Submitted:
03 February 2025
Posted:
04 February 2025
You are already at the latest version
Abstract
Background and Objectives: This study aimed to evaluate the histopathological effects and tissue VEGF levels of combined methylprednisolone and hyaluronic acid treatment in a rat model with experimentally induced Asherman Syndrome prospective laboratory study. Materials and Methods: Twenty-six female Sprague Dawley rats were used. Trichloroacetic acid was applied to the right uterine horns of all groups to induce adhesion formation. First, we induced an Asherman model in 2 rats (Group 1). The remaining rats were divided into 3 groups. Group 2 received intrauterine hyaluronic acid treatment, Group 3 received oral methylprednisolone treatment, and Group 4 received both treatments. Histopathologically inflammation, gland count, and fibrosis levels were assessed. VEGF levels were analyzed immunohistochemically. Results: Hyaluronic acid treatment increased uterine lumen diameter and vascularization. Methylprednisolone treatment increased gland count and uterine wall thickness while decreasing inflammation and fibrosis scores. Combined treatment further enhanced these effects (p<0.05). Conclusions: Methylprednisolone treatment significantly prevented adhesion formation and reduced inflammation and fibrosis scores compared to hyaluronic acid treatment alone. The combined treatment adds to the effects of hyaluronic acid treatment alone and provides better healing.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Animals and Ethical Approval
2.2. Study Design and Estrous Cycle Assessment
2.3. Establishment of the Asherman Syndrome Model
2.4. Groups and Treatment Protocols
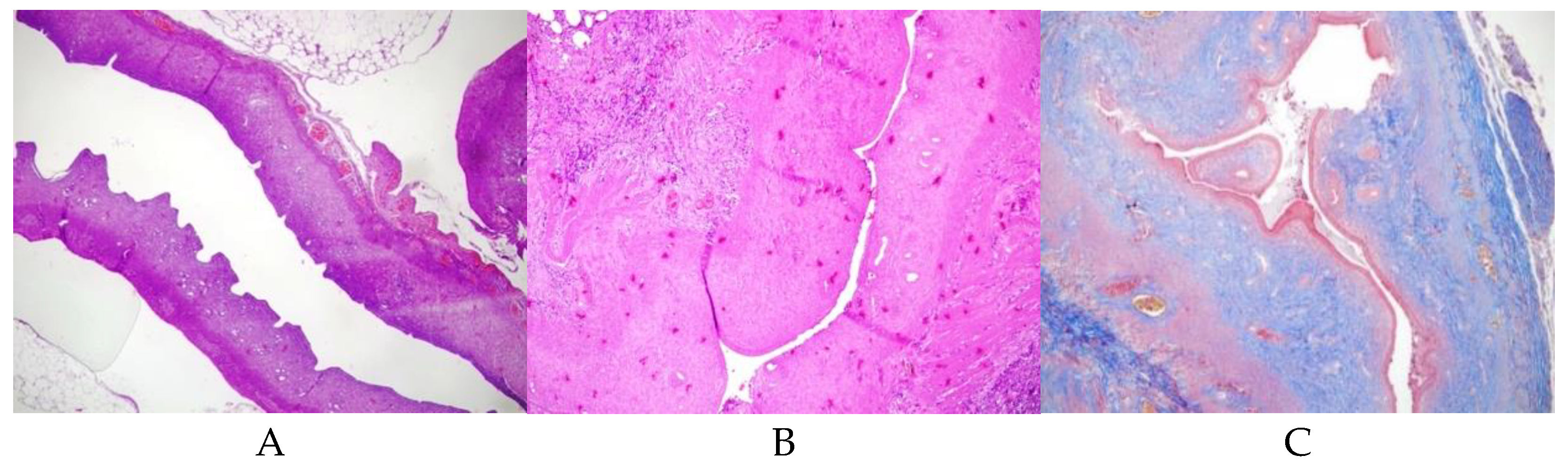
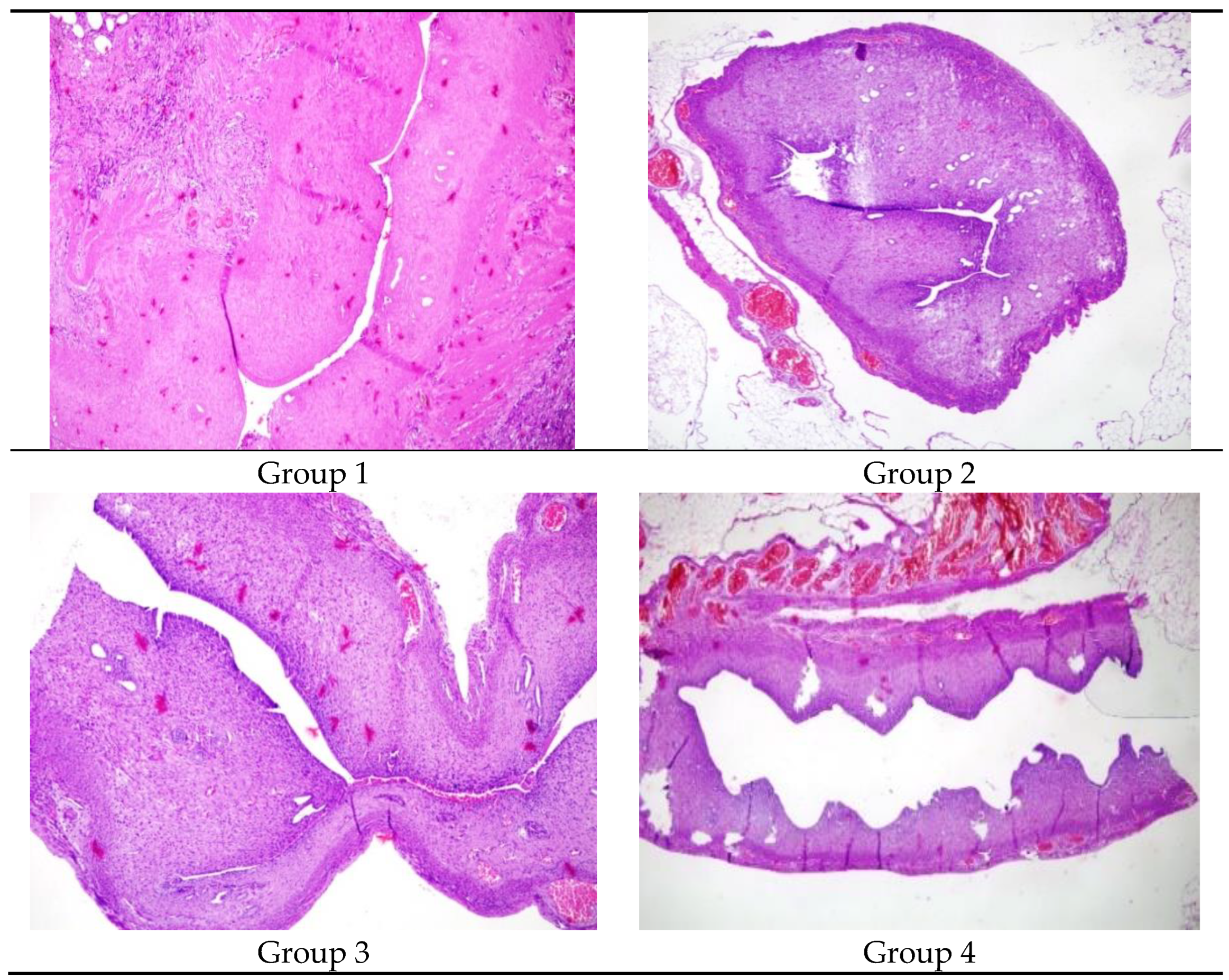
- Group 1 (Control, n=2): AS model induced, no further treatment (Figure 1). This group was conducted solely to confirm the induction of Asherman Syndrome using TCA, and in subsequent groups, it was accepted that Asherman Syndrome was induced with TC.
- Group 2 (Hyaluronic Acid, n=7): Fourteen days (approximately 3 estrous cycles) post-AS induction, a second laparotomy was performed, and 0.01 ml of low molecular weight hyaluronic acid was injected into the right uterine horn.
- Group 3 (Methylprednisolone, n=6): Fourteen days post-AS induction, 1 mg/kg p.o. methylprednisolone was administered daily for 2 weeks.
- Group 4 (Combined Treatment, n=7): Fourteen days post-AS induction, a second laparotomy was performed for intrauterine injection of 0.01 ml hyaluronic acid, and 1 mg/kg p.o. methylprednisolone was given daily for 2 weeks.
2.5. Pathological Evaluation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusion
Author Contributions
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fritsch, H. (1894). Ein fall von volligem schwund der gebormutterhohle nach auskratzung. Zentral Gynaekol, 18, 1337-1342.
- Asherman, J.G. (1948). Amenorrhoea traumatica (atretica). BJOG: An International.
- Journal of Obstetrics & Gynaecology, 55, 23-30. [CrossRef]
- Myers, E.M., and Hurst, B.S. (2012). Comprehensive management of severe.
- Asherman syndrome and amenorrhea. Fertility and Sterility, 97, 160-164. [CrossRef]
- Asherman, J.G. (1950). Traumatic intra-uterine adhesions. BJOG: An International Journal of Obstetrics & Gynaecology, 57, 892-896. [CrossRef]
- International Asherman's Association. (2018). What is Asherman's Syndrome. IAA. URL: http://www.webcitation.org/query?url=http%3A%2F%2Fwww.ashermans.org&date=2018-01-17.
- Gordon, A. G. (2018). Complications of hysteroscopy. GFMER. URL: http://www.webcitation.org/query?url=https%3A%2F%2Fwww.gfmer.ch%2FBooks%2FEndoscopy_book%2FCh24_Complications_hyster.html&date=2018-01-17.
- Friedler, S., Margalioth, E.J., Kafka, I., and Yaffe, H. (1993). Incidence of postabortion intra-uterine adhesions evaluated by hysteroscopy-a prospective study. Human Reproduction, 8, 442-444. [CrossRef]
- Alviggi, C., Mollo, A., De Placido, G., and Magos, A. (2013). The management of Asherman syndrome: a review of literature. Reproductive Biology and Endocrinology, 11, 118. [CrossRef]
- Yu, D., Wong, Y.M., Cheong, Y., Xia, E., and Li, T.C. (2008). Asherman syndromeone century later. Fertility and Sterility, 89, 759-779. 1. [CrossRef]
- İnternet: Gordon, A. G. Complications of hysteroscopy. GFMER. URL: http://www.webcitation.org/query?url=https%3A%2F%2Fwww.gfmer.ch%2FBooks.
- %2FEndoscopy_book%2FCh24_Complications_hyster.html&date=2018-01-17, Son Erişim Tarihi: 17.01.2018.
- Yang, J.H., Chen, C.D., Chen, S.U., Yang, Y.S., and Chen, M.J. (2016). The influence of the location and extent of intrauterine adhesions on recurrence after hysteroscopic adhesiolysis. BJOG: An International Journal of Obstetrics & Gynaecology, 123, 618-623. 94. [CrossRef]
- Yasmin, H. and Adeghe, J. (2004). Severe early-onset intrauterine growth restriction (IUGR) in a woman with Asherman's syndrome. Journal of Obstetrics and Gynaecology, 24, 312-314. [CrossRef]
- Cai Y, Wu F, Yu Y, et al. Porous scaffolds from droplet microfluidics for prevention of intrauterine adhesion. Acta biomaterialia. 2019;84:222-30. [CrossRef]
- Boland GM, Weigel RJ. Formation and prevention of postoperative abdominal adhesions. J Surg Res 2006; 132: 3-12. [CrossRef]
- Haynes RC Jr. Adrenocorticotropic hormone; adrenocortical steroids and their synthesis and action of adrenocortical hormones. In: Goodman and Gilman’s the pharmacological basis of therapeutics. 8th Edition, New York: Oxford Pergomon Press 1990: 1431-1462.
- Rein DT, Schmidt T, Bauerschmitz G, Hampl M, Beyer IM, Paupoo AAV, vd. Treatment of endometriosis with a VEGF-targeted conditionally replicative adenovirus. Fertility and Sterility. Mayıs 2010;93(8):2687-94. [CrossRef]
- Anaf V. Relationship between endometriotic foci and nerves in rectovaginal endometriotic nodules. Human Reproduction. 01 Ağustos 2000;15(8):1744-50. [CrossRef]
- Chen X, Sun J, Li X, et al. Antifibrotic Effects of Decellularized and Lyophilized Human Amniotic Membrane Transplant on the Formation of Intrauterine Adhesion. Experimental and clinical transplantation: official journal of the Middle East Society for Organ Transplantation. 2018. [CrossRef]
- Buckley C. Normal endometrium and non-proliferative conditions of the endometrium. Obstetrical and gynaecological pathology. 2003;5:391-442.
- Jing Z, Qiong Z, Yonggang W, Yanping L. Rat bone marrow mesenchymal stem cells improve regeneration of thin endometrium in rat. Fertile Steril 2014; 101:587-94. [CrossRef]
- Hunter II RK, Nevitt CD, Gaskins JT, Keller BB, Bohler HC Jr, LeBlanc AJ. Adipose-derived stromal vascular fraction cell effects on a rodent model of thin endometrium. Plos One 2015; 10(12):E0144823. [CrossRef]
- Kilic S, Yuksel B, Pinarli F, et al. Effect of stem cell application on Asherman syndrome, an.
- Seval Yılmaz Ergani, Berna Dilbaz, Hasan Murat Ergani , Özlem Moraloğlu Özdemir Effect of intrauterine ozone therapy on Asherman syndrome, an experimental rat model r J Obstet Gynecol Reprod Biol 2022 Oct:277:90-96. experimental rat model. Journal of Assisted Reproduction and Genetics. 2014;31(8):975-82.
- Conforti A, Alviggi C, Mollo A, De Placido G, Magos A. The management of Asherman syndrome: a review of literature. Reproductive Biology and Endocrinology.2013;11(1):118. [CrossRef]
- Roge P, D'ercole C, Cravello L, Boubli L, Blanc B. Hysteroscopic management of uterine synechiae: a series of 102 observations. European Journal of Obstetrics & Gynecology and Reproductive Biology. 1996;65(2):189-93. [CrossRef]
- 29. Seiede Zahra Ghanadzadeh Tafti 1, Atiye Javaheri 1, Razieh Dehghani Firoozabadi 2, Samane Kabirpour Ashkezar 1, Hossein Falahzadeh Abarghouei 3.
- Alponat A, Lakshminarasappa SR, Yavuz N, Goh PM. Prevention of adhesions by Seprafilm, an absorbable adhesion barrier: an incisional hernia model in rats. Am Surg 1997; 63: 818- 819.
- Fei Zheng Xin Xin Fei He Jianyong Liu Yuechong Cui Meta-analysis on the use of hyaluronic acid gel to prevent intrauterine adhesion after intrauterine operations Am J Obstet Gynecol. [CrossRef]

| Uterine cavity lumen diameters (micrometer) | |||
|---|---|---|---|
| Mean±SD | Median (Min-Max) | p value | |
|
Group 1 Right Left |
892,5±668,2 | 892,5(420-1365) | 0.004 |
| 1879,5±311,8 | 1879,5(1659-2100) | ||
|
Group 2 Right Left |
1041,4±560,4 | 980(430-1800) | 0.035 |
| 1915,3±767 | 1870(1100-3100) | ||
|
Group 3 Right Left |
1715,9±775 | 1229(790-2000) | 0.200 |
| 1932,6±768,4 | 1987(680-4070) | ||
|
Group 4 Right Left |
1270,7±455,4 | 1877(549-2875) | 0.655 |
| 2154±1251,4 | 1975(970-3350) | ||
| Uterine cavity lumen diameters (micrometer) | |||
|---|---|---|---|
| Mean±SD | Median (Min-Max) | p value | |
|
Group 1 Right Left |
198,5±16,3 | 198,5(187-210) | 0.004 |
| 810±381,8 | 810(540-1080) | ||
|
Group 2 Right Left |
500,4±350,7 | 410(188-1210) | 0.064 |
| 908,6±373,3 | 980(370-1490) | ||
|
Group 3 Right Left |
536,3±318,1 | 505(369-1080) | 0.055 |
| 601,4±291,3 | 1015(436-1540) | ||
|
Group 4 Right Left |
567±260,9 | 405(196-1005) | 0.848 |
| 1026,8±382,4 | 549(194-1054) | ||
| Uterine Gland Counts | |||
|---|---|---|---|
| Mean±SD | Median (Min-Max) | p value |
|
|
Group 1 Right Left |
7±2,8 | 7(5-9) | 0.029 |
| 12,5±5 | 12,5(9-16) | ||
|
Group 2 Right Left |
6,3±2,2 | 6(3-9) | 0.039 |
| 10,1±3,9 | 9(7-18) | ||
|
Group 3 Right Left |
10,4±5,4 | 7,5(4-13) | 0.077 |
| 10,7±4,4 | 11(7-16) | ||
|
Group 4 Right Left |
7,8±3,1 | 10(4-19) | 0.849 |
| 11,5±3,5 | 10(5-18) | ||
| Inflammation levels | Fibrosis | |||||
|---|---|---|---|---|---|---|
| Mean±SD | Median (Min-Max) | p value |
Mean±SD | Median (Min-Max) | P value |
|
|
Group 1 Right Left |
2,5±0,7 | 2,5(2-3) | 0.050 | 2,5±0,7 | 2,5(2-3) | 0.007 |
| 1,5±0,7 | 1,5(1-2) | 1,5±0,7 | 1,5(1-2) | |||
|
Group 2 Right Left |
1,6±0,8 | 1(1-3) | 0.019 | 2,1±0,7 | 2(1-3) | 0.024 |
| 0,6±0,5 | 1(0-1) | 1,1±0,7 | 1(0-2) | |||
|
Group 3 Right Left |
0,7±0,8 | 0,5(0-2) | 0.665 | 1,7±0,8 | 1,5(1-3) | 0.101 |
| 0,8±0,8 | 1(0-2) | 0,8±0,8 | 1(0-2) | |||
|
Group 4 Right Left |
1,3±0,8 | 1(0-2) | 0.071 | 1,7±0,8 | 2(1-3) | 0.184 |
| 0,6±0,5 | 1(0-2) | 1,1±0,7 | 1(0-2) | |||
| VEGF Staining Intensity | |||
|---|---|---|---|
| Mean±SD | Median (Min-Max) | P Value |
|
|
Group1 Right Left |
1,5±0,7 | 1,5(1-2) | 0.011 |
| 2,5±0,7 | 2,5(2-3) | ||
|
Group 2 Right Left |
1,9±0,7 | 2(1-3) | 0.207 |
| 1,4±0,8 | 1(1-3) | ||
|
Group 3 Right Left |
1,3±0,5 | 1(1-2) | 0.041 |
| 2,3±0,8 | 2,5(1-3) | ||
|
Group 4 Right Left |
1,6±0,5 | 2(1-2) | 0.114 |
| 2,1±0,7 | 2(1-3) | ||
| Uterine cavity lumen diameters P value |
Uterine wall thickness P value |
Uterine Gland Counts P value |
Inflammation levels P value |
VEGF Staining Intensity P value |
Fibrosis P value |
|
|---|---|---|---|---|---|---|
| Right horn | 0.010 | 0.107 | 0.321 | 0.009 | 0.483 | 0.162 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



