
Submitted:
17 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
The role of upfront primary tumor resection (PTR) in patients with unresectable metastatic col-orectal cancer (CRC) without severe symptoms remains controversial. We retrospectively ana-lyzed the role of PTR in overall survival (OS) in different subgroups. Among 331 patients diag-nosed with synchronous metastatic CRC between 2010 and 2020, 223 were analyzed. The PTR group (n = 42) showed better performance (p = 0.038); higher frequencies of right-sided origin (p = 0.014), T4 stage (p = 0.005), M1a stage (p = 0.015), and <2 organ metastases (p = 0.002); and re-ceived fewer targeted agents (p < 0.001) than the chemotherapy group (n = 181). The PTR group showed longer OS (20.5 versus 14.0 months, p = 0.016), but PTR was marginally related to OS in multivariate analysis (p = 0.060). Male sex (p = 0.022), good performance status (p = 0.07), left-sided tumor (p = 0.069), low serum carcinoembryonic antigen level (p = 0.092), T3 stage (p = 0.029), M1a stage (p = 0.025), <2 organ metastases (p = 0.017), and administration of targeted agents, especially bevacizumab (p = 0.024), were related to survival benefit after PTR. Upfront PTR should be considered when selecting patients with favorable prognoses for bevacizumab administration.
Keywords:
colorectal cancer
; primary tumor resection
; synchronous
; metastasis
; asymptomatic
1. Introduction
Systemic chemotherapy is the primary treatment for patients with synchronous stage IV colorectal cancer (CRC). Over the past 20 years, advances in systemic treatments, including biologically targeted agents, have led to dramatic improvements in the overall survival (OS) of patients with stage IV CRC, exceeding 30 months [1]. Primary tumor resection (PTR) has been performed to manage tumor-related symptoms such as obstruction, perforation, and refractory bleeding in these populations. However, the role of upfront PTR in asymptomatic and mildly symptomatic patients remains controversial. Upfront PTR may prevent primary tumor-related complications during the course of treatment, resulting in emergent surgery and poor oncological outcomes [2,3]. It can improve prognosis by removing the primary tumor source and reducing tumor-derived cytokines or chemokines [4]. However, this delays the administration of systemic treatment, and surgery-related complications are concerning [5,6].
Several retrospective, prospective cohorts, or nationwide registry analyses have shown the survival benefit of the upfront PTR in unresectable metastatic CRC [6]. Yet the heterogeneity of the study population, systemic treatment, and inevitable selection bias prevented definitive conclusions. Furthermore, many variables associated with prognosis or clinical outcomes were missing [14,16]. Recent randomized prospective clinical trials have reported that the upfront PTR group did not show a survival benefit or increased 60-day mortality compared with the chemotherapy-first group [17,18,19]. However, most studies closed early owing to poor accrual or futility, and a substantial number of participants did not receive any treatment after randomization.
In this study, we aimed to report the clinical outcomes of synchronous unresectable stage IV CRC patients with or without upfront PTR. A subgroup analysis was performed to determine clinical characteristics associated with better PTR outcomes
2. Materials and Methods
2.1. Ethics statements
This study was approved by the Institutional Review Board of St. Vincent Hospital (number: VC23RISI0179).
2.2. Study design and patients
We retrospectively reviewed the hospital database to identify all patients diagnosed with synchronous stage IV CRC between 2010 and 2020. The inclusion criteria were age 18 years, an initial diagnosis of unresectable stage IV colorectal adenocarcinoma, primary tumors without severe symptoms, and receipt of systemic anti-cancer treatment. Severe primary tumor symptoms were defined as follows: perforation, fistula formation, bleeding causing hemodynamic instability, or obstruction not relieved by a noninvasive procedure.
Among the 331 patients screened, 108 were excluded for the following reasons: 49 patients who received initial metastasectomy for resectable metastases; 32 patients who required emergent primary tumor resection due to severe symptoms; 21 patients who underwent upfront long course chemoradiotherapy; 2 patients had double primary malignancies along with CRC; 4 patients did not receive any systemic chemotherapy. Finally, 223 patients were included in this analysis (Figure 1).
2.3. Treatment and assessment
PTR was performed in the same manner as surgery for non-metastatic CRC, including an adequate level of lymphadenectomy, and 5-fluorouracil-based cytotoxic chemotherapy was selected as first-line systemic treatment. Bevacizumab has been added since 2014, and cetuximab has been added for the population with wild RAS since 2015. Patients were assessed at 6–8-week intervals using computed tomography of the abdomen and chest and serum carcinoembryonic antigen (CEA) levels.
2.4. Statistical analysis
Categorical variables are presented as numbers and percentages and were compared using the chi-square or Fisher exact test. Continuous variables are expressed as median values (range) and were compared using the Student’s unpaired t-test or Mann–Whitney U test, as appropriate. A subgroup analysis was performed to determine clinical characteristics associated with better PTR outcomes. OS was measured from the date of the initial treatment (PTR or systemic treatment) until death due to any cause or the last censored date during follow-up. OS was calculated using the Kaplan–Meier method, and differences in survival between the groups were compared using the log-rank test. Significant variables (p < 0.30) were included in the multivariate model. A backward elimination process was used to develop the final multivariate model, and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. R version 4.2.2 was used to perform all statistical analyses (The R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org/).
3. Results
3.1. Baseline characteristics
Among the 223 patients, 42 (18.8%) were treated with upfront PTR, and 181 (81.2%) were treated with chemotherapy as the final treatment. The baseline patient characteristics are presented in Table 1. The two treatment groups were well balanced in terms of median age, sex, serum CEA level, tumor differentiation, clinical N stage, and RAS status. The median follow-up period was 14.0 months (range, 0.3–92.0 months). Patients who underwent upfront PTR showed a better Eastern Cooperative Oncology Group (ECOG) performance status (0/1, p = 0.038); higher frequencies of right-sided colon cancer (p = 0.014), T4 stage (p = 0.005), and M1a stage (p = 0.015); and a lower number of organ metastases (0/1, p = 0.002).
The upfront chemotherapy group received more irinotecan-based doublets (p < 0.001) and targeted agents (p < 0.001) than the upfront PTR group as the first line of systemic treatment. The mean times to starting systemic treatment were 50.4 (±5.46) days in the upfront PTR group and 17.3 (±1.40) days in the upfront chemotherapy group (p < 0.001). Conversion to R0 resection was performed more frequently in the upfront PTR group than in the upfront chemotherapy group (21.4% vs. 12.2%, p = 0.004).
3.2. Variables associated with OS
The median OS was 16.0 months (range, 0.3–92.0 months) in the whole study population. Kaplan–Meier curves showed that the upfront PTR group had a longer OS than the upfront chemotherapy group (20.5 versus [vs.] 14.0 months, p = 0.016; Figure 2). In univariate analysis, OS was associated with age, ECOG performance status, primary tumor location, serum CEA level, tumor differentiation, administration of targeted agents, and upfront PTR (Table 2). Multivariate analysis showed that old age (HR, 1.530; 95% CI, 1.118–2.093; p = 0.008), poor ECOG performance (HR, 1.445; 95% CI, 1.072–1.948; p = 0.016), high CEA level (HR, 1.465; 95% CI, 1.066–2.013; p = 0.019), poor differentiation (HR, 2.218; 95% CI, 1.217–4.040; p = 0.009), and M1c stage (HR, 1.595; 95% CI, 1.060–2.400; p = 0.025) were associated with poorer OS, whereas administration of targeted agent was associated with a longer OS (HR, 0.569; 95% CI, 0.387–0.837; p = 0.004). Upfront PTR was marginally associated with OS (HR, 0.679; 95% CI, 0.454–1.017; p = 0.060).
3.3. Subgroup analysis favors upfront PTR
Subgroup analyses were performed to identify the clinical subgroups that benefited from upfront PTR (Figure 3). Male sex (p = 0.022), good performance status (p = 0.07), left-sided tumor (p = 0.069), low serum CEA level (p = 0.092), T3 stage (p = 0.029), M1a stage (p = 0.025), and <2 organ metastases (p = 0.017) showed a significant trend toward longer OS when upfront PTR was performed. The RAS mutational status was not significantly different between the two groups. Upfront PTR was associated with longer OS in patients who received targeted agents (p = 0.013), especially in those treated with bevacizumab (p = 0.024).
3.4. Primary tumor-related complications
In the upfront chemotherapy group, 46 (25.4%) patients experienced primary tumor-related complications, including obstruction (17.1%), bleeding (2.8%), pain (1.7%), perforation (1.1%), fistula (1.1%), abscess (1.1%), and ischemic changes (0.6%). There was no significant difference between the right- and left-sided tumors. Twenty-six patients received surgical treatment, 15 patients were relieved by non-surgical treatment, and five patients did not recover and died. The median survival time after complications was 83 (1–1,321) days.
4. Discussion
In this study, less than 20% of patients received upfront PTR among synchronous metastatic CRC patients with no or few primary tumor symptoms. This indicates that PTR was performed in highly selected patients, and most patients received chemotherapy as the initial treatment. The PTR group showed a longer OS in univariate analysis, but this was not statistically significant after adjusting for other variables. PTR seemed to be beneficial in some subgroups: male patients and patients with a good performance status, a left-sided tumor, a low CEA level, a T3 or M1a stage, and <2 organ metastases. Primary tumor-related complications occurred in 25.4% of patients in the upfront chemotherapy group, but most were relieved by surgery or intervention.
Upfront PTR for patients with initial stage IV CRC without severe primary tumor symptoms was performed at various frequencies according to the surgeon’s discretion or multidisciplinary team policy. The overall frequency of PTR has decreased recently [20,21,22], but many clinicians continue to perform upfront PTR before chemotherapy to prevent primary tumor-related complications during the course of treatment and/or to improve OS.
The primary tumor-related complication rate in patients with CRC receiving chemotherapy varies between 11% and 35%, and approximately half of the patients require surgical intervention [5,16,23,24,25,26,27,28]. Here, a quarter of patients in the upfront chemotherapy group experienced primary tumor-related complications. Most complications were relieved by surgery or intervention; however, a few patients did not recover because the complications occurred near the end of life. Obstruction was the most common complication, which is consistent with other studies’ findings [5,28]. Emergent colectomy is associated with higher morbidity and mortality rates than elective surgery [2,3]. In this study, colectomy was performed in only 14 patients, whereas the other patients were treated with bypass, stent insertion, and radiation. To avoid emergency surgery, patients should be carefully monitored for potential bowel obstruction during chemotherapy.
In the era of modern chemotherapy and targeted agents, OS, tumor response, and disease control rates have increased. The frequency of primary tumor-related complications since 2000 has continued to vary; therefore, it is not clear how they have changed since modern systemic treatments have been introduced [6,23,24,25,26,27,29]. Furthermore, there are concerns about the use of bevacizumab when the primary tumor is not resected because bevacizumab can cause bleeding, a fistula, or bowel perforation. The effect of bevacizumab administration on the PTR benefit is still controversial [7,23,25,29]. Some studies have reported that upfront PTR is associated with longer OS in bevacizumab-treated patients with CRC [23,30]. In this study, a higher rate of primary tumor-related complications was observed in the subgroups treated with targeted agents; however, the difference was not statistically significant (22.7% vs. 12.2%, p = 0.136, data not shown), which could be due to the longer OS in this population. The frequency did not differ according to the type of targeted agent used (23.5% for bevacizumab and 20.0% for cetuximab). Yet, surgical treatments were performed more frequently in the bevacizumab-treated subgroup than in the non-bevacizumab treatment subgroup (13.7% vs. 7.9%), which could partially explain why upfront PTR was favored in the bevacizumab subgroup in the subgroup analysis.
The survival benefit of upfront PTR in patients with synchronous metastatic CRC has only been demonstrated in retrospectively analyzed studies. Selection bias was inevitable in cases in which upfront PTR was performed: good performance status, liver-only metastasis, few organ metastases, non-rectal origin, or low serum CEA level [10,15,31,32,33,34,35,36,37,38], which could have misleading results. Additionally, the study population was heterogeneous in terms of the presence of symptoms, timing of PTR (before or during chemotherapy), and/or application or type of systemic treatment [7,8,9,10,11,12,13,15,32,39]. To adjust for these imbalances and heterogeneity, some studies have applied statistical methods, such as multivariate analysis or propensity matching [22,39,40]. Several studies, including ours, have shown that PTR is not associated with improved OS after adjusting for confounding factors [6,22,39,41]. Moreover, prognostic variables and therapeutic strategies have evolved over the decades, and insufficient data collection in many studies makes the role of upfront PTR debatable [14,16].
The role of the PTR in OS remains controversial in the era of biologic-targeted agents [23,39,42]. A few prospective randomized trials comparing upfront PTR with bevacizumab plus chemotherapy have been conducted to answer this question and concluded that upfront PTR was futile in terms of 60-day mortality or OS. However, most were closed early due to poor accrual or the assumed futility of the upfront PTR, which limited the statistical power supporting the conclusions [17,18]. iPACS was the first randomized controlled trial to suggest the utility of upfront PTR for asymptomatic, synchronous, unresectable metastatic CRC. However, it enrolled patients with ≤3 metastatic diseases and more than half were T3 or N0/1, which could question true unresectability [17]. Rahbari et al. also reported that upfront PTR did not prolong OS; however, more patients in the PTR group did not receive any systemic treatment after PTR, similar to that in the iPACS study [19]. This advantage of PTR for asymptomatic patients with CRC is difficult to validate in randomized clinical trials because many factors are involved in the decision-making process of PTR, including patient or clinician preference and various clinical situations that cannot be easily controlled in clinical trials.
Subgroup analyses could provide clues as to which patients could benefit from PTR. First, PTR could be associated with improved OS when performed in patients with a good performance status who can receive systemic treatment after PTR. The administration of polychemotherapy is a key determinant of OS [7]. In particular, patients receiving targeted agents showed a significantly favorable prognosis after PTR compared with the subgroup receiving chemotherapy alone. This indicates that patients with good performance who can tolerate and are willing to receive active systemic treatment could consider upfront PTR to improve their OS. The PTR group showed a considerable delay in chemotherapy administration; therefore, PTR should be avoided in patients whose conditions can rapidly deteriorate.
The extent of metastasis is also an important factor. Our study showed that patients with less extensive organ metastasis had favorable outcomes after PTR, which is consistent with other studies’ results [34,43,44]. The serum CEA level reflects the extent of the tumor burden, and the subgroup with a low CEA level was also associated with PTR benefit [35]. The benefits of PTR on OS differed according to the primary tumor site. In our study, upfront PTR was performed more often in right-sided CRC for diagnostic purposes. However, patients with right-sided CRC did not show a clear benefit from upfront PTR, whereas patients with left-sided CRC showed a trend toward favoring PTR. Several studies have reported similar results in that right-sided colon cancer is related to a reduced OS benefit after PTR compared to left-sided tumors [18,45,46]. Right-sided colon cancer is associated with poorly differentiated histology, advanced stage at diagnosis, BRAF mutations, or consensus molecular subtype 1, which is related to a poor prognosis. Therefore, PTR should be performed with caution in patients with right-sided CRC.
Only a few studies have reported controversial results regarding the presence of tumor RAS mutations [30,47], which were not related to the PTR benefit in this study. Age did not affect the benefit of PTR [21,48], whereas the female sex showed more upfront PTR benefits than the male sex, including in this study [7]. Most subgroups showing an OS benefit after PTR are associated with a favorable prognosis. Therefore, PTR should be considered in patients with stage IV CRC with favorable prognostic factors.
This study had some limitations. First, this study was conducted in a single center, and the sample size was too small, especially in the PTR group, to draw statistically significant results. Second, some data were inaccurate or missing due to the retrospective design of the study. Our study enrolled patients between 2000 and 2010; standard chemotherapy was changed, and some patients did not have molecular results associated with clinical outcomes. Finally, all patients received systemic therapy, which does not reflect the fact that some did not receive further treatment with or without PTR. Nonetheless, we attempted to collect variables associated with clinical outcomes in patients with stage IV CRC and showed the clinical role of PTR on OS according to these variables.
5. Conclusions
Upfront PTR in patients with asymptomatic or symptomatic stage IV CRC should be considered when selecting patients with a favorable prognosis. Caution is warranted in patients with unfavorable characteristics, including a poor performance status, a right-sided tumor, a high CEA level, or extensive metastasis. Systemic chemotherapy, including biological agents, is the main treatment, and upfront PTR may be beneficial, especially for bevacizumab-treated patients with CRC. However, further validation in a larger patient population is required.
Author Contributions
H.J.A. and B.K. conceived of this work; J.E.S., H.J.A., B.Y.S., H.K., H.S.P., H.C., H.K., B.K., R.N.Y. and J.M. performed the data acquisition, analysis, and interpretation; J.E.S. drafted the manuscript; and H.J.A., B.K., S.H.K., J.L., H.C.L., J.J., K.L. and J.M.L substantially revised the manuscript. All authors reviewed the manuscript.
Funding
This study was funded by the Catholic Medical Center Research Foundation in the program year 2023 and a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (number: RS-2023-00249672).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of St. Vincent Hospital (protocol code VC23RISI0179 and date of approval Aug/03/2023).
Informed Consent Statement
Informed consent was waived because of the retrospective nature of the study and the analysis used anonymous clinical data.
Data Availability Statement
The data are available upon request from the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Venook, A.P.; Niedzwiecki, D.; Lenz, H.-J.; Innocenti, F.; Fruth, B.; Meyerhardt, J.A.; Schrag, D.; Greene, C.; O’Neil, B.H.; Atkins, J.N.; et al. Effect of First-Line Chemotherapy Combined With Cetuximab or Bevacizumab on Overall Survival in Patients With KRAS Wild-Type Advanced or Metastatic Colorectal Cancer: A Randomized Clinical Trial. JAMA 2017, 317, 2392–2401. [Google Scholar] [CrossRef] [PubMed]
- Mun, J.Y.; Kim, J.E.; Yoo, N.; Cho, H.M.; Kim, H.; An, H.J.; Kye, B.H. Survival Outcomes after Elective or Emergency Surgery for Synchronous Stage IV Colorectal Cancer. Biomedicines 2022, 10, 3114. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Becerra, A.Z.; Aquina, C.T.; Hensley, B.J.; Justiniano, C.F.; Boodry, C.; Swanger, A.A.; Arsalanizadeh, R.; Noyes, K.; Monson, J.R.; et al. Emergent Colectomy Is Independently Associated with Decreased Long-Term Overall Survival in Colon Cancer Patients. Journal of gastrointestinal surgery: Official journal of the Society for Surgery of the Alimentary Tract 2017, 21, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.Y.; Oskarsson, T.; Acharyya, S.; Nguyen, D.X.; Zhang, X.H.; Norton, L.; Massagué, J. Tumor self-seeding by circulating cancer cells. Cell 2009, 139, 1315–1326. [Google Scholar] [CrossRef]
- Scheer, M.G.; Sloots, C.E.; van der Wilt, G.J.; Ruers, T.J. Management of patients with asymptomatic colorectal cancer and synchronous irresectable metastases. Ann Oncol 2008, 19, 1829–1835. [Google Scholar] [CrossRef]
- Niitsu, H.; Hinoi, T.; Shimomura, M.; Egi, H.; Hattori, M.; Ishizaki, Y.; Adachi, T.; Saito, Y.; Miguchi, M.; Sawada, H.; et al. Up-front systemic chemotherapy is a feasible option compared to primary tumor resection followed by chemotherapy for colorectal cancer with unresectable synchronous metastases. World J Surg Oncol 2015, 13, 162. [Google Scholar] [CrossRef]
- Colloca, G.A.; Venturino, A.; Guarneri, D. Primary tumor resection in patients with unresectable colorectal cancer with synchronous metastases could improve the activity of poly-chemotherapy: A trial-level meta-analysis. Surgical oncology 2022, 44, 101820. [Google Scholar] [CrossRef]
- Stillwell, A.P.; Buettner, P.G.; Ho, Y.H. Meta-analysis of survival of patients with stage IV colorectal cancer managed with surgical resection versus chemotherapy alone. World journal of surgery 2010, 34, 797–807. [Google Scholar] [CrossRef]
- Anwar, S.; Peter, M.B.; Dent, J.; Scott, N.A. Palliative excisional surgery for primary colorectal cancer in patients with incurable metastatic disease. Is there a survival benefit? A systematic review. Colorectal Dis 2012, 14, 920–930. [Google Scholar] [CrossRef]
- Clancy, C.; Burke, J.P.; Barry, M.; Kalady, M.F.; Calvin Coffey, J. A meta-analysis to determine the effect of primary tumor resection for stage IV colorectal cancer with unresectable metastases on patient survival. Annals of surgical oncology 2014, 21, 3900–3908. [Google Scholar] [CrossRef]
- Tarantino, I.; Warschkow, R.; Worni, M.; Cerny, T.; Ulrich, A.; Schmied, B.M.; Güller, U. Prognostic Relevance of Palliative Primary Tumor Removal in 37,793 Metastatic Colorectal Cancer Patients: A Population-Based, Propensity Score-Adjusted Trend Analysis. Ann Surg 2015, 262, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.C.; Ou, Y.C.; Hu, W.H.; Liu, C.C.; Chen, H.H. Meta-analysis of outcomes of patients with stage IV colorectal cancer managed with chemotherapy/radiochemotherapy with and without primary tumor resection. Onco Targets Ther 2016, 9, 7059–7069. [Google Scholar] [CrossRef]
- Ha, G.W.; Kim, J.H.; Lee, M.R. Meta-analysis of oncologic effect of primary tumor resection in patients with unresectable stage IV colorectal cancer in the era of modern systemic chemotherapy. Ann Surg Treat Res 2018, 95, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Harji, D.P.; Vallance, A.; Selgimann, J.; Bach, S.; Mohamed, F.; Brown, J.; Fearnhead, N. A systematic analysis highlighting deficiencies in reported outcomes for patients with stage IV colorectal cancer undergoing palliative resection of the primary tumour. Eur J Surg Oncol 2018, 44, 1469–1478. [Google Scholar] [CrossRef]
- Nitsche, U.; Stöß, C.; Stecher, L.; Wilhelm, D.; Friess, H.; Ceyhan, G.O. Meta-analysis of outcomes following resection of the primary tumour in patients presenting with metastatic colorectal cancer. Br J Surg 2018, 105, 784–796. [Google Scholar] [CrossRef]
- Sterpetti, A.V.; Costi, U.; D’Ermo, G. National statistics about resection of the primary tumor in asymptomatic patients with Stage IV colorectal cancer and unresectable metastases. Need for improvement in data collection. A systematic review with meta-analysis. Surgical oncology 2020, 33, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Ike, H.; Shiomi, A.; et al. Primary Tumor Resection Plus Chemotherapy Versus Chemotherapy Alone for Colorectal Cancer Patients With Asymptomatic, Synchronous Unresectable Metastases (JCOG1007; iPACS): A Randomized Clinical Trial. Journal of clinical oncology: Official journal of the American Society of Clinical Oncology 2021, 39, 1098–1107. [Google Scholar] [CrossRef]
- van der Kruijssen, D.E.W.; Elias, S.G.; Vink, G.R.; van Rooijen, K.L.; t Lam-Boer, J.; Mol, L.; Punt, C.J.A.; de Wilt, J.H.W.; Koopman, M. Sixty-Day Mortality of Patients With Metastatic Colorectal Cancer Randomized to Systemic Treatment vs Primary Tumor Resection Followed by Systemic Treatment: The CAIRO4 Phase 3 Randomized Clinical Trial. JAMA surgery 2021, 156, 1093–1101. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Biondo, S.; Feißt, M.; Bruckner, T.; Rossion, I.; Luntz, S.; Bork, U.; Büchler, M.W.; Folprecht, G.; Kieser, M.; et al. Randomized clinical trial on resection of the primary tumor versus no resection prior to systemic therapy in patients with colon cancer and synchronous unresectable metastases. Journal of Clinical Oncology 2022, 40, LBA3507. [Google Scholar] [CrossRef]
- Sanford, N.N.; Folkert, M.R.; Aguilera, T.A.; Beg, M.S.; Kazmi, S.A.; Sanjeevaiah, A.; Zeh, H.J.; Farkas, L. Trends in Primary Surgical Resection and Chemotherapy for Metastatic Colorectal Cancer, 2000-2016. American journal of clinical oncology 2020, 43, 850–856. [Google Scholar] [CrossRef]
- Xu, H.; Xia, Z.; Jia, X.; Chen, K.; Li, D.; Dai, Y.; Tao, M.; Mao, Y. Primary Tumor Resection Is Associated with Improved Survival in Stage IV Colorectal Cancer: An Instrumental Variable Analysis. Scientific reports 2015, 5, 16516. [Google Scholar] [CrossRef]
- Yun, J.A.; Huh, J.W.; Park, Y.A.; Cho, Y.B.; Yun, S.H.; Kim, H.C.; Lee, W.Y.; Chun, H.K. The role of palliative resection for asymptomatic primary tumor in patients with unresectable stage IV colorectal cancer. Dis Colon Rectum 2014, 57, 1049–1058. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liang, L.; Yu, Y.; Wang, Y.; Zhuang, R.; Chen, Y.; Cui, Y.; Zhou, Y.; Liu, T. Primary Tumour Resection Could Improve the Survival of Unresectable Metastatic Colorectal Cancer Patients Receiving Bevacizumab-Containing Chemotherapy. Cell Physiol Biochem 2016, 39, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Yamazaki, K.; Kinugasa, Y.; Tsukamoto, S.; Yamaguchi, T.; Shiomi, A.; Tsushima, T.; Yokota, T.; Todaka, A.; Machida, N.; et al. Influence of primary tumor resection on survival in asymptomatic patients with incurable stage IV colorectal cancer. Int J Clin Oncol 2014, 19, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Poultsides, G.A.; Servais, E.L.; Saltz, L.B.; Patil, S.; Kemeny, N.E.; Guillem, J.G.; Weiser, M.; Temple, L.K.; Wong, W.D.; Paty, P.B. Outcome of primary tumor in patients with synchronous stage IV colorectal cancer receiving combination chemotherapy without surgery as initial treatment. Journal of clinical oncology: Official journal of the American Society of Clinical Oncology 2009, 27, 3379–3384. [Google Scholar] [CrossRef]
- Cetin, B.; Kaplan, M.A.; Berk, V.; Tufan, G.; Benekli, M.; Isikdogan, A.; Ozkan, M.; Coskun, U.; Buyukberber, S. Bevacizumab-containing chemotherapy is safe in patients with unresectable metastatic colorectal cancer and a synchronous asymptomatic primary tumor. Jpn J Clin Oncol 2013, 43, 28–32. [Google Scholar] [CrossRef]
- Kim, M.S.; Chung, M.; Ahn, J.B.; Kim, C.W.; Cho, M.S.; Shin, S.J.; Baek, S.J.; Hur, H.; Min, B.S.; Baik, S.H.; et al. Clinical significance of primary tumor resection in colorectal cancer patients with synchronous unresectable metastasis. J Surg Oncol 2014, 110, 214–221. [Google Scholar] [CrossRef]
- Tebbutt, N.C.; Norman, A.R.; Cunningham, D.; Hill, M.E.; Tait, D.; Oates, J.; Livingston, S.; Andreyev, J. Intestinal complications after chemotherapy for patients with unresected primary colorectal cancer and synchronous metastases. Gut 2003, 52, 568–573. [Google Scholar] [CrossRef]
- Lee, B.; Wong, H.-L.; Tacey, M.; Tie, J.; Wong, R.; Lee, M.; Nott, L.; Shapiro, J.; Jennens, R.; Turner, N.; et al. The impact of bevacizumab in metastatic colorectal cancer with an intact primary tumor: Results from a large prospective cohort study. Asia Pac J Clin Oncol 2017, 13, 314–321. [Google Scholar] [CrossRef]
- Korkmaz, L.; Coşkun, H.; Dane, F.; Karabulut, B.; Karaağaç, M.; Çabuk, D.; Karabulut, S.; Aykan, N.F.; Doruk, H.; Avcı, N.; et al. Kras-mutation influences outcomes for palliative primary tumor resection in advanced colorectal cancer-a Turkish Oncology Group study. Surgical oncology 2018, 27, 485–489. [Google Scholar] [CrossRef]
- Shida, D.; Hamaguchi, T.; Ochiai, H.; Tsukamoto, S.; Takashima, A.; Boku, N.; Kanemitsu, Y. Prognostic Impact of Palliative Primary Tumor Resection for Unresectable Stage 4 Colorectal Cancer: Using a Propensity Score Analysis. Annals of surgical oncology 2016, 23, 3602–3608. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, H.; Ogawa, Y.; Yamazaki, H.; Honda, M.; Kono, K.; Konno, S.; Fukuhara, S.; Yamamoto, Y. Impact of Primary Tumor Resection on Mortality in Patients with Stage IV Colorectal Cancer with Unresectable Metastases: A Multicenter Retrospective Cohort Study. World journal of surgery 2021, 45, 3230–3239. [Google Scholar] [CrossRef] [PubMed]
- Ferrand, F.; Malka, D.; Bourredjem, A.; Allonier, C.; Bouché, O.; Louafi, S.; Boige, V.; Mousseau, M.; Raoul, J.L.; Bedenne, L.; et al. Impact of primary tumour resection on survival of patients with colorectal cancer and synchronous metastases treated by chemotherapy: Results from the multicenter, randomised trial Fédération Francophone de Cancérologie Digestive 9601. European journal of cancer (Oxford, England: 1990) 2013, 49, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Ruo, L.; Gougoutas, C.; Paty, P.B.; Guillem, J.G.; Cohen, A.M.; Wong, W.D. Elective bowel resection for incurable stage IV colorectal cancer: Prognostic variables for asymptomatic patients. J Am Coll Surg 2003, 196, 722–728. [Google Scholar] [CrossRef]
- Faron, M.; Pignon, J.P.; Malka, D.; Bourredjem, A.; Douillard, J.Y.; Adenis, A.; Elias, D.; Bouché, O.; Ducreux, M. Is primary tumour resection associated with survival improvement in patients with colorectal cancer and unresectable synchronous metastases? A pooled analysis of individual data from four randomised trials. European journal of cancer (Oxford, England: 1990) 2015, 51, 166–176. [Google Scholar] [CrossRef]
- Gresham, G.; Renouf, D.J.; Chan, M.; Kennecke, H.F.; Lim, H.J.; Brown, C.; Cheung, W.Y. Association between palliative resection of the primary tumor and overall survival in a population-based cohort of metastatic colorectal cancer patients. Annals of surgical oncology 2014, 21, 3917–3923. [Google Scholar] [CrossRef]
- Ishihara, S.; Hayama, T.; Yamada, H.; Nozawa, K.; Matsuda, K.; Miyata, H.; Yoneyama, S.; Tanaka, T.; Tanaka, J.; Kiyomatsu, T.; et al. Prognostic impact of primary tumor resection and lymph node dissection in stage IV colorectal cancer with unresectable metastasis: A propensity score analysis in a multicenter retrospective study. Annals of surgical oncology 2014, 21, 2949–2955. [Google Scholar] [CrossRef]
- Park, J.H.; Kim, T.Y.; Lee, K.H.; Han, S.W.; Oh, D.Y.; Im, S.A.; Kang, G.H.; Chie, E.K.; Ha, S.W.; Jeong, S.Y.; et al. The beneficial effect of palliative resection in metastatic colorectal cancer. Br J Cancer 2013, 108, 1425–1431. [Google Scholar] [CrossRef]
- Shida, D.; Boku, N.; Tanabe, T.; Yoshida, T.; Tsukamoto, S.; Takashima, A.; Kanemitsu, Y. Primary Tumor Resection for Stage IV Colorectal Cancer in the Era of Targeted Chemotherapy. Journal of gastrointestinal surgery: Official journal of the Society for Surgery of the Alimentary Tract 2019, 23, 2144–2150. [Google Scholar] [CrossRef]
- Su, Y.C.; Wu, C.C.; Su, C.C.; Hsieh, M.C.; Cheng, C.L.; Kao Yang, Y.H. Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection. Cancers 2022, 14, 2118. [Google Scholar] [CrossRef]
- Alawadi, Z.; Phatak, U.R.; Hu, C.Y.; Bailey, C.E.; You, Y.N.; Kao, L.S.; Massarweh, N.N.; Feig, B.W.; Rodriguez-Bigas, M.A.; Skibber, J.M.; et al. Comparative effectiveness of primary tumor resection in patients with stage IV colon cancer. Cancer 2017, 123, 1124–1133. [Google Scholar] [CrossRef] [PubMed]
- van Rooijen, K.L.; Shi, Q.; Goey, K.K.H.; Meyers, J.; Heinemann, V.; Diaz-Rubio, E.; Aranda, E.; Falcone, A.; Green, E.; de Gramont, A.; et al. Prognostic value of primary tumour resection in synchronous metastatic colorectal cancer: Individual patient data analysis of first-line randomised trials from the ARCAD database. European journal of cancer (Oxford, England: 1990) 2018, 91, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Fields, A.; Pahwa, P.; Chandra-Kanthan, S.; Zaidi, A.; Le, D.; Haider, K.; Reeder, B.; Leis, A. Surgical Resection of Primary Tumor in Asymptomatic or Minimally Symptomatic Patients With Stage IV Colorectal Cancer: A Canadian Province Experience. Clinical colorectal cancer 2015, 14, e41–e47. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.S.; Kim, C.W.; Lim, S.B.; Yu, C.S.; Kim, S.Y.; Kim, T.W.; Kim, M.J.; Kim, J.C. Palliative surgery in patients with unresectable colorectal liver metastases: A propensity score matching analysis. J Surg Oncol 2014, 109, 239–244. [Google Scholar] [CrossRef]
- Zhang, R.X.; Ma, W.J.; Gu, Y.T.; Zhang, T.Q.; Huang, Z.M.; Lu, Z.H.; Gu, Y.K. Primary tumor location as a predictor of the benefit of palliative resection for colorectal cancer with unresectable metastasis. World J Surg Oncol 2017, 15, 138. [Google Scholar] [CrossRef]
- Kim, J.H.; Jin, S.; Jeon, M.J.; Jung, H.Y.; Byun, S.; Jung, K.; Kim, S.E.; Moon, W.; Park, M.I.; Park, S.J. Survival Benefit of Palliative Primary Tumor Resection Based on Tumor Location in Patients with Metastatic Colorectal Cancer: A Single-center Retrospective Study. The Korean journal of gastroenterology = Taehan Sohwagi Hakhoe chi 2020, 76, 17–27. [Google Scholar] [CrossRef]
- Liang, L.; Tian, J.; Yu, Y.; Wang, Z.; Peng, K.; Liu, R.; Wang, Y.; Xu, X.; Li, H.; Zhuang, R.; et al. An Analysis of Relationship Between RAS Mutations and Prognosis of Primary Tumour Resection for Metastatic Colorectal Cancer Patients. Cellular Physiology and Biochemistry 2018, 50, 768–782. [Google Scholar] [CrossRef]
- Gulack, B.C.; Nussbaum, D.P.; Keenan, J.E.; Ganapathi, A.M.; Sun, Z.; Worni, M.; Migaly, J.; Mantyh, C.R. Surgical Resection of the Primary Tumor in Stage IV Colorectal Cancer Without Metastasectomy is Associated With Improved Overall Survival Compared With Chemotherapy/Radiation Therapy Alone. Dis Colon Rectum 2016, 59, 299–305. [Google Scholar] [CrossRef]
Figure 1.
Patient selection flowchart. CRC, colorectal cancer; PTR, primary tumor resection; CTx, chemotherapy.
Figure 1.
Patient selection flowchart. CRC, colorectal cancer; PTR, primary tumor resection; CTx, chemotherapy.
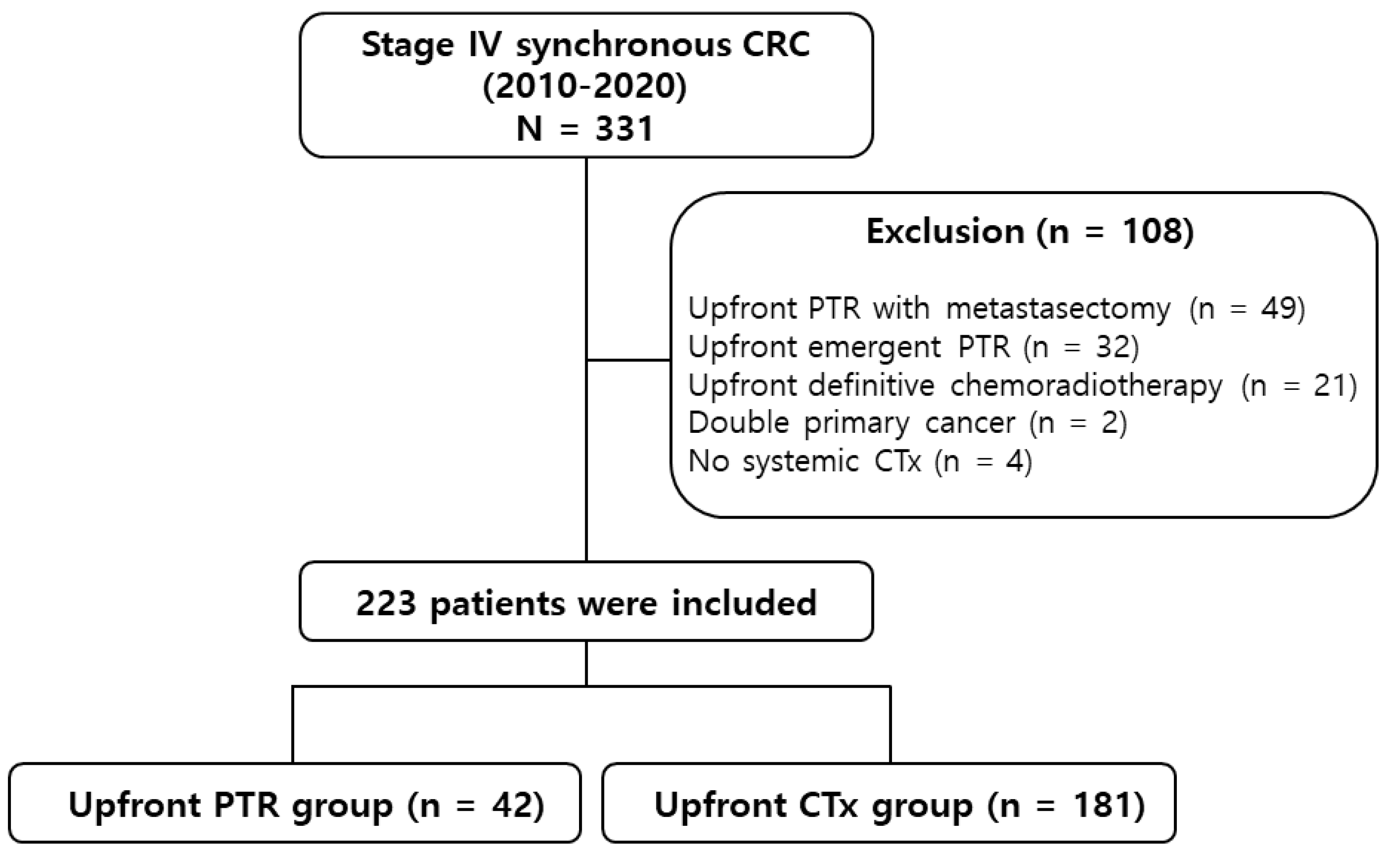
Figure 2.
Kaplan–Meier curves of overall survival. PTR, primary tumor resection.
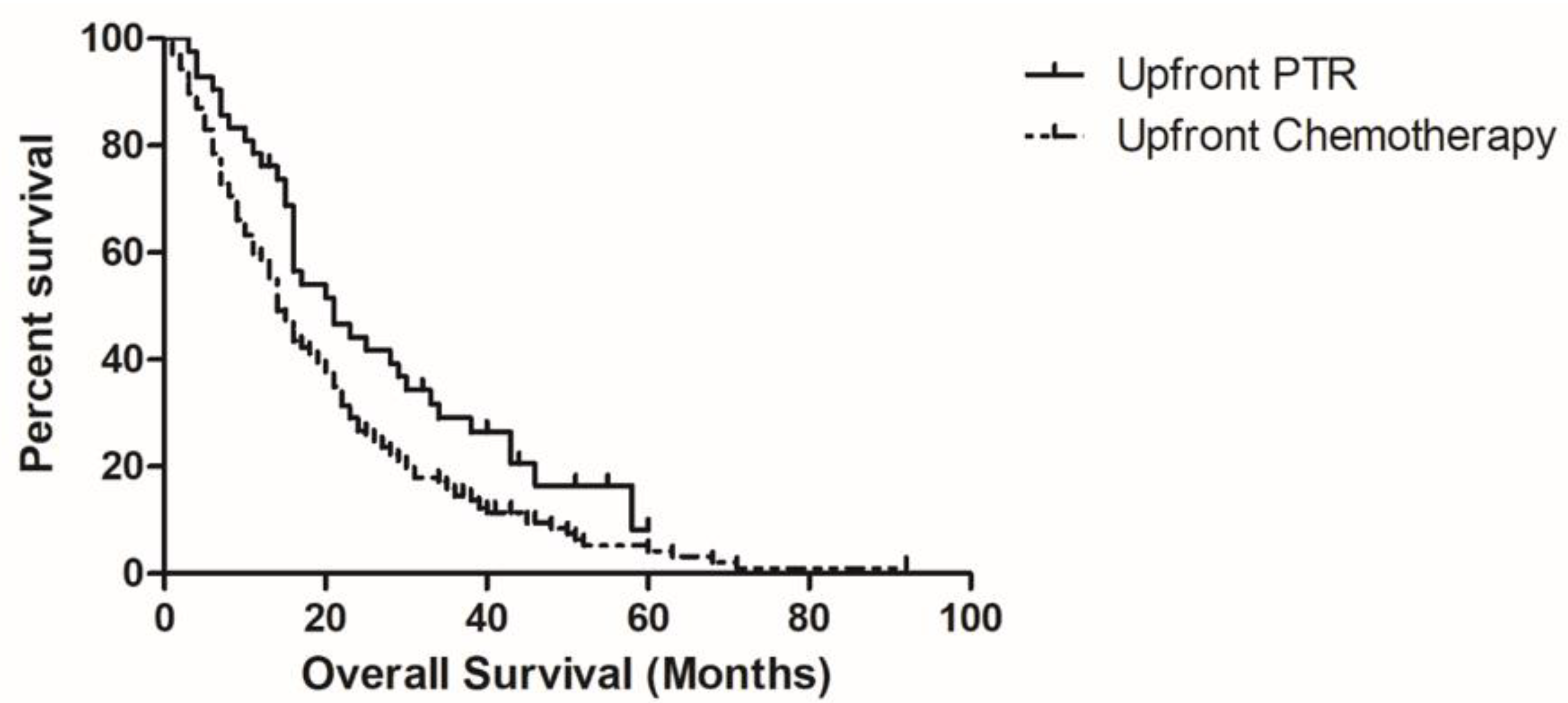
Figure 3.
Forest plot of overall survival. PTR, primary tumor resection; ECOG, Eastern Coopera-tive Oncology Group; CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio.
Figure 3.
Forest plot of overall survival. PTR, primary tumor resection; ECOG, Eastern Coopera-tive Oncology Group; CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio.
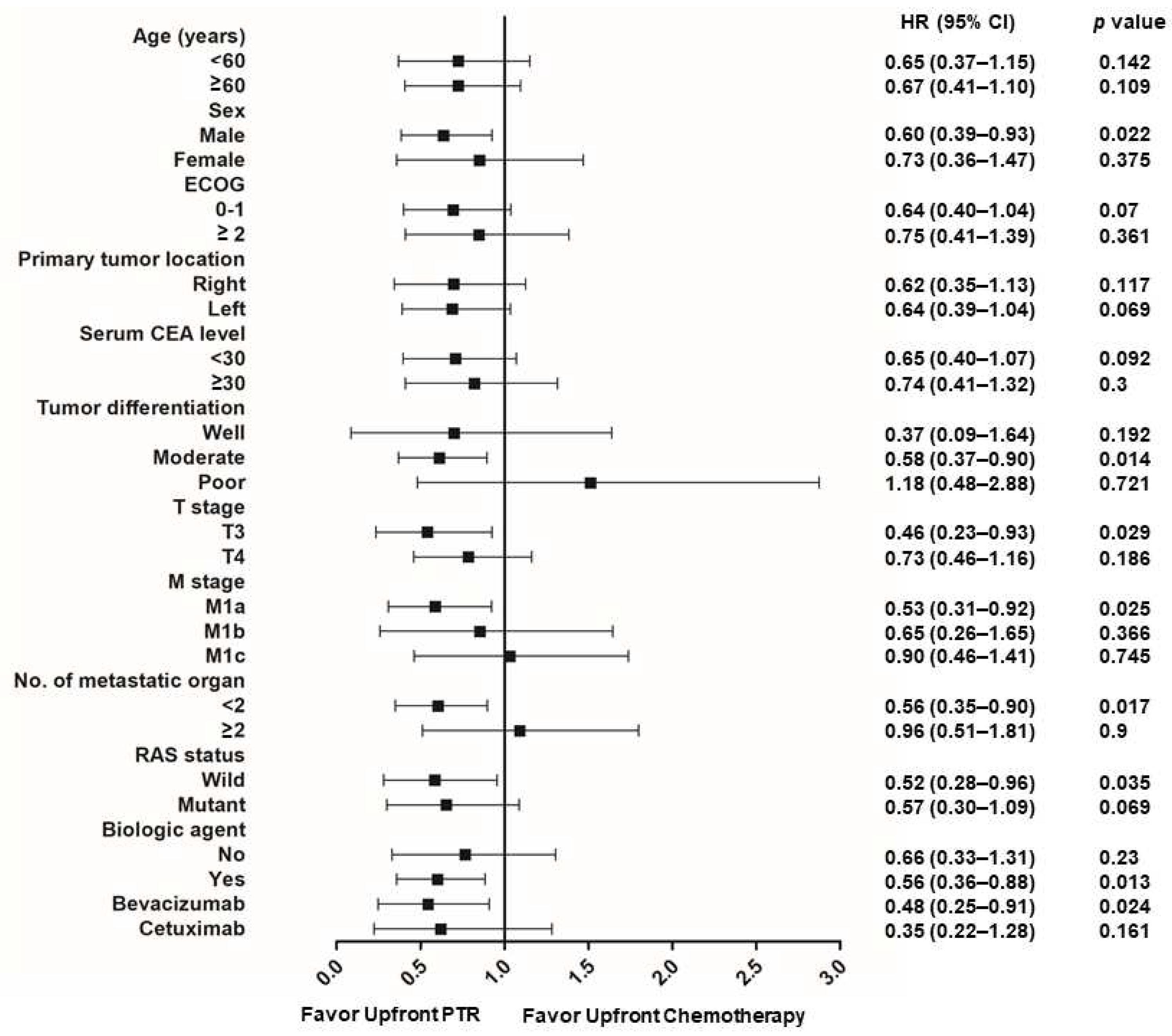

Table 1.
Baseline characteristics.
| Characteristic | Upfront PTR | Upfront chemotherapy | p value |
|---|---|---|---|
| N = 42 (%) | n = 181 (%) | ||
| Age (years) | |||
| Median (range) | 60 (34–84) | 63 (30–82) | 0.264 |
| Sex | |||
| Male | 31 (73.8) | 117 (64.6) | 0.259 |
| Female | 11 (26.2) | 64 (35.4) | |
| ECOG performance status | |||
| 0/1 | 29 (69.0) | 93 (51.4) | 0.038 |
| ≥2 | 13 (31.0) | 88 (48.6) | |
| Primary tumor location | |||
| Right-sided | 17 (40.5) | 46 (25.4) | 0.014 |
| Left-sided | 25 (59.5) | 135 (74.6) | |
| CEA (ng/mL) | 13.32 (1.0–594) | 39.47 (0–86,002) | 0.478 |
| Tumor differentiation | |||
| Well | 4 (9.5) | 20 (11.0) | 0.732 |
| Moderate | 30 (71.4) | 137 (75.7) | |
| Poor | 7 (16.7) | 19 (10.5) | |
| Clinical T stage | |||
| T3 | 13 (31.0) | 100 (55.2) | 0.005 |
| T4 | 29 (69.0) | 81 (44.8) | |
| Clinical N stage | |||
| N0 | 2 (4.8) | 6 (3.3) | 0.757 |
| N1 | 10 (23.8) | 52 (28.7) | |
| N2 | 30 (71.4) | 123 (68.0) | |
| Clinical M stage | |||
| M1a | 21(50.0) | 75 (41.4) | 0.015 |
| M1b | 6 (14.3) | 66 (36.5) | |
| M1c | 15 (35.7) | 40 (22.1) | |
| No. of organ metastasis | |||
| 0 or 1 | 30 (71.4) | 81 (44.8) | 0.002 |
| ≥2 | 12 (28.6) | 100 (55.2) | |
| RAS status | |||
| Wild | 16 (38.1) | 89 (49.2) | 0.707 |
| Mutant | 15 (35.7) | 72 (39.8) | |
| NA | 11 (26.2) | 20 (11.0) | |
| Time to chemotherapy (days) | 50.4 (±5.46) | 17.3 (±1.40) | <0.001 |
| 1st line chemotherapy | |||
| Fluoropyrimidine alone | 5 (11.9) | 1 (0.6) | <0.001 |
| Irinotecan doublet | 15 (35.7) | 108 (59.7) | |
| Oxaliplatin doublet | 22 (52.4) | 72 (39.8) | |
| 1st line targeted gent | |||
| Cetuximab | 9 (21.4) | 78 (43.1) | <0.001 |
| Bevacizumab | 13 (31.0) | 70 (38.7) | |
| No | 20 (47.6) | 34 (18.8) | |
| Administration of targeted agent | 29 (69.0) | 153 (84.5) | 0.021 |
| No. of lines of systemic treatment | 2 (1–7) | 2 (1–7) | 0.448 |
| Conversion resection (R0) | 9 (21.4) | 23 (12.7) | 0.004 |
PTR, Primary Tumor Resection; ECOG, Eastern Cooperative Oncology Group; CEA, carcinoembryonic antigen; NA, not available.
Table 2.
Variables associated with overall survival.
| Univariate | Multivariate | ||
|---|---|---|---|
| p-value | HR (95% CI) | p-value | |
| Age (≥ 60) | 0.001 | 1.530 (1.118–2.093) | 0.008 |
| Male | 0.160 | 1.239 (0.904–1.699) | 0.183 |
| ECOG ≥ 2 | 0.001 | 1.445 (1.072–1.948) | 0.016 |
| Right-side colon cancer | 0.038 | 1.342 (0.962–1.874) | 0.084 |
| CEA ≥ 30 (ng/mL) | 0.012 | 1.465 (1.066–2.013) | 0.019 |
| Tumor differentiation | 0.031 | 2.218 (1.217–4.040) | 0.009 |
| Clinical T4 stage | 0.782 | ||
| Clinical N1/2 stage | 0.399 | ||
| Clinical M1c stage | 0.148 | 1.595 (1.060–2.400) | 0.025 |
| No. of organ metastasis (≥2) | 0.120 | ||
| RAS mutation | 0.718 | ||
| Administration of targeted agent | 0.003 | 0.569 (0.387–0.837) | 0.004 |
| Upfront PTR | 0.019 | 0.679 (0.454–1.017) | 0.060 |
HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; CEA, carcinoembryonic antigen; PTR, Primary Tumor Resection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



