
Submitted:
12 January 2025
Posted:
13 January 2025
You are already at the latest version
Abstract
Background/Objectives: MicroRNAs (miRNAs) are likely to play a significant role in the prediction of rectal cancer response to chemoradiation therapy, offering insights that complement other biological tumour markers. The study aimed to perform miRNA profiling in rectal cancer tissues in patients with good (GR) and bad response (BR) to neoadjuvant chemoradiation therapy (nCRT), select the potentially clinically relevant ones, and further evaluate their relationship with subsequent disease outcomes and survival prognosis. Methods: A total of 40 selected patients with locally advanced rectal cancer who received nCRT and following surgical treatment in the period from 2016 to 2021 were involved. Two study groups were created – GR and BR according to the Dworak tumour regression grading (TRG) system. The identification of 752 miRNAs was conducted in rectal cancer tissue. Results: Six upregulated miRNAs were set as clinically significant within the selected samples and subsequently validated in the BR and GR groups. MiR-142-5p, miR-182-3p, and miR-99a-3p exhibited statistical significance in validation. The results showed that BR to nCRT, lower expression of miRNA-142-5p and miR-99a-3p, and higher expression of miR-182-3p were associated with a trend toward worse local recurrence-free survival, distant metastases-free survival, and overall survival in comparison to GR. Conclusion: MiRNAs may potentially serve as clinical biomarkers in prediction of disease-free survival and overall survival in patients with rectal cancer.
Keywords:
rectal cancer
; biomarker
; microRNA
; chemoradiation therapy
; treatment response
; miRNA 142-5p
; miRNA 182-3p
; miRNA 99a-3p
1. Introduction
Rectal cancer is a highly prevalent type of cancer, accounting for approximately 10-30% of newly diagnosed colorectal cancers (CRC) [1]. CRC is the third most commonly diagnosed malignancy and the second leading cause of cancer-related deaths in the world, with approximately 1.9 million new cases and 935 000 deaths each year [2]. It is a heterogeneous disease that develops via stepwise accumulation of well-characterized genetic and epigenetic alterations [3]. Accurate staging of rectal cancer is crucial as it can influence the choice of treatment strategies [4]. If early rectal cancer is managed by surgical resection alone, then more advanced cases demand neoadjuvant (preoperative) combination of chemoradiation therapy to reach the tumour downstaging or downshifting in order to provide safe resection margins and reduce the risk of local recurrence [5]. However, responses to this therapy can vary widely among patients, influenced by a multitude of factors including genetic makeup, tumour biology, and the tumour microenvironment [6,7,8]. As a result, we encounter a spectrum of tumour reactions – from non-response to complete-response to therapy. Studies show that clinical complete response (cCR) after neoadjuvant chemoradiation therapy (nCRT) can be obtained in 10-40% of cases, and pathological complete response (pCR) is observed in 15-30% of rectal cancer patients [9,10]. Patients with a pCR to nCRT have lower rates of local recurrence, improved survival as compared to patients who don’t achieve pCR. The 5-year recurrence-free survival rates are 90.5%, 78.7% and 58.5% for patients with complete, intermediate and poor response [11]. Furthermore, patients with pCR after nCRT have improved distant metastatic rates compared to poor responders to nCRT – 7-10.5% and 26-31%, respectively [12,13].
Understanding the differences of good and bad responders is not just an academic pursuit; it has profound implications for clinical practice. By identifying the underlying mechanisms that drive varied responses, healthcare providers can tailor treatment strategies more effectively, optimizing therapeutic outcomes and minimizing unnecessary side effects.
There are many studies with variable degrees of clinical significance looking for potential biomarkers that allow to differentiate good responders from bad responders to nCRT [14,15,16]. MiRNAs represent a promising avenue for enhancing the prediction of response to nCRT in rectal cancer, providing a complementary approach to existing biological tumour markers. MiRNAs are small (18–25 nucleotides) single-stranded and non-coding RNAs that downregulate gene expression at the post-transcriptional level through binding to target mRNAs and triggering their degradation or translational blocking [17]. They play a key role in the regulation of biological processes, such as apoptosis, cell differentiation, development, and proliferation, and it is believed that up to 30% of human genes are regulated by miRNAs [18,19,20]. Given the great impact of miRNAs on gene expression, it is not surprising that miRNA deregulation contributes to the initiation, progression, and dissemination of any type of human tumour [20,21,22]. They can act as oncogenic miRNAs (onco-miRNAs) or tumour suppressor miRNAs, depending on the function of the targeted mRNA [13]. Both the overexpression of specific onco-miRNAs and silencing of tumour suppressor miRNAs have been associated with the tumorigenesis of rectal cancer by inhibiting key components of the main signalling pathways altered in this disease. The overexpression of a miRNA can be due to the amplification of its coding gene or augmented transcription, while miRNA downregulation can be caused by epigenetic silencing, deletion of its coding gene, or defective biogenesis [18]. MiRNAs can be secreted into bodily fluids with minimal degradation, present a high stability during storage. All of these advantages facilitate their use in the clinical setting and miRNAs are emerging as stable and non-invasive biomarkers regarding diagnosis, staging, and prognosis in rectal cancer management [18,20,23]. Although several miRNAs have already been described as biomarkers predictive of responses to nCRT in rectal cancer patients, there are a lack of robust established markers available in the clinical routine [20,24,25]. A review by De Palma et al. in 2020, who was assessing 61 articles, identified a total of 77 miRNAs that are holding a predictive value, however, only six miRNAs (let-7f, miR-21, miR-145, miR-622, miR-630, and miR-1183) exhibited significant differences in two or more independent studies [26].
The aim of our study was miRNA profiling in rectal cancer tissue and establishment of their potential association with further prognosis in rectal cancer patients.
2. Materials and Methods
2.1. The Study Characteristics
A retrospective study was conducted in which patients with morphologically and radiologically verified stage II and III rectal adenocarcinoma, who received nCRT followed by surgical treatment during the period from 2016 to 2021 at Pauls Stradiņš Clinical University Hospital (Riga, Latvia), were selected and were either alive or deceased at the time of the study's initiation. A signed informed consent form for participation in the study was obtained from each patient or their family member (if the patient had deceased). Exclusion criteria were as follows: if progression to metastatic disease was detected during or after nCRT, patients with cCR and pCR after nCRT, if non-radical surgical treatment had been performed, if the patient/patient’s relative (if the person was deceased) did not agree to participate in the study.
2.2. Collection of the Tissue Samples
Tissue samples were acquired as part of planned treatment at the hospital. The study did not impose an additional burden on the patients. Tissue samples were obtained from the operative material. The study groups were formed based on the post-operative pathomorphosis of the tumour in the radically resected surgical material, using the Dworak classification (Table 1), which was assessed by two pathologists.
Tumour pathomorphosis was evaluated in formalin-fixed, paraffin-embedded (FFPE) tissue samples, cut with an automatic microtome to a thickness of 4 µm and prepared on slides with haematoxylin-eosin (HE) staining. FFPE tissue samples for further analysis from each patient were obtained, including 10 µm sections from the tumour and the proximal resection line. The tissue samples were stored at -20°C until the next step of the study.
2.3. Formation of the Study Groups
From the initially selected 298 patients, 86 patients were included in the study who met the inclusion and exclusion criteria. Patients were divided into groups according to the Dworak classification: Dworak 0 – 4 patients, Dworak 1 – 13 patients, Dworak 2 – 32 patients, Dworak 3 – 23 patients, Dworak 4 – 14 patients. For further tissue sample analysis, two groups were formed: the bad response (BR) group, consisting of patients with no tumour response or a minimal response to nCRT (corresponding to Dworak 0 and 1), and the good response (GR) group, consisting of patients with a good response to nCRT (corresponding to Dworak 3). Considering that the Dworak 2 group was the most heterogeneous and exhibited the greatest phenotypic variability, it was not analysed further. Additionally, Dworak 4 was not evaluated, as no tumour cells were morphologically detected in that group.
2.4. Characteristics of the Study Groups
A total of 40 patients were included in the study: 17 patients in the BR group and 23 patients in the GR group. The patients were followed up for 3 to 98 months. All patients had morphologically verified rectal adenocarcinoma, and clinical stage evaluation was based on radiological examinations – computed tomography (CT) scans of the abdomen and thorax and pelvic magnetic resonance imaging (MRI). All patients received nCRT and completed the course. Re-staging was performed (pelvic MRI) 6-12 weeks after finishing nCRT. The treatment response was evaluated according to the mrTRG (magnetic resonance imaging tumour regression grade) classification. Radical surgery was performed in all cases. The summary of post-treatment histopathological evaluations, as well as the clinical characteristics of the patients, is summarized in Table 2.
2.5. MiRNA Isolation from the FFPE
Extraction of total RNA (including miRNA) from FFPE tissue samples (tumour tissue and proximal resection line) was performed using the miRNeasy FFPE Kit protocol (miRNeasy FFPE Kit for microRNA Extraction, QIAGEN, ID: 217504). Measurements of total RNA concentration in the samples were conducted by fluorometry using the Qubit™ RNA BR Assay Kit protocol (Invitrogen by Thermo Fisher Scientific; Catalog No. Q10210, Q10211).
2.6. Profiling of miRNA
Six cases were selected from each group (BR and GR group) – a total of 12 tumour samples and 12 proximal resection margin tissue samples. The reverse transcription reaction for generating complementary DNA (cDNA) was conducted using the miRCURY LNA RT Kit (QIAGEN, ID: 339340). Reverse transcription polymerase chain reaction (RT-PCR) for miRNA profiling (a total of 752 miRNAs – listed in Appendix A, Table A1) in the selected samples was performed using the miRCURY LNA miRNA miRNome PCR Panels (QIAGEN, ID: 339322). The data obtained were analysed using the QIAGEN GeneGlobe online data analysis tool [28]. The selection of clinically significant miRNAs for further analysis in the groups was performed by comparing tumour and resection line miRNA profiles. The selected miRNAs were verified using the TaqMan Small RNA Assay. cDNA synthesis was performed with the TaqMan™ MicroRNA Reverse Transcription Kit (ID: 4366596), followed by quantification of the selected miRNAs using the TaqMan™ MicroRNA Assay (ID: 4427975) and TaqMan™ Fast Advanced Master Mix (ID: 4444558). All steps were carried out according to the manufacturer's protocol using the ViiA™ 7 Real-Time PCR System (Applied Biosystems). The selection criteria were as follows: upregulated expression in cancer tissue, quantification of miRNA (fold change of at least two times), and p-value (p < 0.05).
2.7. Statystical Analysis
The sample size for the first discovery experiment was calculated using the R package “size power” [29]. The parameters for the matched two-sample calculation were as follows: the mean number of false positives = 1; the anticipated number of un-differentially expressed genes in the experiment = 752; power level = 0.8; fold change = 2; and the anticipated standard deviation of the difference in log-expression between matched treatment and control conditions = 0.5. The calculated minimum sample size was 5 per group.
A t-test, paired t-test, and Mann-Whitney U test were used for the analysis of verified miRNAs. Local recurrence-free survival (LRFS), distant metastases-free survival (DMFS), disease-free survival (DFS), and overall survival (OS) were estimated using the Kaplan-Meier method. The log-rank test was used to calculate any significant differences between the groups through univariate analysis. Significance levels were set at p<0.05.
DFS (LRFS and DMFS) and OS were considered from the date of surgery to the date of any disease manifestation (local recurrence or metastasis) or patient death.
3. Results
3.1. Profiling of miRNAs in Rectal Cancer Tissue
From 752 identified miRNAs, six miRNAs were selected (three from the BR group and three from the GR group) that had the most statistically significant results and met the selection criteria by comparing miRNA expression in tumour tissues relative to resection margin tissues: miR-665, miR-99a-3p and miR-127-5p from GR group and miR-142-5p, miR-548c-5p, miR-182-3p from BR group. MiR-151-5p was chosen for normalization, as it showed the least variation in fold changes among all tumour samples.
3.2. Verification of Selected miRNA
Subsequently, the verification of the selected miRNAs was performed in other tissue samples from the BR and GR groups using the TaqMan Small RNA Assays protocol (Thermo Fisher Applied Biosystems; ID 002681, 002141, 002229, 002248, 002429, 000483, 002642). MiRNAs with p<0.05 in all statistical tests were selected as clinically significant. Accordingly, in the BR group, miR-142-5p and miR-182-3p met this criterion, and in the GR group it was miRNA-99a-3p (Figure 1).
3.3. The Survival Rates in BR and GR Groups
The following Kaplan-Meier analysis was executed to estimate DFS, LRFS, DMFS, and OS in the BR and GR group (Figure 4).
Afterwards, the population of both study groups was pooled, and the survival parameters (DFS, LRFS, DMFS and OS) were evaluated according to the expression level (lower or higher) of a particular miRNA – miR-142-5p (Figure 5), miR-182-3p (Figure 6), and miR-99a-3p (Figure 7).
Although the p-value in none of the groups reached the threshold of statistical confidence (p<0.05), a similar trend was observed in all categories – the estimated DFS, LRFS, DMFS, and OS were worse in the BR group and in cases of lower expression levels of miR-142-5p and miR-99a-3p, and higher expression of miR-182-3p. We assume that statistically significant results were not established due to the limited number of patients in groups.
4. Discussion
The role of different miRNAs in behaviour of rectal cancer, tumour progression, treatment resistance, and overall patient outcomes has been described in several studies [20,23,30]. This study focused on the miRNA profiling in rectal cancer tissue and verification of clinically relevant ones in association with clinical response to nCRT and survival rates.
We aimed to assess the significance of each miRNA that demonstrated clinical relevance in our study; however, we recognize that miRNAs interact with various factors that may influence their regulation. The importance of miRNA upregulation versus downregulation depends on the specific context and the biological pathways involved. Upregulation of certain miRNAs may be crucial for promoting tumour progression or resistance to therapy, while downregulation of others may be significant for tumour suppression. Therefore, both upregulation and downregulation can play critical roles in various biological processes and disease states, and their importance should be evaluated based on the specific miRNA and the associated conditions [31]. In this study, we primarily focused on upregulated miRNAs, with plans to further analyze downregulated miRNAs and their potential synergistic interactions.
It was observed that miR-142-5p was upregulated in patients with poor response to the nCRT, but its’ lower expression in general was related with worse DFS and OS. The role of miR-142-5p as a possible prognostic marker of poor CRC prognosis has been presented in some studies [32,33,34]. The overexpression of miR-142-5p has been associated with cancer in the proximal colorectum, BRAF positive patients and biological aggressiveness of cancer [6]. The study of Kunigenas et al. in 2020 demonstrated miRNA-142-5p as a diagnostic biomarker of rectal cancer following long-course nCRT. This study showed that miR-142-5p expression levels are significantly increased in rectum tumour tissue samples following long-course nCRT compared to tumour samples collected before the nCRT and compared to adjacent normal rectum tissue. The overexpression of miR-142-5p was observed in patients who received chemotherapy compared to expression levels in the group without the treatment, suggesting that the evaluation of miR-142-5p expression levels could serve as a diagnostic biomarker of cancer therapy [7]. Another study of Shi et al. in 2015 demonstrated that expression of miR-142-5p increases during the infusion chemotherapy in stage III CRC suggesting that miR-124-5p is a potential tumour suppressor in CRC and could serve for evaluation of efficacy of infusion chemotherapy and the progress of CRC [33]. Regarding the importance of miR-142-5p in predicting the tumour response, the study of Cervena et al. in 2021 presented the association of miR-142-5p expression levels and therapy response, respectively, the patients who died within a year after the diagnosis, didn’t have benefit from the therapy or had local recurrence, presented significantly lower expression levels in their second plasma sampling compared to the first one (first one taken at the time of diagnosis and the second one – a year after therapy). These findings suggest that miR-142-5p act as a tumour suppressors. Additionally, miR-142-5p was upregulated in the presence of 5-FU by SMiR-NBI (the Small Molecule-miRNA Network-Based Inference) model and this probably means that the effect of miRNA is potentiated in this way [34].
Another miRNA in the study, that was upregulated in BR group and associated with worse DFS and OS, was miR-182-3p which belongs to the family of miR-182. The evidence suggests that miR-182 has an important role as an onco-miRNA in different types of cancers by promoting tumour cell survival and metastasis. It is often upregulated in various types of tumours and may inhibit apoptosis [36]. In particular, it has been demonstrated that miR-182 plays a key role in CRC tumorigenesis. Several studies have reported that miR-182 expression is upregulated in CRC tissues compared to adjacent non-cancerous tissues [37]. The upregulation of miR-182 has been associated with advanced stage of TNM, i.e., positive regional lymph node status and high depth of tumour invasion and as well with local recurrence of the tumour [38,39]. The study of Yang et al in 2014 suggested that a higher level of miR-182 expression significantly promotes CRC invasion, migration, and cell proliferation in vivo and in vitro [40]. A high level of miR-182 has been observed in 5-FU-resistant CRC cell lines. Upregulation of miR-182 considerably induces drug resistance, proliferation, and colony formation, and causes apoptosis to be reduced in 5-FU-resistant CRC cell lines [41].
Among the miRNAs evaluated, it was observed that miR-99a-3p was upregulated in the group of GR, and lower expression level of miR-99a-3p was associated with worse OS and DFS. The role of miR-99a-3p has been associated with various types of cancer, although the studies revealing the predictive role in CRC are limited. In a study of Pinelo et al. in 2014 expression of miR-99a-3p in stage IV CRC patient blood samples was significantly associated with progression-free survival and OS, and therefore was validated as a predictive marker for chemotherapy response [42].
In the results obtained from this study, we observed a pronounced trend regarding the significance of certain miRNAs in predicting disease behaviour; however, we were unable to achieve statistical significance, which we attribute to several factors. First, the number of patients included in the study was limited due to the selection criteria, as well as the fact that patients with post-treatment pathomorphosis corresponding to Dworak 2 and Dworak 4 were not included. Second, the GR group, whose results were compared to the BR group, cannot be considered a completely favourable response, as it comprises patients whose postoperative morphological examination materials correspond to Dworak 3. A complete favourable response is classified as Dworak 4, where tumour cells are no longer detected, which consequently limits the analysis of this material from a tumour perspective. Lastly, it is important to note that both groups (GR and BR) still exhibit heterogeneity, which only increases during the analysis process. These factors hinder the attainment of statistical significance; nonetheless, the overall trend in the results is evident.
The ability to assess miRNA expression profiles not only enhances our understanding of tumour behaviour but also offers promising avenues for personalized medicine. By integrating miRNA analysis into clinical practice, patient stratification could be improved, enabling more tailored treatment approaches that consider individual molecular profiles. Additionally, miRNAs could serve as valuable prognostic markers, aiding in the prediction of treatment responses and survival outcomes. As research continues to unravel the intricate roles of miRNAs in rectal cancer, future studies should focus on validating these findings in larger, diverse cohorts and exploring the therapeutic potential of targeting miRNAs. Ultimately, the incorporation of miRNA profiles in clinical decision-making could transform the management of rectal cancer, paving the way for improved prognostic assessments and enhanced patient care.
Author Contributions
Conceptualization, L.K., E.M., A.G.; methodology, L.K., E.M., Z.D.; software, L.K., M.Š.; validation, Z.D., E.M.; formal analysis, L.K., M.Š., M.N.M.; investigation, L.K., D.Z., I.N., J.N.; data curation, L.K.; writing—original draft preparation, L.K.; writing—review and editing, L.K., Z.D., E.M.; visualization, L.K., M.N.M.; supervision, E.M., Z.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Riga Stradiņš University (Nr. 2-PĒK-4/120/2023 on 26.01.2023.).
Informed Consent Statement
Informed consent was obtained from all subjects (patient or their family member if the patient had deceased) involved in the study.
Data Availability Statement
Raw data is available from the corresponding author upon request.
Acknowledgments
Gratitude to all the medical professionals and patients involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| miRNAs | micro ribonucleic acids |
| nCRT | neoadjuvant chemoradiation therapy |
| GR | good response |
| BR | bad response |
| TRG | tumour regression grading |
| CRC | colorectal cancer |
| cCR | clinical complete response |
| pCR | pathological complete response |
| onco-miRNAs | oncogenic miRNAs |
| FFPE | formalin-fixed, paraffin-embedded |
| HE | haematoxylin-eosin |
| CT-scan | computed tomography scan |
| MRI | magnetic resonance imaging |
| CEA | carcinoembryonic antigen |
| CA19-9 | carbohydrate antigen 19-9 |
| Gy | gray |
| i/v | intravenous |
| 5FU | fluorouracil |
| FOLFOX6 | leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin |
| AR | anterior resection |
| HP | Hartmann’s Procedure |
| APR | abdominoperineal resection |
| TR | transanal resection |
| RL | resection line |
| cDNA | complementary DNA |
| LRFS | local recurrence-free survival |
| DMFS | distant metastases-free survival |
| DFS | disease-free survival |
| OS | overall survival |
Appendix A

Table A1.
The list of miRNAs identified in the selected samples (12 tumour samples and 12 proximal resection margin tissue samples); performed using the miRCURY LNA miRNA miRNome PCR Panels (QIAGEN, ID: 339322).
Table A1.
The list of miRNAs identified in the selected samples (12 tumour samples and 12 proximal resection margin tissue samples); performed using the miRCURY LNA miRNA miRNome PCR Panels (QIAGEN, ID: 339322).
| hsa-miR-7-5p | hsa-miR-16-5p | hsa-miR-99b-5p | hsa-miR-654-5p | hsa-miR-631 |
| hsa-miR-217-5p | hsa-miR-98-5p | hsa-miR-431-5p | hsa-miR-545-3p | hsa-miR-34c-5p |
| hsa-miR-337-5p | hsa-miR-185-5p | hsa-miR-23b-3p | hsa-miR-29b-2-5p | hsa-miR-211-5p |
| hsa-miR-328-3p | hsa-miR-25-3p | hsa-miR-367-3p | hsa-miR-491-5p | hsa-miR-454-3p |
| hsa-miR-374b-3p | hsa-miR-765 | hsa-miR-505-3p | hsa-miR-92b-3p | hsa-let-7f-5p |
| hsa-miR-143-3p | hsa-miR-24-3p | hsa-miR-18a-5p | hsa-miR-665 | hsa-miR-30e-5p |
| hsa-miR-623 | hsa-miR-369-5p | hsa-miR-92a-3p | hsa-miR-506-3p | hsa-miR-34a-5p |
| hsa-miR-520c-3p | hsa-miR-425-5p | hsa-miR-500a-5p | hsa-miR-363-3p | hsa-miR-663a |
| hsa-miR-557 | hsa-miR-590-5p | hsa-miR-887-3p | hsa-miR-132-3p | hsa-miR-518e-3p |
| hsa-miR-218-5p | hsa-miR-760 | hsa-miR-491-3p | hsa-miR-651-5p | hsa-miR-29b-3p |
| hsa-miR-136-5p | hsa-miR-574-3p | hsa-miR-423-3p | hsa-miR-628-3p | hsa-miR-658 |
| hsa-miR-127-5p | hsa-miR-130b-3p | hsa-miR-126-3p | hsa-miR-432-5p | hsa-miR-572 |
| hsa-miR-140-5p | hsa-miR-30c-5p | hsa-miR-421 | hsa-miR-154-3p | hsa-miR-802 |
| hsa-miR-31-3p | hsa-miR-133b | hsa-miR-376b-3p | hsa-miR-27a-3p | hsa-miR-521 |
| hsa-miR-20b-3p | hsa-miR-524-5p | hsa-miR-302c-3p | hsa-miR-376c-3p | hsa-miR-433-3p |
| hsa-miR-325 | hsa-miR-23a-3p | hsa-miR-625-3p | hsa-miR-940 | hsa-miR-660-5p |
| hsa-miR-509-3-5p | hsa-miR-193b-3p | hsa-miR-339-5p | hsa-miR-22-5p | hsa-let-7c-5p |
| hsa-miR-210-3p | hsa-miR-501-5p | hsa-miR-873-5p | hsa-miR-224-5p | hsa-miR-28-5p |
| hsa-miR-199b-5p | hsa-miR-518c-5p | hsa-miR-323a-3p | hsa-miR-885-5p | hsa-miR-324-5p |
| hsa-miR-194-5p | hsa-miR-130a-3p | hsa-miR-181d-5p | hsa-miR-320a-3p | hsa-miR-219a-5p |
| hsa-let-7g-5p | hsa-miR-933 | hsa-miR-125a-5p | hsa-miR-18b-5p | hsa-miR-19b-3p |
| hsa-miR-203a-3p | hsa-miR-379-5p | hsa-miR-129-5p | hsa-miR-187-3p | hsa-miR-526b-5p |
| hsa-miR-181a-3p | hsa-miR-452-5p | hsa-miR-492 | hsa-miR-516b-5p | hsa-miR-215-5p |
| hsa-miR-137-3p | hsa-miR-589-5p | hsa-miR-20a-5p | hsa-miR-302c-5p | hsa-miR-30b-5p |
| hsa-miR-551b-3p | hsa-miR-141-3p | hsa-miR-374b-5p | hsa-miR-548b-3p | hsa-miR-184 |
| hsa-miR-524-3p | hsa-miR-342-3p | hsa-miR-302d-3p | hsa-miR-186-5p | hsa-miR-422a |
| hsa-miR-486-5p | hsa-miR-668-3p | hsa-miR-346 | hsa-miR-199a-5p | hsa-miR-199a-3p |
| hsa-miR-329-3p | hsa-miR-934 | hsa-miR-151a-3p | hsa-miR-155-5p | hsa-miR-335-5p |
| hsa-miR-487b-3p | hsa-miR-101-3p | hsa-miR-493-3p | hsa-miR-107 | hsa-miR-519a-3p |
| hsa-miR-138-5p | hsa-miR-539-5p | hsa-miR-122-5p | hsa-miR-302b-3p | hsa-miR-21-5p |
| hsa-miR-191-5p | hsa-miR-331-3p | hsa-miR-99a-3p | hsa-miR-662 | hsa-miR-129-2-3p |
| hsa-miR-378a-3p | hsa-miR-499a-5p | hsa-miR-361-5p | hsa-miR-519d-3p | hsa-miR-26b-5p |
| hsa-miR-103a-3p | hsa-miR-196a-5p | hsa-miR-202-3p | hsa-miR-485-3p | hsa-miR-214-3p |
| hsa-miR-890 | hsa-miR-888-5p | hsa-miR-125b-5p | hsa-miR-200b-3p | hsa-miR-32-5p |
| hsa-miR-423-5p | hsa-miR-330-3p | hsa-miR-503-5p | hsa-miR-337-3p | hsa-miR-324-3p |
| hsa-miR-221-3p | hsa-miR-570-3p | hsa-miR-204-5p | hsa-miR-494-3p | hsa-miR-488-3p |
| hsa-miR-301b-3p | hsa-miR-518c-3p | hsa-miR-30d-5p | hsa-miR-371a-3p | hsa-miR-371a-5p |
| hsa-miR-550a-5p | hsa-miR-200a-3p | hsa-miR-301a-3p | hsa-miR-637 | hsa-miR-455-5p |
| hsa-miR-532-5p | hsa-miR-188-5p | hsa-miR-362-5p | hsa-miR-144-3p | hsa-miR-891a-5p |
| hsa-miR-99a-5p | hsa-miR-26a-5p | hsa-miR-30b-3p | hsa-miR-16-1-3p | hsa-miR-549a-3p |
| hsa-miR-205-5p | hsa-miR-498-5p | hsa-miR-296-5p | hsa-miR-216a-5p | hsa-miR-148a-3p |
| hsa-miR-518b | hsa-miR-148b-3p | hsa-miR-20b-5p | hsa-miR-424-5p | hsa-miR-146a-5p |
| hsa-miR-19a-3p | hsa-miR-127-3p | hsa-miR-147a | hsa-miR-921 | hsa-miR-139-5p |
| hsa-miR-150-5p | hsa-miR-598-3p | hsa-miR-198 | hsa-miR-513a-5p | hsa-miR-373-5p |
| hsa-miR-15a-5p | hsa-miR-96-5p | hsa-miR-375-3p | hsa-miR-140-3p | hsa-miR-149-5p |
| hsa-let-7d-3p | hsa-let-7d-5p | hsa-miR-517a-3p | hsa-miR-181a-5p | hsa-miR-642a-5p |
| hsa-miR-608 | hsa-miR-135b-5p | hsa-miR-361-3p | hsa-miR-10a-5p | hsa-miR-31-5p |
| hsa-miR-671-5p | hsa-miR-495-3p | hsa-miR-21-3p | hsa-miR-106a-5p | hsa-miR-451a |
| hsa-miR-497-5p | hsa-miR-299-5p | hsa-miR-373-3p | hsa-miR-182-5p | hsa-miR-620 |
| hsa-miR-877-5p | hsa-miR-34c-3p | hsa-miR-518f-3p | hsa-miR-370-3p | hsa-miR-27b-3p |
| hsa-miR-187-5p | hsa-miR-596 | hsa-miR-222-3p | hsa-miR-576-5p | hsa-miR-523-3p |
| hsa-miR-10b-5p | hsa-miR-744-5p | hsa-miR-617 | hsa-miR-425-3p | hsa-miR-374a-5p |
| hsa-let-7i-5p | hsa-miR-145-5p | hsa-miR-154-5p | hsa-miR-450a-5p | hsa-miR-92a-1-5p |
| hsa-miR-202-5p | hsa-miR-622 | hsa-miR-708-5p | hsa-miR-411-5p | hsa-miR-219a-1-3p |
| hsa-miR-652-3p | hsa-miR-516a-5p | hsa-let-7b-5p | hsa-miR-216b-5p | hsa-miR-1913 |
| hsa-miR-126-5p | hsa-let-7a-5p | hsa-miR-95-3p | hsa-miR-106b-5p | hsa-miR-1245a |
| hsa-miR-30e-3p | hsa-miR-96-3p | hsa-miR-517c-3p | hsa-miR-22-3p | hsa-miR-522-3p |
| hsa-miR-181c-5p | hsa-miR-185-3p | hsa-miR-151a-5p | hsa-miR-510-5p | hsa-miR-571 |
| hsa-miR-9-3p | hsa-miR-615-3p | hsa-miR-502-5p | hsa-miR-212-3p | hsa-miR-323a-5p |
| hsa-miR-548c-3p | hsa-miR-128-3p | hsa-miR-345-5p | hsa-miR-525-5p | hsa-miR-592 |
| hsa-miR-152-3p | hsa-miR-766-3p | hsa-miR-509-3p | hsa-miR-542-5p | hsa-miR-487a-3p |
| hsa-miR-93-5p | hsa-miR-206 | hsa-miR-134-5p | hsa-miR-576-3p | hsa-miR-1249-3p |
| hsa-miR-365a-3p | hsa-miR-298 | hsa-miR-382-5p | hsa-miR-583 | hsa-miR-25-5p |
| hsa-miR-29c-3p | hsa-miR-193a-5p | hsa-miR-490-3p | hsa-miR-483-3p | hsa-miR-922 |
| hsa-miR-372-3p | hsa-miR-449b-5p | hsa-miR-200c-3p | hsa-miR-582-5p | hsa-miR-124-5p |
| hsa-miR-133a-3p | hsa-miR-520d-5p | hsa-miR-30a-5p | hsa-miR-183-5p | hsa-miR-1264 |
| hsa-miR-124-3p | hsa-miR-192-5p | hsa-miR-181b-5p | hsa-miR-33b-5p | hsa-miR-504-5p |
| hsa-miR-190a-5p | hsa-miR-29a-3p | hsa-miR-33a-5p | hsa-miR-193a-3p | hsa-miR-138-1-3p |
| hsa-miR-302a-3p | hsa-miR-18a-3p | hsa-miR-195-5p | hsa-miR-153-3p | hsa-miR-502-3p |
| hsa-miR-595 | hsa-miR-383-5p | hsa-miR-874-3p | hsa-let-7e-5p | hsa-miR-490-5p |
| hsa-miR-602 | hsa-miR-9-5p | hsa-miR-135a-5p | hsa-miR-409-3p | hsa-miR-567 |
| hsa-miR-223-3p | hsa-miR-142-5p | hsa-miR-26a-2-3p | hsa-miR-100-5p | hsa-miR-18b-3p |
| hsa-miR-627-5p | hsa-miR-363-5p | hsa-miR-146b-5p | hsa-miR-629-5p | hsa-miR-125a-3p |
| hsa-miR-34b-3p | hsa-miR-147b-3p | hsa-miR-412-3p | hsa-miR-484 | hsa-miR-653-5p |
| hsa-miR-410-3p | hsa-miR-197-3p | hsa-miR-1-3p | hsa-miR-429 | hsa-miR-891b |
| hsa-miR-17-5p | hsa-miR-597-5p | hsa-miR-299-3p | hsa-miR-30c-2-3p | hsa-miR-144-5p |
| hsa-miR-376a-3p | hsa-miR-326 | hsa-miR-142-3p | hsa-miR-518a-3p | hsa-miR-1538 |
| hsa-miR-514a-3p | hsa-miR-15b-5p | hsa-miR-338-3p | hsa-miR-340-5p | hsa-miR-384 |
| hsa-miR-512-5p | hsa-miR-105-5p | hsa-miR-584-5p | hsa-miR-508-3p | hsa-miR-196b-3p |
| hsa-miR-449a | hsa-miR-196b-5p | hsa-miR-377-3p | hsa-miR-381-3p | hsa-miR-649 |
| hsa-miR-143-5p | hsa-miR-892a | hsa-miR-141-5p | hsa-miR-520h | hsa-miR-518d-3p |
| hsa-miR-1207-5p | hsa-miR-10b-3p | hsa-miR-1269a | hsa-miR-769-5p | hsa-miR-569 |
| hsa-miR-943 | hsa-miR-122-3p | hsa-miR-501-3p | hsa-miR-612 | hsa-miR-125b-1-3p |
| hsa-miR-675-3p | hsa-miR-100-3p | hsa-miR-15b-3p | hsa-miR-1237-3p | hsa-miR-218-2-3p |
| hsa-miR-200b-5p | hsa-miR-769-3p | hsa-miR-146b-3p | hsa-miR-1908-5p | hsa-miR-519c-3p |
| hsa-miR-519e-5p | hsa-miR-300 | hsa-miR-222-5p | hsa-miR-1260a | hsa-miR-554 |
| hsa-miR-942-5p | hsa-miR-518e-5p | hsa-miR-601 | hsa-miR-182-3p | hsa-miR-938 |
| hsa-miR-450b-3p | hsa-miR-489-3p | hsa-miR-924 | hsa-miR-365b-5p | hsa-miR-1243 |
| hsa-miR-553 | hsa-miR-937-3p | hsa-miR-29a-5p | hsa-miR-508-5p | hsa-miR-708-3p |
| hsa-miR-605-5p | hsa-miR-381-5p | hsa-let-7a-2-3p | hsa-miR-671-3p | hsa-miR-1185-5p |
| hsa-miR-24-2-5p | hsa-miR-640 | hsa-miR-520f-3p | hsa-miR-941 | hsa-miR-512-3p |
| hsa-miR-23a-5p | hsa-miR-148b-5p | hsa-miR-101-5p | hsa-miR-23b-5p | hsa-miR-587 |
| hsa-miR-27b-5p | hsa-miR-29c-5p | hsa-miR-520a-3p | hsa-miR-591 | hsa-miR-603 |
| hsa-miR-759 | hsa-miR-499a-3p | hsa-miR-548m | hsa-miR-26b-3p | hsa-miR-1184 |
| hsa-miR-770-5p | hsa-let-7f-1-3p | hsa-miR-517-5p | hsa-miR-519b-3p | hsa-miR-20a-3p |
| hsa-miR-585-3p | hsa-miR-382-3p | hsa-miR-448 | hsa-miR-30d-3p | hsa-miR-588 |
| hsa-miR-376a-5p | hsa-miR-609 | hsa-miR-1296-5p | hsa-miR-518d-5p | hsa-miR-455-3p |
| hsa-miR-507 | hsa-miR-10a-3p | hsa-miR-1537-3p | hsa-miR-212-5p | hsa-miR-582-3p |
| hsa-miR-520b-3p | hsa-miR-106a-3p | hsa-miR-920 | hsa-miR-520e-3p | hsa-miR-409-5p |
| hsa-miR-302f | hsa-let-7e-3p | hsa-miR-1247-5p | hsa-miR-646 | hsa-miR-452-3p |
| hsa-miR-28-3p | hsa-miR-580-3p | hsa-miR-19b-2-5p | hsa-miR-519e-3p | hsa-miR-19b-1-5p |
| hsa-miR-875-5p | hsa-miR-761 | hsa-miR-558 | hsa-miR-626 | hsa-miR-610 |
| hsa-miR-219a-2-3p | hsa-miR-643 | hsa-miR-106b-3p | hsa-miR-26a-1-3p | hsa-miR-511-5p |
| hsa-miR-1183 | hsa-miR-618 | hsa-miR-1258 | hsa-miR-190b | hsa-miR-200c-5p |
| hsa-miR-758-3p | hsa-miR-221-5p | hsa-miR-619-3p | hsa-miR-1471 | hsa-let-7a-3p |
| hsa-miR-1244 | hsa-miR-513b-5p | hsa-miR-208a-3p | hsa-miR-548l | hsa-miR-135a-3p |
| hsa-miR-566 | hsa-miR-411-3p | hsa-miR-17-3p | hsa-miR-586 | hsa-miR-520a-5p |
| hsa-miR-1256 | hsa-miR-19a-5p | hsa-miR-136-3p | hsa-miR-103b | hsa-miR-1468-5p |
| hsa-miR-516a-3p | hsa-miR-338-5p | hsa-miR-877-3p | hsa-miR-488-5p | hsa-miR-628-5p |
| hsa-miR-548c-5p | hsa-miR-1914-3p | hsa-miR-935 | hsa-miR-129-1-3p | hsa-miR-552-3p |
| hsa-miR-496 | hsa-miR-323b-5p | hsa-miR-224-3p | hsa-miR-192-3p | hsa-miR-145-3p |
| hsa-miR-876-3p | hsa-miR-548i | hsa-miR-624-3p | hsa-miR-632 | hsa-miR-378a-5p |
| hsa-miR-532-3p | hsa-miR-541-3p | hsa-miR-767-5p | hsa-miR-181a-2-3p | hsa-miR-7-1-3p |
| hsa-miR-654-3p | hsa-miR-1272 | hsa-miR-559 | hsa-miR-1909-3p | hsa-miR-181c-3p |
| hsa-miR-659-3p | hsa-miR-1205 | hsa-miR-449b-3p | hsa-miR-573 | hsa-miR-195-3p |
| hsa-miR-135b-3p | hsa-miR-544a | hsa-miR-205-3p | hsa-miR-302d-5p | hsa-miR-578 |
| hsa-miR-641 | hsa-miR-431-3p | hsa-miR-604 | hsa-miR-194-3p | hsa-miR-505-5p |
| hsa-miR-2113 | hsa-miR-621 | hsa-miR-130b-5p | hsa-miR-302b-5p | hsa-miR-875-3p |
| hsa-miR-1254 | hsa-miR-556-5p | hsa-miR-149-3p | hsa-miR-551b-5p | hsa-miR-450b-5p |
| hsa-miR-661 | hsa-miR-1267 | hsa-miR-1271-5p | hsa-miR-635 | hsa-miR-876-5p |
| hsa-miR-362-3p | hsa-miR-379-3p | hsa-miR-92b-5p | hsa-miR-1911-3p | hsa-miR-1224-3p |
| hsa-miR-624-5p | hsa-miR-556-3p | hsa-miR-551a | hsa-let-7f-2-3p | hsa-miR-1539 |
| hsa-miR-27a-5p | hsa-miR-614 | hsa-miR-146a-3p | hsa-miR-155-3p | hsa-miR-663b |
| hsa-miR-744-3p | hsa-miR-616-5p | hsa-miR-218-1-3p | hsa-miR-105-3p | hsa-miR-1248 |
| hsa-miR-139-3p | hsa-miR-93-3p | hsa-miR-593-5p | hsa-miR-486-3p | hsa-miR-889-3p |
| hsa-miR-138-2-3p | hsa-miR-1972 | hsa-miR-561-3p | hsa-miR-320b | hsa-miR-1227-3p |
| hsa-miR-655-3p | hsa-miR-616-3p | hsa-miR-767-3p | hsa-miR-296-3p | hsa-miR-548h-5p |
| hsa-miR-99b-3p | hsa-miR-369-3p | hsa-miR-526b-3p | hsa-miR-7-2-3p | hsa-miR-1255b-5p |
| hsa-miR-581 | hsa-miR-2110 | hsa-miR-24-1-5p | hsa-miR-550a-3p | hsa-miR-330-5p |
| hsa-miR-191-3p | hsa-miR-548a-3p | hsa-let-7b-3p | hsa-miR-380-3p | hsa-miR-1238-3p |
| hsa-miR-32-3p | hsa-miR-634 | hsa-miR-193b-5p | hsa-miR-593-3p | hsa-miR-188-3p |
| hsa-miR-1204 | hsa-miR-320c | hsa-miR-335-3p | hsa-miR-1912-3p | hsa-miR-589-3p |
| hsa-miR-548j-5p | hsa-miR-636 | hsa-miR-541-5p | hsa-miR-493-5p | hsa-miR-125b-2-3p |
| hsa-miR-555 | hsa-miR-606 | hsa-miR-30c-1-3p | hsa-miR-432-3p | hsa-miR-16-2-3p |
| hsa-miR-515-5p | hsa-miR-208b-3p | hsa-miR-629-3p | hsa-miR-454-5p | hsa-miR-650 |
| hsa-miR-340-3p | hsa-miR-367-5p | hsa-miR-377-5p | hsa-miR-936 | hsa-miR-1178-3p |
| hsa-miR-513a-3p | hsa-miR-520d-3p | hsa-miR-630 | hsa-miR-30a-3p | hsa-miR-600 |
| hsa-miR-34a-3p | hsa-miR-1265 | hsa-miR-548d-3p | hsa-let-7g-3p | hsa-miR-599 |
| hsa-miR-342-5p | hsa-miR-1203 | hsa-miR-885-3p | hsa-miR-214-5p | hsa-miR-520g-3p |
| hsa-miR-639 | hsa-miR-548k | hsa-miR-320d | hsa-miR-183-3p | hsa-miR-564 |
| hsa-let-7i-3p | hsa-miR-548a-5p | hsa-miR-2053 | hsa-miR-1179 | hsa-miR-132-5p |
| hsa-miR-543 | hsa-miR-1253 | hsa-miR-675-5p | hsa-miR-562 | hsa-miR-577 |
| hsa-miR-645 | hsa-miR-615-5p | hsa-miR-1252-5p | hsa-miR-579-3p | hsa-miR-223-5p |
| hsa-miR-548d-5p | hsa-miR-607 | hsa-miR-548e-3p | hsa-miR-590-3p | hsa-miR-34b-5p |
| hsa-miR-33a-3p | hsa-miR-1208 | hsa-miR-1914-5p | hsa-miR-130a-5p | hsa-miR-888-3p |
| hsa-miR-664a-3p | hsa-miR-302e | hsa-miR-513c-5p | hsa-miR-563 | hsa-miR-424-3p |
| hsa-miR-1911-5p | hsa-miR-1206 | hsa-miR-331-5p | hsa-miR-200a-5p | hsa-miR-339-3p |
| hsa-miR-33b-3p | hsa-miR-1270 | hsa-miR-1182 | hsa-miR-483-5p | hsa-miR-380-5p |
| hsa-miR-638 | hsa-miR-525-3p | hsa-miR-611 | hsa-miR-15a-3p | hsa-miR-647 |
| hsa-miR-515-3p | hsa-miR-1200 | hsa-miR-1181 | hsa-miR-944 | hsa-miR-518f-5p |
| hsa-miR-548n | hsa-miR-92a-2-5p |
References
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol 2019, 14, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Globocan Cancer Observatory. Available online: https://gco.iarc.fr/en (accessed on 25 October 2024).
- Nguyen, L.H.; Goel, A.; Chung, D.C. Pathways of Colorectal Carcinogenesis. Gastroenterol 2020, 158, 291–302. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Rectal Cancer Treatment - Health Professional version. Available online: https://www.cancer.gov/types/colorectal/hp/rectal-treatment-pdq#_19 (accessed on 25 October 2024).
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. ESMO Guidelines. Ann Oncol 2017, 28, 22–40. [Google Scholar] [CrossRef]
- Kalady, M.F.; de Campos-Lobato, L.F.; Stocchi, L.; Geisler, D.P.; Dietz, D.; Lavery, I.C.; Fazio, V.W. Predictive factors of pathologic complete response after neoadjuvant chemoradiation for rectal cancer. Ann Surg 2009, 250, 582–589. [Google Scholar] [CrossRef]
- Spolverato, G.; Pucciarelli, S.; Bertorelle, R.; De Rossi, A.; Nitti, D. Predictive factors of the response of rectal cancer to neoadjuvant radiochemotherapy. Cancers (Basel) 2011, 3, 2176–2194. [Google Scholar] [CrossRef]
- D’Angelo, E.; Fassan, M.; Maretto, I.; Pucciarelli, S.; Zanon, C.; Digito, M.; Rugge, M.; Nitti, D.; Agostini, M. Serum miR 125b is a non-invasive predictive biomarker of the pre-operative chemoradiotherapy responsiveness in patients with rectal adenocarcinoma. Oncotarget 2016, 7, 28647–28657. [Google Scholar] [CrossRef]
- Wei, I.H.; Garcia-Aguilar, J. Non-operative management of rectal cancer: Understanding tumor biology. Minerva Chir 2018, 73, 601–618. [Google Scholar] [CrossRef]
- Hoendervangers, S.; Burbach, J.P.M.; Lacle, M.M.; Koopman, M.; van Grevenstein, W.M.U.; Intven, M.P.W.; Verkooijen, H.M. Pathological Complete Response Following Different Neoadjuvant Treatment Strategies for Locally Advanced Rectal Cancer: A Systematic Review and Meta-analysis. Ann Surg Oncol 2020, 27, 4319–4336. [Google Scholar] [CrossRef]
- Walker, A.S.; Zwintscher, N.P.; Johnson, E.K.; Maykel, J.A.; Stojadinovic, A.; Nissan, A.; Avital, I.; Brücher, B.L.D.M.; Steele, S.R. Future directions for monitoring treatment response in colorectal cancer. J Cancer 2014, 5, 44–57. [Google Scholar] [CrossRef]
- Park, I.J.; You, Y.N.; Agarwal, A.; Skibber, J.M.; Rodriguez-Bigas, M.A.; Eng, C.; Feig, B.W.; Das, P.; Krishnan, S.; Crane, C.H.; Hu, C.Y.; Chang, G.J. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. J Clin Oncol 2012, 30, 1770–1776. [Google Scholar] [CrossRef]
- Fan, W.H.; Xiao, J.; An, X.; Jiang, W.; Li, L.R.; Gao, Y.H.; Chen, G.; Kong, L.H.; Lin, J.Z.; Wang, J.P.; et al. Patterns of recurrence in patients achieving pathologic complete response after neoadjuvant chemoradiotherapy for rectal cancer. J Cancer Res Clin Oncol 2017, 143, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Xiao, Q.; Venkatachalam, N.; Hofheinz, R.D.; Veldwijk, M.R.; Herskind, C.; Ebert, M.P.; Zhan, T. Predicting response to neoadjuvant chemoradiotherapy in rectal cancer: from biomarkers to tumor models. Ther Adv Med Oncol 2022, 14, 17588359221077972. [Google Scholar] [CrossRef] [PubMed]
- Bedin, C.; Crotti, S.; D’Angelo, E.; D’Aronco, S.; Pucciarelli, S.; Agostini, M. Circulating Biomarkers for Response Prediction of Rectal Cancer to Neoadjuvant Chemoradiotherapy. Curr Med Chem 2020, 27, 4274–4294. [Google Scholar] [CrossRef] [PubMed]
- Smolskas, E.; Mikulskytė, G.; Sileika, E.; Suziedelis, K.; Dulskas, A. Tissue-Based Markers as a Tool to Assess Response to Neoadjuvant Radiotherapy in Rectal Cancer-Systematic Review. Int J Mol Sci 2022, 23, 6040. [Google Scholar] [CrossRef]
- Eriksen, A.H.M.; Andersen, R.F.; Pallisgaard, N.; Sørensen, F.B.; Jakobsen, A.; Hansen, T.F. MicroRNA expresion profiling to identify and validate reference genes for the relative quantification of microRNA in rectal cancer. PLoS ONE 2016, 11, e0150593. [Google Scholar] [CrossRef]
- Slaby, O.; Svoboda, M.; Michalek, J.; Vyzula, R. MicroRNAs in colorectal cancer: Translation of molecular biology into clinical application. Mol Cancer 2009, 8, 1–13. [Google Scholar] [CrossRef]
- Agostini, M.; Pucciarelli, S.; Calore, F.; Bedin, C.; Enzo, M.V.; Nitti, D. MiRNAs in colon and rectal cancer: A consensus for their true clinical value. Clin Chim Acta 2010, 411, 17–18. [Google Scholar] [CrossRef]
- Imedio, L.; Cristóbal, I.; Rubio, J.; Santos, A.; Rojo, F.; García-Foncillas, J. MicroRNAs in Rectal Cancer: Functional Significance and Promising Therapeutic Value. Cancers (Basel) 2020, 12, 2040. [Google Scholar] [CrossRef]
- Pettit, C.; Walston, S.; Wald, P.; Webb, A.; Williams, T.M. Molecular profiling of locally-advanced rectal adenocarcinoma using microRNA expression (Review). Int J Oncol 2017, 51, 393–404. [Google Scholar] [CrossRef]
- Rossi, S.; Kopetz, S.; Davuluri, R.; Hamilton, S.R.; Calin, G.A. MicroRNAs, ultraconserved genes and colorectal cancers. Int J Biochem Cell Biol 2010, 42, 1291–1297. [Google Scholar] [CrossRef]
- Azizian, A.; Gruber, J.; Ghadimi, B.M.; Gaedcke, J. MicroRNA in rectal cancer. World J Gastrointest Oncol 2016, 8, 416–426. [Google Scholar] [CrossRef] [PubMed]
- Machackova, T.; Prochazka, V.; Kala, Z.; Slaby, O. Translational potential of microRNAs for preoperative staging and prediction of chemoradiotherapy response in rectal cancer. Cancers (Basel) 2019, 11, 1545. [Google Scholar] [CrossRef] [PubMed]
- Crist, I.; Rubio, J.; Santos, A.; Torrej, B.; Caram, C.; Imedio, L.; Luque, M. MicroRNA-199b downregulation confers and predicts poor outcome and response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer patients. Cancers (Basel) 2020, 12, e1655. [Google Scholar]
- DePalma, F.D.E.; Luglio, G.; Tropeano, F.P.; Pagano, G.; D’Armiento, M.; Kroemer, G.; Maiuri, M.C.; De Palma, G.D. The Role of Micro-RNAs and Circulating Tumor Markers as Predictors of Response to Neoadjuvant Therapy in Locally Advanced Rectal Cancer. Int J Mol Sci 2020, 21, 7040. [Google Scholar] [CrossRef]
- Trakarnsanga, A.; Gönen, M.; Shia, J.; Nash, G.M.; Temple, L.K.; Guillem, J.G.; Paty, P.B.; Goodman, K.A.; Wu, A.; Gollub, M.; et al. Comparison of Tumor Regression Grade Systems for Locally Advanced Rectal Cancer After Multimodality Treatment. J Natl Cancer Inst 2014, 106, dju248. [Google Scholar] [CrossRef]
- Qiagen Gene Globe. Available online: https://geneglobe.qiagen.com/us/analyze (accessed on 21 December 2024).
- Lee, M.-L.T.; Whitmore, G.A. Power and sample size for DNA microarray studies. Stat Med 2002, 21, 3543–3570. [Google Scholar] [CrossRef]
- Gaedcke, J.; Grade, M.; Camps, J.; Søkilde, R.; Kaczkowski, B.; Schetter, A.J.; Difilippantonio, M.J.; Harris, C.C.; Ghadimi, B.M.; Møller, S.; Beissbarth, T.; Ried, T.; Litman, T. The rectal cancer microRNAome microRNA expression in rectal cancer and matched normal mucosa. Clin Cancer Res 2012, 18, 4919–4930. [Google Scholar] [CrossRef]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front Endocrinol (Lausanne) 2018, 3, 402. [Google Scholar] [CrossRef]
- Kunigenas, L.; Stankevicius, V.; Dulskas, A.; Budginaite, E.; Alzbutas, G.; Stratilatovas, E.; Cordes, N.; Suziedelis, K. 3D Cell Culture-Based Global miRNA Expression Analysis Reveals miR-142-5p as a Theranostic Biomarker of Rectal Cancer Following Neoadjuvant Long-Course Treatment. Biomolecules 2020, 10, 613. [Google Scholar] [CrossRef]
- Shi, D.; Zhai, B.; Zheng, Y.; Ren, R.; Han, M.; Wang, X. Transcatheter arterial infusion chemotherapy increases expression level of miR-142-5p in stage III colorectal cancer. Indian J Cancer 2015, 52 Suppl 2, e47–55. [Google Scholar]
- Cervena, K.; Novosadova, V.; Pardini, B.; Naccarati, A.; Opattova, A.; Horak, J.; Vodenkova, S.; Buchler, T.; Skrobanek, P.; Levy, M.; Vodicka, P.; Vymetalkova, V. Analysis of MicroRNA Expression Changes During the Course of Therapy In Rectal Cancer Patients. Front Oncol 2021, 11, 702258. [Google Scholar] [CrossRef] [PubMed]
- Islam, F.; Gopalan, V.; Vider, J.; Lu, CT.; Lam, A.K. MiR-142-5p act as an oncogenic microRNA in colorectal cancer: Clinicopathological and functional insights. Exp Mol Pathol 2018, 104, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Sameti, P.; Tohidast, M.; Amini, M.; Bahojb Mahdavi, S.Z.; Najafi, S.; Mokhtarzadeh, A. The emerging role of MicroRNA-182 in tumorigenesis; a promising therapeutic target. Cancer Cell Int 2023, 23, 134. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Du, L.; Wen, Z.; Yang, Y.; Li, J.; Wang, L.; Zhang, X.; Liu, Y.; Dong, Z.; Li, W.; Zheng, G.; Wang, C. Up-regulation of miR-182 expression in colorectal cancer tissues and its prognostic value. Int J Colorectal Dis 2013, 28, 697–703. [Google Scholar] [CrossRef]
- Rapti, S.M.; Kontos, C.K.; Papadopoulos, I.N.; Scorilas, A. Enhanced miR-182 transcription is a predictor of poor overall survival in colorectal adenocarcinoma patients. Clin Chem Lab Med 2014, 52, 1217–1227. [Google Scholar] [CrossRef]
- Li, X.; Zhang, X.; Zhang, Q.; Lin, R. MiR-182 contributes to cell proliferation, invasion and tumor growth in colorectal cancer by targeting DAB2IP. Oncol Lett 2020, 19, 3923–3930. [Google Scholar] [CrossRef]
- Yang, M.H.; Yu, J.; Jiang, D.M.; Li, W.L.; Wang., S.; Ding, Y.Q. MicroRNA-182 targets special AT-rich sequence-binding protein 2 to promote colorectal cancer proliferation and metastasis. J Transl Med 2014, 12, 109. [Google Scholar] [CrossRef]
- Liu, B.; Liu, Y.; Zhao, L.; Pan, Y.; Shan, Y.; Li, Y.; Jia, L. Upregulation of microRNA-135b and microRNA-182 promotes chemoresistance of colorectal cancer by targeting ST6GALNAC2 via PI3K/AKT pathway. Mol Carcinog 2017, 56, 2669–2680. [Google Scholar] [CrossRef]
- Molina-Pinelo, S.; Carnero, A.; Rivera, F.; Estevez-Garcia, P.; Bozada, J.M.; Limon, M.L.; Benavent, M.; Gomez, J.; Pastor, M.D.; Chaves, M.; Suarez, R.; Paz-Ares, L.; de la Portilla, F.; Carranza-Carranza, A.; Sevilla, I.; Vicioso, L.; Garcia-Carbonero, R. MiR-107 and miR-99a-3p predict chemotherapy response in patients with advanced colorectal cancer. BMC Cancer 2014, 14, 656. [Google Scholar] [CrossRef]
Figure 1.
The results of the statistical analysis of upregulated microRNAs (miRNAs) with a fold change of at least two times in the BR and GR group.
Figure 1.
The results of the statistical analysis of upregulated microRNAs (miRNAs) with a fold change of at least two times in the BR and GR group.
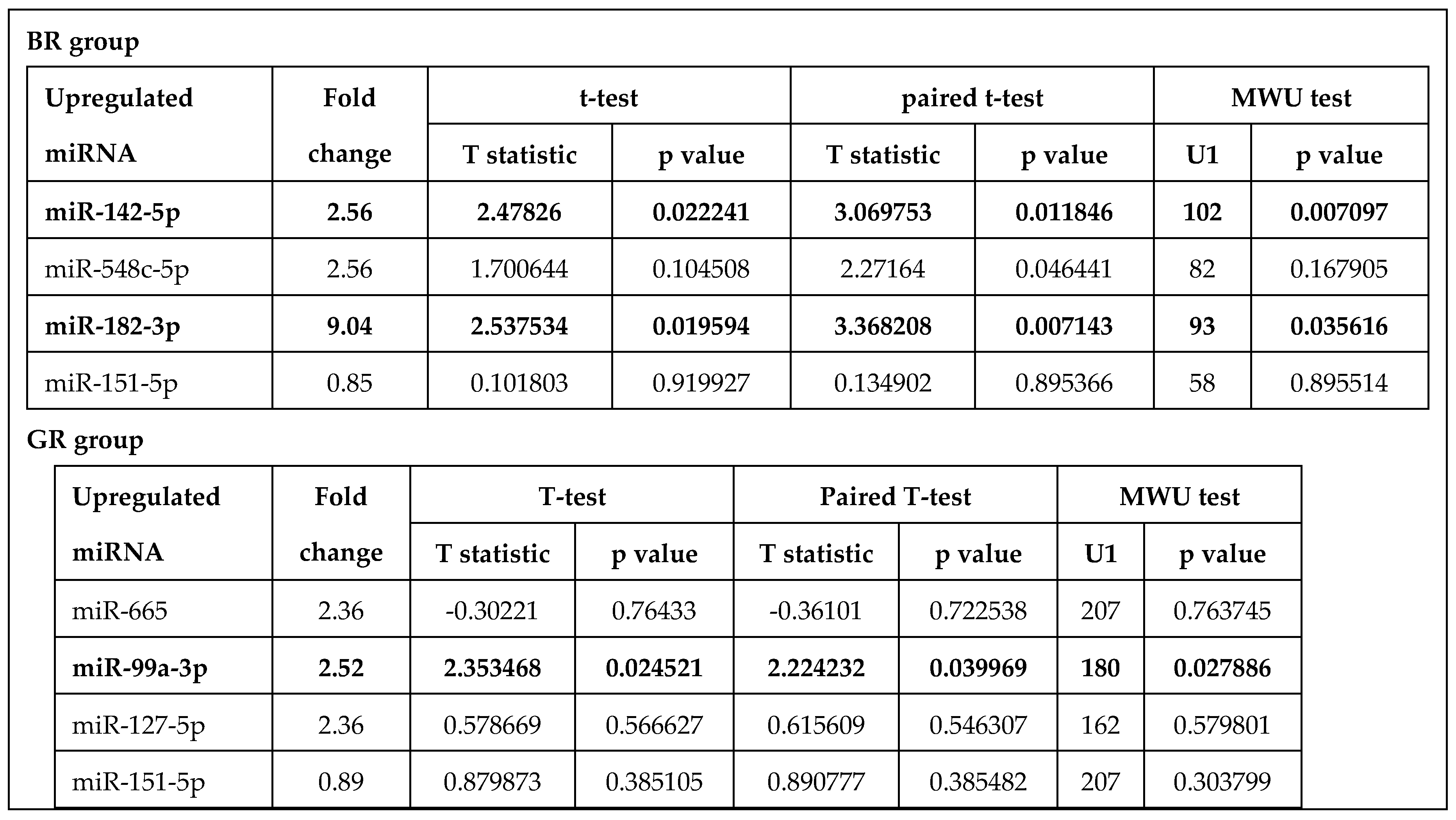
Figure 2.
Target genes of BR group miRNAs and interaction between target gene products.
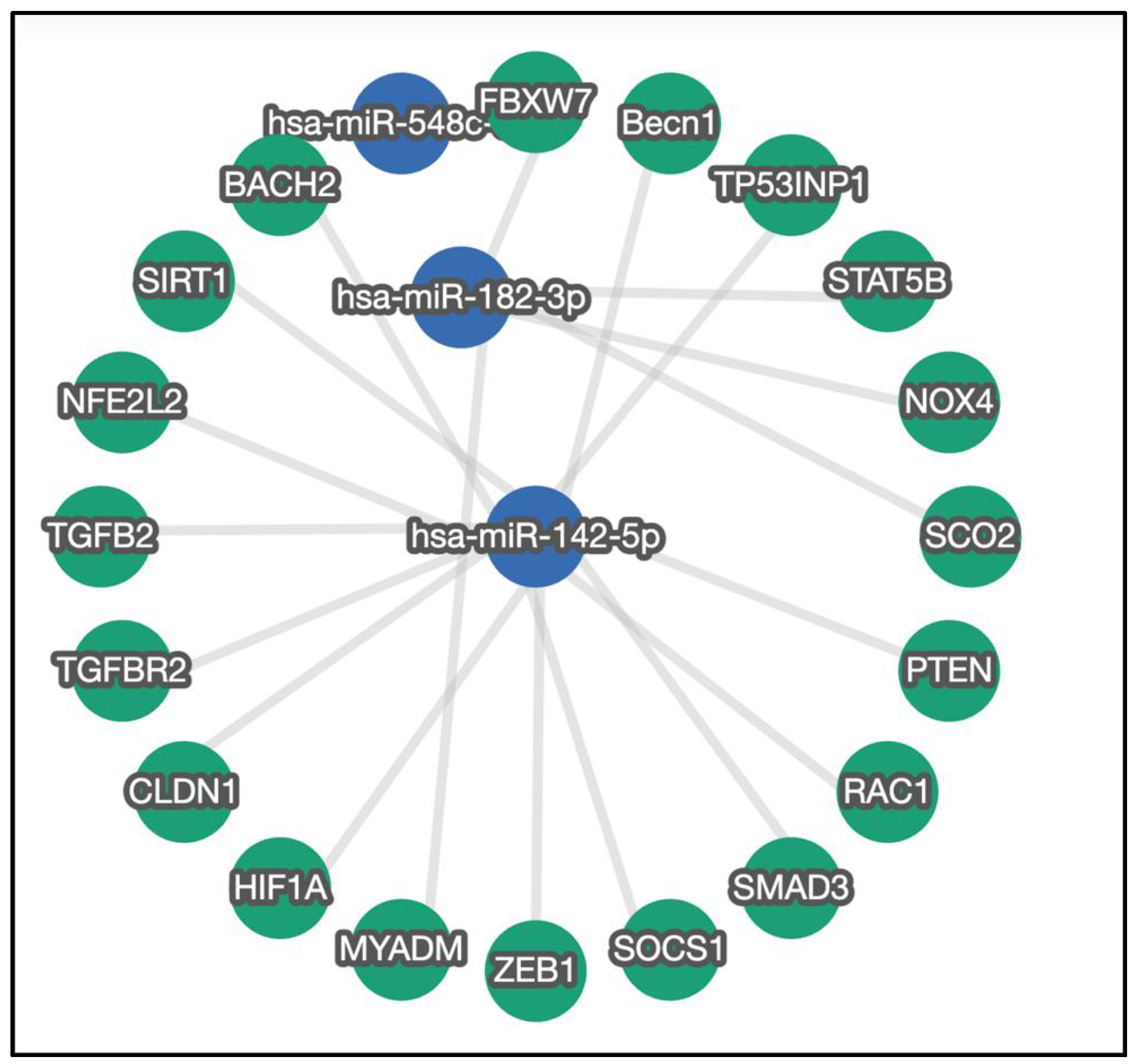
Figure 3.
Target genes of GR group miRNAs and interaction between target gene products. Target of miR-99a-3p are not found in the strong validated criteria, therefore, there is no interaction analysis.
Figure 3.
Target genes of GR group miRNAs and interaction between target gene products. Target of miR-99a-3p are not found in the strong validated criteria, therefore, there is no interaction analysis.
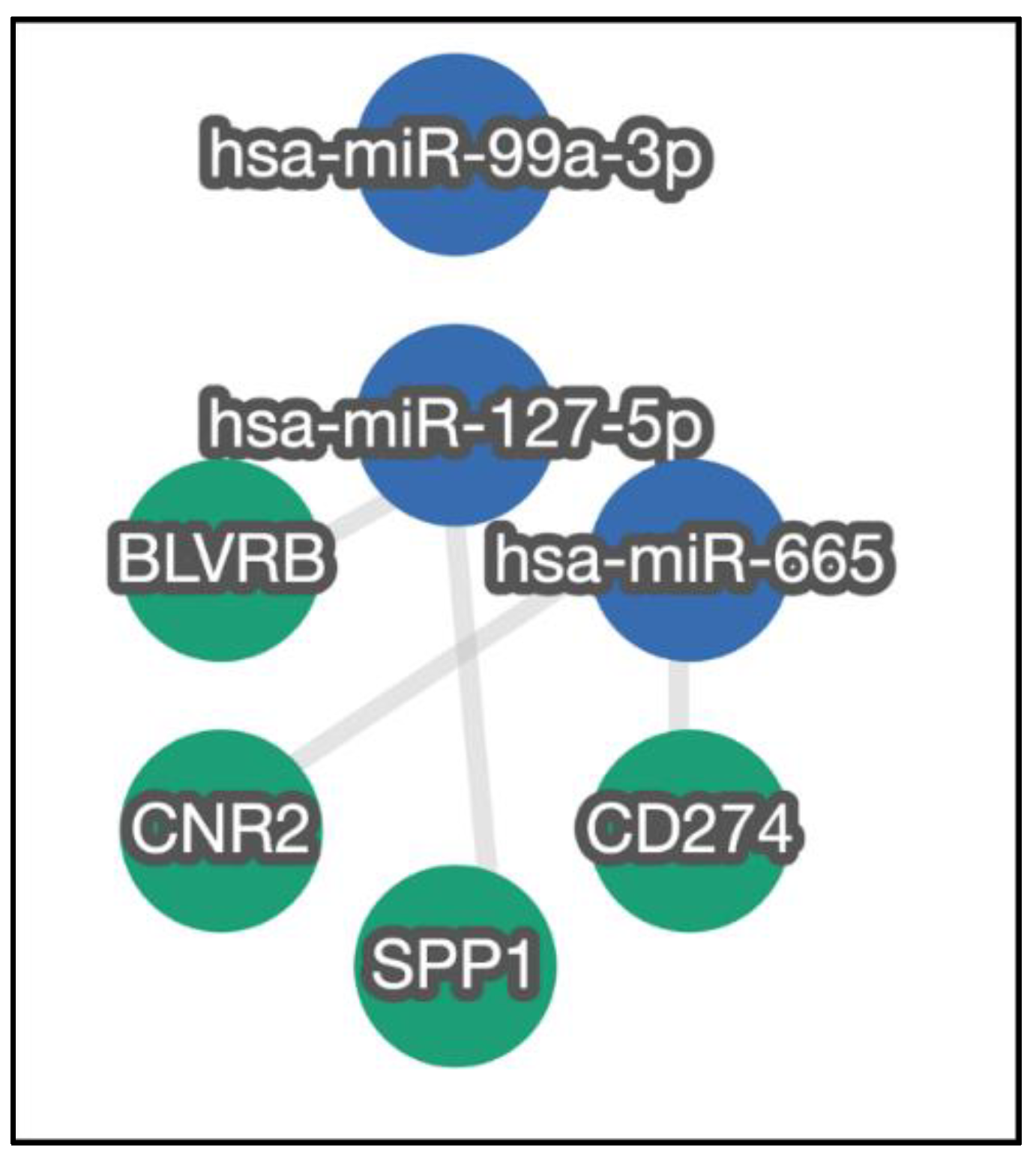
Figure 4.
Survival results based on clinical responses (BR and GR). A – DFS; B – LRFS; C – DMFS; C – OS.
Figure 4.
Survival results based on clinical responses (BR and GR). A – DFS; B – LRFS; C – DMFS; C – OS.
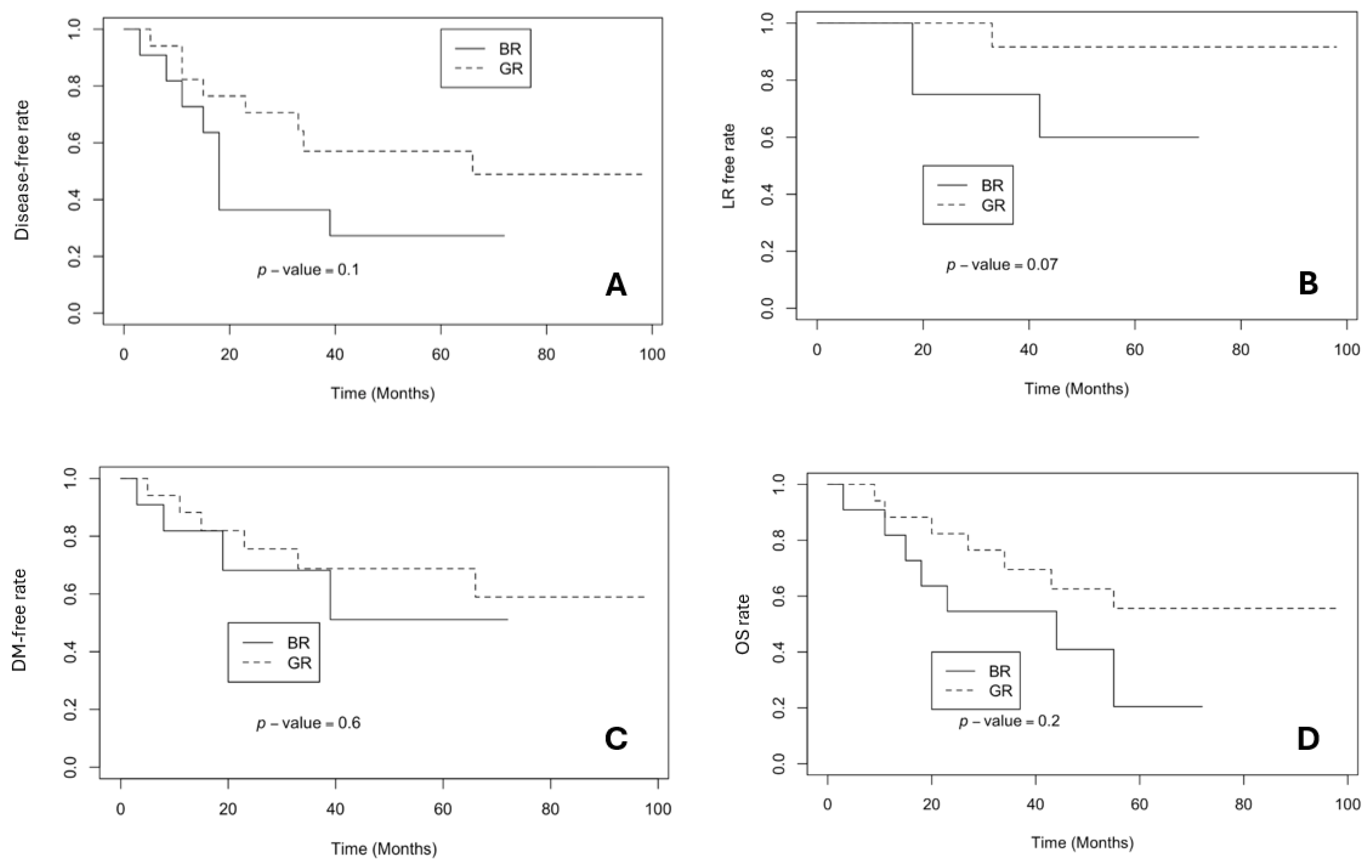
Figure 5.
Survival results based on expression level of miR-142-5p (LRFS and DMFS – data not shown). A – DFS; B – OS.
Figure 5.
Survival results based on expression level of miR-142-5p (LRFS and DMFS – data not shown). A – DFS; B – OS.
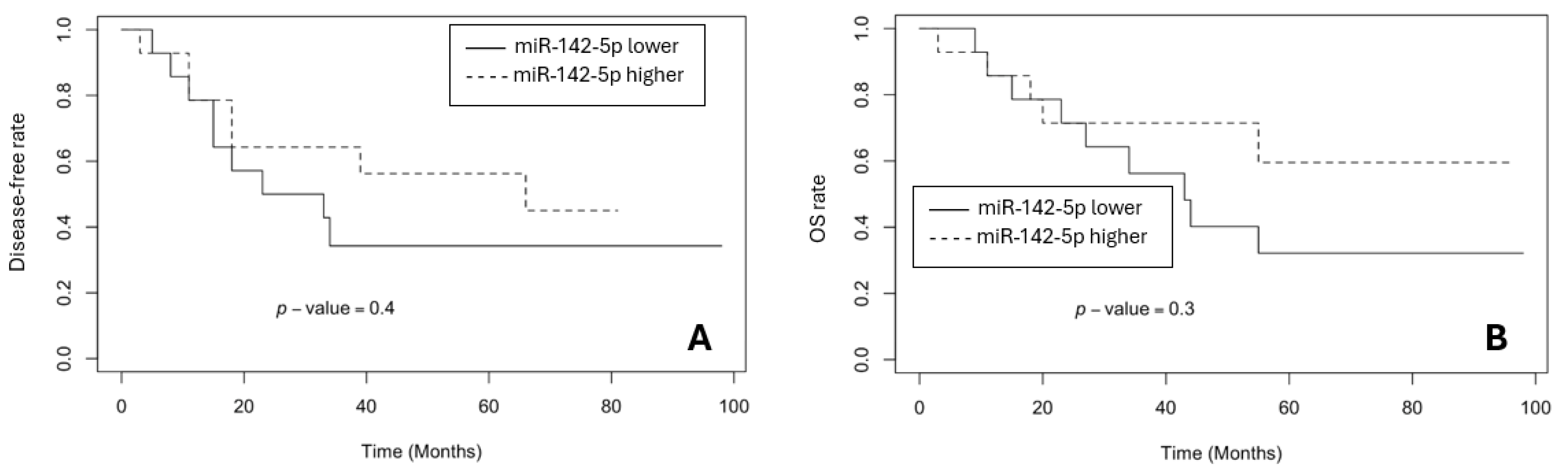
Figure 6.
Survival results based on expression level of miR-182-3p (DMFS data not shown). A – DFS; B – LRFS; C – OS.
Figure 6.
Survival results based on expression level of miR-182-3p (DMFS data not shown). A – DFS; B – LRFS; C – OS.
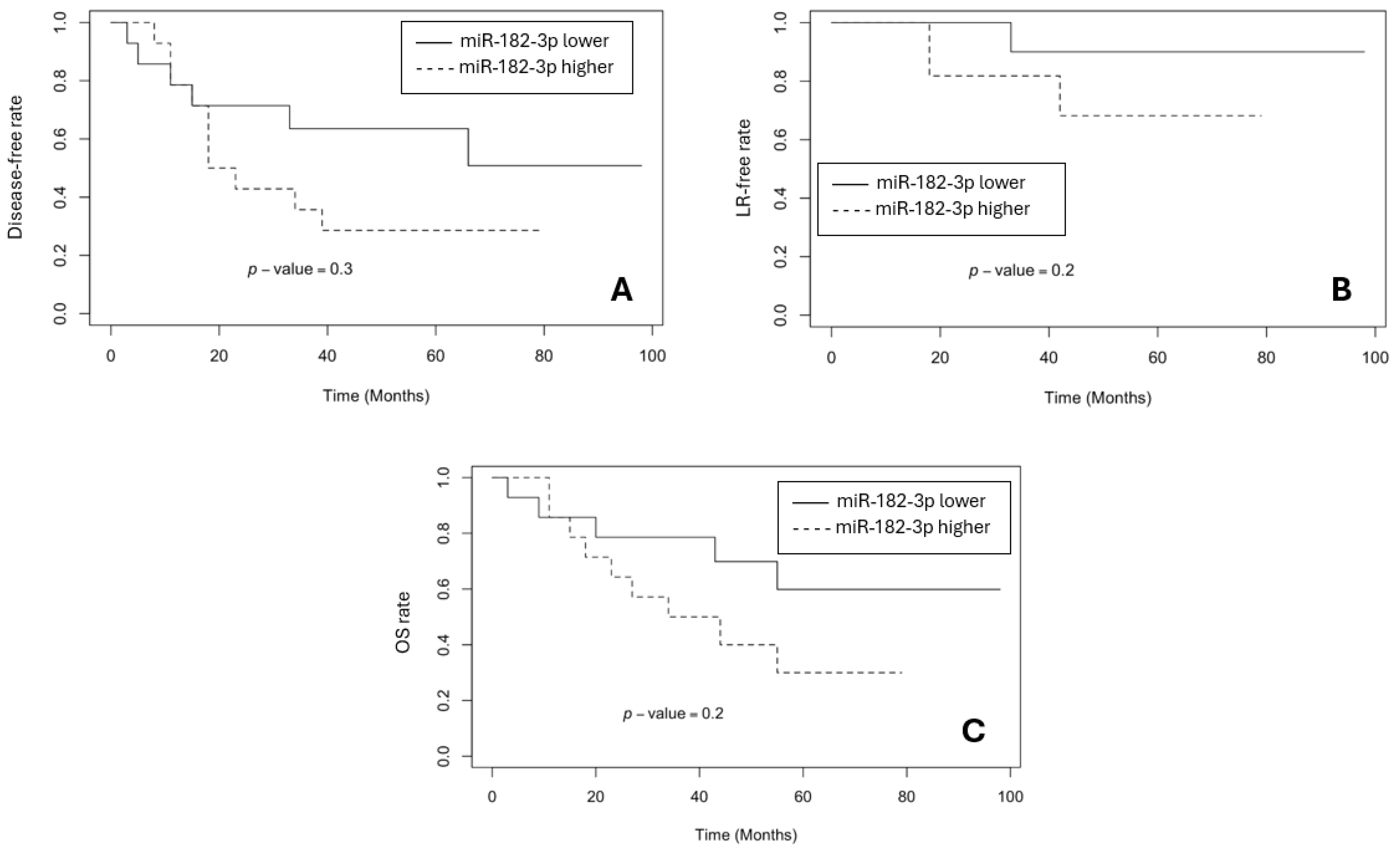
Figure 7.
Survival results based on expression level of miR-99a-3p (LRFS and OS – data not shown). A – DFS; B – DMFS.
Figure 7.
Survival results based on expression level of miR-99a-3p (LRFS and OS – data not shown). A – DFS; B – DMFS.

Table 1.
Dworak classification (adapted from [27]).
Table 1.
Dworak classification (adapted from [27]).
| Dworak | Explanation |
| 0 | No response. |
| 1 | Minimal response to the treatment (predominant tumour tissue with slight fibrosis, vasculopathy; fibrosis <25% of the tumour mass). |
| 2 | Moderate response to the treatment (fibrotic changes dominate, separate tumour groups are observed; fibrosis 25-50% of the tumour mass). |
| 3 | Almost complete response to the treatment (some tumour cells in fibrotic tissue with/without presence of mucin; fibrosis >50% of the tumour mass). |
| 4 | Complete response to the treatment (no tumour cells, only fibrotic tissue or acellular mucin collections). |
Table 2.
Clinical characteristics of the study groups.
| BR group N=17 |
GR group N=23 |
|
|---|---|---|
| PRE-TREATMENT PARAMETERS | ||
|
Gender Male Female |
11 6 |
12 11 |
| Age (mean, range) | 66.47 (41-83) | 65.52 (55-77) |
|
Stage of rectal cancer II III |
3 14 |
1 22 |
|
Tumour grade Grade 1 Grade 2 Grade 3 |
6 10 1 |
9 11 3 |
|
Serum CEA prior to nCRT: CEA ≤5.5 ng/ml CEA >5.5 ng/ml Serum CA19-9 prior to nCRT: CA19-9 ≤33 U/ml CA19-9 >33 U/ml |
15 2 17 0 |
19 4 23 0 |
|
Radiological parameters (pelvic MRI): tumour length (range, mean; cm) tumour circumference (range, mean; %) tumour distance from anal verge (range, mean; cm) node positive disease |
3-11; 6.9 50-100; 88 0-14; 6.9 14 |
3-9; 5.1 25-100; 65 1,5-11; 5.7 21 |
| TREATMENT PARAMETERS | ||
|
Radiation therapy (range of doses; Gy): tumour pelvic lymph nodes |
50.4 – 54 45 – 46.8 |
50.4 – 54 45 – 46.8 |
|
Chemotherapy (type, the way of administration): 5FU, i/v FOLFOX6, i/v Leucovorini + 5FU, i/v Capecitabine, p/o Oxaliplatine, i/v |
12 2 3 0 0 |
13 3 5 1 1 |
|
Surgery: AR HP APR TR |
10 3 4 0 |
12 5 5 1 |
| POST-TREATMENT PARAMETERS | ||
|
Radiological parameters: mrTRG1 mrTRG2 mrTRG3 mrTRG4 mrTRG5 Not done or cannot be evaluated (CT-scan done instead of MRI) |
0 0 7 6 0 4 |
1 8 4 3 0 7 |
|
Morphological parameters Tumour distance from RL (range; cm) Tumour length (range; cm) T stage T1 T2 T3 T4 N stage N0 N1 N2 Mucinous component ≥50% <50% not present Stromal desmoplasia mild moderate severe Inflammatory infiltration mild moderate severe Differentiation Grade 1 Grade 2 Grade 3 Perineural invasion Yes No Vascular invasion Yes No Lymphatic invasion Yes No |
0.5-8 1.5-7.5 1 5 10 1 12 2 3 4 0 13 6 8 3 7 7 3 2 14 1 2 15 1 16 7 10 |
0.5-6 0.8-5 1 9 12 1 16 6 1 0 5 18 14 4 5 18 5 0 4 13 6 4 19 0 23 7 16 |
|
Serum CEA after nCRT: CEA ≤5.5 ng/ml CEA >5.5 ng/ml Serum CA19-9 after nCRT: CA19-9 ≤33 U/ml CA19-9 >33 U/ml |
17 0 17 0 |
23 0 23 0 |
CEA – carcinoembryonic antigen; CA19-9 – carbohydrate antigen 19-9; Gy – gray; i/v – intravenous; 5FU – fluorouracil; FOLFOX6 – leucovorin calcium (folinic acid), fluorouracil, and oxaliplatin; AR – anterior resection; HP – Hartmann’s Procedure; APR – abdominoperineal resection; TR – transanal resection; RL – resection line.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



