Submitted:
22 December 2024
Posted:
23 December 2024
You are already at the latest version
Abstract
Background: Early diagnosis of cholangiocarcinoma (CCA) is still unreliable, resulting in poor patient outcomes. Volatile organic compounds (VOCs), emitted by the body, could help detect disease-related metabolic changes, aiding diagnosis. Objective: This study aims to assess if Gas chromatography ion mobility spectroscopy (GC-IMS) detection of serum VOCs can differentiate CCA from benign biliary diseases (BBD) and evaluate its diagnostic effectiveness. Method:Serum samples from 46 CCA and 46 BBD patients were collected. GC-IMS detected VOCs in the serum groups, and PCA was performed to analyze group differences. Utilize the Receiver Operating Characteristic (ROC) curve to assess the diagnostic efficacy of VOCs in CCA and analyze the correlation between VOCs and pathological characteristics. Resuit: Using GC-IMS, we detected 27 VOCs in two serum samples, including 23 known and 4 unknown. A PCA 3D scatter plot highlights distinct VOC patterns and clustering for CCA patients versus BBD. Statistical analysis reveals significant differences in 14 substances between the BBD and CCA groups, with 8 VOCs exhibiting upregulation and 6 demonstrating downregulation in the CCA group. ROC analysis reveals that (E) -2-nonenal exhibits the highest diagnostic efficiency for CCA, with an AUC value of 0.761 (95%CI: 0.662 - 0.860). Conclusion: Serum VOC analysis could aid the diagnosis and surveillance of CCA.
Keywords:
Cholangiocarcinoma
; GC-IMS
; Volatile organic compounds
; Identify
; Serum
Introduction
Cholangiocarcinoma (CCA) is a diverse malignant tumor originating from the biliary system, comprising approximately 15% of primary liver cancers and 3% of gastrointestinal cancers[1,2,3,4]. Early stage CCA has no specific symptoms. Common auxiliary exams in clinical practice, such as magnetic resonance cholangiopancreatography (MRCP), endoscopic retrograde cholangiopancreatography (ERCP), fluorescence in situ hybridization (FISH) analysis, and bile brush cytology, often have limitations, leading to false negatives and misdiagnoses[5,6,7].A gold standard for tumor diagnosis is pathological tissue biopsy, but it's highly invasive and unsuitable for early cancer screening[8,9]. Minimally invasive methods like tumor marker detection (e.g., CA19-9 and CEA) exist, but current markers lack the specificity and sensitivity needed for early CCA screening and diagnosis, in addition, there is no clear cause for the onset of CCA, leads to most patients being diagnosed late, missing the best treatment window[10,11]. Its aggressive nature and treatment difficulties lead to a high mortality rate, making up 2% of global cancer deaths[12]. The five-year survival rate is 7% to 20%, with a high rate of tumor recurrence after surgery[13]. Thus, creating reliable and effective screening and diagnostic tools is essential.
Volatile organic compounds (VOCs) are defined as organic substances that are present in the vapor phase at ambient room temperature. It not only contaminates the living environment but also poses a significant threat to human life and health. VOCs are categorized as endogenous or exogenous. Exogenous VOCs come from the environment and aren't metabolized by the body, while endogenous VOCs are produced by human cells during metabolism and oxidative stress, being released through tissues, fluids, or exhalation[14], these compounds indicate changes in metabolism and are linked to oxidative stress and inflammation, making them valuable biomarkers for assessing health status[15]. Currently, several studies indicate that VOCs possess distinct differential value in relation to multiple cancer types, including hepatocellular carcinoma[16]、lung cancer[17]、breast cancer[18]and colorectal cancer[19].These compounds can be identified in a range of biological matrices, including tissues, urine, blood. Studies have shown that the most common biomarkers for urinary VOCs are hexanal, dimethyl disulfide and phenol[20]. Suggesting that cancer cells release VOCs into bodily fluids. Subsequently, these compounds are excreted via the pulmonary system and can be detected in exhaled air[21]. Consequently, the investigation of cancer-specific VOCs in biological fluids represents a promising avenue of research that may facilitate the identification of metabolic alterations associated with tumors, thereby enhancing tumor diagnosis.
Gas chromatography ion mobility spectroscopy (GC-IMS) is an emerging desktop technology used for sensitive, rapid, and selective detection of volatile organic compounds [22]. Studies show that GC-IMS effectively analyzes metabolites in urine, breath, serum, plasma, bile, and feces, separating VOC molecules for qualitative and quantitative analysis [23]. The objective of this study is to assess the efficacy of GC-IMS in detecting serum VOCs for differentiating between CCA and benign biliary diseases (BBD).
2. Materials and Methods
2.1. Study Population
We used Power and Sample Size, an online software application, to evaluate the sample size of this study (http: //powerandsamplesize.com/calculators). Relevant parameters compare two means: two-sample, two-sided equality, power oftest, 1-β = 0.9 and type I error rate α = 0.05 were selected. At least 25 samples are required for each group of cancer patients and benign control patients. The study involved 92 eligible patients from the Third Affiliated Provincial Hospital of Shandong University between April 2023 and January 2024, comprising 46 CCA patients and 46 BBD patients. The inclusion criteria for the cancer group are as follows: 1) Participants must have a first-time diagnosis of cholangiocarcinoma; 2) Participants must have no prior history of other malignant tumors; 3) Participants must not have a history of receiving anti-cancer treatments, including radiotherapy and chemotherapy; 4) Participants must not be undergoing radical resection surgery. Patients were included in Group BBD if BBD was verified based on imaging or pathology and other diseases of the liver and digestive tract were excluded.
2.2. Sample Preparation
Blood samples were obtained from the Laboratory Department at the Third Affiliated Hospital of Shandong University, centrifuged at 3000 g for 10 min at 4℃ to extract serum, which was then aliquoted into 1.5 mL sterile tubes and stored at -80℃.
2.3. Analysis of Volatile Organic Compounds in Serum
To detect VOCs in serum with GC-IMS (GAS Dortmund, Germany), incubate 0.2 mL of serum at 37 ℃ for 10 min in a headspace vial, then extract 1 mL of gas. Use nitrogen as the carrier gas, beginning at 2 mL/min for 2 min and ramping up to 150 mL/min over 10 min. Maintain the IMS drift gas at 150 mL/min, with a drift tube temperature of 45 ℃ and a specific column temperature for gas chromatography.
2.4. Statistical Analysis
Analyze the data with IBM SPSS statistics 27.0.1 and Graphpad prism 10. For categorical data, the chi-square test is used and reported as frequency (percentage). For continuous data, the t-test or Mann-Whitney U test is applied, presented as mean ± standard deviation or median (interquartile range).
3. Resules
3.1. Clinical Characteristics of Patients
Ninety-two serum samples were collected from confirmed patients (46 with CCA and 46 with BBD). Statistical analysis revealed that there were no remarkable differences in gender, AFP, WBC, and ALT levels between the two groups. Nevertheless, disparities in age, CEA, CA19-9, ALP, GGT, and AST were detectable between CCA and BBD. More detailed clinical characteristics are listed in Table 1.
#Data represents mean ± standard deviation; *Data represents the median (interquartile range). Abbreviation: CCA, cholangiocarcinoma; BBD, benign biliary dis eases; AFP, Alpha-fetoprotein; CEA, carcinoembryonic antigen; CA19-9, carbohydrate antigen 19-9; WBC white blood cell; ALP alkaline phosphatase; GGT gamma-glutamyl transferase; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
3.2. VOC Profile Analysis in CCA and BBD Patients
Figure 1A shows that VOC signal peaks in serum samples are characterized by retention index, migration time, and peak intensity. Figure 1B and 1C illustrate the differences in peak intensity between CCA and BBD samples in both 3D and 2D spectra, respectively, as indicated by color intensity. From this analysis, a total of 51 volatile organic compound (VOC) signal peaks were identified from the serum samples (Figure 1D). Subsequently, 23 defined VOC substances along with 4 unidentified substances were analyzed using VOCal software (version 0.1.1) for further examination. A PCA 3D scatter plot reveals distinct clusters, indicating differing VOC profiles between CCA patients and those with BBD (Figure 1E).
3.5. Vocs biomarkers in serum and pathological parameters
We investigated the association between serum VOC alterations and CCA progression by analyzing ten crucial VOCs against diverse pathological parameters. Table 4 illustrates the p-values for each VOC and distinct pathological factors. After conducting the Mann-Whitney U test, it was revealed that 1-pentanal and Unk4 had statistical disparities in relation to jaundice, where the median of the non-jaundice group was greater than that of the jaundice group. 3-methylbutyl propanoate-M, 3-methylbutyl propanoate-D, and ethyl acrylate manifested significant differences among the pathological types of cancer, accompanied by a decreasing trend in adenocarcinoma. Detailed data is in Supplementary Table S1.
3.3. Quantitative Analysis of VOCs in serum sample
Quantification used the internal standard method based on VOC peak volume. Specifically, 10 mL of 4-methyl-2-pentanol at 15 mL/L was added to each sample. Figure 2 shows 14 VOC expression differences between CCA and BBD patients., including 8 that are upregulated in CCA patients(3-methylbutyl propanoate-M、3-methylbutyl propanoate-D、1-pentanal、2-butenal, 2-methyl、ethyl acrylate and three unidentified gases Unk2、Unk3 and Unk12)and 6 VOCs downregulated in CCA (1-nonanal-D、1-nonanal-M、E)-2-nonenal、1-octanal、diallyl disulfide and Unk4). No significant differences were found in the other 13 VOCs between CCA and BBD, as shown in Supplementary Figure S1. Detailed data is in Table 2.
3.4. Diagnostic Performance of ROC Analysis for Vocs
ROC analysis showed that VOCs have high specificity (80.4%~100%) for diagnosing CCA, but their sensitivity is low (0%~60.9%). The compounds with AUC values exceeding 0.75 are 1-nonanal-D, (E)-2-nonanal, and Unk4, with (E)-2-nonanal having the highest AUC of 0.761 (95% CI: 0.662-0.860), 56.5% sensitivity, and 80.4% specificity (Table 3).
4. Discussion
Cholangiocarcinoma has a high degree of malignancy and a low survival rate for patients, but its occurrence has no significant signs. The difficulty of early diagnosis is also well known. If early and accurate diagnosis can be made, early intervention measures can be taken to improve survival rates. Recently, the use of VOCs for diagnosing different cancers has attracted increased academic attention. Gui et al[24] used GC-IMS to successfully distinguish VOCs in bile between perihilar cholangiocarcinoma (PHCCA) and BBD. Similarly, Navaneetan U's research showed that bile VOCs could differentiate between CCA and primary sclerosing cholangitis (PSC) stenosis[25]. However, the difficult and distressing process of obtaining bile makes it unsuitable for early screening and diagnosis in routine physical exams.
In metabolomics research, serum is the second most used sample after urine due to its easy collection and low trauma. VOCs in serum, transported via the bloodstream and exhaled, may indicate early metabolic changes in tumor cells[26]. Thus, analyzing serum metabolites as biomarkers for cholangiocarcinoma is a sensible strategy. Sana et al [27] used solid-phase microextraction and gas chromatography/mass spectrometry to study VOCs in the serum of pregnant women with gestational diabetes. They identified 2-propanol as a possible biomarker for cognitive impairment in these women. Liu et al[28] showed that serum VOCs can effectively distinguish esophageal cancer patients from healthy individuals. Wu et al[29] found that HDL in serum mediated the relationship between co-exposure to VOCs and kidney stone formation. Therefore, in this study, we investigated the efficacy of VOCs in serum for diagnosing CCA. Our study is the first to identify significant changes in serum headspace VOCs in CCA and BBD patients. PCA scatter plots show a clear distinction between the two, indicating that CCA patients typically have distinct VOC profiles compared to BBD patients.
Using GC-IMS, we identified 27 substances in two serum sets, comprising 10 aldehydes, 3 esters, 3 alcohols, 2 acids, 2 heterocycles, 1 sulfur compound, 1 ketone, 1 hydrocarbon, and 4 unknowns. Notably, 14 VOCs differed significantly, with 8 being upregulated in CCA(3-methylbutyl propanoate-M、3-methylbutyl propanoate-D、1-pentanal、2-butenal, 2-methyl、ethyl acrylate、Unk2、Unk3 and Unk12)and six substances in CCA exhibit significant downregulation.(1-nonanal-D、1-nonanal-M、E)-2-nonenal、1-octanal、diallyl disulfide and Unk4). Aldehydes are the main type of these substances. E)-2-nonenal, an unsaturated aldehyde from lipid peroxidation, can signal proteins via ROS and is linked to oxidative processes. The exact method is not yet fully understood, but its presence might indicate abnormal oxidative metabolism in cells, possibly related to a cancer-promoting environment[30]. Aldehyde dehydrogenase serves as a crucial catalyst within the human body, facilitating the oxidation of aldehydes to carboxylic acids[31], a carboxylic acid participates in the synthesis of intracellular lipids and provides materials for the cell membrane[32]. Due to the heightened metabolic activity of tumor cells, there is an upregulation in the activity of aldehyde dehydrogenase, which catalyzes the oxidation of a majority of aldehyde compounds into carboxylic acids, thereby facilitating tumor cell proliferation. This biochemical process might explain the notable drop in aldehyde levels in the CCA group versus the benign control group. Monedeiro et al.'s study indicates that (E)-2-nonenal could differentiate oral cancer from oral inflammatory diseases[33]. Our research indicates it can differentiate between cancer and benign disease groups.
Ethanol acrylate is an acrylic monomer utilized in the synthesis of various polymers and copolymers. The International Agency for Research on Cancer (IARC) categorizes it as a Group 2B carcinogen, indicating it is possibly carcinogenic to human[34]. Walker AM et al[35] conducted a retrospective study that revealed a significantly elevated risk of colon cancer mortality among workers exposed to ethyl acrylate. Likewise, our study found a notable rise in its levels among cholangiocarcinoma patients.
Furthermore, within the CCA cohort, a notable reduction was observed in compounds such as diallyl disulfide, a primary organic sulfur constituent found in garlic[36]. Recent research has provided substantial evidence indicating that it demonstrates anti-tumor activity against a variety of tumor cell types, including breast cancer [37]、prostate cancer [38]、lung cancer [39]、gastric cancer [40]、colorectal cancer [41]、hepatocellular carcinoma cell lines[42]. Xia L et al[43] demonstrated that diallyl disulfide can inhibit the expression and activity of Rac1 by suppressing the PI3K/Akt signaling pathway, thereby reducing the invasion and migration capabilities of epithelial-mesenchymal transition (EMT) and colon cancer cells, ultimately exhibiting anti-colon cancer effects. Kim H et al[41] demonstrated that diallyl disulfide can inhibit the progression of colon cancer by downregulating the anti-apoptotic protein Bcl-2, in association with tumor necrosis factor-related apoptosis-inducing ligand (TRAIL). Xiong T et al[44] demonstrated through both in vivo and in vitro experiments that diallyl disulfide significantly inhibits the proliferation, invasion, and migration of breast cancer cells. In our study, we found that the concentration of diallyl disulfide in the cholangiocarcinoma group was significantly lower than that in the control group, corroborating findings from prior research. While the resistance of diallyl disulfide to cholangiocarcinoma has not been previously documented, the differential expression of this compound holds substantial implications for differentiating cholangiocarcinoma from benign biliary diseases.
To assess the diagnostic efficacy of VOCs for CCA, we performed a ROC analysis on 14 key VOCs. The analysis revealed that these VOCs exhibited high specificity, ranging from 80% to 100%, while their sensitivity was relatively low, ranging from 0% to 60%. Among them, (E) -2-nominal has the best AUC value with 56.5% sensitivity and 80.4% specificity at 0.761, respectively. This observation contrasts with the high sensitivity yet low specificity associated with CA19-9. To enhance diagnostic efficiency, it may be beneficial to integrate the detection methods of VOCs with CA19-9. However, the efficacy of such a combined diagnostic approach requires further investigation and exploration.
Although VOCs generally exhibit good performance in differentiating CCA from BBD, not all individual VOCs are correlated with pathological features. In the present study, through the application of the Mann Whitney U test, significant associations were identified between specific VOCs and pathological parameters. We observed that 1-pentanal and Unk4 presented statistically significant differences in terms of jaundice, with the median of the non-jaundice group exceeding that of the jaundice group. The concentrations of 3-methylbutyl propanoate-M, 3-methylbutyl propanoate-D, and ethyl acrylate exhibited remarkable differences among diverse cancer pathological types, and a notably downward regulation was especially detectable in adenocarcinoma patients. These substances demonstrate a remarkable capacity to differentiate between patients with CCA and those with BBD.
However, this observation is based on a limited patient cohort and necessitates validation with larger, independent datasets for external confirmation.
5. Conclusion
In this study, using GC-IMS, we identified 14 VOCs associated with cholangiocarcinoma, which have advantages in distinguishing cholangiocarcinoma patients from benign biliary disease patients. thereby offering a viable approach for CCA detection. The volatile organic compounds in serum are mainly aldehydes, which are of great significance for the differential diagnosis of biliary malignancies. In addition, this study first discovered a correlation between serum volatile organic compounds and pathological parameters in CCA, and analyzed its diagnostic efficiency using ROC. The findings present empirical evidence supporting the application of VOC analysis in CCA, which is anticipated to significantly influence future clinical diagnosis and monitoring of CCA, and has extremely broad clinical application prospects. However, more scientific research is needed to explore the mechanisms of VOCs production and metabolism.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: 13 VOCs with no significant difference between CCA and BBD. Table S1: VOCs and different pathological factors.
Author contributions: Conceptualization: Xuewei Zhuang; Data curation:Jing He; Formal analysis: Jing He, Qi Liu; Investigation: Jing He, Xiaoyue Zhao; Methodology: Jing He; Resources: Jing He, Xuewei Zhuan; Software: Jing He; Supervision: Jing He, Xin Li; Validation: Jing He, Xiaoyue Zhao; Visualization: Jing He, Xin Li; Writing – original draft: Jing He; Writing – review & editing: Jing He, Xuewei Zhuang.
Funding
This work was supported by grants from Shandong Provincial Nature Foundation (Grant No. ZR2020MH321); Shandong Provincial Key Research and Development Program (Grant No.2016GSF201169) and Research on Key Technologies of Molecular POCT Systems in the Field of Infectious Diseases (SLSYKYB2022010).
Institutional Review Board Statement
This study was conducted in accordance with the Helsinki Declaration and has been approved by the Ethics Committee of the Third Hospital of Shandong University (Ethics Review Number: KYLL-2023084).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
Gratitude is extended to Professor Liu Yili from Shandong University for his invaluable assistance in statistical analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- DeOliveira, M. L.; Cunningham, S. C.; Cameron, J. L.; Kamangar, F.; Winter, J. M.; Lillemoe, K. D.; Choti, M. A.; Yeo, C. J.; Schulick, R. D. Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 2007, 245 (5), 755-762. [CrossRef]
- Nakeeb, A.; Pitt, H. A.; Sohn, T. A.; Coleman, J.; Abrams, R. A.; Piantadosi, S.; Hruban, R. H.; Lillemoe, K. D.; Yeo, C. J.; Cameron, J. L. Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg 1996, 224 (4), 463-473; discussion 473-465. [CrossRef]
- Moris, D.; Palta, M.; Kim, C.; Allen, P. J.; Morse, M. A.; Lidsky, M. E. Advances in the treatment of intrahepatic cholangiocarcinoma: An overview of the current and future therapeutic landscape for clinicians. CA Cancer J Clin 2023, 73 (2), 198-222. [CrossRef]
- Vithayathil, M.; Khan, S. A. Current epidemiology of cholangiocarcinoma in Western countries. J Hepatol 2022, 77 (6), 1690-1698. [CrossRef]
- Saluja, S. S.; Sharma, R.; Pal, S.; Sahni, P.; Chattopadhyay, T. K. Differentiation between benign and malignant hilar obstructions using laboratory and radiological investigations: a prospective study. HPB (Oxford) 2007, 9 (5), 373-382. [CrossRef]
- Brindley, P. J.; Bachini, M.; Ilyas, S. I.; Khan, S. A.; Loukas, A.; Sirica, A. E.; Teh, B. T.; Wongkham, S.; Gores, G. J. Cholangiocarcinoma. Nat Rev Dis Primers 2021, 7 (1), 65. [CrossRef]
- Cerrito, L.; Ainora, M. E.; Borriello, R.; Piccirilli, G.; Garcovich, M.; Riccardi, L.; Pompili, M.; Gasbarrini, A.; Zocco, M. A. Contrast-Enhanced Imaging in the Management of Intrahepatic Cholangiocarcinoma: State of Art and Future Perspectives. Cancers (Basel) 2023, 15 (13). [CrossRef]
- Guedj, N. Pathology of Cholangiocarcinomas. Curr Oncol 2022, 30 (1), 370-380. [CrossRef]
- Takahashi, Y.; Dungubat, E.; Kusano, H.; Ganbat, D.; Tomita, Y.; Odgerel, S.; Fukusato, T. Application of Immunohistochemistry in the Pathological Diagnosis of Liver Tumors. Int J Mol Sci 2021, 22 (11). [CrossRef]
- Kosugi, S.; Nishimaki, T.; Kanda, T.; Nakagawa, S.; Ohashi, M.; Hatakeyama, K. Clinical significance of serum carcinoembryonic antigen, carbohydrate antigen 19-9, and squamous cell carcinoma antigen levels in esophageal cancer patients. World J Surg 2004, 28 (7), 680-685. [CrossRef]
- Acharya, A.; Markar, S. R.; Matar, M.; Ni, M.; Hanna, G. B. Use of Tumor Markers in Gastrointestinal Cancers: Surgeon Perceptions and Cost-Benefit Trade-Off Analysis. Ann Surg Oncol 2017, 24 (5), 1165-1173. [CrossRef]
- Banales, J. M.; Marin, J. J. G.; Lamarca, A.; Rodrigues, P. M.; Khan, S. A.; Roberts, L. R.; Cardinale, V.; Carpino, G.; Andersen, J. B.; Braconi, C.; et al. Cholangiocarcinoma 2020: the next horizon in mechanisms and management. Nat Rev Gastroenterol Hepatol 2020, 17 (9), 557-588. [CrossRef]
- Lindnér, P.; Rizell, M.; Hafström, L. The impact of changed strategies for patients with cholangiocarcinoma in this millenium. HPB Surg 2015, 2015, 736049. [CrossRef]
- Phillips, M.; Cataneo, R. N.; Greenberg, J.; Grodman, R.; Gunawardena, R.; Naidu, A. Effect of oxygen on breath markers of oxidative stress. Eur Respir J 2003, 21 (1), 48-51. [CrossRef]
- Kwon, J. W.; Park, H. W.; Kim, W. J.; Kim, M. G.; Lee, S. J. Exposure to volatile organic compounds and airway inflammation. Environ Health 2018, 17 (1), 65. [CrossRef]
- Sukaram, T.; Apiparakoon, T.; Tiyarattanachai, T.; Ariyaskul, D.; Kulkraisri, K.; Marukatat, S.; Rerknimitr, R.; Chaiteerakij, R. VOCs from Exhaled Breath for the Diagnosis of Hepatocellular Carcinoma. Diagnostics (Basel) 2023, 13 (2). [CrossRef]
- Chen, X.; Muhammad, K. G.; Madeeha, C.; Fu, W.; Xu, L.; Hu, Y.; Liu, J.; Ying, K.; Chen, L.; Yurievna, G. O. Calculated indices of volatile organic compounds (VOCs) in exhalation for lung cancer screening and early detection. Lung Cancer 2021, 154, 197-205. [CrossRef]
- Hadi, N. I.; Jamal, Q.; Iqbal, A.; Shaikh, F.; Somroo, S.; Musharraf, S. G. Serum Metabolomic Profiles for Breast Cancer Diagnosis, Grading and Staging by Gas Chromatography-Mass Spectrometry. Sci Rep 2017, 7 (1), 1715. [CrossRef]
- Kononova, E.; Mežmale, L.; Poļaka, I.; Veliks, V.; Anarkulova, L.; Vilkoite, I.; Tolmanis, I.; Ļeščinska, A. M.; Stonāns, I.; Pčolkins, A.; et al. Breath Fingerprint of Colorectal Cancer Patients Based on the Gas Chromatography-Mass Spectrometry Analysis. Int J Mol Sci 2024, 25 (3). [CrossRef]
- (20) da Costa, B. R. B.; De Martinis, B. S. Analysis of urinary VOCs using mass spectrometric methods to diagnose cancer: A review. Clin Mass Spectrom 2020, 18, 27-37. [CrossRef]
- Wen, Q.; Boshier, P.; Myridakis, A.; Belluomo, I.; Hanna, G. B. Urinary Volatile Organic Compound Analysis for the Diagnosis of Cancer: A Systematic Literature Review and Quality Assessment. Metabolites 2020, 11 (1). [CrossRef]
- Capitain, C.; Weller, P. Non-Targeted Screening Approaches for Profiling of Volatile Organic Compounds Based on Gas Chromatography-Ion Mobility Spectroscopy (GC-IMS) and Machine Learning. Molecules 2021, 26 (18). [CrossRef]
- Christmann, J.; Rohn, S.; Weller, P. gc-ims-tools - A new Python package for chemometric analysis of GC-IMS data. Food Chem 2022, 394, 133476. [CrossRef]
- Gui, X.; Zhang, X.; Xin, Y.; Liu, Q.; Wang, Y.; Zhang, Y.; Xu, Y.; Liu, Z.; Liu, W.; Schiöth, H. B.; et al. Identification and validation of volatile organic compounds in bile for differential diagnosis of perihilar cholangiocarcinoma. Clin Chim Acta 2023, 541, 117235. [CrossRef]
- Navaneethan, U.; Parsi, M. A.; Lourdusamy, V.; Bhatt, A.; Gutierrez, N. G.; Grove, D.; Sanaka, M. R.; Hammel, J. P.; Stevens, T.; Vargo, J. J.; et al. Volatile organic compounds in bile for early diagnosis of cholangiocarcinoma in patients with primary sclerosing cholangitis: a pilot study. Gastrointest Endosc 2015, 81 (4), 943-949.e941. [CrossRef]
- Moura, P. C.; Raposo, M.; Vassilenko, V. Breath volatile organic compounds (VOCs) as biomarkers for the diagnosis of pathological conditions: A review. Biomed J 2023, 46 (4), 100623. [CrossRef]
- Sana, S. R.; Chen, G. M.; Lv, Y.; Guo, L.; Li, E. Y. Metabonomics fingerprint of volatile organic compounds in serum and urine of pregnant women with gestational diabetes mellitus. World J Diabetes 2022, 13 (10), 888-899. [CrossRef]
- Liu, Q.; Li, S.; Mao, M.; Gui, X.; Zhang, Y.; Zhao, Y.; Yu, L.; Zhang, X.; Zhang, Y. Serum-volatile organic compounds in the diagnostics of esophageal cancer. Sci Rep 2024, 14 (1), 17722. [CrossRef]
- Wu, M.; Liu, M.; Zhang, Y.; Wu, J.; Gao, M.; Huang, F.; Chen, H.; Zhu, Z. Serum HDL partially mediates the association between exposure to volatile organic compounds and kidney stones: A nationally representative cross-sectional study from NHANES. Sci Total Environ 2024, 907, 167915. [CrossRef]
- Glaab, V.; Collins, A. R.; Eisenbrand, G.; Janzowski, C. DNA-damaging potential and glutathione depletion of 2-cyclohexene-1-one in mammalian cells, compared to food relevant 2-alkenals. Mutat Res 2001, 497 (1-2), 185-197. [CrossRef]
- Shortall, K.; Djeghader, A.; Magner, E.; Soulimane, T. Insights into Aldehyde Dehydrogenase Enzymes: A Structural Perspective. Front Mol Biosci 2021, 8, 659550. [CrossRef]
- Perchuk, I.; Shelenga, T.; Gurkina, M.; Miroshnichenko, E.; Burlyaeva, M. Composition of Primary and Secondary Metabolite Compounds in Seeds and Pods of Asparagus Bean (Vigna unguiculata (L.) Walp.) from China. Molecules 2020, 25 (17). [CrossRef]
- Monedeiro, F.; Monedeiro-Milanowski, M.; Zmysłowski, H.; De Martinis, B. S.; Buszewski, B. Evaluation of salivary VOC profile composition directed towards oral cancer and oral lesion assessment. Clin Oral Investig 2021, 25 (7), 4415-4430. [CrossRef]
- Vainio, H.; Heseltine, E.; Wilbourn, J. Priorities for Future IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Environ Health Perspect 1994, 102 (6-7), 590-591. [CrossRef]
- Walker, A. M.; Cohen, A. J.; Loughlin, J. E.; Rothman, K. J.; DeFonso, L. R. Mortality from cancer of the colon or rectum among workers exposed to ethyl acrylate and methyl methacrylate. Scand J Work Environ Health 1991, 17 (1), 7-19. [CrossRef]
- Bastaki, S. M. A.; Ojha, S.; Kalasz, H.; Adeghate, E. Chemical constituents and medicinal properties of Allium species. Mol Cell Biochem 2021, 476 (12), 4301-4321. [CrossRef]
- Xie, X.; Huang, X.; Tang, H.; Ye, F.; Yang, L.; Guo, X.; Tian, Z.; Xie, X.; Peng, C.; Xie, X. Diallyl Disulfide Inhibits Breast Cancer Stem Cell Progression and Glucose Metabolism by Targeting CD44/PKM2/AMPK Signaling. Curr Cancer Drug Targets 2018, 18 (6), 592-599. [CrossRef]
- Liu, M.; Wu, L.; Montaut, S.; Yang, G. Hydrogen Sulfide Signaling Axis as a Target for Prostate Cancer Therapeutics. Prostate Cancer 2016, 2016, 8108549. [CrossRef]
- Tian, J.; Zhao, W.; Wu, Y.; Shi, Y.; Yu, J.; Zhang, W.; Xing, C.; Zhuang, C.; Qu, Z. Diallyl Disulfide Blocks Cigarette Carcinogen 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanone-Induced Lung Tumorigenesis via Activation of the Nrf2 Antioxidant System and Suppression of NF-κB Inflammatory Response. J Agric Food Chem 2023, 71 (46), 17763-17774. [CrossRef]
- Tang, H.; Kong, Y.; Guo, J.; Tang, Y.; Xie, X.; Yang, L.; Su, Q.; Xie, X. Diallyl disulfide suppresses proliferation and induces apoptosis in human gastric cancer through Wnt-1 signaling pathway by up-regulation of miR-200b and miR-22. Cancer Lett 2013, 340 (1), 72-81. [CrossRef]
- Kim, H. J.; Kang, S.; Kim, D. Y.; You, S.; Park, D.; Oh, S. C.; Lee, D. H. Diallyl disulfide (DADS) boosts TRAIL-Mediated apoptosis in colorectal cancer cells by inhibiting Bcl-2. Food Chem Toxicol 2019, 125, 354-360. [CrossRef]
- Mitra, S.; Das, R.; Emran, T. B.; Labib, R. K.; Noor, E. T.; Islam, F.; Sharma, R.; Ahmad, I.; Nainu, F.; Chidambaram, K.; et al. Diallyl Disulfide: A Bioactive Garlic Compound with Anticancer Potential. Front Pharmacol 2022, 13, 943967. [CrossRef]
- Xia, L.; Lin, J.; Su, J.; Oyang, L.; Wang, H.; Tan, S.; Tang, Y.; Chen, X.; Liu, W.; Luo, X.; et al. Diallyl disulfide inhibits colon cancer metastasis by suppressing Rac1-mediated epithelial-mesenchymal transition. Onco Targets Ther 2019, 12, 5713-5728. [CrossRef]
- Xiong, T.; Liu, X. W.; Huang, X. L.; Xu, X. F.; Xie, W. Q.; Zhang, S. J.; Tu, J. Tristetraprolin: A novel target of diallyl disulfide that inhibits the progression of breast cancer. Oncol Lett 2018, 15 (5), 7817-7827. [CrossRef]
Figure 1.
VOCs profile detected in CCA and BBD. (A) A 3D signal model is actually generated with three dimensions represent peak strength, retention index and migration time respectively. (B) 3D and (C) 2D map shows the difference in the VOCs between a CCA sample and a BBD sample, can intuitively observe the migration time and retention index of different VOCs. (D) The VOCs signal peaks detected in all serum samples with red representing a higher concentration of the substance and blue representing a lower concentration. (E) Principal component analysis (PCA) shows an obvious difference between CCA and BBD.
Figure 1.
VOCs profile detected in CCA and BBD. (A) A 3D signal model is actually generated with three dimensions represent peak strength, retention index and migration time respectively. (B) 3D and (C) 2D map shows the difference in the VOCs between a CCA sample and a BBD sample, can intuitively observe the migration time and retention index of different VOCs. (D) The VOCs signal peaks detected in all serum samples with red representing a higher concentration of the substance and blue representing a lower concentration. (E) Principal component analysis (PCA) shows an obvious difference between CCA and BBD.

Figure 2.
Quantitative analysis of VOCs. The levels of 1-nonanal-M (A),1-nonanal-D (B),1-pentanal (C),1-octanal (D),2-butenal 2-methyl (E),3-methylbutyl propanoate-M (F),3-methylbutyl propanoate-D (G), (E) -2-nonenal (H), allyl disulfide (I), ethyl acrylate (J),Unk2 (K), Unk3 (L), Unk4 (M), Unk12 (N)。* p < 0.05, ** p < 0.01, *** p < 0.001 ,**** p < 0.0001 (Mann–Whitney U test). Data represents the median (interquartile range).Table 2. Quantitative analysis of VOCs.
Figure 2.
Quantitative analysis of VOCs. The levels of 1-nonanal-M (A),1-nonanal-D (B),1-pentanal (C),1-octanal (D),2-butenal 2-methyl (E),3-methylbutyl propanoate-M (F),3-methylbutyl propanoate-D (G), (E) -2-nonenal (H), allyl disulfide (I), ethyl acrylate (J),Unk2 (K), Unk3 (L), Unk4 (M), Unk12 (N)。* p < 0.05, ** p < 0.01, *** p < 0.001 ,**** p < 0.0001 (Mann–Whitney U test). Data represents the median (interquartile range).Table 2. Quantitative analysis of VOCs.
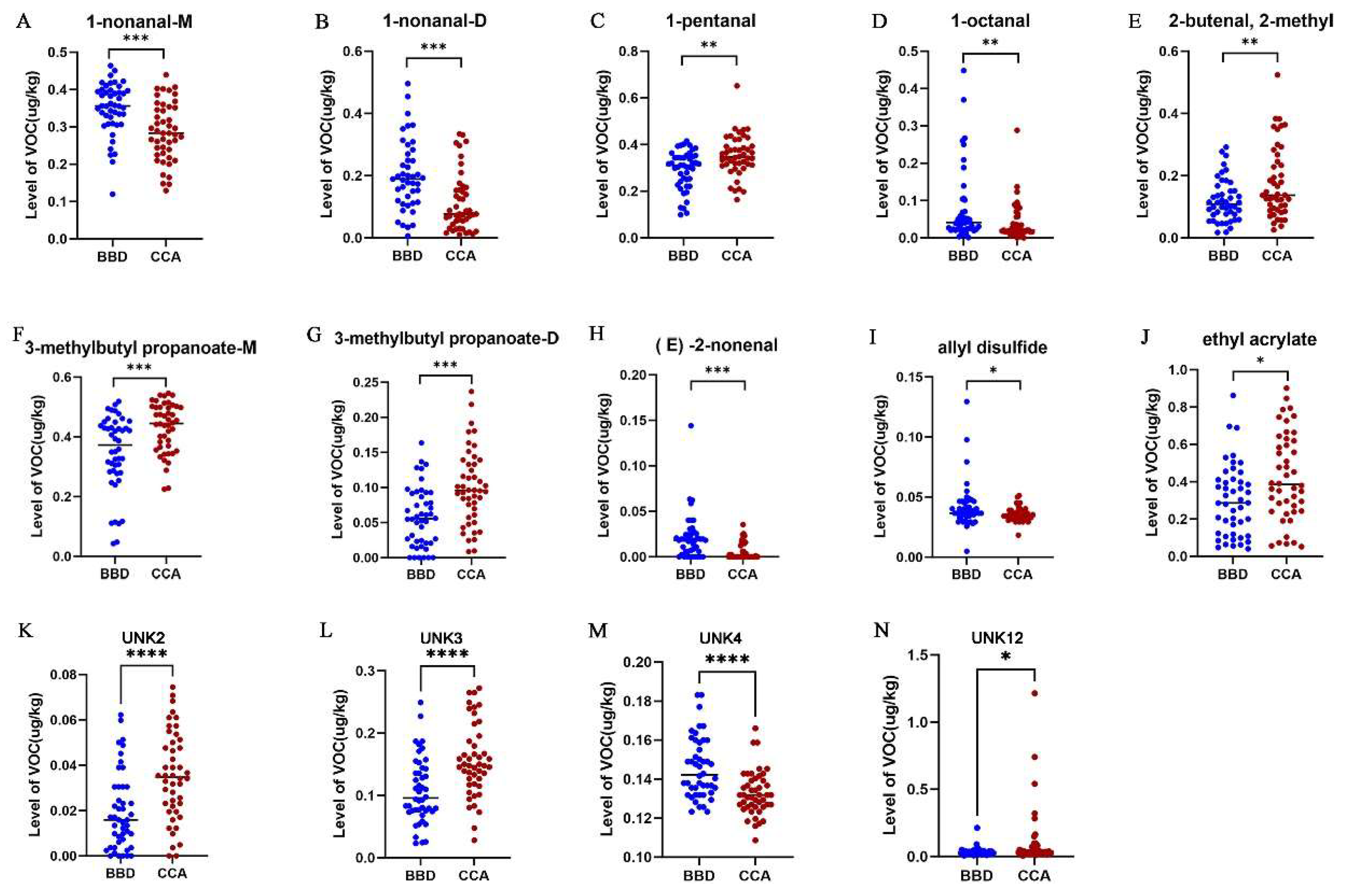

Table 1.
Clinical characteristics of all patients.
| BBD | CCA | p | |
|---|---|---|---|
| Age# | 55.13±17.712 | 70±10.75 | .001 |
| Male/Female | 24/22 | 28/18 | .406 |
| AFP* | 1.515(1.157-2.512) | 1.64(1.052-2.837) | .799 |
| CEA* | 1.590(0.815-2.282) | 2.825(1.775-4.742) | .001 |
| CA199* | 18.45(8.625-38.55) | 278(98.975-854.5) | .001 |
| WBC* | 6.095(5.452-7.020) | 6.980(4.720-8.275) | .689 |
| ALP* | 77(58.25-135) | 221.95(161.5-519.75) | .001 |
| GGT* | 51.6(18-178) | 215(127.75-385) | .001 |
| ALT* | 25.1(14.975-66.175) | 37.3(21.775-70.475) | .161 |
| AST* | 22.1(15.75-36.025) | 41.15(27.325-52.775) | .001 |
Table 2.
Quantitative analysis of VOCs.
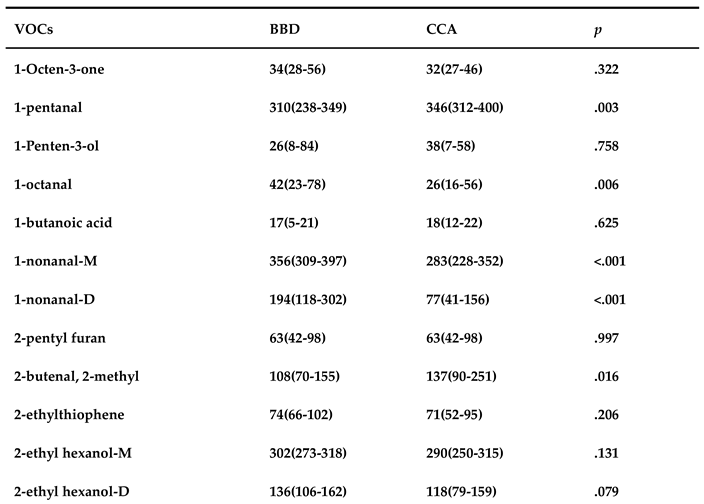
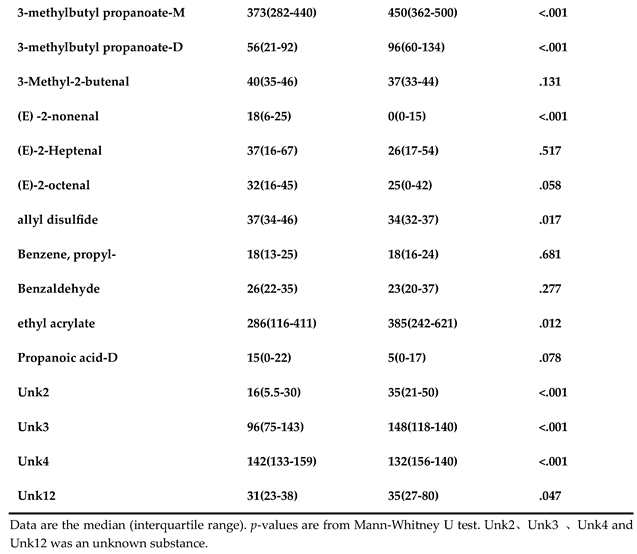
Table 4.
The p-values between each VOC and different pathological factors.
| VOCs | Age | Gender | Areas | Differentiation | Jaundice | Pathological Types |
|---|---|---|---|---|---|---|
| 1-nonanal-M | 0.318 | 0.212 | 0.966 | 0.847 | 0.170 | 0.725 |
| 1-nonanal-D | 0.506 | 0.071 | 0.942 | 0.989 | 0.329 | 0.891 |
| 1-pentanal | 0.233 | 0.589 | 0.158 | 0.280 | 0.039 | 0.055 |
| 1-octanal | 0.894 | 0.552 | 0.811 | 0.503 | 0.667 | 0.560 |
| 2-butenal,2-methyl | 0.381 | 0.906 | 0.650 | 0.201 | 0.254 | 0.631 |
| 3-methylbutyl propanoate-M | 0.203 | 0.831 | 0.233 | 0.639 | 0.313 | 0.004 |
| 3-methylbutyl propanoate-D | 0.866 | 0.884 | 0.128 | 0.295 | 0.763 | 0.036 |
| (E) -2-nonenal | 0.398 | 0.239 | 0.823 | 0.639 | 0.644 | 0.891 |
| allyl disulfide | 0.721 | 0.595 | 0.870 | 0.853 | 0.555 | 0.132 |
| ethyl acrylate | 0.730 | 0.464 | 0.322 | 0.846 | 0.987 | 0.038 |
| Unk2 | 0.750 | 0.457 | 0.694 | 0.221 | 0.245 | 0.369 |
| Unk3 | 0.508 | 0.719 | 0.444 | 0.800 | 0.508 | 0.458 |
| Unk4 | 0.135 | 0.550 | 0.333 | 0.943 | 0.017 | 0.515 |
| Unk12 | 0.903 | 0.606 | 0.877 | 0.659 | 0.861 | 0.492 |
Table 3.
The AUC, sensitivity and specificity of VOCs for CCA diagnosis.
| VOCs | AUC (95%CI) | Sensitivity (%) | Specificity (%) | p |
|---|---|---|---|---|
| 1-nonanal-M | 0.730(0.626 - 0.834) | 60.9 | 84.8 | .000 |
| 1-nonanal-D | 0.757(0.657 - 0.857) | 32.6 | 89.1 | .000 |
| 1-pentanal | 0.318(0.210 - 0.427) | 0 | 97.8 | .003 |
| 1-octanal | 0.666(0.554 - 0.778) | 4.3 | 100 | .006 |
| 2-butenal,2-methyl | 0.355(0.243 - 0.467) | 0 | 97.8 | .016 |
| 3-methylbutylpropanoate-M | 0.288(0.184- 0.392) | 0 | 97.8 | .000 |
| 3-methylbutyl propanoate-D | 0.266(0.164 - 0.367) | 2.2 | 87 | .000 |
| (E) -2-nonenal | 0.761(0.662 - 0.860) | 56.5 | 80.4 | .000 |
| allyl disulfide | 0.644(0.528 - 0.760) | 2.2 | 97.8 | .017 |
| ethyl acrylate | 0.348(0.236- 0.460) | 0 | 97.8 | .012 |
| Unk2 | 0.268(0.164- 0.372) | 4.3 | 89.1 | .000 |
| Unk3 | 0.261(0.158-0.363) | 0 | 97.8 | .000 |
| Unk4 | 0.750(0.652-0.849) | 2.2 | 100 | .000 |
| Unk12 | 0.380(0.264 - 0.495) | 2.2 | 100 | .047 |
Data are the median (interquartile range). p-value <0.05 indicates statistical significance(Mann-Whitney U test). AUC, area under the curve; CI, confidence interval; VOCs, volatile organic compounds.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



