
Submitted:
27 March 2024
Posted:
27 March 2024
You are already at the latest version
Abstract
Conclusions: Our findings suggest that the NMS-E represents a valuable preoperative diagnostic tool for endometriosis, effectively correlating with the disease's severity and surgical outcomes. Incorporating the NMS-E into clinical practice could significantly enhance the management of endometriosis by addressing current diagnostic limitations and guiding surgical planning.
Keywords:
Endometriosis Severity Prediction
; Numerical Multi-Scoring System of Endometriosis (NMS-E)
; Preoperative Diagnostic Method
; deep endometriosis
; Transvaginal Ultrasound
; pelvic examination
; Surgical Duration Estimation
; laparoscopic surgery for endometriosis
; r-ASRM classification.
1. Introduction
Endometriosis, characterized by the aberrant growth of endometrial-like tissue outside the uterine cavity, poses significant diagnostic and therapeutic challenges. Its heterogeneous manifestations, including severe pain, infertility, and diverse lesion morphologies, necessitate a multifaceted diagnostic and management strategy.
A critical examination of current diagnostic and classification methods for endometriosis highlights a range of shortcomings. The revised American Society for Reproductive Medicine (r-ASRM) classification [1,2,3], which was modified in 1996 and is now widely known, utilizes a scoring system based on the size of endometriosis lesions and the extent of adhesions. This system classifies the disease into stages I to IV by accumulating points, with a maximum score of 150 points. While this feature proves to be very useful, the r-ASRM classification also presents significant limitations. Despite its widespread use, it falls short of accurately assessing deep endometriosis (DE) and lacks applicability as a preoperative diagnostic tool.
The Enzian score was initially published in 2005 as an independent postoperative assessment for DE [4]. It has evolved, especially with modifications in 2010 and 2011, to complement the r-ASRM classification by filling in the gaps related to DE [5]. The Enzian score, modeled after the TNM classification for cervical cancer, considers the tumorigenic nature of DE, categorizing lesions in the Douglas' pouch into A, B, and C sections based on location and size. It also describes adenomyosis and bladder endometriosis as 'F' (far). Nonetheless, these were not preoperative diagnostic methods. Recently, an evolved ♯Enzian classification has emerged as a preoperative diagnostic method achievable through transvaginal ultrasonography [6,7], primarily practiced in Europe. This method, however, has its own set of challenges, including the technical difficulty of detecting sub-centimeter-deep lesions via ultrasonography and unclear associations between lesions and pain, among others.
In 2023, the AAGL 2021 Endometriosis Classification [8] was put forward, advancing its original version of the intraoperative classification [9] by adopting transvaginal ultrasonography [7,8], akin to ♯Enzian classification, enabling it as a preoperative diagnostic method. Based on expert surveys, this approach assigns surgical complexity scores to each lesion, providing a singular indicator of the severity of endometriosis [8,9]. Despite its convenience and the availability of a supportive app, this method still faces technical difficulties in assessing peritoneal, tubal, and ureteral lesions via ultrasonography. It does not clarify the relationship between lesions and pain, either.
Other diagnostic methods with unique features have been proposed (such as EFI [10,11], Ultrasound mapping system [12], EBDRECT [13], UBESS [14], and others [15,16]). Still, they have not secured a place as convenient as first-line diagnostic tools, requiring complex evaluation or MRI, not being preoperative or for other reasons.
Pelvic examination remains superior for detecting pelvic pain. The Beecham classification [17] for endometriosis, adept at capturing early lesions, is now rarely practiced, highlighting the missing integration of pelvic examination findings in current diagnostics.
Considering the ideal first-line diagnostic method for endometriosis, various requirements emerge [15], but we believe the following four are crucial:
- A simple, objective, noninvasive method that captures early lesions and the diverse states of endometriosis, including their localization and spread.
- A scoring system to stratify severe cases and guide referrals to specialized facilities.
- An anatomically intuitive and easily shareable format akin to the TNM classification facilitates information exchange between physicians and patients.
- A method capable of capturing temporal changes, useful as an indicator for surgical, medicinal, recurrent, and infertility interventions.
To meet the first condition, the foundational examination methods should include pelvic examination and transvaginal ultrasonography. The second condition requires the technique to be scored. For the third, an easily shareable and anatomically illustrative format is needed. Lastly, the method must be non-invasive and quick to execute by anyone, anywhere, to fulfill the fourth condition.
The Numerical Multi-Scoring System of Endometriosis (NMS-E) was designed as a comprehensive new assessment tool for endometriosis, combining insights from pelvic examination and transvaginal ultrasonography. The full details of this system were published in the Japanese Society of Endometriosis journal in 2015 [18,19,20]. We have already reported on the outcomes related to the leading scores of NMS-E, namely the adhesion score in 2020 [21] and pain score in 2023 [22]. Therefore, in this instance, we retrospectively investigated whether the E-score, a severity indicator in NMS-E, actually correlates with the severity of endometriosis.
This study aims to address the gap in endometriosis diagnosis by evaluating the feasibility and efficacy of the NMS-E in predicting surgical duration and outcomes. By leveraging a retrospective analysis of patients treated for endometriosis at our institution, we seek to validate the NMS-E against traditional scoring systems and assess its potential to enhance surgical planning and patient management. Our hypothesis posits that the NMS-E can provide a more accurate reflection of disease severity, thereby improving preoperative predictions and surgical outcomes for patients with endometriosis.
2. Materials and Methods
2.1. Study Subjects
This diagnostic study used data from a previous study at Nippon Medical School Hospital. Of the 131 cases previously examined [21,22], 111 patients who underwent surgery at Nippon Medical School between 2012 and 2018 were included in the current research and underwent preoperative transvaginal ultrasound and pelvic examination. The 20 cases that were excluded included eight instances of large fibroid removal where the fibroids exceeded 3 cm, 6 cases where there was no complete resolution of Douglas pouch occlusion, 4 cases involving the resection of adenomyosis, and two cases of additional surgeries: one septectomy and one bladder repair due to bladder injury. MI, a physician with extensive experience in diagnosing and operating endometriosis, performed their examination. The Nippon Medical School ethics committee approved this study, and informed consent was obtained from each patient who consented to participate.
2.2. NMS-E Method Overview
NMS-E stands for Numerical multi-scoring system of Endometriosis, a preoperative, no-invasive diagnostic approach that leverages pelvic examination and transvaginal ultrasonography to assess endometriosis comprehensively. This method is structured into three distinct layers, as depicted in Figure 1:
- I.
- Physical finding Map: This foundational layer captures a wide array of endometriosis-related data collected during examinations. It is the basis for the subsequent layers, organizing the extensive information into a visual and anatomical format.
- II.
- NMS-E Summary: Building on the Physical finding Map, this layer condenses the detailed observations into a concise equation, facilitating a standardized summary of the endometriosis condition akin to the TNM classification used in oncology.
- III.
- E-Score: The culmination of the NMS-E method, this layer translates the summarized data into a singular numeric value, representing the severity of endometriosis. The E-Score integrates four critical elements derived from the previous layers: cyst, adhesion, pain, and uterine scores.
2.2.1. Detailed Layer Descriptions
Physical finding Map: This layer involves a detailed mapping of four principal manifestations of endometriosis: I. Endometriomas, II. Adhesions, III. Pain, and IV. Uterine and Surrounding Lesions, including endometriotic nodules (E), retroverted uterus (R), and adenomyosis (A). Data are plotted on three 3x3 grids, mirroring a Rubik’s cube-like representation of the uterus and ovaries from various perspectives (Table 2). The left grid maps the transvaginal ultrasound cross-sectional view of the ovaries-uterus; the middle grid, the longitudinal section of the uterus; and the right grid, pain intensity in seven pelvic regions around the cervix as gauged by the Numeric Rating Scale (NRS).
NMS-E Summary: This layer distills the comprehensive data from the Physical finding Map into a concise formula, summarizing key findings: the size of endometriomas (right/left cm), the strength of adhesions (number of adhesion sites), the intensity of pain (highest NRS value), and identified uterine lesions (abbreviated). Should rare-site endometriosis be detected, it is annotated separately at the end of the summary. Some examples of NMS-E summaries are shown in Appendix A.
E-Score: This final scoring layer quantifies the severity of endometriosis into a single E-Score, integrating the cyst, adhesion, pain, and uterine scores from the Summary layer. The scoring methodology is transparent, with each component—cysts (up to 10 points), adhesions (0-10 points based on presence), pain (highest of 0-10 NRS points), and uterine lesions (3 points per lesion)—contributing to the overall score.
2.2.2. The Measurement and Recording Methods for the Four Conditions of Endometriosis
- I.
- Endometrioma: endometrioma is measured using the maximum diameter in transvaginal ultrasonography (to one decimal place, in cm). The findings are recorded in the central row's left cell of the left 3x3 grid (corresponding to the right adnexal region of the patient) or the right cell (corresponding to the left adnexal region). For multi-cystic conditions, the total maximum diameter is used. For non-endometriomas, the cyst type's initial is prefixed before the size [Appendix A - NMS-E Example 3]. If tubal lesions are identified, their abbreviations (e.g., hydrosalpinx: h.s) are also recorded [Appendix A - NMS-E Example 4]. For summarization, the rounded-up value of the cyst's maximum diameter is recorded as the cyst score for each side. Figure 2 shows a right endometrioma of 6.5cm and a left endometrioma of 2.4cm. For summarization, values are rounded up, resulting in 7/3. The maximum score for a single endometrioma is 5. Thus, the cyst score for this case is right 5 + left 3 = 8 points.
- II.
- Adhesion: Adhesion is measured at ten locations using transvaginal ultrasonography cross-sectional (five locations) and longitudinal (five locations) images of the uterus ovaries. Adhesions are assessed based on the presence or absence of the sliding sign at each location. The sliding sign is a method to diagnose adhesions by checking if there is movement between the target organ and surrounding tissue when pressed with the ultrasound probe [23]. The presence of movement indicates no adhesions (-), while the absence indicates adhesions (+). For more details on the measurement method, refer to the adhesion score paper [21]. Measurement locations include the space between the right ovary and right pelvic wall (Rt. O-side), between the right ovary and uterus (Rt. O-Ut.), between both ovaries (Inter O-O), between the left ovary and uterus (Lt. O-Ut.), between the left ovary and left pelvic wall (Lt. O-Side), and the upper (Upper ant.), middle (Mid. ant.) parts of the anterior surfaces of the uterus, and the upper (Upper post.), middle (Mid.post.), and lower (Lower post.) parts of the posterior surfaces of the uterus. Figure 2 shows adhesions at four locations in the cross-sectional view and three in the longitudinal view, resulting in an adhesion score of 7/10. This value is directly added to the E-score.
- III.
- Pain: Pain is evaluated using NRS out of 10 based on pain induced by palpation during pelvic examination in seven pelvic regions centered around the uterine cervix: I. Right adnexal region, II. Right uterosacral ligament area, III. Anterior vaginal wall area, IV. Cervical area, V. Pouch of Douglas, VI. Left adnexal region, VII. Left uterosacral ligament area. The values are recorded in the corresponding cells of the right 3x3 grid. The details of this mapping, including pain intensity in each region, are referenced in the Pain Score paper [22]. The highest point among the seven areas is the Max Pain score. In Figure 2, the highest point is 8 in the Douglas pouch area, making the patient's Pain score 8. This value is directly added to the E-score.
- IV.
- Uterine Lesion: Uterine lesion is mainly evaluated using transvaginal ultrasonography. The assessed conditions include Retroverted uterus (R), Endometriotic nodules (E), and Adenomyosis (A). Uterine fibroids (M) are evaluated but not scored. All detected conditions, such as R, A, E, and M lesions and their sizes (if applicable), are recorded in the central cell of the middle row of the central grid or the anatomically corresponding cell along with their size. Endometriotic nodules (E) are depicted as hypoechogenic lesions similar to adenomyosis outside the uterus (lesions larger than 1cm in diameter are defined as E in this assessment) [7]. E lesions detected as nodules during pelvic examination are also marked in the corresponding cell on the right grid. The definition of a retroverted uterus (R) is when the angle formed by the cervical and uterine body axes is less than 180 degrees posteriorly [24]. Adenomyosis (A) appears on transvaginal ultrasound as a heterogeneously enlarged uterus with myometrial cysts, asymmetric myometrial thickening, poorly defined areas of echogenicity, etc. [7]. Figure 2 displays a 2.4 cm endometriotic nodule located at the center of the posterior uterine surface, along with adenomyosis. When summarizing, these lesions are shown as A and E, and when scoring, each lesion is given 3 points, giving a total of 6 points. However, in some data of this research, E lesions between 1cm and 2cm are scored as 3 points, between 2cm and 3cm as 6 points, and larger than 3cm as 10 points.
- V.
- Rare-site Endometriosis: Rare-site Endometriosis is treated separately from the abovementioned four states. The diagnostic methods vary depending on the location of the lesion. Lesions considered for rare-site endometriosis evaluation include intestinal endometriosis, bladder endometriosis, ureteral endometriosis, vaginal endometriosis, cutaneous endometriosis, etc. If these are observed, they are added to the end of the NMS-E as additional notation (Appendix A - Example 5). In scoring, rare-site endometriosis is tentatively assigned 10 points.
Note: In our assessment of the adhesion, filmy adhesions were not counted as adhesions; only dense adhesions were considered and calculated. In other words, we regarded adhesions that limit mobility detected by transvaginal ultrasonography as dense adhesions. The transvaginal ultrasonography device used in this study was the Voluson E8 (GE Healthcare, Japan).
2.3. Statistics
Statistical analysis, including the correlation between scores such as the E-score and operation time or the VAS value, was performed using Pearson's correlation coefficient, calculated with the CORREL function in Microsoft Excel (Version 16.77.1, Microsoft Corp., Redmond, WA). Significant differences in uterine scores between groups with and without a retroverted uterus were assessed using a two-tailed Student's t-test with the TTEST function in Excel. A P-value of 0.05 or less was considered to indicate statistical significance.
3. Results
3.1. Demographics, Clinical Presentation, and Surgical Interventions in Endometriosis Patients
In the observed cohort of 111 patients, the mean age was 35.1 years, ranging from 23 to 51. The mean Body Mass Index (BMI) was 20.6 kg/m², ranging from 17.2 to 28.5 kg/m². The average parity was 0.3, with a range between 0 and 2. Out of 111 individuals, 92 (82.9%) were nulliparous.
Clinical symptoms evaluated included dysmenorrhea with a mean Visual Analogue Scale (VAS) score of 6.8, dyspareunia with a mean VAS score of 3.9, dyschezia with a mean score of 3.1, and chronic pelvic pain with a mean score of 2.2. The mean duration of the operation was 189.1 minutes, ranging from 51 to 421 minutes, and the mean blood loss was 65.7 ml, ranging from 0 to 500 ml.
Regarding endometrioma, 0.9% of patients had none, 45.0% had unilateral endometrioma, and 54.1% had bilateral endometrioma. Specific surgical interventions included unilateral salpingo-oophorectomy in 3.6% of patients and unilateral cystectomy in 38.7% of patients. The Douglas' pouch was reported as usual in 28.8% of patients, with partial obstruction in another 28.8% and complete obstruction in 42.3%. In all cases with partial or complete obstruction of the Douglas pouch, a full resolution of the obstruction was achieved.
Other conditions identified were adenomyosis in 24.3% of the cohort, with no patient undergoing resection for large or multiple myomas. A small proportion of patients underwent resection for vaginal endometriosis (2.7%), umbilical endometriosis (0.9%), and inguinal endometriosis (0.9%). Myomas were present in 16.2% of patients, with 8.1% undergoing resection for small myomas.

Table 1.
Patient characteristics and surgeries.
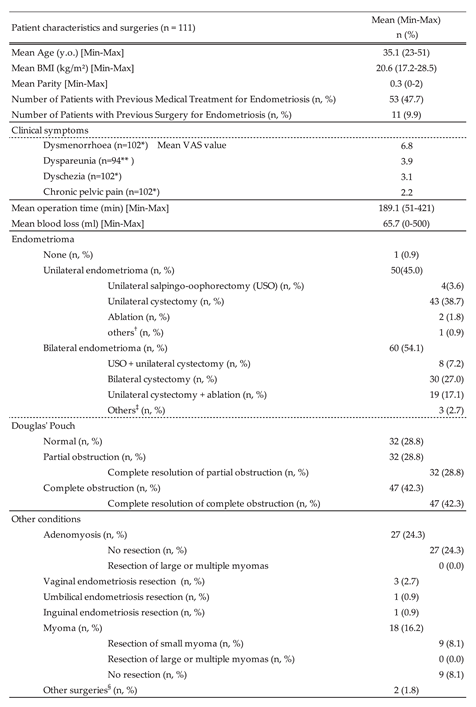
* Due to the preoperative VAS scores being unknown for nine individuals, the data was based on 102 patients. ** For nine individuals, the preoperative VAS scores were obscure, and eight had not been sexually active for some time. Thus, the data was based on 94 patients. † This includes alcohol fixation and aspiration of cystic contents. † This includes alcohol fixation and aspiration of cystic contents. ‡ This includes bilateral heat ablation. § This includes bartholinic cystectomy and endometrial polypectomy. These durations have been subtracted from the total surgical time.
3.1.1. Assessment of Endometriosis Severity Using r-ASRM and E-Score Metrics
In assessing endometriosis severity among the study population (n=111), the mean revised American Society for Reproductive Medicine (r-ASRM) score was 69.3, ranging from 10 to 150. The distribution of severity stages indicated that the majority of the patients were classified with stage IV endometriosis (71.9%), followed by stage III (26.3%), during stages II and I was notably less common, representing 0.9% and 0.0% of the cases, respectively.
The mean E-score, which provides a quantified measure of endometriosis severity, was calculated at 19.67, within a range of 6 to 36. This composite score integrates individual metrics for cysts, adhesions, pain, and uterine abnormalities, with mean scores recorded as 6.16 for cysts, 3.88 for adhesions, 6.05 for pain, and 3.24 for uterine factors. The prevalence of specific uterine conditions was substantial, with endometriotic nodules (E) present in 52.2% of the patients, retroverted uterus (R) in 39.6%, and adenomyosis (A) in 24.3%.
A Rare score assigned for less common sites of endometriosis was applied to 4 patients (3.6% of the study cohort), illustrating the occurrence of rare-site disease.
Table 2.
Endometriosis severity in r-ASRM and NMS-E in endometriosis patients.
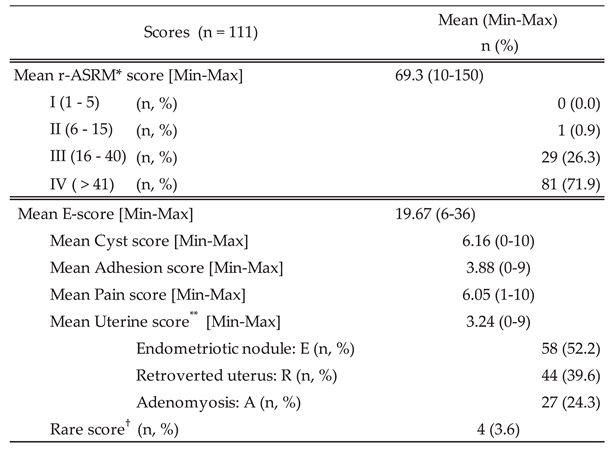
* revised American Society for Reproductive Medicine. ** Uterine Score includes three conditions: Endometriotic nodules categorized as 'E,' retroverted uterus categorized as 'R,' and adenomyosis categorized as 'A.' Below is the breakdown of the number and percentage of the cases. † The Rare Score assigns 10 points to cases with rare-site endometriosis. However, as there were only four instances in the current study, its average score was not calculated.
3.1.2. Correlation of Endometriosis Scoring Systems with Surgical Duration and Blood Loss
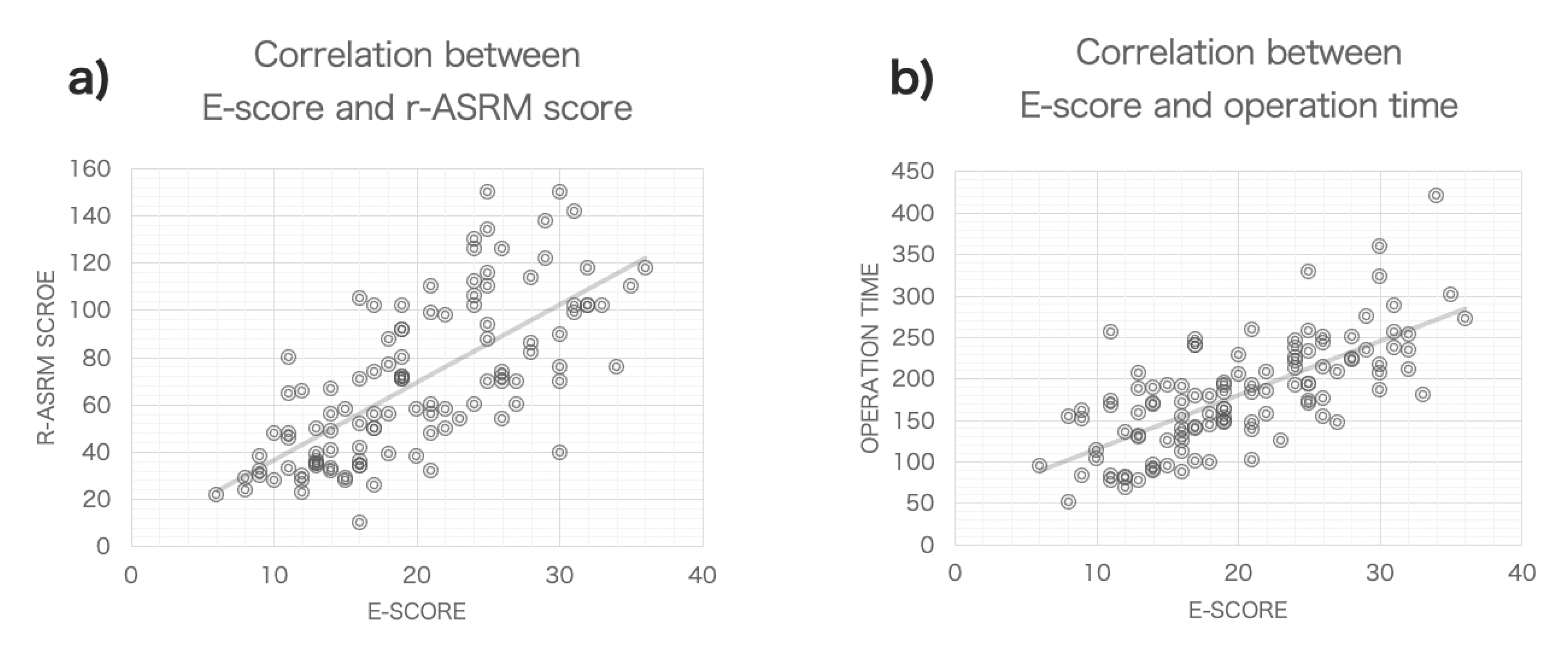
The analysis presented in Figure 3a and Table 3 shows a correlation coefficient of 0.700 between the E-score and the r-ASRM score, indicating a substantial association between these two measures of endometriosis severity. The E-score also demonstrated a slightly stronger correlation with surgical duration, with a coefficient of 0.703 (Figure 3b). This was higher than the correlation between r-ASRM scores and surgical duration, which was 0.642. The adhesion score also showed a notable correlation with surgical duration, with a coefficient of 0.596, and the uterine score followed closely with a coefficient of 0.417, suggesting these factors significantly influence the length of surgery. The correlation between E-score and blood loss was the highest among the scores, with a coefficient of 0.407.
Table 3.
Correlation Between Various Scores, Surgical Duration, and Blood Loss.

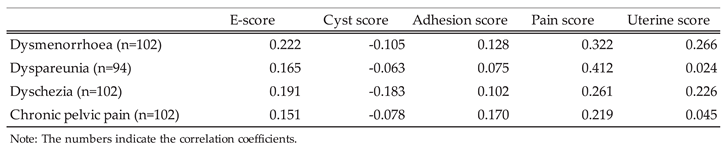
3.1.3. Correlation of Endometriosis Scoring Systems with Clinical Symptoms
The correlation between the E-score and clinical symptoms of endometriosis was examined (Table 4). Overall, the E-score hardly showed a significant correlation with these symptoms. When looking at individual scores, Cyst and Adhesion scores showed no correlation, while the Pain score demonstrated the highest correlation with dyspareunia, as we have previously reported [22]. Furthermore, the Uterine score showed weak correlations with dysmenorrhea (0.266) and dyschezia (0.226). The Uterine score evaluates conditions such as endometriotic nodules (E), retroverted uterus (R), and adenomyosis (A). Notably, patients with retroverted uterus (42 cases) reported significantly higher dyschezia pain scores compared to those without the condition (59 cases) (4.26 vs. 2.23, P=0.0038).
Table 4.
Correlation Between Various Scores and Clinical Symptoms.
3.2. Refinement of Endometriotic Nodules Scoring and Its Impact on Surgical Duration Prediction in Endometriosis Treatment
Building on the data from Table 3, it was evident that the adhesion and uterine scores significantly contribute to surgical duration. This subsection explores how each element of the uterine score impacts operation time and whether modifying specific parameters improves the prediction of surgical duration (Table 5). Centered on the Adhesion score, adding adenomyosis (A) as part of the Uterine score slightly decreased the correlation with operation time (e.g., from 0.596 to 0.532). The addition of retroverted uterus (R lesion) showed little change (e.g., from 0.596 to 0.585), while incorporating endometriotic nodules (E lesion) significantly improved the correlation (e.g., from 0.596 to 0.677). Given the relatively low score typically allocated to E lesions (3 points), employing a modified score that increases with lesion size (namely, assigning 3 points for lesions over 1cm but under 2cm, 6 points for lesions over 2cm but under 3cm, and 10 points for lesions over 3cm) demonstrated an even stronger correlation (from 0.596 to 0.738). Finally, when adjusted to include these modified scores for E lesions, the initial E-score showed an improved correlation coefficient up to 0.754.
Table 5.
Correlation Analysis of Surgical Duration with Combined Scoring of Adhesion, Pain, Cyst, Rare, and Uterine Scores in Endometriosis.
Table 5.
Correlation Analysis of Surgical Duration with Combined Scoring of Adhesion, Pain, Cyst, Rare, and Uterine Scores in Endometriosis.
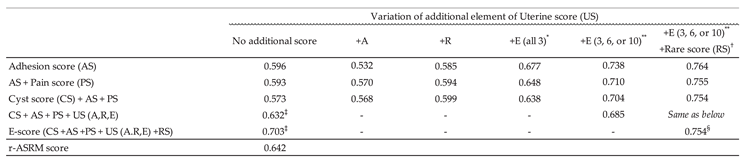
A: Adenomyosis, R: Retroverted uterus, E: Endometriotic nodules. * Uniformly allocate 3 points for each endometriotic nodule identified by ultrasound or similar diagnostic imaging, regardless of the number of lesions. ** Allocate 3 points for endometriotic nodules sized 1-2 cm, 6 points for those sized 2-3 cm, and 10 points for lesions over 3 cm identified by ultrasound or similar diagnostic imaging. For multiple lesions, scores should be cumulatively added. † Add 10 points if rare-site endometriosis, such as vaginal endometriosis, is observed. ‡ The Uterine score has already been added. Endometriotic nodules categorized as 'E' are uniformly allocated 3 points each, irrespective of the number of lesions. § The Uterine score has already been incorporated. Endometriotic nodules categorized as 'E' have been calculated in a format that assigns 3, 6, or 10 points depending on their size.
4. Discussion
This study established that the E-Score of NMS-E, a preoperative diagnostic indicator for assessing endometriosis's severity, strongly correlates with the widely utilized r-ASRM score derived from surgical findings, with a correlation coefficient of 0.700. It also revealed a more substantial association with the duration of surgery (0.703) compared to the r-ASRM score (0.642). Furthermore, regarding blood loss, the E-Score demonstrated a higher correlation than the r-ASRM (0.407 vs. 0.348). These findings imply that the E-Score could be an equally or more precise predictor of endometriosis severity before surgery than the r-ASRM score.
Considering the predictive power of the E-Score for surgical duration, this study found that the expected surgery time based on the E-score can be determined by the equation y = 6.4974x + 50.345. For instance, an E-score of 19 points predicts a surgical time of 174 minutes. It should be noted that this equation might differ from one facility to another or from one surgeon to another, and even for the same surgeon, it could evolve with increasing experience. Nonetheless, with the accumulation of sufficient data, the precision of these predictions is expected to be enhanced, thereby facilitating the strategic planning and readiness for surgeries within the institution.
Looking at individual scores, the adhesion score had the highest correlation with surgical duration (0.596) despite its average value of 3.88 not being the highest among the scores. This implies that the strength of adhesions is the most significant factor determining surgical time or complexity. Following this comes the uterine score (0.417). Indeed, there is a perception that excision of deep endometriosis is time-consuming. Next in line are the Pain score and Cyst score, respectively. It was unexpected that the time taken for cystectomy had a minor impact on the overall surgical time in this study. One reason for this could be that the majority of the subjects (71.9%) were patients with severe conditions at stage IV, suggesting that adhesions and deep endometriosis, more common in severe cases, could have been dictating the surgical duration. The Cyst score might become a more significant determining factor in less severe conditions.
On the other hand, the E-score showed low to almost no correlation with the four major clinical symptoms of endometriosis (0.151-0.222). When examining the correlation with clinical symptoms, it seems better to focus on individual scores. As previously reported, the Pain score had a high correlation with dyspareunia (0.412), and it was found this time that the uterine score showed a weak correlation with dyschezia (0.226). Interestingly, when breaking down the Uterine score, the group with the retroverted uterus (R) had significantly higher dyschezia scores than the group without that (4.26 vs. 2.23, p=0.0038). This may indicate a mechanism of disease where bowel adhesions and consequent uterine retroversion lead to dyschezia. Further investigation is necessary following this. On the other hand, no correlation was observed between the Cyst score, adhesion score, and clinical symptoms.
The significant correlation between the NMS-E E-score and surgical duration underscores the utility of the NMS-E as a predictive tool in clinical settings. This finding is particularly relevant for the surgical management of endometriosis, where estimating procedure length can aid in resource allocation and patient counseling. Unexpectedly, the correlation with blood loss was less pronounced than anticipated, suggesting that while the NMS-E score is a reliable predictor of surgical duration, it may be less applicable for predicting intraoperative blood loss. This discrepancy highlights the complex nature of endometriosis. It suggests that factors beyond the scope of the NMS-E, such as patient-specific anatomical variations or surgical technique, may influence blood loss. These results encourage further refinement of the NMS-E and suggest additional variables for inclusion to enhance its predictive accuracy.
In this study, the E-score of NMS-E showed a high correlation with the r-ASRM score. Here, we want to consider the reason for this. NMS-E was created to enable a non-invasive implementation of the r-ASRM, an intraoperative diagnostic method. Moreover, it incorporates elements of deep endometriosis, such as pain assessment, which are weaknesses of the r-ASRM [15]. Therefore, the correlation of these two diagnostic methods is not coincidental but by design. Here's a detailed explanation. The r-ASRM score is graded out of a total of 150 points: peritoneal lesions: 6 points, endometriomas: 40 points, posterior cul-de-sac obliteration: 40 points, ovarian adhesions: 32 points, and tubal adhesions: 32 points [2].On the other hand, NMS-E grades out of approximately 40 points: endometriomas: 10 points, ovarian adhesions: 10 points, pain: 10 points, and uterine lesions: 9 points (3 points X 3) (In practice, the score limit is not fixed as additional points are given for tubal diseases and rare site endometriosis.). Comparing the elements of both diagnostic methods, the evaluation of the ovaries is nearly the same, and the adhesions are common for the ovaries, with some overlap for posterior cul-de-sac obliteration (adhesion). Regarding pain, it is known that the areas with solid pain are around the cul-de-sac, and cases with posterior cul-de-sac obliteration significantly have higher Pain scores. Therefore, it can be said that the r-ASRM's posterior cul-de-sac obliteration lesions and NMS-E's pain score share some common elements. This means the three main aspects of both diagnostic methods look almost identical. One significant difference is the evaluation of the fallopian tubes. The regular fallopian tubes are rarely visible in transvaginal ultrasonography, so their adhesions are also unknown. Therefore, only when tubal enlargement is observed in NMS-E is graded with 3 points. Another difference is that NMS-E has a uterine score, evaluating deep lesions such as Endometriotic nodules (in r-ASRM, deep lesions are usually rated up to 6 points for peritoneal lesions, which is low compared to other items). The scoring of each element in NMS-E is set to about 1/4 of each item's score in r-ASRM. For these reasons, r-ASRM and NMS-E could show a high correlation.
For preoperative diagnostic methods other than NMS-E, the #Enzian [6] and the 2021 AAGL classifications [8,9] have recently gained attention [25]. It could also be possible to predict surgery times using these scores. However, attempts to predict surgical duration using these are not common, and there are only reports of attempts to predict surgery times using the traditional Enzian classification [26]. Therefore, it is unclear how accurately they can predict surgery times. Nevertheless, even if they could, we still believe NMS-E has several advantages. One of them is the adhesion score, as mentioned above. The adhesion score, which has already been shown to diagnose the temporal change in the strength of postoperative adhesions and can be an indicator of infertility [21], is a unique score of NMS-E that quantitatively measures adhesion strength out of 10 points and is unparalleled. Moreover, it has been demonstrated that it is a significant factor in determining surgery times. This is why we believe NMS-E has superior surgery time prediction capabilities compared to other preoperative diagnostic methods. The base for the adhesion score measurement is also in r-ASRM. In the r-ASRM score, the degree of solid adhesions around the ovary is classified into no adhesion, <1/3, 1/3 < < 2/3, or >2/3, and points are allocated to each adhesion state as 0 points, 4 points, 8 points, and 16 points, respectively [2].
In NMS-E, it is assumed that the enlarged ovaries are placed within an inverted tetrahedron, and the presence of adhesions is evaluated on four surfaces: the ovarian surface (Inter O-O), the uterine surface (Lt O-Ut), the sidewall surface (Lt O-Side), and the upper surface (usually without adhesions). The loss of mobility on each surface is considered as the presence of adhesion. Thus, adhesions on one surface represent 1/4 coverage of adhesions, corresponding to less than 1/3 of adhesions in the r-ASRM. Adhesions on two surfaces represent 2/4 coverage, corresponding to between 1/3 and 2/3 in the r-ASRM, and adhesions on three surfaces represent 3/4 coverage, corresponding to more than 2/3 in the r-ASRM. In the adhesion score, 1, 2, or 3 points are assigned respectively. This ingenuity has led to the adhesion score of NMS-E not only correlating with the adhesion score of r-ASRM but also with the surgical duration.
Another significant advantage of NMS-E is the existence of the Pain score derived from a pelvic examination. Most endometriosis diagnostic methods do not include the assessment of the pelvic examination. Dyspareunia is one of the critical indicators for deciding whether to perform surgery for endometriosis. There is no better method than a pelvic examination to detect such localized pain. Transvaginal ultrasonography accurately diagnoses deep lesions, but reports are scarce on strategies that can simultaneously assess the pain they induce [27]. Moreover, they are not comprehensive preoperative diagnostic methods for endometriosis. NMS-E establishes a system that successfully integrates pelvic examination findings and transvaginal ultrasonography imaging using the Pain score. The Pain score has been shown to correlate most strongly with dyspareunia. These features make NMS-E an unparalleled diagnostic method of great value, capable of predicting not only surgical duration but also the activity of deep lesions.
The limitation of this study is that only one examiner performed this method. As a result, we obtained consistent data, but the possibility of bias is fully considered. Therefore, to prove that this method is universal, it is necessary to check the reproducibility of this data among many examiners and facilities and confirm its effectiveness.
Another problem is the small number of study cases. The current study used data from 111 cases by a single operator for data standardization. Since endometriosis is a disease showing various pathologies, many confounding factors exist. Therefore, in the future, it is necessary to increase the number of cases further and make adjustments through matching and stratification.
Another significant issue in this study is the difficulty in determining the optimal weighting for each disease. In NMS-E, in addition to the central four lesions, there are many parameters. Significant big data and effort are necessary to find optimal solutions for all of them. However, as mentioned before, since NMS-E is somewhat based on the r-ASRM score weighting, there may not be such a significant empirical discrepancy. Nevertheless, to solve this problem relatively quickly, the scoring way in the 2021 AAGL classification is a good reference [9]. In this classification, a survey was conducted on approximately 30 endometriosis expert physicians, and the complexity of each lesion was scored. The allocation of points to each lesion was determined based on the results. For example, Complete Cu-de-sac obliteration scored 9 points, Endometriomas over 3cm is 7 points, Ureteral endometriosis is 6-9 points, and Intestinal endometriosis over 3cm is 8 points. Coincidentally, the scoring is close to NMS-E, where each element is nearly expressed out of a perfect score of 10 points. Also, in this and #Enzian classifications, the score jumps when the lesion size exceeds 3cm. In our current data, the correlation with surgical time improved when we also increased the scoring for the Endometriotic nodules based on size (Table 5). It is necessary to consolidate this information in the future and make fine adjustments to the scoring in NMS-E.
The clinical significance of NMS-E is fourfold. First, using the E-score enables preoperative identification of patients with severe endometriosis. Surgery for severe endometriosis often requires special procedures such as a complete opening of the obliterated cul-de-sac or shaving of intestinal endometriosis [28]. Therefore, patients with severe endometriosis should be operated on by experienced surgeons or at specialized facilities. However, until now, the severity of endometriosis was not apparent preoperatively, which might have led to inadequate triage and lost opportunities for adequate surgery for some patients. The use of the E-score can avoid such situations. Second, it enables accurate prediction of surgery time, allowing for efficient operation room management, which is essential for hospital management and medical economics. Predicting surgery time for endometriosis, which can present complex conditions, was particularly challenging. This could lead to complex cases being scheduled late in the afternoon with short expected surgery time, resulting in complications such as bowel injuries that require cooperation from other departments. On the other hand, if a case is considered mild based on the NMS-E preoperatively, it might be possible to plan more than three surgeries in one day, including that surgery. Third, the NMS-E summary facilitates sharing information about patient conditions among physicians, not just the severity. Although it may initially seem confusing, as seen in some examples in the Appendix A data, one can grasp the overall picture of endometriosis at a glance once accustomed. Finally, the Physical Finding Map allows for understanding the local conditions and the whole picture of endometriosis. This is particularly important as preoperative information. Based on this information, decisions can be made about removing a lesion and to what extent, based on the location of the etiology and its activity (Pain score). The Physical Finding Map becomes an indicator when planning surgical strategies. NMS-E is a non-invasive preoperative diagnostic method that can be easily performed with pelvic examination and transvaginal ultrasonography. With the above features, it realizes the ideal endometriosis diagnostic method initially proposed.
As a future research direction, it is necessary to validate the NMS-E further in more extensive and diverse populations to determine the effectiveness of this comprehensive preoperative diagnostic method for endometriosis, which incorporates numerous variables. Moving forward, collaborative research with multiple physicians and facilities is planned, and individual evaluations of various parameters, such as score limits and allocations, will also be conducted. Furthermore, developing non-invasive infertility prediction using NMS-E is a crucial issue. For this purpose, it is necessary to add the critical information missing in NMS-E. This information pertains to the patency of the fallopian tubes. However, it is impossible to diagnose the patency of the fallopian tubes solely based on the imaging information from transvaginal ultrasonography. Therefore, by combining tests such as the Tubal Insufflation Test (Rubin's Test), Saline-infused hysterosonogram (SIH), Hysterosalpingo-Contrast Sonography (HyCoSy) [29], or Hysterosalpingography (HSG), it may be possible to achieve the objective.
5. Conclusions
The E-score of the NMS-E can be a new indicator of endometriosis severity, enabling the prediction of surgical duration. Furthermore, the comprehensive preoperative diagnostic method NMS-E, with its system for sharing a complete picture of the multifaceted conditions presented by endometriosis, can assist in appropriately referring patients to the proper facilities or physicians and in devising suitable and efficient surgical plans tailored to each patient's specific condition.
Author Contributions
Conceptualization, M.I. and S.A.; methodology, M.I.; software, M.I.; validation, M.I., S.A., Y.K., and S.S.; formal analysis, M.I.; investigation, M.I.; resources, M.I.; data curation, M.I., S.T., N.O., S.M., K.N., and H.K.; writing—original draft preparation, M.I.; writing—review and editing, M.I., M.T., and G.I.; visualization, M.I.; supervision, S.S.; project administration, Y.K. and S.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted by the Declaration of Helsinki and approved by the Institutional Review Board of Nippon Medical School Hospital (protocol code B-2020-261 and date of approval: March 3rd, 2021) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
NMS-E Examples
Example 1:
7/3-7-8-A (E-score=26)
Meaning: There's a 7cm right ovarian chocolate cyst and a 3cm left ovarian chocolate cyst. Adhesions are scored 7/10. The maximum pain during examination is 8/10, indicating severe pain. Adenomyosis is present.
Example 2:
5/N-4-3-N (E-score=12)
Meaning: There's a 5cm right ovarian chocolate cyst. The left ovary is normal. Adhesions score is 4/10. The maximum pain during examination is 3/10, indicating mild pain. The uterus is normal.
Example 3:
3/f3-0-3-N (E-score=6)
Meaning: There's a 3cm right ovarian chocolate cyst and a 3cm functional cyst on the left ovary (not added to E-score). No adhesions are present. The maximum pain during examination is 3/10, indicating mild pain—no abnormalities in the uterus.
Example 4:
N/6p.s-7-5-EMR (E-score=26)
Meaning: The right ovary is normal. A 6cm left ovarian chocolate cyst and a left hydrosalpinx are present. Adhesions score is 7/10. The maximum pain during examination is 5/10, indicating moderate pain. Endometriotic nodules, uterine fibroids, and a retroverted uterus are present. The hydrosalpinx adds 3 points, so 6p.s becomes 8 points. Thus, the E-score for this case is 26.
Example 5:
4/2-6-8-ER-Intestinal endometriosis (E-score=36)
Meaning: There's a 4cm right ovarian chocolate cyst and a 2cm left ovarian chocolate cyst. The adhesions score is 6/10. The maximum pain during examination is 8/10, indicating severe pain. Endometriotic nodules and a retroverted uterus are present. Intestinal endometriosis is also noted.
References
- Society, T.A.F. , Revised American Fertility Society classification of endometriosis: 1985. Fertil Steril 1985, 43, 351–2. [Google Scholar]
- Medicine, A.S.f.R. , Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril 1997, 67, 817–21. [Google Scholar]
- Society, T.A.F. , Classification of endometriosis. The American Fertility Society. Fertil Steril 1979, 32, 633–4. [Google Scholar]
- Tuttlies, F., et al., [ENZIAN-score, a classification of deep infiltrating endometriosis]. Zentralbl Gynakol. 2005, 127, 275–81.
- Haas, D., et al., Efficacy of the revised Enzian classification: a retrospective analysis. Does the revised Enzian classification solve the problem of duplicate classification in rASRM and Enzian? Arch Gynecol Obstet. 2013, 287, 941–5.
- Keckstein, J.; Saridogan, E.; Ulrich, U.A.; Sillem, M.; Oppelt, P.; Schweppe, K.W.; Krentel, H.; Janschek, E.; Exacoustos, C.; Malzoni, M.; et al. The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis. Acta Obstet. et Gynecol. Scand. 2021, 100, 1165–1175. [Google Scholar] [CrossRef]
- Guerriero, S., et al., Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: a consensus opinion from the International Deep Endometriosis Analysis (IDEA) grouUltrasound Obstet Gynecol. 2016, 48, 318–32.
- Abrao, M.S., et al., Preoperative Ultrasound Scoring of Endometriosis by AAGL 2021 Endometriosis Classification Is Concordant with Laparoscopic Surgical Findings and Distinguishes Early from Advanced Stages. J Minim Invasive Gynecol. 2023, 30, 363–373.
- Abrao, M.S.; Andres, M.P.; Miller, C.E.; Gingold, J.A.; Rius, M.; Neto, J.S.; Carmona, F. AAGL 2021 Endometriosis Classification: An Anatomy-based Surgical Complexity Score. J. Minim. Invasive Gynecol. 2021, 28, 1941–1950. [Google Scholar] [CrossRef] [PubMed]
- Adamson, G.D.; Pasta, D.J. Endometriosis fertility index: the new, validated endometriosis staging system. Fertil. Steril. 2010, 94, 1609–1615. [Google Scholar] [CrossRef] [PubMed]
- Tomassetti, C.; Geysenbergh, B.; Meuleman, C.; Timmerman, D.; Fieuws, S.; D'Hooghe, T. External validation of the endometriosis fertility index (EFI) staging system for predicting non-ART pregnancy after endometriosis surgery. Hum. Reprod. 2013, 28, 1280–1288. [Google Scholar] [CrossRef]
- Exacoustos, C.; Malzoni, M.; Di Giovanni, A.; Lazzeri, L.; Tosti, C.; Petraglia, F.; Zupi, E. Ultrasound mapping system for the surgical management of deep infiltrating endometriosis. Fertil. Steril. 2014, 102, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Chattot, C.; Huchon, C.; Paternostre, A.; Du Cheyron, J.; Chouillard, E.; Fauconnier, A. ENDORECT: a preoperative score to accurately predict rectosigmoid involvement in patients with endometriosis. Hum. Reprod. Open 2019, 2019, hoz007. [Google Scholar] [CrossRef] [PubMed]
- Menakaya, U.; Reid, S.; Lu, C.; Bassem, G.; Infante, F.; Condous, G. Performance of ultrasound-based endometriosis staging system (UBESS) for predicting level of complexity of laparoscopic surgery for endometriosis. Ultrasound Obstet. Gynecol. 2016, 48, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Johnson, N.P.; Hummelshoj, L.; Adamson, G.D.; Keckstein, J.; Taylor, H.S.; Abrao, M.S.; Bush, D.; Kiesel, L.; Tamimi, R.; Sharpe-Timms, K.L.; et al. World Endometriosis Society consensus on the classification of endometriosis. Hum. Reprod. 2016, 32, 315–324. [Google Scholar] [CrossRef] [PubMed]
- International working group of Aagl, E.E., et al., Endometriosis classification, staging and reporting systems: a review on the road to a universally accepted endometriosis classification(). Hum Reprod Open. 2021, 2021, hoab025.
- Beecham, C.T. Classification of endometriosis. 1966, 28, 437. [Google Scholar] [PubMed]
- Ichikawa, M. , et al., Shinbu shikyuu naimakushou jutsuzen shindan no yoake NMS-E: Numerical Multi-scoring System of Endometriosis (Surgical Treatment of Deep Infiltrating Endometriosis: The Dawn of Preoperative Diagnosis for Deep Infiltrating Endometriosis - NMS-E; Numerical Multi-scoring System of Endometriosis). Journal of Japan Society of Endometriosis 2015, 36: 77-81.
- Sekine, M., et al., Shikyuu naimaku shou ni taisuru aratana jutsuzen shindan hou: NMS-E no keichitsu eko ni yoru yuchaku hyouka wa kenja kan de saganai (No Differences in the Evaluation of Adhesions by Transvaginal Ultrasound Between Examiners Using the New Preoperative Evaluation Method NMS-E (Numerical Multi-scoring System of Endometriosis). Journal of Japan Society of Endometriosis. 2016, 37, 133–135.
- Ichikawa, M., et al., Naimakushou byōhen no atarashii rinshōteki hyōkahō - Jūrai no shikyūnaimakushō hyōkahō no tokuchō to kadai, soshite saishin no hyōkahō NMS-E no kaisetsu (A New Clinical Evaluation Method for Endometriosis Lesions: Characteristics and Challenges of Traditional Endometriosis Evaluation Methods, and an Explanation of the Latest Evaluation Method NMS-E). Rinshō Fujinka Sanka (Clinical Gynecology and Obstetrics). 2020, 74, 526–537.
- Ichikawa, M.; Akira, S.; Kaseki, H.; Watanabe, K.; Ono, S.; Takeshita, T. Accuracy and clinical value of an adhesion scoring system: A preoperative diagnostic method using transvaginal ultrasonography for endometriotic adhesion. J. Obstet. Gynaecol. Res. 2020, 46, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, M.; Shiraishi, T.; Okuda, N.; Nakao, K.; Shirai, Y.; Kaseki, H.; Akira, S.; Toyoshima, M.; Kuwabara, Y.; Suzuki, S. Clinical Significance of a Pain Scoring System for Deep Endometriosis by Pelvic Examination: Pain Score. Diagnostics 2023, 13, 1774. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.; Lu, C.; Casikar, I.; Reid, G.; Abbott, J.; Cario, G.; Chou, D.; Kowalski, D.; Cooper, M.; Condous, G. Prediction of pouch of Douglas obliteration in women with suspected endometriosis using a new real-time dynamic transvaginal ultrasound technique: the sliding sign. Ultrasound Obstet. Gynecol. 2012, 41, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S.; Ichikawa, M.; Kaseki, H.; Watanabe, K.; Ono, S.; Akira, S.; Takeshita, T. Accuracy of Transvaginal Ultrasonographic Diagnosis of Retroflexed Uterus in Endometriosis, with Magnetic Resonance Imaging as Reference. J. Nippon. Med Sch. 2023, 90, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Enzelsberger, S.; Oppelt, P.; Nirgianakis, K.; Seeber, B.; Drahoňovský, J.; Wanderer, L.; Krämer, B.; Grübling, K.N.; Kundu, S.; Salehin, D.; et al. Preoperative application of the Enzian classification for endometriosis (The cEnzian Study): A prospective international multicenter study. BJOG: Int. J. Obstet. Gynaecol. 2022, 129, 2052–2061. [Google Scholar] [CrossRef]
- Haas, D.; Chvatal, R.; Habelsberger, A.; Schimetta, W.; Wayand, W.; Shamiyeh, A.; Oppelt, P. Preoperative planning of surgery for deeply infiltrating endometriosis using the ENZIAN classification. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 166, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Guerriero, S.; Ajossa, S.; Gerada, M.; Virgilio, B.; Angioni, S.; Melis, G.B. Diagnostic value of transvaginal 'tenderness-guided' ultrasonography for the prediction of location of deep endometriosis. Hum. Reprod. 2008, 23, 2452–2457. [Google Scholar] [CrossRef] [PubMed]
- Donnez, O.; Roman, H. Choosing the right surgical technique for deep endometriosis: shaving, disc excision, or bowel resection? Fertil. Steril. 2017, 108, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Alcázar, J.L.; Martinez, A.; Duarte, M.; Welly, A.; Marín, A.; Calle, A.; Garrido, R.; Pascual, M.A.; Guerriero, S. Two-dimensional hysterosalpingo-contrast-sonography compared to three/four-dimensional hysterosalpingo-contrast-sonography for the assessment of tubal occlusion in women with infertility/subfertility: a systematic review with meta-analysis. Hum. Fertil. 2020, 25, 43–55. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
NMS-E Assessment Sheet.
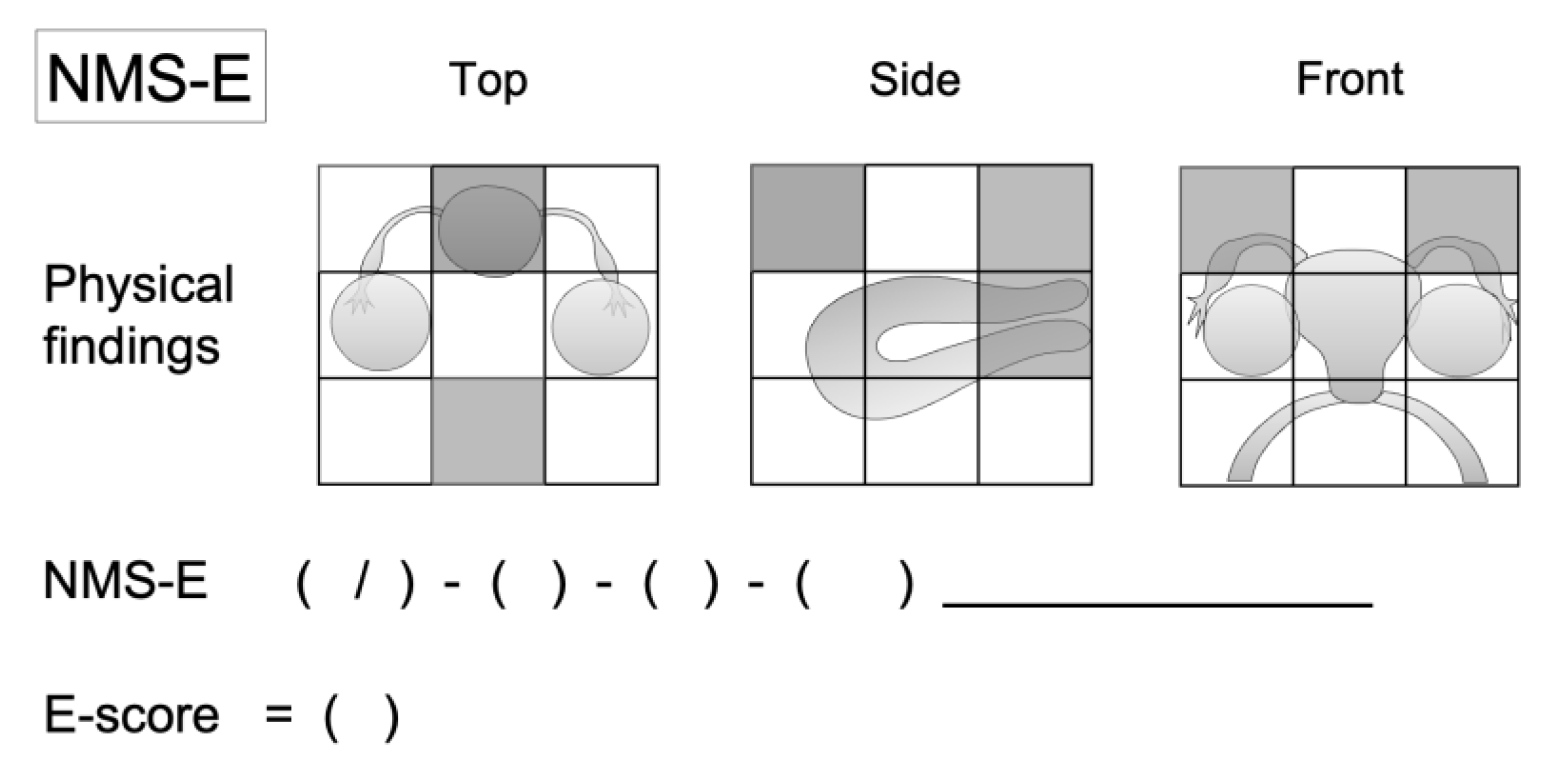
Figure 2.
Instruction for NMS-E The NMS-E assessment sheet offers a streamlined diagnostic approach for endometriosis, using a three-tiered structure: 1) Physical finding Map for a visual representation of findings; 2) NMS-E, which summarizes data into a linear formula; and 3) E-score, quantifying disease severity. Scores for ovarian endometriomas, adhesions, pain, and uterine lesions are totaled for the E-score. Rare-site endometriosis and conditions like tubal hydrosalpinx or pyosalpinx are also scored. The sheet visualizes and quantifies complex clinical data, facilitating a comprehensive understanding of endometriosis severity. .
Figure 2.
Instruction for NMS-E The NMS-E assessment sheet offers a streamlined diagnostic approach for endometriosis, using a three-tiered structure: 1) Physical finding Map for a visual representation of findings; 2) NMS-E, which summarizes data into a linear formula; and 3) E-score, quantifying disease severity. Scores for ovarian endometriomas, adhesions, pain, and uterine lesions are totaled for the E-score. Rare-site endometriosis and conditions like tubal hydrosalpinx or pyosalpinx are also scored. The sheet visualizes and quantifies complex clinical data, facilitating a comprehensive understanding of endometriosis severity. .
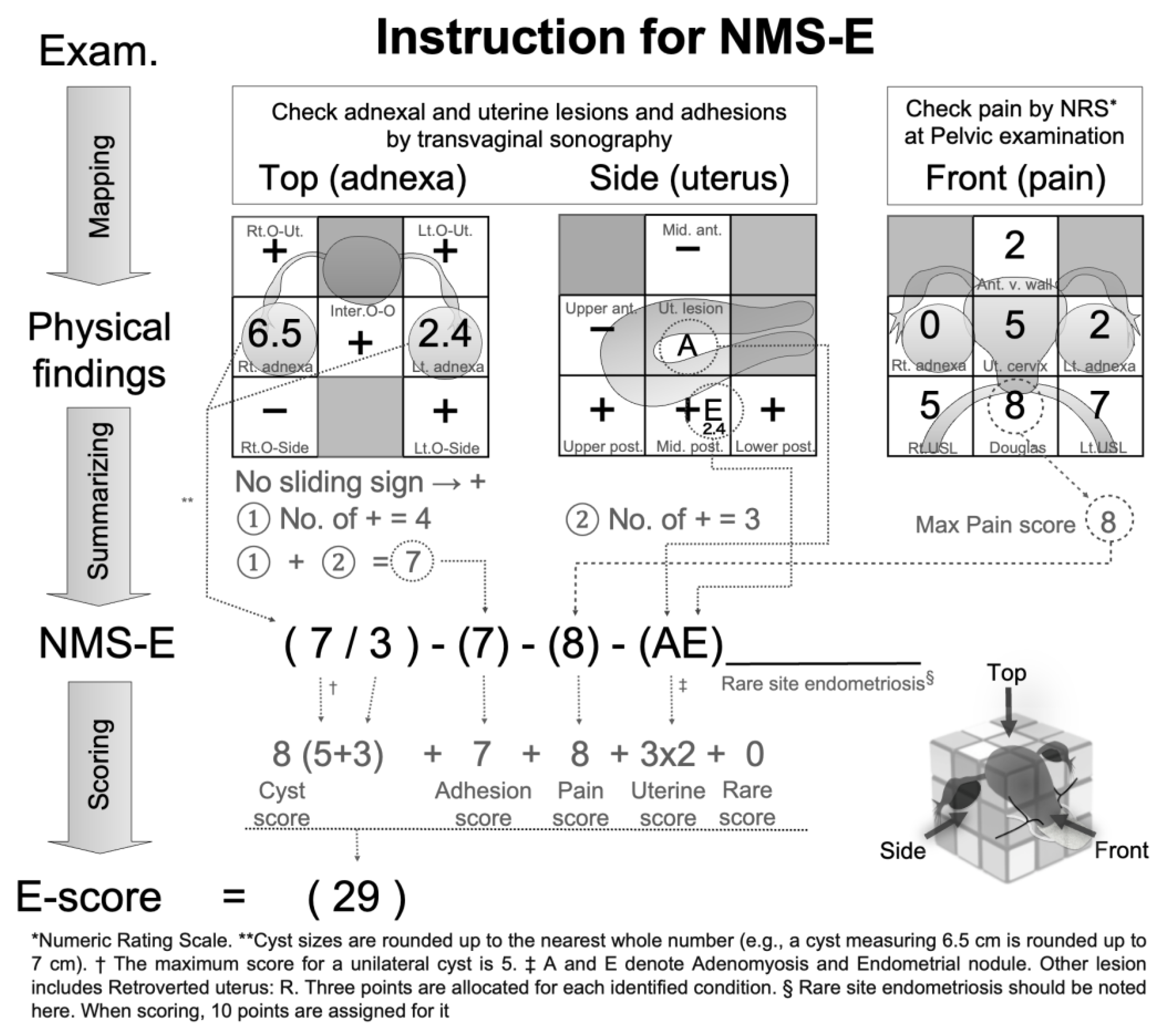
Figure 3.
Correlation Analysis of E-score with r-ASRM Score and Operation Time (a) This figure illustrates the correlation between the E-score and the r-ASRM score. (b) This figure shows the correlation between the E-score and operation time. Both figures are based on data from 111 subjects. The diagonal line in each graph represents the regression line.
Figure 3.
Correlation Analysis of E-score with r-ASRM Score and Operation Time (a) This figure illustrates the correlation between the E-score and the r-ASRM score. (b) This figure shows the correlation between the E-score and operation time. Both figures are based on data from 111 subjects. The diagonal line in each graph represents the regression line.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



