
Submitted:
02 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
Abstract: Background: Irreversible electroporation (IRE) is a form of non-thermal ablation that delivers pulses of high voltage electrical current between electrodes. The role of IRE in the treatment of colorectal hepatic metastases is unestablished. This study is an international ques-tionnaire survey of the use of IRE for colorectal hepatic metastases. Methods: A questionnaire addressing views on the use of IRE for colorectal liver metastases was circulated to clinicians with an interest and/or expertise in this technique. Results: 64 clinicians from 17 different countries replied to the questionnaire. Thirty-six (56%) had experience of treating patients with colorectal liver metastases with IRE. The preferred mode of delivery of IRE was percutaneous treatment under CT guidance. Thirty-three (70% respondents) used IRE exclusively for lesions in proximity to inflow or outflow structures. Twenty (43% respondents) used IRE as their sole ablative treat-ment whilst 19 (40% respondents) used IRE in combination with thermal ablation. The maximum number of lesions that could be treated by IRE was two and preferred size of lesion was
Keywords:
colorectal cancer
; liver metastases
; ablation
; irreversible electroporation
; survey.
1. Introduction
Approximately one fifth of patients with colorectal cancer have metastases either predominantly or exclusively in the liver [1,2]. Treatment typically comprises a combination of systemic chemotherapy and surgery directed at removal of disease at both the primary and metastatic sites with radiotherapy also being integrated into management for selected patients with rectal primary tumours [3,4]. Resection of liver tumours to clear the hepatic metastatic burden improves survival [5,6].
Ablation of liver metastases is an effective and acceptable alternative treatment to resection [7,8]. Thermal ablative techniques include microwave and radiofrequency energy [7,8,9,10]. Thermal ablation of liver metastases is less effective in the vicinity of major blood vessels because of conductive loss, termed the heatsink effect. Thermal ablation close to inflow structures can also be associated with biliary injury [10]. These restrictions limit the use of thermal ablation.
Irreversible electroporation (IRE) is a form of non-thermal ablation that consists of the delivery of pulses of electrical current of high voltage between electrodes [11]. The technique induces sustained depolarisation of cell membranes forming nanopores that lead to dysregulation of cellular homeostasis causing cell death within an ablation zone between these electrodes [11]. An initial study (COLDFIRE-1) established that IRE applied two hours prior to resection was associated with necrosis of liver metastases of colorectal cancer origin [12]. A phase II study (COLDFIRE-2) showed in a series of 51 patients with colorectal liver metastases of 5.0 cm or smaller that IRE was successful in 50 (98%) with local control at 12 months in 74% [13]. In COLDFIRE-2 patients had received a heterogeneous range of interventions before and after IRE.
The current place of IRE in the portfolio of treatments for colorectal hepatic metastases is not established [14,15]. The aim of this study is to conduct a questionnaire survey of clinicians with experience of (and/or interest in) the use of IRE for colorectal hepatic metastases to obtain an overview of opinion on indications, technique and assessment of follow up. This questionnaire survey takes the form of a focus-group interview of clinicians participating in a symposium on irreversible electroporation and specifically addresses the use of IRE for the treatment of colorectal liver metastases.
2. Methods
2.1. Design
This study took the form of a focus-group questionnaire survey of clinicians with experience of (and/or interest in) the use of IRE for the ablation of colorectal hepatic metastases.
2.2. Questionnaire Design and Content
The questionnaire addressed clinicians’ demographics, specialty and experience with IRE for colorectal hepatic metastases. In relation to colorectal hepatic metastases information was sought on physical characteristics of lesions for IRE (size, number), location (proximity to inflow/outflow structures), setting (intact liver, IRE as adjunct to resection, IRE as salvage after prior hepatectomy) and method of use (percutaneous or open, computed tomographic [CT]). Finally, information was sought from participants on the feasibility of participation in future Phase II and III studies. The questionnaire is seen in Appendix A.
2.3. Target Populations
Two overlapping populations were targeted. The first population was clinicians attending the Angiodynamics “Life Through Technology” Symposium on 24th-26th November 2022. The second population was identified by Angiodynamics, Inc. as clinicians whose institutions had purchased NanoKnife (irreversible electroporation; Angiodynamics Inc; New York, New York, USA) in the preceding five years.
2.4. Circulation of Questionnaire
The questionnaire was distributed electronically to participants after the closure of the “Life Through Technology” event. The surveyMonkey online survey (https://www.surveymonkey.co.uk) was used to collect and collate responses. A reminder was sent four weeks after the original circulation. This was a closed survey, open to participants at the symposium, with initial contact and advertising made while a presentation on future evaluation of IRE for colorectal liver metastases. A QR code with access to the survey was provided and delegates were subsequently sent an email inviting them to participate. No financial or other incentives were provided to potential respondents. The survey was closed 16 weeks after the “Life Through Technology” event.
2.5. Collation of Results
Results are reported on clinicians’ primary specialty, the number of patients with colorectal liver metastases seen in their multidisciplinary team meetings and their reported experience with IRE.
Figures are used to show the choice of treatment selected, first in the setting of liver-limited disease in a patient with good performance status and then for the same disease distribution in a patient with a performance status which precludes surgery.
Figures are also used to show answers to questions on resection combined with ablation and the role of ablation in the scenario of liver-limited recurrence after prior hepatectomy.
Data are presented on technical aspects of IRE including preferred choice of approach, number and size of lesions treatable by IRE, method and timing of assessment of lesion response.
2.6. Statistical Analysis
All statistical analyses were performed with R version 3.6.1 (https://www.r-project.org/). The chi-squared test of independence was used to assess the relationship between clinician specialty and the number and size of liver metastases that could be treated with IRE. A two-sided significance level p value of less than 0·05 was regarded as significant.
2.7. Ethics
The NHS Health Research Authority website was consulted on whether or not this study required ethics committee review (http://www.hra-decisiontools.org.uk/research/ accessed 24th November 2022).
As no patients were involved in this study, no treatments were allocated according to the study and the results are not immediately generalisable, the verdict of the decision tool was that ethics committee review was not required.
Informed consent was not obtained from participating clinicians. The decision to participate or not was entirely voluntary. Data are anonymized for analysis and no individualized data are used.
2.8. Role of the Manufacturer in the Study
The first cohort of clinicians for this study was sourced from delegates attending an international scientific conference hosted by the manufacturer and the second cohort of names was provided directly by the manufacturer. The manufacturer had no role in the concept, design or execution of the study and no influence on reporting of the results or on the writing of this manuscript.
3. Results
Sixty-four clinicians from 17 different countries replied to the questionnaire. Note that the denominator for each individual question is different and varies according to number of responses.
3.1. Specialty of Respondents and Exposure to Patients with Colorectal Liver Metastases (Figure 1A,B)
Forty-one (64%) gave their specialty as hepatobiliary and pancreatic surgery with a further 9 (14%) giving General Surgery as their specialty (see Figure 1A). Fourteen (22%) gave their specialty as interventional radiology. Two (3%) respondents gave surgical oncology as an additional sub-specialty.
Sixty-one (95%) stated that they treated patients with hepatic metastases from colorectal cancer with 58 (91%) being a member of a multi-disciplinary team (MDT)/ tumour board for patients with colorectal liver metastases. The number of patients with colorectal hepatic metastases seen at participants’ MDT/tumour boards per annum is seen in Figure 1B with 42 (66% of respondents) seeing more than 51.
3.2. Reported Experience with Irreversible Electroporation for Colorectal Hepatic Metastases (Figure 1C)
Thirty-six (56%) had experience of treating patients with colorectal liver metastases with IRE with the distribution of reported experience seen in Figure 1C. Four (6%) had treated more than 50 patients with IRE for colorectal hepatic metastases and one (2%) more than 100 patients.
3.3. Treatment Options in Specific Scenarios
The treatment responses to four clinical scenarios are seen below. For each scenario more than one choice was permitted.
i) Figure 2A: Preferred treatment in the setting of patients with up to four surgically resectable, bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all <4cm in size, away from liver inflow/outflow structures in the setting of good performance status and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1).
The responses are seen in Figure 2A. There were 61 respondents to this question. The preferred choice was surgical resection (either as a single or staged procedure) stated by 41 (67%). The second preferred choice was a combination of resection together with microwave ablation stated by 31 (51%) and the third most popular response was microwave ablation alone (as part of a single or staged procedure), selected by 18 (30%). IRE as sole treatment was selected by 3 (5%) respondents and resection combined with IRE (± thermal ablation) by 4 (7%). Other choices are seen in Figure 2A and include continuance of maintenance chemotherapy 3 (5%), and intra-arterial chemotherapy 1 (2%).
ii) Figure 2B: Preferred treatment for patients with up to four bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all < 4cm in size, away from liver inflow/outflow in the setting of a performance status which precludes surgery and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1).
The disease distribution is identical to that in the previous question with the sole difference being the performance status. There were 61 respondents to this question.
The first choice in this setting was microwave ablation which was selected by 48 (79%). Second was radiofrequency ablation, selected by 14 (23%) and third was continuance with maintenance chemotherapy, selected by 8 (13%). IRE as sole treatment was selected by 7 (12%) and combined with thermal ablation by 5 (8%). Other responses are seen in Figure 2B.
iii) Figure 3A: Preferred treatment for the patient with bi-lobar hepatic metastases that are not resectable in a single operation (four lesions in total - M1a) all < 4 cm in size, prior systemic chemotherapy, good performance status and with lesions resectable by right hepatectomy leaving two lesions in the left hemi-liver.
There were 59 respondents to this question. Resection combined with thermal ablation for the lesions in the contralateral hemi-liver was the most popular choice, being selected by 33 (56%). Second was modification of the future remnant liver by right portal vein embolization (PVE) to permit subsequent resection of all metastases, selected by 32 (54%), and third was two-stage hepatectomy, selected by 22 (37%). Resection combined with IRE for lesions close to either biliary inflow or hepatic vein outflow was selected by 14 (24%).
iv) Figure 3B: Preferred treatment for the patient with up to two liver-limited hepatic recurrent metastases (both < 4cm in size, one close to inflow), eighteen months after prior right hepatectomy.
There were 59 respondents to this question. Re-do hepatectomy and second line systemic chemotherapy were equal first choice with 13 (22.0%) selecting these. Re-do hepatectomy combined with IRE or IRE plus thermal ablation was selected by 7 (12%) and 4 (7%) respectively (Figure 3B). “Other” was selected by 13 respondents (22%) and consisted of combinations of systemic chemotherapy followed by IRE alone, microwave ablation of lesions away from inflow/outflow with IRE for lesions close, and one suggesting local therapy with adjuvant hepatic intra-arterial chemotherapy.
3.4. Mode of Delivery of IRE (Table 1)
There were 47 respondents to this question. The preferred mode of deliver of IRE was percutaneous treatment under CT guidance, selected by 33 (70%). Thirty-three (70%) used IRE exclusively for lesions in proximity to inflow or outflow structures. Twenty (43%) used IRE as their sole ablative treatment whilst 19 (40%) used IRE in combination with thermal ablation.
3.5. Number and Size of Lesions Treatable by IRE (Figure 4A,B)
There were 46 respondents to this question. The most frequently selected maximum number of lesions that could be treated by IRE was two (17 respondents; 37%) Figure 4A). Five (11%) respondents replied that they would use IRE in more than four lesions.
No respondents stated that they would use IRE for lesions greater than 5 cm in size (4B) and 23 (55% of 42 respondents to this question) stated that they would use IRE for lesions <3 cm in size (Figure 4B). There was no difference in respondent speciality between surgeons and radiologists in the number of lesions deemed safe to be ablated in one session, X2 (4, 40) =1.2967, p=.86. There was no relationship between respondent specialty and the maximum size of lesion deemed treatable with IRE, X2 (2, 40) =0.0889, p=.96.
3.6. Mode and Timing of Assessment of Response to IRE (Figure 4C,D):
There were 45 respondents to this question. Fourteen (31%) routinely undertake a CT scan 24h after IRE and prior to discharge of the patient from hospital. CT as a sole modality was the preferred modality of imaging for assessment of response for 27 (60%) compared to 19 (42%) favouring MR alone. Optimum time for assessment of response (40 respondents to this question) was stated as 3 months by 20 (50%) and 6 weeks by 19 (48%).
3.7. Feasibility and Design of Future Randomized Controlled Trial of IRE
There were 54 respondents to this question. Thirty-eight (71%) thought that there should be a randomized trial to evaluate IRE in the treatment of colorectal liver metastases. Of the 14 respondents who indicated that there should not be a randomized trial, 9 (64% of those responding in this way) stated that their response was because IRE was already an established treatment for colorectal hepatic metastases and 3 (21%) stated that IRE has no role in the treatment of liver metastases from colorectal cancer. Of those who replied affirmatively (40 respondents), 24 (60% of those responding in this way) stated that the comparator treatment should be thermal ablation whilst 15 (38%) thought that the comparator treatment should be liver resection.
4. Discussion
This is thought to be the first international questionnaire survey of the use of irreversible electroporation for treatment of patients with colorectal liver metastases.
Before considering the results, important sources of bias must be considered. First, the study population is small and selected from a group of clinicians with a likely interest in IRE and thus affected by sampling bias [16]. Second, the predominance of surgeons may create bias towards surgical treatment options. In addition, other important types of bias include potential response bias – it is impossible to verify if the responders’ answers are representative of their actual clinical practice and lastly acquiescence bias where responders may have favoured a more positive response to questions about IRE than would be their standard practice as this was a questionnaire on this topic.
These types of bias are inherent in the majority of questionnaire surveys and if these data are interpreted with these limitations in mind, the results provide important insights.
This is a unique survey undertaken at a time where equipoise exists in relation to indications for use, assessment of outcome and potential comparator treatments for IRE [15]. Considering the four clinical scenarios, surgical resection either alone or in combination with thermal ablation would be expected to be the favoured response in the setting of a patient with resectable liver metastases [17,18]. Similarly, it would be expected that thermal ablation and maintenance chemotherapy would be the preferred responses in the setting of a patient with non-resectable disease. The third scenario of a patient with potentially resectable disease but insufficient reserve would lend itself to modification of the future remnant liver as would repeat hepatectomy for a patient with late liver-limited recurrence in the fourth scenario [19,20]. IRE is not a preferred treatment in any of these scenarios.
The questions on the use of IRE yielded interesting answers. Despite the IRE consensus recommending that CT be undertaken prior to discharge, this was only done by 31% of respondents [21]. Although the most frequently selected reply to number of lesions suitable for treatment was two, there were respondents who selected patients with more lesions than this as suitable for IRE. The majority agreed that IRE should be restricted to lesions < 3 cm in size. Follow-up imaging modalities were almost equally divided between MR and CT as was the time of intervention between 6 weeks and 3 months.
The clear preference in terms of route and imaging modality was a percutaneous route under CT guidance.
It seems clear that the landscape on management of liver metastases from colorectal cancer will change in favour of ablation with the longstanding evidence from the EORTC 40004 study being reinforced by the outcomes of the MAVERRIC trial [22,23].
Yet, the route to further evaluation of this technique remains unclear and this is reflected in the responses with 71% of respondents favouring a randomized trial but some stating that it is already established practice and yet others reporting that it has no role in the treatment of colorectal hepatic metastases.
5. Conclusions
In summary, this international questionnaire survey is an important “snapshot” perspective of current views on irreversible electroporation for colorectal hepatic metastases. Although IRE may prove to be a valuable tool in the armamentarium for treatment of individuals with liver-limited or liver-dominant metastases, this study highlights the limits of current evidence and the pressing need for further well-designed clinical evaluation of this technique
Author Contributions
HVM Spiers: Conceptualization, Methodology, validation, data curation, writing original draft, writing – review and editing; S Jamdar: data curation, writing original draft, writing – review and editing; S Jegatheeswaran: Methodology, data curation, writing original draft, writing – review and editing; N de Liguori Carino: data curation, writing original draft, writing – review and editing; P Stathakis: writing original draft, writing – review and editing; V Nadarajah: writing original draft, writing – review and editing; KV Menon: data curation, writing original draft, writing – review and editing; S Pandanaboyana: data curation, writing original draft, writing – review and editing; AE Frampton: data curation, writing original draft, writing – review and editing; TM Wah: Methodology, data curation, writing original draft, writing – review and editing; S Farid: writing original draft, writing – review and editing; HZ Malik: writing original draft, writing – review and editing; R Jones: Methodology, data curation, writing original draft, writing – review and editing; J Evans: writing original draft, writing – review and editing; A K Siriwardena: Conceptualization, methodology, data curation, writing original draft, writing – review and editing; individual with responsibility for integrity of final report. All authors have read and agreed to the published version of the manuscript.”.
Funding
“This research received no external funding”.
Institutional Review Board Statement
The NHS Health Research Authority website was consulted on whether this study required ethics committee review (http://www.hra-decisiontools.org.uk/research/ accessed 24th November 2022). As no patients were involved in this study, no treatments were allocated according to the study and the results are not immediately generalisable, the verdict of the decision tool was that ethics committee review was not required.
Informed Consent Statement
This study did not involve patients and written informed consent is not applicable.
Data Availability Statement
The data for this study – the results of the questionnaire – are available from the principal author on reasonable written request.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Questionnaire survey of the use of IRE for ablation of colorectal hepatic metastases
Question 1:What is your specialty?
- a)
- Interventional radiology
- b)
- General Radiology
- c)
- Hepatobiliary and Pancreatic Surgery
- d)
- Pancreatic Surgery
- e)
- Oncology
- f)
- Other (Please specify)
- g)
- None of the above.
Question 2: This question is about your practice setting
- a)
- Do you treat patients with liver metastases from colorectal cancer?
- b)
- Are you a member of a multidisciplinary team/tumour board for patients with this condition?
Please answer only one of the three questions below, according to your clinical practice:
- c)
- Please select the approximate number of patients with colorectal hepatic metastases that your MDT reviews per year:
Option 1: 1- 10
Option 2: 11-30
Option 3: 31 – 50.
Option 4 >51
- d)
- How many patients with colorectal hepatic metastases have you treated with liver IRE to date
0
1-10
11-20
21-30
31-50
51-100
More than 100.
If the answers to both the first two questions are “NO” there is no need to answer any further questions. Thank you very much for your time.
Question 3: Your preferred treatment for patients with up to four surgically resectable, bi-lobar liver-limited colorectal hepatic metastases (M1a), all < 4 cm in size, away from inflow/outflow in the setting of good performance status and treated by prior systemic chemotherapy, stable disease on RECIST 1.1
- a)
- Hepatic resection (single or staged hepatectomy).
- b)
- Radiofrequency ablation (single or staged procedure)
- c)
- Microwave ablation (single or staged procedure)
- d)
- Irreversible electroporation (single or staged procedure)
- e)
- Irreversible electroporation combined with surgery
- f)
- Irreversible electroporation combined with thermal ablation
- g)
- Intra-arterial infusion of 90Yttrium
- h)
- Intra-arterial chemotherapy
- i)
- Maintenance chemotherapy
- j)
- No intervention
- k)
- Other (Please specify)
Question 4: Your preferred treatment for patients with up to four liver metastases (M1a), all < 4 cm in size, away from inflow/outflow, but a performance status which precludes resection and treated by prior systemic chemotherapy
- a)
- Radiofrequency ablation (single or staged procedure)
- b)
- Microwave ablation (single or staged procedure)
- c)
- Irreversible electroporation
- d)
- Irreversible electroporation combined with thermal ablation
- e)
- Stereotactic ablative radiotherapy (SABR)
- f)
- Intra-arterial infusion of 90Yttrium
- g)
- Intra-arterial chemotherapy
- h)
- Maintenance chemotherapy
- i)
- Another combination of above interventions
- j)
- No intervention
- k)
- Other (Please specify)
Question 5: What is your preferred treatment for the patient with bi-lobar hepatic metastases that are not resectable in a single operation (four lesions in total, [M1a], all < 4 cm in size) prior systemic chemotherapy, good performance status and with lesions resectable by right hepatectomy leaving two lesions in the left hemi-liver.
- a)
- Right portal vein embolisation to facilitate right hepatectomy plus metastasectomy.
- b)
- Two-stage hepatectomy.
- c)
- ALPPS.
- d)
- Resection combined with thermal ablation
- e)
- Resection combined with Irreversible electroporation
- f)
- Resection combined with irreversible electroporation if lesion close to biliary structure or remnant outflow and thermal ablation for remnant lesion.
- g)
- Resection followed by SABR to left lobe remnant lesions.
- h)
- Resection followed by observation of left lobe lesions.
- i)
- Other (please specify).
Question 6: What is your preferred treatment for the patient with up to two liver-limited hepatic recurrent metastases (both <4 cm in size, one close to inflow) 18 months after prior liver resection (right hepatectomy).
- a)
- Systemic chemotherapy.
- b)
- Re-do hepatectomy
- c)
- Re-do hepatectomy combined with thermal ablation
- d)
- Re-do hepatectomy combined with irreversible electroporation
- e)
- SABR
- f)
- Other (please specify)
Question 7:These questions focus on irreversible electroporation. Compliant with the IRE consensus for patient fitness and with cardiac cycle synchronisation, What is your preferred method of delivery of IRE?
- a)
- Percutaneous with ultrasound guidance.
- b)
- Open surgery with ultrasound guidance.
- c)
- Percutaneous with CT guidance.
- d)
- Open surgery with CT guidance
Question 8: Use of IRE within the liver.
- a)
- Do you use IRE solely for lesions close to biliary inflow/vascular outflow structures?
- b)
- Do you use a combination of IRE and thermal ablation?
- c)
- Could you use IRE as sole ablative treatment?
- d)
- What is the maximal number of lesions that you can treat with IRE at one sitting?
- e)
- What is the maximal size of hepatic lesion that you can treat with IRE (in cm)?
Question 9: Assessment of efficacy of IRE
- a)
- Do you routinely undertake a CT scan 24h after IRE and prior to discharge from hospital?
- b)
- What is the optimum imaging modality for assessment of response to IRE? (Text)
- c)
- What is the optimum time after IRE for assessment of ablation?
- d)
- Is RECIST 1.1 the optimum method for assessment of response?
- e)
- If the answer to d is NO, how do you assess response?
Question 10: Your views on a randomized trial for the assessment of IRE?
- a)
- Do you think that there should be a randomized trial to evaluate the role of IRE?
- b)
- If NO, is that because IRE is an established treatment?
- c)
- If NO, is that because IRE has no role as an ablative treatment for colorectal hepatic metastases?
- d)
- If YES – would you compare IRE to liver resection?
- e)
- If YES – would you compare IRE to thermal ablation?
- f)
- If YES – would you compare IRE to resection & ablation (in different settings)?
If you would like to be acknowledged as a Pubmed cited collaborator, please provide your name, institution and an email address below?
Appendix B. PubMed Citable Co-Authors under the LIVERMET-IRE Collaborative
Jose Maria Abadal13, Mohamad Abu Hilal14, Wasfi Alrawashdeh8, Bodil Andersson15, Anita Balakrishnan1,2, Marc Bemelmans16, María Caballero17, Lucia Carrion-Alvarez18, Thiery Chapelle19, Barbaros Erhan Çil20, Alessandra Cristaudi21, Brian Davidson22, Stephen W Fenwick12, Carlos Florez-Zorrilla23, Jacob Freedman24, Åsmund Avdem Fretland25, Stefan Gilg26, Ioannis Gkekas27, Kai-Wen Huang28, Riccardo Inchingolo29, Eduard Jonas30, Robrecht Knapen31, Niels Kok32, Kristel Mils33, Víctor Molina34, María Isabel Pérez Moreiras35, Marco Paci36, Elena Martín Perez37, Teresa Perra38, Panagiotis Petras39, Alberto Porcu40, Raffaello Roesel41, Elgun Samadov42, Erik Schadde43, Hester Scheffer44, Alejandro Serrablo45, Stefan Stättner46, Cornelis Verhoef47, Sheraz Yaqub25, Stojcev Zoran48
Affiliations
13 Hospital Virtual, Madrid, Spain
14Department of Surgery, Poliambulanza Foundation Hospital, Brescia, Italy
15Department of Surgery, Clinical Sciences Lund, Lund University, Skåne University Hospital, Lund, Sweden
16 Department of Surgery, Maastricht University Medical Center+, Maastricht, The Netherlands
17Departamento de Cirugía, Instituto Valenciano de Oncología, Valencia, Spain
18 General Surgery Department, HPB Unit Fuenlabrada University Hospital, Madrid, Spain
19 Department of Hepatobiliary, Transplantation, and Endocrine Surgery, Antwerp University Hospital, Antwerp, Belgium
20Department of Radiology, Koç University School of Medicine, Istanbul, Turkey
21 Department of General and Visceral Surgery, Cantonal Hospital Lugano, Lugano, Switzerland
22 Department of HPB & Liver Transplantation Surgery, Royal Free Hospital, London, UK
23 Departamento de Cirugía, American British Cowdray Medical Center IAP, México
24 Department of Visceral Surgery and Medicine, Inselspital, University Hospital Bern, Bern, Switzerland
25 Department of HPB Surgery, Oslo University Hospital, Oslo, Norway
68Department of Surgery, CLINTEC, Department of surgery and oncology, Karolinska Institutet, Stockholm, Sweden
27Specialistläkare, Kirurgcentrum, Norrlands Universitetssjukhus, Umeå
28Department of Surgery, National Taiwan University Hospital, Taipei, Taiwan
29 Unit of Interventional Radiology, F. Miulli Hospital, Italy
30Department of Surgery, Groote Schuur Hospital, Cape Town
31Department of Radiology and Nuclear Medicine, Maastricht University Medical Center+, Maastricht, The Netherlands
32Department of Surgery, Antoni van Leeuwenhoek - Dutch Cancer Institute, Amsterdam, The Netherlands
35Department of Hepatobiliary Surgery and Liver Transplant Unit, Hospital Universitari Bellvitge, University of Barcelona, Barcelona, Spain
34General and Digestive Surgery Service, Hospital de La Santa Creu I Sant Pau, Barcelona, Spain
35Servicio de Cirugía General y Aparato Digestivo del Hospital Xeral-Calde de Lugo, Lugo, Spain
36Department of HPB Surgery and Liver Transplantation, Assistance Publique Hopitaux de Paris, Beaujon Hospital, University Paris VII, Clichy, France
37 General and Digestive Surgery, Hospital Universitario de La Princesa, France
38Department of Medicine, Surgery and Pharmacy, University of Sassari, Sassari, Italy
39Ippokratio University Hospital of Thessaloniki, 5th Surgical Department of Aristotle University, Thessaloniki, Greece
40Department of Medicine, Surgery and Pharmacy, University of Sassari, Sassari, Italy
41Department of Visceral Surgery, University Hospital of Geneva (HUG), Geneve, Switzerland
42 Leyla Medical Center, Surgery, Azerbaijan
43Department of General, Visceral and Transplant Surgery, Klinik Hirslanden, Zurich, Switzerland
44 Department of Radiology and Nuclear Medicine, VU University Medical Center, Amsterdam, The Netherlands
45 Department of Surgery, Miguel Servet University Hospital, Zaragoza, Spain
46 Department of General, Visceral and Vascular Surgery, Salzkammergutklinikum, Vöcklabruck, Austria
47 Department of Surgery, Erasmus University Medical Centre, Rotterdam, Netherlands
48 Department of Oncology and Breast Diseases, Centre of Postgraduate Medical Education, Warsaw, Poland
References
- Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2021, 19, 329–359. [CrossRef] [PubMed]
- Martin J, Petrillo A, Smyth EC, Shaida N, Khwaja S, Cheow HK et al. World J Clin Oncol 2020, 11, 761–808.
- Siriwardena AK, Mason JM, Mullamitha S, Hancock HC, Jegatheeswaran S. Management of colorectal cancer presenting with synchronous liver metastases. Nat Rev Clin Oncol 2014, 11, 446–459. [Google Scholar] [CrossRef] [PubMed]
- Benson AB, Venook AP, Al-Hawary MM, Cederquist L, Chen YJ, Ciombor KK et al. Rectal Cancer, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2018, 16, 874–901. [CrossRef]
- Stangl R, Altendorf-Hofmann A, Charnley RM, Scheele J. Factors influencing the natural history of colorectal liver metastases. Lancet 1994, 343, 1405–10. [Google Scholar]
- Chan AKC, Mason JM, Baltatzis M, Siriwardena AK; CoSMIC Collaborators. Management of Colorectal Cancer with Synchronous Liver Metastases: An Inception Cohort Study (CoSMIC). Ann Surg Oncol 2022, 29, 1939–1951. [CrossRef] [PubMed]
- Nieuwenhuizen S, Dijkstra M, Puijk RS, Geboers B, Ruarus AH, Schouten EA, Nielsen K, de Vries JJJ, Bruynzeel AME, Scheffer HJ et al. Microwave Ablation, Radiofrequency Ablation, Irreversible Electroporation, and Stereotactic Ablative Body Radiotherapy for Intermediate Size (3-5 cm) Unresectable Colorectal Liver Metastases: a Systematic Review and Meta-analysis. Curr Oncol Rep 2022, 24, 793–808.
- Decadt B, Siriwardena AK. Radiofrequency ablation of liver tumours: systematic review. Lancet Oncol 2004, 5, 550–560. [CrossRef] [PubMed]
- Tago T, Katsumata K, Udou R, Kasahara K, Mazaki J, Kuwabara H et al. Significance of radiofrequency ablation for unresectable colorectal cancer with liver metastases. Anticancer Research. 2021, 41, 5539–5547. [Google Scholar]
- Pillai K, Akhter J, Chua TC, Shehata M, Alzahrani N, Al-Alem I, Morris DL. Heat sink effect on tumour ablation characteristics as observed in monopolar radiofrequency, bipolar, radiofrequency, and microwave, using ex vivo calf liver model. Medicine (Baltimore) 2015, 94, e580.
- Charpentier KP, Wolf F, Noble L, Winn B, Resnick M, Dupuy DE. Irreversible electroporation of the liver and liver hilum in swine. HPB (Oxford). 2011, 13, 168–173. [Google Scholar]
- Scheffer HJ, Nielsen K, van Tilborg AA, Vieveen JM, Bouwman RA, Kazemier G, Niessen HW, Meijer S, van Kuijk C, van den Tol MP, Meijerink MR. Ablation of colorectal liver metastases by irreversible electroporation: results of the COLDFIRE-I ablate-and-resect study. Eur Radiol 2014, 24, 2467–2475.
- Meijerink MR, Ruarus AH, Vroomen LGPH, Puijk RS, Geboers B, Nieuwenhuizen S, van den Bemd BAT, Nielsen K, de Vries JJJ, van Lienden KP et al. Irreversible Electroporation to Treat Unresectable Colorectal Liver Metastases (COLDFIRE-2): A Phase II, Two-Center, Single-Arm Clinical Trial. Radiology 2021, 299, 470–480.
- Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, Seligmann J,De Baere T, Osterlund P, Yoshino T, Martinell E. ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023, 34, 10–32.
- Spiers HVM, Lancellotti F, de Liguori Carino N, Pandanaboyana S, Frampton AE, Jegatheeswaran S et al. Irreversible Electroporation for Liver Metastases from Colorectal Cancer: A Systematic Review. Cancers (Basel) 2023, 15, 2428.
- https://handbook-5-1.cochrane.org/chapter_8/8_4_introduction_to_sources_of_bias_in_clinical_trials.htm (accessed 16th August 2023).
- Adam R, De Gramont A, Figueras J, Guthrie A, Kokudo N, Kunstlinger F,et al. The oncosurgery approach to managing liver metastases from colorectal cancer: a multidisciplinary international consensus. Oncologist. 2012, 17, 1225–1239. [CrossRef] [PubMed]
- Rocha FG and Helton, WS. Resectability of colorectal liver metastases: an evolving definition. HPB (Oxford). 2012, 14, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Imai K, Adam R, Baba H. How to increase the resectability of initially unresectable colorectal liver metastases: A surgical perspective. Ann Gastroenterol Surg, 2019; 3, 476–486.
- Elias D, Lasser P, Hoang JM, Leclere J, Debaene B, Bognel C et al. Repeat hepatectomy for cancer. Br J Surg 1993, 80, 1557–1562. [Google Scholar]
- Ruarus AH, Barabasch A, Catalano O, Leen E, Narayanan G, Nilsson A et al. Irreversible Electroporation for Hepatic Tumors: Protocol Standardization Using the Modified Delphi Technique. J Vasc Interv Radiol 2020, 31, 1765–1771. [CrossRef] [PubMed]
- Ruers T, Punt C, Van Coevorden F, Pierie JPEN, Borel-Rinkes I, Ledermann JA, Poston G, Bechstein W, Lentz MA, Mauer M et al. Radiofrequency ablation combined with systemic treatment versus systemic treatment alone in patients with non-resectable colorectal liver metastases: a randomized EORTC Intergroup phase II study (EORTC 40004). Ann Oncol 2012, 23, 2619–2626.
- Tinguely P, Ruiter SJS, Engstrand J, de Haas RJ, Nilsson H, Candinas D et al. A prospective multicentre trial on survival after Microwave Ablation VErsus Resection for Resectable Colorectal liver metastases (MAVERRIC). Eur J Cancer 2023, 187, 65–76. [CrossRef]
Figure 1.
Specialty and practice profile of respondents and their reported experience with IRE. 1A: Specialties of survey respondents. 1B: Number of patients with colorectal liver metastases seen by participants MDT/tumour boards per annum. MDT = Multidisciplinary team. 1C: Number of patients with colorectal liver metastases treated by IRE by respondents.
Figure 1.
Specialty and practice profile of respondents and their reported experience with IRE. 1A: Specialties of survey respondents. 1B: Number of patients with colorectal liver metastases seen by participants MDT/tumour boards per annum. MDT = Multidisciplinary team. 1C: Number of patients with colorectal liver metastases treated by IRE by respondents.
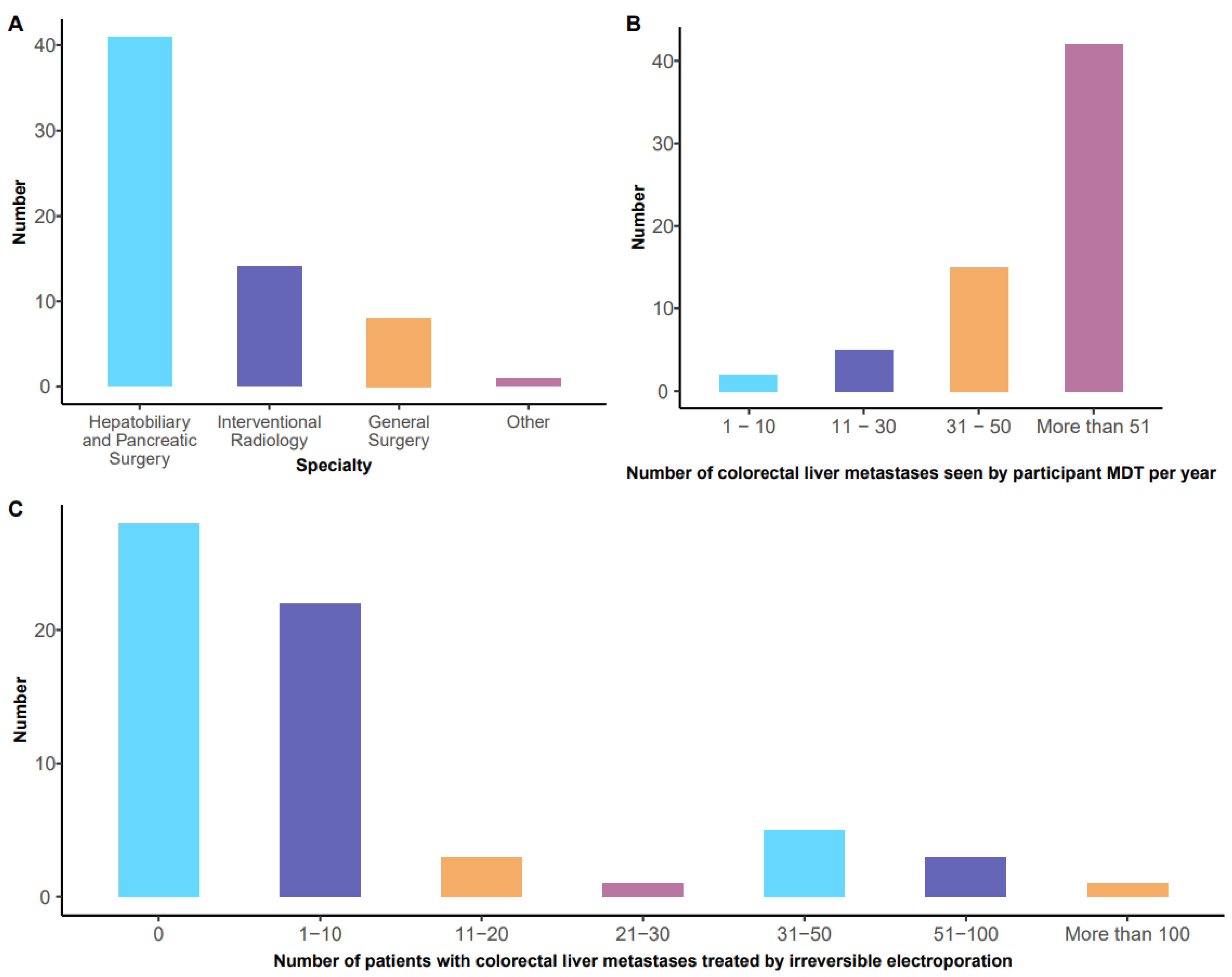
Figure 2.
Clinician responses to specific clinical management scenarios relating to patients with colorectal liver metastases. 2A: Preferred treatment in the setting of patients with up to four surgically resectable, bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all <4cm in size, away from liver inflow/outflow structures in the setting of good performance status and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1). 2B: Preferred treatment for patients with up to four bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all < 4cm in size, away from liver inflow/outflow in the setting of a performance status which precludes surgery and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1).
Figure 2.
Clinician responses to specific clinical management scenarios relating to patients with colorectal liver metastases. 2A: Preferred treatment in the setting of patients with up to four surgically resectable, bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all <4cm in size, away from liver inflow/outflow structures in the setting of good performance status and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1). 2B: Preferred treatment for patients with up to four bi-lobar, liver-limited, colorectal hepatic metastases (M1a), all < 4cm in size, away from liver inflow/outflow in the setting of a performance status which precludes surgery and a background of a single course of systemic chemotherapy otherwise unspecified (stable disease on RECIST 1.1).
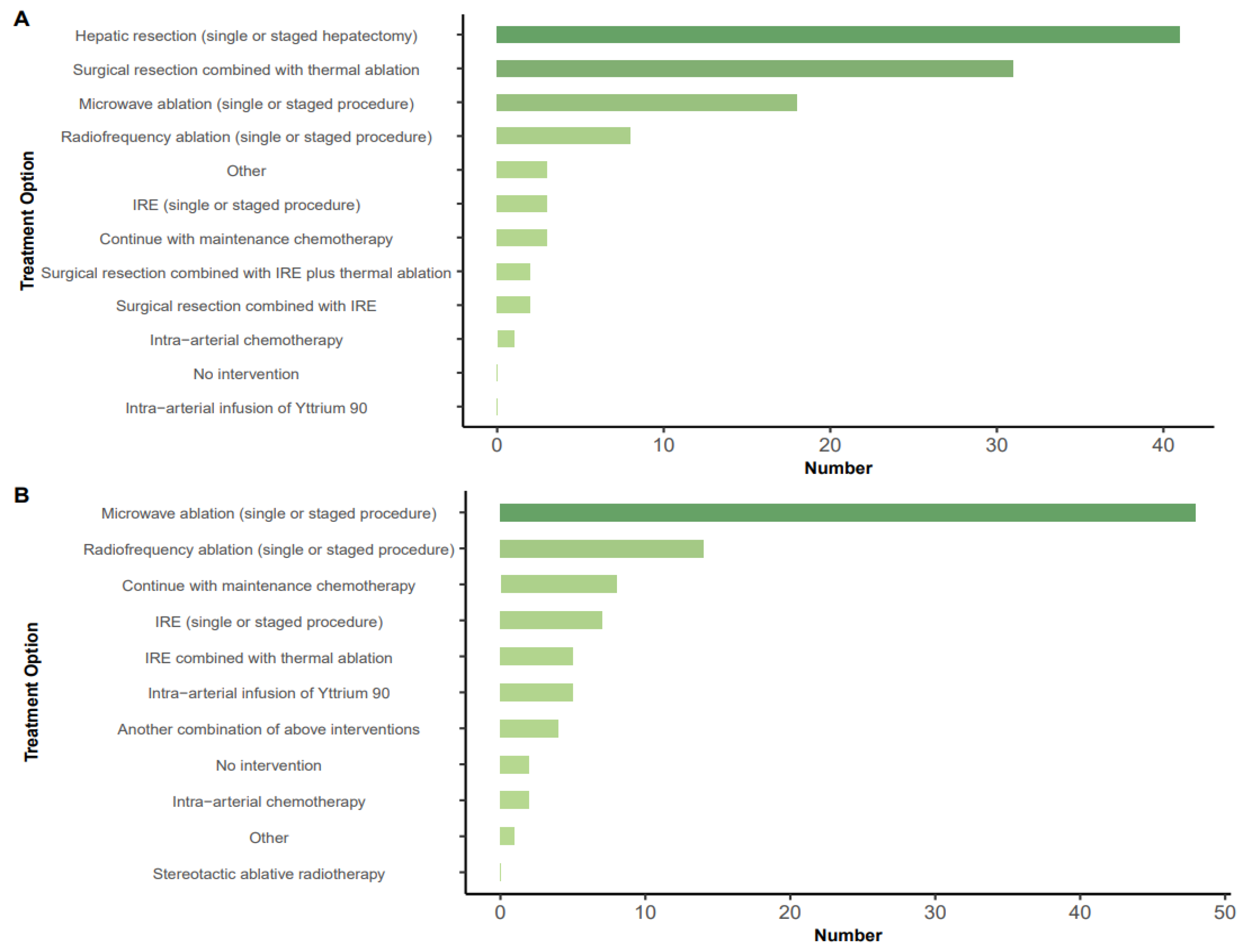
Figure 3.
Preferred treatment for the patient with bi-lobar hepatic metastases that are not resectable in a single operation (four lesions in total - M1a) all < 4 cm in size, prior systemic chemotherapy, good performance status and with lesions resectable by right hepatectomy leaving two lesions in the left hemi-liver. 3B: Preferred treatment for the patient with up to two liver-limited hepatic recurrent metastases (both < 4cm in size, one close to inflow), 18 months after prior right hepatectomy. ALPPS, associated liver partition and portal vein ligation; IRE, irreversible electroporation; SABR, stereotactic ablative radiotherapy.
Figure 3.
Preferred treatment for the patient with bi-lobar hepatic metastases that are not resectable in a single operation (four lesions in total - M1a) all < 4 cm in size, prior systemic chemotherapy, good performance status and with lesions resectable by right hepatectomy leaving two lesions in the left hemi-liver. 3B: Preferred treatment for the patient with up to two liver-limited hepatic recurrent metastases (both < 4cm in size, one close to inflow), 18 months after prior right hepatectomy. ALPPS, associated liver partition and portal vein ligation; IRE, irreversible electroporation; SABR, stereotactic ablative radiotherapy.
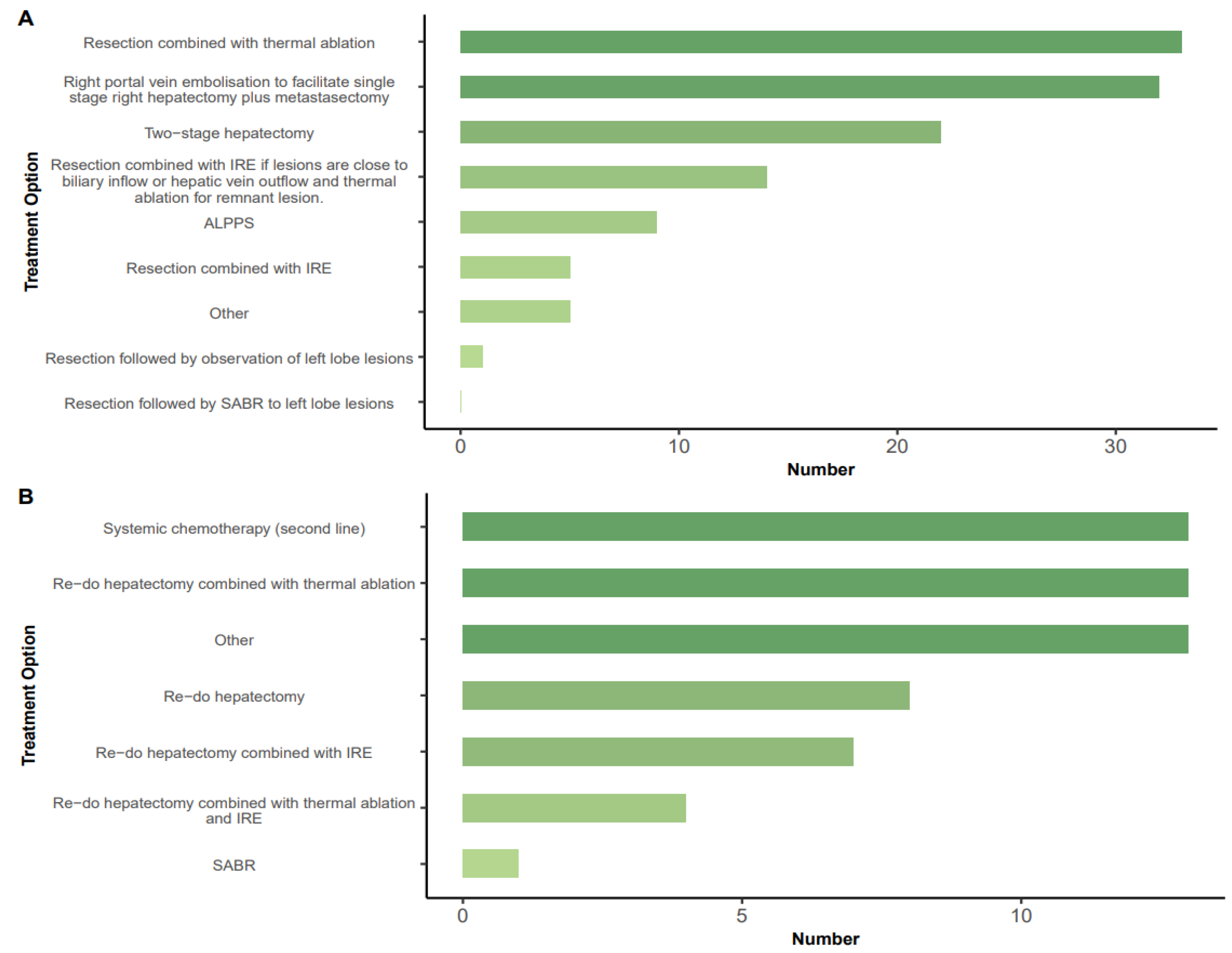
Figure 4.
4A: Suggested maximum number of lesions that could undergo irreversible electroporation (IRE) in a single session. 4B: Suggested maximum size of lesion that could be ablated by irreversible electroporation (IRE). 4C: imaging modality selected for post-IRE assessment. 4D: timing of follow up imaging for lesions treated with IRE. CT, computer tomography; MR, magnetic resonance.
Figure 4.
4A: Suggested maximum number of lesions that could undergo irreversible electroporation (IRE) in a single session. 4B: Suggested maximum size of lesion that could be ablated by irreversible electroporation (IRE). 4C: imaging modality selected for post-IRE assessment. 4D: timing of follow up imaging for lesions treated with IRE. CT, computer tomography; MR, magnetic resonance.
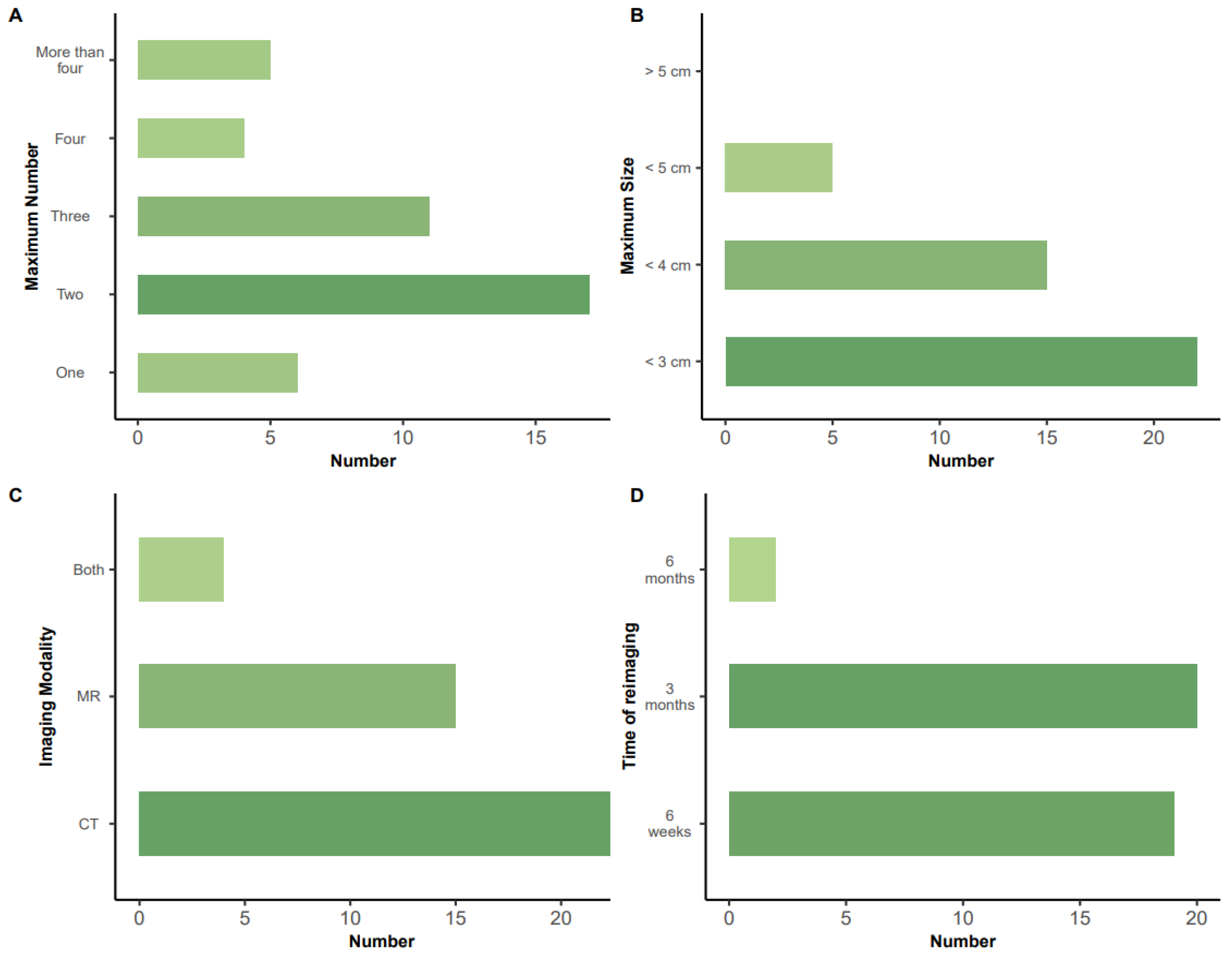

Table 1.
Methods of IRE delivery and their usage. Note that respondents could select more than one option as this was thought to best reflect clinical practice.
Table 1.
Methods of IRE delivery and their usage. Note that respondents could select more than one option as this was thought to best reflect clinical practice.
| Method of treatment | Number (%) (47 respondents) |
|---|---|
| Percutaneous with CT guidance | 33 (70) |
| Percutaneous with ultrasound guidance | 16 (34) |
| Open surgery with ultrasound guidance | 11 (23) |
| Open surgery with CT guidance | 1 (2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



