
Submitted:
21 February 2025
Posted:
24 February 2025
You are already at the latest version
Abstract
Some vaccinees experience cardiac adverse events (AEs) following immunization (AEFI). These AEs include both background events and for some vaccines, vaccine associated AEs. A small subset of AEs experienced by vaccinees are reported to the United States Vaccine Adverse Event Reporting System (VAERS). Herein, VAERS was retrospectively examined to identify cardiac AEFI associations. VAERS data was examined by vaccine type, vaccine source, vaccinee gender, and vaccinee age for infants. Multiple cardiac AEFI association patterns were detected: bradycardia and cardiac arrest for infants age 0, arrhythmia for COVID-19 and HPV vaccines, atrial fibrillation for COVID-19, influenza, and RSV vaccines, myocarditis and pericarditis for anthrax, COVID-19, smallpox, and typhoid vaccines, and chest discomfort, chest pain, palpitations, and tachycardia for multiple vaccines. Gender differences were observed for both myocarditis and palpitation AEFIs. Significant differences in bradycardia and cardiac arrest AEFI normalized frequencies were observed for the same infant vaccines from different manufacturers, suggesting possible manufacturing contaminants (e.g., endotoxins, DNA) as candidate causative components. Conclusions: Infant bradycardia and cardiac arrest AEFIs could be reduced by either delaying specific vaccines until infants are 1 year of age, selecting alternative vaccine options, or reduction or elimination of causative components (e.g., aluminium adjuvant, manufacturing contaminates, etc.). Both male and female myocarditis AEs can be modelled by mathematical age relationships for COVID-19 vaccines that may also apply to additional vaccines, suggesting possible shared etiologies. Multiple vaccines were observed with correlated cardiac AEFIs association signals for chest discomfort, chest pain, palpitations, and tachycardia; elevated histamine levels may contribute to the etiologies of these AEFIs.
Keywords:
arrhythmia
; atrial fibrillation
; bradycardia
; cardia arrest
; myocarditis
; palpitations
; pericarditis
; tachycardia
1. Introduction
Cardiac adverse events (AEs) following immunization (AEFIs) can include serious adverse events (SAEs). These cardiac AEFIs and SAEs may represent background occurrences in the population or immunization associated events. Passive collections of AEs post immunization in databases like the United States Vaccine Adverse Events Reporting System (VAERS) database [1]. The data within VAERS represents population samples of AEFIs. Elevated safety signals for AEFIs can be detected when AEs for one or more vaccines exceed the expected population background occurrence rate for these AEs; the population background occurrence rate can frequently be estimated from other vaccines within the dataset. This focus of this article is the detection of cardiac AEFIs that are occurring at frequencies higher than expected population background occurrence rates.
Cardiac AEFIs have been reported following immunizations for both adults and children. Cardiac AEFIs have been reported for adults for multiple vaccines with [2,3,4] with multiple recent reports associated with COVID-19 vaccines [5,6,7,8,9,10,11,12,13,14,15,16,17,18]. COVID-19 vaccines are associated with arrhythmia [5,6,7,8], atrial fibrillation [9,10,11], chest pain [7,12,13,14,15], myocarditis [5,7,16,17,18], palpitations [7,15], pericarditis [5,12], and tachycardia [15]. In a study of 301 adolescents receiving BNT162b2 mRNA COVID-19 vaccine, the most common cardiovascular AEs were tachycardia (7.64%), palpitation (4.32%), and chest pain (4.32%) with cardiovascular AEs in 29.24% of the adolescents [15]. The majority of these cardiac AEFIs have been reported in teenagers and adults. Children, can also experience cardiac AEFIs. For preterm infants, cases of bradycardia (low heart rate) with diphtheria/tetanus/whole cell pertussis (DTwP) [19] and diphtheria-tetanus-acellular pertussis (DTAP)-Haemophilus influenzae type b (Hib) [19,20], diphtheria-tetanus-pertussis-inactivated polio-Haemophilus influenzae type b (DTP-IPV-Hib) [21], and DTAP-Hib-meningococcal serogroup C (MCC) have been reported [22]. Bradycardia also occurs in extremely low birth weight (ELBW) infants in the immediate post-immunization period [23 and preterm infants [24]. Vaccine dosage levels are not currently adjusted to account for the lower body weight of these infants. The etiology of cardiac AEFIs in adults and children are currently unknown.
Herein, the VAERS database was retrospectively examined to identify cardiac AEFI associations [1]. Multiple cardiac AEFI association safety signals were observed. First, bradycardia AEFIs and cardiac arrest SAEs were observed for infants less than 1 year of age associated with multiple vaccines. Second, myocarditis and pericarditis association signals were observed for multiple vaccines. The myocarditis AE normalized frequencies were consistent with unique log-scale age relationships for both males and females. Third, arrhythmia AEFI signals were observed for COVID-19 and HPV vaccines and atrial fibrillation AEFI signals for COVID-19, influenza, and RSV vaccines. Fourth, chest discomfort, chest pain, palpitations, and tachycardia AEFIs signals were observed for multiple vaccines. Options to reduce bradycardia and cardiac arrest AEFIs in infants include adjusting vaccine dosage levels based on child body weight, delayed immunization until 1 year of age for several vaccines, immunization with alternative options for these vaccines, reduction or elimination of causative components (e.g., aluminum adjuvant or possibly endotoxins or DNA contaminants) from associated vaccines, and avoidance of concomitant vaccination combinations including live attenuated vaccines.
2. Materials and Methods
2.1. Materials
Focusing on cardiac AEs, the VAERS database [1] was retrospectively examined for the AEs designated by the following Medical Dictionary for Regulatory Activities (MedDRA) codes [25]: Arrhythmia, Atrial fibrillation, Bradycardia, Cardiac arrest, Chest discomfort, Chest pain, Myocarditis, Palpitations, Pericarditis, and Tachycardia. MedDRA® the Medical Dictionary for Regulatory Activities terminology is the international medical terminology developed under the auspices of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). The downloaded VAERS data includes all AEs reported from 1990 to June 26, 2024.
2.2. VAERS Retrospective Analysis
The Ruby program vaers_slice4.rb [26] was used for retrospective analysis of the VAERS data files VAERSDATA, VAERSSYMPTOMS, and VAERSVAX for the years 1990 to 2024 and NonDomestic. The vaers_reports.py program tallies vaccine AEs by vaccine, day of onset, age, and concomitant vaccines. The vaers_slice4.rb program takes a list of one or more MedDRA names (used by VAERS) as input.
Vaccines indicated with “foreign”, “no brand name”, “unknown”, are not illustrated in figures to avoid potential sampling biases associated with AE reports. Vaccines with only one AE are also not included to avoid elevated normalized frequencies possibly associated with population sampling in the VAERS reports with the exception for palpitation normalized frequencies for males for comparisons with female normalized frequencies (all of these exceptions have lower male normalized frequencies than the corresponding female normalized frequencies).
2.3. AEFI Formula
For adverse event (X), vaccine (V), cardiac AEFI associated AEs (C), background population rate (B), and population (P), the total expected AEs can be modeled with equation I.
When there are no cardiac AEFI associated AEs (C = 0), this reduces to equation II.
For each AE in VAERS, normalized AE frequencies per P=100,000 VAERS reports for all AEs can be calculated with equation III.
A candidate cardiac AEFI safety signal is detected when AE(X, Vi) is significantly different from AE(X, Vj) which implies the difference is from the CX,V terms because the BX,V should be essentially equivalent when comparing equation I for two vaccines (Vi and Vj).
2.4. Statistical Analysis
Microsoft Excel was used to calculate Pearson correlations and prepare figures. Pearson correlations were done for 119 vaccines with median normalized frequency greater than zero for the MedDRA terms examined (see Supplemental Data tables). Chi-square calculations were performed with online chi-square 2x2 calculator [27].
3. Results
3.1. Arrhythmia AEs
Arrhythmia is a condition with an irregular heartbeat, which can be irregular, rapid, or too slow heartbeat. Normalized frequencies for arrhythmia AEs are illustrated in Figure 1. Nine vaccines have arrhythmia normalized frequencies greater than 200 per 100,000 VAERS reports (>1 in 500 reports) and four with normalized frequencies greater than 500 per 100,000 VAERS reports (>1 in 200 reports) (Figure 1). COVID-19 (Pfizer-BioNTech) has the highest normalized frequency of 1,442 per 100,000 (1 in 69) vaccinees with symptoms reported to VAERS. The COVID-19 Janssen, Moderna, and Novavax vaccines have normalized frequencies ranging from 2.8 to 3.8 times lower (Figure 1). HPV Cervarix vaccine also has a normalized arrhythmia frequency of 572 per 100,000. Arrhythmia AEFI have been previously reported for HPV [28,29] and COVID-19 [5,6,7,8] vaccines. Six vaccines with more than 5,000 VAERS reports have normalized frequencies less than 20 per 100,000 VAERS reports [MENINGOCOCCAL CONJUGATE (MENACTRA), INFLUENZA (SEASONAL) (FLUMIST), HIB (PEDVAXHIB), MENINGOCOCCAL B (BEXSERO), DTAP + HEPB + IPV (PEDIARIX), ROTAVIRUS (ROTARIX)], hence the background population rate (Barrhythmia) may be less than 20 per 100,000 VAERS reports.
3.2. Atrial Fibrillation AEs
Atrial fibrillation is a condition with an irregular and rapid heartbeat. Normalized frequencies of atrial fibrillation AEs are illustrated in Figure 2. Twelve vaccines have atrial fibrillation normalized frequencies greater than 200/100K VAERS reports with nine greater than 500/100K VAERS reports (Figure 2). COVID-19, influenza (seasonal), and RSV vaccines respectively have four, three, and two vaccines with normalized frequencies greater than or equal to 500 per 100,000 VAERS reports. Atrial fibrillation AEFI has been previously reported for COVID-19 vaccines [9,10,11]. Influenza (seasonal) Fluad quadrivalent, Fluzone high-dose quadrivalent, and Fluad are all statistically different from Fluzone quadrivalent by Chi-square test with p-value < 0.00001. Ten vaccines with more than 5,000 VAERS reports have normalized frequencies less than 20 per 100,000 VAERS reports [HEP A (HAVRIX), HEP A (VAQTA), HIB (ACTHIB), HPV (GARDASIL 9), HPV (GARDASIL), MEASLES + MUMPS + RUBELLA (MMR II), MENINGOCOCCAL CONJUGATE (MENACTRA), PNEUMO (PREVNAR), POLIO VIRUS, INACT. (IPOL), VARICELLA (VARIVAX)], hence Batrial fibrillation < 20 per 100,000 VAERS reports. For other cardiac AEs, atrial fibrillation has Pearson correlation coefficients: r=0.42 arrhythmia, 0.24 chest discomfort, 0.17 chest pain, and 0.44 palpitations.
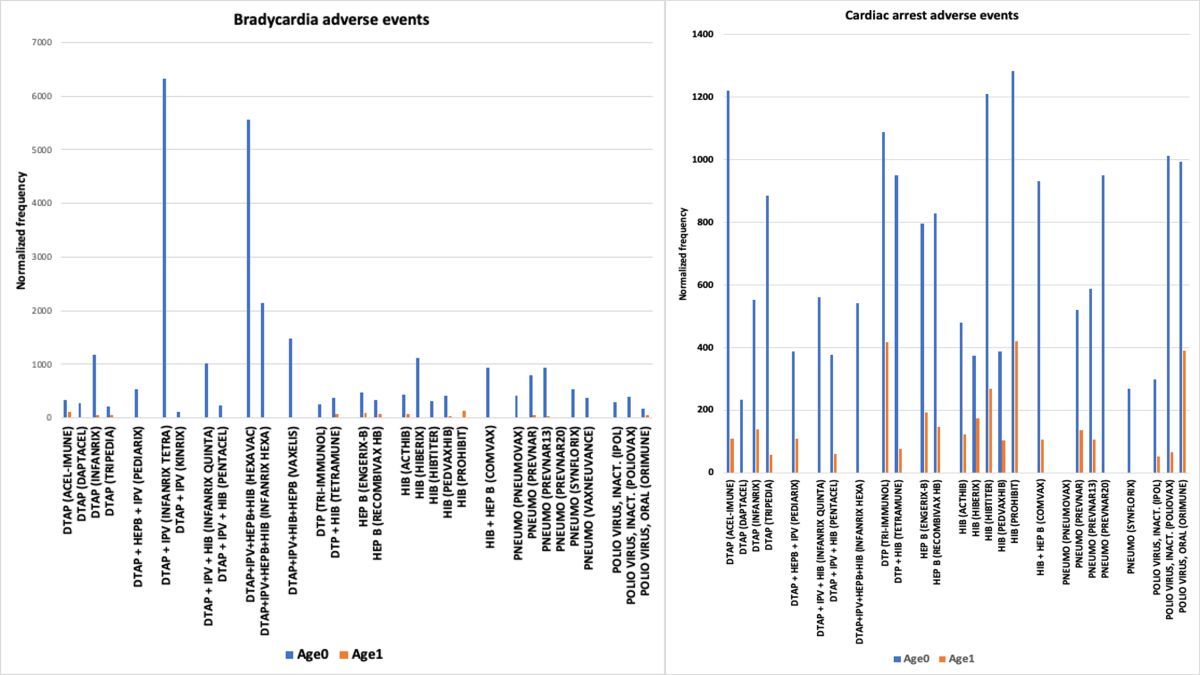
3.3. Bradycardia AEs
Bradycardia is a condition where the heart beats too slowly (less than 60 beats per minute) while at rest. The highest normalized frequencies for bradycardia AEs were concentrated in childhood vaccines (see Supplemental Data table for bradycardia). Normalized frequencies for bradycardia AEs are illustrated for infants aged 0 and 1 in VAERS in Figure 3. Note that DTAP+IPV+HEPB+HIB (HEXAVAC) is no longer authorized. For infants, age 0, 27 have bradycardia normalized frequencies > 200/100K VAERS reports and 12 vaccines > 500/100K VAERS reports (Figure 3); in comparison, for infants, age 1, no vaccines have bradycardia normalized frequencies > 200/100K VAERS reports (Figure 3). For matched vaccine pairs for infants aged 0 there are Chi-squared statistical differences for DTAP Infanrix vs. Tripedia, DTAP + IPV Infanrix tetra vs. Pentacel, and HIB Hiberix vs Hibtiter with p-value < 0.00001. For infants aged 0 vs 1, three vaccines have Chi-squared statistical differences: DTAP Infanrix (p<0.00001), Pneumo Prevnar (p<0.00001), and Pneumo Prevnar13 (p<0.00001). Individual vaccines with normalized frequencies greater than 500 per 100,000 VAERS reports include DTAP (Infanrix: 1182), HIB (Hiberix: 1124), DTP + IPV (Infanrix tetra: 6329), DTAP + IPV + HIB (Infanrix quinta: 1011), DTAP+IPV+HEPB+HIB (Infanrix hexa: 2135), DTAP+IPV+HIB+HEPB (Vaxelis: 1474), HIB + HEPB (Comvax: 931), and Pneumo (Prevnar: 803, Prevnar13: 934, and Synflorix: 535) (Figure 3). Bradycardia has been previously reported associated with preterm infants and ELBW infants [19,20,21]. Five vaccines with more 5,000 VAERS reports have bradycardia normalized frequencies less than 20 per 100,000 VAERS reports [INFLUENZA (SEASONAL) (AFLURIA), INFLUENZA (SEASONAL) (FLUMIST), INFLUENZA (SEASONAL) (FLUZONE HIGH-DOSE), MEASLES + MUMPS + RUBELLA (MMR II)+VARICELLA (VARIVAX), MEASLES + MUMPS + RUBELLA + VARICELLA (PROQUAD)], hence Bbradycardia may be less than 20 per 100,000 VAERS reports. For other cardiac AEs, bradycardia normalized frequencies have Pearson correlation coefficients: r=0.22 arrhythmia, 0.21 cardiac arrest, 0.21 palpitations, 0.28 pericarditis, and 0.20 tachycardia.
Specific concomitant vaccine combinations have higher bradycardia AEFI normalized frequencies (Figure 4). Twenty two vaccines have bradycardia adverse events greater than 1,000 per 100K VAERS reports (Figure 4). Some vaccines occur multiple times in these concomitant combinations, including: 9 - PNEUMO (PREVNAR13) and 4 PNEUMO (PREVNAR), 6 – DTAP+IPV+HEPB+HIB (INFANRIX HEXA), 6 – DTAP+HEPB+IPV (PEDIARIX), 2 – ROTAVIRUS (ROTATEQ), 2 – ROTAVIRUS (ROTARIX), 2 HIB (PEDVAXHIB), 2 – HIB (ACTHIB), 2 – HEP A (HAVRIX), 2 – DTAP (INFANRIX), and 2 – COVID19 (PFIZER-BIOTECH BIVALENT) (Figure 4). These concomitant vaccine combinations are consistent with both additive or synergy safety signals.
3.4. Cardiac Arrest AEs
Cardiac arrest occurs when the heart stops beating. Normalized frequencies for cardiac arrest AEs are illustrated for infants aged 0 and 1 in VAERS in Figure 5. For infants, age 0, 25 vaccines have cardiac arrest normalized frequencies > 200/100K VAERS reports and 17 vaccines > 500/100K VAERS reports (Figure 5); in comparison, for infants, age 1, four vaccines have cardiac arrest normalized frequencies > 200/100K and no vaccines have cardiac arrest normalized frequencies > 500/100K VAERS reports (Figure 5). Four pairs of matched vaccines for infants aged 0 have Chi-squared significant differences: DTAP Acel-imune vs. Daptacel (p=0.000058), DTAP Tripedia vs Daptacel (p=0.00065), Polio virus inactive Poliovax vs Ipol (p=0.000011), and Polio virus oral Orimune vs inactive Ipol (p<0.00001). Comparison of infants aged 0 to age 1 for the same vaccine have Chi-squared significant differences for 13 vaccines: DTAP Acel-immune (p=0.0033), DTAP Infanrix (p=0.000186), DTAP Tripedia (p<0.00001), DTP+HIB Tetramune (p=0.0015), Hep B Recombivax HB (p=0.0067), HIB Acthib (p=0.0001), HIB Hibtiter (p<0.00001), HIB Pedvaxhib (p=0.004671), HIB+HEP B Comvax (p=0.00034), Pneumo Prevnar (p<0.00001), Pneumo Prevnar13 (p<0.00001), polio virus inactive Poliovax (p=0.00030), and polio virus oral Orimune (p=0.00019). Normalized frequencies for infants less than 1 year of age are higher than the normalized frequencies for year old infants (Figure 5). Five vaccines with more 5,000 VAERS reports have cardiac arrest normalized frequencies less than 20 per 100,000 VAERS reports [HPV (GARDASIL 9), INFLUENZA (SEASONAL) (AFLURIA), INFLUENZA (SEASONAL) (FLUMIST), INFLUENZA (SEASONAL) (FLUZONE HIGH-DOSE), TDAP (ADACEL)], hence Bcardiac arrest may be less than 20 per 100,000 VAERS reports. For other cardiac AEs, cardiac arrest normalized frequencies have Pearson correlation coefficients: r=0.21 bradycardia, -0.17 palpitations, and 0.33 tachycardia.
Specific concomitant vaccine combinations have higher normalized frequencies exhibiting synergy safety patterns, including: HIB (ACTHIB)+PNEUMO (PREVNAR13)+ROTAVIRUS (ROTATEQ) at 7,547/100K VAERS reports and DTAP (INFANRIX)+HIB (ACTHIB)+MEASLES + MUMPS + RUBELLA + VARICELLA (PROQUAD) at 7,500/100K VAERS reports; both ROTATEQ and PROQUAD contain live attenuated viruses. Other higher frequency concomitant vaccines include the live attenuated oral polio virus (ORIMNUE) or other combinations including aluminum adjuvants (Supplemental Data, cardiac arrest worksheet, Combination report).
3.5. Chest Discomfort and Chest Pain AEs
Fifty eight vaccines have normalized frequencies for chest discomfort greater than 500 per 100,000 (Figure 6). Fifty five of these vaccines except for Pneumo (Prevnar20) and RSV (Abrysvo and Arexvy) overlap with chest pain AEs (see Supplemental Data tables for chest discomfort and chest pain). Fifty nine vaccines have chest discomfort normalized frequencies greater than 200/100K VAERS reports with 52 vaccines > 500/100K VAERS reports (Figure 6). Sixty five vaccines have chest pain normalized frequencies > 200/100K VAERS reports and 55 vaccines > 500/100K VAERS reports. Chest pain AEFI has been previously reported for COVID-19 vaccines [7,12,13,14,15]. Seven vaccines with more 5,000 VAERS reports have chest discomfort normalized frequencies less than 20 per 100,000 VAERS reports [DTAP + HEPB + IPV (PEDIARIX), DTAP + IPV + HIB (PENTACEL, HIB (ACTHIB), HIB (PEDVAXHIB), HIB + HEP B (COMVAX), ROTAVIRUS (ROTARIX), ROTAVIRUS (ROTATEQ)]; children vaccines are over represented in this list and represent a different age population from Figure 6 vaccines. For other cardiac AEs, chest discomfort normalized frequencies have Pearson correlation coefficients: r=0.24 atrial fibrillation, 0.71 chest pain, 0.53 myocarditis, 0.60 palpitations, and 0.66 pericarditis. Likewise, for other cardiac AEs, chest pain normalized frequencies have Pearson correlation coefficients: r=0.17 arrhythmia, 0.71 chest discomfort, 0.80 myocarditis, 0.54 palpitations, 0.76 pericarditis, and 0.24 tachycardia.
3.6. Myocarditis and Pericarditis AEs
Myocarditis is inflammation of the heart muscle (myocardium). Pericarditis is inflammation of the sac that surrounds the heart (pericardium). Seven vaccines have myocarditis normalized frequencies greater than 200/100K VAERS reports with 6 vaccines > 500/100K VAERS reports (Figure 7). Eight vaccines have pericarditis normalized frequencies greater than 200/100K VAERS reports with 5 vaccines > 500/100K VAERS reports (Figure 7). The normalized frequencies for myocarditis AEs are shown in Figure 8 for males and Figure 9 for females. Age stratified results could be considered consistent with linear relationships when plotted on log scales for both genders for multiple vaccines (Figure 8 and Figure 9). Myocarditis/pericarditis have been previously reported for COVID-19 [5,7,16,17,18] and smallpox [2] vaccines. Analysis of the WHO pharmacovigilance database detected associations for pericarditis and myocarditis with smallpox, anthrax, typhoid, encephalitis, influenza, and coronavirus disease 2019 (COVID-19) adenovirus type 5 (AD5)-vectored vaccines [4]. For COVID-19 mRNA vaccines, circulating Spike proteins are observed in vaccinees with myocarditis [30] along with elevated cardiac troponin levels [31]. COVID-19 mRNA vaccine myocarditis occurs in males with the highest number of cases [32]. Gender differences in cardiac mast cells activation have also been observed [33]. Pericarditis AEs occur with nearly identical pattern of normalized AEs as myocarditis AEs (Figure 7), consistent with a shared etiology for both of these cardiac AEs. Eleven vaccines with more 5,000 VAERS reports have myocarditis normalized frequencies less than 20 per 100,000 VAERS reports [DTAP (DAPTACEL), DTAP + HEPB + IPV (PEDIARIX), DTAP + IPV + HIB (PENTACEL), DTP + HIB (TETRAMUNE), HEP A (VAQTA), HIB (PEDVAXHIB), INFLUENZA (SEASONAL) (FLUVIRIN), INFLUENZA (SEASONAL) (FLUZONE HIGH-DOSE), ROTAVIRUS (ROTATEQ), VARICELLA (VARIVAX), ZOSTER LIVE (ZOSTAVAX)], hence Bmyocarditis may be less than 20 per 100,000 VAERS reports. Fifteen vaccines with more 5,000 VAERS reports have pericarditis normalized frequencies less than 20 per 100,000 VAERS reports [DTAP (DAPTACEL), DTAP (INFANRIX), DTAP (TRIPEDIA), HEP A (VAQTA), HIB (ACTHIB), HIB (PEDVAXHIB), INFLUENZA (H1N1) (H1N1 (MONOVALENT) (SANOFI)), INFLUENZA (SEASONAL) (FLUVIRIN), MEASLES + MUMPS + RUBELLA (MMR II), PNEUMO (PREVNAR), PNEUMO (PREVNAR13), POLIO VIRUS, INACT. (IPOL), POLIO VIRUS, ORAL (ORIMUNE), TDAP (ADACEL), VARICELLA (VARIVAX)], hence Bpericarditis < 20 per 100,000 VAERS reports. For other cardiac AEs, myocarditis normalized frequencies have Pearson correlation coefficients: r=0.53 chest discomfort, 0.80 chest pain, 0.26 palpitations, and 0.76 pericarditis. Likewise, for other cardiac AEs, pericarditis normalized frequencies have Pearson correlation coefficients: r=0.22 arrhythmia, 0.28 bradycardia, 0.66 chest discomfort, 0.76 chest pain, 0.76 myocarditis, and 0.53 palpitations.
3.7. Palpitations
Palpitations are feelings of the heart pounding, racing, or fluttering. The normalized frequencies for palpitation AEs exhibit gender differences across most vaccines (Figure 10). For females, 67 vaccines have palpitations adverse events normalized frequencies > 200/100K VAERS reports and 57 vaccines > 500/100K VAERS reports (Figure 10); for males, 57 have palpitations adverse events normalized frequencies > 200/100K VAERS reports and 35 vaccines > 500/100K VAERS reports (Figure 10). Palpitation AEFI have been previously reported for COVID-19 [7,15] and smallpox [34] vaccines. Seven vaccines with more 5,000 VAERS reports have normalized frequencies less than 20 per 100,000 VAERS reports [DTAP (TRIPEDIA), DTAP + IPV (KINRIX), HIB (HIBTITER), HIB (PEDVAXHIB), POLIO VIRUS, ORAL (ORIMUNE), ROTAVIRUS (ROTARIX), ROTAVIRUS (ROTATEQ)]; children vaccines are over represented in this list and represent a different age population from Figure 10 vaccines. For other cardiac AEs, palpitation normalized frequencies have Pearson correlation coefficients: r=0.23 arrhythmia, 0.44 atrial fibrillation, 0.21 bradycardia, -.017 cardiac arrest, 0.60 chest discomfort, 0.54 chest pain, 0.26 myocarditis, 0.53 pericarditis, and 0.34 tachycardia.
3.8. Tachycardia
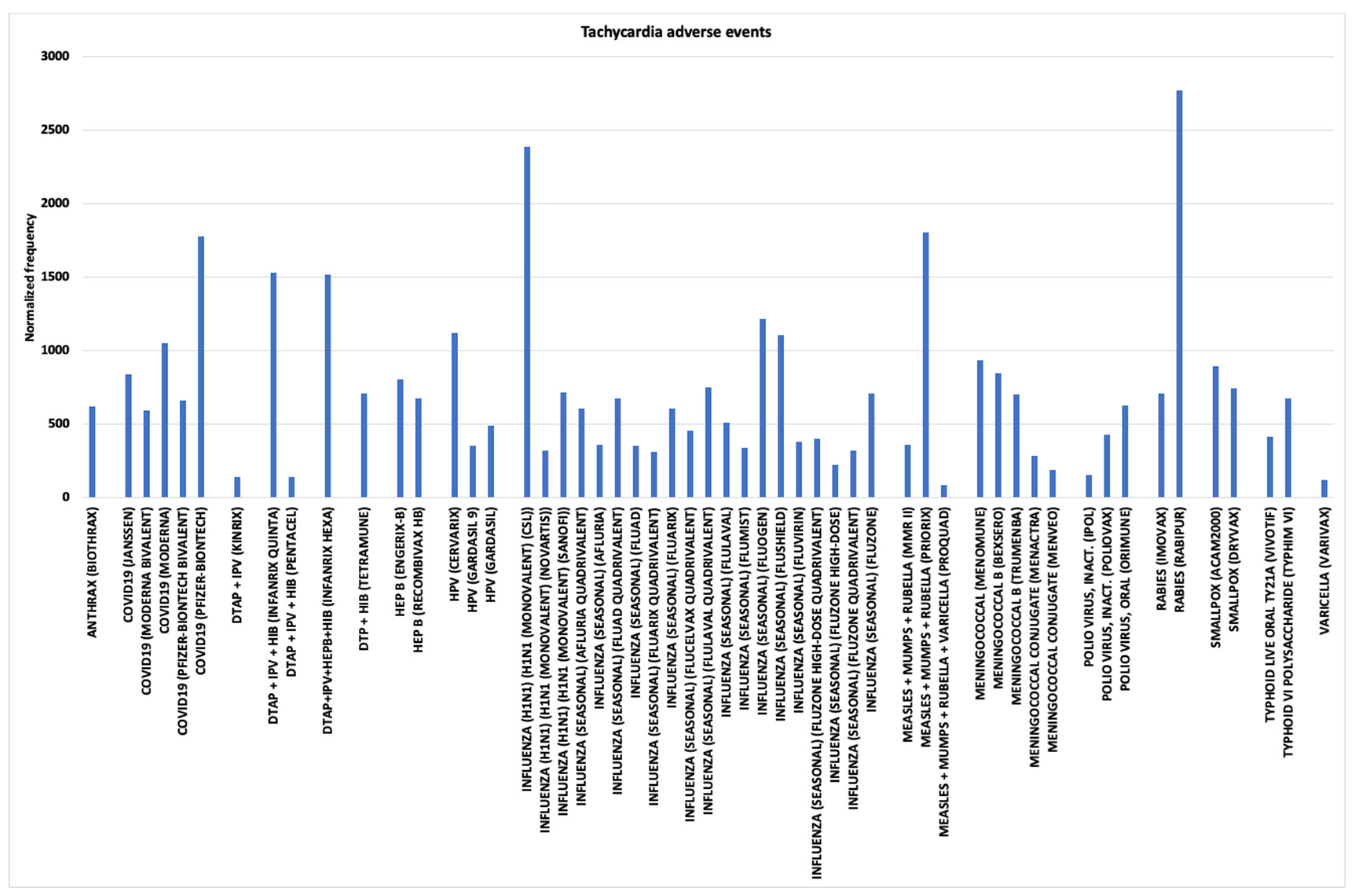
Tachycardia is a condition with a rapid heartbeat. Normalized frequencies for tachycardia AEs are shown in Figure 11 with 42 higher than 500 AEs per 100,000 shots with AEs. Sixty vaccines have tachycardia AEs normalized frequencies > 200/100K VAERS reports and 42 vaccines > 500/100K VAERS reports (Figure 11). No vaccines with more 5,000 VAERS reports have normalized frequencies less than 20 per 100,000 VAERS reports. Tachycardia AEFI/AESIs have been previously reported for COVID-19 [15] and smallpox [34] vaccines. For other cardiac AEs, tachycardia normalized frequencies have Pearson correlation coefficients: r=0.20 bradycardia, 0.33 cardiac arrest, 0.24 chest pain, and 0.34 palpitations.
4. Discussion
Multiple candidate safety signals were detected for the cardiac AEFIs examined; these AEFIs can be clustered into four groups based on the associated vaccines. First, arrhythmia candidate safety signals were observed for COVID-19 vaccines and HPV Cervarix. Second, atrial fibrillation candidate safety signals were observed for COVID-19 vaccines, three influenza vaccines (including two high-dose vaccines), and two RSV vaccines. Third, candidate safety signals were detected affecting infants aged 0 for both bradycardia and cardiac arrest AEFIs for specific vaccines; several of the vaccines have statistically significant lower normalized frequencies for the same vaccines from alternative source(s); one or more causative components differ in concentration between these matched pairs of vaccines. For these vaccines, the dosage levels may need to be adjusted for younger infants based on age/body weight. And, fourth, multiple candidate safety signals were observed for overlapping sets of vaccines for chest discomfort, chest pain, myocarditis, palpitations, pericarditis, and tachycardia AEFIs; the etiologies of these AEFIs are likely shared within each group across different vaccines.
Cardiac AEFIs may be triggered or caused by one or more components within vaccine shots; vaccine components, adjuvants, excipients, or manufacturing contaminant(s) are possible causative agent(s) of SAE associations. Endotoxins are one possible manufacturing contaminant. Exposure to endotoxins have been determined to cause depression of left ventricular function in humans [35,36]. The Toll-like receptor TLR4 is activated by lipopolysaccharide (LPS, endotoxin) of Gram-negative bacteria [37]. It is possible that manufacturing contaminants (e.g., endotoxins or DNA contaminants) may have a role in the etiology of some cardiac AEFI associations.
4.1. Immune System Signaling Molecules
Elevated levels of some molecules are known to be associated with cardiac AEs; their role in cardiac AEFIs have not been elucidated yet. Cardiac adverse events of the β-imanazolylethylamine derivative of histamine include altered blood-pressure, coronary arterioles constriction, pulmonary arterioles constriction, altered heart rate, and heart failure varying by dose and animal species [38]; it is well known that elevated histamine levels can induce a variety of cardiac adverse events [38]. Histamine and other inflammatory molecules are released as part of immune responses to immunization. To prime immune responses against possible future pathogen exposures, immunizations are intended to activate both innate and humoral immune responses to stimulate B cells and T cells that can recognize these target pathogen proteins. Activated innate immune granulocytes, including mast cells, release histamine and other inflammatory molecules. Activated platelets are an additional source of histamine, serotonin, and additional inflammatory molecules. Some individuals have different sensitivity thresholds to elevated histamine levels; histamine intolerance (HIT) is associated with cardiac arrhythmias [39] and cardiac AEs [40]. Ingestion of alcohol, histamine-rich food, drugs that block diamine oxidase (DAO) (histamine metabolism) or release histamine, or pregnancy can affect an individual’s histamine tolerance level [40]. Genetic variants in the DAO enzyme can impact histamine metabolism and tolerance threshold level. Histamine induced contraction of cardiac capillary cells has been proposed as an initial step in myocarditis etiology [41]. Elevated serotonin (5-hydroxytryptamine) is associated with some cardiac diseases and coronary artery disease [42]; serotonin affects the vascular wall, proliferation of smooth muscle cells, promotes thrombogenesis and mitogenesis [42], and vasoconstriction [42,43]. The roles of elevated histamine, serotonin, and other inflammatory molecules in cardiac AEFIs are candidates for future studies.
Multiple cardiac AEFIs may result from immune response signaling molecules, including elevated levels of histamine, serotonin, and other inflammatory molecules. Cardiac AEs are associated with elevated histamine levels [38,39,40]. Elevated histamine and/or serotonin levels may be involved in cardiac capillary vasoconstrictions [38,42,43]; histamine induced contraction of cardiac capillary cells may be involved in cardiac AEFIs including myocarditis and pericarditis [41]. For COVID-19 vaccines, the Spike protein disrupts cardiac pericytes through cluster of differentiation 147 (CD147) receptor-mediated signaling and another unknown mechanism [44]. The Spike protein also activates mast cells via TLR4 and angiotensin-converting enzyme 2 (ACE2) receptors [45]. Gender differences in mast cells activation are known [33]. This is consistent with different patterns of AEFI normalized frequencies for each gender observed in Figure 8 and Figure 9. The first, second, and fourth group of clustered cardiac AEFIs, may have elevated histamine, serotonin, and/or inflammatory molecule levels involved in the arrhythmia (Figure 1), atrial fibrillation (Figure 2), chest discomfort (Figure 6), chest pain, palpitations (Figure 10), tachycardia (Figure 11), and additional cardiac AEFIs etiologies.
Hypothesis:
Some cardiac AEFIs are associated with elevated levels of histamine, serotonin, and other inflammatory molecules released by immune responses to immunization; some vaccinees may have lower threshold levels associated with these AEFIs (with histamine thresholds influenced by consumed foods, alcohol, drugs, and pregnancy).
4.2. Myocarditis and Pericarditis AEFIs
Multiple candidate safety signals were observed for myocarditis and pericarditis for the same set of vaccines (see Figure 7). The normalized frequencies are higher for males than females (see Figure 8 and Figure 9). Gender differences in mast cell activations are known [33].
Hypothesis:
Initial etiology of cardiac myocarditis and pericarditis AEFIs involve activation of cardiac mast cells followed by (1) cardiac capillary vasoconstrictions from contracted pericyte cells and (2) localized cardiac cell death from anoxia (releasing troponin, etc.)
For myocarditis and pericarditis AEFIs, circulating Spike proteins from COVID-19 vaccines contribute to the activation of mast cells, contraction of cardiac capillary pericyte cells, and release of inflammatory molecules from endothelial inflammation [44,45,46]. The proposed model is that the frequencies of myocarditis and pericarditis AEFIs are directly correlated with activation levels of cardiac mast cells/elevated histamine levels inducing contracted cardiac capillary pericyte cells causing vasoconstrictions and localized cardiac myocyte cell death from anoxia; this is being observed for anthrax, COVID-19, smallpox, TD absorbed, tick-borne encephalitis, typhoid, and yellow fever vaccines (Figure 7).
4.3. Cardiac AEFI Comparisons Across Vaccines
Across the cardiac AEFIs examined, five vaccines were frequently observed (Figure 1, Figure 2, Figure 6, Figure 7, Figure 10 and Figure 11): anthrax, COVID-19, influenza, smallpox, and typhoid. For the general population, the highest normalized frequencies were observed for arrhythmia – COVID19 (PFIZER-BIONTECH) (Figure 1), atrial fibrillation – RSV (ABRYSVO) (Figure 2), chest discomfort, myocarditis, and pericarditis – SMALLPOX (ACAM2000) (Figure 6 and Figure 7), palpitations – COVID19 (NOVAVAX) (Figure 10), and tachycardia – RABIES (RABIPUR) (Figure 11). The etiology of these cardiac AEFIs remain unknown. The overall patterns are consistent with AEs associated with elevated histamine, possibly serotonin, and other inflammatory molecules. For the COVID19 vaccines associated myocarditis and pericarditis linked to circulating Spike protein provides the likely trigger molecule [30]. Overall, COVID-19 are associated with all of the examined cardiac AEFIs with other vaccines sometimes having higher normalized frequencies.
4.4. Bradycardia and Cardiac Arrest in Infants Vaccinees Aged 0
Some infants less than 1 year of age are sensitive to one or more components in specific vaccines associated with both bradycardia and cardiac arrest AEFIs (Figure 3, Figure 4 and Figure 5). By age 1, the observed normalized frequencies are consistently much lower, often with statistical significance. For some vaccines, statistically significant differences in normalized frequencies are observed for the same vaccine from different sources for infants aged 0 for both bradycardia and cardiac arrest AEFIs; this is likely due to differences in adjuvants, etc. For the specific vaccines with high normalized frequencies, shared vaccine component (in particular, live attenuated viruses), common adjuvants (e.g., aluminum), common excipients, or possible manufacturing contaminant(s) (e.g., endotoxins, DNA) are likely causative. Elevated normalized frequencies were observed for some concomitant vaccine combinations (Figure 4). These combinations may be indicating that certain combinations should be avoided, possibly including two or more aluminum adjuvanted vaccines, live attenuated virus vaccine with other vaccines, etc.; multiple aluminum adjuvanted vaccines could be exceeding tolerance threshold levels for some infants. Surprisingly, the same pattern for infants aged 0 and the same vaccines was also observed for epilepsy AEs [47]; this is suggestive of a common neurocardiology shared etiology for all three of these AEs. Aluminum adjuvants have also been correlated with persistent asthma [48] and autism spectrum disorders [49]. Cardiac AEs are known to be associated with endotoxin exposures in humans [35,36]. An overall pattern of possible dosage levels being too high for younger infants needs to be seriously considered.
Hypothesis:
The dose levels for infants with bradycardia and cardiac arrest AEFIs may be too high for their body weight/age resulting in over stimulated immune responses; candidate causative components include live attenuated viruses, aluminum adjuvants, and several concomitant vaccine combinations.
The vaccinees body weight is a crucial consideration in determination of treatment dosages. AEFI evidence of infants age 0 having higher AEFI normalized frequencies than infants age 1 is suggestive that the dosage of infant vaccines likely needs to be adjusted (i.e., reduced) for smaller (younger) infants. Lyons-Weiler & Ricketson [50,51] advocate for reconsidering the immunotherapeutic pediatric safe dose levels of aluminum. Applying Occam’s razor to the vaccines and concomitant vaccine combinations, candidate causative components include: (1) live attenuated vaccines and (2) aluminum adjuvanted vaccines (examining vaccine excipients [52]). Adjuvants have been associated with Autoimmune/ inflammatory syndrome induced by adjuvants (ASIA) [53]. Concomitant administration of multiple aluminum adjuvanted vaccines may exceed aluminum tolerance threshold for some infants; other concomitant vaccine combinations may be over stimulating immune responses in younger/smaller infants.
4.5. Study Limitations
Only a small subset of vaccinees AEs are reported to the VAERS database. Reporting biases and exclusion of AEs would perturb calculated AEs normalized frequencies. To estimate population AEFI frequencies, increase the population size (P) to include asymptomatic vaccinees.
4.6. Study Recommendations
The results from this study suggest multiple possible follow-up studies. First, examining some of the detected safety signals for identified vaccines with elevated AEFI normalized frequencies could be included as part of ongoing or future clinical studies. Second, infants age 0 have higher normalized bradycardia and cardiac arrest AEFIs than infants age 1 for several vaccines and concomitant combinations (Figure 3, Figure 4 and Figure 5). Options to minimize these AEFIs, include (1) adjusting vaccine dosage to infant body weight/age, (2) delaying immunization of some of these vaccines for infants aged 0 until older, (3) selecting alternative vaccines that are observed with lower AEFIs frequencies, or (4) avoiding concomitant vaccine combinations associated with increased risk levels (e.g., live attenuated viruses combined with aluminum adjuvant vaccines, etc.). Third, when unavailable, develop alternatives to live attenuated vaccines with improved safety profiles. Fourth, evaluation of antihistamines as possible adjunctive therapies for myocarditis and pericarditis AEFIs. Fifth, development of COVID-19 alternative vaccines (e.g., T-cell vaccines targeting other SARS-CoV-2 proteins) that do not include the Spike protein [54]. Understanding the etiology of these cardiac AEFIs may lead to procedures to minimize their occurrences.
5. Conclusion
Infant bradycardia and cardiac arrest AEFIs can be reduced by either adjusting vaccine dosage level for child body weight/age, delaying specific vaccines until infants are 1 year of age, selecting alternative vaccine options with observed lower AEFI frequencies, avoiding concomitant vaccine combinations with higher combination risk levels, solo administration of live attenuated virus vaccines, or reduction or elimination of causative components (e.g., aluminum adjuvant). Both male and female myocarditis AEs can be modeled by mathematical log scale age relationships for COVID-19 vaccines that may also apply to additional vaccines, suggesting possible shared etiologies with likely involvement of cardiac mast and pericyte cells. Multiple vaccines were observed with correlated cardiac AEFIs association signals for chest discomfort, chest pain, palpitations, and tachycardia; elevated histamine levels may contribute to the etiologies of these AEFIs. Alternatives to COVID-19 Spike vaccines are recommended to eliminate myocarditis and pericarditis associated risks with current SARS-CoV-2 vaccines.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Distribution Statement: A. Approved for public release. Distribution is unlimited. This material is based upon work supported by the Department of the Air Force under Air Force Contract [No. FA8702-15-D-0001]. Any opinions, findings, conclusions, or recommendations expressed in this material are those of the author and do not necessarily reflect the views of the Department of the Air Force.
Acknowledgments
MedDRA® trademark is registered by ICH.
Ethical Approval: Not applicable.
Conflicts of Interest
The author declares no conflict of interest. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- Vaccine Adverse Event Reporting System (VAERS). 2024. Available online: https://vaers.hhs.gov/data.html (accessed on 10 July 2024).
- Cassimatis DC, Atwood JE, Engler RM, Linz PE, Grabenstein JD, Vernalis MN. Smallpox vaccination and myopericarditis: a clinical review. J Am Coll Cardiol. 2004, 43, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Mittermayer, C. Lethal Complications of Typhoid-Cholera-Vaccination (Case Report and Review of the Literature). Beitr Pathol. 1976, 158, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Lee S, Jo H, Lee H, et al. Global estimates on the reports of vaccine-associated myocarditis and pericarditis from 1969 to 2023: Findings with critical reanalysis from the WHO pharmacovigilance database. J Med Virol. 2024, 96, e29693. [Google Scholar] [CrossRef]
- Ho JSY, Sia C-H, Ngiam JN, et al. A review of COVID-19 vaccination and the reported cardiac manifestations. Singapore Med J 2023, 64. [Google Scholar]
- Sangpornsuk N, Rungpradubvong V, Tokavanich N, et al. Arrhythmias after SARS-CoV-2 Vaccination in Patients with a Cardiac Implantable Electronic Device: A Multicenter Study. Biomedicines 2022, 10. [Google Scholar] [CrossRef]
- Chiu S-N, Chen Y-S, Hsu C-C, et al. Changes of ECG parameters after BNT162b2 vaccine in the senior high school students. Eur J Pediatr. 2023, 182, 1155–1162. [Google Scholar] [CrossRef]
- Stowe J, Whitaker HJ, Andrews NJ, Miller E. Risk of cardiac arrhythmia and cardiac arrest after primary and booster COVID-19 vaccination in England: A self-controlled case series analysis. Vaccine: X. 2023, 15, 100418. [Google Scholar] [CrossRef]
- Chen CY, Hsieh MT, Wei CT, Lin CW. Atrial Fibrillation After mRNA-1273 SARS-CoV-2 Vaccination: Case Report with Literature Review. Risk Manag Healthc Policy. 2023, 16, 209–214. [Google Scholar] [CrossRef]
- Ford GA, Hargroves D, Lowe D, et al. Targeted atrial fibrillation detection in COVID-19 vaccination clinics. Eur Heart J Qual Care Clin Outcomes. 2021, 7, 526–528. [Google Scholar] [CrossRef]
- Ruggiero R, Donniacuo M, Mascolo A, et al. COVID-19 Vaccines and Atrial Fibrillation: Analysis of the Post-Marketing Pharmacovigilance European Database. Biomedicines 2023, 11. [Google Scholar] [CrossRef]
- Liao Y-F, Tseng W-C, Wang J-K, et al. Management of cardiovascular symptoms after Pfizer-BioNTech COVID-19 vaccine in teenagers in the emergency department. J Formos Med Assoc. 2023, 122, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Park CH, Yang J, Lee HS, Kim TH, Eun LY. Characteristics of Teenagers Presenting with Chest Pain after COVID-19 mRNA Vaccination. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Kewan T, Flores M, Mushtaq K, et al. Characteristics and outcomes of adverse events after COVID-19 vaccination. J Am Coll Emerg Physicians Open. 2021, 2, e12565. [Google Scholar] [CrossRef] [PubMed]
- Mansanguan S, Charunwatthana P, Piyaphanee W, Dechkhajorn W, Poolcharoen A, Mansanguan C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop Med Infect Dis 2022, 7. [Google Scholar] [CrossRef]
- Ba C-F, Chen B-H, Shao L-S, et al. CMR Manifestations, Influencing Factors and Molecular Mechanism of Myocarditis Induced by COVID-19 Mrna Vaccine. RCM 2022, 23. [Google Scholar] [CrossRef]
- Cushion S, Arboleda V, Hasanain Y, Demory Beckler M, Hardigan P, Kesselman MM. Comorbidities and Symptomatology of SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2)-Related Myocarditis and SARS-CoV-2 Vaccine-Related Myocarditis: A Review. Cureus. 2022, 14, e24084. [Google Scholar] [CrossRef]
- Goyal M, Ray I, Mascarenhas D, Kunal S, Sachdeva RA, Ish P. Myocarditis post-SARS-CoV-2 vaccination: a systematic review. QJM. 2023, 116, 7–25. [Google Scholar] [CrossRef]
- Botham SJ, Isaacs D, Henderson-Smart DJ. Incidence of apnoea and bradycardia in preterm infants following DTPw and Hib immunization: A prospective study. J Paediatr Child Health. 1997, 33, 418–421. [Google Scholar] [CrossRef]
- Sen S, Cloete Y, Hassan K, Buss P. Adverse events following vaccination in premature infants. Acta Paediatr. 2001, 90, 916–920. [Google Scholar] [CrossRef]
- Lee J, Robinson JL, Spady DW. Frequency of apnea, bradycardia, and desaturations following first diphtheria-tetanus-pertussis-inactivated polio-Haemophilus influenzae type B immunization in hospitalized preterm infants. BMC Pediatr. 2006, 6, 20. [Google Scholar] [CrossRef]
- Slack MH, Schapira C, Thwaites RJ, Andrews N, Schapira D. Acellular pertussis and meningococcal C vaccines: cardio-respiratory events in preterm infants. Eur J Pediatr. 2003, 162, 436–437. [Google Scholar] [CrossRef] [PubMed]
- DeMeo SD, Raman SR, Hornik CP, Wilson CC, Clark R, Smith PB. Adverse Events After Routine Immunization of Extremely Low-Birth-Weight Infants. JAMA Pediatr. 2015, 169, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Knuf M, Charkaluk M-L, The Nguyen PN, et al. Penta- and hexavalent vaccination of extremely and very-to-moderate preterm infants born at less than 34 weeks and/or under 1500 g: A systematic literature review. Hum Vaccin Immunother. 2023, 19, 2191575. [Google Scholar] [CrossRef]
- MedDRA. Medical Dictionary for Regulatory Archives, 2024. Available from: www.meddra.org [Last accessed on 2024 Jul 1].
- Ricke, DO. VAERS-Tools; 2024. Available from: https://github.com/doricke/VAERS-Tools [Last accessed on 2024 Jul 1].
- Chi Square Calculator for 2x2. Social Science Statistics, 2024. Available from: https://www.socscistatistics.com/tests/chisquare/ [Last accessed on 2024 Jul 1].
- Dahan S, Segal Y, Dagan A, Shoenfeld Y, Eldar M. Cardiac arrest following HPV Vaccination. Clin Res Trials. 2019, 5. [Google Scholar] [CrossRef]
- Afrin LB, Dempsey TT, Weinstock LB. Post-HPV-Vaccination Mast Cell Activation Syndrome: Possible Vaccine-Triggered Escalation of Undiagnosed Pre-Existing Mast Cell Disease? Vaccines (Basel). 2022, 10. [Google Scholar] [CrossRef]
- Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis. Circulation. 2023, 147, 867–876. [Google Scholar] [CrossRef]
- Bozkurt B, Kamat I, Hotez PJ. Myocarditis With COVID-19 mRNA Vaccines. Circulation. 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Alami A, Villeneuve PJ, Farrell PJ, et al. Myocarditis and Pericarditis Post-mRNA COVID-19 Vaccination: Insights from a Pharmacovigilance Perspective. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Levick SP, Meléndez GC, Plante E, McLarty JL, Brower GL, Janicki JS. Cardiac mast cells: the centrepiece in adverse myocardial remodelling. Cardiovasc Res. 2011, 89, 12–19. [Google Scholar] [CrossRef]
- FDA. JYNNEOS FDA package insert, 2024. Available from: https://www.fda.gov/media/131078/download [Last accessed on 2024 Aug 28].
- Virzì GM, Clementi A, Brocca A, Ronco C. Endotoxin Effects on Cardiac and Renal Functions and Cardiorenal Syndromes. Blood Purif. 2017, 44, 314–326. [Google Scholar] [CrossRef]
- Suffredini Anthony F, Fromm Robert E, Parker Margaret M, et al. The Cardiovascular Response of Normal Humans to the Administration of Endotoxin. N Engl J Med. 1989, 321, 280–287. [Google Scholar] [CrossRef]
- Ciesielska A, Matyjek M, Kwiatkowska K. TLR4 and CD14 trafficking and its influence on LPS-induced pro-inflammatory signaling. Cell Mol Life Sci. 2021, 78, 1233–1261. [Google Scholar] [CrossRef]
- Dale HH, Laidlaw PP. The physiological action of β-iminazolylethylamine. J Physiol. 1910, 41, 318–344. [Google Scholar] [CrossRef] [PubMed]
- Wolff AA, Levi R. Histamine and cardiac arrhythmias. Circ Res. 1986, 58, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr. 2007, 85, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Fremont-Smith M, Gherlone N, Smith N, Tisdall P, Ricke DO. Models for COVID-19 Early Cardiac Pathology Following SARS-CoV-2 Infection. Int J Infect Dis 2021. [Google Scholar] [CrossRef]
- Vikenes K, Farstad M, Nordrehaug JE. Serotonin Is Associated with Coronary Artery Disease and Cardiac Events. Circulation. 1999, 100, 483–489. [Google Scholar] [CrossRef]
- Golino P, Piscione F, Willerson JT, et al. Divergent Effects of Serotonin on Coronary-Artery Dimensions and Blood Flow in Patients with Coronary Atherosclerosis and Control Patients. N Engl J Med. 1991, 324, 641–648. [Google Scholar] [CrossRef]
- Avolio E, Carrabba M, Milligan R, et al. The SARS-CoV-2 Spike protein disrupts human cardiac pericytes function through CD147 receptor-mediated signalling: a potential non-infective mechanism of COVID-19 microvascular disease. Clin Sci. 2021, 135, 2667–2689. [Google Scholar] [CrossRef]
- Tsilioni I, Theoharides TC. Recombinant SARS-CoV-2 Spike Protein Stimulates Secretion of Chymase, Tryptase, and IL-1β from Human Mast Cells, Augmented by IL-33. Int J Mol Sci 2023, 24. [CrossRef]
- Robles JP, Zamora M, Adan-Castro E, Siqueiros-Marquez L, Martinez de la Escalera G, Clapp C. The spike protein of SARS-CoV-2 induces endothelial inflammation through integrin α5β1 and NF-κB signaling. J Biol Chem. 2022/03/01/ 2022, 298, 101695. [Google Scholar] [CrossRef]
- Ricke, DO. Epilepsy adverse events post vaccination. Explor Neurosci. 2024, 3, 508–519. [Google Scholar] [CrossRef]
- Daley MF, Reifler LM, Glanz JM, et al. Association Between Aluminum Exposure From Vaccines Before Age 24 Months and Persistent Asthma at Age 24 to 59 Months. Acad Pediatr. 2023, 23, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Tomljenovic L, Shaw CA. Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J Inorg Biochem. 2011, 105, 1489–1499. [Google Scholar] [CrossRef] [PubMed]
- Lyons-Weiler J, Ricketson R. Reconsideration of the immunotherapeutic pediatric safe dose levels of aluminum. J Trace Elem Med Biol. 2018, 48, 67–73. [Google Scholar] [CrossRef] [PubMed]
- McFarland G, La Joie E, Thomas P, Lyons-Weiler J. Acute exposure and chronic retention of aluminum in three vaccine schedules and effects of genetic and environmental variation. J Trace Elem Med Biol. 2020, 58, 126444. [Google Scholar] [CrossRef]
- Vaccine Excipient Summary, 2024. Available from: https://canvax.ca/sites/default/files/2020-03/USCDC_VaccineExcipientSummary_2020.pdf [Last accessed on 2025 Jan 6].
- Shoenfeld Y, Agmon-Levin N. ‘ASIA’ – Autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmun. 2011, 36, 4–8. [Google Scholar] [CrossRef]
- Ricke, DO. Two Different Antibody-Dependent Enhancement (ADE) Risks for SARS-CoV-2 Antibodies. Front Immunol. 2021, 12, 443. [Google Scholar] [CrossRef]
Figure 1.
Arrhythmia AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
Figure 1.
Arrhythmia AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
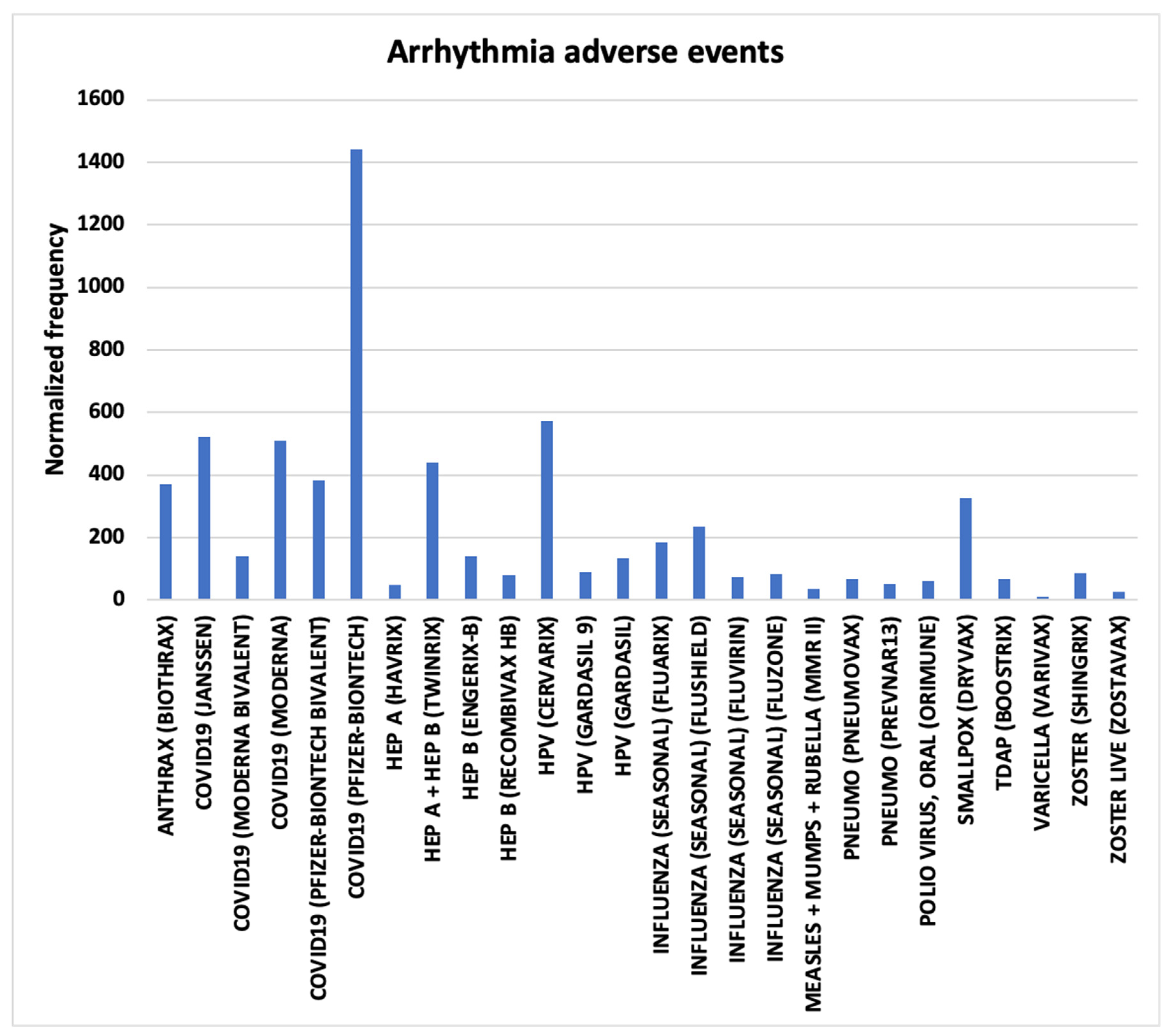
Figure 2.
Atrial fibrillation AEs normalized frequencies from VAERS.
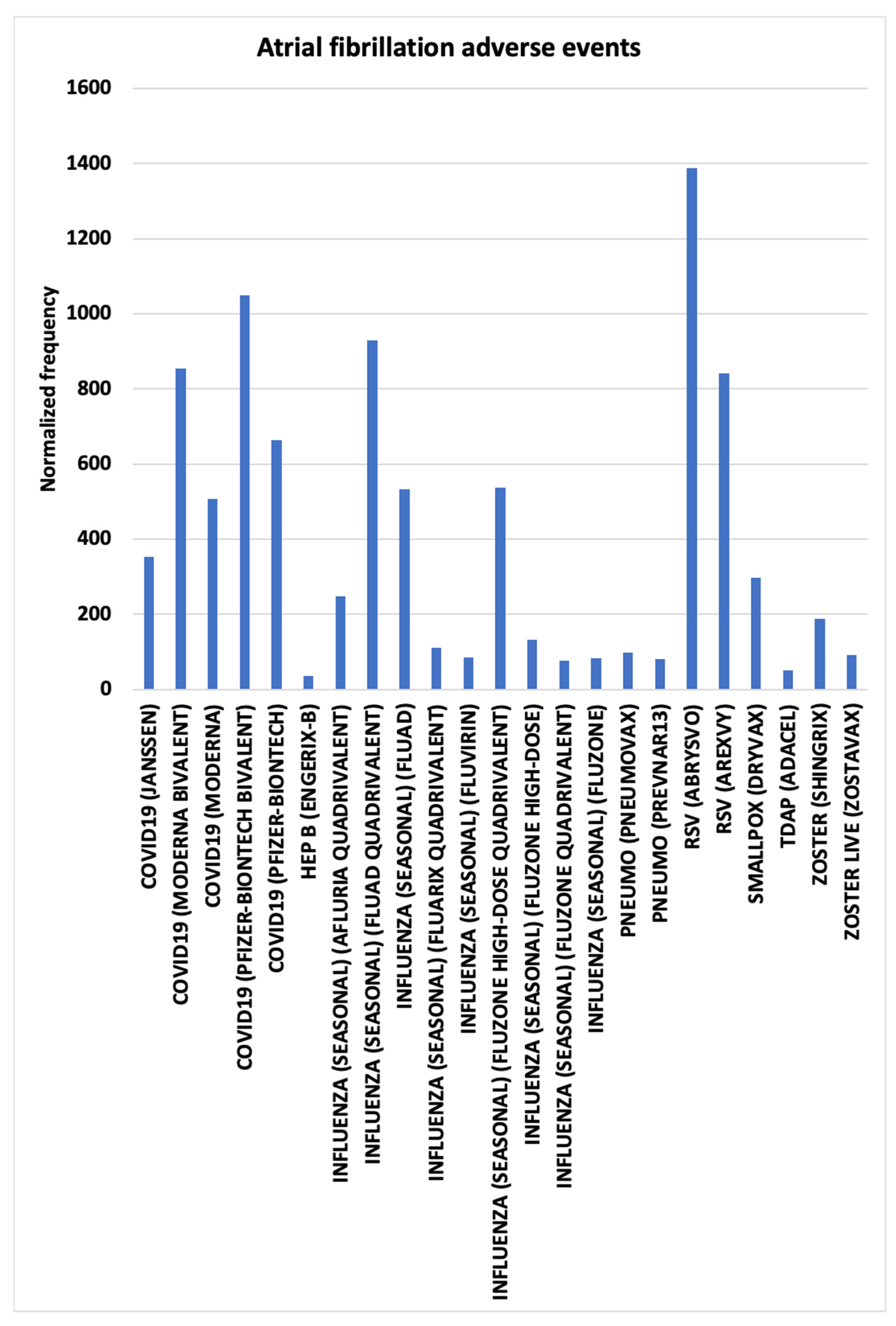
Figure 3.
Bradycardia AEs normalized frequencies for infants aged 0 and 1 from VAERS.
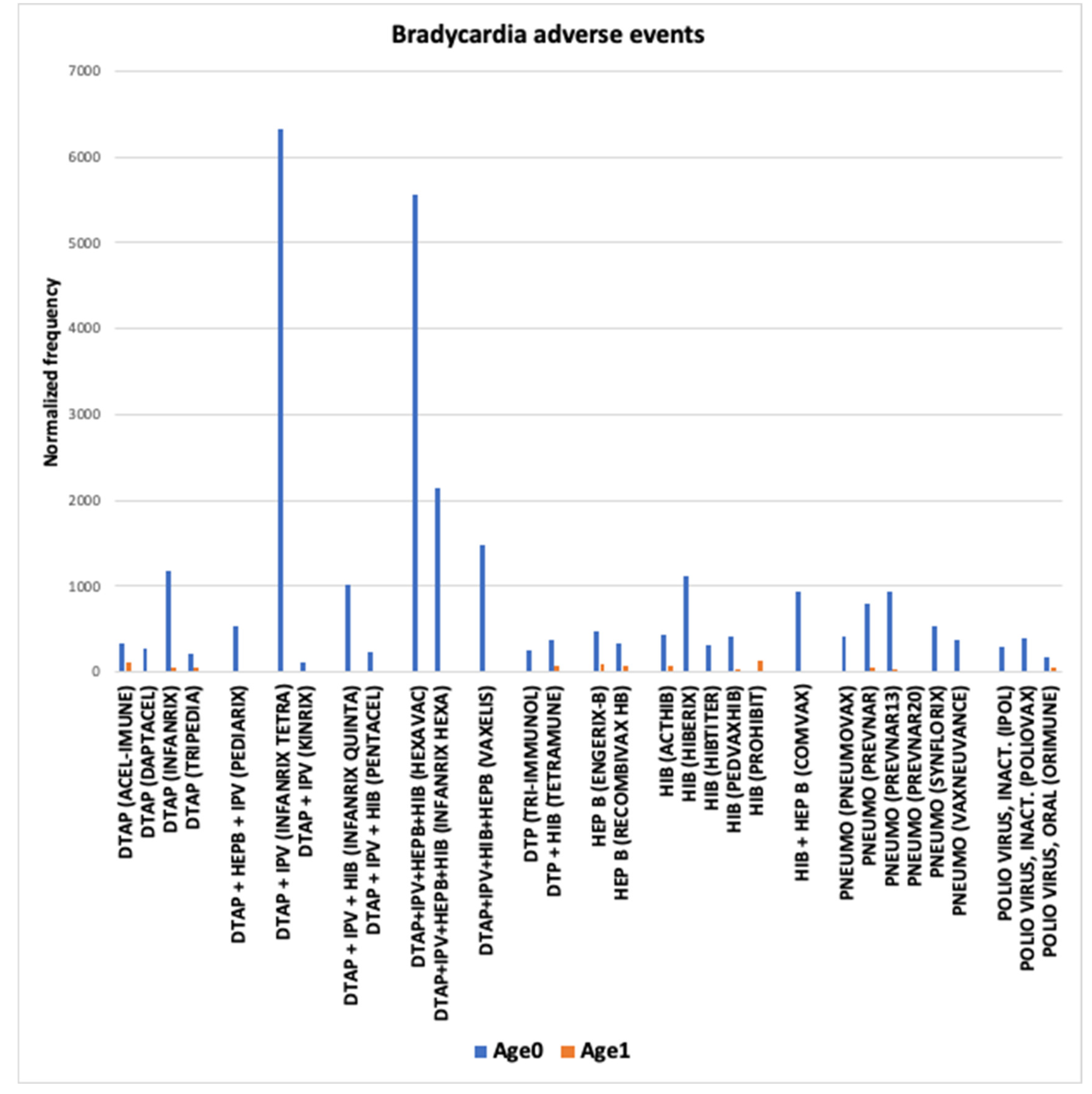
Figure 4.
Bradycardia concomitant vaccines AEs normalized frequencies from VAERS.
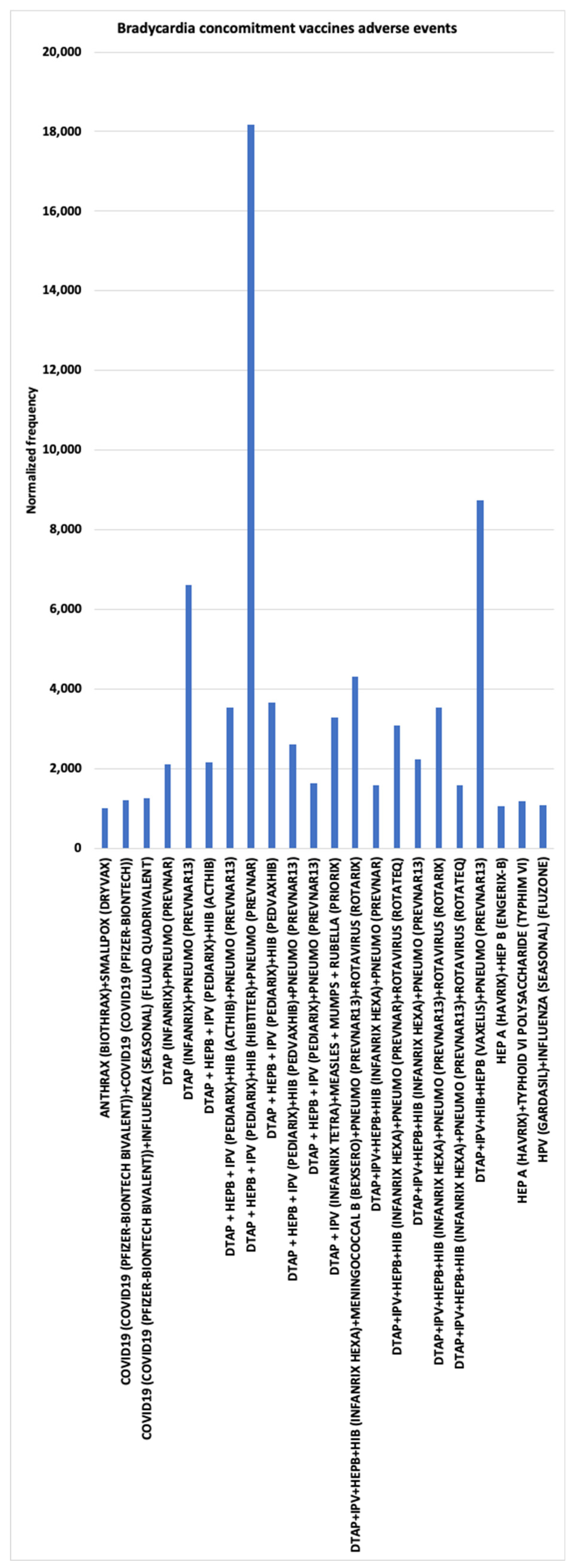
Figure 5.
Cardiac arrest AEs normalized frequencies for infants aged 0 and 1 from VAERS.
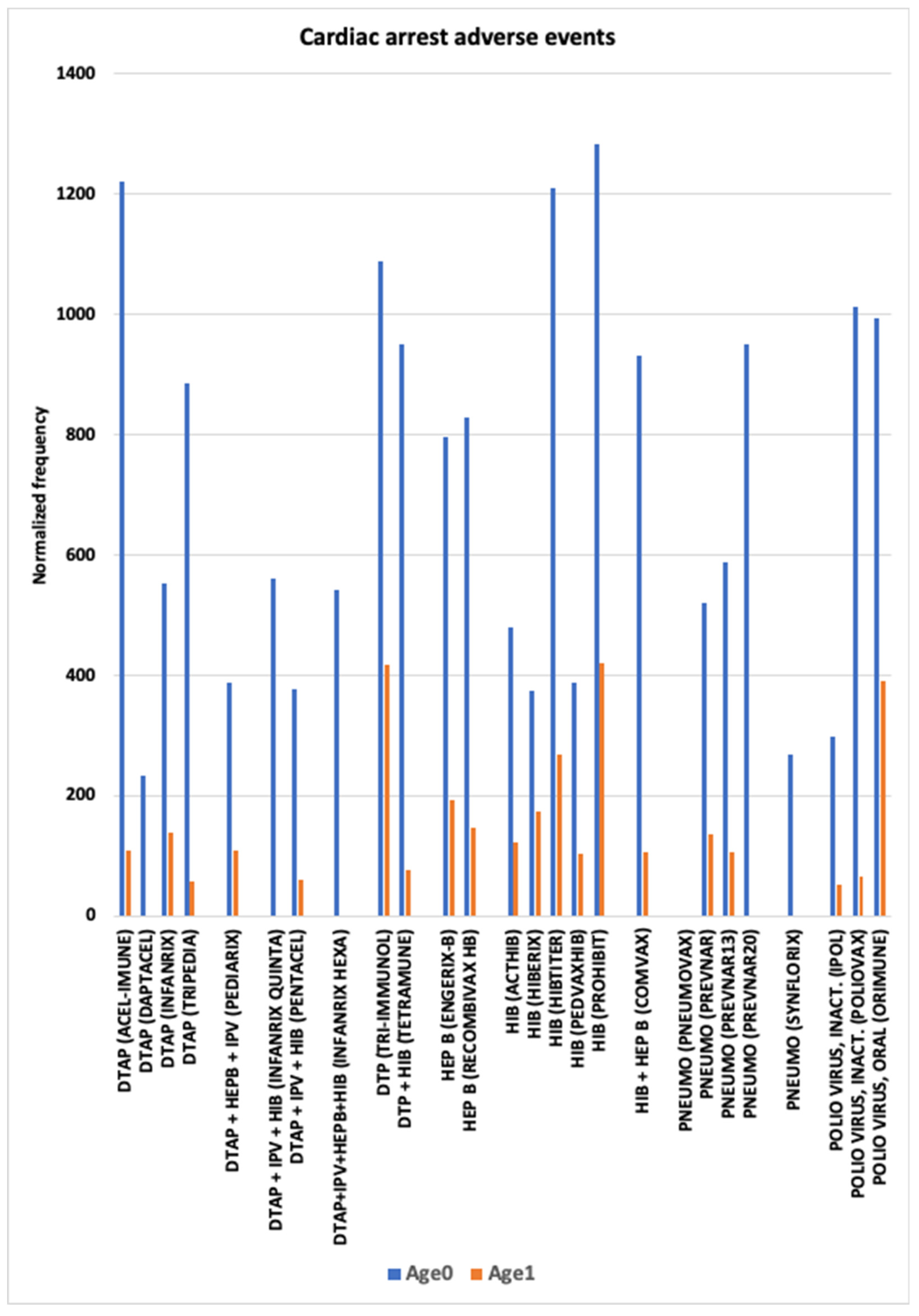
Figure 6.
Chest discomfort AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
Figure 6.
Chest discomfort AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
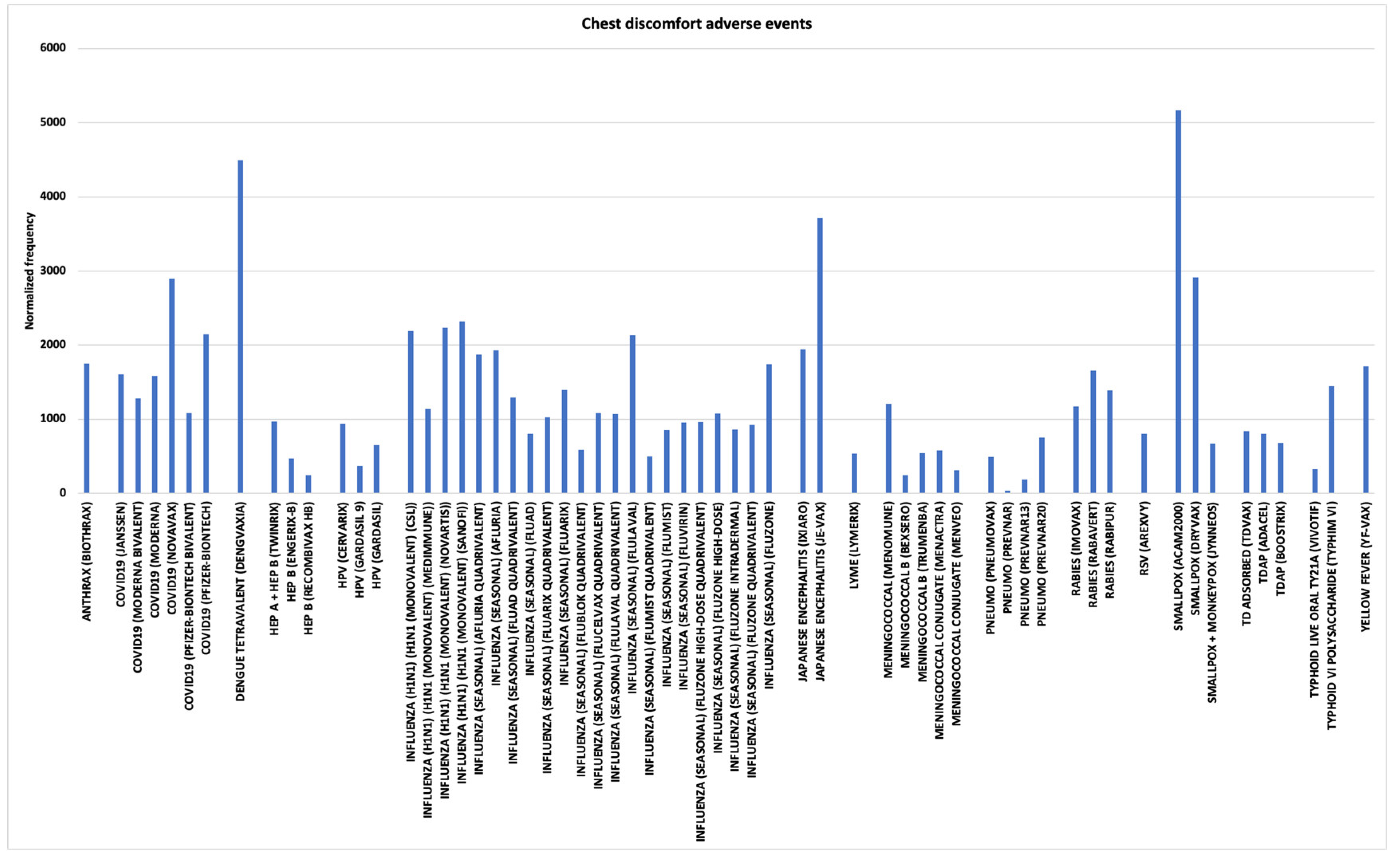
Figure 7.
Myocarditis and Pericarditis AEs normalized frequencies.
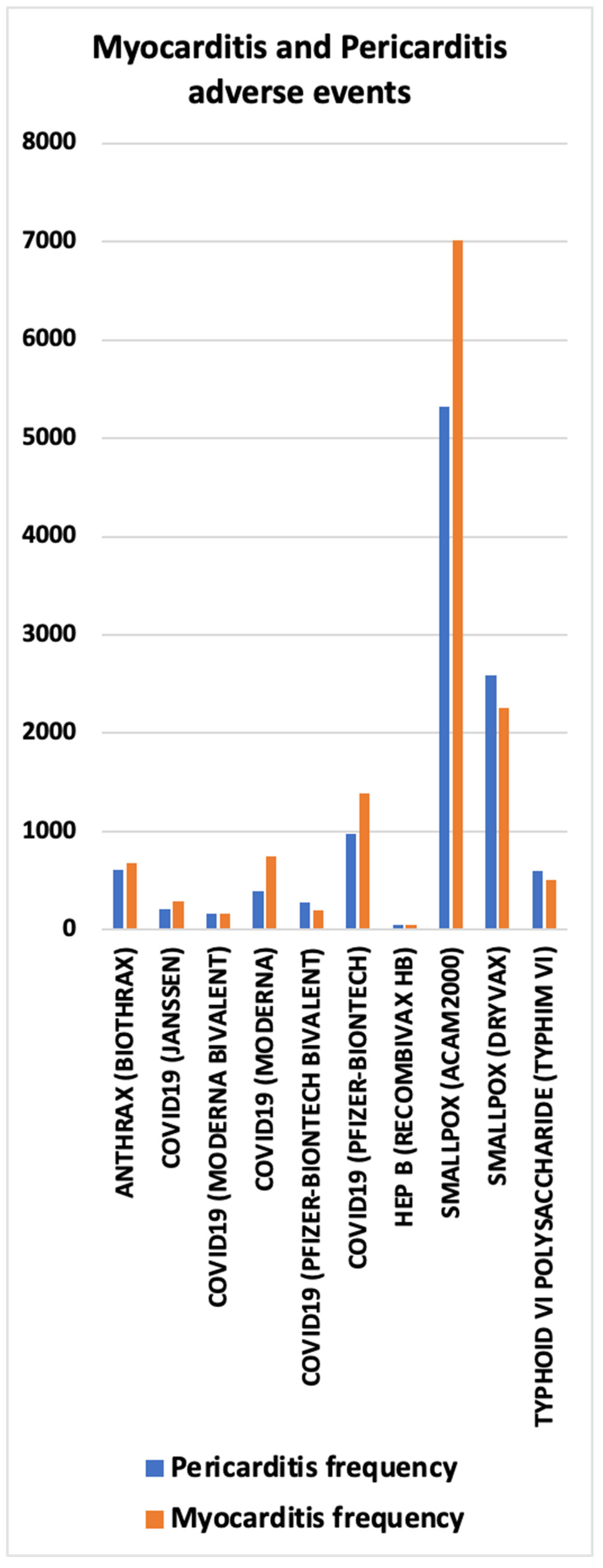
Figure 8.
Myocarditis AEs in males by age group normalized frequencies from VAERS.
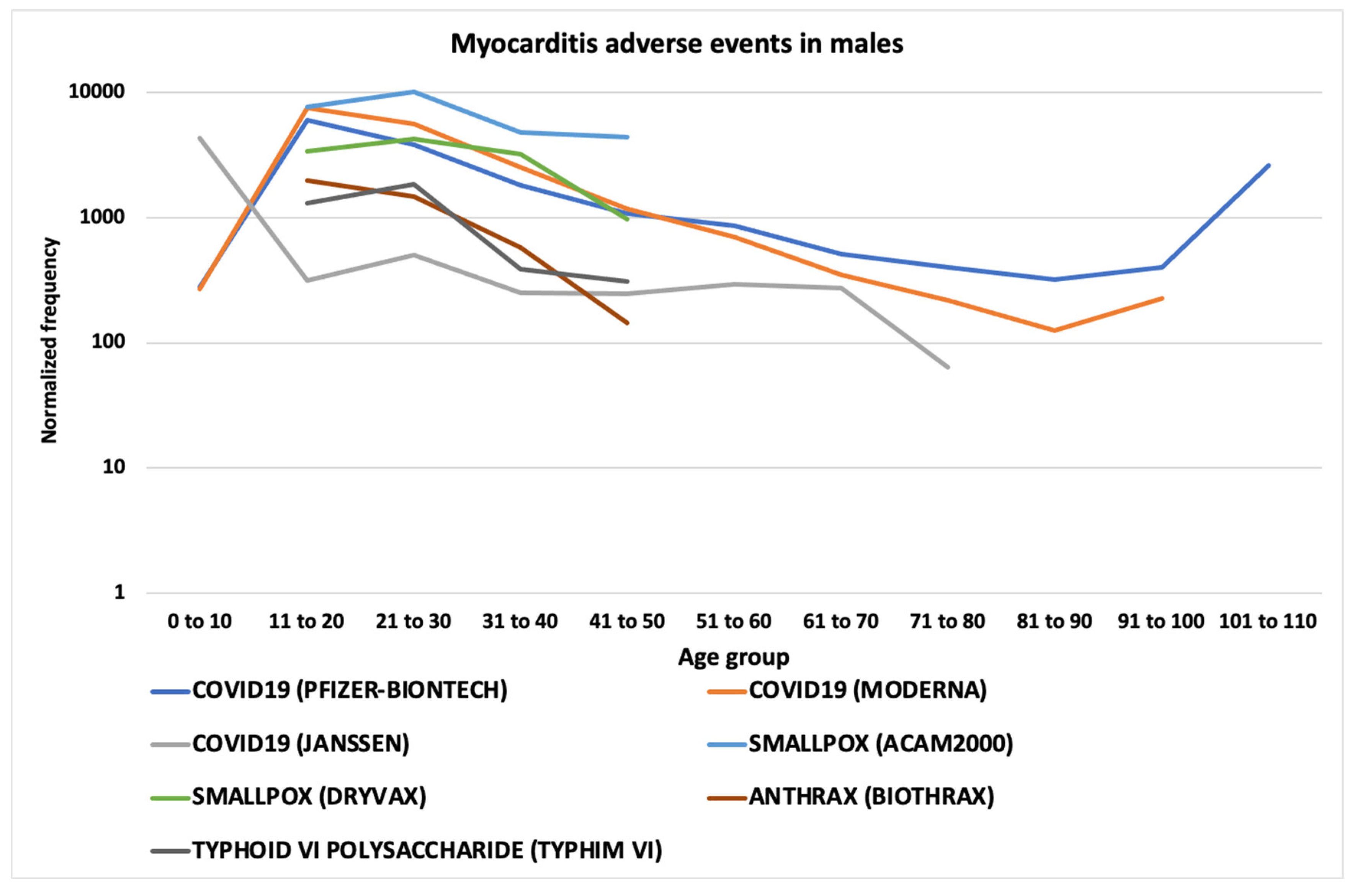
Figure 9.
Myocarditis AEs in females by age group normalized frequencies from VAERS.
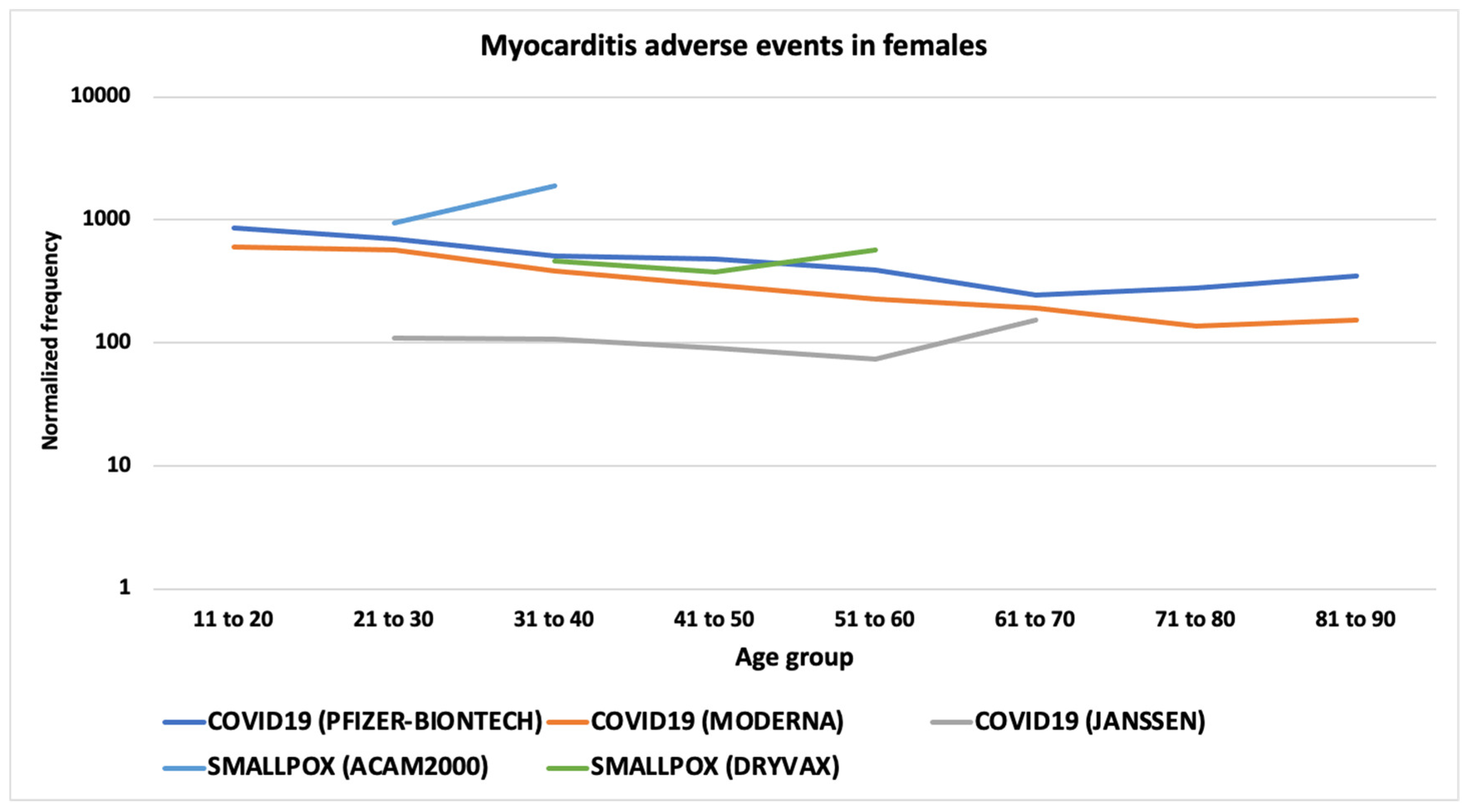
Figure 10.
Palpitations AEs normalized frequencies from VAERS.
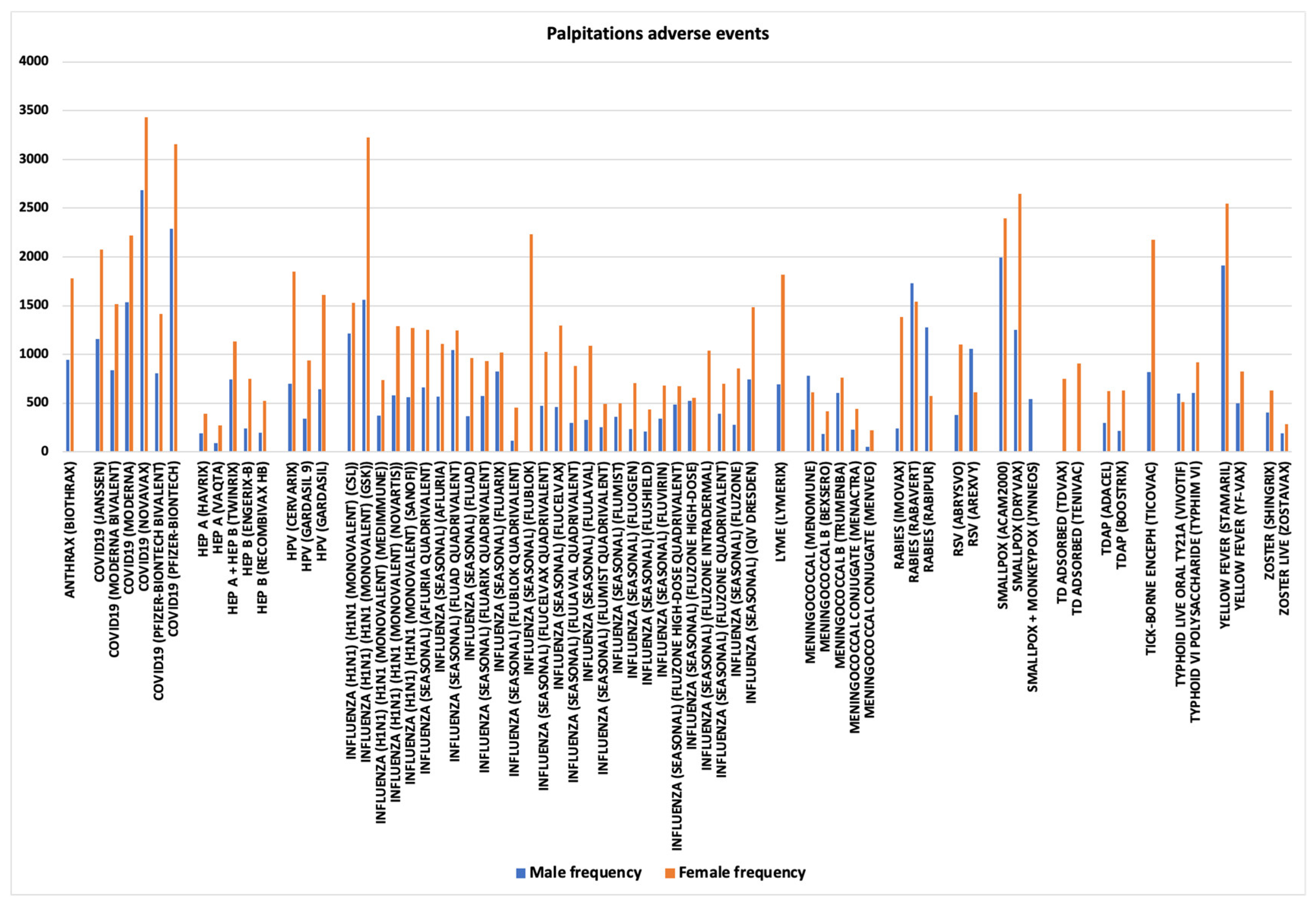
Figure 11.
Tachycardia AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
Figure 11.
Tachycardia AEs normalized frequencies from VAERS; data shown for vaccines with 10 or more AEs.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



