Submitted:
13 September 2024
Posted:
14 September 2024
You are already at the latest version
Abstract
Aural rehabilitation with hearing aids can decrease the attentional requirements of cognitive resources by amplifying the deteriorated-frequency sound in hearing loss patients and improve the auditory discrimination ability like speech-in-noise perception. As aural rehabilitation with an intelligible-hearing sound also can be hopeful, the aim of this study was to evaluate the effectiveness of the aural rehabilitation with intelligible-hearing sound for hearing loss patients. Adult native Japanese speakers (17 males and 23 females, 68.43±9.23 years) showed over 30 dB at 125, 250, 500, 1000, 2000, 3000, 4000, 8000, 10000, and 12000Hz on any side, were recruited and underwent Mini-Mental State Examination Japanese. we conducted self-evaluation questionnaire for hearing problems of voice, gap detection test, fast speech test, and speech-in-noise test, pure tone audiogram, speech perception test using Japanese 67-S, cortical auditory evoked fields, and magnetic mismatch negativity before and after the non-intelligible-hearing (N=20) and intelligible-hearing (N=20) sound therapy with listening to music for one hour a day for 35 days. Better hearing ear was defined using a four-frequency pure-tone average at the thresholds of 500, 1000, 2000 and 4000 Hz. After the sound therapy, speech-in-noise test with signal to noise ratio +10 in better hearing ear showed significant improvement (p<0.05), and N1m-P2m amplitudes showed the significant increase in Lt superior temporal gyrus at the stimulus from better hearing ear (p<0.05). The significant enhancement of the magnetic mismatch negativity amplitude at Lt superior temporal gyrus was exhibited after the sound therapy (p<0.01). Intelligible-hearing sound therapy can improve the ability of speech-in-noise perception in better hearing ear and the enhancement of central cortex response, which reflect the ability of working memory, was proved by cortical auditory evoked fields and magnetic mismatch negativity. Intelligible-hearing sound therapy can be a valuable aural rehabilitation method for sensory neural hearing loss as same as hearing aids.
Keywords:
intelligible-hearing (IH) sound
; sensory neural hearing loss
; speech-in-noise perception
; cortical auditory evoked fields (AEF)
; N1m-P2m amplitude
; magnetic mismatch negativity (MMNm)
1. Introduction
Sensorineural hearing loss, including age-related, noise-induced, sudden, and genetic types, is associated with a lower quality of life due to difficulties in communication. Hearing loss impairs the ability to hear and understand speech, especially in background noise [1], and deteriorates speech recognition, leading to increased listening effort (LE) compared to individuals with normal hearing [2,3]. LE refers to the attentional requirements of cognitive resources required to comprehend auditory tasks [4,5]. Increased LE, along with additional requirements such as lip reading and top-down processing to understand conversations, further impairs listening-in-noise abilities [6,7] and causes fatigue [8,9,10,11]. The impact of fatigue, along with environmental and circumstantial factors, negatively affects cognitive processing, quality of life, and workplace productivity in individuals with hearing loss [4,9]. Additionally, sensorineural hearing loss like age-related hearing loss exacerbates speech comprehension difficulties due to combined effects of degraded speech signal transmission from the cochlea to the central nervous system for cognitive and linguistic processing and declines in episodic memory, processing speed, and working memory. These sensory deficits from peripheral to central nervous systems accelerate cognitive and neural decline, often accompanied by fatigue. Regarding hearing disabilities, including fatigue induced by hearing loss, aural rehabilitation is an effective treatment. This encompasses hearing aids, hearing assistive technologies, auditory training, music therapy, counseling, and support groups. Aural rehabilitation can improve or mitigate cortical and cognitive function decline, as well as subcortical physiological deterioration [12]. Significant improvements in working memory, encompassing both cognitive and neural functions, have been demonstrated after six months of hearing aid use [12]. Additionally, improvements in short-term memory and learning ability have also been recognized after six months of hearing aid use [13]. Hearing aids are effective for tinnitus as they transmit high-frequency sounds that adequately stimulate the hearing pathway, leading to inhibition in the cortex and auditory pathway, which causes tinnitus. Neuro-music therapy is effective for recent-onset tinnitus [14], and constraint-induced sound therapy can prevent maladaptive auditory cortex reorganization in cases of sudden sensorineural hearing loss [15]. The effectiveness of aural rehabilitation, as mentioned above, makes hearing aids the most common treatment for mild-to-moderate hearing loss and tinnitus by amplifying deteriorated-frequency sounds. However, many people do not consistently use hearing aids [16,17,18]. Around 50% of users wear their hearing aids for less than 8 hours per day, and about 40% do not use them daily [19]. Dissatisfaction with hearing aids often arises from various factors such as handling ability, sound quality, type of hearing aid, listening situation, level of experience, expectations, personality, and user attitude [20,21]. The key to successful rehabilitation is selecting aural rehabilitation methods that patients can maintain over the long term and the duration of rehabilitation. Considering aural rehabilitation compliance, other forms of aural rehabilitation besides hearing aids are also promising for hearing disturbances. Our previous report mentioned that rehabilitation with intelligible-hearing (IH) sound using an IH loudspeaker, which emphasizes high tone ranges and reduces sound distortion, can improve pronunciation discrimination by enhancing cortical auditory processing [22].
The mechanisms of aural rehabilitation primarily involve stimulating cortical auditory processing by supporting degraded hearing ability through the amplification of high-frequency sound ranges. Providing intelligible sound from a speaker or other rehabilitation system without causing dissatisfaction in its use will help hearing loss patients continue aural rehabilitation over the long term. Therefore, the concept of a personal communication support system (COMUOON pocket, Universal Sound Design, Tokyo, Japan) was developed based on the technology of the IH loudspeaker (a communication support system, COMUOON, Universal Sound Design, Tokyo, Japan). The sound collector emphasizes high frequency sound ranges and reduces distortion of higher harmonics, similar to COMUOON. The improvement in hearing ability after using the COMUOON pocket is suggested by some patient-oriented self-assessment results in their daily lives.
To effectively measure the impact of aural rehabilitation, it is essential to monitor cortical function, which includes cognitive and neural functions, alongside physiological changes in auditory response. Cortical auditory evoked potentials (AEPs) and auditory evoked fields (AEFs) are long-latency potentials generated in response to auditory stimuli. The AEPs is dominated by the P1-N1-P2 waveform complex, with P1 originating primarily in the lateral portion of Heschl’s gyrus [23,24], N1 in the primary and secondary auditory cortices [25,26,27,28], and P2 in multiple generators within the primary and secondary auditory cortex in Heschl’s gyrus of both hemispheres [29]. AEPs/AEFs can be elicited by the onset, offset, or change in an ongoing sound and are generated without active participant attention or behavioral response [30]. AEPs/AEFs have been measured as objective markers for hearing, cognition, and various physical and mental illnesses [31,32,33].
Mismatch negativity (MMN) and magnetic MMN (MMNm) are pre-attentive auditory event-related potential (ERP) components elicited by infrequent changes in a repetitive acoustic pattern, reflecting the brain’s automatic response to auditory stimuli changes. MMN/MMNm is attributed to neural generators within the temporal and frontal lobes and represents higher-order processes in auditory deviance detection [34]. MMN/MMNm is used to assess the accuracy of central auditory processing, auditory discrimination abilities, and sensory memory. MMN/MMNm has been measured to evaluate the effectiveness of hearing aids and other auditory devices in speech-in-noise perception [35,36]. Therefore, the AEPs with the P1-N1-P2 waveform complex and MMN/MMNm have been used to detect the response of the auditory cortex, demonstrating the effectiveness of aural rehabilitation.
As improvements in hearing ability in daily life after using the COMUOON pocket are occasionally recognized, we hypothesized that aural rehabilitation with IH sound in hearing loss patients can decrease the attentional requirements of cognitive resources by amplifying deteriorated-frequency sounds. This can alter the response of cortical auditory processing, thereby improving auditory discrimination ability in conversations with or without noise. Given the potential of aural rehabilitation with IH sound to enhance discrimination ability in ordinary conversations with or without environmental noise, the aim of this study was to evaluate the relationships between aural rehabilitation with IH sound for hearing loss patients and improvements in hearing level, speech perception ability, self-assessment of hearing loss, and various hearing abilities associated with auditory processing. This evaluation included AEFs and MMNm analysis to assess changes in auditory processing.
2. Materials and Methods
2.1. Participants
Participants underwent pure-tone audiometric tests (PTA) to measure both air-conduction (125, 250, 500, 1000, 2000, 3000, 4000, 8000, 10000, and 12000Hz) and bone-conduction (250, 500, 1000, 2000, 3000, and 4000Hz) thresholds. Adult participants with hearing impairment, native Japanese speakers (17 males and 23 females, 68.43±9.23 years), who showed thresholds over 30 dB at the above frequencies in either ear, were recruited for this study. They had no history of neurological or psychiatric diseases and were not current hearing aid users (3 participants had previously used hearing aids for 1 to 8 years, with a period of 1 to 7 years since last use). None of the participants were musicians or had received any special musical training.
The study protocol was approved by the Ethics Committee of Hiroshima University. All participants provided written consent prior to participation and received compensation for the study.
2.2. Study Design
All participants underwent cognitive evaluation using the Mini-Mental State Examination Japanese (MMSE-J: cutoff value ≤23 for dementia, ≤27 for mild cognitive impairment) on day 1. Participants in this prospective study were fitted with earphone-type sound collectors. Normal sound therapy using a standard sound collector was provided to participants randomly assigned to the control group (Ctrl). The IH sound collector (COMUOON pocket, Universal Sound Design, Tokyo, Japan), which provides high-quality sound by emphasizing high-frequency ranges and reducing distortion of higher harmonics for better formant perception, was provided to the other participants as the IH sound therapy group (HQ). Both groups received sound therapy through the sound collectors by listening to preferred songs and/or tunes selected by each participant for one hour a day for 35 days. Self-evaluation questionnaires for hearing problems related to voice (Figure 1) [37], auditory processing tests (APT) including gap detection test (GDT), fast speech test (FST), and speech-in-noise test (SINT: signal-to-noise ratio (S/N) +10, +5, 0, -5, -10, -15), PTA as described above, and speech perception tests using Japanese 67-S were conducted on days 1 and 35. The better hearing ear was defined using a four-frequency pure-tone average (PTA) at the thresholds of 500, 1000, 2000, and 4000 Hz [38].
1.GDT test
The GDT was utilized to assess temporal processing ability. Each trial included three presentations of white noise without a silent gap and one presentation with a silent gap, with durations ranging from 2 to 34 ms. Participants responded to the presence of a gap in each trial. The stimuli were adaptively varied, and the threshold of gap duration yielding a 50% correct performance was measured.
2.FST test
The FST was employed to evaluate auditory closure ability. The stimuli comprised 20 context-free Japanese three-clause sentences, delivered at three different speaking speeds: normal, 1.5x, and 2x. Participants were required to respond to the sentences at each speed. The percentages of correct responses were calculated for the beginning, middle, and end of the clauses at each speaking speed.”
3.SINT
The SINT was utilized to assess auditory closure ability. The stimuli consisted of a mixture of 36 two-mora Japanese words and speech-spectrum noise, with signal-to-noise ratios (S/N) of -15, -10, -5, 0, +5, and +10 dB. Participants responded to the presented words, which were simultaneously and randomly delivered to both ears. The accuracy rates of SINT at each S/R were calculated.
2.3. Magnetoencephalography Recording
Magnetoencephalography (MEG) recordings were conducted in a magnetically shielded room (MSR). Due to equipment repairs, 27 recruited participants were examined (Table 1). Functional auditory evoked fields (AEFs) and MMNm were measured using a 306-channel MEG system (Vectorview; ELEKTA Neuromag, Helsinki, Finland) with 102 identical triple sensor elements: two orthogonal planar gradiometers and one magnetometer coupled to a multi-superconducting quantum interference device (SQUID), providing three independent measurements of the magnetic fields. Data were recorded with a band-pass filter of 0.1–200 Hz and digitized at 1000 Hz. Epochs with MEG signals larger than 3.0 pT/cm were excluded from averaging. Collected MEG signals from 204-channel planar-type gradiometers were analyzed with an offline band-pass filter of 1-50Hz.
1. Auditory evoked fields (AEFs)
A train of clicks (60 ms) was presented as the auditory stimulus, consisting of single sine waves of 1 ms at 1000 Hz and 4000 Hz, with a repetitive frequency of 3.33 Hz, at three different sound pressures (50 dB, 55 dB, and 60 dB HL), with 240 repeats of the same click. Auditory stimuli were presented bilaterally, respectively. Each stimulus was started at 50 dB HL and increased in steps of 55 dB and 60 dB HL. Additional bilateral auditory stimuli (1000 Hz, 60 dBHL) were also presented to identify auditory cortical regions. Sound stimuli were delivered through plastic tubes and earpieces (E-A-RTone 3A; Aero Company, Indianapolis, IN) using the NBS Presentation software (Neurobehavioral Systems, Albany, CA, USA).
An equivalent current dipole (ECD) analysis was applied using Neuromag source modeling software (ELEKTA Neuromag, Helsinki, Finland). The ECD model of magnetic N1 (N1m) was estimated using 14-20 sensors (7-10 pairs of gradiometers) in the bilateral hemispheres with bilateral auditory stimulation (1000 Hz, 60 dBHL). The ECD coordinates estimated in the bilateral superior temporal gyrus (STG) based on a goodness of fit (GOF) exceeding 80% were selected. The ECD coordinates were superimposed on the responses recorded with the other conditions. The peak-to-peak amplitude of N1m-P2m (magnetic P2) in each task was analyzed before and after the sound therapy.”
2.MMNm
The oddball task was presented from the bilateral ear with two random auditory stimuli: a deviant stimulus (20%, 1000 Hz) and a standard stimulus (80%, 500 Hz), both with a repetitive frequency of 3.33 Hz and a sound pressure of 50 dB HL. The response were analysis in the same manner as in the AEFs analysis. MMNm responses were computed by subtracting the evoked response for the standard stimulus from that of the deviant stimulus, and the peak-to-peak amplitude around 150 ms was analyzed before and after the sound therapy.”
2.4. Statistical Analysis
Experimental data were analyzed using paired t-tests and two-sample t-tests. All p-values were two-tailed, and p<0.05 was considered significant. All statistical analyses were performed using SPSS software (SPSS version 24; IBM, NY). Numerical data are represented as mean ± SD.
3. Results
3.1. The Participants
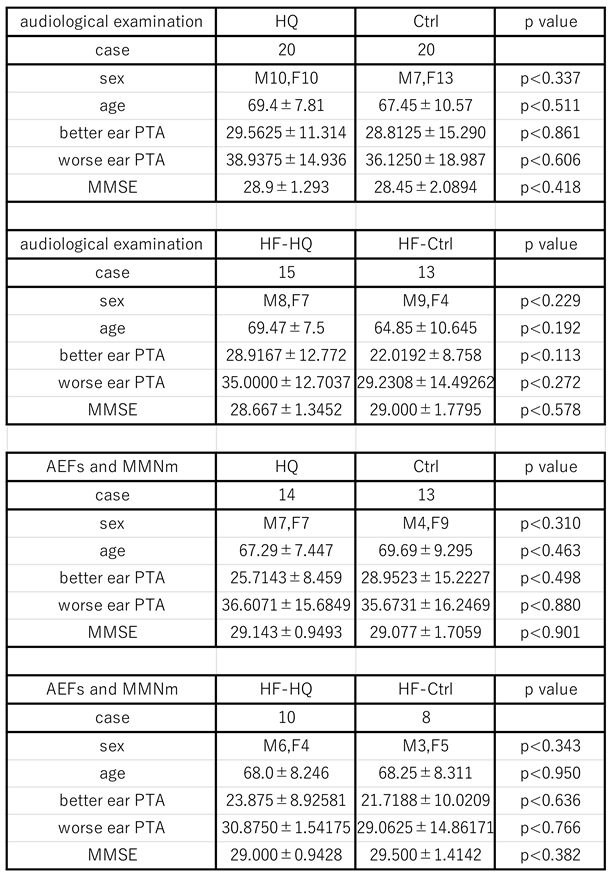
Patient demographics are shown in Table 1. There were no significant differences in the demographics of participants between the two sound therapy groups. The IH sound collector primarily emphasizes high frequency ranges and reduces distortion of higher harmonics to improve formant perception. Therefore, we created subcategory groups, excluding those with a threshold level over 70 dB at 10,000 Hz bilaterally (HF-Ctrl: high-frequency hearing loss control / HF-HQ: high-frequency hearing loss HQ), to analyze the effectiveness of the IH sound therapy. The maximum output level of the IH sound collector is approximately 75-80 dB HL in high-frequency ranges around 10,000 Hz. The better hearing ear was defined based on the average threshold level according to WHO criteria, averaging thresholds at 500, 1000, 2000, and 4000 Hz. All PTA, SPT, and auditory processing tests were analyzed in terms of the better or worse hearing ear based on the PTA results from day 1.
3.2. Self-Evaluation Questionnaire
The self-evaluation questionnaire for hearing problems related to voice did not show any differences among the sound therapy groups, including HF-Ctrl and HF-HQ, on days 1 and 35, nor in the changes between days 1 and 35.
3.3. PTA Measurement and Speech Perception Test
The average threshold level in air-conduction PTA, the sound levels at 50% perception, and the maximum perception percentage in SPT did not show any differences among the sound therapy groups, including HF-Ctrl and HF-HQ, on days 1 and 35, nor in the changes between days 1 and 35.
3.4. Auditory Processing Test
1. GDT
GDT did not show any differences among the sound therapy groups, including HF-Ctrl and HF-HQ, on days 1 and 35, nor in the changes between days 1 and 35.
2. FST
FST did not show any differences among the sound therapy groups, including HF-Ctrl and HF-HQ, on days 1 and 35, nor in the changes between days 1 and 35.
3. SINT
SINT with S/N+10 in the better hearing ear showed significant improvement after sound therapy in HQ and HF-HQ groups (p<0.05) (Figure 2), whereas Ctrl and HF-Ctrl groups did not exhibit any significant differences. The improved accuracy rate in HQ and HF-HQ, calculated by subtracting the pre-therapy accuracy rate from the post-therapy accuracy rate, showed a significantly higher improvement rate in HF-HQ compared to HF-Ctrl in SINT with S/N+10 in the better hearing ear (p<0.01). The improvement in SINT with S/N+10 after sound therapy was widely recognized in HQ, independent of the hearing level in the better hearing ear and the accuracy rate in S/N+10 before sound therapy.
3.5. Magnetoencephalography Recording
1. ECD analysis moment and Auditory evoked potentials
Bilateral auditory stimuli of 1000 Hz at three different sound pressures (50 dB, 55 dB, and 60 dB HL) elicited clear magnetic deflections (N1m and P2m) after stimulus onset in the bilateral STG in response to each stimulus side. However, auditory stimuli of 4000 Hz at the same sound pressures did not show clear magnetic deflections of N1m and P2m under any conditions on day 1 (Figure 3). Based on these results, we analyzed the N1m and P2m components in the auditory stimuli of 1000 Hz. Inter-peak amplitudes of N1m-P2m were measured by subtracting the instantaneous amplitude at the peak latency of P2m from the instantaneous amplitude at the peak latency of N1m. Given that SINT with S/N+10 in the better hearing ear at HQ and HF-HQ showed significant improvement after sound therapy, we analyzed AEFs, including both latency and amplitude of N1m and N1m-P2m peak-to-peak in the left STG, between pre- and post-sound therapy and between HQ/HF-HQ and Ctrl/HF-Ctrl. Compared to Ctrl/HF-Ctrl, HQ/HF-HQ showed a significant increase in the amplitude of N1m-P2m in the left STG at stimuli of 55 dB (HQ) and 60 dB (HQ/HF-HQ) from the better hearing ear (P<0.05) after sound therapy (Figure 4). The latency and amplitude of N1m did not show any significant differences in any group in this study in either STG (data not shown).
2.MMNm
Superimposed auditory-evoked fields in HQ and Ctrl are shown in Figure 5. Clear deflections (MMNm) were observed around 100-250 ms. MMNm was measured and analyzed between HQ/HF-HQ and Ctrl/HF-Ctrl. In HQ and HF-HQ, a significant increase in MMNm amplitude was observed at the left STG after sound therapy (p<0.01 for HQ and p<0.05 for HF-HQ), whereas no significant differences were observed at the right STG in HQ/HF-HQ or at either STG in HF-Ctrl (Figure 6).
4. Discussion
The effectiveness of aural rehabilitation for hearing disturbances, such as hearing loss and tinnitus, is widely recognized. Hearing aids, a common method of aural rehabilitation, are extensively used worldwide, especially for patients with hearing loss. Sensory devices like hearing aids can mitigate the effects of sensory loss by restoring certain aspects of sensory functioning [40,41]. Hearing aids can improve speech-in-noise perception, which is linked to cognitive and signal processing [42]. Additionally, the use of hearing aids enhances working memory performance, which is often diminished by hearing loss, and increases cortical amplitudes, correlating with changes in working memory [12]. These findings suggest that aural rehabilitation for sensorineural hearing loss can improve cognitive and neural functions by restoring the sensory-cognitive connection, thereby enhancing speech-in-noise perception through improved working memory performance. In this study, IH sound therapy improved the SINT of S/N+10 in the better hearing ear, with significant improvement also observed in HF-HQ compared to HF-Ctrl. The effectiveness of IH sound therapy was evident in hearing loss up to around 60 dB, and the improved accuracy rate appeared to be inversely proportional to the pre-accuracy rate of SINT of S/N+10. These results suggest that IH sound therapy is as effective in improving hearing function as hearing aids. The IH sound collector can amplify sound up to approximately 75-80 dB at around 10,000 Hz (company-provided data; not shown), and IH sound therapy was particularly effective for patients with sensorineural hearing loss who can hear high-frequency sounds at 10,000 Hz at 70 dB. Adequate intelligibility stimulation in the high-frequency range is necessary to mitigate the effects of sensory hearing loss and improve speech-in-noise perception in these patients. Improvement in the SINT of S/N+10 in the better hearing ear was also observed after normal sound therapy in some Ctrl and HF-Ctrl cases. Patients who cannot hear high-frequency sounds at 10,000 Hz at 70 dB cannot receive high-frequency sound stimulation from the sound therapy due to limitations in both cochlear function and sound collector specifications, but they can still receive adequate low-frequency sound stimulation.
Based on the improved accuracy rates between Ctrl and HF-Ctrl, the enhancement provided by standard sound therapy was primarily observed in patients with severe high-frequency hearing loss, specifically those with thresholds exceeding 70 dB at 10,000 Hz. The results suggest that some patients with severe sensorineural hearing loss at 10,000 Hz can benefit from low-frequency stimulation without intelligibility, as it effectively stimulates the auditory system. These findings indicate that early-stage sensorineural hearing loss (up to 70 dB at 10,000 Hz) requires high-frequency intelligibility sound stimulation to restore the sensory-cognitive connection. In contrast, late-stage sensorineural hearing loss (over 70 dB at 10,000 Hz) benefits more from low-frequency sound stimulation due to severe high-frequency hearing loss than early-stage sensorineural hearing loss. Sound therapy for severe high-frequency hearing loss may improve speech-in-noise perception even without intelligibility sound. This is likely because sensorineural hearing loss typically begins in the high-frequency range and progresses to lower frequencies. In the early stages, patients lack high-frequency information and need high-frequency intelligibility sound. In the late stages, they require a full range of frequency information but cannot receive adequate high-frequency stimulation due to cochlear limitations and sound collector specifications. It is recognized that most patients with high-frequency hearing loss can utilize low-frequency speech cues better than those with normal hearing, as the brain areas usually responsive to high frequencies adapt to analyze low-frequency sounds [43]. In this context, some patients can reestablish the sensory-cognitive connection even with low-quality sound, as it still provides some stimulation to the central cortex. Our results showed that the improvement rate of speech-in-noise perception varied from poor to good with non-IH sound therapy and from fair to good with IH sound therapy. This indicates that non-IH sound therapy can sometimes offer better stimulation for speech-in-noise perception but can also occasionally worsen it due to the lack of intelligibility sound, which may fail to stimulate or even deteriorate the sensory-cognitive connection. Conversely, IH sound therapy consistently provides better stimulation with intelligibility sound, effectively stimulating the sensory-cognitive connection in all hearing loss patients. Therefore, IH sound therapy is superior to non-IH sound therapy and is recommended for all patients with sensorineural hearing loss.
However, it remains unknown whether aural rehabilitation using IH sound therapy can counteract the deterioration of brain function associated with auditory processing. The N1m-P2m complex, a component of the AEFs, originates primarily in the auditory cortex and is associated with the detection and processing of auditory stimuli [29,44]. The amplitude and latency of these waves can vary depending on cognitive load and the individual’s working memory capacity, reflecting the brain’s increased effort to process and store auditory information [44,45]. The N1-P2 complex is also a marker of sensory memory [46] and auditory learning plasticity [47,48,49]. The N1-P2 response has advantages such as better frequency specificity, inclusion of higher neurologic centers, and less reliance on patient relaxation [50]. Consequently, the N1-P2 complex has been studied in various contexts, including its relationship with cognitive processes like working memory [51,52]. MMN/MMNm is also measured to evaluate automatic cortical auditory processing, selective attention, and neuronal memory trace [53,54]. MMN/MMNm depends on the degree of sensorineural hearing loss and the intensity of stimuli (sound volumes) [55], with significantly reduced amplitude and prolonged latency in hearing-impaired individuals compared to those with normal hearing [56,57]. Music training can shorten the latencies to harmonic, complex, and speech stimuli, possibly facilitating neural processing of acoustic parameters, which manifests in concomitant behaviors like speech perception [58]. The shortening of MMN/MMNm latencies and increased MMN/MMNm amplitude by speech stimuli were also observed after using IH loudspeakers for IH sound stimulation, which is the basis of this study. Therefore, MMN is measured to evaluate hearing levels and discriminative functions, including speech perception, and to analyze the effectiveness of aural rehabilitation [22]. In our study, HQ/HF-HQ exhibited significant improvement in N1m-P2m amplitude at 55 dB (HF-HQ) and 60 dB (HQ/HF-HQ) (p<0.05) in the left superior temporal gyrus (Lt STG). Additionally, HQ/HF-HQ showed a significant increase in MMNm amplitude at Lt STG (p<0.01 for HQ, p<0.05 for HF-HQ) after sound therapy. This proves that repetitive stimulation of the auditory cortex can enhance auditory processing [59]. These results demonstrate that IH sound therapy can provide superior sound stimulation to improve cognitive processes, including working memory and auditory learning plasticity. As MMN/MMNm amplitude reflects automatic cortical auditory processing, selective attention, and neuronal memory trace, and is closely associated with the enhancement of discriminative functions such as speech perception regardless of effort, these results explain the improved SINT scores in S/N+10 in the better hearing ear after IH sound therapy. The improvement in speech-in-noise perception is likely induced by aural rehabilitation using IH sound therapy, with sound being a key factor in stimulating the auditory cortex and enhancing cognitive processes, including working memory. Furthermore, the effectiveness of sound therapy with music has already been demonstrated. Previous reports have indicated that constrained listening rehabilitation with music, in addition to corticosteroid therapy, can significantly improve both hearing levels and auditory cortex responses in cases of sudden sensorineural hearing loss [15]. In our study, we used music for sound therapy, which may also contribute to the positive results in speech-in-noise perception in the better hearing ear. Hearing impairment induces a decline in speech perception, especially in noisy situations, leading to poor communicative ability and a decline in cognitive function, which often complicates other dysfunctions such as dementia [60]. Therefore, various aural rehabilitation methods have been investigated, but no unified method has been established [61,62]. On the other hand, hearing aids can improve speech-in-noise perception by enhancing cognitive function through changes in the central cortex response. The development of hearing aids has focused on device modifications to reduce user dissatisfaction, but some individuals persistently refuse to use them. IH sound therapy with repetitive music stimuli also shows potential for improving speech-in-noise perception, similar to hearing aids. The duration of rehabilitation is a crucial aspect of aural rehabilitation. IH sound therapy with repetitive music stimuli is likely more enjoyable than simply hearing natural sounds, and the sound collector provides only music without amplifying background environmental noise. Therefore, improved sound intelligibility mixed with music may become an alternative method for hearing-impaired patients instead of hearing aids.
However, there are some limitations. In this study, we could not analyze the optimal periods for IH sound therapy, such as the duration of daily use and the total time of sound therapy. Additionally, we could not include more severe hearing loss patients to determine whether they could be candidates for IH sound therapy, and we did not assess satisfaction with IH sound therapy compared to hearing aids. These aspects should be evaluated for IH sound therapy to become a more common aural rehabilitation method in the future. Further studies are needed to investigate the efficacy and satisfaction of IH sound therapy for sensorineural hearing loss.
Conclusions
IH sound therapy can improve speech-in-noise perception in the better hearing ear, as demonstrated by AEFs and MMNm results, which reflect enhanced central cortex response and working memory ability. Therefore, IH sound therapy can be a valuable aural rehabilitation method for sensorineural hearing loss, comparable to hearing aids.
Author Contributions
Conceptualization, T.I. and K.N.; data curation, F.H. and N.C.; formal analysis, T.I.; funding acquisition, L.Y.; investigation, T.I., K.N.,T.O., M.N. and Y.H.; methodology, T.I. and K.N.; project administration, T.I.,K.N. and S.T.; resources, T.T., T.H. and T.U.; software, K.N.; supervision, L.Y. and S.T.; validation, T.I., S.H., R.F., C.I., T.K. and K.T.; visualization, T.I.; writing—original draft preparation, T.I.; writing—review and editing, T.I. and K.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded partly by the Japan Society for the Promotion of Science KAK ENHI grant: 22K09668, the Health Labor Sciences Research grant: H30-Nanchitou (Nan)-Ippan- 016, and the Research Collaboration Fund with Universal Sound Design Inc. (2F, Marinx Tower, 1-9-11, Kaigan, Minato-ku, Tokyo, 105-0022): 0G20KA7383.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Hiroshima University Hospital, Hiroshima University, Hiroshima, Japan (CRB6180006; 11 Dec 2019 as date of approval).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the hearing loss patients.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Acknowledgments
We acknowledge Yukako Okamoto for her technical support.
Conflicts of Interest
The authors declare that this study received funding from Universal Sound Design Inc. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
References
- Kramer, SE.; Kapteyn, TS.; Houtgast, T. Occupational performance: comparing normally-hearing and hearing-impaired employees using the Amsterdam Checklist for Hearing and Work. Int J Audiol 2006, 45, 503-12. PMID: 17005493. [CrossRef]
- Krueger, M.; Schulte, M.; Zokoll, MA.; Wagener, KC.; Meis, M.; Brand, T.; Holube, I. Relation Between Listening Effort and Speech Intelligibility in Noise. Am J Audiol 2017, 26, 378-392. PMID: 29049622. [CrossRef]
- Schepker, H.; Haeder, K.; Rennies, J.; Holube, I. Perceived listening effort and speech intelligibility in reverberation and noise for hearing-impaired listeners. Int J Audiol 2016, 55, 738-747. Epub 2016 Sep 14. PMID: 27627181. [CrossRef]
- Pichora-Fuller, MK.; Kramer, SE.; Eckert, MA.; Edwards, B.; Hornsby, BW.; Humes, LE.; Lemke, U.; Lunner, T.; Matthen, M.; Mackersie, CL.; Naylor, G.; Phillips, NA.; Richter, M.; Rudner, M.; Sommers, MS.; Tremblay, KL.; Wingfield, A. Hearing Impairment and Cognitive Energy: The Framework for Understanding Effortful Listening (FUEL). Ear Hear 2016, 37, Suppl 1:5S-27S. PMID: 27355771. [CrossRef]
- Downs, DW. Effects of hearing and use on speech discrimination and listening effort. J Speech Hear Disord 1982, 47, 189-93. PMID: 7176597. [CrossRef]
- Hétu, R.; Riverin, L.; Lalande, N.; Getty, L.; St-Cyr, C. Qualitative analysis of the handicap associated with occupational hearing loss. Br J Audiol 1988, 22, 251-64. PMID: 3242715. [CrossRef]
- Holman, JA.; Drummond, A.; Hughes, SE.; Naylor, G. Hearing impairment and daily-life fatigue: a qualitative study. Int J Audiol 2019, 58, 408-416. Epub 2019 Apr 28. PMID: 31032678; PMCID: PMC6567543. [CrossRef]
- Bess, FH.; Hornsby, BW.; Commentary: listening can be exhausting--fatigue in children and adults with hearing loss. Ear Hear 2014, 35, 592-9. PMID: 25255399; PMCID: PMC5603232. [CrossRef]
- Hornsby, BW.; Naylor, G.; Bess, FH. A Taxonomy of Fatigue Concepts and Their Relation to Hearing Loss. Ear Hear 2016, 37 Suppl 1(Suppl 1), 136S-44S. PMID: 27355763; PMCID: PMC4930001. [CrossRef]
- Key, AP.; Gustafson, SJ.; Rentmeester, L.; Hornsby, BWY.; Bess, FH. Speech-Processing Fatigue in Children: Auditory Event-Related Potential and Behavioral Measures. J Speech Lang Hear Res 2017, 60, 2090-2104. PMID: 28595261; PMCID: PMC5831094. [CrossRef]
- McGarrigle, R.; Dawes, P.; Stewart, AJ.; Kuchinsky, SE.; Munro, KJ. Measuring listening-related effort and fatigue in school-aged children using pupillometry. J Exp Child Psychol 2017, 161, 95-112. Epub 2017 May 12. PMID: 28505505. [CrossRef]
- Karawani, H.; Jenkins, K.; Anderson S. Restoration of sensory input may improve cognitive and neural function. Neuropsychologia 2018, 114, 203-213. Epub 2018 May 2. PMID: 29729278; PMCID: PMC5988995. [CrossRef]
- Choi, AY.; Shim, HJ.; Lee, SH.; Yoon, SW.; Joo, EJ. Is cognitive function in adults with hearing impairment improved by the use of hearing AIDS? Clin Exp Otorhinolaryngol 2011, 4, 72-76. Epub 2011 May 31. PMID: 21716953; PMCID: PMC3109330. [CrossRef]
- Grapp, M.; Hutter, E.; Argstatter, H.;, Plinkert, PK.; Bolay, HV. Neuro-Music Therapy for Recent-Onset Tinnitus. SAGE Open, 2013, 3, 215824401348969. [CrossRef]
- Okamoto, H.; Fukushima, M.; Teismann, H.; Lagemann, L.; Kitahara, T.; Inohara, H.; Kakigi, R.; Pantev, C. Constraint-induced sound therapy for sudden sensorineural hearing loss--behavioral and neurophysiological outcomes. Sci Rep. 2014, 4, 3927. PMID: 24473277; PMCID: PMC3905271. [CrossRef]
- Bisgaard, N.; Ruf, S. Findings From EuroTrak Surveys From 2009 to 2015: Hearing Loss Prevalence, Hearing Aid Adoption, and Benefits of Hearing Aid Use. Am J Audiol 2017, 26, :451-461. PMID: 29049628. [CrossRef]
- Hoppe, U.; Hesse, G. Hearing aids: indications, technology, adaptation, and quality control. GMS Curr Top Otorhinolaryngol Head Neck Surg 2017, 16, Doc08. PMID: 29279726; PMCID: PMC5738937. [CrossRef]
- Johnson, CE.; Jilla, AM.; Danhauer, JL.; Sullivan, JC.; Sanchez, KR. Benefits from, Satisfaction with, and Self-Efficacy for Advanced Digital Hearing Aids in Users with Mild Sensorineural Hearing Loss. Semin Hear 2018, 39, 158-171. Epub 2018 Jun 15. PMID: 29915453; PMCID: PMC6003810. [CrossRef]
- Staehelin, K.; Bertoli, S.; Probst, R.; Schindler, C.; Dratva, J.; Stutz, EZ. Gender and hearing aids: patterns of use and determinants of nonregular use. Ear Hear 2011, 32, e26-37. PMID: 21795978. [CrossRef]
- Wong, LL.; Hickson, L.; McPherson, B. Hearing aid satisfaction: what does research from the past 20 years say? Trends Amplif 2003, 7, 117-161. PMID: 15004650; PMCID: PMC4168909. [CrossRef]
- Bertoli, S.; Staehelin, K.; Zemp, E.; Schindler, C.; Bodmer, D.; Probst, R. Survey on hearing aid use and satisfaction in Switzerland and their determinants. Int J Audiol 2009, 48, 183-95. PMID: 19363719. [CrossRef]
- Nakagawa, K.; Nakaishi, S.; Imura, T.; Kawahara, Y.; Hashizume, A.; Kurisu, K.; Yuge, L. Neuromagnetic evaluation of a communication support system for hearing-impaired patients. NeuroReport 2017, 28, 712-719. August 16, 2017. |. [CrossRef]
- Vaughan, HG Jr.; Ritter, W. The sources of auditory evoked responses recorded from the human scalp. Electroencephalogr Clin Neurophysiol. 1970, 28, 360-367. PMID: 4191187. [CrossRef]
- Liégeois-Chauvel, C.; Musolino, A.; Badier, JM.; Marquis, P.; Chauvel, P. Evoked potentials recorded from the auditory cortex in man: evaluation and topography of the middle latency components. Electroencephalogr Clin Neurophysiol 1994, 92, 204-214. PMID: 7514990. [CrossRef]
- Scherg, M.; Von, Cramon, D. Two bilateral sources of the late AEP as identified by a spatio-temporal dipole model. Electroencephalogr Clin Neurophysiol 1985, 62, 32-44. PMID: 2578376. [CrossRef]
- Näätänen, R.; Picton, T. The N1 wave of the human electric and magnetic response to sound: a review and an analysis of the component structure. Psychophysiology 1987, 24, 375-425. PMID: 3615753. [CrossRef]
- Scarff, CJ.; Reynolds, A.; Goodyear, BG.; Ponton, CW.; Dort, JC.; Eggermont, JJ. Simultaneous 3-T fMRI and high-density recording of human auditory evoked potentials. Neuroimage 2004, 23, 1129-1142. PMID: 15528112. [CrossRef]
- Wyss, C.; Boers, F.; Kawohl, W.; Arrubla, J.; Vahedipour, K.; Dammers, J.; Neuner, I.; Shah, NJ. Spatiotemporal properties of auditory intensity processing in multisensor MEG. Neuroimage 2014, 102, 465-473. Epub 2014 Aug 13. PMID: 25132019. [CrossRef]
- Lightfoot, G. Summary of the N1-P2 Cortical Auditory Evoked Potential to Estimate the Auditory Threshold in Adults. Semin Hear 2016, 37, 1-8. PMID: 27587918; PMCID: PMC4910570. [CrossRef]
- Morse, K.; Vander, Werff, KR. Onset-offset cortical auditory evoked potential amplitude differences indicate auditory cortical hyperactivity and reduced inhibition in people with tinnitus. Clin Neurophysiol 2023, 149, 223-233. Epub 2023 Feb 23. PMID: 36963993. [CrossRef]
- Sharma, A.; Martin, K.; Roland, P.; Bauer, P.; Sweeney, MH.; Gilley, P.; Dorman, M. P1 latency as a biomarker for central auditory development in children with hearing impairment. J Am Acad Audiol 2005, 16, 564-573. PMID: 16295243. [CrossRef]
- Ching, TY.; Zhang, VW.; Hou, S.; Van, Buynder, P. Cortical Auditory Evoked Potentials Reveal Changes in Audibility with Nonlinear Frequency Compression in Hearing Aids for Children: Clinical Implications. Semin Hear 2016, 37, 25-35. PMID: 27587920; PMCID: PMC4910568. [CrossRef]
- Soleimani, M.; Rouhbakhsh, N.; Rahbar, N. Towards early intervention of hearing instruments using cortical auditory evoked potentials (CAEPs): A systematic review. Int J Pediatr Otorhinolaryngol 2021, 144, 110698. Epub 2021 Mar 27. PMID: 33839460. [CrossRef]
- Takasago, M.; Kunii, N.; Komatsu, M.; Tada, M.; Kirihara, K.; Uka, T.; Ishishita, Y.; Shimada, S.; Kasai, K.; Saito, N. Spatiotemporal Differentiation of MMN From N1 Adaptation: A Human ECoG Study. Front Psychiatry 2020, 11, 586. PMID: 32670112; PMCID: PMC7333077. [CrossRef]
- Kucuk, CA.; Dere, HH.; Mujdeci, B. Evaluating the Effectiveness of a New Auditory Training Program on the Speech Recognition Skills and Auditory Event-Related Potentials in Elderly Hearing Aid Users. Audiol Neurootol 2022, 27, 368-376. Epub 2022 Apr 8. PMID: 35398843. [CrossRef]
- Ibraheem, OA.; Kolkaila, EA.; Nada, EH.; Gad, NH. Auditory cortical processing in cochlear-implanted children with different language outcomes. Eur Arch Otorhinolaryngol 2020, 277, 1875-1883. Epub 2020 Apr 8. PMID: 32270327. [CrossRef]
- Onuma, N.; Mizuno,E. Needs Assessment for Audiological Support According to the Self-Evaluation of Hearing Problems in Elderly People. Tsukuba College of Technology Techno Report 2001, 8, 145-152.
- Humes, LE. The World Health Organization's hearing-impairment grading system: an evaluation for unaided communication in age-related hearing loss. Int J Audiol 2019, 58, 12-20. Epub 2018 Oct 15. PMID: 30318941; PMCID: PMC6351193. [CrossRef]
- Inui, K.; Okamoto, H.; Miki, K.; Gunji, A.; Kakigi, R. Serial and parallel processing in the human auditory cortex: a magnetoencephalographic study. Cereb Cortex 2006, 16, 18-30. Epub 2005 Mar 30. PMID: 15800024. [CrossRef]
- Gil, D.; Iorio, MC. Formal auditory training in adult hearing aid users. Clinics (Sao Paulo) 2010, 65, 165-174. PMID: 20186300; PMCID: PMC2827703. [CrossRef]
- Lavie, L.; Banai, K.; Karni, A.; Attias, J. Hearing Aid-Induced Plasticity in the Auditory System of Older Adults: Evidence From Speech Perception. J Speech Lang Hear Res 2015, 58, 1601-1610. PMID: 26163676. [CrossRef]
- Yumba, WK. Cognitive Processing Speed, Working Memory, and the Intelligibility of Hearing Aid-Processed Speech in Persons with Hearing Impairment. Front Psychol 2017, 15, 1308. PMID: 28861009; PMCID: PMC5559705. [CrossRef]
- Moore, BC.; Vinay, SN. Enhanced discrimination of low-frequency sounds for subjects with high-frequency dead regions. Brain 2009, 132(Pt 2), 524-36. Epub 2008 Nov 26. PMID: 19036764. [CrossRef]
- Andrillon, T.; Kouider, S.; Agus, T.; Pressnitzer, D. Perceptual learning of acoustic noise generates memory-evoked potentials. Curr Biol 2015, 25, 2823-2829. Epub 2015 Oct 8. PMID: 26455302. [CrossRef]
- Gommeren, H.; Bosmans, J.; Cardon, E.; Mertens, G.; Cras, P.; Engelborghs, S.; Van, Ombergen, A.; Gilles, A.; Lammers, M.; Van, Rompaey, V. Cortical Auditory Evoked Potentials in Cognitive Impairment and Their Relevance to Hearing Loss: A Systematic Review Highlighting the Evidence Gap. Front Neurosci 2021, 15, 781322. PMID: 34867176; PMCID: PMC8637533. [CrossRef]
- Picton, T. Hearing in time: evoked potential studies of temporal processing. Ear Hear 2013, 34, 385-401. PMID: 24005840. [CrossRef]
- Ben-David, BM.; Campeanu, S.; Tremblay, KL.; Alain, C. Auditory evoked potentials dissociate rapid perceptual learning from task repetition without learning. Psychophysiology 2011, 48, 797-807. Epub 2010 Nov 5. PMID: 21054432. [CrossRef]
- Ross, B.; Jamali, S.; Tremblay, KL. Plasticity in neuromagnetic cortical responses suggests enhanced auditory object representation. BMC Neurosci 2013, 14, 151. PMID: 24314010; PMCID: PMC3924184. [CrossRef]
- Tremblay, K.; Kraus, N.; McGee, T.; Ponton, C.; Otis, B. Central auditory plasticity: changes in the N1-P2 complex after speech-sound training. Ear Hear 2001, 22, 79-90. PMID: 11324846. [CrossRef]
- Lightfoot, G.; Kennedy, V. Cortical electric response audiometry hearing threshold estimation: accuracy, speed, and the effects of stimulus presentation features. Ear Hear 2006, 27, 443-456. PMID: 16957496. [CrossRef]
- Petersen, EB. Hearing-Aid Directionality Improves Neural Speech Tracking in Older Hearing-Impaired Listeners. Trends Hear 2022, 26, 23312165221099894. PMID: 35730193; PMCID: PMC9228639. [CrossRef]
- Van, Dun, B.; Kania, A.; Dillon, H. Cortical Auditory Evoked Potentials in (Un)aided Normal-Hearing and Hearing-Impaired Adults. Semin Hear 2016, 37, 9-24. PMID: 27587919; PMCID: PMC4910567. [CrossRef]
- Näätänen, R.; Paavilainen, P.; Rinne, T.; Alho, K. The mismatch negativity (MMN) in basic research of central auditory processing: a review. Clin Neurophysiol 2007, 118, 2544-2590. Epub 2007 Oct 10. PMID: 17931964. [CrossRef]
- Cheng, CH.; Baillet, S.; Hsiao, FJ.; Lin, YY. Effects of aging on the neuromagnetic mismatch detection to speech sounds. Biol Psychol 2015, 104, 48-55. Epub 2014 Nov 15. PMID: 25451380. [CrossRef]
- Korczak, PA.; Kurtzberg, D.; Stapells, DR. Effects of sensorineural hearing loss and personal hearing AIDS on cortical event-related potential and behavioral measures of speech-sound processing. Ear Hear 2005, 26, 165-185. PMID: 15809543. [CrossRef]
- Cai, Y.; Zheng, Y.; Liang, M.; Zhao, F.; Yu, G.; Liu, Y.; Chen, Y.; Chen, G. Auditory Spatial Discrimination and the Mismatch Negativity Response in Hearing-Impaired Individuals. PLoS One 2015, 10, e0136299. PMID: 26305694; PMCID: PMC4549058. [CrossRef]
- Fu, M.; Wang, L.; Zhang, M.; Yang, Y.; Sun, X. A mismatch negativity study in Mandarin-speaking children with sensorineural hearing loss. Int J Pediatr Otorhinolaryngol 2016, 91, 128-140. Epub 2016 Oct 24. PMID: 27863627. [CrossRef]
- Nikjeh, DA.; Lister, JJ.; Frisch, SA. Preattentive cortical-evoked responses to pure tones, harmonic tones, and speech: influence of music training. Ear Hear 2009, 30, 432-446. PMID: 19494778. [CrossRef]
- Zhang, D.; Ma, Y. Repetitive transcranial magnetic stimulation improves both hearing function and tinnitus perception in sudden sensorineural hearing loss patients. Sci Rep 2015, 5, 14796. PMID: 26463446; PMCID: PMC4604476. [CrossRef]
- Uchida, Y.; Nishita, Y.; Tange, C.; Sugiura, S.; Otsuka, R.; Ueda, H.; Nakashima, T.; Ando, F.; Shimokata, H. The Longitudinal Impact of Hearing Impairment on Cognition Differs According to Cognitive Domain. Front Aging Neurosci 2016, 8, 201. PMID: 27597827; PMCID: PMC4992677. [CrossRef]
- Acar, B.; Yurekli, MF.; Babademez, MA.; Karabulut, H.; Karasen, RM. Effects of hearing aids on cognitive functions and depressive signs in elderly people. Arch Gerontol Geriatr 2011, 52, 250-252. Epub 2010 May 15. PMID: 20472312. [CrossRef]
- Allen, NH.; Burns, A.; Newton, V.; Hickson, F.; Ramsden, R.; Rogers, J.; Butler, S.; Thistlewaite, G.; Morris, J. The effects of improving hearing in dementia. Age Ageing 2003, 32, 189-193. PMID: 12615563. [CrossRef]
Figure 1.
Self-evaluation questionnaire for hearing problems related to voice. The total score was calculated. The translated version of the test is shown above, and the original test used in this study is shown below.
Figure 1.
Self-evaluation questionnaire for hearing problems related to voice. The total score was calculated. The translated version of the test is shown above, and the original test used in this study is shown below.
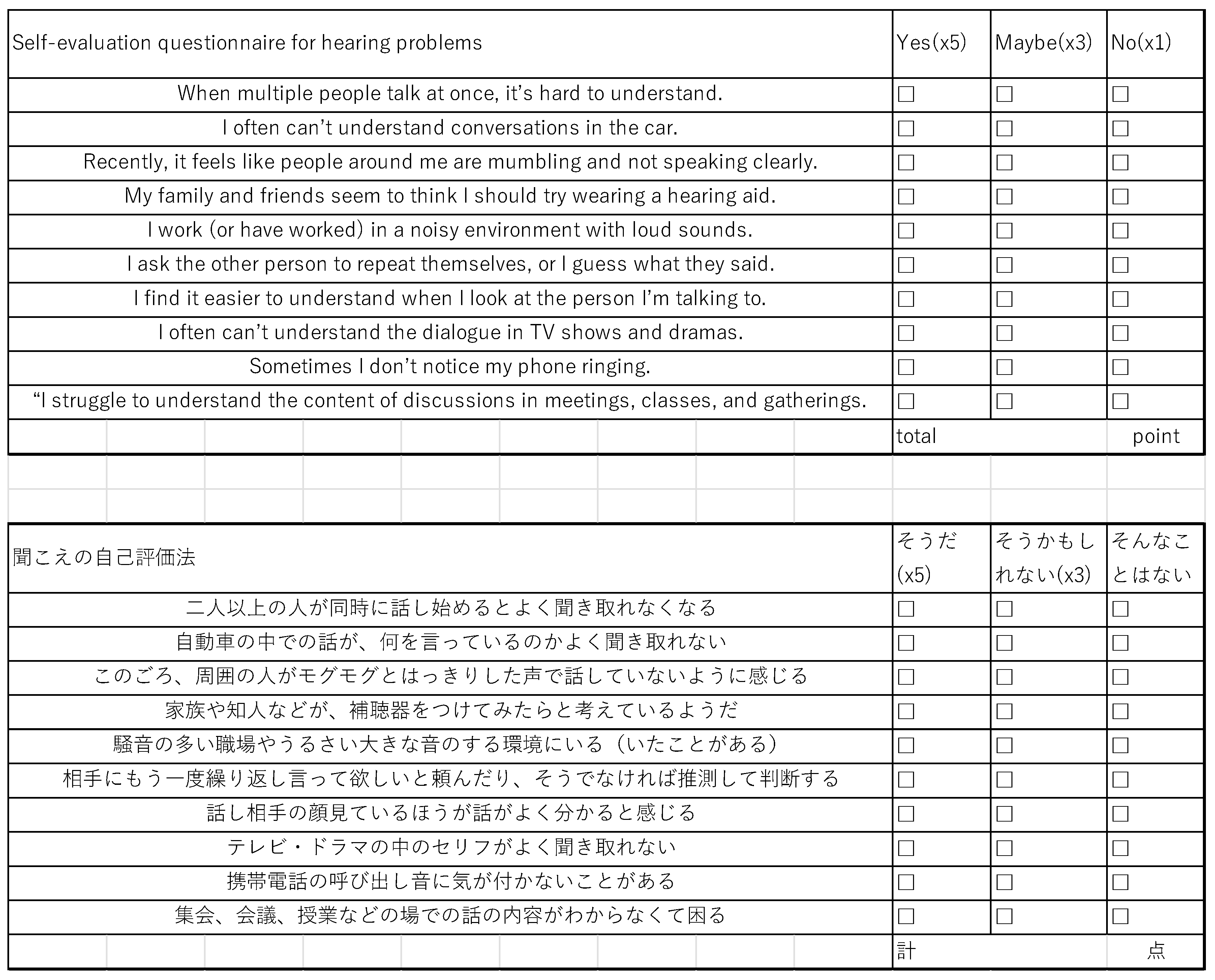
Figure 2.
SINT in the better hearing ear: HQ and HF-HQ exhibited significant improvement in S/N+10 after sound therapy (A, D), whereas Ctrl and HF-Ctrl did not show any significant differences (B, E). The improved accuracy rate in the better hearing ear in HQ did not show any significant differences compared to Ctrl (C), but HF-HQ exhibited significant improvement in S/N+10 compared to HF-Ctrl (F). (G) Hearing level in the better hearing ear and improved accuracy rate with the accuracy rate in S/N+10 before sound therapy in HQ. Improvement in SINT in S/N+10 was observed across all hearing levels in this study, with the higher improvement seen in those with low accuracy rates before sound therapy.
Figure 2.
SINT in the better hearing ear: HQ and HF-HQ exhibited significant improvement in S/N+10 after sound therapy (A, D), whereas Ctrl and HF-Ctrl did not show any significant differences (B, E). The improved accuracy rate in the better hearing ear in HQ did not show any significant differences compared to Ctrl (C), but HF-HQ exhibited significant improvement in S/N+10 compared to HF-Ctrl (F). (G) Hearing level in the better hearing ear and improved accuracy rate with the accuracy rate in S/N+10 before sound therapy in HQ. Improvement in SINT in S/N+10 was observed across all hearing levels in this study, with the higher improvement seen in those with low accuracy rates before sound therapy.

Figure 3.
STG responses to 1000 Hz and 4000 Hz pure tone stimulation at 50, 55, and 60 dB (HQ group, n=14) (Lt: left, Rt: right): Stimulation at 1000 Hz elicited N1m and P2m responses, whereas stimulation at 4000 Hz did not elicit any clear magnetic deflections.
Figure 3.
STG responses to 1000 Hz and 4000 Hz pure tone stimulation at 50, 55, and 60 dB (HQ group, n=14) (Lt: left, Rt: right): Stimulation at 1000 Hz elicited N1m and P2m responses, whereas stimulation at 4000 Hz did not elicit any clear magnetic deflections.
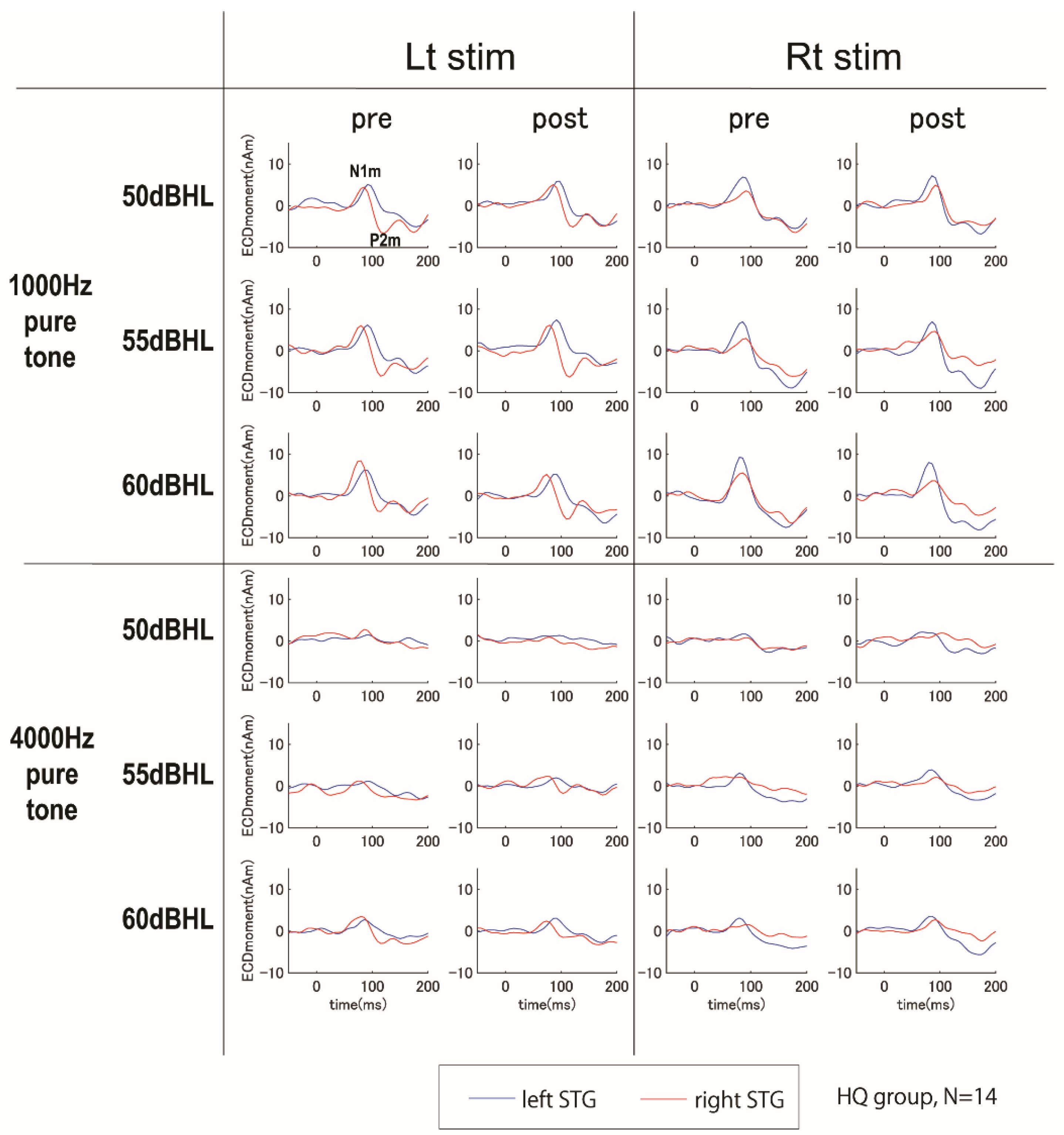
Figure 4.
N1m-P2m amplitude in the left STG (Lt STG): HQ (A) and HF-HQ (B) exhibited significant improvement in N1m-P2m amplitude at 55 dB (HF-HQ) and 60 dB (HQ/HF-HQ) (p<0.05), whereas Ctrl/HF-Ctrl did not show any significant change in the left STG after sound therapy.
Figure 4.
N1m-P2m amplitude in the left STG (Lt STG): HQ (A) and HF-HQ (B) exhibited significant improvement in N1m-P2m amplitude at 55 dB (HF-HQ) and 60 dB (HQ/HF-HQ) (p<0.05), whereas Ctrl/HF-Ctrl did not show any significant change in the left STG after sound therapy.
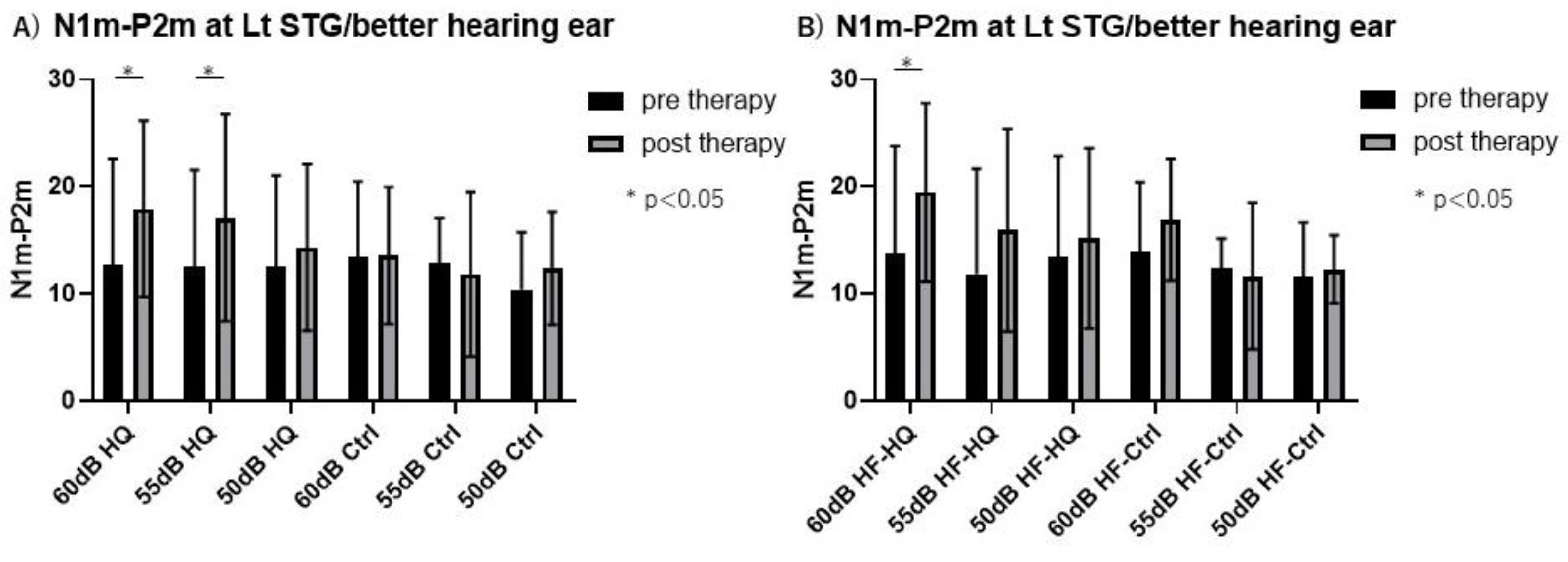
Figure 5.
Superimposed auditory-evoked fields in HQ and Ctrl. Blue indicates pre-sound therapy, and red indicates post-sound therapy. Clear deflections (MMNm) were observed around 100-250 ms in both STG for HQ and Ctrl. Data are represented as mean ± SD.
Figure 5.
Superimposed auditory-evoked fields in HQ and Ctrl. Blue indicates pre-sound therapy, and red indicates post-sound therapy. Clear deflections (MMNm) were observed around 100-250 ms in both STG for HQ and Ctrl. Data are represented as mean ± SD.
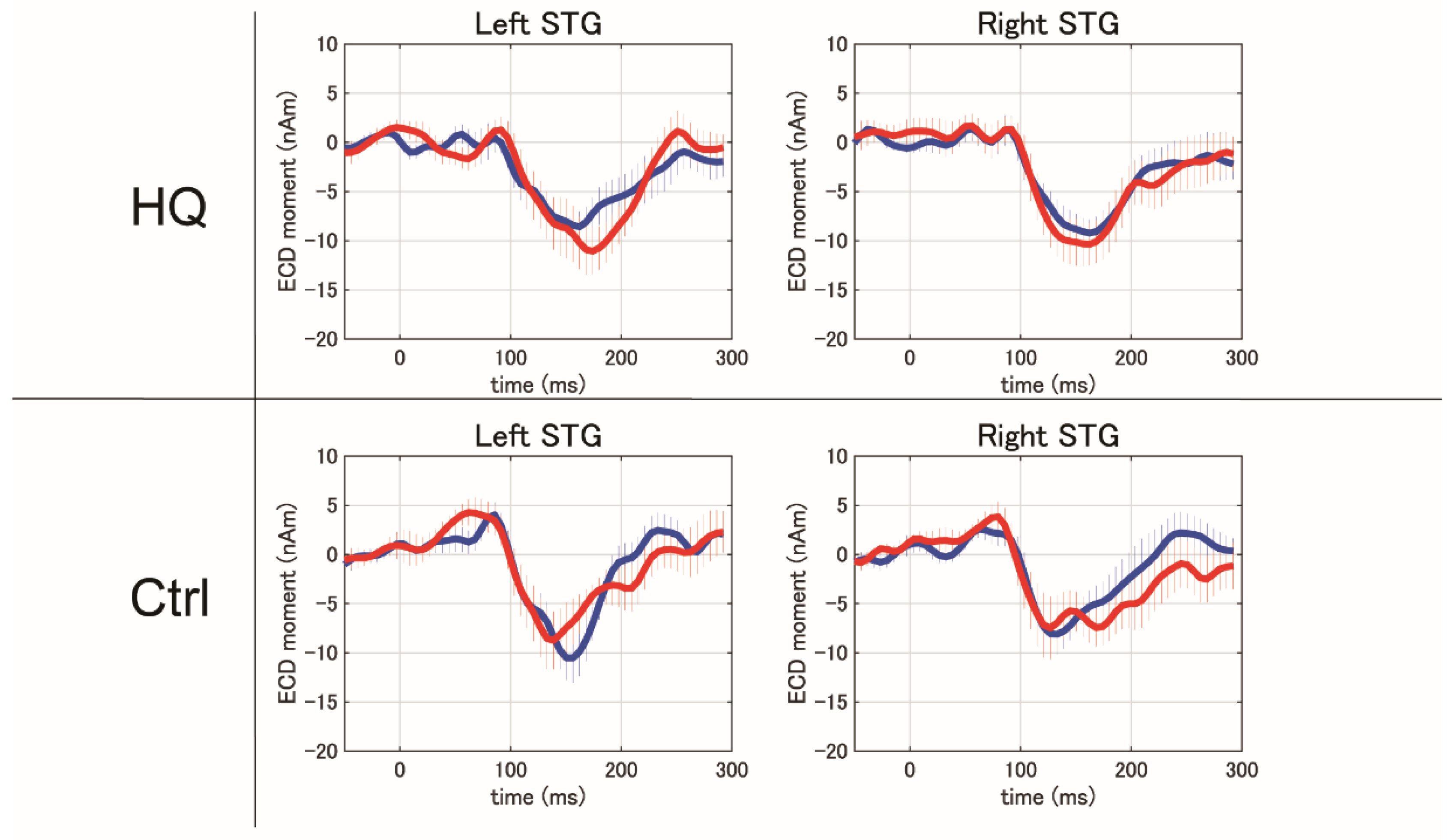
Figure 6.
MMNm amplitude in left (Lt) and right (Rt) STG at pre- and post-sound therapy: HQ/HF-HQ showed a significant increase in MMNm amplitude at the left STG after sound therapy (p<0.01 for HQ and p<0.05 for HF-HQ), whereas Ctrl/HF-Ctrl did not exhibit any significant differences between pre- and post-sound therapy.
Figure 6.
MMNm amplitude in left (Lt) and right (Rt) STG at pre- and post-sound therapy: HQ/HF-HQ showed a significant increase in MMNm amplitude at the left STG after sound therapy (p<0.01 for HQ and p<0.05 for HF-HQ), whereas Ctrl/HF-Ctrl did not exhibit any significant differences between pre- and post-sound therapy.
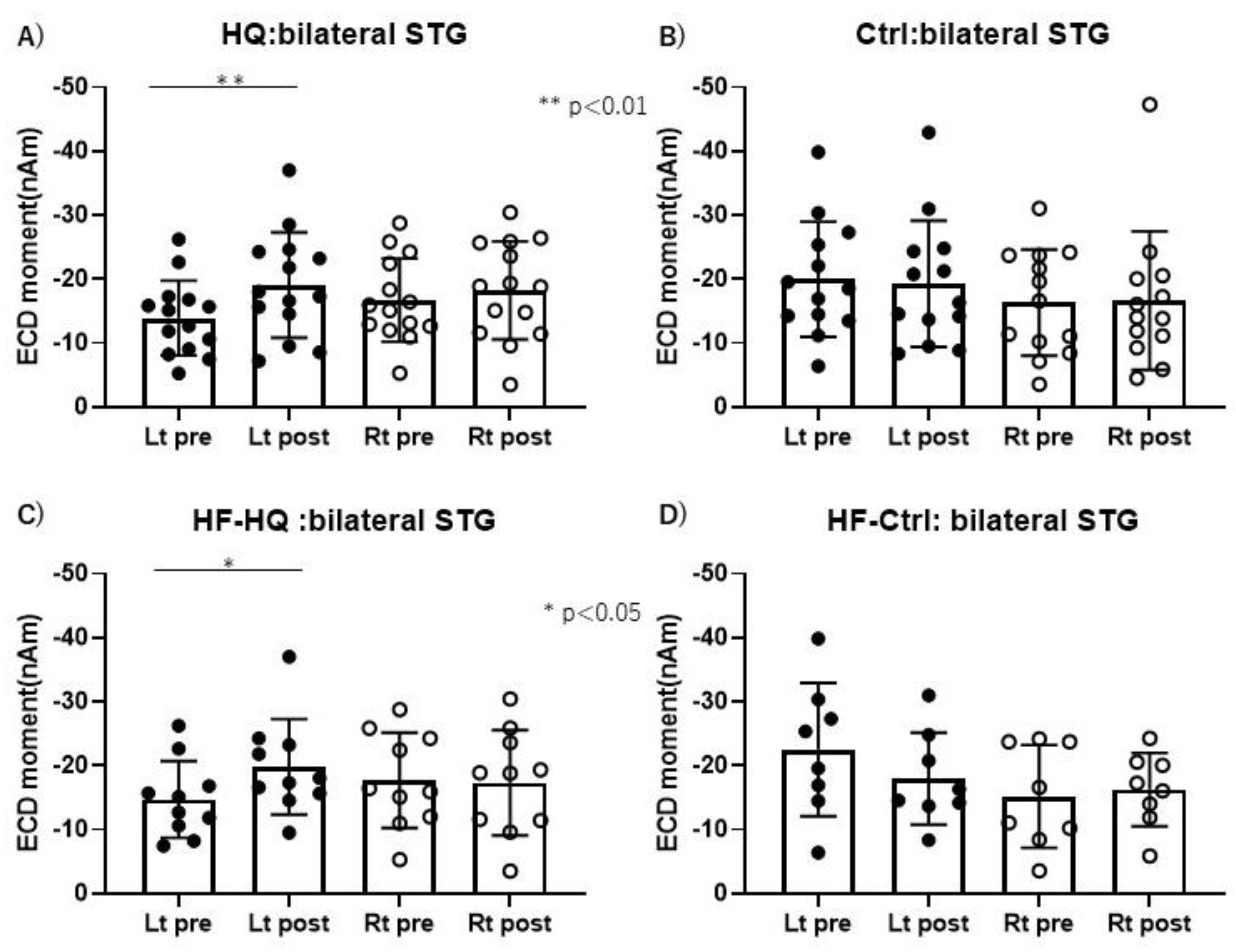

Table 1.
patient’s demographics. There were no significant differences in the demographics of participants between the two sound therapy groups.
Table 1.
patient’s demographics. There were no significant differences in the demographics of participants between the two sound therapy groups.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



