
Submitted:
11 December 2024
Posted:
12 December 2024
You are already at the latest version
Abstract
Autoimmune blistering diseases (AIBD) involve autoantibodies targeting proteins in the epidermal/epithelial desmosome (pemphigus) or basement membrane zone (pemphigoid).
Despite widespread antigen distribution, lesions exhibit a scattered involvement pattern. This study maps the frequency/severity of AIBD lesions in various body parts and investigates whether differential antigen expression contributes to specific predilection sites.
We analyzed affected sites presenting blisters/erosions, erythematous/urticarial lesions, and mucosal lesions in bullous pemphigoid (BP-cohort 1, n=65; BP-cohort 2, n=119), pemphigus vulgaris (PV, n=67), and pemphigus foliaceus (PF, n=20) patients. To assess antigen expression, we conducted indirect immunofluorescence (IF) staining of 11 AIBD antigens from 13 anatomical sites of 10 body donors without AIBD.
In BP, blisters/erosions and erythematous/urticarial lesions predominantly affected arms and legs, while PV/PF patients exhibited frequent involvement of buccal mucosa and back, respectively. IF staining identified significant regional differences in BP180, BP230, and integrin β4 expression, although these variations did not correlate with a higher lesion frequency/severity. Other antigens showed consistent expression across all regions.
Our findings suggest that predilection sites for BP and PV/PF are largely unaffected by regional variations in antigen expression but may be influenced by factors like microbiota, mechanical stress, sunlight exposure, local immunity, or genetics.
Keywords:
autoimmune blistering disease
; bullous pemphigoid
; pemphigus
; predilection sites
; antigen expression
1. Introduction
Autoimmune blistering diseases (AIBD) are a paradigm of organ-specific, autoantibody-mediated autoimmune diseases that can be classified into two groups based on the location of split formation: intraepidermal blistering in the pemphigus group and subepidermal blistering in the pemphigoid group and dermatitis herpetiformis [1]. In pemphigus, autoantibodies target desmosomal cadherins, desmoglein (Dsg) 1 and Dsg3, which disrupt epithelial cell-cell adhesion, leading to intraepithelial blisters and erosions of the skin and the surface-close mucous membranes [2,3]. In contrast, pemphigoid diseases are characterized by autoantibodies against structural proteins at the dermal-epidermal junction [4,5].
Bullous pemphigoid (BP), the most common AIBD, is caused by autoantibodies against two hemidesmosomal proteins, BP180 (BPAG2, type XVII collagen) and BP230 (BPAG1, dystonin) [6]. In epidermolysis bullosa acquisita, autoantibodies target type VII collagen, while mucous membrane pemphigoid is distinguished by predominant mucosal involvement and autoantibodies against BP180, laminin 332, type VII collagen, BP230, and α6β4 integrin [7].
A key, yet unresolved, question in AIBD concerns the distribution of cutaneous and/or mucosal lesions, which tend to appear in specific anatomical regions with varying frequency and severity. One possible explanation is that these regions exhibit higher levels of the target antigens, making them more susceptible to blister formation. This hypothesis is supported by findings showing that human mucosal keratinocytes express high levels of pemphigus vulgaris (PV) antigens but lower levels of pemphigus foliaceus (PF) antigens [8].
To investigate this hypothesis, we systematically examined the predilection sites of clinical lesions in patients with BP, PV, and PF. Additionally, we semi-quantitatively assessed the expression levels of key AIBD target antigens, including Dsg1, Dsg3, BP180, BP230, collagen VII, laminin α3, laminin β3, integrin α6, integrin β4, plectin, and cytokeratin 14, across 13 anatomical regions, aiming to identify potential correlations between antigen expression levels and lesion distribution.
2. Materials and Methods
2.1. Human Material
The study included the following cohorts patients with AIBD: (i) BP cohort 1 (n = 65; females [56.9%], males [43.1%]; mean age, 79.9 years; median age, 83 years), (ii) BP cohort 2 (n = 119; 49 females (41%), 70 males (59%); mean age, 75 years; median age, 77 years), (iii) PV cohort (n = 67; females [56.2%], males [43.8%]; mean age, 65.6 years; median age, 55 years), and (iv) PF cohort (n = 20; females [38.8%], males [61.2%]; mean age, 66.9 years; median age, 71 years).
BP patients were diagnosed according to the following diagnostic criteria: (i) a compatible clinical picture without predominant mucosal involvement, (ii) positive IgG staining on the epidermal side of 1 M human salt-split skin by indirect immunofluorescence (IF) microscopy, (iii) presence of circulating IgG autoantibodies against BP180-NC16A or BP230 by ELISA (Euroimmun, Lübeck, Germany), and/or linear IgG and/or C3c deposition along the basement membrane zone (BMZ) by direct IF microscopy of perilesional skin biopsies [9,10]. Disease activity at initial diagnosis was assessed using the Bullous Pemphigoid Disease Activity Index (BPDAI) [11], which differentiates between blisters/erosions and erythematous/urticarial lesions.
Pemphigus was diagnosed based on the clinical picture, intercellular IgG binding to the epithelium of monkey esophagus, and IgG reactivity to Dsg1 and/or Dsg3 by ELISA [3,12]. Disease severity was assessed using the Pemphigus Disease Area Index (PDAI) scoring system [13], which distinguishes between (i) cutaneous activity (i.e., blisters, erosions, and new erythema), (ii) damage (i.e., post-inflammatory hyperpigmentation and erythema from resolving lesions), and (iii) mucosal lesions. Both BPDAI and PDAI scores range from 0 to 10 based on severity. All patients were newly diagnosed and had not received systemic immunosuppressive treatment prior to inclusion.
In cohorts 1, 3, and 4, site involvement was determined using BPDAI and PDAI data from clinical records. In cohort 2, lesions were recorded retrospectively from clinical photographs routinely taken between January 2012 and September 2023. For patients with multiple time points, only images from the first visit were analyzed.
For analysis of antigen expression, skin and mucosal punch biopsies were obtained from 10 body donors (4 males and 6 females, all > 70 years old) with no history of AIBD. From each body donor, 5-mm postmortem biopsies were taken from 13 anatomical sites, including buccal mucosa, lower labial mucosa, lower conjunctiva, cheek, central sweating line of the breast, central sweating line of the back, flank at umbilical level, medial upper leg, dorsal lower leg, sole, medial upper arm, medial forearm, and palm. Tissue samples were embedded in Tissue-Tek O.C.T. compound (Sakura Finetek, Staufen, Germany) for IF examination.
2.2. Immunofluorescence Studies
IF staining was performed to semi-quantitatively assess the expression of key AIBD antigens, including Dsg1, Dsg3, BP180, BP230, collagen VII, laminin α3, laminin β4, integrin α6, integrin β4, plectin, and cytokeratin 14, across 13 different body sites. Tissue sections, 6 µm thick, were air-dried and incubated with serial dilutions of primary antibodies in PBS for 1 hour at room temperature (RT). Isotype controls served as negative controls. Following washing with PBS, sections were incubated with secondary antibodies for 1 hour at RT, washed, and mounted with DAPI Fluoromount-G®® (SouthernBiotech, Birmingham, AL, USA). The stained sections were visualized using a Keyence microscope (BZ-9000E series, Keyence GmbH, Neu-Isenburg, Germany). Endpoint titers for each antibody were defined as the highest dilution showing positive staining. A detailed list of the primary and secondary antibodies used is available in Table S1.
2.3. Statistics
To assess differences in BPDAI and PDAI scores across body sites, the non-parametric Friedman test was employed, using subjects as blocks. The null hypothesis was that scores would be consistent across all sites. When a significant result was observed at the 5% level, rank-based Tukey contrasts (all pairwise comparisons) were conducted to avoid false positives from multiple pairwise tests. For BPDAI pigmentation, categorized as present or absent, Cochran’s Q test was used, followed by post-hoc McNemar’s test.
The Friedman test was also utilized to compare antigen distributions across body sites, accounting for individual variability. Global P values were adjusted for the analysis of 11 proteins using the Holm method. Site-specific differences were defined by adjusted P values < 0.05, and pairwise post-hoc comparisons were performed with Tukey contrasts. To further adjust for multiple comparisons, P values were refined using the Bonferroni method.
Body donor sites were aligned with BPDAI/PDAI skin or mucosal blister sites, and the correlation between mean antibody titers and clinical scores across sites was estimated with the Spearman method. All statistical analysis was conducted using R (version 4.1, 2021, The R Foundation for Statistical Computing) with the R packages rstatix (https://CRAN.R-project.org/package=rstatix) and multcomp [14].
3. Results
3.1. Arms and Legs Are the Most Common Sites for Blisters/Erosions and Erythematous/Urticarial Lesions in BP
In BP cohort 1, all patients presented with cutaneous blisters/erosions, with arms (53.8%) and legs (50.7%) being the most frequently affected areas, followed by abdomen, back/buttocks, feet, hands, and chest (Figure 1A, Table S2). Notably, the most severe blisters/erosions also occurred in arms, legs, and feet. Additionally, a substantial proportion of patients had erythematous/urticarial lesions on arms (53.8%, score 1), followed by legs, back/buttocks, abdomen, and chest. These lesions rarely reached a severity score greater than 2 (Figure 1B, Table S3).
Mucosal involvement was observed in 10.8% of patients in BP cohort 1, although no mucosal region exceeded a BPDAI score of 2 (Table S4). Buccal mucosa (7.7%) and soft palate (4.6%) were the most commonly affected mucosal sites. One patient had involvement of the nose, hard palate, lower gingiva, and anogenital region, with a clinical score of 2, in addition to extensive skin lesions. Notably, no lesions were detected in eyes, floor of the mouth, or posterior pharynx. Pigmentation was noted in 47.7% of patients, predominantly on arms and legs (36.9% each) (Table S5).
These findings were consistent with BP cohort 2, where arms (77%) and legs (75.8%) were again the most common sites for blistering/erosions, followed by back/buttocks, feet, hands, and chest (Figure 1A, Table S2). Similarly, legs, arms, and feet were the most severely affected areas. The severity and frequency of erythematous/urticarial lesions (Figure 1B, Table S3) and the pattern of mucosal involvement (Table S4) closely mirrored the observations from BP cohort 1.
3.2. Trunk and Buccal Mucosa Are Predilection Sites in PV
In PV, mucosal lesions primarily affected the buccal mucosa (53.7%), while eyes were not affected (Figure 2B, Table S6). For cutaneous blisters/erosions, the most common and severely affected areas were back/buttocks (38.8%), chest (37.3%), abdomen (37.3%), arms (25.4%), and face (22.4%) (Figure 2A, Table S7). As anticipated, no ocular involvement was found in PV patients.
3.3. Trunk and Face Are Predilection Sites for Skin Blistering in PF
In PF, skin blistering predominantly affected the back/buttocks, face, abdomen, and chest (Figure 3, Table S7). As expected, no mucosal involvement was observed in PF.
3.4. AIBD Antigen Expression Shows Slight Variations in Different Skin and Mucosal Regions
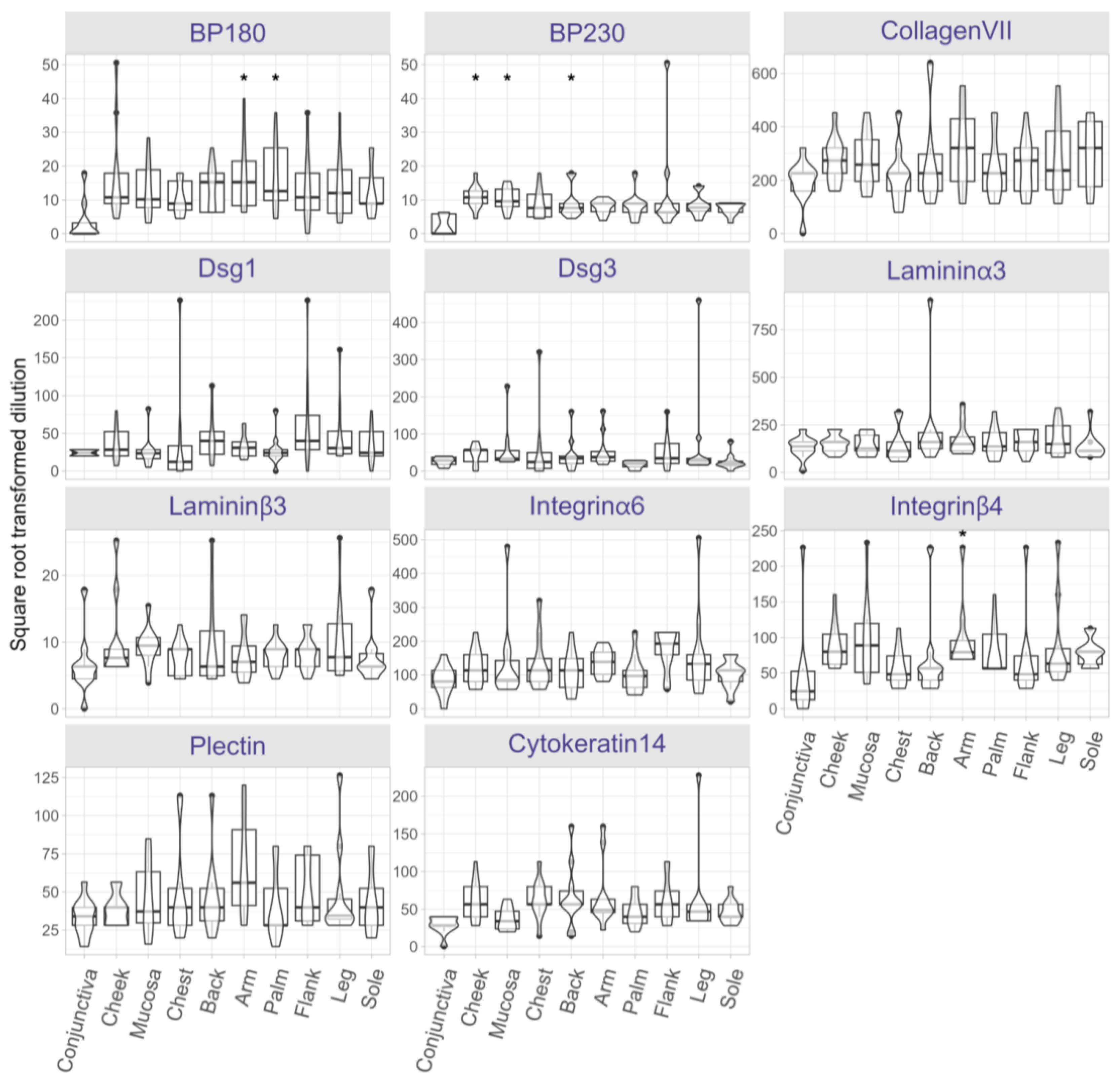
To evaluate AIBD antigen expression across clinical predilection sites, antigen distribution was semi-quantified on skin and mucosal tissues obtained from 13 distinct anatomical sites of ten post-mortem body donors. The endpoint titer (i.e., highest titer) for each antibody was determined at each body site (Figure S1). Following correction for multiple comparisons using the Holm method, statistically significant differences (adjusted P < 0.05) were found for BP230, BP180, and integrin β4. Across all sites, BP180 expression was significantly higher in skin biopsies from arms (P = 0.0003) and palms (P = 0.0007) compared to conjunctiva (Figure 4). BP230 expression was more abundant in cheek (P = 0.00002), oral mucosa (P = 0.00004), and back (P = 0.0091) relative to conjunctiva. Additionally, integrin β4 expression was significantly higher in arms (P = 0.0007) compared to conjunctiva. No significant differences in the expression of other antigens were found between the body sites.
3.5. Expression Levels of AIBD Antigens Do Not Correlate with Clinical Scores
Lastly, we explored the correlation between antigen expression and clinical disease severity scores. We compared BP180, BP230, and integrin β4 expression in regions corresponding to BPDAI and PDAI scoring sites (e.g., conjunctiva, cheek, oral mucosa, chest, back/buttocks, arms, and legs). Despite the observed regional differences in antigen levels, no significant correlation was found between antigen expression and BPDAI/PDAI scores, suggesting that other factors may influence lesion severity and distribution.
4. Discussion
Blister formation in AIBD occurs where structural proteins, targeted by autoantibodies, are expressed. Although these target antigens are broadly distributed in the skin and mucosa, blistering occurs preferentially at specific sites rather than being randomly distributed. The role of regional antigen expression as a determinant of this scattered blistering pattern, however, remains largely unexplored.
In this study, we systematically analyzed the clinical scores of BP patients using the validated BPDAI scoring system. We found that skin blisters/erosions and erythematous/urticarial lesions primarily affected arms and legs, findings that were corroborated in a second BP cohort (cohort 2). In our PV cohort, skin lesions were most prevalent on the back, abdomen, and chest, with buccal mucosa being the most commonly affected mucosal surface. PF patients had skin lesions predominantly on the trunk (back, chest, and abdomen), face, and arms. Of note, the scoring systems used do not differentiate between the upper back and lower back or the buttocks.
Next, we examined antigen expression in different anatomical regions by incubating skin and mucosal tissues with antibodies against AIBD antigens. BP180 expression was significantly higher in arms and palms, while BP230 expression was significantly higher in cheek, buccal/lower labial mucosa, and back compared to conjunctiva. Additionally, higher expression of integrin β4 was observed in arms. Recently, we reported that laminin β4 is highly expressed in extremities and trunk [15]. Despite these variations, no significant expression differences were seen for other antigens across body sites. Also, we found no correlation between antigen expression (BP180, BP230, and integrin β4) and BPDAI/PDAI clinical scores. This suggests that antigen expression does not fully explain the localized distribution of lesions in AIBD. It is important to note that our antigen expression data came from healthy body donors with no history of AIBD. Our results are consistent with previous studies showing minor proteomic differences of primary human keratinocytes across sex, age, and anatomical location [16]. In contrast, Ioannides et al., demonstrated variability in the distribution, density, and expression of pemphigus antigens between human skin regions [8]. This discrepancy may be due to methodological variations; e.g., Ioannides et al., used patient sera for antibody titration, whereas we used commercially available antibodies.
Several skin disorders are characterized by epidermal changes that affect epidermal thickness. A systematic review by Lintzeri et al., found that, aside from the statistically thicker epidermis in the palmoplantar area, which is adapted to withstand mechanical stress and friction, the epidermis in most anatomical sites showed no significant differences in thickness [17]. Similarly, a review by Xu et al., reported that the palms and soles were notably thicker compared to the head and neck regions [18].
Our study suggests that factors beyond regional variations in antigen expression, such as genetics, epigenetics, microbial, or environmental triggers, may influence where lesions develop in AIBD. We observed that AIBD lesions frequently occur at sites exposed to mechanical stress, such as the extremities in BP and the oral mucosa in PV, likely due to friction-induced immune activation and epidermal disruption. This aligns with findings in experimental epidermolysis bullosa acquisita, where mechanical irritation has been linked to non-healing wounds and chronic inflammation [19]. Epidermal disruption further exacerbates blistering following autoantibody binding and complement activation [20]. Even without epidermal disruption, mechanical irritation via removing the stratum corneum or simple irritation can trigger lesion formation in this model [21].
The role of the human microbiome in skin diseases has recently gained interest [22]. Different body sites harbor distinct microbial communities, and conditions like AIBD disrupt this balance, increasing susceptibility to blistering. A study by Belheouane et al., revealed significant differences in the skin microbiota between BP patients and matched controls, with a loss of protective microbes and an increase in Staphylococcus aureus, a pro-inflammatory species [23]. However, the study suggested that the skin microbiota in BP patients is influenced more by disease status than by body site.
Viral infections, particularly herpesviruses, have also been implicated in triggering and exacerbating AIBD, including PV [24], PF [25], and BP [26]. However, the precise link between viral infections and lesion localization remains uncertain.
Additionally, UV-induced cell damage has been proposed as a trigger for autoimmune responses, impairing the skin barrier and causing blister formation [27]. For instance, Kano et al., demonstrated that UV-irradiated sites in photoinduced PF exhibited increased autoantibody binding, potentially leading to acantholysis [28]. Similarly, pemphigus lesions often appear in sun-exposed areas, likely due to enhanced antigen expression and UV-induced autoantibody binding [29]. BP lesions may develop on pre-existing psoriatic lesions, possibly triggered by UVB and PUVA exposure [30,31]. BP has also been observed following burns, skin grafts, trauma, surgical wounds, or scabies [32,33,34,35,36,37,38], with the affected areas becoming immunocompromised and susceptible to secondary diseases, such as localized BP, for varying periods ranging from days to decades [39].
Anatomical variations in lesion localization may also be influenced by the immune microenvironment. Tertiary lymphoid structures form in response to immunological needs, generating local immune responses [40]. During cutaneous acquired immune responses, T cells, dendritic cells, and perivascular macrophages form a leukocyte-clustering structure called the inducible skin-associated lymphoid tissue in the dermis [41], serving as a site for antigen presentation [42]. A recent study has shown tertiary lymphoid structures with Dsg-specific B cells in chronic pemphigus blisters [43], suggesting that chronic lesions may be caused by autoantibodies secreted by lesion-resident cells and inflammation mediated by T cell subsets [44]. In vitiligo, anatomically defined subsets of dermal fibroblasts exhibit distinct chemokine expression that recruits CD8+ cytotoxic T cells and drives the characteristic depigmentation pattern [45]. Whether similar immune mechanisms contribute to AIBD remains to be explored.
Genetic factors may also influence lesion localization [46]. For instance, certain gene mutations in inflammatory bowel disease, such as those in the NOD2/CARD15 gene, have been associated with Crohn’s disease. Other genetic factors influence whether the disease affects the colon or the small intestine [47]. At the translational level, scalp psoriasis samples showed increased modulation of genes involved in TNFα/IL-17/IL-22-induced keratinocyte responses compared to that of skin psoriasis samples [48].
In conclusion, our study provides a comprehensive profile of AIBD antigen expression, showing slight regional variations. Lesion localization in AIBD appears to be largely independent of site-specific antigen expression. The interplay between antigen distribution, density, immune response, genetics, and environmental factors is likely to determine blister sites in AIBD patients.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Author Contributions
ES, MH, and SE designed the study; TRL, LM, LR, JP, CK, SE, and SE conducted the experiments and gathered the data; TRL, LM, LR, SS, MH, ES, and SE performed the data analyses and interpretation; HOD, NvB, IW, and ES provided clinical samples; TLR, LM, LR, and SE generated the figures. SE drafted the manuscript, which was reviewed and approved by all authors.
Funding
This research was supported by the German Research Foundation through the Schleswig-Holstein Excellence Cluster Precision Medicine in Chronic Inflammation (DFG EXC 2167/1, TI-3 to ES), the CRU 303 Pemphigoid Diseases (to ES), the CRC 1526 Pathomechanisms of Antibody-mediated Autoimmunity (to ES, MHH, SS), a research grant from the University of Lübeck (J13-2022 to SE), and an individual grant (DFG EM 362/1-1 to SE). Additional support was provided by RTG2633 Defining and Targeting Autoimmune Pre-Disease (to TRL).
Institutional Review Board Statement
The study was approved by the ethics committee of the University of Lübeck (#12-178, 15-051, 18-046, 20-017, 2023-674) and adhered to the Declaration of Helsinki Principles.
Informed Consent Statement
All patients provided informed consent. Human body donors were used with permission under the „Gesetz über das Leichen-, Bestattungs- und Friedhofswesen (Bestattungsgesetz (burial law)) des Landes Schleswig-Holstein from 04th of February 2005 (GVOBI.Schl. -H S.70) as amended on February 16, 2009 (GVOBI.Schl. -H S.56), § 9 Abschnitt (3) (anatomische Leichenöffnung).
Data availability statement
The data supporting the results of this study are available from the corresponding author, SE, upon reasonable request.
Acknowledgments
We are grateful to all the patients and body donors who participated in this study. We thank Vanessa Krull and Roland Krampitz (Department of Dermatology, University of Lübeck, Lübeck, Germany) for excellent technical assistance and help to retrieve patient photographs, respectively. We also acknowledge Dr. Christian Probst (Euroimmun AG, Lübeck, Germany) for providing us with the anti-desmoglein antibodies and Dr. Katharina Boch (Department of Dermatology and Allergy, University Hospital Schleswig-Holstein, Kiel, Germany) for preparing ethical approval for the retrospective analysis of patient photographs.
Conflicts of Interest
ES and NvB have a joint research project and a patent pending with Euroimmun. No other conflicts of interest have been declared.
Abbreviations
Autoimmune blistering diseases (AIBD); basement membrane zone (BMZ); bullous pemphigoid (BP); Bullous Pemphigoid Disease Activity Index (BPDAI); desmoglein (Dsg); epidermal thickness (ET); Pemphigus Disease Area Index (PDAI); pemphigus vulgaris (PV); pemphigus foliaceus (PF)
References
- Zeng, F.A.P. and D.F. Murrell, State-of-the-art review of human autoimmune blistering diseases (AIBD). Vet Dermatol, 2021. 32(6): p. 524-e145.
- Emtenani, S., et al., Mouse models of pemphigus: valuable tools to investigate pathomechanisms and novel therapeutic interventions. Front Immunol, 2023. 14: p. 1169947.
- Schmidt, E., M. Kasperkiewicz, and P. Joly, Pemphigus. Lancet, 2019. 394(10201): p. 882-894.
- Schmidt, E. and D. Zillikens, Pemphigoid diseases. Lancet, 2013. 381(9863): p. 320-32.
- van Beek, N., et al., Incidence of pemphigoid diseases in Northern Germany in 2016 - first data from the Schleswig-Holstein Registry of Autoimmune Bullous Diseases. J Eur Acad Dermatol Venereol, 2021. 35(5): p. 1197-1202.
- Holtsche, M.M., K. Boch, and E. Schmidt, Autoimmune bullous dermatoses. J Dtsch Dermatol Ges, 2023. 21(4): p. 405-412.
- Du, G., et al., Mucous membrane pemphigoid. Autoimmun Rev, 2022. 21(4): p. 103036.
- Ioannides, D., et al., Regional variation in the expression of pemphigus foliaceus, pemphigus erythematosus, and pemphigus vulgaris antigens in human skin. J Invest Dermatol, 1991. 96(2): p. 159-61.
- Borradori, L., et al., Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol, 2022. 36(10): p. 1689-1704.
- Schmidt, E., et al., S2k guideline for the diagnosis of pemphigus vulgaris/foliaceus and bullous pemphigoid. J Dtsch Dermatol Ges, 2015. 13(7): p. 713-27.
- Murrell, D.F., et al., Definitions and outcome measures for bullous pemphigoid: recommendations by an international panel of experts. J Am Acad Dermatol, 2012. 66(3): p. 479-85.
- Joly, P., et al., Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the european academy of dermatology and venereology (EADV). J Eur Acad Dermatol Venereol, 2020. 34(9): p. 1900-1913.
- Murrell, D.F., et al., Consensus statement on definitions of disease, end points, and therapeutic response for pemphigus. J Am Acad Dermatol, 2008. 58(6): p. 1043-6.
- Hothorn, T., F. Bretz, and P. Westfall, Simultaneous inference in general parametric models. Biom J, 2008. 50(3): p. 346-63.
- Goletz, S., et al., Laminin beta4 is a constituent of the cutaneous basement membrane zone and additional autoantigen of anti-p200 pemphigoid. J Am Acad Dermatol, 2024. 90(4): p. 790-797.
- Sprenger, A., et al., Consistency of the proteome in primary human keratinocytes with respect to gender, age, and skin localization. Mol Cell Proteomics, 2013. 12(9): p. 2509-21.
- Lintzeri, D.A., et al., Epidermal thickness in healthy humans: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol, 2022. 36(8): p. 1191-1200.
- Xu, H., et al., Reference values for skin microanatomy: A systematic review and meta-analysis of ex vivo studies. J Am Acad Dermatol, 2017. 77(6): p. 1133-1144 e4.
- Niebuhr, M., et al., Epidermal Damage Induces Th1 Polarization and Defines the Site of Inflammation in Murine Epidermolysis Bullosa Acquisita. J Invest Dermatol, 2020. 140(9): p. 1713-1722 e9.
- Pinkus, H., Examination of the epidermis by the strip method of removing horny layers. I. Observations on thickness of the horny layer, and on mitotic activity after stripping. J Invest Dermatol, 1951. 16(6): p. 383-6.
- Hundt, J.E., et al., Visualization of autoantibodies and neutrophils in vivo identifies novel checkpoints in autoantibody-induced tissue injury. Sci Rep, 2020. 10(1): p. 4509.
- Carmona-Cruz, S., L. Orozco-Covarrubias, and M. Saez-de-Ocariz, The Human Skin Microbiome in Selected Cutaneous Diseases. Front Cell Infect Microbiol, 2022. 12: p. 834135.
- Belheouane, M., et al., Characterization of the skin microbiota in bullous pemphigoid patients and controls reveals novel microbial indicators of disease. J Adv Res, 2023. 44: p. 71-79.
- Tufano, M.A., et al., Detection of herpesvirus DNA in peripheral blood mononuclear cells and skin lesions of patients with pemphigus by polymerase chain reaction. Br J Dermatol, 1999. 141(6): p. 1033-9.
- Fernandes, N.C., et al., Refractory pemphigus foliaceus associated with herpesvirus infection: case report. Rev Inst Med Trop Sao Paulo, 2017. 59: p. e41.
- Jang, H., et al., Bullous pemphigoid associated with chronic hepatitis C virus infection in a hepatitis B virus endemic area: A case report. Medicine (Baltimore), 2018. 97(15): p. e0377.
- Sanchez-Palacios, C. and L.S. Chan, Development of pemphigus herpetiformis in a patient with psoriasis receiving UV-light treatment. J Cutan Pathol, 2004. 31(4): p. 346-9.
- Kano, Y., et al., Pemphigus foliaceus induced by exposure to sunlight. Report of a case and analysis of photochallenge-induced lesions. Dermatology, 2000. 201(2): p. 132-8.
- Safadi, M.G., et al., Pemphigus vulgaris and foliaceus localized to the nose: Report of 2 cases. JAAD Case Rep, 2021. 15: p. 129-132.
- George, P.M., Bullous pemphigoid possibly induced by psoralen plus ultraviolet A therapy. Photodermatol Photoimmunol Photomed, 1995. 11(5-6): p. 185-7.
- Wilczek, A. and M. Sticherling, Concomitant psoriasis and bullous pemphigoid: coincidence or pathogenic relationship? Int J Dermatol, 2006. 45(11): p. 1353-7.
- Massa, M.C., R.J. Freeark, and J.S. Kang, Localized bullous pemphigoid occurring in a surgical wound. Dermatol Nurs, 1996. 8(2): p. 101-3.
- Danescu, S., et al., Role of physical factors in the pathogenesis of bullous pemphigoid: Case report series and a comprehensive review of the published work. J Dermatol, 2016. 43(2): p. 134-40.
- Lo Schiavo, A., et al., Bullous pemphigoid initially localized around the surgical wound of an arthroprothesis for coxarthrosis. Int J Dermatol, 2014. 53(4): p. e289-90.
- Neri, I., et al., Bullous pemphigoid appearing both on thermal burn scars and split-thickness skin graft donor sites. J Dtsch Dermatol Ges, 2013. 11(7): p. 675-6.
- Ghura, H.S., G.A. Johnston, and A. Milligan, Development of a bullous pemphigoid after split-skin grafting. Br J Plast Surg, 2001. 54(5): p. 447-9.
- Moro, F., et al., Bullous Pemphigoid: Trigger and Predisposing Factors. Biomolecules, 2020. 10(10).
- Konishi, N., et al., Bullous eruption associated with scabies: evidence for scabetic induction of true bullous pemphigoid. Acta Derm Venereol, 2000. 80(4): p. 281-3.
- Baroni, A., et al., Localized bullous pemphigoid occurring on surgical scars: an instance of immunocompromised district. Indian J Dermatol Venereol Leprol, 2014. 80(3): p. 255.
- Jones, G.W. and S.A. Jones, Ectopic lymphoid follicles: inducible centres for generating antigen-specific immune responses within tissues. Immunology, 2016. 147(2): p. 141-51.
- Honda, T., G. Egawa, and K. Kabashima, Antigen presentation and adaptive immune responses in skin. Int Immunol, 2019. 31(7): p. 423-429.
- Kabashima, K., et al., The immunological anatomy of the skin. Nat Rev Immunol, 2019. 19(1): p. 19-30.
- Han, D., et al., Microenvironmental network of clonal CXCL13+CD4+ T cells and Tregs in pemphigus chronic blisters. J Clin Invest, 2023. 133(23).
- Xu, C., et al., Integrative single-cell analysis reveals distinct adaptive immune signatures in the cutaneous lesions of pemphigus. J Autoimmun, 2023. 142: p. 103128.
- Wang, S., et al., Plasma levels of D-dimer and fibrin degradation products correlate with bullous pemphigoid severity: a cross-sectional study. Sci Rep, 2021. 11(1): p. 17746.
- Olbrich, M., et al., Genetics and Omics Analysis of Autoimmune Skin Blistering Diseases. Front Immunol, 2019. 10: p. 2327.
- Zhang, Y.Z. and Y.Y. Li, Inflammatory bowel disease: pathogenesis. World J Gastroenterol, 2014. 20(1): p. 91-9.
- Ruano, J., et al., Molecular and Cellular Profiling of Scalp Psoriasis Reveals Differences and Similarities Compared to Skin Psoriasis. PLoS One, 2016. 11(2): p. e0148450.
Figure 1.
Skin blisters/erosions and erythematous/urticarial lesions occur predominantly on arms and legs in bullous pemphigoid patients. (A) Arms and legs were the most frequently and severely affected sites by skin blisters/erosions, followed by back/buttocks, abdomen, feet, hands, and chest. (B) Erythematous/urticarial lesions were predominantly observed on arms, followed by legs and trunk. Data include both BP cohorts (n = 105).
Figure 1.
Skin blisters/erosions and erythematous/urticarial lesions occur predominantly on arms and legs in bullous pemphigoid patients. (A) Arms and legs were the most frequently and severely affected sites by skin blisters/erosions, followed by back/buttocks, abdomen, feet, hands, and chest. (B) Erythematous/urticarial lesions were predominantly observed on arms, followed by legs and trunk. Data include both BP cohorts (n = 105).
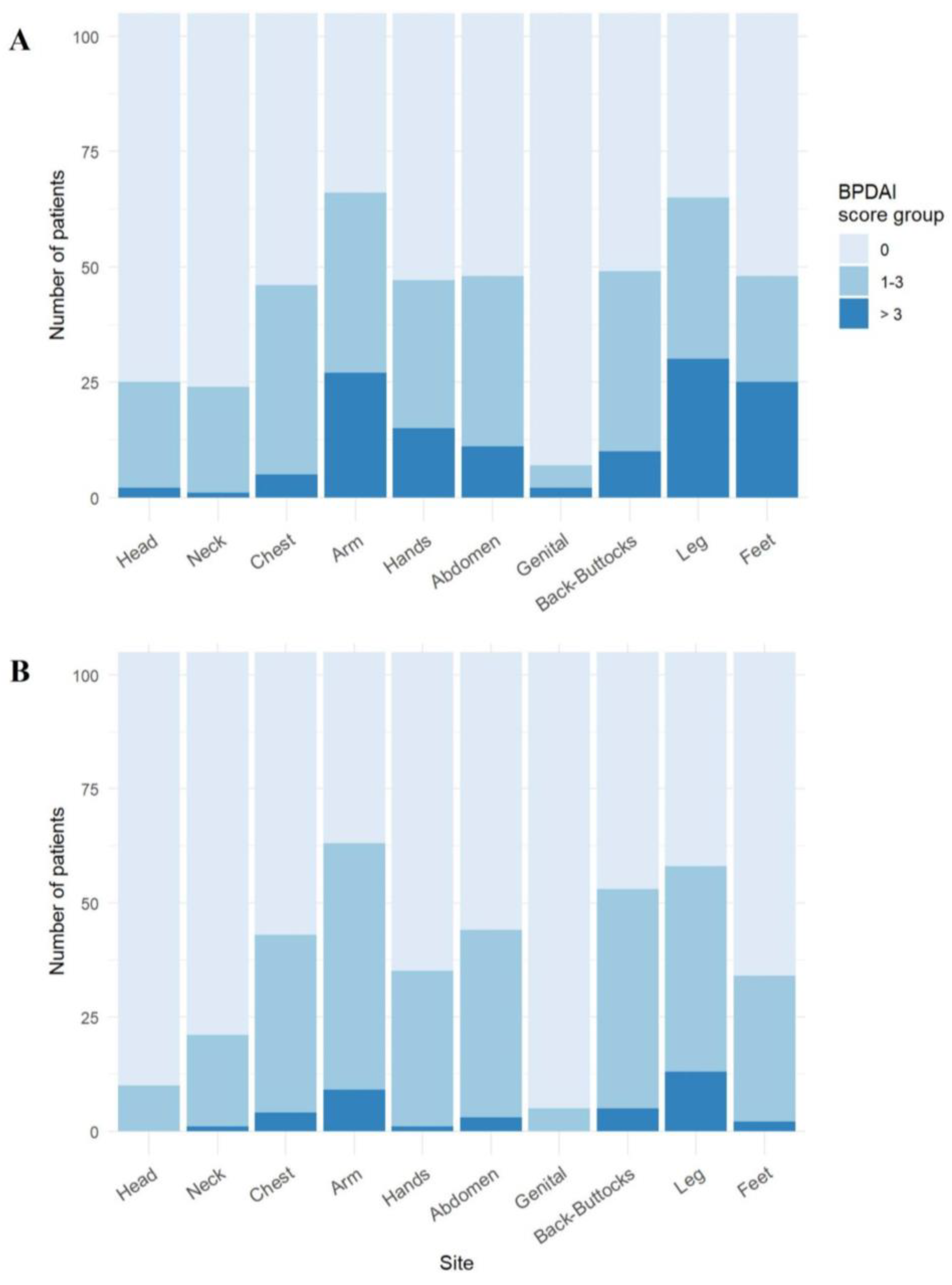
Figure 2.
Trunk and buccal mucosa are the most frequently and severely affected sites in pemphigus vulgaris. (A) In PV patients (n = 67), the trunk area, including back/buttocks, chest, and abdomen, was the most affected by skin blisters. (B) Mucosal involvement was predominantly seen in buccal mucosa and gingiva, with additional lesions in the nasal and genital areas.
Figure 2.
Trunk and buccal mucosa are the most frequently and severely affected sites in pemphigus vulgaris. (A) In PV patients (n = 67), the trunk area, including back/buttocks, chest, and abdomen, was the most affected by skin blisters. (B) Mucosal involvement was predominantly seen in buccal mucosa and gingiva, with additional lesions in the nasal and genital areas.
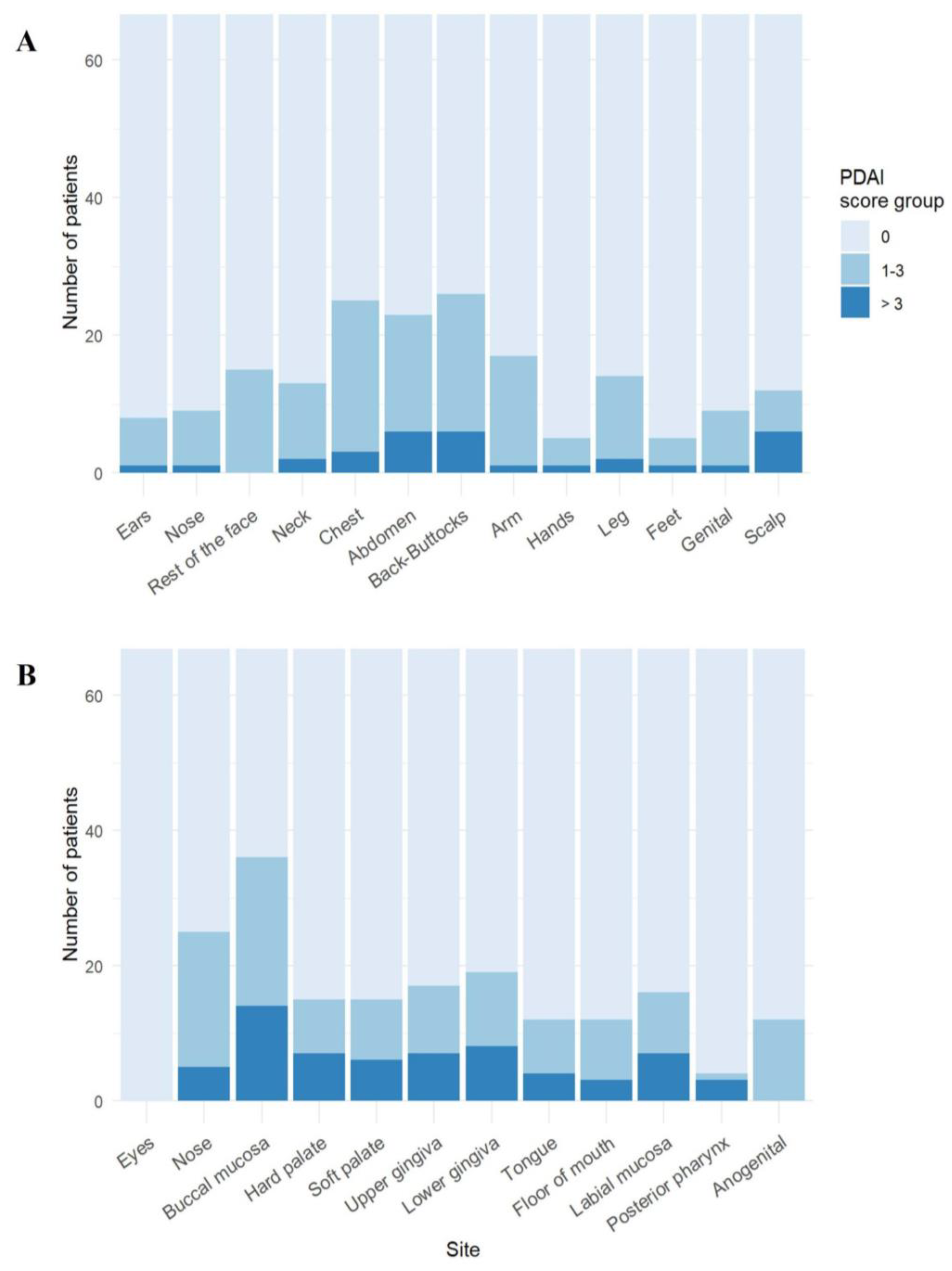
Figure 3.
Pemphigus foliaceus skin lesions mainly affect trunk and face. In the PF cohort (n = 20), the trunk and face were the primary areas affected by skin lesions.
Figure 3.
Pemphigus foliaceus skin lesions mainly affect trunk and face. In the PF cohort (n = 20), the trunk and face were the primary areas affected by skin lesions.
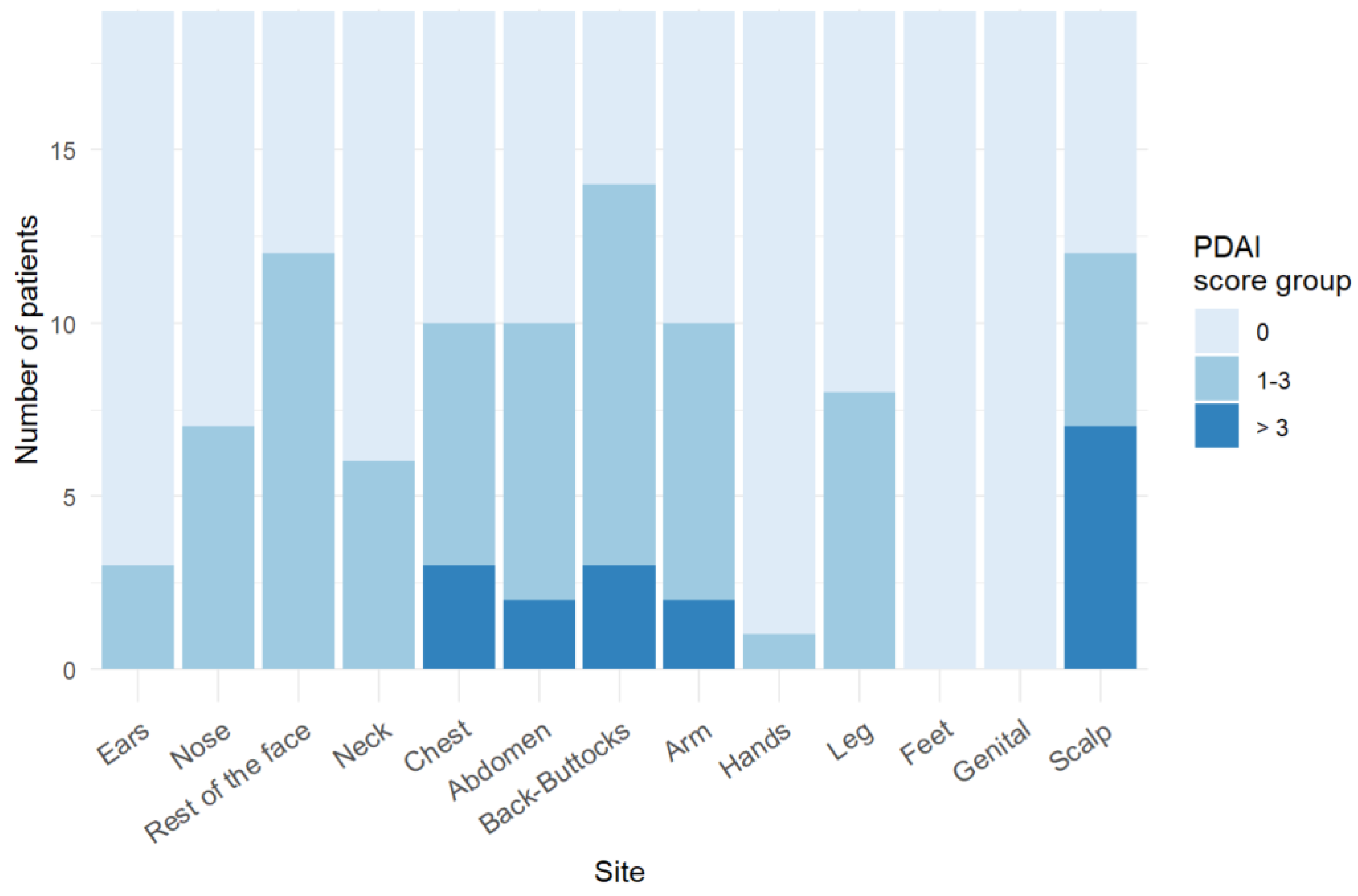
Figure 4.
Protein expression landscape reveals slight variations in AIBD antigen expression across skin and mucosal regions. Protein expression of AIBD antigens was assessed in skin and mucosal tissue sections using serial dilutions of BP180, BP230, collagen VII, desmoglein (Dsg) 1, Dsg3, laminin α3, laminin β3, integrin α6, and integrin β4, plectin, and cytokeratin 14. Notable differences include significantly higher BP180 expression in skin biopsies from arms (P = 0.0003) and palms (P = 0.0007) compared to conjunctiva, which had the lowest expression. BP230 expression was significantly higher in cheek (P = 0.00002), oral mucosa (P = 0.00004), and back (P = 0.0091) relative to conjunctiva. Likewise, integrin β4 expression was significantly higher in arms (P = 0.0007) versus conjunctiva. Other antigens displayed no significant regional differences. Significant expression differences are marked with an asterisk.
Figure 4.
Protein expression landscape reveals slight variations in AIBD antigen expression across skin and mucosal regions. Protein expression of AIBD antigens was assessed in skin and mucosal tissue sections using serial dilutions of BP180, BP230, collagen VII, desmoglein (Dsg) 1, Dsg3, laminin α3, laminin β3, integrin α6, and integrin β4, plectin, and cytokeratin 14. Notable differences include significantly higher BP180 expression in skin biopsies from arms (P = 0.0003) and palms (P = 0.0007) compared to conjunctiva, which had the lowest expression. BP230 expression was significantly higher in cheek (P = 0.00002), oral mucosa (P = 0.00004), and back (P = 0.0091) relative to conjunctiva. Likewise, integrin β4 expression was significantly higher in arms (P = 0.0007) versus conjunctiva. Other antigens displayed no significant regional differences. Significant expression differences are marked with an asterisk.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



