
Submitted:
30 December 2024
Posted:
03 January 2025
You are already at the latest version
Abstract
Background: Coagulopathies are common in patients with septic shock, trauma, or post-cardiac arrest syndrome, resulting from endothelial injury due to hypoperfusion in shock-induced endotheliopathy (SHINE). However, the prognostic efficacy of SHINE-associated coagulopathies has not been studied widely and there is no assessment of prognostic value for coagulation parameters measured by rotational thromboelastometry (ROTEM®) in this group of patients. Methods: We retrospectively analyzed data from consecutive adult patients with SHINE who underwent ROTEM® testing within 72 hours of admission to our mixed medical-surgical ICU from January 2020 to December 2023. We evaluated the association between clotting times (CTs) in the extrinsic (EXTEM) and intrinsic (INTEM) coagulation pathways and 30-day mortality. Results: There were 114 patients included (mean age of 49.3 years, 66.7% males), with 30-day mortality rate of 45.6%. CT EXTEM and CT INTEM were significantly prolonged in non-survivors compared to survivors (median [IQR]; 95.5 [72.0-176.3] vs. 74.5 [65.8-83.5] seconds, p < 0.001 and median [IQR]; 268.0 [229.0-361.5] vs. 201.0 [175.8-251.0] seconds, p <0.001, respectively). In multivariable logistic regression, both CT EXTEM and CT INTEM were independently associated with a higher risk of mortality, even after adjusting for age and APACHE II scores (OR = 1.024; 95% CI = 1.011-1.038; p < 0.001 for EXTEM; OR 1.006; 95% CI = 1.001-1.010; p = 0.009 for INTEM) and in ROC analysis demonstrated predictive value for 30-day mortality, with AUC values of 0.727, p < 0.001 and 0.741, p < 0.001, respectively. Conclusions: Prolonged CTs in EXTEM and INTEM are independent predictors of 30-day mortality in critically ill patients with SHINE-associated coagulopathies. ROTEM® parameters should be considered as early predictors of mortality in this group of patients.
Keywords:
rotational thromboelastometry
; coagulopathy
; endotheliopathy
; sepsis
; trauma
; cardiac arrest
1. Introduction
Coagulopathies in critically ill patients are complex conditions that can lead to frequent and serious complications, resulting in increased morbidity and mortality, with higher healthcare costs. The pathogenesis, laboratory test results, clinical presentation, and outcomes may differ significantly depending on the specific cause of coagulation abnormalities, making it crucial to accurately diagnose the underlying condition and initiate appropriate treatment as soon as possible. Coagulopathies can be classified into two main types: thrombotic, which may result in hypercoagulation and impaired fibrinolysis, and hemorrhagic, which may present with both hypocoagulability and hyperfibrinolysis [1]. Numerous altered coagulation parameters can be easily measured, such as prothrombin time (PT), International Normalized Ratio (INR), activated partial thromboplastin time (aPTT), fibrinogen levels, thrombocytopenia, and elevated concentrations of fibrin split products [2]. Prolonged PT and aPTT occur in 14%–28% of general intensive care patients, with higher frequency in trauma patients, and are strong, independent predictors of mortality [3]. However, a more detailed understanding of coagulation processes using viscoelastic hemostatic assays (VHAs), such as rotational thromboelastometry (ROTEM®) or thromboelastography (TEG®), is necessary to detect the specific type of coagulopathy at an early stage.
There are several conditions particularly associated with coagulopathies in critically ill patients, such as septic shock, trauma, and Post-Cardiac Arrest Syndrome (PCAS). All of these conditions share common pathologies – hypoperfusion, endothelial damage, and glycocalyx shedding – and are known as SHock-Induced Endotheliopathy (SHINE) [4]. Physiologically, the endothelium and glycocalyx counterbalance the prothrombotic properties of blood. However, their disruption due to hypoxemia caused by shock may initially lead to thrombotic complications in microvasculature by exposing the subendothelial layer and later to a hypocoagulable state with hyperfibrinolysis through release of their anti-thrombotic mediators [5].
In septic shock, there is a life-threatening host response to infection that can result in Sepsis-Induced Coagulopathy (SIC) or even Disseminated Intravascular Coagulation (DIC) [6]. Proinflammatory cytokines enhance the induction of Tissue Factor (TF) on endothelium and monocytes, which activates coagulation and leads to excessive thrombin generation, resulting in the conversion of fibrinogen into an insoluble fibrin network [1]. Additionally, fibrinolysis can be impaired by increased production and release of Plasminogen Activator Inhibitor-1 (PAI-1), Thrombin-Activable Fibrinolysis Inhibitor (TAFI) and decreased levels of tissue Plasminogen Activator (tPA). Prakash S. et al. (2015) demonstrated that inhibition of fibrinolysis, which can be detected by rotational thromboelastometry, increases the risk of Multi-Organ Dysfunction Syndrome (MODS) in septic shock [7]. Initially, in SIC, the interaction between immune and hemostatic systems activates the endothelium and releases extracellular vesicles (EVs) containing TF and phosphatidylserine (PS), leading to hypercoagulable and hypofibrinolytic state. Therefore, in some cases, coagulation abnormalities may only be reflected by VHAs, as conventional coagulation tests (CCTs) are more sensitive to the initiation rather than the propagation and lysis phases of hemostasis [8,9,10,11]. The interaction between immune cells, Neutrophil Extracellular Traps (NETs), Damage-Associated Molecular Patterns (DAMPs), Pathogen-Associated Molecular Patterns (PAMPs), Interleukin-8 (IL-8) and coagulation factors has been termed “immunothrombosis”, which leads to microthrombi formation [1]. In the early stages, hypercoagulability may be a beneficial process that limits the infection spread, but further progression causes DIC, resulting in widespread tissue damage [12]. However, the initial phase of evolution from SIC to DIC is often difficult to identify. Czempik et al. (2024) showed that coagulopathies detected by rotational thromboelastometry occur more often in the non-survivor group of septic patients [13].
Even up to 40-50% patients with massive bleeding following trauma will die, either early from hemorrhage or later from multiple organ failure [14]. In trauma associated with bleeding, profound hypotension, and severe coagulopathies often occur, and in some cases, are associated with a 5-fold increase in mortality [15]. The coagulation abnormalities in trauma consist of acute traumatic coagulopathy (ATC) and trauma-induced coagulopathy (TIC). It has been known for decades that the ATC results from the loss of plasma clotting factors and platelets, as well as iatrogenic dilutional effects from excessive crystalloid infusion [16,17]. However, the later studies have found that additional coagulation abnormalities, such as TIC, may occur and are associated with very high mortality. The main drivers of TIC are endothelial injury, glycocalyx shedding, and the release of thrombomodulin-thrombin complex, which reacts with the Endothelial Protein C Receptor (EPCR) to form activated Protein C (aPC). APC degrades the active forms of Factor V, Factor VIII, and PAI-1 [18]. Furthermore, the consumption of fibrinogen and the exhaustion or dysfunction of platelets play a major role in the progression of hypocoagulation. This results in prolonged initiation of clot formation and auto-heparinization [19]. Moreover, damage to the endothelium causes the systemic release of Weibel-Palade bodies containing tPA and the formation of fibrinogen degradation products (FDP), meaningly contributing to hyperfibrinolysis [17]. It is well-known that prolonged PT is associated with higher mortality in trauma patients, but CCTs are time-consuming, making them unfit for direct therapeutic management in emergent situations [20,21]. Hence, VHAs have become more widely used in these clinical scenarios over the past few years. Smith A. et al. (2020) showed that abnormalities in the APTEM pathway, measured by rotational thromboelastometry, significantly predict mortality [22].
Cardiac arrest (CA) is a serious danger to human life, with very high mortality. Less than 10% of patients who experience out-of-hospital cardiac arrest (OHCA) and less than 20% of those with in-hospital cardiac arrest (IHCA) survive to hospital discharge [23]. During CA, severe hypoxia and acidosis, which affect every tissue in the body, can cause damage to vascular endothelial cells. Additionally, after Return of Spontaneous Circulation (ROSC) the reperfusion begins generating the Reactive Oxygen Species (ROS), which intensify the acute inflammatory response. The injured endothelium becomes prothrombotic and simultaneously hyperfibrinolytic due to the release of tPA from Weibel-Palade bodies. These changes manifest as PCAS, resembling sepsis-like symptoms such as systemic inflammatory response, capillary leakage, and dysregulation of hemostasis [23,24,25]. Numerous studies have demonstrated that cardiac arrest-associated coagulopathy (CAAC) is related to higher mortality [26,27,28].
The coagulation process involves traditionally recognized intrinsic and extrinsic pathways, each crucial for hemostasis. Despite the newer cell-based model of coagulation, these pathways are still recognized as valuable diagnostic measures and are used in both VHAs and CCTs. However, CCTs often fail to provide timely and comprehensive information necessary for rapid decision-making, which is especially relevant in the ICU. CCTs have limited ability to extensively characterize the hemostatic profile and forecast thrombotic or bleeding complications in critically ill patients. They cannot assess clot strength and stability, as these tests measure the early phase of fibrin polymerization, when only 5% of thrombin generation occurs [29,30,31]. In addition, plasma samples are used for conducting CCTs, meaning that information regarding platelet function, fibrinolysis, and hypercoagulability is not provided [32]. VHAs are more modern coagulation tests and include rotational thromboelastography (TEG®) and rotational thromboelastometry (ROTEM®). They utilize whole blood samples and allow for the assessment of dynamic changes in clot viscoelastic properties by using graphs that show the amplitude representing clot formation and lysis over time [33]. Therefore, rotational thromboelastometry is regarded as faster and more versatile than CCTs for diagnosing and managing complex coagulation disorders in critically ill patients [34]. While numerous studies have validated the role of ROTEM® in diagnosing coagulopathies, its prognostic value, specifically the comparative analysis of intrinsic and extrinsic pathways in predicting short-term mortality, has not been widely studied in patients with endothelial injury due to shock caused by septic shock, trauma, or cardiac arrest [3].
This study aims to compare the prognostic efficacy of intrinsic and extrinsic coagulation pathway parameters assessed by rotational thromboelastometry in relation to 30-day mortality in critically ill patients with SHINE.
2. Materials and Methods
We conducted a single-center retrospective analysis of patients hospitalized in a mixed medical-surgical intensive care unit (ICU) at the University Hospital in Krakow, Poland (44 beds, approximately 900 admissions annually). The observation period was from January 2020 to December 2023, and the study included 114 critically ill patients.
The inclusion criteria were patients at least 18 years of age, requiring support for at least one organ, and having undergone rotational thromboelastometry within 72 hours of ICU admission. The exclusion criteria included known liver disease and conditions other than septic shock, trauma, or PCAS as reasons for admission to ICU.
Sepsis was defined according to the third international consensus criteria for sepsis and the septic shock was defined as sepsis in patients who required vasopressor support [6]. Additionally, in our study, a procalcitonin > 0.5 ng/mL was used to confirm the presence of systemic infection. Trauma was defined as an injury to at least two organs, with each organ injury requiring hospitalization. CA was defined as the cessation of effective blood flow due to either asystole, pulseless electrical activity, pulseless tachycardia, or ventricular fibrillation.
The study was approved by the Bioethics Committee of the Jagiellonian University in Krakow, Poland, on June 20, 2024 (No. 118.0043.1.224.2024), and conducted in compliance with the World Medical Association (WMA) Declaration of Helsinki (1975, as revised in 2013). The requirement for specific informed consent form (ICF) was waived because this was a retrospective observational study. The study was conducted in adherence to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [35].
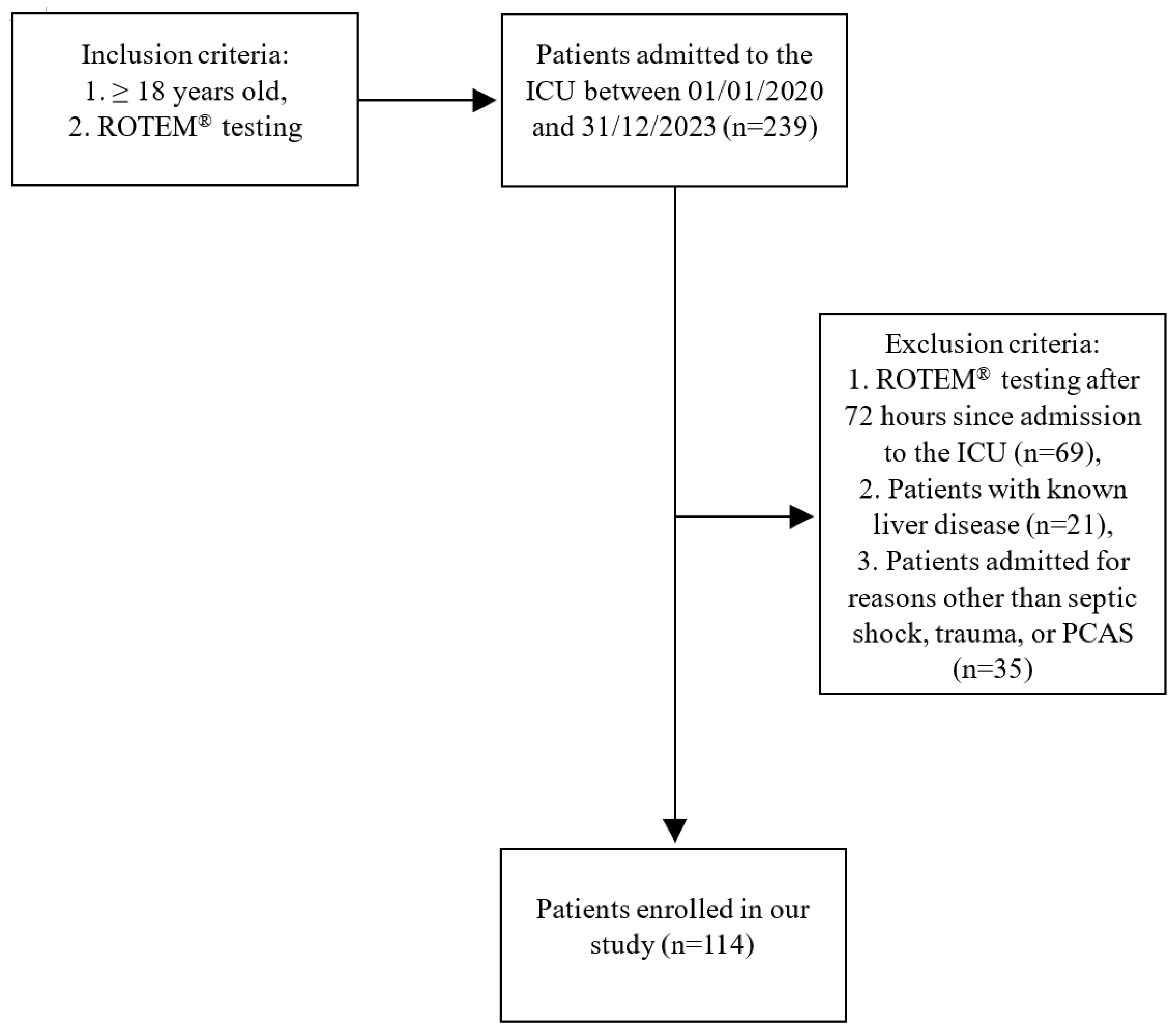
Figure 1.
The study flow chart.
2.1. Collected Clinical Data
Clinical data included APACHE II score, hospital and ICU lengths of stay, amount of blood products and coagulation factors concentrates transfused, ICU mortality, and time to death.
2.2. Collected Laboratory Data
In all patients laboratory data included CCTs and rotational thromboelastometry parameters obtained within the first 72 hours of ICU admission. Samples for rotational thromboelastometry were collected in S-Monovette® Citrate 9NC 0.106 mol/l/3.0 ml vials (SARSTEDT AG & Co. KG, Sarstedtstraße 1, 51588 Nümbrecht, Germany) and for other tests in S-Monovette® EDTA K3E/2.6 ml, Citrate 9NC 0.106 mol/l/3.0 ml, and Serum Gel CAT/4.7 ml vials (SARSTEDT AG & Co. KG, Sarstedtstraße 1, 51588 Nümbrecht, Germany). In our ward, we use systems that continuously flush arterial lines with a 0.9% NaCl solution without anticoagulant. Prior to sample collection, nurses aspirate and discard 3 mL of the patient’s blood. Immediately after sample collection, tests were performed by an experienced anesthesiologist on the rotational thromboelastometry machine (ROTEM® Sigma, SN 10494, Tem Innovations GmbH, Martin-Kollar-Straße 13-15, 81829 Munich, Germany ) or sent to the hospital laboratory (CCTs).
2.3. Principle of Operation of Rotational Thromboelastometry
Different chemical reagents are added to each cup containing the patient’s whole blood to activate specific coagulation pathways. The pin rotates within the cup, and as clot formation occurs, the viscosity of the blood increases, which enhances resistance to the rotating pin. This resistance is recorded as an amplitude on a graphical trace. Rotational thromboelastometry enables a detailed assessment of whole blood clotting competence by evaluating the phases of clot initiation, amplification, propagation, and termination, including fibrinolysis [36]. Key parameters include, among others: Clotting Time (CT) - the duration needed for the clot to reach a 2 mm amplitude, correlating with standard measures such as INR and aPTT; Clot Formation Time (CFT) - the time required for the clot to increase from a 2 mm to a 20 mm amplitude, reflecting the rate of fibrin polymerization; Maximum Clot Firmness (MCF) - the highest amplitude achieved, representing the strength of the clot due to fibrin-platelet interactions and crosslinking; Maximum Lysis (ML) – defined as a change in MCF over a specified time, indicating the extent of clot breakdown due to fibrinolysis.
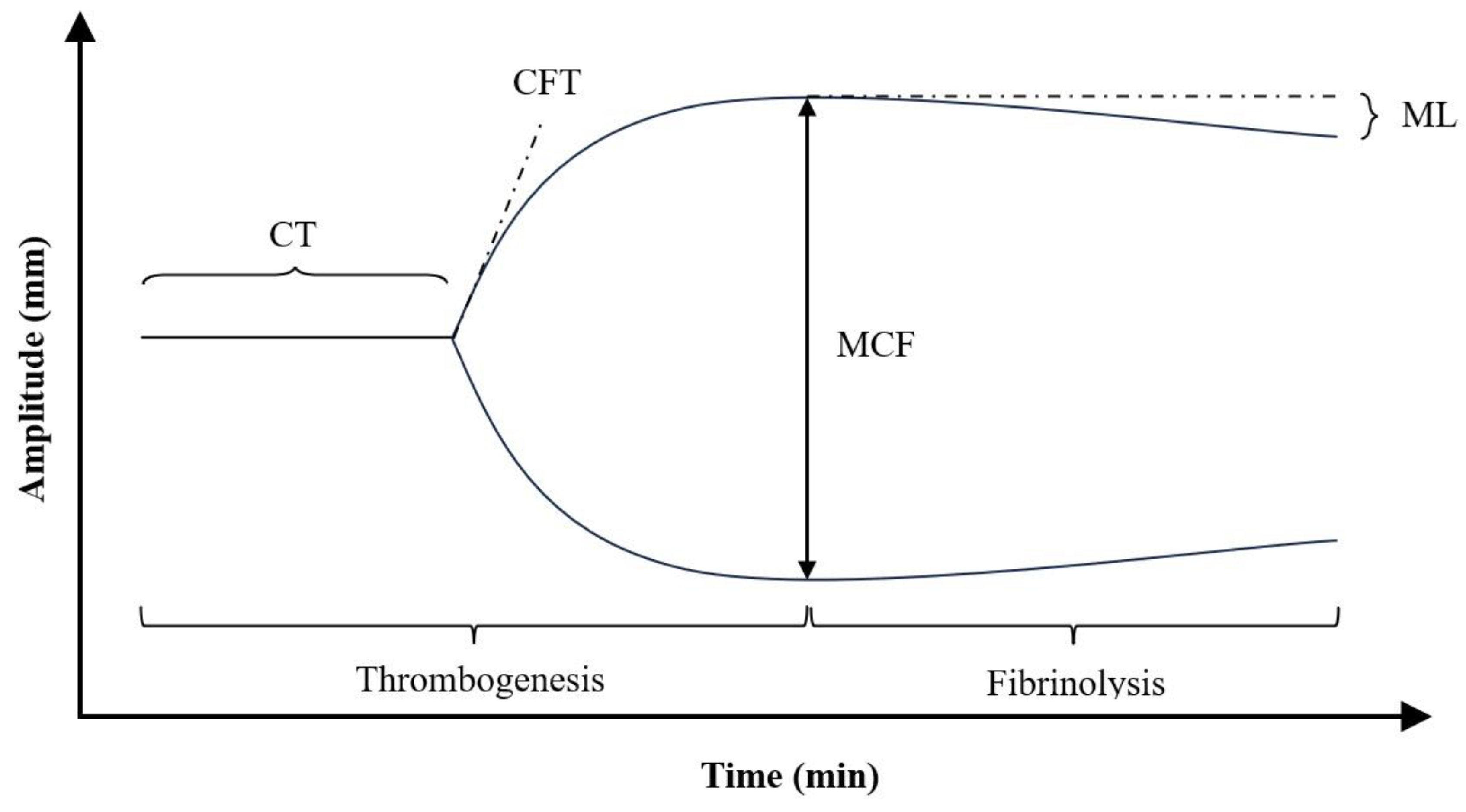
Figure 2.
Representative normocoagulable rotational thromboelastometry tracing with their respective parameters defined. CT, clotting time; CFT, clot formation time; MCF, maximum clot firmness; ML, maximum lysis.
Figure 2.
Representative normocoagulable rotational thromboelastometry tracing with their respective parameters defined. CT, clotting time; CFT, clot formation time; MCF, maximum clot firmness; ML, maximum lysis.
Basic ROTEM® assesses four distinct coagulation pathways. EXTEM uses TF to initiate clotting through the extrinsic pathway, predominantly evaluating the activity of clotting factors VII and X, alongside contributions from fibrinogen and platelets. INTEM, using ellagic acid as an activator, evaluates the intrinsic coagulation pathway and primarily measures the functionality of factors VIII, IX, XI, and XII, along with contributions from fibrinogen and platelet. This assay is commonly employed in cases such as hemophilia or during anticoagulation therapy. FIBTEM, incorporating cytochalasin D, a platelet inhibitor, isolates fibrin polymerization from platelet activity. It specifically measures the fibrinogen contribution to clot firmness, making it particularly useful for detecting hypofibrinogenemia or assessing fibrinogen dysfunction. APTEM, with aprotinin as its active component, inhibits fibrinolysis by blocking plasmin activity. It is primarily used to detect hyperfibrinolysis. By comparing APTEM results with EXTEM, clinicians can distinguish between fibrinolytic activity and other coagulation defects. [29].
2.4. Primary and Secondary Endpoints
Primary outcome was 30-day mortality since admission to ICU.
Secondary outcomes included the occurrence of overt DIC according to the modified International Society on Thrombosis and Haemostasis (ISTH) criteria for DIC (mISTH-DIC) total hospital and ICU lengths of stay, and the amounts of blood products and clotting factors concentrates transfused [37].
2.5. Statistical Analysis
The distribution of categorical variables was presented as counts and percentages, and numerical as means with standard deviations (SD) for normally distributed continuous variables and as medians with interquartile ranges (IQR) for non-normally distributed continuous variables. The Kolmogorov-Smirnov test was used to confirm the normality of distribution. Equality of variances was assessed using Levene’s test. Student’s t-test or Welch’s t-test was used, depending on the equality of variances, for normally distributed variables. The Mann-Whitney U-test was used for non-normally distributed continuous variables and Pearson’s chi-square test for categorical variables. Multivariable logistic regression analyses were carried out to determine independent predictors of 30-day mortality, with results presented as odds ratios (OR) and 95% confidence intervals (CI). Spearman’s rank correlation coefficient was used to assess the relationships between variables. All analyses were performed in SPSS version 29.0.2.0 (20) for Windows (IBM SPSS Statistics, Armonk, New York, USA). Two-tailed tests were applied, and a p-value of ≤ 0.05 was regarded statistically significant.
3. Results
A total of 239 patients, aged 18 years or older and having undergone rotational thromboelastometry, were admitted to the ICU from January 2020 to December 2023. Among them, 114 had septic shock, trauma, or PCAS, did not have any known liver disease, and underwent both CCTs and thromboelastometry testing within 72 hours of ICU admission. The mean (SD) age of the analyzed cohort was 49.3 (19.9) years, with males comprising the majority (66.7%). The primary diagnoses were septic shock in 51 (44.7%), trauma in 46 (40.4%), and CA in 17 (14.9%) patients. The 30-day mortality rate was 45.6% (52 patients), with the mean (SD) time to death since admission to ICU of 10.8 (26.2) days. The median (IQR) hospital length of stay was 18.5 (7.0-35.0), while the median ICU length of stay was 9.5 (2.0-19.25) days.
Surgical interventions were performed in 78 (68.4%) patients.
Table 1 summary of clinical data for the patients.
Patients in the non-survivor group were older and had higher mean (SD) APACHE II (Acute Physiology and Chronic Health Evaluation II) scores, reflecting greater severity of illness compared to the survivor group. The mean (SD) hospital and ICU lengths of stay were shorter among non-survivors compared to survivors.
Both CCTs and rotational thromboelastometry identified notable differences between survivors and non-survivors. The INR and aPTT values were significantly prolonged in non-survivors, non-survivors exhibited longer clotting times (CTs) in both EXTEM and INTEM.
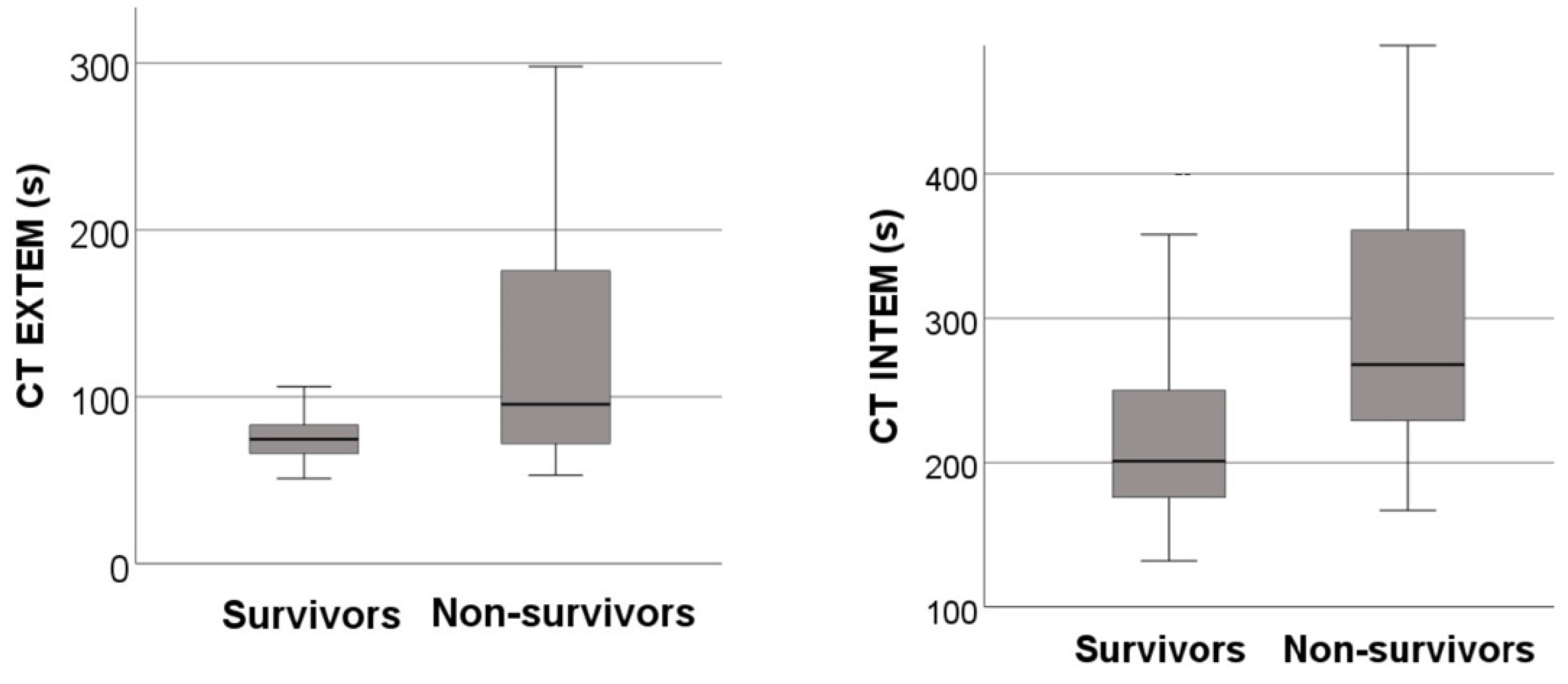
Figure 3.
(A) Box and whisker plot showing the distributions of CT EXTEM in survivors and non-survivors. (B) Box and whisker plot showing the distributions of CT INTEM in survivors and non-survivors.
Figure 3.
(A) Box and whisker plot showing the distributions of CT EXTEM in survivors and non-survivors. (B) Box and whisker plot showing the distributions of CT INTEM in survivors and non-survivors.
Additionally, in the same coagulation pathways (EXTEM and INTEM) maximum lysis (ML) was reduced in the non-survivors.
The patients who died received twice as many units of Fresh Frozen Plasma (FFP) as survivors. However, no statistically significant differences were observed in platelet counts, fibrinogen levels, or the amount of clotting concentrate factors administered, such as Octaplex® or Fibryga®.
In comparison of mISTH-DIC frequency we confirmed that overt DIC was significantly more common in non-survivors than in survivors.
Table 2 summary of study results in survivors and non-survivors.
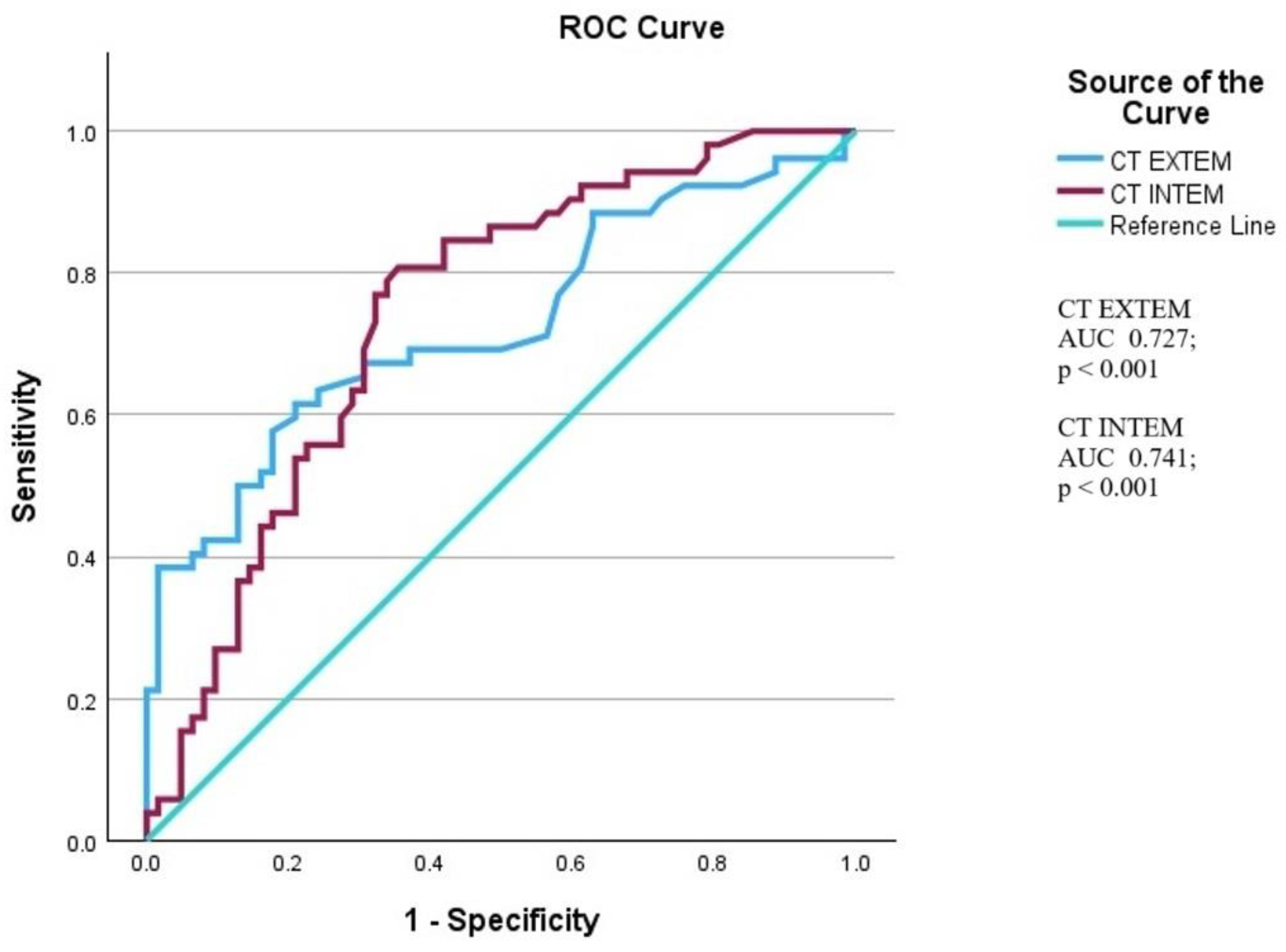
In multivariable logistic regression, both CT EXTEM and CT INTEM were independently associated with an increased risk of mortality, even after adjusting for age and APACHE II scores. Both parameters also demonstrated predictive value for 30-day mortality, with AUC values of 0.727 and 0.741 for the ROC curves of EXTEM and INTEM, respectively.
Table 3 summary of multivariable logistic regression analysis in two models.
Moreover, CT EXTEM and CT INTEM were negatively correlated with hospital length of stay and positively correlated with the presence of mISTH-DIC, as well as with INR and aPTT values.
Table 4 summary of Spearman’s rank correlation coefficient of CT EXTEM and CT INTEM with outcomes.
Figure 4.
Receiver operating characteristic (ROC) curves illustrating the diagnostic performance of CT EXTEM and CT INTEM in predicting 30-day mortality in the ICU.
Figure 4.
Receiver operating characteristic (ROC) curves illustrating the diagnostic performance of CT EXTEM and CT INTEM in predicting 30-day mortality in the ICU.
4. Discussion
Coagulopathy is an inherent sign of critical illness, reflecting severe systemic insults including endothelial injury, glycocalyx shedding, hypoperfusion, inflammation, and catecholamine surge, as a whole, described as SHINE. In critically ill patients, particularly those with septic shock, trauma, or PCAS, dysregulation of the coagulation cascade frequently occurs, leading to hypercoagulable or hypocoagulable states. These extremes can manifest as SIC, DIC, TIC, or CAAC, with microvascular thrombosis contributing to organ dysfunction and mortality. Maintaining hemostatic balance is essential not only for preventing excessive bleeding but also for ensuring adequate tissue perfusion and immunological response. Dysregulated hemostasis exacerbates ischemic injury and increases mortality by promoting MODS.
The cohort analyzed in our study reflects the heterogeneity and complexity of patients admitted to a tertiary hospital ICU. With a mean (SD) age of 49.3 (19.9) years and a predominance of male patients (66.7%), the demographics align with other critical care studies [38,39,40]. The high prevalence of septic shock (44.7%) and trauma (40.4%) in our database underscores the substantial burden of these conditions in the ICU setting. In addition, patients with PCAS, along with those above-mentioned groups, represent some of the most common reasons for ICU admission [41]. Interestingly, the 30-day mortality rate in our cohort (45.6%) is higher than that reported in some previous studies, likely reflecting greater illness severity [42]. The shorter ICU and hospital lengths of stay among non-survivors highlight the rapid progression of critical illness in this group, often culminating in early mortality. These findings are consistent with literature indicating that critically ill patients with severe coagulopathy often experience rapid clinical deterioration [43]. The observation that surgical interventions were performed in 68.4% of patients and that 61.4% required CRRT further illustrates the complexity of our patient population. Such interventions are often indicative of the severity of illness and may exacerbate coagulation abnormalities, complicating management and potentially influencing outcomes [44].
Our study demonstrates the prognostic value of thromboelastometry parameters, particularly CT EXTEM and CT INTEM results, in predicting mortality risk in a mixed group of ICU patients. In the comparative analysis, CT was statistically significantly prolonged across all coagulation pathways assessed by rotational thromboelastometry (FIBTEM, EXTEM, INTEM and APTEM) in non-survivors. The results of our study showed a mean (SD) value of A5 FIBTEM 11.6 (8.2 and 8.7) mm in both groups, suggesting neither fibrinogen dysfunction nor fibrinogen low levels. The constellation of prolonged CT in EXTEM or/and INTEM with an A5 FIBTEM value ≥ 9 mm indicates dysfunction of plasma clotting factors and impaired thrombin generation. In multivariable logistic regression analysis, both CT EXTEM and CT INTEM were independently associated with higher mortality risk, even after adjusting for confounders such as age and APACHE II scores. The odds ratios (OR) for these parameters (1.024, 95% CI 1.011-1.038, p < 0.001 for CT EXTEM and 1.006, 95% CI 1.001-1.010, p 0.009 for CT INTEM) show that increases in CT are associated with a rise in mortality risk. This predictive value was further supported by the area under the curve (AUC) values for the ROC curves, which were 0.727 for CT EXTEM, p < 0.001, and 0.741 for CT INTEM, p < 0.001, demonstrating good discriminative ability. These findings underscore the utility of rotational thromboelastometry as a tool worth recommending for risk stratification in critically ill patients. Notably, the prolonged CTs observed in non-survivors suggest a delay in the initiation of clot formation and underscore the sensitivity of thromboelastometry in detecting clinically relevant coagulopathies associated with SHINE. Furthermore, we identified a negative correlation between CT EXTEM and CT INTEM with the hospital length of stay, proving that more severe coagulation abnormalities are associated with shorter survival durations. Interestingly, despite substantial differences in CTs, no significant differences were observed in parameters related to MCF between survivors and non-survivors. This observation may be attributed to the acute-phase response at the early stage of illness, characterized by elevated fibrinogen levels in SIC, CAAC, and platelet release from the spleen in TIC.
The delayed initiation of clot formation can be explained by coagulopathy associated with SHINE, which shares a common pathophysiological etiology: de-endothelialization of blood vessels. This process exposes the subendothelial layer, leading to capillary leakage and microvascular thrombosis, which further exacerbate endothelial hypoxemia. Consequently, an exaggerated physiological response emerges to maintain perfusion, creating hypocoagulable and hypofibrinolytic states [5]. Physiologically, the endothelium and glycocalyx contain numerous natural anticoagulants, including heparonoids, antithrombin (AT), tissue factor pathway inhibitor (TFPI), protein C/thrombomodulin, tissue-type Plasminogen Activator (tPA) and urokinase-type Plasminogen Activator (uPA), which can be released into the bloodstream [45]. Soluble thrombomodulin (sTM) converts protein C into activated protein C (APC), which in turn degrades active forms of Factor V, Factor VIII, and PAI-1. Catecholamines released by the stimulated hypothalamic-pituitary-adrenal axis can further activate and damage the endothelium. Additionally, perivascular sympathetic nerves can release enzymatically active tPA [46]. Rotational thromboelastometry tracings often progress from a normal state to hypercoagulable, then hypocoagulable, and finally hyperfibrinolytic states [5]. Therefore, we observe the significantly prolonged CTs in the rotational thromboelastometry in the non-survivors as a consequence of diminished plasma clotting factors contribution to coagulation cascade. Several studies indicate that plasma transfusion in trauma and therapeutic plasma exchange (TPE) with FFP in sepsis patients may exert a protective effect on injured endothelium [47-52]. Moreover, El-Nawawyy et. al (2021) showed that the early use of FFP, low-dose heparin, and tranexamic acid (TXA) in the pediatric population, with very low plasma clotting factors and AT levels secondary to SIC, improved survival and prevented the progression to overt DIC [53].
In our study, we observed decreased ML EXTEM and ML INTEM in non-survivors, highlighting the role of impaired fibrinolysis, which has been linked to the development of microvascular thrombosis and organ failure [54]. This abnormality, referred as “fibrinolytic shutdown”, is a common feature of SIC, PCAS, and certain stages of trauma. Impaired fibrinolysis is a major contributor to microvascular thrombi formation, leading to the ongoing consumption of platelets and clotting factors. Ultimately, it causes microvasculature failure and DIC, which are key drivers of MODS [55]. A critical factor in this process is neutrophil elastase bound to the DNA of neutrophil extracellular traps (NETs) [56]. While free elastase is degraded by its primary inhibitor, an alpha 1-protease inhibitor, DNA-bound elastase becomes resistant to inhibition and cleaves plasminogen into fragments incapable of generating plasmin. A study by Hayakawa et al. (2010) showed that sivelestat, a selective neutrophil elastase inhibitor, decreased mortality in patients with acute respiratory distress syndrome (ARDS) and DIC [57]. Additionally, in some cases, an increased concentration of PAI-1, produced by endothelial cells, and TAFI as a response for thrombin burst further contribute to fibrinolysis shutdown [58-59]. Similar to our findings, Ostrowski et al. (2013) found that around half of sepsis patients had a normal coagulation profile, while others exhibited hypocoagulability or hypercoagulable states accompanied by hypofibrinolysis [11]. In trauma patients, despite the presence of hyperfibrinolysis in many cases during the early stage the fibrinolytic phase often terminates (within hours after trauma) due to increased PAI-1 production by endothelial cells and platelets, contributing to fibrinolysis shutdown, which has been proven to increase mortality [60]. Routine administration of TXA in trauma patients may, in certain cases, facilitate fibrinolytic resistance, predisposing to hypofibrinolysis. Therefore, it may be advised to guide TXA usage based on VHAs results rather than relying on empirical practices [61].
In our cohort, INR and aPTT values were significantly prolonged in non-survivors compared to survivors, indicating the association between coagulopathy and mortality in critically ill patients, particularly those with septic shock and trauma [22,62,63]. Clinicians have been using CCTs for a long time as standard tools for assessing coagulation status in critically ill patients. These tests provide basic information on specific components of the coagulation cascade. However, they asses only the time required to initiate clot formation without details about clot strength and fibrinolysis. Despite these limitations, our study underlines their importance, because CCTs are relatively cheap and widely available, unlike the VHAs. Non-survivors received twice as many units of FFP as survivors, further suggesting a greater degree of plasma clotting factor depletion in this group. It is important to note that glycocalyx shading, commonly observed in critically ill patients, exacerbates coagulopathy through auto-heparinization. Animal studies have shown that plasma transfusion may partially restore the glycocalyx [64,65,66,67,68]. However, while FFP transfusion is often used to correct coagulopathy, it carries significant risks associated with blood products transfusion. Moreover, patients with SHINE typically have capillary leakage, so the large volumes of FFP required for coagulation correction may contribute to fluid overload, tissue edema, and further deterioration of patients outcomes. Alternatively, the use of Prothrombin Complex Concentrate (PCC) is becoming increasingly common, particularly in conditions requiring fluid restriction, such as traumatic brain injury (TBI). PCC can be used as a more targeted approach to correcting coagulopathies without causing volume overload.
Interestingly, our study showed lower platelet count in patients who died; however, the difference was not statistically significant. Previous studies have identified thrombocytopenia as a frequent laboratory abnormality in critically ill patients and have established it as an independent predictor of increased mortality [69]. However, thrombocytopenia often develops at the later stage of ICU stay and can be caused by factors such as infection, heparin-induced thrombocytopenia (HIT), or surgical interventions. Therefore, our early assessment within the first 72 hours may not have captured these later changes [70]. It is important to emphasize that, at the onset of an acute process, it is not the drop in the platelet count but rather platelet dysfunction that develops [71]. In DIC, there is overt consumption of platelets, fibrinogen, and clotting factors due to thrombi formation, resulting in a thrombotic and/or bleeding diathesis. Our study demonstrated a statistically significant elevated risk of developing DIC, based on the mISTH criteria, in patients with higher mortality. Uncontrolled overt DIC leads to massive consumption of plasma clotting factors and, in the late phase, can be easily detected by CCTs, which will show prolonged INR and aPTT if coagulation factors are below 50% normal levels.
CCTs remain an important part of routine coagulation assessment, but they have limitations. These tests do not provide the dynamic evaluation of clot formation. Furthermore, CCTs are often performed in hospital laboratories, so results are usually delayed due to the time required for sample transport and processing. In our study, the results obtained from CCTs and VHAs were comparable; however, it is imperative to remember that both tests were conducted within the 72-hour timeframe following ICU admission. Using these tests immediately upon admission to the ICU during the early stage of coagulopathy associated with SHINE, may not reveal abnormalities detectable only through VHAs. These limitations underscore the need for VHAs, which provide near real-time, dynamic, and comprehensive coagulation assessments. VHAs allow for individualized and goal-directed resuscitation strategies [72,73]. For example, VHAs-guided therapy has been shown to reduce blood product usage and improve hemostasis, although its impact on mortality remains uncertain.
This study has some limitations. We had a relatively small database, so results may not properly represent the characteristics of a larger ICU population with SHINE. The retrospective nature of our study introduces a risk of selection bias. Additionally, we did not have the clear guidelines indicating the need for performing rotational thromboelastometry in septic shock and PCAS patients in our ward, which lead us to collect data over a broad time span (0 to 72 hours of ICU admission). Larger, multicenter prospective studies with strict guidelines are required to confirm the associations observed in this paper, minimize bias, and explore their adoption to patients with SHINE in routine clinical practice. The association between abnormal rotational thromboelastometry parameters and mortality is convincing, as we showed in this study; however, it remains uncertain whether targeted interventions based on these findings can improve survival outcomes. Future research should investigate whether allocating patients with SHINE-associated coagulopathies to a higher risk group upon ICU admission, based on deranged rotational thromboelastometry results, can improve management and reduce bleeding and/or thrombotic complications.
5. Conclusions
Our study demonstrates the important role of rotational thromboelastometry in evaluating coagulopathies and predicting mortality in critically ill patients. The key finding includes the association of prolonged CT EXTEM and CT INTEM with higher 30-day mortality in patients with SHINE and suggests that these parameters can be used for standard prognostication upon ICU admission. This study also shows that simple parameters, such as INR and aPTT, may be useful predictors of higher mortality risk in patients with endotheliopathy related to hypoperfusion. However, rotational thromboelastometry remains the gold standard due to its rapid and comprehensive diagnostic capabilities, which can quickly detect “phenotype switching” between pro- and antithrombotic, as well as pro- and antifibrinolytic states. This facilitates the introduction of personalized and goal-directed therapy for critically ill patients with coagulopathies. Despite some challenges, such as relatively high costs and limited accessibility, particularly in developing countries, further research is essential to implement rotational thromboelastometry into routine intensive care practice as an early predictor of mortality.
Authors Contributions
Author Contributions: Conceptualization, W.S. and M.T.; methodology, M.C.; software, T.S.; validation, W.S., M.T. and T.D.; formal analysis, T.L.; investigation, W.S.; resources, M.T.; data curation, W.S.; writing—original draft preparation, W.S.; writing—review and editing, M.T.; visualization, T.L.; supervision, M.C.; project administration, M.T. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was provided.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee of Jagiellonian University in Krakow, Poland on June, 20, 2024 (No. 118.0043.1.224.2024).
Informed Consent Statement
The was no requirement for obtaining the Informed Consent Form (ICF) because this was a retrospective observational study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon request.
Acknowledgments
We sincerely thank our colleagues of the Student’s Scientific Group in the Department of Interdisciplinary Intensive Care, Jagiellonian University Medical College, Krakow, Poland, for their participation in data collection: Maria Marusińska, Gabriela Piotrowska, Aleksandra Sielska, Weronika Skoczeń, Ewa Imielska, Anna Chlubek, Alicja Warecka, Martyna Narożniak, Daria Orzechowska
Conflicts of Interest
The authors declare no conflict of interest.
References
- Helms, J.; Iba, T.; Connors, J.M.; Gando, S.; Levi, M.; Meziani, F.; Levy, J.H. How to manage coagulopathies in critically ill patients. Intensive Care Med 2023, 49:273-290. [CrossRef]
- Levi, M.; Opal, S.M. Coagulation abnormalities in critically ill patients. Critical Care 2006, 10:222. [CrossRef]
- MacLeod, J.B.A.; Lynn, M.; McKenney, M.G.; Cohn, S. M.; Murtha, M. Early coagulopathy predicts mortality in trauma. J Trauma 2003, 55(1):39-44. [CrossRef]
- Johansson, P.I.; Stensballe, J.; Ostrowski, S.R. Shock induced endotheliopathy (SHINE) in acute critical illness – a unifying pathophysiologic mechanism. Crit Care. 2017, Feb 9;21(1):25. [CrossRef]
- Johansson, P.I.; Ostrowski, S.R. Acute coagulopathy of trauma: balancing progressive catecholamine induced endothelial activation and damage by fluid phase anticoagulation. Med Hypothes. 2010, Dec;75(6):564-7. [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J-D.; Coopersmith, C.M.; Hotchkiss, R.S.; Levy, M.M.; Marshall, J.C.; Martin, G.S., Opal, S.M.; Rubenfeld, G.D.; van der Poll, T.; Vincent, J-L.; Angus, D. C. The third international consensus definitions for sepsis and septic shock (Sepsis 3). JAMA 2016, 315(8):801-10. [CrossRef]
- Prakash, S.; Verghese, S.; Roxby, D.; Dixon, D.; Bihari, S.; Bersten, A. Changes in fibrinolysis and severity of organ failure in sepsis: a prospective observational study using point-of-care test-ROTEM. J Crit Care 2015, 30(2):264-70. [CrossRef]
- Daudel, F.; Kessler, U.; Folly, H.; Lienert, J.S.; Takala, J.; Jakob, S.M. Thromboelastometry for the assessment of coagulation abnormalities in early and established adult sepsis: a prospective cohort study. Crit Care 2009, 13(2): R42. [CrossRef]
- Collins, P.W.; Macchiavello, L.I.; Lewis, S.J.; Macartney, N.J.; Saayman, A.G.; Luddington, R.; Baglin, T.; Findlay, G.P. Global tests of haemostasis in critically ill patients with severe sepsis syndrome compared to controls. Br J Haematol 2006, 135(2):220-7. [CrossRef]
- Simmons, J.; Pittet, J-F. The coagulopathy of acute sepsis. Curr Opin Anaesthesiol 2015, 28(2):227-36. [CrossRef]
- Ostrowski, S.R.; Windeløv, N.A.; Ibsen, M.; Haase, N.; Perner, A.; Johansson, P.I. Consecutive thromboelastography clot strength profiles in patients with severe sepsis and their association with 28-day mortality; a prospective study. J Crit Care 2013, 28(3):317.e1-11. [CrossRef]
- Davies, G.R.; Pillai, S.; Lawrence, M.; Mills, G.M.; Aubrey, R.; D’Silva, L.; Battle, C.; Williams, R.; Brown, R.; Thomas, D.; Morris, K.; Evans, P.A. The effect of sepsis and its inflammatory response on mechanical clot characteristics; a prospective observational study. Intensive Care Med 2016, 42(12):1990-1998. [CrossRef]
- Czempik, P.F.; Wiórek, A. Rotational thromboelastometric profile in early sepsis: a prospective cohort study. Biomedicine 2024, 12(8):1880. [CrossRef]
- Brohi, K.; Gruen, R. L.; Holcomb, J.B. Why are bleeding trauma patients still dying? Intensive Care Med 2019, 45(5):709-711. [CrossRef]
- Brohi, K.; Singh, J.; Heron, M.; Coats, T. Acute traumatic coagulopathy. J Trauma 2003, 54(6):1127-30. [CrossRef]
- Cap, A.; Hunt, B.J. The pathogenesis of traumatic coagulopathy. Anaesthesia 2015, 70: Suppl 1:96-101, e32-4. [CrossRef]
- Simmons, J.W.; Powell, M.F. Acute traumatic coagulopathy: pathophysiology and resuscitation. Br J Anaesth 2016, 117(suppl 3):iii31-iii43. [CrossRef]
- Sillen, M.; Declerck, P.J. A narrative review on plasminogen activator inhibitor-1 and its (patho)physiological role: to target or not to target? Int J Mol Sci. 2021, Mar 8;22(5):2721. [CrossRef]
- Brohi, K.; Cohen, M.J.; Ganter, M.T.; Schultz, M.J.; Levi, M.; Mackersie, R.; Pittet, J-F. Acute coagulopathy of trauma: hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J Trauma 2008, 64(5):1211-7. [CrossRef]
- Puranik, N.G.; Verma, T.Y.P.; Pandit, G.A. The study of coagulation parameters in polytrauma patients and their effects on outcome. J Hematol 2018, 7(3):107-111. [CrossRef]
- Davenport, R. Pathogenesis of acute traumatic coagulopathy. Transfusion 2013, 53 Suppl 1:23S27S. [CrossRef]
- Smith, A.R.; Karim, S.A.; Reif, R.R.; Beck, W.C.; Taylor, J.R.; Davis, B.L.; Bhavaraju, A.V.; Jensen, H.K.; Kimbrough, M.K.; Sexton, K.W. ROTEM as a predictor of mortality in patients with severe trauma. J Surg Res 2020, 251:107-111. [CrossRef]
- Adrie, C.; Monchi, M.; Laurent, I.; Um, S.; Yan, S.B.; Thuong, M.; Cariou, A.; Charpentier, J.; Dhainaut, J-F. Coagulopathy after successful cardiopulmonary resuscitation following cardiac arrest: implication of the protein C anticoagulant pathway. J Am Coll Cardiol 2005, 46(1):21-8. [CrossRef]
- Gando, S.; Wada, T. Disseminated intravascular coagulation in cardiac arrest and resuscitation. J Thromb Haemost 2019, 17(8):1205-16. [CrossRef]
- Lee, D.H.; Lee, B.K.; Jeung, K.W.; Jung, Y.H.; Lee, S.M.; Cho, Y.S.; Yun, S-W.; Min, Y.I. Disseminated intravascular coagulation is associated with the neurologic outcome of cardiac arrest survivors. Am J Emerg Med 2017, 35(11):1617-1623. [CrossRef]
- Shinada, K.; Koami, H.; Mastuoka, A.; Sakamoto, Y. Prediction of spontaneous return f circulation in out-of-hospital cardiac arrest with non-shockable initial rhythm using point- of care testing: a retrospective observational study. World J Emerg Med 2023, 14(2):89-95. [CrossRef]
- Schöchl, H.; Cadamuro, J.; Seidl, S.; Franz, A.; Solomon, C.; Schlimp, C.J.; Ziegler, B. Hyperfibrinolysis is common in out-of-hospital cardiac arrest: results from a prospective observational thromboelastometry study. Resuscitation 2013, 84(4): 454-9. [CrossRef]
- Kaomi, H.; Sakamoto, Y.; Sakurai, R.; Ohta, M.; Imahase, H.; Yahata, M.; Umeka, M.; Miike, T.; Nagashima, F.; Iwamura, T.; Yamada, K.C.; Inoue, S. Thromboelastometric analysis of the risk factors for return of spontaneous circulation in adult patients with out- of- hospital cardiac arrest. PLoS One 2017, 12(4):e0175257. [CrossRef]
- Lier, H.; Vorweg, M.; Hanke, A.; Görlinger, K. Thromboelastometry guided therapy of severe bleeding. Essener Runde algorithm. Hamostaseologie 2013, 33(1):51-61. [CrossRef]
- Ng, V.L. Liver disease, coagulation testing, and hemostasis. Clin Lab Med 2009, 29(2):265-82. [CrossRef]
- Levi, M.; Schultz, M.; van der Poll, T. Coagulation biomarkers in critically ill patients. Crit Care Clin 2011, 27(2):281-97. [CrossRef]
- Meybohm, P.; Zacharowski, K.; Weber, C.F. Point-of-care coagulation management in intensive care medicine. Crit Care 2013, 17(2):218. [CrossRef]
- Benes, J.; Zatloukal, J.; Kletecka, J. Viscoelastic methods of blood clotting assessment - a multidisciplinary review. Front Med (Lausanne) 2015, 14:2:62. [CrossRef]
- Spalding, G.J.; Hartrumpf, M.; Sierig, T.; Oesberg, N.; Kirschke, C.G.; Albes, M.J. Cost reduction of perioperative coagulation management in cardiac surgery: value of “bedside” thromboelastography (ROTEM). Eur J Cardiothorac Surg 2007, 31(6):1052-7. [CrossRef]
- von Elm, E., Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008, Apr;61(4):344-9. [CrossRef]
- Curry, N.S.; Davenport, R.; Pavord, S.; Mallett, S.V.; Kitchen, D.; Klein, A.A.; Maybury, H.; Collins, P.W.; Laffan, M. The use of viscoelastic assays in the management of major bleeding: a British Society for Haematology guideline. Br J Haematol. 2018, Sep;182(6):789-806. [CrossRef]
- Taylor, F.B., Jr.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M.; Scientific Subcommittee on Disseminated Intravascular Co-agulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and la-boratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [CrossRef]
- Heubner , L.; Hattenhauer, S.; Güldner, A.; Petrick, P.L.; Rößler, M.; Schmitt, J.; Schneider, R.; Held, H.C.; Mehrholz, J.; Bodechtel, U.; Ragaller, M.; Koch, T.; Spieth, P.M. Characteristics and outcomes of sepsis patient with and without COVID-19. J Infect Public Health 2022, Jun;15(6):670-676. [CrossRef]
- Wilson, A.J.; Magee, F.; Bailey, M.; Pilcher, D.V.; French, C,; Nichol, A.; Udy, A.; Hodgson, C.L.; Cooper, D.J.; Reade, M.C.; Young, P.; Bellomo, R. Characteristics and outcomes of critically ill trauma patients in Australia and New Zealand (2005-2017). Crit Care Med. 2020, May;48(5):717-724. [CrossRef]
- Jansen, G.; Sauzet, O.; Borgstedt, R.; Entz, S.; Holland, F.O.; Lamprinaki, S.; Thies, K-C.; Scholz, S.S.; Rehberg, S.W. Incidence, characteristics and predictors of mortality following cardiac arrest in ICUs of a German university hospital: A retrospective cohort study. Eur J Anaesthesiol. 2022, May 1;39(5):452-462. [CrossRef]
- Karwa, M.L.; Naqvi, A.A.; Betchen, M.; Puri, A.K. In-hospital triage. Crit Care Clin 2024, Jul;40(3):533-548. [CrossRef]
- Shafigh, N.; Hasheminik, M.; Shafigh, E.; Alipour, H.; Sayyadi, S.; Kazeminia, N.; Khoundabi, B.; Salarian, S. Prediction of mortality in ICU patients: A comparison between SOFA and other indicators. Nurs Crit Care. 2024, Nov;29(6):1619-1622. [CrossRef]
- Alhamdi, Y.; Toh, C-H. Recent advances in pathophysiology of disseminated intravascular coagulation: the role of circulating histones and neutrophil extracellular traps. F1000Res. 2017, Dec 18:6:2143. [CrossRef]
- Song, M.J.; Jang, Y.; Legrand, M.; Park, S.; Ko, R.F.; Suh, G.Y.; Oh, D.K.; Lee, S.Y.; Park, M.H.P.; Lim, C-M.; Jung, S.Y.; Lim, S.Y.; Korean Sepsis Alliance (KSA) investigator. Epidemiology of sepsis-associated acute kidney injury in critically ill patients: a multicenter, prospective, observational cohort study in South Korea. Crit Care. 2024, Nov 24;28(1):383. [CrossRef]
- Levi, M.; van der Poll, T. The role of natural anticoagulants in the pathogenesis and management of systemic activation of coagulation and inflammation in critically ill patients. Semin Thromb Hemost. 2008, Jul;34(5):459-68. [CrossRef]
- Kwaan. H.C. From fibrinolysis to plasminogen-plasmin system and beyond: a remarkable growth of knowledge, with personal observations on the history of fibrinolysis. Semin Thromb Hemost. 2014, Jul 40;(5):585-91. [CrossRef]
- Moore, H.B.; Moore, E.E.; Chapman, M.P.; McVaney, K.; Bryskiewicz, G.; Blechar, R.; Chin, T.; Burlew, C.C.; Pieracci, F.; West, F.B.; Fleming, C.D.; Ghasabyan, A.; Chandler, J.; Silliman, C.C.; Banerjee, A.; Sauaia, A. Plasma-first resuscitation to treat haemorrhage shock during emergency ground transportation in an urban area; a randomised trial. Lancet. 2018, Jul 28;392(10144):283-291. [CrossRef]
- Sperry, J.L.; Guyette, F.X.; Brown, J.B.; Yazer, M.H.; Triulzi, D.J.; Early-Young, B.J.; Adams, P.W.; Daley, B.J.; Miller, R.S.; Harbrecht, B.G.; Claridge, J.A.; Phelan, H.A.; Witham, W.R.; Putnam, A.T.; Duane, T.M.; Alarcon, L.H.; Callaway, C.W.; Zuckerbraun, B.S.; Neal, M.D.; Rosengart, M.R.; Forsythe, R.M.; Billiar, T.R.; Yealy, D.M.; Peitzman, A.B.; Zenati, M.S.; PAMPer Study Group. Prehospital plasma during air medical transport in trauma patients at risk for hemorrhagic shock. N Engl J Med. 2018, Jul 26;379(4):315-326. [CrossRef]
- Pusateri, A.E.; Moore, E.E.; Moore, H.B.; Le, T.D.; Guyette, F.X.; Chapman, M.P.; Sauaia, A.; Ghasabyan, A.; Chandler, J.; McVaney, J.; Brown, J.B.; Daley, B.J.; Miller, R.S.; Harbrecht, B.G.; Claridge, J.A.; Phelan, H.A.; Witham, W.R.; Putnam, A.T.; Sperry, J.L. Association of prehospital plasma transfusion wit survival in trauma patients with hemorrhagic shock when transport Times are longer than 20 minutes: a post hoc analysis of the PAMPer and COMBAT trials. JAMA Surg. 2020, Feb 1;155(2):e195085. [CrossRef]
- Drost, C.C.; Rovas, A.; Kümpers, P. Protection and rebuilding of the endothelial glycocalyx in sepsis – science or fiction? Matrix Biol Plus. 2021, Nov 3:12:100091. [CrossRef]
- Pape, T.; Hunkemöller, A.M.; Kümpers, P.; Haller, H.; David, S.; Stahl, K. Targeting the „sweet spot” in septic shock – a perspective on endothelial glycocalyx regulating proteins Heparanase-1 and -2. Matrix Biol Plus. 2021, Dec 2:12:100095. [CrossRef]
- Stahl, K.; Hillebrand, U.C.; Kiyan, Y.; Seeliger, B.; Schmidt, J.J.; Schenk, H.; Pape, T.; Schmidt, B.M.W.; Welte, T.; Hoeper, M.M.; Sauer, A.; Wygrecka, M.; Bode, C.; Wedemeyer, H.; Haller, H.; David, S. Effects of therapeutic plasma exchange on the endothelial glycocalyx in sepsis. Intensive Care Med. Exp. 2021, Nov 24;9(1):57. [CrossRef]
- El-Nawawy, A.A.; Elshinawy, M.I.; Khater, D.M.; Moustafa, A.A.; Hassanein, N.M.; Wali, Y.A.; Nazir, H.F. Outcome of early hemostatic intervention in children with sepsis and nonovert disseminated intravascular coagulation admitted to PICU: a randomized controlled trial. Pediatr Crit Care Med. 2021, 22:e168-e177. [CrossRef]
- Gando, S.; Levi, M.; Toh, C-T. Trauma-induced innate immune activation and disseminated intravascular coagulation. J Thromb Haemost. 2024, Feb;22(2):337-351. [CrossRef]
- Wheeler, A.P.; Bernard, G.R. Treating patients with severe sepsis. NEJM 1999, 340:207-214. [CrossRef]
- Barbosa da Cruz, D.; Helms, J.; Aquino, L.R.; Stiel, L.; Cougourdan, L.; Broussard, C.; Chafey, P.; Riès-Kautt, M.; Meziani, F.; Toti, F.; Gaussem, P.; Anglés-Cano, E. DNA bound elastase of neutrophil extracellular traps degrades plasminogen, reduces plasmin formation, and decreases fibrinolysis: proof of concept in septic shock plasma. FASEB J. 2019, 33:14270-14280. [CrossRef]
- Hayakawa, M.; Katabami, K.; Wada, T.; Sugano, M.; Hoshino, H.; Sawamura, A.; Gando, S. Sivelestat (selective neutrophil elastase inhibitor) improves the mortality rate of sepsis associated with both acute respiratory distress syndrome and disseminated intravascular coagulation patients. Shock 2010, Jan;33(1):14-8. [CrossRef]
- Semeraro, N.; Ammollo, C.T.; Semeraro, F.; Colucci, M. Coagulopathy of acute sepsis. Semin Thromb Hemost. 2015, Sep;41(6):650-8. [CrossRef]
- Coleman, J.R.; Moore, E.E.; Kelher, M.R.; Jones, K.; Cohen, M.J.; Banerjee, A.; Silliman, C.C. Elucidating the molecular mechanisms of fibrinolytic shutdown after severe injury: the role of thrombin-activatable fibrinolysis inhibitor. J Trauma Acute Care Surg. 2023, Jun 1;94(6):857-862. [CrossRef]
- Favors, L.; Harrell, K.; Miles, V.; Hicks, R.C.; Rippy, M.; Parmer, H.; Edwards, A.; Brown, C.; Stewart, K.; Day, L.; Wilson, A.; Maxwell, R. Analysis of fibrinolytic shutdown in trauma patients with traumatic brain injury. Am J Surg. 2024, Jan:227:72-76. [CrossRef]
- Moore, H.B.; Moore, E.E.; Huebner, B.R.; Stettler, G.R.; Nunns, G.R.; Einersen, P.M.; Silliman, C.C.; Sauaia, A. Tranexamic acid is associated with increased mortality in patients with physiological fibrinolysis. J Surg Res. 2024, Dec:220:438-443. [CrossRef]
- Xie, Z.; Zhu, S.; Wang, J.; Zhang, M.; Lv, X.; Ma, Y.; Shan, H.; Zhong, Y. Relationship between coagulopathy score and ICU mortality: analysis of the MIMIC-IV database. Heliyon. 2024, Jul 14;10(14):e34644. [CrossRef]
- Richards, J.E.; Yang, S.; Kozar, R.A.; Scalea, T.M.; Hu, P. A machine learning-based coagulation risk index predicts acute traumatic coagulopathy in bleeding trauma patients. J Trauma Acute Care Surg. 2024, Sept 27. [CrossRef]
- Hu, L.; Wang, J.; Zhang, Y.; Wang, J.; Wei, B. Predictive value of SYN-1 levels for mortality in sepsis patients in the emergency department. J Inflamm Res. 2024, Nov 26:17:9837-9846. [CrossRef]
- Johansson, P.I.; Vigstedt, M.; Curry, N.S.; Davenport, R.; Juffermans, N.P.; Stanworth, S.J.; Maegele, M.; Gaarder, C.; Brohi, K.; Stensballe, J.; Henriksen, H.H.; Targeted Action for Curing Trauma-Induced Coagulopathy (TACTIC) Collaborators. Trauma induced coagulopathy is limited to only one out of four shock induced coagulopathy (SHINE) phenotypes among moderate-severely injured trauma patients: an exploratory analysis. Scand J Trauma Resusc Emerg Med. 2024, Aug 19;32(1):71. [CrossRef]
- Matsumoto, H.; Annen, S.; Mukai, N.; Ohshita, M.; Murata, S.; Harima, Y.; Ogawa, S.; Okita, M.; Nakabayashi, Y.; Kikuchi, S.; Takeba, J.; Sato, N. Circulating Syndecan-1 levels are associated with chronological coagulofibrinolytic responses and the development of disseminated intravascular coagulation (DIC) after trauma: a retrospective observational study. J Clin Med. 2023, Jun29;12(13):4386. [CrossRef]
- Kravitz, M.S.; Kattouf, N.; Stewart, I.J.; Ginde, A.A.; Schmidt, E.P.; Shapiro, N.I. Plasma for prevention and treatment of glycocalyx degradation in trauma and sepsis. Crit Care. 2024, Jul 20;28(1):254. [CrossRef]
- Kozar, R.A.; Peng, Z.; Zhang, R.; Holcomb, J.B.; Pati, S.; Park, P.; Ko, T.C.; Paredes, A. Plasma restoration of endothelial glycocalyx in a rodent model of hemorrhagic shock. Anesth Analg. 2011, Jun;112(6):1289-95. [CrossRef]
- Guo, Q-Y.; Peng, J.; Shan, T-C.; Xu, M. Risk factors for mortality in critically ill patients with coagulation abnormalities: a retrospective cohort study. Curr Med Sci. 2024, Oct;44(5):912 922. [CrossRef]
- Greinacher, A.; Selleng, K. Thrombocytopenia in the intensive care unit patient. Hematology Am Soc Hematol Educ Program 2010, 2010:135-43. [CrossRef]
- Asiri, A.; Price, J.M.J.; Hazeldine, J.; McGee, K.C.; Sardeli, A.V.; Chen, Y-Y.; Sullivan, J.; Moiemen, N.S.; Harrison, P. Measurement of platelet thrombus formation in patients following severe thermal injury. Platelets. 2024, Dec;35(1):2420952. [CrossRef]
- Stettler, G.R.; Moore, E.E.; Moore, H.B.; Nunns, G.R.; Silliman, C.C.; Banerjee, A.; Sauaia, A. Redefining postinjury fibrinolysis phenotypes using two viscoelastic assays. J Trauma Acute Care Surg. 2019, Apr;86(4):679-685. [CrossRef]
- McKinley, T.O.; Lisboa, F.A.; Horan, A.D.; Gaski, G.E.; Mehta, S. Precision medicine applications to manage multiply injured patients with orthopaedic trauma. J Orthop Trauma. 2019, Jun:33 Suppl 6:S25-S29. [CrossRef]

Table 1.
Characteristics of study population.
| Characteristics | Summary measure (n = 114) |
| Age [years] | 49.3 (19.9) |
| Male | 76 (66.7%) |
| Septic shock | 51 (44.7%) |
| Trauma | 46 (40.4%) |
| CA | 17 (14.9%) |
| 30-day mortality | 52 (45.6%) |
| Time do death [days] | 10.8 (26.2) |
| Hospital length of stay [days] | 18.5 (7.0-35.0) |
| ICU length of stay [days] | 9.5 (2.0-19.25) |
| Surgery | 78 (68.4%) |
| CRRT | 70 (61.4%) |
Continuous variables are presented as means (standard deviation) or medians (interquartile range) unless indicated otherwise; CA, cardiac arrest; ICU, intensive care unit; CRRT, continuous renal replacement therapy.
Table 2.
Characteristics of patients by 30-day mortality.
| Characteristics | Survivors, n = 62 (54.4%) | Non-survivors, n =52 (45.6%) | p-value |
| Male | 44 (71%) | 32 (61.3%) | |
| Age [years] | 45.4 (19.5) | 54 (19.5) | 0.021 |
| APACHE II [points] | 24.8 (6.5) | 28.9 (7.3) | 0.002 |
| SAPS [points] | 59.6 (16.0) | 70.5 (17.2) | < 0.001 |
| Hospital LOS [days] | 35.9 (23.8) | 10.0 (10.0) | < 0.001 |
| ICU LOS [days] | 23.3 (22.7) | 7.0 (8.1) | < 0.001 |
| CT FIBTEM [seconds] | 73.0 (63.0-98.5) | 94.5 (69.0-220.5) | 0.009 |
| A5 FIBTEM [mm] | 11.6 (8.2) | 11.6 (8.7) | 0.995 |
| MCF FIBTEM [mm] | 14.4 (10.3) | 15.0 (11.2) | 0.777 |
| ML FIBTEM [%] | 0.0 (0.0-0.0) | 0.0 (0.0-0.0) | 0.592 |
| CT EXTEM [seconds] | 74.5 (65.8-83.5) | 95.5 (72.0-176.3) | < 0.001 |
| MCF EXTEM [mm] | 57.4 (10.8) | 51.8 (17.1) | 0.044 |
| ML EXTEM [%] | 7.0 (3.0-13.0) | 4.0 (0.3-8.0) | 0.009 |
| CT INTEM [seconds] | 201.0 (175.8-251.0) | 268.0 (229.0-361.5) | < 0.001 |
| MCF INTEM [mm] | 53.6 (11.0) | 49.8 (14.8) | 0.138 |
| ML INTEM [%] | 7.0 (2.8-11.0) | 4.0 (0.0-9.0) | 0.035 |
| CT APTEM [seconds] | 67.0 (60.8-87.3) | 93.0 (75.3-186.0) | < 0.001 |
| MCF APTEM [mm] | 56.4 (10.1) | 52.1 (15.1) | 0.091 |
| ML APTEM [%] | 5.5 (2.0-11.0) | 3.0 (0.0-7.0) | 0.008 |
| INR | 1.3 (1.1-1.7) | 2.0 (1.4-3.4) | < 0.001 |
| aPTT [seconds] | 35.9 (32.7-49.4) | 54.6 (44.6-92.1) | < 0.001 |
| Fibrinogen [g/L] | 1.9 (1.2-2.9) | 2.2 (0.9-3.2) | 0.974 |
| D-dimer [μg/L] | 13.3 (6.0-35.2) | 17.4 (6.0-35.2) | 0.571 |
| pRBC [units] | 4.0 (2.0-9.0) | 2.0 (0.3-5.8) | 0.024 |
| FFP [units] | 2.0 (0.0-6.0) | 4.0 (2.0-8.0) | 0.022 |
| Platelets [units] | 0.0 (0.0-1.0) | 0.0 (0.0-1.8) | 0.5 |
| Cryoprecipitate [units] | 0.0 (0.0-0.0) | 0.0 (0.0-0.0) | 0.798 |
| Prothrombin concentrate [units] | 0.0 (0.0-0.0) | 0.0 (0.0-0.0) | 0.827 |
| Fibrinogen concentrate [grams] | 0.0 (0.0-2.0) | 2.0 (0.0-3.8) | 0.281 |
| mISTH-DIC | 17 (27.4) | 25 (48.1) | 0.023 |
| CRP [mg/L] | 39.1 (2.7-133.5) | 62.3 (3.1-133.5) | 0.491 |
| Procalcitonin [ng/mL] | 1.5 (0.6-11.6) | 4.2 (0.9-9.2) | 0.425 |
SAPS, The Simplified Acute Physiology Score; LOS, Length of Stay.
Table 3.
Multivariable logistic regression analysis of rotational thromboelastometry results associated with 30-day mortality in critically ill patients.
Table 3.
Multivariable logistic regression analysis of rotational thromboelastometry results associated with 30-day mortality in critically ill patients.
| Predictor | OR | 95% CI | p-value | |
| Model 1 including an external pathway of coagulation cascade | ||||
| CT EXTEM | 1.024 | 1.011-1.038 | < 0.001 | |
| Age in years | 1.027 | 1.003-1.051 | 0.026 | |
| APACHE II | 1.070 | 1.001-1.142 | 0.045 | |
| Model 2 including an internal pathway of coagulation cascade | ||||
| CT INTEM | 1.006 | 1.001-1.010 | 0.009 | |
| Age in years | 1.018 | 0.997-1.040 | 0.094 | |
| APACHE II | 1.065 | 1.001-1.134 | 0.047 | |
Table 4.
The correlation between CT EXTEM, CT INTEM, CCTs and outcomes.
| CT EXTEM | CT INTEM | |||
| Outcome | r | p-value | r | p-value |
| Hospital length of stay | -0.331 | < 0.001 | -0.292 | 0.002 |
| mISTH-DIC | 0.390 | < 0.001 | 0.373 | < 0.001 |
| INR | 0.599 | < 0.001 | ||
| aPTT | 0.718 | < 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



