
Submitted:
01 April 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
Background/Objectives: This population-based study examined epidemiological trends of primary cancers in adolescents and young adults (AYA) to enhance the understanding of the specific spectrum of cancers impacting AYA in Belgium. Methods: Data on incidence, prevalence, mortality, and survival were obtained from the Belgian Cancer Registry (2004–2020, N=43,535). (A)APC statistics were compared with children (5–14 years) and adults (40–49 years). Results: Cancer incidence increased by 0.4% annually from 66 to 80 per 100,000 person-years (ESR2013) but stabilized after 2015, except for Hodgkin lymphoma, chronic myeloid neoplasms, testicular, and breast cancer, which continued to rise. Mortality decreased by 1% annually, from 10 to 7 per 100,000 person-years (2004–2019). Five-year relative survival (RS) was 87% but remained low for certain cancers, including ovary (78%), central nervous system (67%), precursor haematopoietic neoplasms (64%), gastrointestinal (excl. colorectal) (49%), and lung-bronchus-trachea cancers (42%). Conclusions: From 2004–2020, the cancer burden among AYAs in Belgium increased due to improved survival, while incidence stabilized after 2015. Five-year RS exceeds 80% overall but remains lower for some cancers compared to children (e.g., precursor haematopoietic neoplasms) or older adults (e.g., breast cancer, sarcoma). The Belgian epidemiological trends align with those in neighbouring countries (Netherlands, France, Germany).
Keywords:
adolescents and young adults
; AYA
; incidence
; survival
; prevalence
; mortality
; cancer trends
; Belgium
; cancer epidemiology
1. Introduction
In Belgium, cancer predominantly affects older individuals, with 70% of women and 81% of men aged 60 years or older at diagnosis in 2022 [1]. Given that approximately 19% of the Belgian population is 65+, these figures highlight the disproportionately high cancer incidence among older adults [2]. Although cancers in adolescents and young adults (AYA) are rare, they represent the fourth leading disease-related cause of death in this population in high- and middle-income countries [3]. Trama et al. (2020) [4] reported approximately 112,000 new cancer cases among AYA in Europe, representing 5% of the new cancers diagnosed in the total population of the EU countries selected for their study. Gupta et al. (2020) [5] studied incidence trends of AYA cancers in 41 countries, spread across the continents, for the period 1998-2012. Data from the International Agency for Research on Cancer’s CI5plus database [6] were used. The authors reported an increase of AYA cancer incidence in 23 countries, predominantly industrialized ones, with colorectal, thyroid, testicular cancer, and melanoma types (particularly in European countries) being the highest attributors. You et al. [7] used data from the Global Burden of Disease 2019 study [8] to assess epidemiological trends for AYA cancer in 204 countries, from 1990 to 2019. The authors stated that incidence of cancer in AYA increased slightly with 0.4% annually in Western Europe.
EUROCARE-5 demonstrated that survival rates in AYAs trail behind those in children for several cancers that affect both groups, especially for more common haematological malignancies [9]. Inferior survival rates of AYA have been attributed to various factors, such as differences in biological characteristics or pathophysiology, variations in the pharmacokinetics of chemotherapeutic agents, less inclusion of AYA in clinical trials, and delays in diagnosis and treatment [10,11]. Additionally, other important attributing factors are the lack of specialized guidelines and education, and inadequate tailored healthcare professional attention and awareness [12].
The definition of AYA with cancer is not fixed and deeply vary according to countries. The age range of adolescence (15-19 years) [13] is generally accepted in the literature, even though it is sometimes suggested to start younger from 14, 13 or puberty. There is, however, still a lack of consensus concerning the upper age limit of young adulthood, varying from 20 to 39. In 2006, the United States National Cancer Institute’s (NCI) Adolescent and Young Adult Oncology Progress Review Group defined AYA with cancer as those diagnosed at age 15-39 years [14]. This definition was adopted by the European Network for Cancer in Children and Adolescents (ENCCA) and the Joint Cancer in the AYA ESMO/SIOPE Working Group. Heterogeneous age groups are currently used in different European countries. The AYA definition influences the way this age group is managed, depending on the national / regional cancer care organisation, either in adult ward or in the paediatric setting or in a specific AYA unit [15]. In Belgium, the AYA age group has been defined as 16-35 years, as per the RIZIV-INAMI convention on psychosocial care for AYA [16], where 16 corresponds to the upper age limit for paediatric wards.
Cancers in AYA are distinguished from those in children and older adults because of important differences in the distribution of cancer types, risk factor profiles, cancer biology, survivorship, and long-term health consequences [11]. AYA cancers represent a heterogeneous spectrum of malignancies, with the distribution of cancer types varying significantly by age: ranging from paediatric cancers like acute lymphoblastic leukaemia (ALL) to adult cancers such as carcinoma and melanoma. Moreover some cancer types exhibit an incidence peak in the AYA age group such as testicular cancers and Hodgkin lymphoma [11,17]. Due to this heterogeneity in cancer types, overlapping with children and older adult cancer types, AYA patients fall between the paediatric and adult oncology or haematology care settings. As a result, this group is generally overlooked and understudied [12].
Classification of cancers diagnosed in the adulthood mostly relies on locations while in paediatrics, cancers are grouped by main morphology types [18]. Since AYA cancers are specific and intermediate between paediatric and older adult cancers, the Surveillance, Epidemiology, and End Results Program (SEER) proposed another way to group the ICD-O codes (combination of diagnostic and morphology criteria) to fit the specific distribution of cancer types in AYA. The SEER AYA site recode classification scheme is adapted from the classification scheme proposed by Barr et al. [17,19].
The distinction between AYA and other age categories is not restricted to diagnosis and survival but also concerns the psychosocial level. AYA find themselves in a very specific stage of life with a life-threatening disease and therefore experience specific needs and problems. Young cancer patients and survivors often face long-lasting physical side effects and psychological consequences. These influence the quality of life, social life, professional/student and intimate relationships negatively [20,21].
The Belgian Cancer Registry (BCR) is a national and population-based cancer registry that has collected and maintained epidemiological data on cancer across the country since 2004. BCR regularly release reports on cancer incidence, prevalence, and survival in Belgium on the BCR website. In addition to three reports released in 2013, 2019 and 2023 that focused on cancers diagnosed in children and adolescents (0-19 years old) [22,23,24], a recent report [25] presents epidemiological data on cancers in AYAs, with the age range defined by the previously mentioned RIZIV-INAMI Convention [16] aged between 16 and 35 years.
This study is the first to provide a broad perspective on the epidemiological trends of AYA cancer patients in Belgium over time, by age sub-groups and by placing these trends in an international context. Using the international AYA definition (15–39 years) and standardized cancer classifications, meaningful international comparisons were facilitated.
2. Materials and Methods
2.1. Data Source and Selection
Cancer registration in Belgium has a legal basis. In 2003 the Royal Decree concerning the oncological care programs describing the reimbursement of the multidisciplinary oncological consult (MOC) was enacted [26]. In 2006, the law concerning the Cancer Registry was created, making cancer registration compulsory for oncological care programs and for laboratories for pathological anatomy [27]. The law also authorizes using the national social security number as the unique identifier of the patient and linkage with other medical and/or administrative databases. Additionally, through linkage with the Crossroads Bank for Social Security, this unique number enables the Cancer Registry to perform active follow-up on the vital status and date of death of the patients.
All malignant neoplasms (ICD-O-3 behaviour code /3) and all neoplasms whatever the behaviour (/0 benign, /1 intermediate) for CNS tumours in Belgian residents, aged 15–39 years and diagnosed between 2004 and 2020, were extracted from the BCR database. Incidence data with ICD-O-3 classification were grouped according to the SEER AYA site recode classification scheme [19]. The classification is filed in the Table S1. Cancers classified under the SEER code 10 (Miscellaneous specified neoplasms) and 11 (Unspecified malignant neoplasms except for CNS) were grouped and renamed to ‘Other Neoplasms’.
For the generation of mortality data (which are classified according to the ICD-10 classification), the grouping was adapted to match as much as possible the ICD-O-3-derived SEER classification. Haematological malignancies could not be subdivided due to a discrepant subclassification by diagnosis, location, and topography. Belgian population data are obtained from the Directorate-General Statistics Belgium (Statbel) [28]. Data transmitted by Statbel, available up to the year of incidence 2019, were used to generate mortality data. ICD-10 is a classification for all diseases, not only cancers. Statbel provides data exclusively on malignant neoplasms (group C) in an aggregated format, with BCR utilises to estimate cancer mortality in Belgium. Sex, age, and calendar year-specific population data were retrieved from Statbel as well.
Although the AYA age group is defined as 16-35 in Belgium, the age range 15-39 years – of the US NCI [14] and the Joint Cancer in AYA ESMO/SIOPE WG [29] - was selected for this study, as this definition is widely used in international literature and consequently enables making a comparison between Belgium and other countries. To overcome analyses with small numbers, the data were aggregated in age groups (15-19 years, 20-24 years, 25-29 years, 30-34 years, 35-39 years) for the calculation of Belgian incidence, prevalence, mortality, and survival data. The rates for each sex were presented separately whenever possible. Otherwise, data for men and women were grouped. Results of children (5-14 years) and older adults (40-49 years) were also included to allow comparison of AYA trends and specificities with their closest age groups. Younger children, especially infants (<5 years old), and elderly adults (>50 years old) have very different characteristics and prognostic factors which may modify survival and incidence.
Carcinoma of the gastrointestinal (GI) tract, except colorectal and pancreas carcinoma, (SEER code 9.3, carcinoma of the oesophagus, stomach, small intestine, liver-intrahepatic bile ducts, pancreas) were kept combined under the term ‘Rest of the carcinomas of GI tract’, seen the small numbers in the AYA-population.
To enable international comparisons of trends in incidence and mortality, the (A)APC values were calculated for France, Germany, and the Netherlands. The data sources for these countries were as follows: 1) the Netherlands: population data were obtained from the Centraal Bureau voor Statistiek [30], while mortality and incidence data came from the Integraal Kankercentrum Nederland [31], 2) France: population data were sourced from the Institut National de la Statistique et des Etudes Economiques [32], and mortality and incidence data from the Institut National du Cancer [33], 3) Germany: population data were retrieved from DeStatis Statistisches Bundesamt [34], and mortality and incidence data from Zentrum Für Krebsregisterdaten [35].
2.2. Analysis
Descriptive analyses were performed on the data provided by BCR: the total cases for incidence, mortality, 5- and 10-year prevalence, 5-year relative survival. Annual-specific rates were calculated per 100,000 person-years by BCR using the mid-year population size obtained from Statbel. The total studied period is 17 years (2004-2020). Incidence, mortality and prevalence rates were age-standardised (ASR) with weights based on the five-year age groups from the 1976 and 2013 European standard population (ESP) [36], and the World standard population (WSP) [37]. Since the structure of the Belgian AYA population is comparable with the ESP 2013, the ESR 2013 was used as ASR throughout this study. For sections comparing the results internationally, the WSR was used. In the supplementary materials, the results are showed in crude rates, ESR, ESR2013, and WSR.
Relative survival data were calculated and provided by BCR. One-, five- and ten-year relative survival rates by sex and age group (15-19, 20-24, 25-29, 30-34, 35-39 years old) are presented and compared with a younger age group (5-14 years) and an older age group (40-49 years). Expected survival calculations were based on sex-, age, and calendar-year-specific Belgian life tables [28], according to the Ederer II method. This method is based on the actual follow-up time rather than the potential follow-up time to estimated survival [38]. Relative survival data with N at risk <50 were not included in the analysis, because they are below the statistical reliability threshold.
For the international comparison, annual-specific rates were calculated per 100,000 person-years by direct standardization. Incidence, and mortality rates were age-standardized (ASR) with weights based on the five-year age groups from the 2013 European standard population (ESP2013).
Since data have been collected from 2004 onwards, results can also be compared over time. In total, 17 consecutive years of incidence and 16 years of mortality data were used in this study. Because of the low incidence of cancers in the AYA-population, incidence and mortality rates are aggregated over two age groups, 15-29 years and 30-39 years. To assess the average annual percentage change (AAPC), the freely available Joinpoint Regression Program version 5.0.2 [39] was used, by fitting joinpoint models to the log-transformed age-standardized incidence and mortality rates. All models were plotted using the ‘grid search method’ and the ‘uncorrelated error model’. The number of points to place between adjacent observed x-values in the grid search method was set at 2 (0 at default). Correlation of the random errors in the data were analysed by repeating the analyses multiple times, each time with a different value of the autocorrelation parameter (0.1, 0.2, and 0.3). Outcomes were similar to those obtained with the uncorrelated error model, which was then selected for the final analyses, as correcting for autocorrelation can reduce the power to detect joinpoints. A minimum of zero and a maximum of two joinpoints were allowed in this 16/17-years analysis, since it is recommended that at least seven data points be observed to consider allowing a joinpoint [40]. Selection of the final model was done using the recommended Bayesian information criteria 3 (BIC3). Further parameters within the Joinpoint program were kept at their default setting. Joinpoint analysis with too low values, resulting in negative log-transformed values, is not possible. Trends were considered stable if they did not reject the null hypothesis, corresponding to zero lying within the AAPC 95% confidence interval.
3. Results
3.1. Incidence
A total of 43,535 patients aged 15-39 years were diagnosed with cancer (all cancers excluding non-melanoma skin cancer) in the period 2004-2020 in Belgium. Overall, AYA cancers represented 4% of the Belgian cancers diagnosed in the studied period. The age distribution in this cohort was, 6%, 10%, 17%, 26%, 41% in the respective age groups 15-19, 20-24, 25-29, 30-34 years and 35-39 years old at diagnosis (Table S2).
The overall age-adjusted incidence rates were higher in female AYA than in male AYA, with a female to male ratio of 1.65 (94 vs 57 cases per 100,000 population, during 2004-2020). Cancer incidence rates are slightly higher in male AYA aged 15 to 19 years (25 vs 22 cases per 100,000 population in males and females, respectively, during 2004-2020), mostly because of testis cancer, sarcoma, and haematological neoplasms (4, 4, 3 cases per 100,000 population respectively). The rates did not differ between both sexes in the 20-24 age group (38 cases per 100,000 population for males and 39 for females). Rates in women compared with men, however, are 30% higher in AYA aged 25 to 29 years (69 vs 54 per 100,000 population) and nearly double in those aged 30 to 39 years (158 vs 79 per 100,000 population), primarily because of the substantially higher incidence of breast, thyroid, and genital cancers (mostly cervix cancer), and melanoma of the skin in women. For example, thyroid cancer incidence rates among women in their late twenties are almost 5-fold higher than those among men (9 vs 2 per 100,000 population during 2004-2020, respectively).
Among AYA, incidence increases with advancing age for all cancer types except for Hodgkin lymphoma, precursor haematopoietic neoplasms, testis tumour and histiocytic and dendritic cell neoplasms (HDCN).
In general, the cancer type distribution shifted considerably with age (Figure 1) from a higher proportion of childhood cancers (e.g. precursor haematopoietic neoplasms, mostly acute lymphoblastic leukaemia/lymphoma – ALL/L) in adolescents (individuals aged 15-19 years) to more adulthood cancers in the 35-39 young adults (e.g. carcinomas). Moreover, some cancer types occur more specifically in the AYA subgroup: Hodgkin lymphoma and testis tumour exhibit a peak of incidence in AYA, in the age group 20-24 year old and in 25-34 year old respectively.
3.2. Mortality
A shift with age is also abserved for mortality by cancer type. During the period 2004-2019, haematological malignancies, CNS tumours and sarcoma were among the leading cancer-causes of death in younger AYA (aged 15-29 years), similarly as in children (5-14 years). In the older AYA (aged 30-39 years, the top 5 leading cancer causes of death were similar to those identified in the older adults (40-49 years) but not in the same order: breast cancer was followed by CNS tumours and haematological malignancies while cancer of lung, broncus, trachea was the leading cancer-cause of death, followed by breast cancer and CNS tumours (Figure 2, Table S3).
3.3. Long-Term Trends in Incidence and Mortality
Long-term trends in cancer incidence and mortality rates by age group among AYA compared to children and patients in their fourties are shown in Figure 3. The age-standardized incidence rates among AYA slightly increased by 0.2% per year from 2004 to 2020 (Table S4). However, breaking down the trend, it is observed that this increase occurs from 2004 to 2015, as from that year on, the rates become too scattered and a trend could not be detected. In younger women (15-29 years old) the incidence even moderatly decreased by -1% per year since 2015. It is noteworthy that the incidence remained stable over the whole studied period for patients in their fourties while no significant trend could observed over time for children, mainly due to a lack of robustness.
Four cancer types showed an increase in incidence during 2004-2020. The moderate increase in incidence for breast cancer in AYA (0.3% per year) during the whole period 2004-2020 seems largely attributable to the rising incidence rates in the younger AYA (15-29 years, 2% per year). At the same time, the incidence in older adults (40-49 years) slightly significantly declined (-0.1% per year). Testis cancer increased over time for AYA (1% per year), as well as for patients in their fourties (3% per year). A significant rising trend was detected for the incidence rates of Hodgkin lymphoma in AYA (+1% per year) over the 17-year period. In older adults (40-49 years) no significant trend could be observed over time for this cancer type. The incidence for chronic myeloid neoplasms increased over time for AYA (+3% per year), as well as in patients aged 40-49 years (+1% per year). The incidence decreased over time for carcinoma of genital sites excl. ovary and testis (mostly cervix cancer) by -1% per year.
For 3 cancer types, the incidence initially increased, but from a certain point in time either the incidence rates became too scattered and a significant trend could not be observed or the incidence rates decreased significantly. This was the case for thyroid cancer (+4% per year until 2012, from then on a decrease with 1% per year), colorectal cancer (increase with 3% per year, and from 2013 no trend) and skin melanoma (+2% per year and from 2010 onwards no trend).
However, a trend in incidence could not be observed in the studied 17 year-period for most cancer types, eg. CNS tumour, sarcoma, non-colorectal cancer of the GI tract, lung/bronchus/trachea cancer, urinary tract carcinoma, head and neck cancer, gonadal non-testicular tumours (mostly ovarian cancer), precursor haematopoietic and mature B-cell neoplasms. The Belgian mortality rates in AYA decreased significantly by 1% per year (Figure 4 and Table S4). Where a trend in mortality over time in children could not be detected, the mortalite rates decreased in older adults with 1% per year.
The Belgian mortality rates decreased significantly for all AYA age-groups and for both sexes in the studied period 2004-2019, where cancer mortality rates were generally higher for female AYA. The mortality decreased more in the younger AYA group (15-29 years, -2% per year) compared to the older AYA group (30-39 years, -1% per year). Due to low numbers, mortality trends for most cancer types could not be calculated. Nonetheless, a decrease in mortality since 2004 was observed in older AYA (aged 30-39 years) with breast cancer (-3% per year), where the mortality decreased faster than in patients aged 40-49 years (-2% per year). Significant rising trends could not be observed.
3.4. Relative Survival
The short-term 1-year relative survival (RS) rates for all cancers together, diagnosed between 2004 and 2020, show a very good result with 94% one-year RS in males and 97% in females, aged 15-39 years (Table S5). The slight difference in survival for males versus females is confirmed in the longer term; the overall five-year RS male-female (15-39 years) is 84% versus 89% and 81% versus 85% for the 10-year RS. The long-term RS rates for females remain above 80% for all age groups while it drops below 80% in males from 35 (79% and 75% at 5- and 10-year RS respectively). Although the RS rates (1-, 5- and 10-RS) remained above 90% for all age groups for Hodgkin lymphoma, chronic myeloid neoplasms, melanoma, testis cancer, HDCN, thyroid carcinoma (Figure 5), 5-year RS remained under 80% for AYA with ovary cancer (78%), CNS (67%), precursor haematopoietic neoplasms (64%), non-colorectal carcinoma of the GI tract (49%), and carcinoma of the lung-trachea-bronchus (42%).
Where the 5-year RS for most cancer types decreased with age (haematological malignancies, lung/bronchus/trachea, ovarian cancer, cancer of the GI tract, testis cancer, CNS tumours) or remained stable over the age groups (thyroid carcinoma, testis cancer, skin melanoma), it slightly increased with age for sarcomas and breast cancer, with the poorest survival outcome in adolescents (sarcoma) and 20-24 year old (breast cancer), compared to older adults (5-year RS of respectively 70% vs 82% in sarcoma, and 87% vs 94% in breast cancer). The 5-year relative survival (RS) is higher in AYAs than in children and older adults for chronic myeloid neoplasms (94% in AYAs, 88% in children, 92% in older adults) and CNS tumours (67% in AYAs, 63% in children, 43% in older adults).
3.5. Prevalence
It was estimated that on 31st December 2020, 9,722 AYA (3,929 males, 5,793 females) who had been diagnosed with at least one type of cancer (excluding non-melanoma skin cancer) within the past 5 years were living in Belgium and 15,192 (6,358 males, 8,834 females) within the past 10 years. This represents respectively 0.3% and 0.4% of the Belgian AYA population in 2020. Prevalence data are detailed in Table S6.
The five primary cancers with the highest 5-year prevalence in Belgian AYA (15-39 years) were carcinoma of the breast, skin melanoma, testis cancer, thyroid carcinoma, and Hodgkin lymphoma (Figure 6). The distribution of the most prevalent cancers also shifted with age. Youngest age group (15-29 year) was composed of a mix of cancers highly prevalent in children as well other cancers, such as melanoma, testis and thyroid cancers. These three latter cancer types stay in the top five most prevalent cancers in AYA older than 20 years. The most prevalent cancer in these younger age groups was Hodgkin lymphoma. Sarcoma was the second most prevalent cancer in adolescents (15-19 years), followed by precursor haematopoietic neoplasms, CNS, and mature B-cell neoplasms. As from age 25 onwards, breast cancer introduces itself and is the most prevalent cancer in AYA older than 30. Cancer of genital sites (excl. ovary, testis) – mostly cervix cancer – is highly prevalent in AYA older than 30 years. Colorectal cancer can be found in the top ten most prevalent cancers in children, AYA and older adults.
3.6. International Comparison
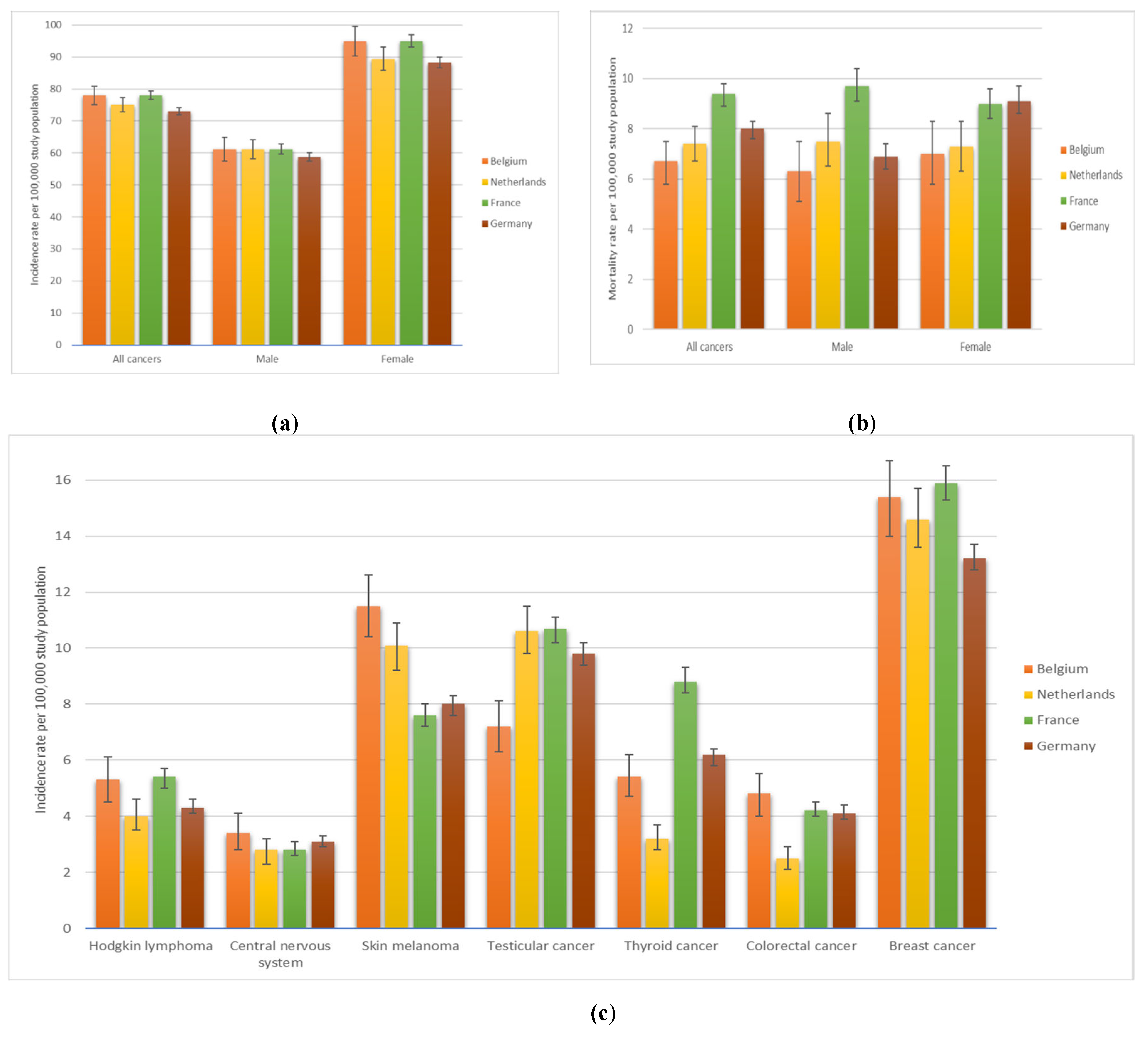
When comparing the Belgian incidence and mortality data with the neighbouring countries (the Netherlands, France, Germany), the rates in 2019 are aligned (Figure 7, Table S7 and Table S7.1). The incidence year 2019 (instead of 2020) was selected for comparison to avoid any potential impact of the COVID-19 pandemic on the interpretation of the results. While Belgian incidence rates are comparable to those in the Netherlands, France, and Germany, overall cancer mortality rates in Belgium are relatively lower than in neighboring countries. Mortality rates in AYA have decreased in Belgium as well as in surrounding countries and at a somehow same percentage in Belgium, the Netherlands and France (-1% per year) (Table S7).
The incidence trends are generally aligned (Table S7). While no clear trend in Hodgkin lymphoma incidence was observed in the Netherlands, an increase of approximately 1% per year was noted in Belgium, France and Germany. Over the last decade of the observed period, incidence rates for skin melanoma remained relatively stable in Belgium, but showed a significant decline in the Netherlands, France, and Germany, with annual decreases of -1%, -1%, and -2% respectively. In 2019, the incidence of skin melanoma in Belgium (12 per 100,000 population) was slightly higher than in the Netherlands (10 per 100,000) and France and Germany (both 8 per 100,000 population). While colorectal cancer incidence remained relatively stable in Belgium over the last decade of the observed period and in the Netherlands from 2004 to 2020, it showed a gradual increase in Germany and France, with annual rises of +1% and +3%, respectively. In 2019, Belgium had a lower incidence of testicular cancer (7 per 100,000) compared to the Netherlands, France (11 per 100,000), and Germany (10 per 100,000). Belgium's incidence increased by 1% annually, similar to France (+2% per year). In the Netherlands, the trend initially rose but stabilized from 2014 to 2020, while no trend was observed in Germany. Comparable incidence trends for thyroid cancer were observed in Belgium, the Netherlands, France, and Germany. Initially rising, the incidence then either decreased (Belgium since 2012 and France since 2013) or stabilized (Netherlands since 2014 and Germany since 2009). Between 2004 and 2020, breast cancer incidence in Belgium increased by 0.3%, a trend also observed in France (+0.5%), the Netherlands and Germany (both +0.3%).
4. Discussion
This study provides insight into the epidemiological trends among AYA aged 15 to 39 years old at diagnosis of cancer in Belgium, between 2004 and 2020. The key findings are that
(I) the spectrum of cancers in AYA is greatly distinct and heterogeneous justifying the importance of distinguishing AYA based on age and sex instead of grouping them all together for analytical purposes;
(II) the standardised incidence trend is stabilised in the more recent years after a slightly increasing trend between 2004 and 2015, with variations depending on cancer types as well as on sex, age;
(III) the Belgian incidence and mortality trends align with those observed in surrounding countries, while the mortality rate for AYA in Belgium generally remained lower than in neighbouring nations.
The results of this study are in line with Trama et al [4], reporting that testis cancer is the most common cancer among young men aged 15-39 years and Li et al [41] reporting that among women early-onset breast cancer had the highest incidence. The Belgian incidence rate for skin melanoma was slightly higher than the European average reported by Trama et al., but is comparable to neighbouring countries Germany and the Netherlands [4]. The higher cancer incidence rate in female AYA is mostly explained by the higher incidence of thyroid and breast cancer in female AYA in the 30-39 age subgroup. The relative higher cancer incidence rates among female AYA older than 20 years, compared to male AYA, have been observed in Europe and globally [4,41].
The incidence rates in the Belgian AYA population generally slightly rose from 2004 to 2015. This finding aligns with Trama et al. [4], who reported a steady rise in European incidence (1998–2012).
Although the aetiology of early-onset cancer is still uncertain, it can most likely be linked to exposure to risk factors at an early age. Risk factors are multifactorial, resulting from a combination of environmental and lifestyle factors in addition to a genetic susceptibility, with differences between the specific cancer types, sex, age [42,43]. The genetic predisposition of cancer in AYA (as well as in childhood) is higher than in older patients [44]. The contribution of established risk factors to the increasing incidence of AYA is uncertain, necessitating additional research. It might be that a better survival of childhood cancers and the higher risk of developing subsequent malignancies in survivors when compared with the general population [45], might slightly contribute to this increase in AYA cancer. Macq et al [46] studied the epidemiology of multiple primary cancers in Belgium and found that the odds of having more primary cancers increase with age and depend on the cancer site. However, this study could not test this hypothesis.
Since 2015, however, the Belgian incidence trend stabilised, and even decreased in female AYA aged 15-29 years. This observation aligns with Zhang et al. [47], who analysed epidemiological trends among US AYA from 2016 to 2021 and found that after a period of rising incidence rates, they stabilized from 2016 onward. Additionally, Voeltz et al. [48] observed similar incidence trends, reporting a rise in German early-onset cancer cases from 1990 to 2010, followed by a decline from 2010 onward.
This plateauing trend in Belgian incidence is mainly driven by the stabilisation or decline in incidence rates for skin melanoma, thyroid cancer, and colorectal cancer, starting from 2010, 2012, and 2013 respectively.
The incidence rates for skin melanoma in Belgian AYA are relatively high, compared to the European rate [4]. Where the incidence steadily increased over time for AYA aged 30-39 with 1% per year, it declined from 2010 onward in younger AYA (aged 15-29). Similarly, Zhang et al [47] found that from 2016 onward US incidence for this cancer type decreased in AYA. The prominent increases in skin melanoma among older AYA (aged 30-39) over time likely result from (unprotected) increased sun exposure. It could also reflect increased cancer awareness, resulting in more detection as well as more systematic registration. Earlier studies suggest that younger people might be more biologically susceptible to the carcinogenic effects of artificial UV radiation, increasing the risk of early-onset melanoma in a dose-response way with first exposure at early age and frequency of exposure [49,50]. The decrease in incidence in younger AYA (15-29 years old) since 2010, on the other hand, might indicate that primary preventive actions in early-life (e.g. education on sun protective behaviour) are effective [51]. Despite this positive message, the Belgian organisation Foundation Against Cancer warns that awareness amongst 16-24 year olds has been decreasing in the recent years [52].
It remains unclear what causes the higher thyroid cancer incidence among female AYA exactly [53]. The incidence rose significantly by 4% per year until 2012, after which it declined by 1% annually. In older patients, aged 40-49 years, the initial change in incidence stabilized as from 2015 onward. A stable trend was observed in the US for this cancer type in AYA between 2016 and 2021 [47]. However, in the Netherlands [54] (AYA, 1990-2016) and in Germany [48] (early-onset, 1999-2019), an upward trend was observed in incidence for this cancer type. There is some evidence suggesting that exposure to ionizing radiation could influence the incidence of thyroid carcinomas in AYA [55]. However, in low-risk regions, such as Belgium, increasing incidence trends in thyroid carcinoma could be attributed to overdiagnosis [56,57]. Van den Bruel et al [58] showed in 2013 that regional variations in incidence of thyroid cancer in Belgium were attributable to variations in imaging detection rates ; the latter leading to overdiagnosis.
Belgian incidence rates of colorectal cancer in AYA increased with 3% per year until 2013, stabilizing from that year on. The incidence for this cancer type remained somewhat stable in Belgian adults aged 40-49 years. The 5-year RS for the overall group of AYA remains above 80%, however, there is a considerable difference in survival between AYA aged 15-29 years (91%) and the ones aged 30-39 years (77%). Delays in the detection of cancer for this age group might lead to more progressed stages of cancer at the time of the diagnosis [59,60,61]. Dutch incidence rates for CRC in AYA increased between 1990 and 2016 [54]. Voeltz et al [48] observed on the other hand stable incidence trends in early-onset colorectal cancer (Germany, 1999-2019). Zhang et al [47] reported an increase in rectal cancer and a stable trend in incidence of colon cancer in AYA over 2016-2021. An increase in colorectal cancer among young European adults from 1990 to 2016 was reported by Vuik et al [62]. Modifiable risk factors, such as a Westernized diet (processed meat, low vegetable, fish, and fruit intake), obesity, alcohol intake, smoking, and lack of physical activity were found to be associated with early-onset colorectal cancer, as well as non-modifiable factors such as male sex, Caucasian race, inherited predisposition and personal history of inflammatory bowel disease [63,64]. A hypothesis is that colorectal cancer in AYA has a unique biology relative to those arising at older ages, exhibiting a more aggressive phenotype, but knowledge is limited on this specific topic [59,65].
Most cancer types showed stable trends in incidence from 2004 to 2020. This is the case for CNS tumours, sarcoma, non-colorectal cancer of the GI tract, lung/bronchus/trachea cancer, urinary tract carcinoma, head and neck cancer, gonadal non-testicular tumours (mostly ovarian cancer), precursor haematopoietic and mature B-cell neoplasms.
From 2004 to 2020, incidence rates for CNS tumours remained stable among AYA, which is in line with observations in Belgian’s neighbouring countries [48,54]. The 5-year relative survival rate for malignant brain tumours ranges from 71% in younger AYA to 65% in the group aged 30-39 years, largely reflecting differences in the aggressiveness of glioma subtypes by age. For example, 15% of the gliomas in AYA aged 15-29 years were glioblastomas, compared to 27% in those aged 30-39 years.
The incidence in cervix cancer steadily decreased from 2004 to 2020 with 1% per year. In Belgium, cervix cancer is the only cancer with a population-based screening program that includes the AYA age group, with organized screening in Flanders and opportunistic screening in Wallonia and Brussels. Since 2013, woman aged 25 to 64 have been invited every three years for a cyto-histopathological screening, including Human Papillomavirus (HPV) triage for equivocal results [66]. The result of this screening program is reflected in the decreasing incidence trend for cancer of genital sites excl. ovary and testis (mostly cervix).
Where most cancer types showed decreasing/stable trends in from 2004 to 2020 or in the recent years, four cancer types demonstrated a steady increase in incidence: chronic myeloid neoplasms, testis cancer, Hodgkin lymphoma, and breast cancer. These observations are aligned with those in early-onset German cancers [48] except for an increase in thyroid cancer reported there.
The adaptation to classification changes may partly explain the increased incidence trend for chronic myeloid neoplasms in the 2000s.
Where for the majority of the studied cancer types the incidence rates increase (linearly) with age, it seems that for testis cancer and Hodgkin lymphoma other drivers (e.g. environmental factors) influence the incidence of AYA as well. Although the causal pathway of testis cancer is poorly understood, there is a consensus that the aetiology is multifactorial encompassing genetic and environmental factors. Common environmental risk factors include cryptorchidism [67], family history of testicular cancer [68], infections (Human papillomavirus, Epstein-Barr virus, Cytomegalovirus, Parvovirus B-19, and Human immunodeficiency virus) [69], intrauterine exposure to high oestrogen levels [70] and smoking [71], low birth weight [67], intratubular germ cell neoplasm, and prior history of testis cancer [72]. The incidence rates of testis tumours increased significantly over the years for AYA and older adults aged 40-49 years, which is in line with Voeltz et al [48] reporting an increase (Germany, early onset, 1990-2019). However, in Belgian AYA aged 30-39 years, from 2015 onwards no trend could be observed. These observations are aligned with the publication of Zhang et al [47] reporting a stable trend among AYA in the US from 2016-2021.
The survival in Belgian AYA for Hodgkin lymphoma (HL) is very good for this cancer type (5-year RS is 97%), however, survivors face significant late morbidity and mortality, necessitating lifelong clinical follow-up [73,74]. The Belgian incidence rates for HL among AYA steadily increased over the studied period, aligning with Dutch observations among AYA (1990-2016) [54]. The Belgian incidence rate, reported by Trama et al [4] is slightly above the European rate. Huang et al [75] found that, the past decade, worldwide there has been generally an increase in incidence of HL in patients younger than 40 years. The triggers for this increase remain uncertain, however, there is a hypothesis that this could be related to lifestyle, the prevalence of metabolic syndromes and improved early detection.
Breast cancer incidence among Belgian female AYA aged 15-29 years increased with 1.5% per year, where the trend remained stable in older AYA (aged 30-39 years). The incidence in older adults aged 40-49 years decreased from 2004-2020. Van der Meer et al [54] reported an increase in breast cancer among Dutch AYA between 1990-2016. The incidence of early-onset breast cancer increased in Germany as well between 1999-2019 [48]. AYA are more likely than older women with breast cancer to present with unfavourable biology and advanced disease [76,77]. Two key reasons for age-related diagnostic delays are young women's lack of awareness of early-onset breast cancer and the dismissal of suspicious signs as unimportant due to their age [78]. In addition, mammographic screening is not recommended for AYA at average breast cancer risk, reflecting diagnostic delays. Hormonal factors that increase early-onset breast cancer risk include early menarche, oral contraceptives, anovulatory infertility, and late parity after age 30 [79]. AYA breast cancer is more frequently familial, and approximately half of AYA women with breast cancer under the age of 30 have a germline predisposing mutation in BRCA1, BRCA2, or TP53 genes [80]. A potential hypothesis is that the increased focus on more active follow-up of individuals with a familial history and/or predisposition to breast cancer, may contribute to earlier diagnoses by identifying malignancies or precancerous lesions in resection specimens.
The mortality rates decreased significantly for all AYA age groups and both sexes in the studied period 2004-2020. These findings align with observations in the Netherlands for AYA over the period 1990-2016 [54], in Germany for early-onset cancer over 1999-2019 [48], and at the international level in AYA over 2000-2021 [41].
The Belgian relative survival for AYA is generally above the European average, for multiple cancer types [9]. There is however room for improvement for cancers of lung/bronchus/trachea, cancer of the gastro-intestinal tract (excl. colorectal), precursor haematopoietic neoplasms, ovarian cancer, and tumours of the central nervous system, whose 5-year RS vary between 42% and 78%. The survival gap with children remains for haematological malignancies (mainly for precursor haematopoietic neoplasms), which is in line with Trama et al [81], reporting that European AYA survival rates for ALL improved from 1978 to 2006 but did not reach the levels seen in children. The 5-year survival is generally better in AYA than in older adults aged 40-49 years, except for breast cancer and sarcoma. Causes for this survival gap may be differences in disease biology, treatment, therapy-related toxicities, and psychosocial factors [82]. There is a sex difference in survival, with an overall better prognosis for female AYA. Compared to females and other age groups, the five-year RS is the lowest in male AYA aged 35-39 years. This sex difference in survival reflects the better prognosis of breast carcinomas compared to cancers diagnosed in male AYA (such as cancer of head and neck, cancer of the GI tract excluding colorectal). Other variables that might lead to this survival gap between sexes are the stage of cancer at diagnosis, and socioeconomic status [83]. These variables were however not included in the dataset.
4.2. Strengths and Limitations
The conclusions drawn from this research stem from nearly twenty years of high-quality data, meticulously provided by registrars and physicians from Belgian oncology care programmes and laboratories for pathological anatomy and collected by skilled data managers from BCR. This study also has a number of limitations. The interpretation of results for rare cancers should be done with caution as random fluctuations due to a low number of cases may erroneously appear as noteworthy trends. Also, low case numbers during certain sub-analyses lead to the inability to calculate average annual percentage change statistics for various cancer types. Another limitation is that it could be that the trends observed in this study are the results of using all stages combined, whereas some trends might only become apparent with individual disease stages. Finally, due to the SEER AYA classification and the small size of some of the cancer subgroups, cancer types with heterogeneous incidence and/or survival rates had to be combined into larger categories. The international comparison was limited because of differences in exhaustivity of registration, used classification and standardised rates.
However, the use of population-based data from BCR can be considered a major strength as selection bias is limited due to the inclusion of the entire Belgian population. Consequently, a comprehensive depiction of trends related to incidence, survival, and mortality within the Belgian AYA population was made possible. Stratification in five-year age groups allowed for a detailed assessment of age-specific trends within the AYA population, which is another major strength of this study considering that AYA are often grouped together, masking important age-related differences. Moreover the long observation period (17 years) allowed to analyse long term incidence and survival trends.
5. Conclusions
Although cancer in AYA might seem to be a transitional phase between childhood and adulthood cancer due to the presence of both paediatric cancers and carcinomas, it should be viewed as a distinct category. This is not only because of the higher incidence of certain cancer types in the AYA population, but also due to their specific characteristics in addition to their psychosocial needs.
It is crucial to monitor early-onset cancer trends to determine whether the stabilizing and decreasing patterns persist or if the increasing trends reverse. While it appears that some cancers are being brought under control through the reduction of known risk factors, early detection by increased awareness, and advancements in treatment, it is essential to recognize that the decline in incidence is associated with a reduced mortality, likely due to improvements in medical care, more effective treatments. This dual trends lead to an increase in the overall cancer burden among AYA and subsequently of the associated demands on healthcare resources. Given that the cancer burden is increasing in Belgium and AYA have many years of life ahead, contributing significantly to the economy, there should be a stronger emphasis on improving prevention of AYA cancers, awareness to foster early detection in complement to maintain precise epidemiological surveillance.
This population remains underrepresented in cancer research, and a clear understanding of the biological and genetic drivers for several cancer types is still lacking. In line with recent recommendations, enhancing the availability of and participation in clinical trials by overcoming known barriers is crucial to advancing AYA oncology outcomes. To address more complex research questions, large prospective datasets with detailed patient, clinical, and treatment information are needed. Since such data resources are limited, there must be increased efforts to initiate these collections. The launch of the Belgian AYA-dedicated program in November 2023 [16] made a significant step in addressing these issues.
Additionally, increased collaboration between paediatric and adult medical oncologists and haematologists at both national and international levels is necessary to address the distinct needs and challenges faced by this unique population. This study is the first to show that the increased cancer burden in AYA Belgium is mostly due to the improved survival with a stabilised incidence in the recent years and is comparable to what is observed in neighbouring countries. This study offers valuable insights to support policymakers in optimizing AYA cancer management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: SEER classification, Table S2: Number of new diagnoses, Table S3: Cancer causes of death, Table S4: AAPC, Table S5: Survival, Table S6: Prevalence, Table S7: International comparison, Table S7.7: International comparison Classification
Author Contributions
Conceptualization, F.V.A and H.A.P.; methodology, F.V.A.; software, F.V.A.; validation, F.V.A., B.V.G., N.V.D. and H.A.P.; formal analysis, F.V.A, H.A.P.; investigation, F.V.A, H.A.P.; resources, F.V.A., B.V.G., N.V.D.; data curation, F.V.A., B.V.G., N.V.D.; writing—original draft preparation, F.V.A., H.A.P.; writing—review and editing, F.V.A., B.V.G., N.V.D., and H.A.P.; visualization, F.V.A..; supervision, H.A.P..; project administration, F.V.A..; funding acquisition, H.A.P. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Belgian Cancer Registry. https://kankerregister.org/default.aspx?lang=EN.
- StatBel. Structure of the Population Based on the National Register: 2024. https://statbel.fgov.be/.
- GBD 2019 Adolescent Young Adult Cancer Collaborators. The Global Burden of Adolescent and Young Adult Cancer in 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Oncol. 2022, 23, 27–52. [Google Scholar] [CrossRef]
- Trama, A.; Stark, D.; Bozovic-Spasojevic, I.; Gaspar, N.; Peccatori, F.; Toss, A.; Bernasconi, A.; Quarello, P.; Scheinemann, K.; Jezdic, S.; Blondeel, A.; Mountzios, G.; Bielack, S.; Saloustros, E.; Ferrari, A. Cancer Burden in Adolescents and Young Adults in Europe. ESMO Open 2023, 8, 100744. [Google Scholar] [CrossRef]
- Gupta, S.; Harper, A.; Ruan, Y.; Barr, R.; Frazier, L.; Ferlay, J.; Steliarova-Foucher, E.; Fidler-Benaoudia, M. International Trends in the Incidence of Cancer Among Adolescents and Young Adults. Journal of the National Cancer Institute 2020, 112. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC), WHO. Cancer Incidence in Five Continents (CI5). https://ci5.iarc.fr/ci5plus/.
- You, L.; Lv, Z.; Li, C.; Ye, W.; Zhou, Y.; Jin, J.; Han, Q. Worldwide Cancer Statistics of Adolescents and Young Adults in 2019: A Systematic Analysis of the Global Burden of Disease Study 2019. ESMO Open 2021, 6, 100255. [Google Scholar] [CrossRef] [PubMed]
- Global Burden of Disease (GBD) 2021; Institute for Health Metrics and Evaluation (IHME)., 2024. http://www.healthdata.org/results/data-visualizations.
- Trama, A.; Botta, L.; Stiller, C.; Visser, O.; Cañete-Nieto, A.; Spycher, B.; Bielska-Lasota, M.; Katalinic, A.; Vener, C.; Innos, K.; Marcos-Gragera, R.; Paapsi, K.; Guevara, M.; Demuru, E.; Mousavi, S.M.; Blum, M.; Eberle, A.; Ferrari, A.; Bernasconi, A.; Lasalvia, P. Survival of European Adolescents and Young Adults Diagnosed with Cancer in 2010–2014. European Journal of Cancer 2024, 202, 113558. [Google Scholar] [CrossRef]
- Trama, A.; Botta, L.; Foschi, R.; Ferrari, A.; Stiller, C.; Desandes, E.; Maule, M.M.; Merletti, F.; Gatta, G. Survival of European Adolescents and Young Adults Diagnosed with Cancer in 2000-07: Population-Based Data from EUROCARE-5. Lancet Oncol 2016, 17, 896–906. [Google Scholar] [CrossRef]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer Statistics for Adolescents and Young Adults, 2020. CA Cancer J Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Stark, D.; A Peccatori, F.; Fern, L.; Laurence, V.; Gaspar, N.; Bozovic-Spasojevic, I.; Smith, O.; De Munter, J.; Derwich, K.; Hjorth, L.; T A van der Graaf, W.; Soanes, L.; Jezdic, S.; Blondeel, A.; Bielack, S.; Douillard, J.-Y.; Mountzios, G.; Saloustros, E. Adolescents and Young Adults (AYA) with Cancer: A Position Paper from the AYA Working Group of the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE). ESMO Open 2021, 6, 100096. [Google Scholar] [CrossRef] [PubMed]
- Barr, R. Common Cancers in Adolescents. Cancer treatment reviews 2007, 33, 597–602. [Google Scholar] [CrossRef]
- US Department of Health And Human Services; US National Institutes of Health; US National Cancer Institute; Adolescent and Young Adult Oncology Progress Report Group. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancers, 2006. https://www.livestrong.org/sites/default/files/what-we-do/reports/ayao_prg_report_2006_final.pdf.
- Saloustros, E.; Stark, D.; Michailidou, K.; Mountzios, G.; Brugieres, L.; Peccatori, F.; Jezdic, S.; Essiaf, S.; Douillard, J.-Y.; Bielack, S. The Care of Adolescents and Young Adults with Cancer: Results of the ESMO/SIOPE Survey. ESMO Open 2017, 2, e000252. [Google Scholar] [CrossRef]
- Convention Entre Le Comité de l’assurance Du Service Des Soins de Santé de l’INAMI et Les Établissements Hospitaliers Pour Le Financement Des Équipes de Référence AJA Visant à Soutenir Des Soins Sur Mesure Aux AJA Atteints d’un Cancer. Note CSS 2023/321 (8 November 2023). Overeenkomst Tussen Het Verzekeringscomité van de Gezondheidszorgdienst van Het RIZIV En de Ziekenhuizen Voor de Financiering van AJA-Referentieteams Met Als Doel Op Maat Gemaakte Zorg Te Ondersteunen Voor AYA’s (Adolescenten En Jongvolwassenen) Die Getroffen Zijn Door Kanker. Nota CSS 2023/321 (8 November 2023). https://www.inami.fgov.be/fr/actualites/cancer-une-prise-en-charge-sur-mesure-pour-les-adolescents-et-jeunes-adultes-grace-a-notre-financement-d-equipes-de-reference-aja ; https://www.riziv.fgov.be/nl/nieuws/zorg-op-maat-voor-adolescenten-en-jongvolwassenen-met-kanker-dankzij-onze-vergoeding-van-aya-referentieteams (accessed 2024-08-22).
- Barr, R.; Ries, L.; Trama, A.; Gatta, G.; Steliarova-Foucher, E.; Stiller, C.; Bleyer, A. A System for Classifying Cancers Diagnosed in Adolescents and Young Adults. Cancer 2020, 126. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E.; Stiller, C.; Lacour, B.; Kaatsch, P. International Classification of Childhood Cancer, Third Edition. Cancer 2005, 103, 1457–1467. [Google Scholar] [CrossRef]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. AYA Site Recode 2020 Revision. 2020. https://seer.cancer.gov/ayarecode/aya-2020.html.
- Berkman, A.M.; Mittal, N.; Roth, M.E. Adolescent and Young Adult Cancers: Unmet Needs and Closing the Gaps. Current Opinion in Pediatrics 2023, 35, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Victorson, D.; Garcia, S.; Sanford, S.; Snyder, M.; Lampert-Okin, S.; Salsman, J. A Qualitative Focus Group Study to Illuminate the Lived Emotional and Social Impacts of Cancer and Its Treatment on Young Adults. Journal of Adolescent and Young Adult Oncology 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- BSPHO: Yves Benoit, An Van Damme, Christophe Chantrain, Anne Uyttebroeck. Cancer Incidence in Belgium, 2010. Special Issue: Cancer in Children and Adolescents, 2013. https://kankerregister.org/en/publicaties/cancer-incidence-belgium-2010-special-issue-cancer-children-and-adolescents.
- Cancer in Children and Adolescents in Belgium, 2004-2020, D/2023/11.846/1; Belgian Cancer Registry, 2023. https://kankerregister.org/en/publicaties/cancer-children-and-adolescents-belgium-2004-2020.
- Cancer in Children and Adolescents in Belgium, 2004-2016; D/2019/11.846/1. Belgian Cancer Registry, 2019. https://kankerregister.org/en/publicaties/cancer-children-and-adolescents-belgium-2004-2016.
- Cancer in Adolescents and Young Adults, Belgium 2004-2022; D/2025/11.846/1; Belgian Cancer Registry: Brussels, 2025; https://kankerregister.org/en/publicaties/cancer-adolescents-and-young-adults-belgium-2004-2022.
- Federale Overheidsdienst Volksgezondheid, Veiligheid van de Voedselketen En Leefmilieu/Service Public Federal Sante Publique, Securite de La Chaine Alimentaire et Environnement. Koninklijk Besluit Houdende Vaststelling van de Normen Waaraan Het Zorgprogramma Voor Oncologische Basiszorg En Het Zorgprogramma Voor Oncologie Moeten Voldoen Om Te Worden Er-Kend/Arrêté Royal Fixant Les Normes Auxquelles Le Programme de Soins de Base En Oncologie et Le Programme de Soins d’oncologie Doivent Répondre Pour Être Agréés.; 2003. https://etaamb.openjustice.be/nl/koninklijk-besluit-van-21-maart-2003_n2003022324 https://etaamb.openjustice.be/fr/arrete-royal-du-21-mars-2003_n2003022324.
- Federale Overheidsdienst Volksgezondheid, Veiligheid van de Voedselketen En Leefmilieu/Service Public Federal Sante Publique, Securite de La Chaine Alimentaire et Environnement. Wet Houdende Diverse Bepalingen Betreffende Gezondheid/Loi Portant Dispositions Diverses En Matière de Santé.; 2006. https://etaamb.openjustice.be/nl/wet-van-13-december-2006_n2006023386.html https://etaamb.openjustice.be/fr/loi-du-13-decembre-2006_n2006023386.
- Statbel. Mortality, Life Expectancy and Causes of Death. 2023. https://statbel.fgov.be/en/themes/population/mortality-life-expectancy-and-causes-death.
- ESMO/SIOPE Adolescents and Young Adults Working Group.
- Centraal Bureau voor de Statistiek (CBS). https://www.cbs.nl/nl-nl (accessed 2025-01-27).
- Integraal Kankercentrum Nederlands (IKNL). https://nkr-cijfers.iknl.nl/ (accessed 2025-01-27).
- Institut National de la Statistique et des Etudes Economiques (Insee). https://www.insee.fr/ (accessed 2025-01-27).
- Institut National du Cancer. https://www.e-cancer.fr/ (accessed 2025-01-27).
- DeStatis Statistisches Bundesamt. https://www.destatis.de/EN/Themes/Society-Environment/Population/ (accessed 2025-01-27).
- Zentrum Für Krebsregisterdaten, Robert Koch Institut. https://www.krebsdaten.de/Krebs/ (accessed 2025-01-27).
- Eurostat’s task force, M. and W. papers. Revision of the European Standard Population. 2013. https://ec.europa.eu/eurostat/documents/3859598/5926869/KS-RA-13-028-EN.PDF.pdf/e713fa79-1add-44e8-b23d-5e8fa09b3f8f?t=1414782757000.
- Ahmad, O.B.; Boschi Pinto, C.; Lopez, A.D. Age Standardization of Rates: A New WHO Standard; GPE Discussion Paper Series: No 31; 2001; pp. 10–12. [Google Scholar]
- EDERER, F.; AXTELL, L.; CUTLER, S. The Relative Survival Rate: A Statistical Methodology. Natl Cancer Inst Monogr 1961, 6, 101–121. [Google Scholar]
- Joinpoint Regression Program, Version 5.0.2. 2023. https://surveillance.cancer.gov/joinpoint/.
- National Cancer Institute - Surveillance Research Program. Number of Joinpoints—Joinpoint Help System. https://surveillance.cancer.gov/ help/joinpoint/setting-parameters/advanced-tab/number-of-joinpoints (accessed 2024-01-02).
- Li, W.; Liang, H.; Wang, W.; Liu, J.; Liu, X.; Lao, S.; Liang, W.; He, J. Global Cancer Statistics for Adolescents and Young Adults: Population Based Study. Journal of Hematology & Oncology 2024, 17, 99. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, L.; Sun, J.; Song, M.; Wang, L.; Yuan, S.; Zhu, Y.; Wan, Z.; Larsson, S.; Tsilidis, K.; Dunlop, M.; Campbell, H.; Rudan, I.; Song, P.; Theodoratou, E.; Ding, K.; Li, X. Global Trends in Incidence, Death, Burden and Risk Factors of Early-Onset Cancer from 1990 to 2019. BMJ Oncology 2023, 2, e000049. [Google Scholar] [CrossRef]
- Ugai, T.; Sasamoto, N.; Lee, H.-Y.; Ando, M.; Song, M.; Tamimi, R.M.; Kawachi, I.; Campbell, P.T.; Giovannucci, E.L.; Weiderpass, E.; Rebbeck, T.R.; Ogino, S. Is Early-Onset Cancer an Emerging Global Epidemic? Current Evidence and Future Implications. Nature Reviews Clinical Oncology 2022, 19, 656–673. [Google Scholar] [CrossRef]
- Toss, A.; Quarello, P.; Mascarin, M.; Banna, G.L.; Zecca, M.; Cinieri, S.; Peccatori, F.A.; Ferrari, A. Cancer Predisposition Genes in Adolescents and Young Adults (AYAs): A Review Paper from the Italian AYA Working Group. Current Oncology Reports 2022, 24, 843–860. [Google Scholar] [CrossRef]
- Finkelstein, D.M.; Horick, N.K.; Ramchandani, R.; Boyd, K.L.; Rana, H.Q.; Bychkovsky, B.L. Are Rare Cancer Survivors at Elevated Risk of Subsequent New Cancers? BMC Cancer 2019, 19, 166. [Google Scholar] [CrossRef]
- Macq, G.; Silversmit, G.; Verdoodt, F.; Van Eycken, E. The Epidemiology of Multiple Primary Cancers in Belgium (2004–2017): Incidence, Proportion, Risk, Stage and Impact on Relative Survival Estimates. BMC Cancer 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Muscat, J.E.; Chinchilli, V.M.; Behura, C.G. Trends in Cancer Incidence and Mortality in US Adolescents and Young Adults, 2016–2021. Cancers 2024, 16. [Google Scholar] [CrossRef]
- Voeltz, D.; Baginski, K.; Hornberg, C.; Hoyer, A. Trends in Incidence and Mortality of Early-Onset Cancer in Germany between 1999 and 2019. European Journal of Epidemiology 2024, 39, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W. F.; Pfeiffer, R.M.; Tucker, M.A.; Rosenberg, P.S. Divergent Cancer Pathways for Early-Onset and Late-Onset Cutaneous Malignant Melanoma. Cancer 2009, 115, 4176–4185. [Google Scholar] [CrossRef]
- An, S.; Kim, K.; Moon, S.; Ko, K.-P.; Kim, I.; Lee, J.; Park, S. Indoor Tanning and the Risk of Overall and Early-Onset Melanoma and Non-Melanoma Skin Cancer: Systematic Review and Meta-Analysis. Cancers 2021, 13, 5940. [Google Scholar] [CrossRef]
- Del Marmol, V. Prevention and Screening of Melanoma in Europe: 20 Years of the Euromelanoma Campaign. Journal of the European Academy of Dermatology and Venereology 2022, 36, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Stichting Tegen Kanker - Fondation Contre le Cancer. Ondanks preventie neemt huidkanker toe - Malgré la prévention, les cancers de la peau sont en hausse. https://kanker.be/resource/ondanks-preventie-neemt-huidkanker-toe/ - https://cancer.be/ressource/malgre-la-prevention-les-cancers-de-la-peau-sont-en-hausse/ (accessed 2025-02-02).
- LeClair, K.; Bell, K.; Furuya-Kanamori, L.; Doi, S.; Francis, D. Evaluation of Gender Inequity in Thyroid Cancer Diagnosis: Differences by Sex in US Thyroid Cancer Incidence Compared With a Meta-Analysis of Subclinical Thyroid Cancer Rates at Autopsy. JAMA Internal Medicine 2021, 181. [Google Scholar] [CrossRef]
- van der Meer, D.J.; Karim-Kos, H.E.; van der Mark, M.; Aben, K.K.H.; Bijlsma, R.M.; Rijneveld, A.W.; van der Graaf, W.T.A.; Husson, O. Incidence, Survival, and Mortality Trends of Cancers Diagnosed in Adolescents and Young Adults (15-39 Years): A Population-Based Study in The Netherlands 1990-2016. Cancers 2020, 12, 3421. [Google Scholar] [CrossRef]
- Iglesias, M.L.; Schmidt, A.; Ghuzlan, A.A.; Lacroix, L.; Vathaire, F. de; Chevillard, S.; Schlumberger, M. Radiation Exposure and Thyroid Cancer: A Review. Archives of Endocrinology and Metabolism 2017, 61. [Google Scholar] [CrossRef]
- Massimino, M.; Evans, D.; Podda, M.; Spinelli, C.; Collini, P.; Pizzi, N.; Bleyer, A. Thyroid Cancer in Adolescents and Young Adults. Pediatric Blood & Cancer 2018, 65, e27025. [Google Scholar] [CrossRef]
- Zaridze, D.; Maximovitch, D.; Smans, M.; Stilidi, I. Thyroid Cancer Overdiagnosis Revisited. Cancer Epidemiol. 2021, 74, 102014. [Google Scholar] [CrossRef] [PubMed]
- Van den Bruel, A.; Francart, J.; Dubois, C.; Adam, M.; Vlayen, J.; De Schutter, H.; Stordeur, S.; Decallonne, B. Regional Variation in Thyroid Cancer Incidence in Belgium Is Associated With Variation in Thyroid Imaging and Thyroid Disease Management. The Journal of Clinical Endocrinology & Metabolism 2013, 98, 4063–4071. [Google Scholar] [CrossRef]
- Levine, O.; Zbuk, K. Colorectal Cancer in Adolescents and Young Adults: Defining a Growing Threat. Pediatric Blood & Cancer 2019, 66, e27941. [Google Scholar] [CrossRef]
- Connell, L.C.; Mota, J.M.; Braghiroli, M.I.; Hoff, P.M. The Rising Incidence of Younger Patients With Colorectal Cancer: Questions About Screening, Biology, and Treatment. Current Treatment Options in Oncology 2017, 18, 23. [Google Scholar] [CrossRef]
- Frostberg, E.; Rahr, H.B. Clinical Characteristics and a Rising Incidence of Early-Onset Colorectal Cancer in a Nationwide Cohort of 521 Patients Aged 18-40 Years. Cancer Epidemiology 2020, 66, 101704. [Google Scholar] [CrossRef]
- Vuik, F.E.; Nieuwenburg, S.A.; Bardou, M.; Lansdorp-Vogelaar, I.; Dinis-Ribeiro, M.; Bento, M.J.; Zadnik, V.; Pellisé, M.; Esteban, L.; Kaminski, M.F.; Suchanek, S.; Ngo, O.; Májek, O.; Leja, M.; Kuipers, E.J.; Spaander, M.C. Increasing Incidence of Colorectal Cancer in Young Adults in Europe over the Last 25 Years. Gut 2019, 68, 1820–1826. [Google Scholar] [CrossRef]
- Danial, D.; Youssef, E.D.; Maryam, B.M.; Mohammad, A.; Moein, B.M.; Liliane, D. Risk Factors of Young-Onset Colorectal Cancer: Analysis of a Large Population-Based Registry. Canadian Journal of Gastroenterology and Hepatology 2022, 2022, 3582443. [Google Scholar] [CrossRef] [PubMed]
- Hua, H.; Jiang, Q.; Sun, P.; Xu, X. Risk Factors for Early-Onset Colorectal Cancer: Systematic Review and Meta-Analysis. Frontiers in Oncology 2023, 13, 1132306. [Google Scholar] [CrossRef]
- Tricoli, J.; Bleyer, A. Adolescent and Young Adult Cancer Biology. The Cancer Journal 2018, 24, 267–274. [Google Scholar] [CrossRef]
- Cervical cancer screening program. https://baarmoederhalskanker.bevolkingsonderzoek.be/en (accessed 2025-02-02).
- Johanne Spanggaard Piltoft, L.C.; Larsen, S. B.; Dalton, S. O.; Johansen, C.; Baker, J. L.; Cederkvist, L.; Andersen, I. Early Life Risk Factors for Testicular Cancer: A Case-Cohort Study Based on the Copenhagen School Health Records Register. Acta Oncologica 2017, 56, 220–224. [Google Scholar] [CrossRef]
- Del Risco Kollerud, R.; Ruud, E.; Haugnes, H.S.; Cannon-Albright, L.A.; Thoresen, M.; Nafstad, P.; Vlatkovic, L.; Blaasaas, K.G.; Næss, Ø.; Claussen, B. Family History of Cancer and Risk of Paediatric and Young Adult’s Testicular Cancer: A Norwegian Cohort Study. British Journal of Cancer 2019, 120, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- Garolla, A.; Vitagliano, A.; Muscianisi, F.; Valente, U.; Ghezzi, M.; Andrisani, A.; Ambrosini, G.; Foresta, C. Role of Viral Infections in Testicular Cancer Etiology: Evidence From a Systematic Review and Meta-Analysis. Frontiers in Endocrinology 2019, 10. [Google Scholar] [CrossRef]
- Fénichel, P.; Chevalier, N. Is Testicular Germ Cell Cancer Estrogen Dependent? The Role of Endocrine Disrupting Chemicals. Endocrinology 2019, 160, 2981–2989. [Google Scholar] [CrossRef] [PubMed]
- Hermansen, M.; Hjelmborg, J.; Thinggaard, M.; Znaor, A.; Skakkebæk, N.E.; Lindahl-Jacobsen, R. Smoking and Testicular Cancer: A Danish Nationwide Cohort Study. Cancer Epidemiology 2025, 95, 102746. [Google Scholar] [CrossRef]
- Gaddam, S.J.; Chestnut, G.T. Testicle Cancer.; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Hochberg, J.; Waxman, I.M.; Kelly, K.M.; Morris, E.; Cairo, M.S. Adolescent Non-Hodgkin Lymphoma and Hodgkin Lymphoma: State of the Science. British Journal of Haematology 2009, 144, 24–40. [Google Scholar] [CrossRef]
- Brenner, H.; Gondos, A.; Pulte, D. Ongoing Improvement in Long-Term Survival of Patients with Hodgkin Disease at All Ages and Recent Catch-up of Older Patients. Blood 2008, 111, 2977–2983. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Pang, W.S.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M.; Wong, M.C.S.; NCD Global Health Research Group, A. of P. R. U. (APRU). Incidence, Mortality, Risk Factors, and Trends for Hodgkin Lymphoma: A Global Data Analysis. Journal of Hematology & Oncology 2022, 15, 57. [Google Scholar] [CrossRef]
- Murphy, B.L.; Day, C.N.; Hoskin, T.L.; Habermann, E.B.; Boughey, J.C. Adolescents and Young Adults with Breast Cancer Have More Aggressive Disease and Treatment than Patients in Their Forties. Ann Surg Oncol 2019, 26, 3920–3930. [Google Scholar] [CrossRef]
- Johnson, R.H.; Anders, C.K.; Litton, J.K.; Ruddy, K.J.; Bleyer, A. Breast Cancer in Adolescents and Young Adults. Pediatr Blood Cancer 2018, 65, e27397. [Google Scholar] [CrossRef]
- Kumar, R.; Saini, S.; Ganguly, N.K. Year-Round Breast Cancer Awareness: Empowering Young Women in the Fight against Breast Cancer. Indian Journal of Medical Research 2023, 158. [Google Scholar] [CrossRef]
- Kotsopoulos, J.; Lubinski, J.; Moller, P.; Lynch, H.T.; Singer, C.F.; Eng, C.; Neuhausen, S.L.; Karlan, B.; Kim-Sing, C.; Huzarski, T.; Gronwald, J.; McCuaig, J.; Senter, L.; Tung, N.; Ghadirian, P.; Eisen, A.; Gilchrist, D.; Blum, J.L.; Zakalik, D.; Pal, T.; Sun, P.; Narod, S.A. Hereditary Breast Cancer Clinical Study Group. Timing of Oral Contraceptive Use and the Risk of Breast Cancer in BRCA1 Mutation Carriers. Breast Cancer Res Treat 2014, 143, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Lalloo, F.; Varley, J.; Moran, A.; Ellis, D.; O’dair, L.; Pharoah, P.; Antoniou, A.; Hartley, R.; Shenton, A.; Seal, S.; Bulman, B.; Howell, A.; Evans, D. BRCA1, BRCA2 and TP53 Mutations in Very Early-Onset Breast Cancer with Associated Risks to Relatives. Eur J Cancer 2006, 42, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Trama, A.; Bernasconi, A.; McCabe, M.G.; Guevara, M.; Gatta, G.; Botta, L.; Group, the Rarecare. W; Ries, L.; Bleyer, A. Is the Cancer Survival Improvement in European and American Adolescent and Young Adults Still Lagging behind That in Children? Pediatric Blood & Cancer 2019, 66, e27407. [Google Scholar] [CrossRef]
- Keegan, T.H.M.; Ries, L.A.G.; Barr, R.D.; Geiger, A.M.; Dahlke, D.V.; Pollock, B.H.; Bleyer, W.A.; for the National Cancer Institute Next Steps for Adolescent and Young Adult Oncology Epidemiology Working Group. Comparison of Cancer Survival Trends in the United States of Adolescents and Young Adults with Those in Children and Older Adults. Cancer 2016, 122, 1009–1016. [Google Scholar] [CrossRef]
- Moke, D.; Tsai, K.-Y.; Hamilton, A.; Hwang, A.; Liu, L.; Freyer, D.; Deapen, D. Emerging Cancer Survival Trends, Disparities, and Priorities in Adolescents and Young Adults: A California Cancer Registry-Based Study. JNCI cancer spectrum 2019, 3, pkz031. [Google Scholar] [CrossRef]
Figure 1.
Relative frequencies (%) of cancer types, by age group for (a) male and (b) female cancer patients, Belgium, 2004-2020.
Figure 1.
Relative frequencies (%) of cancer types, by age group for (a) male and (b) female cancer patients, Belgium, 2004-2020.
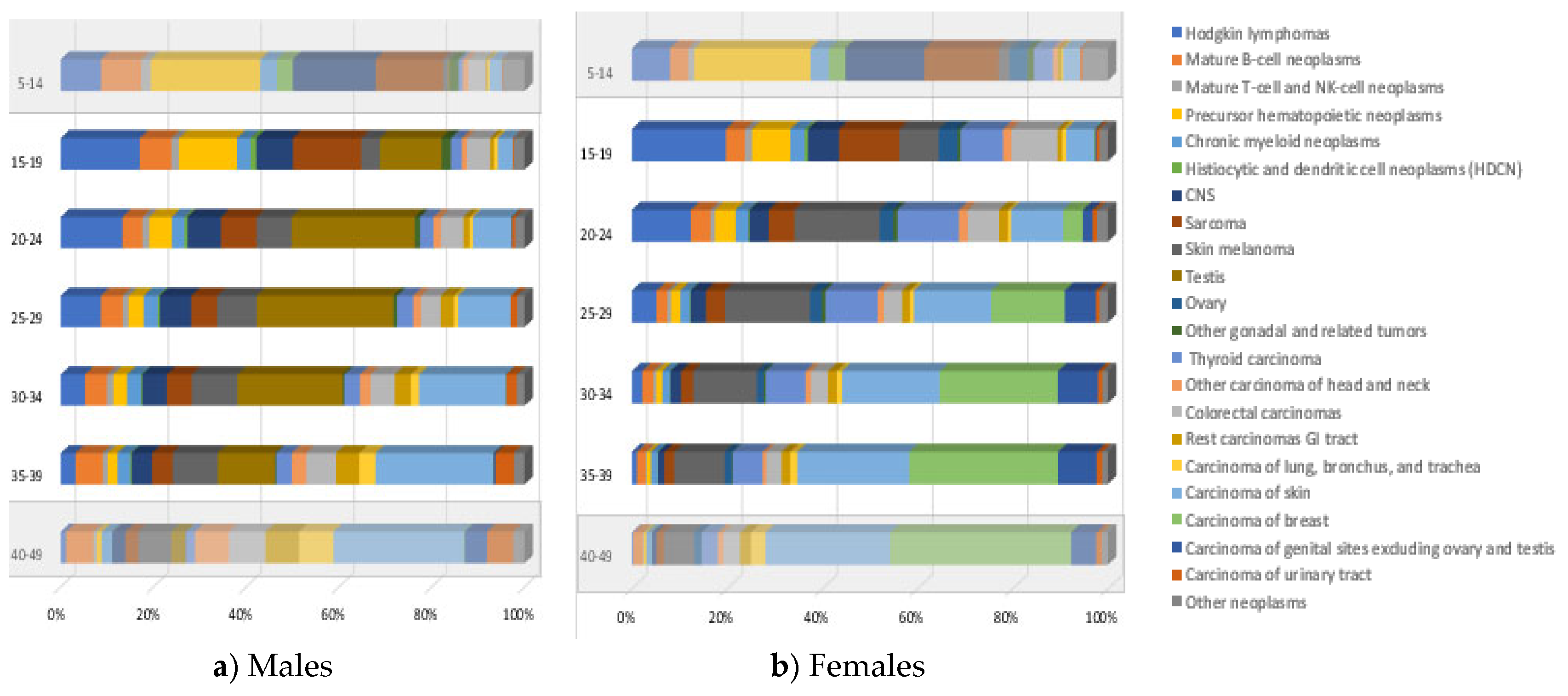
Figure 2.
Cancer-causes of death in children (5-14 years), AYA (15-39 years), older adults (40-49 years), Belgium, 2004-2019.
Figure 2.
Cancer-causes of death in children (5-14 years), AYA (15-39 years), older adults (40-49 years), Belgium, 2004-2019.
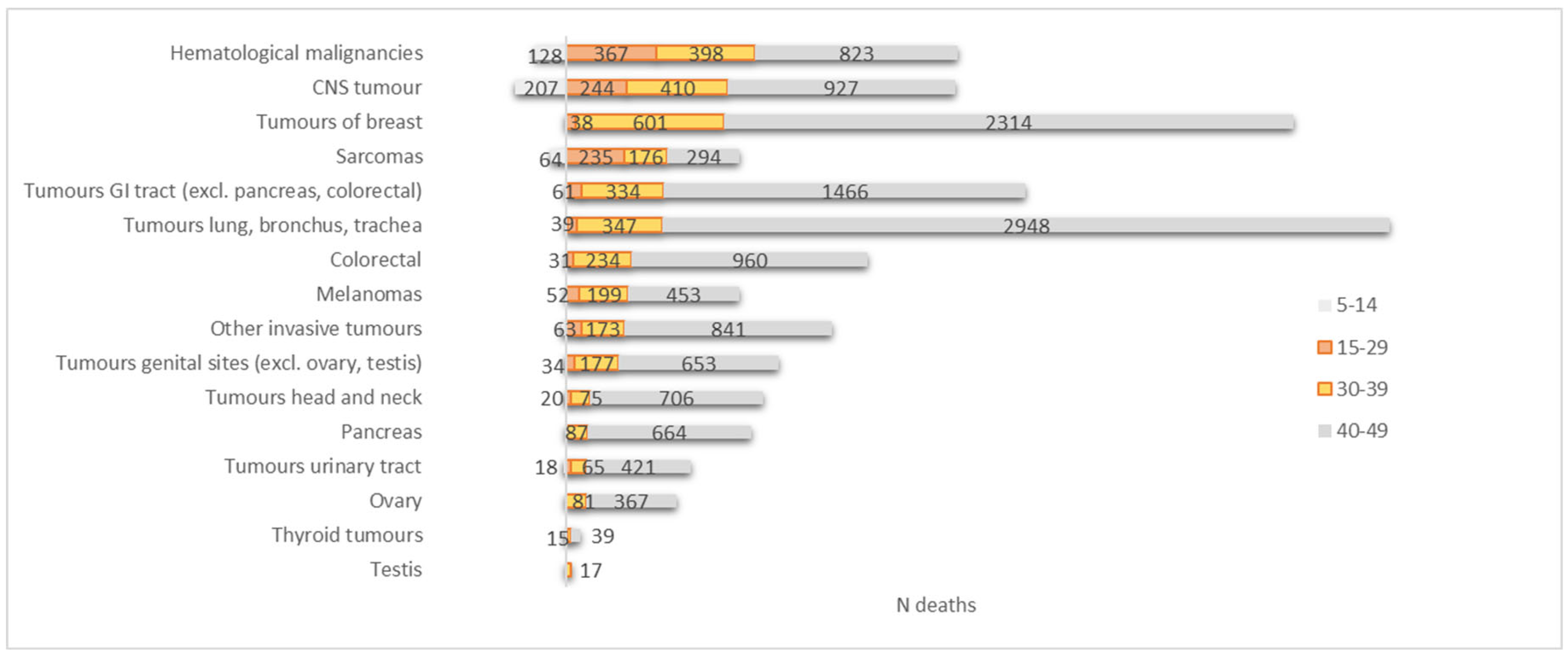
Figure 3.
Trends in cancer incidence rates for all cancers combined, 2004 to 2020, Belgium. Rates are age adjusted to the 2013 European standard population. (a) Children aged 5-14 years, (b) AYA aged 15-29 years, (c) AYA aged 30-39 years, (d) adults aged 40-49 years.
Figure 3.
Trends in cancer incidence rates for all cancers combined, 2004 to 2020, Belgium. Rates are age adjusted to the 2013 European standard population. (a) Children aged 5-14 years, (b) AYA aged 15-29 years, (c) AYA aged 30-39 years, (d) adults aged 40-49 years.
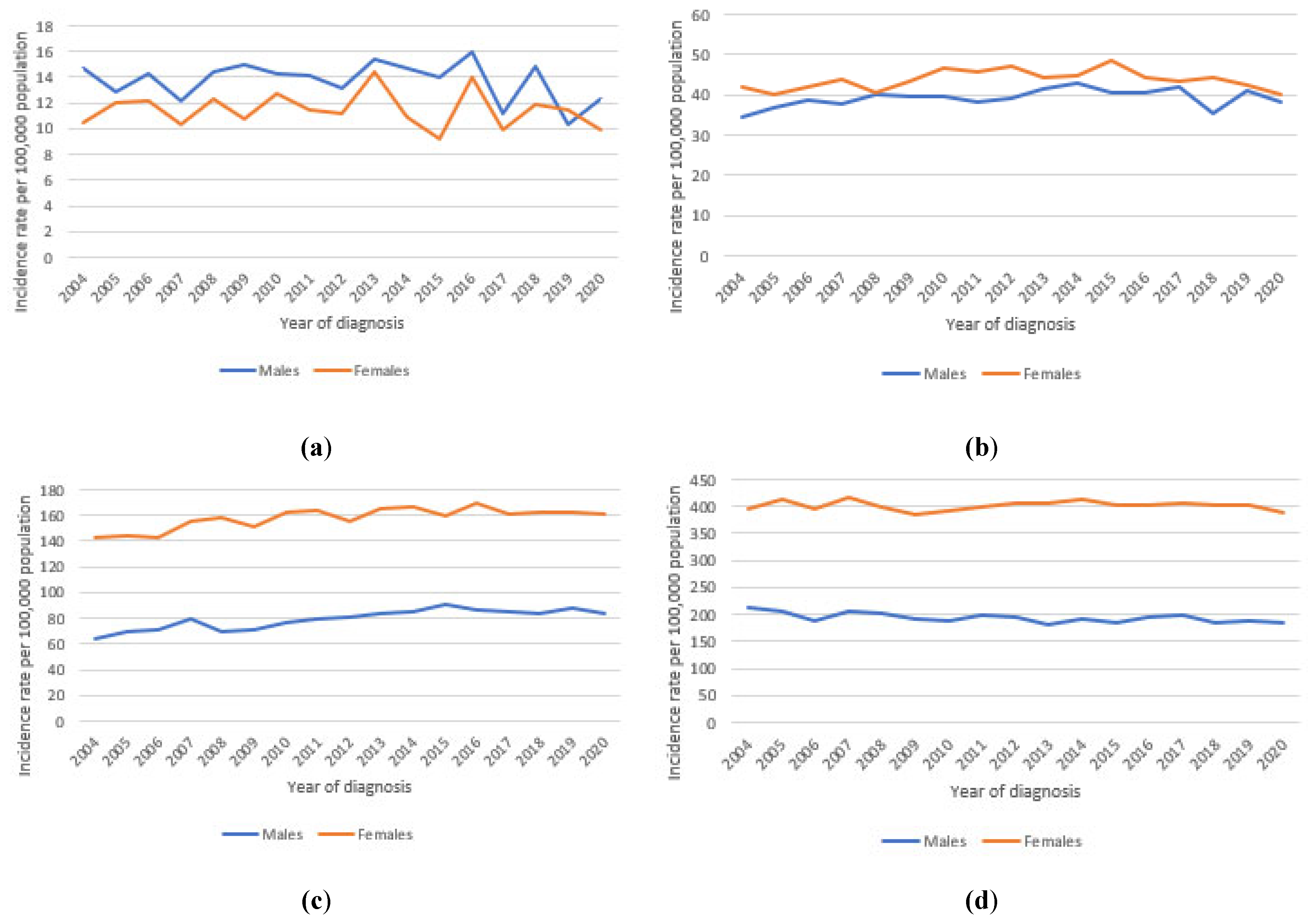
Figure 4.
Trends in cancer mortality rates for all cancers combined, 2004 to 2019, Belgium. Rates are age adjusted to the 2013 European standard population. (a) Children aged 5-14 years, (b) AYA aged 15-29 years, (c) AYA aged 30-39 years, (d) older adults aged 40-49 years.
Figure 4.
Trends in cancer mortality rates for all cancers combined, 2004 to 2019, Belgium. Rates are age adjusted to the 2013 European standard population. (a) Children aged 5-14 years, (b) AYA aged 15-29 years, (c) AYA aged 30-39 years, (d) older adults aged 40-49 years.
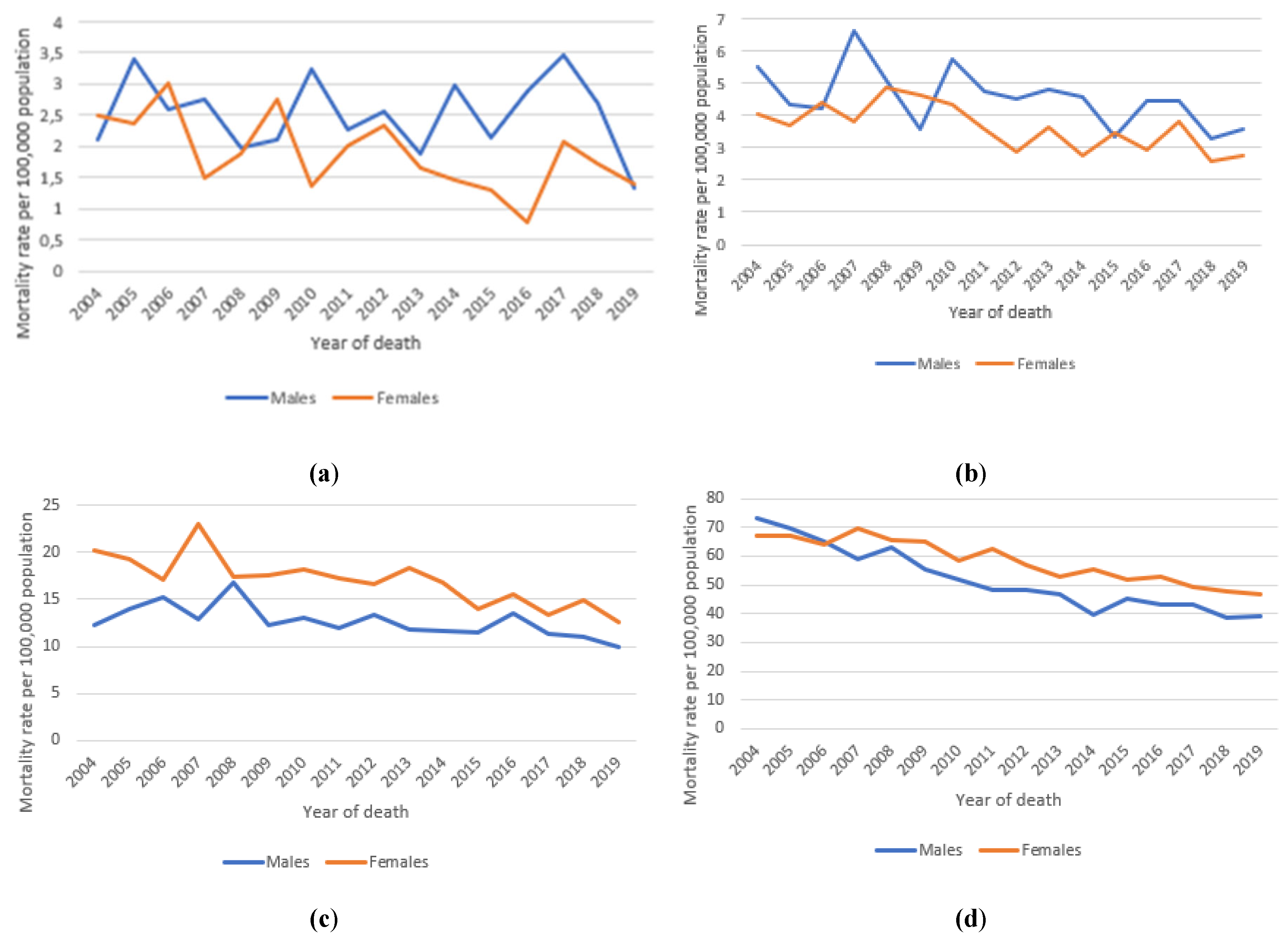
Figure 5.
5- and 10-year relative survival (with 95% CI) per cancer type, Belgium, 2004-2020.
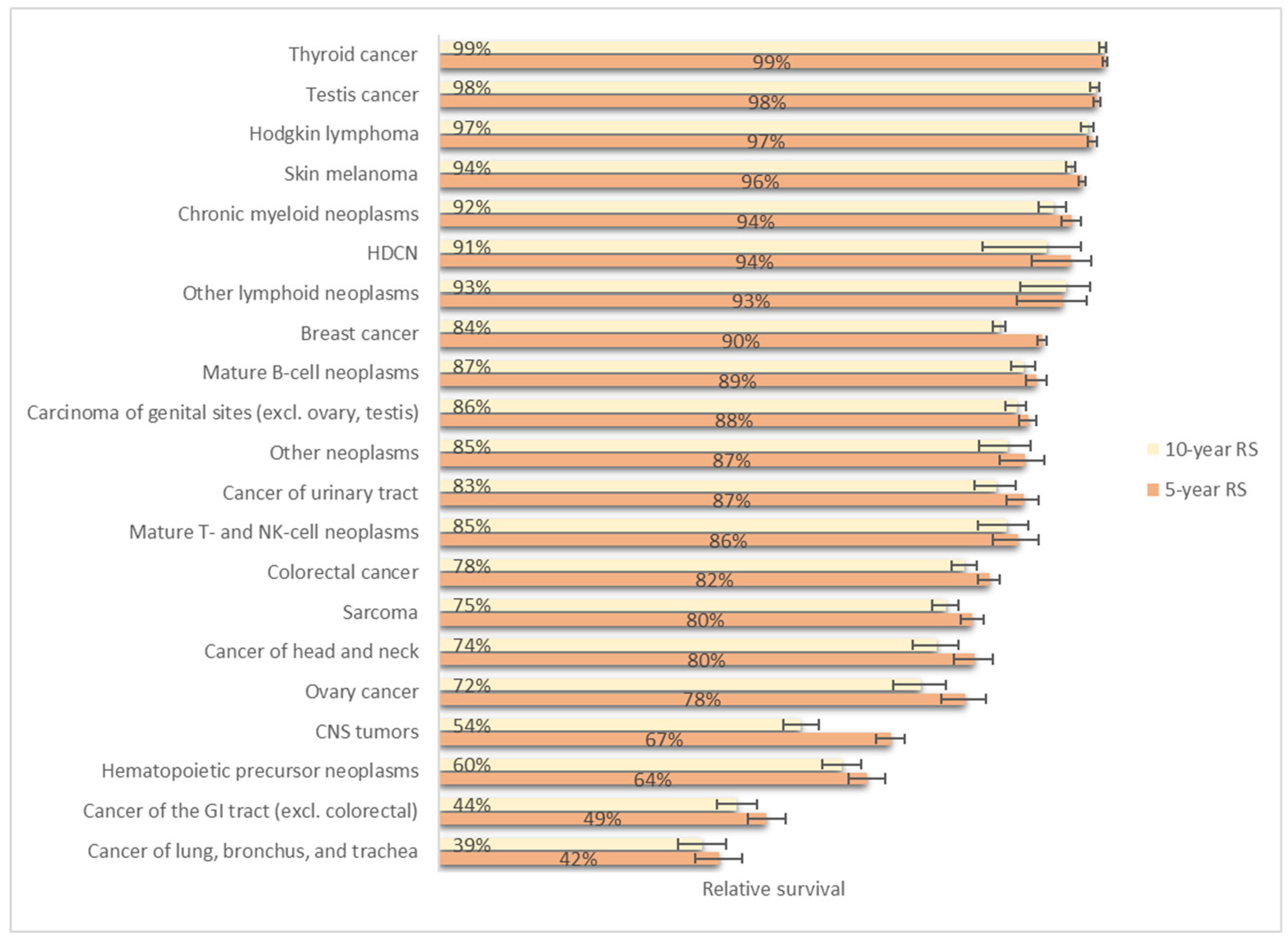
Figure 6.
The ten most 5-year prevalent cancer types (excl. carcinoma of skin) in AYA, (a) per sex, AYA 15-39 years, (b) both sexes, per age group (children (5-14 years), AYA (15-29 years, and 30-39 years), older adults (40-49 years)), Belgium, 31 Dec 2020.
Figure 6.
The ten most 5-year prevalent cancer types (excl. carcinoma of skin) in AYA, (a) per sex, AYA 15-39 years, (b) both sexes, per age group (children (5-14 years), AYA (15-29 years, and 30-39 years), older adults (40-49 years)), Belgium, 31 Dec 2020.
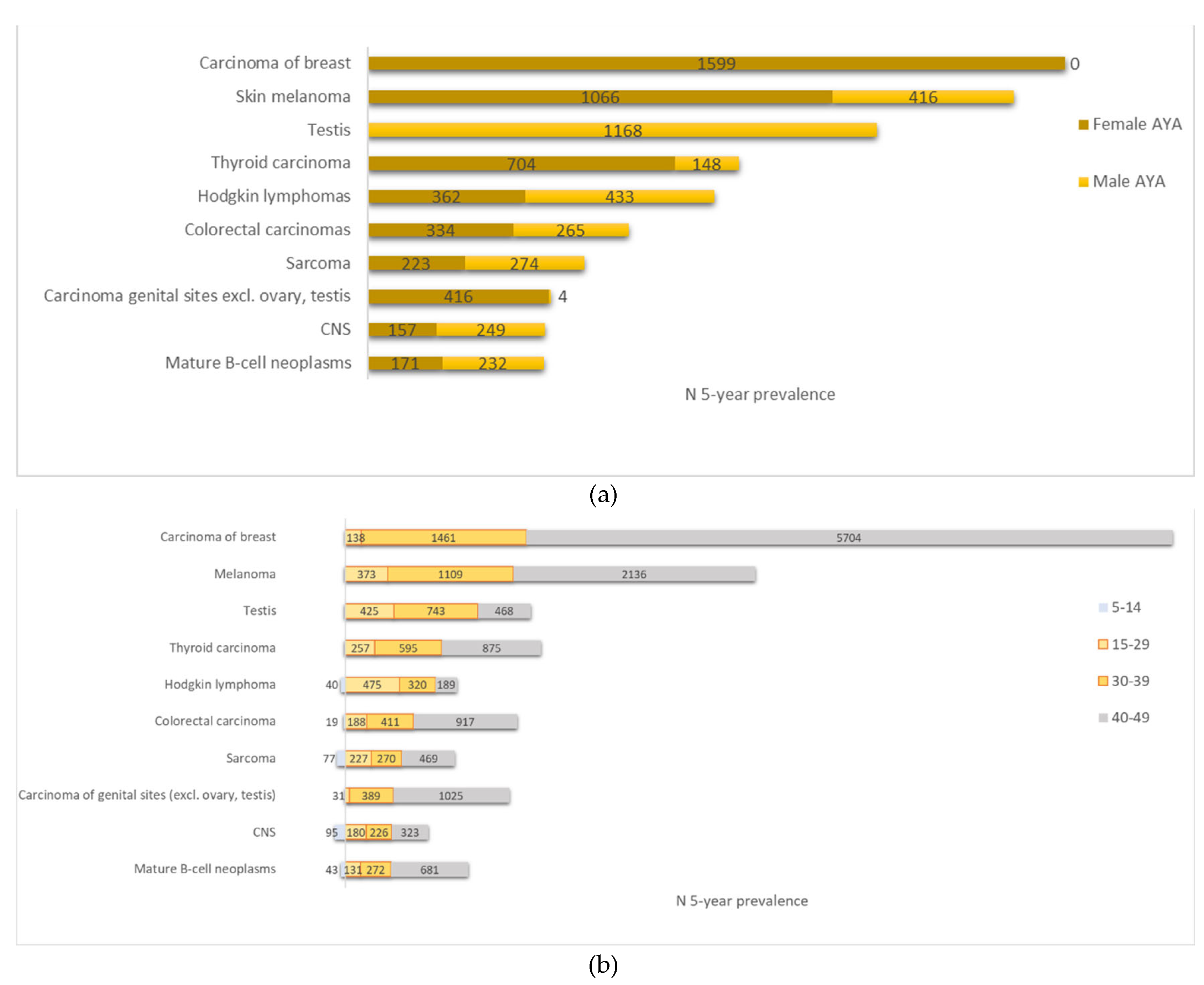
Figure 7.
Comparison of Belgian incidence and mortality rates in 2019 with those of the Netherlands, France, and Germany. Rates are age adjusted to the 2013 European standard population. (a) Incidence all cancers, (b) Mortality all cancers, (c) Incidence selected cancer types.
Figure 7.
Comparison of Belgian incidence and mortality rates in 2019 with those of the Netherlands, France, and Germany. Rates are age adjusted to the 2013 European standard population. (a) Incidence all cancers, (b) Mortality all cancers, (c) Incidence selected cancer types.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



