
Submitted:
21 April 2024
Posted:
07 May 2024
You are already at the latest version
Abstract
In the majority of children with growth hormone (GH) deficiency (GHD), normal GH secretion may occur before the attainment of final height. The aim of the study was to assess the incidence of persistent and transient GHD and the effectiveness of recombined human GH (rhGH) therapy in children with isolated idiopathic GHD, with respect to the moment of therapy withdrawal and according to different diagnostic criteria of GHD. Analysis included 260 patients (173 boys, 87 girls) with isolated idiopathic GHD who completed rhGH therapy and have reassessed GH and IGF-1 secretion. The incidence of transient GHD with respect to different pre- and post-treatment criteria was compared together with assessment of GH therapy effectiveness. Incidence of transient GHD, even with respect to pediatric criteria was very high. Normal GH secretion occurred before the attainment of near-final height. Application of more restricted criteria decreased the number of children diagnosed with GHD but not the incidence of transient GHD among them. Poor response to GH therapy was observed mainly in patients with normal IGF-1 before treatment, suggesting that diagnosis of GHD may be false positive. Further efforts should be made to avoid overdiagnosis GHD and overtreatment of the patients.
Keywords:
growth hormone deficiency
; growth hormone therapy
; near-final height
; retesting
; insulin-like growth factor-1
1. Introduction
According to current recommendations, the goals of growth hormone (GH) therapy in patients with GH deficiency (GHD) include not only promotion of linear growth in childhood but also correction of wide spectrum of metabolic disorders caused by GHD and improvement of the quality of life in all its periods. It became a premise for continuing treatment with recombined human GH (rhGH) in adulthood and for rhGH administration in the patients with adult-onset GHD. However, the therapy beyond the period of growing is indicated only in the patients with severe GHD and requires the use of lower rhGH doses than in childhood. As peak bone mass and adult muscle composition is reached few years later than the attainment of final height (FH), continuation of treatment with appropriate rhGH doses in this time – referred to as the transition period – is of particular importance if GH secretion is insufficient [1,2]. Thus, it is recommended to re-assess GH secretion in all patients after withdrawal the growth-promoting therapy and to identify ones with persistent severe GHD [1]. Taking into account the lower cut-off values for GH peak in stimulation tests confirming GHD in retesting than that established for children, as well as the observed normalization of previously decreased GH secretion in the majority of patients with isolated, idiopathic GHD, diagnosed in childhood, only a small proportion of them should continue rhGH therapy during adult life. Very important problem is the moment at which this retesting should be performed.
In the Consensus of GH Research Society (GHRS) from 2000 [3] it was recommended to repeat GH stimulation tests after the attainment of FH and to diagnose severe GHD in case of GH peak in insulin tolerance test (ITT) below 3.0 µg/l. This threshold have seemed too low for the patients in transition period. In 2005, Clayton et al. [4] proposed to increase the cut-off value for the patients in late puberty up to 5.0 µg/l. Two years later, in the Consensus of GH Research Society in cooperation with Endocrine Societies from Europe, US, Japan and Australia [5], a cut-off value of GH peak in stimulation tests diagnostic for GHD at transition period was established at the level of 6.0 µg/l. According to recent American guidelines [6], the patients with a diagnosis of isolated idiopathic GHD who had IGF-1 SDS over 0.0 after rhGH therapy withdrawal and wash-out period do not require retesting to exclude persistent GHD.
In 2016, Grimberg at al. [1] strongly recommended that rhGH treatment at pediatric doses should not be continued after the attainment of near-FH, defined as height velocity (HV) below 2-2.5 cm/year in boys with bone age (BA) 16-17 years and in girls with BA 14-15 years. All the patients who fulfilled these criteria should have reassessed GH secretion, as rhGH therapy should be resumed only in the case of confirmed persistent severe GHD. More recent studies of Penta et al. [7] and of Cavarzere et al. [8] have shown that normalization of GH secretion in children with isolated idiopathic GHD may occur in mid-puberty, before the attainment of near-FH. Moreover, already in 2002, Loche at al. [9] reported the possibility of even earlier normalization of GH secretion in children previously diagnosed with GHD.
According to the considerations of Bright et al. [10], the rate of false-positive results of GH stimulation tests, resulting in false-positive diagnoses of GHD, may be higher (even much higher) than the rate of true-positives. The authors have stressed the need to improve the diagnostic scheme due to the “low probability of GHD in a child with short stature and positive growth hormone stimulation tests”. The same problem with respect to children with idiopathic isolated GHD has been discussed in a recent paper of Allen [11]. Such situation is suggested to be an important cause of overdiagnosis GHD, leading to overtreatment of short children with rhGH. Moreover, the phenomenon of “transient” GHD may also be considered as a falsely-positive diagnosis of GHD, not necessarily as the evidence of normalization of previously decreased GH secretion. However, there are no diagnostic tools to clearly evaluate, in which patients this could occur.
Insulin-like growth factor-1 (IGF-1) is the main peripheral mediator of GH action. In the classification of pediatric endocrine diagnoses, provided by Wit et al. in 2007 [12], GHD was described as a synonym of secondary IGF-1 deficiency. Nevertheless, in the same year, GHRS published the update of Consensus concerning GHD in adults, in which the authors clearly stated that in adults normal IGF-1 concentration did not exclude GHD [5]. The same statement was confirmed by other authors [13,14]. However, according to more recent guidelines, the diagnosis of GHD have seemed unlikely in the patients with IGF-1 concentration over the median value in the population (i.e. IGF-1 SDS over 0.0) and the patients with a diagnosis of isolated idiopathic GHD and IGF-1 SDS over 0.0 after rhGH therapy withdrawal and wash-out period do not require retesting to exclude persistent GHD [6,15].
In 2020, Wit et al. [16] proposed to use serum IGF-1 concentration as a part of screening in children with growth failure, with different cut-offs, established with respect to the clinical likelihood of GHD. The authors decided to introduce IGF-1 SDS for BA and pubertal stage, not only for chronological age (CA) of children.
In Poland, during last 20 years, different criteria of rhGH therapy withdrawal have been applied for children diagnosed with GHD. Initially, rhGH therapy was discontinued when the child attained height corresponding to the value of 10th centile for the age of 18 years (170 cm for boys and 158 cm for girls), according to Polish reference charts [17] or BA equal or above 16 years in boys and 14 years in girls, with the possibility of earlier cessation of ineffective treatment if patient’s HV was below 3 cm/year. Next, when the availability of rhGH improved and the knowledge of its metabolic effects increased, the period of treatment has been extended up to the attainment of BA above 18 years in boys and above 16 years in girls, independently from patient’s height and current HV, still with the recommendation for its earlier termination due to HV below 3 cm/year but only in patients with BA below 16 years in boys and below 14 years in girls. The latter criteria have been modified according to the guidelines of Grimberg et al. [1] in mid-2022, i.e. after closing the database for present study. However, in practice, some patients who attained satisfactory height and/or experienced a significant slowdown of HV have decided to stop treatment before fulfilling the withdrawal criteria. This was especially true of boys with BA over 16 years and girls with BA over 14 years. Unfortunately, some of them have done it without consulting a doctor, thus becoming lost to follow-up. All the patients remaining under observation were asked to be subjected for retesting after rhGH therapy discontinuation and wash-out period. This re-evaluation of GH secretory status included at least one GH stimulation test in each patient and measurement of IGF-1 concentration. Thus, we have been able to collect retrospective data of a cohort of patients diagnosed with GHD in childhood, who completed growth promoting therapy and had performed retesting.
The aim of present study was to assess the incidence of persistent and transient GHD and the effectiveness of rhGH therapy in the patients diagnosed in childhood with isolated idiopathic GHD, with respect to the moment of rhGH therapy withdrawal (before or after the attainment of near-FH), according to different diagnostic criteria of GHD for childhood and for transition period. Taking into account the greater number of boys than girls qualified for rhGH therapy, as well as the gender-related criteria of rhGH therapy withdrawal, the patients were also divided by sex during the analysis.
2. Results
Retrospective analysis covered the data of 260 patients (173 boys, 87 girls) treated with rhGH in childhood due to isolated idiopathic GHD, who completed growth-promoting therapy and have reassessed GH secretory status after the wash-out period.
2.1. Assessment of the Incidence of Transient GHD with Respect to Pediatric Criteria from 2000 (GH Peak below 10 µg/l, IGF-1 Deficiency Not Required) [3] in Relation to the Moment of rhGH Therapy Withdrawal and Patients’ Sex
The detailed characteristic, including pre-treatment data, effectiveness of rhGH therapy and hormonal findings in retesting for the whole studied group and for the subgroups who completed treatment either before (Group PRE) or after (Group POST) the attainment of near-FH is presented in Table 1. At rhGH therapy onset, there was no significant difference between the Groups PRE and POST in height SDS at therapy onset (hSDS-0) and in the results of hormonal tests (GH peak and IGF-1 SDS). There was also no difference in both GH peak and IGF-1 SDS at retesting between these Groups.
The increase of hSDS-R with respect to hSDS-0 (Δ hSDS) was significant (p<0.001) in both Groups. During retesting, GH peak and IGF-1 SDS were significantly (p<0.001) higher than before treatment in each Group; moreover, median GH peak and median IGF-1 SDS were normal in both Groups (see Figure 1).
Despite significantly (p<0.001) shorter duration of rhGH therapy in Group PRE than in POST, both height SDS at retesting (hSDS-R) and the increase of height SDS (Δ hSDS) were significantly (p<0.001) higher in Group PRE than in POST. Nevertheless, hSDS-R was very close to target height (TH) SDS in both Groups, with no significant difference between PRE and POST (for details see Table 1).
Normalization of GH secretion at retesting with respect to the criteria for children (i.e. GH peak over 10.0 µg/l) was observed in 168 out of 260 patients (64.6%), 58 patients had GHD only with respect to pediatric criteria (i.e. GH peak between 6.0 and 10.0 µg/l), while only 34 patients (13.1%) had persistent GHD according to the criteria for transition period (i.e. GH peak below 6.0 µg/l), including only 10 patients (3.8%) fulfilling current criteria of persistent severe GHD (i.e. GH peak below 3.0 µg/l). There was no significant difference in the frequency of normal GH peaks in retesting according to pediatric criteria between Groups PRE and POST. This observation indicates that normalization of GH secretion took place before the attainment of near-FH. Detailed data with respect to different cut-offs of GH peak in retesting is provided in Table 2.
Despite this, the frequency of transient GHD with respect to pediatric criteria was significantly (p=0.008) higher in boys than in girls. Detailed data with respect to different cut-offs of GH peak in retesting and patients’ sex is provided in Table 3.
The only differences between boys and girls, both before treatment and at retesting, were related to patients’ age (significantly younger in girls, p<0.001 at both timepoints), GH peak in retesting and Δ GH peak (significantly higher in boys, p<0.001), and Δ hSDS (significantly better in boys), while there was no significant difference in other analyzed auxological indices (for details see Table 4). The increases of GH peak and of IGF-1 SDS in retesting with respect to pretreatment values, as well as of hSDS-R with respect to hSDS-0 were significant (p<0.001) both in boys and in girls.
The presented analyses have shown the predominance of boys in the group of treated children and the high incidence of transient GHD, even with respect to the criteria for childhood and even if retesting was performed before the attainment of near-FH, especially in boys. Effectiveness of rhGH therapy was better in the patients who stopped treatment before the attainment of near-FH (that may be a kind of bias as some patients who did not respond well could be treated longer than good responders who gave up treatment after the attainment of satisfactory height). Thus, the first important conclusion from our study could be the statement that normalization of GH secretion in stimulation tests occurred in the majority of patients with childhood-onset isolated, idiopathic GHD and took place before the attainment of near-FH. Moreover, cessation of rhGH therapy before the attainment of near-FH appeared to have no adverse effect on its effectiveness.
The overall high frequency of transient GHD, even higher in boys than in girls, has suggested the possibility of overdiagnosis GHD (and overtreatment with rhGH) of a significant proportion of the patients, especially of boys.
Thus we decided to check, if applying more restricted diagnostic criteria of GHD, proposed in recent years [15], could be useful to overcome these problems.
2.2. Verification of GHD Diagnosis in Childhood and the Incidence of Transient GHD with Respect to Currently Proposed Pediatric Criteria [15]
For the next part of the analysis, the following three subgroups of patients were extracted:
- ✓
- “Unlikely” GHD – the patients with IGF 1 SDS over 0.0, who could have GHD excluded without stimulation tests;
- ✓
- “Doubtful” GHD – the patients with IGF-1 SDS below 0.0 and GH peak in stimulation tests between 7.0 µg/l and 10.0 µg/l, who did not fulfill the criteria of GHD after applying lower cut-off of GH peak in stimulation tests;
- ✓
- “True” GHD – the patients with IGF-1 SDS below 0.0 and GH peak below 7.0 µg/l, the only subgroup that should be treated with rhGH according to current guidelines [15].
Consequently, at retesting we decided to qualify as non-GH-deficient all the patients with IGF-1 SDS over 0.0 (regardless of the results of GH stimulation tests) and to use the cut-off values 7.0 µg/l and 5.0 µg/l for GH peak in the patients with IGF-1 SDS below 0.0. Thus, we divided the patients with respect to the criteria for transition period into the following groups:
- ✓
- transient GHD (Group transGHD) – patients with IGF-1 SDS at retesting over 0.0 or GH peak at retesting over 7.0 µg/l,
- ✓
- “childhood-only” GHD (Group childGHD) – patients with IGF-1 SDS below 0.0 and GH peak 5.0-7.0 µg/l
- ✓
- persistent GHD (Group persistGHD) – patients with IGF-1 SDS below 0.0 and GH peak in retesting below 5.0 µg/l.
Transient GHD with respect to pre-treatment criteria for children was observed in 89.1% of children with “Unlikely” GHD before treatment, 89.6% of those with “Doubtful” GHD and as much as 86.2% of those diagnosed with “True GHD”. Thus, the change of diagnostic criteria of GHD in childhood could decrease the number of patients qualified to rhGH but not the incidence of transient GHD in retesting with respect to pre-treatment criteria. Numbers of patients in individual groups and subgroups are presented in Table 5.
Significant differences in the effectiveness of rhGH therapy between the groups with “Unlikely”, “Doubtful” and “True” GHD were observed. Post-hoc analysis showed that hSDS-R was significantly (p<0.001) lower in the patients with “Unlikely” GHD than in the remaining groups (the same concerned corr hSDS-R), while Δ hSDS was significantly (p=0.010) higher in “Doubtful” GHD than in other groups. Nevertheless, hSDS-R exceeded hSDS-0 significantly (p<0.001) in all groups. In the group with “Unlikely” GHD, lower quartile of hSDS-R was below -2.0, which means that over 25% of patients from this group had short stature at retesting.
Despite pre-treatment difference in IGF-1 SDS, defining the selection of the patients to “Unlikely” GHD and to the remaining groups (“Doubtful” and “True” GHD), the differences of IGF-1 SDS at retesting between these Groups were insignificant. However, IGF-1 SDS increased in “True” GHD and “Doubtful GHD, while decreased in “Unlikely” GHD. The differences in Δ IGF-1 SDS between the group with “Unlikely” GHD and the remaining groups (“Doubtful” and “True” GHD) were significant (p<0.001), with no significant difference between “True” GHD and “Doubtful” GHD. For details see Table 6 and Figure 2.
2.3. Characteristics of the Patients with Persistent Severe GHD According to Current Criteria (GH Peak in Retesting below 3.0 µg/l) [18].
Only 10 of 260 patients (3.85%), including 7 of 173 boys (4.05%) and 3 of 87 girls (3.45%) had GH peak in retesting below 3.0 µg/l, including 7 patients (5 boys and 2 girls) with IGF-1 SDS below -2.0 that additionally confirmed the diagnosis of severe GHD. Among these 7 patients, 5 were diagnosed in childhood with “True” GHD, while 1 boy with “Unlikely” GHD and 1 girl with “Doubtful” GHD. This boy was the youngest patient in the whole Group (3.5 years at diagnosis, 3.7 years at rhGH therapy onset), with a very severe deficit of height (hSDS 5.98) and very low GH peak (1.2 µg/l) but “normal” IGF-1 SDS. The patient was diagnosed in 1997 and had IGF-1 measured with RIA method that was used for a relatively small number of patients and has not been used in our center for 20 years, so it is difficult to explain the situation. The girl was aged 11.7 years at diagnosis, she had severe deficit of height (hSDS -3.13), GH peak 7.43 µg/l and severe IGF-1 deficiency (IGF-1 SDS 2.11) that persisted at retesting (IGF-1 SDS -2.57). She attained FH SDS -1.47 thus improving height by 1.66 SD with respect to hSDS at diagnosis. Among the remaining 3 patients with GH peak in retesting below 3.0 µg/l, two boys had relatively high IGF-1 SDS (0.83 and 1.03) and one girl had the “borderline” IGF-1 SDS (0.09) that could suggest falsely positive results of GH stimulation tests during retesting in them; among them, a girl and one boy had pre-treatment IGF-1 SDS over 0.0, while the second boy had at diagnosis GH peak 2.72 ng/ml and IGF-1 SDS below -2.0.
2.4. Effect of Application of Diagnostic Strategy Proposed by Wit et al. [16] on the Diagnosis of GHD in Childhood and during Retesting
According to the proposal of Wit et al. [16], IGF-1 assessment should be a part of laboratory screening of GHD to assess the pre-test likelihood of disease. This approach assumes subjecting to GH stimulation tests only the patients with real likelihood of GHD, based on clinical assessment and IGF-1 concentration, interpreted with respect to BA or pubertal stage. According to the proposed criteria and taking to account the inclusion criteria for the current study, our patients had low, very low or rather low pre-test likelihood of GHD, so the cut-off for IGF-1 SDS for them should be -2.0 or -1.0. In the retrospective analysis it was difficult to clearly distinguish the patients between these three subgroups, nevertheless none of our patients had moderate or high pre-test likelihood of GHD. Unfortunately, for some patients, exact data concerning pubertal stage was missing or reported as intermediate between subsequent Tanner stages. So, we decided to calculate IGF-1 SDS with respect to BA and to apply the cut-off for IGF-1 SDS at the level of -1.0. Thus, all the patients with IGF-1 SDS for BA over -1.0 were qualified independently from the results of GH stimulation tests to the Group “Pre-test Unlikely” GHD (that is not the same as “Unlikely” in previous analysis), while the remaining ones were qualified to the Groups with “Excluded” or “Confirmed” GHD, depending on GH peak in stimulation tests (below or over 7.0 µg/l). At retesting, “Transient” GHD (T-GHD) was defined as IGF-1 SDS over -1.0 or GH peak over 7.0 µg/l, “Non-transient” GHD (NT-GHD) as IGF-I SDS below -1.0 and GH peak between 5.0 and 7.0 µg/l, while “Persistent” GHD (P-GHD) as IGF-I SDS below -1.0 and GH peak below 5.0 µg/l (please note that this is not the same group as persistGHD in previous analysis).
As a result, 168 patients (64.6%) were qualified to “Pre-test Unlikely” Group, 45 ones (13.5%) were recognized as those with “Excluded” GHD, while only 47 patients (18.1%) were diagnosed with “Confirmed GHD”. At retesting, only 50 patients had IGF-1 SDS below -1.0 and only 13 of them (9 boys, 4 girls) had GH peak in retesting below 7.0 µg/l, among them only 3 patients had GH peak between 5.0 and 7.0 µg/l. The incidence of “Transient” GHD with respect to pre-treatment criteria was still very high: 87.2% in the “Confirmed” GHD Group, 93.3% in “Excluded” GHD Group and 97.6% in “Pre-test Unlikely” GHD Group. Unfortunately, only 6 out of 13 patients fulfilling pre-treatment criteria of GHD in retesting would be qualified as ones with “Confirmed” GHD and subjected to rhGH therapy according to the proposed criteria, while the remaining 7 could remain untreated (for details see Table 7). So, applying more restrictive criteria for diagnosing GHD might significantly decrease the number of treated patients, however, after applying the same criteria for retesting, the incidence of transient GHD remained very high.
The effectiveness of rhGH therapy was lower in the patients with “Pre-test Unlikely” GHD than in the remaining Groups (“Excluded” and “Confirmed” GHD), as post-hoc analysis showed that hSDS-R was significantly lower in “Pre-test Unlikely” GHD than in both “Excluded” GHD (p=0.006) and “Confirmed” GHD (p=0.03), the same was true for the corresponding differences in Δ hSDS (p=0.018 and p=0.013, respectively). There was no difference in any of the auxological indices of rhGH therapy effectiveness (hSDS-R, corr hSDS-R, Δ hSDS) between the patients with “Excluded” and “Confirmed” GHD, and the only differences between these two Groups concerned the results of GH stimulation test. Despite the fact that GH peak in retesting was significantly lower in the Group with “Confirmed” GHD than in both “Excluded” GHD (p<0.001) and “Pre-test Unlikely” GHD (p=0.16), median value of GH peak in retesting was over the cut-off for diagnosis in all Groups. Moreover, the value of lower quartile of GH peak in retesting did not exceed this cut-off only in “Confirmed” GHD. Nevertheless, as both Groups were treated with rhGH, it is very difficult to speculate, if one of these Groups should be treated, while the second could really remain untreated. Detailed data is presented in Table 8.
2.5. Characteristics of Poor Responders to rhGH Therapy
At retesting, 44 patients with Δ hSDS below 1.0 fulfilled the criteria of poor response to rhGH therapy. This was not consistent with the number of patients who did not reach “normal” height as in some patients hSDS at retesting remained below -2.0 despite its significant improvement with respect to pre-treatment value. Thus, non-responders constituted 16.92% of the entire Group. It seems important that over one third (33.36%) of patients with “Unlikely” GHD, while only every tenth with “Doubtful” GHD (10.42%) and every eighth with “True” GHD (12.84%), classified according to the criteria of GHRS from 2019 [15] turned out to be non-responders.
Especially important seem to be the distribution of poor responders among the Groups extracted according to the criteria proposed by Wit et al. [16], as only 5 of them were in the “Confirmed” GHD Group (10.64% of the Group), 3 in the “Excluded” GHD Group (6.67% of the Group), while the remaining 36 in “Pre-test Unlikely” GHD Group (28.13% of the Group). Moreover, at retesting all poor responders had transient GHD with respect to pre-treatment criteria of Wit et al. [16].
3. Discussion
Previous studies conducted in the last decade of the 20th century showed that a significant proportion of patients with GHD diagnosed in childhood had sufficient GH secretion during retesting after completion of linear growth, especially if deficit of GH was idiopathic and not associated with other disorders of pituitary function [19,20,21]. The results of other studies pointed at the possibility of earlier normalization of GH secretion, raising up the questions concerning the optimal duration of rhGH therapy. In 1992, Cacciari at al. [22] observed normalization of previously decreased GH secretion after 1 month withdrawal of rhGH therapy in the majority of pubertal children but in none of those who were still prepubertal at retesting, which indicated that some children diagnosed as GH-deficient did not have a true GHD. Ten years later, Loche at al. [9] reported normal GH response to pharmacological stimulation in 28 of 33 prepubertal children with normal MRI of pituitary region, diagnosed with GHD on the ground of the same stimulation tests just 1-6 months earlier. The authors pointed at the need to follow-up and reassess such patients before a diagnosis of GHD was definitely established. In 2006, Zucchini et al. [23] reported normal GH secretion at puberty in one third of children diagnosed with isolated GHD before puberty. Moreover, despite the withdrawal of rhGH therapy in this group of children, the attained adult height was similar in them and in the remaining patients who completed treatment when their HV slowed down below 1 cm/year and BA was at least 17 years in boys and 15 years in girls. In the paper published in 2015, Bizzarri et al. [24] demonstrated normalization of GH secretion in retesting performed during puberty or even before its onset in 36 of 38 children with previous diagnosis of idiopathic GHD; in the remaining 2 subjects GH peak was decreased but IGF-1 levels were normal. The authors pointed at the high rate of falsely positive results of GH stimulation tests and the need for early retesting in the case of unsatisfactory response to GH therapy. Five years ago, Penta et al. [7] have reported persistent GHD (however with normal IGF-1 levels) in transition period in only 5 of 31 patients diagnosed with idiopathic GHD in childhood. In conclusion, they suggested that the timing of retesting should be anticipated in order to avoid overtreatment. In 2020, Cavarzere et al. [8] have documented normal GH secretion in retesting, performed in the intermediate stage of puberty, after the wash-out period, in 55% of children diagnosed previously with GHD and treated with GH for at least 2 years. Similarly to previous observations of Zucchini et al. [23], definitive discontinuation of treatment in this group of patients did not impair their growth potential (their adult height was similar as in the remaining 45% of children with confirmed GHD, treated up to the attainment of near-FH).
On the other hand, Lanzetta et al. [25] have reported similar effectiveness of rhGH therapy in the patients with definite GHD (confirmed genetic defect, combined pituitary hormone deficiency, anatomical hypothalamic-pituitary abnormality) and with “short stature unresponsive to stimulation” (decreased GH peak in stimulation tests but no identified cause of impaired GH secretion).
In our previous study [26] the incidence of persistent GHD (with the cut-off limit for GH peak in 2 stimulation tests appropriate for transition period, i.e. 6 µg/l) in the patients diagnosed with isolated, non-acquired GHD in childhood, who completed growth-promoting treatment and attained FH, was only 12%.
In the already quoted paper, Cacciari et al. [22] stated that the observed discrepancies between the results of repeated GH stimulation tests were caused by errors in the diagnosis of GHD, including variability in GH response to stimulation (pharmacological or physiological), transient GHD and the difficulties in distinguishing true GHD from delayed puberty.
It seems very important to recognize if we are dealing with real (true) normalization of GH secretion at puberty in children, who have actually been GH-deficient before puberty, or with poor reproducibility of the results of GH stimulation tests, manifesting as apparent (false) GHD that disappears at the time of retesting.
The incidence of transient GHD with respect to pre-treatment criteria among our patients was high and independent from the moment of retesting (before or after the attainment of near-FH) that confirms that GH secretion appears normal earlier than the patients fulfill current exclusion criteria for rhGH treatment. Unfortunately, applying more restrictive diagnostic criteria in childhood may decrease the number of patients qualified to rhGH therapy but not the incidence of transient GHD if the same criteria are used for retesting, which indicates that the problem of overdiagnosing childhood-onset idiopathic isolated GHD may be only partially resolved by such modifications.
In our study, similarly as in the majority of papers concerning rhGH therapy in children with GHD, the number of boys exceeded the number of girls, suggesting the higher incidence of GHD among boys than among girls. However, according to the report of Tanaka et al. [27], this difference seems to reflect a selection bias related to a higher proportion of boys among children seeking treatment due to short stature. Interestingly, the incidence of transient GHD was higher among boys than among girls, with similar number of male and female patients fulfilling the criteria of persistent GHD. Our study was limited to the patients with isolated GHD, nevertheless, the obtained results seem to stay in line with the very recent report of Henry et al. [28], who observed male predominance in referrals to clinic for short stature, but not among the patients with abnormal pituitary MRI and/or multiple pituitary hormone deficiency. It seems worth considering that real incidence of GHD may be definitely lower than the frequency of diagnosing this disease in children and independent from the patients' sex.
We observed a wide range of growth responses to rhGH therapy, with the highest rate of poor responders among the patients with “Pre-test Unlikely” GHD, according to the criteria proposed by Wit at al. [16]. Moreover, with respect to the same criteria, none of the poor responders had persistent GHD. These findings suggest the possibility of other causes of short stature in a significant proportion of poor responders, who were all ineffectively treated as GH-deficient. It seems impossible to forecast, what would happen if the modified diagnostic criteria were applied for our patients. Nevertheless, our results confirm the need for further research on the diagnostic criteria of idiopathic isolated GHD in children and on the optimal rhGH therapy duration.
One direction of research should be introducing prediction models of rhGH therapy effectiveness into clinical practice in order to have reasonable expectations about the effects of treatment and to identify poor responders as early and possible. Prediction models are developed for many years with use of different methods, like linear and non-linear regression, neural networks or other advanced computational techniques, however only few of them allows to predict the therapy outcome [29,30,31,32,33,34]. It seems that the availability of such models in the form of easy-to-use calculators would facilitate the decision to discontinue GH therapy and to perform retesting earlier.
Second direction is better identification of the moment of normalization of GH secretion in order to discontinue treatment in the patients in whom GHD was transient. In poor responders the extended diagnostics should be considered, especially in the case of transient GHD, as the real cause of short stature in them might remain unrecognized. In this aspect, very important seems to be the recent project of Brettell et al. [35] who decided to assess the effect on FH of discontinuation versus continuation of rhGH therapy in pubertal children with isolated GHD.
Last but not least, it seems that high incidence of falsely positive results of GH stimulation tests in children with short stature should be taken into account. According to previous studies, this problem may concern a relatively high proportion of the patients [10,11,16,36].
It has been proposed to use sex steroid priming in selected groups of children and it was done in Poland many years ago. The patients subjected to the present study did not have such priming due to the lack of clear national recommendation at the moment of their diagnostics. Priming has been recommended in the guidelines of Grimberg et al. [1] and in more recent papers [15,37,38,39], thus it is a potential solution to decrease the number of the patients overdiagnosed with GHD. It seems possible that the problem of falsely positive results of GH stimulation tests may – at least to some extend – concern retesting, however there is no sufficient data on this issue. This could explain the diagnosis of persistent GHD at retesting in some patients who did not fulfill current diagnostic criteria of this disease in childhood, however this is more of an assumption than a conclusion.
Another topic for further research should be revision of the criteria of rhGH therapy effectiveness in children diagnosed with isolated idiopathic GHD in the context of exclusion of previous diagnosis in the majority of treated patients. If some of them were GH-deficient not during the whole therapy duration or even falsely diagnosed as GH-deficient, it is possible that some of apparently good responders could grow-up well without treatment. Such eventuality has been suggested in a recent paper of Bright et al. [10]. On the other hand, in our study the highest proportion of poor responders was among the patient who should have excluded or unlikely GHD according to current criteria. Labelling such patients as GH-deficient might lead to completion of diagnostics for other causes of short stature, while, in recent years, the possibilities of revealing genetic defects in children previously treated as having idiopathic short stature, have significantly expanded [40]. Until the optimal criteria for the diagnosis of childhood isolated idiopathic GHD are established, earlier retesting of poor responders to rhGH therapy, followed by extended genetic diagnostics in the case of not confirmed GHD, seems worth considering as an alternative for long-term ineffective treatment.
4. Materials and Methods
Retrospective analysis included 260 patients (173 boys, 87 girls) with short stature, who fulfilled diagnostic criteria of isolated idiopathic GHD and were treated with rhGH in childhood, completed growth-promoting therapy and have reassessed GH secretory status after the wash-out period. The patients with other hormonal deficits (except for well controlled primary hypothyroidism), malnutrition, chronic diseases, neoplastic processes, diagnosed or suspected skeletal dysplasia, long-term or recurrent glucocorticoid administration and other therapies that might disturb growth or the function of somatotropic axis were excluded from the study; pubertal development was spontaneous and completed at therapy withdrawal in each case, however it could have been delayed. All girls included had normal female karyotype (46,XX). Magnetic resonance imaging (MRI) of hypothalamic-pituitary region was performed in each case before treatment and all the patients with pituitary/hypothalamic structural defects (except for isolated decreased size of anterior pituitary) and/or with the history of brain injuries, neurosurgery or tumors were excluded from the study. The diagnosis of GHD in childhood was based on auxological and hormonal criteria.
4.1. Auxological Indices
Auxological criteria included: short stature below 3rd centile according to national growth charts [17], slow HV expressed as decrease of patient’s height standard deviation score (hSDS) during at least 6 months of observation and delayed BA.
For 224 patients, data concerning the heights of their parents were available and target heights SDS (TH SDS) were calculated. Patients’ corrected height SDS (corr hSDS) at diagnosis were calculated as the difference between hSDS at diagnosis (hSDS-0) and TH SDS.
During rhGH treatment, the patients had routinely assessed BA at least once a year, including the last X-ray at therapy withdrawal. For each patient, near-FH was defined in concordance with the recommendations of Grimberg et al. [1] as achieving BA over 16 years in boys and over 14 years in girls, together with deceleration of HV below 2.5 cm/year (based on measurements at least 6 months apart). That allowed to classify the patients with respect to the moment of rhGH therapy withdrawal into Group PRE – patients who completed treatment before the attainment of near-FH or Group POST – ones who were treated up to the attainment of near-FH or longer. The patients in whom the advancement of BA had not fully corresponded to the growth rate were not included in the study due to the difficulties in clear determining the moment of the attainment of near-FH.
At retesting, patients’ heights were measured and the value of hSDS (hSDS-R) for age and sex were calculated and compared with hSDS-0 (Δ hSDS was calculated as the difference between hSDS-R and hSDS-0). The patients with Δ hSDS below 1.0 were classified as poor responders to rhGH therapy. The difference between hSDS-R and TH SDS (corr hSDS-R) was calculated as an additional index of rhGH therapy effectiveness.
4.2. Hormonal Tests
Hormonal confirmation of GHD in childhood was GH peak below 10.0 µg/l in two stimulation tests: with clonidine 0.15 mg/m2, orally (GH concentrations measured every 30 minutes from 0 to 120 minute of the test) and with glucagon 0.03 mg/kg (not exceeding 1.0 mg), intramuscularly (GH concentrations measured in 0, 90, 120, 150 and 180 minute of the test). However, taking into account the suggestions from more recent studies [15,42,43] that this threshold might be too high, for several analyses a subgroup of children with GH peak in both tests below 7.0 µg/l was extracted.
Reassessment of GH secretion (retesting) was performed after completion of rhGH therapy and a wash-out period (between 1 and 6 months). All the patients had performed insulin tolerance test (ITT) with insulin in a dose 0.1 IU/kg, intravenously (GH and glucose concentrations measured every 30 minutes from 0 to 120 minute of test; the test had to be repeated if there was no glucose decrease below 40.0 mg/dl or by at least 50% of initial value) and the second test with clonidine, with the drug dose and timepoints of GH sampling as in childhood (this test could be withdrawn in the patients with GH peak in ITT over 10.0 µg/l).
The three cut-off values were applied in the first statistical analysis: 3.0 µg/l (cut-off value for diagnosing persistent severe GHD in adults) 6.0 µg/l (cut-off value suggested for the patients in transition period) and 10.0 µg/l as a standard threshold for diagnosing GHD in children. Next, we chose lower thresholds for GH peak in retesting: 5.0 µg/l (according to most recent guidelines) [6] and 7.0 µg/l (the same value as recently proposed for children). Using the same cut-offs of GH peak in retesting as in childhood seemed justified as the analysis included the patients who stopped treatment before the attainment of near-FH.
The concentrations of GH were measured by the two-site chemiluminescent enzyme immunometric assay (hGH IMMULITE, DPC) for the quantitative measurement of human GH, calibrated to WHO IRP 80/505 standard or to 98/574 standard (as provided by the manufacturer).
In all patients IGF-1 concentrations were assessed both before treatment and during retesting. In the years 2003-2016, IGF-1 concentrations were measured with solid-phase, enzyme-labelled chemiluminescent immunometric assays (IMMULITE, DPC), calibrated to WHO NIBSC 1st IRR 87/518. Since 2017 new IGF-1 assays, standardized to WHO 1st International Standard 02/254, become available, that resulted in the need of conversion of the obtained results, according to the equation provided in Siemens Healthcare Diagnostics Customer Bulletin for IMMULITE® 2000 Immunoassay System, from May 2016 [44]. The agreement of IGF-1 measurements by different assays, especially for lower limits of reference values and with differences on raw values but not on SDS values, has been confirmed in dedicated studies [45,46]. All IGF-1 values were expressed as IGF-1 SDS for age and sex, according to the formula proposed by Blum & Schweitzer [47] and reference data for the laboratory method used [48]. Up to 2003, IGF-1 concentrations were measured with IGF-I-D-RIA-CT (Biosource Europe, Belgium); this method was used only for 74 patients in pre-treatment period, for these measurements, IGF-1 SDS values were calculated according to the reference data provided with the kits.
For the last analysis IGF-1 SDS for BA were calculated, according to the same rules as for CA (which was clearly indicated), everywhere else, IGF-1 SDS values refer to CA.
It should be noted that IGF-1 deficiency was not listed among the criteria of qualification patients to rhGH therapy in Poland, thus some children diagnosed with GHD could have normal IGF-1 levels before treatment, including ones with IGF-1 SDS over 0.0.
Taking into account the rule that isolated idiopathic GHD is unlikely in the patients with IGF-1 SDS over 0.0 [6,15], this cut-off value was applied in some analyses. Finally, the criteria of pre-test likelihood of GHD proposed by Wit et al. [16], based on clinical positive and negative clues, and IGF-1 concentration, were retrospectively applied in our cohort of patients.
4.3. Statistical Analysis
Statistical analysis was performed for the subgroups of patients, divided according to the moment of rhGH therapy withdrawal and sex, as well as with respect to different cut-offs of GH peak in stimulation tests and IGF-1 SDS at diagnosis and during retesting.
First, the distributions of the analysed variables were assessed with Shapiro-Wilk test. As they usually did not follow normal distribution in at least one group, descriptive statistics reported median and interquartile ranges of variables. The comparisons between the groups of patients were performed with nonparametric tests: Mann-Whitney U test was selected for comparisons of continuous variables between two groups, while Kruskal-Wallis ANOVA with appropriate post-hoc tests for more than two groups. Two measurements of the same variable in the same group in different time points were compared by Wilcoxon test; t test for repeated measurements was not chosen since normality assumption was often violated. Fisher exact test was used for the assessment of differences in the frequency of persistent and transient GHD, as well as in proportions of males and females in particular groups. Analysis was performed with Statistica 13.3.
5. Conclusions
Normalization of GH secretion in the patients diagnosed in childhood with idiopathic isolated GHD is observed in most patients and occurs before the attainment of near-final height.
Applying more restrictive diagnostic criteria of GHD in childhood (the necessity to confirm IGF-1 deficiency, lower cut-off for GH peak in stimulation tests) may decrease the number of patients qualified to rhGH therapy but not the incidence of transient GHD among treated patients, if the same pre-treatment criteria are applied during retesting.
Taking into account the available knowledge and emerging doubts or uncertainties concerning the diagnosis of isolated idiopathic GHD in childhood, further efforts should be made for avoiding overdiagnosis and overtreatment of the patients with only apparent disease and for rationalization of rhGH treatment costs.
Special attention should be paid on poor responders to rhGH therapy in whom the diagnosis of GHD may be false positive and the real cause of short stature undiagnosed..
Author Contributions
Conceptualization, J.S.; methodology, J.S. and U.S; validation, R.S, M.H. and A.L.; formal analysis, J.S.; investigation, J.S., M. H. and R.S.; resources, J.S., M. H. and R.S.; data curation, U.S.; writing—original draft preparation, J.S.; writing—review and editing, M.H., U.S., A.L. and R.S.; visualization, J.S.; supervision, R.S. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: “This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Polish Mother’s Memorial Hospital – Research Institute in Lodz, Poland.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grimberg, A.; DiVall, S.A.; Polychronakos, C.; Allen, D.B.; Cohen, L.E.; Quintos, J.B.; Rossi, W.C.; Feudtner, C.; Murad, M.H. Guidelines for Growth Hormone and Insulin-Like Growth Factor-I Treatment in Children and Adolescents: Growth Hormone Deficiency, Idiopathic Short Stature, and Primary Insulin-Like Growth Factor-I Deficiency. Horm. Res. Paediatr. 2016, 86, 361–397. [Google Scholar] [CrossRef] [PubMed]
- Ahmid, M.; Perry, C.G.; Ahmed, S.F.; Shaikh, M.G. Growth hormone deficiency during young adulthood and the benefits of growth hormone replacement. Endocr. Connect. 2016, 5, R1–R11. [Google Scholar] [CrossRef] [PubMed]
- Growth Hormone Research Society Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH Research Society. GH Research Society. J. Clin. Endocrinol. Metab. 2000, 85, 3990–3993. [CrossRef]
- Clayton, P.E.; Cuneo, R.C.; Juul, A.; Monson, J.P.; Shalet, S.M.; Tauber, M. Consensus statement on the management of the GH-treated adolescent in the transition to adult care. Eur. J. Endocrinol. 2005, 152, 165–170. [Google Scholar] [CrossRef]
- Ho, K.K.Y. Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: A statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. Eur. J. Endocrinol. 2007, 157, 695–700. [Google Scholar] [CrossRef]
- Yuen, K.C.J.; Biller, B.M.K.; Radovick, S.; Carmichael, J.D.; Jasim, S.; Pantalone, K.M.; Hoffman, A.R. American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Growth Hormone Deficiency in Adults and Patients Transitioning From Pediatric To Adult Care. Endocr. Pract. 2019, 25, 1191–1232. [Google Scholar] [CrossRef]
- Penta, L.; Cofini, M.; Lucchetti, L.; Zenzeri, L.; Leonardi, A.; Lanciotti, L.; Galeazzi, D.; Verrotti, A.; Esposito, S. Growth hormone (GH) therapy during the transition period: Should we think about early retesting in patients with idiopathic and isolated GH deficiency? Int. J. Environ. Res. Public Health. 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Cavarzere, P.; Gaudino, R.; Sandri, M.; Ramaroli, D.A.; Pietrobelli, A.; Zaffanello, M.; Guzzo, A.; Salvagno, G.L.; Piacentini, G.; Antoniazzi, F. Growth hormone retesting during puberty: a cohort study. Eur. J. Endocrinol. 2020, 182, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Loche, S.; Bizzarri, C.; Maghnie, M.; Faedda, A.; Tzialla, C.; Autelli, M.; Casini, M.R.; Cappa, M. Results of early reevaluation of growth hormone secretion in short children with apparent growth hormone deficiency. J. Pediatr. 2002, 140, 445–449. [Google Scholar] [CrossRef]
- Bright, G.M.; Morris, P.A.; Rosenfeld, R.G. When Is a Positive Test for Pediatric Growth Hormone Deficiency a True-Positive Test? Horm. Res. Paediatr. 2022, 94, 399–405. [Google Scholar] [CrossRef]
- Allen, D.B. Diagnosis of Growth Hormone Deficiency Remains a Judgment Call-and That Is Good. Horm. Res. Paediatr. 2022, 94, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Wit, J.-M.; Ranke, M.B.; Kelnar, C.J.H. The ESPE classification of paediatric endocrine diagnoses. Horm. Res. 2007, 68, 1–120. [Google Scholar]
- Gasco, V.; Corneli, G.; Beccuti, G.; Prodam, F.; Rovere, S.; Bellone, J.; Grottoli, S.; Aimaretti, G.; Ghigo, E. Retesting the childhood-onset GH-deficient patient. Eur. J. Endocrinol. 2008, 159, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Meazza, C.; Gertosio, C.; Pagani, S.; Pilotta, A.; Tinelli, C.; Buzi, F.; Farello, G.; Genoni, G.; Bona, G.; Bozzola, M. Is retesting in growth hormone deficient children really useful? Minerva Endocrinol. 2017, 42, 325–330. [Google Scholar] [CrossRef]
- Collett-Solberg, P.F.; Ambler, G.; Backeljauw, P.F.; Bidlingmaier, M.; Biller, B.M.K.; Boguszewski, M.C.S.; Cheung, P.T.; Choong, C.S.Y.; Cohen, L.E.; Cohen, P.; et al. Diagnosis, Genetics, and Therapy of Short Stature in Children: A Growth Hormone Research Society International Perspective. Horm. Res. Paediatr. 2019, 92, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Wit, J.M.; Bidlingmaier, M.; de Bruin, C.; Oostdijk, W. A Proposal for the Interpretation of Serum IGF-I Concentration as Part of Laboratory Screening in Children with Growth Failure. J. Clin. Res. Pediatr. Endocrinol. 2020, 12, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Palczewska I, Niedźwiecka Z. Indices of somatic development of children and adolescents in Warsaw. Develop. Pediatr. Med. 2001, Suppl 1 to 5, 17–118. [in Polish].
- Lewiński, A.; Smyczyńska, J.; Stawerska, R.; Hilczer, M.; Stasiak, M.; Bednarczuk, T.; Bolanowski, M.; Junik, R.; Ruchała, M.; Syrenicz, A.; et al. National Program of Severe Growth Hormone Deficiency Treatment in Adults and Adolescents after Completion of Growth Promoting Therapy. Pol. J. Endocrinol. 2018, 69, 468–524. [Google Scholar] [CrossRef]
- Tauber, M.; Moulin, P.; Pienkowski, C.; Jouret, B.; Rochiccioli, P. Growth hormone (GH) retesting and auxological data in 131 GH-deficient patients after completion of treatment. J. Clin. Endocrinol. Metab. 1997, 82, 352–356. [Google Scholar] [CrossRef]
- Maghnie, M.; Strigazzi, C.; Tinelli, C.; Autelli, M.; Cisternino, M.; Loche, S.; Severi, F. Growth hormone (GH) deficiency (GHD) of childhood onset: reassessment of GH status and evaluation of the predictive criteria for permanent GHD in young adults. J. Clin. Endocrinol. Metab. 1999, 84, 1324–1328. [Google Scholar] [CrossRef]
- Aimaretti, G.; Baffoni, C.; Bellone, S.; Di Vito, L.; Corneli, G.; Arvat, E.; Benso, L.; Camanni, F.; Ghigo, E. Retesting young adults with childhood-onset growth hormone (GH) deficiency with GH-releasing-hormone-plus-arginine test. J. Clin. Endocrinol. Metab. 2000, 85, 3693–3699. [Google Scholar] [CrossRef]
- Cacciari, E.; Tassoni, P.; Parisi, G.; Pirazzoli, P.; Zucchini, S.; Mandini, M.; Cicognani, A.; Balsamo, A. Pitfalls in diagnosing impaired growth hormone (GH) secretion: retesting after replacement therapy of 63 patients defined as GH deficient. J. Clin. Endocrinol. Metab. 1992, 74, 1284–1289. [Google Scholar] [CrossRef]
- Zucchini, S.; Pirazzoli, P.; Baronio, F.; Gennari, M.; Bal, M.O.; Balsamo, A.; Gualandi, S.; Cicognani, A. Effect on adult height of pubertal growth hormone retesting and withdrawal of therapy in patients with previously diagnosed growth hormone deficiency. J. Clin. Endocrinol. Metab. 2006, 91, 4271–4276. [Google Scholar] [CrossRef]
- Bizzarri, C.; Pedicelli, S.; Boscherini, B.; Bedogni, G.; Cappa, M.; Cianfarani, S. Early retesting by GHRH + arginine test shows normal GH response in most children with idiopathic GH deficiency. J. Endocrinol. Invest. 2015, 38, 429–436. [Google Scholar] [CrossRef]
- Lanzetta, M.A.; Dalla Bona, E.; Tamaro, G.; Vidonis, V.; Vittori, G.; Faleschini, E.; Barbi, E.; Tornese, G. Clinical and laboratory characteristics but not response to treatment can distinguish children with definite growth hormone deficiency from short stature unresponsive to stimulation tests. Front. Endocrinol. (Lausanne). 2024, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Smyczyńska, J.; Stawerska, R.; Lewiński, A.; Hilczer, M. Incidence and predictors of persistent growth hormone deficiency (GHD) in patients with isolated, childhood-onset GHD. Pol. J. Endocrinol. 2014, 65, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Soneda, S.; Sato, N.; Kishi, K.; Noda, M.; Ogasawara, A.; Nose, O.; Nakano, Y.; Kinoshita, E.; Mochizuki, T.; et al. The Boy:Girl ratio of children diagnosed with growth hormone deficiency-induced short stature is associated with the boy:Girl ratio of children visiting short stature clinics. Horm. Res. Paediatr. 2021, 94, 211–218. [Google Scholar] [CrossRef]
- Henry, R.K.; Mamilly, L.; Chaudhari, M.; Klamer, B.G.; Nikahd, M.; Pyle-Eilola, A.L. Beyond the bias! Sex distribution in paediatric growth hormone deficiency reexamined. Clin. Endocrinol. (Oxf). 2024, 100, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Migliaretti, G.; Ditaranto, S.; Guiot, C.; Vannelli, S.; Matarazzo, P.; Cappello, N.; Stura, I.; Cavallo, F. Long-term response to recombinant human growth hormone treatment: a new predictive mathematical method. J. Endocrinol. Invest. 2018, 41, 839–848. [Google Scholar] [CrossRef]
- Smyczyńska, U.; Smyczyńska, J.; Hilczer, M.; Stawerska, R.; Tadeusiewicz, R.; Lewiński, A. Pre-treatment growth and IGF-I deficiency as main predictors of response to growth hormone therapy in neural models. Endocr. Connect. 2018, 7, 239–249. [Google Scholar] [CrossRef]
- Carel, J.C.; Ecosse, E.; Nicolino, M.; Tauber, M.; Leger, J.; Cabrol, S.; Bastie-Sigeac, I.; Chaussain, J.L.; Coste, J. Adult height after long term treatment with recombinant growth hormone for idiopathic isolated growth hormone deficiency: observational follow up study of the French population based registry. BMJ 2002, 325, 70. [Google Scholar] [CrossRef] [PubMed]
- de Ridder, M.A.J.; Stijnen, T.; Hokken-Koelega, A.C.S. Prediction of adult height in growth-hormone-treated children with growth hormone deficiency. J. Clin. Endocrinol. Metab. 2007, 92, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Ranke, M.B.; Lindberg, A.; Martin, D.D.; Bakker, B.; Wilton, P.; Albertsson-Wikland, K.; Cowell, C.T.; Price, D.A.; Reiter, E.O.; Kabi Intl Growth Study Pfizer, I. The mathematical model for total pubertal growth in idiopathic growth hormone (GH) deficiency suggests a moderate role of GH dose. J. Clin. Endocrinol. Metab. 2003, 88, 4748–4753. [Google Scholar] [CrossRef] [PubMed]
- Lonero A, Giotta M, Guerrini G, Calcaterra V, Galazzi E, Iughetti L, Cassio A, Wasniewska GM, Mameli C, Tornese G, Salerno M, Cherubini V, Caruso Nicoletti M, Street ME, Grandone A, Giacomozzi C, Faienza MF, Guzzetti C, Bellone S, Parpagnoli M, Musolino G, Maggio MC, Bozzola M, Trerotoli P, Delvecchio M; Study Group on Physiopathology of growth processes of ISPED. Isolated childhood growth hormone deficiency: a 30-year experience on final height and a new prediction model. J. Endocrinol. Invest 2022, 45, 1709–1717. [CrossRef] [PubMed]
- Brettell, E.; Högler, W.; Woolley, R.; Cummins, C.; Mathers, J.; Oppong, R.; Roy, L.; Khan, A.; Hunt, C.; Dattani, M. The Growth Hormone Deficiency (GHD) Reversal Trial: effect on final height of discontinuation versus continuation of growth hormone treatment in pubertal children with isolated GHD—a non-inferiority Randomised Controlled Trial (RCT). Trials 2023, 24, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hilczer, M.; Smyczyńska, J.; Lewiński, A. Limitations of clinical utility of growth hormone stimulating tests in diagnosing children with short stature. Endocr. Regul. 2006, 40, 69–75. [Google Scholar] [PubMed]
- Kamoun, C.; Hawkes, C.P.; Grimberg, A. Provocative growth hormone testing in children: how did we get here and where do we go now? J. Pediatr. Endocrinol. Metab. 2021, 34, 679–696. [Google Scholar] [CrossRef] [PubMed]
- Partenope, C.; Galazzi, E.; Albanese, A.; Bellone, S.; Rabbone, I.; Persani, L. Sex steroid priming in short stature children unresponsive to GH stimulation tests: Why, who, when and how. Front. Endocrinol. (Lausanne). 2022, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Binder, G.; Reinehr, T.; Ibáñez, L.; Thiele, S.; Linglart, A.; Woelfle, J.; Saenger, P.; Bettendorf, M.; Zachurzok, A.; Gohlke, B.; et al. GHD Diagnostics in Europe and the US: An Audit of National Guidelines and Practice. Horm. Res. Paediatr. 2020, 92, 150–156. [Google Scholar] [CrossRef]
- Rapaport, R.; Wit, J.M.; Savage, M.O. Growth failure: ‘Idiopathic’ only after a detailed diagnostic evaluation. Endocr. Connect. 2021, 10, R125–R138. [Google Scholar] [CrossRef]
- Greulich, W.W.; Pyle, S.I. Radiographic Atlas of Skeletal Development of the Hand and Wrist, 2nd ed.; Stanford University Press: Stanford, 1993; pp. 1–272. [Google Scholar]
- Felício, J.S.; Janaú, L.C.; Moraes, M.A.; Zahalan, N.A.; de Souza Resende, F.; de Lemos, M.N.; de Souza Neto, N.J.K.; Farias de Franco, I.I.; Leitão, L.T.C.; Silva, L. de S. d. A.; et al. Diagnosis of Idiopathic GHD in Children Based on Response to rhGH Treatment: The Importance of GH Provocative Tests and IGF-1. Front. Endocrinol. (Lausanne). 2019, 10, 1–9. [CrossRef] [PubMed]
- Guzzetti, C.; Ibba, A.; Pilia, S.; Beltrami, N.; Di Iorgi, N.; Rollo, A.; Fratangeli, N.; Radetti, G.; Zucchini, S.; Maghnie, M.; et al. Cut-off limits of the peak GH response to stimulation tests for the diagnosis of GH deficiency in children and adolescents: Study in patients with organic GHD. Eur. J. Endocrinol. 2016, 175, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Siemens Healthcare Diagnostics Inc. Introducing the Restandardized Insulin-Like Growth Factor-I (IGF-I) Assay. Cust. Bull. 2016, 5.
- Chanson, P.; Arnoux, A.; Mavromati, M.; Brailly-Tabard, S.; Massart, C.; Young, J.; Piketty, M.L.; Souberbielle, J.C. Reference values for IGF-I serum concentrations: Comparison of six immunoassays. J. Clin. Endocrinol. Metab. 2016, 101, 3450–3458. [Google Scholar] [CrossRef] [PubMed]
- Aneke-Nash, C.S.; Dominguez-Islas, C.; Bůžková, P.; Qi, Q.; Xue, X.; Pollak, M.; Strickler, H.D.; Kaplan, R.C. Agreement between circulating IGF-I, IGFBP-1 and IGFBP-3 levels measured by current assays versus unavailable assays previously used in epidemiological studies. Growth Horm. IGF Res. 2016, 26, 11–16. [Google Scholar] [CrossRef]
- Blum, W.F.; Schweizer, R. Insulin-like growth factors and their binding proteins. In Diagnostics of Endocrine Function in Children and Adolescents; Ranke, M.B., Ed.; Karger, Basel, 2003; pp. 166–169.
- Elmlinger, M.W.; Kühnel, W.; Weber, M.M.; Ranke, M.B. Reference ranges for two automated chemiluminescent assays for serum insulin-like growth factor I (IGF-I) and IGF-binding protein 3 (IGFBP-3). Clin. Chem. Lab. Med. 2004, 42, 654–664. [Google Scholar] [CrossRef]
Figure 1.
Comparisons of GH peak (a), IGF-1 SDS (b) and height SDS (c) at diagnosis and during retesting in the groups PRE and POST; all values are presented as median (point), interquartile range (box) and non-outlier range (whiskers); differences significant (p<0.001) in Wilcoxon test are marked with * and #.
Figure 1.
Comparisons of GH peak (a), IGF-1 SDS (b) and height SDS (c) at diagnosis and during retesting in the groups PRE and POST; all values are presented as median (point), interquartile range (box) and non-outlier range (whiskers); differences significant (p<0.001) in Wilcoxon test are marked with * and #.
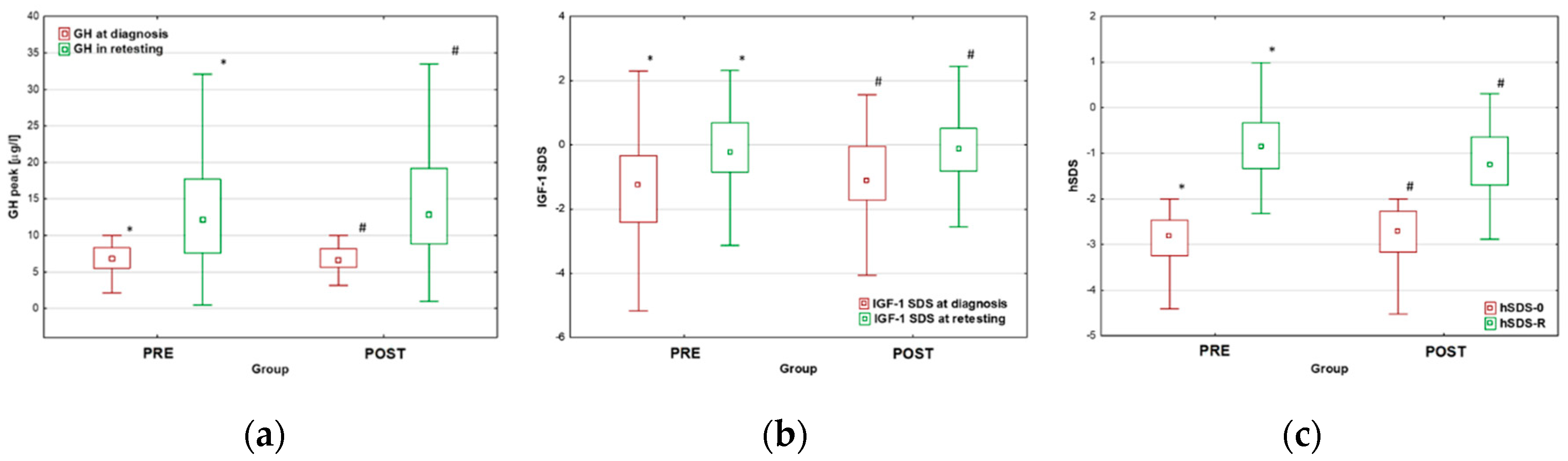
Figure 2.
Comparisons of GH peak (Fig. 1A), IGF-1 SDS (Fig. 1B) and hSDS (Fig. 1C) at diagnosis and during retesting between the groups with “Unlikely, “Doubtful” and “True” GHD; all values are presented as median (point), interquartile range (box) and non-outlier range (whiskers); differences significant (p<0.001) in Wilcoxon test are marked with *, # and x.
Figure 2.
Comparisons of GH peak (Fig. 1A), IGF-1 SDS (Fig. 1B) and hSDS (Fig. 1C) at diagnosis and during retesting between the groups with “Unlikely, “Doubtful” and “True” GHD; all values are presented as median (point), interquartile range (box) and non-outlier range (whiskers); differences significant (p<0.001) in Wilcoxon test are marked with *, # and x.
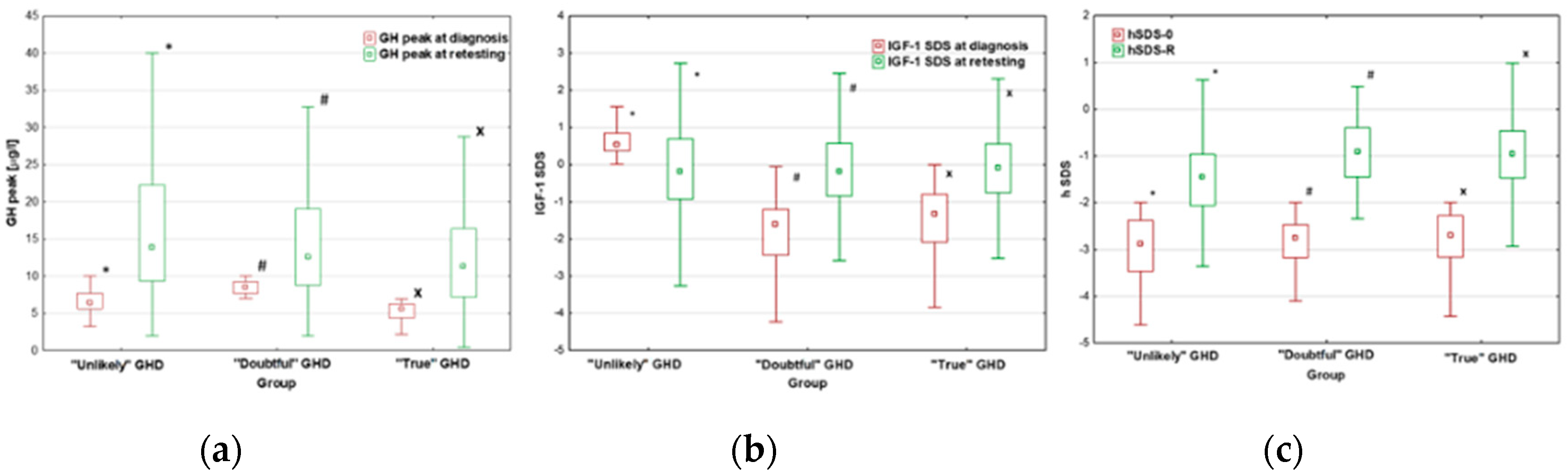

Table 1.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients who completed GH therapy before (Group PRE) or after (Group POST) the attainment of near-FH.
Table 1.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients who completed GH therapy before (Group PRE) or after (Group POST) the attainment of near-FH.
| All | Group PRE | Group POST | p | |
|---|---|---|---|---|
| N (boys/girls)* | 260 (173/87) | 121 (92/29) | 139 (81/58) | |
| Age at therapy onset [years] Age at retesting [years] Therapy duration [years] |
13.2 (11.9-14.4) 17.6 (16.5;18.3) 4.2 (3.4;5.2) |
13.7 (12.4;14.7) 17.6 (16.8;18.3) 3.9 (2.9;4.7) |
12.7 (11.5;14.0) 17.6 (16.4;18.3) 4.5 (3.8;5.6) |
0.001 0.985 <0.001 |
| GH peak at diagnosis [µg/l] GH peak in retesting [µg/l] Δ GH peak [µg/l] |
6.80 (5.58-8.23) 12.40 (7.98;18.45) 7.54 (1.25;11.29) |
6.86 (5.51;8.30) 12.20 (7.57;17.70) 7.22 (0.90;10.70) |
7.22 (0.90;10.70) 12.80 (8.84;19.20) 7.82 (1.81;11.95) |
0.960 0.262 0.328 |
| IGF-1 SDS at diagnosis IGF-1 SDS at retesting Δ IGF-1 SDS |
-1.23 (-1.94;-0.18) -0.18 (-0.81;0.58) 0.99 (0.04;2.11) |
-1.26 (-2.42;-0.33) -0.23 (-0.84;0.69) 1.30 (0.17;2,65) |
-1.12 (-1.72;-0.05) -0.13 (-0.82;0.51) 1.04 (0.17;1,91) |
0.135 0.879 0.209 |
| hSDS-0 TH SDS corr hSDS-0 hSDS-R corr hSDS-R Δ hSDS |
-2.76 (-3.20;-2.43) -1.08 (-1.58;-0.50) -1.70 (-2.31;-1.12) -1.02 (-1.54;-0.52) -0.01 (-0.59;0.57) 1.74 (1.29;2.28) |
-2.81 (-3.26;-2.47) -0.92 (-1.41;-0.46) -1.89 (-2.42;-1.43) -0.86 (-1.33;-0.33) 0.09 (-0.52;0.62) 2.01 (1.56;2.56) |
-2.71 (-3.17;-2.27) -1.21 (-1.70;-0.58) -1.58 (-2.19;-0.99) -1.26 (-1.70;-0.64) -0.01 (-0.60;0.57) 1.58 (1.01;2.06) |
0.166 0.029 0.010 <0.001 0.024 <0.001 |
* Values except for the number of patients are expressed as medians and interquartile range (25 centile;75 centile); p-values reported in the right column, concerning the differences between Groups PRE and POST, were calculated with U Mann-Whitney test.
Table 2.
Number of patients with normal and subnormal GH peak in retesting according to cut-off values for persistent severe GHD, for transition period and for childhood in particular groups of patients with respect to the moment of therapy withdrawal.
Table 2.
Number of patients with normal and subnormal GH peak in retesting according to cut-off values for persistent severe GHD, for transition period and for childhood in particular groups of patients with respect to the moment of therapy withdrawal.
| GH peak [µg/l] | All (n=260) | Group PRE (n=121) | Group POST (n=139) |
|---|---|---|---|
|
<3.0 3.0-6.0 6.0-10.0 |
10 (3.85%) 24 (9.23%) 58 (22.31%) |
9 (7.44%) 12 (9.91%) 97 (19.83%) |
1 (0.72%) 12 (8.63%) 34 (24.46%) |
| >10.0 | 168 (64.61%) | 76 (62.81%) | 92 (66.19%) |
Table 3.
Number of boys and girls with normal and subnormal GH peak in retesting according to cut-off values for persistent severe GHD, for transition period and for childhood.
Table 3.
Number of boys and girls with normal and subnormal GH peak in retesting according to cut-off values for persistent severe GHD, for transition period and for childhood.
| GH peak [µg/l] | Boys (n=173) | Girls (n=87) |
|---|---|---|
|
<3.0 3.0-6.0 6.0-10.0 |
7 (4.05%) 13 (7.51%) 29 (16.76%) |
3 (3.45%) 11 (12.65%) 29 (33.33%) |
| >10.0 | 124 (71.68%*) | 92 (66.19%*) |
* significant (p=0.008) difference between boys and girls
Table 4.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting in boys and girls.
Table 4.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting in boys and girls.
| Boys | Girls | p | |
| N (%)* | 173 (66.5%) | 87 (33.5%) | |
| Age at therapy onset [years] Age at retesting [years] Therapy duration [years] |
13.8 (12.6;14.8) 18.0 (17.5;18.7) 4.3 (3.4;5.3) |
11.9 (10.7;12.8) 16.1 (15.4;16.9) 4.1 (3.3;5.1) |
<0.001 <0.001 0.442 |
| GH peak at diagnosis [µg/l] GH peak in retesting [µg/l] Δ GH peak [µg/l] |
6.53 (5.28;8.20) 14.20 (8.91;19.30) 7.85 (2.60;12.20) |
7.20 (5.97;8.28) 10.20 (7.19;14.70) 2.96 (0.28;7.50) |
0.117 <0.001 <0.001 |
| IGF-1 SDS at diagnosis IGF-1 SDS at retesting Δ IGF-1 SDS |
-1.26 (-2.06;-0.24) -0.05 (-0.84;0.61) 1.23 (0.11;2.32) |
-1.05 (-1.80;-0.16) -0.34 (-0.79;0.42) 0.98 (-0.24;1.93) |
0.314 0.261 0.267 |
| hSDS-0 TH SDS corr hSDS-0 hSDS-R corr hSDS-R Δ hSDS |
-2.84 (-3.30;-2.49) -1.00 (-1.58;-0.50) -1.79 (-2.31;-1.18) -1.07 (-1.45;-0.46) 0.03 (-0.59;0.62) 1.81 (1.40;2.31) |
-2.65 (-3.12;-2.24) -1.08 (-1.67;-0.50) -1.62 (-2.32;-0.97) -0.98 (-1.66;-0.58) 0.00 (-0.58;0.47) 1.61 (1.15;2.09) |
0.519 0.910 0.330 0.519 0.640 0.020 |
* Values except for the number of patients are expressed as medians and interquartile range (25 centile;75 centile); p-values reported in the right column, concerning the differences between boys and girls, were calculated with U Mann-Whitney test.
Table 5.
Number of patients with normal and subnormal GH peak in retesting according to cut-off values for severe GHD in adulthood, for transition period and for childhood in particular groups of patients according to the recent criteria of GHRS [15].
Table 5.
Number of patients with normal and subnormal GH peak in retesting according to cut-off values for severe GHD in adulthood, for transition period and for childhood in particular groups of patients according to the recent criteria of GHRS [15].
|
Childhood Retesting |
“Unlikely” GHD (n=55) |
“Doubtful” GHD (n=96) |
“True” GHD (n=109) |
||||
| Boys (n=37) |
Girls (n=18) |
Boys (n=62) |
Girls (n=34) |
Boys (n=74) |
Girls (n=35) |
||
| transGHD (n=139) | 34 | 15 | 58 | 28 | 64 | 30 | |
|
childGHD (n=15) persistGHD (n=16) |
1 2 |
2 1 |
3 1 |
4 2 |
5 5 |
0 5 |
|
Table 6.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients with respect to the likelihood of GHD in childhood according to the current criteria [15].
Table 6.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients with respect to the likelihood of GHD in childhood according to the current criteria [15].
| “Unlikely” GHD | “Doubtful” GHD | “True” GHD | p | |
|---|---|---|---|---|
| N (boys/girls)* | 55 (37/18) | 96 (62/32) | 109 (74/35) | |
| Age at therapy onset [years] Age at retesting [years] Therapy duration [years] |
12.8 (11.3-14.7) 17.3 (16.3;18.5) 4.1 (2.9;5.7) |
13.2 (11.9;14.2) 17.5 (16.3;18.2) 4.1 (3.3;5.1) |
13.3 (12.0;14.5) 17.7 (17.1;18.4) 4.2 (3.6;5.1) |
0.001 0.985 <0.001 |
| GH peak at diagnosis [µg/l] GH peak in retesting [µg/l] Δ GH peak [µg/l] |
6.41 (5.60;7.70) 12.90 (9.30;22.30) 7.70 (3.50;16.00) |
8.52 (7.68;9.25) 12.60 (8.78;19.05) 4.20 (0.69;10.38) |
5.60 (4.40;6.28) 11.30 (7.17;16.40) 6.22 (1.11;11.19) |
<0.001 0.017 0.018 |
| IGF-1 SDS at diagnosis IGF-1 SDS at retesting Δ IGF-1 SDS |
0.54 (0.37;0.85) -0.41 (-0.93;0.69) -1.12 (-1.56;0.05) |
-1.60 (-2.43;-1.20) -0.19 (-0.85;0.57) 1.60 (0.61;2.78) |
-1.33 (-2.09;-0.80) -0.09 (-0.75;0.56) 1.50 (0.60;2.22) |
<0.001 0.991 <0.001 |
| hSDS-0 TH SDS corr hSDS-0 hSDS-R corr hSDS-R Δ hSDS |
-2.88 (-3.47;-2.38) -1.39 (-1.68;-0.75) -1.57 (-2.28;-0.99) -1.45 (-2.06;-0.96) -0.15 (-0,73;0.12) 1.41 (0.91;2.08) |
-2.76 (-3.18;-2.47) -0.92 (-1.51;-0.49) -1.86 (-2.39;-1.17) -0.91 (-1.45;-0.40) 0.12 (-0.62;0.78) 1.94 (1.48;2.30) |
-2.70 (-3.17;-2.28) -1.06 (-1.58;-0.50) -1.66 (-2.28;-1.03) -0.96 (-1.47;-0.46) 0.08 (-0.52;0.61) 1.69 (1.34;2.31) |
0.272 0.109 0.468 <0.001 0.020 0.010 |
* Values except for the number of patients are expressed as medians and interquartile range (25 centile;75 centile); p-values reported in the right column, concerning the differences between the groups with “True”, “Doubtful” and “unlikely” GHD, were calculated with Kruskall-Wallis ANOVA test.
Table 7.
Number of patients with persistent or non-transient and transient GHD peak in retesting in the Groups of patients divided according to the criteria including pre-test likelihood of GHD in childhood, proposed by Wit et al. [16]
Table 7.
Number of patients with persistent or non-transient and transient GHD peak in retesting in the Groups of patients divided according to the criteria including pre-test likelihood of GHD in childhood, proposed by Wit et al. [16]
|
Childhood Retesting |
“Pre-test unlikely” GHD (n=168) |
“Excluded” GHD (n=45) |
“Confirmed” GHD (n=47) |
||||
| Boys (n=110) |
Girls (n=58) |
Boys (n=62) |
Girls (n=32) |
Boys (n=74) |
Girls (n=35) |
||
| T-GHD (n=247) | 107 | 57 | 32 | 10 | 25 | 16 | |
|
NT-GHD (n=3) P-GHD (n=10) |
1 0 |
1 2 |
1 0 |
0 2 |
0 5 |
0 1 |
|
Table 8.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients with respect to the diagnosis including pre-test likelihood of GHD in childhood according to the criteria proposed by Wit et al. [16].
Table 8.
Pre-treatment characteristics, indices of GH therapy effectiveness and hormonal status at retesting of patients with respect to the diagnosis including pre-test likelihood of GHD in childhood according to the criteria proposed by Wit et al. [16].
| “Pre-test Unlikely” GHD | “Excluded” GHD | “Confirmed” GHD | p | |
| N (boys/girls)* | 168 (110/58) | 45 (33/12) | 47 (30/17) | |
| Age at therapy onset [years] Age at retesting [years] Therapy duration [years] |
12.8 (11.6;14.2) 17.4 (16.4;18.4) 4.3 (3.4;5.4) |
13.7 (12.7;14.4) 17.8 (17.0;18.2) 4.1 (3.4;4.6) |
13.7 (12.1;14.8) 17.7 (17.0;18.3) 4.0 (3.4;5.1) |
0.471 0.233 0.425 |
| GH peak at diagnosis [µg/l] GH peak in retesting [µg/l] Δ GH peak [µg/l] |
6.75 (5.63;8.09) 13.90 (9.06;20.15) 7.38 (2.33;13.18) |
8.69 (7.60;9.38) 12.40 (8.37;17.80) 3.72 (-0.68;8.57) |
4.84 (3.73;5.97) 8.40 (4.06;13.00) 4.03 (0.62;8.10) |
<0.001 0.017 0.018 |
| IGF-1 SDS for CA at diagnosis IGF-1 SDS for BA at diagnosis IGF-1 SDS for CA at retesting Δ IGF-1 SDS for CA |
-0.59 (-1.24;0.35) 0.14 (-0.48;0.78) 0.04 (-0.58;0.69) 0.52 (-0.69;1.55) |
-2.45 (-3.03;-1.91) -1.73 (-2.42;1.27) -0.46 (-1.04;0.33) 2.15 (1.34;3.29) |
-2.48 (-3.30;-1.64) -1.52 (-2.35;1.23) -0.46 (-0.95;0.56) 2.06 (0.87;3.07) |
<0.001 <0.001 0.069 <0.001 |
| hSDS-0 TH SDS corr hSDS-0 hSDS-R corr hSDS-R Δ hSDS |
-2.71 (-3.17;-2.38) -1.08 (-1.67;-0.50) -1.65 (-2.31;-1.13) -1.18 (-1.66;-1.04) -0.04 (-0,63;0.36) 1.58 (1.13;2.14) |
-2.81 (-3.32;-2.53) -1.08 (-1.57;-0.58) -1.76 (-2.27;-1.14) -0.79 (-1.34;-0.21) 0.37 (-0.22;0.88) 2.12 (1.73;2.51)) |
-2.84 (-3.24;-2.28) -1.07 (-1.58;-0.33) -1.78 (-2.35;-0.97) -0.76 (-1.42;-0.29) 0.12 (-0.59;0.70) 2.02 (1.46;2.66) |
0.425 0.685 0.964 0.011 0.009 <0.001 |
* Values except for the number of patients are expressed as medians and interquartile range (25 centile;75 centile); p-values reported in right column, concerning the differences between the Groups, were calculated with Kruskall-Wallis ANOVA test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



