
Submitted:
27 November 2024
Posted:
27 November 2024
You are already at the latest version
Abstract
Senear-Usher syndrome or pemphigus erythematosus (PE) is a rare autoimmune disorder characterized by the coexistence of features from both lupus erythematosus (LE) and pemphigus foliaceus (PF). We describe a 41-year-old patient initially diagnosed with systemic lupus erythematosus (SLE), who after a few years developed new skin lesions: erythematous and erosive eruptions partially covered by crusts on the trunk and flaccid blisters on the extremities. Additional testing, revealing autoantibodies against the intercellular cement substance of the epidermis and direct immunofluorescence (DIF) examination allowed a diagnosis of pemphigus vulgaris coexisting with SLE. Despite temporary improvement, the patient experienced relapses. Further, DIF study revealed granular deposits of IgG in the intercellular spaces of the epidermis and granular deposits of the complement (C3) along the basement membrane. It led to suspicion of Senear-Usher syndrome in this patient. This case report delves into the diagnostic challenges posed by the patient's overlapping symptoms and immunological findings, suggesting a rare manifestation of Senar-Usher syndrome or a combination of SLE and pemphigus vulgaris. The case highlights the complexity of chronic inflammatory skin diseases and the need for tailored treatment approaches in such cases. We performed a descriptive literature review of the case reports of PE published in the last 24 years and prepared a summary of the characteristics emphasizing the importance of proper recognition, clinical features, and treatment of this rare disorder.
Keywords:
pemphigus erythematosus
; Senear-Usher syndrome
; pemphigus vulgaris
; SLE
1. Introduction
Senar-Usher syndrome also known as pemphigus erythematosus (PE) is a challenging and rare clinical condition. This dermatosis is the co-occurrence of features of both lupus erythematosus and pemphigus foliaceus [1]. The clinical features of this disease are seborrheic lesions located on the skin of the nose, nasolabial folds and the cheeks with “butterfly” distribution [2]. The overlap of autoimmune pathologies in PE underscores the diagnostic and therapeutic challenges associated with managing chronic inflammatory skin diseases.
2. Case Report
In 2006, a 41-year-old, female patient was referred to the Department of Dermatology and Venerology. Numerous, scattered erythematous and scarring lesions with follicular hyperkeratosis were present on the skin of the face and head, upper back, and lateral surface of the arms. The skin lesions were not accompanied by itching or pain. Based on the clinical picture and histopathological examination, a disseminated form of discoid cutaneous lupus erythematosus (DDLE) was diagnosed. Moreover, the patient reported hypertension arterial and gastroesophageal reflux in the medical interview. The family history of dermatological and autoimmune diseases was negative. The patient was treated with oral chloroquine and ointments with topical glucocorticosteroids. The patient tolerated the treatment well and achieved clinical remission of the disease. For the next 10 years, the patient was under the care of another medical facility.
In 2016, due to the exacerbation of skin lesions in the course of DDLE, diagnostics were expended: antinuclear antibodies (ANA) titer was determined, obtaining a result of 1:640, negative in the specification (Table 1). The serum complement level of C3 was normal at 1.07 (norm: 0.75-1.4 g/L) and slightly decreased level of C4 at 0.08 (norm: 0.09-0.36 g/L), Coombs test was positive. The patient met the criteria for systemic lupus erythematosus (SLE) according to The Systemic Lupus International Collaborating Clinics (SLICC) [4]. Due to the predominance of joint problems, methotrexate was added to the treatment at a dose of 12.5 mg per week. The patient continued therapy for 6 months. Because of ineffectiveness, the drug was no longer recommended and the patient was treated with arechin (in a dose of 500 mg per day) for the next few years.
In February 2021, a patient reported an exacerbation of skin lesions, which were associated with COVID-19 infection. The patient was treated on an outpatient basis at that time and methylprednisolone at a dose of 32 mg per day was added to the treatment with subsequent dose reduction to 24 mg per day. A slight improvement in skin lesions was observed. However, the patient developed new skin lesions, with a different clinical picture in July 2021 (Figure 1). Erythematous and erosive eruptions appeared, partially covered with scabs, yellowish crusts disseminated on the trunk and flaccid blisters with serous content. Erosions of the mucosal lip, whitening of the cheek mucosa, as well as scarring in the places of previous skin lesions, were visible. The patient reported pain in the area of oral erosions. ANA test with specification was performed again (ANA 1:320, Scl 70(+)) (Table 1).
Diagnostic tests were extended to tests for autoimmune bullous diseases. Pemphigus/pemphigoid antibodies were determined, obtaining the positive result of anti-desmoglein 1 (anti-DSG1) antibodies 1:40, anti-desmoglein 3 (anti-DSG3) antibodies 1:20 (BIOCHIP , Euroimmun, Germany), antibodies on monkey esophagus substrate 1:20 (IIF, Euroimmun, Germany) (Table 1). Direct immunofluorescence (DIF) test confirmed the presence of deposits of IgG (++) and IgA (++) in the intercellular spaces of the epidermis. In histopathological examination of skin biopsy acantholytic epidermis with preserved basal and spinous layers with lymphocyte infiltration in the stroma (Table 1) was described. Based on the clinical picture and the results of additional tests, a diagnosis of pemphigus vulgaris coexisting with SLE was made.
Treatment with prednisone at a dose of 80 mg per day and azathioprine at 100 mg per day was started. The patient achieved clinical response. New skin eruptions had not been observed for 5 months. Significant clinical improvement allowed a gradual reduction of the dose of prednisone to 5 mg (the dose of azathioprine was maintained). Despite of improvement in the clinical picture in December 2021 there was described an increase in anti DSG-3 titer from 1:40 to 1:80 (Table 1). The patient remained under the care of an outpatient clinic.
In October 2022 again a follow-up antibody test was performed, obtaining a negative result (Table 1). The patient continued treatment until April 2023 with satisfactory clinical effect. Then due to the presence of erosions and erythematous lesions on the scalp (Figure 2), topical treatment was intensified, whereas azathioprine (100 mg per day) and prednisone (5mg per day) were maintained at the previous doses, achieving temporary improvement. The patient reported that she was under strict photoprotection all the time.
Another exacerbation of the disease occurred in October 2023. A follow-up ANA, pemphigus/pemphigoid antibodies, and skin samples for DIF and lupus band test (LBT) examination were taken. DIF showed granular deposits of IgG (+) in the intercellular spaces of the epidermis and granular C3 (+) deposits along the dermo-epidermal junction, the LBT was negative (Table 1, Figure 3). The results of these tests led to the suspicion of pemphigus erythematosus. Additionally, HCV antibodies were present, whereas HCV RNA was negative. Anti-HBc antibodies were positive and HBs antigen was negative. The Quantiferon test was negative. A diagnostic imaging was also carried out. A chest X-ray was performed, showing no abnormalities, while an abdominal ultrasound revealed a fatty liver and pancreas, a 9-mm cyst in the left kidney, and atheromatic changes in the aorta.
We did not decide to increase the dose of oral glucocorticosteroids due to blood pressure spikes, the development of steroid-induced diabetes, and poor tolerance of steroids in the past (hot flashes). The patient was referred to the Infectious Diseases Department, where the acute phase of hepatitis infection was excluded and entecavir was started due to chronic hepatitis B. In March 2024, due to insufficient clinical response to the previously used immunosuppressive treatment and chronic side effects of steroid therapy, the patient was qualified for treatment with rituximab (1 g on day one and 1 g on day 15). The patient tolerated the treatment well and remains in clinical remission till the article is published.
3. Discussion
Although the described patient did not present typical seborrheic eruptions, skin lesions may appear as circumscribed erythematous erosions, partially covered with scabs [5]. Mucosal involvement is rare. [6] However, in this patient, it was present as well as erythematous erosions covered with crusts were observed. Typical predilection sites are the trunk, face, scalp, and less frequently limbs [2,7]. Two types of lesions may occur on the trunk: small and flaccid blisters and skin lesions covered with scales or scabs with visible seborrheic keratosis, which disappear with hyperpigmentation.
The predominance of pemphigus erythematosus is observed in women. The progression of the disease is usually slow, which is what we observed in our female patient [8]. Immunological phenomena in patients with pemphigus erythematosus include features typical of pemphigus foliaceus: the presence of anti-DSG1 antibodies and the erosions on the mucous membranes. [9,10]. A typical histopathological picture for PE was observed in this case—the pathologist described the presence of acantholytic epidermis and lymphocyte infiltration in the stroma.
The second DIF examination of the described patient showed granular deposits of IgG in the intercellular spaces of the epidermis and granular deposits of the C3 along the basement membrane. Jabłonska and Chorzelski reported that 83% of patients with pemphigus erythematosus (5 of 6 patients) had IgG deposits along the basement membrane in the skin samples from erythematous lesions from the face [11]. The LBT in our patient was negative. However, the LBT is positive in 70-80% of sun-exposed non-lesional skin specimens obtained from patients with SLE and approximately in 55% of SLE cases when sun-protected, non-lesional skin is analyzed [12]. Our patient used strict photoprotection, which may have influenced the LBT result.
In the literature many authors reported positive ANA antibodies in patients with PE [3,13]. The described patient had positive ANA antibodies all the time (ranging from 1:80 to 1:640). In the literature titer of these antibodies ranged from 1:10 to 1:320, most often with a homogeneous type of fluorescence [14].
In our patient, both types of antibodies (against DSG1 and DSG3) were initially detectable. The experiment conducted by P’erez-P´erez et al. also showed the presence of antibodies directed against DSG1 and DSG3 in 8 out of 10 patients with PE. Researchers proposed that this phenomenon may result from the spread of the epitope, but the role of this phenomenon in the formation of blisters is not yet fully explained [15].
In the literature, a similar case of Senear-Usher syndrome was described by Chandan et al. who described a patient with significant involvement of the scalp and no characteristic skin lesions in the seborrheic area or “butterfly” erythema. The patient had antibodies against DSG1 and DSG3 and the DIF examination revealed IgG and C3 deposition both intercellularly and at the dermo-epidermal junction [16]. Henington et al. [17] addressed a report of 8 patients with pemphigus erythematosus, 2 of which developed acute pemphigus vulgaris [17]. This suggests that Senear-Usher syndrome may appear in the spectrum of pemphigus vulgaris, as it was in our patient.
Using the PubMed database, we performed a descriptive literature review of the case reports and case series applying keywords: ‘Senear Usher syndrome’, ‘Senear Usher’ and ‘pemphigus erythematosus’ published between the last 24 years (2000-2024). After the removed irrelevant articles based on the titles, abstracts, and full-text articles and papers that did not report a case of PE, 18 articles were included in this review. 2 of the papers were a case series without specific clinical information of each patient and were also excluded of the review. Therefore, a total of 16 articles describing 23 patients were included in the literature review, and clinical, histopathological, and immunological information are summarised in Table 2.
The mean age of the patients was 47,39 years with a range of 7 to 80 years. 14 of the cases (60,9%) were females and 9 (39,1%) were men. The most common locations of skin lesions were: the face and trunk followed by the extremities and scalp. Face involvement was observed in 20 (87%) patients and trunk in 16 (70%) patients. Mucosa involvement was seen only in 3 patients (13%).
Characteristic skin lesions were usually scaly, crusty, dusky erythematous plaques. Flaccid vesiculobullous, widespread erosions, and scattered erosive erythema were present. In one patient keratotic hyperpigmented papules were described. Histopathologic examination revealed acantholysis in the epidermis and inflammatory infiltrate in the dermis consisting of neutrophils and eosinophils. In one patient hyperkeratosis was seen. The intraepithelial blister was described in 6 patients, whereas the subcorneal blister in 6 patients.
DIF examination the most common revealed IgG and C3 deposition (15 of 23 patients, 65,2%) in the intercellular spaces of the epidermis. Fibrin deposits were additionally present in one patient similarly to IgA deposition which was also noted in one patient. Along dermo-epidermal junction (DEJ), IgG and C3 depositions were also the most commonly reported. However, fibrin, IgM, and IgA were also noted. ANA titer was checked in 15 patients, and in 7 of them (46,7%) was positive. Autoantibodies against DSG-1 were checked in 14 patients and were elevated in all of them (100%), whereas anti-DSG1 together with anti-DSG3 was present only in 1 patient.
We have also performed a literature review of the case reports describing the coexistence of pemphigus vulgaris and lupus erythematosus applying keywords ‘pemphigus vulgaris’ and ‘lupus erythematosus’. Only 4 cases describing the co-occurrence of these two diseases have been published in the last 24 years (2000-2024). The data are summarized in Table 3.
One case report described the coexistence of DLE with pemphigus vulgaris and the other 3 described co-occurrence of SLE with pemphigus vulgaris. The mean age of the patients was 40,5 years with a range of 36 to 46 years. 3 of 4 cases (75%) were females and 1 (25%) was a man. The involvement of oral mucosa was the main character feature. However, the skin lesions did not exhibit the same pattern of appearance. In the histopathological examination, typical intraepidermal blister and acantholysis were seen and in DIF examination only IgG or IgG with C3 deposition in the intercellular spaces of the epidermis. In one DIF the deposition along the DEJ was present, which is representative of SLE. ANA was present in 100% of patients and only 1 of 4 patients was checked for the anti-DSG1 and anti-DSG3 antibodies and had the latter. Some authors tried to differentiate these cases from pemphigus erythematosus and the main differentiating features are primarily facial eruptions and bullous lesions on the chest, upper back, intertriginous areas, and generally minimal clinical signs of lupus erythematosus in cases of pemphigus erythematosus [18].
3. Etiopathogenesis
The prevalence of this disease ranges from 0.5 to 3.2 cases per 100,000 people in the general population. The mode of genetic inheritance remains unclear. It was first described by E. Senear, an American dermatologist, and B. Usher, a Canadian dermatologist. The frequency of the disease is higher among individuals with the HLA A10, DRW6, and A26 alleles [36].The exact etiopathogenesis of the PE remains unclear. Several external factors can trigger PE in individuals who are genetically predisposed. These factors include drugs, viral infections, and exposure to physical agents such as heat, and ultraviolet radiation, as well as surgical and cosmetic procedures [20]. In our literature review, we find two cases of PE associated with drug intake, one with atorvastatin [19] and others with cefuroxime [20] in a young boy. One case report was triggered by ultraviolet B radiation [28]. Ormsby and Mitchell initially reported the inaugural case of this disease, followed shortly by Senear and Usher, who documented a cohort of 11 patients with pemphigus erythematosus. These patients exhibited clinical characteristics reminiscent of lupus erythematosus and biopsy findings revealed acantholysis [37].
4. Clinical Picture
The Senear-Usher syndrome manifests with two distinctive features. Firstly, facial symptoms include an eruption that can resemble typical lupus erythematosus, with discoid lesions featuring ‘carpet tack’ scales in the butterfly area. The second aspect involves body eruptions, which typically start as bullae. These blisters are usually small and flaccid, easily rupturing and leading to the development of two types of lesions: reddish patches and yellowish scale crusts [2]. The disease is usually accompanied by pruritis, stinging, or pain within lesions. While PE has been observed in various age groups, including children as youngs, it most commonly begins in middle-aged adults, typically appearing in individuals in their forties and fifties [38]. The disease is more often diagnosed in women [8]. As this syndrome is typically described as a coexistence of LE with pemphigus foliaceus, involvement of the oral mucosa is very rare [6]. The skin appendages are not affected.
5. Diagnosis
The diagnostic criteria of PE contains: the histopathology of PF with DIF findings of intercellular deposits of IgG and IgG and/or C3 deposits along the DEJ [8]. Histological findings include acantholysis at the level of the granular layer or below, as well as the formation of blisters in the subcorneal layer of the epidermis. Dermal edema and perivascular infiltration may be also seen [6,9]. Testing for the presence of antibodies in tissues by DIF is the gold standard in the diagnosis of blistering diseases.
In pemphigus erythematosus IgG/IgM and/or complement (C3) deposits are located not only in the intercellular spaces of the epidermis (typical for pemphigus) but also there are granular deposits of IgG or IgM and/or C3 along the dermal-epidermal junction (typical for lupus erythematosus) [6]. The presence of deposits along the basement membrane is important because it supports the diagnosis of PE [27,39]. Lupus band test is a direct immunopathological examination of unaffected skin exposed to UV radiation. In patients with PE, IgG/IgM and/or complement deposits are observed at the dermal-epidermal junction [27].
Jabłonska and Chorzelski conducted a study on 54 patients with PE and 81% of the patients had positive DIF, but only 23% had a positive LBT [13]. Diagnostics also include blood serum tests for the presence of ANA antibodies and antibodies against cell membrane components.
Since pemphigus erythematosus is considered a variant of pemphigus foliaceus, scientists expect the presence of antibodies against DSG1 in sera of these patients [40]. DSG1 is a 160-kDa transmembrane protein and is part of the desmoglein subfamily of the cell adhesion supergene family. Its intracellular domain interacts with plakoglobin, a component of desmosomal plaques, thereby connecting DSG1 to the cytoskeleton for structural support. The extracellular domain of DSG1 contains epitopes relevant to disease and is involved in mediating cell adhesion through heterophilic interactions. This dual functionality underscores the critical role of DSG1 in maintaining epidermal integrity and how its dysfunction contributes to the acantholysis [41].
However, patients with PE can have antibodies against DSG3 too. This phenomenon may depend on epitope spreading. It refers to a phenomenon in which the immune system’s recognition of epitopes diversifies over time and can broaden the immune response in autoimmune diseases such as SLE, multiple sclerosis, pemphigus, bullous pemphigoid [42]. Besides the antiepithelial antibodies, the antinuclear antibodies are also present in patients with PE.
Pérez-Pérez et al. examined 10 patients with a diagnosis of pemphigus erythematosus and the presence of both antiepithelial and antinuclear antibodies. Because the autoantibodies in the patient’s serum did not show cross-reactivity, the researchers concluded they were produced by independent clones of B cells. Moreover, they disclosed that the desmosome is the immunodominant epitope because the titer of antiepithelial antibodies was always higher than the antinuclear titer [15].
6. Treatment
Due to the infrequent occurrence of the disease, there are unfortunately no clear therapeutic guidelines and recommendations. The choice of treatment is most often based on the analysis of case reports and disease descriptions. Therefore, the evidence regarding optimal therapy is limited. Because pemphigus erythematosus is usually considered a mild variant or subtype of pemphigus foliaceus similar therapies are used as in the latter.
For all types of pemphigus the first-line treatment is generally recommended systemic corticosteroids. They can be used in monotherapy or combination with other immunosuppressants. Disease control is usually achieved with low doses (0.5-1mg/kg/day) of prednisone or equivalent. Doses generally do not need to exceed 1 mg/kg/day of prednisone but sometimes as high as 1.5mg/kg/day are necessary and also acceptable [43,44,45]. Taking high doses of steroids should be continued until new lesions no longer appear. The dose of the medicine can then be gradually lowered to the minimum required to control the disease. In addition to the oral form, glucocorticosteroids such as metyloprednizolon can also be used in intravenous administration in the form of pulses. Appropriate monitoring is critical when using steroids. In the case of chronic glucocorticosteroid therapy, the use of proton pump inhibitors or H2 blockers as a prophylaxis of peptic ulcer disease, potassium supplementation and osteoporosis counseling and prevention (vitamin D and calcium intake or even bisphosphonates) should be considered [45,46].
Most often, the group of immunosuppressive drugs other than general glucocorticoids includes: azathioprine, mycophenolate mofetil (MMF), cyclophosphamide, and methotrexate (MTX) [24,43,44,45,47,48,49]. The use of these drugs as adjuvants usually is aimed at reducing the dose of systemic steroids and/or shortening the need for their administration, thus reducing the risk of side effects of glucocorticoid therapy. Also, they are recommended when the disease’s course is more severe. As monotherapy, they may be suggested in patients with contraindications to systemic corticosteroid treatment.
The usual doses of azathioprine are 1–2.5 mg/kg/day. Treatment should start with a lower dose (50mg/day) and gradually increase it under the control of blood counts and thiopurine methyltransferase (TPMT) activity to avoid adverse effects such as eg. bone marrow toxicity (when TPMT serum level is low or intermediate) or, on the contrary, to avoid lack of therapeutic effectiveness (when TPMT serum level is very high). The disadvantage of azathioprine is its delayed action because it has an immunosuppressive effect only 6-8 weeks after starting therapy [45,50]. Mycophenolate mofetil shows similar tolerance, safety, and efficiency to azathioprine in patients with pemphigus foliaceus [51].
Cases of effective use of hydroxychloroquine [52] or dapsone [45,53,54] in addition to immunosuppressive drugs have also been reported. Using dapson allowed for a reduction of the daily dose of corticosteroids in patients with stable disease and the improvement was visible after just a few weeks of therapy. However, one should remember about possible side effects, such as methemoglobinemia. Contraindications to the use of dapsone are confirmed drug hypersensitivity, anemia and deficiency of glucose-6-phosphate dehydrogenase (G-6-PD) [55]. Campolmi et al. reported three patients with recurrence of pemphigus erythematosus despite maintenance dose steroid therapy, who achieved remission when cyclosporine A (5 mg/kg/day) was added to prednisone (1 mg/kg/day) [56].
According to the literature other effective but less frequently used drugs or procedures in the therapy of pemphigus erythematosus are tetracycline plus niacinamide, plasmapheresis, or intravenous infusion of immunoglobulin [45,48,57,58]. Some biological drugs also appear promising in the treatment of pemphigus erythematosus. These data are based on case series studies. The benefits of these drugs are usually seen in steroid-dependent patients or in those who do not respond to oral corticosteroid-sparing drugs or who experience unacceptable side effects of current therapy.
Rituximab, a chimeric anti-CD20 monoclonal antibody targeting pre-B cells and mature B cells, approved by the FDA for the treatment of pemphigus vulgaris, used as a single agent or in combination with other immunosuppressants to taper their doses [45,48,59]. De Vries et al. described the case of a patient with Senear-Usher syndrome who did not initially respond to treatment of systemic prednisone and MMF but achieved remission of the disease after the use of rituximab as an adjuvant therapy [29].
The use of another monoclonal humanized anti-CD20 antibody—veltuzumab also shown promising results [60]. Recently, two case reports revealed successful usage of dupilumab (human monoclonal antibody directed against IL-4 alpha receptor that inhibits the signaling of IL-4 and IL-13), in the treatment of PE. Both patients were managed with glucocorticoid in combination with dupilumab, resulting in symptoms diminished and providing relief from itching [21]. Infliximab, adalimumab, and etanercept (TNF-α inhibitors) have also been tried, but limited data is available [48].
Topical treatment is usually used as a complementary therapy to systemic drugs, or it may be sufficient as the only form of treatment in very mild cases or in localized forms of disease [45,61,62].
In pemphigus erythematosus topical steroids are most commonly chosen. The strength, dose and form of the drug depend on various factors such as the patient’s age, the location of skin lesions, characteristics of the lesion, and potential for steroid adverse effects [63]. With long-term local treatment, glucocorticosteroids may be replaced with topical calcineurin inhibitors; tacrolimus or pimecrolimus are used less frequently from the beginning of therapy [61,63,64]. Other drugs supporting the treatment of pemphigus may be local analgesics and antiseptics. We should not forget to recommend photoprotection, including the use of UV protective clothing and daily sunscreen because sunlight may exacerbate disease activity [25].
Treatment should be carried out by a dermatologist experienced in the treatment of pemphigus in close cooperation with a clinical center, where laboratory diagnosis and treatment control will be possible because the disease is chronic and recurrent. Monitoring should include the patient’s clinical condition, immunological parameters of the disease, and the occurrence of potential side effects of the drugs used, which will ultimately enable the assessment of the effectiveness and safety of the therapy.
7. Conclusions
This case can be described as multiple autoimmune processes. Considering the clinical picture, results of immunological tests and histopathological examination we can treat this patient as an atypical case of Senar-Usher syndrome, in the spectrum of pemphigus vulgaris with involvement of mucous membranes. In our opinion the patient clinically more closely resembles pemphigus erythematosus (erythematous and erosive eruptions, covered with scab, yellowish crusts, and flaccid blisters in typical localization) and is consistent with other characteristic features of patients with PE showed in Table 2. Moreover, systemic symptoms of SLE were not very pronounced in this patient. The conclusions of this case report may foster academic discussion and inspire further exploration into the nuanced presentations of chronic inflammatory skin diseases. This review also emphasize the importance of individualized diagnostic approaches in complex autoimmune skin diseases.
Author Contributions
Conceptualization, A.Ż.; writing—original draft preparation, M.K. (Magdalena Kutwin), M.K.( Marcelina Kądziela), T.S.; visualization M.K.-G.; writing—review and editing, A.Ż, M.K-G.M.K.(Kutwin). All authors have read and agreed to the published version of the manuscript.
Funding
Work was completed as part of the statutory work of the Medical University Lodz—503/1-152-01/503-11-002.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Consent was obtained from the subject involved in the study.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- SAIKIA NK, MACCONNELL LES. Senear-Usher syndrome and internal malignancy. Br J Dermatol. 1972, 87, 1–5. Available from: https://pubmed.ncbi.nlm.nih.gov/4557734/. [CrossRef]
- Steffen C, Thomas D. The men behind the eponym: Francis E. Senear, Barney Usher, and the Senear-Usher syndrome. Am J Dermatopathol. 2003 Oct, 25(5):432–436. Available from: https://pubmed.ncbi.nlm.nih.gov/14501294/.
- Aringer M, Petri M. New classification criteria for systemic lupus erythematosus. Curr Opin Rheumatol. 2020, 32, 590–596. Available from: https://pubmed.ncbi.nlm.nih.gov/32925250/. [CrossRef]
- Ahmed AR, Graham J, Jordon RE, Provost TT. Pemphigus: current concepts. Ann Intern Med. 1980, 92, 396–405. Available from: https://pubmed.ncbi.nlm.nih.gov/6986830/. [CrossRef]
- RATTNER H, CORNBLEET T, KAGEN MS. Pemphigus Erythematosus. Int J Dermatol. 1985, 24, 16–25. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-4362.1985.tb05349.x. [CrossRef]
- Rosenberg FR, Sanders S, Nelson CT. Pemphigus: a 20-year review of 107 patients treated with corticosteroids. Arch Dermatol. 1976, 112, 962–970. Available from: https://pubmed.ncbi.nlm.nih.gov/820270/. [CrossRef]
- Hobbs LK, Noland MMB, Raghavan SS, Gru AA. Pemphigus erythematosus: A case series from a tertiary academic center and literature review. J Cutan Pathol. 2021, 48, 1038–1050. Available from: https://pubmed.ncbi.nlm.nih.gov/33609053/. [CrossRef]
- Maize JC, Green D, Provost TT. Pemphigus foliaceus: a case with serologic features of Senear-Usher syndrome and other autoimmune abnormalities. J Am Acad Dermatol. 1982, 7, 736–741. Available from: https://pubmed.ncbi.nlm.nih.gov/6757284/. [CrossRef]
- Abréu-Vélez AM, Yepes MM, Patiño PJ, Bollag WB, Montoya F. A sensitive and restricted enzyme-linked immunosorbent assay for detecting a heterogeneous antibody population in serum from people suffering from a new variant of endemic pemphigus. Arch Dermatol Res. 2004, 295, 434–441. Available from: https://pubmed.ncbi.nlm.nih.gov/14730452/. [CrossRef]
- CHORZELSKI T, JABLOŃSKA S, BLASZCZYK M. Immunopathological investigations in the Senear-Usher syndrome (coexistence of pemphigus and lupus erythematosus). Br J Dermatol. 1968, 80, 211–217. Available from: https://pubmed.ncbi.nlm.nih.gov/4869676/. [CrossRef]
- Reich A, Marcinow K, Bialynicki-Birula R. The lupus band test in systemic lupus erythematosus patients. Ther Clin Risk Manag. 2011, 7, 27–32. Available from: https://pubmed.ncbi.nlm.nih.gov/21339940/. [CrossRef]
- Jablońska S, Chorzelski T, Blaszczyk M, Maciejewski W. Pathogenesis of pemphigus erythematosus. Arch Dermatol Res. 1977, 258, 135–140. Available from: https://pubmed.ncbi.nlm.nih.gov/326203/. [CrossRef]
- Amerian ML, Ahmed AR. Pemphigus erythematosus: Presentation of four cases and review of the literature. J Am Acad Dermatol. 1984, 10, 215–222. Available from: http://www.jaad.org/article/S0190962284700259/fulltext. [CrossRef]
- Pérez-Pérez ME, Avalos-Díaz E, Herrera-Esparza R. Autoantibodies in Senear-Usher Syndrome: Cross-Reactivity or Multiple Autoimmunity? Autoimmune Dis. 2012, PMID: 23320149, Available from: /pmc/articles/PMC3539423/.
- Chandan N, Lake EP, Chan LS. Unusually extensive scalp ulcerations manifested in pemphigus erythematosus. Dermatol Online J. 2018,24, PMID: 29469763. [CrossRef]
- Henington VM, Kennedy B, Loria PR. The Senear-Usher syndrome (pemphigus erythematodes); a report of eight cases. South Med J. 1958, 51, 577–585. Available from: https://pubmed.ncbi.nlm.nih.gov/13556160/. [CrossRef]
- Garcia-Souto F, Sosa-Moreno F. Visual Dermatology: Pemphigus Erythematosus (Senear-Usher Syndrome). J Cutan Med Surg. 2020, 24, 190. Available from: https://pubmed.ncbi.nlm.nih.gov/32208026/. [CrossRef]
- Schiavo A Lo, Puca RV, Romano F, Cozzi R. Pemphigus erythematosus relapse associated with atorvastatin intake. Drug Des Devel Ther. 2014, 8, 1463. Available from: /pmc/articles/PMC4173814/. [CrossRef]
- Baroni A, Puca R V., Aiello FS, Palla M, Faccenda F, Vozza G, et al. Cefuroxime-induced pemphigus erythematosus in a young boy. Clin Exp Dermatol. 2003, 34, 708–710. Available from: https://pubmed.ncbi.nlm.nih.gov/19077088/. [CrossRef]
- Chen J, Chen S, Wu X, Jiang X, Wang Y, Cheng H. The complicated use of dupilumab in the treatment of atypical generalized pemphigus Erythematous: A report of two cases. Hum Vaccin Immunother. 2023, 19. Available from: https://pubmed.ncbi.nlm.nih.gov/36798973/. [CrossRef]
- Bilgic Temel A, Ergün E, Poot AM, Bassorgun CI, Akman-Karakaş A, Uzun S, et al. A rare case with prominent features of both discoid lupus erythematosus and pemphigus foliaceus. Journal of the European Academy of Dermatology and Venereology. 2019, 33, 5–7. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/jdv.15099. [CrossRef]
- Sawamura S, Kajihara I, Makino K, Makino T, Fukushima S, Jinnin M, et al. Systemic lupus erythematosus associated with myasthenia gravis, pemphigus foliaceus and chronic thyroiditis after thymectomy. Australasian Journal of Dermatology. 2017 ,58, 120–122. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/ajd.12510. [CrossRef]
- Gupta MT, Jerajani HR. Control of childhood pemphigus erythematosus with steroids and azathioprine. Br J Dermatol. 2004, 150, 163–164. Available from: https://pubmed.ncbi.nlm.nih.gov/14746642/. [CrossRef]
- Pritchett EN, Hejazi E, Cusack CA. Pruritic, Pink Scaling Plaques on the Face and Trunk. Pemphigus erythematosus. JAMA Dermatol. 2015, 151, 1123–1124. Available from: https://pubmed.ncbi.nlm.nih.gov/26267852/. [CrossRef]
- Diab M, Bechtel M, Coloe J, Kurtz E, Ranalli M. Treatment of refractory pemphigus erythematosus with rituximab. Int J Dermatol. 2008, 47, 1317–1318. Available from: https://pubmed.ncbi.nlm.nih.gov/19126029/. [CrossRef]
- Oktarina DAM, Poot AM, Kramer D, Diercks GFH, Jonkman MF, Pas HH. The IgG “lupus-band” deposition pattern of pemphigus erythematosus: association with the desmoglein 1 ectodomain as revealed by 3 cases. Arch Dermatol. 2012, 148, 1173–1178. Available from: https://pubmed.ncbi.nlm.nih.gov/22801864/. [CrossRef]
- Makino T, Seki Y, Hara H, Mizawa M, Matsui K, Shimizu K, et al. Induction of skin lesions by ultraviolet B irradiation in a case of pemphigus erythematosus. Acta Derm Venereol. 2014, 94, 487–248. Available from: https://pubmed.ncbi.nlm.nih.gov/24356850/. [CrossRef]
- de Vries JM, Moody P, Ojha A, Grise A, Sami N. A Recalcitrant Case of Senear-Usher Syndrome Treated With Rituximab. Cureus. 2023, 15, 10. Available from: https://pubmed.ncbi.nlm.nih.gov/37954755/. [CrossRef]
- Shankar S, Burrows NP. Case 1. Clin Exp Dermatol. 2004, 29, 437–438. Available from: https://dx.doi.org/10.1111/j.1365-2230.2004.01588.x. [CrossRef]
- Chavan SA, Sharma YK, Deo K, Buch AC. A Case of Senear-Usher Syndrome. Indian J Dermatol. 2013, 58, 329. Available from: /pmc/articles/PMC3726916/.
- Hidalgo-Tenorio C, Sabio-Sánchez JM, Tercedor-Sánchez J, León-Ruíz L, Pérez-Alvarez F, Jiménez-Alonso J. Pemphigus vulgaris and systemic lupus erythematosus in a 46-y-old man. Lupus. 2001, 10, 824–826. Available from: https://pubmed.ncbi.nlm.nih.gov/11789495/. [CrossRef]
- Thongprasom K, Prasongtanskul S, Fongkhum A, Iamaroon A. Pemphigus, discoid lupus erythematosus, and dermatomyositis during an 8-year follow-up period: a case report. J Oral Sci. 2013, 55, 255–258. Available from: https://pubmed.ncbi.nlm.nih.gov/24042593/. [CrossRef]
- Nanda A, Kapoor MM, Dvorak R, Al-Sabah H, Alsaleh QA. Coexistence of pemphigus vulgaris with systemic lupus erythematosus. Int J Dermatol [Internet]. 2004, 43, 393–394. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-4632.2004.02105.x. [CrossRef]
- Calebotta A, Cirocco A, Giansante E, Reyes O. Systemic lupus erythematosus and pemphigus vulgaris: association or coincidence. Lupus. 2004, 13, 951–953. Available from: https://pubmed.ncbi.nlm.nih.gov/15645751/. [CrossRef]
- Syndromes: Rapid Recognition and Perioperative Implications, 2e | AccessAnesthesiology | McGraw Hill Medical. Available from: https://accessanesthesiology.mhmedical.com/book.aspx?bookID=2674.
- Jordon RE. “An unusual type of pemphigus combining features of lupus erythematosus” by Senear and Usher, June 1926. Commentary: Pemphigus erythematosus, a unique member of the pemphigus group. Arch Dermatol. 1982 Oct [cited 2024, 118, 723–742. Available from: https://pubmed.ncbi.nlm.nih.gov/6753755/. [CrossRef]
- Maize JC, Green D, Provost TT. Pemphigus foliaceus: a case with serologic features of Senear-Usher syndrome and other autoimmune abnormalities. J Am Acad Dermatol [Internet]. 1982, 7, 736–741. Available from: https://pubmed.ncbi.nlm.nih.gov/6757284/. [CrossRef]
- Rutnin S, Chanprapaph K. Vesiculobullous diseases in relation to lupus erythematosus. Clin Cosmet Investig Dermatol. 2019, 12, 653–667. Available from: https://pubmed.ncbi.nlm.nih.gov/31564947/. [CrossRef]
- Amann PM, Megahed M. Pemphigus erythematosus. Hautarzt. 2012, 63, 365–367. Available from: https://pubmed.ncbi.nlm.nih.gov/22527297/.
- Hacker-Foegen MK, Janson M, Amagai M, Fairley JA, Lin MS. Pathogenicity and epitope characteristics of anti-desmoglein-1 from pemphigus foliaceus patients expressing only IgG1 autoantibodies. J Invest Dermatol. 2002, 121, 1373–1378. Available from: https://pubmed.ncbi.nlm.nih.gov/14675185/. [CrossRef]
- Cornaby C, Gibbons L, Mayhew V, Sloan CS, Welling A, Poole BD. B cell epitope spreading: mechanisms and contribution to autoimmune diseases. Immunol Lett. 2015, 163, 56–68. Available from: https://pubmed.ncbi.nlm.nih.gov/25445494/. [CrossRef]
- Martin LK, Werth VP, Villaneuva E V., Murrell DF. A systematic review of randomized controlled trials for pemphigus vulgaris and pemphigus foliaceus. J Am Acad Dermatol. 2011, 64, 903–908. Available from: https://pubmed.ncbi.nlm.nih.gov/21353333/. [CrossRef]
- Schmidt E, Zillikens D. The Diagnosis and Treatment of Autoimmune Blistering Skin Diseases. Dtsch Arztebl Int. 2011, 108, 399. Available from: /pmc/articles/PMC3123771/. [CrossRef]
- Joly P, Horvath B, Patsatsi, Uzun S, Bech R, Beissert S, et al. Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the european academy of dermatology and venereology (EADV). J Eur Acad Dermatol Venereol 2020, 34, 1900–13. Available from: https://pubmed.ncbi.nlm.nih.gov/32830877/. [CrossRef]
- Caplan A, Fett N, Rosenbach M, Werth VP, Micheletti RG. Prevention and management of glucocorticoid-induced side effects: A comprehensive review: A review of glucocorticoid pharmacology and bone health. J Am Acad Dermatol. 2017, 76, 1–9. Available from: https://pubmed.ncbi.nlm.nih.gov/27986132/. [CrossRef]
- PASRICHA JS, SOOD VD, MINOCHA Y. Treatment of pemphigus with cyclophosphamide. Br J Dermatol. 1975, 93, 573–576. Available from: https://pubmed.ncbi.nlm.nih.gov/1106754/. [CrossRef]
- Dick SE, Werth VP. Pemphigus: a treatment update. Autoimmunity. 2006, 39, 591–599. Available from: https://pubmed.ncbi.nlm.nih.gov/17101503/. [CrossRef]
- Kasperkiewicz M, Ellebrecht CT, Takahashi H, Yamagami J, Zillikens D, Payne AS, et al. Pemphigus. Nat Rev Dis Primers. 2017, 11, 3, 17026. Available from: https://pubmed.ncbi.nlm.nih.gov/28492232/. [CrossRef]
- Meurer M. Immunosuppressive therapy for autoimmune bullous diseases. Clin Dermatol. 2012, 30, 78–83. Available from: https://pubmed.ncbi.nlm.nih.gov/22137230/. [CrossRef]
- Beissert S, Werfel T, Frieling U, Böhm M, Sticherling M, Stadler R, et al. A comparison of oral methylprednisolone plus azathioprine or mycophenolate mofetil for the treatment of pemphigus. Arch Dermatol. 2006, 142, 1447–1454. [CrossRef]
- SR H, RE J. Pemphigus foliaceus. Use of antimalarial agents as adjuvant therapy. Arch Dermatol. 1992, 128, 1462–1464. [CrossRef]
- PIAMPHONGSANT T. Pemphigus controlled by dapsone. Br J Dermatol. 1976, 94, 681–686. Available from: https://pubmed.ncbi.nlm.nih.gov/779820/. [CrossRef]
- Basset N, Guillot B, Michel B, Meynadier J, Guilhou JJ. Dapsone as Initial Treatment in Superficial Pemphigus: Report of Nine Cases. Arch Dermatol. 1987, 123, 783–785. Available from: https://jamanetwork.com/journals/jamadermatology/fullarticle/548362. [CrossRef]
- Grcan HM, Ahmed AR. Efficacy of dapsone in the treatment of pemphigus and pemphigoid: analysis of current data. Am J Clin Dermatol. 2009, 10, 383–396. Available from: https://pubmed.ncbi.nlm.nih.gov/19824739/. [CrossRef]
- Campolmi P, Bonan P, Lotti T, Palleschi GM, Fabbri P, Panconesi E. The Role of Cyclosporine A in the Treatment of Pemphigus Erythematosus. Int J Dermatol. 1991, 30, 890–892. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-4362.1991.tb04361.x. [CrossRef]
- Tan-Lim R, Bystryn JC. Effect of plasmapheresis therapy on circulating levels of pemphigus antibodies. J Am Acad Dermatol. 1990, 22, 35–40. Available from: http://www.jaad.org/article/0190962290700042/fulltext. [CrossRef]
- Chaffins ML, Collison D, Fivenson DP. Treatment of pemphigus and linear IgA dermatosis with nicotinamide and tetracycline: a review of 13 cases. J Am Acad Dermatol. 1998, 28, 998–1000. Available from: https://pubmed.ncbi.nlm.nih.gov/8496464/. [CrossRef]
- P J, M D, P M. Rituximab for pemphigus vulgaris. N Engl J Med [Internet]. 2007, 356, 521–522. Available from: https://pubmed.ncbi.nlm.nih.gov/17267915/. [CrossRef]
- Jangid SD, Madke B, Singh A, Bhatt DM, Khan A, Jangid SD, et al. A Case Report on Senear-Usher Syndrome. Cureus. 2023, 15, 11. Available from: https://www.cureus.com/articles/203747-a-case-report-on-senear-usher-syndrome. [CrossRef]
- Kunadia A, Moschella S, McLemore J, Sami N. Localized Pemphigus Foliaceus: Diverse Presentations, Treatment, and Review of the Literature. Indian J Dermatol. 2023, 68, 123. Available from: https://pubmed.ncbi.nlm.nih.gov/37151255/. [CrossRef]
- Dumas V, Roujeau JC, Wolkenstein P, Revuz J, Cosnes A. The treatment of mild pemphigus vulgaris and pemphigus foliaceus with a topical corticosteroid. Br J Dermatol. 1999, 140, 1127–1129. Available from: https://pubmed.ncbi.nlm.nih.gov/10354082/. [CrossRef]
- Stacey SK, McEleney M. Topical Corticosteroids: Choice and Application. Am Fam Physician. 2021 Mar 15 [cited 2024, 103, 337–343. Available from: https://www.aafp.org/pubs/afp/issues/2021/0315/p337.html.
- Tyros G, Kalapothakou K, Christofidou E, Kanelleas A, Stavropoulos PG. Successful Treatment of Localized Pemphigus Foliaceus with Topical Pimecrolimus. Case Rep Dermatol Med. 2013, PMCID: PMC3789317, 1–3. Available from: /pmc/articles/PMC3789317/. [CrossRef]
Figure 1.
Dermatological examination: A-Erythematous and erosive eruptions partially covered with scab, yellowish crust disseminated on the scalp and face. B-Blisters and erosions covered with scabs on the trunk. C- Erosions of the mucosal lip, whitening of the oral mucosa.
Figure 1.
Dermatological examination: A-Erythematous and erosive eruptions partially covered with scab, yellowish crust disseminated on the scalp and face. B-Blisters and erosions covered with scabs on the trunk. C- Erosions of the mucosal lip, whitening of the oral mucosa.
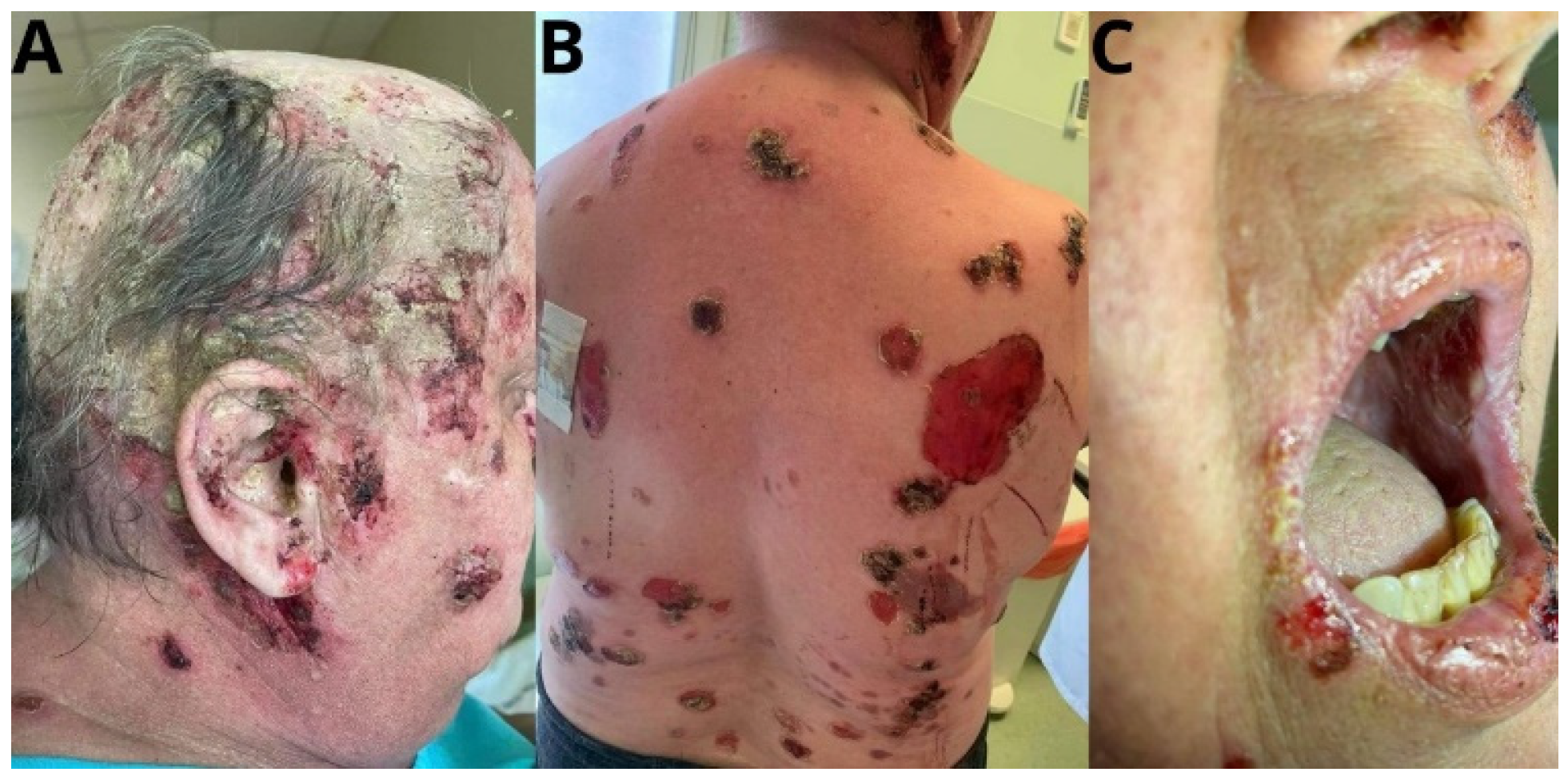
Figure 2.
Clinical examination: A-Scarring lesions with follicular hyperkeratosis, erythematous lesions, erosions covered with scab. B-Post-inflammatory discoloration on the skin of the trunk.
Figure 2.
Clinical examination: A-Scarring lesions with follicular hyperkeratosis, erythematous lesions, erosions covered with scab. B-Post-inflammatory discoloration on the skin of the trunk.

Figure 3.
Direct immunofluorescence examination: A-Direct immunofluorescence is seen with intraepidermal intercellular deposition of granular IgG. B-Direct immunofluorescence is seen with granular deposition of C3 along the dermo-epidermal junction.
Figure 3.
Direct immunofluorescence examination: A-Direct immunofluorescence is seen with intraepidermal intercellular deposition of granular IgG. B-Direct immunofluorescence is seen with granular deposition of C3 along the dermo-epidermal junction.
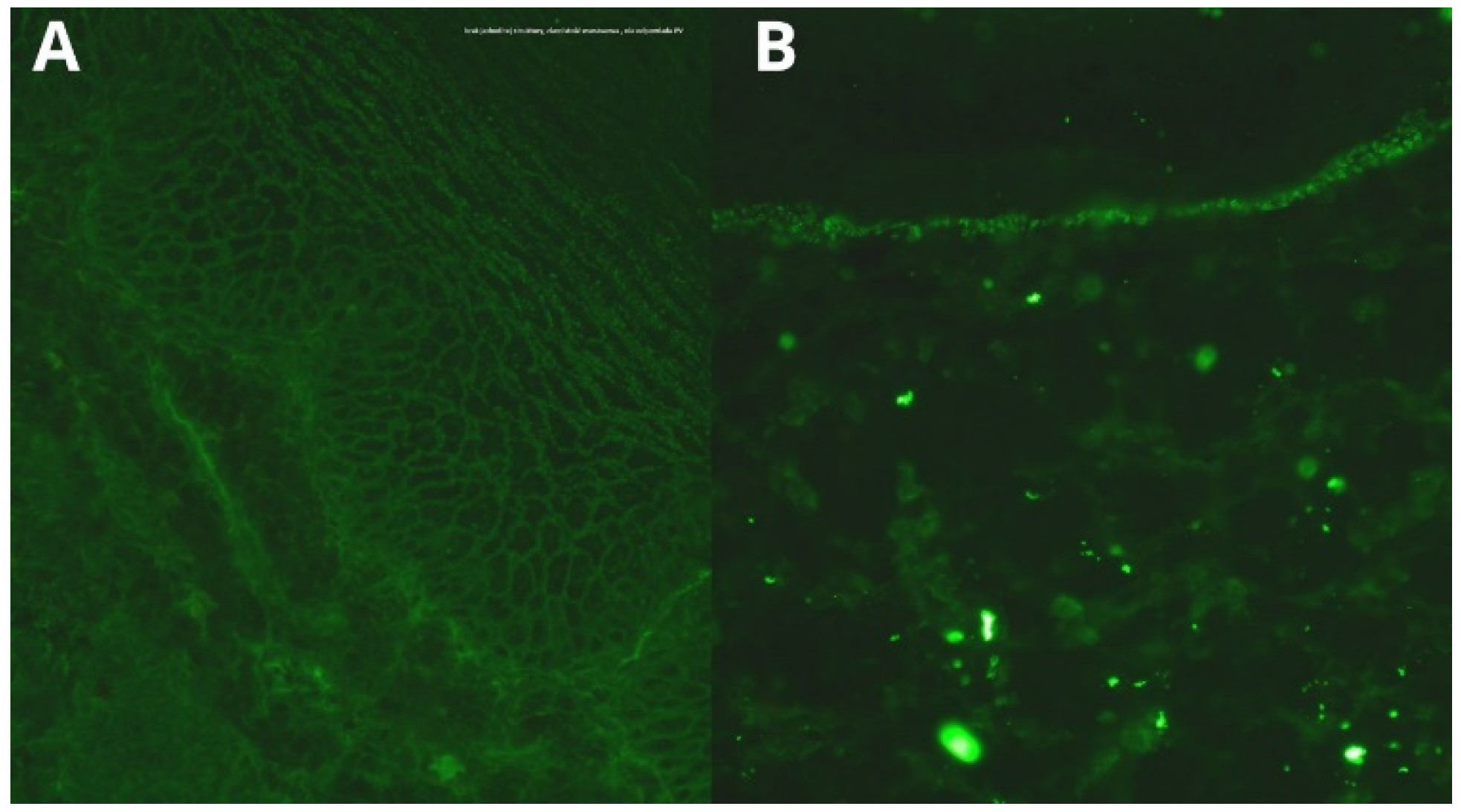

Table 1.
Results of diagnostic tests.
| Date | 2016 | July 2021 | December 2021 | October 2022 | April 2023 |
October 2023 |
|---|---|---|---|---|---|---|
| ANA antibodies titer and type of fluorescence | 1:640 speckled-granular and mitochondrial | 1:320 nuclear 1:320 granular | 1:320 nuclear 1:160 granular, 1:80 cytoplasmic | |||
| ANA specificity antibodies | negative | Scl 70 (+) | ||||
| anti-DSG1 antibodies titer | 1:40 | 1:80 | negative | 1:40 | 1:80 | |
| anti-DSG3 antibodies titer | 1:20 | 1:20 | negative | 1:20 | 1:40 | |
| Antibodies on monkey esophagus substrate | 1:20 | 1:10 | 1:40 |
1:40 | Negative | |
| DIF | deposits of IgG (++) and IgA (++) in the intercellular spaces of the epidermis | granular deposits of IgG (+) in the intercellular spaces of the epidermis, granular C3 (+) deposits along the dermoepidermal junction | ||||
| LBT | Negative | |||||
|
Histopathology |
skin section covered with acantholytic epidermis with preserved basal and spinous layers (bottom of the blister) with lymphocyte infiltration in the stroma—the image may correspond to the diagnosis of pemphigus |
Table 2.
Characteristics and clinical and serological features of patients with PE between 2000 and 2024.
Table 2.
Characteristics and clinical and serological features of patients with PE between 2000 and 2024.
| Paper | Demographic | Location of lesions | Appearance of skin lesions | Histopathology examination | DIF—ICS | DIF-DEJ | ANA | DSG-1 | DSG-3 |
|---|---|---|---|---|---|---|---|---|---|
| Hobbs, 2021 [8] | 37,f | scalp and face |
thick, scaly, crusty erythematous plaques | epidermis: acantholysis dermis: perivascular and interstitial infiltrate | IgG | granular IgG and C3, fibrin (focal) deposition | negative | NA | NA |
| Hobbs, 2021 [8] | 44,f | face and oral mucosa |
heavy scale, underlying erythema without blisters or erosions | epidermis: acantholysis dermis: inflammatory infiltrate |
- | IgG, C3, fibrin around dermal vessels |
negative | positive | NA |
| Hobbs, 2021 [8] | 68,m | trunk and scalp |
classic raw erosive changes with some crusting |
epidermis: acantholysis, dermis: perivascular infiltrate | IgG, C3, fibrin |
C3 | NA |
NA |
NA |
| Hobbs, 2021 [8] | 53,f | face |
scaly, dusky plaques with erythematous raised borders | epidermis: keratinocyte necrosis and vacuolar alteration of the basal cell layer along with apoptotic bodies, dermis: perivascular infiltrate |
IgG, C3 |
granular C3, focal IgM, granular IgA |
positive | positive | NA |
| Hobbs, 2021 [8] | 17, m | face, extremities, trunk, and oral mucosa | crusted, vegetative plaques, intact tense small bullae and vesicles |
epidermis: acantholysis |
IgG, C3 |
granular C3 |
NA |
NA |
NA |
| Garcia-Souto, 2020 [18] | 53, f | face |
crusted erosions over the face |
intraepidermal blister with acantholysis of the granular layer |
IgG, C3 |
- |
NA |
NA |
NA |
| Lo Schiavo, 2014 [19] | 70, m | face and trunk |
erythematous scaly plaques which involved the cheeks in a butterfly distribution symmetrically and crusted lesions localized on the upper part of the chest | intraepithelial superficial blister |
IgG, C3 |
IgG, C3 |
positive | positive | NA |
| Neha Chandan, 2018 [16] | 24, f | trunk, extremities, and face |
erythematous, eroded, boggy scalp, crusting, and scale adherent to the residual hair, with yellow to brown debris |
suprabasal and intraepidermal acantholysis with no interface or basal vacuolar changes |
IgG |
IgG, C3 |
negative | positive | positive |
| Baroni, 2009 [20] | 14, m | scalp |
flaccid vesiculobullae, erosions, and crusted lesions over the upper part of the chest and face, and diffuse scaly plaques on the scalp |
intraepidermal superficial blistering containing a few acantholytic cells |
IgG, C3 |
- | NA | positive | negative |
| Chen, 2023 [21] | 39, m | face, trunk, and extremities |
extensive blistering and ulceration on the face, trunk, abdomen, and extremities |
intraepithelial cleavage with detached keratinocytes primarily localized just under the stratum corneum |
IgG, C3 |
- | NA | NA | NA |
| Chen, 2023 [21] | 59, f | face, trunk, and extremities |
widespread erosions affecting the face, trunk, abdomen, and limbs |
subcorneal split directly below the stratum corneum |
IgG, C3 |
- | NA | NA | NA |
| Bilgic, 2018 [22] | 54, m | face, scalp |
well-demarcated, erythematous -squamous plaques, some with atrophic center or with cicatricial alopecia, on the scalp, nose, malar area and lips, bullae, and erosions with scale crusts on the trunk |
compatible with DLE and PF | IgG |
- | negative | positive | negative |
| Sawamura, 2016 [23] | 65, f | face, trunk, and extremities |
scattered erosive erythema with scaling and crusting throughout the body including the face |
intraepidermal blisters containing neutrophils and acantholytic keratinocytes |
IgG |
IgG |
NA |
positive | negative |
| Gupta, 2004 [24] | 7,m | extremities, face, scalp |
generalized scaling and redness associated with edema of the upper and lower extremities, flaccid blisters on the scalp, face, and both lower extremities |
compatible with pemphigus erythematosus |
IgG, C3 |
IgG, C3 |
negative | positive | negative |
| Pritchett, 2015 [25] | 40, f | face and trunk |
pruritic, pink scaling plaques on her face and neck, lesions subsequently involved chest, abdomen, and back, and flared with sun exposure |
epidermal acanthosis, spongiosis, and acantholytic keratinocytes lymphoplasmacellular infiltrate was seen in the dermis, with scattered neutrophils and eosinophils, foci of eosinophilic spongiosis in the epidermis | IgG, C3 |
IgG, C3 |
positive | NA | NA |
| Diab, 2008 [26] | 18, f | face, trunk, extremities |
keratotic hyperpigmented papules and plaques on the face, upper trunk, and proximal extremities |
acantholysis within the granular cell layer with concomitant interface dermatitis |
IgG, C3 |
IgM |
NA | positive | NA |
| Dyah, 2012 [27] | 80, f | face, trunk, extremities |
generalized progressive erythematous skin lesions with pustules and flaccid blisters | subcorneal blisters |
IgG, C3 |
- |
negative | positive | negative |
| Dyah, 2012 [27] | 76, f | face, scalp, trunk, extremities | itching plaques all over body and scalp except her legs |
ulcerative and erosive inflammation and secondary impetigo with beginning reepithelialization |
IgG, C3 |
IgG, C3, IgM |
Negative | positive | negative |
| Dyah, 2012 [27] | 68, m | scalp, extremities, trunk | red scaly skin lesions starting on the face, chest, and back, blisters on the whole body, including the scalp and extremities | remainder of a blister in the corneal layer and subepidermal neutrophilic infiltrates surrounding the blood vessels | IgG, IgA, C3 |
IgG, IgA, and C3 |
negative | positive | negative |
| Makino, 2014 [28] | 62,f | face, trunk, extremities | pruritic and slightly erythematous lesions with erosions on the nose, chest, and extremities |
detachment of the stratum corneum, infiltration of lymphocytes |
IgG |
IgM, C3 |
positive | positive | negative |
| de Vries, 2023 [29] | 51,m | face, scalp, and trunk |
pruritic scaly plaques on the face, scalp, and trunk |
acantholysis and granular layer separation |
NA |
NA |
positive | positive | negative |
| Shankar, 2004 [30] | 59, f | face, trunk, scalp, extremities |
pruritic rash on the upper chest and upper back, face, scalp and thighs |
acantholysis of the superficial epidermis with the formation of a subcorneal bulla and a very mild patchy interface dermatitis |
IgG, C3 |
IgM, C3 |
positive | NA | NA |
| Chavan, 2013 [31] | 32, f | face, scalp, trunk, extremities, oral mucosa |
erythematous papules over cheeks, ears, scalp, upper back, “V” of the chest and extensors of forearms and dorsal of hands, crusted scaly, plaques with surrounding erythema, erosions over upper gingiva | hyperkeratosis, subcorneal acantholysis, basal cell vacuolation, dermo-epidermal separation and superficial perivascular lymphocytic infiltrate |
IgG |
IgM, IgG |
positive | NA | NA |
Table 3.
Characteristics and clinical and serological features of patients with pemphigus vulgaris and SLE between 2000 and 2024.
Table 3.
Characteristics and clinical and serological features of patients with pemphigus vulgaris and SLE between 2000 and 2024.
| Paper | Demographic | Location of lesions | Appearance of skin lesions | Histopathology examination | DIF—ICS | DIF-DEJ | ANA | DSG-1 | DSG-3 |
|---|---|---|---|---|---|---|---|---|---|
| Hidalgo, 2001 [32] | 46, m | chest, extremities | pruritic eruption of symmetric lesions of 0.5–1 cm in diameter, consisting of vesicles on the chest, back, shoulders and legs |
intraepidermal detachment forming blisters and fissures in a suprabasal portion of the epidermis, with acantholysis, next to spongiform vesicles filled with polymorphs and several eosinophils |
IgG, C3 |
- | positive | NA | NA |
| Thongprasom, 2013 [33] | 36, f | oral mucosa, face |
desquamative gingivitis, erythematous facial rash with acne-like papules |
acantholysis of the epithelial cells, which exhibited intraepithelial separation, particularly in the lower spinous cell layer and perivascular infiltration of lymphocytes in the lamina propria |
IgG |
- | positive | NA | NA |
| Nanda, 2004 [34] | 45, f | oral mucosa |
ulcers on the buccal mucosa and soft palate with inflammation of the gums and soft pharynx |
intraepithelial blister with acantholytic cells |
IgG, C3 |
- | positive | negative | positive |
| Calebotta, 2004 [35] | 35, f | extremities, face, and oral mucosa |
generalized multiple erosions with zero-hematic crusts on the trunk and both legs, flaccid bullae with serous content located on the thigh, multiple erosions on oral mucosa |
separation in a plane above the basal layer of the epidermis |
IgG |
IgM, C3 |
positive | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



