
Submitted:
08 July 2024
Posted:
09 July 2024
You are already at the latest version
Abstract
The treatment of patients with metastatic colorectal cancer (mCRC) is complex and impacted by the location of the primary tumor (LPT). Our study aims to emphasize the importance of LPT as a prognostic and predictive marker, as well as to examine the significance of HER2 overexpression in patients with mCRC, particularly in relation to response to anti-EGFR therapy. In this study, 181 patients with KRAS wild-type mCRC who received anti-EGFR therapy were included. Among them, 101 had left colon cancer (LCC) and 80 had right colon cancer (RCC). Results demonstrated that patients with KRAS wild-type LCC had better median overall survival (OS) (43 vs. 33 months, p = 0.005) and progression-free survival (PFS) (6 vs. 3 months, p < 0.001) compared to those with RCC. Multivariate analysis identified mucinous adenocarcinoma (p < 0.001), RCC location (p = 0.022), perineural invasions (p = 0.034), and tumors at the resection margin (p = 0.001) as independent predictors of OS, while mucinous adenocarcinoma (p = 0.001) and RCC location (p = 0.004) independently correlated with significantly shorter PFS. In addition, HER2 positive expression was significantly associated with worse PFS compared to HER2 negative results (p < 0.001). In conclusion, LPT is an important marker for predicting outcomes in the treatment of wild-type mCRC using anti-EGFR therapy, since patients with RCC have a statistically significantly shorter PFS and OS. Further investigation is needed to understand the role of HER2 overexpression in wild-type mCRC, as these patients also exhibit shorter survival.
Keywords:
metastatic colorectal cancer
; primary tumour localization
; anti EGFR therapy
; KRAS status
; HER2 expression
1. Introduction
Localization of the primary tumor (LPT) is an important prognostic and predictive factor that helps to a great extent in individualizing and personalizing treatments of patients with metastatic colorectal cancer (mCRC) [1]. The exact boundary between the left and right colons is still not precisely defined. Most often, the point of separation is the lienal flexure, so the right colon is to the lienal flexure (vermiform appendix, appendix, ascending part, transverse part of the colon) and the distal part belongs to the left colon (descending part of the colon, sigmoid part and rectum) [2]. Although considered as a single organ, segments of the colon are different from each other, histologically, physiologically, and molecularly [3,4,5,6,7]. One of the possible reasons for these differences lies in the fact that the left and right colon originate from different layers of the endoderm, the right colon (vermiform appendix, appendix, ascending part, proximal two-thirds of the transverse part of the colon) originates from the anterior and the left, (distal third of the transverse part, descending part of the colon, sigmoid part and rectum) from the posterior layer [2]. Recent studies have found that both left and right colon cancers behave differently regarding epidemiology, pathohistology, clinical presentation, molecular characteristics, and metastatic patterns [3,8,9,10,11,12,13,14]. These multifactorial differences, caused by LPT, might eventually lead to prognostic variations between RCC and LCC.
For CRC, it is important to determine all RAS mutations including mutations in the KRAS gene at exon 2 (codon 12/13), exons 3 and 4, and N-RAS mutations at exons 2, 3, 4 [15]. About 40% of colon tumors have mutations in the KRAS proto-oncogene, which are associated with resistance to biological therapy, i.e. monoclonal antibodies directed against epidermal growth factor receptor (anti-EGFR). Patients with KRAS wild-type (wt) tumor may have NRAS mutations in 10% of cases, making them resistant to the anti-EGFR therapy [16]. However, there are patients who, despite the absence of KRAS and NRAS mutations, still do not respond to targeted therapy. One reason for this is the BRAF mutation that occurs in about 8-12% of cases in patients who have all RAS wild-type tumors. BRAF has both prognostic and predictive significance in mCRC. Detection of the BRAF mutation indicates an unfavorable prognosis and predicts non-response to anti-EGFR therapy [17,18,19].
One of the potential predictive factors in CRC could be HER2 (human epidermal growth factor receptor 2) [20]. The expression of these receptors in CRC is about 5% of patients, but the prevalence is higher, 5% -14%, in RAS/BRAF wild-type tumors [16]. Since 2011, there has been a discussion of a possible effect of overexpression of HER2 receptors on resistance to biological therapy with anti-EGFR antibodies. The role of the HER2 receptor as a prognostic factor is still unclear. Some authors associate overexpression of HER2 receptors with a worse prognosis, including shorter time to disease progression and shorter overall survival [21], although this association has not been confirmed in similar studies [22,23].
This study aims to examine the predictive and prognostic role of the localization of the primary tumor (LPT) in the treatment of mCRC patients since the ultimate goal of the treatment is to improve the effectiveness and specificity of anti-EGFR therapy. Also, given the existing variability of clinical outcomes and responses to the treatment of patients with mCRC, it is clear that there is a need to identify new molecular biomarkers for the most accurate personalization and individualization in the treatment. Although the HER2 amplifications could predict a lack of response to anti-EGFR therapy in patients with mCRC, we also wanted to examine the importance of overexpression of HER2 in our cohort of wt mCRC patients.
2. Materials and Methods
The study included a total of 181 patients with pathohistologically verified colon cancer in the period from January 2009 to July 2021, who at the time of diagnosis had a metastatic disease or developed metastases during the disease. Data on clinically pathological parameters were collected from the medical documentation of the Oncology Institute of Vojvodina of patients located in the electronic database. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Oncology Institute of Vojvodina (protocol code 4/17/1-386272-20, date of approval 05.12.2017).
Concerning the localization of the primary tumor, patients were divided into two groups: 1. Patients with KRAS wild-type CRC localized in the right part of the colon (right colon cancer-RCC) (101 patients) and 2. Patients with KRAS wild-type CRC localized in the left part of the colon (left colon cancer-LCC) (80 patients). Pathological parameters of the tumor (pathohistological type of tumor, degree of differentiation, presence of vascular and perineural invasion (LVI, PNI), tumor infiltration lymphocytes (TIL), lymph nodes involvement, number of examined lymph nodes, positivity of resection margins, clinical course of the disease, progression-free survival (PFS), overall survival (OS), were analyzed in all patients. KRAS status was determined by Cobas DNA Sample Preparation Kit at Cobas z480 instrument, using PCR method of DNA extraction form FFPE tumor tissue, as part of a standard clinical procedure for metastatic CRC patients. Patients with mCRC KRAS wt tumor received anti-EGFR therapy (cetuximab and panitumumab) in addition to standard chemotherapy protocols. The patient’s response to the applied therapy was monitored using radiological methods such as computed tomography scan (CTS) or magnetic resonance imaging (MRI). As an additional prognostic parameter in patients with mCRC, an immunohistochemical examination of tumor tissue for the presence of HER2 gene protein product expression was performed by DAKO Polyclonal Rabbit Anti-Human c-erbB2 oncoprotein. Determination of the intensity of the immunohistochemical reaction was performed according to the consensus recommendations of the panel of pathologists, ie. HERACLES diagnostic criteria from the study of the same name [24]. According to HERACLES diagnostic criteria [24], positive expression results are recorded only in cases with intense circumferential, basolateral, or lateral response in more than 10% of cells.
For statistical data processing, the software package Statistical Package for Social Sciences - SPSS 21 was used. Numerical features are presented by medians (arithmetic mean) and measures of variability (range of values, standard deviation), and attribute features using frequencies and percentages. The comparison of the values of numerical features between the two groups was performed using the Student's t-test, ie. the non-parametric Mann-Whitney test. Testing the difference in the frequencies of attribute features was performed using the χ2 test. The examination of the connection between the two traits was performed using the Pearson correlation coefficient. In order to analyse the time to disease progression as well as mortality, Kaplan-Meier assessment of survival function and comparison using log-rank test was used. The Cox regression survival model was used to analyse the influence of the traits on the survival of the subjects. Statistically significant were considered the values of significance levels p < 0.05.
3. Results
3.1. Patient Characteristics According to the LPT
The study included 181 patients with KRAS wild-type mCRC. Average age of patients in relation to gender and LPT is represented in Table 1. Male patients were statistically significantly older than female patients (men 62.8 ± 9.3; women 58.6 ± 11.7, p = 0.011). Men were significantly older than women in the group of patients with left localization (62.9 ± 9.1 vs. 57.6 ± 10.4, p = 0.015), while there was no significant age difference among genders in the group of patients with right localization of cancer (men 62.6 ± 9.8; women 59.9 ± 12.8, p = 0.227). There was no difference in the average age in relation to cancer localization (left 61.6 ± 9.6; right 61.4 ± 11.1, p = 0.902).
The distribution of patient characteristics by localization of primary colon tumor is shown in Table 2. Mucinous type of cancer was statistically significantly more represented in the group of patients with an RCC (p = 0.001). Poorly differentiated tumor G3 is more common in patients with RCC, G1 in LCC (p = 0.031). There is no statistically significant difference in the distribution of the disease stage concerning the localization of the primary tumor (p = 0.283) (Table 2). The average number of examined lymph nodes was statistically significantly higher (p = 0.003) in the group of patients with RCC (18.2 ± 9.6) than on the left side (14.4 ± 8.7). The average number of organs/systems affected by metastases was statistically significantly higher (p = 0.035) in the group of patients with RCC (1.60 ± 0.79) than LCC (1.37 ± 0.66) (Table 2).
Lymphovascular invasion (LVI) (p = 0.332), perineural invasion (PNI) (p = 0.905), and the occurrence of ileus (p = 0.737) do not show statistically significant differences with respect to the localization of the primary tumor (Table 2). The average disease-free survival (DFS) was 16.4 months (SD = 12.8; range 2-72). The most common metastases were found in the liver (72.9%), lungs (21.5%), and lymph nodes of the abdomen (18.2%) (Table 2). The DFS was 17.9 months (SD = 14.4; range 2-72) in the LCC group and 15.0 months (SD = 10.8; range 2-45) in the RCC group, with no statistically significant difference (p = 0.243). In patients with RCC, metastases in the lymph nodes of the abdomen were statistically significantly more frequent (left - 12.9%; right - 25.0%; p = 0.036) (Table 2). Additionally, patients with RCC had more common metastases in the lymph nodes of the chest (left - 1.0%; right - 7.5%; p = 0.062), carcinosis of the peritoneum (left - 3.0%; right - 8.9%; p = 0.091), and in the lymph nodes of the pelvis (left - 5.0%; right - 11.2%; p = 0.115) (Table 2).
Anti-EGFR monoclonal antibodies (Cetuximab, Panitumumab) were commonly used in the third line of therapy, with 87.1% usage in left-sided localizations and 90.0% in right-sided localizations. There was no statistically significant difference in the localization of the primary tumor (p = 0.162) (Table 3).
3.2. Overall and Progression-Free Survival According to the LPT
The average overall survival (OS) of patients with LCC is significantly better than that of patients with RCC (47.22 ± 27.9 vs. 38.2 ± 22.2 months, p = 0.007) (Figure 1a). In the stage III disease group, OS was better for patients with LCC (n = 39) compared to RCC patients (n = 35), but the difference is not statistically significant (p = 0.145). The average progression-free survival (PFS) for patients with LCC is significantly better than that for patients with RCC (8.07 ± 7.17 vs. 4.27 ± 4.56 months, p <0.001) (Figure 1b).
Multivariate Cox regression analysis obtained independent predictors of cumulative survival (OS) of patients with colorectal cancer: mucinous adenocarcinoma (p < 0.001), right localization (p = 0.022), the presence of perineural invasion (p = 0.034) and the presence of tumors in resection margin (p = 0.049) (Table 4).
In the group of patients with LCC, Cox regression analysis obtained only one independent predictor of cumulative survival (OS), and that is the presence of perineural invasion (p = 0.038). Patients with perineural invasion have 1.60 times less survival rate than patients without perineural invasion (Table 5). In the group of patients with RCC, Cox regression analysis also obtained only one independent predictor of cumulative survival (OS), and that is mucinous adenocarcinoma (p = 0.038). Patients with mucinous adenocarcinoma have a 3.12 times lower survival rate (Table 5).
Cox regression analysis obtained independent predictors of cumulative progression-free survival (PFS) of patients with colon cancer: mucinous adenocarcinoma (p = 0.001) and right localization (p = 0.004) (Table 6). Patients with mucinous adenocarcinoma have a 2.53 times less survival rate than patients with classic NOS adenocarcinoma (Table 6). Patients with localization of the primary tumor on the right side of the colon have a 1.60 times lower survival rate than patients with primary tumor localized on the left side of the colon (Table 6).
3.3. Response to the Anti-EGFR Therapy in KRAS Wild-Type mCRC Patients
According to the response to anti-EGFR therapy, patients with KRAS wild-type mCRC were divided into two groups: 1. Patients who responded well to anti-EGFR therapy (no disease progression after the first 3 months) (n = 102 - 56.4%); and 2. Patients who did not respond well to anti-EFGR therapy (with disease progression in the first 3 months) (n = 79 - 43.6%). Patients with LCC responded statistically significantly better to anti-EGFR therapy (p < 0.001) (left 70.3%: right 30.8%). Patients with mucinous adenocarcinoma responded statistically significantly worse to anti-EGFR therapy (p = 0.001) (mucinous 16.7%: NOS, Singnet ring c. 60.7%) (Table 7). There was no statistically significant difference in the distribution of responses to anti-EGFR therapy compared to other unfavorable prognosis parameters (Table 7).
3.4. HER2 Expression
HER2 positive (3+) was registered in only 4 patients (2.21%), potentially positive HER2 (2+) in 7 patients (3.87%), HER2 (1+) in 26 patients (14.36%), and in the other 144 patients HER2 overexpression was negative (79.56%) (Figure 2). There was no statistically significant difference in the distributions of the unfavorable prognosis parameters and HER2 overexpression (p ˃ 0.05 in all tests, results not shown).
OS of patients with HER2 positive (3+) is worse than that of patients with HER2 negative (0, 1+, 2+), but due to the small number of patients with HER2 positive, no statistically significant difference was obtained (p = 0.339) (Figure 3A). PFS of patients with HER2-positive results was statistically significantly worse (p < 0.001) compared to the patients with HER2-negative results (despite a small number of patients with HER2-positive results) (Figure 3B).
4. Discussion
The treatment strategy for metastatic colorectal cancer (mCRC) is a significant aspect of clinical oncology due to the frequency of this disease. One-third of patients are diagnosed with the disease in the metastatic stage, and half of them develop metastases during their illness, which significantly contributes to the high mortality rates associated with colorectal cancer [25]. According to our study data, at the time of diagnosis, the most common disease stage was stage IV (43.6%), followed by stage III (40.9%), and stage II was only 15.5%.
Standard chemotherapy, combined with targeted biological therapy, forms the foundation of treatment for patients with mCRC [26]. The principles of modern oncology aim to customize and personalize the treatment of patients with cancer. Tumor molecular characteristics, such as predictive biomarkers, are essential in tailoring and personalizing therapy. Prognostic and predictive factors are crucial in effectively treating mCRC patients, as they help identify those who are more likely to benefit from therapy. This approach helps minimize unnecessary exposure to toxicities and potential harm from therapy that is unlikely to be beneficial [27].
Multivariate analysis of 1,437,846 patients in sixty-six studies published between 1995 and 2016 showed that the location of the primary tumor in the distal (left) relative to the proximal (right) colon was associated with better survival (HR 0.82, CI95% 0.79-0.84, p < 0.001) [28]. In addition to outcomes, differences in epidemiology, pathogenesis, genetic and epigenetic changes, and molecular pathways between tumors localized in the left and right colon have also been identified [28]. Accordingly, the results of our study showed a connection between RCC and poorer prognosis in terms of shorter time to disease progression and overall survival compared to patients with LCC. However, our study did not analyze predictive markers, such as MSI and BRAF status.
The survival rates of patients with CRC in our study were 92.8% at 12 months and 22.3% at 5 years. The average survival time was 41.9 months (range 6-196) with a median survival of 37 months. The median cumulative survival (OS) for left-sided colon cancer (LCC) was 43 months and for right-sided colon cancer (RCC) was 33 months. Our study revealed that tumors on the right side were associated with poorer survival (HR 1.46; 95% CI 1.06 - 2.01; p = 0.022). Additionally, we found differences in survival by stages between tumors localized in the left and right parts of the colon. In the third stage, patients with LCC showed better overall survival compared to patients with RCC, but the difference was not statistically significant (p=0.145; LCC n = 39, RCC n = 35). Based on literature data [29], RCC is predominantly diagnosed in advanced stages of the disease, although we did not observe a statistically significant difference in the distribution of disease stages based on the tumor location (p = 0.283). Some studies suggest that patients with RCC have a better prognosis in the second and third stages compared to patients with LCC, while they have a worse prognosis in the fourth stage, including shorter progression-free survival (PFS) and overall survival (OS). This was observed in similar CRC studies, specifically in a study of 2,027 patients treated with first-line chemotherapy, where RCC patients had better OS and PFS [7,30,31].
In stage III, patients with adjuvant therapy for RCC had a worse prognosis compared to those with LCC who received adjuvant chemotherapy [32]. Our study found that LCC generally also has a better prognosis in stage III. In the group of patients diagnosed in stage III with LCC (n = 39), overall survival was better compared to patients with RCC (n = 35) in the same stage, although the difference was not statistically significant (p = 0.145). Additionally, among patients in stage III who received adjuvant chemotherapy, those with LCC (n = 33) had better survival compared to those with RCC (n = 27), but the difference was not statistically significant (p = 0.234).
In a combined retrospective analysis, the predictive and prognostic value of primary tumor localization in the treatment of patients with antiEGFR therapy, cetuximab, and panitumumab, was evaluated. The study involved 38% of the 5,760 patients enrolled in the CRISTAL, FIRE-3, PEAK, PRIME, 181, and CALGB studies [4,33]. The analysis revealed that primary tumor localization is an important prognostic factor and a significant predictive factor [4,33]. Therefore, choosing the first-line systemic therapy for patients with mCRC should take into consideration the molecular characteristics of the tumor as well as the localization of the primary tumor, in addition to patient preferences, comorbidities, and general condition of the patient [10,30]. The Republic Health Insurance guidelines in our country approve the use of anti-EGFR therapy in the third line of treatment for patients with wild-type mCRC, or in the first line of treatment for a limited number of cycles for potentially resectable metastasis in the liver. As a result, the majority of patients received anti-EGFR therapy in the third line (87.1% in the left and 90.0% in the right localizations). There was no statistically significant difference in relation to the localization of the primary tumor (p = 0.162). According to NCCN recommendations, the use of antiEGFR therapy is suggested in the first line of treatment for patients with LCC. In the second and third lines, it is given regardless of the location of the primary tumor [26].
In our study, the progression-free survival (PFS) for metastatic colorectal cancer (mCRC) patients after 12 months of anti-EGFR monoclonal antibody treatment was 13.8%, and after 24 months, it was 4.1%. The average PFS was 6.39 months, with a median PFS of 5 months. Left-sided colon cancer (LCC) patients had a better PFS compared to right-sided colon cancer (RCC) patients (p < 0.001). The median cumulative progression-free survival for LCC patients was 6 months, while for RCC patients, it was 3 months. RCC patients experienced a significantly shorter time to disease progression (PFS) (p= 0.004). Since the NRAS and BRAF status were not determined in this study, we cannot be certain about the factors influencing these results, which is one of the limitations of this study. It is evident that for our patients with RCC, the time to disease progression is shorter in the second and third line of systemic treatment.
One possible reason is the overexpression of the HER2 receptor in patients with mCRC. Unlike breast cancer, where about 30% of cases show HER2 overexpression, the data for CRC varies. Several studies suggest that only 3% of CRC patients have HER2 overexpression, with a higher prevalence in RAS/BRAF wild-type tumors, at about 5-14% of cases [34,35,36,37], as they enhance HER2 amplifications [30]. Though the overexpression of HER2 receptors in CRC is still relatively low, the role of HER2 expression itself is significant, as it impacts cancer development and progression, leading to increased tumor cell proliferation and metastasis [38]. There are several factors that could explain the variation in expression rates, including small study populations, the use of different antibodies for immunohistochemistry (IHC), analysis of different patient subgroups with heterogeneous clinical and pathological characteristics of CRC, and the application of different scoring systems [35].
In our study, we observed a low percentage (2.21% - 4 out of 181) of overexpression of HER2 receptors in patients with mCRC. This low positivity may be due to the age of biological samples, which directly affects the immunohistochemical analysis. Tissue degradation can result in the absence of staining from applied immunohistochemical antibodies, including HER2. Another reason for the low positivity is pre-analytical. In standardized laboratories, the fixative used is buffered 10% formalin. However, in the past, many secondary centers in Vojvodina used alcohol instead of formalin for fixing biological material, leading to partial or complete absence of IHH staining. This issue can be partially mitigated by returning the biological material to the initial treatment process, specifically by dewaxing, pre-treating, and reprocessing it through a standardized procedure. However, this is not a guarantee that IHH staining will succeed.
Studies have analyzed HER2 overexpression in relation to the location of the primary tumor. The PETACC-3 study found that HER2 receptor expression is more likely to be higher in tumors located on the left side of the colon [39]. Similar results were observed in patients with advanced colorectal cancer (CRC). A retrospective analysis revealed a higher incidence of HER2 overexpression in rectal cancer compared to descending or right colon cancer. In the HERACLES clinical study, among 33 patients with HER2-positive metastatic CRC, 64% had distal tumors and 21% had rectal tumors [36]. Retrospective data from the phase II EXPERT trial, which involved patients with high-risk, locally advanced rectal cancer who received neoadjuvant therapy with capecitabine and oxaliplatin with chemoradiotherapy with or without cetuximab, showed a 4.3% prevalence of HER2 overexpression. These findings are consistent with the 5.4% HER2-positivity rate for rectal cancer as described by Marshall and colleagues [40]. In our study, although the number of HER2-positive tumors was very small, we did not observe a higher incidence in the rectum.
The research findings on the relationship between HER2 receptor overexpression and overall survival (OS) in patients with colorectal cancer (CRC) have been conflicting. Some studies show no difference in survival between patients with HER2 positive and negative CRC, while others suggest an association between HER2 receptor overexpression and poorer three-year (70.8% vs. 83.7%) and five-year survival (55.1% versus 78.3%, P <0.05) [41]. Our own study also found that the cumulative survival (OS) of patients with HER2 positive results is worse compared to patients with HER negative results. However, due to the small number of patients with HER2 positive results, we did not obtain a statistically significant difference (p = 0.339). The cumulative progression-free survival of patients with HER2-positive results was found to be statistically significantly worse (p <0.001) compared to patients with HER2-negative tumors, despite the small number of patients with HER2-positive findings. With the low positivity of HER2 overexpression, more studies are now analyzing patients with low HER2 overexpression, such as tumors with HER2 2+ positivity with a negative FISH finding, or HER2 1+. It has been demonstrated that patients with low HER2 overexpression have a better prognosis than HER2 positive, and behave similarly to HER2 negative, standing out as a special subgroup of patients [39]. As our understanding of CRC and its genomic profile evolves, therapeutic strategies need to be updated to improve the survival of patients with this disease. Despite promising results from early research, targeted anti-HER2 therapy in the treatment of advanced CRC requires further research [42,43].
5. Conclusions
With this study, we wanted to highlight the importance of primary tumor location (LPT) in the treatment of metastatic colorectal cancer (mCRC). Our main treatment goal for these patients is to improve treatment effectiveness without increasing toxicity. By selecting the right patients for specific treatments, we can reduce potential therapy toxicity. Therefore, identifying the primary tumor location should be a standard prognostic and predictive factor in everyday clinical practice. We couldn't emphasize the prognostic and predictive significance of excessive HER2 expression due to the low percentage in our sample. Further randomized studies are necessary to establish the significance of HER2 receptor overexpression in mCRC patients. Our study had some limitations. We lacked data on comorbidities, which could impact overall survival. Additionally, we didn't have all the molecular tumor characteristics such as NRAS and BRAF mutations, which also affect the response to anti-EGFR antibody therapy. Despite these limitations, our results reinforce the importance of primary tumor location as a crucial prognostic and predictive biomarker for everyday clinical practice.
Author Contributions
J. R. conceptualization, writing—original draft preparation, methodology, investigation; I.N. conceptualization, methodology, formal analysis, supervision; I. K. B. conceptualization, writing—original draft preparation, methodology, investigation; T. V. investigation, methodology, visualization; A. Đ. investigation, formal analysis; V. V. investigation, formal analysis; B. K. writing—review and editing, data curation, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Oncology Institute of Vojvodina (protocol code 4/17/1-386272-20, date of approval 05.12.2017)..
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nagai Y, Kiyomatsu T, Gohda Y, Otani K, Deguchi K, Yamada K. The primary tumor location in colorectal cancer: A focused review on its impact on surgical management. GHM 2021;3:386–93. [CrossRef]
- Venook AP, Niedzwiecki D, Innocenti F, Fruth B, Greene C, O’Neil BH, et al. Impact of primary (1o) tumor location on overall survival (OS) and progression-free survival (PFS) in patients (pts) with metastatic colorectal cancer (mCRC): Analysis of CALGB/SWOG 80405 (Alliance). JCO 2016;34:3504–3504. [CrossRef]
- Li F, Lai M. Colorectal cancer, one entity or three. J Zhejiang Univ Sci B 2009;10:219–29. [CrossRef]
- Tejpar S, Stintzing S, Ciardiello F, Tabernero J, Van Cutsem E, Beier F, et al. Prognostic and Predictive Relevance of Primary Tumor Location in Patients With RAS Wild-Type Metastatic Colorectal Cancer: Retrospective Analyses of the CRYSTAL and FIRE-3 Trials. JAMA Oncol 2017;3:194–201. [CrossRef]
- Loupakis F, Yang D, Yau L, Feng S, Cremolini C, Zhang W, et al. Primary tumor location as a prognostic factor in metastatic colorectal cancer. J Natl Cancer Inst 2015;107:dju427. [CrossRef]
- Arnold D, Lueza B, Douillard J-Y, Peeters M, Lenz H-J, Venook A, et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Annals of Oncology 2017;28:1713–29. [CrossRef]
- Weiss JM, Pfau PR, O’Connor ES, King J, LoConte N, Kennedy G, et al. Mortality by Stage for Right- Versus Left-Sided Colon Cancer: Analysis of Surveillance, Epidemiology, and End Results–Medicare Data. JCO 2011;29:4401–9. [CrossRef]
- Lei S, Ge Y, Tian S, Cai B, Gao X, Wang N, et al. Colorectal Cancer Metastases to Brain or Bone and the Relationship to Primary Tumor Location: a Population-Based Study. J Gastrointest Surg 2020;24:1833–42. [CrossRef]
- Jess T, Horváth-Puhó E, Fallingborg J, Rasmussen HH, Jacobsen BA. Cancer Risk in Inflammatory Bowel Disease According to Patient Phenotype and Treatment: A Danish Population-Based Cohort Study. American Journal of Gastroenterology 2013;108:1869–76. [CrossRef]
- Araki K, Furuya Y, Kobayashi M, Matsuura K, Ogata T, Isozaki H. Comparison of Mucosal Microvasculature between the Proximal and Distal Human Colon. Journal of Electron Microscopy 1996;45:202–6. [CrossRef]
- Kohoutova D, Smajs D, Moravkova P, Cyrany J, Moravkova M, Forstlova M, et al. Escherichia colistrains of phylogenetic group B2 and D and bacteriocin production are associated with advanced colorectal neoplasia. BMC Infect Dis 2014;14:733. [CrossRef]
- Gao Z, Guo B, Gao R, Zhu Q, Qin H. Microbiota disbiosis is associated with colorectal cancer. Front Microbiol 2015;6. [CrossRef]
- Missiaglia E, Jacobs B, D’Ario G, Di Narzo AF, Soneson C, Budinska E, et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Annals of Oncology 2014;25:1995–2001. [CrossRef]
- Brouwer NPM, Van Der Kruijssen DEW, Hugen N, De Hingh IHJT, Nagtegaal ID, Verhoeven RHA, et al. The Impact of Primary Tumor Location in Synchronous Metastatic Colorectal Cancer: Differences in Metastatic Sites and Survival. Ann Surg Oncol 2020;27:1580–8. [CrossRef]
- Petrelli F, Coinu A, Cabiddu M, Ghilardi M, Barni S. KRAS as prognostic biomarker in metastatic colorectal cancer patients treated with bevacizumab: a pooled analysis of 12 published trials. Med Oncol 2013;30:650. [CrossRef]
- Linardou H, Briasoulis E, Dahabreh IJ, Mountzios G, Papadimitriou C, Papadopoulos S, et al. All about KRAS for clinical oncology practice: Gene profile, clinical implications and laboratory recommendations for somatic mutational testing in colorectal cancer. Cancer Treatment Reviews 2011;37:221–33. [CrossRef]
- Davis AA, Cristofanilli M. Detection of Predictive Biomarkers Using Liquid Biopsies. In: Badve S, Kumar GL, editors. Predictive Biomarkers in Oncology, Cham: Springer International Publishing; 2019, p. 107–17. [CrossRef]
- Schirripa M, Cohen SA, Battaglin F, Lenz H-J. Biomarker-driven and molecular targeted therapies for colorectal cancers. Seminars in Oncology 2018;45:124–32. [CrossRef]
- Sjoquist KM, Renfro LA, Simes RJ, Tebbutt NC, Clarke S, Seymour MT, et al. Personalizing Survival Predictions in Advanced Colorectal Cancer: The ARCAD Nomogram Project. JNCI: Journal of the National Cancer Institute 2018;110:638–48. [CrossRef]
- Ahcene Djaballah S, Daniel F, Milani A, Ricagno G, Lonardi S. HER2 in Colorectal Cancer: The Long and Winding Road From Negative Predictive Factor to Positive Actionable Target. American Society of Clinical Oncology Educational Book 2022:219–32. [CrossRef]
- Meric-Bernstam F, Hurwitz H, Raghav KPS, McWilliams RR, Fakih M, VanderWalde A, et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): an updated report from a multicentre, open-label, phase 2a, multiple basket study. The Lancet Oncology 2019;20:518–30. [CrossRef]
- Iqbal N, Iqbal N. Human Epidermal Growth Factor Receptor 2 (HER2) in Cancers: Overexpression and Therapeutic Implications. Molecular Biology International 2014;2014:1–9. [CrossRef]
- Press MF, Bernstein L, Thomas PA, Meisner LF, Zhou JY, Ma Y, et al. HER-2/neu gene amplification characterized by fluorescence in situ hybridization: poor prognosis in node-negative breast carcinomas. JCO 1997;15:2894–904. [CrossRef]
- Sartore-Bianchi A, Trusolino L, Martino C, Bencardino K, Lonardi S, Bergamo F, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, phase 2 trial. The Lancet Oncology 2016;17:738–46. [CrossRef]
- Poston GJ, Figueras J, Giuliante F, Nuzzo G, Sobrero AF, Gigot J-F, et al. Urgent Need for a New Staging System in Advanced Colorectal Cancer. JCO 2008;26:4828–33. [CrossRef]
- National Comprehensive Cancer Network Washington: Clinical Practice Guidelines in Oncology, Inc n.d. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon_blocks.pdf (accessed on 3 July 2023).
- Siravegna G, Mussolin B, Buscarino M, Corti G, Cassingena A, Crisafulli G, et al. Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat Med 2015;21:795–801. [CrossRef]
- Lee GH, Malietzis G, Askari A, Bernardo D, Al-Hassi HO, Clark SK. Is right-sided colon cancer different to left-sided colorectal cancer? – A systematic review. European Journal of Surgical Oncology (EJSO) 2015;41:300–8. [CrossRef]
- Baran B, Mert Ozupek N, Yerli Tetik N, Acar E, Bekcioglu O, Baskin Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol Res 2018;11:264–73. [CrossRef]
- De Cuyper A, Van Den Eynde M, Machiels J-P. HER2 as a Predictive Biomarker and Treatment Target in Colorectal Cancer. Clinical Colorectal Cancer 2020;19:65–72. [CrossRef]
- Boeckx N, Koukakis R, Op De Beeck K, Rolfo C, Van Camp G, Siena S, et al. Primary tumor sidedness has an impact on prognosis and treatment outcome in metastatic colorectal cancer: results from two randomized first-line panitumumab studies. Annals of Oncology 2017;28:1862–8. [CrossRef]
- Bustamante-Lopez LA, Nahas SC, Nahas CSR, Pinto RA, Marques CFS, Cecconello I. IS THERE A DIFFERENCE BETWEEN RIGHT- VERSUS LEFT-SIDED COLON CANCERS? DOES SIDE MAKE ANY DIFFERENCE IN LONG-TERM FOLLOW-UP? ABCD, Arq Bras Cir Dig 2019;32:e1479. [CrossRef]
- Venderbosch S, Nagtegaal ID, Maughan TS, Smith CG, Cheadle JP, Fisher D, et al. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FOCUS Studies. Clinical Cancer Research 2014;20:5322–30. [CrossRef]
- Wu S, Ma C, Li W. Does overexpression of HER-2 correlate with clinicopathological characteristics and prognosis in colorectal cancer? Evidence from a meta-analysis. Diagn Pathol 2015;10:144. [CrossRef]
- Yalikong A, Li X-Q, Zhou P-H, Qi Z-P, Li B, Cai S-L, et al. A Triptolide Loaded HER2-Targeted Nano-Drug Delivery System Significantly Suppressed the Proliferation of HER2-Positive and BRAF Mutant Colon Cancer. IJN 2021;Volume 16:2323–35. [CrossRef]
- Raghav K, Loree JM, Morris JS, Overman MJ, Yu R, Meric-Bernstam F, et al. Validation of HER2 Amplification as a Predictive Biomarker for Anti–Epidermal Growth Factor Receptor Antibody Therapy in Metastatic Colorectal Cancer. JCO Precision Oncology 2019:1–13. [CrossRef]
- Hainsworth JD, Meric-Bernstam F, Swanton C, Hurwitz H, Spigel DR, Sweeney C, et al. Targeted Therapy for Advanced Solid Tumors on the Basis of Molecular Profiles: Results From MyPathway, an Open-Label, Phase IIa Multiple Basket Study. JCO 2018;36:536–42. [CrossRef]
- Ingold Heppner B, Behrens H-M, Balschun K, Haag J, Krüger S, Becker T, et al. HER2/neu testing in primary colorectal carcinoma. Br J Cancer 2014;111:1977–84. [CrossRef]
- Yagisawa M, Sawada K, Nakamura Y, Fujii S, Yuki S, Komatsu Y, et al. Prognostic Value and Molecular Landscape of HER2 Low-Expressing Metastatic Colorectal Cancer. Clinical Colorectal Cancer 2021;20:113-120.e1. [CrossRef]
- Puccini A, Lenz H-J, Marshall JL, Arguello D, Raghavan D, Korn WM, et al. Impact of Patient Age on Molecular Alterations of Left-Sided Colorectal Tumors. The Oncologist 2019;24:319–26. [CrossRef]
- Park DI, Kang MS, Oh SJ, Kim HJ, Cho YK, Sohn CI, et al. HER-2/neu overexpression is an independent prognostic factor in colorectal cancer. Int J Colorectal Dis 2007;22:491. [CrossRef]
- Siena S, Sartore-Bianchi A, Marsoni S, Hurwitz HI, McCall SJ, Penault-Llorca F, et al. Targeting the human epidermal growth factor receptor 2 (HER2) oncogene in colorectal cancer. Annals of Oncology 2018;29:1108–19. [CrossRef]
- Parikh A, Atreya C, Korn WM, Venook AP. Prolonged Response to HER2-Directed Therapy in a Patient With HER2-Amplified, Rapidly Progressive Metastatic Colorectal Cancer. J Natl Compr Canc Netw 2017;15:3–8. [CrossRef]
Figure 1.
Overall survival (a) and progression-free survival (b) of patients with wt KRAS mCRC according to localization of the primary tumor. OS-overall survival; PFS-progression-free survival; LCC-left colon cancer; RCC-right colon cancer.
Figure 1.
Overall survival (a) and progression-free survival (b) of patients with wt KRAS mCRC according to localization of the primary tumor. OS-overall survival; PFS-progression-free survival; LCC-left colon cancer; RCC-right colon cancer.
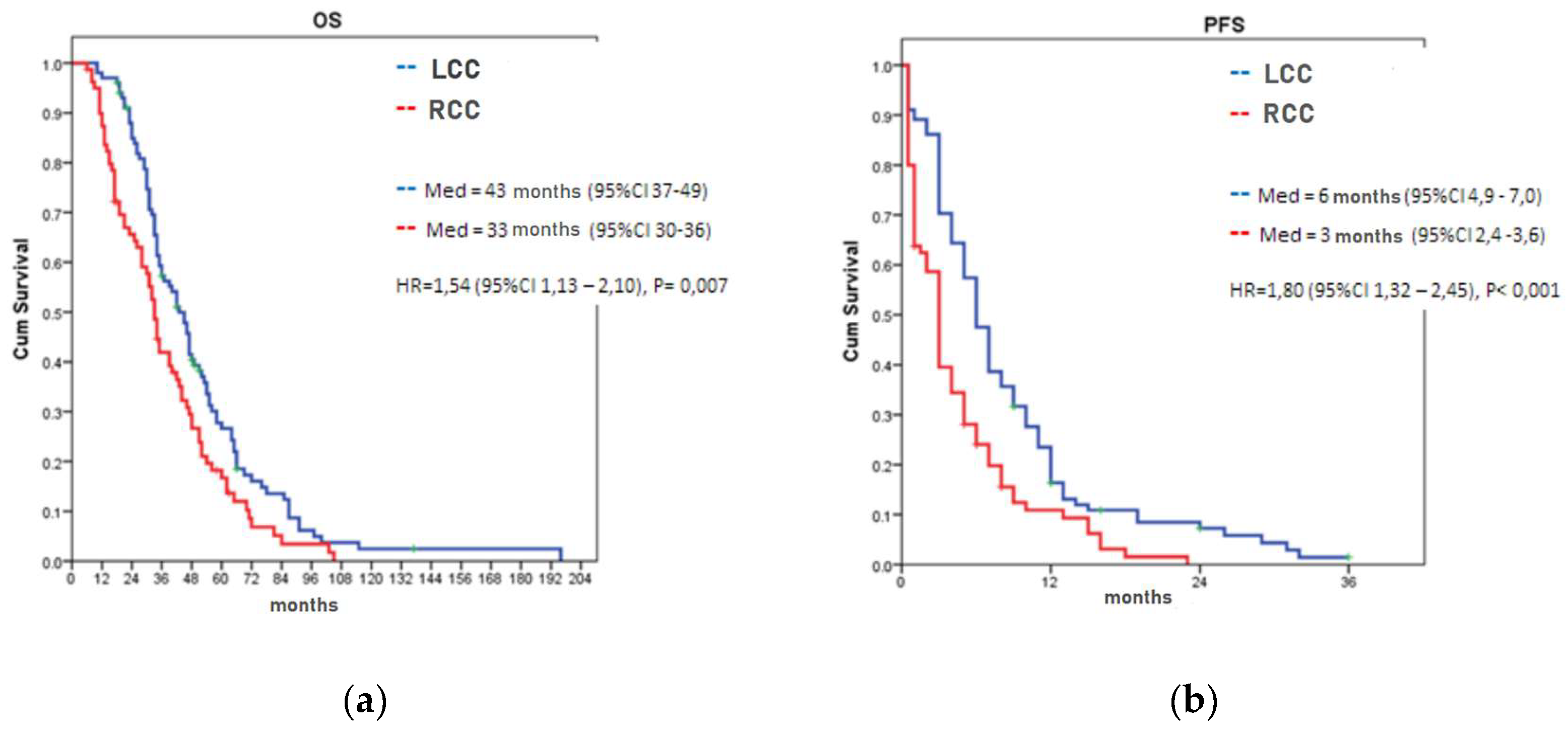
Figure 2.
Immunohistochemical evaluation of HER2 antibody in colorectal cancer: A - negative tumor cells (Score 0); B - weak positivity of cellular membranes (Score 1+); C - incomplete membrane staining positivity in more than 10% of tumor cells in some tumor areas (Score 2+); D - complete membrane staining in more than 10% of colorectal tumor cells..
Figure 2.
Immunohistochemical evaluation of HER2 antibody in colorectal cancer: A - negative tumor cells (Score 0); B - weak positivity of cellular membranes (Score 1+); C - incomplete membrane staining positivity in more than 10% of tumor cells in some tumor areas (Score 2+); D - complete membrane staining in more than 10% of colorectal tumor cells..
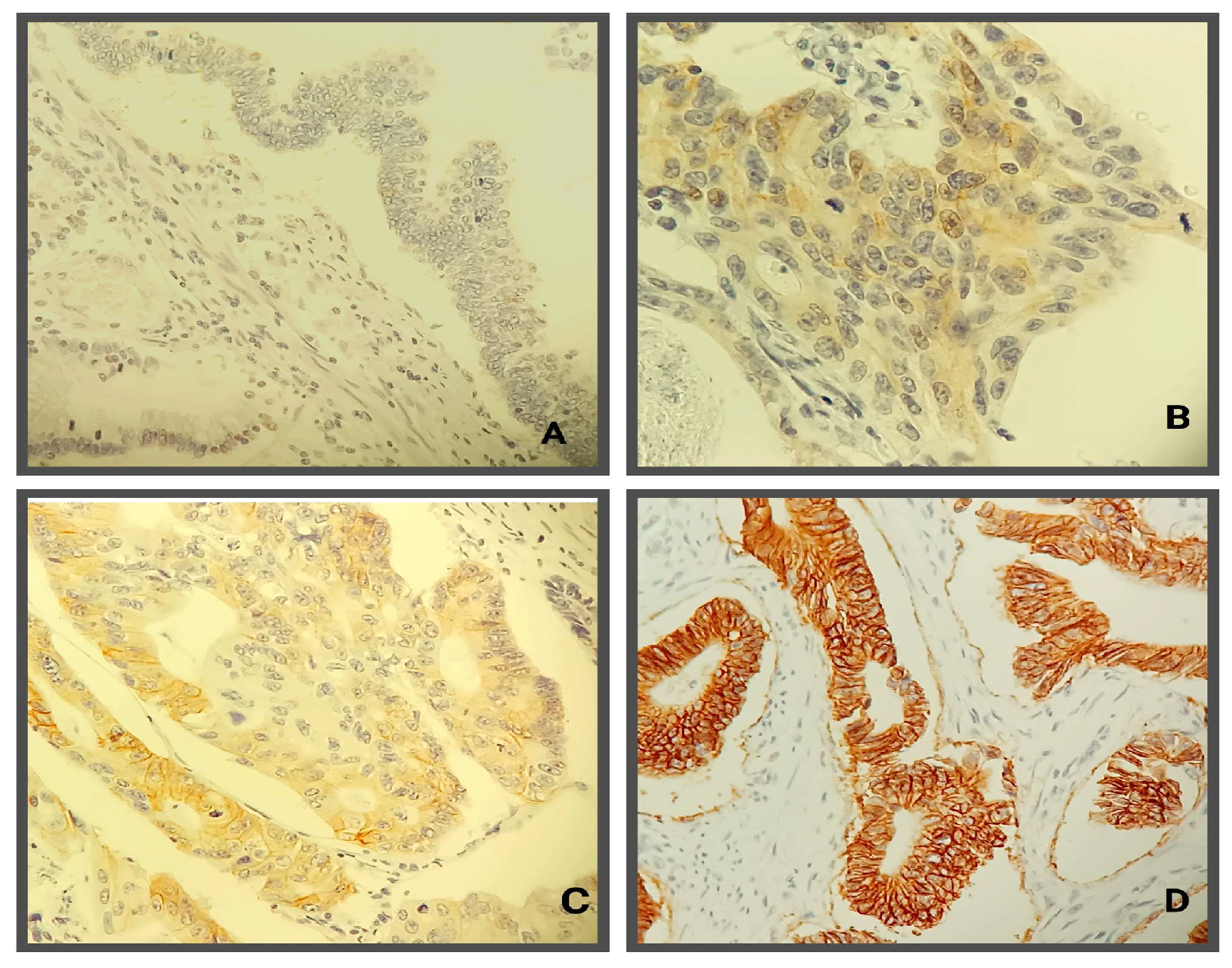
Figure 3.
Overall survival (a) and progression-free survival (b) of patients with wt KRAS mCRC according to the HER2 expression status. OS-overall survival; PFS-progression-free survival
Figure 3.
Overall survival (a) and progression-free survival (b) of patients with wt KRAS mCRC according to the HER2 expression status. OS-overall survival; PFS-progression-free survival
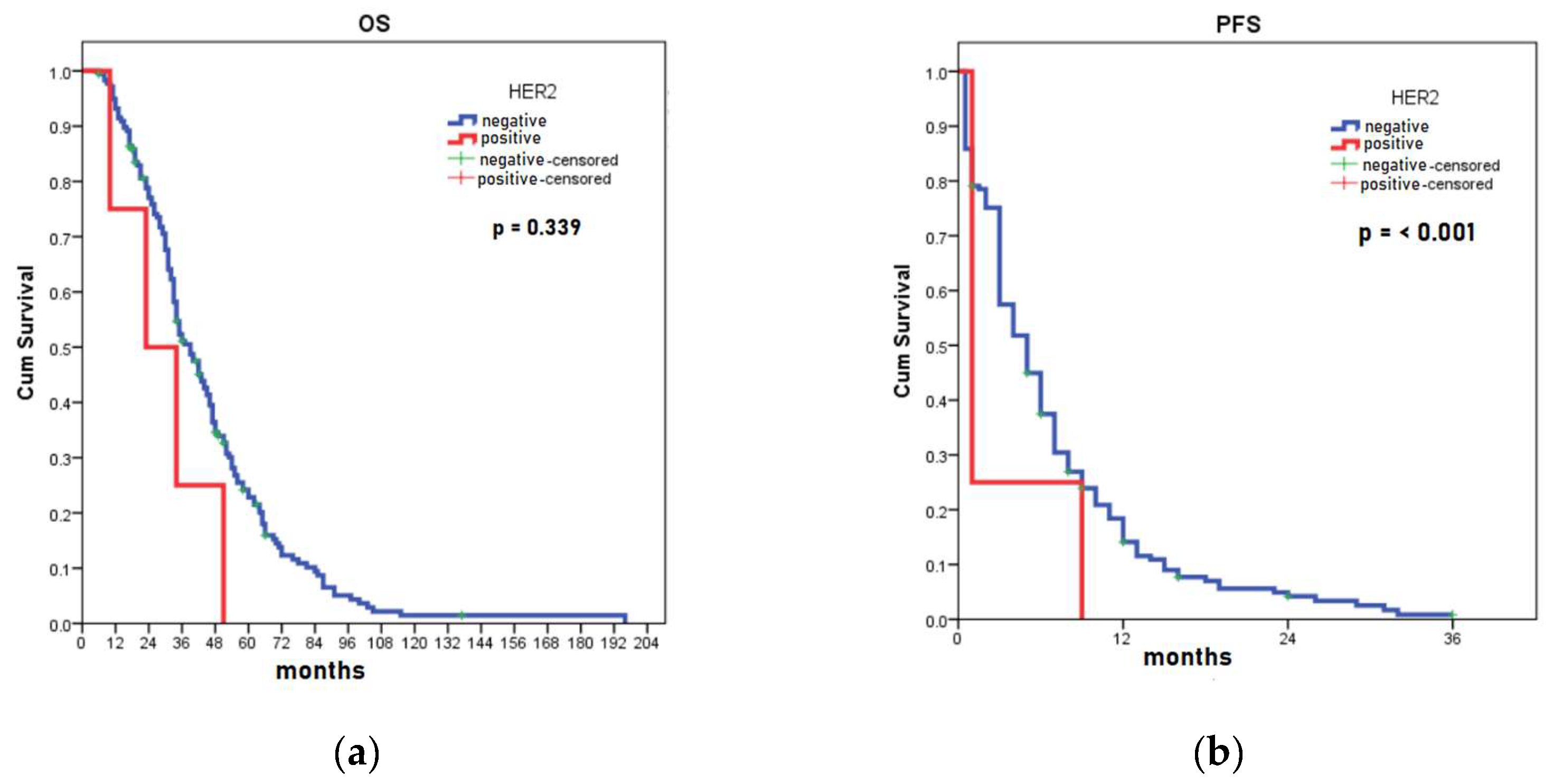

Table 1.
Distribution of average age of the patients in relation to gender and LPT.
| Gender | values | LCC n=75/26/101 |
RCC n=49/31/81 |
Total n=124/57/81 |
P value1 |
| Male | average (SD) | 62.9 (9.1) | 62.6 (9.8) | 62.8 (9.3) | 0.833 |
| min-max | 30 – 75 | 36 - 76 | 30 – 76 | ||
| Female | average (SD) | 57.6 (10.4) | 59.5 (12.8) | 58.6 (11.7) | 0.553 |
| min-max | 37 - 79 | 21 - 76 | 21 – 79 | ||
| All | average (SD) | 61.6 (9.6) | 61.4 (11.1) | 61.5 (10.3) | 0.902 |
| min-max | 30 - 79 | 21 - 76 | 21 – 79 | ||
| P value1 | 0.015 | 0.227 | 0.011 |
1P values obtained using the Student's t-test or the non-parametric Mann-Whitney test. LCC-left colon cancer; RCC-right colon cancer; SD-standard deviation.
Table 2.
Pathohistological characteristics of CRC patients and LPT.
| Parameters | Values | LCC n=101 |
RCC n=81 |
P value1 |
| Pathohistological type of tumor | Mucinous | 3 (3.0%) | 15 (18.8%) | 0.001 |
| NOS | 97 (96.0%) | 63 (78.8%) | ||
| Singnet ring cell | 1 (1.0%) | 2 (2.5%) | ||
| Differentiation | Good | 15 (14.9%) | 7 (7.8%) | 0.031 |
| Moderate | 75 (74.3%) | 53 (66.2%) | ||
| Poor | 11 (10.9%) | 20 (25.0%) | ||
| Resection margins | R0 | 85 (84.2%) | 72 (90.0%) | 0.442 |
| R1 | 6 (5.9%) | 4 (5.0%) | ||
| palliative surgery | 10 (9.9%) | 4 (5.0%) | ||
| Tumor infiltration lymphocyte | dense | 19 (18.8%) | 11 (13.8%) | 0.176 |
| poor | 23 (22.8%) | 28 (35.0%) | ||
| moderate | 59 (58.4%) | 41 (51.2%) | ||
| Stage at diagnosis | II | 13 (12.9%) | 15 (18.8%) | 0.283 |
| III | 39 (38.6%) | 35 (43.8%) | ||
| IV | 49 (48.5%) | 30 (37.5%) | ||
| No. of examined LN | average (SD) | 14.4 (8.7) | 18,2 (9.6) | 0.003 |
| min-max | 0 – 40 | 0 - 50 | ||
| No. of positive LN | average (SD) | 4.19 (4.7) | 5.29 (5.8) | 0.414 |
| min-max | 0 - 25 | 0 - 25 | ||
| No. of metastatic sites | average (SD) | 1.37 (0.66) | 1.60 (0.79) | 0.035 |
| min-max | 1 - 5 | 1 - 4 | ||
| Lymph node involvement |
present | 6 (5.9%) | 3 (3.8%) | 0.742 |
| Lymphovascular invasion |
present | 76 (75.2%) | 55 (68.8%) | 0,332 |
| Perineural invasion | present | 64 (63.4%) | 50 (62.5%) | 0.905 |
| Ileus | present | 28 (27.7%) | 24 (30.0%) | 0.737 |
| Metastatic sites | Liver | 73.9% | 72.5% | 0.908 |
| Lung | 20,8% | 22,5% | 0.781 | |
| LN of abdomen | 12,9% | 25,0% | 0.036 | |
| local recurrence | 9.9% | 6.2% | 0.376 | |
| LN of pelvis | 5.0% | 11.2% | 0.115 | |
| Carcinosis of peritoneum | 3.0% | 8.9% | 0.091 | |
| LN of thorax | 1.0% | 7.5% | 0.062 | |
| Ovary | 3.0% | 1.2% | 0.785 | |
| Bouns | 2.0% | 1.2% | 1.000 | |
| Adrenal gland | 2.0% | 1.2% | 1.000 | |
| Brain | 1.0% | 1.2% | 1.000 | |
| Urinary bladder | 2.0% | 0.0% | 0.582 | |
| Prostate | 1.0% | 0.0% | 1.000 | |
| Pancreas | 1.0% | 0.0% | 1.000 |
1All P values obtained using the the χ2 test, except for number of examined LN, positive LN, and metastatic sites where Student's t-test or the non-parametric Mann-Whitney test were used. LCC-left colon cancer; RCC-right colon cancer; NOS-not otherwise specified; LN-lymph nodes; SD-standard deviation.
Table 3.
Systemic treatment wt mCRC with anti-EFGR therapy according to the LPT.
| Line of therapy |
LCC n= 101 |
RCC n= 80 |
Total n= 181 |
P value1 |
| II | 3 (3.0%) | 5 (6.2%) | 8 (4.4%) | 0.162 |
| III | 88 (87.1%) | 72 (90.0%) | 160 (88.4%) | |
| IV | 10 (9.9%) | 3 (3.8%) | 13 (7.2%) |
1 P value obtained using the χ2 test. LCC-left colon cancer; RCC-right colon cancer.
Table 4.
Unfavorable prognosis parameters for OS in CRC patients.
| Predictors in CRC | B | SE | P1 | Exp(B) | 95% CI |
| Mucinous adenocarcinoma | 0.990 | 0.269 | <0.001 | 2.69 | 1.59-4.56 |
| Right localization of primary tumor | 0,.375 | 0.164 | 0.022 | 1.46 | 1.06-2,01 |
| Perineural invasion | 0.355 | 0.167 | 0.034 | 1.43 | 1.03-1.98 |
| Resection margins end palliative surgery |
0.518 | 0.263 | 0.049 | 1.68 | 1.02-2.81 |
1P value obtained using the Cox regression analysis (Conditional forward method).
Table 5.
Unfavorable prognosis parameters for cumulative OS in patients with LCC and RCC.
| Predictors in LCC | B | SE | P1 | Exp(B) | 95% CI |
| Perineural invasion | 0.468 | 0.225 | 0.038 | 1.60 | 1.03-2.48 |
| Predictors in RCC | B | SE | P1 | Exp(B) | 95% CI |
| Mucinous adenocarcinoma | 1.136 | 0.304 | <0.001 | 3.12 | 1.72-5.66 |
1P value obtained using the Cox regression analysis (Conditional forward method).
Table 6.
Unfavorable prognosis parameters for PFS in CRC patients.
| Predictors in CRC | B | SE | P1 | Exp(B) | 95% CI |
| Mucinous adenocarcinoma | 0.927 | 0.270 | 0.001 | 2.53 | 1.49-4.29 |
| Right localization of primary tumor | 0.471 | 0.165 | 0.004 | 1.60 | 1.16-2.21 |
1P value obtained using the Cox regression analysis (Conditional forward method).
Table 7.
Unfavorable prognosis parameters according to response to anti-EGFR therapy.
| Parameters | Characteristics | Not responded n=79 |
Good response n=102 |
P value1 |
| LPT | right | 49 (61.2%) | 31 (30.8%) | < 0,001 |
| left | 30 (29.7%) | 71 (70.3%) | ||
| Pathohistological type of tumor | NOS, SRCC | 64 (39.3%) | 99 (60.7%) | 0.001 |
| mucionus | 15 (83.3%) | 3 (16.7%) | ||
| Differentiation | good | 7 (31.8%) | 15 (68.2%) | 0.233 |
| Moderate, poor | 72 (45.3%) | 87 (54.7%) | ||
| Stage of disease | II | 11 (39.3%) | 17 (60.7%) | 0.613 |
| III, IV | 68 (44.4%) | 85 (55.6%) | ||
| No examined LN | <11 | 18 (34.6%) | 34 (65.4%) | 0.120 |
| 12< | 61 (47.3%) | 68 (52.7%) | ||
| Involved LN | No | 16 (36.4%) | 28 (63.6%) | 0.263 |
| Yes | 63 (46.0%) | 74 (54.0%) | ||
| Resection margins and palliative surgery |
R0 |
69 (43.9%) | 88 (56.1%) | 0.541 |
| R1, R2 | 10 (41.7%) | 14 (58.3%) | ||
| LVI | No | 20 (40.0%) | 30 (60.0%) | 0.188 |
| Yes | 59 (45.0%) | 72 (55.0%) | ||
| PNI | No | 25 (37.3%) | 42 (62.7%) | 0.834 |
| Yes | 54 (47.4%) | 60 (52.6%) | ||
| TIL | Poor, moderate | 25 (49.0%) | 26 (51.0%) | 0.361 |
| Dense | 54 (41.5%) | 76 (58.5%) |
1P value obtained using the χ2 test. LPT- location of the primary tumor; NOS- not otherwise specified; SRCC-Signet ring cell carcinoma; LN-lymph nodes; LVI-lymphovascular invasion; PNI-perineural invasion; TIL-tumor infiltration lymphocyte.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



