
Submitted:
18 April 2024
Posted:
22 April 2024
You are already at the latest version
Abstract
Background: Endometriosis is a female chronic inflammatory disease in which endometrial tissue develops outside the uterine cavity. It is a complex pathology, that significantly contributes to morbidity in premenopausal women, leading to chronic pain, infertility, and subfertility negatively impacting the physical, and emotional well-being and overall quality of life. The public health burden of endometriosis remains elusive and challenging to determine, and this uncertainty can lead to inadequate healthcare services and treatments. Objective: To estimate the incidence and prevalence of endometriosis in Italy using the hospital discharge records database. Population-based retrospective study. Nationwide between 2011 and 2020. Methods: From the National Hospital Discharge Database were selected all admissions with a diagnosis of endometriosis (ICD-9-CM, codes 617.x), supported by the presence of a procedure code of laparoscopy or any other surgical procedure allowing direct visualisation of the lesions. Main outcomes measures Incidence and prevalence of endometriosis were estimated for the entire 2010-2020 period and by individual year, analysing the time trend and variability in different geographical areas of Italy. Results: A total of 134,667,646 women aged 15–50 years with one or more hospitalisations for endometriosis in all Italian hospitals. The incidence of endometriosis in Italy during this period was 0.839 per 1000 women (CI95% 0.834-0.844), exhibiting a statistically significant decreasing trend over the years. A discernible north-south gradient was observed, with higher rates documented in the northern regions. The prevalence rate stood at 14.0 per 1000 during the same period, and a similar north-south geographical gradient was identifiable in the prevalence rates as well. Conclusions: The utilization of national-level hospital data enables the generation of incidence and prevalence data for endometriosis without variations in methods and definitions, facilitating the evaluation of temporal trends and regional comparisons. Understanding and quantifying this phenomenon is essential for appropriate healthcare planning in various Italian regions.
Keywords:
Endometriosis
; epidemiology
; incidence
; prevalence
; population-based
Introduction
Endometriosis is a female chronic inflammatory disease in which endometrial tissue develops outside the uterine cavity. It is a complex pathology [1] that significantly contributes to morbidity in premenopausal women, leading to chronic pain, infertility, and subfertility negatively impacting the physical, and emotional well-being and overall quality of life [2,3].
The aetiology of endometriosis is not well understood and diagnosis usually requires imaging techniques or surgery for more complex cases [4]. Underdiagnoses, diagnostic delays, as well as the lack of reliable data on prevalence and incidence data of this pathology have strong clinical and social implications. The public health burden of endometriosis remains elusive and challenging to determine, and this uncertainty can lead to inadequate healthcare services and treatments [5,6].
Epidemiological studies conducted over the past three decades have aimed to determine the incidence and prevalence of endometriosis. Most studies focused on specific populations with pelvic pain, infertility, or gynecological conditions. However, there is a lack of data based on the general population. Notably, an Australian cohort study found a cumulative prevalence of clinically confirmed endometriosis of 6.0% by age 40-44, increasing to 11.4% when including clinically suspected cases [7]. In Europe, a Spanish study estimated an overall incidence of 1.61 per 1,000 women [8]. A systematic review with meta-analysis reported a pooled incidence rate of 1.36 per 1,000 person-years, highlighting the methodological heterogeneity in defining and studying endometriosis [9].
In Italy, there are no national data on incidence and prevalence. However, in the Friuli-Venezia Giulia (FVG) region, an epidemiological register was enacted in 2011 to estimate the incidence and prevalence of endometriosis, combining hospitalization and anatomopathological data from the regional automated centralized record system [10]. The incidence of endometriosis in women aged 15–50 years was thus estimated to be 1.1 per 1000 resident women and prevalence, estimated from incidence, to be 18 per 1000.
The present study aimed to estimate the incidence and prevalence of endometriosis in Italy using the hospital discharge records database. Despite potentially underestimating the phenomenon by only counting hospitalized cases, this data source enables a national estimate and analysis of differences among various geographical areas within the country.
Methods
Hospitalisation data for the decade 2011-2020 were analysed using the National Hospital Discharge Database (NHDB), which is collected by the Minister of Health and managed by the Statistical Service of the Italian National Institute for Health. The NHDB collects data on all hospitalization episodes provided in public and private hospitals in Italy including demographic data (e.g., age, sex, residence, level of education), characteristics of the hospitalization, and clinical features (main and concomitant diagnosis, diagnostic or therapeutic procedures coded according to the International Classification of Diseases, Ninth Revision Clinical Modification (ICD-9-CM)).
All admissions with a main and concomitant diagnosis of endometriosis (ICD-9-CM, codes 617. x), supported by the presence of a procedure code of laparoscopy or any other surgical procedure allowing direct visualization of the lesions were selected (Table 1), as recommended by the 2014 guidelines of the European Society of Human Reproduction and Embryology [11]. Women diagnosed with endometriosis in the previous 10 years were excluded to identify only incident cases. Only women aged 15 to 50 residing in Italy with a reliable pseudo-anonymized identifying code were selected, given the need to specifically identify newly diagnosed cases. Data were extracted at both the national and regional levels.
Statistical Analysis
Crude rates were calculated as the number of cases per 1000 female population aged 15 to 50 residing in Italy [12] with a 95% CI assuming the binomial distribution. Rates were calculated for each year from 2010 to 2020
Starting from incidence data and as suggested in the FVG study [10], prevalence was calculated considering that endometriosis most commonly affects women during their reproductive years and tends to decrease after menopause. If (prevalence) = (incidence rate) x (average duration of the disease), and endometriosis is a chronic disease that lasts from diagnosis until at least menopause, incident cases will continue to accumulate until women reach menopause. We thus depicted the declining prevalence situation after menopause under the simplified assumption that menopause begins following a Gaussian curve with a mean of 51 years and a 95% confidence interval of ± 5 years (standard deviation=2.5). To further simplify, we assumed that all women would enter menopause between the ages of 45 and over and converted the probabilities from the Gaussian distribution to follow this assumption. Lastly, to represent the decline, lacking real data to base our decline in prevalence on, we arbitrarily decided that starting at age 45, each year, 20% of women entering menopause would cease to have the disease.
To validate the estimated incidence rate calculated by NHDB and understand how many cases are overlooked by this count due to not being hospitalized, a comparison was conducted in two regions: FVG and Puglia. In these regions, a local project integrated data from an administrative database with those coming from a pathological anatomy registry.
Results
During the period 2011-2020, 112,945 new diagnoses of endometriosis, confirmed through direct tissue visualization, were recorded for 134,667,646 women aged 15 to 50 resident in Italy. The incidence of endometriosis in Italy during this period was 0.839 (CI 95% 0.834-0.844) per 1000 women, displaying a significantly decreasing trend (p-value for trend <0.001), notably in the year 2020, likely due to reduced access to healthcare services caused by the SARS-CoV-2 pandemic (Figure 1). As expected, the incidence increases with age (Figure 2) and reaches its highest value in the age group between 31 and 35 years (1.21 per 1000 at the national level), with a similar trend in all regions. In terms of prevalence, it was estimated that 1,889,983 cases were prevalent during the period 2010-2020, resulting in a prevalence rate of 14.0 per 1000 over the same period. The age-specific prevalence rates follow an increasing trend, reaching a peak at 48 years of age.
Incidence rates are not homogeneous across Italian regions (Table 2). Over the years, a north-south gradient is observed, with generally higher rates in the northern regions (0.944 per 1000, 0.881 in the Northwest and 1.030 in the Northeast) compared to those in central (0.765 per 1000) and southern Italy (0.373 per 1000) The Islands, however, deviate from this pattern, displaying an incidence rate (0.906 x 1000) similar to that of the Northern Regions. All regions exhibit a decreasing trend, with a more significant decline in the northern and central regions of Italy. As expected, the same north-south geographical gradient is identifiable in the prevalence rates (Figure 3).
Sensitivity Analysis
The comparison between the incident cases identified by the NHDB and those identified in FVG and Puglia, which integrated the Regional Hospital Discharge Database with the pathological anatomy register, shows that, when information on pathological anatomy is added, higher estimates of 10% in FVG and 17% in Puglia are obtained (2225 vs 2441 incident cases identified in FVG; 7189 vs 8388 incident cases identified in Puglia).
Discussion
Principal Results
In this national retrospective, population-based study, it was possible to quantify for the first time the number of hospitalizations diagnosed with endometriosis in Italy. In the decade 2011-2020, 112,945 Italian women had a first diagnosis of this condition for an overall incidence rate of 0.84 per 1000. Over the years the values have decreased in almost all Italian regions. A north-south regional gradient was observed. The peak of incident cases was found in the 31-35 age group, and it was estimated that 14 out of 1000 women receive a diagnosis of endometriosis during childbearing age.
Strengths and Limitations
This is the first study that attempts to provide an estimate of the incidence and prevalence of endometriosis cases in Italy based on the single data source of hospitalizations, which are available over a long period throughout the country. The main strength of this study is the use of an administrative database available at national level which allowed to estimate the incidence and prevalence of endometriosis in Italy without differences in methods and definitions, to evaluate the time trend and to compare data by region.
The estimates provided are certainly an underestimate of the real burden of this pathology. In fact, it should be considered that administrative databases, such as the hospital discharge records database, only allow for the identification of a portion of endometriosis cases.
Interpretation and Comparison with Prior Work
The accurate evaluation of the real incidence and prevalence of endometriosis remains a difficult task. The use of hospital data at national level allows to produce estimates without differences in methods and definitions, to evaluate time trends and to compare regional data, but only identifies a limited number of cases. Several cases may not require hospitalization or receive a formal diagnosis, especially in young women, in case of good response to hormonal treatment [14,15]. Furthermore, the use of non-invasive diagnostic techniques, such as ultrasound and magnetic resonance imaging, may allow outpatients diagnosis of the condition. The reliability of these imaging techniques is becoming increasingly high and their use has been incorporated in the more recent guidelines [4,16]. Only the active search of the disease in unselected samples of women of reproductive age (i.e., using questionnaires investigating the presence of typical symptoms, followed by an adequate diagnostic path) can lead to accurate estimates of the prevalence and incidence of endometriosis. The result of the study by Ferrero et al. suggests that about 6 out of 10 cases of endometriosis had not been identified before the active search of the disease [17]. A small part of this gap can be filled through data linkage systems, as we saw in FVG and Puglia regions with the adding of data from the pathological anatomy records. Unfortunately, this data linkage is not possible for Italy on a national level.
Our estimates are based on the decision to assess them in women of reproductive age (between 15 and 50 years). This decision was taken for two reasons: 1) endometriosis affects mainly women in their fertile age. Symptoms are in fact strongly linked to the menstrual cycle, period in which the endometriotic tissue located outside the endometrium bleeds, causing swelling and inflammations; 2) to avoid the problem of possible overlap with the diagnosis of adenomyosis. Our national estimate consistent with the regional [10,18] and international estimates from other countries that have used the same data sources and age groups. [6,19].
An interesting result is the decreasing time trend of endometriosis diagnosed in hospital. The decreasing time trend of incidence and prevalence of endometriosis was also found in other countries [8,20,21]. This phenomenon can be explained by clinical reasons, i.e., the improvement in non-invasive diagnostic methods [4] with a consequent reduction in the number of hospital admissions related to the need for diagnosis, or the reduction in the use of laparoscopy in the diagnosis of infertility and the consequent reduction in the diagnosis of asymptomatic cases [22]. Furthermore, in Italy an increased attention was paid to endometriosis over the years at political, cultural and clinical level: several Italian Regions (i.e., Puglia, Campania, Friuli Venezia Giulia) set up observatories of endometriosis; since 2017 endometriosis was introduced into the Italian Essential Levels of Assistance (LEA) and included in the list of chronic and disabling diseases; the Italian Ministry of Health funded projects to evaluate incidence and pathogenic mechanisms of the disease; national on-line training initiatives for health professionals have been developed by the Italian National Agency for Regional Healthcare Services (AGENAS) together with awareness-raising initiatives for women [23]; from 2014 a Word Endometriosis Day was established, with awareness initiatives carried out throughout the country. The increased knowledge and awareness of the disease may have led to its earlier recognition by health professionals and to an early start of hormonal therapy without any hospital access.
In Italy, the geographical distribution of endometriosis shows a clear north-south gradient. This phenomenon has already been seen for other health conditions (i.e., the coverage of mammography or colorectal cancer screening) [24] and can be due to an underdiagnoses of the disease in the south region. Part of the explanation could be in the possible differentiated attention by regional governments and health services (which in Italy are regional) and in the imbalance of available resources (i.e., health spending per capita shows a similar north-south gradient, with lower resources available in south Italy regions [25]). The greater presence of the private healthcare sector and the lower presence of specialised endometriosis centres in southern Italian regions may further explain the loss of cases. To this, the effect of a different geographic structure of fertility in Italy could be added, which sees women residing in the central-northern regions having, on average, a higher age at childbirth and a greater number of children, especially in the early years of analysis [17]. Another hypothesis, which deserves further investigation, is that this gradient is also partly explained by the role of environmental factors. The literature hypothesizes a growing evidence of association between environmental pollutants and endometriosis [26,27,28], including in Italy [18]. Northern regions in Italy are known to have higher levels of exposure to environmental pollution. This hypothesis requires further investigation, which could be done through spatial analyses that take into account the possible pollutants present in the area versus those nearby.
Conclusions
This study allowed estimating the presence in Italy of approximately 176,000 women with a confirmed diagnosis of endometriosis. The number rises further when considering the limitations of this study, which only counts cases intercepted by hospital admissions. To assess the extent of this underestimation an active search of the disease in unselected samples of women of reproductive age is needed. This activity is ongoing in areas of three Italian regions (FVG, Toscana and Puglia) [17]. However, according to the hypothesis that only one-third of women with endometriosis reach a confirmed diagnosis [17], in Italy, there would be more than 500,000 women with this condition, demonstrating its significant burden on the population. On the other hand, the study of hospital admissions can provide information about the provision of healthcare services, and analysis using administrative data can be useful for improving healthcare planning in different regions.
Future developments in the analysis of the hospital discharge records database may include assessing the spatial distribution of endometriosis within each region to determine whether there are high-risk areas associated with specific environmental exposure profiles.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The study was funded by the Italian Ministry of Health, Finalized Research project ENDO-2021-12371967. “Development of a national epidemiological register on endometriosis based on administrative data and investigation of pathogenetic hypotheses”.
References
- Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020 Mar 26;382(13):1244-1256.
- As-Sanie S, Black R, Giudice LC, Gray Valbrun T, Gupta J, Jones B, et al. Assessing research gaps and unmet needs in endometriosis. Am J Obstet Gynecol. 2019 Aug;221(2):86-94. [CrossRef]
- Nnoaham KE, Hummelshoj L, Webster P, d'Hooghe T, de Cicco Nardone F, de Cicco Nardone C, Jenkinson C, et al.; World Endometriosis Research Foundation Global Study of Women's Health consortium. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. 2011 Aug;96(2):366-373.e8. [CrossRef]
- . Becker CM, Bokor A, Heikinheimo O, Horne A, Jansen F, Kiesel L, et al.; ESHRE Endometriosis Guideline Group. ESHRE guideline: endometriosis. Hum Reprod Open. 2022 Feb 6;2022(2):hoac009.
- Hudson N. The missed disease? Endometriosis as an example of 'undone science'. Reprod Biomed Soc Online. 2021 Aug 13;14:20-27.
- Abbas, S.; Ihle, P.; Köster, I.; Schubert, I. Prevalence and incidence of diagnosed endometriosis and risk of endometriosis in patients with endometriosis-related symptoms: findings from a statutory health insurance-based cohort in Germany. Eur J Obstet Gynecol Reprod Biol, 2012, 160, 79–83. [CrossRef]
- Rowlands IJ, Abbott JA, Montgomery GW, Hockey R, Rogers P, Mishra GD. Prevalence and incidence of endometriosis in Australian women: a data linkage cohort study. BJOG. 2021 Mar;128(4):657-665. [CrossRef]
- Ávalos Marfil A, Barranco Castillo E, Martos García R, Mendoza Ladrón de Guevara N, Mazheika M. Epidemiology of Endometriosis in Spain and Its Autonomous Communities: A Large, Nationwide Study. Int J Environ Res Public Health. 2021 Jul 25;18(15):7861.
- Sarria-Santamera A, Orazumbekova B, Terzic M, Issanov A, Chaowen C, Asúnsolo-Del-Barco A. Systematic Review and Meta-Analysis of Incidence and Prevalence of Endometriosis. Healthcare (Basel). 2020 Dec 30;9(1):29. [CrossRef]
- Morassutto C, Monasta L, Ricci G, Barbone F, Ronfani L. Incidence and Estimated Prevalence of Endometriosis and Adenomyosis in Northeast Italy: A Data Linkage Study. PLoS One. 2016 Apr 21;11(4):e0154227.
- Dunselman GA, Vermeulen N, Becker C, Calhaz-Jorge C, D'Hooghe T, De Bie B, Heikinheimo O, Horne AW, Kiesel L, Nap A, Prentice A, Saridogan E, Soriano D, Nelen W; European Society of Human Reproduction and Embryology. ESHRE guideline: management of women with endometriosis. Hum Reprod. 2014 Mar;29(3):400-12.
- ISTAT Popolazione residente [cited 2024 Feb 01]. Available from: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_POPRES1.
- Zhang S, Gong TT, Wang HY, Zhao YH, Wu QJ. Global, regional, and national endometriosis trends from 1990 to 2017. Ann N Y Acad Sci. 2021 Jan;1484(1):90-101. [CrossRef]
- Pino I, Belloni GM, Barbera V, Solima E, Radice D, Angioni S, et al.; “Endometriosis Treatment Italian Club” (ETIC”. "Better late than never but never late is better", especially in young women. A multicenter Italian study on diagnostic delay for symptomatic endometriosis. Eur J Contracept Reprod Health Care. 2023 Feb;28(1):10-16. [CrossRef]
- . Tu FF, Du H, Goldstein GP, Beaumont JL, Zhou Y, Brown WJ. The influence of prior oral contraceptive use on risk of endometriosis is conditional on parity. Fertil Steril. 2014 Jun;101(6):1697-704. [CrossRef]
- Taylor HS, Adamson GD, Diamond MP, Goldstein SR, Horne AW, Missmer SA, Snabes MC, Surrey E, Taylor RN. An evidence-based approach to assessing surgical versus clinical diagnosis of symptomatic endometriosis. Int J Gynaecol Obstet. 2018 Aug;142(2):131-142.
- Ferrero S, Arena E, Morando A, Remorgida V. Prevalence of newly diagnosed endometriosis in.
- women attending the general practitioner. Int J Gynaecol Obstet. 2010; 110:203–7. [CrossRef]
- Migliaretti G, Deltetto F, Delpiano EM, Bonino L, Berchialla P, Dalmasso P, et al. Spatial analysis of the distribution of endometriosis in northwestern Italy. Gynecol Obstet Invest. 2012;73(2):135-40. [CrossRef]
- Saavalainen L, Lassus H, But A, Tiitinen A, Härkki P, Gissler M, Heikinheimo O, Pukkala E. A Nationwide Cohort Study on the risk of non-gynecological cancers in women with surgically verified endometriosis. Int J Cancer. 2018 Dec 1;143(11):2725-2731. [CrossRef]
- Zhang S, Gong TT, Wang HY, Zhao YH, Wu QJ. Global, regional, and national endometriosis trends from 1990 to 2017. Ann N Y Acad Sci. 2021 Jan;1484(1):90-101. [CrossRef]
- Christ JP, Yu O, Schulze-Rath R, Grafton J, Hansen K, Reed SD. Incidence, prevalence, and trends in endometriosis diagnosis: a United States population-based study from 2006 to 2015. Am J Obstet Gynecol. 2021 Nov;225(5):500.e1-500.e9. [CrossRef]
- Motan T, Antaki R, Han J, Elliott J, Cockwell H. Guideline No. 435: Minimally Invasive Surgery in Fertility Therapy. J Obstet Gynaecol Can. 2023 Apr;45(4):273-282.e2. [CrossRef]
- Agenzia Nazionale per i Servizi Sanitari Regionali [cited 2024 Feb 01]. Available from: https://endometriosi.agenas.it/.
- Rapporto Osservasalute 2022[cited 2024 Feb 01]. Available from: https://osservatoriosullasalute.it/osservasalute/rapporto-osservasalute-2022.
- Agenzia per la Coesione Territoriale, Nucleo di verifica e controllo (NUVEC), La spesa in Sanità: i dati CPT per un’analisi in serie storica a livello territoriale, CPT Informa n. 3/2020 [cited 2024 Feb 01]. Available from:https://www.agenziacoesione.gov.it/wp-content/uploads/2020/09/CPT_Informa_Sanitax.pdf.
- Vallée A, Ceccaldi PF, Carbonnel M, Feki A, Ayoubi JM. Pollution and endometriosis: A deep dive into the environmental impacts on women's health. BJOG. 2023 Oct 9. Authors.
- Cano-Sancho G, Ploteau S, Matta K, Adoamnei E, Louis GB, Mendiola J, Darai E, Squifflet J, Le Bizec B, Antignac JP. Human epidemiological evidence about the associations between exposure to organochlorine chemicals and endometriosis: Systematic review and meta-analysis. Environ Int. 2019 Feb;123:209-223. [CrossRef]
- Upson K. Environmental risk factors for endometriosis: A critical evaluation of studies and recommendations from the epidemiologic perspective. Curr Epidemiol Rep. 2020 Sep;7(3):14. [CrossRef]
Figure 1.
Annual temporal trend of endometriosis incidence during the 2010–2020 period.
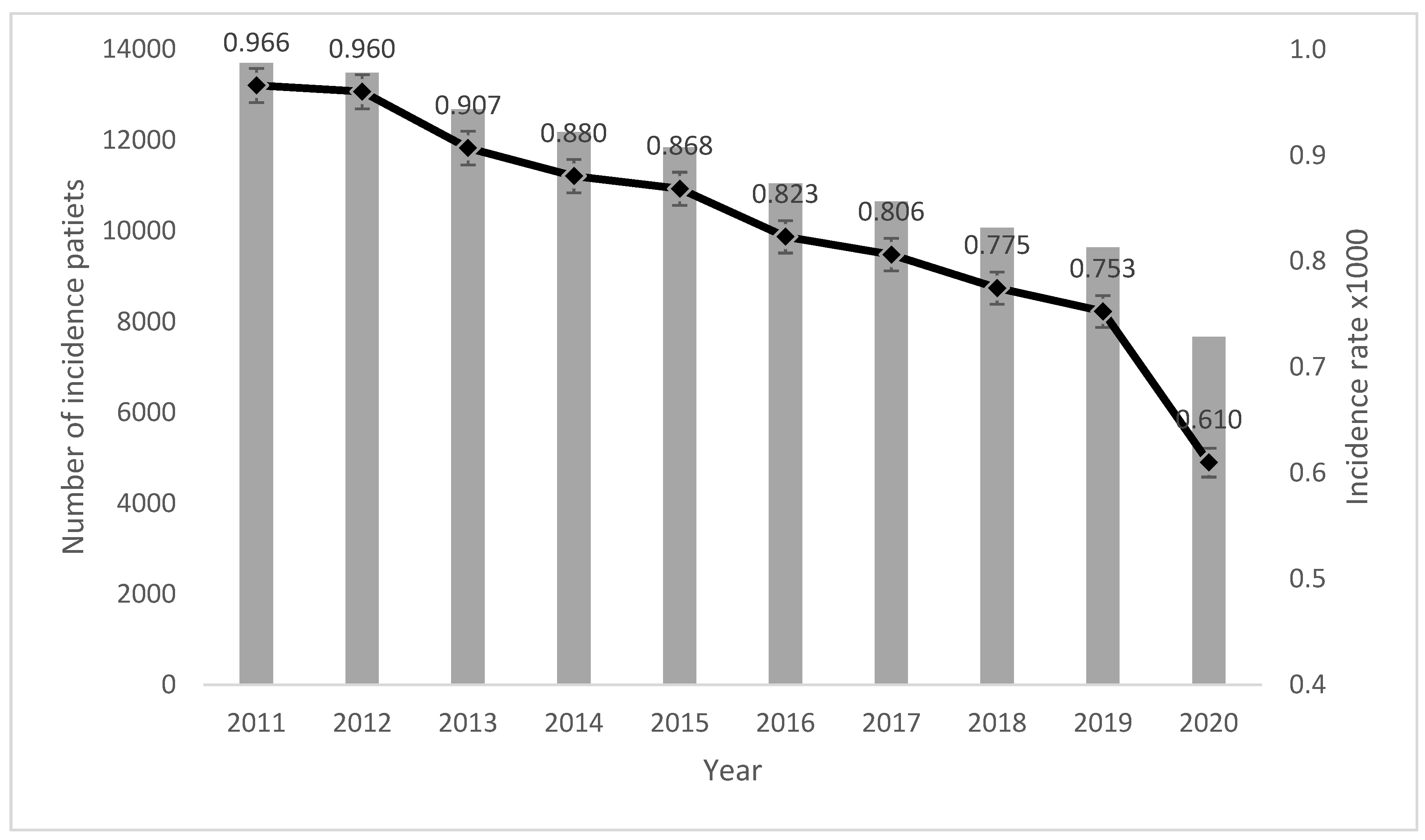
Figure 2.
Age-specific rate of incidence and prevalence of endometriosis during the 2010–2020 period.
Figure 2.
Age-specific rate of incidence and prevalence of endometriosis during the 2010–2020 period.
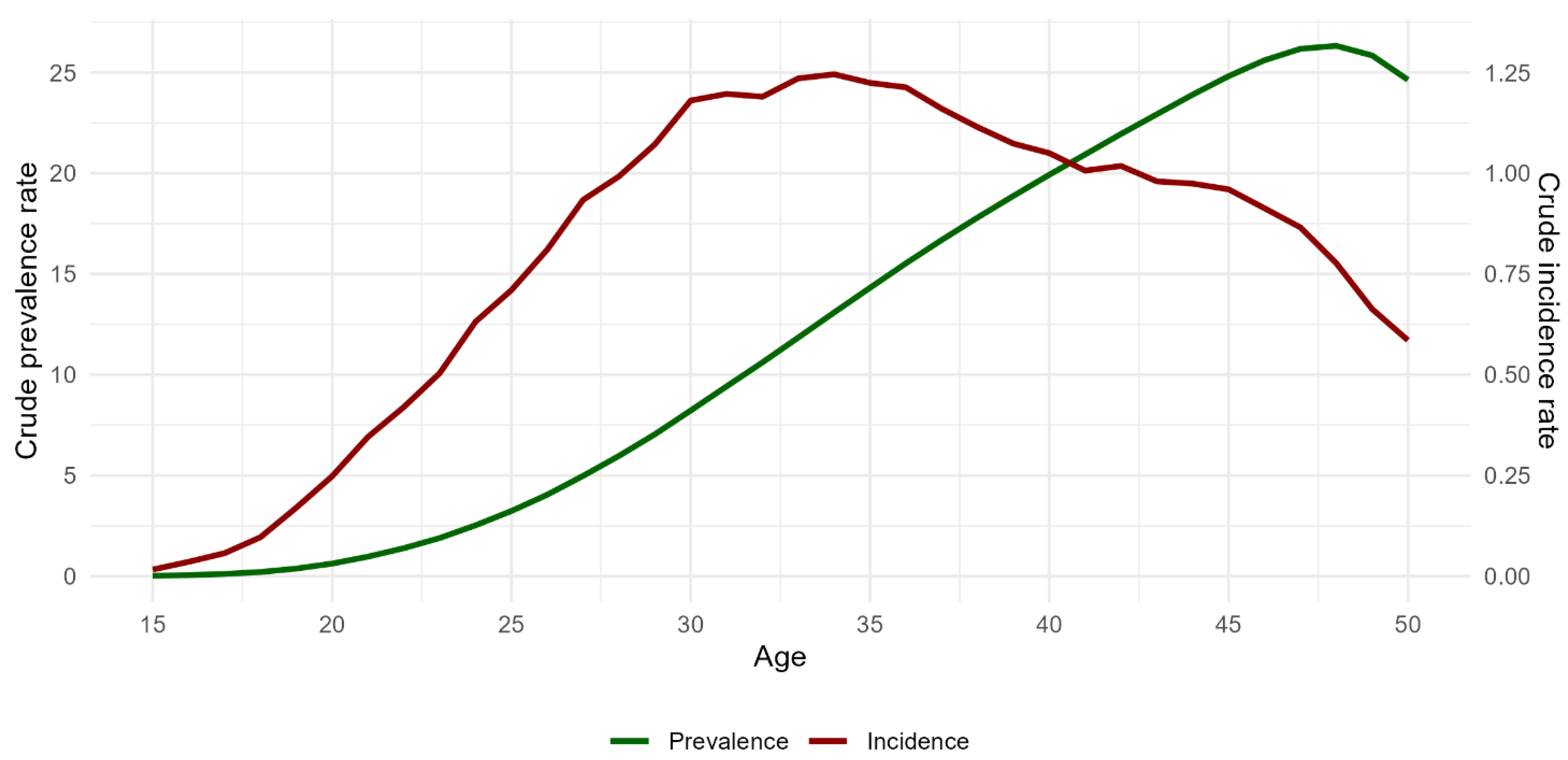
Figure 3.
Regional geographical distribution of incidence (a) and prevalence (b) rates, years 2010–2020.
Figure 3.
Regional geographical distribution of incidence (a) and prevalence (b) rates, years 2010–2020.
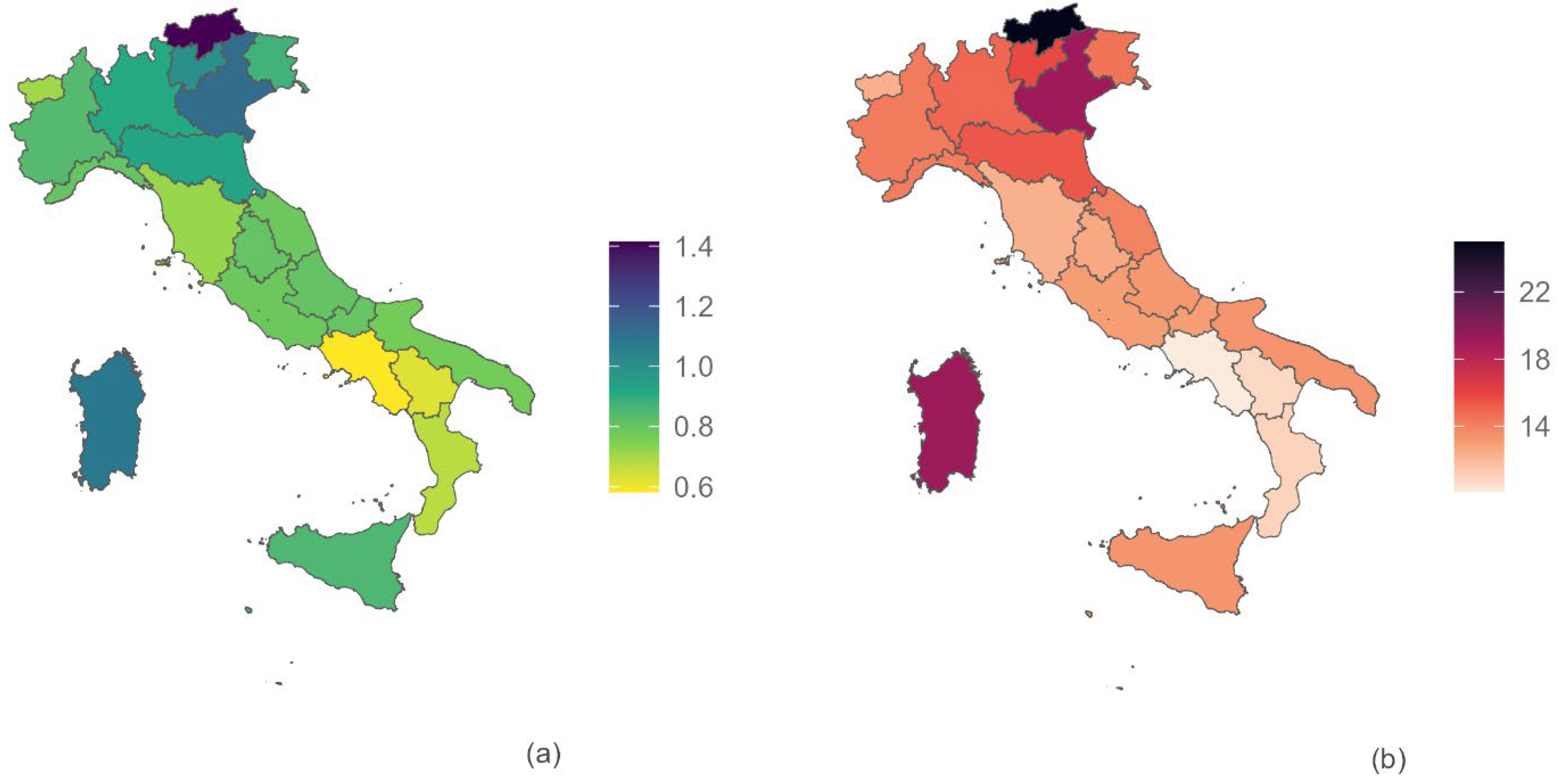

Table 1.
Codes for the selection of endometriosis in hospital discharge records.
| ICD-9-CM diagnosis code | AND | ICD-9-CM prodedure code |
| 617 or 617.0 or 617.1 or 617.2 or 617.3 or 617.4 or 617.5 or 617.6 or 617.8 or 617.9 | 34.81 or 37.34 or 45.23 or 45.24 or 45.26 or 45.62 or 45.72 or 45.76 or 45.94 or 46.04 or 46.11 or 46.21 or 47.01 or 47.19 or 47.99 or 48.62 or 48.63 or 48.69 or 48.82 or 49.39 or 51.23 or 54.11 or 54.12 or 54.19 or 54.21 or 54.23 or 54.24 or 54.4 or 54.51 or 54.59 or 54.73 or 55.51 or 56.74 or 56.99 or 57.32 or 57.6 or 57.99 or 59.00 or 59.02 or 59.03 or 65.01 or 65.12 or 65.13 or 65.23 or 65.24 or 65.25 or 65.29 or 65.31 or 65.41 or 65.49 or 65.51 or 65.52 or 65.53 or 65.54 or 65.61 or 65.62 or 65.63 or 65.74 or 65.79 or 65.81 or 65.89 or 65.91 or 65.99 or 66.19 or 66.29 or 66.39 or 66.4 or 66.51 or 66.52 or 66.61 or 66.62 or 66.63 or 66.69 or 67.39 or 67.4 or 68.12 or 68.13 or 68.14 or 68.15 or 68.16 or 68.29 or 68.39 or 68.41 or 68.49 or 68.51 or 68.59 or 68.61 or 68.69 or 68.71 or 68.9 or 69.19 or 69.29 or 70.32 or 70.77 or 86.3 or 87.83 or 97.83 |
Table 2.
Endometriosis incidence rate per 1000 women aged 15-50 years by region from the 2010-2020 period.
Table 2.
Endometriosis incidence rate per 1000 women aged 15-50 years by region from the 2010-2020 period.
| Region | Incidence annual rate x1000 | Total 2011-2020 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | n | rate | 95% CI | |||||
| Piemonte | 1,064 | 1,022 | 0,878 | 0,937 | 0,841 | 0,771 | 0,688 | 0,766 | 0,835 | 0,540 | 7810 | 0,840 | ( | 0,822 | - | 0,859 | ) |
| Valle D'Aosta | 0,549 | 0,587 | 1,247 | 0,876 | 0,679 | 0,657 | 0,746 | 0,495 | 0,775 | 0,395 | 194 | 0,705 | ( | 0,609 | - | 0,812 | ) |
| Lombardia | 1,118 | 1,068 | 1,001 | 0,942 | 0,941 | 0,930 | 0,945 | 0,856 | 0,687 | 0,597 | 20126 | 0,912 | ( | 0,900 | - | 0,925 | ) |
| Liguria | 0,964 | 1,051 | 0,958 | 0,853 | 0,721 | 0,778 | 0,758 | 0,532 | 0,754 | 0,561 | 2504 | 0,801 | ( | 0,770 | - | 0,833 | ) |
| Northwest | 1,085 | 1,050 | 0,966 | 0,932 | 0,892 | 0,872 | 0,859 | 0,801 | 0,732 | 0,577 | 30634 | 0,881 | ( | 0,871 | - | 0,891 | ) |
| PA Bolzano | 1,677 | 1,867 | 1,762 | 1,688 | 1,651 | 1,374 | 1,158 | 1,014 | 0,997 | 0,884 | 1706 | 1,414 | ( | 1,348 | - | 1,483 | ) |
| PA Trento | 1,259 | 1,051 | 1,149 | 1,212 | 1,001 | 0,888 | 0,797 | 0,943 | 0,993 | 0,689 | 1198 | 1,002 | ( | 0,946 | - | 1,060 | ) |
| Veneto | 1,208 | 1,212 | 1,144 | 1,159 | 1,211 | 1,182 | 1,035 | 1,060 | 1,049 | 0,879 | 12085 | 1,117 | ( | 1,098 | - | 1,138 | ) |
| Friuli-Venezia Giulia | 1,074 | 0,952 | 0,882 | 0,864 | 0,830 | 0,921 | 0,799 | 0,808 | 0,905 | 0,695 | 2225 | 0,876 | ( | 0,840 | - | 0,913 | ) |
| Emilia Romagna | 1,017 | 1,059 | 0,972 | 1,015 | 0,972 | 0,930 | 0,934 | 0,840 | 0,839 | 0,672 | 8963 | 0,928 | ( | 0,909 | - | 0,947 | ) |
| Northest | 1,147 | 1,151 | 1,082 | 1,102 | 1,093 | 1,055 | 0,968 | 0,943 | 0,949 | 0,772 | 26177 | 1,030 | ( | 1,017 | - | 1,042 | ) |
| Toscana | 0,938 | 0,885 | 0,804 | 0,791 | 0,683 | 0,607 | 0,596 | 0,668 | 0,646 | 0,495 | 5732 | 0,716 | ( | 0,698 | - | 0,735 | ) |
| Umbria | 0,837 | 0,981 | 1,001 | 0,976 | 0,901 | 0,722 | 0,736 | 0,661 | 0,651 | 0,492 | 1532 | 0,802 | ( | 0,763 | - | 0,844 | ) |
| Marche | 0,887 | 0,815 | 0,931 | 0,865 | 0,779 | 0,649 | 0,808 | 0,763 | 0,748 | 0,572 | 2616 | 0,785 | ( | 0,755 | - | 0,816 | ) |
| Lazio | 0,980 | 0,937 | 0,869 | 0,803 | 0,790 | 0,721 | 0,721 | 0,699 | 0,661 | 0,629 | 10346 | 0,784 | ( | 0,769 | - | 0,799 | ) |
| Centre | 0,945 | 0,909 | 0,867 | 0,820 | 0,764 | 0,678 | 0,695 | 0,695 | 0,667 | 0,572 | 20226 | 0,765 | ( | 0,754 | - | 0,776 | ) |
| Abruzzo | 0,780 | 0,872 | 0,916 | 0,830 | 0,888 | 0,802 | 0,743 | 0,860 | 0,746 | 0,584 | 2355 | 0,805 | ( | 0,773 | - | 0,838 | ) |
| Molise | 0,742 | 0,910 | 0,774 | 0,686 | 0,742 | 0,907 | 0,776 | 0,655 | 0,673 | 1,145 | 538 | 0,799 | ( | 0,733 | - | 0,869 | ) |
| Campania | 0,633 | 0,659 | 0,650 | 0,609 | 0,586 | 0,551 | 0,587 | 0,532 | 0,557 | 0,429 | 8155 | 0,582 | ( | 0,569 | - | 0,594 | ) |
| Puglia | 0,801 | 0,800 | 0,802 | 0,785 | 0,823 | 0,821 | 0,743 | 0,776 | 0,724 | 0,578 | 7189 | 0,768 | ( | 0,750 | - | 0,786 | ) |
| Basilicata | 0,571 | 0,849 | 0,706 | 0,649 | 0,616 | 0,574 | 0,683 | 0,608 | 0,513 | 0,442 | 799 | 0,625 | ( | 0,582 | - | 0,670 | ) |
| Calabria | 0,692 | 0,755 | 0,756 | 0,664 | 0,728 | 0,653 | 0,704 | 0,650 | 0,605 | 0,487 | 3031 | 0,673 | ( | 0,649 | - | 0,697 | ) |
| South | 0,702 | 0,744 | 0,737 | 0,690 | 0,705 | 0,673 | 0,669 | 0,652 | 0,628 | 0,508 | 22067 | 0,673 | ( | 0,665 | - | 0,682 | ) |
| Sicilia | 0,955 | 0,923 | 0,847 | 0,863 | 0,909 | 0,833 | 0,849 | 0,781 | 0,867 | 0,659 | 9899 | 0,851 | ( | 0,835 | - | 0,868 | ) |
| Sardegna | 1,174 | 1,219 | 1,147 | 1,056 | 1,176 | 1,122 | 1,085 | 1,012 | 0,945 | 0,812 | 3942 | 1,081 | ( | 1,048 | - | 1,115 | ) |
| Islands | 1,008 | 0,994 | 0,919 | 0,909 | 0,972 | 0,902 | 0,905 | 0,835 | 0,885 | 0,695 | 13841 | 0,906 | ( | 0,891 | - | 0,921 | ) |
| ITALY | 0,966 | 0,960 | 0,907 | 0,880 | 0,868 | 0,823 | 0,806 | 0,775 | 0,753 | 0,610 | 112945 | 0,839 | ( | 0,834 | - | 0,844 | ) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



