
Submitted:
21 December 2024
Posted:
10 January 2025
You are already at the latest version
Abstract
Background/Objectives: This study investigates the relationship between the H2FPEF score and the quality of life in patients with heart failure with preserved ejection fraction; Methods: We performed a prospective observational analysis on 158 hospitalized patients diagnosed with HFPEF who were followed for 12 months after discharge. During hospitalization, we calculated the H2FPEF score for each patient. In addition, we have registered the patients with a severe form of the disease, the patients who were admitted with NYHA class IV and who were discharged with NYHA class III. The follow-up after discharge aimed to monitor the limitation of the usual physical activity, the recently installed fatigue, the presence of leg edema, the ability to exercise regularly and the sadness. We thus obtained data about the quality of life of these patients, the physical and mental limitations, the number of readmissions and the percentage of mortality. To estimate the relationship between the H2FPEF score and each variable we used logistic regression models, providing probabilities for each sign or symptom of the disease mentioned by the patient; Results: All observed variables show statistical significance. The strongest relationship with the H2FPEF score is observed in marked limitations of physical activity, followed by edema and regular exercise; Conclusions: By quickly calculating the H2FPEF score we can predict which patients are at high risk and require more medical resources. Through telemedicine methods, health professionals can do more to treat HFPEF by remotely monitoring the patients. Active management can be implemented through periodic follow-ups to monitor the quality of life and through strategies to prevent and limit the number of decompensations of the disease in vulnerable patients.
Keywords:
cardiovascular disease
; heart failure
; H2FPEF
; risk stratification
; telemedicine
1. Introduction
Heart failure with preserved ejection fraction, HFPEF, also known as diastolic heart failure, accounts for up to 54% of heart failure (HF) cases. HFPEF is defined by symptoms and signs of heart failure as the result of high left ventricular (LV) filling pressure despite normal LV ejection fraction (LVEF; ≥50 percent) [1,2,3,4].
It is very important to diagnose this disease given the increased prevalence and the unfavorable prognosis, which is like the one of heart failure with reduced ejection fraction (HFPEF) [3]. A patient diagnosed with this disease has a 20% chance of surviving another 10 years, this prognosis being worse than for most forms of cancer [4,5].
The burden of the disease is felt by the patient, in the decreased quality of life and functional disability; by family, through the need to take care of him/her, being dependent on a family member for the regular physical activities; by society, the patient is often unable to work and is socially marginalized due to a lack of activities adapted to the disease. [6,7,8,9].
In Romania, but also globally, in 2024, cardiac recovery and rehabilitation programs are beginning to be developed. These programs are needed because the patient hospitalized for heart failure almost always returns home upon discharge, under the same environmental conditions and with insufficient medical education on the correction of precipitating risk factors. Moreover, returning home makes it almost impossible to follow them at least in the short term when these patients are in the vulnerable period of the disease [9,10,11].
A quick solution until the development of such monitoring and recovery programs and centers is complete is telemedicine.
To date, there are limited studies targeting the H2FPEF score. They provided data on the prognosis of the disease, the association of ischemic heart disease and comorbidities. [11,12,13,14]
In the management of the disease, we consider it very useful to follow patients at home, to be able to intervene quickly with therapeutic measures before HF decompensation. Currently, there is limited data on the quality of life at home of these patients [15,16,17]. We used the most accessible signs and symptoms of the disease that can be easily identified by the patient and that reflect the quality of life (difficulty in performing regular physical activities, presence of leg edema and inability to exercise). During hospitalization, we identified the most vulnerable patients with the highest risk of HF decompensation. Thus, we recorded patients who were admitted with the highest NYHA class, NYHA class IV, and patients who were discharged with NYHA class III.
We wanted to be able to predict from the moment the patients came to the hospital which one of them will be more vulnerable at home and which will require more frequent medical check-ups. Thus, in our study, we calculated the H2FPEF score for each patient at the time of admission and associated each score value with the signs and symptoms mentioned. We have obtained statistically significant results that predict the health status of patients at home. We have shown that follow-up can also be done through telemedicine, an accessible, cheap and effective solution.
2. Materials and Methods
2.1. Study Design and Study Population
The present prospective, observational study was conducted in the Cardiology Department of the “Bagdasar-Arseni” Emergency Hospital in Bucharest, Romania, during an enrollment period of 1 year and 6 months, from May 2021 to October 2022 and following the patients’ evolution after discharge for 12 months, from May 2022 to April 2023. The study was conducted on a sample of 158 patients, over 18 years old and diagnosed with preserved LVEF. The cohort was constituted of patients admitted with a diagnosis of heart failure with preserved ejection fraction, LVEF ≥50 percent.
The follow-up was carried out by phone call in the first year after the discharge, due to the difficulty of follow-up in the cardiology clinic in the context of the recent SARS-COV2 virus pandemic.
The inclusion criteria were: (1) patients over 18 years old; (2) patients of either sex; (3) patients with signs/symptoms of heart failure; (4) patients with NT-proBNP >=300ug/ml; (5) patients with LVEF (left ventricular ejection fraction) >=50% objectified echocardiographically; (6) patients with only signs and symptoms specific to the disease; (7) patients who signed the informed consent and agreed the prospective follow-up and to participate in the evaluation through telephone.
The exclusion criteria were: (1) patients with LVEF < 50%; (2) patients with NT-proBNP < 300ug/ml; (3) patients with severe valvular diseases; (4) patients with severe neuropsychiatric diseases; (5) patients with severe liver, kidney or lung disease; (6) patients with ongoing infection; (7) patients diagnosed with autoimmune diseases or malignancy; (8) patients with moderate and severe anemia; (9) patients with hope of survival less than 1 year; (10) patients who did not sign the informed consent and did not wish to be contacted by phone.
All the patients had venous blood samples collected within 30 minutes from admission. The NT-proBNP level was evaluated through the Elisa method with a PATHFAST compact autoanalyzer.
The LVEF (left ventricular ejection fraction) values were obtained using transthoracic echocardiography performed during the hospitalization. The modified Simpson biplane method was used to calculate the left ventricular end-systolic volumes (LVESVs) and end-diastolic volumes (LVEDVs) from 4 and 2-chamber views. The LV volumes were corrected for body surface areas.
The demographic data considered were age, gender, emergency admission or appointment, NYHA class, normal or arterial hypertension, atrial fibrillation, overweight and obesity. The mean age of the patients enrolled in the study was 72.21, the minimum age was 40 and the maximum age was 93.

Table 1.
Age of the studied population.
| Age | |
|---|---|
| count = 158 | |
| mean | 72.21519 |
| std | 10.4524 |
| min | 40 |
| max | 93 |
| 25% | 66 |
| 50% | 72.5 |
| 75% | 80 |
Figure 1.
Age distribution of the studied population.
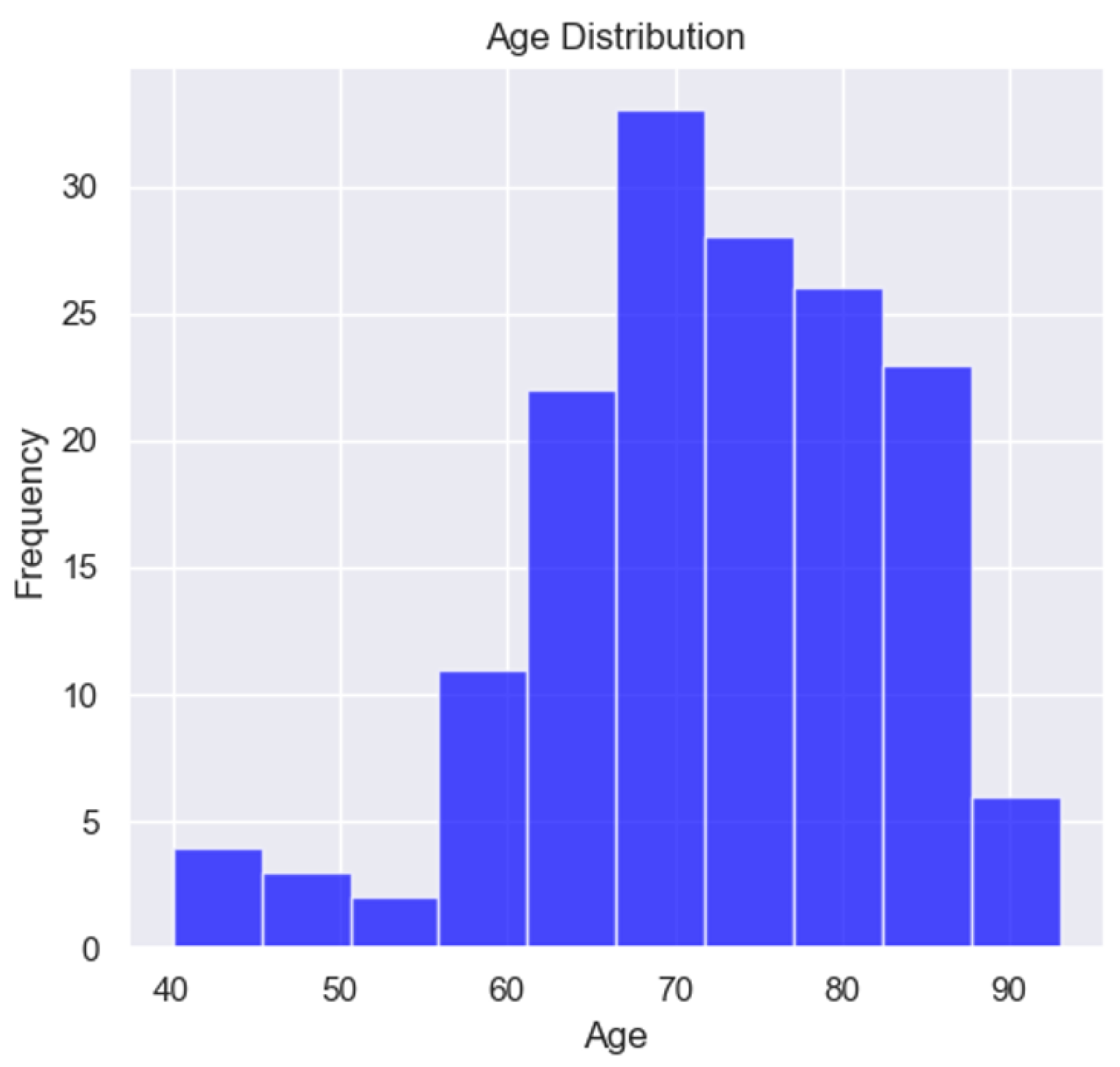
In the study, only 9 patients were under 60 years old, suggesting a prevalence of the disease in elderly patients, a characteristic of HFPEF.
Table 2.
Demographic and clinical characteristics of the studied population.
| Variable | Prevalence % |
|---|---|
| Female | 63% |
| Male | 37% |
| Admission Emergency | 72% |
| Admission Appointment | 28% |
| NYHA class I | 1% |
| NYHA class II | 9% |
| NYHA class III | 53% |
| NYHA class IV | 37% |
| Normal blood pressure | 3% |
| Hypertension stage I | 11% |
| Hypertension stage II | 30% |
| Hypertension stage III | 56% |
| Atrial fibrillation | 46% |
| Overweight and obesity | 78% |
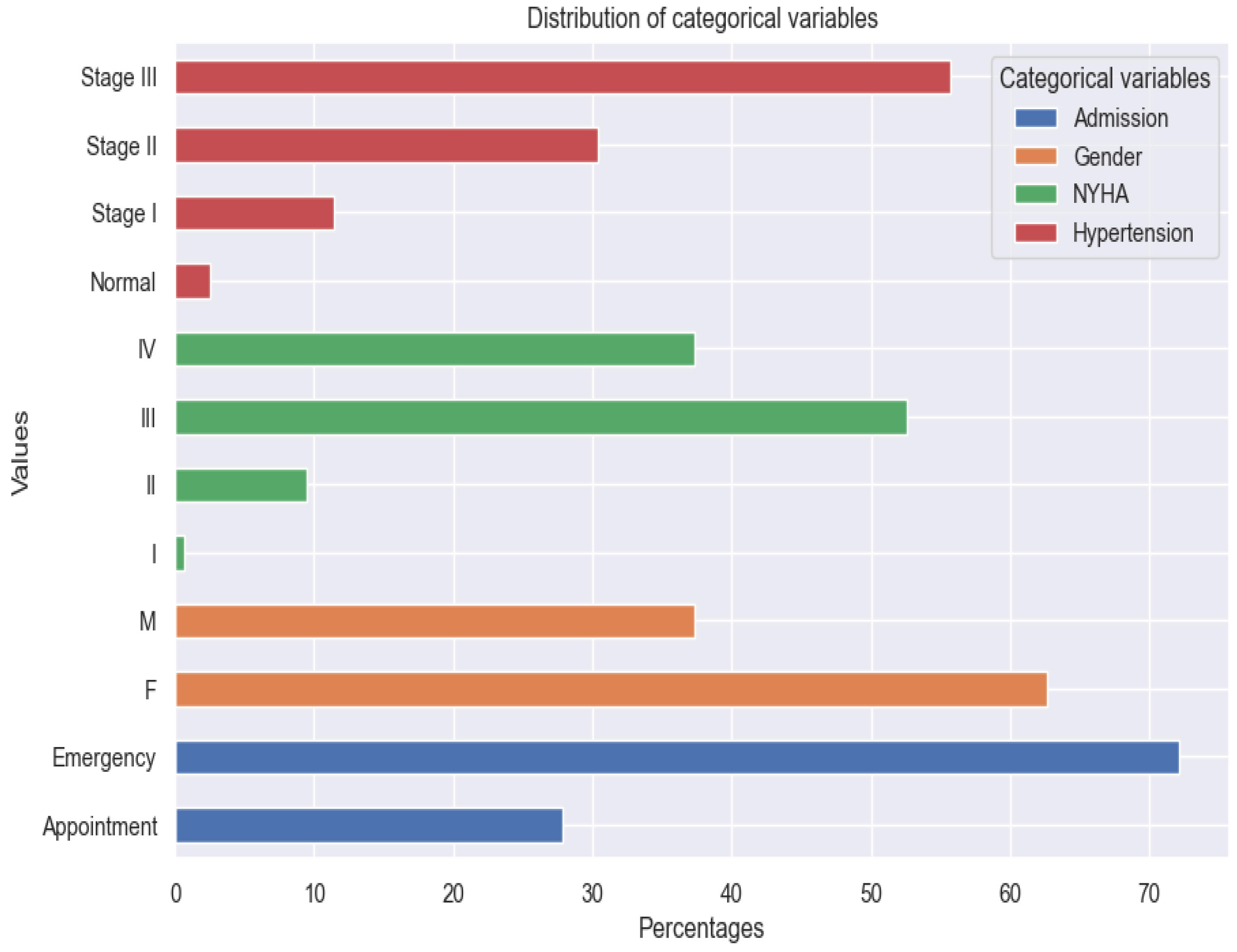
Figure 2.
Distribution of categorical variables.
The tracked quality-of-life factors were the following: marked limitation of physical activity, edema, recent fatigue, the ability to exercise and sadness. Data about the NYHA class at admission and at discharge and about palpitations was collected from the last clinical examination.
All the variables used are binary described by the following summary statistics table.
Table 3.
All variables used in the research.
| Variable | Count | True | False | True Percentage |
|---|---|---|---|---|
| Pitting Edema | 142 | 56 | 86 | 39% |
| Marked Limitation of Physical Activity | 142 | 101 | 41 | 71% |
| Sadness | 142 | 93 | 49 | 65% |
| Ability to Exercise | 142 | 37 | 105 | 26% |
| Palpitations | 158 | 59 | 99 | 37% |
| NYHA class III at Discharge | 158 | 27 | 131 | 17% |
| NYHA class IV at Admission | 158 | 59 | 99 | 37% |
| Recent Fatigue | 142 | 99 | 43 | 70% |
These variables were chosen to describe patients' quality of life because they have a direct impact on lifestyle and show the symptoms and limitations caused by heart failure decompensation. For example, the presence of pitting edema, marked limitation of physical activity and fatigue at regular exertion indicate an exacerbation of the disease. These patients should be medically reassessed as soon as possible.
The inability to exercise daily is a parameter that is associated with the limitations of the disease and contributes to the unfavorable evolution.
Illness means physical and mental limitations so we wanted to identify also which patients were sad and could benefit from psycho-emotional support.
We considered it useful to use some parameters from the hospitalization of the patients to determine if there is a relationship between them and the H2FPEF score. One variable was the presence of palpitations. This parameter is a symptom of the disease and at the same time contributes to the course of the disease. It suggests a possible cause - atrial fibrillation - which must be investigated and treated if it exists.
Also, important in our study was the follow-up of patients who were admitted with NYHA class IV and those who were discharged with NYHA class III. They are the most vulnerable patients during hospitalization and at home and they require prolonged active follow-up.
Below, we have the distribution of the independent variable used in this research, the H2FPEF score, a specific indicator of Heart Failure with Preserved Ejection Fraction.
Figure 3.
(a, b) Distribution of the H2FPEF score.
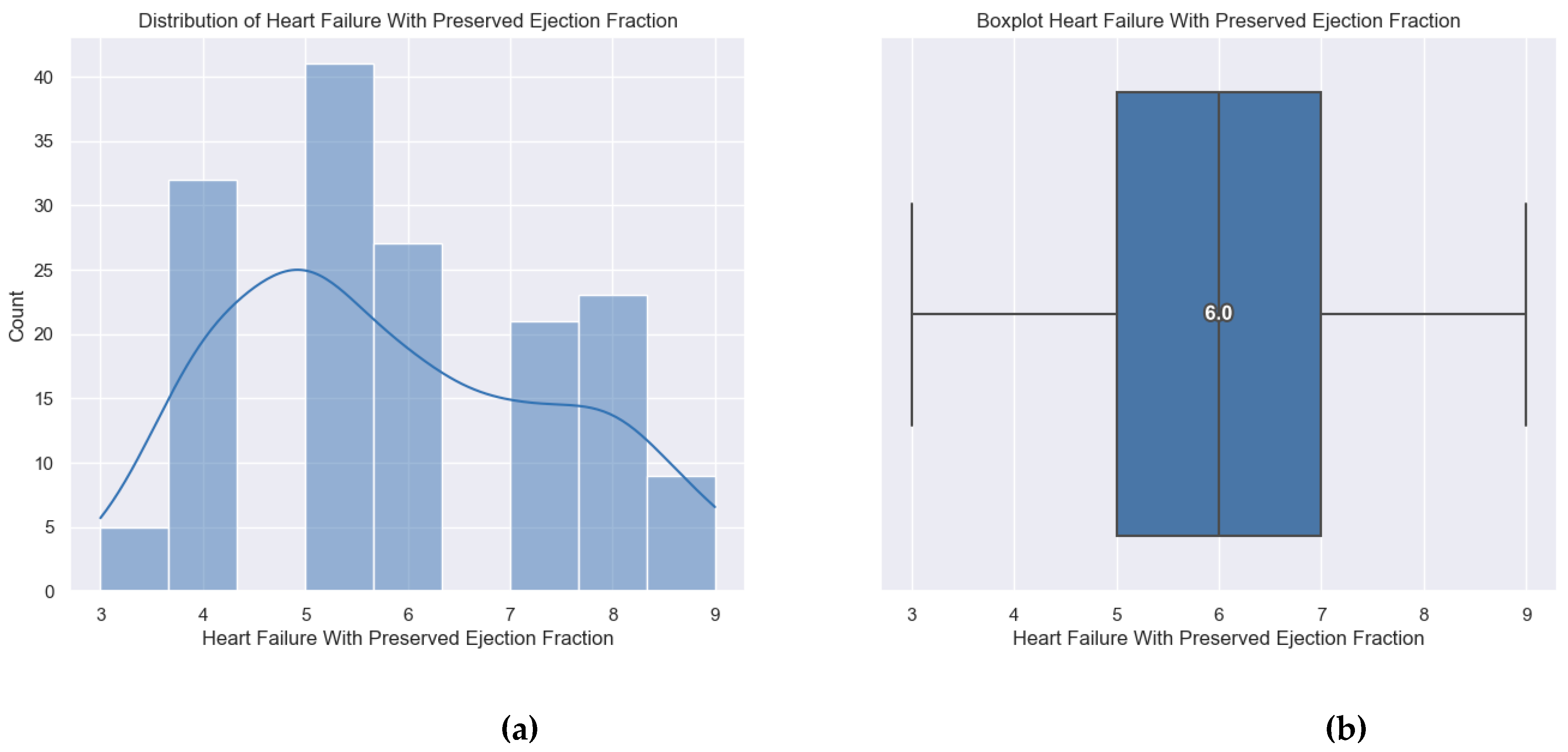
The patients enrolled in the study had a minimum H2FPEF score of 3 points, a maximum score of 9 points and the average score was 6 points.
Quality of life data was obtained through a telephone interview in which patients answered the questions below. The average duration of a phone call was 15 minutes. Also, the patients received indications regarding lifestyle optimization, about precipitating factors, about the need for periodic monitoring and about a new clinical reassessment, for symptomatic patients.
It should be mentioned that 16 patients died, representing 10% of the total number. The main cause was HF for 10 patients, stroke for 4 patients and neoplasia diagnosed after discharge for 2 patients.
We mention that for the parameters recorded during hospitalization (NYHA class IV at admission, NYHA class III at discharge and palpitations) we performed statistical analysis on data obtained from all 158 patients. For the variables obtained from the answers provided during the phone interview (marked limitation of physical activity, pitting edema, recent fatigue, ability to exercise and sadness) we recorded and analyzed data for only 142 patients. The other 16 patients died within the first year after discharge.
During the first year of follow-up, 31% of patients had at least one readmission for heart failure worsening.
The questions of the phone interview were:
- In the last month, have you breathed harder during physical efforts?
- Do you have pitting edemas?
- Are you feeling more tired lately?
- Do you manage to exercise minimum 30 min/day, minimum 5 days/week?
- Are you sad? Is your sadness caused by the cardiovascular disease?
- Have you been admitted to a cardiology ward in the last year? If the answer was Yes, the reason for hospitalization was also specified.
We mention that only the answers that were related to the evolution of heart failure were considered.
We tried to find a correlation between the answers provided and the value of the H2FPEF score to be able to predict which patients are at higher risk and thus be able to make an early identification of the vulnerable ones. These patients require closer follow-up through frequent check-ups with a general practitioner or cardiologist. They and their families should be medically educated about the precipitating factors and the signs and symptoms of the disease’s decompensation to get to the doctor faster.
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania (protocol code PO-35-F-03, October 1st, 2021).
2.2. Statistical Analysis
To better understand the impact of the Heart Failure with Preserved Ejection Fraction score (H2FPEF) on binary life quality indicators, logistic regression analysis was conducted. This approach allows the estimation of the probability of each indicator based on the H2FPEF score, assessing statistical significance through associated p-values. A p-value threshold of 0.05 was used. If the p-value was below the threshold, the model was considered statistically significant. The research design involved running separate logistic regressions for each life quality indicator, treating the H2FPEF score as the independent variable and the indicators as the dependent variables. All analyses were performed using Python, utilizing standard statistical packages such as Pandas, Statsmodels and Scikit-learn.
3. Results
This section presents the results of the logistic regression analyses, highlighting the impact of the H2FPEF score on the probability of the studied variables.
3.1. Marked Limitation of Physical Activity
There is a pronounced effect of the H2FPEF score on the likelihood of experiencing limitations in physical activity. The coefficient is 0.6211, indicating a positive relationship, with a p-value that is very close to 0, suggesting strong statistical significance.
Table 4.
Logistic regression applied to Marked limitation of physical activity based on H2FPEF score.
Table 4.
Logistic regression applied to Marked limitation of physical activity based on H2FPEF score.
| Dep. Variable: | Marked Limitation of Physical Activity | No. Observations: | 142 | |||
| Model: | Logit | Df Residuals: | 140 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.1258 | |||
| Converged: | True | LL-Null: | -85.344 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -2.5011 | 0.817 | -3.062 | 0.002 | -4.102 | -0.9 |
| Heart Failure with Preserved Ejection Fraction | 0.6211 | 0.153 | 4.065 | 0 | 0.322 | 0.921 |
Figure 4.
The probabilities of having limitation of physical activities associated with each score.
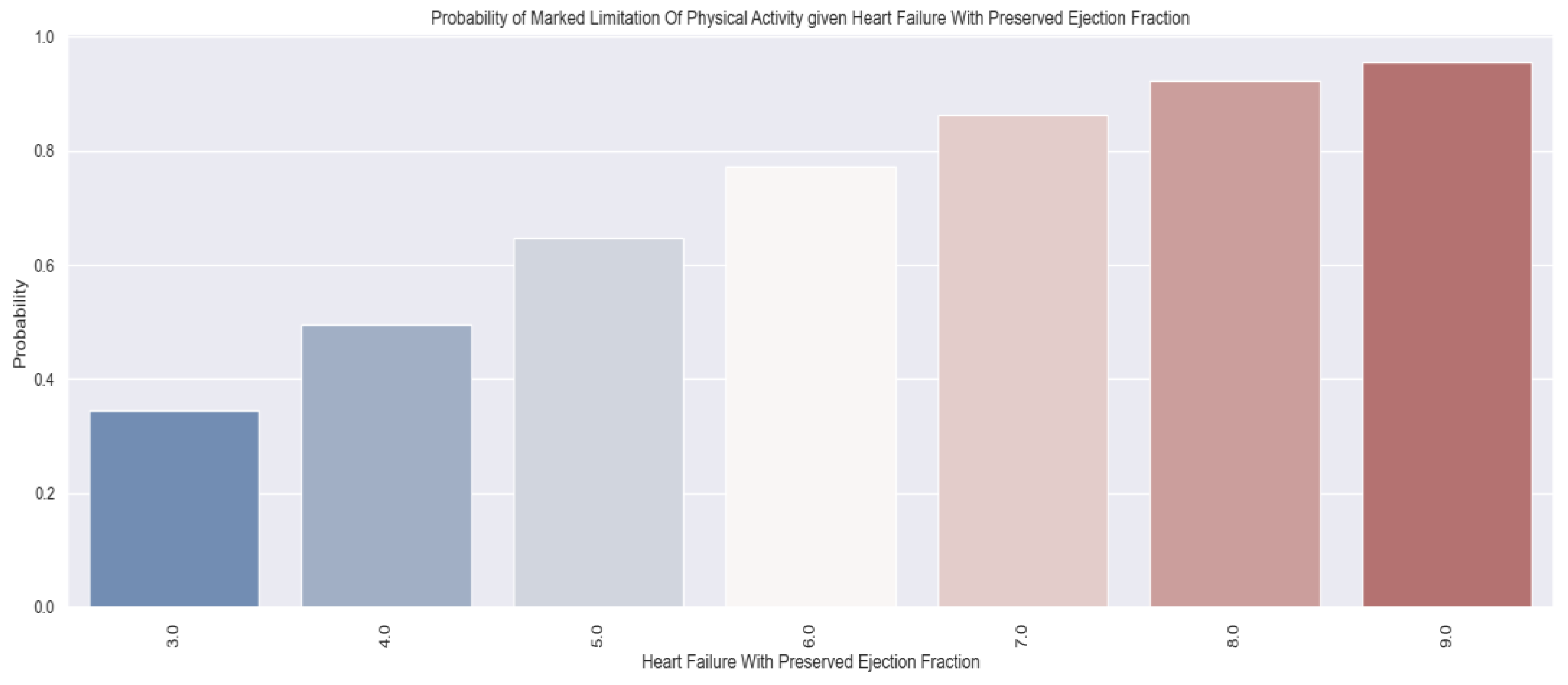
The higher the H2FPEF score, the higher the probability of not being able to perform usual physical activities. Thus, at an H2FPEF score of only 4 points, approximately 50% of patients could not perform usual physical exertion, while at a score of 7 points, over 80% of patients had significant limitations of physical activity.
Figure 5.
(a, b, c) H2FPEF score grouped by Marked limitation of physical activity.
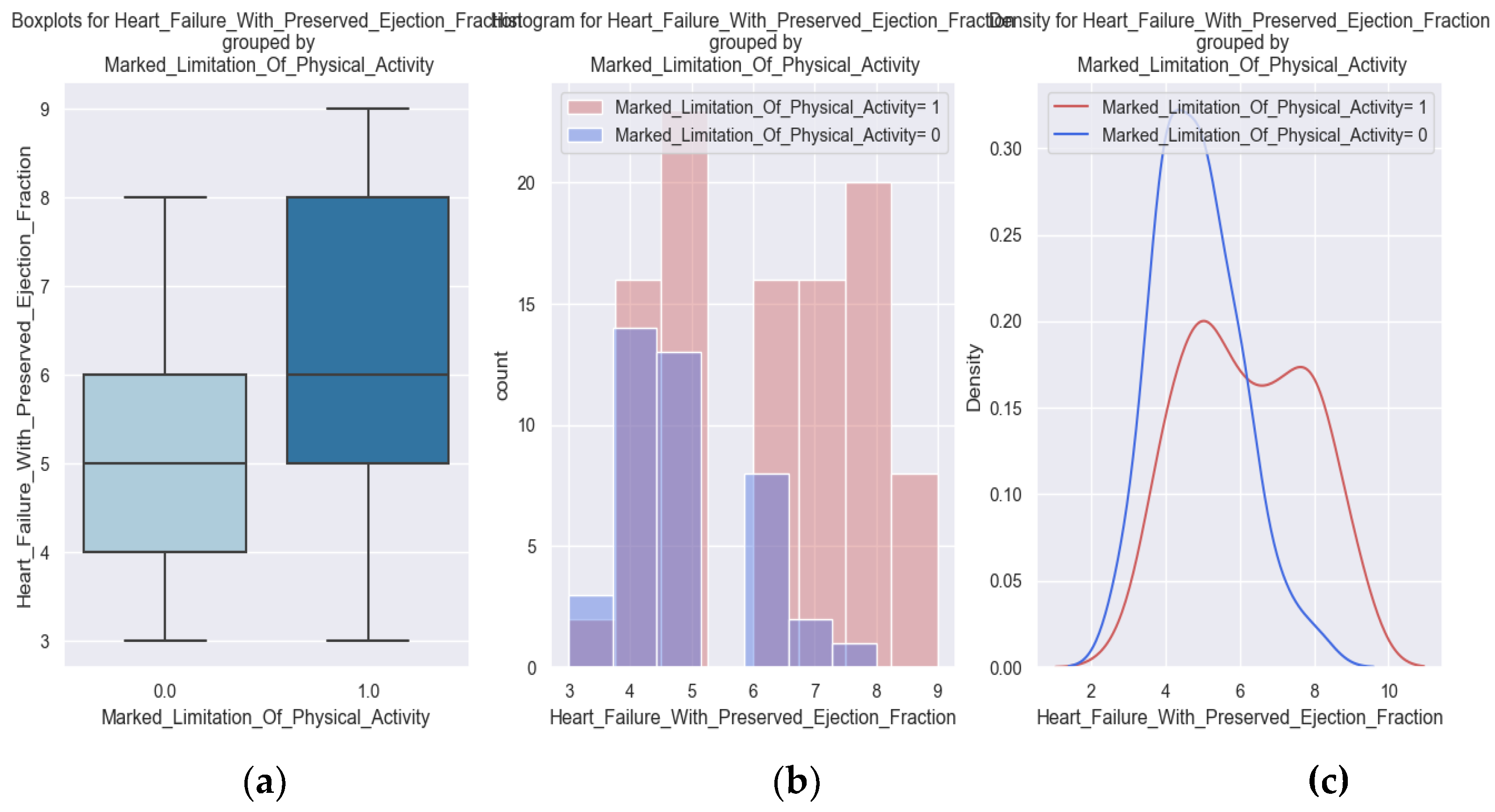
The limitation of physical activity caused by the disease is also highlighted in the diagrams above. A higher score is correlated with a greater probability for the patients to have important limitations.
3.2. Edema
Edema is a sign of heart failure that can be easily identified by patients. Weight gain and signs such as pitting edema should determine the patient to go to the doctor as soon as possible for adjustment of the therapeutic regimen. Knowing which patients could develop pitting edema according to the H2FPEF score is useful for preventing the decompensation of the disease.
Table 5.
Logistic regression applied to Pitting edema based on H2FPEF score.
| Dep. Variable: | Pitting Edema | No. Observations: | 142 | |||
| Model: | Logit | Df Residuals: | 140 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.08172 | |||
| Converged: | True | LL-Null: | -95.234 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -3.0206 | 0.723 | -4.176 | 0 | -4.438 | -1.603 |
| Heart Failure with Preserved Ejection Fraction | 0.4387 | 0.117 | 3.748 | 0 | 0.209 | 0.668 |
Figure 6.
The probability of having edema based on the value of the H2FPEF score.
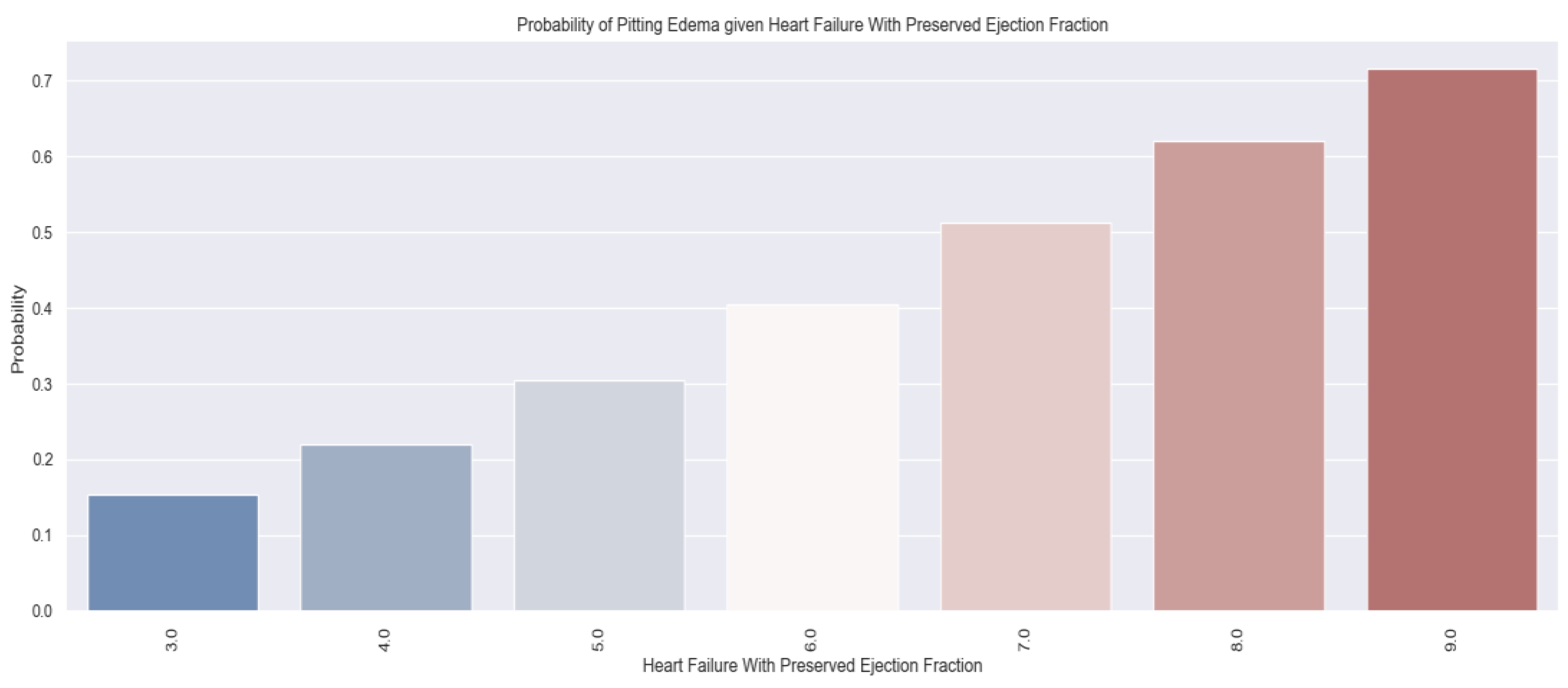
As the score is increasing, the probability of having edema is increasing. The patient with a H2FPEF score of 7 points has a probability of 50% of having pitting edema.
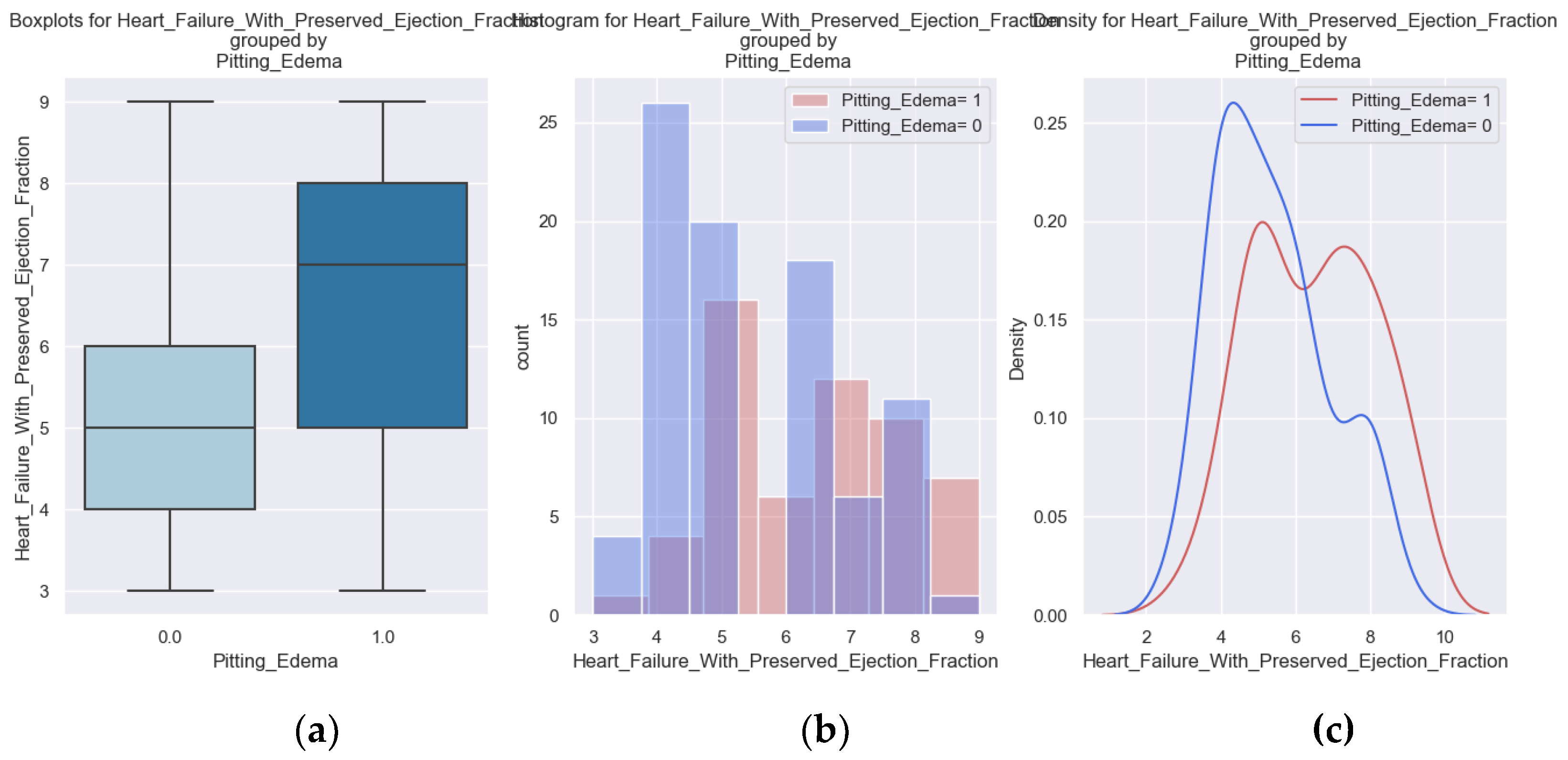
Figure 7.
(a, b, c) Boxplots and diagrams for Pitting edema and H2FPEF score.
3.3. Recent Fatigue
Fatigue is another indicator of the disease that we tracked during the phone interview. The installation of fatigue and its presence at small efforts means decompensation of the disease. The logistic regression demonstrates that as the H2FPEF score increases, the probability of experiencing fatigue rises. The regression coefficient is positive (0.3795), with a corresponding p-value of 0.003, indicating statistical significance.
Table 6.
Logistic regression applied to Fatigue based on H2FPEF score.
| Dep. Variable: | Recent Fatigue | No. Observations: | 142 | |||
| Model: | Logit | Df Residuals: | 140 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.05591 | |||
| Converged: | True | LL-Null: | -87.079 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -1.2961 | 0.724 | -1.79 | 0.073 | -2.715 | 0.123 |
| Heart Failure with Preserved Ejection Fraction | 0.3795 | 0.129 | 2.943 | 0.003 | 0.127 | 0.632 |
Figure 8.
The probability of experiencing Fatigue based on H2FPEF score.
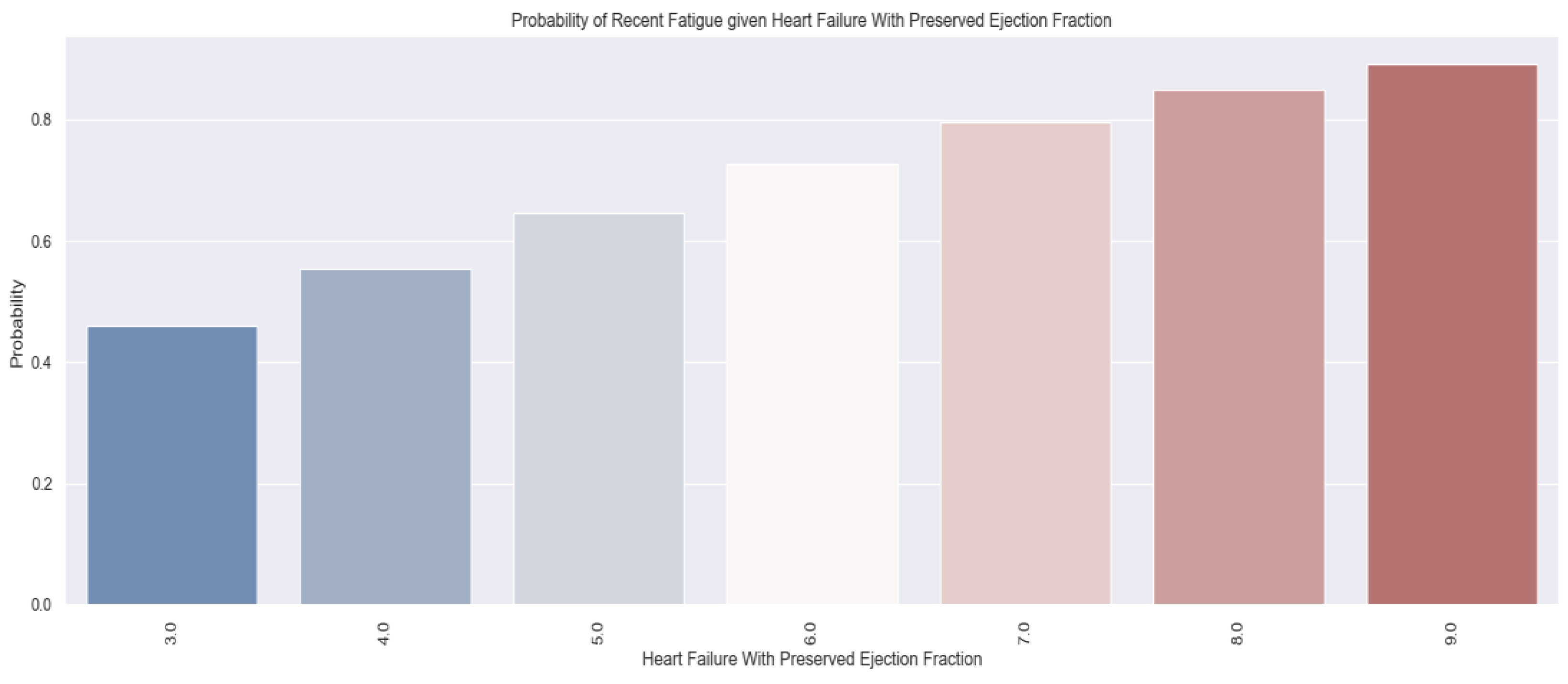
Almost all patients with a score of 9 points felt tired at home. The fatigue was caused by the disease. For patients with an H2FPEF score of 4 points, the probability of fatigue on regular exertion is greater than 50%.
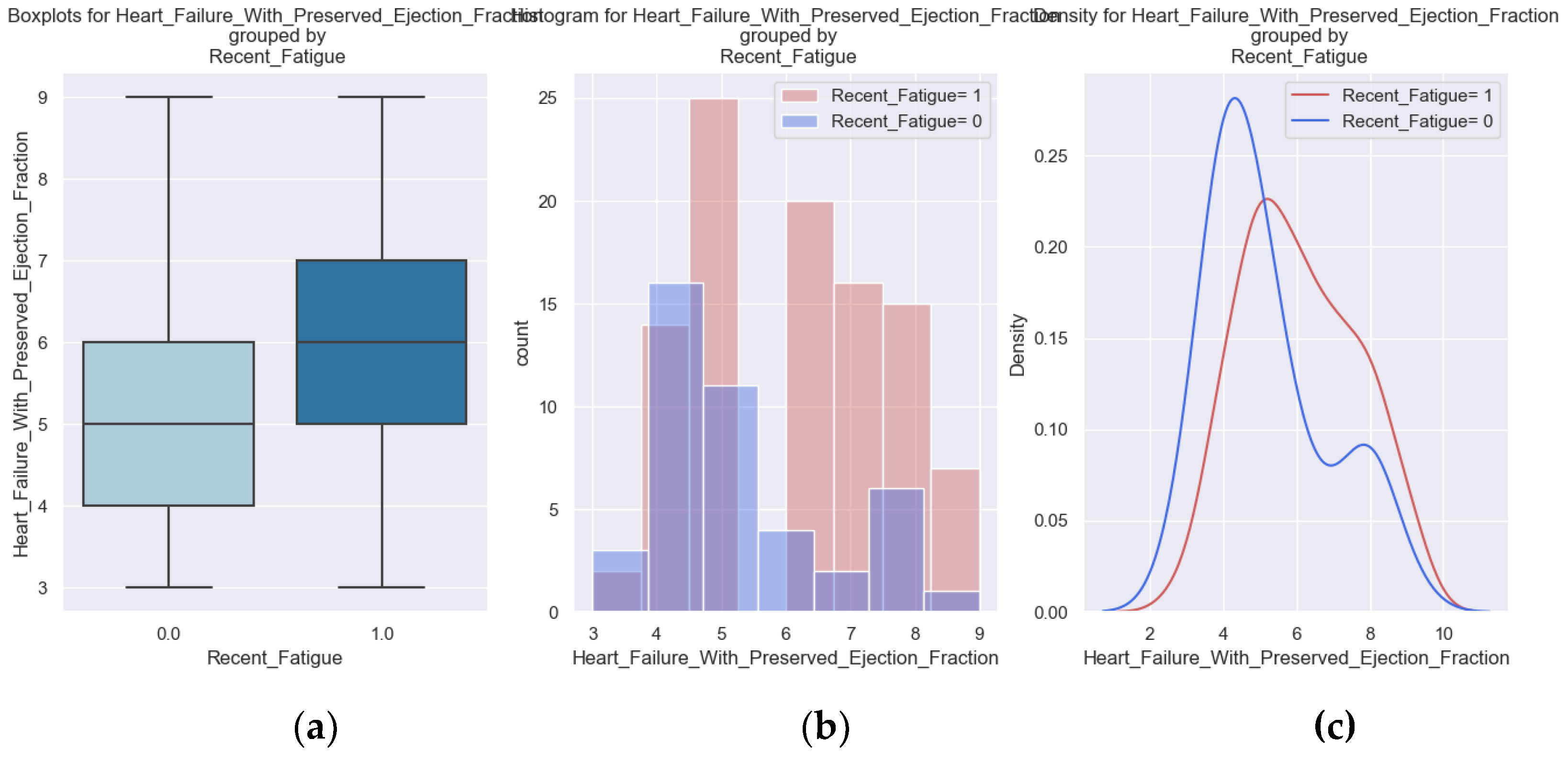
Figure 9.
(a, b, c) Boxplots and diagrams for Fatigue and H2FPEF score.
3.3. Regular Exercise
The indication to exercise regularly, within the limit of personal tolerance and with a gradual increase in effort, is received by all patients with heart failure. However, the disease, readmissions, diuretic medication and physical deconditioning limit patients' possibilities to do it.
Sustained medical education of patients and their family members and participation in cardiac recovery programs can improve the physical capacity of patients.
Table 7.
Logistic regression applied for Regular exercise based on H2FPEF score.
| Dep. Variable: | Sport | No. Observations: | 142 | |||
| Model: | Logit | Df Residuals: | 140 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.06212 | |||
| Converged: | True | LL-Null: | -81.458 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | 1.242 | 0.763 | 1.627 | 0.104 | -0.254 | 2.738 |
| Heart Failure with Preserved Ejection Fraction | -0.4112 | 0.139 | -2.967 | 0.003 | -0.683 | -0.14 |
The logistic regression demonstrates that when the H2FPEF score is increasing, the probability of exercising decreases. The regression coefficient is negative (-0.4112), with a corresponding p-value of 0.003, indicating statistical significance.
Figure 10.
The probability of exercising regularly according to the H2FPEF score value.
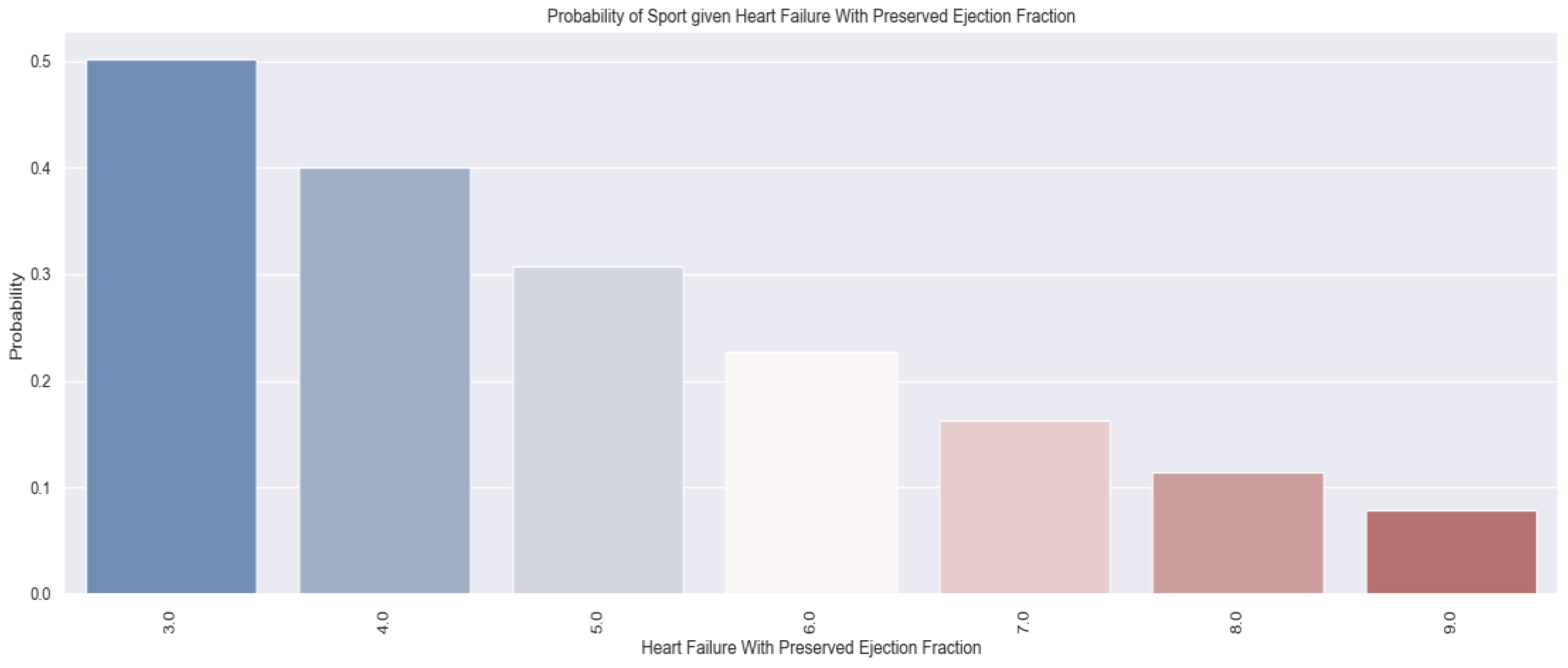
We notice that only 15% of patients with a score of 7 points exercise regularly.
One in two patients with a H2FPEF score of 3 points manage to perform the recommended regular exercises, while a patient with a score of 9 points has a probability of exercising lower than 10%.
Knowing these probabilities, we must instruct these patients to participate in cardiac recovery programs to improve their physical capacity.
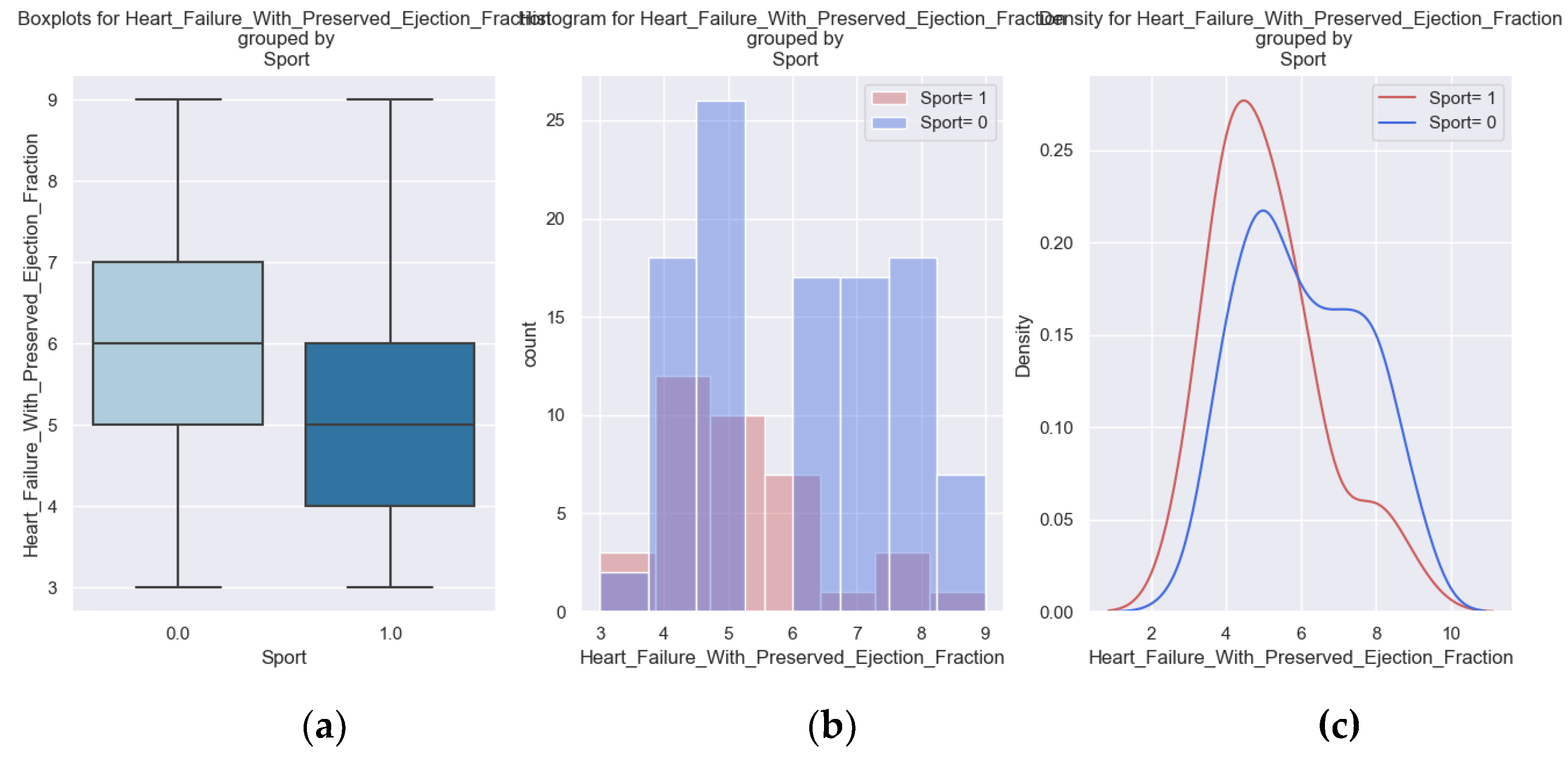
Figure 11.
(a, b, c) Boxplots and diagrams for Regular exercise and the H2FPEF score.
3.4. Sadness
HFPEF is a disease with many physical, social and mental limitations, so patients with heart failure are prone to be sad. The improvement of the mental state has beneficial effects on the evolution of disease. The patient shows up on time for medical check-ups, administers their treatment correctly and completely and performs the recommended regular physical activity.
Table 8.
Logistic regression applied for Sadness based on H2FPEF score.
| Dep. Variable: | Sadness | No. Observations: | 142 | |||
| Model: | Logit | Df Residuals: | 140 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.06504 | |||
| Converged: | True | LL-Null: | -91.496 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -1.6508 | 0.71 | -2.324 | 0.02 | -3.043 | -0.259 |
| Heart Failure with Preserved Ejection Fraction | 0.4064 | 0.125 | 3.24 | 0.001 | 0.161 | 0.652 |
The regression coefficient is positive (0.4064), with a corresponding p-value of 0.001, indicating statistical significance.
Figure 12.
The probability of Sadness according to the H2FPEF score.
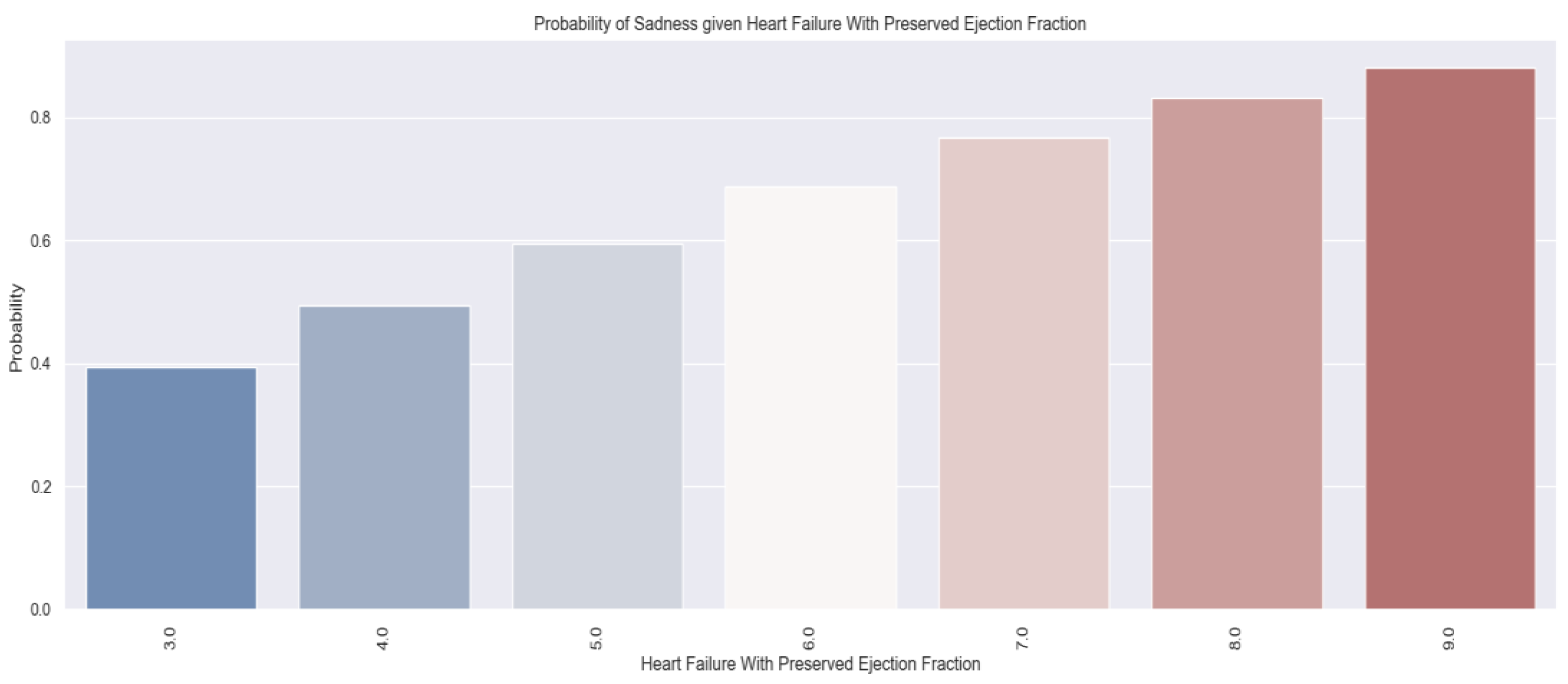
As the score increases, the likelihood of feeling sad increases. Patients with an H2FPEF score of 7 points have a more than 70% probability of being sad. According to the table and the graphs above, the H2FPEF score can be a good predictor for sadness. By knowing which patients are vulnerable, psycho-emotional counseling measures can be taken.
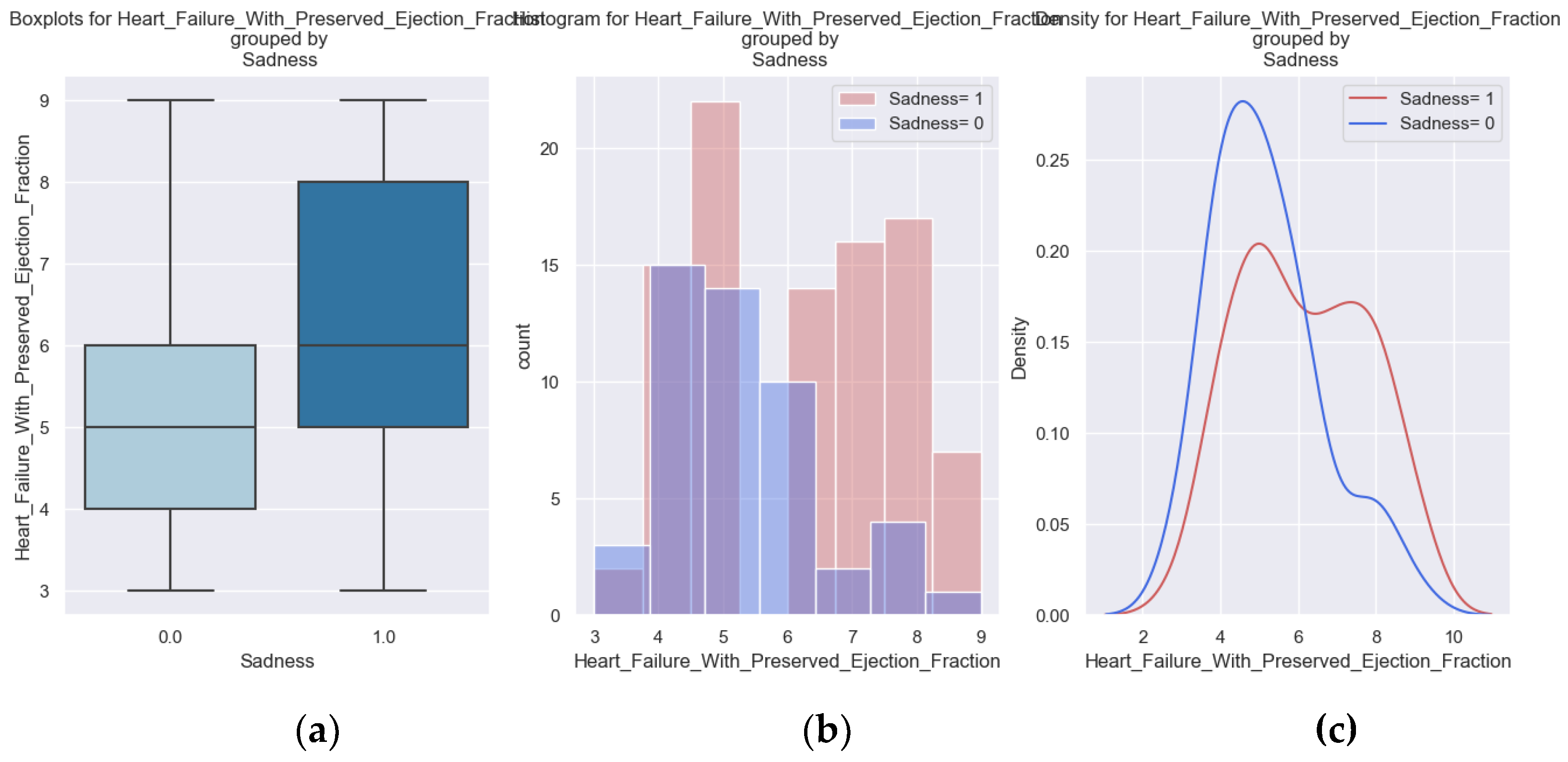
Figure 13.
(a, b, c) Boxplots and diagrams for Sadness and H2FPEF score.
3.5. Palpitations
The logistic regression below demonstrates that as the H2FPEF score increases, the probability of experiencing palpitations rises. The regression coefficient is positive (0.3218), with a corresponding p-value of 0.003, indicating statistical significance.
Table 9.
Logistic regression applied for Sadness based on H2FPEF score.
| Dep. Variable: | Sadness | No. Observations: | 158 | |||
| Model: | Logit | Df Residuals: | 156 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.0451 | |||
| Converged: | True | LL-Null: | -104.4 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -2.4251 | 0.668 | -3.629 | 0 | -3.735 | -1.115 |
| Heart Failure with Preserved Ejection Fraction | 0.3218 | 0.108 | 2.991 | 0.003 | 0.111 | 0.533 |
To gain a clearer understanding of the probability associated with each score value, the following probabilities were derived from the estimated model.
Figure 14.
The probability of Palpitation based on the H2FPEF score.
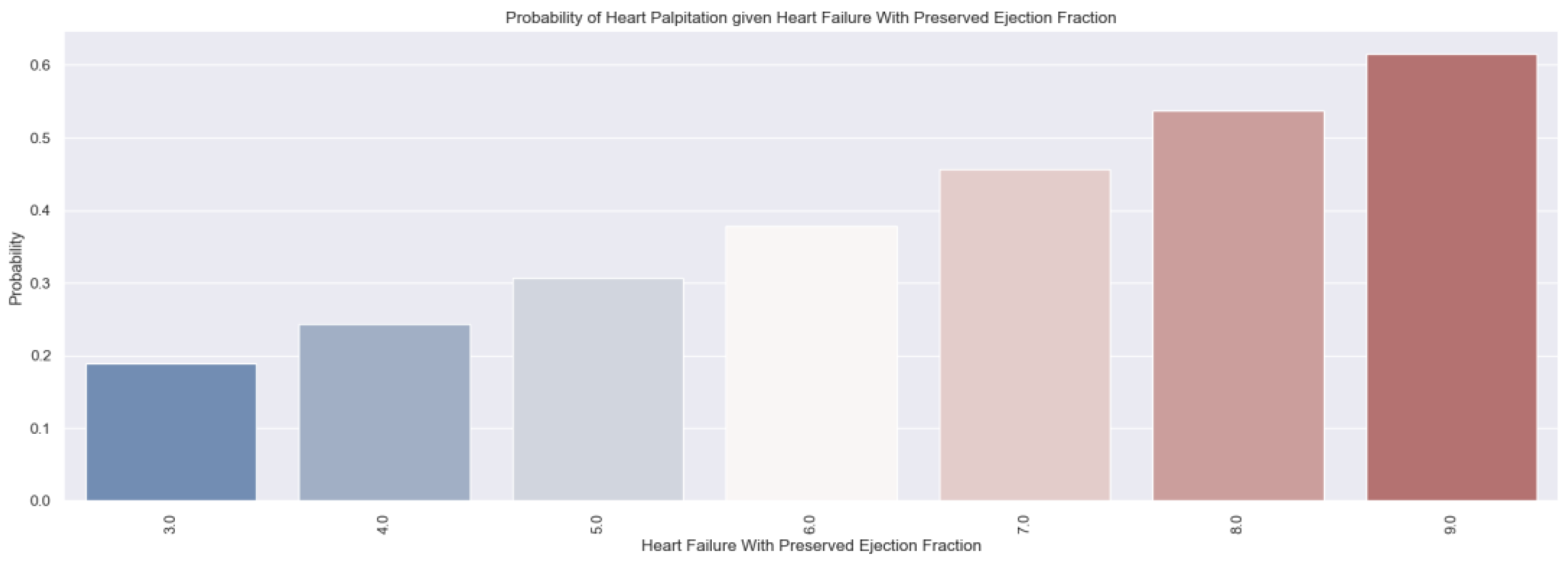
It is important to know which patients have palpitations. They are caused by the decompensation of the disease and the possible onset of atrial fibrillation. Detecting palpitations early is beneficial because measures to control the rhythm, the heart rate and prevent cardioembolic complications can be taken quicker.
According to the obtained results, we expect a patient with a high H2FPEF score to have palpitations and require additional treatment to improve his prognosis.
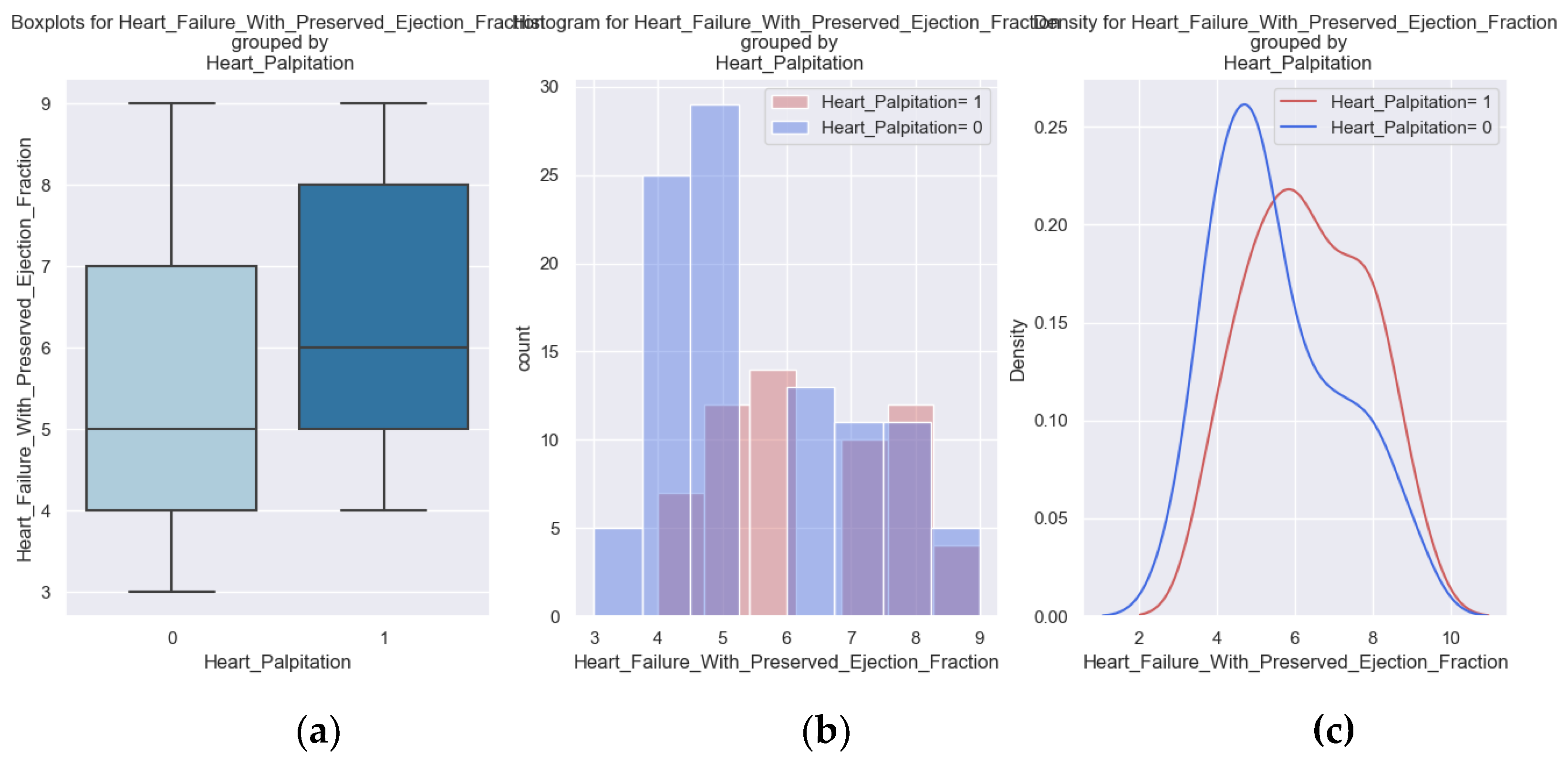
Figure 15.
(a, b, c) Boxplots and diagrams for Palpitation and H2FPEF score.
3.6. NYHA Class IV at Admission
37% of HFPEF patients in our study were admitted with the highest functional class, NYHA class IV, which shows the severity and difficulty of managing this disease.
Table 10.
Logistic regression of NYHA class IV at admission and H2FPEF score.
| Dep. Variable: | Sadness | No. Observations: | 158 | |||
| Model: | Logit | Df Residuals: | 156 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.03916 | |||
| Converged: | True | LL-Null: | -104.4 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -2.2871 | 0.663 | -3.452 | 0.001 | -3.586 | -0.989 |
| Heart Failure with Preserved Ejection Fraction | 0.2988 | 0.107 | 2.797 | 0.005 | 0.089 | 0.508 |
The probability of being classified as NYHA IV at admission is significantly associated with the H2FPEF score. With a p-value of 0.005 and a coefficient of 0.2988, this indicates that as the score increases, the likelihood of being in NYHA class IV at admission also rises.
Figure 16.
The probability of NYHA class IV at admission given by the H2FPEF score.
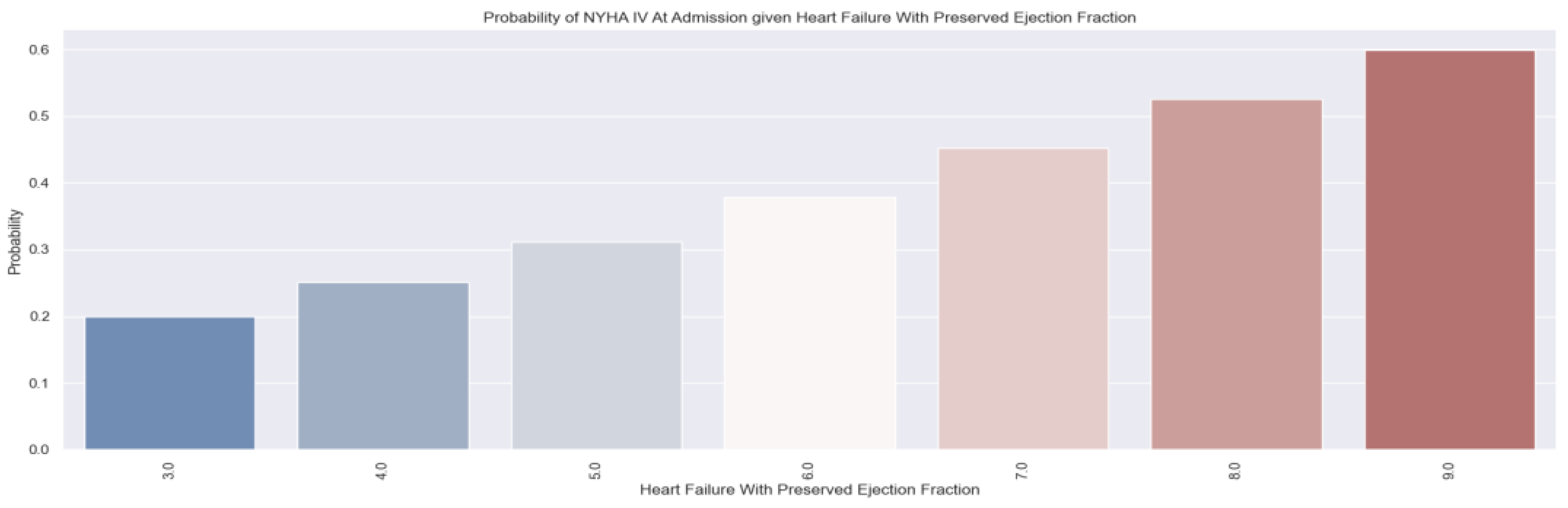
We wanted to see how likely a patient it is to be in NYHA class IV at admission based on the H2FPEF score. For example, a patient who has an H2FPEF score of 7 points has a probability of 50% of being admitted in the most serious condition. This shows from the start that he/she is a high-risk patient and requires more medical interventions.
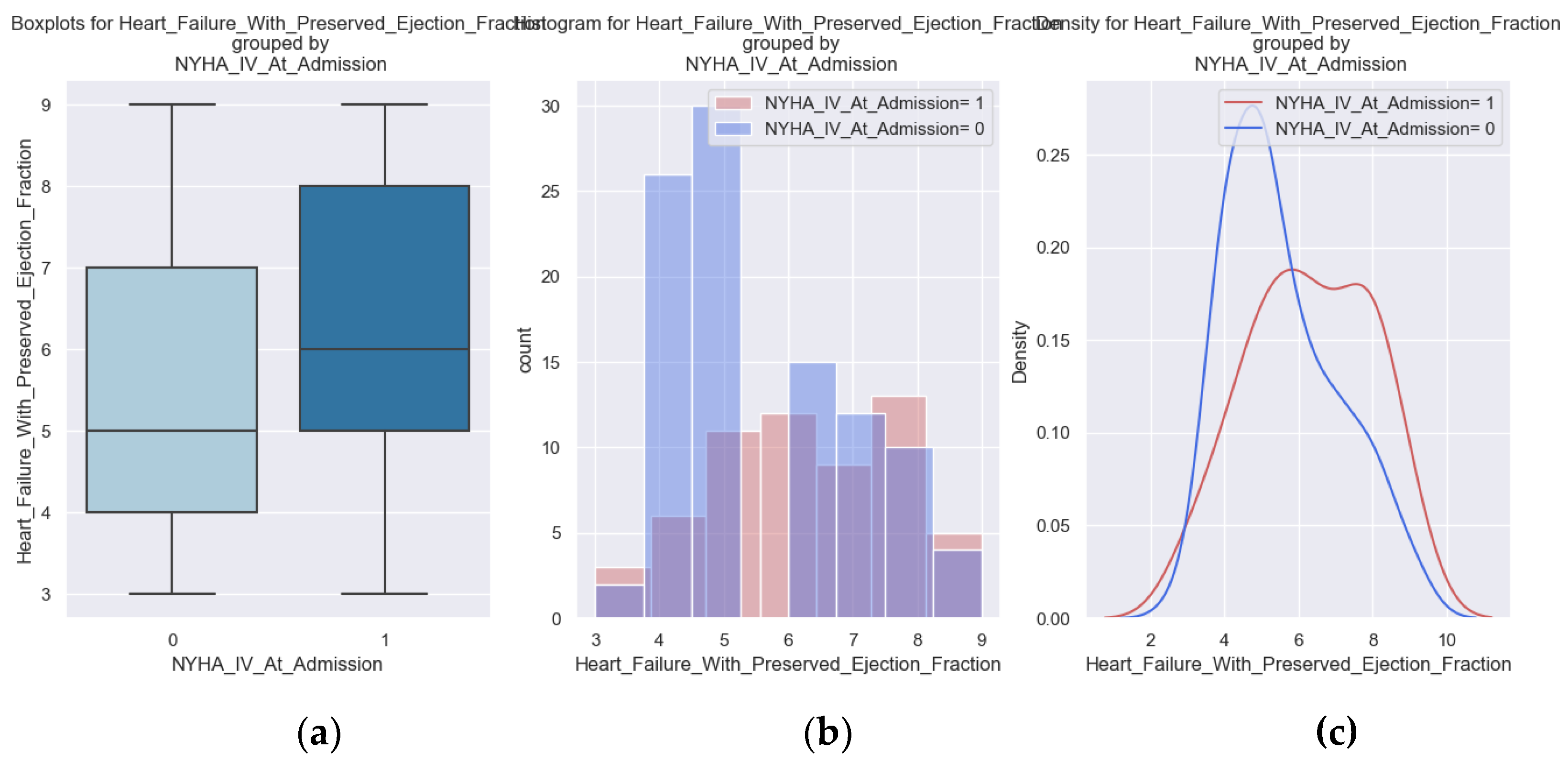
Figure 17.
(a, b, c) Boxplots and diagrams for NYHA class IV at admission and H2FPEF score.
3.7. NYHA Class III at Discharge
17% of the enrolled patients were discharged with NYHA class III, which means that they become symptomatic at the slightest effort, through dyspnea, fatigue, palpitations and angina.
Table 11.
Logistic regression applied to NYHA class III at discharge and the H2FPEF score.
| Dep. Variable: | Sadness | No. Observations: | 158 | |||
| Model: | Logit | Df Residuals: | 156 | |||
| Method: | MLE | Df Model: | 1 | |||
| Date: | Sun, 29 Sep 2024 | Pseudo R-squ.: | 0.04509 | |||
| Converged: | True | LL-Null: | -72.252 | |||
| Coef | Std err | z | P>|z| | [0.025 | 0.975] | |
| Intercept | -3.6401 | 0.885 | -4.112 | 0 | -5.375 | -1.905 |
| Heart Failure with Preserved Ejection Fraction | 0.337 | 0.134 | 2.507 | 0.012 | 0.074 | 0.6 |
As the score increases, the probability of being in NYHA class III at discharge is rising. The coefficient is positive, and the p-value associated is 0.012 which indicates statistical significance.
Figure 18.
The probability of NYHA class III at discharge given by the H2FPEF score.
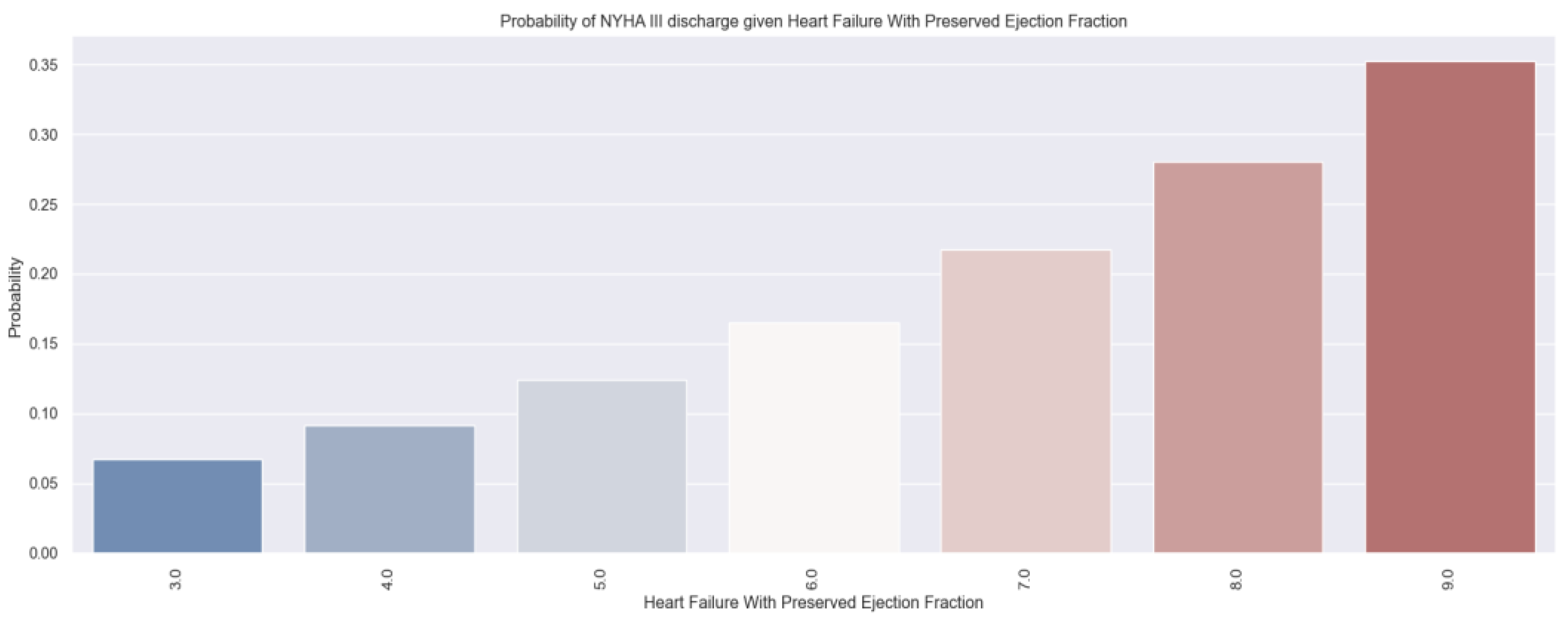
A patient with an H2FPEF score of 7 points has an under 25% probability of being discharged with NYHA class III. Knowing this low probability, we can provide indications for a more frequent follow-up of these patients immediately after discharge. These patients must participate in cardiac recovery programs.
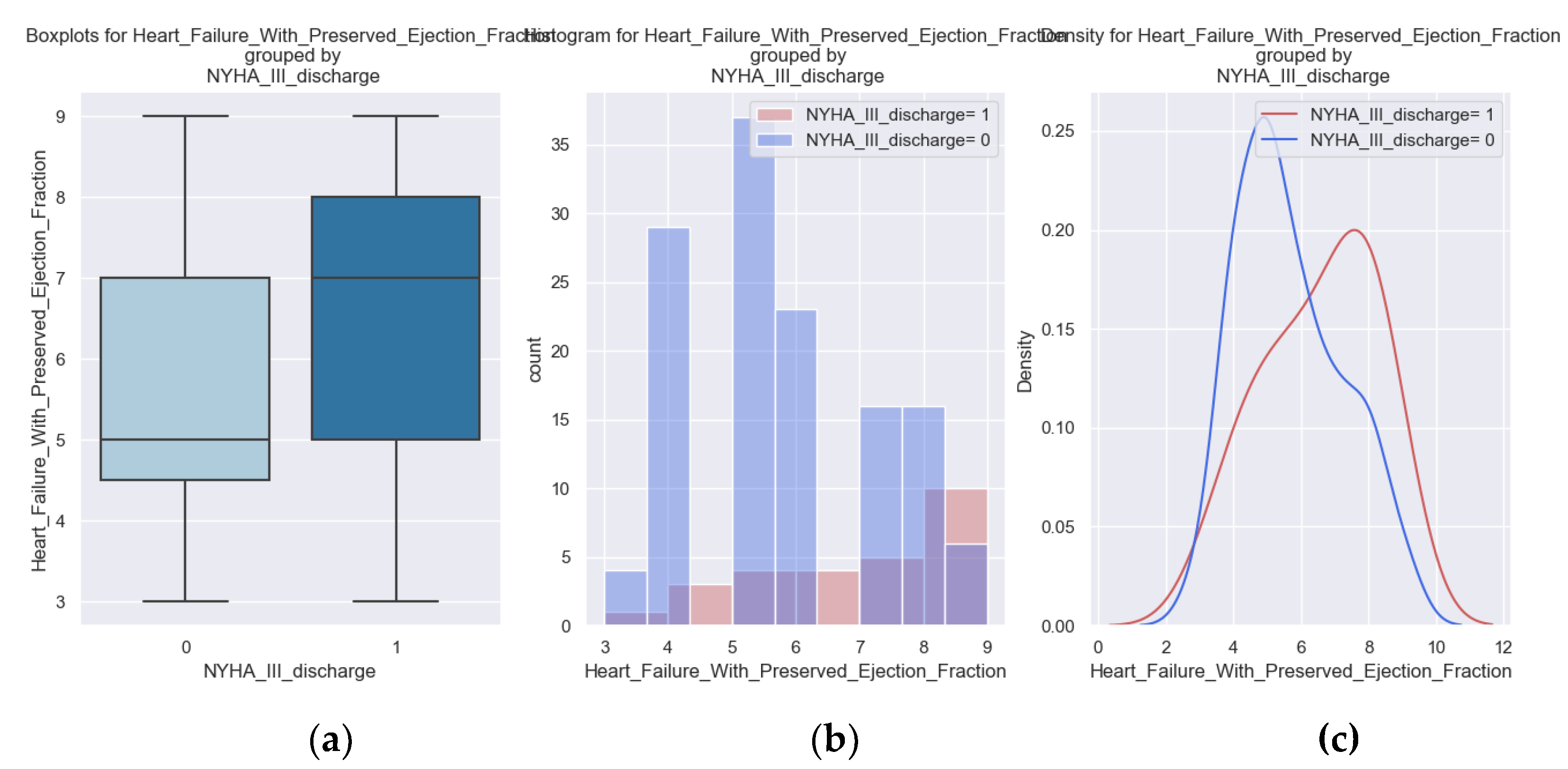
Figure 19.
(a, b, c) Boxplots and diagrams for NYHA class III at discharge and H2FPEF score.
3.7. Comparing Results
Table 12.
Relationship between the H2FPEF score and the quality-of-life factors.
| Dependent variable | r squared | Independent variable | Coef | p value |
| Pitting Edema | 0.0451 | Heart Failure with Preserved Ejection Fraction | 0.3218 | 0.003 |
| Marked Limitation of Physical Activity | 0.1258 | Heart Failure with Preserved Ejection Fraction | 0.6211 | 0 |
| Sadness | 0.04509 | Heart Failure with Preserved Ejection Fraction | 0.337 | 0.012 |
| Ability to Exercise | 0.03916 | Heart Failure with Preserved Ejection Fraction | 0.2988 | 0.005 |
| Palpitations | 0.08172 | Heart Failure with Preserved Ejection Fraction | 0.4387 | 0 |
| NYHA class III at Discharge | 0.05591 | Heart Failure with Preserved Ejection Fraction | 0.3795 | 0.003 |
| NYHA class IV at Admission | 0.06504 | Heart Failure with Preserved Ejection Fraction | 0.4064 | 0.001 |
| Recent Fatigue | 0.06212 | Heart Failure with Preserved Ejection Fraction | -0.4112 | 0.003 |
This table displays the coefficients from the logistic regression along with their associated p-values, providing a comprehensive summary of the relationships outlined previously. All variables exhibit statistical significance. The strongest relationship with the H2FPEF score is observed in marked limitations of physical activity, followed by edema and regular exercise.
4. Discussion
4.1. Limitations of the Study
The limitations of our study are related to the fact that only patients from a single medical center were enrolled and in a relatively small number. This emphasizes the need for further studies to estimate even more accurately the correlation between the H2FPEF score and quality of life. Additional questions can be added to the questionnaire for the assessment of the disease. Here the number of questions was smaller, because the interview was over the phone. In addition, a long-term follow-up of these patients is needed.
Telemedicine helped us to follow these patients, in the context of difficult access to the clinic during the SARS-COV2 virus pandemic, but this has limits, representing an incomplete medical examination.
Despite all these limitations, our study highlights the importance of the H2FPEF score for risk stratification to be able to actively intervene in vulnerable patients.
4.2. Future Directions
Telemedicine needs to develop even more, and this study has shown its importance. It must be accessible to both medical staff and the patient. It is necessary to communicate with the patient, to find out how he/she feels, to teach him/her about his/her disease, to teach him/her how to live to prevent decompensation, to know what the signs of evolution of the disease are and be able to go to the hospital quicker if necessary. Complications and unfavorable evolution of the disease can be prevented or mitigated in this way.
Combining machine learning technologies to understand aggravating factors and assess patient risk with continuous monitoring through telemedicine can enhance lifespan.
5. Conclusions
This study showed the frailty of patients with HFPEF and brought information about their quality of life and about the evolution of the disease (readmissions and mortality). We obtained an important statistical correlation between the H2FPEF score, and all the parameters investigated (simple indicators for the patient).
We can use in the daily clinical practice the results obtained by calculating each patient's H2FPEF score and this way we can estimate how he/she will feel at home immediately after discharge. We will know which patients need more frequent monitoring.
We need to take a step forward for the development of telemedicine so that by detecting early the signs and symptoms of heart failure decompensation, human and financial resources are used more effectively.
Author Contributions
Conceptualization, A.C.T and S.G.; methodology, A.C.T.; software, O.C.; validation, A.C.T., C.L.A and S.G.; formal analysis, A.C.T.; investigation, A.C.T., S.G.; resources, A.C.T., and S.G.; data curation, A.C.T.; writing—original draft, preparation, A.C.T and S.G.; writing—review and editing, A.C.T., C.L.A., and S.G.; visualization, C.J.S., C.L.A., and S.G.; supervision, C.J.S., C.L.A., and S.G. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania (protocol code PO-35-F-03, October 1st, 2021).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in this study.
Data Availability Statement
The data presented in this study is available on request from the corresponding author. The data is not publicly available due to privacy issues.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Metra M, Teerlink JR. Heart failure. The Lancet. 2017;390(10106):1981-1995.
- Owan, T.E.; Redfield, M.M. Epidemiology of Diastolic Heart Failure. Prog. Cardiovasc. Dis. 2005, 47, 320–332. [CrossRef]
- Chan MMY, Lam CSP. How do patients with heart failure with preserved ejection fraction die? European J of Heart Fail. 2013;15(6):604-613.
- Henkel DM, Redfield MM, Weston SA, Gerber Y, Roger VL. Death in Heart Failure: A Community Per-spective. Circ: Heart Failure. 2008;1(2):91-97.
- Borlaug, B.A. The pathophysiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2014, 11, 507–515. [CrossRef]
- Borlaug, B.A.; Paulus, W.J. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur. Hear. J. 2011, 32, 670–679. [CrossRef]
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129-2200.
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Asso-ciation Task Force on Practice Guidelines. Circulation. 2013;128(16):1810-1852.
- Hwang, S.-J.; Melenovsky, V.; Borlaug, B.A. Implications of Coronary Artery Disease in Heart Failure With Preserved Ejection Fraction. Circ. 2014, 63, 2817–2827. [CrossRef]
- Mentz, R.J.; Kelly, J.P.; von Lueder, T.G.; Voors, A.A.; Lam, C.S.; Cowie, M.R.; Kjeldsen, K.; Jankowska, E.A.; Atar, D.; Butler, J.; et al. Noncardiac Comorbidities in Heart Failure With Reduced Versus Preserved Ejection Fraction. Circ. 2014, 64, 2281–2293. [CrossRef]
- Ergatoudes, C.; Schaufelberger, M.; Andersson, B.; Pivodic, A.; Dahlström, U.; Fu, M. Non-cardiac comorbidities and mortality in patients with heart failure with reduced vs. preserved ejection fraction: a study using the Swedish Heart Failure Registry. Clin. Res. Cardiol. 2019, 108, 1025–1033. [CrossRef]
- Mentz, R.J.; Felker, G.M. Noncardiac Comorbidities and Acute Heart Failure Patients. Hear. Fail. Clin. 2013, 9, 359–367. [CrossRef]
- van Deursen, V.M.; Damman, K.; van der Meer, P.; Wijkstra, P.J.; Luijckx, G.-J.; van Beek, A.; van Veldhuisen, D.J.; Voors, A.A. Co-morbidities in heart failure. Hear. Fail. Rev. 2012, 19, 163–172. [CrossRef]
- Van Deursen VM, Urso R, Laroche C, et al. Co-morbidities in patients with heart failure: an analysis of the European Heart Failure Pilot Survey. European J of Heart Fail. 2014;16(1):103-111.
- Kotecha, D.; Lam, C.S.; Van Veldhuisen, D.J.; Van Gelder, I.C.; Voors, A.A.; Rienstra, M. Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation. Circ. 2016, 68, 2217–2228. [CrossRef]
- Tao, Y.; Wang, W.; Zhu, J.; You, T.; Li, Y.; Zhou, X. H2FPEF score predicts 1-year rehospitalisation of patients with heart failure with preserved ejection fraction. Postgrad. Med J. 2020, 97, 164–167. [CrossRef]
- Sueta, D.; Yamamoto, E.; Nishihara, T.; Tokitsu, T.; Fujisue, K.; Oike, F.; Takae, M.; Usuku, H.; Takashio, S.; Arima, Y.; et al. H2FPEF Score as a Prognostic Value in HFpEF Patients. Am. J. Hypertens. 2019, 32, 1082–1090. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



