Submitted:
09 December 2024
Posted:
10 December 2024
You are already at the latest version
Abstract
Speech disorders encompass a complex interplay of neuroanatomical, genetic, and environmental factors affecting individuals' communication ability. This review synthesizes current insights into the neuroanatomy, genetic underpinnings, and environmental influences contributing to speech disorders. Neuroanatomical structures such as Broca's area, Wernicke's area, the arcuate fasciculus, and basal ganglia, along with their connectivity, play critical roles in speech production, comprehension, and motor coordination. Advances in functional neuroimaging have highlighted the intricate brain networks involved in language, offering insights into typical speech development and the pathophysiology of speech disorders. Genetic studies have identified key genes involved in neural migration and synaptic connectivity, further elucidating the role of genetic mutations in speech disorders, such as stuttering and speech sound disorders. Beyond the biological mechanisms, the review explores the profound impact of psychological factors, including anxiety, depression, and ADHD, on individuals with speech disorders. Psychosocial comorbidities often exacerbate speech disorders, complicating diagnosis and treatment and underscoring the need for a holistic approach to managing these conditions. Furthermore, the review emphasizes the importance of interdisciplinary interventions integrating speech therapy, cognitive-behavioral therapies, and neurogenetic insights to offer personalized treatment options. Future directions point toward leveraging genetic testing, digital technologies, and personalized therapies, alongside addressing the psychosocial dimensions, to improve outcomes for individuals with speech disorders. This comprehensive overview aims to inform future research and therapeutic advancements, particularly in treating fluency disorders like stuttering.
Keywords:
Speech disorders
; Neuroanatomy
; Genetics
; Environmental factors
; Language pathophysiology
; Psychosocial comorbidities
; Stuttering
1. Introduction
Speech disorders are manifested due to dysfunctions in neuroanatomy, genetics and the environment [1,2]. Neuroanatomical aspects of speech are orchestrated by a dynamic interplay between various brain regions, including Broca's area and Wernicke's area, which are essential for language production and comprehension, respectively [3]. Functional imaging techniques such as fMRI have unveiled the neural circuits that activate during speech tasks, revealing the intricate choreography of motor planning, auditory feedback, and syntactic processing [4]. Genetic studies have identified key genes involved with neural migration and synaptic connectivity that are associated with language development [5]. The interaction between genetics and neuroscience of normal speech could lead to a deeper comprehension of language disorders and potential interventions. We have reviewed advances in speech disorders, the impact of comorbidities of neurogenic disorders, and psychological influences on this disorder. The review aims to understand the advances in the field, inform the next phase of a study, and evaluate the progress in therapies for stuttering. We plan to conduct surveys and interviews of speech therapists who treat patients with speech disorders.
2. Neuroanatomy of Speech
Speech development is a multifaceted process that begins in infancy and continues through early childhood, with the brain undergoing significant structural and functional changes to support this process. The neuroanatomy of speech development is deeply embedded in the dynamic interactions between various cortical and subcortical regions and the integration of sensory feedback with motor control (Figure 1)[6]. This extended overview explores these connections in greater detail.
2.1. Neuroanatomical Structures Involved in Speech Development
2.1.1. Broca's Area: Motor Aspects of Speech Production
Broca's area (Brodmann areas 44 and 45), located in most individuals' left inferior frontal gyrus, is critical for the motor aspects of speech production. This region is responsible for generating the motor plans required for fluent speech and the complex syntactic structuring of sentences [7]. The role of Broca's area extends beyond mere speech production; it is also involved in aspects of language comprehension that require processing of complex syntax, such as understanding sentences with non-canonical word orders [8]. Broca's area undergoes gradual maturation during speech development, closely tied to the child's increasing ability to produce coherent speech. Functional MRI studies have shown that activation in this region becomes more specialized for language production as children transition from babbling to producing meaningful words and sentences [9].
2.1.2. Wernicke's Area: Language Comprehension
Wernicke's area, located in the posterior part of the superior temporal gyrus, is primarily responsible for language comprehension. This region is heavily involved in processing auditory information, particularly the recognition of phonemes and words. The development of Wernicke's area parallels a child's growing ability to understand spoken language, evident in the early stages of speech development when infants begin to recognize familiar words and respond to spoken commands [10]. Neuroimaging studies have demonstrated that Wernicke's area and adjacent auditory cortex regions are highly active when children listen to spoken language. As language comprehension skills develop, the connectivity between Wernicke's area and other language-related regions, such as Broca's area, strengthens, facilitating more efficient communication between language production and comprehension networks [11].
2.1.3. Arcuate Fasciculus: Connectivity and Coordination
The arcuate fasciculus, a white matter tract connecting Broca's and Wernicke's areas, is crucial in integrating speech production and comprehension. It is essential for repeating words and sentences and tasks that require auditory feedback, such as mimicking sounds or learning new words. Damage to the arcuate fasciculus can result in conduction aphasia, where individuals struggle to repeat spoken words despite having intact comprehension and speech production abilities [12]. During early childhood, the arcuate fasciculus undergoes significant myelination, enhancing communication speed and efficiency between the frontal and temporal language regions. This process is vital for developing phonological working memory, a key component of language acquisition that allows children to hold and manipulate sound patterns in their minds while learning to speak [13].
2.1.4. Basal Ganglia: Modulation of Motor Speech
The basal ganglia, a group of subcortical nuclei, are involved in the modulation of motor activities, including speech. These structures regulate speech timing, rhythm, and the smooth execution of articulatory movements. Dysfunction in the basal ganglia is associated with motor speech disorders such as dysarthria, where speech becomes slurred or slow [14]. In speech development, the basal ganglia work with cortical motor areas to refine the motor commands necessary for clear and fluent speech. Research suggests that these structures also play a role in acquiring language skills, particularly in procedural memory, which supports learning speech patterns and grammar rules through repeated practice [15].
2.1.5. Cerebellum: Coordination and Timing
The cerebellum, traditionally associated with motor coordination and balance, also contributes to speech development by ensuring the precise timing and smooth execution of speech movements. The cerebellum interacts with cortical speech regions to fine-tune the motor commands for articulation, helping to coordinate the rapid and intricate movements of the mouth, tongue, and vocal cords required for fluent speech [14]. Functional neuroimaging studies have shown that the cerebellum is activated during speech production tasks that require precise motor control, such as speaking rapidly or articulating complex sentences. The cerebellum's role in speech is also evident in developmental disorders like ataxic dysarthria, where cerebellar dysfunction leads to difficulty coordinating speech movements [16].
2.1.6. Primary Motor Cortex: Execution of Speech Movements
The primary motor cortex, particularly the area responsible for controlling the mouth, face, and tongue muscles, is crucial for the physical execution of speech. This region receives input from the premotor cortex and sensory cortices to generate the motor commands for articulate speech [17]. In speech development, the primary motor cortex works closely with subcortical regions like the basal ganglia and cerebellum to refine speech-motor control. As children practice speaking, the neural circuits in the motor cortex are fine-tuned to produce smooth and coordinated speech. This is supported by feedback from sensory systems, which helps adjust motor outputs based on auditory and tactile sensations [18].
2.2. Neurodevelopmental Changes in Speech and Language Acquisition
During infancy and early childhood, the brain undergoes critical periods of plasticity where it is particularly receptive to language input. During these periods, the language networks in the brain are shaped by exposure to spoken language, leading to the development of neural circuits that support speech production and comprehension [19] For instance, infants are born able to distinguish between the phonemes of all human languages. Still, by the end of the first year, their brains become specialized for the phonemes of their native language, primarily influenced by the environment in which they are raised [20]. This specialization reflects changes in the connectivity and functionality of brain regions involved in speech and language processing. The maturation of white matter tracts, such as the arcuate fasciculus, is essential during this period, as it supports the integration of auditory and motor systems necessary for speech development [13]. Similarly, the myelination of other speech-related pathways continues throughout childhood, contributing to refining language skills, including vocabulary expansion and the ability to construct complex sentences.
The neuroanatomy of speech development is a dynamic and interconnected system that involves several key brain regions, including Broca's and Wernicke's areas, the arcuate fasciculus, the basal ganglia, the cerebellum, and the primary motor cortex. These structures work together to support the intricate processes of speech production, language comprehension, and motor coordination, which are crucial for successful speech development. The interplay between these regions and the continuous refinement of neural circuits highlights the brain's remarkable plasticity during early language acquisition, shaping the foundations for lifelong communication skills.
3. Genetics of Speech
Speech is defined as the ability to express one’s thoughts and feelings through articulate sounds, and it comprises three main components – articulation, voice, and fluency. Several aspects of speech can be understood, but in this section, we will focus on the genetic mechanisms of speech, explicitly stuttering [21,22,23]. A proper understanding of the genetic mechanisms of speech requires a thorough exploration of the genetic causes of certain speech disorders, such as Verbal dyspraxia, Speech Language Impairment, and Stuttering. Although speech disorders are caused by several factors, which may be environmental or genetic, it is observed that in several cases, by studying the genomes of people with speech disorders, we can ascertain specific genes that majorly contribute to the presentation of these disorders. This is done through linkage and association studies, which mark the approximate location of an etiologic genetic variant (such as an SNP) in a segment of DNA. Multiple genes are required for the normal functioning of the genetic mechanisms of speech (Table 1). A single gene or a group of genes participate in specific pathways that make speech and related functions possible, such as processing, understanding, formation, production, and fluency (Figure 2). Single nucleotide polymorphisms (SNPs) are irregular base changes in DNA that mutate and can affect the functioning of genes in speech-related pathways. This can give rise to speech disorders. In this paper, only a few significant pathways are discussed in detail.
4. Speech Disorders
Speech disorders encompass a broad range of conditions affecting an individual's ability to produce sounds that result in fluent and clear speech vocabulary, syntax, morphology, semantics or a combination of these elements of speech [36]. These disorders are heterogenous in nature and affect. These conditions can be congenital or acquired, and often present alongside various comorbidities, impacting quality of life and communication abilities.
The American Speech-Language-Hearing Association (ASHA) classifies speech disorders into organic (caused by neurological, motor, anatomical, or sensory impairments) and functional (without a known cause). While many classification systems exist, most agree on overlapping error patterns in speech quality, voice, and fluency. This review adopts the following categories (Figure 3)
4.1. Speech Sound Disorders
4.1.1. Articulation Disorders
Articulation disorders involve atypical speech production through substitution, omission, addition, or distortion of sounds, often leading to unintelligible speech [37]. These disorders typically result from motor control issues in speech muscles, affecting sounds like /r/, /l/, and /s/, and are linked to atypical brain development in areas like the motor cortex and cerebellum [38]. In children, they manifest as mild-to-moderate speech defects and are often associated with hearing loss [39]. Prevalence ranges from 2.3% to 24.6% in school-aged children, with higher rates in boys and influenced by ethnicity. In adults, articulation disorders are linked to traumatic brain injuries, strokes, and neurological conditions, and often co-occur with other disorders such as stuttering, ADHD, and language impairments [40]. Dyslalia refers to the misarticulation of phenomes, often due to learning errors or structural abnormalities like cleft palate or dental issues. Neurobiologically, dyslalia is less about neural deficits and more about physical anomalies in the speech producing organs. Poor oral habits such as nail biting, thumb sucking, as well as atypical swallowing have been ascribed as causing dyslalia although with insufficient evidence to support the claim [37].
4.1.2. Phonological Disorders
Phonological disorders involve difficulty learning a language's sound system, leading to speech sound errors. This is linked to atypical neural processing in areas responsible for phonological representation and auditory processing. One theory suggests individuals with phonological disorders struggle to grasp the phonological rules of a language [38]. Researchers agree that early speech errors predict phonological disorders [41,42]. Another theory links phonological disorders to executive dysfunction, which affects higher cognitive functions like reasoning, pattern recognition, and memory retention [43]. Impairments in executive functioning may result in errors in phonological speech production.
4.2. Motor Speech Disorders
Verbal speech production involves a sequence of motor coordination and executive functions. Motor speech disorders (MSD) are caused due to impairments in motor systems that result in speech production deficits. Impairments in motors systems can be due to neuromuscular dysfunction or disruption in higher-level motor commands [44]. The most commonly occurring motor-speech disorders are Dysarthria, speech disorders resulting from disrupted muscular control, and Apraxia of speech, speech impairments due to disrupted motor planning [45].
4.2.1. Apraxia of Speech
Apraxia of speech is a motor speech disorder in which individuals have difficulty planning and coordinating the movements necessary for speech [46]. Individuals with AOS often have trouble communicating what they want to say as result of faulty brain pathways in planning the sequence of speech sound production. It involves ‘effortful groping for articulatory movements’ in speech production [47]. The clinical presentation of Apraxia is a slow rate of speech with consonants and vowel distortions, sound substitutions, and prosodic abnormalities [48]. Apraxia of speech can either be acquired or is present from birth. Acquired AOS or Neurological AOS is predominantly a result of left-hemispheric strokes and neurodegenerative diseases. Childhood Apraxia of speech is characterized by inconsistent speech production, vowel and voicing errors, consonant cluster deletions and prosodic disruptions [49].
4.2.2. Dysarthria
Dysarthria is a motor speech disorder resulting from neurological injury to the motor components of the speech production system. It results from disturbance in respiration, phonation, resonance, articulation, and prosody [50]. About 90% of individuals suffering from Parkinson’s disease [51] and 10-60% of individuals with a traumatic brain injury develop dysarthria [52]. There are several types of dysarthria, each associated with damage to different parts of the nervous system: Flaccid, Spastic, Ataxic, Hypokinetic, Hyperkinetic, and Mixed Dysarthria.
4.3. Fluency Disorders
About 1% of children and adolescents in the global population suffer from stuttering, and even less from cluttering [53]. ASHA defines fluency as ‘continuity, smoothness, rate, and effort in speech production’. Therefore, interruption in the flow of speaking due to atypical speech rate, rhythm of speaking, accompanied by irregular repetitions of words/syllables, prolongation of sounds is classified as fluency disorder. Individuals suffering from fluency disorders have deficits in secondary mannerisms such as speaking avoidance, anxiety, emotional and psychological distress, as well as avoidance of social situations that require speaking [54].
4.3.1. Stuttering
Stuttering is characterized by a disrupted rate of speech, prolongation of sounds, difficulty in starting to speak, use of filler words, and repetitions. It is more common than cluttering in children and in some cases, children outgrow it without any therapeutic interventions. Some degree of disfluency in speech is expected in all speakers, especially the repeated use of filler words. However, prolonged disfluency can be distressing to the individual as they are self-aware of the condition and can lead to avoiding talking all together [55]. While idiopathic stuttering occurs due to functional or structural cerebral anomalies and is often limited to childhood, acquires stuttering occurs due to brain injury irrespective of age. In an extremely rare scenario, an individual can develop a psychogenic stuttering, usually after puberty, because of either an underlying psychiatric illness or psychological trauma [56].
4.3.2. Cluttering
In contrast to stuttering, cluttering is characterised by rapid or irregular speech, with abnormal pauses, omission or contraction of syllables, and dysregulated speech rhythm that is not typical of stuttering [57]. While there is repetition of speech, it is mostly repetition of words and parts of sentences as opposed to sounds and syllables in stuttering. Cluttering is also characterised by monotonous speech, impaired word retrieval, and semantic-lexical impairments [53]. A key differentiation between stuttering and cluttering is that the latter is accompanied by poor spelling and writing abilities which is intact in stuttering. Cluttering often occurs alongside auditory processing disorders, Tourette’s syndrome, ADHD, ASD, and learning disabilities.
4.4. Dysphonia or Voice Disorder
Dysphonia is a disorder characterized by difficulties in voice production, often due to problems with the vocal cords or the muscles controlling them. It is often called “hoarseness” and is an observable decline in voice quality [58]. Recent studies have shown an onset of Dysphonia in individuals affected by COVID-19 [59].
4.4.1. Mutism
Mutism is the inability or unwillingness to speak in certain situations despite having the ability to speak in others. It rarely occurs in isolation and is often accompanied by behavioral and psychological disturbances [60].
4.4.2. Selective Mutism
4.4.3. Cerebellar Mutism
This category of mutism often occurs post-posterior fossa tumor resection in children, but it can also occur due to vascular incidents and infections [63]. The clinical presentation is characterized by delayed onset (1-6 days post tumor resection) and rapid and spontaneous recovery period (within 4months) with speech dysarthria.
4.4.4. Speech Dysrhythmia
Speech Dysrhythmia involves disruptions in the rhythm and timing of speech, often seen in conditions like stuttering. Rhythm perception is crucial for synchronization of voice, movement, and emotion with whom we are interacting [64]. Clinical presentation of speech dysrhythmia is arrested speech usually at the beginning of the sentence or word, prolongation of words along which if often accompanied by stuttering.
4.4.5. Childhood Speech Disorders
Childhood speech disorders encompass a range of speech impairments that occur during the developmental period. These can include any of the previously mentioned disorders but are often associated with developmental conditions like autism spectrum disorder (ASD) or developmental language disorder (DLD). One in twenty pre-school children show signs of developmental speech and language disorder stemming from learning and intellectual impairments aside from genetic contributions [65]. Childhood speech disorders are frequently linked to atypical development of language-related brain regions, such as the superior temporal gyrus and the arcuate fasciculus, a white matter tract that connects Broca's and Wernicke's areas [66].
4.4.6. Broca’s Aphasia
Broca’s aphasia is one of the most commonly occurring expressive aphasia, language impediments caused from damage to the brain regions responsible for language. Although not a speech disorder, it often occurs with apraxia of speech and dysarthria. Broca’s Aphasia results from damage to the brain region referred to as Broca’s area or the inferior frontal lobe of the dominant hemisphere which is responsible for making sounds to create a word. One of the clinical presentations of Broca’s aphasia includes an inability to produce words which affects the fluency of normal speech [67].
5. Psychological Comorbidities
Psychological comorbidities refer to the simultaneous presence of two or more psychological conditions in an individual. These comorbidities can complicate diagnosis and treatment, making it essential to explore their impact on overall health and treatment outcomes [68,69]. The dynamic nature of stuttering has led to various theories about its causes, with individuals often experiencing significant psychological distress. People who stutter frequently report feeling more comfortable speaking alone rather than in group settings. Common psychological issues associated with stuttering include fear of negative evaluation, heightened communication apprehension, and poor self-perception regarding communication competence. These factors can severely affect an individual’s quality of life [70,71,72,73]. Research has shown that adolescents and adults who stutter often face poorer psychosocial outcomes, including increased anxiety, particularly in those who have experienced childhood bullying [74,75]. Efforts have been made to explore the links between stuttering and various biopsychosocial factors such as temperament, anxiety, depression, and ADHD. These studies aim to identify potential comorbid conditions in children, adolescents, and adults with stuttering [70,76].
5.1. Social Factors of Stuttering & Its Comorbidities
5.1.1. Cultural and Environmental Factors
Cultural and societal norms are also suggested to affect stuttering. In a study by Tellis et al., 22.4% of Hispanic-American college students believed that the pressure placed by parents on a child to speak two languages caused stuttering, and 39.4% agreed with the statement that switching from the L1 (Spanish) to L2 (English) was the source of stuttering [77]. Nwokah et al., suggested that experience might interact with stuttering severity. Igbo children with negative school experiences stuttered more in English, the language of instruction, while those who faced challenges at home stuttered more in Igbo, their home language [78]. Dale et al., suggested that parental dissatisfaction with their children's "imperfect" Spanish, along with labeling common disfluencies in four Cuban-American children, was the primary cause of stuttering [79]. Environmental context reflects the influence of other people in the speaker’s life. The environmental context can influence the speaker via a conversation partner or, more generally, via society as a whole [80]. Studies suggest that speaking pressure, whether real or perceived, can have a negative impact on people who stutter [81,82]. This is compounded by societal stigma, which often portrays stuttering as abnormal, reinforcing negative public opinions [83,84]. Self-stigma arises when individuals internalize negative societal expectations, such as the ideal of fluency, and view their stuttering as a personal shortcoming. Furthermore, the pressure to meet these external expectations can lead to heightened physical tension during speech, which may exacerbate stuttering severity and create additional challenges in communication [54,80].
5.1.2. Bilingualism
Early research showed that bilingual children exhibited more disfluencies in speech than their monolingual counterparts. [85,86]. Bilinguals have been observed to perform worse than monolinguals on tasks requiring lexical access such as naming objects [87] and verbal-fluency tasks (eg- coming up with as many words as possible for a given letter) irrespective of dominant or non-dominant language being used. This has been attributed to the difference in vocabulary size with their monolingual peers in each of the two languages [88], as well as to the interference in lexical access between the languages [89,90]. Van Borsel et al., (2001) proposed that early exposure to several languages could be a risk factor in stuttering [91]. As an extension, bilingualism was also suggested as a risk factor for developing stuttering in children [92]. On the flip side, other aspects of cognition such as inhibitory control and task switching improve [93,94]. These advantages are presumed to result from practice shifting from one language to another and inhibiting the language not used. Given that people with stuttering (PWS) may have reduced executive functions, a counterargument would be that bilingualism is a protective factor in children at risk for stuttering [95]. Such an effect as yet to be documented; however, Kornisch (2021) hypothesizes that bilingualism may act to offset deficits in executive functions that have been identified in numerous studies of monolingual PWS [96]. Other studies have shown no significant differences in executive functioning between monolingual and bilingual populations of school children [97,98]. There is yet to form a consensus among researchers as to whether bilingualism would act as a protective factor or risk factor in the case of stuttering.
5.1.3. Linguistic Factors
Various studies have suggested that differences in disfluencies across languages spoken by BWS can be attributed to language-specific variations in morphosyntax, phonology, and syllabic structure [99,100]. These claims are yet to be empirically tested and remain theoretical for now. While linguistic differences in areas like word formation, inflection, and sentence types [101] complicate comparisons of stuttering severity across languages, various studies have explored this notion of complexity. For instance, Brown et al., identified phoneme position, sentence position, grammatical class, and word length as factors contributing to higher stuttering frequency [102]. Other studies by Howell et al., and Ononiwu focused on phonological complexity between languages [103,104]. One notable method for assessing this complexity is the Index of Phonetic Complexity (IPC) Scheme [105], which evaluates eight factors such as consonant and vowel class, word shape, word length, and contiguous consonants. A study in 2007 and 2011 applied the IPC scheme to compare stuttering frequency in monolingual Spanish and English-speaking individuals, revealing that English function words were more complex than Spanish ones [56,106]. In 2013 Al-Tamini et al., this approach was adapted to Arabic with the development of an Arabic IPC (AIPC), finding that stuttered Arabic words were more phonetically complex than non-stuttered ones [107]. Another study in 2010 by Ononiwu extended the examination of phonological complexity across seven languages (Afrikaans, English, French, Igbo, Kannada, Mandarin, and Spanish) using various analytical methods, such as a four-factor phonological analysis and stress/rhythmic analysis, with English emerging as the most phonologically complex language based on these criteria [104]. Although these studies suggest that linguistic complexity may influence stuttering, the evidence remains largely correlational rather than causally proven. There is a need for more comprehensive experimental research to solidify these attributions and their practical applications. Investigating comorbidities in stuttering is crucial for several reasons. It enhances our understanding of the disorder’s presentation and the individual differences in experiences. This knowledge is essential for developing effective treatment plans tailored to the specific needs of individuals with stuttering and their comorbid conditions.
5.1.4. Anxiety
Anxiety is a future-oriented emotion that is a long-acting response broadly focused on a diffuse threat characterised by cognitive components of negative thoughts and beliefs of upcoming events, behavioural components of the desire to escape situations and the physiological components of activation of the sympathetic nervous system [108,109]. It comprises a transitory state known as the state anxiety and a relatively permanent state known as the trait anxiety reflecting one’s personality characteristic of responding anxiously to potentially threatening situations [110]. Anxiety disorders such as the Generalised Anxiety Disorder are diagnosed as a result of abnormally high levels of anxiety such that the symptoms reflect the maladaptive behaviours of an individual impacting their daily functioning in multiple contexts. More particularly, social anxiety disorder refers to the fear or avoidance of social interactions and situations that may result in scrutiny. Early research concluded the association between anxiety and stuttering to be weak [111]. This was also based on the difficulty in interpreting this link due to reasons such as the multidimensional nature of anxiety, small sample sizes in studies, differences in treatment status of patients based on when they are included in a study and the measures used to assess anxiety [112].
Studies show variable results for elevated anxiety among CWS. Prominent narrative reviews in this field suggest that CWS may not be predisposed to anxiety through increased familial risk or temperament traits but they are at a higher risk of developing anxiety as they are more likely to be exposed to negative peer reactions, bullying and stereotyping during adolescence [70,109]. With limited results for pinning down a particular age for this, some studies indicate school age and teenage years as crucial periods for this development and manifestation of social anxiety; while negative attitudes towards speech develop at a young age they worsen as they grow older [113,114]. CWS in school and adolescents with additional disorders also appear to be at a higher risk for developing social anxiety [115]. Comparatively, a recent meta-analysis by Bernard et al. (2022) found a moderate summary effect size difference indicating that children and adolescents who stutter present with increased anxiety symptoms (g = 0.42, p = 0.02, 95% CI [0.1, 0.743], df = 9.45) as against non-stuttering peers (presented statistic is mean effect size difference called ‘Hedge’s g’ for 851 participants of whom 384 with stutter across the 11 studies considered). Upon performing a meta-regression analysis for situation-specific (state anxiety and social anxiety subscales) and general anxiety domains (trait anxiety and generalised anxiety subscales) they found that while elevated anxiety was observed in measures for both the domains of social and general anxiety, the measures used were not sufficiently sensitive to distinguish between the two and rather a longitudinal approach would help determine the differences. It is important to note that elevated anxiety scores among CWS do not necessarily point towards clinical anxiety disorder but are mentioned in relation to differences in symptom summary scores [76]. However, the authors strongly suggest that the influence of recruitment bias accrued to clinically ascertained cohorts that make up over half of the included studies in the current review eventually leading to the question of representativeness. Using a broader group of CWS from the population including those who receive and those who do not receive clinical treatment could lead to more generalizable findings.
With some improvement in the methodological issues of studying links between anxiety and stutter, meta-analyses have shown that persistent stuttering in adults is associated with significantly elevated trait and social anxiety when compared to non-stuttering adults [116]. Adults who stutter are shown to be at an increased risk of meeting the diagnostic criteria for clinical anxiety disorders, particularly social anxiety disorder [117,118]. It is supposed that increasing self-awareness, and exposure to negative reactions from peers especially due to increased demands of academic, vocational, social and interpersonal aspects during adolescence and early adulthood lead to anxiety in AWS [109]. An interesting hypothesis about the link between the motor symptoms of stuttering and anxiety shows the unidirectional relationship between the two. While reducing anxiety may not work towards improving fluency amongst AWS, improvement in fluency may result in reduced anxiety [119,120,121]. However, there have been mixed results for the latter [122,123].
5.1.5. Depression
The American Psychological Association (2013) characterizes depression as a prolonged sad, empty or irritable mood along with somatic and cognitive changes that have a substantial impact functionally. There have been mixed findings regarding elevated depression symptoms in some adolescents and young adults who stutter such that some find differences compared to controls [124,125] and some do not [126]. Bernard et al. (2022) suggest differences in depression scores that were high among the stuttering group for four out of the five measures reported across three studies but the difference was not statistically significant in any study. They attribute this ambiguous result to the age range of the sample across studies (<15 years) given the later onset of depression in the general population [76].
5.1.6. Temperament
Temperament is referred to as the biologically determined part of personality that is assumed to be constitutional; inherent and relatively stable [127]. It could also be described as the individual differences in one’s emotion-based habit patterns [128]. Research in this domain with regard to stuttering has given rise to the assumption that people with this condition tend to have a reactive temperament that is they are more emotionally sensitive which interacts with their linguistic or motor problems of stutter. It is proposed that these traits can increase the risk of developing chronic stuttering as it is believed that people with stutter may react with a stronger muscular tension to emotional problems [129]. Children with stutter who experience greater negative reactivity are also more likely to develop anxiety [130]. Theoretically, it has been proposed that young children with a genetic predisposition to stuttering with typical temperamental tendencies of increased negative affect, reduced emotional and attentional regulation may be likely to start stuttering, with an increased risk of developing negative reactions to stuttering and reduced resilience to coping in the long term [129,131,132]. However, in their review, Van Riper (1982) did not find any substantial difference in the personality of people who stutter [133]. The evidence from parent-report measures and experimental tasks has not been able to corroborate the relationship between stuttering severity and/or frequency with temperamental traits in CWS using these two measures [70]. Jones et al. (2014) suggest that experimental studies with CWS under 7 years have generally been able to find a relationship between temperament domains of emotional reactivity and regulation and stuttering severity and/or frequency [134]. On the other hand, parent-report measures of temperament with this age group show inconsistent results [135,136,137,138,139].
Alm (2014) discusses the possibility of a subgroup of children who stutter (CWS) exhibiting traits of hyperactivity and impulsivity, which may result in lower scores for shyness. This suggestion is based on findings that CWS display significantly lower perceptual sensitivity (possibly indicating inattention), reduced inhibitory control, poorer attentional shifting, and higher activity levels compared to children who do not stutter (CWNS). Additionally, some results, though not statistically significant, suggest that certain CWS may show lower anxiety traits than CWNS [135]. Delpeche et al. (2022) state that the varied findings are a result of methodological differences such as the use of small sample sizes in some studies, varied age ranges included and the kind of sample studied (community, clinical or research). Differences in investigating stuttering frequency or severity along with the measures used to assess them also add to the mixed literature [140]. Parent and child perceptions of temperament were both considered to determine its role in stuttering frequency and impact in children under the age of 7 years. While negative reactivity was associated with stuttering impact in CWS regardless of age from a parent’s perspective, it was not the case when children reported their attitudes towards communication. Positive reactivity and emotional regulation were not associated with stuttering impact in young CWS from both perspectives. Temperament was not associated with stuttering frequency [140].
5.1.7. ADHD
Attention Deficit Hyperactivity Disorder (ADHD) is characterised as a neurodevelopmental disorder with a combination of persistent behaviours of inattention, impulsivity and hyperactivity that begins in childhood (National Institute of Mental Health). The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) defines inattention and disorganisation as the inability to stay on task and listening issues that are not in accordance with one’s age or developmental level [141]. Hyperactivity-impulsivity can be indicated by overactivity, fidgeting, difficulty in staying seated, intruding into other people’s activities and inability to wait. ADHD is diagnosed in a person when their attention difficulties or hyperactivity exceeds what is generally seen in their equivalent mental age group. People with this disorder can exhibit a combined presentation; predominantly on attention or predominantly on hyperactivity-impulsivity (American Psychiatric Association, 2013).
The commonality between people who stutter and people who have ADHD is confirmed by evidence of attention issues and speech disfluencies occurring in both these conditions highlighting the fact that they may share similar psychological, social and neural issues [142,143,144,145,146,147,148,149]. Parent-reported surveys: Studies using tools like the Children's Behaviour Questionnaire and the Behavioural Style Questionnaire consistently found significant differences between CWS and Children Who Do Not Stutter (CWNS) in ADHD-related traits. Children who stutter (CWS) exhibit several traits that overlap with characteristics commonly associated with ADHD. These include lower perceptual sensitivity and poor adaptability, potentially indicating inattention [135,150]. Additionally, CWS demonstrate lower inhibitory control and poorer attentional shifting, which are core ADHD traits [151]. A higher activity level is also observed in CWS, aligning with hyperactive tendencies seen in ADHD [135]. Furthermore, CWS show lower emotional regulation and heightened emotional reactivity, characteristics that similarly overlap with ADHD profiles [152,153].
Experimental studies supported the parent-reported findings, with some CWS showing a tendency toward impulsivity and lower inhibitory control. This suggests that a subset of CWS may have traits consistent with ADHD, though not all cases of stuttering involve these traits [154,155]. Some studies suggest that ADHD traits in CWS may have a genetic or neurological basis. CWS with neurological incidents linked to ADHD traits might experience more persistent stuttering, which could contribute to a higher incidence of Adults Who Stutter (AWS) [142]. These findings indicate that the ADHD-like traits in CWS may be part of a broader neurodevelopmental profile. The speech disorder of cluttering, often associated with ADHD-like tendencies such as impulsivity and disorganized speech, may provide another explanation for the link between ADHD traits and stuttering [148]. This suggests that cluttering and stuttering may sometimes overlap, further complicating the relationship between stuttering and ADHD. Recovery from stuttering: Interestingly, some studies suggest that hyperactivity and lower emotional reactivity may actually serve as positive prognostic factors in childhood stuttering. Children with these traits might have a higher likelihood of recovering from stuttering compared to those who do not exhibit these traits [145,156]. This offers a nuanced view of ADHD-like traits, indicating they may not always worsen stuttering outcomes.
While both stuttering and ADHD conditions are said to affect working memory, more nuanced details are required to check their similarities in cognitive architecture [157,158,159,160]. Kazazi et al., probes into newer and more contemporary research methods to determine the link between the two disorders [161]. They suggest the use of Network Modelling that is used in studies of comorbidities amongst disorders wherein they are viewed as clusters of directly related symptoms that can interact with one another and be supposedly causally linked [162,163,164]. These networks of symptoms are then used to find and analyse statistical relationship patterns in multivariate psychological data [165]. Using this method they also suggested that symptoms of stuttering and ADHD while impacting the frontal cortex are not comorbid meaning their cognitive architectures may be different. While working memory and executive function are impaired in both these disorders, they affect different types of attention in both. Inattention in people with stuttering issues can be assessed better using an auditory selective attention task while the same can be assessed better using sustained attention tasks in people with ADHD. They propose the use of Network Models so that clinicians can better assess these conditions and provide new treatment strategies [161].
The relationship of stuttering with temperament, anxiety, depression and ADHD has a complex nature. However, research about these links has helped zoom into the nuances of experiences of people with stutter. Recent evidence suggests that higher negative reactivity scores and lower positive reactivity and self-regulation scores are associated with elevated levels of anxiety and depression who stutter showing an interrelation among temperament, anxiety and depression [166]. Temperament and ADHD have also been linked to suggest that emotional reactivity and hyperactivity in CWS could potentially be positive prognostic factors [145,151]. Kazazi et al.,, also explored contemporary techniques such as Virtual Reality (VR), Network Modelling and a combination of cognitive, behavioural and physiological assessments that probe deeper into the relationship between stuttering and ADHD. VR can be useful in creating an immersive environment and precise measurement of attention in behavioural, oculomotor and EEG data when working with assessing links between stutter and ADHD. The mixed methods approach emphasises the triangulation of data that can help overcome deficits in inconsistencies in results observed through the use of a single approach. The use of network modelling as an in-depth method of assessing interrelationships between various symptoms across disorders can also delve deeper into the structure of comorbidities [161,167].
6. Future Outlook
The future of research and treatment in speech disorders is set to evolve with advancements in neuroscience, genetics, digital and machine learning technologies. The intersection of these technologies will help map out the intricate neural circuits that underlie speech production, comprehension, and motor control with greater precision. By identifying specific neural pathways disrupted in speech disorders, targeted interventions that address the underlying neural dysfunctions, have the potential to transform methods in speech therapy. As genetic testing becomes more affordable and accessible, personalized genetic profiling can enable clinicians to diagnose speech disorders at an earlier stage and tailor interventions to a patient’s specific genetic makeup. Gene therapy for genetic hearing disorders are in clinical trials, and can also be applied to speech disorders by targeting and correcting the specific genetic abnormalities. The integration of digital therapies combined with machine learning based speech recognition tools can be applied to personalized therapy programs that adjust to the patient’s needs in real-time. Music-based therapies are already main-stream therapies. The NIH has allocated significant funds for research on the use of music therapies, spearheaded by the ex-Director, Francis Collins (NIH 2019). The use of rhythm, timing, and melody in music therapy is already being applied to speech production and motor coordination, helping patients—particularly those with fluency disorders like stuttering—overcome disfluencies. The role of psychological treatment in managing speech disorders are utilizing integrated care models, where speech-language pathologists, psychologists and other mental health professionals are addressing the emotional and psychological components of speech disorders. This holistic approach will help reduce the stigma associated with speech disorders and provide patients with more comprehensive care, improving outcomes in both speech fluency and mental well-being. In conclusion, the future of speech disorder treatment is headed toward more individualized, multidisciplinary, and technologically advanced solutions. By harnessing the power of genetics, neuroscience, digital innovation, and psychological care, the field will move closer to offering patients more effective, precise, and accessible treatments tailored to their unique needs.
References
- Mountford HS, Braden R, Newbury DF, Morgan AT. The Genetic and Molecular Basis of Developmental Language Disorder: A Review. Children (Basel). 2022 Apr 20;9(5). [CrossRef]
- Morgan AT, Amor DJ, St John MD, Scheffer IE, Hildebrand MS. Genetic architecture of childhood speech disorder: a review. Molecular Psychiatry. 2024 May 1;29(5):1281–92. [CrossRef]
- Fujii M, Maesawa S, Ishiai S, Iwami K, Futamura M, Saito K. Neural Basis of Language: An Overview of An Evolving Model. Neurol Med Chir (Tokyo). 2016 Jul 15;56(7):379–86. [CrossRef]
- Loucks T, Kraft SJ, Choo AL, Sharma H, Ambrose NG. Functional brain activation differences in stuttering identified with a rapid fMRI sequence. J Fluency Disord. 2011 Dec;36(4):302–7. [CrossRef]
- den Hoed J, Fisher SE. Genetic pathways involved in human speech disorders. Current Opinion in Genetics & Development. 2020 Dec 1;65:103–11. [CrossRef]
- Rogalsky C, Basilakos A, Rorden C, Pillay S, LaCroix AN, Keator L, et al. The Neuroanatomy of Speech Processing: A Large-scale Lesion Study. J Cogn Neurosci. 2022 Jul 1;34(8):1355–75. [CrossRef]
- Friederici AD. The brain basis of language processing: from structure to function. Physiol Rev. 2011 Oct;91(4):1357–92. [CrossRef]
- Rogalsky C, Matchin W, Hickok G. Broca’s area, sentence comprehension, and working memory: an fMRI Study. Front Hum Neurosci. 2008;2:14. [CrossRef]
- Redcay E, Courchesne E. Deviant functional magnetic resonance imaging patterns of brain activity to speech in 2-3-year-old children with autism spectrum disorder. Biol Psychiatry. 2008 Oct 1;64(7):589–98. [CrossRef]
- Rosselli M, Ardila A, Matute E, Vélez-Uribe I. Language Development across the Life Span: A Neuropsychological/Neuroimaging Perspective. Neurosci J. 2014;2014:585237. [CrossRef]
- Skeide MA, Friederici AD. The ontogeny of the cortical language network. Nat Rev Neurosci. 2016 May;17(5):323–32. [CrossRef]
- Catani M, Mesulam M. The arcuate fasciculus and the disconnection theme in language and aphasia: history and current state. Cortex. 2008 Sep;44(8):953–61. [CrossRef]
- Paus T, Zijdenbos A, Worsley K, Collins DL, Blumenthal J, Giedd JN, et al. Structural maturation of neural pathways in children and adolescents: in vivo study. Science. 1999 Mar 19;283(5409):1908–11. [CrossRef]
- Ackermann H. Cerebellar contributions to speech production and speech perception: psycholinguistic and neurobiological perspectives. Trends Neurosci. 2008 Jun;31(6):265–72. [CrossRef]
- Ullman MT, Pierpont EI. Specific language impairment is not specific to language: The procedural deficit hypothesis. Cortex. 2005;41(3):399–433. [CrossRef]
- Stoodley CJ, Schmahmann JD. Evidence for topographic organization in the cerebellum of motor control versus cognitive and affective processing. Cortex. 2010 Aug;46(7):831–44. [CrossRef]
- Guenther FH. Cortical interactions underlying the production of speech sounds. Journal of Communication Disorders. 2006 Sep;39(5):350–65. [CrossRef]
- Tourville JA, Guenther FH. The DIVA model: A neural theory of speech acquisition and production. Lang Cogn Process. 2011 Jan 1;26(7):952–81. [CrossRef]
- Kuhl PK. Brain mechanisms in early language acquisition. Neuron. 2010 Sep 9;67(5):713–27. [CrossRef]
- Werker JF, Tees RC. Cross-language speech perception: Evidence for perceptual reorganization during the first year of life. Infant Behavior and Development. 1984 Jan 1;7(1):49–63. [CrossRef]
- Polikowsky HG, Shaw DM, Petty LE, Chen HH, Pruett DG, Linklater JP, et al. Population-based genetic effects for developmental stuttering. HGG Adv. 2022 Jan 13;3(1):100073. [CrossRef]
- Shaw DM, Polikowsky HP, Pruett DG, Chen HH, Petty LE, Viljoen KZ, et al. Phenome risk classification enables phenotypic imputation and gene discovery in developmental stuttering. The American Journal of Human Genetics. 2021 Dec;108(12):2271–83. [CrossRef]
- Neef NE, Chang SE. Knowns and unknowns about the neurobiology of stuttering. PLoS Biol. 2024 Feb;22(2):e3002492. [CrossRef]
- Morgan A, Fisher SE, Scheffer I, Hildebrand M. FOXP2-Related Speech and Language Disorder. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, et al., editors. GeneReviews(®). Seattle (WA): University of Washington, Seattle Copyright © 1993-2024, University of Washington, Seattle. GeneReviews is a registered trademark of the University of Washington, Seattle. All rights reserved.; 1993.
- Rappold G, Siper P, Kostic A, Braden R, Morgan A, Koene S, et al. FOXP1 Syndrome. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, et al., editors. GeneReviews(®). Seattle (WA): University of Washington, Seattle Copyright © 1993-2024, University of Washington, Seattle. GeneReviews is a registered trademark of the University of Washington, Seattle. All rights reserved.; 1993.
- Newbury DF, Gibson JL, Conti-Ramsden G, Pickles A, Durkin K, Toseeb U. Using Polygenic Profiles to Predict Variation in Language and Psychosocial Outcomes in Early and Middle Childhood. J Speech Lang Hear Res. 2019 Sep 20;62(9):3381–96. [CrossRef]
- Han TU, Root J, Reyes LD, Huchinson EB, Hoffmann JD, Lee WS, et al. Human GNPTAB stuttering mutations engineered into mice cause vocalization deficits and astrocyte pathology in the corpus callosum. Proc Natl Acad Sci U S A. 2019 Aug 27;116(35):17515–24. [CrossRef]
- Kazemi N, Estiar MA, Fazilaty H, Sakhinia E. Variants in GNPTAB, GNPTG and NAGPA genes are associated with stutterers. Gene. 2018 Mar 20;647:93–100. [CrossRef]
- Chen H, Wang G, Xia J, Zhou Y, Gao Y, Xu J, et al. Stuttering candidate genes DRD2 but not SLC6A3 is associated with developmental dyslexia in Chinese population. Behav Brain Funct. 2014 Sep 1;10(1):29. [CrossRef]
- Lan J, Song M, Pan C, Zhuang G, Wang Y, Ma W, et al. Association between dopaminergic genes (SLC6A3 and DRD2) and stuttering among Han Chinese. J Hum Genet. 2009 Aug;54(8):457–60. [CrossRef]
- Anthoni H, Sucheston LE, Lewis BA, Tapia-Páez I, Fan X, Zucchelli M, et al. The aromatase gene CYP19A1: several genetic and functional lines of evidence supporting a role in reading, speech and language. Behav Genet. 2012 Jul;42(4):509–27. [CrossRef]
- Mohammadi H, Joghataei MT, Rahimi Z, Faghihi F, Khazaie H, Farhangdoost H, et al. Sex steroid hormones and sex hormone binding globulin levels, CYP17 MSP AI (-34T:C) and CYP19 codon 39 (Trp:Arg) variants in children with developmental stuttering. Brain Lang. 2017 Dec;175:47–56. [CrossRef]
- Morgan AT, Scerri TS, Vogel AP, Reid CA, Quach M, Jackson VE, et al. Stuttering associated with a pathogenic variant in the chaperone protein cyclophilin 40. Brain. 2023 Dec 1;146(12):5086–97. [CrossRef]
- Sun Y, Gao Y, Zhou Y, Zhou Y, Zhang Y, Wang D, et al. IFNAR1 gene mutation may contribute to developmental stuttering in the Chinese population. Hereditas. 2021 Dec;158(1):46. [CrossRef]
- Rehman AU, Hamid M, Khan SA, Eisa M, Ullah W, Rehman ZU, et al. The Expansion of the Spectrum in Stuttering Disorders to a Novel ARMC Gene Family (ARMC3). Genes (Basel). 2022 Dec 6;13(12):2299. [CrossRef]
- Feldman HM. How Young Children Learn Language and Speech. Pediatr Rev. 2019 Aug;40(8):398–411. [CrossRef]
- Rey OA, Sánchez-Delgado P, Palmer MRS, De Anda MCO, Gallardo VP. Exploratory study on the prevalence of speech sound disorders in a group of Valencian School students belonging to 3rd grade of infant school and 1st grade of primary school. Psicología Educativa Revista de los Psicólogos de la Educación. 2022;28(2):195–207. [CrossRef]
- Dodd B. Differential Diagnosis of Pediatric Speech Sound Disorder. Current Developmental Disorders Reports. 2014 Sep 1;1(3):189–96. [CrossRef]
- Jiramongkolchai P, Kumar MS, Chinnadurai S, Wootten CT, Goudy SL. Prevalence of hearing loss in children with 22q11.2 deletion syndrome. Int J Pediatr Otorhinolaryngol. 2016 Aug;87:130–3. [CrossRef]
- Feldman HM, Messick C. Language and speech disorders. Developmental behavioral pediatrics. 2008;467–82. [CrossRef]
- Newbury DF, Monaco AP. Genetic advances in the study of speech and language disorders. Neuron. 2010 Oct 21;68(2):309–20. [CrossRef]
- Hayiou-Thomas ME, Carroll JM, Leavett R, Hulme C, Snowling MJ. When does speech sound disorder matter for literacy? The role of disordered speech errors, co-occurring language impairment and family risk of dyslexia. J Child Psychol Psychiatry. 2017 Feb;58(2):197–205. [CrossRef]
- Pauls LJ, Archibald LM. Executive Functions in Children With Specific Language Impairment: A Meta-Analysis. J Speech Lang Hear Res. 2016 Oct 1;59(5):1074–86. [CrossRef]
- Basilakos A, Fridriksson J. Types of motor speech impairments associated with neurologic diseases. Handb Clin Neurol. 2022;185:71–9. [CrossRef]
- Pernon M, Assal F, Kodrasi I, Laganaro M. Perceptual Classification of Motor Speech Disorders: The Role of Severity, Speech Task, and Listener’s Expertise. J Speech Lang Hear Res. 2022 Aug 17;65(8):2727–47. [CrossRef]
- Landin-Romero R, Liang CT, Monroe PA, Higashiyama Y, Leyton CE, Hodges JR, et al. Brain changes underlying progression of speech motor programming impairment. Brain Commun. 2021;3(3):fcab205. [CrossRef]
- Webb WG. 8 - Clinical Speech Syndromes of the Motor Systems. In: Webb WG, editor. Neurology for the Speech-Language Pathologist (Sixth Edition). Mosby; 2017. p. 160–80.
- Jacks A, Haley KL. Apraxia of Speech. In: The Handbook of Language and Speech Disorders. 2021. p. 368–90.
- Malmenholt A, Lohmander A, McAllister A. Childhood apraxia of speech: A survey of praxis and typical speech characteristics. Logoped Phoniatr Vocol. 2017 Jul;42(2):84–92. [CrossRef]
- Enderby P. Disorders of communication: dysarthria. Handb Clin Neurol. 2013;110:273–81. [CrossRef]
- Atalar MS, Oguz O, Genc G. Hypokinetic Dysarthria in Parkinson’s Disease: A Narrative Review. Sisli Etfal Hastan Tip Bul. 2023;57(2):163–70. [CrossRef]
- Mitchell C, Bowen A, Tyson S, Butterfint Z, Conroy P. Interventions for dysarthria due to stroke and other adult-acquired, non-progressive brain injury. Cochrane Database Syst Rev. 2017 Jan 25;1(1):Cd002088. [CrossRef]
- Neumann K, Euler HA, Bosshardt HG, Cook S, Sandrieser P, Sommer M. The Pathogenesis, Assessment and Treatment of Speech Fluency Disorders. Dtsch Arztebl Int. 2017 Jun 5;114(22–23):383–90. [CrossRef]
- Tichenor S, Yaruss JS. Repetitive Negative Thinking, Temperament, and Adverse Impact in Adults Who Stutter. Am J Speech Lang Pathol. 2020 Feb 7;29(1):201–15. [CrossRef]
- Türkili S, Türkili S, Aydın ZF. Mental well-being and related factors in individuals with stuttering. Heliyon. 2022 Sep;8(9):e10446. [CrossRef]
- Van Borsel J. Acquired stuttering: A note on terminology. Journal of Neurolinguistics. 2014 Jan 1;27(1):41–9. [CrossRef]
- Bóna J. Characteristics of pausing in normal, fast and cluttered speech. Clin Linguist Phon. 2016;30(11):888–98. [CrossRef]
- Krouse HJ, Reavis CCW, Stachler RJ, Francis DO, O’Connor S. Plain Language Summary: Hoarseness (Dysphonia). Otolaryngol Head Neck Surg. 2018 Mar;158(3):427–31. [CrossRef]
- Saniasiaya J, Kulasegarah J, Narayanan P. New-Onset Dysphonia: A Silent Manifestation of COVID-19. Ear Nose Throat J. 2023 Apr;102(4):Np201-np202. [CrossRef]
- Aggarwal A, Sharma DD, Kumar R, Sharma RC. Mutism as the presenting symptom: three case reports and selective review of literature. Indian J Psychol Med. 2010 Jan;32(1):61–4. [CrossRef]
- Mulligan C, Shipon-Blum E. Selective Mutism: Identification of Subtypes and Implications for Treatment. Journal of Education and Human Development. 2015 01;4. [CrossRef]
- Oerbeck B, Overgaard KR, Stein MB, Pripp AH, Kristensen H. Treatment of selective mutism: a 5-year follow-up study. Eur Child Adolesc Psychiatry. 2018 Aug;27(8):997–1009. [CrossRef]
- Gudrunardottir T, De Smet HJ, Bartha-Doering L, van Dun K, Verhoeven J, Paquier P, et al. Chapter 11 - Posterior Fossa Syndrome (PFS) and Cerebellar Mutism. In: Mariën P, Manto M, editors. The Linguistic Cerebellum. San Diego: Academic Press; 2016. p. 257–313. [CrossRef]
- Launay J, Grube M, Stewart L. Dysrhythmia: a specific congenital rhythm perception deficit. Front Psychol. 2014;5:18. [CrossRef]
- Morgan A, Ttofari Eecen K, Pezic A, Brommeyer K, Mei C, Eadie P, et al. Who to Refer for Speech Therapy at 4 Years of Age Versus Who to “Watch and Wait”? J Pediatr. 2017 Jun;185:200-204.e1. [CrossRef]
- Benítez-Burraco A, Lattanzi W, Murphy E. Language Impairments in ASD Resulting from a Failed Domestication of the Human Brain. Front Neurosci. 2016;10:373. [CrossRef]
- Ripamonti E, Frustaci M, Zonca G, Aggujaro S, Molteni F, Luzzatti C. Disentangling phonological and articulatory processing: A neuroanatomical study in aphasia. Neuropsychologia. 2018 Dec;121:175–85. [CrossRef]
- Angold A, Costello EJ, Erkanli A. Comorbidity. J Child Psychol Psychiatry. 1999 Jan;40(1):57–87.
- Albert U, Rosso G, Maina G, Bogetto F. Impact of anxiety disorder comorbidity on quality of life in euthymic bipolar disorder patients: differences between bipolar I and II subtypes. J Affect Disord. 2008 Jan;105(1–3):297–303. [CrossRef]
- Alm PA. Stuttering in relation to anxiety, temperament, and personality: review and analysis with focus on causality. J Fluency Disord. 2014 Jun;40:5–21. [CrossRef]
- Craig A, Blumgart E, Tran Y. The impact of stuttering on the quality of life in adults who stutter. J Fluency Disord. 2009 Jun;34(2):61–71. [CrossRef]
- Blood GW, Blood IM, Tellis G, Gabel R. Communication apprehension and self-perceived communication competence in adolescents who stutter. Journal of Fluency Disorders. 2001 Sep;26(3):161–78. [CrossRef]
- Messenger M, Onslow M, Packman A, Menzies R. Social anxiety in stuttering: measuring negative social expectancies. J Fluency Disord. 2004;29(3):201–12. [CrossRef]
- Blood GW, Blood IM. Long-term Consequences of Childhood Bullying in Adults who Stutter: Social Anxiety, Fear of Negative Evaluation, Self-esteem, and Satisfaction with Life. J Fluency Disord. 2016 Dec;50:72–84. [CrossRef]
- Cook S, Howell P. Bullying in Children and Teenagers Who Stutter and the Relation to Self-Esteem, Social Acceptance, and Anxiety. Perspect Fluen Fluen Disord. 2014 Dec;24(2):46–57. [CrossRef]
- Bernard R, Hofslundsengen H, Frazier Norbury C. Anxiety and Depression Symptoms in Children and Adolescents Who Stutter: A Systematic Review and Meta-Analysis. J Speech Lang Hear Res. 2022 Feb 9;65(2):624–44. [CrossRef]
- Tellis G. Multicultural Considerations in Assessing and Treating Hispanic Americans who Stutter. Perspect Fluen Fluen Disord. 2008 Nov;18(3):101–10. [CrossRef]
- Nwokah EE. The imbalance of stuttering behavior in bilingual speakers. Journal of Fluency Disorders. 1988 Oct;13(5):357–73. [CrossRef]
- Dale P. Factors related to dysfluent speech in bilingual Cuban-American adolescents. Journal of Fluency Disorders. 1977 Dec;2(4):311–3. [CrossRef]
- Tichenor SE, Herring C, Yaruss JS. Understanding the Speaker’s Experience of Stuttering Can Improve Stuttering Therapy. Topics in Language Disorders. 2022 Jan;42(1):57–75. [CrossRef]
- Yaruss JS. Dismissal Criteria for School-Age Children Who Stutter: When Is Enough Enough? One Opinion…. Perspect Fluen Fluen Disord. 2005 Apr;15(1):9–11. [CrossRef]
- Reitzes P. Response from the editor—Stuttering: Inspiring Stories and Professional Wisdom. Journal of Fluency Disorders. 2013 Jun;38(2):235. [CrossRef]
- Boyle MP. Assessment of Stigma Associated With Stuttering: Development and Evaluation of the Self-Stigma of Stuttering Scale (4S). J Speech Lang Hear Res. 2013 Oct;56(5):1517–29. [CrossRef]
- Boyle MP. Enacted stigma and felt stigma experienced by adults who stutter. Journal of Communication Disorders. 2018 May;73:50–61. [CrossRef]
- Blanton S. A survey of speech defects. Journal of Educational Psychology. 1916 Dec;7(10):581–92.
- Karniol R. Stuttering, language, and cognition: A review and a model of stuttering as suprasegmental sentence plan alignment (SPA). Psychological Bulletin. 1995;117(1):104–24. [CrossRef]
- Gollan TH, Montoya RI, Fennema-Notestine C, Morris SK. Bilingualism affects picture naming but not picture classification. Memory & Cognition. 2005 Oct;33(7):1220–34. [CrossRef]
- Sandoval TC, Gollan TH, Ferreira VS, Salmon DP. What causes the bilingual disadvantage in verbal fluency? The dual-task analogy. Bilingualism. 2010 Apr;13(2):231–52. [CrossRef]
- Pelham SD, Abrams L. Cognitive advantages and disadvantages in early and late bilinguals. Journal of Experimental Psychology: Learning, Memory, and Cognition. 2014;40(2):313–25. [CrossRef]
- Chaudhary C, Maruthy S, Guddattu V, Krishnan G. A systematic review on the role of language-related factors in the manifestation of stuttering in bilinguals. Journal of Fluency Disorders. 2021 Jun;68:105829. [CrossRef]
- Van Borsel J, Maes E, Foulon S. Stuttering and bilingualism. Journal of Fluency Disorders. 2001 Sep;26(3):179–205. [CrossRef]
- Howell P, Davis S, Williams R. The effects of bilingualism on stuttering during late childhood. Archives of Disease in Childhood. 2009 Jan 1;94(1):42–6. [CrossRef]
- Bialystok E, Poarch G, Luo L, Craik FIM. Effects of bilingualism and aging on executive function and working memory. Psychology and Aging. 2014 Sep;29(3):696–705. [CrossRef]
- Sullivan MD, Janus M, Moreno S, Astheimer L, Bialystok E. Early stage second-language learning improves executive control: Evidence from ERP. Brain and Language. 2014 Dec;139:84–98. [CrossRef]
- Bernstein Ratner N, Brundage SB. Advances in Understanding Stuttering as a Disorder of Language Encoding. Annu Rev Linguist. 2024 Jan 16;10(1):127–43. [CrossRef]
- Kornisch M. Bilinguals who stutter: A cognitive perspective. Journal of Fluency Disorders. 2021 Mar;67:105819. [CrossRef]
- Loe IM, Feldman HM. The Effect of Bilingual Exposure on Executive Function Skills in Preterm and Full-Term Preschoolers. J Dev Behav Pediatr. 2016 Sep;37(7):548–56. [CrossRef]
- Arizmendi GD, Alt M, Gray S, Hogan TP, Green S, Cowan N. Do Bilingual Children Have an Executive Function Advantage? Results From Inhibition, Shifting, and Updating Tasks. LSHSS. 2018 Jul 5;49(3):356–78. [CrossRef]
- Carias S, Ingram D. Language and disfluency: Four case studies on Spanish-English bilingual children. Journal of Multilingual Communication Disorders. 2006 Jan;4(2):149–57. [CrossRef]
- Kashyap P, Maruthy S. Stuttering frequency and severity in Kannada-English balanced bilingual adults. Clinical Linguistics & Phonetics. 2020 Mar 3;34(3):271–89. [CrossRef]
- Tsai C. Linguistic Know-How: The Limits of Intellectualism. Theoria. 2011 Mar;77(1):71–86.
- Brown SF. The Loci of Stutterings In The Speech Sequence. J Speech Disord. 1945 Sep;10(3):181–92. [CrossRef]
- 103. Howell P, Van Borsel J, editors. Multilingual Aspects of Fluency Disorders [Internet]. Multilingual Matters; 2011 [cited 2024 Nov 13]. Available from: https://www.degruyter.com/document/doi/10.21832/9781847693570/html.
- Ononiwu, CA.THE IMPACT OF SYLLABLE STRUCTURE COMPLEXITY ON STUTTERING FREQUENCY FOR BILINGUALS AND MULTILINGUALS WHO STUTTER.
- Jakielski KJ. The Index of Phonetic Complexity: At-a-Glance Scoring System, Terminology, Instructions, & Data Forms.
- Howell P, Au-Yeung J. Phonetic complexity and stuttering in Spanish. Clinical Linguistics & Phonetics. 2007 Jan;21(2):111–27. [CrossRef]
- Al-Tamimi F, Khamaiseh Z, Howell P. Phonetic complexity and stuttering in Arabic. Clinical Linguistics & Phonetics. 2013 Dec;27(12):874–87. [CrossRef]
- Essau CA, Olaya B, Ollendick TH. Classification of Anxiety Disorders in Children and Adolescents. In: Essau CA, Ollendick TH, editors. The Wiley-Blackwell Handbook of The Treatment of Childhood and Adolescent Anxiety [Internet]. 1st ed. Wiley; 2013 [cited 2024 Nov 13]. p. 1–21. Available from: https://onlinelibrary.wiley.com/doi/10.1002/9781118315088.ch1.
- Smith KA, Iverach L, O’Brian S, Kefalianos E, Reilly S. Anxiety of children and adolescents who stutter: a review. J Fluency Disord. 2014 Jun;40:22–34. [CrossRef]
- McWilliams LA, Cox BJ, Enns MW. Use of the Coping Inventory for Stressful Situations in a clinically depressed sample: factor structure, personality correlates, and prediction of distress. J Clin Psychol. 2003 Apr;59(4):423–37. [CrossRef]
- Ingham RJ. Stuttering and behavior therapy. San Diego, Calif: College-Hill Pr; 1984. 480 p.
- Menzies RG, Onslow M, Packman A. Anxiety and Stuttering: Exploring a Complex Relationship. Am J Speech Lang Pathol. 1999 Feb;8(1):3–10. [CrossRef]
- Craig A, Hancock K, Tran Y, Craig M. Anxiety levels in people who stutter: a randomized population study. J Speech Lang Hear Res. 2003 Oct;46(5):1197–206. [CrossRef]
- De Nil LF, Brutten GJ. Speech-associated attitudes of stuttering and nonstuttering children. J Speech Hear Res. 1991 Feb;34(1):60–6. [CrossRef]
- Blood GW, Blood IM, Maloney K, Meyer C, Qualls CD. Anxiety levels in adolescents who stutter. J Commun Disord. 2007;40(6):452–69. [CrossRef]
- Craig A, Tran Y. Trait and social anxiety in adults with chronic stuttering: conclusions following meta-analysis. J Fluency Disord. 2014 Jun;40:35–43. [CrossRef]
- Iverach L, O’Brian S, Jones M, Block S, Lincoln M, Harrison E, et al. Prevalence of anxiety disorders among adults seeking speech therapy for stuttering. J Anxiety Disord. 2009 Oct;23(7):928–34. [CrossRef]
- Iverach L, Rapee RM. Social anxiety disorder and stuttering: current status and future directions. J Fluency Disord. 2014 Jun;40:69–82. [CrossRef]
- Bloodstein O. Interpersonal dynamics and the treatment of the stutterer. Journal of Communication Disorders. 1967 May;1(1):58–65.
- Blomgren M, Roy N, Callister T, Merrill RM. Intensive stuttering modification therapy: a multidimensional assessment of treatment outcomes. J Speech Lang Hear Res. 2005 Jun;48(3):509–23. [CrossRef]
- Menzies RG, O’Brian S, Onslow M, Packman A, St Clare T, Block S. An experimental clinical trial of a cognitive-behavior therapy package for chronic stuttering. J Speech Lang Hear Res. 2008 Dec;51(6):1451–64. [CrossRef]
- Craig A. An investigation into the relationship between anxiety and stuttering. J Speech Hear Disord. 1990 May;55(2):290–4. [CrossRef]
- Ingham RJ, Andrews G. The relation between anxiety reduction and treatment. Journal of Communication Disorders. 1971 Dec;4(4):289–301. [CrossRef]
- Briley PM, Ellis C. The Coexistence of Disabling Conditions in Children Who Stutter: Evidence From the National Health Interview Survey. J Speech Lang Hear Res. 2018 Dec 10;61(12):2895–905. [CrossRef]
- Doruk A, Türkbay T, Yelbo Z, Sütçigil L, Özflahin A. Autonomic Nervous System Imbalance in Young Adults with Developmental Stuttering. 2008;18(4).
- Bray MA, Kehle TJ, Lawless KA, Theodore LA. The relationship of self-efficacy and depression to stuttering. Am J Speech Lang Pathol. 2003 Nov;12(4):425–31. [CrossRef]
- Rothbart MK, Ahadi SA, Evans DE. Temperament and personality: origins and outcomes. J Pers Soc Psychol. 2000 Jan;78(1):122–35. [CrossRef]
- Cloninger CR. Temperament and personality. Curr Opin Neurobiol. 1994 Apr;4(2):266–73. [CrossRef]
- Walden TA, Frankel CB, Buhr AP, Johnson KN, Conture EG, Karrass JM. Dual diathesis-stressor model of emotional and linguistic contributions to developmental stuttering. J Abnorm Child Psychol. 2012 May;40(4):633–44. [CrossRef]
- Côté SM, Boivin M, Liu X, Nagin DS, Zoccolillo M, Tremblay RE. Depression and anxiety symptoms: onset, developmental course and risk factors during early childhood. J Child Psychol Psychiatry. 2009 Oct;50(10):1201–8. [CrossRef]
- Conture EG, Walden TA. DUAL DIATHESIS-STRESSOR MODEL OF STUTTERING.
- Rocha MS, Yaruss JS, Rato JR. Temperament, Executive Functioning, and Anxiety in School-Age Children Who Stutter. Front Psychol. 2019;10:2244. [CrossRef]
- Harris KS. The nature of stuttering (2nd Ed.). Charles Van Riper. Englwewood Cliffs, N.J.: Prentice-Hall, 1982. Pp. x + 468. Applied Psycholinguistics. 1983 Jun;4(2):177–9.
- Jones R, Choi D, Conture E, Walden T. Temperament, emotion, and childhood stuttering. Semin Speech Lang. 2014 May;35(2):114–31. [CrossRef]
- Eggers K, De Nil LF, Van den Bergh BRH. Temperament dimensions in stuttering and typically developing children. J Fluency Disord. 2010 Dec;35(4):355–72. [CrossRef]
- Kefalianos E, Onslow M, Ukoumunne OC, Block S, Reilly S. Temperament and Early Stuttering Development: Cross-Sectional Findings From a Community Cohort. J Speech Lang Hear Res. 2017 Apr 14;60(4):772–84. [CrossRef]
- Kraft SJ, Lowther E, Beilby J. The Role of Effortful Control in Stuttering Severity in Children: Replication Study. Am J Speech Lang Pathol. 2019 Feb 21;28(1):14–28. [CrossRef]
- Jo Kraft S, Ambrose N, Chon H. Temperament and environmental contributions to stuttering severity in children: the role of effortful control. Semin Speech Lang. 2014 May;35(2):80–94. [CrossRef]
- Tumanova V, Zebrowski PM, Throneburg RN, Kulak Kayikci ME. Articulation rate and its relationship to disfluency type, duration, and temperament in preschool children who stutter. Journal of Communication Disorders. 2011 Jan;44(1):116–29. [CrossRef]
- Delpeche S, Millard S, Kelman E. The role of temperament in stuttering frequency and impact in children under 7. Journal of Communication Disorders. 2022 May;97:106201. [CrossRef]
- Alderson RM, Rapport MD, Sarver DE, Kofler MJ. ADHD and Behavioral Inhibition: A Re-examination of the Stop-signal Task. J Abnorm Child Psychol. 2008 Oct;36(7):989–98. [CrossRef]
- Alm PA, Risberg J. Stuttering in adults: the acoustic startle response, temperamental traits, and biological factors. J Commun Disord. 2007;40(1):1–41. [CrossRef]
- Bental B, Tirosh E. The relationship between attention, executive functions and reading domain abilities in attention deficit hyperactivity disorder and reading disorder: a comparative study. J Child Psychol Psychiatry. 2007 May;48(5):455–63. [CrossRef]
- Chhabildas N, Pennington BF, Willcutt EG. A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. J Abnorm Child Psychol. 2001 Dec;29(6):529–40. [CrossRef]
- Donaher J, Richels C. Traits of attention deficit/hyperactivity disorder in school-age children who stutter. J Fluency Disord. 2012 Dec;37(4):242–52. [CrossRef]
- Druker K, Hennessey N, Mazzucchelli T, Beilby J. Elevated attention deficit hyperactivity disorder symptoms in children who stutter. J Fluency Disord. 2019 Mar;59:80–90. [CrossRef]
- Engelhardt PE, Corley M, Nigg JT, Ferreira F. The role of inhibition in the production of disfluencies. Mem Cognit. 2010 Jul;38(5):617–28. [CrossRef]
- Healey EC, Reid R. ADHD and stuttering: a tutorial. J Fluency Disord. 2003;28(2):79–92; quiz 93. [CrossRef]
- Lee H, Lee H, Baik B, Kim K, Kim R. Failure mode and effects analysis drastically reduced potential risks in clinical trial conduct. Drug Design, Development and Therapy. 2017;11:3035–43. [CrossRef]
- Anderson JD, Pellowski MW, Conture EG, Kelly EM. Temperamental characteristics of young children who stutter. J Speech Lang Hear Res. 2003 Oct;46(5):1221–33. [CrossRef]
- Karrass J, Walden TA, Conture EG, Graham CG, Arnold HS, Hartfield KN, et al. Relation of emotional reactivity and regulation to childhood stuttering. J Commun Disord. 2006;39(6):402–23. [CrossRef]
- Martel MM, Nigg JT. Child ADHD and personality/temperament traits of reactive and effortful control, resiliency, and emotionality. J Child Psychol Psychiatry. 2006 Nov;47(11):1175–83. [CrossRef]
- Walcott CM, Landau S. The relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol. 2004 Dec;33(4):772–82. [CrossRef]
- Eggers K, De Nil LF, Van den Bergh BRH. Inhibitory control in childhood stuttering. J Fluency Disord. 2013 Mar;38(1):1–13. [CrossRef]
- Schwenk KA, Conture EG, Walden TA. Reaction to background stimulation of preschool children who do and do not stutter. J Commun Disord. 2007;40(2):129–41. [CrossRef]
- Ambrose NG, Cox NJ, Yairi E. The genetic basis of persistence and recovery in stuttering. J Speech Lang Hear Res. 1997 Jun;40(3):567–80. [CrossRef]
- Jacquemot C, Scott SK. What is the relationship between phonological short-term memory and speech processing? Trends in Cognitive Sciences. 2006 Nov;10(11):480–6. [CrossRef]
- Marchetta NDJ, Hurks PPM, Krabbendam L, Jolles J. Interference control, working memory, concept shifting, and verbal fluency in adults with attention-deficit/hyperactivity disorder (ADHD). Neuropsychology. 2008 Jan;22(1):74–84. [CrossRef]
- Martinussen R, Hayden J, Hogg-Johnson S, Tannock R. A meta-analysis of working memory impairments in children with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2005 Apr;44(4):377–84. [CrossRef]
- Postma A, Kolk H. The covert repair hypothesis: prearticulatory repair processes in normal and stuttered disfluencies. J Speech Hear Res. 1993 Jun;36(3):472–87.
- Kazazi F. Assessing Executive Function Impairments and Comorbidity between ADHD and Stuttering.
- Borsboom D, Cramer AOJ. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9:91–121. [CrossRef]
- Cramer AOJ, Waldorp LJ, van der Maas HLJ, Borsboom D. Comorbidity: a network perspective. Behav Brain Sci. 2010 Jun;33(2–3):137–50; discussion 150-193. [CrossRef]
- Epskamp S, Rhemtulla M, Borsboom D. Generalized Network Psychometrics: Combining Network and Latent Variable Models. Psychometrika. 2017 Dec;82(4):904–27. [CrossRef]
- Borsboom D, Deserno MK, Rhemtulla M, Epskamp S, Fried EI, McNally RJ, et al. Network analysis of multivariate data in psychological science. Nat Rev Methods Primers. 2021 Aug 19;1(1):58. [CrossRef]
- Eggers K, Millard SK, Kelman E. Temperament, anxiety, and depression in school-age children who stutter. J Commun Disord. 2022;97:106218. [CrossRef]
- Kohmäscher A, Primaßin A, Heiler S, Avelar PDC, Franken MC, Heim S. Effectiveness of Stuttering Modification Treatment in School-Age Children Who Stutter: A Randomized Clinical Trial. J Speech Lang Hear Res. 2023 Nov 9;66(11):4191–205. [CrossRef]
Figure 1.
Key brain regions responsible for speech and language processing, including areas involved in speech production, language comprehension and sound processing. (Figure created using BioRender).
Figure 1.
Key brain regions responsible for speech and language processing, including areas involved in speech production, language comprehension and sound processing. (Figure created using BioRender).
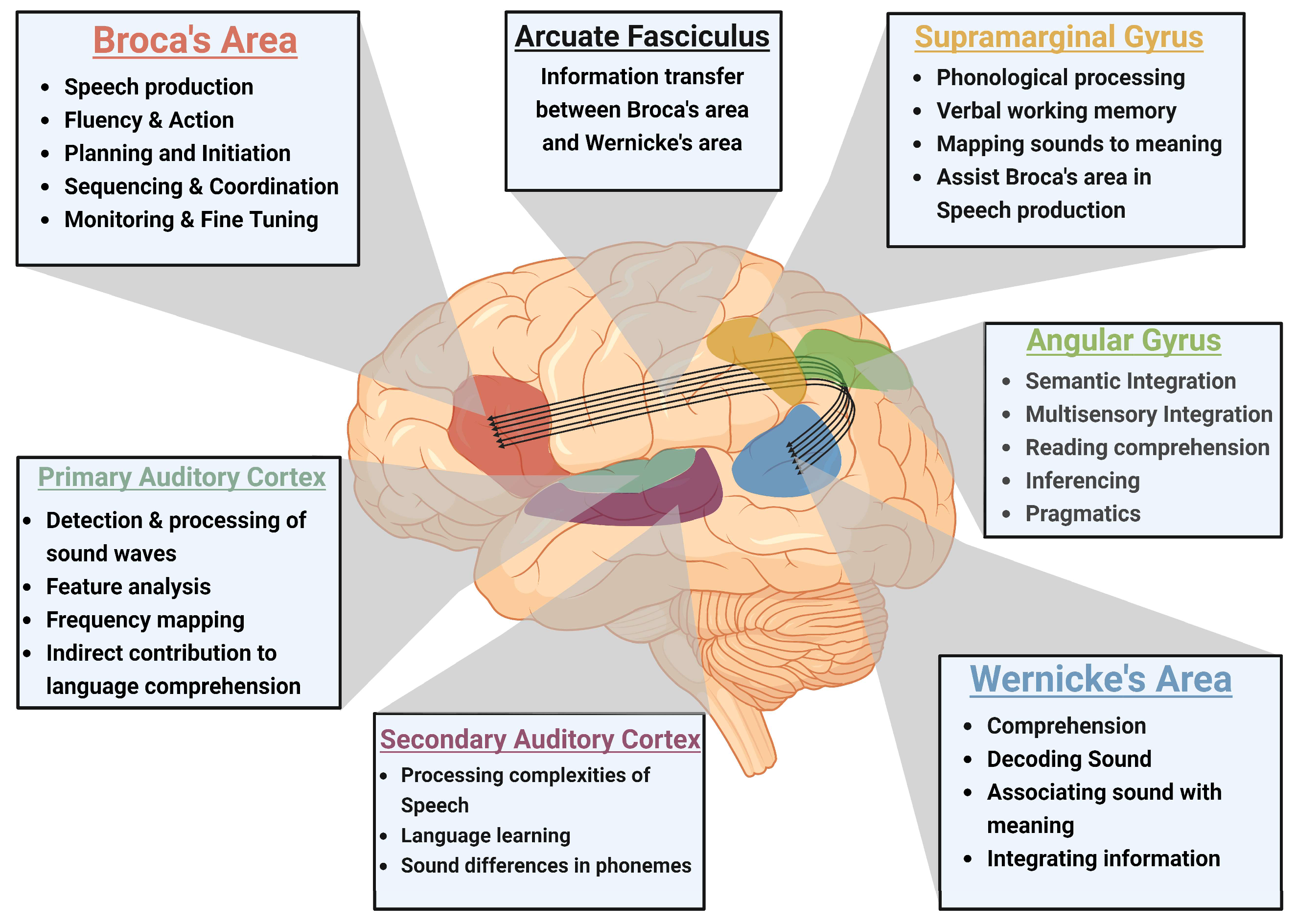
Figure 2.
The image shows a network graph depicting gene interactions related to various speech and language disorders. Each node represents a gene, and the edges (lines) between them indicate known or predicted interactions. The legend in the bottom-right corner explains the color-coding of the nodes based on the type of disorder they are associated with: Red: Speech Disorder, Yellow: Specific Developmental Disorder, Green: Speech-Language Disorder-1, Blue: Stuttering, Pink: Specific Language Impairment. Multiple connections between key genes like FOXP2, CNTNAP2, DRD2, and NAGPA suggest they may play central roles in the network of genetic interactions related to the speech disorder in different ethnicities. Although the legend does not specify it, the thickness and color of the edges may indicate the strength or type of relationship between genes.
Figure 2.
The image shows a network graph depicting gene interactions related to various speech and language disorders. Each node represents a gene, and the edges (lines) between them indicate known or predicted interactions. The legend in the bottom-right corner explains the color-coding of the nodes based on the type of disorder they are associated with: Red: Speech Disorder, Yellow: Specific Developmental Disorder, Green: Speech-Language Disorder-1, Blue: Stuttering, Pink: Specific Language Impairment. Multiple connections between key genes like FOXP2, CNTNAP2, DRD2, and NAGPA suggest they may play central roles in the network of genetic interactions related to the speech disorder in different ethnicities. Although the legend does not specify it, the thickness and color of the edges may indicate the strength or type of relationship between genes.
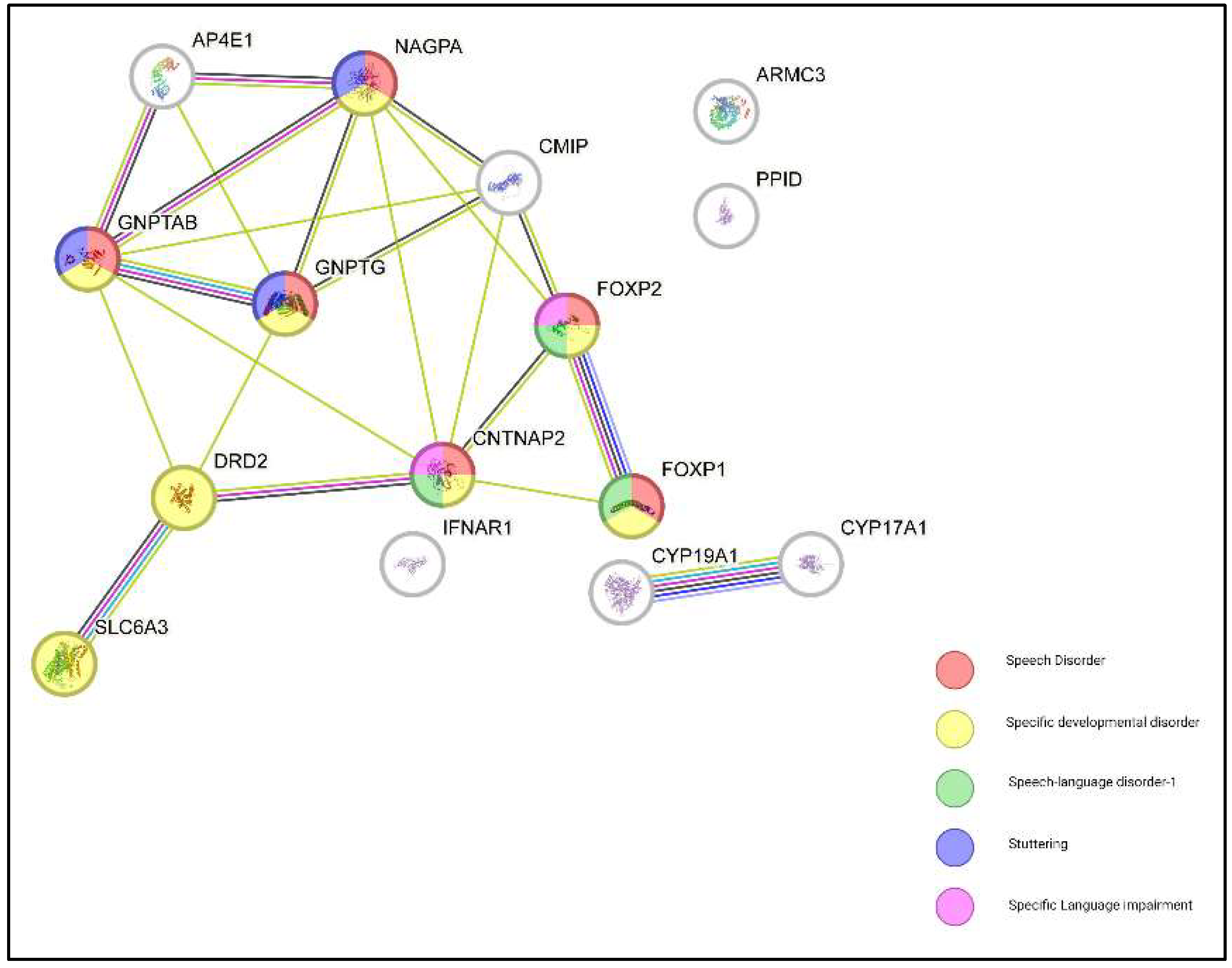
Figure 3.
The figure provides a hierarchical representation of how communication disorders are classified based on their specific characteristics, highlighting the distinction between language and speech disorders. (Figure created using BioRender).
Figure 3.
The figure provides a hierarchical representation of how communication disorders are classified based on their specific characteristics, highlighting the distinction between language and speech disorders. (Figure created using BioRender).
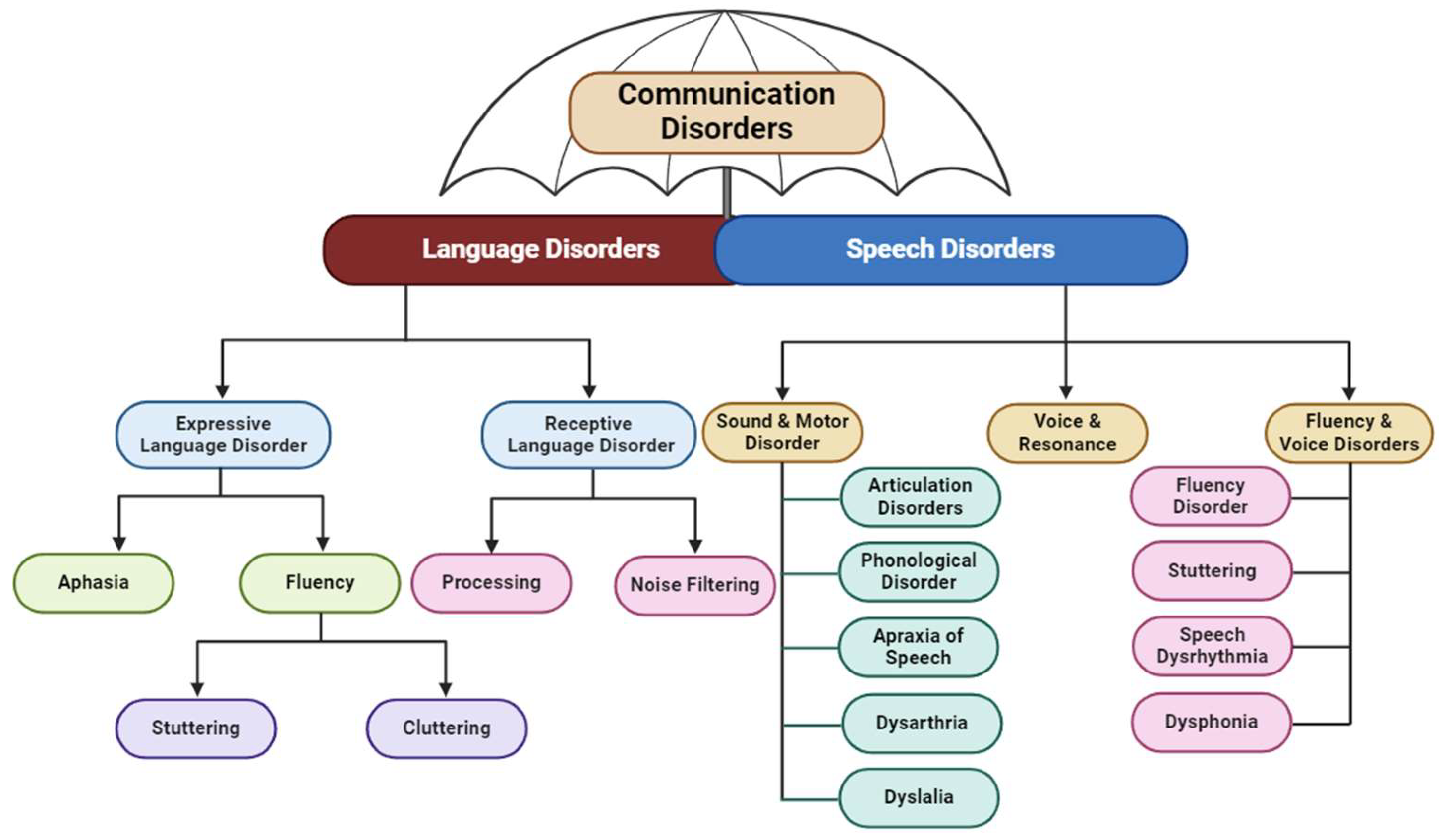

Table 1.
The table summarizes the roles of key genes involved in speech and language development and their contributions to specific disorders.
Table 1.
The table summarizes the roles of key genes involved in speech and language development and their contributions to specific disorders.
| Gene | Associated Disorder/Function | Chromosomal Location | Role in Speech and Language | Refs |
|---|---|---|---|---|
| FOXP2 | Verbal Dyspraxia | Chromosome 7q | Regulates genes in brain regions for motor control, impacting speech and language. Disruption leads to speech deficits. Acts as a transcription factor, reducing neural gene expression. | [24] |
| FOXP1 | Speech and Language Mechanisms | Chromosome 3 | Involved in neural circuitry for speech and language development. Disruption causes speech delays and developmental issues. | [25] |
| CNTNAP2 | Complex Language Impairment | Chromosome 7q35-q36.1 | Encodes a neurexin protein for synapse function. Mutations linked to SLI and SSD. Works with FOXP2 in gene-expression networks. | [26] |
| GNPTAB | Stuttering | Various chromosomes (2,3,5,7,9) | Involved in the lysosomal enzyme pathway. Mutations linked to stuttering. | [27] |
| GNPTG | Stuttering | Chromosome 7 | Similar to GNPTAB, involved in lysosomal enzyme pathway. Mutations linked to stuttering. | [27] |
| NAGPA | Stuttering | Chromosome 16p13.3 | Involved in lysosomal enzyme targeting. Mutations contribute to stuttering. | [28] |
| CMIP | Specific Language Impairment (SLI) and Autism Spectrum Disorder (ASD) | Chromosome 16q23.2 | Regulates phonological memory, critical for language acquisition. Linked to SLI and ASD. | [26] |
| TCF4, STOX1A | Combinatorial Gene-Expression Network in Speech | Chromosome 18q21.2, Chromosome 10q22.1 | Involved in gene networks with FOXP2 and CNTNAP2 for speech and language development. | [1,26] |
| DRD2 | Stuttering | Chromosome 11q23.2 | Encodes dopamine receptor D2, linked to susceptibility to stuttering. | [29] |
| SLC6A3 | Stuttering | Chromosome 5p15.33 | Encodes dopamine transporter (DAT); mutations affect speech and language, linked to stuttering. | [30] |
| CYP19A1 | Neurodevelopmental Disorders | Chromosome 15q21.1 | Involved in estrogen synthesis, potentially linked to neurodevelopmental speech disorders. | [31] |
| CYP17A1 | Neurodevelopmental Processes | Chromosome 10q24.32 | Influences steroid hormone biosynthesis; role in speech disorders unclear. | [32] |
| PPID | Persistent Stuttering | Chromosome 4q33 | Involved in protein folding; mutations linked to stuttering by affecting brain development. | [33] |
| AP4E1 | Neuroanatomical Anomalies | Chromosome 15q21.2 | Mutations associated with brain anomalies in people who stutter. | [22] |
| IFNAR1 | Developmental Stuttering | Chromosome 21q22.11 | Mutations linked to stuttering in certain populations. | [34] |
| ARMC3 | Persistent Stuttering | Chromosome 10p15.3 | Associated with non-syndromic persistent stuttering in specific populations. | [35] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



