
Submitted:
02 January 2025
Posted:
03 January 2025
You are already at the latest version
Abstract
Introduction: Differentiated thyroid cancer (DTC) in children and adolescents is a ra-re, but significant malignancy, often presenting at more advanced stages compared to adults, although it is associated with favorable long-term outcomes. This study aimed to identify prognostic factors and perform risk stratification with the goal of identify-ing low-risk patients who would benefit from less radical treatment approach. Meth-ods: This retrospective cohort study included patients aged 21 years and younger with DTC, treated at the Institute for Oncology and Radiology of Serbia between 1980 and 2024. Results: The study analyzed 99 patients (39 children, 60 adolescents) with a me-dian follow-up of 15.6 years (range: 0.6–43.6 years). No significant differences in long-term outcomes were observed between children and adolescents. Multivariate regression analysis identified a total number of more than 10.5 positive lymph nodes and extrathyroidal tumor extension as independent predictors of adverse events and event-free interval (EFI). Based on these prognostic factors, patients were stratified in-to low-, intermediate-, and high-risk groups. Statistically significant differences in EFI were observed among the three groups. Notably, none of the patients in the low-risk group had evidence of disease after treatment. Patients classified as having no evidence of disease after treatment demonstrated significantly better EFI compared to those with evidence of disease. Conclusion: Our findings highlight the importance of meticulous risk stratification in predicting long-term outcomes and might serve as a basis for developing personalized therapeutic strategies. Identifying low-risk patients who may benefit from a less aggressive treatment approach, while ensuring optimal treatment and follow-up for high-risk patients, remains a central objective in the mod-ern management of DTC.
Keywords:
differentiated thyroid cancer
; children
; adolescents
; prognostic factors
; long-term outcomes
; risk stratification
1. Introduction
Thyroid cancer is a rare, yet significant malignancy in children and adolescents, with differentiated thyroid cancer (DTC) being the most prevalent. Worldwide, the annual incidence of DTC in children ranges from 0.5 to 10.0 cases per 100,000 [1]. In prepubertal children, DTC occurs at similar rates in males and females. However, with the onset of puberty, the female-to-male ratio increases to as high as 6:1, making thyroid cancer the second most common malignancy in adolescent girls [2]. The incidence of DTC is rising globally among children, adolescents, and young adults. While improved detection efforts contribute to this trend, they alone cannot fully explain the rise. Potential environmental, dietary, and genetic factors should be explored to better understand the underlying causes [3]. DTC is frequently diagnosed as a radiation-induced second primary malignancy (SPM), particularly in survivors of childhood lymphoma and leukemia who have undergone radiotherapy [4,5].
Thyroid nodules in children warrant thorough evaluation due to their significantly higher malignancy rates compared to adults, ranging from 10% to 50% [6]. Additionally, children with DTC often present with more advanced disease, characterized by a higher incidence of lymph node involvement at diagnosis (up to 90% in children versus 20–50% in adults) and a greater frequency of distant metastases, particularly to the lungs (20–30% in children compared to less than 10% in adults) [7,8,9,10]. Despite pediatric and adolescent patients often presenting with more advanced disease, their prognosis is generally more favorable than that of adults [1]. Achieving a cure while minimizing treatment-associated morbidity has become the primary objective in the modern management of DTC in children and adolescents [7]. In 2015, the American Thyroid Association (ATA) released its first guidelines for the treatment of well-differentiated thyroid cancer in children, which have since become a cornerstone of clinical practice for managing this condition [11]. The most recent guidelines for pediatric DTC were published by the European Thyroid Association (ETA) in 2022 [12]. The development of specific guidelines for the pediatric population underscores the recognition that this disease represents a distinct entity in children, differing significantly from its presentation and management in adults.
This retrospective study aimed to identify prognostic factors of DTC in children and adolescents and perform risk stratification with the goal of identifying low-risk patients who would benefit from less radical treatment approach.
2. Materials and Methods
2.1. Patients and Data
This retrospective cohort study was conducted on patients treated between 1980 and 2024 at Institute for Oncology and Radiology of Serbia (IORS), including those who had a part of their treatment outside IORS. The study included all patients aged 21 years and younger with DTC. Patients with other types of thyroid cancers and with incomplete medical records were excluded from the study. As a part of the preoperative evaluation, all patients underwent neck and abdominal ultrasound, tracheal and chest X-ray examinations, laryngoscopy for vocal cord function evaluation, thyroid function analysis, along with anesthesiologic assessment of perioperative risk. The final treatment strategy was determined by a multidisciplinary team (tumor board for endocrine pathology). Preoperative, operative and follow-up data was extracted from the clinic’s patient database. Any missing information was retrospectively obtained from patient records or via telephone inquiries. Data was validated by two independent researchers. This study received approval from the IORS Ethics Committee.
2.2. Treatment
The treatment plan for patients with DTC at IORS included total (or near total) thyroidectomy combined with central neck dissection. Based on institutional protocols, patients without clinically evident lateral neck metastases underwent sentinel lymph node biopsy using original technique by professor Radan Dzodic, previously published in referent literature [13]. If lateral neck metastases were clinically evident or if the sentinel lymph node biopsy result was positive, modified radical neck dissection of the affected side was conducted. Following surgical treatment, based on the protocols of the time, patients with multifocal or multicentric tumors, locoregionally advanced disease, or radioiodine-avid metastatic disease received radioactive iodine (RAI) treatment. Patients with locally advanced unresectable disease or non-radioiodine-avid metastatic disease received external beam radiotherapy. All patients were prescribed lifelong postoperative TSH-suppressive therapy with L-thyroxine. Patients with negative post-RAI treatment whole-body 131I scan, and those with negative neck ultrasound if they didn’t undergo RAI treatment were classified as having no evidence of disease (NED). Patients with residual disease after treatment were classified as having evidence of disease (ED).
2.3. Follow-Up and Long-Term Outcomes
The follow-up regimen included quarterly appointments during the first-year post-surgery, shifting to 6-months visits from the second through the fifth year, and annual check-ups thereafter. At each visit, patients underwent a comprehensive physical examination with neck ultrasound and laboratory analyses, including TSH, FT4, thyroglobulin, and thyroglobulin antibodies. As there were no deaths, long-term outcomes were evaluated through disease-free interval (DFI), progression-free interval (PFI) and event-free interval (EFI). DFI was calculated only for patients classified as NED after treatment, while PFI only for patients classified as ED. EFI was calculated for the entire study population. DFI and PFI referred to the period from completion of initial treatment to disease relapse and progression, respectively. EFI was defined as the time from initial treatment completion to any adverse event (local or distant disease relapse or disease progression). For all long-term outcomes, the last check-up was used as censoring date for living patients without disease relapse.
2.4. Statistical Analysis
Categorical variables were described using frequencies (percentages), while mean, median, standard deviation (SD) and range were used for numeric variables. Firstly, patients were stratified into two groups: children aged 16 years and younger, and adolescents aged 17 years and older to examine potential differences between these two age groups. Besides age, the entire study population was tested to identify potential prognostic factors for adverse event occurrence. Receiver Operating Characteristic (ROC) curve analysis was conducted to assess the accuracy of tumor size and the total number of positive lymph nodes in predicting the occurrence of adverse events. The area under the ROC curve (AUC ROC) was calculated using DeLong’s method, and the likelihood ratio test was applied to evaluate the AUC ROC. The optimal cutoff values for tumor size and the total number of positive lymph nodes were determined as the points with maximum sensitivity and specificity. Patients were further categorized based on these cutoff values, provided the AUC ROC exceeded 70% [14]. The predictive value of all variables significantly associated with adverse events was assessed by univariate and a multivariate logistic regression model. Results were given as odds ratio with 95% confidence interval. Survival analysis methods were used to analyze long-term treatment outcomes (Kaplan-Meier method for cumulative probability curves; median with 95% confidence interval-CI; log-rank test). Variables identified as significant by Survival analysis were further evaluated using univariate and multivariate Cox proportional hazards regression models (Hazard ratio-HR with 95% CI; Wald and Likelihood ratio tests). Significant prognostic factors were subsequently utilized to stratify the study population into three risk categories: low-risk, intermediate-risk, and high-risk. P-value of less than 0.05 was deemed statistically significant. Statistical analyses were performed using R software (version 4.3.1 (2023-06-16 ucrt) -- “Beagle Scouts”; Copyright (C) 2023 The R Foundation for Statistical Computing; Platform: x86_64-w64-mingw32/x64 (64-bit)) (available at: www.r-project.org; downloaded: August 21, 2023).
3. Results
3.1. Patients and Treatment
A total of 99 patients met the inclusion criteria for this study, with a median follow-up of 15.6 years (range: 0.6-43.6 years). The demographical and treatment characteristics of the study cohort are summarized in Table 1. Of these, 39 (39.39%) were children aged 16 years or younger, while the remaining 60 (60.61%) were adolescents. Female patients predominated in both groups. Four patients had a history of prior radiation therapy for cancer treatment: three received whole-body irradiation for acute lymphoblastic leukemia, and one underwent neck irradiation for Hodgkin lymphoma. At diagnosis, 85 (85.86%) patients presented with clinical signs or symptoms, with thyroid nodules, neck lymphadenopathy, or both observed in 79.8% of cases. Remaining patients were asymptomatic at presentation.
Fine-needle aspiration biopsy (FNAB) was performed in 23 (23.23%) patients, while others were operated due to suspicious clinical findings. Nineteen (19.19%) patients presented with cervical lymphadenopathy and were diagnosed following surgical removal of pathological cervical lymph node. Eight (8.08%) patients had distant metastatic disease at the time of diagnosis, all with lung involvement. All patients underwent surgical treatment. Among them, 75 (75.75%) received radioactive iodine (RAI) treatment, and four required postoperative external beam radiotherapy.
3.2. Postoperative Staging, Pathohistological Characteristics and Long-Term Outcomes
As shown in Table 2, the most common histological type in the cohort was papillary thyroid cancer (PTC), identified in 95 (95.96%) patients. Children had a slightly larger mean tumor size compared to adolescents, though this difference was not statistically significant. No significant difference was noted in the number of positive central and lateral lymph nodes between the two groups. On the other hand, in the subgroup of patients that had at least one positive lymph node, children had a significantly higher number of positive lateral lymph nodes compared to adolescents with 9.38 (SD 6.70) vs. 5.95 (SD 5.76) positive lymph nodes; p = 0.02. Multifocal tumors, capsular invasion, and extrathyroidal extension were more frequently observed in children than in adolescents. A total of 91 (91.91%) patients were classified as NED after completing treatment, and there was no significant difference between children and adolescents in the proportion of NED and ED patients.
Long-term treatment outcomes are summarized in Table 3. In total 24 (24.24%) patients had an adverse event (disease relapse or disease progression), with no significant difference in incidence between children and adolescents. ED patients experienced adverse events in 87.5% of the cases compared to 18.68% in NED patients. The median DFI and EFI were not reached (Figures 1A and 1C), while the median PFI was 5 years (95%CI >1.8 years; Figure 1B). The DFI, PFI, and EFI for the entire cohort are depicted in Figure 1D. No significant differences in DFI, PFI, or EFI were observed between the two age groups. No deaths were recorded during the entire follow-up period.
3.3. Potential Prognostic Factors for Long-Term Outcomes
The ROC curve analysis (Figure 2) identified a tumor size of 30.5mm as the most reliable cutoff for predicting adverse events, with a sensitivity of 54.17% (95% CI: 33.33–75.00%), a specificity of 85.33% (95% CI: 76.00–92.00%), and an AUC of 71.14% (95% CI: 58.83–83.44%; p<0.01). Similarly, a total number of positive lymph nodes of 10.5 emerged as the most reliable predictor of adverse event occurrence, with a sensitivity of 83.33% (95% CI: 66.67–95.83%), a specificity of 77.33% (95% CI: 68.00–86.67%), and an AUC of 85.86% (95% CI: 78.21–93.51%; p <0.01).
Tumor size greater than 30.5 mm, presence of distant metastases at the diagnosis, capsular invasion, a total number of positive lymph nodes exceeding 10.5, and extrathyroidal tumor extension were identified as potential prognostic factors for the occurrence of adverse events and EFI. The results of the analysis are presented in Table 4.
3.4. Univariate and Multivariate Regression Analysis and Risk Stratification
The results of univariate analysis (logistic regression in Table 5; Cox proportional hazards regression in Table 6) confirmed the same prognostic factors for the adverse events and EFI, respectively. But multivariate analysis (logistic regression in Table 5; Cox proportional hazards regression in Table 6) confirmed only total number of positive lymph nodes greater than 10.5, and extrathyroidal tumor extension as significant independent predictors of adverse events and EFI.
Patients were further stratified into risk categories based on the prognostic factors identified through regression analysis:
- Low-risk (LR) group: patients with a total number of positive lymph nodes fewer than 10.5 and without extrathyroidal extension,
- Intermediate-risk (IR) group: patients with either a total number of positive lymph nodes exceeding 10.5 or extrathyroidal tumor extension,
- High-risk (HR) group: patients with both total number of positive lymph nodes exceeding 10.5 and extrathyroidal tumor extension
The EFI for all three risk groups is illustrated in Figure 3, with statistically significant difference between all three groups (log rank test: p<0.01). The median EFI for the LR and IR groups was not reached, while the median EFI for the HR group was 2.4 years (95% CI: >1.6 years). The ten-year event-free rates were 96% (95% CI: 90.8–100%) for LR patients, 77.1% (95% CI: 61.2–97.2%) for IR patients, and 38.3% (95% CI: 22.5–65.5%) for HR patients.
4. Discussion
For a long time, the radical treatment approach for pediatric and adolescent DTC patients was predominantly based on evidence from studies conducted in adult populations. Given the excellent outcomes and low mortality rates in younger patients, the focus has gradually shifted from a radical approach to an individually tailored treatment strategy. Identifying patients at increased risk of disease relapse or progression is a critical step in the treatment process. Numerous studies have sought to identify potential risk factors, often producing conflicting results, while others have focused on refining treatment approaches through risk stratification systems.
In our study, the proportion of female patients was significantly higher than that of male patients. The children group comprised 74.36% females, while the adolescent group included 76.67% females, which is consistent with other published studies reporting female proportions ranging from 65.7% to 85.7% [15,16,17,18,19]. Some studies described the sex difference increasing with age, especially after puberty [3,16,17,20]. A possible explanation for why the same difference was not observed in our study could lie in the cut-off age of 16 years, which included both pre-pubertal and post-pubertal patients within the children group. Consequently, this age grouping may have made the differences within the children’s group more pronounced.
The most common histological type was PTC accounting for 95.96% of all DTC cases with no significant difference between children and adolescents. Similar results were published by other teams for PTC prevalence, ranging from 84-93.1% [1,7,17]. It is worth mentioning that aggressive subtypes of PTC are present in 15-37% of pediatric patients [21]. Nevertheless, pediatric patients with aggressive histological subtypes do not experience worse event-free survival in contrast to adults [19]. PTC subtype was not routinely reported in our institution especially in patients treated before 2015. DTC in children tends to present as a more advanced disease, usually with extensive lymph node involvement and distant metastases [8,9]. Burgard et al. reported prepubertal patients presenting with higher T and M stages, compared to pubertal/postpubertal patients [10]. Other studies reported younger age as being associated with larger tumor size at diagnosis [1]. No significant difference was observed in TNM stage between children and adolescents in our study, with mean tumor size being slightly larger in children, but without statistical significance. No difference in the number of positive central and lateral neck lymph nodes between children and adolescents was observed in our study. Interestingly, among patients with at least one positive lateral lymph node, the number of positive lateral lymph nodes was higher in children, consistent with the more aggressive behavior of DTC observed in pediatric patients. Moreover, children were more likely to have multifocal tumors, capsular invasion and extrathyroidal extension. Ren et al. reported no difference in multifocality and extrathyroidal extension between DTC patients aged 18 and younger and those aged 19-21. Extrathyroidal extension was more common in children than in young adults (21-44 years of age) in the same study [22]. Several possible explanations for more advanced disease in young patients have been proposed, including larger tumor size relative to thyroid gland in younger patients (and subsequent earlier extrathyroidal spread), difference in metabolic and genetic status of DTC in children, and delayed diagnosis [16]. It is noteworthy that the ATA guidelines apply the same TNM staging system for pediatric patients as for adults, despite the significant differences in thyroid gland size between these populations. In children, the size of the thyroid gland changes with growth and development, with the most substantial increase in size occurring between the ages of 11 and 15 [23]. This raises the question of possible individualized staging, considering tumor to thyroid gland size ratio. Despite initially more advanced disease, pediatric and adolescent patients usually face better prognosis compared to adults [1]. Moreover, our study showed no difference in disease outcomes in children and adolescents, both in the number of adverse events and in the time-to-event analysis. The adverse event rate of 24.24% observed in our study was comparable to findings reported in other studies [24,25].
Risk factors in DTC are usually divided in two groups: patient- (age and sex) and tumor-related (histological type, size, multifocality, extrathyroidal extension, lymph node and distant metastases). Our study did not identify any patient-related risk factors, such as age or sex, as being associated with adverse event occurrence or EFI. Similar results have been published by other teams [26,27]. Given the established association of tumor size and lymph node metastases with long-term outcomes [8,25,28], ROC curve analysis was utilized to determine optimal cutoff values for tumor size and the total number of positive lymph nodes. In multivariate logistic regression, the independent predictors of adverse event occurrence were a total number of positive lymph nodes exceeding 10.5 and extrathyroidal tumor extension. The presence of metastatic disease at initial diagnosis showed a strong trend toward predicting adverse events, but it was not statistically significant with OR: 9.0 (95%CI: 0.9–93). This lack of significance is likely attributable to the small sample size. Regarding time-to-event analysis, the strongest independent predictor of shorter EFI in the multivariate Cox regression analysis was a total number of positive lymph nodes greater than 10.5. Extrathyroidal tumor extension also emerged as a significant predictor of EFI, consistent with its role in predicting adverse event occurrence.
Considering the large number of proposed predictors of long-term outcomes and the often-conflicting results across studies, a more comprehensive approach was essential for accurate risk evaluation. Over time, risk stratification emerged as one of the key aspects of DTC treatment. Several risk stratification systems have been proposed, with TNM/AJCC staging system, ATA risk stratification in children and adolescents with DTC and Dynamic risk stratification (DRS) being most widely used. Risk assessment may encompass various outcomes, including the risk of relapse, progression, or even mortality. Although the TNM/AJCC is the most widely used staging system, its risk stratification capability has been debated. Primarily centered on evaluating mortality risk, this system exhibits limited discriminatory power in patient populations where overall survival approaches 100%. In this system, all patients under the age of 55 are classified as either stage I or stage II based exclusively on their M status: M0 corresponds to stage I, while M1 corresponds to stage II [29]. Low discriminatory power, combined with the exclusion of other well-established mortality predictors, has significantly constrained the applicability of this system in risk assessment. On the other hand, ATA risk stratification for children and adolescents focuses on identifying patients at risk of persistent cervical disease and/or distant metastases following the completion of initial treatment. This approach enables a tailored follow-up strategy based on the patient’s assigned risk level (low, intermediate, or high risk). However, despite accounting for histopathological data, a significant limitation of this system is its failure to incorporate the response to therapy. Moreover, the specific number of positive lymph nodes used for patient stratification was not explicitly defined. Instead, stratification was based on the classifications of minimal and extensive N1a and N1b disease [1,11]. Tuttle et al. emphasized the importance of incorporating therapy response variables into risk stratification to enable dynamic risk assessment [30]. Dynamic risk stratification recognizes that a patient’s risk may evolve over time. Within this system, patients are categorized into four risk groups: excellent response, biochemical incomplete response, structural incomplete response, and indeterminate response [31]. While numerous studies have validated this system’s ability to predict disease outcomes in DTC patients, only a few have specifically examined its applicability in pediatric and adolescent populations [27,32,33].
Given that our study encompassed a patient population treated over a span of 44 years, during which various diagnostic tools and laboratory assays were used for disease evaluation, the full application of the DRS system was not feasible. Instead, the patients were stratified in three risk groups according to risk factors detected in regression analysis. The current ATA guidelines for pediatric patients recommend total thyroidectomy for all patients, regardless of their risk level [11]. In contrast, the ATA guidelines for adult patients suggest lobectomy as a treatment option for those in the LR category [34]. Some studies have proposed that lobectomy may also be an adequate treatment option for LR pediatric patients [24,25,35]. Massimino et al. reported that treatment outcomes were comparable between radical and conservative approaches, while complications were significantly more frequent with the radical surgical approach [36]. Among the 52 patients in the LR group in our study, 25 did not undergo RAI treatment, while 27 did, with no significant difference in the number of adverse events and EFI between these two subgroups. The excellent treatment outcomes observed in our study, with a 10-year event-free rate of 96% in LR patients, highlight the potential for adopting a less radical treatment approach. This suggests that strategies such as lobectomy and the omission of RAI treatment could be viable options within a less aggressive treatment framework. Notably, among the eight patients classified as ED after treatment, six were in the HR group, while only two were categorized as IR. In the LR group, all patients were NED following treatment. Furthermore, time-to-event analysis revealed that patients classified as ED after treatment experienced significantly worse outcomes compared to NED patients (Figure 1D).
5. Conclusions
Our study confirmed excellent long-term outcomes and no significant differences between pediatric and adolescent populations with differentiated thyroid cancer. A total number of positive lymph nodes exceeding 10.5 and extrathyroidal tumor extension were identified as independent predictors of adverse events and EFI. Patients classified as low risk, based on identified prognostic factors, demonstrated significantly better outcomes, supporting the potential for adopting a less radical treatment strategy in this group. Conversely, patients with evident disease after treatment experienced significantly worse EFI compared to NED patients, underscoring the importance of more stringent follow-up in these cases. Moving forward, the primary goal remains the implementation of an individualized treatment approach, focusing on minimizing aggressive interventions in low-risk patients, while ensuring rigorous follow-up for those at high risk.
Author Contributions
Conceptualization: M.B., J.R. and D.G.; methodology: M.B. and J.R.; software: D.G.; validation: N.S. (Nada Santrac), M.G.; formal analysis: D.G.; investigation: N.J. (Nikola Jeftic), J.R. and S.P.; resources: I.M., and M.B.; data curation: N.J. (Nikola Jeftic), N.S. (Nevena Savkovic), J.R., S.P., and A.C. writing—original draft preparation: N.J. (Nikola Jeftic), J.R., and S.P.; writing—review and editing, N.S. (Nada Santrac), M.G., N.S. (Nevena Savkovic), M.Z., N.J. (Neven Jokic), A.C., M.S., and A.J..; visualization: D.G. and J.R.; supervision: M.B. and I.M.; project administration: M.B., and N.S. (Nada Santrac).; funding acquisition: M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Institute for Oncology and Radiology of Serbia (protocol code 01-1/2024/4012; December 20th, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
To protect the privacy and confidentiality of patients in this study, clinical data have not been made publicly available in a repository or in the supplementary material of the article; however, they will be made available upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zanella, A.B.; Scheffel, R.S.; Weinert, L.; Dora, J.M.; Maia, A.L. New insights into the management of differentiated thyroid carcinoma in children and adolescents (Review). Int. J. Oncol. 2021, 58, 1–11. [Google Scholar] [CrossRef]
- Gupta, A.; Ly, S.; Castroneves, L.A.; Frates, M.C.; Benson, C.B.; Feldman, H.A.; Wassner, A.J.; Smith, J.R.; Marqusee, E.; Alexander, E.K.; et al. A Standardized Assessment of Thyroid Nodules in Children Confirms Higher Cancer Prevalence Than in Adults. J. Clin. Endocrinol. Metab. 2013, 98, 3238–3245. [Google Scholar] [CrossRef] [PubMed]
- Vergamini, L.B.; Frazier, A.L.; Abrantes, F.L.; Ribeiro, K.B.; Rodriguez-Galindo, C. Increase in the Incidence of Differentiated Thyroid Carcinoma in Children, Adolescents, and Young Adults: A Population-Based Study. J. Pediatr. 2014, 164, 1481–1485. [Google Scholar] [CrossRef] [PubMed]
- Black, P.; Straaten, A.; Gutjahr, P. Secondary thyroid carcinoma after treatment for childhood cancer. Med Pediatr. Oncol. 1998, 31, 91–95. [Google Scholar] [CrossRef]
- Tonorezos, E.S.; Barnea, D.; Moskowitz, C.S.; Chou, J.F.; Sklar, C.A.; Elkin, E.B.; Wong, R.J.; Li, D.; Tuttle, R.M.; Korenstein, D.; et al. Screening for thyroid cancer in survivors of childhood and young adult cancer treated with neck radiation. J. Cancer Surviv. 2016, 11, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Moleti, M.; Aversa, T.; Crisafulli, S.; Trifirò, G.; Corica, D.; Pepe, G.; Cannavò, L.; Di Mauro, M.; Paola, G.; Fontana, A.; et al. Global incidence and prevalence of differentiated thyroid cancer in childhood: systematic review and meta-analysis. Front. Endocrinol. 2023, 14, 1270518. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Sharabiani, M.; Tumino, D.; Wadsley, J.; Gill, V.; Gerrard, G.; Sindhu, R.; Gaze, M.; Moss, L.; Newbold, K. Differentiated Thyroid Cancer in Children: A UK Multicentre Review and Review of the Literature. Clin. Oncol. 2019, 31, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Dinauer, C.A.W.; Tuttle, M.; Robie, D.K.; McClellan, D.R.; Svec, R.L.; Adair, C.; Francis, G.L. Clinical features associated with metastasis and recurrence of differentiated thyroid cancer in children, adolescents and young adults. Clin. Endocrinol. 1998, 49, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Chaukar, D.A.; Rangarajan, V.; Nair, N.; Dcruz, A.K.; Nadkarni, M.S.; Pai, P.S.; Mistry, R.C. Pediatric thyroid cancer. J. Surg. Oncol. 2005, 92, 130–133. [Google Scholar] [CrossRef]
- Burgard, C.; Zacherl, M.J.; Todica, A.; Hornung, J.; Grawe, F.; Pekrul, I.; Zimmermann, P.; Schmid-Tannwald, C.; Ladurner, R.; Krenz, D.; et al. Primary presentation and clinical course of pediatric and adolescent patients with differentiated thyroid carcinoma after radioiodine therapy. Front. Oncol. 2023, 13, 1237472. [Google Scholar] [CrossRef]
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid cancer: The American Thyroid Association guidelines task force on pediatric thyroid cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [PubMed]
- A Lebbink, C.; Links, T.P.; Czarniecka, A.; Dias, R.P.; Elisei, R.; Izatt, L.; Krude, H.; Lorenz, K.; Luster, M.; Newbold, K.; et al. 2022 European Thyroid Association Guidelines for the management of pediatric thyroid nodules and differentiated thyroid carcinoma. Eur. Thyroid. J. 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Dzodic, R. Sentinel Lymph Node Biopsy May Be Used to Support the Decision to Perform Modified Radical Neck Dissection in Differentiated Thyroid Carcinoma. World J. Surg. 2006, 30, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Polo, T.C.F.; Miot, H.A. Aplicações da curva ROC em estudos clínicos e experimentais. J. Vasc. Bras. 2020, 19. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, N.L.; Bhattacharyya, N. Population-Based Outcomes for Pediatric Thyroid Carcinoma. Laryngoscope 2005, 115, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Lazar, L.; Lebenthal, Y.; Steinmetz, A.; Yackobovitch-Gavan, M.; Phillip, M. Differentiated Thyroid Carcinoma in Pediatric Patients: Comparison of Presentation and Course between Pre-pubertal Children and Adolescents. J. Pediatr. 2009, 154, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, S.; Gao, Z.; Tao, Y.; Wang, X.; Cheng, J. Children and adolescents with differentiated thyroid cancer from 1998 to 2018: a retrospective analysis. J. Pediatr. Endocrinol. Metab. 2024. [Google Scholar] [CrossRef] [PubMed]
- Puga, F.M.; Correia, L.; Vieira, I.; Caetano, J.S.; Cardoso, R.; Dinis, I.; Mirante, A. Differentiated Thyroid Cancer in Children and Adolescents: 12-year Experience in a Single Center. J. Clin. Res. Pediatr. Endocrinol. 2024, 16, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Balachandar, S.; La Quaglia, M.; Tuttle, R.M.; Heller, G.; Ghossein, R.A.; Sklar, C.A. Pediatric Differentiated Thyroid Carcinoma of Follicular Cell Origin: Prognostic Significance of Histologic Subtypes. Thyroid® 2016, 26, 219–226. [Google Scholar] [CrossRef]
- Mao, X.-C.; Yu, W.-Q.; Shang, J.-B.; Wang, K.-J. Clinical characteristics and treatment of thyroid cancer in children and adolescents: a retrospective analysis of 83 patients. J. Zhejiang Univ. B 2017, 18, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Paulson, V.A.; Rudzinski, E.R.; Hawkins, D.S. Thyroid Cancer in the Pediatric Population. Genes 2019, 10, 723. [Google Scholar] [CrossRef]
- Ren, P.-Y.; Liu, J.; Xue, S.; Chen, G. Pediatric differentiated thyroid carcinoma: The clinicopathological features and the coexistence of Hashimoto's thyroiditis. Asian J. Surg. 2019, 42, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Taş, F.; Bulut, S.; Eğilmez, H.; Öztoprak, I.; Ergür, A.T.; Candann, F. Normal thyroid volume by ultrasonography in healthy children. Ann. Trop. Paediatr. 2002, 22, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Sugino, K.; Nagahama, M.; Kitagawa, W.; Ohkuwa, K.; Uruno, T.; Matsuzu, K.; Suzuki, A.; Tomoda, C.; Hames, K.Y.; Akaishi, J.; et al. Risk Stratification of Pediatric Patients with Differentiated Thyroid Cancer: Is Total Thyroidectomy Necessary for Patients at Any Risk? Thyroid® 2020, 30, 548–556. [Google Scholar] [CrossRef]
- Wada, N.; Sugino, K.; Mimura, T.; Nagahama, M.; Kitagawa, W.; Shibuya, H.; Ohkuwa, K.; Nakayama, H.; Hirakawa, S.; Yukawa, N.; et al. Treatment Strategy of Papillary Thyroid Carcinoma in Children and Adolescents: Clinical Significance of the Initial Nodal Manifestation. Ann. Surg. Oncol. 2009, 16, 3442–3449. [Google Scholar] [CrossRef] [PubMed]
- Vaisman, F.; Bulzico, D.A.; Pessoa, C.H.C.N.; Bordallo, M.A.N.; De Mendonça, U.B.T.; Dias, F.L.; Coeli, C.M.; Corbo, R.; Vaisman, M. Prognostic factors of a good response to initial therapy in children and adolescents with differentiated thyroid cancer. Clinics 2011, 66, 281–286. [Google Scholar] [CrossRef]
- Zanella, A.B.; Scheffel, R.S.; Nava, C.F.; Golbert, L.; Meyer, E.L.d.S.; Punales, M.; Gonçalves, I.; Dora, J.M.; Maia, A.L. Dynamic Risk Stratification in the Follow-Up of Children and Adolescents with Differentiated Thyroid Cancer. Thyroid® 2018, 28, 1285–1292. [Google Scholar] [CrossRef]
- Lee, Y.-M.; Lo, C.-Y.; Lam, K.-Y.; Wan, K.-Y.; Tam, P.K. Well-differentiated thyroid carcinoma in Hong Kong Chinese patients under 21 years of age: a 35-year experience. J. Am. Coll. Surg. 2002, 194, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Tala, H.; Shah, J.; Leboeuf, R.; Ghossein, R.; Gonen, M.; Brokhin, M.; Omry, G.; Fagin, J.A.; Shaha, A. Estimating Risk of Recurrence in Differentiated Thyroid Cancer After Total Thyroidectomy and Radioactive Iodine Remnant Ablation: Using Response to Therapy Variables to Modify the Initial Risk Estimates Predicted by the New American Thyroid Association Staging System. Thyroid® 2010, 20, 1341–1349. [Google Scholar] [CrossRef]
- Momesso, D.P.; Tuttle, R.M. Update on Differentiated Thyroid Cancer Staging. Endocrinol. Metab. Clin. North Am. 2014, 43, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Lazar, L.; Lebenthal, Y.; Segal, K.; Steinmetz, A.; Strenov, Y.; Cohen, M.; Yaniv, I.; Yackobovitch-Gavan, M.; Phillip, M. Pediatric Thyroid Cancer: Postoperative Classifications and Response to Initial Therapy as Prognostic Factors. J. Clin. Endocrinol. Metab. 2016, 101, 1970–1979. [Google Scholar] [CrossRef]
- Sung, T.Y.; Jeon, M.J.; Lee, Y.H.; Lee, Y.-M.; Kwon, H.; Yoon, J.H.; Chung, K.-W.; Kim, W.G.; Song, D.E.; Hong, S.J. Initial and Dynamic Risk Stratification of Pediatric Patients with Differentiated Thyroid Cancer. J. Clin. Endocrinol. Metab. 2016, 102, 793–800. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Newman, K.D.; Black, T.; Heller, G.; Azizkhan, R.G.; Holcomb, G.W.; Sklar, C.; Vlamis, V.; Haase, G.M.; La Quaglia, M.P. Differentiated Thyroid Cancer: Determinants of Disease Progression in Patients <21 Years of Age at Diagnosis. Ann. Surg. 1998, 227, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Massimino, M.; Collini, P.; Leite, S.F.; Spreafico, F.; Zucchini, N.; Ferrari, A.; Mattavelli, F.; Seregni, E.; Castellani, M.R.; Cantù, G.; et al. Conservative surgical approach for thyroid and lymph-node involvement in papillary thyroid carcinoma of childhood and adolescence. Pediatr. Blood Cancer 2005, 46, 307–313. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Disease outcomes in the study population: (A) DFI for NED patients; (B) PFI for ED patients; EFI for all patients; (D) DFI, PFI and EFI for all patients. Legend: NED-no evidence of disease; ED-evidence of disease; pts-patients; DFI-disease-free interval; PFI-progression-free interval; EFI-event-free interval.
Figure 1.
Disease outcomes in the study population: (A) DFI for NED patients; (B) PFI for ED patients; EFI for all patients; (D) DFI, PFI and EFI for all patients. Legend: NED-no evidence of disease; ED-evidence of disease; pts-patients; DFI-disease-free interval; PFI-progression-free interval; EFI-event-free interval.
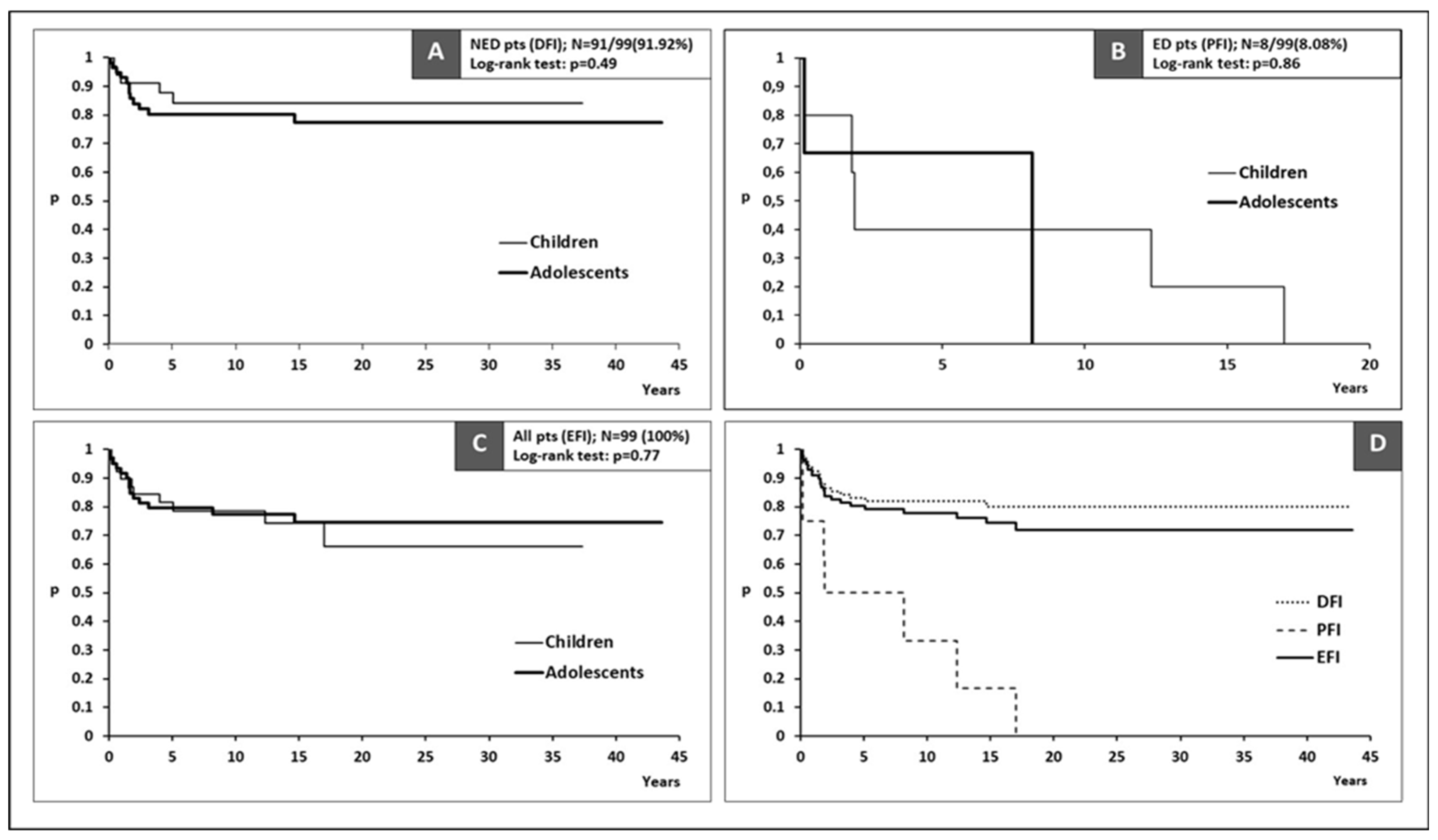
Figure 2.
ROC curve analysis cut-off value for predicting adverse event for (A) tumor size and (B) total number of positive lymph nodes.
Figure 2.
ROC curve analysis cut-off value for predicting adverse event for (A) tumor size and (B) total number of positive lymph nodes.
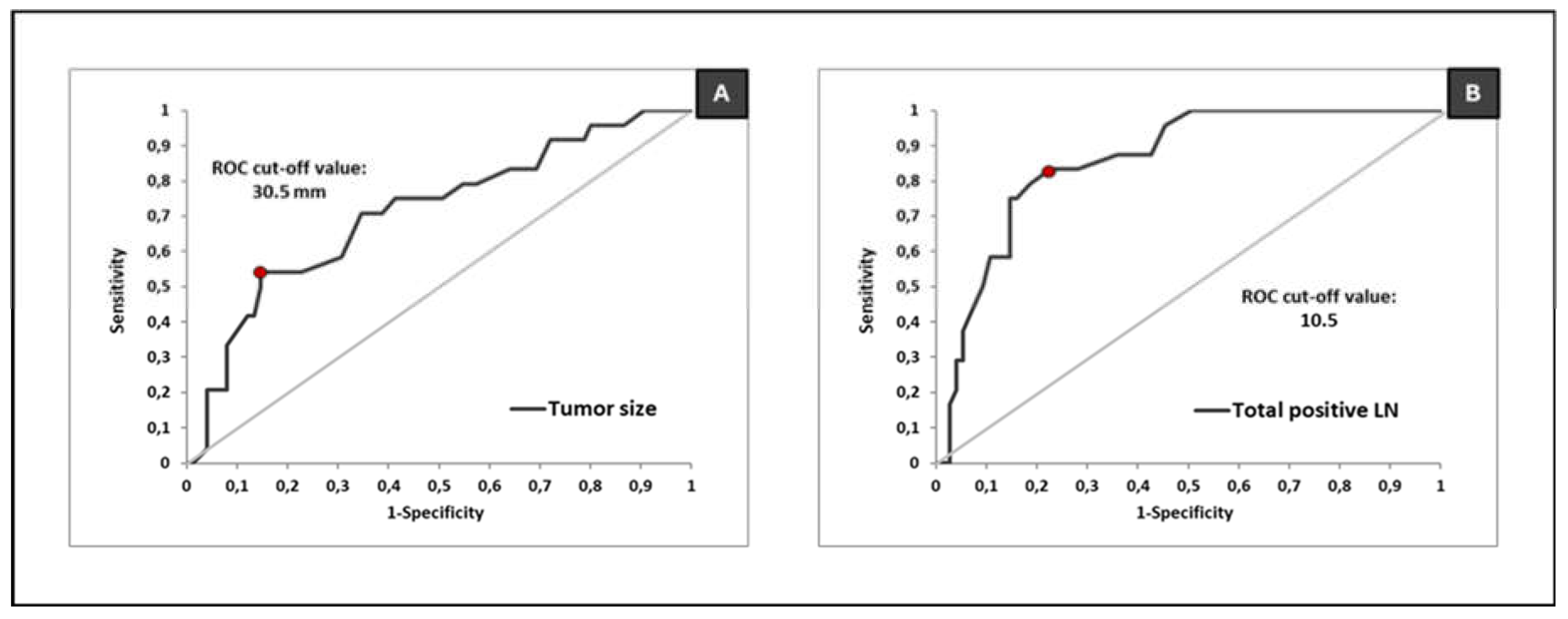
Figure 3.
Event-free interval after risk stratification according to regression analysis. Legend: LR-low-risk group; IR-intermediate-risk group; HR-high-risk group.
Figure 3.
Event-free interval after risk stratification according to regression analysis. Legend: LR-low-risk group; IR-intermediate-risk group; HR-high-risk group.
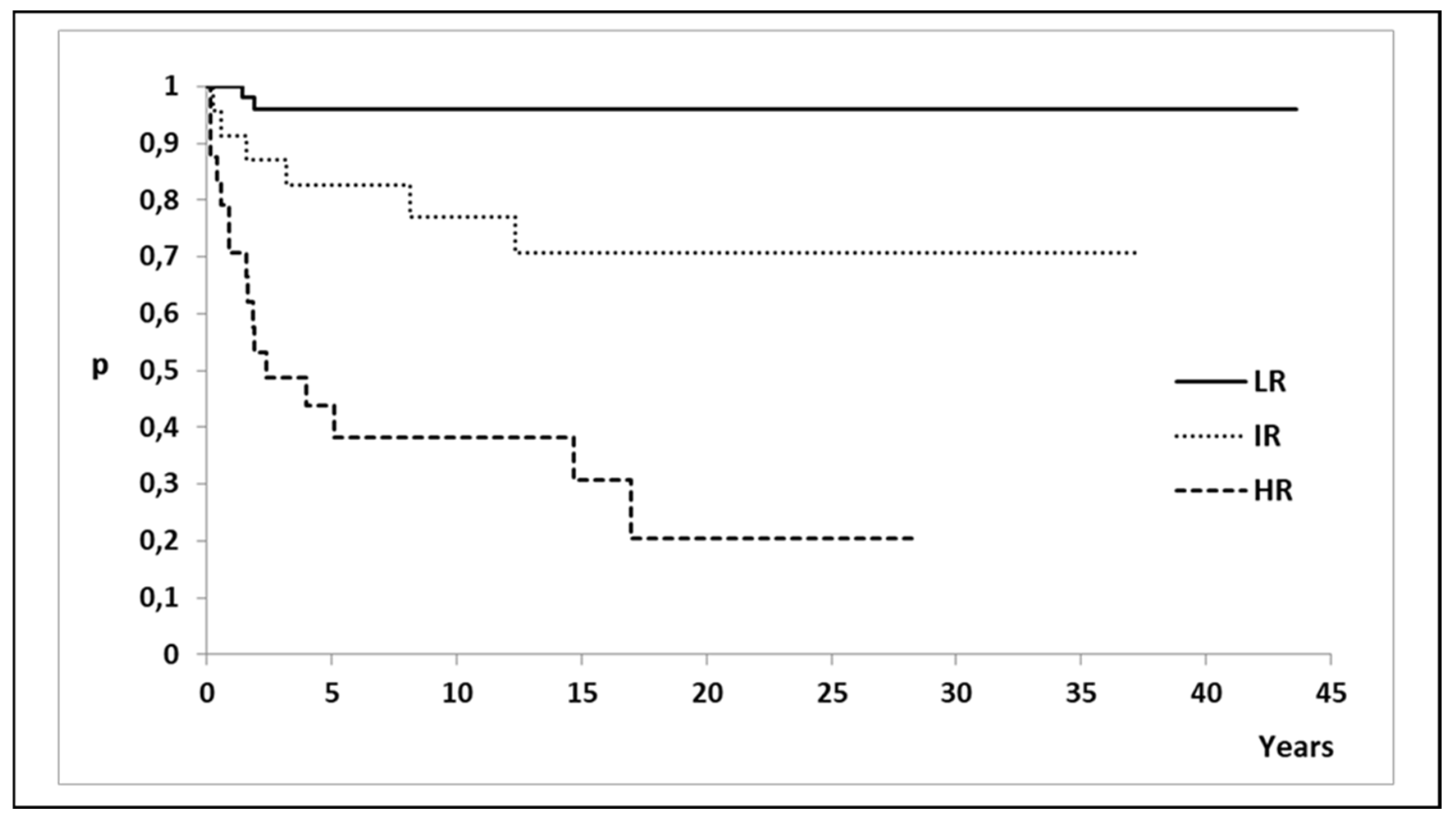

Table 1.
Demographical and treatment characteristics of the study population.
| Characteristics | Total | Children (≤16) | Adolescents (>16) | Pearson χ2 test |
| Follow-up (years) | ||||
| Mean (SD) | 16.2 (10.3) | 15.8 (10.7) | 16.5 (10.1) | ns# |
| Median (Range) | 15.6 (0.6-43.6) | 14.8 (0.7-39.9) | 16.3 (0.6-43.6) | |
| Patient characteristics | ||||
| Sex | ||||
| Female | 75 (75.76%) | 29 (74.36%) | 46 (76.67%) | ns |
| Male | 24 (24.24%) | 10 (25.64%) | 14 (23.33%) | |
| Age (years) | ||||
| Mean (SD) | 16.66 (3.41) | 13.08 (2.14) | 18.98 (1.61) | - |
| Median (Range) | 17 (7-21) | 13 (7-16) | 20 (17-21) | |
| Preoperative RT* | ||||
| Yes | 4 (4.04%) | 3 (7.69%) | 1 (1.67) | ns♦ |
| No | 95 (95.96%) | 36 (92.31%) | 59 (98.33%) | |
| Surgery | ||||
| Thyroid | ||||
| TT | 96 (96.97%) | 39 (100%) | 57 (95%) | ns♦ |
| Near TT | 3 (3.03%) | 0 (0%) | 3 (5%) | |
| CND | ||||
| Yes | 94 (94.95%) | 37 (94,87%) | 57 (95%) | ns♦ |
| No | 5 (5.05%) | 2 (5.13%) | 3 (5%) | |
| SLNB | ||||
| Yes | 50 (50.51%) | 18 (46.15%) | 32 (53.33%) | ns |
| No | 49 (49.49%) | 21 (53.85%) | 28 (46.67%) | |
| MRND | ||||
| Unilateral | 50 (50.51%) | 18 (46.15%) | 32 (53.33%) | ns |
| Bilateral | 18 (18.18%) | 11 (28.21%) | 7 (11.67%) | |
| No | 31 (31.31%) | 10 (25.64%) | 21 (35%) | |
| RAI treatment | ||||
| Yes | 74 (74.75%) | 32 (82.05%) | 42 (70%) | ns |
| No | 25 (25.25%) | 7 (17.95%) | 18 (30%) | |
| Postoperative external beam RT | ||||
| Yes | 4 (4.04%) | 1 (2.56%) | 3 (5%) | ns♦ |
| No | 95 (95.96%) | 38 (97.44%) | 57 (95%) | |
| Total | 99 (100%) | 39 (100%) | 60 (100%) | |
SD-standard deviation; RT-radiotherapy; NL-neck lymphadenopathy; TT-total thyroidectomy; CND-central neck dissection; SLNB-sentinel lymph node biopsy; MRND-modified radical neck dissection; RAI-radioactive iodine; ns-no statistical significance; #Wilcoxon rank sum test; ♦Fischer exact test; *for other primary malignancy.
Table 2.
Pathohistological characteristics and TNM staging of the study population.
| Characteristics | Total | Children (≤16) | Adolescents (>16) | Pearson χ2 test |
| Thyroid cancer type | ||||
| PTC | 95 (95.96%) | 37 (94.87%) | 58 (96.67%) | ns♦ |
| FTC | 3 (3.03%) | 2 (5.13%) | 1 (1.67%) | |
| Hürthle cell | 1 (1.01%) | 0 (0%) | 1 (1.67%) | |
| TNM staging* | ||||
| pT | ||||
| pT1a | 20 (20.20%) | 7 (17.95%) | 13 (21.67%) | ns |
| pT1b | 28 (28.28%) | 7 (17.95%) | 21 (35%) | |
| pT2 | 17 (17.17%) | 5 (12.82%) | 12 (20%) | |
| pT3 | 20 (20.20%) | 11 (28.21%) | 9 (15%) | |
| pT4 | 14 (14.14%) | 9 (23%) | 5 (8.33%) | |
| pN | ||||
| pN0 | 27 (27.27%) | 11 (28.21%) | 16 (26.67%) | ns♦ |
| pN1a | 8 (8.08%) | 2 (5.13%) | 6 (10%) | |
| pN1b | 64 (64.65%) | 26 (66.67%) | 38 (63.33%) | |
| cM | ||||
| cM0 | 91 (91.92%) | 34 (87.18%) | 57 (95%) | ns♦ |
| cM1 | 8 (8.08%) | 5 (12.82%) | 3 (5%) | |
| Tumor size (mm) | ||||
| Mean (SD) | 22.3 (14.94) | 26.23 (16.77) | 19.75 (13.14) | ns# |
| Median (range) | 19 (0-70) | 22 (1-70) | 18 (0-60) | |
| Central lymph nodes (number) | ||||
| Positive | ||||
| Mean (SD) | 5.1 (6) | 5.23 (5.57) | 5.02 (6.3) | ns# |
| Median (range) | 4 (0-29) | 4 (0-20) | 3 (0-29) | |
| Total | ||||
| Mean (SD) | 10. 76 (7.66) | 10.82 (7.2) | 10.72 (8) | ns# |
| Median (range) | 8 (0-30) | 11 (0-25) | 7.5 (0-30) | |
| Lateral lymph nodes (number) | ||||
| Positive | ||||
| Mean (SD) | 4.69 (6.18) | 6.26 (7.04) | 3.67 (5.36) | ns# |
| Median (range) | 2 (0-25) | 4 (0-24) | 2 (0-25) | |
| Total | ||||
| Mean (SD) | 17.45 (13.4) | 19.84 (14.55) | 17.44 (12.12) | ns# |
| Median (range) | 16 (0-60) | 19 (1-60) | 15 (1-48) | |
| Multifocality | ||||
| No | 50 (50.51%) | 12 (30.77%) | 38 (63.33%) | <0.01 |
| Yes | 49 (49.49%) | 27 (69.23%) | 22 (36.67%) | |
| Capsular invasion | ||||
| No | 44 (44.44%) | 10 (25.64%) | 34 (56.67%) | <0.01 |
| Yes | 55 (55.56%) | 29 (74.36%) | 26 (43.33%) | |
| Extrathyroidal extension | ||||
| No | 65 (65.66%) | 21 (53.85%) | 44 (73.33%) | <0.05 |
| Yes | 34 (34.34%) | 18 (46.15%) | 16 (26.67%) | |
| Evidence of disease | ||||
| NED | 91 (91.92%) | 34 (87.18%) | 57 (95%) | ns♦ |
| ED | 8 (8.08%) | 5 (12.82%) | 3 (5%) | |
| Total | 99 (100%) | 39 (100%) | 60 (100%) | |
PTC-papillary thyroid cancer; FTC-follicular thyroid cancer; TNM-tumor, node, metastasis; *AJCC/UICC 8th edition; SD-standard deviation; NED-no evidence of disease; ED-evidence of disease; ns-no statistical significance; #Wilcoxon rank sum test with continuity correction; ♦Fischer exact test.
Table 3.
Disease outcomes in the study population.
| Outcome | Total | Children (≤16) | Adolescents (>16) | Pearson χ2 test |
| Event | ||||
| NED pts | ||||
| With recurrence | 17 (18.68%) | 5 (14.71%) | 12 (21.05%) | ns |
| Without recurrence | 74 (81.32%) | 29 (85.29%) | 45 (78.95%) | |
| Total | 91 (100%) | 34 (100%) | 57 (100%) | - |
| ED pts | ||||
| With progression | 7 (87.5%) | 5 (100%) | 2 (66.67%) | ns♦ |
| Without progression | 1 (12.5%) | - | 1 (33.33%) | |
| Total | 8 (100%) | 5 (100%) | 3 (100%) | - |
| Adverse events in all pts | ||||
| With adverse event | 24 (24.24%) | 10 (25.64%) | 14 (23.33%) | ns |
| Without adverse event | 75 (75.76%) | 29 (74.36%) | 46 (76.67%) | |
| Total | 99 (100%) | 39 (100%) | 60 (100%) | - |
| Time to event | ||||
| DFI (years) for NED pts | ||||
| Median (95%CI) | NR | NR | NR | ns* |
| PFI (years) for ED pts | ||||
| Median (95%CI) | 5 (>1.8) | 1.9 (>1.8) | 8.1 (>0.2) | ns* |
| EFI (years) for all pts | ||||
| Median (95%CI) | NR | NR | NR | ns* |
NED-no evidence of disease; pts-patients; ED-evidence of disease; DFI-disease-free interval; PFI-progression-free interval; EFI-event-free interval; CI-confidence interval; NR-not reached; ♦Fischer exact test; *Log-rank test.
Table 4.
Demographic and pathological characteristics as prognostic factors.
| Characteristics | Event (relapse/progression) | Event-free interval (years) | |||
| Without | With | Test | Median EFI (95%CI) | Log-rank test | |
| Age (years) | |||||
| Children | 29 (38.67%) | 10 (41.67%) | ns | NR (>17) | ns |
| Adolescents | 46 (61.33%) | 14 (58.33%) | NR | ||
| Sex | |||||
| Female | 56 (74.67%) | 19 (79.17%) | ns | NR | ns |
| Male | 19 (25.33%) | 5 (20.83%) | NR | ||
| Tumor size (ROC) | |||||
| ≤30.5 mm | 64 (85.33%) | 11 (45.83%) | <0.01 | NR | <0.01 |
| >30.5 mm | 11 (14.67%) | 13 (54.17%) | 4.8 (>1.6) | ||
| Multifocality | |||||
| No | 41 (54.67%) | 9 (37.5%) | ns | NR | ns |
| Yes | 34 (45.33%) | 15 (62.5%) | NR (>17) | ||
| cM1 at diagnosis | |||||
| No | 74 (98.67%) | 17 (70.83%) | <0.01 | NR | <0.01 |
| Yes | 1 (1.33%) | 7 (29.17%) | 5 (>1.8) | ||
| Capsular invasion | |||||
| No | 41 (54.67%) | 3 (12.5%) | <0.01 | NR | <0.01 |
| Yes | 34 (45.33%) | 21 (87.5%) | NR (>12.3) | ||
| Positive LN (ROC) | |||||
| ≤10.5 | 58 (77.33%) | 4 (16.67%) | <0.01 | NR | <0.01 |
| >10.5 | 17 (22.67%) | 20 (83.33%) | 12.3 (>3.2) | ||
| Extrathyroidal extension | |||||
| No | 59 (78.67%) | 6 (25%) | <0.01 | NR | <0.01 |
| Yes | 16 (21.33%) | 18 (75%) | 14.7 (>1.8) | ||
| Total | 75 (100%) | 24 (100%) | - | - | - |
ROC-receiver operating characteristic curve analysis cut-off value; cM1-clinically verified distant metastasis, LN-lymph node; EFI-event-free interval; CI-confidence interval; NR-not reached; ns-not statistically significant.
Table 5.
Univariate and multivariate logistic regression analysis results for adverse event occurrence.
Table 5.
Univariate and multivariate logistic regression analysis results for adverse event occurrence.
| Characteristics | Logistic regression for event (relapse/progression) | |||
| Univariate | Multivariate | |||
| OR (95%CI) | Wald Test | OR (95%CI) | Wald Test | |
| Tumor size (ROC) | ||||
| >30.5 mm: ≤30.5 mm | 6.9 (2.5-19.2) | <0.01 | - | ns |
| Initially metastatic | ||||
| Yes: No | 30.5 (3.5-264.2) | <0.01 | - | ns |
| Capsular invasion | ||||
| Yes: No | 8.4 (2.3-30.7) | <0.01 | - | ns |
| Positive LN (ROC) | ||||
| >10.5: ≤10.5 | 17.1 (5.1-56.7) | <0.01 | 6.4 (1.7-24.6) | <0.01 |
| Extrathyroidal extension | ||||
| Yes: No | 11.1 (3.8-32.5) | <0.01 | 5.1 (1.4-18.3) | <0.01 |
ROC-receiver operating characteristic curve analysis cut-off value; LN-lymph node; OR-odds ratio; CI-confidence interval; ns-not statistically significant.
Table 6.
Univariate and multivariate Cox proportional hazard regression analysis results for event-free interval.
Table 6.
Univariate and multivariate Cox proportional hazard regression analysis results for event-free interval.
| Characteristics | Cox regression for EFI | |||
| Univariate | Multivariate | |||
| HR (95%CI) | Wald Test | HR (95%CI) | Wald Test | |
| Tumor size (ROC) | ||||
| >30.5 mm: ≤30.5 mm | 5.63 (2.49-12.71) | <0.01 | - | ns |
| Initially metastatic | ||||
| Yes: No | 6.6 (2.72-16.01) | <0.01 | - | ns |
| Capsular invasion | ||||
| Yes: No | 6.76 (2.01-22.69) | <0.01 | - | ns |
| Positive LN (ROC) | ||||
| >10.5: ≤10.5 | 11.36 (3.87-33.36) | <0.01 | 6.48 (2.05-20.51) | <0.01* |
| Extrathyroidal extension | ||||
| Yes: No | 8.02 (3.17-20.29) | <0.01 | 3.83 (1.42-10.36) | |
ROC-receiver operating characteristic curve analysis cut-off value; LN-lymph node; EFI-event-free interval; HR-hazard ratio; CI-confidence interval; ns-not statistically significant; * Likelihood ratio test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



