Submitted:
23 December 2024
Posted:
25 December 2024
You are already at the latest version
Abstract
The retrospective study was carried out in the II Obstetrics-Gynecology Clinic of the "Sf Apostol Andrei" Constanta County Emergency Clinical Hospital on a group of 171 patients who presented with placental abruption and gave birth in the clinic. The patients were selected from the case file of our clinic among the patients who presented placental abruption. The study included only patients aged between 18 and 30 years, an interval considered by us to be the most suitable for reproduction. We took this approach to ensure that the age factor did not influence the study results. Patient observation sheets and operative protocol registers were used as working material. The patients were categorized based on age, gestational grade, parity, type of presentation, gender of the fetus, live births by Apgar score, and hematoma volume. Particular attention was given to the following factors: types of anesthesia, types of incisions, emergency hysterectomies. A total of 17 emergency hysterectomies were performed and 38 cases of fetal mortality were encountered. Male fetuses predominated at 55.5%. Placental abruption remains one of the biggest obstetric emergencies, both due to the large number of complications it associates with and due to their evolution that can often be unpredictable.
Keywords:
placental abruption
; retroplacental hemorrhages
; fetal death
1. Introduction
- Historical
Riglay was the first to describe, in 1811 [1,2], the retroplacental hematoma; Baudeloque in 1832 isolates retroplacental hematoma from hemorrhagic syndromes calling it “hidden hemorrhage” and describes “retroplacental depression” [3]. Pinard and Varnier in 1892 specified the location of the hematoma, caducus serotin [3]. De Lee, in 1901, described, on the occasion of a retroplacental hematoma, the syndrome of hemorrhage due to acquired afibrinogenemia, whose pathogenic explanation was given in 1936 by Dieckmann [1]. Couvelaire, in 1911, uses the term “uteroplacental apoplexy” [4] which clinically corresponds not only to a detachment of the placenta, but to a set of blood suffusions that can extend to the entire genital apparatus and even to other viscera. He, therefore, replaces the purely anatomical conception of the hematoma, with a complex of etiological and pathogenic notions. The condition is not only a local accident but the vascular manifestation of a general illness. The importance of this new notion has caused it to be called “Couvelaire’s disease” in Anglo-Saxon countries. In 1942, Young named it “Obstetrical Crush Syndrome” due to severe uterine hemorrhagic suffusions (crush syndrome phenomenon) [2]. From a pathogenic point of view, Reilly succeeded in experimentally reproducing uteroplacental apoplexy lesions [1].
Although there is no unanimous consensus on the nomenclature and the production mechanism, these terms mean the detachment of the placenta before the expulsion of the fetus due to a hemorrhage produced in the thickness of the basal decidua. Specialized literature uses several names to define this condition: placental abruption, uteroplacental hematoma, uteroplacental apoplexy, retro-placental hematoma, abruptio placentae, and ablatio placentae. Pritchard proposes the classification of the syndrome according to the clinical appearance and the type of bleeding, which can be external (encountered in 80% of cases); in this case, the hematoma detaches the membranes, externalizing via the vaginal route. Internal bleeding occurs in about 20% of cases. [2,4]. Another classification, proposed by Benson (1984), divides the syndrome into premature detachment of the normally inserted placenta, which can be either total or partial. [1,4].
To distinguish it from placenta praevia hemorrhage, in Anglo-Saxon countries the term accidental hemorrhage is used for placental abruption, because in placenta praevia the bleeding is unprovoked [2,4,5].
Leaving aside this rich terminology proposed by various authors, today it is customary to name the condition by the generic term of premature detachment of the normally inserted placenta.
2. Materials and Methods
The retrospective study was carried out in the II Obstetrics-Gynecology Clinic of the “Sf Apostol Andrei” Constanta County Emergency Clinical Hospital on a group of 171 patients who presented with placental abruption and gave birth in the clinic. The patients were selected from the case file of our clinic among the patients who presented premature detachment of the normally inserted placenta. The study included only patients aged between 18 and 30 years, an interval considered by us to be the most suitable for reproduction.
Patient observation sheets and operative protocol registers were used as working material. The patients were categorized based on gestational grade, parity, type of presentation, gender of the fetus, live births by Apgar score, and hematoma volume. Particular attention was given to the following factors: types of anesthesia, types of incisions, emergency hysterectomies.
3. Results
In the entire patient group, 0.79% were under 18 years old, 67.58% were between 18 and 30 years old, and 31.62% were over 30 years old.
Within the studied group, there were 171 patients between the ages of 18 and 30.
The distribution of patients by gestational stage was as follows (Table 1):
The distribution of patients by degree of parity was as follows (Table 2):
Of the 173 newborns, 38 were dead (22 male, 16 female) and 135 alive (74 male, 61 female) (Chart 1).
The Apgar score distribution of the live babies was as follows (Chart 2):
161 fetuses were found in cranial presentation, and 9 fetuses were in pelvic presentation. In 3 cases, the presentation type was not specified due to the small gestational age.
2 cases of twin pregnancy were encountered.
The distribution according to the volume of the retroplacental hematoma was as follows (Chart 3):
A case of true umbilical cord knot was encountered.
109 spinal anesthesias, 59 general anesthesias with O.T.I., 2 epidural anesthesias, and one subarachnoid anesthesia were performed (Chart 4).
70 incisions were of median pubosubumbilical type and 101 Phannenstiel type.
17 necessary hysterectomies were performed as follows: 2 subtotal hysterectomies, 4 total hysterectomies with bilateral adnexectomy, 2 total hysterectomies with left adnexectomy and 9 total hysterectomies (Chart 5).
4. Discussion
Leaving aside this rich terminology proposed by various authors, today it is customary to name the condition by the generic term of premature detachment of the normally inserted placenta. The possibility of its manifestation under two anatomical-clinical aspects is also admitted:
- retroplacental hematoma consists in the rapid formation of a blood collection between the maternal face of the placenta and the uterine wall, before the expulsion of the fetus, after the 20th week of gestation; it is a milder lesion, with reduced symptoms and often discovered only during the inspection of the placenta or during routine ultrasound checks; in this case, the detachment is mild, it may involve one or two placental cotyledons; larger hematomas can also be found, located in the center of the placenta, which can take off up to 50% of the placental surface and can also have an important clinical impact.
- The recurrence
The risk of recurrence of placental abruption in subsequent births is increased [7,8]. A study by Pritchard et al (1970) reported a recurrence of 1:8 [9], while in their study, Hibbard and Jeffcoate (1966) observed a recurrence of 1:6 [2]. Karegard and Gennser, in a study conducted in 1986, report a recurrence of 1:10 [1]. They also note that placental abruption can occur at any time, even far from term or at an early stage; after the initial period of fetal well-being, fetal death can occur rapidly. [1,10,11,12,13,14].
Most authors consider that the placental abruption, in one of its forms, is a manifestation of dysgravity equivalent to some extent to eclampsia. It is also admitted that retroplacental hemorrhages would be nothing more than the noisy local manifestation, at the level of the uterus, of a general syndrome likely to damage different organs and especially the kidney (renal lesions, generally less expressed and manifested later, can sometimes be particularly serious: “crush syndrome” with oliguria and uremia) [2,4,6,15].
The incidence of placental abruption was 0.56% of the total number of births. The specialized literature reports incidences of placental abruption between 0.5 and 1.5% of births for singleton pregnancies [1,3,10,11,16,17].
The distribution of patients by gestational and parity degrees did not provide significant data regarding the etiology of the disease. On the studied group, primigeste and primiparous patients predominated (Table 1, Table 2).
Placental abruption is a condition frequently associated with fetal suffering or mortality [1,3,10,11,12,13,14,15,16,17,18,19].
The large number of dead fetuses, 38 out of 173 (Chart 1), certifies the fact that placental abruption represents perhaps the largest and most complex obstetric emergency. Fetal mortality was 21.96% of cases, a percentage in accordance with the reports of specialized studies [1,3,10,11,12,13,14,15,16,17].
The efficiency of the on-call teams in our clinic in detecting this condition as quickly as possible and implementing its surgical solution in the optimal time is supported by the large number of live children who had Apgar scores 7 or above—104 children (Chart 2).
A percentage of 40% of the fetuses had Apgar scores below 7, practically associating different degrees of fetal distress.
Male fetuses predominated (55.5%).
Among the dead, 57.9% were male, and among the living, 54.8% were male.
Placental abruption is a last-trimester dysgravity that often requires the initiation of premature birth, associating various degrees of fetal prematurity [1,3,18,20,21]. In the studied group, 4.66% of the fetuses had a gestational age under 32 weeks, 4.66% between 32 and 34 weeks and 35.79% between 34 and 37 weeks. Specialized literature defines as premature any birth occurring before 37 gestational weeks [2]. In the studied group, 45.13% of the fetuses were born before 37 weeks of gestation (premature).
A percentage of 35.01% of the fetuses weighed less than 2500 g.
Intrauterine growth restriction of the fetus is found in approximately 3-10% of normal pregnancies [4]. The fact that 35% of the fetuses had birth weights below 2500 g is due to both prematurity and intrauterine growth restriction of the fetus, found especially in patients with essential hypertension aggravated by pregnancy [5].
The cranial presentation was found in a percentage of 93%. Pelvic presentation was found in 5.2% of cases, and those unspecified due to small gestational ages in 1.73% of cases. Vicious presentations can be etiological factors of placental abruption [1,3,21].
As the placental abruption represents a major obstetric emergency [1,3,6,10,11,12,13,14,15,18,19,21], a percentage of 41.1% of the incisions were of the median pubosubumbilical type, 34.38% of the anesthetics were general with O.T.I (Chart 4).
There are no precise methods for predicting placental abruption, existing methods having a prediction accuracy of 12-13% [22].
In most cases the patient is pale, sweaty, anxious.
The pain caused by the permanent contraction of the uterus - the wooden uterus - described by Couvelaire, is an important symptom but it can be easily confused with the pain caused by the bursting or torsion of an ovarian cyst [23] especially in pregnant women who associate ovarian tumors.
Placental vasculature can undergo substantial changes in these cases. Injection of placental arteries with plastic can prove this fact [24,25]
Hysterectomy was performed on patients whose uteri showed varying degrees of tetanization or even necrosis, the Reeb test being negative (lack of contractility of the uterus upon oxytocin stimulation). In cases where blood suffusions or areas of necrosis were observed and at the adnexal level (compromising the function of the organ), adnexectomy was also performed. This therapeutic attitude, although mutilating for young women, remains the only alternative in serious cases when the life of the mother takes precedence over the preservation of reproductive capacity [3,6,21].
Hematomas with a volume of less than 500 ml predominated 74%, which proves once again the efficiency of the medical teams that quickly diagnosed the condition and treated it adequately (Chart 3).
A clear preponderance of large retroplacental hematomas is observed in the group of patients who presented serious clinical forms requiring hysterectomy. Part of the specialized literature considers that the severity of the clinical form is not always closely related to the retroplacental hematoma volume but accepts that most cases with large retroplacental hematomas associate serious clinical forms [1,6,26]. The volume of the retroplacental hematoma cannot always be properly assessed, especially in cases where the hematoma detaches the membranes, and is partially externalized via the vaginal route [6,16,20,27].
The large number of emergency hysterectomies performed - 17 emergency hysterectomies as follows: 2 subtotal hysterectomies with adnexal preservation, 4 total hysterectomies with bilateral adnexectomy, 2 total hysterectomies with left adnexectomy and 9 total hysterectomies with adnexal preservation, proves that hysterectomy can be the only solution which saves the mother’s life (Chart 5). This traumatic operation for the woman, especially in cases of dead fetus, raises great psychological problems. If it also results in bilateral adnexectomy, when the process of necrosis seriously compromises the ovarian functionality, the woman is practically induced into surgical menopause, with all its consequences. The woman loses the fetus, uterus and reproductive capacity. In general, these cases are accompanied by severe depressive syndromes.
In the group of hysterectomized patients, most of the particularly serious cases were associated with large volumes of retroplacental hematomas, the fetal mortality being over 80%, in contrast to the total group of patients who presented placental abruption where the fetal mortality was 22.56%.
It is therefore observed that, in cases with large retroplacental hematomas, we encounter a high incidence of fetal suffering, increased rates of fetal mortality and numerous hemostasis hysterectomies. Practically, 84% of hysterectomies were performed on patients with retroplacental hematomas larger than 500 ml, and 16% of cases on patients in whom we have sufficient reason to believe that the volume of the retroplacental hematoma was not assessed correctly (patients complained of quite heavy bleeding abundant vaginally, which leads us to think of the possibility of the membranes detaching from the retroplacental hematoma with the externalization of an appreciable amount of blood on vaginal route).
Spinal anesthesia predominated, the breakdown by type of anesthesia being - 109 spinal anesthesia, 59 general anesthesia with I.O.T., 2 epidural anesthesia and one subarachnoid anesthesia) (Chart 4). Although the condition is one of the greatest obstetric emergencies and should have predominated general anesthesia with I.O.T. due to the fact that most cases were caught at an early stage. This is also proven by the large number of Phannensthiel type incisions, only 40% of the incisions were median pubosubumbilical type and the rest Phannenstiel type.
In the case of serious clinical forms, the types of median pubosubumbilical incision (88%) and general anesthesia with I.O.T. (60%) predominated, a fact that once again confirms the fact that the severity of the clinical form weighs a lot in the decision on the type of anesthesia and incision [28,29].
Fetal heart rates are closely related to the severity of the form of placental abruption [30]. Thus, in almost all severe cases of placental abruption we encountered fetal bradycardia (< 120 beats/minute). Fetal bradycardia was directly proportional to the size of retroplacental hematomas. Severe fetal bradycardia (< 70 beats/minute) was found in all patients with retroplacental hematomas of more than 500 ml.
5. Conclusions
Placental abruption remains one of the biggest obstetric emergencies, both by the large number of complications it associates and by the evolution that can often be unpredictable.
In severe cases of placental abruption, the only saving solution can be the necessary hysterectomy, sometimes with unilateral or bilateral adnexectomy.
The associated high fetal mortality raises, in addition to direct clinical problems, important social and psychological problems.
The predominance of the condition in male fetuses opens up new horizons for hormonal or genetic research.
Author Contributions
Conceptualization, L.Ș.; methodology, L.Ș., M.S. and P.I.; software, L.Ș. and S.M.; validation, L.Ș., S.M. and P.I., resources, L.Ș., S.M. and P.I.; data curation, L.Ș., S.M. and P.I.; writing—original draft preparation, L.Ș.; writing—review and editing, L.Ș., S.M. and P.I; visualization, L.Ș., S.M. and P.I; supervision, L.Ș. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by Ethical Committee of II Obstetrics-Gynecology Clinic of the “Sf Apostol Andrei” Constanta County Emergency Clinical Hospital (approval no.008/17.08.2024) and complied with the revised ethical guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. All patients admitted to our clinic give their consent for their clinical data to be included in the studies respecting their confidentiality.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author, Lucian Șerbănescu.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Oyelese, Y., & Ananth, C. V. (2006). Placental abruption. Obstetrics & Gynecology, 108(4), 1005–1016.
- Ananth, C. V., Smulian, J. C., Srinivas, N., Getahun, D., & Salihu, H. M. (2005). Risk of infant mortality among twins in relation to placental abruption: Contributions of preterm birth and restricted fetal growth. Twin Research and Human Genetics, 8(5), 524–531.
- Berceanu, S., & Georgescu Brăila, M. (1998). Obstetrica, Vol. II, Part II. Craiova: Editura Aius.
- Djakovic, A., Rieger, L., Wirbelauer, J., Kalla, J., & Dietl, J. (2007). Schwere intrauterine Wachstumsretardierung bei Uterus bicornis, Insertio velamentosa und vorzeitiger partieller Plazentalösung in der 26. Schwangerschaftswoche—eine Kasuistik. Z Geburtshilfe Neonatol, 211(4), 169–173.
- Ananth, C. V., Peltier, M. R., Kinzler, W. L., Smulian, J. C., & Vintzileos, A. M. (2007). Chronic hypertension and risk of placental abruption: Is the association modified by ischemic placental disease? American Journal of Obstetrics and Gynecology, 197(3), 273.e1-7.
- Cunningham, G. F., MacDonald, P. C., Gant, N. F., et al. (1993). Obstetrical hemorrhage. In Williams Obstetrics (19th ed., pp. 819–851). Norwalk, CT: Appleton and Lange.
- Medina, T. M., & Hill, D. A. (2006). Preterm premature rupture of membranes: Diagnosis and management. American Family Physician, 73(4), 659–664.
- Vârtej, P. (1997). Obstetrică fiziologică şi patologică. Bucureşti: Editura All.
- Könegärd, M., & Gennser, G. (1986). Incidence and recurrence rate of abruptio placentae in Sweden. Obstetrics & Gynecology, 67, 523.
- Hladky, K., Yankowitz, J., & Hansen, W. F. (2002). Placental abruption. Obstetrics & Gynecology Survey, 57(5), 299–305.
- Alghamdi, N. G., Khoj, Z. M., et al. (2018). Placental abruption. Indo American Journal of Pharmaceutical Sciences, 5(11), 11900–11904.
- Riihimäki, O., Metsäranta, M., Paavonen, J., Luukkaala, T., Gissler, M., Andersson, S., Nuutila, M., & Tikkanen, M. (2018). Placental abruption and child mortality. Pediatrics, 142(2), e20173915.
- Siddique, S., Afridi, H., Riaz, B., & Afridi, I. U. K. (2021). Fetomaternal outcome in placental abruption. Pakistan Journal of Medical & Health Sciences, 15(8), 1971–1974.
- Downes, K. L., Shenassa, E. D., & Grantz, K. L. (2017). Neonatal outcomes associated with placental abruption. American Journal of Epidemiology, 186(12), 1319–1328.
- Braila, A. D., Gluhovschi, A., Neacsu, A., Lungulescu, C. V., Braila, M., Vircan, E. L., Cotoi, B. V., & Goganau, A. M. (2018). Placental abruption: Etiopathogenic aspects, diagnostic and therapeutic implications. Romanian Journal of Morphology and Embryology, 59(1), 187–195.
- Dafallah, S. E., & Babikir, H. E. (2004). Risk factors predisposing to abruptio placentae. Maternal and fetal outcome. Saudi Medical Journal, 25(9), 1237–1240.
- Thieba, B., Lankoande, J., Akotionga, M., Kyelem, C., Ouedraogo, A., Ouedraogo, C. M., & Koné, B. (2003). Hématome rétroplacentaire: Aspects épidémiocliniques et pronostiques à propos d’une série de 177 cas. Gynecology Obstetrics Fertility, 31(5), 429–433.
- Nayama, M., Tamakloé-Azamesu, D., Garba, M., Idi, N., Djibril, B., Kamayé, M., Marafa, A., Touré, A., Diallo, F. Z., & Houfflin-Debarge, V. (2007). Hématome rétroplacentaire. Prise en charge dans une maternité de référence du Niger. Etude prospective à propos de 118 cas sur un an. Gynecology Obstetrics Fertility, 35(10), 975–981.
- Markhus, V. H., Rasmussen, S., Lie, S. A., & Irgens, L. M. (2011). Placental abruption and premature rupture of membranes. Acta Obstetricia et Gynecologica Scandinavica, 90, 1024–1029.
- Tica, V. I., Şerbănescu, L., & Tica, I. (2006). Etiologic, clinical and prognostic correlations in abruptio placentae. Revista Medico-Chirurgicală a Societății de Medicină și Natură Iași, 110(3), 633–638.
- Vârtej, P. (2000). Apoplexia uteroplacentară. In Munteanu Ioan (Ed.), Tratat de obstetrică (pp. 1234–1245). Bucureşti: Editura Academiei Române.
- Odibo, A. O., Cahill, A. G., Stamilio, D. M., Stevens, E. J., Peipert, J. F., & Macones, G. A. (2007). Predicting placental abruption and previa in women with a previous cesarean delivery. American Journal of Perinatology, 24(5), 299–305.
- Costea, D. O., Șerbănescu, L., Badiu, D., Ardeleanu, V., Branescu, C. M., Zgura, A., & Costea, A. C. (2022). Pain management in the right iliac fossa during the COVID-19 pandemic. Journal of Mind and Medical Sciences, 9(1), 162–167.
- Bordei, P., Surdu, L. S., Șerbănescu, L., & Tudorache, I. S. (2019). Morphometry of placental vessels. Revue de Chimie (Bucharest), 70(11), 4119–4122.
- Dommisse, J., & Tiltman, J. (1992). Placental bed biopsies in placental abruption. BJOG, 99(8), 651–654.
- Ananth, C. V., Berkowitz, T. S., Savitz, D. A., et al. (1999). Placental abruption and adverse perinatal outcomes. JAMA, 282, 1646–1651.
- Tikkanen, M., Nuutila, M., Hiilesmaa, V., Paavonen, J., & Ylikorkala, O. (2006). Clinical presentation and risk factors of placental abruption. Acta Obstetricia et Gynecologica Scandinavica, 85(6), 700–705.
- Tikkanen, M., Gissler, M., Metsäranta, M., Luukkaala, T., Hiilesmaa, V., Andersson, S., Ylikorkala, O., Paavonen, J., & Nuutila, M. (2009). Maternal deaths in Finland: Focus on placental abruption. Acta Obstetricia et Gynecologica Scandinavica, 88(10), 1124–1127.
- Saeed, M., & Rana, T. (2011). Fetomaternal outcome in pregnancies complicated with placental abruption. Pakistan Journal of Medical & Health Sciences, 5(1), 140–143.
- Usui, R., Matsubara, S., Ohkuchi, A., Kuwata, T., Watanabe, T., Izumi, A., & Suzuki, M. (2008). Fetal heart rate pattern reflecting the severity of placental abruption. Archives of Gynecology and Obstetrics, 277(3), 249–253.
- Pelinescu-Onciul, D., & Bari, M. (2005). Ecografia în obstetrică şi ginecologie: Semiologie ecografică normală. Bucureşti: Editura Didactică şi Pedagogică.
- Glantz, C., & Purnell, L. (2002). Clinical utility of sonography in the diagnosis and treatment of placental abruption. Journal of Ultrasound in Medicine, 21(8), 837–840.
- Sohn, C., Voigt, H. J., & Vetter, K. (2004). Vascular supply of the uteroplacental unit and techniques for examination of individual vessels. In Doppler Ultrasound in Gynecology and Obstetrics (pp. 123–145). Stuttgart: Thieme.
- Urban, G., Vergani, P., Ghidini, A., Tortoli, P., Ricci, S., Patrizio, P., & Paidas, M. J. (2007). State of the art: Non-invasive ultrasound assessment of the uteroplacental circulation. Seminars in Perinatology, 31(4), 232–239.
Chart 1.
Distribution by alive/dead fetuses.
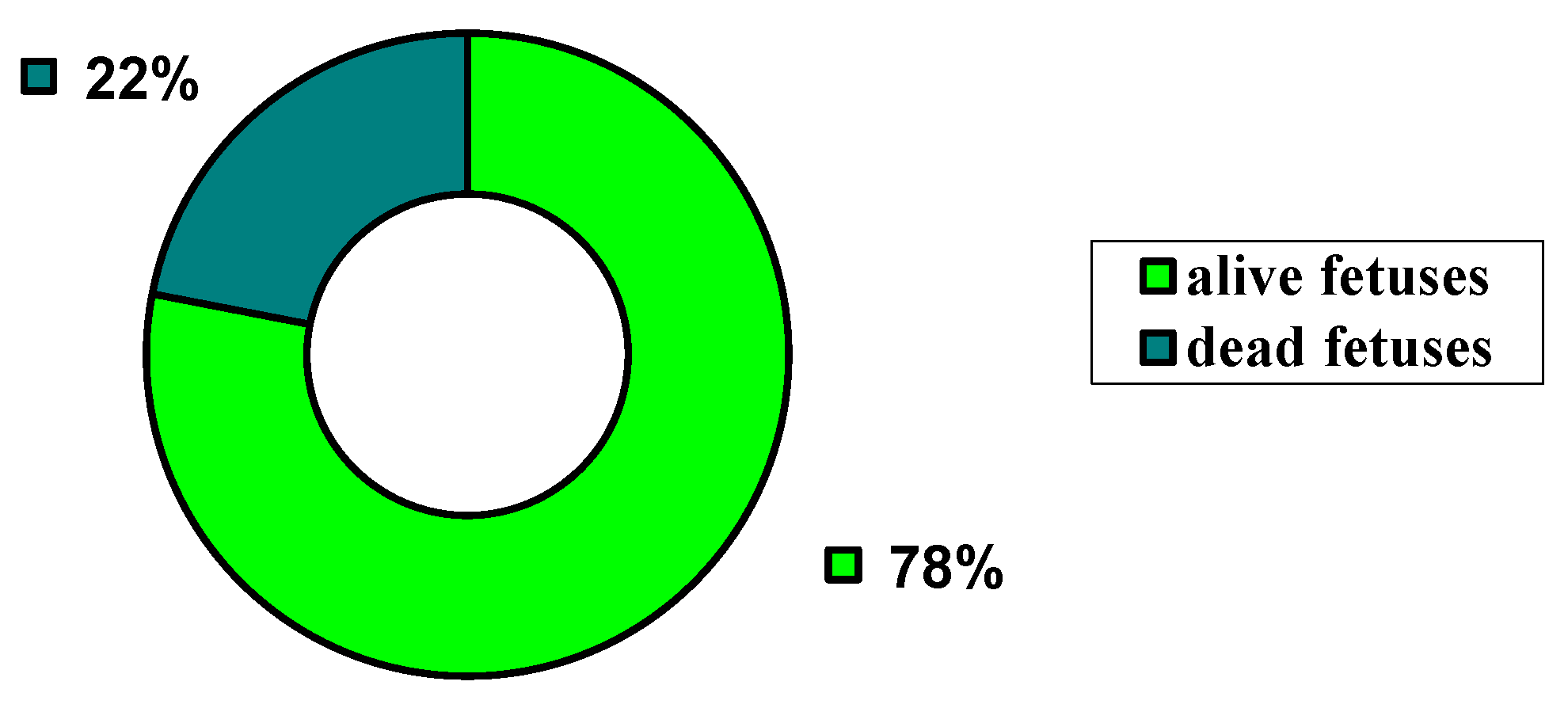
Chart 2.
The Apgar score distribution.
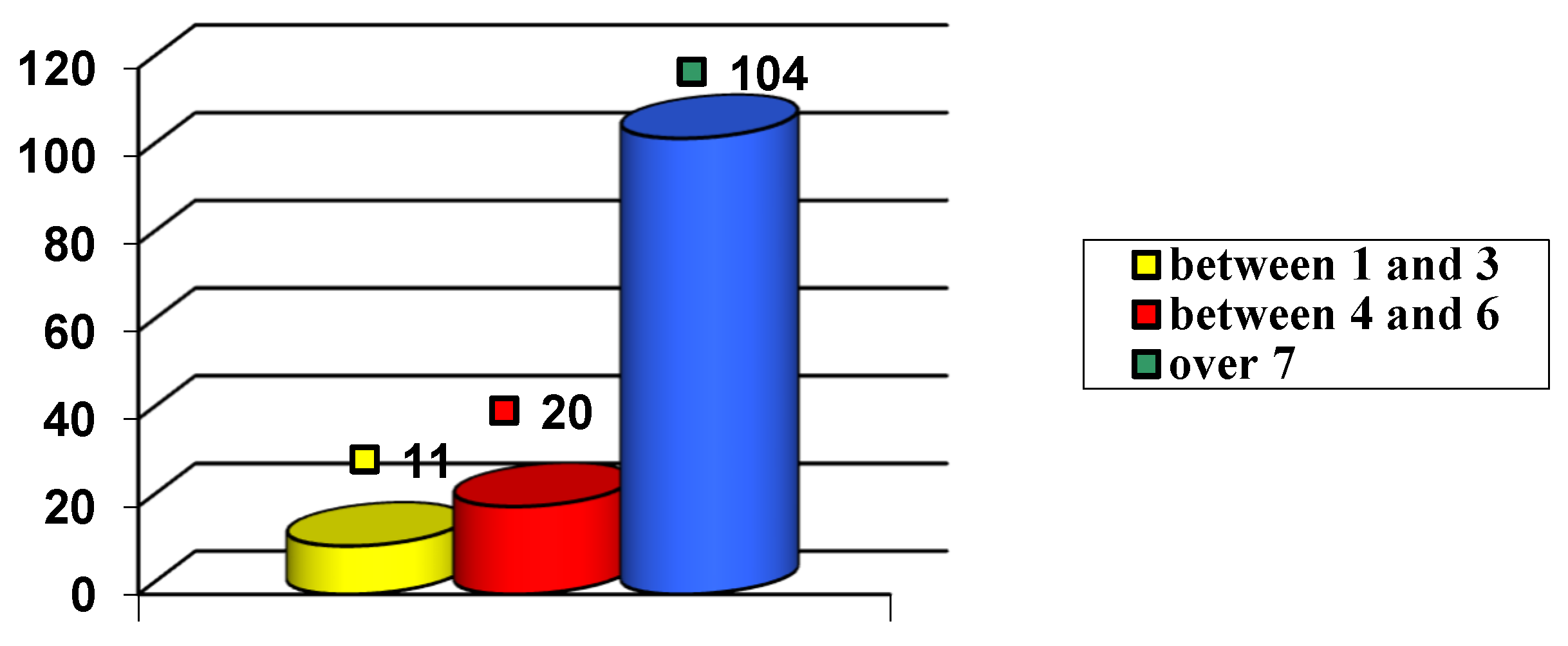
Chart 3.
Volume of retroplacental hematoma.
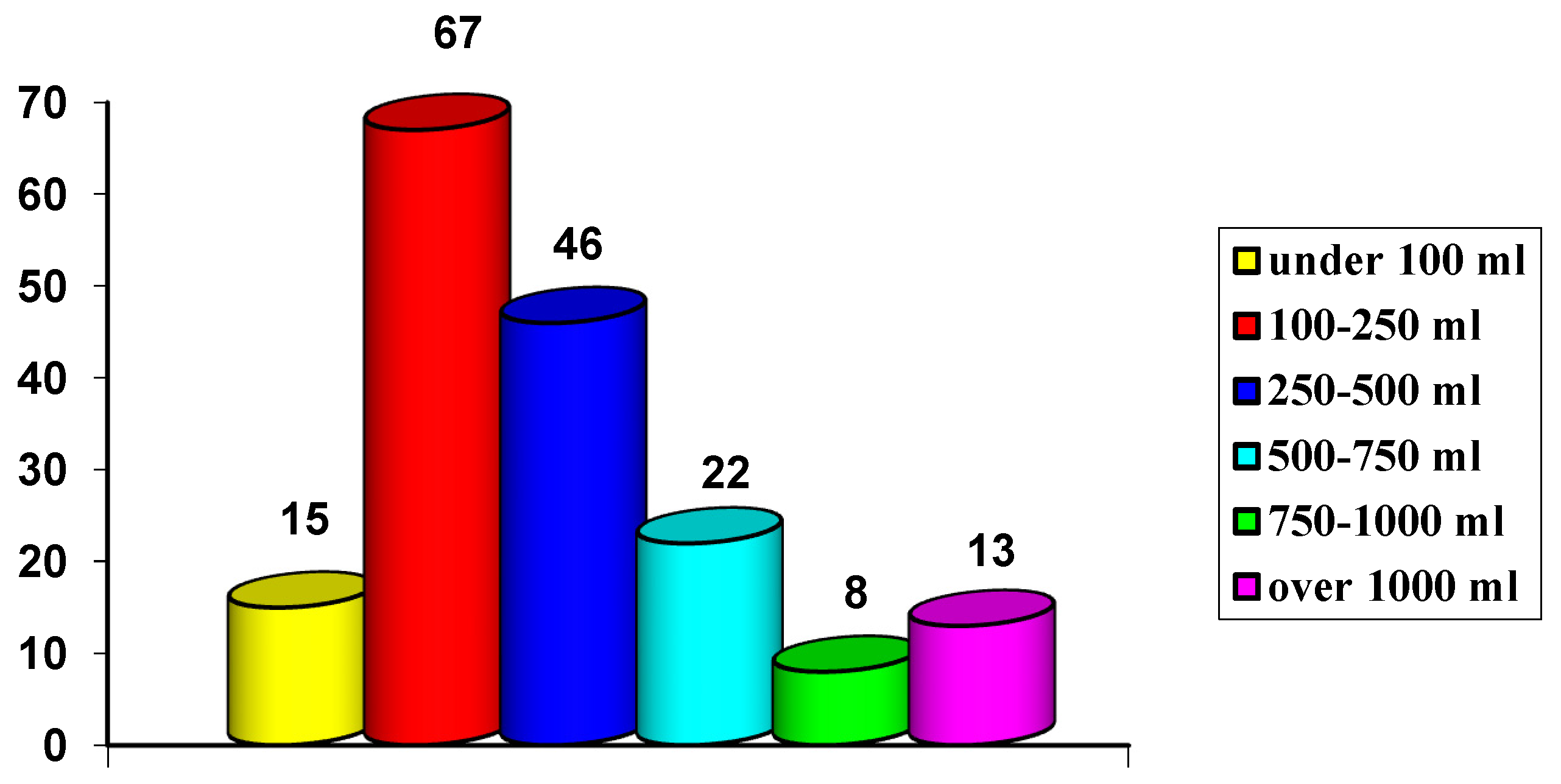
Chart 4.
Types of anesthesia.
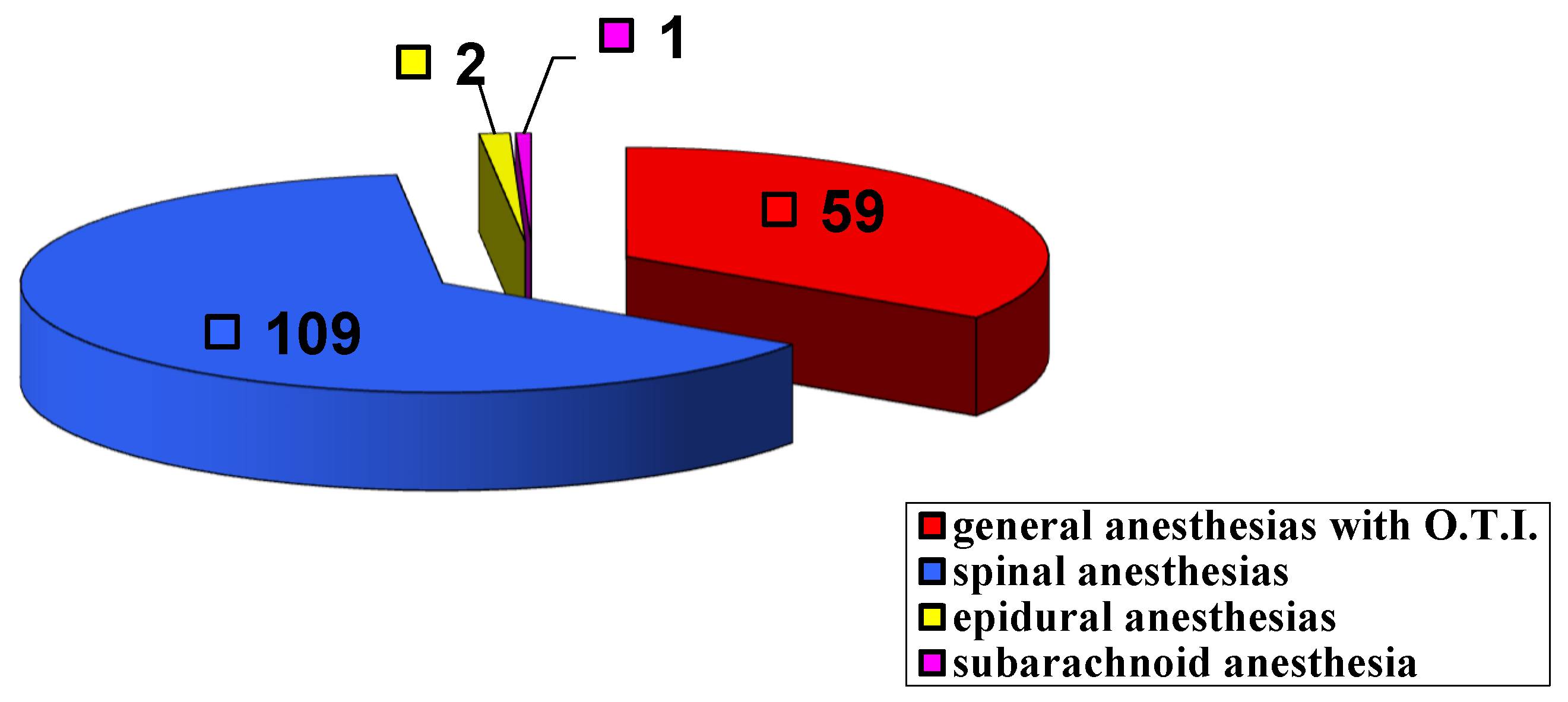
Chart 5.
Hysterectomies.
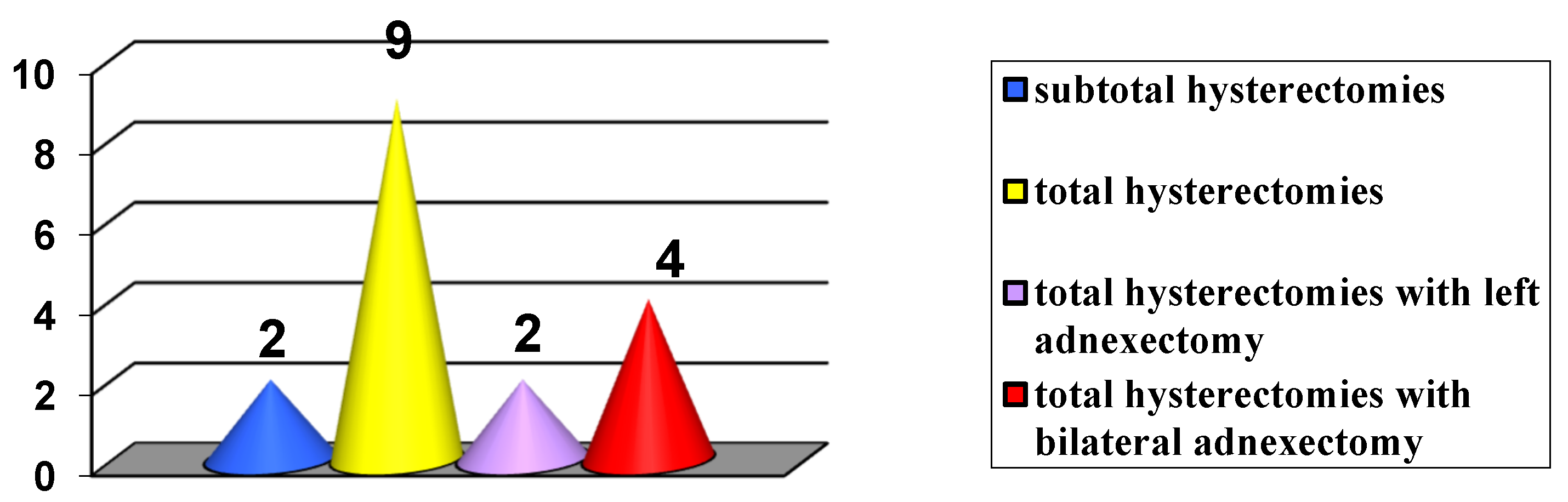

Table 1.
The distribution of patients by gestational stage.
| I G | II G | III G | IV G | V G | VI G | VII G | VIII G | IX G |
| 74 | 35 | 23 | 11 | 14 | 3 | 4 | 4 | 3 |
Table 2.
The distribution of patients by degree of parity.
| I P | II P | III P | IV P | V P | VI P | VII P | VIII P |
| 114 | 35 | 12 | 3 | 4 | 0 | 2 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



