
Submitted:
31 October 2024
Posted:
01 November 2024
You are already at the latest version
Abstract
To evaluate the effectiveness of a dual approach involving time-restricted eating (TRE) at different times-of-day combined with physical activity (PA) on functional capacity and metabolic health in overweight or obese women. Random allocation of sixty-one participants into four groups: early time-restricted eating plus physical activity (ETRE-PA, n=15, 31.8±10.56 years, 89.68±10.56 kg, 33.5±5.53 kg/m²), late time-restricted eating with physical activity (LTRE-PA, n=15, 30.60±7.94 years, 94.45±15.36 kg, 34.37±7.09 kg/m²), late time-restricted eating only (LTRE, n=15, 27.93±9.79 years, 88.32±10.36 kg, 32.71±5.15 kg/m²) and a control group (CG, n=15, 36.25±11.52 years, 89.01±11.68 kg, 33.66±6.18 kg/m²). The intervention lasted 12 weeks for all groups. Both ETRE-PA and LTRE-PA groups engaged in a rigorous combined aerobic and resistance-training program. Significant reductions in body weight and body mass index were observed in ETRE-PA and LTRE-PA compared to CG and LTRE groups in post-intervention (p<0.0005). Only ETRE-PA group exhibited a significant decrease in fat mass (p=0.02), low-density lipoprotein cholesterol (p=0.01) and aspartate aminotransferase (p=0.002). Significant reductions in alanine aminotransferase levels were observed in ETRE-PA (p=0.004) and LTRE-PA (p=0.02) groups. These two latter groups achieved higher performances in the 6-min walking test, bench press, 30-second squat, crunch test, vertical jump (p<0.0005 for both) and leg extension (p<0.02 for both) when compared to LTRE and CG groups. In conclusion, the integration of TRE with PA leads to greater improvements in body composition, lipid profile, and physical performance with no significant differences between ETRE-PA and LTRE-PA approaches. This combined strategy offers a promising solution in overweight or obese women.
Keywords:
Time-restricted eating
; circadian rhythms
; metabolic health
; physical performance
1. Introduction
Obesity is a major public health concern with over 2.5 billion adults classified as overweight (body mass index, BMI ≥25 kg/m2) and 890 million with obesity (BMI >30) [1]. The current rise of obesity prevalence [2] is associated with increased risk for chronic illness [3]. Furthermore, it is established that even a small amount of body weight loss can reduce the risk of cardiovascular disease [4]. Up until now, efforts to treat and prevent overweight and obesity through dietary approaches have been focused on decreasing calorie intake and enhancing the overall quality of the diet [5]. However, maintaining these strategies over time has been challenging, leading to limited success. Moreover, research has shown that irregular eating patterns can have negative effects on body’s circadian rhythms regardless of meal size or macronutrient composition [6]. Notably, dietary approaches that prioritize the timing of eating and length of fasting periods known as chrono-nutrition have been shown to enhance metabolic health irrespective of the kind, quality or quantity of foods consumed without necessarily resulting in weight loss [7]. Indeed, intermittent fasting (IF) has become a popular weight loss strategy that involves refraining from ingesting food and caloric beverages for specified times [8,9]. A specialized IF technique called time-restricted eating (TRE) involves regular fasting and eating windows that fall within a 24-hour cycle is highly recommended for persons living with obesity [10]. Earlier studies looked into how TRE might affect body composition [11] and metabolic health markers [12]. While the timing of daily meals in TRE can range from 4 to 12 hours with food intake periods starting either early (ETRE) or later in the day (LTRE). So far, few studies have compared ETRE and LTRE outcomes on metabolic health and fitness [13]. Despite the potential effects of physical exercise on physical fitness and physiological adaptation during fasting, only few studies investigated the combined effect of physical activity and TRE in metabolic disorders [14]. A review by Albosta et al. [15] concluded that endurance exercise practiced in fasted state induced a greater improvement in insulin sensitivity in type 2 diabetes patients comparatively with exercise in fed state. Furthermore, a meta-analysis conducted by Vieira et al. [16] showed that the combination of TRE and aerobic exercise induced greater body weight loss, a decrease in the liver genes related to lipogenesis and an improvement in fatty acid oxidation compared to control group. However, previous studies have highlighted metabolic differences between early and late TRE schedules [17]. Research indicated variability in how each approach impacts circadian rhythms and glucose metabolism, especially concerning breakfast consumption and the timing of exercise relative to the last meal [18]. Early TRE typically concluding in the afternoon, appeared more aligned with circadian rhythms, potentially enhancing insulin sensitivity and glucose control. While late TRE may be less effective in this area despite supporting overall caloric restriction [19]. Moreover, the timing of exercise has a profound impact on metabolic responses. Exercising in fasted state promotes fat oxidation and enhances metabolic flexibility, while postprandial exercise relies more on carbohydrate stores and may affect glucose dynamics after activity [20]. These aspects highlighted the importance of adapting TRE to individual health objective and chronobiological needs.
Moreover, a study by Wilson et al. [21] showed that 12 weeks of intermittent fasting with or without high intensity interval training (HIIT) exercise prevented weight gain and improved lipid profile in obese rats. To the best of the authors’ knowledge, few studies have compared between TRE interventions practiced at different time of day (TOD) combined with PA in overweight or obese women.
Thus, the aim of the present study was to investigate the effect of concurrent (aerobic and resistance) training in combination with ETRE or LTRE on body composition, metabolic profile and functional capacity in overweight or obese women. We hypothesized that exercise intervention associated with ETRE-PA may improve body composition, biomarkers of metabolic profile and functional capacity.
2. Materials and Methods
2.1. Participants
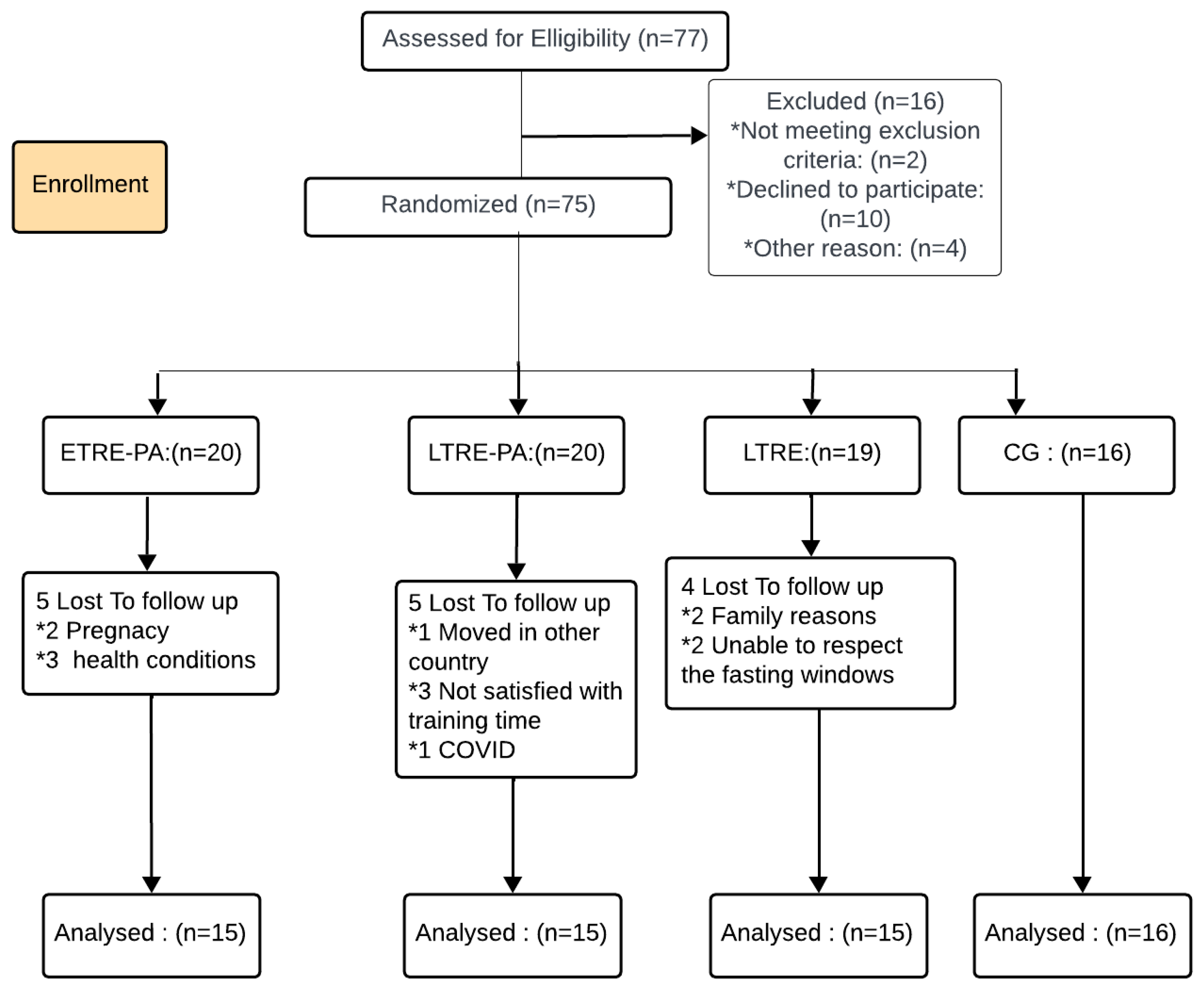
The required sample size was determined a priori using G*Power software, following the recommended procedures by Beck [22] and based on a previous study employing the same paradigm. Statistical power was estimated at 0.85 with an alpha level of 0.05 [23]. A minimum of 40 participants were deemed necessary. This rigorous approach in determining the sample size helps to ensure that the study has sufficient statistical power to detect meaningful effects and to minimize the risk of incurring a type 2 statistical error. Initially, seventy-seven women volunteered to participate in the present study have been recruited. Before agreeing to participate, each participant was provided with a detailed description of the protocol, as well as an explanation of the potential risks and benefits involved. All the participants gave their written informed consent before participating in the study. The inclusion criteria required the participants to have a body mass index greater than 25 kg/m2, to be able to attend laboratory assessment and training sessions, free from any known cardiovascular disease, and not pregnant. Despite an attrition rate of 21%, the study successfully enrolled 61 sedentary women who were overweight or obese. Participants body composition was assessed with a bioelectrical impedance (Model TBF-300, Tanita Corp, Tokyo, Japan) [24]. The study design has been approved by the local ethics committee (CPP SUD, n ° 0460/2022, Sfax, Tunisia, approval date: 16 December 2022) and was registered in the Pan African Clinical Trials Registry PACTR202301473691345 and has been conducted in accordance with the Helsinki guidelines.
Figure 1.
Flow chart of participants’ recruitment. ETRE-PA: Early time-restricted eating combined with physical activity group; LTRE-PA: Late time-restricted eating combined with physical activity group, LTRE: Late time-restricted eating group; CG: Control group.
Figure 1.
Flow chart of participants’ recruitment. ETRE-PA: Early time-restricted eating combined with physical activity group; LTRE-PA: Late time-restricted eating combined with physical activity group, LTRE: Late time-restricted eating group; CG: Control group.
2.2. Study Design
Participants were randomly assigned to one of four groups: ETRE-PA (n=15, 31.8±10.56 years, 89.68±10.56 kg, 33.5±5.53 kg/m²), LTRE-PA (n=15, 30.60±7.94 years, 94.45±15.36 kg, 34.37±7.09 kg/m²), LTRE (n=15, 27.93 ± 9.79 years, 88.32 ± 10.36 kg, 32.71± 5.15 kg/m²) and CG (n=16, 36.25 ±11.52 years, 89.01±11.68 kg, 33.66±6.18 kg/m²). The two experimental groups adhered to a time-restricted eating (TRE) protocol ad libitum and participated in training sessions that combined aerobic exercises with muscle-strengthening activities (Figure 2). The intervention spanned twelve weeks, during which body composition, biochemical and physical performance were measured. The participants of the control group (CG) were advised to maintain their regular daily meal and bedtime routines throughout the study. To ensure consistency, all measurements were taken between 7:00 am and 12:00 pm after a 16-hour fast. The three intervention groups (ETRE-PA, LTRE-PA, and LTRE) received dietary guidelines with specific recommendations on meal timing, daily caloric intake and macronutrient distribution, designed to achieve a total daily intake of 1,200–1,500 kcal. Participants were instructed to consume three daily meals without additional snacks, all within 8-hour period followed by 16-hour fasting period. However, a 4-hour difference was established between the meal timing of ETRE-PA group, LTRE-PA and LTRE groups. Participants in ETRE-PA group were required to abstain from consuming any calories between 4:00 pm and 8:00 am the following day throughout the intervention. In contrast, participants in LTRE-PA and LTRE groups were instructed to follow their customary dietary patterns but within a designated eating window from 12:00 pm to 8:00 pm, allowing an 8-hour period for food consumption while restricting intake outside this timeframe.
2.3. Training Sessions
ETRE-PA and LTRE-PA participants were required to attend all physical training sessions at the fitness center, where they engaged in a 70-minute workout three times a week. Each training session consisted of a comprehensive routine, including warm-up (5 minutes), aerobic exercise (30 minutes), strength training (30 minutes), and stretching and breathing exercises (5 minutes).
2.3.1. Endurance Training
The training program incorporated auditory stimulation and intensity modulation (tempo). Sessions were scheduled three times per week on Monday, Wednesday, and Friday at the end of the feeding window for each group (i.e., at 4:00 pm for ETRE-PA and 8:00 pm for LTRE-PA). The intervention was divided into four phases with progressive increase of intensity within each phase lasting three weeks (nine training sessions). In the first phase, participants exercised for 30 minutes at 50-60% of their estimated maximum heart rate (HRmax: 220—age) with an auditory tempo of 135-140 beats per minute (BPM). The second phase involved exercising for 30 minutes at 55-65% of HRmax with the same tempo. In the third phase, participants exercised for 30 minutes at an intensity of 60-70% of HRmax with a faster auditory tempo of 140-152 BPM. Finally, the fourth phase required participants to exercise for 60 minutes at an intensity of 65-75% of HRmax, with the same tempo as phase three.
2.3.2. Strength Training
The training was structured as circuit weight training, incorporating handheld weights, weight machines (Technogym, Italia), and participants’ own body weight. Each participant engaged in two preliminary training sessions to become familiarized with the equipment and to master the correct techniques for executing the exercises [25].
2.4. Outcome Measures
The study spanned a period of 14 weeks, with the 12-week intervention starting after one week of baseline measures. Throughout this period, all participants maintained their usual dietary intake. Outcome measures were taken at both baseline and post-intervention. Body composition was assessed by measuring total body mass and composition including lean mass, fat-free mass (FFM), bone mass and total water before and after the intervention period, using bioelectrical impedance analysis (Model TBF-300, Tanita Corp, Tokyo, Japan). Measurements were taken in the morning following an overnight fast, with participants dressed simply and without shoes or socks. A wall-mounted stadiometer was used to measure the participants standing height to the nearest 0.1 cm.
2.5. Blood Samples
Blood samples were obtained from antecubital vein after an overnight fasting 16-hour fasting period, between 7:00 and 10:00 am, both three days before and after the intervention. Participants were advised to maintain their regular diet and avoid vigorous physical activity within 48 hours prior to each blood sampling session. The blood samples were immediately placed in an ice bath to prevent degradation and then centrifuged at 2500 rpm for 10 minutes at 4°C. The resulting plasma was divided into smaller aliquots to avoid multiple freeze-thaw cycles and stored at -80°C for 2 weeks until analysis. All measurements were performed using the Cobas 6000 ™ machine from Roche Diagnostics Manheim. The lipid profile variables, including total cholesterol (TC) and triglycerides (TG), were assessed using an enzymatic colorimetric technique. High-density lipoprotein cholesterol (HDL-c) was determined through a direct enzymatic colorimetric method, while low density lipoprotein (LDL-c) levels were calculated using the Friedewald formula:
[LDL] = [TC] − ([HDL] + [TG/2.2]) [26]
For the glycemic profile, fasting blood glucose was measured using an enzymatic hexokinase assay, and insulin levels were assessed using an electrochemical luminescence-based assay. Insulin resistance was quantified using the homeostatic model assessment (HOMA-IR), calculated as [insulinemia (U/mL) × glycemia (mmol/L)] / 22.5. Aspartat aminotransferase (ASAT) and alanine aminotransferase (ALAT) levels were determined using the UV kinetic assay to assess liver function. Total Bilirubin levels were measured using a colorimetric technique, creatinine, was assessed using an enzymatic method. Alkaline phosphatase levels were assessed using a visible kinetic assay, which measures the enzyme’s activity at a wavelength of 405 nm. This method involves monitoring the rate of reaction over time as the substrate is converted into product, allowing for the quantification of alkaline phosphatase activity in the samples. This measurement is crucial for assessing bone and liver health. Finally, C-Reactive protein (CRP), was measured using the immuno-turbidimetric method. All measurements were conducted within a single assay run by the same experienced experimenter.
2.6. Functional Capacity
2.6.1. Six-Minute Walk Test (6MWT)
The 6-minute walk test (6MWT) was conducted to measure functional capacity [27]. During this test, participants were instructed to walk along a 30-meter corridor at their maximum speed for six minutes. The corridor was marked every 5 meters with colored tape to allow for precise measurement of the distance covered (6MWD). Before the test began, participants rested for about 10 minutes on a chair located near the starting point. Blood pressure was measured during this period to establish a baseline value. Once the participants began walking, the stopwatch was started, and each completed lap was recorded when participants returned to the starting point. In addition to the completed laps, any extra distance covered beyond the 30-meter corridor was also recorded using the nearest colored tape marker on the floor. This procedure ensured the collection of accurate and reliable data during the test.
2.6.2. Strength Tests
For strength assessments, we recorded the one repetition maximum (1-RM) for both the bench press and leg press exercises. Each 1-RM assessment was preceded by a specific warm-up routine, which involved performing five repetitions with a weight typically manageable for ten repetitions, following the techniques outlined in previous studies [28,29]. The 1-RM measurements were conducted at the beginning of the study and after 12 training sessions for all prescribed exercises. This allowed us to make necessary adjustments to account for any potential increases in strength that may have occurred during the course of the training program. To estimate 1-RM values, we employed the Epley method, which calculates the 1-RM as follows: 1-RM = Weight Lifted × (1 + 0.0333 × Number of Repetitions) [28].
2.6.3. Vertical Jump Test
To assess lower body explosiveness, a Takei Vertical Jump Meter (Takei, Niigata, Japan) was used. Three maximum attempts were measured with a 30-second rest time between jumps. The participants were encouraged throughout the testing process. The highest jump was selected for additional analysis.
2.6.4. 30 s Crunch and Squat Test
The 30-Second Crunch Test is a simple fitness assessment designed to evaluate the strength and endurance of the abdominal muscles. To conduct the test, the participant lies on a mat with knees bent at a 90-degree angle and feet flat on the floor. The arms are either crossed over the chest. The test begins by engaging the core muscles and lifting the shoulder blades off the ground, raising the upper body towards the knees until the elbows touch the thighs or reach a 30-degree angle. The movement is then reversed to return to the starting position. This action is repeated continuously and rhythmically for 30 seconds, with each complete crunch being counted.
The squat test was used to assess lower body strength and endurance either. Participants were instructed to stand with their feet shoulder-width apart, engage their core, bend their knees, and lower their hips towards the ground. It is important to maintain proper form by keeping the back straight and the knees in line with the toes. Once in a seated position, participants must stand back up by pushing through their heels and engaging their glutes and thigh muscles. The test lasts for 30 seconds, during which participants should aim to complete as many correctly executed squats as possible.
3. Statistical Analysis
Statistical analyses were conducted using SPSS software (v.23, IBM, New York, USA). All data were presented as mean ± standard deviation (SD). Parametric tests were performed after confirming the assumption of normality using the Kolmogorov-Smirnov test. A two-way ANOVA for repeated measures was used to evaluate differences across groups (4 groups (ETRE-PA, LTRE-PA, LTRE, CG) x Two measurement points (before and after the intervention)). This analysis was applied to assess changes in body composition parameters (body weight, BMI, FM, FFM, MM and TBW), cardiometabolic parameters (Glycemic profile (Fasting Glycemia, Fasting insulin, Insulin Resistance), hepatic profile ASAT, ALAT, Gamma GT, TB, creatinine) lipid profile (LDL-c, HDL-c, TC) and TG. CRP and Cortisol levels), 6MW distance (6MWD), 1-RM for extension leg (1-RM EL), 1-RMfor bench press (1-RM BP), squat performance, and crunch performance. ANOVA effect sizes were calculated using partial eta squared (ηp²) to assess the magnitude of the observed effects. When significant main or interaction effects were observed, pairwise comparisons were performed using the Bonferroni post-hoc test. The significance level for all statistical procedures was set at p<0.05.
4. Results
4.1. Body Composition
Two way ANOVA for repeated measures showed significant changes over time for body weight (F(1, 57)=127.41, p<0.0005, ɳp²=0.69), BMI (F(1, 57)=76.61, p<0.0005, ɳp²=0.57) , FM (F(1, 57)= 8.16, p=0.006, ɳp²=0.12) and LM (F(1, 57)=4.29, p=0.04, ɳp²= 0.07). A group effect was observed only for FM (F(3, 57)=3.01, p=0.03, ɳp²=0.13). A (Group x Time) interaction was identified for weight (F(3, 57)=30.88, p<0.0005, ɳp²=0.61), BMI (F(3, 57)=15.62, p<0.0005, ɳp²=0.57) and LM (F(3, 57)=3.08, p=0.03, ɳp²=0.14). The Bonferroni post hoc analysis revealed a significant decrease in body weight for both ETRE-PA (p<0.0005, ∆ (%) = -10.98) and LTRE-PA (p<0.0005, ∆ (%) = -7.99) groups after the intervention compared to before the intervention. Furthermore, during the post-intervention these decreases were also significant in ETRE-PA and LTRE-PA when compared to CG and LTRE groups (p<0.0005). Additionally, a significant reduction in BMI was observed in both the ETRE-PA (p<0.0005, ∆ (%) = -12.06) and LTRE-PA (p<0.0005, ∆ (%) = -8.39) groups after the intervention. However, during post-intervention only ETRE-PA group showed a significant lower BMI compared to CG group (p=0.02). Significant decrease of FM (p=0.02, ∆ (%) = -7.44) and LM (p=0.01, ∆ (%) = -7.32) was observed in ETRE-PA only after the intervention. No significant difference was observed between the groups concerning TBW.
4.2. Metabolic Parameters
ANOVA for repeated measures showed a significant time effect in TC, LDL-c and ALAT, ASAT, and Alkaline Phosphatase (Table 1). Furthermore, group effect was observed only in Alkaline Phosphatase (F(3, 57)=7.33, p<0.0005, ɳp²=0.27). However, interaction effect (Group x Time) was observed only in TC (F (3, 57)=3.16, p<0.0005, ɳp²=0.14). When comparing before to after the intervention, the Bonferroni post hoc analysis showed a significant reduction in ALAT levels in both the ETRE-PA (p=0.004, ∆ (%) = -47.75) and LTRE-PA (p=0.02, ∆ (%) = -37.58) groups. Additionally, only the ETRE-PA group showed a higher decrease in TC (p=0.001, ∆ (%) = -14.58) and LDL-c (p=0.01, ∆ (%) = -14.29 ). Conversely, only the LTRE-PA group exhibited a reduction in ASAT levels (p=0.02, ∆ (%) = -24.61). Furthermore, when comparing between groups, a significant difference was observed in Alkaline Phosphatase between ETRE-PA and CG groups (p=0.002) and LTRE-PA and CG (p<0.005) groups. Glucoregulatory factors, HDL-c, Gamma GT, cortisol, bilirubin, creatinine, CRP, and TSH levels remained unaffected by either intervention (p>0.05).
4.3.1. 6 MWT
Two way ANOVA for repeated measure revealed a significant effect of time (F(1, 57)=76.29, p<0.0005, ηp²= 0.57 ), group (F(3, 57)=22.29, p <0.0005, ηp²=0.54) and (Group x Time) interaction (F(3, 57)=23.43, p<0.0005, ηp²=0.55). Bonferroni post hoc analysis showed higher performances in both ETRE-PA and LTRE-PA when comparing after-intervention to before-intervention (Figure 3). When comparing between groups, a significantly higher 6MWD performance was observed in ETRE-PA and LTRE-PA groups compared to CG group (p<0.0005).
4.3.2. LE and BP 1-RM
Two way ANOVA showed significant effects of time on both LE 1-RM (F(1, 57)=29.67, p<0.0005, ηp²=0.31) and BP 1-RM (F(1, 57)= 12.94, p=0.001, ηp²=0.18). Additionally, group effect (F(3, 57)= 14.67, p<0.0005, ηp²=0.43 ; F(3, 57)=11.02, p<0,0005, ηp²= 0.99, respectively) were observed for the same parameters. However, interaction effects were revealed only in LE 1-RM (F(3, 57)=9.68, p<0.0005, ηp²=0.33). The Bonferroni post hoc analysis showed significantly greater improvements in LE 1-RM in ETRE-PA and LTRE-PA groups compared to LTRE (p=0.001, p<0.0005, respectively) and CG groups (p<0.0005). Moreover, when comparing before- to post-intervention, both ETRE-PA and LTRE-PA demonstrated enhanced performance in LE 1-RM (p<0.0005) and BP 1-RM (p<0.005).
4.3.3. Explosiveness and Endurance Strength
Two way ANOVA for repeated measures revealed significant effect of time in the vertical jump test (F(1, 57)=91.19, p=0.001, ηp²=0.61), 30-second squat test (F(1, 57)=45.24, p<0.0005, ηp²=0.44) and 30-second crunch test (F(1, 57)=24.54, p<0.0005, ηp²=0.30). A group effect was observed in the vertical jump test (F(3, 57)=9.95, p<0.0005, ηp²=0.34), 30-second squat test (F(3, 57)=19.05, p<0.0005, ηp²=0.50) and 30-second crunch test (F(3, 57)=7.12, p<0.0005, ηp²=0.27 Furthermore, an interaction (Group x time) effect was observed for these parameters (F(3, 57)=16.28, p<0.0005, ηp²= 0.46; F(3, 57)=8.57, p<0.0005, ηp²=0.31; F(3, 57)=14.45, p<0.0005; ηp²=0.43, respectively). The Bonferroni post hoc analysis showed a higher performance in the vertical jump test, 30-second squat test and 30-second crunch and when comparing before- to after-intervention (Figure 3a,b). Both ETRE-PA and LTRE-PA groups exhibited improvements in the vertical jump test when compared to CG (p<0.0005) and LTRE (p<0.0005). In the squat test, both ETRE-PA and LTRE-PA groups exhibited higher improvements in squat test when compared to CG (p<0.0005) and LTRE groups. (p<0.0005, p=0.008, respectively) Additionally, in crunch test both the ETRE-PA and LTRE-PA groups exhibited greater improvements compared to CG (p<0.0005) and LTRE (p=0.01, p=0.003, respectively). (Figure 3c).
5. Discussion
The present study investigated for the first time the impact of ETRE and LTRE combined with physical activity compared to LTRE and CG on body composition, cardiometabolic health and physical performance among women with overweight or obesity. The main findings revealed significant reductions in body weight and body mass index (BMI) in both ETRE-PA and LTRE-PA groups. Specifically, ETRE-PA group showed reductions in FM, FFM, LDL-c, and ALAT levels. Conversely, LTRE-PA group showed reductions in ALAT and ASAT levels. However, glycemic profile, cortisol, bilirubin, creatinine, CRP and TSH levels were not affected by either intervention. Regarding physical performance, ETRE-PA and LTRE-PA groups showed higher significant improvements in all tests compared to LTRE and CG. Previous studies have established TRE as an effective lifestyle intervention to improve body composition and overall health [6,11,30,31]. The impact of the timing of food intake ETRE vs. LTRE on body composition has gained considerable interest in recent years [32]. Few studies have compared the effects of ETRE vs. LTRE combined with physical exercise on body composition and health parameters. The existing literature presents mixed results mostly without notable differences [33], which aligns with our study.
Queiroz et al. [34] compared the effects of ETRE (8:00 a.m. to 4:00 p.m.), LTRE (12:00 p.m. to 8:00 p.m.) and a control condition (8:00 a.m. to 8:00 p.m.) in overweight and obese adults. Significant decreases in FFM and fat mass were observed in all three groups without notable differences between them. Additionally, a 14-week study by Jamshed et al. [35] compared ETRE (7:00 a.m. to 3:00 p.m.) to a control group (eating window ≥ 12 hours). The ETRE group showed a greater weight loss. A single long-term trial (12 months) presented by Liu et al. [36] compared ETRE (8 a.m. to 4 p.m.) with a CG on a hypocaloric diet (1500-1800 kcal/day for men, 1200-1500 kcal/day for women) in overweight and obese adults. After 12 months, reductions in fat mass (5.9 and 4.5 kg, respectively) and lean mass (1.7 and 1.4 kg, respectively) were statistically significant in both the ETRE and control groups with no notable differences between groups. Similarly, our study showed a significant decrease in lean in ETRE-PA group when comparing pre- and post-intervention values. The decrease in lean mass may be explained by insufficient protein intake [37] . Other mechanisms, such as the disruption of anabolic hormones like growth hormone (GH) may also play a role. An alteration in GH secretion can disrupt protein synthesis, leading to a reduction in lean mass [38]. Additionally, an insufficiency of ketone bodies as an energy source may contribute to the degradation of skeletal muscles [39]. Furthermore, the present study demonstrated that ETRE-PA led to a selective loss of fat mass when comparing pre- and post-intervention results with no significant difference when comparing between groups. These results are consistent with those of Low et al. [40], who also indicated ETRE as an effective intervention to reduce fat mass. This effectiveness could be attributed to the alignment of the body’s circadian rhythms with ETRE, which has been shown to improve metabolic processes and reduce the risk of metabolic disorders as reported by Patterson et al. [41]. In the other hand, Kotarsky et al. [42] showed that 8 weeks of TRE combined with training compared to control condition reduce body weight (-3.3% vs. -0.2%) as well as fat mass (-9.0% vs. -3.3%) and increased lean mass percentage (+2.4% vs. +1.2%). According to Boyd et al. [43], these improvements may be attributed to a reduction in energy intake throughout the study. Indeed, it has been shown that the type of diet plays a crucial role in the effects of TRE on health oy. Fasting has been proven to stimulate fat metabolism and promote the metabolic transition from glucose oxidation to fat oxidation when glycogen stores are depleted [42,44]. This can be accompanied by increased lipolysis of adipose tissue and the release of free fatty acids and glycerol into the plasma [45,46]. Mobilization and use of fatty acids in adipocytes increase caloric expenditure, which can prevent obesity [47]. Regarding cardiometabolic health, previous studies [6,48,49] have shown that late eating is associated with poorer cardiometabolic health. The circadian misalignment could explain these results [50]. Additionally, glucose tolerance is better in the biological morning which seems to be related to diurnal variations in β-cell response, peripheral insulin sensitivity, insulin clearance and glucose efficiency [51,52]. Fatty acid oxidation in skeletal muscles and the thermic effect of food are also higher in the morning. This suggests that it is optimal to consume the majority of daily calories earlier in the day, while reserving the late-afternoon and the night for fasting and sleep [53]. In the present study, our results showed that a combination of LTRE and physical exercise had no negative effect on cardiometabolic health. In contrast, we observed that the combination of physical training and LTRE resulted in significant improvements in markers of liver damage (ASAT, ALAT and alkaline phosphatase). Additionally, the ETRE-PA group showed a significant improvement in lipid profile (TC and LDL-c) as well as liver markers (ALAT and alkaline phosphatase), suggesting a synergistic effect of combination between both interventions. These results are consistent with a meta-analysis by Dai et al. [54] that reported a significant improvement in lipid and glycemic profile after combining TRE and physical exercise. Furthermore, another study conducted by Real-Hohn et al. [55] showed a significant decrease in insulin, improved oxidative stress biomarkers, better glucose tolerance and hexokinase activity in the liver, heart and skeletal muscles after intermittent fasting combined with high interval training group compared to the control group. It is important to note that the improvements observed in lipid profiles and liver enzymes in our study were independent of factors regulating blood glucose, cortisol, CRP, and TSH levels, suggesting that TRE may have direct effects on lipid metabolism and liver function. However, we also observed a trend towards reductions in blood glucose regulation parameters, including insulin sensitivity, fasting insulin, and blood glucose levels in the ETRE-PA and LTRE-PA groups after the intervention. Perhaps an increase in exercise intensity could further improve these parameters. Another study by Wei et al. [56] showed no change in glycemic profile during similar intermittent fasting. The same researchers explained this stagnation by the fact that the baseline levels of participants were below 9.9 mmol/l. Therefore, they suggested that an improvement in fasting blood glucose might be observable beyond these values. One of the main objectives of the present study was to highlight the effectiveness of TRE and physical activity in improving various aspects of physical performance. To our knowledge, this study is the first to examine the combined effects of different TRE times during the day and physical activity on physical performance in overweight and obese women by evaluating the exercise capacity in various intervention groups and compared them to a control group. Our results showed that a 16/8 TRE regimen followed for 12 weeks resulted in a significant improvement in the walking distance during a 6MWT in the ETRE-PA and LTRE-PA groups. Most of previous studies [57,58,59,60,61,62] have evaluated the effect of fasting combined with physical exercise on athletes, and produced mixed results. During Ramadan (14/10), negative effects on performance appear likely due to factors such as disrupted sleep and hydration. These effects were more pronounced in elite athletes, but among amateur athletes, the difference is minimal [59,60,62]. Conversely, no significant differences were observed after TRE (16/8) in aerobic [63,64,65,66], anaerobic [60,64,67], as well as strength and power [57,62,64,66,68,69]. However, a meta-analysis by Zouhal et al. [70] mentioned that fasting training in sedentary and untrained subjects could promote muscle physiological adaptations, potentially leading to improved endurance performance.
Limitations:
This study has some limitations. First, it remains unclear whether the metabolic health benefits associated with time-restricted eating (TRE) are due to the shortened eating window, a potential reduction in energy intake, or a combination of both, as neither caloric intake nor protein consumption were assessed across the groups during the intervention. Moreover, the intensity of the muscle-strengthening exercises may have been insufficient to prevent the loss of lean mass. Additionally, menstrual cycle variations were not accounted for due to the longitudinal design of the study, making it difficult to completely exclude their potential influence on the outcomes. Lastly, future studies could consider incorporating an additional group that engages solely in physical activity, to determine whether the observed benefits can be attributed exclusively to the exercise intervention.
6. Conclusion
Our findings suggest that combining TRE and physical activity positively affects body composition, cardiometabolic health, and functional capacity. Both the ETRE-PA and LTRE-PA interventions contributed to improved patient outcomes, with exercise reduced some of the adverse effects of LTRE on body composition and cardiometabolic health in patients reported in the literature. However, no significant effects on some metabolic parameters related to glycemic variables were observed, indicating that maintaining a relatively short eating window may lead to better outcomes. Finally, incorporating calorie restriction during the TRE period could be an additional strategy to enhance results in future research.
Author Contributions
Conceptualization, TD., O.H. and S.M.; methodology, S.M.; S.C.M; F.N., M.F.N. R.A. and S.J.M.; writing— original draft preparation, S.M, T.D. and O.H.; data analysis, S.M.; writing—review and editing, S.M., T.D. and O.H. All authors have read and agreed to the published version of the manuscript. Funding: This research received no external funding.
Funding
This research received no external funding.
Institutional Review Board Statement
All the procedures were approved by the local ethics committee (CPP SUD, n ° 0460/2022, Sfax, Tunisia, approval date: 16 December 2022) and registered in the Pan African Clinical Trial Registry (Tri-al ID: PACTR202301473691345). This study was conducted according to the Declaration of Helsinki. Informed Consent Statement: Informed consent was obtained from all the subjects involved in the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Acknowledgments
The authors express their sincere gratitude to all the participants for their in-valuable cooperation, without which the realization of this paper would not have been possible. All of them have consented to the acknowledgement.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Okunogbe, A.; Nugent, R.; Spencer, G.; Powis, J.; Ralston, J.; Wilding, J. Economic Impacts of Overweight and Obesity: Current and Future Estimates for 161 Countries. BMJ Glob Health 2022, 7, e009773. [Google Scholar] [CrossRef] [PubMed]
- Hales, C. M.; Carroll, M. D.; Fryar, C. D.; Ogden, C. L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017-2018. NCHS Data Brief 2020, 360, 1–8. [Google Scholar]
- McDonough, D.; Su, X.; Gao, Z. Health Wearable Devices for Weight and BMI Reduction in Individuals with Overweight/Obesity and Chronic Comorbidities: Systematic Review and Network Meta-Analysis. British Journal of Sports Medicine 2021, 55, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Brown, J. D.; Buscemi, J.; Milsom, V.; Malcolm, R.; O’Neil, P. M. Effects on Cardiovascular Risk Factors of Weight Losses Limited to 5-10. Transl Behav Med 2016, 6, 339–346. [Google Scholar] [CrossRef]
- Kim, J. Y. Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance. J Obes Metab Syndr 2021, 30, 20–31. [Google Scholar] [CrossRef]
- Lesani, A.; Barkhidarian, B.; Jafarzadeh, M.; Akbarzade, Z.; Djafarian, K.; Shab-Bidar, S. Time-Related Meal Patterns and Breakfast Quality in a Sample of Iranian Adults. BMC Nutrition 2023, 9, 13. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R. A.; Della Manna, D. L.; Yang, E. S.; Ravussin, E.; Peterson, C. M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, E1234. [Google Scholar] [CrossRef]
- da Silva, R. A. D.; Szmuchrowski, L. A.; Rosa, J. P. P.; Santos, M. A. P. dos; de Mello, M. T.; Savoi, L.; Porto, Y. F.; de Assis Dias Martins Júnior, F.; Drummond, M. D. M. Intermittent Fasting Promotes Weight Loss without Decreasing Performance in Taekwondo. Nutrients 2023, 15, 3131. [Google Scholar] [CrossRef]
- James, D. L.; Hawley, N. A.; Mohr, A. E.; Hermer, J.; Ofori, E.; Yu, F.; Sears, D. D. Impact of Intermittent Fasting and/or Caloric Restriction on Aging-Related Outcomes in Adults: A Scoping Review of Randomized Controlled Trials. Nutrients 2024, 16, 316. [Google Scholar] [CrossRef]
- Chen, W.; Liu, X.; Bao, L.; Yang, P.; Zhou, H. Health Effects of the Time-Restricted Eating in Adults with Obesity: A Systematic Review and Meta-Analysis. Front Nutr 2023, 10, 1079250. [Google Scholar] [CrossRef]
- Thomas, E. A.; Zaman, A.; Sloggett, K. J.; Steinke, S.; Grau, L.; Catenacci, V. A.; Cornier, M.-A.; Rynders, C. A. Early Time-Restricted Eating Compared with Daily Caloric Restriction: A Randomized Trial in Adults with Obesity. Obesity 2022, 30, 1027–1038. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Sun, Y.; Ye, Y.; Hu, D.; Zhang, H.; He, Z.; Zhao, H.; Yang, H.; Mao, Y. Randomized Controlled Trial for Time-Restricted Eating in Healthy Volunteers without Obesity. Nat Commun 2022, 13, 1003. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A. T.; Regmi, P.; Manoogian, E. N. C.; Fleischer, J. G.; Wittert, G. A.; Panda, S.; Heilbronn, L. K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity (Silver Spring) 2019, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Kazeminasab, F.; Baharlooie, M.; Karimi, B.; Mokhtari, K.; Rosenkranz, S. K.; Santos, H. O. Effects of Intermittent Fasting Combined with Physical Exercise on Cardiometabolic Outcomes: Systematic Review and Meta-Analysis of Clinical Studies. Nutrition Reviews 2023, nuad155. [Google Scholar] [CrossRef]
- Albosta, M.; Bakke, J. Intermittent Fasting: Is There a Role in the Treatment of Diabetes? A Review of the Literature and Guide for Primary Care Physicians. Clin Diabetes Endocrinol 2021, 7, 3. [Google Scholar] [CrossRef]
- Vieira, R. F. L.; Muñoz, V. R.; Junqueira, R. L.; de Oliveira, F.; Gaspar, R. C.; Nakandakari, S. C. B. R.; Costa, S. de O.; Torsoni, M. A.; da Silva, A. S. R.; Cintra, D. E.; de Moura, L. P.; Ropelle, E. R.; Zaghloul, I.; Mekary, R. A.; Pauli, J. R. Time-Restricted Feeding Combined with Aerobic Exercise Training Can Prevent Weight Gain and Improve Metabolic Disorders in Mice Fed a High-Fat Diet. The Journal of Physiology 2022, 600, 797–813. [Google Scholar] [CrossRef]
- Petridi, F.; Geurts, J. M. W.; Nyakayiru, J.; Schaafsma, A.; Schaafsma, D.; Meex, R. C. R.; Singh-Povel, C. M. Effects of Early and Late Time-Restricted Feeding on Parameters of Metabolic Health: An Explorative Literature Assessment. Nutrients 2024, 16, 1721. [Google Scholar] [CrossRef]
- Boege, H. L.; Bhatti, M. Z.; St-Onge, M.-P. Circadian Rhythms and Meal Timing: Impact on Energy Balance and Body Weight. Current Opinion in Biotechnology 2021, 70, 1–6. [Google Scholar] [CrossRef]
- Zaman, A.; Grau, L.; Jeffers, R.; Steinke, S.; Catenacci, V. A.; Cornier, M.-A.; Rynders, C. A.; Thomas, E. A. The Effects of Early Time Restricted Eating plus Daily Caloric Restriction Compared to Daily Caloric Restriction Alone on Continuous Glucose Levels. Obesity Science & Practice 2023, 10, e702. [Google Scholar] [CrossRef]
- Maaloul, R.; Ben Dhia, I.; Marzougui, H.; Turki, M.; Kacem, F. H.; Makhlouf, R.; Amar, M. B.; Kallel, C.; Driss, T.; Elleuch, M. H.; Ayadi, F.; Ghroubi, S.; Hammouda, O. Is Moderate-Intensity Interval Training More Tolerable than High-Intensity Interval Training in Adults with Obesity? Biol Sport 2023, 40, 1159–1167. [Google Scholar] [CrossRef]
- Wilson, R. A.; Deasy, W.; Stathis, C. G.; Hayes, A.; Cooke, M. B. Intermittent Fasting with or without Exercise Prevents Weight Gain and Improves Lipids in Diet-Induced Obese Mice. Nutrients 2018, 10, E346. [Google Scholar] [CrossRef] [PubMed]
- Beck, T. W. The Importance of a Priori Sample Size Estimation in Strength and Conditioning Research. J Strength Cond Res 2013, 27, 2323–2337. [Google Scholar] [CrossRef] [PubMed]
- Miladi, S.; Hammouda, O.; Ameur, R.; Miladi, S. C.; Feki, W.; Driss, T. Time-Restricted Eating Benefits on Pulmonary Function and Postural Balance in Overweight or Obese Women. Nutrients 2024, 16, 2919. [Google Scholar] [CrossRef]
- Brunani, A.; Perna, S.; Soranna, D.; Rondanelli, M.; Zambon, A.; Bertoli, S.; Vinci, C.; Capodaglio, P.; Lukaski, H.; Cancello, R. Body Composition Assessment Using Bioelectrical Impedance Analysis (BIA) in a Wide Cohort of Patients Affected with Mild to Severe Obesity. Clinical Nutrition 2021, 40, 3973–3981. [Google Scholar] [CrossRef]
- Beqa Ahmeti, G.; Idrizovic, K.; Elezi, A.; Zenic, N.; Ostojic, L. Endurance Training vs. Circuit Resistance Training: Effects on Lipid Profile and Anthropometric/Body Composition Status in Healthy Young Adult Women. Int J Environ Res Public Health 2020, 17, 1222. [Google Scholar] [CrossRef]
- Friedewald, W. T.; Levy, R. I.; Fredrickson, D. S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin Chem 1972, 18, 499–502. [Google Scholar] [CrossRef]
- de Souza, S. A. F.; Faintuch, J.; Fabris, S. M.; Nampo, F. K.; Luz, C.; Fabio, T. L.; Sitta, I. S.; de Batista Fonseca, I. C. Six-Minute Walk Test: Functional Capacity of Severely Obese before and after Bariatric Surgery. Surg Obes Relat Dis 2009, 5, 540–543. [Google Scholar] [CrossRef]
- Hunter, G.; Seelhorst, D.; Snyder, S. Comparison of Metabolic and Heart Rate Responses to Super Slow Vs. Traditional Resistance Training. Journal of strength and conditioning research / National Strength & Conditioning Association 2003, 17, 76–81. [Google Scholar] [CrossRef]
- Macarilla, C. T.; Sautter, N. M.; Robinson, Z. P.; Juber, M. C.; Hickmott, L. M.; Cerminaro, R. M.; Benitez, B.; Carzoli, J. P.; Bazyler, C. D.; Zoeller, R. F.; Whitehurst, M.; Zourdos, M. C. Accuracy of Predicting One-Repetition Maximum from Submaximal Velocity in The Barbell Back Squat and Bench Press. J Hum Kinet 2022, 82, 201–212. [Google Scholar] [CrossRef]
- Crose, A.; Alvear, A.; Singroy, S.; Wang, Q.; Manoogian, E.; Panda, S.; Mashek, D. G.; Chow, L. S. Time-Restricted Eating Improves Quality of Life Measures in Overweight Humans. Nutrients 2021, 13, 1430. [Google Scholar] [CrossRef]
- Kim, J.; Song, Y. Early Time-Restricted Eating Reduces Weight and Improves Glycemic Response in Young Adults: A Pre-Post Single-Arm Intervention Study. Obes Facts 2022, 16, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Aragon, A. A.; Schoenfeld, B. J. Does Timing Matter? A Narrative Review of Intermittent Fasting Variants and Their Effects on Bodyweight and Body Composition. Nutrients 2022, 14, 5022. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yi, P.; Liu, F. The Effect of Early Time-Restricted Eating vs Later Time-Restricted Eating on Weight Loss and Metabolic Health. J Clin Endocrinol Metab 2023, 108, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, J. do N.; Macedo, R. C. O.; Dos Santos, G. C.; Munhoz, S. V.; Machado, C. L. F.; de Menezes, R. L.; Menzem, E. N.; Moritz, C. E. J.; Pinto, R. S.; Tinsley, G. M.; de Oliveira, A. R. Cardiometabolic Effects of Early v. Delayed Time-Restricted Eating plus Energetic Restriction in Adults with Overweight and Obesity: An Exploratory Randomised Clinical Trial. Br J Nutr. [CrossRef]
- Jamshed, H.; Steger, F.; Bryan, D.; Richman, J.; Warriner, A.; Hanick, C.; Martin, C.; Salvy, S.-J.; Peterson, C. Effectiveness of Early Time-Restricted Eating for Weight Loss, Fat Loss, and Cardiometabolic Health in Adults With Obesity: A Randomized Clinical Trial. JAMA Internal Medicine 2022, 182. [Google Scholar] [CrossRef]
- Liu, D.; Huang, Y.; Huang, C.; Yang, S.; Wei, X.; Zhang, P.; Guo, D.; Lin, J.; Xu, B.; Li, C.; He, H.; He, J.; Liu, S.; Shi, L.; Xue, Y.; Zhang, H. Calorie Restriction with or without Time-Restricted Eating in Weight Loss. New England Journal of Medicine 2022, 386, 1495–1504. [Google Scholar] [CrossRef]
- Tagawa, R.; Watanabe, D.; Ito, K.; Ueda, K.; Nakayama, K.; Sanbongi, C.; Miyachi, M. Dose–Response Relationship between Protein Intake and Muscle Mass Increase: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrition Reviews 2021, 79, 66–75. [Google Scholar] [CrossRef]
- Young, J. A.; Zhu, S.; List, E. O.; Duran-Ortiz, S.; Slama, Y.; Berryman, D. E. Musculoskeletal Effects of Altered GH Action. Frontiers in Physiology 2022, 13. [Google Scholar] [CrossRef]
- Yakupova, E. I.; Bocharnikov, A. D.; Plotnikov, E. Y. Effects of Ketogenic Diet on Muscle Metabolism in Health and Disease. Nutrients 2022, 14, 3842. [Google Scholar] [CrossRef]
- Lowe, D. A.; Wu, N.; Rohdin-Bibby, L.; Moore, A. H.; Kelly, N.; Liu, Y. E.; Philip, E.; Vittinghoff, E.; Heymsfield, S. B.; Olgin, J. E.; Shepherd, J. A.; Weiss, E. J. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern Med 2020, 180, 1491–1499. [Google Scholar] [CrossRef]
- Patterson, R. E.; Laughlin, G. A.; Sears, D. D.; LaCroix, A. Z.; Marinac, C.; Gallo, L. C.; Hartman, S. J.; Natarajan, L.; Senger, C. M.; Martínez, M. E.; Villaseñor, A. INTERMITTENT FASTING AND HUMAN METABOLIC HEALTH. J Acad Nutr Diet 2015, 115, 1203–1212. [Google Scholar] [CrossRef]
- Kotarsky, C. J.; Johnson, N. R.; Mahoney, S. J.; Mitchell, S. L.; Schimek, R. L.; Stastny, S. N.; Hackney, K. J. Time-Restricted Eating and Concurrent Exercise Training Reduces Fat Mass and Increases Lean Mass in Overweight and Obese Adults. Physiological Reports 2021, 9, e14868. [Google Scholar] [CrossRef] [PubMed]
- Boyd, P.; O’Connor, S. G.; Heckman-Stoddard, B. M.; Sauter, E. R. Time-Restricted Feeding Studies and Possible Human Benefit. JNCI Cancer Spectr 2022, 6, pkac032. [Google Scholar] [CrossRef] [PubMed]
- Vasim, I.; Majeed, C. N.; DeBoer, M. D. Intermittent Fasting and Metabolic Health. Nutrients 2022, 14, 631. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Mottillo, E. P. Adipocyte Lipolysis: From Molecular Mechanisms of Regulation to Disease and Therapeutics. Biochem J 2020, 477, 985–1008. [Google Scholar] [CrossRef]
- Zhang, S.; Williams, K. J.; Verlande-Ferrero, A.; Chan, A. P.; Su, G. B.; Kershaw, E. E.; Cox, J. E.; Maschek, J. A.; Shapira, S. N.; Christofk, H. R.; Vallim, T. Q. de A.; Masri, S.; Villanueva, C. J. Acute Activation of Adipocyte Lipolysis Reveals Dynamic Lipid Remodeling of the Hepatic Lipidome. Journal of Lipid Research 2024, 65. [Google Scholar] [CrossRef]
- Schirinzi, V.; Poli, C.; Berteotti, C.; Leone, A. Browning of Adipocytes: A Potential Therapeutic Approach to Obesity. Nutrients 2023, 15, 2229. [Google Scholar] [CrossRef]
- Taetzsch, A.; Roberts, S. B.; Bukhari, A.; Lichtenstein, A. H.; Gilhooly, C. H.; Martin, E.; Krauss, A. J.; Hatch-McChesney, A.; Das, S. K. Eating Timing: Associations with Dietary Intake and Metabolic Health. J Acad Nutr Diet 2021, 121, 738–748. [Google Scholar] [CrossRef]
- Almeida, G.; Souza, M.; Pereira, L. Relationship between Omitting Breakfast and Late Eating with Obesity and Metabolic Disorders: A Review Focusing on Chrononutrition. Archives of Health 2023, 4, 466–483. [Google Scholar] [CrossRef]
- Dragoo, J. L.; Shapiro, S. A.; Bradsell, H.; Frank, R. M. The Essential Roles of Human Adipose Tissue: Metabolic, Thermoregulatory, Cellular, and Paracrine Effects. Journal of Cartilage & Joint Preservation 2021, 1, 100023. [Google Scholar] [CrossRef]
- Yadav, R. L.; Yadav, P. K.; Yadav, L. K.; Agrawal, K.; Sah, S. K.; Islam, M. N. Association between Obesity and Heart Rate Variability Indices: An Intuition toward Cardiac Autonomic Alteration—a Risk of CVD. Diabetes Metab Syndr Obes 2017, 10, 57–64. [Google Scholar] [CrossRef]
- Lucidi, P.; Perriello, G.; Porcellati, F.; Pampanelli, S.; Fano, M.; Tura, A.; Bolli, G.; Fanelli, C. Diurnal Cycling of Insulin Sensitivity in Type 2 Diabetes: Evidence for Deviation From Physiology at an Early Stage. Diabetes 2023, 72. [Google Scholar] [CrossRef] [PubMed]
- Lewis, P.; Oster, H.; Korf, H. W.; Foster, R. G.; Erren, T. C. Food as a Circadian Time Cue—Evidence from Human Studies. Nat Rev Endocrinol 2020, 16, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Dai, Z.; Wan, K.; Miyashita, M.; Ho, R. S.; Zheng, C.; Poon, E. T.; Wong, S. H. The Effect of Time-Restricted Eating Combined with Exercise on Body Composition and Metabolic Health: A Systematic Review and Meta-Analysis. Advances in Nutrition 2024, 0. [Google Scholar] [CrossRef] [PubMed]
- Real-Hohn, A.; Navegantes, C.; Ramos, K.; Ramos-Filho, D.; Cahuê, F.; Galina, A.; Salerno, V. P. The Synergism of High-Intensity Intermittent Exercise and Every-Other-Day Intermittent Fasting Regimen on Energy Metabolism Adaptations Includes Hexokinase Activity and Mitochondrial Efficiency. PLoS One 2018, 13, e0202784. [Google Scholar] [CrossRef]
- Wei, M.; Brandhorst, S.; Shelehchi, M.; Mirzaei, H.; Cheng, C. W.; Budniak, J.; Groshen, S.; Mack, W. J.; Guen, E.; Di Biase, S.; Cohen, P.; Morgan, T. E.; Dorff, T.; Hong, K.; Michalsen, A.; Laviano, A.; Longo, V. D. Fasting-Mimicking Diet and Markers/Risk Factors for Aging, Diabetes, Cancer, and Cardiovascular Disease. Sci Transl Med 2017, 9, eaai8700. [Google Scholar] [CrossRef]
- Moro, T.; Tinsley, G.; Bianco, A.; Marcolin, G.; Pacelli, Q. F.; Battaglia, G.; Palma, A.; Gentil, P.; Neri, M.; Paoli, A. Effects of Eight Weeks of Time-Restricted Feeding (16/8) on Basal Metabolism, Maximal Strength, Body Composition, Inflammation, and Cardiovascular Risk Factors in Resistance-Trained Males. Journal of Translational Medicine 2016, 14, 290. [Google Scholar] [CrossRef]
- Tinsley, G. M.; Moore, M. L.; Graybeal, A. J.; Paoli, A.; Kim, Y.; Gonzales, J. U.; Harry, J. R.; VanDusseldorp, T. A.; Kennedy, D. N.; Cruz, M. R. Time-Restricted Feeding plus Resistance Training in Active Females: A Randomized Trial. Am J Clin Nutr 2019, 110, 628–640. [Google Scholar] [CrossRef]
- Abaïdia, A.-E.; Daab, W.; Bouzid, M. A. Effects of Ramadan Fasting on Physical Performance: A Systematic Review with Meta-Analysis. Sports Med 2020, 50, 1009–1026. [Google Scholar] [CrossRef]
- Correia, J. M.; Santos, I.; Pezarat-Correia, P.; Silva, A. M.; Mendonca, G. V. Effects of Ramadan and Non-Ramadan Intermittent Fasting on Body Composition: A Systematic Review and Meta-Analysis. Front Nutr 2020, 7, 625240. [Google Scholar] [CrossRef]
- Correia, J. M.; Santos, P. D. G.; Pezarat-Correia, P.; Minderico, C. S.; Infante, J.; Mendonca, G. V. Effect of Time-Restricted Eating and Resistance Training on High-Speed Strength and Body Composition. Nutrients 2023, 15, 285. [Google Scholar] [CrossRef]
- Perez-Montilla, J. J.; Cuevas-Cervera, M.; Gonzalez-Muñoz, A.; Garcia-Rios, M. C.; Navarro-Ledesma, S. Efficacy of Nutritional Strategies on the Improvement of the Performance and Health of the Athlete: A Systematic Review. International Journal of Environmental Research and Public Health 2022, 19, 4240. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Longo, G.; Grigoletto, D.; Bianco, A.; Ferraris, C.; Guglielmetti, M.; Veneto, A.; Tagliabue, A.; Marcolin, G.; Paoli, A. Time-Restricted Eating Effects on Performance, Immune Function, and Body Composition in Elite Cyclists: A Randomized Controlled Trial. J Int Soc Sports Nutr 2020, 17, 65. [Google Scholar] [CrossRef] [PubMed]
- Aird, T. P.; Farquharson, A. J.; Bermingham, K. M.; O’Sulllivan, A.; Drew, J. E.; Carson, B. P. Divergent Serum Metabolomic, Skeletal Muscle Signaling, Transcriptomic, and Performance Adaptations to Fasted versus Whey Protein-Fed Sprint Interval Training. Am J Physiol Endocrinol Metab 2021, 321, E802–E820. [Google Scholar] [CrossRef] [PubMed]
- Brady, A. J.; Langton, H. M.; Mulligan, M.; Egan, B. Effects of 8 Wk of 16:8 Time-Restricted Eating in Male Middle- and Long-Distance Runners. Med Sci Sports Exerc 2021, 53, 633–642. [Google Scholar] [CrossRef]
- Kang, J.; Ratamess, N. A.; Faigenbaum, A. D.; Bush, J. A.; Beller, N.; Vargas, A.; Fardman, B.; Andriopoulos, T. Effect of Time-Restricted Feeding on Anthropometric, Metabolic, and Fitness Parameters: A Systematic Review. J Am Nutr Assoc 2022, 41, 810–825. [Google Scholar] [CrossRef]
- Tovar, A. P.; Richardson, C. E.; Keim, N. L.; Van Loan, M. D.; Davis, B. A.; Casazza, G. A. Four Weeks of 16/8 Time Restrictive Feeding in Endurance Trained Male Runners Decreases Fat Mass, without Affecting Exercise Performance. Nutrients 2021, 13, 2941. [Google Scholar] [CrossRef]
- Tinsley, G. M.; Forsse, J. S.; Butler, N. K.; Paoli, A.; Bane, A. A.; La Bounty, P. M.; Morgan, G. B.; Grandjean, P. W. Time-Restricted Feeding in Young Men Performing Resistance Training: A Randomized Controlled Trial. Eur J Sport Sci 2017, 17, 200–207. [Google Scholar] [CrossRef]
- Correia, J. M.; Santos, I.; Pezarat-Correia, P.; Minderico, C.; Schoenfeld, B. J.; Mendonca, G. V. Effects of Time-Restricted Feeding on Supramaximal Exercise Performance and Body Composition: A Randomized and Counterbalanced Crossover Study in Healthy Men. Int J Environ Res Public Health 2021, 18, 7227. [Google Scholar] [CrossRef]
- Zouhal, H.; Bagheri, R.; Ashtary-Larky, D.; Wong, A.; Triki, R.; Hackney, A. C.; Laher, I.; Abderrahman, A. B. Effects of Ramadan Intermittent Fasting on Inflammatory and Biochemical Biomarkers in Males with Obesity. Physiology & Behavior 2020, 225, 113090. [Google Scholar] [CrossRef]
Figure 2.
Study Design. ETRE-PA: Early time-restricted eating combined with physical activity; LTRE-PA: Late time-restricted eating combined with physical activity; LTRE: Late time-restricted eating; CG: Control group.
Figure 2.
Study Design. ETRE-PA: Early time-restricted eating combined with physical activity; LTRE-PA: Late time-restricted eating combined with physical activity; LTRE: Late time-restricted eating; CG: Control group.
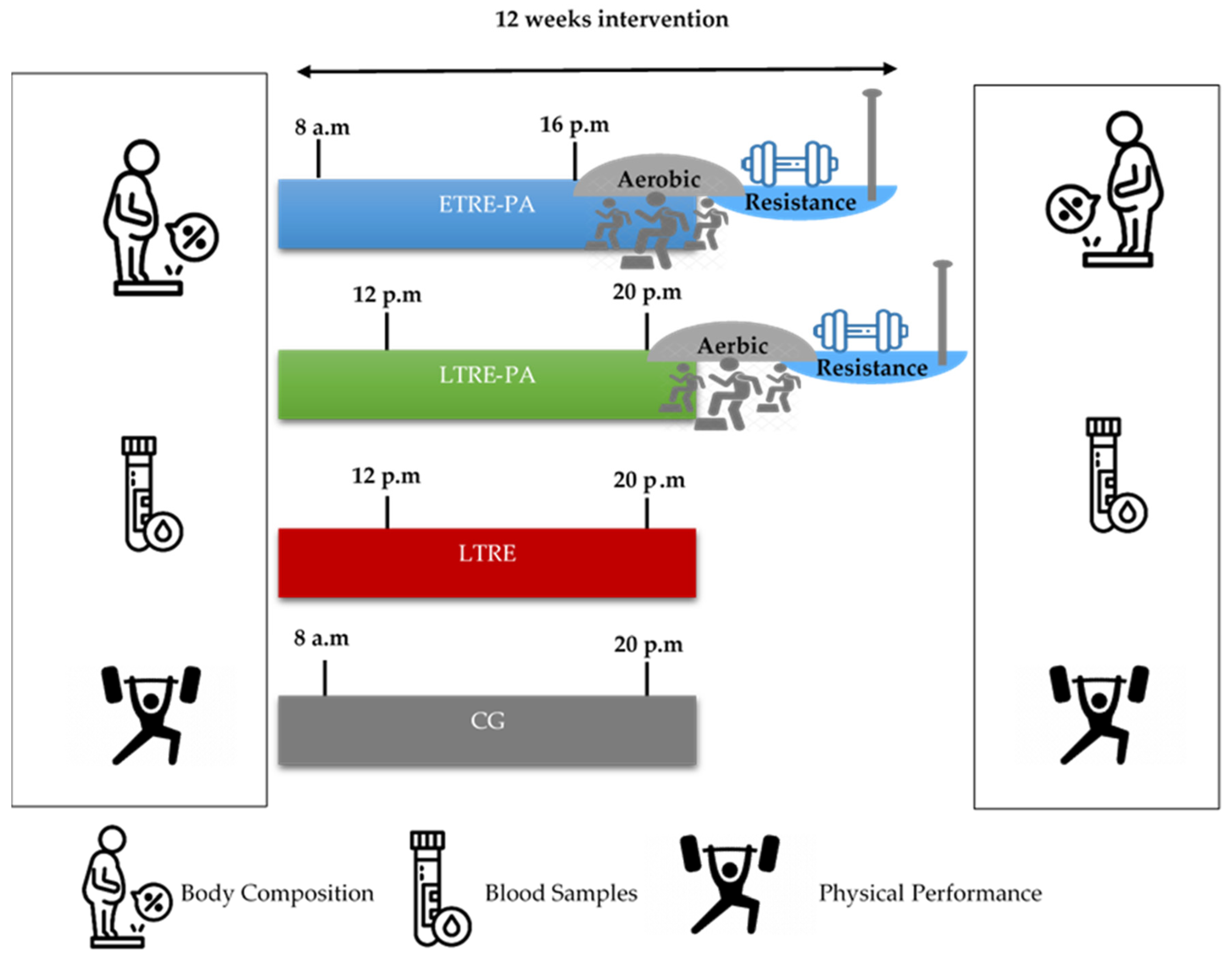
Figure 3.
Physical performance indices between groups. ETRE-PA: Early time-restricted eating combined with physical activity; LTRE-PA: Late time-restricted eating combined with physical activity; LTRE: Late-time restricted eating; CG: Control Group; PRE: Before the intervention; POST: After the intervention; VJ: Vertical jump test. ***p<0.0005; ## p<0.01; ### p<0.0005.
Figure 3.
Physical performance indices between groups. ETRE-PA: Early time-restricted eating combined with physical activity; LTRE-PA: Late time-restricted eating combined with physical activity; LTRE: Late-time restricted eating; CG: Control Group; PRE: Before the intervention; POST: After the intervention; VJ: Vertical jump test. ***p<0.0005; ## p<0.01; ### p<0.0005.
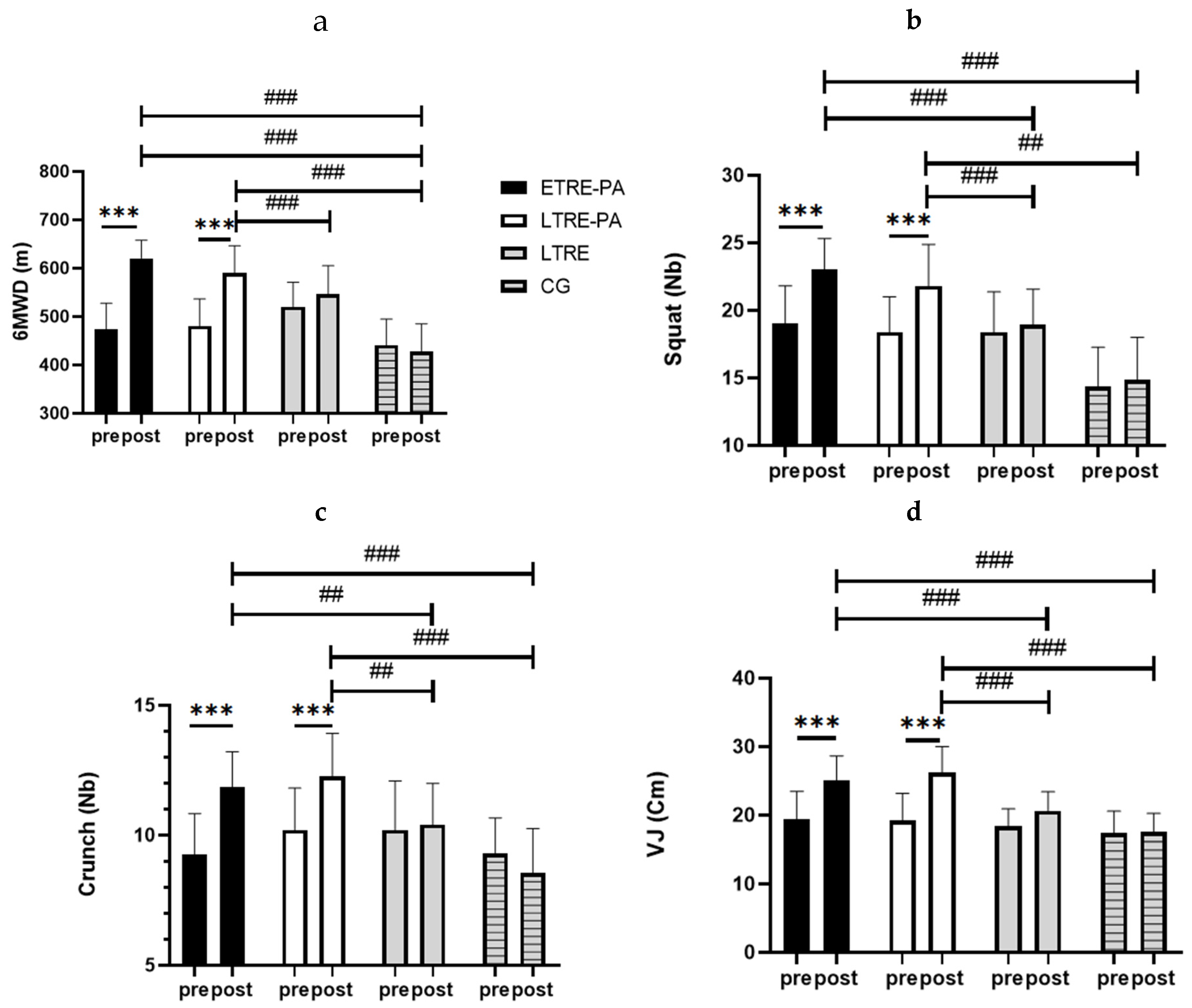

Table 1.
Biochemical parameters before and after the intervention.
| Biomarkers | ETRE-PA | LTRE-PA | LTRE | CG | ANOVA | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | F(1, 57) | P (Time) |
ηp² (Time) | |
| LDL-c (mmol/L) | 2.75±0.76 | 2.32**±0.54 | 2.65±0.76 | 2.46±0.95 | 2.38±0.72 | 2.12±0.54 | 3.17±1.08 | 2.39±0.63 | 24.27 | 0.000 | 0.29 |
| TC (mmol/L) | 4.47±0.90 | 3.76***±0.64 | 4.29±0.96 | 3.98.96±1.38 | 4.13±0.91 | 3.69**±0.69 | 4.96±1.24 | 3.87±0.85 | 43.07 | 0.000 | 0.43 |
| ALAT (UI/L) | 14.73±10 | 6.38**±2.14 | 13.60 ±7.28 | 7.04* ±3.34 | 12.66 ±10.8 | 7.80±2.27 | 19.07±15.66 | 11.31±7.69 | 24.97 | 0.000 | 0.30 |
| ASAT (UI/L) | 18.13±6.45 | 12.53 ±2.16 | 20.20 ±14.10 | 12.60*±5.69 | 19.86±10.09 | 15.33±8.98 | 21.31±15.41 | 15.68±7.94 | 12.85 | 0.001 | 0.18 |
| Phosphatase Alcalin (UI/L) | 77.06±34.77 | 79.6±21.56 | 61.60±13.08 | 56.93±16.69 | 79.60±21.56 | 72.00±20.72 | 59.37±14.54 | 45.37±15.51 | 5.62 | 0.02 | 0.09 |
Values are means ± SD. ETRE-PA: Early time-restricted eating combined with physical exercise group; LTRE-PA: Late time-restricted eating combined with physical exercise group; LTRE: Late time-restricted eating group; CG: Control group; LDL-c: Low Density lipoprotein; TC: Total Cholesterol; ALAT: Alanine aminotransferase; ASAT: Aspartate aminotransferase.* : p<0.05; ** : p<0.01 ; ***: p<0.001. 4.3. Functional Capacity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



