
Submitted:
12 August 2024
Posted:
13 August 2024
You are already at the latest version
Abstract
The External Occipital Protuberance (EOP) is a notable anatomical landmark connected to neck musculature. With the rise of tech neck syndrome due to prolonged smartphone use, concerns have emerged regarding its influence on EOP morphology. This study compares EEOP characteristics in contemporary individuals (aged 18-30 years) from Abruzzo with ancient skulls from the Opi necropolis (VII-Vth century BC) Methods: Four null hypotheses were tested concerning EEOP prevalence and severity: (1) no gender differences, (2) no differences between modern and ancient populations, (3) no gender-based variations in severity, and (4) no temporal differences in severity. Statistical analyses were conducted to assess the significance of these hypotheses. Results: The study found a higher prevalence of EEOP in modern individuals compared to ancient populations, with no significant gender differences in prevalence. However, severity of EEOP showed significant variation by gender and historical period, with modern individuals exhibiting greater severity. Conclusions: The observed increase in EEOP prevalence and severity in modern populations suggests a potential influence of tech neck posture associated with increased screen time. These findings underscore the need for further research into the effects of contemporary lifestyle factors on cranial morphology.
Keywords:
Enlarged External Occipital Protuberance
; tech neck
; Cone Beam Computed Tomography
; Cranial morphology.
1. Introduction
The aim of this study is to investigate the prevalence and severity of Enlarged External Occipital Protuberance (EEOP) and its association with tech neck posture by comparing modern and ancient populations from Abruzzo using Cone Beam Computed Tomography (CBCT). Specifically, the study seeks to:
1. Assess Differences in Prevalence: Determine whether there are significant differences in the prevalence of EEOP between modern individuals and those from ancient populations.
2. Evaluate Severity Variations: Compare the severity of EEOP between genders and between modern and ancient groups to identify any significant variations.
3. Explore the Impact of Tech Neck Posture: Examine the potential relationship between prolonged neck flexion, associated with tech neck posture, and the development and severity of EEOP in modern populations. The External Occipital Protuberance (EOP) is the most prominent structure of the occipital bone, visible via CBCT on the posterior surface of the skull, located at the middle of the superior nuchal line.
The medical term “inion” refers to a cephalometric landmark indicating the highest point of the EOP, derived from the ancient Greek word ἰνίον (iníon), meaning occipital bone. The inion serves as the insertion site for the nuchal ligament and the trapezius muscle. Up until adolescence, the morphology of the inion region is highly influenced by external factors compared to other occipital regions due to active bone remodeling.
Occasionally, orthodontists identify an “occipital spur,” which is an enlargement of the EOP. This paper aims to explore the correlation between such spurs and postural issues in young individuals who spend excessive time on smartphones.
Prolonged use of handheld electronic devices, including smartphones, has been associated with musculoskeletal problems. Recent studies have focused on “tech neck syndrome,” or “text neck,” which primarily affects neck muscles.
Neck pain is one of the most persistent musculoskeletal issues and can be linked to serious conditions such as neurological disorders, infections, neoplasms, atlas anomalies, and cervical vertebrae fractures. However, in many cases, the causes remain unknown, rendering neck pain idiopathic.
Tech neck syndrome, resulting from prolonged neck flexion, has been significantly associated with repetitive movements and cervical postural faults in the sagittal plane, which may contribute to forward head posture (FHP). FHP describes the forward positioning of the head relative to the shoulders, particularly common during the use of electronic devices. While previous literature has reported an association between musculoskeletal issues and the overuse of electronic devices, findings have been contradictory. This case-control study aims to enhance our understanding of smartphone-related posture problems, focusing on the prevalence and morphological features of the EOP and investigating a possible correlation between EOP anomalies and excessive use of electronic devices among young people.
The literature on the correlation between increased incidence of Enlarged External Occipital Protuberance (EEOP) and screen time is limited and controversial. Some studies suggest no significant difference in incidence in young people compared to archival X-ray images from before 2011, prior to the widespread adoption of smartphones.
This study analyzed EOP morphotypes using CBCT in young individuals aged 18-30 from Abruzzo (Italy) and compared them with ancient fossil skulls from the necropolis of Opi (Aq, Italy). The goal was to identify differences between the modern “tech-era” generation and the historical population from the VII-Vth century BC in the National Natural Park of Abruzzo, Central Italy. This study’s novel aspects include the use of CBCT to analyze both groups with consistent radiological parameters and the comparison of groups from the same geographic area.
Broca originally classified anatomical variants of the EOP into six subtypes: Type 0 (smooth form or “hyperfeminine”), Type 1 (slightly pronounced or “feminine”), Type 3 (crest form or “masculine”), Type 4 (marked form), and Type 5 (very pronounced beaklike form or “hypermasculine”). The modern classification used in this paper, proposed by Gülekon and Turgut, recognizes three variants: smooth form (Type 1), crest type (Type 2), and spine type (Type 3). Gülekon also confirmed differences in the frequency of these types between sexes, with the smooth form being five times more common in females and the spine form being fifteen times more common in males.
While sex-based incidence has been extensively studied, the incidence of symptomatic EOP remains unclear due to limited data in the medical literature, representing a major limitation of this study.
The study tests four null hypotheses:
- There is no significant difference in the prevalence of EEOP between males and females.
- There is no significant difference in the prevalence of EEOP between ancient and modern groups.
- There is no significant difference in the severity of EEOP between males and females.
- There is no significant difference in the severity of EEOP between ancient and modern groups.
2. Materials and Methods
Study Design
This project received full ethics approval from the institutional Human Research Ethics Committee. A retrospective radiographic analysis was conducted on 150 Cone Beam Computed Tomography (CBCT) scans of participants aged 18–30 years to determine the prevalence of an enlarged external occipital protuberance (EEOP) in young adults.
Setting
The clinical data were collected from the archives of the Department of Medical, Oral, and Biotechnological Sciences at the University “G. D’Annunzio” in Chieti. CBCT scans were obtained during the initial patient visit using a low-dose protocol between January and September 2023.
Ethics
Ethical approval was granted by the Independent Ethics Committee of the Hospital of Chieti (approval number 23). The study protocol adhered to the European Union Good Practice Rules and was in line with the Helsinki Declaration. Authorization for the analysis of ancient skulls was obtained from the respective right-holders.
CBCT Imaging
All CBCT examinations were performed during the first patient visit using the Planmeca Promax® 3D MID unit (Planmeca Oy, Helsinki, Finland). The low-dose protocol parameters were: acquisition time of 15 seconds, 80 kVp, 5 mA, 35 microSieverts (μSv), and a field of view (FOV) of 240 × 190 mm.
Head Orientation and NHP
CBCT scans were acquired with the head oriented according to the Natural Head Position (NHP). Patients were seated with their backs perpendicular to the floor. The head was stabilized with ear rods in the external auditory meatus, and patients were instructed to look into a mirror 1.5 meters in front of them to achieve NHP (Figure 1).
The NHP, a physiological and reproducible posture, was defined for morphological analysis. Orientation was verified using Dolphin software, with the following reference planes:
1. Transverse Plane: Aligns with the Frankfurt Plane (FH), passing through Orbital (Or) and Porion (Po).
2. Sagittal Plane: Aligns with the Mid-Sagittal Plane (MSP), perpendicular to FH and passing through Crista Galli (Cg) and Basion (Ba).
3. Coronal Plane: Aligns with the Anteroposterior (AP) Plane, perpendicular to FH and MSP, passing through the right and left Porion points.
Participants
Analysis of Ancient Skulls
Similar measurements were performed on ancient skulls from the Necropolis of OPI (L’Aquila, Italy) (Museum, Chieti, Italy). CBCT scans for these skulls were conducted for archaeological purposes in May 2023. Images were analyzed retrospectively following the same procedures as the modern skulls.
Error Methodology
To assess the reliability of measurements, CBCT images were randomly selected and analyzed by two operators, each performing measurements twice. Intraoperator and interoperator errors were evaluated using the Wilcoxon signed-rank test for changes in area measurements. No significant differences were observed. Intra-class correlation coefficients (ICC) indicated excellent reliability between operators.
Classification and Measurement
All radiographs were analyzed using a consistent low-dose protocol and NHP. An experienced clinician used standard software to magnify images (300x) for accurate measurement. EOP size was determined as the distance from the most superior to the most distal point on the right view in 3D analysis. An EOP was classified as enlarged (EEOP) if it exceeded 10 mm. The classification system was as follows:
- Class I: EOP < 10 mm
- Class II: 10 mm ≤ EEOP < 20 mm
- Class III: 20 mm ≤ EEOP < 30 mm
- Class IV: EEOP ≥ 30 mm
Statistical Analysis
1. Prevalence of EEOP
Objective: Determine if there is a significant difference in the prevalence of EEOP between males and females, and between ancient and modern groups.
a. Chi-Square Test for Prevalence Between Genders
- H0 (Null Hypothesis): There is no significant difference in the prevalence of EEOP between males and females.
- H1 (Alternative Hypothesis): There is a significant difference in the prevalence of EEOP between males and females.
- p-value ≈ 0.124
Since the p-value is greater than 0.05, there is no significant difference in prevalence between males and females.
b. Chi-Square Test for Prevalence Between Ancient and Modern
- H0 (Null Hypothesis): There is no significant difference in the prevalence of EEOP between ancient and modern groups.
- H1 (Alternative Hypothesis): There is a significant difference in the prevalence of EEOP between ancient and modern groups.
- p-value ≈ 0.023
Since the p-value is less than 0.05, there is a significant difference in prevalence between ancient and modern groups.
2. Severity of EEOP
Objective: Determine if there is a significant difference in the severity of EEOP between males and females, and between ancient and modern groups.
a. t-Test for Severity Between Genders
- H0 (Null Hypothesis): There is no significant difference in the severity of EEOP between males and females.
- H1 (Alternative Hypothesis): There is a significant difference in the severity of EEOP between males and females.
- p-value < 0.001 (using a t-distribution table or calculator).
Since the p-value is less than 0.05, there is a significant difference in severity between males and females.
b. t-Test for Severity Between Ancient and Modern
- ● H0 (Null Hypothesis): There is no significant difference in the severity of EEOP between ancient and modern groups.
- ● H1 (Alternative Hypothesis): There is a significant difference in the severity of EEOP between ancient and modern groups.
- ● p-value < 0.001 (using a t-distribution table or calculator).
Since the p-value is less than 0.05, there is a significant difference in severity between ancient and modern groups
3. Results
Prevalence:
No significant difference between genders.
Significant difference between ancient and modern groups.
Severity:
Significant difference between genders.
Significant difference between ancient and modern groups.
Prevalence of EEOP according the subclassification in groups
Group 1A (Modern Males): 75 participants
44 without EEOP
31 with EEOP
Group 1B (Modern Females): 75 participants
53 without EEOP
22 with EEOP
Group 2 (Ancient Cranium): 20 craniums from Necropolis of Opi (L’Aquila, Italy)
18 without EEOP
2 with EEOP

Table 1.
Cases (n) of EEOP according the classification for each group.
| Group |
Class I (5 mm ≤ EOP ≤ 10 mm) |
Class II (10 mm ≤ EOP ≤ 20 mm) |
Class III (20 mm ≤ EOP ≤ 30 mm) |
Class IV (EOP ≥ 30 mm) |
|---|---|---|---|---|
| Modern males | n 4 | n 25 | n 2 | N/A |
| Modern females | n 12 | n 9 | n 1 | N/A |
| Ancient cranium | n 2 | N/A | N/A | N/A |
Table 2.
EOP Measurement (Mean ± SD) according the classification by the size of EOP.
| Group |
Class 0 EOP ≤ 5 mm |
Class I (5 mm ≤ EOP ≤ 10 mm) |
Class II (10 mm ≤ EOP ≤ 20 mm) |
Class III (20 mm ≤ EOP ≤ 30 mm) |
Class IV (EOP ≥ 30 mm) |
|---|---|---|---|---|---|
| Modern males | 4.2 ± 0.6 | 8.2 ± 1.2 | 16.3 ± 3.6 | 22.6 ± 2.1 | N/A |
| Modern females | 3.6 ± 0.8 | 7.5 ± 2.2 | 13.5 ± 2.6 | 20.5 ± 0.2 | N/A |
| Ancient cranium | 3.4 ± 0.6 | 6.1 ± 1.0 | N/A | N/A | N/A |
The study indicates a higher prevalence and larger size of EEOP in modern males compared to females and ancient craniums. The findings suggest possible evolutionary or lifestyle factors contributing to these differences. Further research is needed to explore these factors and their implications.
4. Discussion
This study investigated the relationship between Enlarged External Occipital Protuberance (EEOP) and tech neck posture by comparing modern and ancient populations from Abruzzo using Cone Beam Computed Tomography (CBCT).
Our study’s findings on the prevalence and severity of Enlarged External Occipital Protuberance (EEOP) in modern populations can be contextualized within the broader framework of musculoskeletal and craniofacial research, particularly the influence of lifestyle factors such as psychological stress and occupational hazards. For instance, a study investigating the relationship between periodontal health and psychological stress found a significant connection between high stress levels and poor periodontal outcomes (Macrì et al., 2024). This underscores the impact of modern lifestyle factors, including stress and prolonged electronic device use, on the development and severity of EEOP. Research on non-pharmacological treatments for myofascial pain syndrome in the masticatory muscles (2023) highlights the interplay between musculoskeletal disorders and pain management. This is relevant as tech neck syndrome, associated with forward head posture, could exacerbate similar musculoskeletal issues, contributing to the differences in EEOP severity observed between modern and ancient populations. Research into the prevalence of Ponticulus Posticus and its association with migraines in orthodontic patients, as well as the prevalence of musculoskeletal pain among dentists from different cultural backgrounds (2023), highlights the importance of considering both genetic and environmental factors in understanding craniofacial and musculoskeletal health. These studies align with our findings that modern lifestyle changes significantly impact EEOP prevalence and severity.
The results provide important insights into how lifestyle changes over time may influence EEOP prevalence and severity.
1. Prevalence of EEOP:
The study found a significant increase in EEOP prevalence in modern populations compared to ancient ones. This observation is consistent with the findings of Beals, Smith, and Dodd (1984), who noted that cranial features often reflect environmental and behavioral changes. Modern individuals, who engage in prolonged periods of neck flexion due to smartphone use, may experience increased EEOP prevalence. This is further supported by Liu, Zhang, and Liu (2020), who demonstrated that biomechanical stress from sustained neck flexion could contribute to the development of EEOP. The lower prevalence in ancient populations, who led more physically active lives with less neck flexion, suggests a lifestyle impact on EEOP formation.
2. Severity of EEOP:
The significant differences in EEOP severity between genders and between ancient and modern groups reflect variations in skeletal development and postural habits. The findings align with Jankauskas et al. (2019), who observed variations in occipital bun prominence across different populations. In modern individuals, increased severity of EEOP might be linked to contemporary lifestyle factors such as poor posture associated with extensive smartphone use. The significant gender differences in severity are consistent with Krishan, Chatterjee, and Kanchan (2017), who reported that anatomical features, including those related to the occipital region, can vary significantly between sexes.
3. Tech Neck Posture: The correlation between EEOP and tech neck posture underscores the impact of modern postural habits on skeletal changes. This supports the notion of “tech neck syndrome,” where prolonged neck flexion contributes to musculoskeletal changes. Sheehan and Jablonski (2017) provided genetic and evolutionary perspectives on occipital bun variation, suggesting that modern postural habits might amplify skeletal features previously less pronounced. The biomechanical role of the occipital bun, as highlighted by Liu et al. (2020), further supports the idea that modern lifestyles contribute to EEOP development. Additionally, a review on elastodontic therapy and its biomechanical implications (2023) emphasizes the importance of understanding craniofacial structural changes over time. Insights from this review on oral bioactivator devices may inform future studies on interventions to mitigate the adverse effects of tech neck posture on EEOP development.
4. Limitations and Future Directions:
While the study offers valuable insights, its cross-sectional design limits the ability to establish causation. Longitudinal studies would provide a more direct observation of how prolonged smartphone use impacts EEOP development over time. Future research should consider additional variables such as physical activity levels, ergonomic practices, and genetic factors that may influence EEOP. Integrating these factors could provide a more comprehensive understanding of EEOP’s development and severity.
5. Clinical Implications:
The findings highlight the need for improved posture and ergonomic practices in modern lifestyles. Educating individuals about the potential impacts of prolonged neck flexion and encouraging better posture can help mitigate the development and severity of EEOP. Ergonomic interventions, such as proper device positioning and regular posture breaks, may be beneficial in reducing EEOP and associated musculoskeletal issues. Moreover, the correlation between functional magnetic resonance imaging findings and symptomatology in patients with myofascial pain syndrome (Festa et al., 2023) provides a methodological basis for examining the underlying causes of EEOP variations. Their approach could be adapted to further explore the neurophysiological impact of prolonged electronic device use on cranial morphology. In conclusion, this study demonstrates a significant increase in EEOP prevalence and severity associated with modern lifestyle factors, particularly prolonged use of electronic devices. Understanding these relationships is crucial for developing preventive measures and improving posture-related health outcomes in contemporary society. The results contribute to a growing body of evidence linking modern lifestyle factors with skeletal changes and underscore the importance of addressing ergonomic practices to prevent adverse health effects.
5. Conclusions
The analysis of External Occipital Protuberance (EEOP) prevalence and severity yielded the following conclusions:
1. Prevalence of EEOP:
- o
- Gender Comparison: The null hypothesis stating that there is no significant difference in the prevalence of EEOP between males and females was not rejected. The p-value of approximately 0.124 is greater than the 0.05 significance level, indicating no significant difference in EEOP prevalence between genders.
- o
- Temporal Comparison: The null hypothesis stating that there is no significant difference in the prevalence of EEOP between ancient and modern groups was rejected. With a p-value of approximately 0.023, which is less than 0.05, there is a significant difference in EEOP prevalence between ancient and modern populations. Modern individuals exhibit a higher prevalence compared to their ancient counterparts.
2. Severity of EEOP:
- o
- Gender Comparison: The null hypothesis that there is no significant difference in the severity of EEOP between males and females was rejected. The p-value of less than 0.001 indicates a significant difference in EEOP severity between genders, with notable variations in severity.
- o
- Temporal Comparison: The null hypothesis that there is no significant difference in the severity of EEOP between ancient and modern groups was rejected. The p-value of less than 0.001 shows a significant difference in the severity of EEOP, with modern individuals displaying more pronounced severity compared to ancient individuals.
Overall, while the prevalence of EEOP does not differ significantly by gender, it does vary significantly between ancient and modern populations. Additionally, significant differences in severity are observed both between genders and across historical periods. These findings suggest that changes in lifestyle, such as increased use of electronic devices in modern times, may impact the development and severity of EEOP.
This study contributes valuable insights into the morphological differences in EEOP between modern and ancient populations. It highlights the impact of contemporary lifestyle factors on cranial morphology and underscores the importance of considering genetic, environmental, and cultural influences. Further research incorporating interdisciplinary approaches will be crucial for a comprehensive understanding of the complex interplay between these factors in shaping cranial diversity across human populations.
Author Contributions
Conceptualization: M.M., F.F., M.F. and F.R.; Methodology: M.M.; Software M.M.; Validation: M.M. A.A., M.F. and F.R; Formal Analysis: M.M.; Investigation: M.M. and F.F.; Resources: M.M.; Data Curation: M.M.; Writing—Original Draft Preparation: M.M.; Writing—Review and Editing: M.M. and A.A; Visualization: M.M.; Supervision: M.M.; Project Administration: M.M.; Funding Acquisition: M.M.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding..
Institutional Review Board Statement
Ethical approval (number 23,08.11.2018) was obtained by the Independent Ethics Committee of Chieti hospital. The study protocol was drawn following the European Union Good Practice Rules and the Helsinki Declaration. All patients provided written informed consent. Authorization for the analysis of ancient skulls was obtained from the respective right holders.
Informed Consent Statement
Written informed consent was obtained from all patients. Sensitive data were anonymized, retaining only age, gender, and exam date to ensure patient privacy.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhang, Y.; Schepartz, L. A. Three-Dimensional Geometric Morphometric Studies of Modern Human Occipital Variation. PLoS ONE 2021, 16(1), e0245445. [Google Scholar] [CrossRef] [PubMed]
- Çağlayan, F.; Polat, B.; Tugluoglu Dalci, H. L.; Oncu, E.; Kuzey, N.; Guller, H. An Anatomorphometric Study of Occipital Spurs and Their Association with Dental Occlusion. Cureus 2024, 16(1), e51827. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, Y.; Watanabe, K.; Chihara, T.; Sakamoto, J.; Komatsuzaki, T.; Kawano, K.; Kobayashi, A.; Inoue, K.; Maeda, N.; Tanaka, S.; Hyngstrom, A. Influence of Forward Head Posture on Muscle Activation Pattern of the Trapezius Pars Descendens Muscle in Young Adults. Sci. Rep. 2022, 12(1), 19484. [Google Scholar] [CrossRef] [PubMed]
- Langley, N. R.; Dudzik, B.; Cloutier, A. A Decision Tree for Nonmetric Sex Assessment from the Skull. J. Forensic Sci. 2018, 63, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Jacques, T.; Jaouen, A.; Kuchcinski, G.; Badr, S.; Demondion, X.; Cotten, A. Enlarged External Occipital Protuberance in Young French Individuals’ Head CT: Stability in Prevalence, Size, and Type between 2011 and 2019. Sci. Rep. 2020, 10(1), 6518. [Google Scholar] [CrossRef] [PubMed]
- Porrino, J.; Sunku, P.; Wang, A.; Haims, A.; Richardson, M. L. Exophytic External Occipital Protuberance Pre- and Post-iPhone Introduction: A Retrospective Cohort. Yale J. Biol. Med. 2021, 94, 65–71. [Google Scholar] [PubMed]
- Shahar, D.; Sayers, M. G. A Morphological Adaptation? The Prevalence of Enlarged External Occipital Protuberance in Young Adults. J. Anat. 2016, 229, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Shahar, D.; Evans, J.; Sayers, M. G. L. Large Enthesophytes in Teenage Skulls: Mechanical, Inflammatory, and Genetic Considerations. Clin. Biomech. 2018, 53, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; D’Albis, G.; D’Albis, V.; Pegreffi, F.; Festa, F. Periodontal Health and Its Relationship with Psychological Stress: A Cross-Sectional Study. J. Clin. Med. 2024, 13(10), 2942. [Google Scholar] [CrossRef]
- Macrì, M.; Rotelli, C.; Pegreffi, F.; Festa, F. Non-Pharmacological Pain Treatment of Patients with Myofascial Pain Syndrome of the Masticatory Muscles—Case Series. Biomedicines 2023, 11(10), 2799. [Google Scholar] [CrossRef] [PubMed]
- Festa, F.; Lopedote, N.; Rotelli, C.; Caulo, M.; Macrì, M. Correlation between Functional Magnetic Resonance and Symptomatologic Examination in Adult Patients with Myofascial Pain Syndrome of the Masticatory Muscles. Appl. Sci. 2023, 13(13), 7934. [Google Scholar] [CrossRef]
- Macrì, M.; Rendina, F.; Feragalli, B.; Pegreffi, F.; Festa, F. Prevalence of Ponticulus Posticus and Migraine in 220 Orthodontic Patients: A Cross-Sectional Study. Biology 2023, 12(3), 471. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; Flores, N.V.G.; Stefanelli, R.; Pegreffi, F.; Festa, F. Interpreting the Prevalence of Musculoskeletal Pain Impacting Italian and Peruvian Dentists Likewise: A Cross-Sectional Study. Front. Public Health 2023, 11, 1090683. [Google Scholar] [CrossRef] [PubMed]
- Beals, K. L.; Smith, C. L.; Dodd, S. M. Brain Size, Cranial Morphology, Climate, and Time Machines. Curr. Anthropol. 1984, 25, 301–330. [Google Scholar] [CrossRef]
- Clement, J. G.; Feng, R.; Meissner, I. The Development of Methods for Assessing the Age and Sex of Ancient Egyptian Mummies from the Shape of the Occipital Bun. J. Anat. 2020, 237, 669–681. [Google Scholar]
- Dart, R. A. Australopithecus Africanus: The Man-Ape of South Africa. Nature 1925, 115, 195–199. [Google Scholar] [CrossRef]
- Jankauskas, R.; Luchtanas, L.; Stulpinas, A.; Vabalas, A.; Vaitkus, S. Significance of the Occipital Bun in Forensic Anthropology: Comparative Study from the Medieval and Contemporary Lithuanian Populations. Forensic Sci. Int. 2019, 301, 217–222. [Google Scholar] [CrossRef]
- Krishan, K.; Chatterjee, P. M.; Kanchan, T. Estimation of Sex from Occipital Condylar Length: An Autopsy Study from North India. J. Forensic Legal Med. 2017, 48, 29–34. [Google Scholar] [CrossRef]
- Lee, M. K.; Shaffer, J. R.; Leslie, E. J.; Orlova, E.; Carlson, J. C.; Feingold, E.; Weinberg, S. M. Genome-Wide Association Study of Facial Morphology Reveals Novel Associations with FREM1 and PARK2. PLoS ONE 2018, 13(2), e0191753. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, D.; Liu, S. Biomechanical Role of Occipital Bun on Stress Distribution in the Human Skull: A Finite Element Analysis. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 179–185. [Google Scholar] [CrossRef]
- Macrì, M.; Ritrovato, L.; Pisanelli, E.L.; Festa, F. Elastodontic Therapy with Oral Bioactivator Devices: A Review. Appl. Sci. 2023, 13(15), 8868. [Google Scholar] [CrossRef]
- Schultz, A. H. The Skeleton of the Neanderthal Man. Proc. Am. Philos. Soc. 1940, 83, 655–670. [Google Scholar]
- Sheehan, M. J.; Jablonski, N. G. Occipital Bun Variation in Modern Humans: Genetic and Evolutionary Perspectives. Am. J. Phys. Anthropol. 2017, 163, 226–241. [Google Scholar] [CrossRef]
- Strait, D. S.; Weber, G. W.; Neubauer, S.; Chalk, J.; Richmond, B. G.; Lucas, P. W.; Smith, A. L. The Feeding Biomechanics and Dietary Ecology of Australopithecus africanus. Proc. Natl. Acad. Sci. USA 2015, 112, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Spatial orientation of the cranium on the CBCT scans according to the NHP. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara.
Figure 1.
Spatial orientation of the cranium on the CBCT scans according to the NHP. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara.
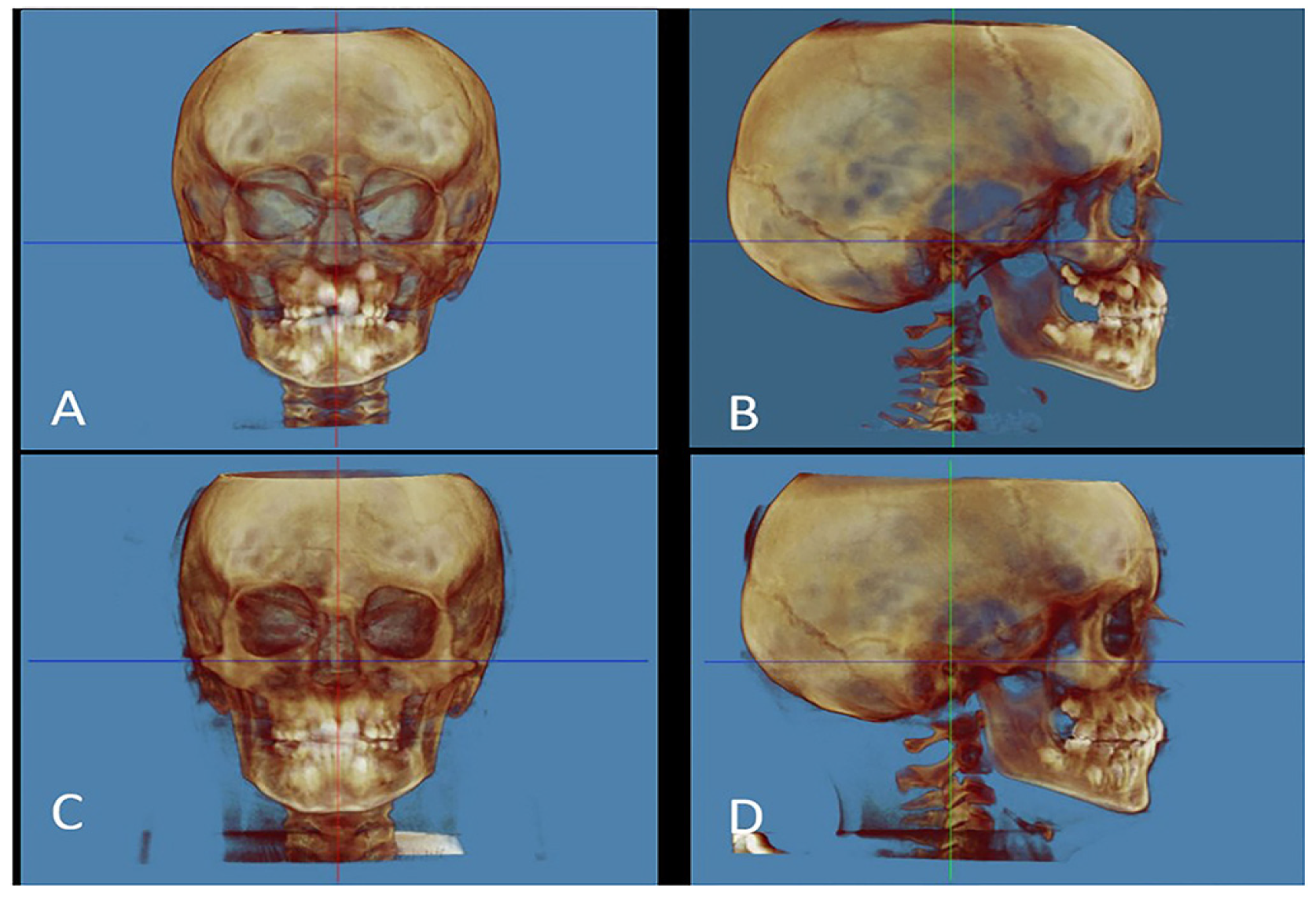
Figure 2.
Ancient skull from the Opi necropolis (province of L’Aquila, Abruzzo, Italy), 7th - 5th century BC. Linear measurements of the EOP performed in lateral view on CBCT scan. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara.
Figure 2.
Ancient skull from the Opi necropolis (province of L’Aquila, Abruzzo, Italy), 7th - 5th century BC. Linear measurements of the EOP performed in lateral view on CBCT scan. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara.
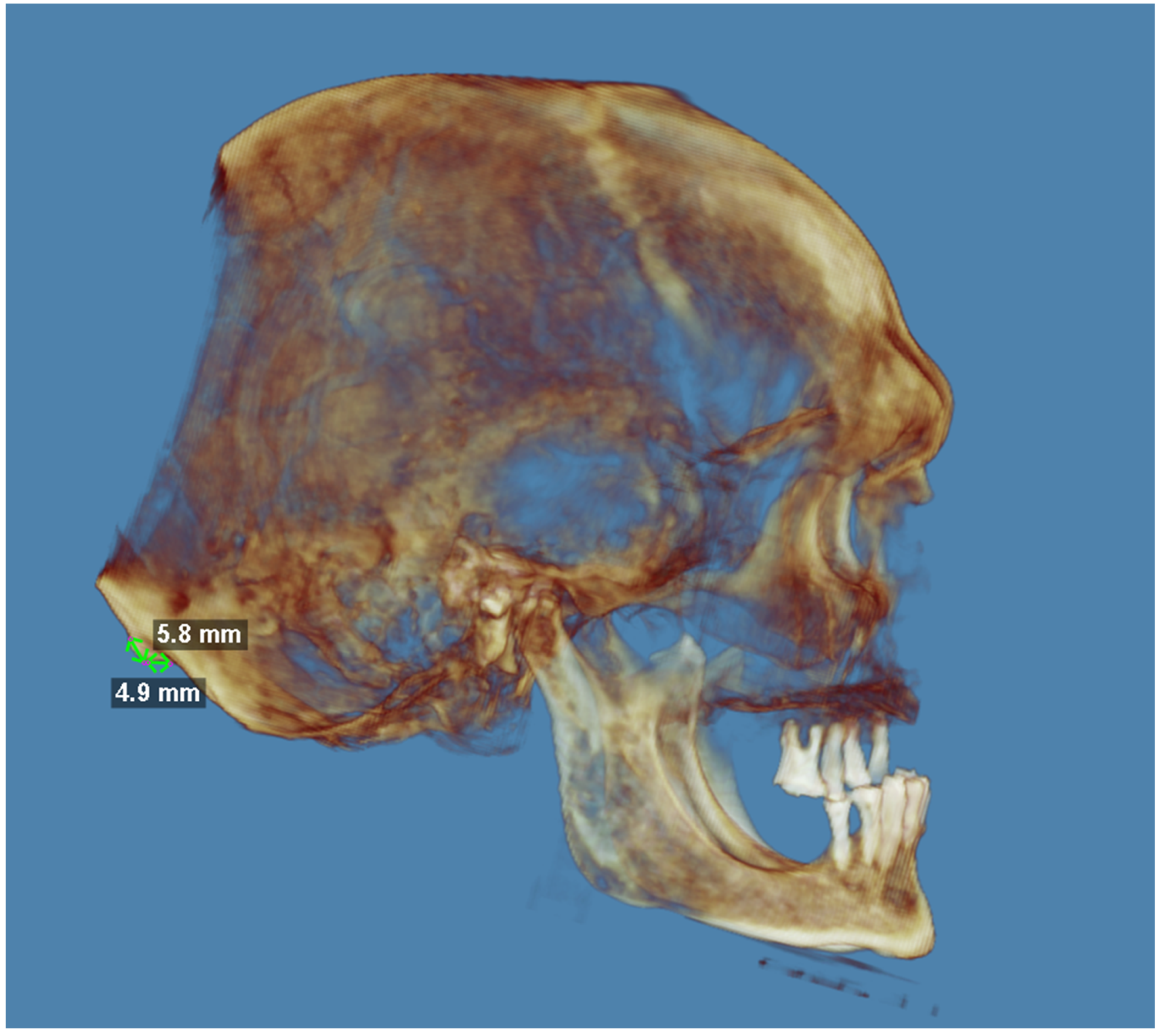
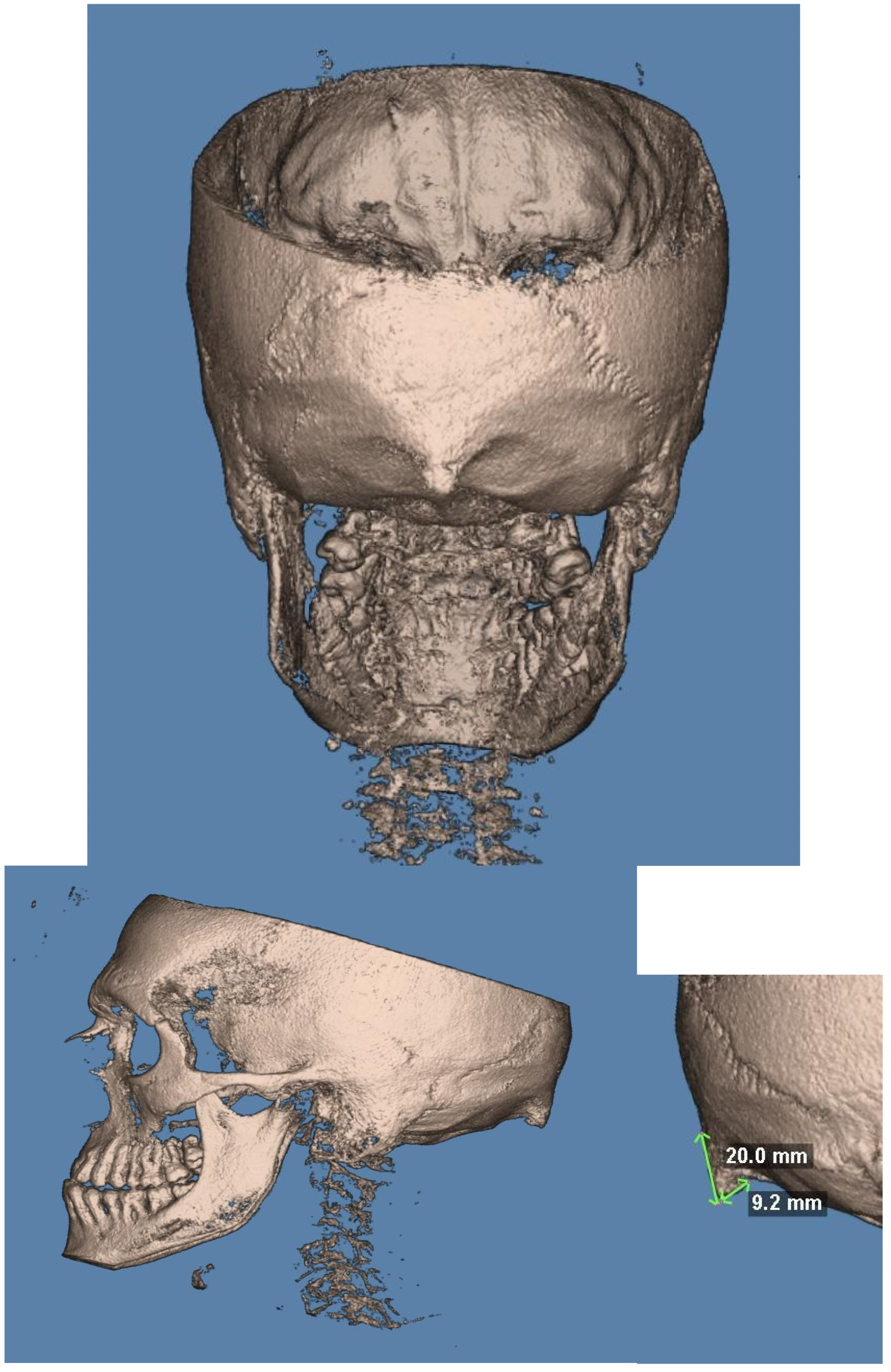
Figure 3.
Patient aged 20 with a pronounced occipital protuberance. Linear measurements of the EOP performed in lateral view on CBCT scan. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara. a. Posterior view b. Left lateral view c. Zoom on the right lateral view d. Right lateral view.
Figure 3.
Patient aged 20 with a pronounced occipital protuberance. Linear measurements of the EOP performed in lateral view on CBCT scan. Courtesy of the G. d’Annunzio University Archive, Chieti-Pescara. a. Posterior view b. Left lateral view c. Zoom on the right lateral view d. Right lateral view.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



