1. Introduction
The rate of postpartum depression (PPD) along with other disorders are reach from 12.9 till 20.4% [
1,
2]. When not diagnosed in time, PPD could cause harmful effects on mothers, newborns and their relatives. Although many studies explore different roles of natural and synthetic oxytocin (synOT) hormone in intrapartum period, until present, no other studies are convincing regarding the association between OT and PPD [
3]. Therefore, more animal studies have been made on association between OT and normal maternal behaviour [
4,
5], or postpartum depressive symptoms [
6,
7]. These studies suggest that the use of synOT in intrapartum could have long-time positive consequences on mothers and on the bond between mothers and newborns. This led to introduction of OT in practice as potential therapeutic benefits in order to achieve different psychiatric disorders [
8,
9]. The level of OT in maternal human plasma have been associated with emotional binding [
10], including mother-to-child attachment. Recent research accentuates the role of perinatal stages in OT and depression binding [
11]. Although there is an interest in OT use as a potential target in PPD, little information exists on the use of synOT in clinical practice. Starting with 1950s the synOT has been used for augmentation or labor induction including postpartum hemorrhage prevention [
12].
For these reasons, there is a need in growing demand for improving PPD therapies. Today, first-line therapies include psychotherapy or talk therapy along with social healthcare [
13] although available therapies are having under 50% rate of success in severe cases [
14]. Together with this therapies synOT is included, which is a hormone with different potential in promoting the positive behaviour, and social memories [
15]. It was shown that in patients with anxiety, a single synOT does attenuate negative thoughts in stressful situations [
16]. With all this, World Health Organization recommend that synOT should be used only in the active phase of labor [
17].
Interestingly, one study found that the prevalence of depressive symptoms in the postpartum period was found significantly higher than its incidence in late pregnancy. Although depression symptoms reached the highest level in the 12th week, the late pregnancy OT level was significantly higher than the postpartum OT level. Therefore, applying linear regression analysis for this study, it was showed that there was a negative relationship model between PPD symptoms and the late pregnancy OT level [
18].
Another study sustained the opposite effect, in which women exposed to synOT were more likely to have depressive symptoms in the postpartum period. The results show that there is a difference in natural and synOT, in which synOT do not present effects on neuroendocrine mechanisms of the brain, without influencing the maternal mood [
19]. In the same context, synOT is the only able to cross the placenta and downregulate fetal OT receptors [
20]. Further, synOT have been also shown to elicit uterine hyperstimulation, giving a reverse impact on fetal oxygen saturation [
21]. However, there are mixed evidence until present [
22] although
synOT administered intrapartum showed that it doesn’t affect maternal mood immediately but only after weeks after childbirth in order to protect mothers from developing PPD symptoms. The same study suggest that women exposed to intrapartum synOT would be at a lower risk of early postpartum mood named maternity blues and then PPD, comparing to women without such exposure. Further, this shows that synOT effects would be more obvious immediately after delivery which attenuate over time [
22]
.
Although the results of some studies are conflicting, Zhu et al. [
23] showed that synOT might improve the cognition of women with postpartum depression to their infants. Further randomized controlled trials with larger samples and more careful assessment are needed to better reveal its efficacy on PPD [
23].
Given the importance of the increasing rates of synOT use nowadays, it is fundamental to better understand the influence of synOT on the well-being of women after birth. The objective of this study was to examine the association between intrapartum synOT administration and maternal development of PPD in the 2nd day postpartum.
2. Materials and Methods
2.1. Study Design and Participants
We conducted an observational prospective study on women observed on the delivery time, and on immediate postpartum period, who delivered in our Department of Obstetrics & Gynecology. All participants were informed regarding the aims and procedures, that the questionnaire was voluntary and confidential. The participants had the possibility to withdraw from the study at any point. Before study starts, we obtained the informed consent from all participants in the study. Between August 2019 and April 2021, we included 904 women from 2
nd day after delivery. Participants were recruited by convenience and mothers were allocated into two groups according to the presence or absence of PPD using Edinburgh Postnatal Depression Scale (EPDS) [
24]: women with PPD (n=236) and controls (i.e., women without PPD, n=668).
2.2. Demographic Characteristics
The demographic and clinical features of the analyzed women concerning age, parity, ethnicity, delivery type, and postpartum hospitalization days were extracted from electronic and medical file records.
2.3. Inclusion and Exclusion Criteria
We included 18-45 years old women, without an identified physical or mental abnormality, who delivered a single baby. We excluded women (1) ages less than 18 and more than 45; (2) with multiple pregnancies; (3) who had a psychiatric disorder which required or not treatment; (4) with alcohol or drug abuse; (5) who doesn’t accept to be involved in the study; and (6) who couldn’t read or speak Romanian language. All the participants completed the EPDS questionnaire.
2.4. Intrapartum Synthetic Oxytocin
In intrapartum period, synOT was administrated intravenous at selected women including but not limited to augmentation or labor induction by synOT when natural labor had or had not begun. This was registered as ‘yes’ and ‘no’, and the exact dose was provided depending on medical need. These data were extracted from medical file records entered by our specialists.
All participants were informed of the aims and procedures and had the option to withdraw from the study at any time. The study was conducted in accordance with the Helsinki Declaration on Human Rights and the informed consent from all participants in the study as well as the Agreement of the Ethics Commission (No. 29726/31.05.2021) were obtained.
2.5. Statistical Analysis
Statistical analysis in this study was carried out utilizing IBM SPSS statistics software version 28 as well as Microsoft Excel. The analytical techniques employed included descriptive statistics, represented in the form of graphs, and statistical assessments. Data were presented in various formats: mean, and standard deviation were used for continuous variables, and counts and percentages were used for categorical variables. In terms of hypothesis testing, we employed various tests, namely the Independent Samples Mann-Whitney U test (for non-normally distributed data), Independent Samples T-test, and Chi-Square Test for the comparison of proportions. The choice of the test depended on the nature of the variables under analysis. The level of significance was predetermined at < 0.05.
3. Results
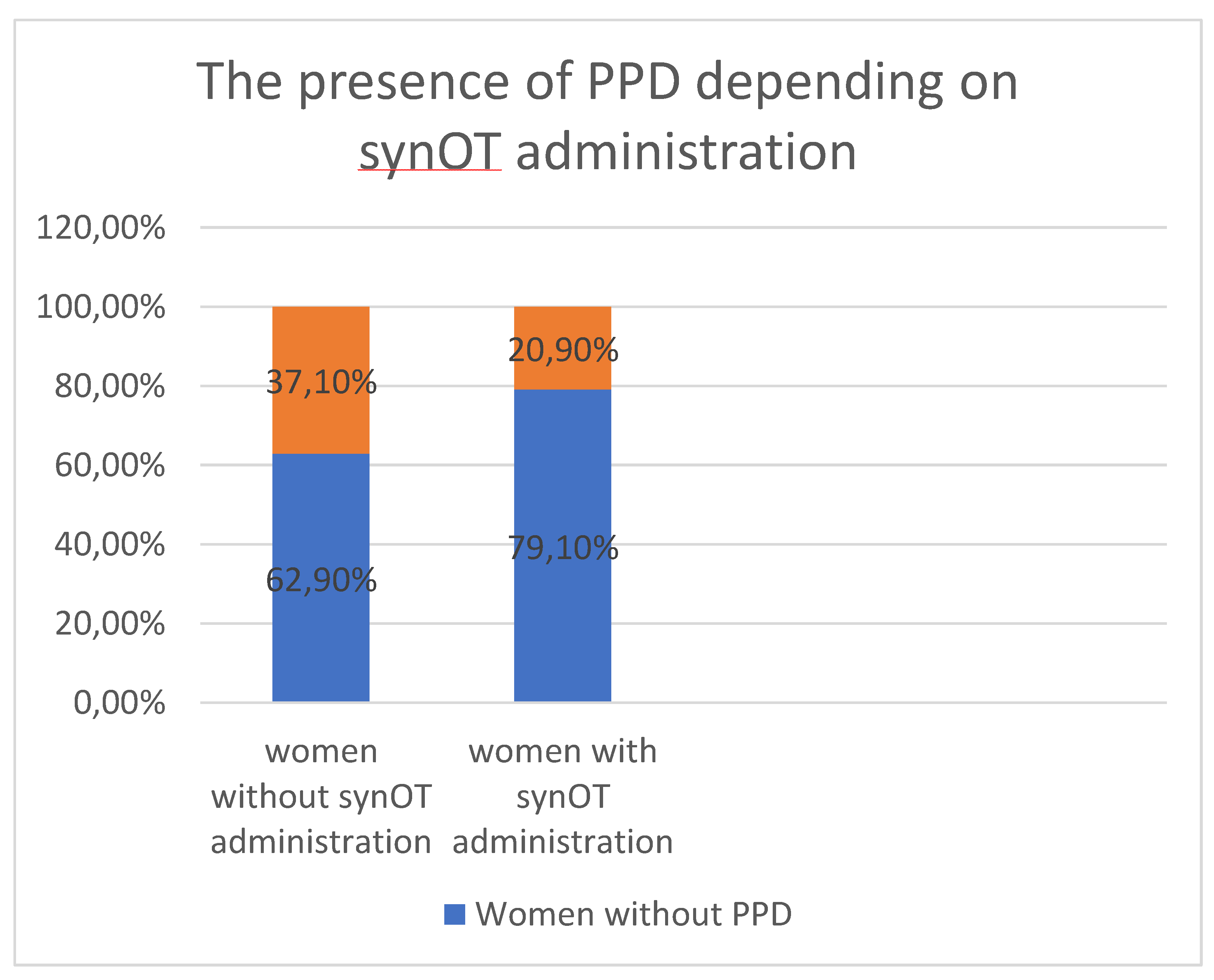
From the total number of patients (n=904), the presence of PPD was detected in 26.10% (n=236) women. Our results showed that from the total of 904 women involved in the study, 609 (32.63%) women received synOT and 295 (67.36%) women did not receive synOT. Therefore, it was shown that the rate of PPD was lower in women with synOT administration, in comparison with the women without synOT administration (20.9% vs. 37.10%, p<0.001), being statistically significant. SynOT was administrated at selected women for induction of labor (
Figure 1). Therefore, the administration of synOT seems to decrease the appearance of PPD in such women in comparison with the women who did not receive synOT in intrapartum period.
The demographic characteristics of participants with or without intrapartum synOT administration are represented in
Table 1.
The mean age of the women with synOT administration was younger in comparison with women without synOT administration (29.2 vs. 27.4, p<0.001), being statistically significant, sustaining the fact that mothers with older ages are more suspected to develop PPD.
Our results showed also that women with synOT administration were primiparous in comparison with women without synOT administration in which were secundiparous (i.e., 53.85% vs. 49.83%, p<0.001), being statistically significant. Therefore, the results suggest that the higher the parity, the higher the depression rate. From the women with synOT administration, 25.94% were secundiparous and about 20.19% were women with 3 or more deliveries. From the women without synOT administration, 36.94% were primiparous and only 13.21% were had 3 or more deliveries.
The number of Romanian women were similar in both groups of women with or without synOT administration (i.e., 80.4% vs. 86.4%, p=0.01), being statistically significance. Although other different ethnicities can also be found, the prevalence was higher from Romanian women. From the women with synOT administration, 13.3% were Gypsy, Russian and Syrian women had the same values (i.e., 0.16%) and 5.9% were Turkish women. From the women without synOT administration, there were seen similar values for Gypsy and Turkish women (i.e., 6.77%), without any Russian or Syrian women.
There was also a statistical significance between delivery types from both women groups. The major of the women with synOT administration had a spontaneously vaginal delivery in comparison with the women without synOT administration (i.e., 74.38% vs. 6.77%, p<0.001). The rate of caesarean section was 25.91% for women with synOT administration and 93.22% for women without synOT administration. This shows that spontaneously delivery have somehow a more protective role in PPD in comparison with caesarean section.
It was noted that women with synOT administration were having less hospitalization days in comparison with women without synOT administration (i.e., 0.43% vs. 0.93%, p<0.001). This shows also that the administration of synOT could be involved in more advanced recovery of the mothers after birth.
4. Discussion
There is still an aversion in the use of antidepressants in PPD treatments, knowing the side effects or the incapability in using it during breastfeeding [
25]. Such reasons make OT an important candidate in mothers with PPD, being a natural hormone involved in birth, mother-newborn bonding and breastfeeding. Currently, OT is involved in emotion regulation [
26], emotion recognition [
27] facial communication [
28] or eye contact [
29]. After daily OT administration together with 12 sessions of weekly course of psychotherapy, Clarici and contributors [
30] assessed depression symptoms, without any significant differences in low mood between synOT administration and controls.
When advised used, synOT has immediate medical benefits. By mimicking the body’s natural OT system, it shows to stimulates contractions and prevents postpartum hemorrhage. No evidence-based guidelines regarding the dose or patient response exist, and the decision to administer synOT is taken more subjective [
31]. Possible synOT risks associated include uterine hyperstimulation and fetal distress, including abnormal fetal heart rate and uterine rupture [
32].
Although the effect of synOT as an antidepressive and anxiolytic mediator, this could be due to many results achieved with intranasal administration in which clinical trials use a standard dose, ranging from 18 to 40 IU [
33], whereas the dose in our investigation was determined by medical need. It could be possible that the effects of synOT on different receptors are moderated by gender, dose and the time of application. Moreover, the effects of synOT on social cognition and social integration are nuanced, depending in the end on the individual personal behaviour [
34]. Therefore, the same may apply to the effect of synOT on general mental health. Though our findings are preliminary and effects may be small, these results point to a need for further investigation of these associations in larger cohort studies. This synOT feature could also inform future policy concerning usage in labor management at specifically dose and timing [
34].
The exact role of synOT administration in intrapartum period and the association with PPD is still scarce nowadays. Some studies investigate the bond between maternal plasma OT and depressive symptoms [
35]. Therefore, one study aimed to use lactation as a physiologic challenge to quantify the extent to which feelings, stress and anxiety symptoms are associated with reduced OT during breastfeeding. The authors followed the expected OT levels in all breastfeeding women, in which OT rose immediately after the beginning of the feed [
35].
Interestingly, it was shown that one single dose of synOT administered during labor was firmly correlated with both endogenous OT levels and depression at 2 months postpartum [
36]. Furthermore, in breastfeeding women, lower doses of synOT were observed compared with exclusively formula-feeding women at 2 months postpartum. In contrary, higher synOT dose was associated with significantly greater symptoms of depression, anxiety, and somatization at 2 months postpartum [
36].
The data suggest that intrapartum synOT administration may have negative effects on mother’s mood only after several weeks after birth, in which depression following treatments were measured just one time [
37]. Moreover, this analysis showed that synOT measured across different regions could have different implications on full-term delivery spectrum [
38]. Considering the fact that 22% of births are induced by using synOT administration from 4 million of total birth from the United States since 2014 [
39], little research has been follow-up around synOT impact or as potential mediation on PPD. Our study showed that intrapartum exposure to synOT may alleviate the risk of developing PPD symptoms in new mothers with higher impact (p<0.001). Moreover, women with synOT administration were much younger, and the major of them were primiparous in comparison with those without synOT administration (p<0.001). The major of the women were Romanian women and had spontaneously delivery in comparison with those without synOT administration (p<0.001) and less postpartum hospitalization days (p<0.001).
In contradiction with our study, the results of Kroll-Desrosiers and contributors [
19] and Gu and contributors [
36], found that women with intrapartum synOT administration were at a higher risk of depression and anxiety than women without synOT administration. This mismatch could be explained by a different synOT dosage in intrapartum period. When synOT was used suboptimally, it led to an excessively short and painful labor or, on the contrary, to a longer labor with complications associated with PPD [
40]. Therefore, the association between synOT administration and PPD appearance could be indicated by each birth experience. However, it seems that women who evaluated their birth experience positively were at a lower risk of PPD provided that they received synOT, in comparison with the women which saw their childbirth experience as negative. Interestingly, the study of Hinshaw et al. [
41] showed that nulliparous women with primary dysfunctional labour, and synOT induction it was showed that it doesn’t reduce caesarean section or short-term postnatal depression. However, synOT administration showed to shortens labour and may reduce operative vaginal deliveries.
Our study did not measure endogen OT also in these analysed women with or without synOT administration. It has been wised to compare the endogen and synOT at the same women sample, considering the fact that endogenous level of OT is at higher risk of PPD than recommended synOT administration. However, larger studies should assess PPD at different points in time, measuring also both endogenous and synOT in mothers. In this way, the results could shed more light on the association between synOT and PPD.
5. Conclusions
There are specific needs for studies on the impact of intrapartum synOT on maternal PPD, which can be revealed as a potential mediator and would clinically be safer in different labor conditions. However, in our study, intrapartum synOT administration was positively associated with the PPD appearance. The clinical relevance of our study showed a higher impact on a population with an increased risk of PPD.
Author Contributions
Conceptualization, S.O. and V.T.; methodology, S.O. and D.B.; validation, S.O. and V.T.; formal analysis, S.O. and M.R.; data curation, S.O., and D.B.; writing - original draft preparation, S.O. and D.B.; writing - review and editing, S.O., C.D. and V.T.; supervision, V.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Helsinki Declaration on Human Rights. The informed consent from all participants in the study as well as the Agreement of the Ethics Commission from University Emergency County Hospital Constanta were obtained (No 29726/31.05.2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Andersson, A.; Garcia-Argibay, M.; Viktorin, A.; Ghirardi, L.; Butwicka, A.; Skoglund, C.; Bang Madsen, K.; D'onofrio, B.M.; Lichtenstein, P.; Tuvblad, C.; Larsson, H. Depression and anxiety disorders during the postpartum period in women diagnosed with attention deficit hyperactivity disorder. J. Affect. Disord. 2023, 325, 817-823.
- Kendall-Tackett, K.A. Screening for Perinatal Depression: Barriers, Guidelines, and Measurement Scales. J. Clin. Med. 2024, 13, 6511.
- Biaggi, A.; Conroy, S.; Pawlby S.; Pariante, C.M. Identifying the women at risk of antenatal anxiety and depression: A systematic review. J. Affect. Disord. 2016, 191, 62-77.
- Taylor, J.H.; Carp, SB.; French, J.A. Vasopressin, but not oxytocin, modulates responses to infant stimuli in marmosets providing care to dependent infants. Dev. Psychobiol. 2020, 62(7), 932-940.
- Bachner-Melman, R.; Ebstein R.P. The role of oxytocin and vasopressin in emotional and social behaviors. Handb. Clin. Neurol. 2014, 124, 53-68.
- Speranza, L.; Filiz, K.D.; Lippiello, P.; Ferraro, M.G.; Pascarella, S.; Miniaci, M.C.; Volpicelli, F. Enduring Neurobiological Consequences of Early-Life Stress: Insights from Rodent Behavioral Paradigms. Biomedicines 2024, 12, 1978.
- Perani, C.V.; Slattery, D.A. Using animal models to study postpartum psychiatric disorders. British Journal of Pharmacology 2014, 171(20), 4539-4555.
- Kimmel, M.; Clive, M.; Gispen, F.; Guintivano, J.; Brown, T.; Cox, O.; Beckmann, M.W.; Kornhuber, J.; Fasching, P.A.; Osborne, L.M.; Binder, E.; Payne, J.L.; Kaminsky, Z. Oxytocin receptor DNA methylation in postpartum depression. Psychoneuroendocrinology 2016, 69, 150-60.
- Uzefovsky, F.; Shalev I.; Israel, S.; Edelman, S, Raz, Y.; Mankuta, D.; Knafo-Noam, A.; Ebstei,n R.P. Oxytocin receptor and vasopressin receptor 1a genes are respectively associated with emotional and cognitive empathy. Hormones and Behavior 2015, 67, 60–5.
- Pierzynowska, K.; Gaffke, L.; Żabińska, M.; Cyske, Z.; Rintz, E.; Wiśniewska, K.; Podlacha, M.; Węgrzyn, G. Roles of the Oxytocin Receptor (OXTR) in Human Diseases. Int. J. Mol. Sci. 2023, 24, 3887.
- Mohiyeddini, C.; Opacka-Juffry, J. Disentangling the link between depressive symptoms and plasma oxytocin in men: The role of brooding rumination. Hormones and Behavior 2015, 75, 142-149.
- Fields, H.; Greene, J.W.J.; Franklin, R.R. Intravenous pitocin in induction and stimulation of labor: A study of 3754 cases. Obstetrics and Gynecology 1959, 13(3), 353-359.
- Batt, MM.; Duffy, K.A.; Novick, A.M.; Metcalf, C.A.; Epperson, C.N. Is Postpartum Depression Different From Depression Occurring Outside of the Perinatal Period? A Review of the Evidence. Focus (Am Psychiatr Publ). 2020, 18(2), 106-119.
- Dimcea, D.A.M.; Petca, R.C.; Dumitrașcu, M.C.; Șandru, F.; Mehedințu, C.; Petca, A. Postpartum Depression: Etiology, Treatment, and Consequences for Maternal Care. Diagnostics 2024, 14, 865.
- Stroobants, S.; Creemers, J.; Bosmans, G.; D’Hooge, R. Post-weaning infant-to-mother bonding in nutritionally independent female mice. PLoS ONE 2020, 15(1), e0227034.
- Jones, C.; Barrera, I.; Brothers, S.; Ring, R.; Wahlestedt, C. Oxytocin and social functioning. Dialogues Clin. Neurosci. 2017, 19(2), 193-201.
- Westhoff, G.; Cotter, AM.; Tolosa, J.E. Prophylactic oxytocin for the third stage of labour to prevent postpartum haemorrhage. Cochrane Database of Systematic Reviews 2013, 10, 1-93.
- Cevik, A.; Alan, S. Are pregnancy and postpartum oxytocin level a predictive biomarker for postpartum depression? J. Obstet. Gynaecol. Res. 2021, 47(12), 4280-4288.
- Kroll-Desrosiers, A.R.; Nephew, B.C.; Babb, J.A.; Guilarte-Walker, Y.; Moore Simas, T.A.; Deligiannidis, K.M. Association of peripartum synthetic oxytocin administration and depressive and anxiety disorders within the first postpartum year. Depress. Anxiety 2017, 34, 137-146.
- Nilvér, H.; Berg, M. The Birth Companions’ Experience of the Birthing Room and How It Influences the Supportive Role: A Qualitative Study. HERD: Health Environments Research & Design Journal. 2023, 16(3), 156-167.
- Zhou, Y.; Liu, W.; Xu, Y.; Zhang, X.; Miao, Y.; Wang, A.; Zhang, Y. Effects of different doses of synthetic oxytocin on neonatal instinctive behaviors and breastfeeding. Sci. Rep. 2022, 12, 16434.
- Takács, L.; Seidlerová, J.M.; Štěrbová, Z.; Čepický, P.; Havlíček, J. The effects of intrapartum synthetic oxytocin on maternal postpartum mood: findings from a prospective observational study. Arch. Womens Ment. Health 2019, 22(4), 485-491.
- Zhu, J.; Jin J.; Tang, J. Oxytocin and Women Postpartum Depression: A Systematic Review of Randomized Controlled Trials. Neuropsychiatr. Dis. Treat. 2023, 19, 939-947.
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. British Journal of Psychiatry 1987, 150(6), 782-786.
- Pettman, D.; O’Mahen, H.; Blomberg, O.; Svanberg, A.S.; von Essen, L.; Woodford, J. Effectiveness of cognitive behavioural therapy-based interventions for maternal perinatal depression: a systematic review and meta-analysis. BMC Psychiatry 2023, 23, 208.
- Shahrestani, S.; Kemp, AH.; Guastella, A.J. The impact of a single administration of intranasal oxytocin on the recognition of basic emotions in humans: a meta-analysis. Neuropsychopharmacology 2013, 38(10), 1929-1936.
- Whitley, J.; Wouk, K.; Bauer, A.E.; Grewen, K.; Gottfredson, N.C.; Meltzer-Brody, S.; Propper, C.; Mills-Koonce, R.; Pearson, B.; Stuebe A. Oxytocin during breastfeeding and maternal mood symptoms. Psychoneuroendocrinology 2020, 113, 104581.
- Daughters, K.; Manstead, A.S.R.; van der Schalk, J. Oxytocin and emotion recognition: Investigating the possible roles of facial synchrony and eye gaze. Current Research in Ecological and Social Psychology 2021, 2, 100019.
- Auyeung, B.; Lombardo, M.V.; Heinrichs, M.; Chakrabarti, B.; Sule, A.; Deakin, J.B.; Bethlehem, R.A.; Dickens, L.; Mooney, N.; Sipple, J.A.; Thiemann, P.; Baron-Cohen, S. Oxytocin increases eye contact during a real-time, naturalistic social interaction in males with and without autism. Transl. Psychiatry 2015, 5(2), e507.
- Clarici, A.; Pellizzoni, S.; Guaschino, S.; Alberico, S.; Bembich, S.; Giuliani, R.; Short, A.; Guarino, G.; Panksepp, J. Intranasal administration of oxytocin in postnatal depression: implications for psychodynamic psychotherapy from a randomized double-blind pilot study. Front. Psychol. 2015, 6, 426.
- Clark, S.L.; Simpson, K.R.; Knox, GE.; Garite, T.J. Oxytocin: New perspectives on an old drug. Am. J. Clin. Exp. Obstet. Gynecol. 2009, 200(1), 31-36.
- Buckley, S.J. Undisturbed birth: Nature’s blueprint for ease and ecstasy. J. Prenat. Perinat. Psychol. Health 2003, 17(4), 261-288.
- MacDonald, E.; Dadds, M.R.; Brennan, J.L.; Williams, K.; Levi, F.; Cauchi, A.J. A review of safety, side-effects and subjective reactions to intranasal oxytocin in human research. Psychoneuroendocrinology 2011, 36(8), 1114-1126.
- Bartz, J.A.; Zaki, J.; Bolger, N.; Ochsner, K.N. Social effects of oxytocin in humans: Context and person matter. Trends. Cogn. Sci. 2011, 15(7), 301-309.
- Nagel, E.M.; Howland, M.A.; Pando, C.; Stang, J.; Mason, S.M.; Fields, D.A.; Demerath, E.W. Maternal Psychological Distress and Lactation and Breastfeeding Outcomes: a Narrative Review. Clin. Ther. 2022, 44(2), 215-227.
- Gu, V.; Feeley, N.; Gold, I.; Hayton, B.; Robins, S.; Mackinnon, A.; Samuel, S.; Carter, CS.; Zelkowitz, P. Intrapartum synthetic oxytocin and its effects on maternal well-being at 2 months postpartum. Birth 2016, 43(1), 28-35.
- Cuthbert, B.N.; Insel, T.R. Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med. 2013, 11, 126.
- Goetz, L.; Jarvers, I.; Schleicher, D.; Mikan, K.; Brunner, R.; Kandsperger, S. The role of the endogenous oxytocin system under psychosocial stress conditions in adolescents suffering from anxiety disorder: study protocol for a parallel group-controlled trial. BMC Psychol. 2021, 9, 61.
- Hamilton, B.E.; Martin, J.A.; Osterman, M.J.; Curtin, C.S.; Matthews, T.J. Births: Final data for 2014. National Vital Statistics Reports 2014, 64(12), 1-63.
- Simkin, P. Just another day in a woman's life? Women's long-term perceptions of their first birth experience. Part I. Birth (Berkeley, Calif.). 1991, 18(4), 203-210.
- Hinshaw, K.; Simpson, S.; Cummings, S.; Hildreth, A.; Thornton, J. A randomised controlled trial of early versus delayed oxytocin augmentation to treat primary dysfunctional labour in nulliparous women. BJOG 2008, 115(10), 1289-95; discussion 1295-6.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).