
Submitted:
26 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
Background. Toxin-producing strains of Clostridioides difficile are the most commonly identified cause of healthcare-associated infection in the elderly. Risk factors include advanced age, hospitalisation, prior or concomitant systemic antibacterial therapy, chemotherapy, and gastrointestinal surgery. Patients with unspecified and new-onset diarrhoea with ≥3 unformed stools in 24 hours are a target population for testing for C. difficile infection (CDI). Objective. To present data on the risk factors in current practices for clinical diagnoses used in managing CDI. Materials and Methods. We studied 116 clinical stool specimens from inpatients with acute diarrhoea suspected of nosocomial or antibiotic-associated diarrhoea (AAD) due to C. difficile from two general hospitals. Enzyme Immunoassay card tests (EIA) for detecting C. difficile toxins A (cdtA) and B (cdtB) from stool, аutomated CLIA assay for the detection of C. diff. GDH antigen and qualitative determination of cdtA and B in human faeces, and anaerobic stool culture were applied for CDI laboratory diagnostic. MALDI-TOF (Bruker) identified the suspected anaerobic bacterial colonies. The following methods were used as differential diagnostics LAMP method for evidence of Salmonella spp. and simultaneous detection of Campylobacter jejuni and C. coli, E. coli Typing RT-PCR detection kit (ETEC, EHEC, STEC, EPEC, EIEC), API 20E, and aerobic stool culture methods. Results. Forty toxigenic C. difficile strains were isolated from all 116 diarrhoeal stool specimens tested, of which 38 (38/40) produced toxin B and two strains (2/40) were positive for both cdtA and cdtB. Of the faecal samples positive for cdtA (6/50) and/or cdtB (44/50) by EIA, 33 samples were C. diff culture negative, but positive for the following diarrhoea agents: 1/33 – Salmonella enterica subsp. Arizonae (LAMP, culture, API 20E); 2/33 C. jejuni (LAMP, culture, MALDI TOF); 1/33 – ETEC O142 and 2/33 - STEC O145 and O138 (E. coli Typing RT-PCR detection kit, culture); 2/33 C. perfringens (anaerobic culture, MALDI TOF); 2/33 – hyper-mycotic enterotoxigenic K. pneumonia and 2/33– enterotoxigenic P. mirabilis (culture; PCR LT-toxin-encoding). Two of the 66 cdtB-positive samples (2/66) exhibited a similar misdiagnosis when analysed using the CLIA method. However, the PCR analysis indicated that they were cdtB-negative. In contrast, the LAMP method identified a positive result for C. jejuni in one sample and another one was STEC positive (stx1+/stx2+) by RT-PCR. Furthermore, there is an additional discrepancy in the CDI testing results. EPEC O86 (RT-PCR eae+) was isolated from a faecal sample that was positive for GHA enzyme (CLIA) and negative for cdt A and cdtB (CLIA and PCR assay). However, the C. diff culture was negative. The findings support the hypothesis that certain human bacterial pathogens that produce enterotoxins other than C. difficile, as well as intestinal commensal microorganisms, including Klebsiella sp. and Proteus sp., contribute to false-positive EAI card tests for C. difficile A and B toxins, which are the most widely used in the laboratory diagnosis of CDI. In conclusion, C. difficile infection represents a significant challenge to clinical practice, both in terms of management and prevention of recurrence. It is recommended that toxin-only EAI tests should not be used as a stand-alone diagnostic tool for CDI and that their use should be limited to the detection of toxins A and B. Accurate diagnosis of CDI requires a combination of clinical evaluation, diagnostic methods, and management practices.
Keywords:
Clostridioides difficile
; cdtA
; cdtB
; managing CDI
; laboratory diagnostic
1. Introduction
Clostridioides difficile, also known as Clostridium difficile (C. diff) is a Gram-positive, spore-forming anaerobic, toxin-producing bacterium, that exists in the environment, in the gastrointestinal tract of animals and humans, which is a major cause of healthcare-associated (nosocomial) infections and is an increasingly frequent cause of morbidity and mortality among older adult hospitalized patients [1,2]. Its prevalence among the older population is higher because this age group has a large number of risk factors, such as comorbidity, frequent exposure to healthcare or housing environments, immunosenescence, and greater consumption of antibiotics and antacids [3]. Furthermore, C. diff is a common cause of antibiotic-associated diarrhoea (AAD), which often results from the disruption of normal gut flora due to antibiotic use, and manifestations ranging from asymptomatic carriage, mild to fulminant diarrhoea, toxic megacolon, and pseudomembranous colitis due to virulence factors: an enterotoxin (toxin A) disrupts actin-filament assembly and a cytotoxin (toxin B), which mediates cell-surface binding and intracellular translocation [4,5]. The spores and vegetative cells of C. difficile colonise the human intestinal tract via the faecal-oral route, the most vegetative cells are killed in the stomach, however, the spores of the toxin-producing bacillus are acid-resistant and they germinate in the small bowel upon exposure to bile acids. It is known, that the primary bile acids stimulate this germination process. C. difficile multiplies in the colon, where vegetative cells produce toxins A and B and hydrolytic enzymes [6,7]. The primary reservoirs of C. difficile include colonised or infected patients and contaminated environments and surfaces within hospitals, the hands of hospital personnel, and long-term care facilities. C. difficile can be spread by patients with CDI not only during their diarrheal episode but even after therapy has ended. [7,8]. Antibiotic exposure (especially fluoroquinolones, third or fourth-generation cephalosporins, clindamycin, carbapenems), prior hospitalization, advanced age, an increase in the severity of underlying illness, immunocompromising conditions, gastrointestinal manipulation, and proton-pump inhibitors are all risk factors for C. difficile infection. IBD patients, especially those with ulcerative colitis, are more susceptible to both primary CDI and recurrent disease, as well as increased morbidity and mortality from CDI [2,9,10]. The epidemiology of C. difficile in children has shown that many infants and young children (<3 years of age) have asymptomatic colonization with either toxigenic or nontoxigenic strains, making it an important feature. Colonisation rates decrease with increasing age [10,11,12]. The risk factors for CDI in children are identical to those in adults, except for advanced age. The development of CDI is generally linked to changes in gut microbiota that increase the risk of being colonized by C. difficile and the subsequent development of CDI [13,14]. Testing in this population should only be done if other infectious and non-infectious causes of diarrhoea have been excluded. Although C. difficile infection is not likely to occur in young children, asymptomatically colonised infants and children may transmit the disease to adults, which can result in CDI among adult contacts [9,10,11,12,13,14].
Accurate diagnosis of CDI is essential for effective prevention and treatment. Several diagnostic tests are used, including Enzyme Immunoassay (EIA) for C. difficile Toxins A and B, Glutamate Dehydrogenase (GDH) Assay to detect the enzyme GDH, which is present in all C. difficile strains, Polymerase Chain Reaction (PCR) to detect C. difficile toxin genes, Stool Culture, Endoscopy to visualise pseudomembranous plaques in the colon, Imaging- X-ray or CT scans to evaluate complications such as toxic megacolon or perforation. However, no single test is sufficient to diagnose all cases, and diagnostic algorithms are commonly employed [1,5,9,10].
The objective of this article is to evaluate the risk factors inherent to the current clinical diagnostic practices applied in the management of Clostridioides difficile infection (CDI) in routine healthcare settings across diverse medical centres.
2. Materials and Methods
2.1. Patients Selection
We defined patients as suspected of CDI in accordance with the CDC and ESCMID recommendations that patients with unspecified and recent onset diarrhoea characterised by the formation of ≥3 stools within 24 hours should undergo testing for Clostridioides difficile infection. In the study, conducted 68 men and 48 women (in the 12- 80 age bracket), were admitted to two different general hospitals.
2.2. Samples
A total of 116 unformed faecal samples, defined as Bristol stool form scale type 6 and 7 [15], from inpatients with diarrhoea were examined before the ethiological antibiotic exposure. The two hospitals are conventionally denoted by the following symbols: SF and DT. SF-hospital provided data on 66 stool samples, positive for C. diff tested with PCR and CLIA, whereas DT-hospital provided data on 50 EIA positive for C. diff samples. The faecal samples were submitted to the NRL for Enteric diseases on the day of deposition to ensure the efficacy of the bacterial culturing techniques employed. None of the source hospitals provide culture methods for CD.
Enzyme Immunoassay (EIA) testing was conducted to determine the presence of toxin A and toxin B of Clostridioides difficile. In the clinical laboratories or the hospital departments, faecal samples were subjected to an EIA card test for the detection of both toxins A and B within a period of two hours following the initial sampling. The result is conveyed within ten minutes of the administration of the card test drip.
Faecal samples were treated using the alcohol shock method to inhibit non-sporulating organisms and thereby improve the isolation of C. difficile. A pea-sized portion of the sample was transferred to 350 µl of absolute alcohol, and the suspension was allowed to stand at room temperature for 30 minutes, after which 100–150 µl of the suspension was inoculated onto Brain Heart Agar, 10% sheep blood (Oxoid, UK) and incubate at 37-38°C for 48-72 hours under anaerobic conditions maintain with gas packs (Oxoid, UK). Furthermore, faeces were cultured on MacConkey agar, Levin agar, and SS-agar at 37-38°C for 18-20 hours, and subsequently cultured after pre-enrichment in Selenite broth for 18-20 hours at 37-38°C.
The obtained cultures under both anaerobic and aerobic conditions were identified using MALDI-TOF (Bruker). On several occasions, API 20E biochemical tests were employed for final subspecies identification followed by phenotypical serotyping (anti-E.coli sera, SSI, Denmark).
2.3. DNA-Extraction
Whole genomic DNA was extracted from each stool sample using a commercial DNA extraction kit (QIAamp PowerFecal Pro DNA Kit, Germany) following the manufacturer's instructions. The extracted DNA samples were subsequently stored at -20°C in preparation for subsequent molecular analysis.
2.4. Molecular Methods
A commercial gastrointestinal panel for the detection and differentiation of bacterial, viral, and parasitic target pathogenes (QIAstat-Dx Gastrointestinal Panel 2) including C. diff (toxin A/B). The following methods were used for differential diagnosis: LAMP method for detection of Salmonella spp. and simultaneous detection of Campylobacter jejuni and C. coli for only 35 minutes; commercial E. coli Typing RT-PCR detection kit (CerTest BIOTEC, Spain) for detection of virulence genes of enterotoxigenic E. coli; enterohemorrhagic E. coli; Shiga toxin-producing E. coli and enteropathogenic E. coli and enteroinvasive E. coli (ETEC, EHEC, STEC, EPEC, EIEC). Adishanal molecular analysis PCR for investigation LT-toxin-encoding lth gene in Enterobacteriales related to diarrhoea syndrome.
2.5. Chemiluminescence Immunoassay (CLIA)
Define an algorithm that consists of two steps for diagnosing CD as recommended by ESCMID Clinical Guidelines (EU) and Clinical Practice Guideline (USA), an automated CLIA assay for the detection of CD GDH antigen was conducted, followed by a CLIA assay for the qualitative determination of toxins A and B in human faeces (Diasorin’s LIAISON®).
3. Results
Given the disparate financial resources available at the two hospitals, we assess the quality of C. diff diagnosis across the various methods employed by the health units, rather than focusing on the diagnostic capabilities of the hospitals themselves. Our findings will help to inform the development of an appropriate health policy.
Forty toxigenic C. difficile strains (34,4%) were isolated from all 116 diarrhoeal stool specimens tested, of which 38 (38/40) produced toxin B and two strains (2/40) were positive for both toxins A+ B+. Toxigenic profiles were determined by the EAI card test for free toxins in faeces in DT-hospital and from bacterial culture in NCIPD, as well as the CLIA assay (Diasorin’s LIAISON®) for the detection of C. diff GDH antigen, followed by an assay for the qualitative determination of toxins A and B in human faeces. Additionally, the samples that were identified as GDH+, cdtA- and cdtB- or those that were identified as GDH-, cdtA+ and/or cdtB+, were subjected to further analysis via PCR for C. difficile toxins A and B (QIAstat-Dx) at ST-hospital. The culture of the C. diff bacillus was obtained and identified with MALDI- TOF at NCIPD (Figure 1).
Of the fifty faecal samples (50/116), that were tested with EIA assays (NADAL®) and were found to be positive for cdtA+ (6/50) and cdtB+ (44/50), seventeen stool cultures of C. difficile (17/50) were isolated, all of which were positive for the cdtB. The examination of the faeces (4/50) yielded positive results for the detection of free cdtA+ cdtB- (EIA), demonstrating the presence of diarrhoeal agents through the utilisation of aerobic and anaerobic stool culturing. The identified agents were C. perfringens (2/6), monocultures of two hyper-mycotic Klebsiella pneumoniae (2/16) and two Proteus mirabilis strains (2/6). Furthermore, the presence of the LT-toxin-encoding lth gene was investigated in Klebsiella and Proteus strains using PCR. The specific primers are designed based on the E. coli gene from the GENEBANK database, and the PCR mix and reaction conditions are previously described by Adriana Janczura et al. [16]. The analysis of cdtA-/cdtB+ (EAI) stool samples that were culture-negative for C. difficile (31/48) evidenced the presence of pathogenic agents. This was conducted through the utilisation of aerobic stool culturing and LAMP molecular methodology as a differential diagnostic approach. A single faecal sample was identified as positive for Salmonella spp. (1/10) through the use of LAMP, while two additional samples were determined to be positive for C. jejuni (2/10). Bacterial cultures were obtained from these samples and subsequently confirmed by MALDI-TOF and biochemical typing of Salmonella as enterica subsp. arizonae with an API 20E test. Three out of ten faecal samples yielded enteropathogenic E. coli (EPEC), which were phenotypically serotyped (anti-E. coli sera, SSI, Denmark) as enterotoxigenic E. coli (ETEC) O142 and two strains of Shiga-toxin producing E. coli (STEC) O145 and STEC O138. Following molecular genotyping with E. coli typing RT-PCR kit (CerTest) from bacterial culture detected virulence genes for heat-labile enterotoxin (lt) and heat-stable enterotoxin (st) in E. coli O142, as well as genes for Shiga toxins (stx1+ and stx2+) in O145 and stx1+ in STEC O138 (Table 1).
All 66 faecal samples from the SF-hospital were subjected to primary testing for Clostridioides difficile infection through the use of a commercial enzyme-linked immunosorbent assay (ELISA) for the detection of the GDH enzyme, followed by quantification of the cdtA/B genes. If the faecal specimen was not submitted to the clinical microbiology laboratory for testing within a timeframe of 2-3 hours following disposal, even in the absence of a positive GDH result, toxin testing was conducted. For samples that tested positive for GDH and cdtA-/cdtB-, as well as for samples that tested negative for GDH but positive for toxins, a repeat confirmatory test utilizing PCR for cdtA/B was performed.
Two of the 66 cdtB+ samples (2/66) exhibited a similar misdiagnosis when analysed using the CLIA method, however, the PCR analysis indicated that they were cdtB-negative. In contrast, the LAMP method identified a positive result for C. jejuni in one sample and another one was STEC positive (stx1+/stx2+) by RT-PCR. Furthermore, there is an additional discrepancy in the CDI testing results- EPEC O86 (RT-PCR eae+) was isolated from a faecal sample (1/66) that was positive for GDH enzyme (CLIA) and cdtA- and cdtB- (CLIA and PCR assay). However, the C. diff culture was negative (Table 2) (Figure 2).
4. Discussion
To realistically assess the management of CDI in health facilities, particularly timely and accurate diagnosis to limit the spread of the bacillus as nosocomial infections, we selected one of the largest hospitals in the country and a randomly selected smaller hospital in the countryside, both of which regularly record cases of postadmission acquired diarrhoea and health-care serving a large number of patients from different areas of the country In this study, the main methods used for the diagnosis of CDI were those available at the health facilities that were tested. These included EIA tests that were limited to the detection of cdtA and cdtB and did not have the capability to detect a GDH enzyme. Additionally, there was an automated CLIA assay for the detection of C. diff GDH antigen and an assay for the qualitative determination of cdtA and cdtB in human faeces. At the NRL for Enteric Diseases, Microbiology Dep., NCIPD, we performed a range of tests, including culturing of faecal samples, and molecular, biochemical and phenotypic methods for identification and serotyping of enteric pathogens. Accurate diagnosis of CDI requires a combination of understanding the clinical presentation, diagnostic methods, and management practices of CDI. A comprehensive and precise examination of both clinical and laboratory data is imperative for the accurate interpretation of test results for Clostridioides difficile. In order to interpret the results, it would be beneficial to consider the patient's symptoms, such as any new-onset diarrhoea, defined as three or more unformed stools within 24 hours. It may be the case that the presence of these symptoms suggests active infection with C. difficile. For illustration, a positive result from a laboratory test in the absence of clinical symptoms may indicate colonisation rather than active infection [5,8,10,17]. It would be remiss of us not to consider the patient's history, including previous infections with C. difficile, antibiotic exposure and comorbidities when interpreting the results. In this study, patients had experienced at least one hospitalisation before the current admission. The patients were admitted to the health facility in the absence of diarrhoea. A referral for a differential examination for CDI was made based on the sudden onset of diarrhoea (within 72 hours after the addition), as assessed using the Bristol type 6 and 7 scale [15], with a minimum of three bowel movements in a 24-hour period. All patients had received antibiotics within the previous six months. The aforementioned criteria collectively defined the profile of the subjects as susceptible to CDI. Sixty-eight men and forty-eight women in the 12- 80 age bracket were conducted in this study. It is of the essence that potential cases of CDI are identified at the earliest opportunity, thus allowing laboratory diagnostic techniques to be employed for the purpose of confirming the diagnosis [18]. Forty toxigenic C. difficile strains (34,4%) were isolated from all 116 diarrhoeal stool specimens tested, of which 38 (38/40) produced toxin B and two strains (2/40) were positive for both toxins A+ B+. Laboratory tests performed for the diagnosis of CDI identified toxin B as the predominant toxigenic profile of C. difficile isolates from patients in a hospital. This is in line with findings from country studies in Bulgaria, where it was concluded that the majority of pathogenic Bulgarian C. difficile isolates harbour the tcdB+ gene. Moreover, laboratory-confirmed cases of C. difficile expressing both toxins simultaneously remain exceedingly rare in the country [19,20]. It is notable that a considerable number of EIA false-positive rapid tests for C. diff toxA+ (12/50; 12%) exhibited cross-reactions with enterotoxins derived from members of the Enterobacteriales, namely Klebsiella pneumoniae and Proteus mirabilis. These cross-reactions have also been observed in instances of antibiotic-associated and sporadic diarrhoea, as well as in cases of Clostridium perfringens, which is recognised as the causative agent of food poisoning outbreaks. Furthermore, LJ Forward and colleagues indicate the prospect of identifying toxins produced by C. difficile and C. perfringens in instances of community-acquired diarrhoea using commercially available EIAs [21,22,23]. Laboratory tests such as EIAs for cdtA and cdtB are essential for diagnosing infection. These tests only confirm the presence of the bacterium and its toxins if they are administered according to two-step diagnostic protocols. First, they detect the enzyme GDH, which confirms the presence of CD. Then, they proceed with proof of the presence of toxins A and B [9,10]. Although EIA tests that combine GDH with ToxA/B are commercially available, Bulgarian microbiological laboratories use binary tests for CD toxins in hospital CD management practice. The reason is most likely the lower cost of the tests. These widespread tests pose significant risks to both clinicians using them as rapid diagnostic tests and to clinical laboratories. Conversely, a considerable number of EIA and CLIA tests report cdtB+ (7,7%), though they lag behind campylobacteriosis, salmonellosis, and STEC infections, which could be an essential marker for CDI superdiagnosis. In the context of preventing CDI, clinicians order these examinations in an effort to achieve the desired outcome. It would be reasonable to posit that toxin-positive CD tests without GDH present may serve as a clue marker for non-clostridial bacterial enterocolitis. In order to provide an answer to this question, it would be necessary to carry out a comprehensive study involving a significant number of patients with diarrhoea and a range of confirmatory tests. Alternatively, a complete differential diagnosis of the syndrome would have to be carried out, supported by clinical data.
Nevertheless, in clinical practice, rapid assays (especially Enzyme Immunoassay (EIA), PCRs, and Chemiluminescence immunoassay (CLIA) techniques) are frequently employed as standalone tests rather than as components of an algorithm, including stool culture, which is considered the gold standard. This may, in turn, result in C. difficile colonization being misclassified as CDI. In order for an infection to be defined as healthcare-associated, a number of specific circumstances must be taken into consideration. Firstly, if symptoms began 72 hours or more after admission. Secondly, in the event that an individual was diagnosed with an infection with C. difficile within four weeks of discharge from any healthcare facility. Finally, in cases where the infected person was a healthcare worker in contact with patients [24]. The implementation of these criteria facilitates the identification of instances of healthcare-associated infection, thereby enabling the implementation of appropriate control and prevention measures. Finally, it is important to consider the potential for misclassification and inappropriate antimicrobial therapy when using a rapid non-culture independent test for the clinical management of CDI. It is therefore recommended that etiologic therapy be employed in order to avoid the risk of recurrent CDI, prevent the acquisition of antibiotic-associated infections, and limit the spread of medically-associated infections.
5. Conclusions
A comprehensive approach to diagnosing CDI is essential to ensure an accurate diagnosis and management. This requires considering a range of factors, including clinical data- infection presentation, antibiotic exposure, history of hospitalisations, previous CDI, the presence of colonoscope-evidenced pseudomembranous colitis, and laboratory data- including combinations of non-cultured and cultured methods, as well as antibiotic susceptibility testing. This multi-faceted approach enables the determination of the most appropriate treatment for the patient.
Author Contributions
Conceptualization, A.K., M.R.P. and V.V.; methodology, M.P., M.R.P and A.K; software, Y. M-, M.; validation, M.R.P. and V.V.; formal analysis, R.S.; investigation, M.R.P., M.P., A.K. and R.S.; resources, M.P. and Y. M-, M.; data curation, V.V.; writing—original draft preparation, A.K., M.R.P.; writing—review and editing, V.V., M.R.P., A.K.; visualization, R.S.; supervision, M.R.P.; project administration, A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of “Ajibadem City Clinic -Tokuda” University General Hospital, Sofia, Bulgaria (Nr. 226/19.11.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
All data generated or analyzed during this study are included in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Johnson, S.; Lavergne, V.; Skinner, AM.; Gonzales-Luna, A. J.; Garey, K. W.; Kelly, C. P.; Wilcox M., H. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin Infect Dis. 2021, 5, e1029–e1044. [Google Scholar] [CrossRef] [PubMed]
- Vivian, G. L.; Bourgault, A.; Poirier, L.; Lamothe, F.; Michaud, S.; Turgeon, N.; Toye, B.; Beaudoin, A.; Frost, E.H.; Gilca, R.; et al. Host and Pathogen Factors for Clostridium difficile Infection and Colonization. N Engl J Med. 2011, 18, 1693–1703. [Google Scholar] [CrossRef]
- Pareja-Sierra, T. Diarrea asociada a Clostridium difficile en el anciano: nuevas perspectivas. Revista Española de Geriatría y Gerontología. 2015, 4, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Letourneur, O.; Ottone, S.; Delauzun, V.; Bastide, M.-C.; Foussadier, A. Molecular cloning, overexpression in Escherichia coli, and purification of 6x his-tagged C-terminal domain of Clostridium difficile toxins A and B. Protein Expr Purif. 2003, 31, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Bishop, E.J.; Tiruvoipati, R. Management of Clostridioides difficile infection in adults and challenges in clinical practice: review and comparison of current IDSA/SHEA, ESCMID and ASID guidelines. J Antimicrob Chemother. 2022, 78, 21–30. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carey-Ann, B.D.; Carroll, K.C. Diagnosis of Clostridium difficile Infection: an Ongoing Conundrum for Clinicians and for Clinical Laboratories. Clin Microbiol Rev. 2013, 26, 604–30. [Google Scholar] [CrossRef]
- Poutanen, S.M.; Simor, A.E. Clostridium difficile-associated diarrhea in adults. CMAJ. 2004, 171, 51–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Crobach, M.T.; Vernon, J.J.; Loo, V.G.; Kong, L.Y.; Péchiné, S.; Wilcox, M.H.; Kuijper, E.J. Understanding Clostridium difficile Colonization. Clin Microbiol Rev. 2018, 31, e00021-17. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- CDC. Clinical Guidance for C. diff Prevention in Acute Care Facilities. March 8, 2024.
- McDonald, L. C.; Gerding, D. N.; Johnson, S.; Bakken, J. S.; Carroll, K. C.; Coffin, S. E.; Dubberke, E. R.; Garey, K. W.; Gould, C. V.; Kelly, C. et. al. , Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clinical Infectious Diseases 2018, 7, e1–e48. [Google Scholar] [CrossRef]
- Rousseau, C.; Lemée, L.; Monnier, A.; Poilane, I.; Pons, J. L.; Collignon, A. Prevalence and diversity of Clostridium difficile strains in infants. J Med Microbiol. 2011, 60, 1112–8. [Google Scholar] [CrossRef]
- Krutova, M.; de Meij, T. J.; Fitzpatrick, F.; Drew, R. J.; Wilcox, M. H.; Kuijper, E. J. How to: Clostridioides difficile infection in children. Clin Microbiol Infect. 2022, 8, 1085–1090. [Google Scholar] [CrossRef]
- Chilton, C. H.; Pickering, D. S.; Freeman, J. Microbiologic factors affecting Clostridium difficile recurrence. Clin Microbiol Infect. 2018, 24, 476–482. [Google Scholar] [CrossRef]
- Reeves, A. E.; Theriot, C. M.; Bergin, I. L.; Huffnagle, G. B.; Schloss, P. D.; Young, V. B. The interplay between microbiome dynamics and pathogen dynamics in a murine model of Clostridium difficile Infection. Gut Microbe. 2011, 2, 145–58. [Google Scholar] [CrossRef] [PubMed]
- Chumpitazi, B. P,.; Self, M. M.; Czyzewski, D. I., Cejka, S.; Swank, P. R.; Shulman, R. J. Bristol Stool Form Scale reliability and agreement decreases when determining Rome III stool form designations. Neurogastroenterol Motil. 2016, 3, 443–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Janczura, A.; Smutnicka, D.; Junka, A.; Gościniak, G. The detection and expression of enterotoxinencoding lth gene among Klebsiella spp. isolated from diarrhea. Central European Journal of Biology. 2013, 8, 121–129. [Google Scholar] [CrossRef]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect. 2021, 2, 1–21. [Google Scholar] [CrossRef]
- Di Bella, S.; Ascenzi, P.; Siarakas, S.; Petrosillo, N.; Di Masi, A. Clostridium difficile Toxins A and B: Insights into Pathogenic Properties and Extraintestinal Effects. Toxins 2016, 8, 134. [Google Scholar] [CrossRef]
- Dobreva E., G.; Ivanov I., N.; Vathcheva-Dobrevska, R. S.; Ivanova, K. I.; Asseva, K.; Petrov, P. K.; Kantardjiev, T. V. ; Advances in molecular surveillance of Clostridium difficile in Bulgaria. J Med Microbiol. 2013, 62, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Dobreva, Е.; Ivanov I., N.; Vatcheva-Dobrevska, R.; Ivanova, K.; Marina, M.; Petrov, P.; Kantardjiev, T.; Kuijper, E. Toxin encoding genes characterization of Bulgarian Clostridium difficile clinical strains. C. R. Acad. Bulg. Sci. 2012, 65, 1365–1372. [Google Scholar]
- Forward, L. J.; Tompkins, D. S.; Brett, M. M. Detection of Clostridium difficile cytotoxin and Clostridium perfringens enterotoxin in cases of diarrhoea in the community. J Med Microbiol. 2003, 52, 753–757. [Google Scholar] [CrossRef]
- Youn, Y.; Lee, S.W.; Cho, H. H.; Park, S.; Chung, H. S.; Seo, J. W. Antibiotics-Associated Hemorrhagic Colitis Caused by Klebsiella oxytoca: Two Case Reports. Pediatr Gastroenterol Hepatol Nutr. 2018, 2, 141–146. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Selvaraj, V.; Alsamman, M. A. Antibiotic-Associated Diarrhea Beyond C. Difficile: A Scoping Review. Brown Hospital Medicine 2022, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Khanafer, N.; Vanhems, P.; Bennia, S.; Martin-Gaujard, G.; Juillard, L.; Rimmelé, T.; Argaud, L.; Martin, O.; Huriaux, L.; Marcotte, G.; et., al. Factors Associated with Clostridioides (Clostridium) Difficile Infection and Colonization: Ongoing Prospective Cohort Study in a French University Hospital. Int J Environ Res Public Health. 2021, 18, 7528. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Examination of 50 clinical stool samples cdtA+/cdtB+ by EIAs from DT-hospital. Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
Figure 1.
Examination of 50 clinical stool samples cdtA+/cdtB+ by EIAs from DT-hospital. Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
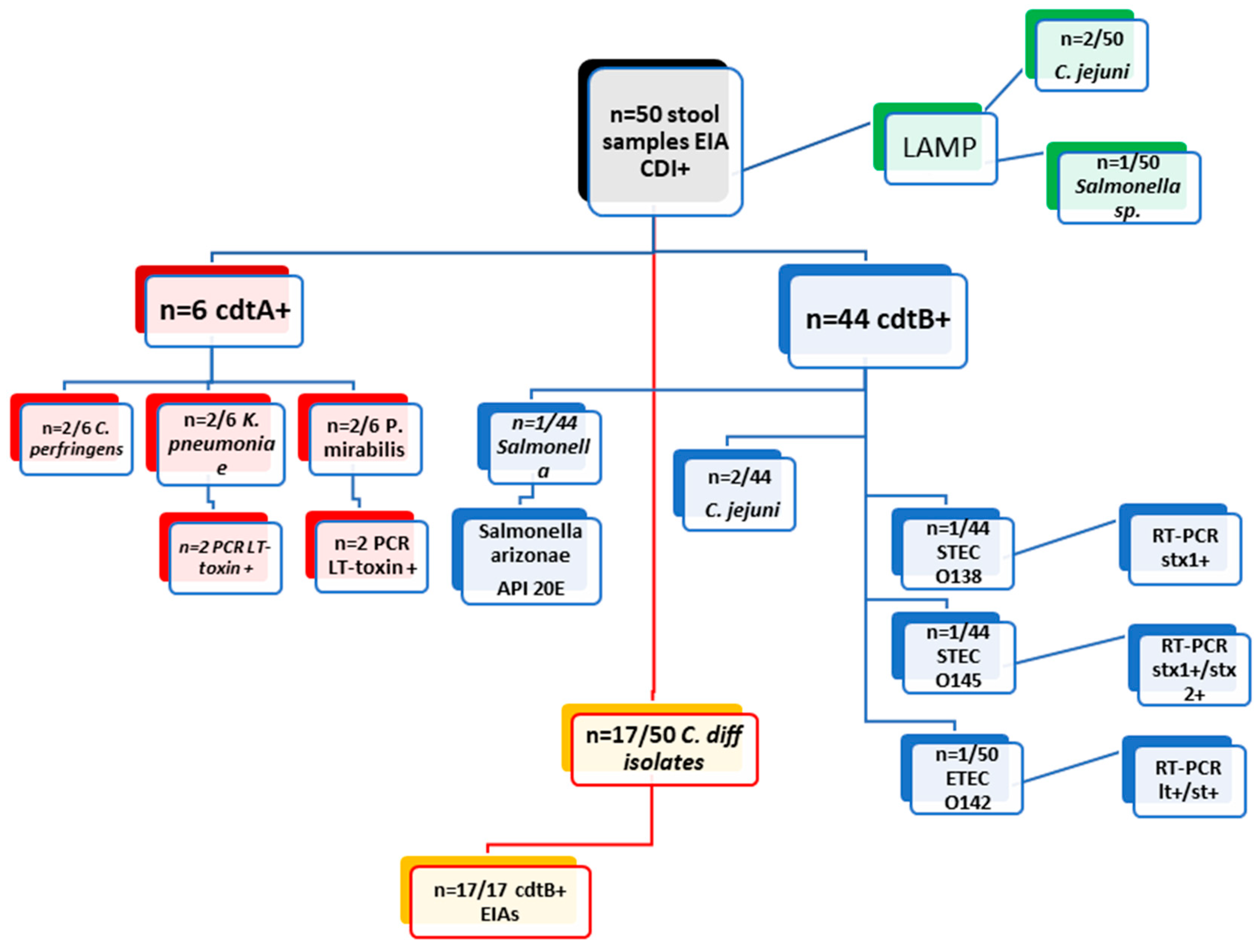
Figure 2.
Examination of 66 clinical stool samples CLIA and RCR tested for CDI from SF-hospital. Here are presented the differences in the laboratory diagnostic methods. Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
Figure 2.
Examination of 66 clinical stool samples CLIA and RCR tested for CDI from SF-hospital. Here are presented the differences in the laboratory diagnostic methods. Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
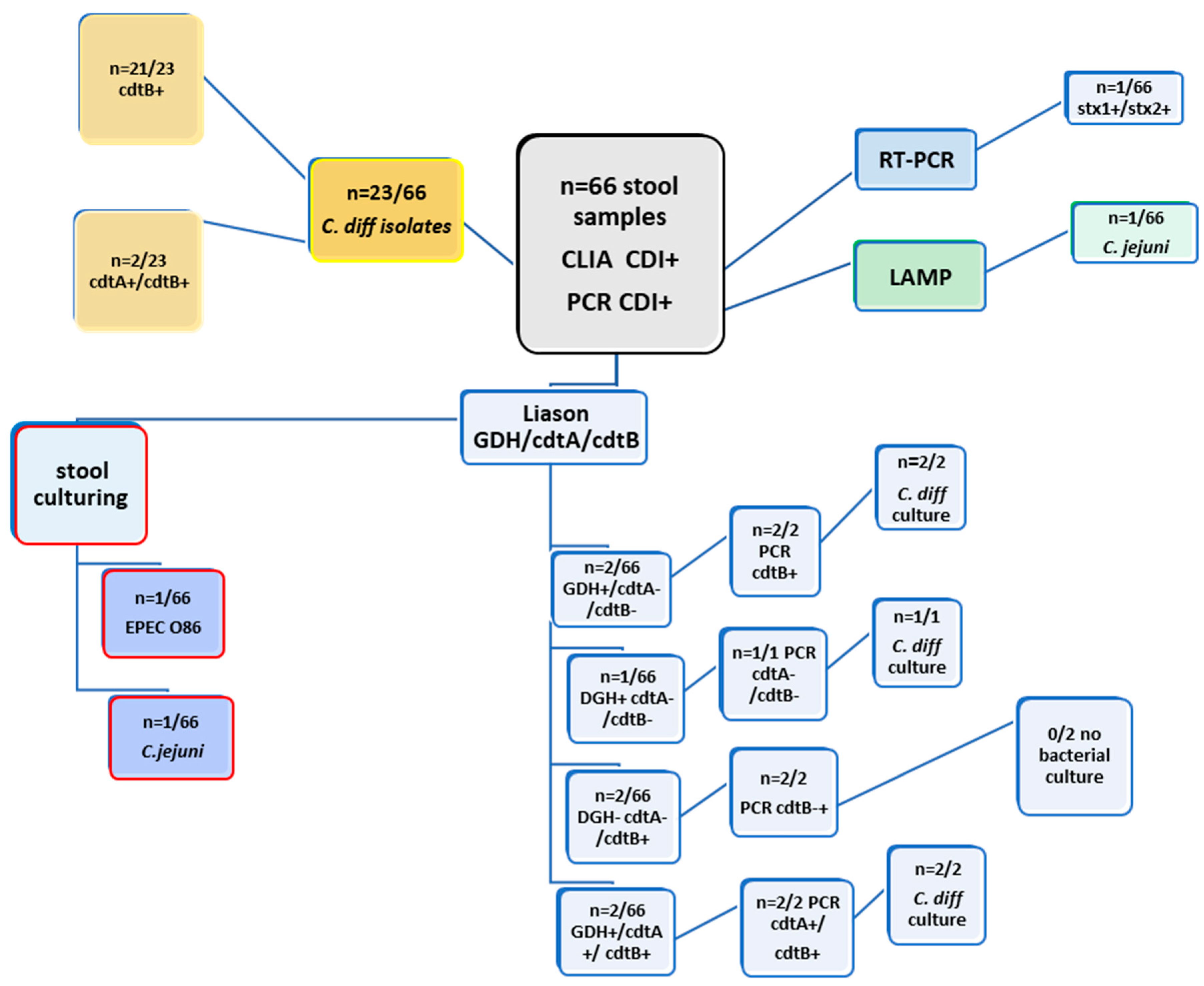

Table 1.
Results from examining 50 clinical stool samples from DT-hospital by different laboratory methods- Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
Table 1.
Results from examining 50 clinical stool samples from DT-hospital by different laboratory methods- Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
| Examination of 50 clinical stool samples cdtA+/cdtB+ by EIAs from DT-hospital | |||||||||
| methods | EIA cdtA + ( n= 6/50) | EIA cdtB + ( n= 44/50) | |||||||
| culture | C. perfringens (2/6) | K. pneumoniae (2/6) | P. Mirabilis (2/6) | Salmonella | C. difficile (17/44) | C. jejuni (2/44) | STEC O138 (1/44) | STEC O145 (n=1) | ETEC 142 (1/44) |
| PCR | x | LT toxin (n=2) | LT toxin (n=2) | x | x | x | stx1+ (n=1) | stx1+/stx2+ (n=1) | lt+/st+ (n=1) |
| API20E | x | x | x | Salmonella arizonae | x | x | x | x | x |
| LAMP (Salmonella/ Campylobacter) | negative | negative | negative | Salmonella | negative | C. jejuni (2/44) | negative | negative | negative |
Table 2.
Results from examining 66 clinical stool samples from SF-hospital by different laboratory methods- CLIA and RCR assays for CDI Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
Table 2.
Results from examining 66 clinical stool samples from SF-hospital by different laboratory methods- CLIA and RCR assays for CDI Stool culturing, RT-PCR for E. coli typing, LAMP assay for Salmonella and Campylobacter, and EIAs cdtA/B.
| Examination of 66 clinical stool samples by CLIA (GDH; cdtA/B) and PCR (cdtA; cdtB) from SF-hospital | ||||||||
| METHODS | Liason GDH | Liason cdtA | Liason cdtB | PCR cdtA | PCR cdtB | culture | LAMP | RT-PCR (STEC) |
| 2/66 | negative | negative | negative | 2/66 | C. difficile (n=2/66) | negative | x | |
| 1/66 | negative | negative | negative | negative | C.difficile(n=1/66) | negative | x | |
| negative | negative | 2/66 | negative | 2/66 | negative | negative | x | |
| negative | negative | 1/66 | negative | 1/66 | C.jejuni(n=1/66) | C.jejuni | x | |
| negative | negative | 1/66 | negative | 1/66 | EPEC O86 | negative | stx1+/stx2+ | |
| 2/66 | 2/66 | 2/66 | 2/66 | 2/66 | 2/66 | negative | x | |
| negative | negative | 21/23 | negative | 21/23 | C. difficile (n=23/66) | negative | x | |
| negative | 2/23 | 2/23 | negative | 2/23 | C.difficile (n=23/66) | negative | x | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



