Submitted:
27 August 2024
Posted:
29 August 2024
Read the latest preprint version here
Abstract
Nasal tumors are some of the most common tumors in aged golden retrievers. Nasal tumors are mostly found to be adenocarcinomas or carcinomas. Radiation therapy is the first option to debulk the tumor, and oral or intravenous chemotherapy is administered depending on the prognosis. Therefore, it is important to select the most appropriate drug for chemotherapy considering the price and the presence of concurrent disease. Anticancer drugs include first-generation chemotherapies, second-generation targeted anticancer drugs, and third-generation immunotherapy drugs. Considering their price and effectiveness, first- or second-generation anticancer drugs are mainly used.
We report a case in which a retriever with a nasal tumor was successfully treated and managed using a combination of chlorambucil (4mg/day, SID) and prednisolone (10mg/day) orally for 9 months at a general practice. A 35 kg spayed female golden retriever aged 8 years and 8 months visited the Bundang New York Animal Hospital in July 2023. A protocol of 4 weeks of chemotherapy followed by 1 week of rest was repeated, and the nasal exudate persisted. The exudate was significantly reduced. The size of the nasal tumor was monitored using CT imaging at a referral hospital, and the images were taken in the following order: 1. before radiation therapy at the referral hospital and before chemotherapy; 2. after radiation therapy and before chemotherapy; and 3. after radiation therapy and after chemotherapy. Since the first instance of nasal bleeding, 12 months have passed (as of July 24). The nasal exudate is barely visible, and the retriever’s vital signs and weight remain stable. The size of the nasal tumor significantly decreased after 9 months of chemotherapy without moderate side effects. This study demonstrates that a prednisolone/chlorambucil metronomic combination can be an alternative to second-generation anticancer drugs as it is the cheapest and most effective way to manage tumors along with conventional radiation therapy.
Keywords:
nasal tumor
; nasal carcinoma
; prednisolone/chlorambucil metronomic combination
; First-generation chemotherapy
Introduction
Nasal tumors are often seen in retrievers. Radiation therapy is used to debulk the tumor, and then oral or intravenous chemotherapy is administered, depending on the prognosis. Anticancer drugs include first-generation chemotherapy, second-generation targeted anticancer drugs, and third-generation immunotherapy drugs. Considering their price and effectiveness, first- or second-generation anticancer drugs are mainly used. In this paper, we report a case in which a retriever with a nasal tumor was successfully treated and managed using a metronomic combination of chlorambucil (commercial name: Leukeran) and prednisolone, which are commonly used in combination for cat nasal tumors. A 35kg neutered female retriever aged 8 years and 8 months visited the hospital with nosebleeds as the main complaint. At the referral hospital, she was first diagnosed with immune-mediated thrombocytopenia (IMT) and concurrent hypothyroidism. The concurrent disease was treated for 4 weeks, and bloodwork results normalized except for epistaxis, which decreased but persisted. A CT scan was performed, and a diagnosis of a tumor with first occurrence was given. The nasal carcinoma diagnosis was confirmed via consecutive fine-needle aspiration (FNA). A histopathology examination was not performed because of a technical issue related to the clients’ consent. The nasal carcinoma was treated with radiation therapy three times (10gy). Then, while management with the second-generation anticancer drug sorafenib continued, nasal exudation persisted, so the client consented to switching from sorafenib to the first-generation anticancer drug combination chlorambucil/prednisolone. These were given as a combination consisting of 10mg/day of prednisolone and 4mg/day of chlorambucil PO. The protocol of 4 weeks of chemotherapy followed by 1 week of rest was repeated, and the nasal exudate decreased significantly.
Material and Methods
A CT scan and radiation therapy were performed on a 35 kg spayed female Golden Retriever aged 8 years and 8 months at a referral hospital (Juk-Jeon Sky Animal Hospital). Three rounds of radiation therapy at 10gy were given at the Royal Animal Hospital, along with a CT scan. Fine-needle aspiration (FNA) was used to diagnose the carcinoma. After 9 months of chemotherapy with chlorambucil (3.67mg/m2; SID; PO) and prednisolone (0.28mg/kg; SID; PO) at Bundang New York Animal Hospital (general practice), a CT scan was performed for a recheck of the tumor size at the referral hospital.
Results
Since completing 4 months of this cycle, chemotherapy has been continued without rest or pause with a combined metronomic dose of chlorambucil (3.67mg/m2; SID; PO) and prednisolone (0.28mg/kg; SID; PO). Oral administration of Methotrexate (2.5mg/day) and Cyclophosphamide (50mg/day) was attempted once but stopped immediately because of a GI tract suppression side effect. The exudate was significantly reduced. The size of the nasal tumor was monitored using CT imaging, and images were taken in the following order: 1. before radiation therapy and before chemotherapy; 2. after radiation therapy and before chemotherapy; and 3. after radiation therapy and after chemotherapy. Since the first symptom of nasal bleeding appeared, 12 months have passed (as of July 24, 2024). The nasal exudate has become barely visible, and the retriever’s vital signs remain stable with mild palpable lymph node enlargement. Hypothyroidism is being managed by continuously administering levothyroxine sodium, and the retriever’s body weight has increased from 35kg to 39kg despite chemotherapy. No other tumor was detected via a recent CT scan except for a liver mass (2.1*2.5cm), which was present before the nasal tumor and was diagnosed benign via an ultrasound scan. There was no sign of Cushing’s disease despite the frequent use of prednisolone, and the retriever’s appetite was great throughout the entire process.
Discussion
The combination of prednisolone and chlorambucil to treat nasal tumors is often used in cats [1] [2] but not in dogs. This study is the first report of successfully treating nasal carcinoma in a dog using the metronomic combination. It is known that a high corticosteroid dose decreases the toxicity of Interleukin (IL)-2, which is mainly secreted by activated T cells and facilitates the migration of macrophages by inhibiting migration inhibitory factor [3]. Also, glucocorticoids are empirically used to treat emesis and directly destroy leukemic lymphoblasts [4]. Therefore, steroids are commonly used to treat various types of cancer along with chemotherapy. Chlorambucil induces apoptosis through the alkylation of cross-linked cell DNA strands [5]. In contrast, Sorafenib is a multi-kinase inhibitor (Raf serine/threonine kinases, vascular endothelial growth factor receptor, platelet-derived growth factor receptor-β, and tyrosine kinases) [6]. Therefore, the side effects of chlorambucil may be more significant than those of sorafenib. Fortunately, the typical side effects of chlorambucil, which include bone marrow suppression (anemia), gastrointestinal signs (vomiting and diarrhea), and alopecia, were not seen in this case. Liver enzymes were mildly elevated during chemotherapy, but other bloodwork results were normal (BUN 33.2 (9.2~29.2), CRE 0.94 (0.4~1.4), ALT 93 (17~78), AST 34 (17~44), and ALP 439 (47~254)).
The advantage of chlorambucil is that it is easier to obtain and cheaper than sorafenib. Chemotherapy for large dogs requires a greater quantity of drugs than for small dogs, so many owners hesitate to opt for chemotherapy because of the high cost of treatment. Therefore, metronomic chlorambucil/prednisolone chemotherapy could be an excellent choice for clients who are willing to choose chemotherapy at a general practice rather than a referral hospital because of the high price.
The results of this study do not guarantee that chlorambucil/prednisolone chemotherapy can be used alone without radiation therapy, and more background study is needed. However, they do suggest the possibility of successfully managing nasal carcinoma at a relatively low price in general practice.
Figure 1.
(A,B,C,D). Cellularity was high and cell shedding was very severe, although cells with a very high degree of malignancy were not observed. The cell integrity of the aspirate was very high, and the blood was severely infiltrated. Various types of nasal epithelial cells, such as columnar ciliated epithelium, columnar epithelium, and goblet cells, were observed in large and small groups. Neutrophils were observed in small numbers. Moderate nuclear anisotropy was observed, and three small nucleoli were clearly observed in a thick chromatin pattern. A basophilic amorphous substance thought to be nasal exudate was observed, and many melanin granules and eosinophilic granules were observed in the background. Perinuclear vacuoles, which are mainly observed in squamous cell carcinoma cells, were observed. Considering this comprehensively, the possibility of nasal carcinoma was considered, and histopathological examination was required for confirmation. Specimen: nasal cavity; single; size 5*2*3cm; incisional.
Figure 1.
(A,B,C,D). Cellularity was high and cell shedding was very severe, although cells with a very high degree of malignancy were not observed. The cell integrity of the aspirate was very high, and the blood was severely infiltrated. Various types of nasal epithelial cells, such as columnar ciliated epithelium, columnar epithelium, and goblet cells, were observed in large and small groups. Neutrophils were observed in small numbers. Moderate nuclear anisotropy was observed, and three small nucleoli were clearly observed in a thick chromatin pattern. A basophilic amorphous substance thought to be nasal exudate was observed, and many melanin granules and eosinophilic granules were observed in the background. Perinuclear vacuoles, which are mainly observed in squamous cell carcinoma cells, were observed. Considering this comprehensively, the possibility of nasal carcinoma was considered, and histopathological examination was required for confirmation. Specimen: nasal cavity; single; size 5*2*3cm; incisional.
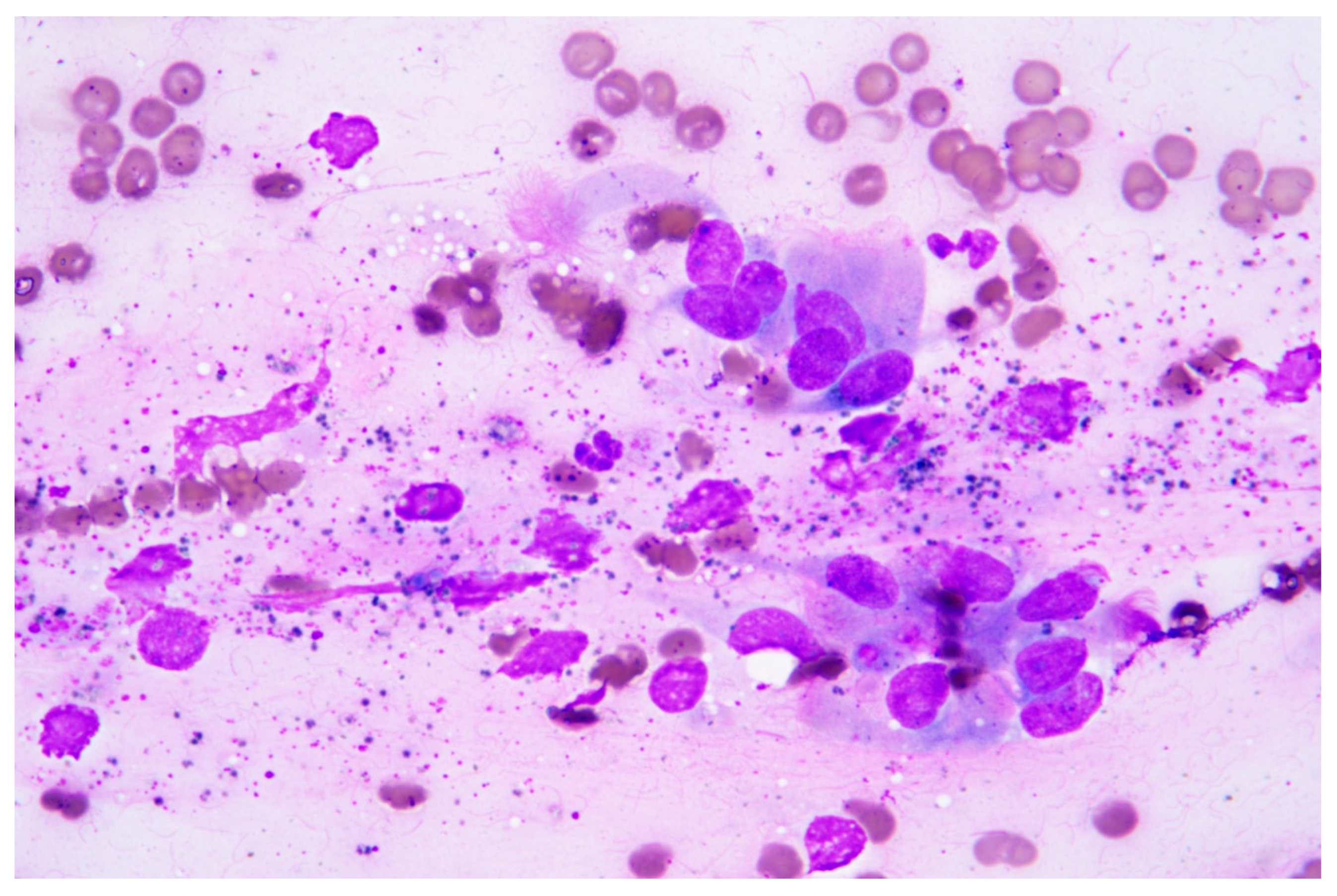
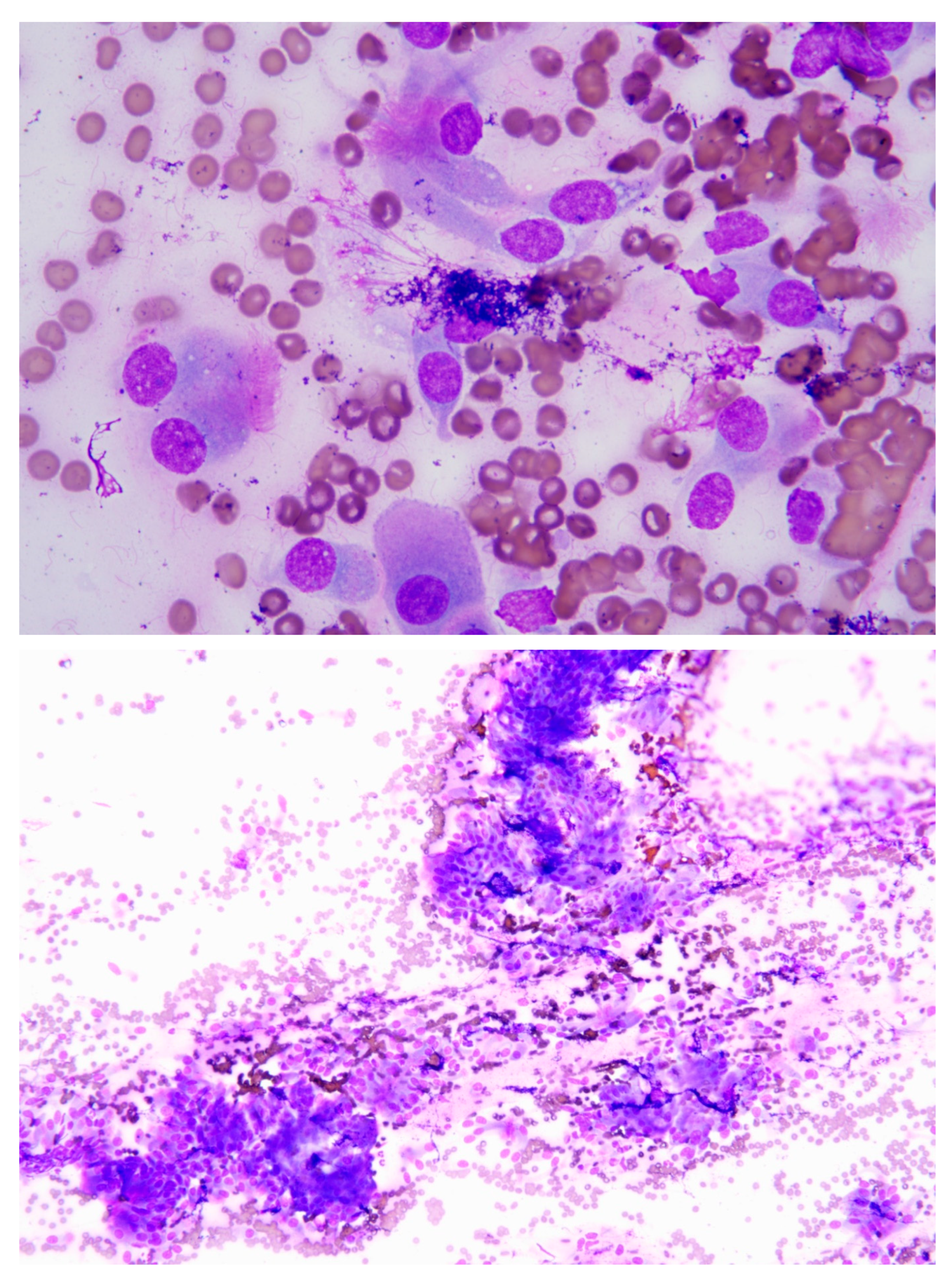
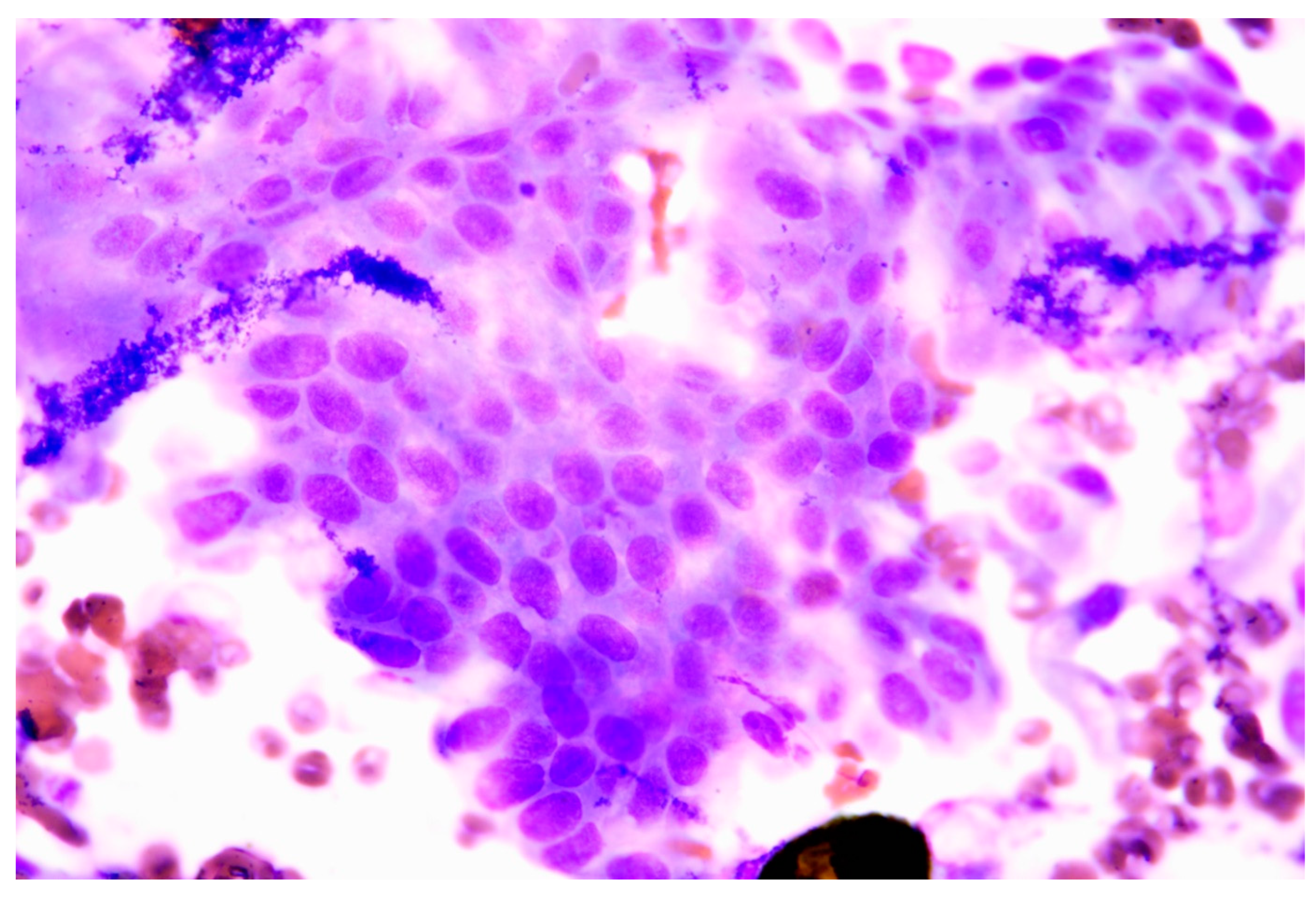
Figure 2.
(A,B,C). Axial view of CT scan of skull. The size of the tumor decreased significantly after radiation/chemotherapy compared with before radiation/chemotherapy, after radiation, and before chemotherapy (Asteroid).
Figure 2.
(A,B,C). Axial view of CT scan of skull. The size of the tumor decreased significantly after radiation/chemotherapy compared with before radiation/chemotherapy, after radiation, and before chemotherapy (Asteroid).
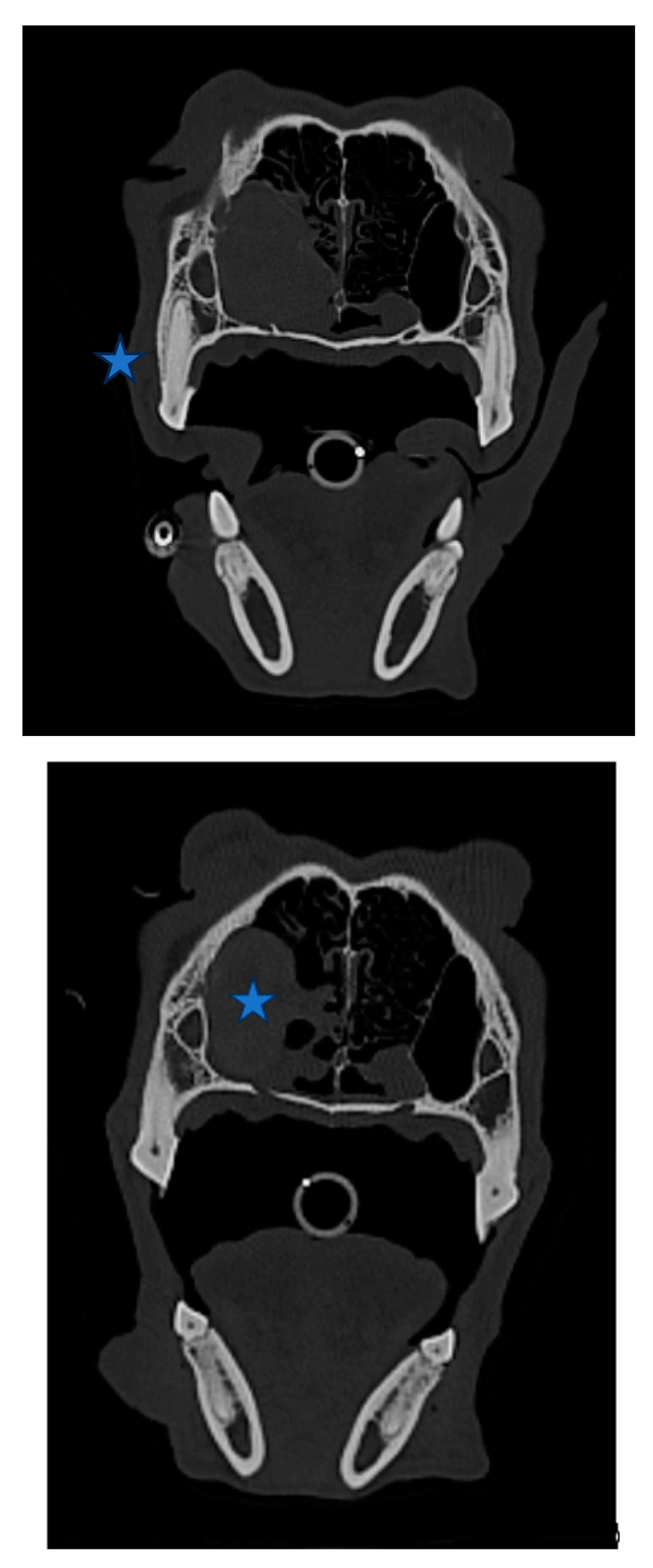
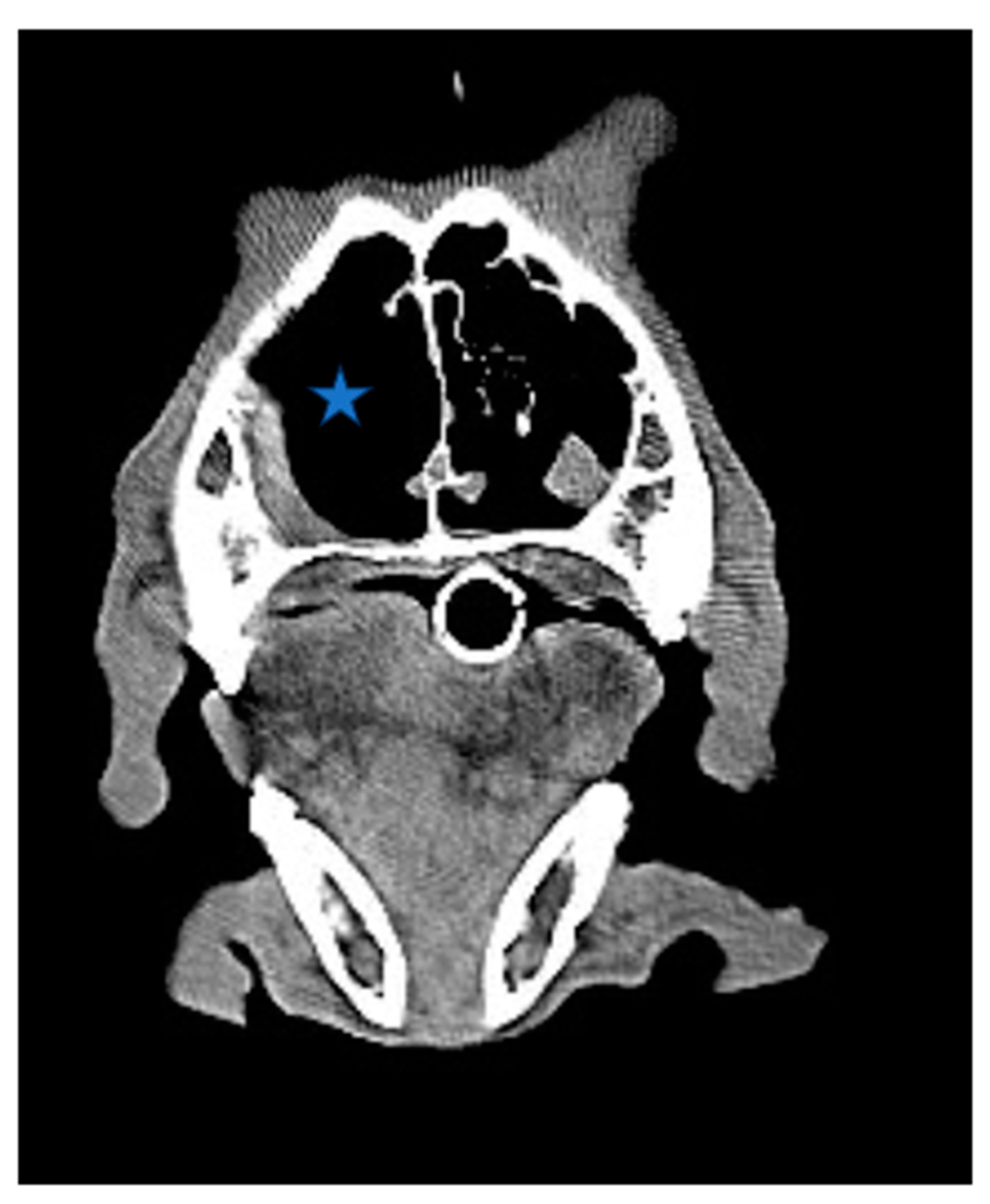
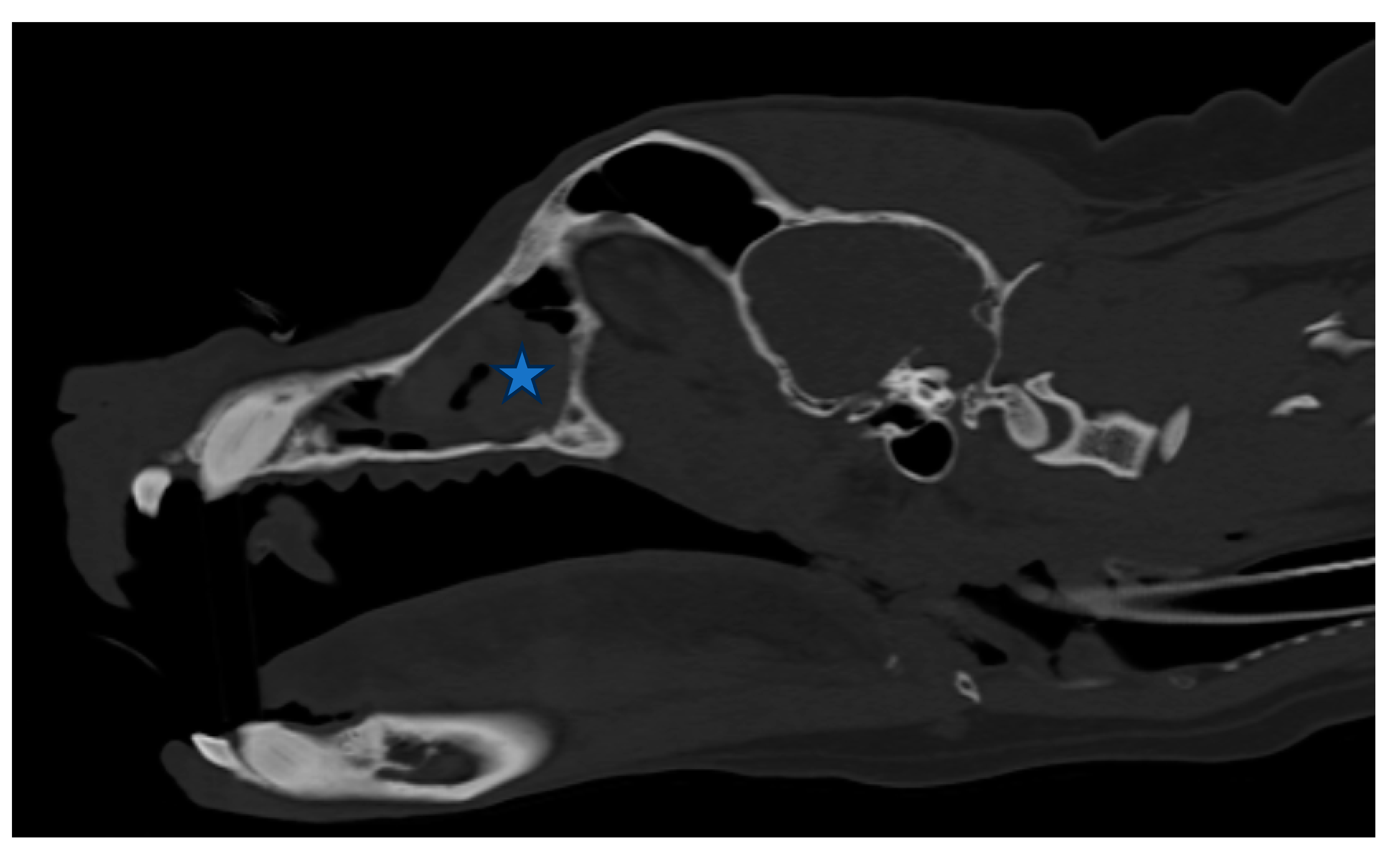
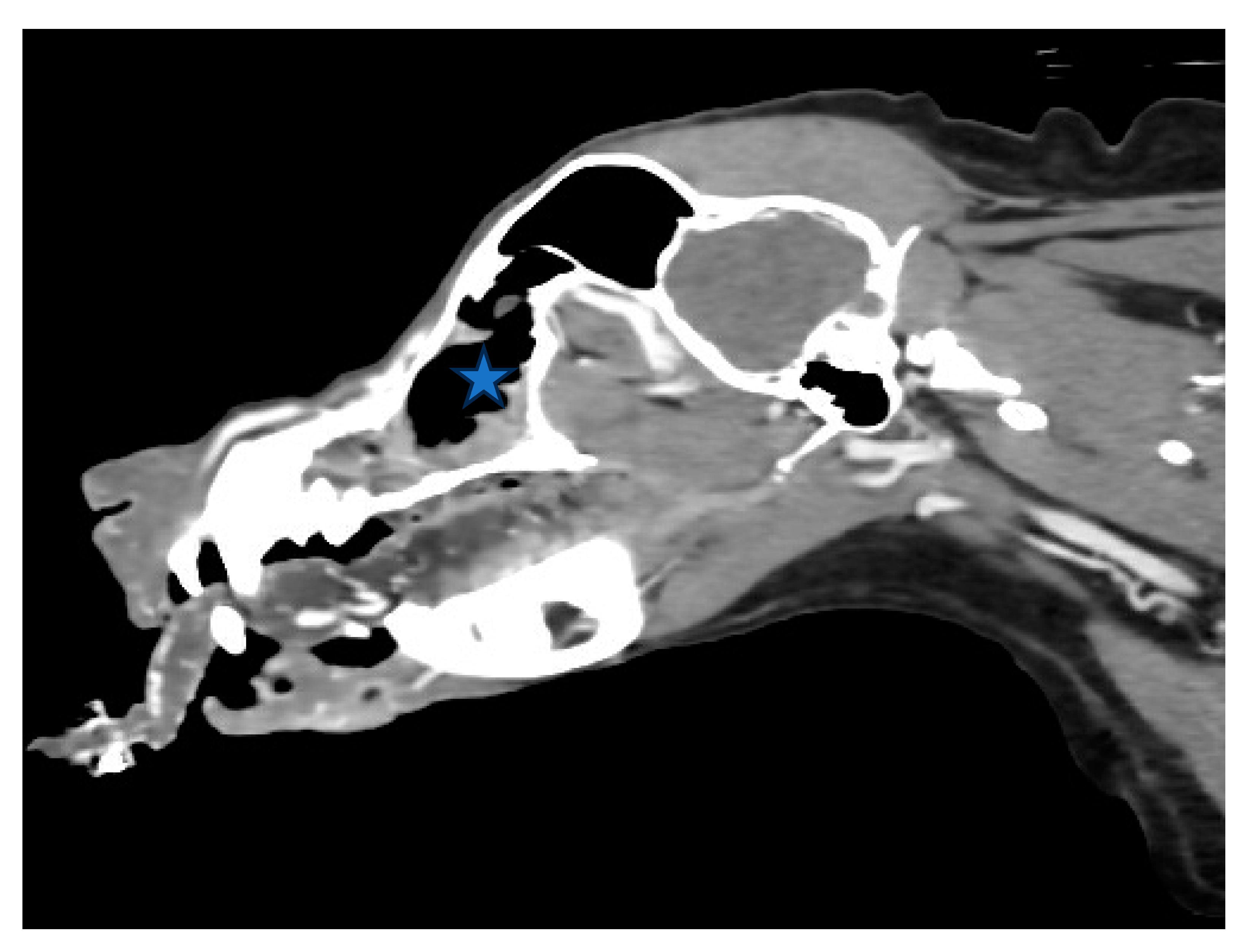
Figure 3.
(A,B). Sagittal view of CT scan of skull. The size of the nasal tumor decreased significantly (Asteroid).
Figure 3.
(A,B). Sagittal view of CT scan of skull. The size of the nasal tumor decreased significantly (Asteroid).
Acknowledgements
I would like to thank Juk-Jeon Sky Animal Hospital for the CT scan and the FNA test before diagnosis, Royal Animal Hospital for the radiation therapy and CT scan, and Bundang Leaders Animal Hospital for the CT scan after chemotherapy.
References
- Ng, K.W.L.; Beatty, J.A.; Tse, M.P.Y.; Giuliano, A. Nasal Lymphoma with Low Mitotic Index in Three Cats Treated with Chlorambucil and Prednisolone. Veter- Sci. 2022, 9, 472. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Baba, T.; Hirokawa, M.; Miyajima, M.; Kishimoto, M.; Kimura, J.; Kondo, H.; Ohmori, K. Long-term management of a cat with nasopharyngeal lymphoma by chlorambucil. Open Veter- J. 2021, 11, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Papa, M.; Vetto, J.; Ettinghausen, S.; Mule, J.; Rosenberg, S. EFFECT OF CORTICOSTEROID ON THE ANTITUMOR-ACTIVITY OF LYMPHOKINE-ACTIVATED KILLER-CELLS AND INTERLEUKIN-2 IN MICE. Cancer research, 1986, 46, 5618–5623.
- Yu, W.-B.; McElwain, M.C.; Modzelewski, R.A.; Russell, D.M.; Smith, D.C.; Trump, D.L.; Johnson, C.S. Enhancement of 1,25-Dihydroxyvitamin D3-Mediated Antitumor Activity With Dexamethasone. JNCI J. Natl. Cancer Inst. 1998, 90, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Begleiter, A.; Mowat, M.; Israels, L.G.; Johnston, J.B. Chlorambucil in Chronic Lymphocytic Leukemia: Mechanism of Action. Leuk. Lymphoma 1996, 23, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Takimoto, C.H.; Awada, A. Safety and anti-tumor activity of sorafenib (Nexavar®) in combination with other anti-cancer agents: a review of clinical trials. Cancer Chemother. Pharmacol. 2007, 61, 535–548. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



