from 32,856 patients from the UK Biobank [40,41]. We split the patients into a coeliac disease group (n=3,094) and a control group (n=29.762) based on their responses to the online coeliac disease and dietary questionnaires, as well as their health records. To identify genetic risk factors, we created an HLA typing code using the UK Biobank’s imputation threshold [42]. This code leveraged specific allele combinations to identify HLA genotypes associated with an increased risk of coeliac disease [43].
3. Results
The findings of this audit are presented in three parts: (1) the diagnostic categories and frequency of biopsies in each category; (2) the keywords identifying the minor diagnostic categories unlikely, for patient safety reasons, to be amenable to automated diagnosis and (3) an exploration of the characteristics of cases showing isolated intraepithelial lymphocytosis.
3.1. Breakdown of Diagnostic Categories
6245 endoscopic duodenal biopsies were received over the 18-month period (Table 1). The proportions of the distinct diagnoses, derived from the histopathology reports, are illustrated in Figure 1.
The two largest diagnostic categories were those of normal histology with 4606 (73.68%) biopsies and active coeliac disease with 344 (5.50%) biopsies. Additionally, within the spectrum of coeliac disease-related pathology, eight (0.13%) were diagnosed as villous atrophy alone, five (0.08%) as villous atrophy with raised intraepithelial lymphocytes, and three (0.05%) as gluten sensitive enteropathy. A total of 172 (2.75%) biopsies were from patients previously diagnosed with coeliac disease who were on a gluten-free diet (GFD). Of these, 119 (1.90%) biopsies displayed complete healing of duodenal mucosa while 53 (0.85%) showed only partial mucosal recovery. Finally, 20 (0.32%) biopsies were diagnosed as refractory coeliac disease. Hence, a total of 552 biopsies (8.84%) exhibited features associated with coeliac disease, some probably representing similar conditions given semantically different labels, spanning a spectrum from active disease status to normal histology.
A total of 227 (3.63%) biopsies were reported as having isolated intraepithelial lymphocytosis (commonly considered as more than 25 lymphocytes per 100 epithelial cells), [24] with a comment advising the treating physician to correlate biopsy findings with clinical information to determine the diagnosis. The diagnosis of “non-specific inflammation” was given to 404 (6.46%) biopsies. This category included patients presenting with a diverse array of reported symptoms, with the biopsy showing mixed chronic or active chronic inflammation in the mucosa and/or lamina propria. Other notable groups were adenomas, comprising 116 (1.86%) of the cases, focal gastric heterotropia with 104 (1.66%) cases, and gastric metaplasia with 48 (0.77%) cases. Furthermore, 28 biopsies (0.45%) were diagnosed with carcinoma, which included 21 cases of primary duodenal adenocarcinomas and 7 cases of metastatic carcinoma.
Minor diagnostic categories included lymphangiectasia with 25 (0.40%) cases and ulceration with 25 (0.40%) cases. There were 20 (0.32%) biopsies from intestinal transplant recipients showing healthy graft status (15 biopsies, 0.24%), mild rejection (two biopsies, 0.032%), bacterial infection (two biopsies, 0.032%), and post-transplant lymphoproliferative disorder (one biopsy, 0.016%). Additionally, seven (0.11%) duodenal biopsies were from peripheral blood, bone marrow, or renal transplant recipients demonstrating graft-versus-host disease. Furthermore, there were twelve (0.19%) biopsies diagnosed with giardiasis, ten (0.16%) cases of mucosal erosion, nine (0.14%) cases showing Helicobacter pylori infection, seven (0.11%) cases each of regenerative mucosal changes and hyperplasia without dysplasia, six (0.10%) cases each of lymphoma and lipoma, five (0.08%) cases of drug-induced enteropathy, five (0.08%) cases of Crohn’s disease, four (0.06%) cases each of neuroendocrine tumour and viral enteropathy, three (0.05%) cases of lymphoid aggregates, and two (0.03%) cases each with granulomas and flat (non-adenomatous) dysplasia.
Finally, the following diagnoses contributed one (0.02%) case each: common variable immunodeficiency syndrome, amyloidosis, thrombus, pseudolipomatosis, spindle cell tumour, pseudomelanosis, and gangliocytic paraganglioma.
3.2. Keywords for Minor Diagnostic Categories
Each biopsy request is generally accompanied by clinical information from the treating physician. Commonly mentioned clinical features of coeliac disease include iron deficiency anaemia, weight loss, diarrhoea, abdominal pain, dyspepsia, and/or nutrient deficiency. Exploring this aspect, we identified certain keywords used in the clinical request forms accompanying the biopsy that suggested abnormal conditions other than coeliac disease. If utilising a potential automated diagnostic tool, these keywords could act as indicators for triaging biopsies and prioritising them for evaluation by a pathologist (Table 2).
3.3. Isolated Intraepithelial Lymphocytosis
Intraepithelial lymphocytosis is a descriptive histological feature rather than a distinct diagnostic entity. Accordingly, the group of 227 biopsies with isolated intraepithelial lymphocytosis was subjected to a chart review. Iron deficiency anaemia was found to be the most common clinical presentation (Table 3).
To assess the potential presence for (undiagnosed) coeliac disease, we analysed these 227 cases of isolated intraepithelial lymphocytosis (Table 4). Among these cases, 24 patients eventually received a CeD diagnosis either before or after the biopsy. Specifically, 9 cases (3.96%) had already been diagnosed with CeD prior to the biopsy and were already following a gluten-free diet, 13 cases (5.73%) were diagnosed via subsequent clinicopathological correlation, and 2 cases (0.88%) received a CeD diagnosis following an additional biopsy. Moreover, 9 biopsies (3.96%) showed CeD-related laboratory results: 5 (2.20%) exhibited clear positive findings for both tissue transglutaminase IgA (tTG) and endomysial antibody (EMA), while 4 cases (1.76%) had a positive IgA tTG result with a negative or missing EMA result. HLA typing data were available for 21 of these patients. Of these, 4 were diagnosed with CeD following biopsy based on alternative criteria, and all 4 carried a CeD-associated HLA type. Among the remaining 17 patients, who had no other evidence supporting a CeD diagnosis, 10 (59%) carried a CeD-associated HLA type. This closely mirrors the prevalence of CeD-associated HLA types in the non-CeD control group from the UK Biobank (58%), meaning that it cannot be used to comment on the probability of CeD in this group of patients (see Supplementary Material A). These findings underscore the need for thorough investigation of raised IEL cases to ensure that all patients who eventually receive a CeD diagnosis are correctly classified when developing high-quality AI training datasets.
Patients with isolated intraepithelial lymphocytosis also had a higher prevalence of hypothyroidism, Graves’ disease, microscopic colitis, pernicious anaemia, Crohn’s disease, ankylosing spondylosis, ulcerative colitis and Addison’s disease compared to the general population (Table 5). A significant portion of these cases remained without a final diagnosis despite abnormal laboratory tests, elevated faecal calprotectin being the most frequent finding (Table 6). Finally, 119 cases (52.42%) lacked information alluding to any abnormality, presenting a definitive diagnostic challenge.
4. Discussion
We showed here that the majority of endoscopic duodenal biopsies are either normal (73.76%) or show coeliac disease-associated pathology (8.83%). It is worth noting that the diagnostic proportions in our study may not be fully generalisable due to variations in case mix and protocols leading to patient referral for endoscopy, as well as age, ethnicity, and socioeconomic factors of the patient population served by other hospitals. Nonetheless, automated diagnostic approaches aimed at efficiently identifying normal histology and coeliac disease could provide automated diagnosis for >80% of duodenal biopsies, providing one means of mitigating the shortage of pathologists and preventing backlogs associated with endoscopic duodenal biopsies.
When considering a novel diagnostic strategy, prioritising safety is paramount. Approaches designed to identify the two largest categories of “normal” and “coeliac disease”, for instance one involving AI-based image analysis, are more achievable as opposed to an approach that can specifically recognise all major and minor pathologies, due principally to insufficient numbers of examples of such cases for training and testing of an AI system. Therefore, binomial classification strategies require a safety feature to flag biopsies that can rapidly and significantly harm a patient, if misidentified as normal or coeliac disease.
Accordingly, we examined clinical details associated with abnormal, non-coeliac biopsies and compiled keywords related to potentially rapidly harmful conditions, including ulceration, dysplasia, benign and malignant tumours (Table 2). These terms could potentially be used to triage biopsies for immediate evaluation by a pathologist. We found that the presence of polyps or tumours on endoscopy, gastrointestinal bleeding, jaundice or biliary obstruction, and underlying systemic diseases, immunosuppression, or hereditary cancer syndromes indicated diagnoses with poorer prognosis. Therefore, any biopsy received with clinical information containing these keywords or indicating that the patient has had a transplant should be flagged for immediate examination by a pathologist. Notably, the keywords for giardiasis overlapped with those commonly used for coeliac disease, rendering this method unsuitable for such cases. This suggests that, to automate the diagnosis of suspected coeliac disease biopsies, a recognition mechanism for Giardia parasites in histological sections would need to be developed. However, this triaging method is reliant on the provision of comprehensive clinical details, presenting a challenge to its practical implementation.
In our review of 227 biopsies diagnosed as isolated intraepithelial lymphocytosis, a descriptive histological finding rather than a distinct diagnostic entity, we sought to identify potential underlying CeD and related conditions. Iron deficiency anaemia emerged as the most common clinical presentation. Notably, 24 patients eventually received a CeD diagnosis, either before or after the biopsy. Additionally, CeD-related laboratory abnormalities were identified in 9 biopsies, with positive tissue transglutaminase IgA (tTG) or endomysial antibody (EMA) results. Patients with isolated intraepithelial lymphocytosis also exhibited a higher prevalence of autoimmune and inflammatory disorders compared to the general population. Despite these findings, a significant proportion of cases remained without a definitive diagnosis. Overall, these results underscore the diagnostic challenges associated with raised IELs and highlight the need for comprehensive investigations to ensure accurate classification, particularly when developing high-quality AI training datasets.
We have applied a simple audit approach to a large cohort of duodenal biopsies, and our results show that a system capable of identifying most biopsies with normal mucosa and those with features of coeliac disease might achieve automated diagnosis of around 80% of duodenal biopsies. These data can be utilised for designing a strategy for AI-mediated automation of duodenal biopsy diagnosis. Moreover, our data provide a baseline for assessment of the expected output of such an AI-mediated system. It would be important to audit diagnostic outputs of any such system against these figures following implementation. Due to differences in case mix and endoscopy referral practices, it may be necessary to undertake a small baseline audit in each centre before introducing any automation to the process of duodenal biopsy diagnosis. This study demonstrates the feasibility and utility of undertaking an audit of this nature.
Author Contributions
Conceptualization, methodology, funding acquisition, resources, supervision, E.S; data collection, E.S., K.N.L.H, V.S., J.W.; formal analysis, visualization V.S., J.L.J., A.B.W.W., N.P.R.M.M., F.J.; writing—original draft preparation, V.S.; writing—review and editing, F.J., E.S.; project administration, S.C.E. All authors have read and agreed to the published version of the manuscript.
Funding
J.L.J was funded by Kings College, University of Cambridge. A.B.W.W. and N.P.R.M.M. were funded by the Pathological Society of Great Britain and Ireland. K.N.L.H. was funded by a Coeliac UK Sponsored Dissertation Grant and University of Cambridge Department of Pathology PhD Grant. S.E. was funded by Coeliac UK and Innovate UK. J.W. and F.J. were funded by an NIHR i4i PDA grant (to E.S.).
Institutional Review Board Statement
The primary audit did not require ethical approval. For the UK Biobank data, all participants provided electronic signed consent to take part in UK Biobank and for UK Biobank to perform ongoing linkage to health-related records. UK Biobank received approval from the National Information Governance Board for Health and Social Care and the National Health Service North West Centre for Research Ethics Committee (Ref: 11/NW/0382).
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author. This study includes data from UK Biobank, a major biomedical database (https://www.ukbiobank.ac.uk/).
Conflicts of Interest
EJS and FJ are shareholders in the digital image analysis company, Lyzeum Ltd. The other authors do not have any conflicts of interest.
References
- Metter, D.M.; Colgan, T.J.; Leung, S.T.; Timmons, C.F.; Park, J.Y. Trends in the US and Canadian Pathologist Workforces From 2007 to 2017. JAMA Network Open 2019, 2, e194337. [Google Scholar] [CrossRef] [PubMed]
- APW.Pdf. Available online: https://www.rcpa.edu.au/getattachment/4a38b4f9-5f6a-45eb-8947-dfa072797685/APW.aspx (accessed on 22 January 2024).
- Märkl, B.; Füzesi, L.; Huss, R.; Bauer, S.; Schaller, T. Number of Pathologists in Germany: Comparison with European Countries, USA, and Canada. Virchows Arch 2021, 478, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Robboy, S.J.; Weintraub, S.; Horvath, A.E.; Jensen, B.W.; Alexander, C.B.; Fody, E.P.; Crawford, J.M.; Clark, J.R.; Cantor-Weinberg, J.; Joshi, M.G.; Cohen, M.B.; Prystowsky, M.B.; Bean, S.M.; Gupta, S.; Powell, S.Z.; Speights, V.O., Jr; Gross, D.J.; Black-Schaffer, W.S.; additional members of the Workforce Project Work Group. Pathologist Workforce in the United States: I. Development of a Predictive Model to Examine Factors Influencing Supply. Archives of Pathology & Laboratory Medicine 2013, 137, 1723–1732. [Google Scholar] [CrossRef]
- Mudenda, V.; Malyangu, E.; Sayed, S.; Fleming, K. Addressing the Shortage of Pathologists in Africa: Creation of a MMed Programme in Pathology in Zambia. Afr J Lab Med 2020, 9, 974. [Google Scholar] [CrossRef]
- Bychkov, A.; Schubert, M. Constant Demand, Patchy Supply. The Pathologist 2023, 88, 18–27. [Google Scholar]
- Meeting-Pathology-Demand-Histopathology-Workforce-Census-2018.Pdf. https://www.rcpath.org/static/952a934d-2ec3-48c9-a8e6e00fcdca700f/Meeting-Pathology-Demand-Histopathology-Workforce-Census-2018.pdf (accessed 2024-01-22).
- Histopathologists.Pdf. https://www.rcpath.org/static/797e5533-d718-442a-be4ee7e695a5550e/Histopathologists.pdf (accessed 2024-01-19).
- Adesina, A.; Chumba, D.; Nelson, A.M.; Orem, J.; Roberts, D.J.; Wabinga, H.; Wilson, M.; Rebbeck, T.R. Improvement of Pathology in Sub-Saharan Africa. The Lancet Oncology 2013, 14, e152–e157. [Google Scholar] [CrossRef]
- Diagnosis. Coeliac UK. https://www.coeliac.org.uk/healthcare-professionals/diagnosis/ (accessed 2024-01-22).
- Downey, L.; Houten, R.; Murch, S.; Longson, D. Recognition, Assessment, and Management of Coeliac Disease: Summary of Updated NICE Guidance. Bmj 2015, 351. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac Disease: A Comprehensive Current Review. BMC Med 2019, 17, 142. [Google Scholar] [CrossRef]
- full-guideline-pdf-438530077.pdf. https://www.nice.org.uk/guidance/ng20/evidence/full-guideline-pdf-438530077 (accessed 2024-01-22).
- Tsung, J.S.H. Institutional Pathology Consultation. The American Journal of Surgical Pathology 2004, 28, 399. [Google Scholar] [CrossRef]
- Frable, W.J. Surgical Pathology—Second Reviews, Institutional Reviews, Audits, and Correlations: What’s Out There? Error or Diagnostic Variation? Archives of Pathology & Laboratory Medicine 2006, 130, 620–625. [Google Scholar] [CrossRef]
- Ordi, J.; Castillo, P.; Saco, A.; Pino, M. del; Ordi, O.; Rodríguez-Carunchio, L.; Ramírez, J. Validation of Whole Slide Imaging in the Primary Diagnosis of Gynaecological Pathology in a University Hospital. Journal of Clinical Pathology 2015, 68, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Denholm, J.; Schreiber, B.A.; Jaeckle, F.; Wicks, M.N.; Benbow, E.W.; Bracey, T.S.; Chan, J.Y.H.; Farkas, L.; Fryer, E.; Gopalakrishnan, K.; Hughes, C.A.; Kirkwood, K.J.; Langman, G.; Mahler, B.; McMahon, R.F.T.; Myint, K.L.W.; Natu, S.; Robinson, A.; Sanduka, A.; Sheppard, K.A.; Tsang, Y.W.; Arends, M.J.; Soilleux, E.J. Digital Pathology Reporting of Coeliac Disease: An Inter-Observer Agreement Study.
- Villanacci, V.; Lorenzi, L.; Donato, F.; Auricchio, R.; Dziechciarz, P.; Gyimesi, J.; Koletzko, S.; Mišak, Z.; Laguna, V.M.; Polanco, I.; Ramos, D.; Shamir, R.; Troncone, R.; Vriezinga, S.L.; Mearin, M.L. Histopathological Evaluation of Duodenal Biopsy in the PreventCD Project. An Observational Interobserver Agreement Study. APMIS 2018, 126, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Picarelli, A.; Borghini, R.; Donato, G.; Di Tola, M.; Boccabella, C.; Isonne, C.; Giordano, M.; Di Cristofano, C.; Romeo, F.; Di Cioccio, G.; Marcheggiano, A.; Villanacci, V.; Tiberti, A. Weaknesses of Histological Analysis in Celiac Disease Diagnosis: New Possible Scenarios. Scandinavian Journal of Gastroenterology 2014, 49, 1318–1324. [Google Scholar] [CrossRef]
- Arguelles-Grande, C.; Tennyson, C.A.; Lewis, S.K.; Green, P.H.R.; Bhagat, G. Variability in Small Bowel Histopathology Reporting between Different Pathology Practice Settings: Impact on the Diagnosis of Coeliac Disease. J Clin Pathol 2012, 65, 242. [Google Scholar] [CrossRef]
- Alessio, M.G.; Tonutti, E.; Brusca, I.; Radice, A.; Licini, L.; Sonzogni, A.; Florena, A.; Schiaffino, E.; Marus, W.; Sulfaro, S.; Villalta, D.; Study Group on Autoimmune Diseases of Italian Society of Laboratory Medicine. Correlation between IgA Tissue Transglutaminase Antibody Ratio and Histological Finding in Celiac Disease. J Pediatr Gastroenterol Nutr 2012, 55, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Villanacci, V.; Zambelli, C.; Milione, M.; Luinetti, O.; Vindigni, C.; Chioda, C.; Albarello, L.; Bartolini, D.; Donato, F. Comparison of the Interobserver Reproducibility With Different Histologic Criteria Used in Celiac Disease. Clinical Gastroenterology and Hepatology 2007, 5, 838–843. [Google Scholar] [CrossRef]
- Montén, C.; Bjelkenkrantz, K.; Gudjonsdottir, A.H.; Browaldh, L.; Arnell, H.; Naluai, Å.T.; Agardh, D. Validity of Histology for the Diagnosis of Paediatric Coeliac Disease: A Swedish Multicentre Study. Scandinavian Journal of Gastroenterology 2016, 51, 427–433. [Google Scholar] [CrossRef]
- Hayat, M.; Cairns, A.; Dixon, M.F.; O’Mahony, S. Quantitation of Intraepithelial Lymphocytes in Human Duodenum: What Is Normal? Journal of Clinical Pathology 2002, 55, 393. [Google Scholar] [CrossRef]
- Marsh, M.N.; Rostami, K. What Is A Normal Intestinal Mucosa? Gastroenterology 2016, 151, 784–788. [Google Scholar] [CrossRef]
- Oberhuber, G. Histopathology of Celiac Disease. Biomedicine & Pharmacotherapy 2000, 54, 368–372. [Google Scholar] [CrossRef]
- Collin, P.; Wahab, P.J.; Murray, J.A. Intraepithelial Lymphocytes and Coeliac Disease. Best Practice & Research Clinical Gastroenterology 2005, 19, 341–350. [Google Scholar] [CrossRef]
- Hammer, S.T.G.; Greenson, J.K. The Clinical Significance of Duodenal Lymphocytosis with Normal Villus Architecture. Arch Pathol Lab Med 2013, 137, 1216–1219. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.M.; Papanicolas, I.N. Impact of Symptoms on Quality of Life before and after Diagnosis of Coeliac Disease: Results from a UK Population Survey. BMC Health Serv Res 2010, 10, 105. [Google Scholar] [CrossRef] [PubMed]
- Diagnosis. Coeliac UK. https://www.coeliac.org.uk/healthcare-professionals/diagnosis/ (accessed 2024-01-22).
- Holten-Rossing, H.; Talman, M.-L. M.; Jylling, A.M.B.; Lænkholm, A.-V.; Kristensson, M.; Vainer, B. Application of Automated Image Analysis Reduces the Workload of Manual Screening of Sentinel Lymph Node Biopsies in Breast Cancer. Histopathology 2017, 71, 866–873. [Google Scholar] [CrossRef]
- Ström, P.; Kartasalo, K.; Olsson, H.; Solorzano, L.; Delahunt, B.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Grignon, D.J.; Humphrey, P.A.; Iczkowski, K.A.; Kench, J.G.; Kristiansen, G.; Kwast, T.H. van der; Leite, K.R.M.; McKenney, J.K.; Oxley, J.; Pan, C.-C.; Samaratunga, H.; Srigley, J.R.; Takahashi, H.; Tsuzuki, T.; Varma, M.; Zhou, M.; Lindberg, J.; Lindskog, C.; Ruusuvuori, P.; Wählby, C.; Grönberg, H.; Rantalainen, M.; Egevad, L.; Eklund, M. Artificial Intelligence for Diagnosis and Grading of Prostate Cancer in Biopsies: A Population-Based, Diagnostic Study. The Lancet Oncology 2020, 21, 222–232. [Google Scholar] [CrossRef]
- Brodsky, V.; Levine, L.; Solans, E.P.; Dola, S.; Chervony, L.; Polak, S. Performance of Automated Classification of Diagnostic Entities in Dermatopathology Validated on Multisite Data Representing the Real-World Variability of Pathology Workload. Archives of Pathology & Laboratory Medicine, 2022. [Google Scholar] [CrossRef]
- Al-Janabi, S.; Huisman, A.; Van Diest, P.J. Digital Pathology: Current Status and Future Perspectives. Histopathology 2012, 61, 1–9. [Google Scholar] [CrossRef]
- Jahn, S.W.; Plass, M.; Moinfar, F. Digital Pathology: Advantages, Limitations and Emerging Perspectives. Journal of Clinical Medicine 2020, 9, 3697. [Google Scholar] [CrossRef]
- International evaluation of an AI system for breast cancer screening | Nature. https://www.nature.com/articles/s41586-019-1799-6 (accessed 2023-04-17).
- Denholm, J.; Schreiber, B.A.; Evans, S.C.; Crook, O.M.; Sharma, A.; Watson, J.L.; Bancroft, H.; Langman, G.; Gilbey, J.D.; Schönlieb, C.-B.; Arends, M.J.; Soilleux, E.J. Multiple-Instance-Learning-Based Detection of Coeliac Disease in Histological Whole-Slide Images. Journal of Pathology Informatics 2022, 13, 100151. [Google Scholar] [CrossRef]
- Jaeckle, F.; Bryant, R.; Denholm, J.; Romero Diaz, J.; Schreiber, B.; Shenoy, V.; Ekundayomi, D.; Evans, S.; Arends, M.; Soilleux, E. Interpretable Machine Learning Based Detection of Coeliac Disease. medRxiv 2025, 2025–03. [Google Scholar]
- Jaeckle, F.; Denholm, J.; Schreiber, B.; Evans, S.C.; Wicks, M.N.; Chan, J.Y.H.; Bateman, A.C.; Natu, S.; Arends, M.J.; Soilleux, E. Machine Learning Achieves Pathologist-Level Celiac Disease Diagnosis. NEJM AI 2025, 2. [Google Scholar] [CrossRef]
- Watts, G. UK Biobank Opens Its Data Vaults to Researchers, 2012. https://www.bmj.com/content/344/bmj.e2459.full (accessed 2025-02-19).
- Bahcall, O.G. UK Biobank–a New Era in Genomic Medicine. Nature reviews genetics 2018, 19, 737–738. [Google Scholar] [CrossRef]
- UK Biobank, Resource 182. https://biobank.ctsu.ox.ac.uk/crystal/refer.cgi?id=182.
- Ting, Y.T.; Dahal-Koirala, S.; Kim, H.S.K.; Qiao, S.-W.; Neumann, R.S.; Lundin, K.E.A.; Petersen, J.; Reid, H.H.; Sollid, L.M.; Rossjohn, J. A Molecular Basis for the T Cell Response in HLA-DQ2.2 Mediated Celiac Disease. Proceedings of the National Academy of Sciences of the United States of America 2020, 117, 3063. [Google Scholar] [CrossRef] [PubMed]
- Torres-Bondia, F.; de Batlle, J.; Galván, L.; Buti, M.; Barbé, F.; Piñol-Ripoll, G. Evolution of the Consumption Trend of Proton Pump Inhibitors in the Lleida Health Region between 2002 and 2015. BMC Public Health 2022, 22, 818. [Google Scholar] [CrossRef]
- Brennan, R.; Wazaify, M.; Shawabkeh, H.; Boardley, I.; McVeigh, J.; Van Hout, M.C. A Scoping Review of Non-Medical and Extra-Medical Use of Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Drug Saf 2021, 44, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Hackett, R.J.; Preston, S.L.H. Pylori Infection, Part I: Clinical Burden and Diagnosis. Trends in Urology & Men’s Health 2021, 12, 13–19. [Google Scholar] [CrossRef]
- Irritable-Bowel-Syndrome-in-Adults-Qs-Briefing-Paper2.Pdf. https://www.nice.org.uk/guidance/QS114/documents/irritable-bowel-syndrome-in-adults-qs-briefing-paper2 (accessed 2023-10-23).
- Context | Thyroid disease: assessment and management | Guidance | NICE. https://www.nice.org.uk/guidance/ng145/chapter/Context (accessed 2023-10-23).
- Prevalence | Background information | Hyperthyroidism | CKS | NICE. https://cks.nice.org.uk/topics/hyperthyroidism/background-information/prevalence/ (accessed 2023-10-23).
- Green, H.D.; Beaumont, R.N.; Thomas, A.; Hamilton, B.; Wood, A.R.; Sharp, S.; Jones, S.E.; Tyrrell, J.; Walker, G.; Goodhand, J.; Kennedy, N.A.; Ahmad, T.; Weedon, M.N. Genome-Wide Association Study of Microscopic Colitis in the UK Biobank Confirms Immune-Related Pathogenesis. J Crohns Colitis 2019, 13, 1578–1582. [Google Scholar] [CrossRef]
- Mohamed, M.; Thio, J.; Thomas, R.S.; Phillips, J. Pernicious Anaemia. BMJ 2020, 369, m1319. [Google Scholar] [CrossRef]
- Pasvol, T.J.; Horsfall, L.; Bloom, S.; Segal, A.W.; Sabin, C.; Field, N.; Rait, G. Incidence and Prevalence of Inflammatory Bowel Disease in UK Primary Care: A Population-Based Cohort Study. BMJ Open 2020, 10, e036584. [Google Scholar] [CrossRef]
- Prevalence and incidence | Background information | Rheumatoid arthritis | CKS | NICE. https://cks.nice.org.uk/topics/rheumatoid-arthritis/background-information/prevalence-incidence/ (accessed 2023-10-23).
- Prevalence | Background information | Ankylosing spondylitis | CKS | NICE. https://cks.nice.org.uk/topics/ankylosing-spondylitis/background-information/prevalence/ (accessed 2023-10-23).
- Prevalence | Background information | Gastrointestinal tract (lower) cancers - recognition and referral | CKS | NICE. https://cks.nice.org.uk/topics/gastrointestinal-tract-lower-cancers-recognition-referral/background-information/prevalence/ (accessed 2023-10-23).
- Prevalence | Background information | Gastrointestinal tract (upper) cancers - recognition and referral | CKS | NICE. https://cks.nice.org.uk/topics/gastrointestinal-tract-upper-cancers-recognition-referral/background-information/prevalence/ (accessed 2023-10-23).
- Sen, R.; Goyal, A.; Hurley, J.A. Seronegative Spondyloarthropathy. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Burton, C.; Cottrell, E.; Edwards, J. Addison’s Disease: Identification and Management in Primary Care. Br J Gen Pract 2015, 65, 488–490. [Google Scholar] [CrossRef]
- Nhsbt-Annual-Report-on-Intestine-Transplantation-202122.Pdf. https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/27817/nhsbt-annual-report-on-intestine-transplantation-202122.pdf (accessed 2023-10-23).
- Delle Fave, G.; Kwekkeboom, D.J.; Van Cutsem, E.; Rindi, G.; Kos-Kudla, B.; Knigge, U.; Sasano, H.; Tomassetti, P.; Salazar, R.; Ruszniewski, P.; all other Barcelona Consensus Conference participants. ENETS Consensus Guidelines for the Management of Patients with Gastroduodenal Neoplasms. Neuroendocrinology 2011, 95, 74–87. [Google Scholar] [CrossRef]
Figure 1.
Pie charts depicting major and minor diagnostic categories. This pie-within-pie chart visualises the distribution of the distinct pathological categories outlined in Table 1. The distribution of normal biopsies, coeliac-associated biopsy categories and non-specific inflammation is represented in the larger pie chart, with a detailed breakdown of abnormal, non-coeliac diagnostic categories depicted in the smaller embedded pie chart. The segment labelled “miscellaneous” in the smaller pie chart comprises minor diagnostic categories containing one case each (common variable immunodeficiency syndrome, amyloidosis, thrombus, pseudolipomatosis, spindle cell tumour, pseudomelanosis, and gangliocytic paraganglioma).
Figure 1.
Pie charts depicting major and minor diagnostic categories. This pie-within-pie chart visualises the distribution of the distinct pathological categories outlined in Table 1. The distribution of normal biopsies, coeliac-associated biopsy categories and non-specific inflammation is represented in the larger pie chart, with a detailed breakdown of abnormal, non-coeliac diagnostic categories depicted in the smaller embedded pie chart. The segment labelled “miscellaneous” in the smaller pie chart comprises minor diagnostic categories containing one case each (common variable immunodeficiency syndrome, amyloidosis, thrombus, pseudolipomatosis, spindle cell tumour, pseudomelanosis, and gangliocytic paraganglioma).
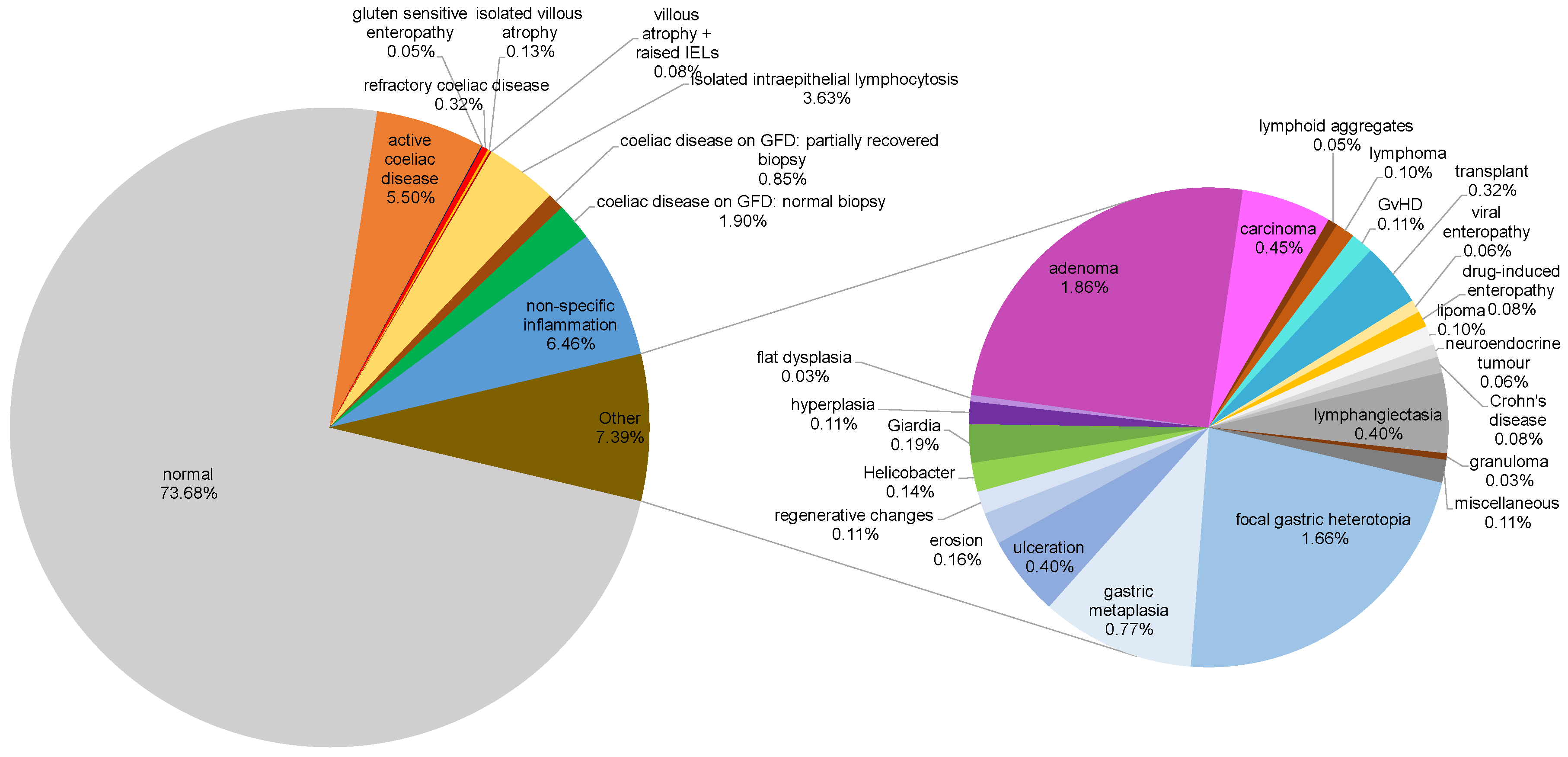

Table 1.
Distribution of diagnostic categories. The total frequency (n, %) of biopsies belonging to each distinct diagnostic category over the audit period of 18 months is shown. The diagnostic category was determined using histopathology reports.
Table 1.
Distribution of diagnostic categories. The total frequency (n, %) of biopsies belonging to each distinct diagnostic category over the audit period of 18 months is shown. The diagnostic category was determined using histopathology reports.
| Classification | Total (n) | Percentage (%) |
| Normal | 4606 | 73.68 |
| Coeliac-associated diagnoses | ||
| Active coeliac disease | 344 | 5.50 |
| Coeliac disease on GFD1: normal biopsy | 119 | 1.90 |
| Coeliac disease on GFD: partially recovered biopsy | 53 | 0.85 |
| Refractory coeliac disease | 20 | 0.32 |
| Isolated villous atrophy | 8 | 0.13 |
| Villous atrophy + raised IELs2 | 5 | 0.08 |
| Gluten sensitive enteropathy | 3 | 0.05 |
| Isolated intraepithelial lymphocytosis | 227 | 3.63 |
| Non-specific inflammation | 404 | 6.46 |
| Neoplastic changes | ||
| Adenoma | 116 | 1.86 |
| Carcinoma | 28 | 0.45 |
| Hyperplasia | 7 | 0.11 |
| Lymphoma | 6 | 0.10 |
| Lipoma | 6 | 0.10 |
| Neuroendocrine tumour | 4 | 0.06 |
| Flat dysplasia | 2 | 0.03 |
| Infections | ||
| Giardiasis | 12 | 0.19 |
| Helicobacter pylori infection | 9 | 0.14 |
| Viral enteropathy | 4 | 0.06 |
| Benign gastric epithelium-related changes | ||
| Focal gastric heterotopia | 104 | 1.66 |
| Gastric metaplasia | 48 | 0.77 |
| Duodenal mucosal surface changes | ||
| Ulceration | 25 | 0.40 |
| Lymphangiectasia | 25 | 0.40 |
| Erosion | 10 | 0.16 |
| Regenerative changes | 7 | 0.11 |
| Autoimmune/Inflammatory conditions | ||
| Crohn's disease | 5 | 0.08 |
| Drug-induced enteropathy | 5 | 0.08 |
| Lymphoid aggregates | 3 | 0.05 |
| Granuloma | 2 | 0.03 |
| Transplant-related diagnoses | ||
| Transplant | 20 | 0.32 |
| Graft versus host disease (GvHD) | 7 | 0.11 |
| Miscellaneous | 7 | 0.11 |
| Total | 6245 | 100 |
1GFD – Gluten-free diet. 2IEL – Intraepithelial lymphocytes.
Table 2.
Keywords associated with certain abnormal, non-coeliac diagnostic entities.
| Biopsy diagnostic category* | Clinical keywords |
| Adenoma | Gastrointestinal bleeding, familial adenomatous polyposis (FAP), polyp or papillary tumours on endoscopy |
| Amyloidosis | Systemic infiltrative disease |
| Carcinoma | Jaundice, gastrointestinal bleeding, bowel obstruction, mass or dilated bile duct on imaging or endoscopic examination, previous diagnosis of malignancy of any organ |
| Common variable immunodeficiency | Background of immunodeficiency syndrome, opportunistic infections (norovirus in our data) |
| Crohn’s disease | Previous diagnosis of Crohn’s disease, stricture, fistula |
| Drug induced enteropathy | Established autoimmune disease on immunomodulators/NSAIDs* |
| Flat (non-adenoma) dysplasia | Gastrointestinal bleeding, necrotic ulcer |
| Focal gastric heterotopia | Polyp on endoscopy |
| Gastric metaplasia | Polyp on endoscopy |
| Giardia | Iron deficiency anaemia, weight loss, abdominal pain |
| Granuloma | History of tuberculosis or Crohn’s disease |
| Hyperplasia without dysplasia | Polyp on endoscopy |
| Lipoma | Nodule on endoscopy |
| Lymphangiectasia | Gastrointestinal bleeding, ill-defined mass on endoscopy |
| Lymphoid aggregates | Mass on endoscopy |
| Lymphoma | Duodenal mass, gastrointestinal bleeding, previous diagnosis of lymphoma |
| Neuroendocrine tumour | Nodule/polyp |
| Ulceration | Gastrointestinal bleeding, abnormal barium study, relevant drug history (NSAIDs†) |
| Viral enteropathy | Immune suppression |
* - This list is not exhaustive due to some diagnostic categories having too few numbers and/or inadequate clinical information. †NSAID – Non-steroidal anti-inflammatory drug.
Table 3.
Demographic and clinical characteristics of patients with isolated intraepithelial lymphocytosis.
Table 3.
Demographic and clinical characteristics of patients with isolated intraepithelial lymphocytosis.
| Characteristic | Finding (n = 227) |
| Median age in years (standard deviation) | 49 (17.72) |
| Female sex (%) | 163 (71.81) |
| Male sex (%) | 64 (28.19) |
| Indications for biopsy (%) | |
| Iron deficiency anaemia | 108 (47.58) |
| Diarrhoea | 44 (19.38) |
| Abdominal pain | 32 (14.10) |
| Weight loss | 33 (14.54) |
| Dyspepsia | 24 (10.57) |
| Reflux | 16 (7.05) |
| Nausea or vomiting | 9 (3.96) |
| Folate deficiency | 9 (3.96) |
| Nonspecific altered bowel movements | 8 (3.52) |
| Dysphagia | 8 (3.52) |
| Bloating | 7 (3.08) |
| Constipation | 4 (1.76) |
| Vitamin B12 deficiency | 4 (1.76) |
| No information provided | 23 (10.13) |
Table 4.
Features suspicious for CeD in 33 (28.94%) of 227 cases of isolated intraepithelial lymphocytosis. Percentage stated in brackets is relative to the 33 cases with features suspicious of CeD.
Table 4.
Features suspicious for CeD in 33 (28.94%) of 227 cases of isolated intraepithelial lymphocytosis. Percentage stated in brackets is relative to the 33 cases with features suspicious of CeD.
| Characteristic | Finding (n = 33) |
| Median age in years (standard deviation) | 48 (16.63) |
| Female sex (%) | 23 (69.70) |
| Male sex (%) | 10 (30.30) |
| Integrated clinical diagnosis of coeliac disease (%) | n=24 |
| Prior to biopsy | 9 (27.27) |
| Subsequent to biopsy | 13 (39.39) |
| After further biopsy | 2 (6.06) |
| Features strongly suspicious for coeliac disease (%) | n=9 |
| positive IgA(tTG) & positive EMA | 5 (15.15) |
| positive IgA(tTG) & negative/missing EMA | 4 (12.12) |
Table 5.
Comorbidities among patients with isolated intraepithelial lymphocytosis and their prevalence in the UK population.
Table 5.
Comorbidities among patients with isolated intraepithelial lymphocytosis and their prevalence in the UK population.
| Associated Condition | Number of Cases, n (%)(N = 227) | Prevalence in UK Population (from published studies) |
| Proton pump inhibitor use | 26 (11.45) | 18.04% [44] |
| NSAID1 use | 18 (7.93) | Variable [45] |
| Helicobacter pylori infection | 12 (5.29) | Up to 35% [46] |
| Irritable bowel disease | 9 (3.96) | 10 – 20% [47] |
| Hypothyroidism | 8 (3.52) | 2% [48] |
| Graves’ disease | 6 (2.64) | 0.75% [49] |
| Microscopic colitis | 4 (1.76) | 0.1% [50] |
| Pernicious anaemia | 3 (1.32) | 0.05 – 0.2% [51] |
| Crohn’s disease | 3 (1.32) | 0.27% [52] |
| Rheumatoid arthritis | 3 (1.32) | 1% [53] |
| Ankylosing spondylitis | 3 (1.32) | 0.05 – 0.2% [54] |
| Gastrointestinal adenocarcinoma | 3 (1.32) | Variable [55,56] |
| Ulcerative colitis | 2 (0.88) | 0.39% [52] |
| Seronegative spondyloarthropathy | 2 (0.88) | 0.5 – 1.9% [57] |
| Addison’s disease | 2 (0.88) | 0.01% [58] |
| Transplanted ileum and colon | 1 (0.44) | 19 cases in 2018-19 [59] |
| Duodenal neuroendocrine tumour | 1 (0.44) | 0.00017% [60] |
1NSAID – Non-steroidal anti-inflammatory drug.
Table 6.
Miscellaneous abnormal laboratory investigations in patients with isolated intraepithelial lymphocytosis.
Table 6.
Miscellaneous abnormal laboratory investigations in patients with isolated intraepithelial lymphocytosis.
| Abnormal Laboratory Test | Number of Cases, n |
| Elevated faecal calprotectin | 37 |
| Elevated ESR1 | 17 |
| Elevated CRP2 | 15 |
| IgA3 deficiency | 10 |
| Elevated ANA4 | 8 |
| Elevated rheumatoid factor | 7 |
| Elevated p-ANCA5 | 3 |
| Elevated anti-cyclic citrullinated protein | 2 |
| Elevated c-ANCA | 1 |
| Elevated anti-U1 RNP6 | 1 |
1ESR – Erythrocyte sedimentation rate. 2CRP – C-reactive protein. 3IgA – Immunoglobin. 4ANA – Antinuclear antibody. 5ANCA – Antineutrophil cytoplasmic antibody. 6Anti-U1 RNP - Antibody to U1 ribonucleoprotein.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



