
Submitted:
29 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
Background/Objectives: Normal remodeling of the extracellular matrix of the endometrium is a necessary condition for implantation of a blastocyst. We evaluated whether the use of histochemical «reticulin-collagen» staining can improve the assessment of the extracellular matrix of the middle secretory endometrium in recrudescent clinical/biochemical pregnancy losses in comparison with ultrasound and routine histological examination. Methods: We compared the histochemical pattern of «reticulin-collagen» endometrial biopsy (21st day of the cycle) with ultrasonography and standard histological examination of the endometrium in groups: (1) fertile women with gravity≥2, (gravity=parity) and (2) women with two or more clinical/biochemical pregnancy losses. Results: NP with ordered reticulin fibers forming cellular structures was determined in 92% of biopsies with physiological reproductive status and 44% of biopsies with recrudescent reproductive failures (p<0.05). Despite the fact that there were no differences in ultrasonography and standard histological examination between the groups (p>0.05). Histochemical pattern with disordered abnormal noodle-like reticulin fibers was more common in recrudescent reproductive failures (56%) than in physiological reproductive status (8%) (p<0.001), despite the fact that aNPS was detected only in recrudescent reproductive failures, and in physiological reproductive status was not detected (p<0.00001). Conclusions: We determined the histochemical pattern of the extracellular matrix of the endometrium by the type of «reticulin-collagen», associated in our study with recrudescent clinical/biochemical pregnancy losses, with improved predictability compared to ultrasonography and standard histological examination. We propose to use the method of histochemical evaluation of the «reticulin-collagen» pattern in order to stratify a group of women of fertile age with a risk of reproductive failures.
Keywords:
collagen
; extracellular matrix
; middle secretory endometrium
; histochemistry
; histology
; ultrasonography
; clinical and biochemical pregnancy loss
1. Introduction
The endometrium is a unique tissue that plays an important role in reproduction. Its functional transformation throughout the menstrual cycle provides optimal conditions for embryo implantation. This process includes several critical stages: primary contact with the endometrium, introduction into the stroma, and maintenance of trophoblast invasion [1,2,3]. Successful completion of these stages depends on a strictly regulated uterine microheart, in which the extracellular matrix acts as a key modulator. The endometrial extracellular matrix is a dynamic structure that forms a mechanical and biochemical environment for cellular adhesion, migration, and differentiation [4,5,6,7]. Among its components, collagen plays a special role, determining its biomechanical properties [8,9,10]. Collagen I forms strong fibrils that increase tissue rigidity, reticulin is characterized by increased elasticity and immaturity of the structure. The balance between these collagen types is important for the regulation of tissue stiffness and the stability of the extracellular matrix structure [11,12,13]. In addition, collagen affects a wide range of cellular processes, including cell migration and differentiation, as well as limiting excessive trophoblast invasion [14,15,16].
Scientific studies show that changes in collagen expression in the endometrium are associated with reproductive losses, including implantation failures [17,18,19,20]. These changes can also disrupt the process of transformation of stromal fibroblasts into the decidual phenotype - a key stage of successful implantation [21,22,23]. Immunological, transcriptomic and proteomic studies have shown that the endometrium in miscarriage and infertility has structural and functional abnormalities compared to normally functioning endometrium at the same stage of the menstrual cycle [24,25,26,27,28,29,30,31]. Furthermore, accumulating data indicate that changes in the endometrial microenvironment include increased activity of matrix metalloproteinases leading to excessive collagen degradation [24,32]. Such structural and molecular changes contribute to the maintenance and prolongation of adverse changes, which may lead to persistent changes in the extracellular matrix.
Despite significant advances in the study of the endometrial extracellular matrix, the identification of its microstructural histochemical features remains a challenge in routine clinical practice. Traditional diagnostic methods such as ultrasonography and standard histology have limited sensitivity for detecting microstructural changes in the extracellular matrix in reproductive dysfunction. The present study aims to fill one aspect of this gap. We describe histochemical patterns of the extracellular matrix with an assessment of the distribution of reticulin and collagen in midsecretory phase endometrial biopsies. By comparing the reticulin-collagen histochemical pattern in women with physiological reproductive status and in women with recurrent reproductive losses, we present evidence for the utility of this diagnostic approach for stratifying women at risk of reproductive failure.
2. Materials and Methods
2.1. Study Design and Inclusion/Exclusion Criteria
Here we present cross-blind research conducted by comparing the histochemical pattern of the endometrium with ultrasound characteristics and the results of a standard histological examination of the endometrium of the middle stage of the secretion phase in groups of fertile women with physiological reproductive status and recrudescent reproductive failures. Patients were recruited between January and May 2024. Written informed consent was obtained from all patients before endometrial sampling. All methods were performed in accordance with the Declaration of Helsinki. The study was approved by the Local Bioethics Commission of the NCJSC “Karaganda Medical University” (Protocol No. 1 of 29.12.2023).
We formed two groups to study the histochemical pattern of the endometrium:
The group of women with physiological reproductive status (group 1) consisted of fertile women with at least two pregnancies with a live fetus delivery in the anamnesis (the number of pregnancies was equal to the number of births).
The group of women with recrudescent reproductive failures (group 2) consisted of fertile women with at least two clinical or biochemical pregnancy losses or at least two unsuccessful cycles of extracorporal fertilization with embryos of good quality.
Clinical data were obtained from medical records in a complex medical information system.
Exclusion criteria: (1) women under 20 years of age or over 40 years of age, body mass index (BMI) >29.9 kg/m2; (2) congenital uterine abnormalities or acquired uterine diseases, including endometrial polyps, submucous myomas, uterine synechias, and adenomyosis; (3) chronic endometritis; (4) hydrosalpinx; (5) positive antibodies to lupus anticoagulant and anticardiolipin; (6) gynecological operations in the preceding two months, intrauterine device or any form of hormonal contraception during the six months preceding the study; (7) genetic abnormalities of the fetus; (8) elevated or decreased levels of thyroid stimulating hormone (TSH), follicle-stimulating hormone (FSH) or luteinizing hormone (LH), estradiol (E2) (9) polycystic ovary syndrome.
In our study, the physiological reproductive status was defined as the ability to achieve clinical pregnancy without assisted reproductive technologies and with a live fetus delivery.
In our study, reproductive failure was defined as the absence of pregnancies (infertility 1 or infertility 2 type) or spontaneous termination of clinical pregnancy (loss of pregnancy after spontaneous conception, assisted reproductive technologies, ectopic pregnancy, hydatidiform mole) or biochemical pregnancy (failure of implantation).
Biochemical pregnancy is a pregnancy diagnosed based on a set of signs: (1) β-HCG (<100 mlU/ml); (2) a rapid drop in the concentration of β-HCG in urine or serum [33].
Clinical pregnancy is a pregnancy diagnosed by ultrasound imaging of one or more intrauterine embryos or obvious clinical signs of intrauterine pregnancy [33].
Stimulated cycles (SC) is a pharmacological therapy in a woman to form regular ovulatory cycles [34].
Natural cycles (NC) are menstrual cycles without pharmacological drug usage [34].
Assisted reproductive technologies involve in vitro processing of human oocytes and spermatozoa or embryos for reproduction [33].
2.2. Sample Size Calculation
The formula for comparing two independent proportions was used to calculate the sample size, assuming a significance level of 5% and a test power of 80%. The initial proportions for the two groups were p1 = 0.70 (physiological reproductive status group) and p2 = 0.40 (recurrent reproductive loss group), based on the results of the preliminary analysis of our pilot study, which resulted in an estimated sample size of 40 participants in each group. To account for possible dropouts or exclusions, the sample was increased by 20%, after which the result was rounded to the nearest ten. As a result, the total sample size was 100 participants, equally distributed between the two groups.
2.3. Methodology of Ultrasound Assessment of the Endometrium
A General Electric Voluson E8 ultrasound system with a 2D vaginal sensor with a 5-8 MHz frequency was used for ultrasonography examination. All ultrasonography studies were conducted by the same doctor using the same ultrasound device.
Transvaginal ultrasonography was performed in the morning before the endometrial biopsy. The estimated parameters included the thickness of the endometrium [37,38,39,40], the homogeneity/heterogeneity of the echo of the functional layer of the endometrium [37,38,40,41] with the presence/absence of a central echogenic line of the endometrium [42] according to the approved protocol.
The thickness of the endometrium was evaluated as the distance between the border of the endometrium and the myometrium of the anterior and posterior walls of the uterus, measured at a distance of 2 cm from the uterine fundus in the projection of the median longitudinal axis of the uterus. The measurement was carried out three times, and the average value was calculated. Images of the endometrium in the longitudinal direction were taken on the 21st day of the cycle. Clinicians examined the pattern and thickness of the endometrium on the day of the examination. After that, two researchers re-evaluated the endometrial echo simultaneously to assess the homogeneity and visibility of the median line.
2.4. Methods of Endometrial Biopsy Sampling and Their Histological Examination
All endometrial biopsies were taken on the 21st day of the cycle, on an outpatient basis, using a suction curette (Pipelle de Cornier, Prodimed, Neuillyen Thelle, France). Biopsies were taken from the fundus and upper part of the anterior and posterior walls of the uterus to assess the zones of maximum physiological development [47].
After fixation with 10% formalin at 4 °C for 24 hours, sections with a thickness of 5 microns were stained at room temperature according to standard protocols with hematoxylin and eosin (H&E), Masson trichrome [48] and Gomori’s silver plating [49].
Morphometric analysis of histological preparations was carried out blindly by two independent pathologists. In case of disagreement, a consensus diagnosis was made.
The main morphometric measurements and photographs were carried out using a light microscope and digital color microphotography with «Image» software. The material with an area of more than 1 cm2 was considered a sufficient volume for the study.
Histological examination was performed according to a standard established protocol (Mayer’s hematoxylin, Bio-Optica (Italy)).
2.4.1. Glandular Epithelium
The pattern of the glandular epithelium of the endometrium was evaluated using established criteria [50,51]. When dating the endometrium, the days of the menstrual cycle and histological dating criteria were considered [50,52]. The histological diagnosis of the glandular epithelium pattern mismatch of the middle stage of secretion was defined as the asynchronous development of the glands with a delay/advance of the cycle day of more than 3 days [53].
2.4.2. Pinopods
Pinopods are cytoplasmic evagination of the apical surface of the cytosolic membrane of the glandular epithelium of the endometrium [54,55,56,57].
According to the relative number of pinopods, the micropreparations were divided into two subgroups:
- numerous, densely packed microvilli occupying most (>50%) of the apical membrane of epithelial cells;
- few rare microvilli occupying less than half (<50%) of the apical membrane of epithelial cells [56].
Histochemical evaluation of the endometrial extracellular matrix by the reticulin-collagen pattern
A histochemical examination was carried out to evaluate the extracellular matrix of the endometrium according to the «reticulin-collagen» phenotype.
2.4.3. Reticulin Fibers of the Extracellular Matrix
The histochemical examination was carried out by Gomori’s silver plating (a kit of Reticulum stains (modified Gomori’s) (ab236473), Bio-Optica (Italy)) according to the standard research protocol. Reticulin fibers were defined as black or dark brown fibers with gray nuclei.
2.4.4. Collagen Fibers of the Extracellular Matrix
The histochemical examination was carried out by staining (Trichrome Stain Kit (Connective Tissue Stain) (ab150686), Bio-Optica (Italy)) according to the standard research protocol. Collagen fibers were defined as dark blue fibers with black nuclei.
2.4.5. Interpretation of the Histochemical Pattern of the Extracellular Matrix of the Endometrium by the Reticulin-Collagen Phenotype
The histochemical pattern was determined under a light microscope at x100 magnification.
The normal typical pattern of remodeling of the extracellular matrix of the endometrium of the middle stage of the secretion phase according to the type «reticulin-collagen» (NP) was defined as reticulin fibers that were arranged in an orderly manner, forming clear cellular structures; collagen fibers are thin filamentous ordered, located mainly around blood vessels and glands. The pattern prevails over more than 70% of the histological section.
Abnormal remodeling of the extracellular matrix of the endometrium of the middle stage of the secretion phase according to the «reticulin-collagen» type has two phenotypes: (1) abnormal noodle-like pattern without collagenosis (aNP); (2) abnormal noodle-like pattern with collagenosis.
Abnormal noodle-like pattern without collagenosis (aNP) was defined as a pattern in which reticulin fibers take on a wavy, tortuous shape, resembling “boiled noodles”. These fibers appear chaotically intertwined, wavy, forming loops, turns and twists with areas of rarefaction and disorganization (Figure 2g). Importantly, collagen I fibers remain thin, filiform and uniformly distributed in the endometrial stroma around blood vessels and glands, without evidence of focal or diffuse deposits of dense homogeneous collagen masses (Figure 2h). This reticulin pattern must occupy more than 30% of the histological section to meet the diagnostic criteria for aNP.
Abnormal noodle-like pattern with collagenosis (aNPC) – is characterized by a combination of changes in the reticulin structure (noodle-like pattern) and clusters of collagen fibers. A distinctive feature is the presence of focal or diffuse dense deposits of homogeneous masses of collagen I in the endometrial stroma (Figure 2l). These changes occupy more than 30% of the area of the histological section and reflect significant changes in the structure of the extracellular matrix.
The patterns are determined under magnification x100 for a general overview and x400 for a detailed assessment of the morphological features of reticulin and collagen fibers.
2.5. Statistical Analysis
The obtained data were subjected to statistical processing using parametric and nonparametric analysis methods. The analysis, systematization and visualization of the obtained results were carried out using the IBMSPSS Statistics v.22 program (StatSoft, Inc., USA). Quantitative variables were initially analyzed using the Shapiro-Wilk test to determine the normality of distribution using the Levene test to check the homogeneity of variances. For quantitative characteristics, if the distribution was recognized as normal, the mean, standard deviation and 95% confidence interval (95%CI) were calculated. Sets of quantitative indicators, with a different distribution, were described using the median (Me) and the upper and lower quartiles (Q1-Q3). Nominal data are presented as absolute values and percentages. To compare the frequencies of distribution by qualitative characteristics between groups, the chi-square statistical test with Yates’ correction or Fisher’s exact test was used. Proportions are presented with 95% confidence intervals (CI) calculated by the Clopper-Pearson method. To compare independent populations in cases where there were no signs of normal data distribution, the Mann-Whitney U test was used. When comparing mean values in normally distributed populations of quantitative data, the independent Student’s t-test was calculated. A value was considered statistically significant at p < 0.05.
3. Results
3.1. Demographic and Clinical Characteristics of the Study Groups
Demographic and clinical baseline characteristics of women from groups with physiological reproductive status and recrudescent reproductive failures are presented in Table 1.
The groups were comparable in age, BMI, and cycle duration and did not differ in serum levels of TSH, FSH, LH, and E2 measured on the 2nd or 3rd day of the menstrual cycle. At the same time, women with recrudescent reproductive failures had a more significant number of clinical and biochemical pregnancies in the anamnesis and, in 34 (68%) cases, had stimulated cycles.
3.2. Characterization of Histochemical Patterns of Reticulin and Collagen in the Endometrial Extracellular Matrix
The histochemical pattern of endometrial extracellular matrix remodeling according to the «reticulin-collagen» type is demonstrated in Table 2 and Figure 1 and Figure 2.
In 46(92%) (95% Cl:82.2-97.1%) endometrial biopsies of women with physiological reproductive status, NP was determined in 4(8%) (95% Cl:3.0-17.9%) aNP biopsies; there were no cases with aNPS in this group.
In the group of women with recrudescent reproductive failures, NP was detected in 22(44%) (95% Cl:30.6-58.2%) biopsies, of them with NC 7(28.6%), with SC 15(71.4%). aNP was observed in 21(42%) (95% Cl:28.2-55.9%) biopsies, of them with NC 6(28.6%), with SC 15(71.4%). aNPC in 7 (14%) biopsies, of them with NC 3(42.9%), with SC 4(57.1%).
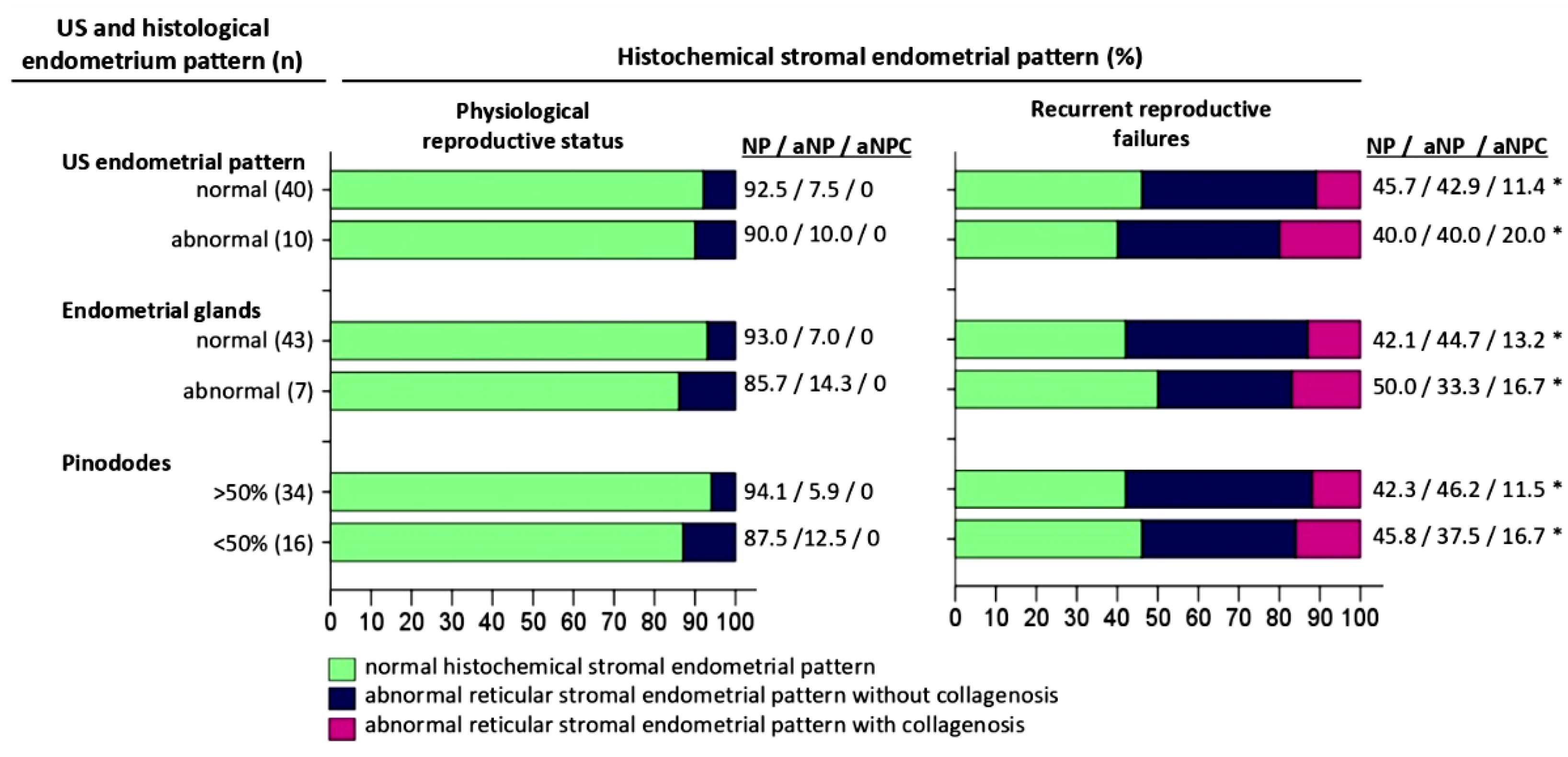
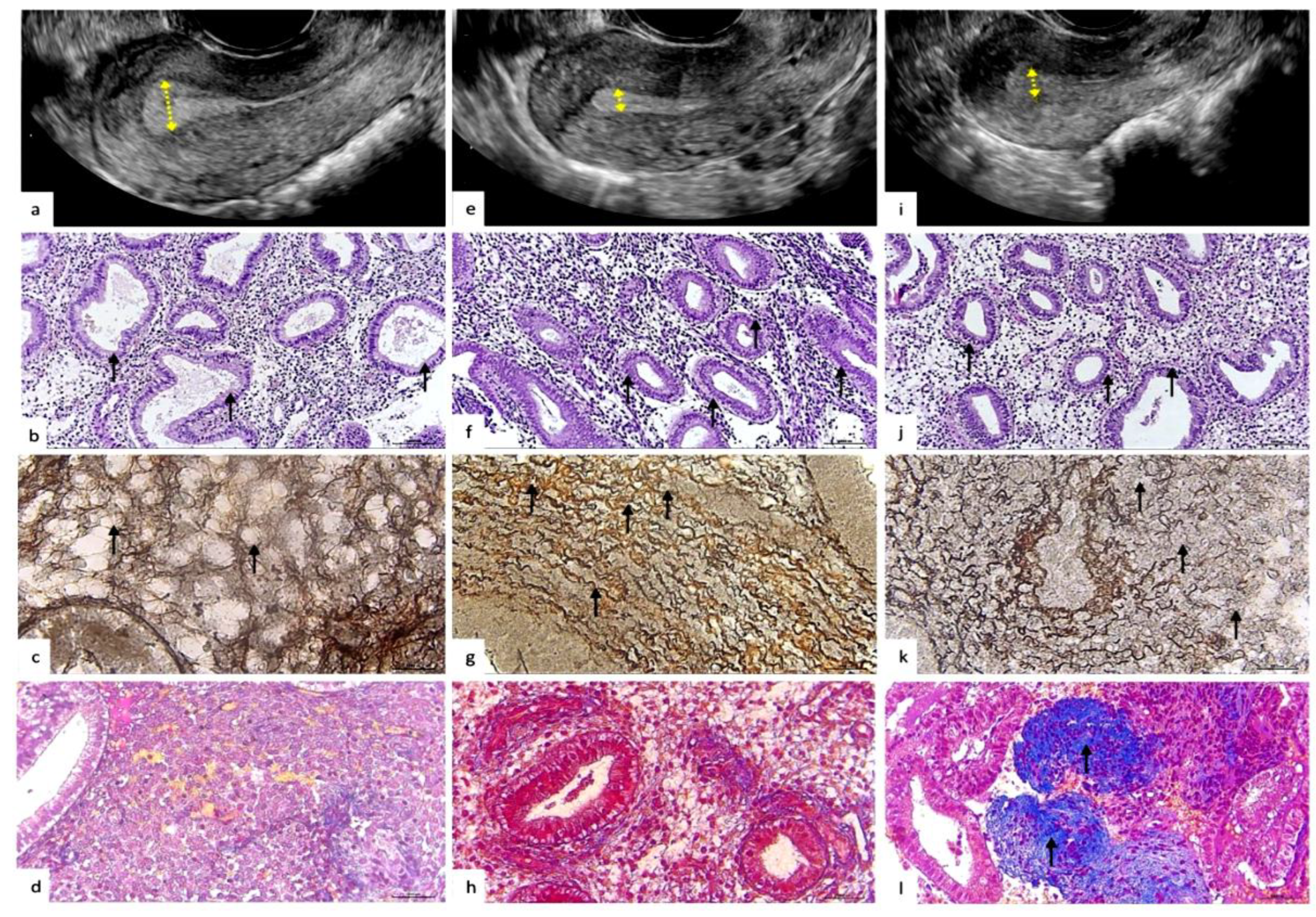
Figure 1.
Comparative characteristics of histochemical pattern, ultrasound and histological pattern of the endometrium from the middle stage secretion phase of menstrual cycle. Abbreviations: US – ultrasonografic investigation, NP - normal histochemical “reticulin-collagen”stromal endometrial pattern, aNP - abnormal reticular stromal endometrial pattern without collagenosis, aNPC - abnormal reticular stromal endometrial pattern with collagenosis (a) Description of what is contained in the first panel; (b) Description of what is contained in the second panel. Figures should be placed in the main text near to the first time they are cited. Statistically significant difference versus Physiological reproductive status (p<0.05).
Figure 1.
Comparative characteristics of histochemical pattern, ultrasound and histological pattern of the endometrium from the middle stage secretion phase of menstrual cycle. Abbreviations: US – ultrasonografic investigation, NP - normal histochemical “reticulin-collagen”stromal endometrial pattern, aNP - abnormal reticular stromal endometrial pattern without collagenosis, aNPC - abnormal reticular stromal endometrial pattern with collagenosis (a) Description of what is contained in the first panel; (b) Description of what is contained in the second panel. Figures should be placed in the main text near to the first time they are cited. Statistically significant difference versus Physiological reproductive status (p<0.05).
Figure 2.
Representative ultrasonographic, histological and histochemical endometrium patterns from physiological and pathological reproductive status. a-d: Ultrasound and histopathological pattern of the endometrium with normal secretory transformation for the middle stage of the secretory phase ovarian cycle. a - Ultrasonography. Homogeneous echogenic endometrium, endometrial thickness – 12 mm (arrows). Echogenic pattern is typical for the secretory phase of the menstrual cycle. b - Histopathological pattern. Convoluted endometrial glands with pseudostratified nuclei and vacuolated cytoplasm, distinct subnuclear vacuoles located predominantly apically (arrows). The pattern of the glandular epithelium corresponds to the middle stage of the secretion phase. H&E staining: x100. c - Histochemical pattern of stromal reticular fibers (collagen type III). Reticulin fibers are arranged in an orderly manner, forming clear cellular structures; compartmented reticular stromal structure with formation of endometrial stromal channels (arrows). Gomori’s staining: x400. d - Histochemical pattern of stromal collagen (collagen type I). Thin filamentous collagen fibers located in the stroma of the endometrium (arrows). Masson’s trichrome staining: x100. e-l: Ultrasound and histopathological pattern of the endometrium with defective/insufficient and irregular secretory transformation of the glandular and stromal compartments. e,i - Ultrasonography. Thin endometrium, thickness 5.5mm and 6.5mm, respectively (arrows). f,j - Histopathological pattern. Endometrial glands with pseudostratified nuclei and vacuolated cytoplasm and distinct parabasal vacuoles (arrows). The pattern of glandular epithelium with delayed secretory transformation, corresponds to the early stage of the secretion phase. H&E staining: x100. g,k - Histochemical pattern of stromal reticular fibers (collagen type III). g - Reticulin fibers are disordered, wave-like, tortuous, “noodle-like” pattern (arrows). k - Reticulin fibers with diffuse edema with microfragmentation and areas of disorganization (arrows). Gomori’s staining: x400. h,l - Histochemical pattern of stromal collagen (collagen type I). h – Normal fine thread-like ordered collagen fibers, located mainly around the vessels and glands. l – Abnormal foci of periglanduar and perivascular deposition of homogeneous collageneous masses (arrows). Masson’s trichrome staining: x100.
Figure 2.
Representative ultrasonographic, histological and histochemical endometrium patterns from physiological and pathological reproductive status. a-d: Ultrasound and histopathological pattern of the endometrium with normal secretory transformation for the middle stage of the secretory phase ovarian cycle. a - Ultrasonography. Homogeneous echogenic endometrium, endometrial thickness – 12 mm (arrows). Echogenic pattern is typical for the secretory phase of the menstrual cycle. b - Histopathological pattern. Convoluted endometrial glands with pseudostratified nuclei and vacuolated cytoplasm, distinct subnuclear vacuoles located predominantly apically (arrows). The pattern of the glandular epithelium corresponds to the middle stage of the secretion phase. H&E staining: x100. c - Histochemical pattern of stromal reticular fibers (collagen type III). Reticulin fibers are arranged in an orderly manner, forming clear cellular structures; compartmented reticular stromal structure with formation of endometrial stromal channels (arrows). Gomori’s staining: x400. d - Histochemical pattern of stromal collagen (collagen type I). Thin filamentous collagen fibers located in the stroma of the endometrium (arrows). Masson’s trichrome staining: x100. e-l: Ultrasound and histopathological pattern of the endometrium with defective/insufficient and irregular secretory transformation of the glandular and stromal compartments. e,i - Ultrasonography. Thin endometrium, thickness 5.5mm and 6.5mm, respectively (arrows). f,j - Histopathological pattern. Endometrial glands with pseudostratified nuclei and vacuolated cytoplasm and distinct parabasal vacuoles (arrows). The pattern of glandular epithelium with delayed secretory transformation, corresponds to the early stage of the secretion phase. H&E staining: x100. g,k - Histochemical pattern of stromal reticular fibers (collagen type III). g - Reticulin fibers are disordered, wave-like, tortuous, “noodle-like” pattern (arrows). k - Reticulin fibers with diffuse edema with microfragmentation and areas of disorganization (arrows). Gomori’s staining: x400. h,l - Histochemical pattern of stromal collagen (collagen type I). h – Normal fine thread-like ordered collagen fibers, located mainly around the vessels and glands. l – Abnormal foci of periglanduar and perivascular deposition of homogeneous collageneous masses (arrows). Masson’s trichrome staining: x100.
3.3. Comparative Analysis of Histochemical Patterns of the Endometrial Extracellular Matrix and Ultrasonography Endometrial Pattern
In the group with physiological reproductive status in 40(80%) (95% Cl:73.7-88.9%) women, a homogeneous endometrium with central echogenic line and thickness of more than 7 mm was determined by ultrasonography examination (Figure 2,а), of them with NP 37(92.5%) and aNP 3(7.5%) endometrial biopsies. On the other hand, the ultrasonography pattern did not correspond to the stage of secretion in 10(20%) (95% Cl:10.7-32.4%) biopsies, of them with NP 9(90%) and with aNP 1(10%) cases.
In the group of women with recrudescent reproductive failures, an ultrasonography pattern corresponding to the middle stage of the secretion phase was observed in 35(70%) (95% Cl:58.9-78.3%) cases, of them with NP 16(45.7%), with aNP 15(42.9%), with aNPC 4(11.4%) biopsies; with NC 10(28.6%), with SC 25(71.4%). On the other hand, ultrasonography pattern not corresponding to the middle stage of the secretion phase was detected in 15(30%) (95% Cl:19.7-43.9%) biopsies, of them with NP 6(40%), aNP 6(40%), aNPC 3(20%); with NC 6(40%) and SC 9(60%).
3.4. Comparative Analysis of Histochemical Patterns of Extracellular Matrix and Histological Features of Glandular Epithelium of the Endometrium
The histophenotype of the extracellular matrix of the endometrium of the middle stage of the secretion phase and the histological pattern of the glandular endometrium are presented in Table 4 and Figure 2,b,f,j.
In the group of women with physiological reproductive status 43(86%) (95% Cl:78.9-92.9%) biopsies showed convoluted endometrial glands with pseudo laminated nuclei and vacuolized cytoplasm, clear subnuclear vacuoles located mainly apically with the presence of secretions in the lumen of the glands (Figure 4), of them with NP 40(93%) and aNP 3(7%) endometrial biopsies. The histological pattern of the glandular epithelium did not correspond to the middle phase of the secretion stage in 7(14%) (95% Cl:6.2-26.1%) biopsies, of them with NP 6(85.7%) and aNP 1(14.3%).
In the group of women with recrudescent reproductive failures, in 38(76%) (95% Cl:64.4-84.2%) cases, the histophenotype of the endometrial glands corresponded to the middle stage of the secretion phase (Figure 5), of them with NP 16(42.1%), with aNP 17(44.7%), with aNPC 5(13.2%) biopsies, with NC 11(28.9%) and SC 27(71.1%). Although, the histological pattern of the glands did not correspond to the intermediate stage of the secretion phase in 12(24%) (95% Cl:13.9-37.4%) biopsies, of them with NP 6(50%), with aNP 4(33.3%), with aNPC 2(16.7%); with NC 5(41.7%) and SC 7(58.3%).
3.5. Comparative Analysis of Histochemical Patterns of Extracellular Matrix and the Number of Pinopodia in the Endometrial Epithelium in the Middle of the Secretory Phase
The relative number of the pinopods of the superficial endometrial epithelium are presented in Table 5.
In the group of women with physiological reproductive status pinopods covering most (>50%) of the apical cell membrane were observed in 34(68%) (95% Cl:57.6-77.6%) biopsies, of them with NP 32(94.1%) and aNP 2(5.9%). Pinopods covering a minor part (<50%) of the apical cell membrane were detected in 16(32%) (95% Cl:20.9-43.8%) biopsies, of them with NP 14(87.5%) and aNP 2(12.5%) cases.
In the group of women with recrudescent reproductive failures, pinopods covering >50% of the apical cell membrane were observed in 26(52%) (95% Cl:40.0-63.5%) biopsies, of them with NP 11 (42.3%), aNP 12(46.2%) and aNPC 3(11.5%); with NC 9(34.6%) and SC 17(65.4%) biopsies. On the other hand, pinopods covering less than 50% of the apical membrane were detected in 24(48%) (95% Cl:36.5-60.0%) biopsies, of them with NP 11(45.8%), aNP 9(37.5%), with aNPC 4(16.7%); NC 7(29.2%) and SC 17(70.8%) cases.
4. Discussion
We compared the histochemical pattern of the middle secretory endometrium with the ultrasonography pattern, the histological pattern of glandular epithelium, and relative number of the pinopods between groups of women with recrudescent reproductive failures and physiological reproductive status.
We found that the histochemical pattern of the extracellular matrix of the endometrium of the «reticulin-collagen» type differs in physiological reproductive status and in recrudescent reproductive failures (p<0.05). Thus, we identified two histochemical patterns: the first with ordered reticulin fibers forming clear cellular structures (Figure 2c), associated in more than 90% of cases with physiological reproductive status.
The second type of extracellular matrix is characterized by disordered reticulin fibers that acquire a wavy, tortuous shape, forming loops, turns and twists resembling “boiled noodles” (Figure 2,g) with diffuse rarefactions and areas of disorganization (Figure 2k), which was observed in more than 50% of cases of recurrent reproductive disorders.
In turn, this stromal pattern, that often associated with reproductive failures, has two main phenotypes: (1) abnormal noodle-like pattern without collagenosis (aNP) (Figure 2h); (2) abnormal noodle-like pattern with collagenosis (aNPC) (Figure 2l). We believe that the abnormal histochemical phenotype of reticulin-collagen of the endometrial stroma may reflect the pathological remodeling of the extracellular matrix of the endometrium of the middle stage of the secretion phase.
Further, we found that the abnormal reticulin-collagen pattern of the endometrial stroma was detected in all groups: with physiological reproductive status in less than 10 percent of cases and with recrudescent reproductive failures in more than 50% of cases, despite the fact that pathological remodeling of the extracellular matrix with collagenosis, characterized by focal and diffuse well-visually detecs collagen bundles, was noted only with recrudescent reproductive failures, but with physiological pregnancy no cases of collagenosis were found. Qualitative and quantitative disorders and collagen abnormalities in the stroma were previously described in the intestine with collagenous microscopic colitis [58,59,60] and decidual tissue with clinically unexplained recurrent pregnancy loss [20,61]. It is unclear whether abnormal collagen expression is the cause or result of recrudescent miscarriage, but as previously shown [62,63,64,65], collagen may play an important role in indicating immune tolerance. Furthermore, the adequate remodeling of the collagenous extracellular matrix of the endometrium of the middle phase of the cycle plays an important role in forming a favorable implantation field and the diffusion and perfusion potential of the endometrium for implanted blastocytes. Our findings are consistent with and complement previous studies [30,66] by showing that focal collagen remodeling plays an important role in recurrent reproductive failure. This observation highlights the need for further studies to refine our understanding of the dynamics of interactions between structural components of the endometrial extracellular matrix in the context of reproductive failure.
Further, we showed that in the group with physiological reproductive status, in more than 90% of biopsies, clearly formed mesh-cellular structures of the «honeycomb» type with evenly distributed thin reticulin fibers and single filamentous collagen fibers were determined. Similar structures were described earlier in chorionic villi, represented as stromal channels, the value of which is defined as the formation of connecting links implementing the function of transport and exchange between mother and fetus [67]. We believe that normal remodeling of proteins, in particular reticulin-collagen, the extracellular matrix of the endometrium with physiological reproductive status is necessary for the formation of stromal channels to increase and improve the diffusion potential of the endometrium during implantation of blastocysts. Previously was shown that pronounced edema develops in the endometrial stroma during implantation [68]. In our study, in more than 50% of cases with recrudescent reproductive failures, we found histopathological signs of diffuse edema of the endometrial stroma with fibrinization and disorganization of reticulin and collagen fibers. In contrast, in the group with physiological reproductive status, such a histopattern was absent and characterized only by the stroma’s micro-focal rarefaction. We believe that the normal remodeling of the endometrial matrix is associated not so much with stroma edema as with the formation of a highly specialized stromal skeleton with the presence of stromal channels, and stromal edema highly likely is a pathological structural change in the endometrium, which can mimic the normal ultrasound and histological pattern.
We found that endometrial ultrasonography patterns and histophenotype differed between the groups. In the group with recrudescent reproductive failures, cases were often associated with a thin endometrium (Figure 2e,i,f,j), delayed maturation of the glandular epithelium, and a low number of pinopods in comparison with the endometrium from physiological reproductive status.
The cases with stimulated menstrual cycle and reproductive failures were more often associated with ultrasonographic and histological signs of mature and complete endometrium, in comparison with the subgroup with natural menstrual cycle and reproductive failures. This finding confirms previously published data that hormonal stimulation of the cycle accelerates the endometrium’s maturation and increases the endometrium’s thickness [69,70]. However, statistically significant differences were not found between the hormonal induced and non-induced cycle (p>0.05) when assessing the histochemical phenotype «reticulin-collagen». This may indicate the existence of endogenous factors that play a key role in the pathological regulation of the endometrial extracellular matrix, not directly related to hormonal stimulation, which are manifested in both induced and natural cycles and require further study.
Our study showed significant differences in the histopatterns of the endometrial extracellular matrix in physiological reproductive status and in recurrent reproductive failures. However, it remains unclear whether these changes are the cause of reproductive disorders or their consequence.
Persistent inflammation and hormonal imbalance can initiate structural disorders of the extracellular matrix, creating unfavorable conditions for blastocyst implantation. In particular, proinflammatory cytokines mediate hyperactivity of matrix metalloproteinases, which leads to degradation of key components of the extracellular matrix and disorganization of its structure [71,72,73]. Genetic factors, particularly mutations in genes encoding matrix components such as collagen or matrix metalloproteinases, may also reduce the ability of the endometrium to support blastocyst implantation and trophoblast invasion. On the other hand, implantation failures may trigger compensatory remodeling characterized by excessive collagen accumulation and dysfunctional matrix regulation. This may form a “vicious circle” where abnormalities in the structure of the endometrial extracellular matrix enhance subsequent reproductive failures. Longitudinal studies aimed at studying the dynamics of the histophenotype of the endometrial extracellular matrix at different periods of the menstrual cycle, as well as at different stages of pregnancy planning, are needed to elucidate this relationship in more detail.
We also identified 2 (4%) cases with thin and immature histological and abnormal histochemical endometrial pattern in the group with physiological reproductive status, which were associated with unfavorable pregnancy outcome with placental abruption and intrauterine fetal growth retardation. Previously, several papers showed that the pathological thin and immature endometrium for the phase of menstrual cycle is often associated with antenatal hypoxic-ischemic events in the placenta and fetus [74,75]. Therefore, we believe that pathological remodeling of the extracellular matrix of the endometrium is a high risk factor not only for reproductive failures but also for long-term adverse consequences of pregnancy. However, this statement is speculative and requires further study.
It can be assumed, on the one hand, the discrepancy between endometrial ultrasonography and histopattern may be associated with delay in the growth and maturation of the endometrium; on the other hand, it may be due to the persistence of insufficient endometrial remodeling, which cases may indirectly be indicated with collagenosis of the extracellular matrix in the group with recrudescent reproductive losses, which in our study were not detected with physiological reproductive status.We propose the use of the term «insufficient secretory endometrial transformation», which refers to the structural inconsistency of the glandular or extracellular matrix of the endometrium for the phase of the menstrual cycle according to a combination of ultrasonography, histological and histochemical examination methods of the endometrium and which allows to stratify a group of women with high risk of insufficient/abnormal formation of endometrial implantation platform with structural inconsistence of the epithelial-stromal compartment of the endometrium.
The strengths of this study include comparative characteristics of the histophenotypic pattern of the endometrium of the middle secretory phase in recrudescent reproductive failures and in physiological reproductive status. Limitations of the study include data fluctuations that may be due to the small number of cases in subgroups, as well as the lack of long-term follow-up to assess the impact of the identified histophenotypes on conception and pregnancy outcomes. Conducting multicenter studies with an increased sample size and taking into account different cycle stimulation protocols will increase the representativeness and validity of the results. To clarify the prognostic role of histochemical patterns of the endometrial extracellular matrix, it is necessary to conduct long-term longitudinal studies that will assess the impact of histophenotype on conception, implantation success and pregnancy outcomes. These studies will contribute to the development of a personalized approach in reproductive medicine, clarify the prognostic significance of the identified histophenotypes and can facilitate integration into clinical practice to improve risk stratification and prognosis of reproductive losses.
5. Conclusions
We determined the histochemical pattern of the extracellular matrix of the endometrium by the type of «reticulin-collagen», associated in our study with recrudescent clinical/biochemical pregnancy losses, with improved predictability compared to ultrasonography and standard histological examination. We propose to use the method of histochemical evaluation of the «reticulin-collagen» pattern in order to stratify a group of women of fertile age with a risk of reproductive failures.
Author Contributions
Conceptualization, N.O., D.K., A.T., and Zh.A.; methodology, N.O., D.K., A.T., and Zh.A.; validation, D.K., Ye. K., and I.K.; formal analysis, N.O., R.G., Ye. K., K.M., and I.K.; investigation, N.O., R.G., K.M., Ye. K., and I.K.; resources, D.K., A.T., and Zh.A.; data curation, D.K., A.T., and Zh.A.; writing—original draft preparation, N.O.; writing—review and editing, D.K., A.T., and Zh.A.; supervision, D.K., A.T., and Zh.A.; project administration, N.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All methods were performed in accordance with the Declaration of Helsinki. The study was approved by the Local Bioethics Commission of the NCJSC “Karaganda Medical University” (Protocol No. 1 of 29.12.2023).
Informed Consent Statement
Written informed consent was obtained from all patients before endometrial sampling.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Muter J, Lynch VJ, McCoy RC, Brosens JJ. Human embryo implantation. Development. 2023;150(10):dev201507. [CrossRef]
- Bazer FW, Spencer TE, Johnson GA, Burghardt RC, Wu G. Comparative aspects of implantation. Reproduction. 2009;138(2):195-209. [CrossRef]
- Benagiano G, Mancuso S, Guo SW, Di Renzo GC. Events Leading to the Establishment of Pregnancy and Placental Formation: The Need to Fine-Tune the Nomenclature on Pregnancy and Gestation. Int J Mol Sci. 2023;24(20):15420. Published 2023 Oct 21. [CrossRef]
- O’Connor BB, Pope BD, Peters MM, Ris-Stalpers C, Parker KK. The role of extracellular matrix in normal and pathological pregnancy: Future applications of microphysiological systems in reproductive medicine. Exp Biol Med (Maywood). 2020; 245(13):1163-1174. [CrossRef]
- Pelham RJ Jr, Wang Yl. Cell locomotion and focal adhesions are regulated by substrate flexibility. Proc Natl Acad Sci U S A. 1997;94(25):13661-13665. [CrossRef]
- Xu P, Wang Y, Piao Y, et al. Effects of matrix proteins on the expression of matrix metalloproteinase-2, -9, and -14 and tissue inhibitors of metalloproteinases in human cytotrophoblast cells during the first trimester. Biol Reprod. 2001;65(1):240-246. [CrossRef]
- Liu R, Dai M, Gong G. et al. The role of extracellular matrix on unfavorable maternal–fetal interface: focusing on the function of collagen in human fertility. J Leather Sci Eng 4. 2022(13. [CrossRef]
- Aplin JD, Charlton AK, Ayad S. An immunohistochemical study of human endometrial extracellular matrix during the menstrual cycle and first trimester of pregnancy. Cell Tissue Res. 1988;253(1):231-240. [CrossRef]
- Kisling A, Lust RM, Katwa LC. What is the role of peptide fragments of collagen I and IV in health and disease?. Life Sci. 2019;228:30-34. [CrossRef]
- Kisalus LL, Herr JC, Little CD. Immunolocalization of extracellular matrix proteins and collagen synthesis in first-trimester human decidua. Anat Rec. 1987;218(4):402-415. [CrossRef]
- Tang VW. Collagen, stiffness, and adhesion: the evolutionary basis of vertebrate mechanobiology. Mol Biol Cell. 2020;31(17):1823-1834. [CrossRef]
- Schlunck G, Han H, Wecker T, Kampik D, Meyer-ter-Vehn T, Grehn F. Substrate rigidity modulates cell matrix interactions and protein expression in human trabecular meshwork cells. Invest Ophthalmol Vis Sci. 2008;49(1):262-269. [CrossRef]
- Sternberg AK, Buck VU, Classen-Linke I, Leube RE. How Mechanical Forces Change the Human Endometrium during the Menstrual Cycle in Preparation for Embryo Implantation. Cells. 2021;10(8):2008. Published 2021 Aug 6. [CrossRef]
- Abbas Y, Carnicer-Lombarte A, Gardner L, et al. Tissue stiffness at the human maternal-fetal interface. Hum Reprod. 2019;34(10):1999-2008. [CrossRef]
- Okada H, Tsuzuki T, Murata H. Decidualization of the human endometrium. Reprod Med Biol. 2018;17(3):220-227. Published 2018 Feb 1. [CrossRef]
- Ma Z, Sagrillo-Fagundes L, Mok S, Vaillancourt C, Moraes C. Mechanobiological regulation of placental trophoblast fusion and function through extracellular matrix rigidity. Sci Rep. 2020;10(1):5837. Published 2020 Apr 3. [CrossRef]
- Iwahashi M, Muragaki Y, Ooshima A, Nakano R. Decreased type IV collagen expression by human decidual tissues in spontaneous abortion. J Clin Endocrinol Metab. 1996;81:2925–9. [CrossRef]
- Fu Q, Sun Y, Tao Y, et al. Involvement of the JAK-STAT pathway in collagen regulation of decidual NK cells. Am J Reprod Immunol. 2017;78(6):10.1111/aji.12769. [CrossRef]
- Yoshii N, Hamatani T, Inagaki N, et al. Successful implantation after reducing matrix metalloproteinase activity in the uterine cavity. Reprod Biol Endocrinol. 2013;11:37. [CrossRef]
- Fu Q, Tao Y, Piao H, Du MR, Li DJ. Trophoblasts and decidual stromal cells regulate decidual NK cell functions via interaction between collagen and LAIR-1. Am J Reprod Immunol. 2014;71:368–78. [CrossRef]
- Lucas ES, Dyer NP, Murakami K, et al. Loss of Endometrial Plasticity in Recurrent Pregnancy Loss. Stem Cells. 2016;34(2):346-356. [CrossRef]
- Salker M, Teklenburg G, Molokhia M, et al. Natural selection of human embryos: impaired decidualization of endometrium disables embryo-maternal interactions and causes recurrent pregnancy loss. PLoS One. 2010;5(4):e10287. [CrossRef]
- Salker MS, Nautiyal J, Steel JH, et al. Disordered IL-33/ST2 activation in decidualizing stromal cells prolongs uterine receptivity in women with recurrent pregnancy loss. PLoS One. 2012;7(12):e52252. [CrossRef]
- Potiris A, Alyfanti E, Drakaki E, et al. The Contribution of Proteomics in Understanding Endometrial Protein Expression in Women with Recurrent Implantation Failure. J Clin Med. 2024;13(7):2145. [CrossRef]
- Ticconi C, Pietropolli A, Di Simone N, Piccione E, Fazleabas A. Endometrial Immune Dysfunction in Recurrent Pregnancy Loss. Int J Mol Sci. 2019;20(21):5332. [CrossRef]
- You S, Zhu Y, Li H, et al. Recombinant humanized collagen remodels endometrial immune microenvironment of chronic endometritis through macrophage immunomodulation. Regen Biomater. 2023;10:rbad033. Published 2023 Apr 3. [CrossRef]
- Watt FM, Huck WT. Role of the extracellular matrix in regulating stem cell fate. Nat Rev Mol Cell Biol. 2013;14(8):467-473. [CrossRef]
- Wei Y, Deng Z, Yin T. Are we closer to robust predictors of recurrent pregnancy loss by means of integrating different types of omics data?. Expert Rev Mol Diagn. 2024;24(7):561-563. [CrossRef]
- Messaoudi S, El Kasmi I, Bourdiec A, et al. 15 years of transcriptomic analysis on endometrial receptivity: what have we learnt?. Fertil Res Pract. 2019;5:9. [CrossRef]
- Fu X, Guo X, Xu H, et al. Varied cellular abnormalities in thin vs. normal endometrium in recurrent implantation failure by single-cell transcriptomics Reprod Biol Endocrinol. 2024 Aug 27;22(1):109. [CrossRef]
- Davalieva K, Kocarev D, Plaseska-Karanfilska D. Decoding recurrent pregnancy loss: insights from comparative proteomics studies. Biol Reprod. Published online September 17, 2024. [CrossRef]
- Latifi Z, Fattahi A, Ranjbaran A, Nejabati HR, Imakawa K. Potential roles of metalloproteinases of endometrium-derived exosomes in embryo-maternal crosstalk during implantation. J Cell Physiol. 2018;233(6):4530-4545. [CrossRef]
- Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, Rienzi L, Sunde A, Schmidt L, Cooke ID, Simpson JL, van der Poel S. The International Glossary on Infertility and Fertility Care, 2017. Hum Reprod. 2017 Sep 1;32:1786-1801. [CrossRef]
- Li L, Gao DD, Zhang Y, Song JY, Sun ZG. Comparison of Stimulated Cycles with Low Dose r-FSH versus Hormone Replacement Cycles for Endometrial Preparation Prior to Frozen-Thawed Embryo Transfer in Young Women with Polycystic Ovarian Syndrome: A Single-Center Retrospective Cohort Study from China. Drug Des Devel Ther. 2021;15:2805-2813. [CrossRef]
- Shein-Chung Chow, Hansheng Wang, Jun Shao. Sample Size Calculations in Clinical Research. New York: Marcel Dekker; 2003.
- Kang H. Sample size determination and power analysis using the G*Power software. J Educ Eval Health Prof. 2021;18:17. [CrossRef]
- Gonen Y, Casper RF, Jacobson W, Blankier J. Endometrial thickness and growth during ovarian stimulation: a possible predictor of implantation in in vitro fertilization. Fertil Steril. 1989;52(3):446-450. [CrossRef]
- Zhao J, Zhang Q, Li Y. The effect of endometrial thickness and pattern measured by ultrasonography on pregnancy outcomes during IVF-ET cycles. Reprod Biol Endocrinol. 2012;10:100. [CrossRef]
- Ma NZ, Chen L, Dai W, Bu ZQ, Hu LL, Sun YP. Influence of endometrial thickness on treatment outcomes following in vitro fertilization/intracytoplasmic sperm injection. Reprod Biol Endocrinol. 2017;15(1):5. [CrossRef]
- McWilliams GD, Frattarelli JL. Changes in measured endometrial thickness predict in vitro fertilization success. Fertil Steril. 2007;88(1):74-81. [CrossRef]
- Zhao J, Zhang Q, Wang YG, Li YP. Endometrial pattern, thickness and growth in predicting pregnancy outcome following 3319 ivf cycle. Reprod BioMed Online. 2014;29:291-298. [CrossRef]
- Zhang CH, Chen C, Wang JR, et al. An endometrial receptivity scoring system basing on the endometrial thickness, volume, echo, peristalsis, and blood flow evaluated by ultrasonography. Front Endocrinol (Lausanne). 2022;13:907874. [CrossRef]
- Forrest TS, Elyaderani MK, Muilenburg MI, Bewtra C, Kable WT, Sullivan P. Cyclic endometrial changes: US assessment with histologic correlation. Radiology. 1988;167(1):233-237. [CrossRef]
- Li TC, Nuttall L, Klentzeris L, Cooke ID. How well does ultrasonographic measurement of endometrial thickness predict the results of histological dating?. Hum Reprod. 1992;7(1):1-5. [CrossRef]
- Singh N, Bahadur A, Mittal S, Malhotra N, Bhatt A. Predictive value of endometrial thickness, pattern and sub-endometrial blood flows on the day of hCG by 2D doppler in in-vitro fertilization cycles: A prospective clinical study from a tertiary care unit. J Hum Reprod Sci. 2011;4(1):29-33. [CrossRef]
- Taizhanova, D.Z., Zubkov, D.V., Komlichenko, E.V., Magalov, I.S., Sorokina, M.A., Bespalova, N.V., Maidanova, Z.O., The possibilities of adverse pregnancy outcomes predicting based on laboratory markers of reproductive losses. Medicine and ecology. 202;.77–84. [CrossRef]
- Johannisson E, Parker RA, Landgren BM, Diczfalusy E. Morphometric analysis of the human endometrium in relation to peripheral hormone levels. Fertil Steril. 1982;38(5):564-571. [CrossRef]
- Masson’s Trichrome Staining Protocol for Collagen Fibers. Available online: https://ihcworld.com/2024/01/26/massons-trichrome-staining-protocol-for-collagen-fibers/ (accessed 25.03.2025).
- Reticulum Stain Kit (Modified Gomori’s) For the Histological Visualization of Reticular Fibers. Version 1 Last updated 27 June 2018 ab236473 Available online: https://www.abcam.com/ps/products/236/ab236473/documents/ab236473%20-%20Reticulum%20Stain%20Kit%20(Modified%20Gomori’s)%20v1a%20(website).pdf?srsltid=AfmBOoq1ulkwp1N_1Z2pdyiRwQhqo2CC3FiyCB_n4ad8LHG3DYi7u1GD (accessed 25.03.2025).
- Noyes RW, Hertig AT, Rock J. Dating the endometrial biopsy. Am J Obstet Gynecol. 1975;122(2):262-263. [CrossRef]
- Hendrickson MR, Kempson RL. Decision tree for endometrial dating. In: Benningtoon JL, ed. Surgical pathology of the uterine corpus. Philadelphia: WB Saunders, 1980:80 -5.
- Murray MJ, Meyer WR, Zaino RJ, et al. A critical analysis of the accuracy, reproducibility, and clinical utility of histologic endometrial dating in fertile women. Fertil Steril. 2004;81(5):1333-1343. [CrossRef]
- Dallenbach-Hellweg G. The endometrium of infertility. A review. Pathol Res Pract. 1984;178(6):527-537. [CrossRef]
- Acosta AA, Elberger L, Borghi M, et al. Endometrial dating and determination of the window of implantation in healthy fertile women. Fertil Steril. 2000;73(4):788-798. [CrossRef]
- Jin XY, Zhao LJ, Luo DH, et al. Pinopode score around the time of implantation is predictive of successful implantation following frozen embryo transfer in hormone replacement cycles. Hum Reprod. 2017;32(12):2394-2403. [CrossRef]
- Develioglu OH, Nikas G, Hsiu JG, Toner JP, Jones HW Jr. Detection of endometrial pinopodes by light microscopy. Fertil Steril. 2000;74(4):767-770. [CrossRef]
- Nikas G, Makrigiannakis A, Hovatta O, Jones HW Jr. Surface morphology of the human endometrium. Basic and clinical aspects. Ann N Y Acad Sci. 2000;900:316-324. [CrossRef]
- Boland K, Nguyen GC. Microscopic Colitis: A Review of Collagenous and Lymphocytic Colitis. Gastroenterol Hepatol (N Y). 2017;13(11):671-677.
- Lazenby AJ, Yardley JH, Giardiello FM, Jessurun J, Bayless TM. Lymphocytic (“microscopic”) colitis: a comparative histopathologic study with particular reference to collagenous colitis. Hum Pathol. 1989;20(1):18-28. [CrossRef]
- Yuan L, Wu TT, Zhang L. Microscopic colitis: lymphocytic colitis, collagenous colitis, and beyond. Hum Pathol. 2023;132:89-101. [CrossRef]
- Iwahashi M, Nakano R. Decreased type V collagen expression in human decidual tissues of spontaneous abortion during early pregnancy. J Clin Pathol. 1998;51(1):44-46. [CrossRef]
- Foy M, Anézo O, Saule S, Planque N. PRL-3/PTP4A3 phosphatase regulates integrin β1 in adhesion structures during migration of human ocular melanoma cells. Exp Cell Res. 2017;353(2):88-99. [CrossRef]
- Shi JW, Lai ZZ, Yang HL, et al. Collagen at the maternal-fetal interface in human pregnancy. Int J Biol Sci. 2020;16(12):2220-2234. [CrossRef]
- Rygiel TP, Stolte EH, de Ruiter T, van de Weijer ML, Meyaard L. Tumor-expressed collagens can modulate immune cell function through the inhibitory collagen receptor LAIR-1. Mol Immunol. 2011;49(1-2):402-406. [CrossRef]
- Lv S, Lu C, Li M, et al. The dynamic changes in myocardial collagen metabolism in experimental autoimmune myocarditis rats. Hellenic J Cardiol. 2018;59(4):234-237. [CrossRef]
- Li M, Yao L, Xin M, Gao M. Dysregulation of collagen expression in peri-implantation endometrium of women with high ovarian response. J Obstet Gynaecol Res. 2019;45(5):1035-1044. [CrossRef]
- Kaufmann P, Stark J, Stegner HE. The villous stroma of the human placenta. I. The ultrastructure of fixed connective tissue cells. Cell Tissue Res. 1977;177(1):105-121. [CrossRef]
- Okada Y, Asahina T, Kobayashi T, Goto J, Terao T. Studies on the mechanism of edematous changes at the endometrial stroma for implantation. Semin Thromb Hemost. 2001;27(2):67-77. [CrossRef]
- Saadat P, Boostanfar R, Slater CC, Tourgeman DE, Stanczyk FZ, Paulson RJ. Accelerated endometrial maturation in the luteal phase of cycles utilizing controlled ovarian hyperstimulation: impact of gonadotropin-releasing hormone agonists versus antagonists. Fertil Steril. 2004;82(1):167-171. [CrossRef]
- Corbacioglu A, Baysal B. Effects of steroid hormone levels on the ultrasound appearance of the preovulatory endometrium in controlled ovarian hyperstimulation cycles. Int J Fertil Steril. 2012;5(4):203-206.
- Nissinen L, Kähäri VM. Matrix metalloproteinases in inflammation. Biochim Biophys Acta. 2014;1840(8):2571-2580. [CrossRef]
- Lee HS, Kim WJ. The Role of Matrix Metalloproteinase in Inflammation with a Focus on Infectious Diseases. Int J Mol Sci. 2022;23(18):10546. Published 2022 Sep 11. [CrossRef]
- Chen K, Xu M, Lu F, He Y. Development of Matrix Metalloproteinases-Mediated Extracellular Matrix Remodeling in Regenerative Medicine: A Mini Review. Tissue Eng Regen Med. 2023;20(5):661-670. [CrossRef]
- Pezaro S, Pearce G, Reinhold E. Hypermobile Ehlers-Danlos syndrome during pregnancy, birth and beyond. Br J Midwifery 2018;26:217-23. [CrossRef]
- Ganer Herman H, Volodarsky-Perel A, Ton Nu TN, et al. Pregnancy complications and placental histology following embryo transfer with a thinner endometrium. Hum Reprod. 2022;37(8):1739-1745. [CrossRef]

Table 1.
Demographic and clinical baseline characteristics.
| Patient characteristics | Groups (N-100) | p-value | |
|
Physiological reproductive pattern (n-50) |
Recurrent reproductive failures (n-50) |
||
| Age, mean ± SD | 31.14 ± 4.66 | 32.08 ± 4.37 | 0.236 |
| Body Mass Index (BMI), (kg/m2) | 24.4 (95% СI:23.5-25.3) | 24.9 (95% СI:24.0-25.7) | 0.389 |
| Pregnancies: number and outcomes | |||
| Gravida, median (IQR) | 2 (1) | 3 (1) | 0.002 |
| Clinical pregnancy loss, median (IQR) | 0 (0) | 2 (1) | - |
| Biochemical pregnancy loss, median (IQR) | 0 (0) | 1 (2) | - |
| Number of live births, median (IQR) | 2 (1) | 0 (0) | - |
| Preterm birth, median (IQR) | 1 (2) | 0 (0) | - |
| Term delivery, median (IQR) | 2 (1) | 0 (0) | - |
| Hormons | |||
| TSH (uU/mL) | 2.41 ± 0.86 | 2.62 ± 0.92 | 0.211 |
| Basal FSH (IU/L) | 7.81 (95% СI:7.2-8.4) | 7.49 (95% СI:6.6-8.3) | 0.934 |
| Basal LH (IU/L) | 4.92 ± 2.24 | 4.86 ± 1.42 | 0.667 |
| Basal serum estradiol (E2) (pg/mL) | 39.03 ± 17.48 | 42.40 ± 21.82 | 0.627 |
Abbreviations: IUGR – intrauterine fetal growth restriction, TSH - Thyroid-stimulating hormone, FSH - Follicle-Stimulating Hormone, LH - luteinizing hormone.
Table 2.
Histochemical reticulin-collagen pattern of endometrial extracellular matrix remodeling in the middle stage of the ovarian cycle secretion phase.
Table 2.
Histochemical reticulin-collagen pattern of endometrial extracellular matrix remodeling in the middle stage of the ovarian cycle secretion phase.
| Correspondence to the ovarian cycle | Physiological reproductive status | Recurrent reproductive failures | ||
| Yes | No | Yes | No | |
| Normal reticulin-collagen pattern (NP) |
46(92%) | 4(8%) | 22(44%) | 28(56%)* |
| Natural cycles, n (%) | 46(100%) | 4(100%) | 7(28.6%) | 9(32.1%) |
| Stimulated cycles, n (%) | - | - | 15(71.4%) | 19(67.9%) |
| Pathological stromal reticulin pattern without collagenosis (aNP) |
4(8%) | 46(92%) | 21(42%)* | 29(58%) |
| Natural cycles, n (%) | 4(100%) | 46(100%) | 6(28.6%) | 10(34.5%) |
| Stimulated cycles, n (%) | - | - | 15(71.4%) | 19(65.5%) |
| Pathological stromal reticulin pattern with collagenosis (aNPС) |
0(0%) | 50(100%) | 7(14%)* | 43(86%) |
| Natural cycles, n (%) | - | 50(100%) | 3(42.9%) | 13(30.2%) |
| Stimulated cycles, n (%) | - | - | 4(57.1%) | 30(69.8%) |
*Statistically significance versus Physiological reproductive status (p<0.05).
Table 3.
Ultrasonografic (US) endometrium pattern in the middle stage of the ovarian cycle secretion phase.
Table 3.
Ultrasonografic (US) endometrium pattern in the middle stage of the ovarian cycle secretion phase.
| US-pattern correspondence to the cycle | Physiological reproductive status | Recurrent reproductive failures | ||
| Yes | No | Yes | No | |
| Common numbers, n (%) | 40(80%) | 10(20%) | 35(70%) | 15(30%) |
| Natural cycles, n (%) | 40(100%) | 10(100%) | 10(28.6%) | 6(40.0%) |
| Stimulated cycles, n (%) | - | - | 25(71.4%)* | 9(60.0%) |
*Statistically significance versus endometrium pattern from normal ovarian cycle (p<0.05).
Table 4.
Histological pattern of endometrial glandular epithelium in the middle stage of the ovarian cycle secretion phase.
Table 4.
Histological pattern of endometrial glandular epithelium in the middle stage of the ovarian cycle secretion phase.
|
Corresppondence to the cycle |
Physiological reproductive status | Recurrent reproductive failures | ||
| Yes | No | Yes | No | |
| Common numbers, n (%) | 43(86%) | 7(14%) | 38(76%) | 12(24%) |
| Natural cycles, n (%) | 43(100%) | 7(100%) | 11(28.9%) | 5(41.7%) |
| Stimulated cycles, n (%) | - | - | 27(71.1%)* | 7(58.3%) |
*Statistically significance versus endometrium pattern from normal ovarian cycle (p<0.05).
Table 5.
Relative number of pinopodes of the superficial endometrial epithelium in the middle stage of the ovarian cycle secretion phase.
Table 5.
Relative number of pinopodes of the superficial endometrial epithelium in the middle stage of the ovarian cycle secretion phase.
| Relative number of pinopodes | Physiological reproductive status | Recurrent reproductive failures | ||
| >50% | <50% | >50% | <50% | |
| Common numbers, n (%) | 34 (68%) | 16(32%) | 26(52%) | 24(48%) |
| Natural cycles, n (%) | 34 (100%) | 16(100%) | 9(34.6%) | 7(29.2%) |
| Stimulated cycles, n (%) | - | - | 17(65.4%) | 17(70.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



