
Submitted:
19 October 2025
Posted:
21 October 2025
You are already at the latest version
Abstract
High-risk pulmonary embolism (PE) is a life-threatening condition characterized by he-modynamic instability, often leading to catastrophic outcomes such as cardiac arrest and cardiogenic shock. We conducted a retrospective analysis of patients diagnosed with high-risk PE at a single tertiary center between 2018 and 2024. Catastrophic PE was de-fined as high-risk PE with hemodynamic collapse, including cardiac arrest and/or the requirement for high-dose vasopressors. Data on clinical characteristics, treatments, and outcomes were analyzed. Catastrophic PE accounted for 59% of cases. Systemic throm-bolysis was the most frequent reperfusion strategy (67%), while catheter-directed therapies (35.4%) and VA-ECMO (11.4%) were used selectively. Despite aggressive management, catastrophic PE exhibited significantly higher mortality rates at 7 days (40%) and 30 days (49%) compared to non-catastrophic cases (9% and 12.5%, respectively). These patients also showed higher rates of multiorgan failure and required more invasive support. This study underscores the importance of early recognition and tailored treatment strategies for catastrophic PE, highlighting its distinct clinical presentation and worse outcomes compared to non-catastrophic high-risk PE. Further research is essential to refine treatment protocols and improve survival in this critically ill population, emphasizing the utility of a standardized classification to enhance clinical management and research consistency.
Keywords:
pulmonary embolism
; high risk
; systemic thrombolysis
1. Introduction
High-risk pulmonary embolism (PE) is characterized by the presence of hemodynamic instability or obstructive shock at presentation, conditions strongly linked to high mortality rate. Despite variability among studies, an in-hospital mortality rate of 28% is reported for high-risk PE, increasing to over 65% in cases of cardiocirculatory arrest [1]. These discrepancies likely reflect differences in clinical severity, particularly the presence of profound obstructive shock, rather than hypotension alone. Importantly, high-risk PE encompasses not only low arterial pressure but also broader indicators of hemodynamic compromise, which may necessitate distinct therapeutic approaches.
Catastrophic PE is a term now increasingly recognized to describe the most critical cases of high-risk PE characterized by hemodynamic collapse, (those requiring high-dose vasopressors due to concern for impending cardiac arrest or experiencing cardiac arrest with or without cardiopulmonary resuscitation efforts) [2]. This study provides one of the first European perspectives to adopt the terminology of catastrophic PE, aiming to clarify its clinical significance and explore specific treatment outcomes.
This study offers one of the first European perspectives to adopt the term catastrophic pulmonary embolism (PE), aligning with emerging literature to better characterize the most critically ill subset of high-risk PE patients. By applying this terminology, we aim to clarify its clinical relevance and explore its implications for treatment and outcomes. Specifically, the objective of this study was to compare the clinical characteristics, management strategies, and mortality rates between patients with catastrophic and non-catastrophic high-risk PE treated at a single tertiary center.
2. Materials and Methods
We conducted a retrospective analysis of all patients diagnosed with high-risk PE at our single tertiary center from 2018 to 2024. High-risk PE was defined as hypotension with sustained systolic blood pressures below 90 mmHg, a drop of 40 mmHg or more from usual systolic blood pressure, or the need for vasopressor support [3]. At presentation, catastrophic PE was defined per Kobayashi et al.: those requiring high-dose vasopressors due to concern for impending cardiac arrest or experiencing cardiac arrest with or without cardiopulmonary resuscitation efforts [2]. High-dose vasopressors were defined as noradrenaline (NAd) dosing exceeding 0.4μg/kg/min or the concurrent use of two vasopressors [4]. Non-Catastrophic High-Risk PE included patients with sustained hypotension who did not meet the criteria for catastrophic PE. Haemorrhagic complications were classified as major bleeding episodes according to the Control of Anticoagulation Subcommittee of the ISTH [5], and reperfusion failure was defined as persistent clinical instability within the first 36 hours [6].
Data Collection and Statistical Analysis
Data on clinical characteristics, laboratory results, imaging tests, treatments, and outcomes were collected. Statistical analysis included the Mann-Whitney U test for non-normally distributed continuous variables, and Kaplan Meier survival analysis. Categorical variables were compared using chi-squared or Fisher’s exact tests. A two-sided p-value of less than 0.05 was considered statistically significant.
3. Results
During the study period, 79 patients with high-risk PE were included. Most of the patients were female (54.4%), with a mean age of 61.8 years and a body mass index of 29.9 kg/m². The diagnosis of PE was confirmed by computed tomography pulmonary angiogram (CTPA) in 96.2% of patients, and formal transthoracic echocardiography (TTE) was performed in 32.9%. Half of all patients (50.6%) experienced cardiac arrest at presentation, requiring cardiopulmonary resuscitation (CPR) with a median duration to Return of Spontaneous Circulation (ROSC) of 24 minutes. Most patients required vasopressors (75%) and mechanical ventilation (58.4%). Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) was performed in 9 patients (11.4%). Systemic thrombolysis (ST) was the most common reperfusion therapy, administered to 67% of patients, followed by catheter-directed therapies (CDT) in 35.4%, some patients received more than one therapy. Isolated anticoagulation was administered to 8 (10.1%) patients, and one patient underwent surgical embolectomy. Combined reperfusion therapies were employed in 19(24%) patients due to reperfusion failure: CDT was performed in 17 patients following ST, and ST was administered to 2 patients after CDT. Endovascular thrombectomy accounted for the majority of CDT cases (25 out of 28; 89%). The median ICU length of stay (LOS) was 5 days, with a total LOS of 13 days. Major bleeding occurred in 25.3% of patients. Unadjusted 7-day mortality was 27.8%, with 30-day and 90-day all-cause mortality rates of 34.2% and 36.7%, respectively (Table A1).
Differences between patients with catastrophic and non-catastrophic high-risk PE are summarized in Table 1. Forty-seven patients were classified as catastrophic high-risk PE (59.5%). Catastrophic PE patients were more likely to present with syncope (61.7% vs 31.3%; p = 0.005), lower mean arterial pressure (65 mmHg vs 76 mmHg; p = 0.012) and higher heart rate (102 bpm vs 87 bpm; p = 0.029). Blood tests revealed significantly higher serum lactate levels (74.9 mg/dl vs. 12.7 mg/dl; p =< 0.001), SpO2/FiO2 ratio (203 vs 260; p = 0.013), PaCO2 (54.2 mmHg vs. 35.6 mmHg; p =< 0.001), creatinine (1.54 mg/dl vs 0.94 mg/dl; p =< 0.001), High-sensitivity Troponin I (1727.7 ng/ml vs 44.2 ng/ml; p = 0.011) and liver enzymes. They also required mechanical ventilation more frequently (81% vs. 22%; p =< 0.001) and were more likely to need vasopressors. Multiorgan failure was more common in catastrophic PE (34% vs 6.3%; p = 0.002). Consequently, SAPS II and SOFA severity scoring were higher too (76 vs 30; p < 0.001 and 11 vs 5; p < 0.001, respectively).
Regarding treatment, patients with catastrophic PE were more likely to receive ST (89% vs 43.8%; p = 0.001) and VA-ECMO (19%vs 0%; p = 0.009) without significant differences in the use of CDT (34% vs 37.5%; p = 0.830). Reperfusion failure was more common in catastrophic PE patients (34% vs 9.4%; p = 0.015).
Finally, unadjusted 7-day, 30-day, and 90-day hospital mortality rates were significantly higher in catastrophic PE patients compared to non-catastrophic patients (7-day: 40.4% vs 9.4%, p = 0.002; 30-day: 49% vs 12.5%, p = 0.002; 90-day: 49% vs 19%, p = 0.024), as illustrated in Figure 1. Catastrophic PE patients had also shorter LOS (7 days vs 15 days; p = 0.05), with no significant differences in major bleeding compared to patients with non-catastrophic high-risk PE.
4. Discussion
This study presents a cohort of high-risk PE patients with a 30-day mortality rate of 34% and a major bleeding rate of 25.3%. These results align with previous observational studies, which have reported mortality rate ranging from 20% to 60% [7,8] as well as similar patterns of bleeding complications. Notably, most patients in our cohort received reperfusion therapies, with systemic thrombolysis being the most frequent (65%), contrasting with earlier reports that indicated lower rates of reperfusion in real-world settings[9]. Our findings highlight key differences in clinical presentation, treatment requirements, and outcomes between patients with catastrophic high-risk PE and those with high-risk PE without hemodynamic collapse. Patients with catastrophic PE exhibited more profound hemodynamic instability, higher rates of multiorgan failure, and were more likely to receive mechanical ventilation and VA-ECMO. Importantly, this group also demonstrated markedly elevated serum lactate levels (74.9 mg/dl vs 12.7 mg/dl) alongside other markers of organ dysfunction such as creatinine, PaCO2, liver enzymes, and High-sensitivity Troponin I. The significantly higher lactate levels observed in catastrophic PE patients suggest that lactate may serve as a useful biomarker to identify individuals at risk of progressing to hemodynamic collapse. This opens the possibility of using lactate to further stratify patients within the sustained hypotension phenotype, potentially distinguishing those with early signs of obstructive cardiogenic shock. While previous studies have shown that elevated lactate levels in hemodynamically stable PE patients can predict adverse outcomes [10], its role in high-risk PE populations remains less defined and warrants further investigation.
Additionally, patients with catastrophic PE had a higher rate of systemic thrombolysis (83.3% vs 46.4%), reflecting the urgency for reperfusion in severely unstable patients, where invasive techniques may be less feasible.
These findings are consistent with Kobayashi et al., who described a similar trend in more critically ill patients [2]. However, our cohort had a higher incidence of cardiac arrest at presentation (50.6%), which may explain why our patients were twice as likely to receive systemic thrombolysis in comparison.
Our findings are further contextualized by the recent work of Stadlbauer et al., who reported on a large cohort of high-risk PE patients, emphasizing a broader management approach [11]. Their observations, particularly regarding the benefit of VA-ECMO for stabilization in severe presentations to facilitate subsequent reperfusion strategies, align with the clinical course and interventions observed in our catastrophic PE cohort. This underscores the evolving paradigm for managing the most critically ill PE patients, where advanced hemodynamic support, such as VA-ECMO, plays a crucial role in enabling definitive therapies.
Importantly, this study is among the first European investigations to use the term catastrophic PE, marking a further step in standardizing terminology for more precise patient stratification and treatment strategies.
5. Conclusions
These findings underscore the importance of early identification and tailored management strategies for catastrophic PE. Given the high mortality and complexity of treatment in this very high-risk population, further research is needed to refine treatment protocols and explore additional therapeutic options to improve patient outcomes. Furthermore, this study emphasizes the utility of the term catastrophic PE, paving the way for its broader adoption in clinical practice to enhance stratification and management of the most critically ill patients
6. Limitations
Limitations of the present study are its descriptive and uncontrolled design as well as its single-center setting, which may affect the generalizability of the findings. Additionally, the relatively small sample size, particularly in the subgroup analyses, reduces the statistical power.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org: Baseline Characteristics of 79 patients with High-Risk PE.
Author Contributions
Conceptualization, J.M. and J.O.; methodology, J.M., JO and M.M.; formal analysis, J.O. I.E. and M.M.; data curation, J.M., NA and I.E.; writing—original draft preparation, M.M.; writing—review and editing, J.M, J.O, P.C, JA, AG, ES, SJ; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Hospital Clínic de Barcelona (HCB/2025/0169) on May 20th, 2025.
Acknowledgments
During the preparation of this manuscript, the authors used Microsoft Copilot for grammar editing. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ALT | Alanin Aminotransferase |
| AST | Aspartate Aminotransferase |
| COPD | Chronic Obstructive Pulmonary Disease |
| CTPA | Computed Tomography Pulmonary Angiography |
| CPR | Cardiopulmonary Resuscitation |
| ICU | Intensive Care Unit |
| LOS | Lenght of Stay |
| PE | Pulmonary Embolism |
| ROSC | Return of Spontaneous Circulation |
| TTE | Transthoracic Echocardiography |
| VA-ECMO | Venoarterial Extracorporeal Membrane Oxygenation |
| eCPR | Venoarterial Extracorporeal Membrane Oxygenation during CPR |
Appendix A

Table A1.
Baseline Characteristics of 79 patients with High-Risk PE.
| Demographics | |
| Age (years) ± SD | 61,8 ± 15.3 |
| Sex (female) n (%) | 43 (54.4%) |
| Body Mass Index (Kg/m2) ± SD | 29.9 ± 7.7 |
| Past medical history | |
| Smoking n (%) | 32 (40.5) |
| Arterial hypertension, n (%) | 33 (41.8) |
| Dyslipidemia, n (%) | 29 (36.7) |
| History of cancer, n (%) | 16 (20.3) |
| Diabetes mellitus, n (%) | 11 (13.9) |
| Chronic obstructive pulmonary disease, n (%) | 9 (11.4) |
| Chronic renal disease, n (%) | 6 (7.6) |
| History of stroke, n (%) | 5 (6.3) |
| History of liver disease, n (%) | 3 (3.8) |
| Atrial fibrillation, n (%) | 3 (3.8) |
| Coronary artery disease, n (%) | 2 (2.5) |
| Previous myocardial infarction, n (%) | 2 (2.5) |
| Previous percutaneous coronary intervention, n (%) | 2 (2.5) |
| History of coagulopathy, n (%) | 1 (1.3) |
| History of platelet dysfunction, n (%) | 1 (1.3) |
| Chronic heart failure, n (%) | 1 (1.3) |
| Predisposing factors for venous thrombo-embolism | |
| Prolonged bed rest, n (%) | 19 (24.1) |
| Surgery 1-2 weeks previous (%) | 13 (16.5) |
| Immobilization, n (%) | 14 (17.7) |
| Hystory of thromboembolic disease, n (%) | 10 (12.7) |
| Active Cancer, n (%) | 9 (11.4) |
| Deep vein thrombosis, n (%) | 8 (10.1) |
| Hormonal contraceptives (%) | 4 (5.1) |
| Clinical Presentation | |
| Sudden Dyspnea, n (%) | 70 (88.6) |
| Cardiac arrest, n (%) | 40 (50.6) |
| Syncope, n (%) | 39 (49.4) |
| Cardiogenic shock, n (%) | 31 (39.2) |
| Chest pain, n (%) | 20 (25.3) |
| Fever, n (%) | 4 (5.1) |
| Hemoptysis, n (%) | 1 (1.3) |
| Cardiopulmonary resucitation, n (%) | 40 (50.6) |
| CPR duration (min), median [IQR] | 24 [9-43] |
| eCPR, n (%) | 3 (3.8) |
| Diagnostic tests | |
| CTPA, n (%) | 76 (96.2) |
| TTE at presentation, n(%) | 26 (32.9) |
| RV disfunction, n (%); n = 26 | 26 (100) |
| TAPSE [mm], (SD); n = 17 | 15.6 +- 9.6 |
| PASP [mmHg], (SD); n = 12 | 38 +- 29.9 |
| Intracavitary thrombus(%); n = 17 | 1 (5.6) |
| Treatment | |
| Un-fractioned Heparin, n(%) | 62 (78.5) |
| Argatroban, n(%) | 1(1.3) |
| Lepirudin, n(%) | 1(1.3) |
| Systemic thrombolysis, n(%) | 53 (67%) |
| Pre-hospital ST, n(%); n = 53 | 15 (28.3) |
| In-hospital ST, n(%); n = 53 | 38 (71.7) |
| Catheter directed therapies, n(%) | 28 (35.4) |
| Endovascular thrombectomy, n(%); n = 28 | 25 (89.3) |
| Catheter directed thrombolysis, n(%); n = 28 | 6(21.4) |
| Surgical embolectomy, n(%) | 1(1.3) |
| Support treatment | |
| Mechanical Ventilation, n(%) | 45 (58.4) |
| Norepinephrine, n(%) | 59 (74.7) |
| Epinephrine, n(%) | 23 (29.1) |
| Dobutamine, n(%) | 40 (50.6) |
| Vasopressin n(%) | 1 (1.3) |
| VA-ECMO n(%) | 9 (11.4) |
| Vital signs | |
| Systolic blood pressure [mmHg], median [IQR] | 115 [101-125] |
| Mean blood pressure [mmHg], median [IQR] | 77 [70-87] |
| Heart rate [beats per minute], median [IQR] | 90 [84-105] |
| SpO2/FiO2 ratio, ± SD | 316 ±108 |
| Outcomes | |
| Major bleeding*, n (%) | 20 (25.3) |
| Reperfusion failure, n (%) | 19 (24) |
| Stroke, n (%) | 4 (5.1) |
| Recurrent PE, n (%) | 5 (7.1) |
| Ventilator Associated Pneumonia, n (%) | 11 (13.9) |
| Multiorgan failure, n (%) | 18 (22.8) |
| Sepsis, n (%) | 9 (11.4) |
| Acute Kidney Injury, n(%) | 39 (49.4) |
| Renal replacement therapy, n(%) | 6 (7.6) |
| ICU LOS, days, median [IQR] | 5 [2-20] |
| LOS, days, median [IQR] | 13 [4-32] |
| 7- days mortality, n(%) | 22 (27.8) |
| 30-days mortality, n (%) | 27 (34.2) |
| 90- days mortality, n(%) | 29 (36.7) |
CTPA: computed tomography pulmonary angiography; ICU: Intensive Care Unit; LOS: length of stay; TTE: transthoracic echocardiography; eCPR: Venoarterial extracorporeal membrane oxygenation during cardiopulmonary resuscitation.
References
- Chopard, R.; Behr, J.; Vidoni, C.; Ecarnot, F.; Meneveau, N. An Update on the Management of Acute High-Risk Pulmonary Embolism. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Pugliese, S.; Sethi, S.S.; Parikh, S.A.; Goldberg, J.; Alkhafan, F.; Vitarello, C.; Rosenfield, K.; Lookstein, R.; Keeling, B.; et al. Contemporary Management and Outcomes of Patients With High-Risk Pulmonary Embolism. J Am Coll Cardiol 2024, 83, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S. V.; Meyer, G.; Bueno, H.; Galié, N.; Gibbs, J.S.R.; Ageno, W.; Agewall, S.; Almeida, A.G.; Andreotti, F.; Barbato, E.; et al. 2019 ESC Guidelines for the Diagnosis and Management of Acute Pulmonary Embolism Developed in Collaboration with the European Respiratory Society (ERS). Eur Heart J 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Pölkki, A.; Pekkarinen, P.T.; Hess, B.; Blaser, A.R.; Bachmann, K.F.; Lakbar, I.; Hollenberg, S.M.; Lobo, S.M.; Rezende, E.; Selander, T.; et al. Noradrenaline Dose Cutoffs to Characterise the Severity of Cardiovascular Failure: Data-Based Development and External Validation. Acta Anaesthesiol Scand 2024, 68, 1400–1408. [Google Scholar] [CrossRef] [PubMed]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S. Definition of Clinically Relevant Non-Major Bleeding in Studies of Anticoagulants in Atrial Fibrillation and Venous Thromboembolic Disease in Non-Surgical Patients: Communication from the SSC of the ISTH. Journal of Thrombosis and Haemostasis 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Meneveau, N.; Séronde, M.-F.; Blonde, M.-C.; Legalery, P.; Didier-Petit, K.; Briand, F.; Caulfield, F.; Schiele, F.; Bernard, Y.; Bassand, J.-P. Management of Unsuccessful Thrombolysis in Acute Massive Pulmonary Embolism. Chest 2006, 129, 1043–1050. [Google Scholar] [CrossRef]
- Lin, B.W.; Schreiber, D.H.; Liu, G.; Briese, B.; Hiestand, B.; Slattery, D.; Kline, J.A.; Goldhaber, S.Z.; Pollack, C. V. Therapy and Outcomes in Massive Pulmonary Embolism from the Emergency Medicine Pulmonary Embolism in the Real World Registry. American Journal of Emergency Medicine 2012, 30, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Calé, R.; Ascenção, R.; Bulhosa, C.; Pereira, H.; Borges, M.; Costa, J.; Caldeira, D. In-Hospital Mortality of High-Risk Pulmonary Embolism: A Nationwide Population-Based Cohort Study in Portugal from 2010 to 2018. Pulmonology 2024, 000. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, D.; Bikdeli, B.; Barrios, D.; Quezada, A.; Del Toro, J.; Vidal, G.; Mahé, I.; Quere, I.; Loring, M.; Yusen, R.D.; et al. Epidemiology, Patterns of Care and Mortality for Patients with Hemodynamically Unstable Acute Symptomatic Pulmonary Embolism. Int J Cardiol 2018, 269, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Vanni, S.; Socci, F.; Pepe, G.; Nazerian, P.; Viviani, G.; Baioni, M.; Conti, A.; Grifoni, S. High Plasma Lactate Levels Are Associated with Increased Risk of In-Hospital Mortality in Patients with Pulmonary Embolism. Academic Emergency Medicine 2011, 18, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, A.; Verbelen, T.; Binzenhöfer, L.; Goslar, T.; Supady, A.; Spieth, P.M.; Noc, M.; Verstraete, A.; Hoffmann, S.; Schomaker, M.; et al. Management of High-Risk Acute Pulmonary Embolism: An Emulated Target Trial Analysis. Intensive Care Med 2025. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan Meier 90-day mortality curves comparing patients diagnosed with catastrophic Pulmonary Embolism and non-catastrophic Pulmonary Embolism.
Figure 1.
Kaplan Meier 90-day mortality curves comparing patients diagnosed with catastrophic Pulmonary Embolism and non-catastrophic Pulmonary Embolism.
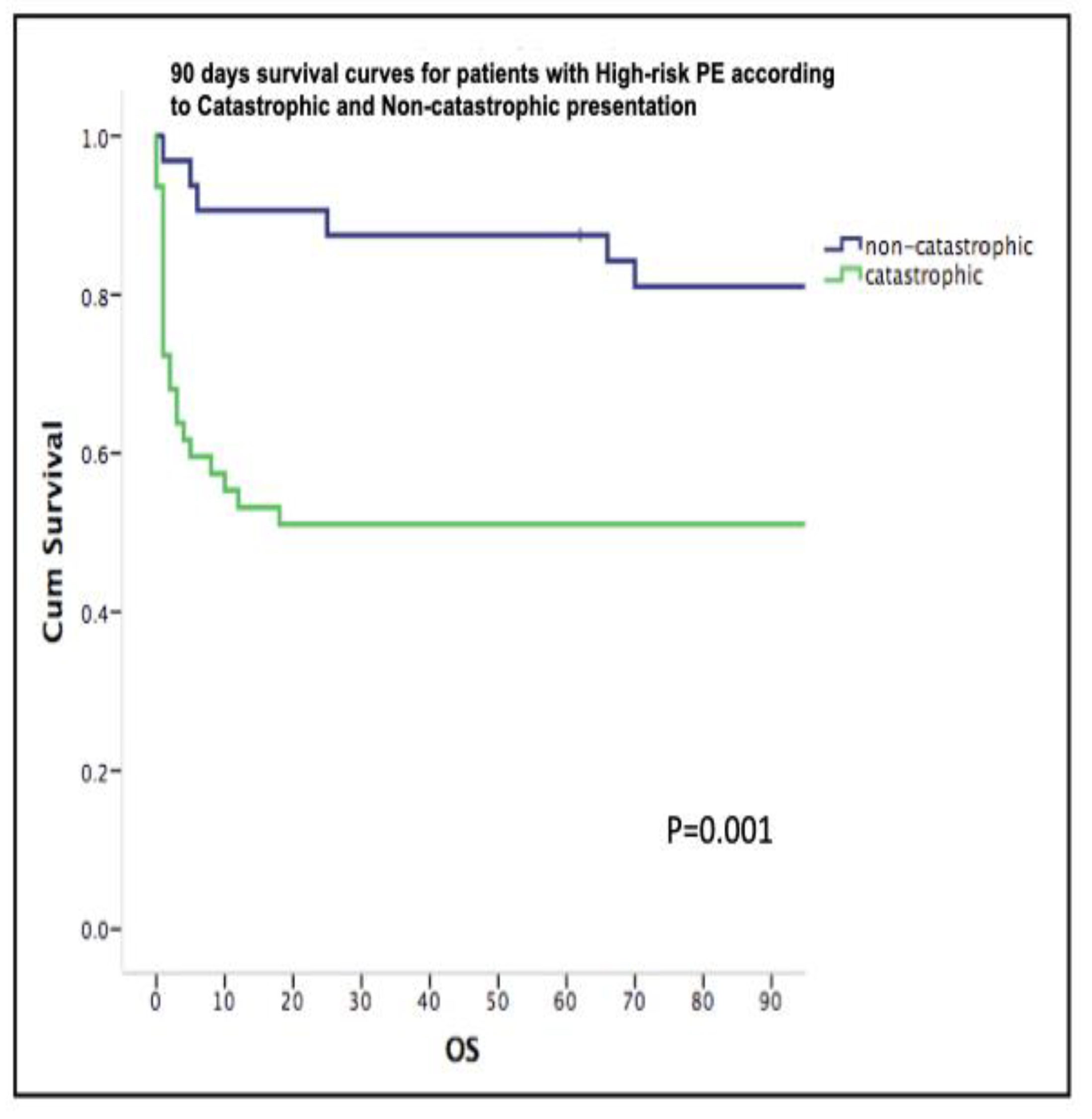
Table 1.
Baseline characteristics in Catastrophic and Non-catastrophic High-risk PE.
|
Catastrophic PE n = 47 |
High-Risk PE n = 32 |
p value | |
| Demographics | |||
| Age [years], ± SD | 60.4 ± 16.5 | 63.8 ± 13.2 | 0.614 |
| Sex [male], n (%) | 19 (40.4) | 17 (53.1) | 0.077 |
| Body mass index [kg/m²], ± SD | 28.6 ± 6.2 | 31.7 ± 9 | 0.495 |
| Past medical history | |||
| Smoking, n (%) | 18 (38.3) | 14(47.8) | 0.815 |
| Arterial hypertension, n (%) | 16 (34) | 15 (53.12) | 0.108 |
| Dyslipidemia, n (%) | 14 (29.8) | 15 (46.9) | 0.156 |
| Diabetes mellitus, n (%) | 6 (12.8) | 5 (15.6) | 0.750 |
| History of stroke, n (%) | 2 (4.3) | 3 (9.4) | 0.475 |
| History of liver disease, n (%) | 1 (2.1) | 2 (6.3) | 0.383 |
| History of cancer, n (%) | 7(14.9) | 9 (28.1) | 0.167 |
| COPD, n (%) | 4 (8.5) | 5(13.5) | 0.473 |
| Atrial fibrillation, n (%) | 0 | 3 (9.4) | 0.063 |
| Chronic heart failure, n (%) | 0 | 1 (3.1) | 0.405 |
| Coronary artery disease, n (%) | 0 | 2 (6.3) | 0.161 |
| Chronic renal disease, n (%) | 4 (8.5) | 2 (6.3) | 0.533 |
| Predisposing factors for venous thrombo-embolism | |||
| Hormonal contraceptives (%) | 4 (8.5) | 0 | 0.140 |
| Surgery 1-2 weeks previous (%) | 7 (14.9) | 6 (18.8) | 0.764 |
| Prolonged bed rest, n (%) | 10 (21.3) | 9 (28.1) | 0.596 |
| Immobilization (%) | 7 (14.9) | 7 (21.9) | 0.552 |
| Hystory of thromboembolic disease (%) | 5(10.6) | 5 (15.6) | 0.540 |
| Active Cancer, n (%) | 3 (6.4) | 6 (18.8) | 0.149 |
| Clinical presentation | |||
| Sudden Dyspnea, n (%) | 40 (85.1) | 30 (93.75) | 1 |
| Syncope, n (%) | 29 (61.7) | 10 (31.3) | 0.005 |
| Chest pain, n (%) | 10 (21.3) | 10 (31.3) | 0.598 |
| Fever, n (%) | 0 | 4 (12.5) | 0.030 |
| Hemoptysis, n (%) | 0 | 1 (3.1) | 0.427 |
| Lung infarction, n (%) | 17 (36.2) | 7 (21.9) | 0.210 |
| Inferior Vena Cava Reflux, n(%) | 21 (44.7) | 17 (53.1) | 0.797 |
| Laboratory at admission | |||
| Lactate [mg/dl], median [IQR] | 74.9 [40.75-127.8] | 12.7 [8.2-22.7] | <0.001 |
| pH, median [IQR] | 7.238 [6.99-7.33] | 7.436 [7.36-7.47] | <0.001 |
| PaO2 [mmHg], median [IQR] | 113 [72.1-203.9] | 69.3 [51.6-88.9] | <0.001 |
| PaCO2 [mmHg], median [IQR] | 54.2 [42.4-74.8] | 35.6 [29.8-41] | <0.001 |
| Creatinine [mg/dl], mean (SD) | 1.54 [1.19-2.2] | 0.94 [0.66-1.26] | <0.001 |
| Bilirrubin [mg/dl], median [IQR] | 1 [0.5-1.6] | 0.8 [0.5-1] | 0.097 |
| AST [U/I], median [IQR] | 244.5 [110.3-681] | 28 [17.3-54.5] | <0.001 |
| ALT [U/I], median [IQR] | 242.5 [80.3-440.3] | 27.5[13-80.3] | <0.001 |
| GGT [U/I], median [IQR] | 95 [42-191] | 39 [22.8-67.3] | 0.002 |
| Hemoglobin [g/dl], median [IQR] | 12.9 [11.2-14.4] | 11.8 [10.4-13.3] | 0.148 |
| Leukocyte count [G/l], median [IQR] | 15 [10.4-20.6] | 12.7 [7.9-14.9] | 0.016 |
| Platelet count [G/l], median [IQR] | 176 [123-230.8] | 211 [174-290] | 0.07 |
| Fibrinogen [mg/dl], median [IQR] | 1.8 [0.5-3.5] | 4.5 [3.4-5.5] | 0.003 |
| aPTT [sec], median [IQR] | 46 [30.8-88.3] | 32.1 [25.2-36.9] | 0.001 |
| INR, median [IQR] | 1.58 [1.33 2.5] | 1.23 [1.12-1.32] | <0.001 |
| HS Troponin I | 1727.7 [3.7-3960] | 44.2 [1.03-392.4] | 0.011 |
| C-reactive protein [mg/dl], median [IQR] | 3.91 [1.4-10.5] | 5.27 [2.7-16.78] | 0.080 |
| Severity scoring systems at admission | |||
| SAPS II score, median [IQR] | 76 [60-90] | 30 [22-35.8] | <0.001 |
| SOFA score, median [IQR] | 11 [8-13] | 5 [3-6] | <0.001 |
| Supportive care | |||
| Mechanical Ventilation, n (%) | 38 (80.9) | 7 (21.9) | <0.001 |
| Noradrenaline, n (%) | 42 (89.4) | 17 (53.1) | <0.001 |
| Dobutamine, n(%) | 31 (66) | 9 (28.1) | 0.001 |
| Adrenaline, n (%) | 22 (46.8) | 1 (3.1) | <0.001 |
| Inferior Vena Cava Filter, n(%) | 9 (19.1) | 13 (40.6) | 0.122 |
| VA-ECMO, n(%) | 9 (19.1) | 0 | 0.009 |
| Treatment | |||
| Un-fractioned Heparin, n(%) | 36 (76.6) | 26 (81.3) | 1 |
| Systemic thrombolysis, n(%) | 39 (83) | 14 (43.8) | 0.001 |
| Alteplase, n(%) | 31 (66) | 10 (31.3) | 0.006 |
| Tenecteplase, n(%) | 7 (14.9) | 2 (6.3) | 0.300 |
| Catheter directed therapies, n(%) | 16 (34) | 12 (37.5) | 0.803 |
| Surgical embolectomy, n(%) | 1 (2.1) | 0 | 1 |
| Treatment sequence | |||
| Anticoagulation alone, n(%) | 3 (6.4) | 5 (15.6) | .001 |
| First line Systemic thrombolysis, n(%) | 38 (80.9) | 13 (40.6) | |
| First line Catheter directed Therapies, n(%) | 5 (10.6) | 14 (43.8) | |
| First line Surgical embolectomy, n(%) | 1 (2.1) | 0 | |
| Vital signs | |||
| Systolic blood pressure (mmHg), median [IQR] | 90 [81.3-107] | 110 [91.5-126] | 0.006 |
| Mean blood pressure (mmHg), median [IQR] | 65 [59.5-76] | 76 [65-85] | 0.012 |
| Heart rate (bpm), median [IQR] | 102 [87.8-120] | 87 [85-110] | 0.029 |
| SpO2/FiO2 ratio, ± SD | 203 ± 83 | 260 ± 100 | 0.013 |
| Vital signs at 48hrs | |||
| Systolic blood pressure (mmHg), median [IQR] | 104 [90-123] | 120 [111-125] | 0.014 |
| Mean blood pressure (mmHg), median [IQR] | 69 [65-81] | 78 [75-93] | 0.002 |
| Heart rate (bpm), median [IQR] | 100 [86-110] | 87 [82-97] | 0.015 |
| SpO2/FiO2 ratio, ± SD | 283 ± 119 | 344 ± 93 | 0.036 |
| Outcomes | |||
| Major bleeding*, n (%) | 14 (29.8) | 6 (18.8) | 0.194 |
| Stroke, n (%) | 4 (8.5) | 0 | 0.129 |
| Recurrent PE, n (%) | 1 (2.1) | 4 (12.5) | 0.159 |
| Ventilator Associated Pneumonia, n (%) | 6 (12.8) | 5 (15.6) | 1 |
| Multiorgan failure, n (%) | 16 (34) | 2 (6.3) | 0.002 |
| Sepsis, n (%) | 5 (10.6) | 4 (12.5) | 1 |
| Acute Kidney Injury, n(%) | 27 (57.4) | 12 (37.5) | 0.037 |
| Renal replacement therapy, n(%) | 5 (10.6) | 1 (3.1) | 0.231 |
| ICU LOS, days, median [IQR] | 6 [1-19.5] | 5 [4-22] | 0.302 |
| LOS, days, median [IQR] | 7 [1-36] | 15 [8.5-29.3] | 0.05 |
| 7 days mortality, n (%) | 19 (40.4) | 3 (9.4) | 0.002 |
| 30-days mortality, n (%) | 23 (48.9) | 4 (12.5) | 0.001 |
| 90-days mortality, n (%) | 23 (48.9) | 6 (18.8) | 0.009 |
| Reperfusion failure, n(%) | 16 (34) | 3 (9.4) | 0.015 |
COPD: Chronic Obstructive Pulmonary Disease; CTPA: computed tomography pulmonary angiography; ICU: Intensive Care Unit; LOS: length of stay; TTE: transthoracic echocardiography; VA-ECMO: Venoarterial extracorporeal membrane oxygenation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



