Submitted:
10 January 2024
Posted:
11 January 2024
You are already at the latest version
Abstract
Pediatric brain tumors are the most common solid tumors in children, causing the highest number of cancer-related deaths at young ages. Although existing therapies have improved the 5-year overall survival rate of PBT patients, some high-risk brain tumors continue to resist current treatments. Additionally, the survivors endure devastating long-term side effects, including cognitive defects and sensory and endocrinal dysfunctions. In the past two decades, immunotherapies have evolved significantly, with great success in many cancers. Immunotherapies developed specifically for PBTs also show promising results. Currently, scores of clinical trials are underway to evaluate the safety and feasibility of a wide-range of immunotherapeutics for PBTs, and this review overviews the most recent advances, including the exciting progress made toward treating medulloblastoma, pediatric glioma, and ependymoma. We summarized the cutting-edge immunotherapies under development, including immune checkpoint blockade, chimeric antigen receptor (CAR)-T cell therapy, natural killer (NK)-cell therapy, cancer vaccines, and oncolytic virus therapy. We find that the results from the recently concluded or ongoing clinical trials on safety and feasibility are very encouraging; however, non-responsiveness and tumor recurrence still haunt them. While this review judges the scope of the current immunotherapies, it also lays out strategies to find alternate solutions for persisting issues.
Keywords:
medulloblastoma
; pediatric glioma
; DIPG
; ependymoma
; immunotherapy
Pediatric brain tumors (PBTs), accounting for a staggering 25% of all childhood solid tumors, are the leading cause of cancer-related deaths in this age group [1]. With continued advancements in modern therapeutic approaches, the 5-year survival rate has been significantly improved in some PBTs (e.g., medulloblastoma (MB)). In general, the conventional medical procedure involves maximal surgical resection followed by craniospinal irradiation and adjuvant chemotherapy [2]. However, the long-term side effects resulting from this treatment, such as cognitive deficits, hearing loss, and endocrine dysfunction, significantly compromise the quality of life for PBT survivors [3]. Furthermore, the unamenable location of the tumors for surgery and their frequent metastasis make some PBTs (e.g., diffuse intrinsic pontine glioma, glioblastoma) more lethal than others [4,5]. Thus, these clinically unmet PBTs urgently warrant new therapeutic strategies, and the emerging state-of-the-art immunotherapies could fill this gap.
As our understanding of the immune system and molecular characteristics of tumors have significantly improved in the past decades, immunotherapies have achieved new heights with tremendous success in treating many cancers. The most common immunotherapies are immune checkpoint blockade, adoptive cell transfer, cancer vaccine, and oncolytic virus [6]. Immune checkpoint inhibitors (ICIs) are primarily antibodies that block PD-1, CTLA-4, or PD-L1, abrogating T-cell inhibition and enhancing anti-tumor activity [7]. Adoptive cell therapy refers to engineering and/or expanding ex vivo autologous immune cells (mostly T cells and NK cells) and transferring them to the host to enhance tumor cell killing [8]. Cancer vaccines destroy tumor cells by detecting tumor-associated antigens (TAAs) or tumor-specific antigens (TSAs) that are specifically expressed in tumor cells, while normal cells with little or no expression are spared. TAAs or TSAs could be loaded in dendric cells (DCs) or used as peptide-based vaccines to direct the immune system to kill tumor cells specifically [9]. Oncolytic viruses are engineered human or non-human viruses that specifically kill tumor cells by replicating in them, while they lack the ability to infect and kill normal cells [10]. These revolutionary strategies that are being developed to treat many cancers have also been continuously adapted to treat PBTs. Among the PBTs, the most common ones are low-grade gliomas (LGGs), high-grade gliomas (HGGs), ependymomas, and embryonal tumors (mostly MB), as per the World Health Organization (WHO) [11,12,13]. In this review, we overview the remarkable advances made in treating these PBTs with the game-changing new immunotherapeutic technologies, while we also discuss their pros and cons and the remaining challenges and weigh in their scope in PBT clinical use.
1. Medulloblastoma
Medulloblastoma is the most common pediatric malignant brain tumor, constituting 20% of all cases [14,15]. The incidence of this tumor is about 5 cases/million children with a median diagnostic age of 6 compared to only 0.5 cases/million in adults [16,17]. WHO classifies MB as a grade IV tumor and reports a 5-year survival rate of over 70% with current standard therapy that involves maximal surgical resection followed by risk-adapted craniospinal irradiation and adjuvant chemotherapy [18,19]. As mentioned above, such treatments usually lead to many undesirable long-term side effects, including neurocognitive impairment, hearing loss, and endocrine deficits [3].
Based on the molecular characteristics, MB is divided into four subgroups: Wingless-activated (WNT) (Group 1), Sonic Hedgehog-activated (SHH) (Group 2), and non-WNT/non-SHH (Groups 3 and 4) [19,20], which is further classified into 12 subgroups [21]. WNT subgroup accounts for ~10% of all MB cases and has the most favorable prognosis with a 5-year survival rate of 90% [22,23]. This subgroup is characterized by aberrant activation of the WNT pathway with mutations in genes CTNNB1 (encoding β-catenin) and APC [24]. SHH subgroup accounts for 25-30% of all MB cases. This subtype has a characteristic feature of activated SHH signaling with mutations and amplification of genes in the SHH pathway, such as loss-of-function mutations or deletions of protein patched homolog 1 (PTCH1) (43% of all SHH patients), SUFU negative regulator of hedgehog signaling (SUFU) (10%), smoothened (SMO) (9%), amplifications of transcription factors GLI1/2 (GLI1/GLI2) (9%) or MYCN proto-oncogene (MYCN) (7% of SHH patients) [25,26]. SHH subgroup has intermediate outcomes overall, but SHH patients harboring Tp53 mutation have the poorest prognosis with a 5-year survival rate of 40%, which prompts WHO to classify it as a very high-risk group [27,28]. Group 3 MB accounts for 25% of all MB cases. It has the worst prognosis among all subgroups, with an overall survival rate of 50%. 17% of group 3 patients have a characteristic MYC amplification. Other somatic mutations (e.g., SMRCA4, KBTBD4, CTDNEP1, and KMT2D) are rare, representing less than 10% of all patients. In addition, amplification of driver transcription factors, such as MYCN and OTX2, has also been reported [29]. Among all these mutations and amplifications, MYC amplification or overexpression of group 3 MB is associated with the poorest outcomes [21]. Group 4 MB accounts for 35% of all cases with an intermediate outcome. As with group 3, group 4 MB patients lack consensus mutations in particular genes similar to WNT and SHH. The most prevalent genetic alteration is the enhancer hijacking-induced overexpression of PRDM6 (~17%). Cytogenetically, group 4 MBs also feature high rates of isochromosome 17q (80%), loss of chromosomes 8 and 11, or a gain of chromosome 7 [29,30]. Similar to group 3, group 4 MBs also harbor amplification of MYCN, OTX2, and somatic mutations of KBTBD4 [29]. Recently, groups 3 and 4 have been further subdivided as types I to VIII based on a cohort containing 1,501 patients with group 3/4 [21,31,32]. Each subtype is driven by different molecular and cytogenetic events. Additionally, subtypes I, V, and VII have shared biological features of groups 3 and 4. Subtype II, III, and V are high-risk subtypes characterized by MYC/MYCN amplification.
1.1. ICI for MB
MB has a limited number of infiltrating PD-1+ T cells in the tumor microenvironment, and these tumor cells express low levels of PD-L1 across all subtypes in human samples (most cases <1%), suggesting that MB might not respond well to PD-1 checkpoint blockade [33]. In addition, the expression of the level of PD-L1 differs in subtypes, with SHH group showing the highest (<2%)[34,35]. However, this observation contradicts a study that used anti-PD-1 antibody to treat SHH and group 3 MB in mouse models and found that PD-1 blockade has better antitumor efficacy in mice that orthotopically transplanted with group 3 MB cells than those transplanted with SHH MB [36]. Moreover, it has also been reported that groups 3 and 4 tumors have higher cytotoxic lymphocytes [35,36]. These results could probably be explained by the alternative checkpoint pathways (e.g., B7H3) or different tumor microenvironments. SHH MB has also been reported to have higher infiltration of fibroblasts, T cells, and macrophages (including tumor-associated macrophages and myeloid-derived suppressor cells) [35,36]. In conclusion, whether MB patients could benefit from immune checkpoint inhibitors is still unclear. A better understanding of tumor heterogeneity and the tumor microenvironment may help redefine the therapy. Nevertheless, a phase 1b/2 study investigated nivolumab (NIVO) combined with ipilimumab (NIVO + IPI) in pediatric patients with high-grade CNS tumors and has just released their results (NCT03130959) (summarized in Table 1) [37]. The trial recruited five cohorts, including newly diagnosed diffuse intrinsic pontine glioma (DIPG), recurrent/progressive high-grade glioma, relapsed/resistant MB, relapsed/resistant ependymoma, and other recurrent/progressive CNS tumors. 14.1% of patients received NIVO, and 27.2% received NIVO + IPI showed grade 3/4 treatment-related adverse events. They further concluded that NIVO ± IPI did not show clinical benefit compared to historical data. Currently, a phase I clinical trial using pembrolizumab is underway, studying safety and dose in young patients with recurrent, progressive, or refractory high-grade gliomas, DIPG, hypermutated brain tumors, ependymoma or MB (NCT02359565), and the results are anxiously awaited.
In summary, ICI therapies for MB have not yet shown promising clinical outcomes, probably due to the cold tumor microenvironment with a low number of immune cell infiltration [38]. Based on early indications from related studies, we believe we can achieve better efficacy if ICI therapy is combined with another therapy, such as CAR T cell therapy or oncolytic virus therapy.
1.2. Chimeric Antigen Receptor (CAR)-T Cell and TCR Modificed T Cell Therapy for MB
Several targets in MB have been identified for developing CAR T cell therapy and mouse xenograft models have been used to test their efficacy. Here, we outline the notable developments that hold promise for treating MB. Human epidermal growth factor receptor 2 (HER2) CAR is the first to be tested in MB [39]. HER2, also known as ErbB2, is a receptor tyrosine kinase that belongs to the EGFR family. HER2 is expressed in about 40% of MB samples, contributing to poor prognosis [40]. Studies demonstrated that HER2 CAR T cells caused cytotoxicity in DAOY (SHH subtype), D283 (Group 4/3, no MYC amplification), and primary MB cells [39,41,42]. When DAOY and D283 xenograft mouse models were treated with HER2 CAR T cells, tumor cells were completely eliminated, and mouse survival was significantly extended [39,41]. The safety of intraventricular administration of HER2 CAR T cells was tested in non-human primates, given that an earlier report indicated that intravenous HER2 CAR T therapy for colon cancer metastatic patient showed on-target and off-tumor effects in lung epithelial cells [43]. The result showed that the immune response was restricted to the animals’ brains and not detectable in the peripheral region, a promising perspective on safety in humans [41].
PRAME, an antigen preferentially expressed in melanoma, was also expressed in MB [44]. About 80% of MB expressed PRAME when 60 samples comprising all four subgroups were tested [45]. PRAME-specific TCR-containing T cells (SLL TCR T cells) showed cytotoxicity towards HLA-A*02+ DAOY cells as well as primary MB cells. When evaluated in DAOY orthotopic xenograft models, treating with SLL TCR T cells significantly increased mouse survival rate [45].
B7H3 is a checkpoint molecule found in multiple pediatric tumors. Almost all MB samples (23/24) and cell lines express B7H3 [46,47,48]. Two SHH (DAOY and SJMBSHH-13-5634) and one group 3 MYC-amplified cell line (D425) xenografted mice model have been tested for B7H3 CAR T efficacy. All of them showed complete eradication of tumor cells, suggesting that this therapy could have promising efficacy in humans [47,48]. Currently, a phase I clinical trial is ongoing to evaluate the safety of using B7H3 CAR T cells in young patients with primary CNS tumors, including MB, high-grade glioma, glioblastoma, DIPG, ependymoma (NCT05835687).
Interleukin-13 receptor subunit alpha-2 (IL13Rα2) is a high-affinity monomeric receptor for Th2 cytokine IL-13. It has been found in the majority of MB tumor samples and cell lines [49,50]. First-generation CAR T cells (IL13-zetakine) containing IL13(E13Y) and CD3ζ showed almost complete regression of tumors in a preclinical DAOY MB orthotopic xenograft model [51]. A recent study compared 763 human MB and normal brain tissues, revealing that three CAR T cell targets (EPHA2, HER2, and IL-13Rα2), previously identified in glioblastoma, have also been recognized in group 3 MB. CAR T cells targeting all three (TRI-CAR) or EPHA2 (EPHA2-CAR) remarkably improved the survival of mice transplanted with group 3 MB cells [50]. Currently, a phase I clinical trial for IL13Rα2-targeting CAR T cell therapy is recruiting children with recurrent/refractory malignant brain tumors (NCT04510051).
Collectively, antigens that are upregulated in many solid tumors, such as breast cancer, melanoma, and other brain tumors, were also fortunately upregulated in MB, which helps accelerate CAR T cell therapy for this brain cancer. The early results are exciting; however, most of these studies are still in phase I clinical trials. The results obtained will have to be further tested in larger cohorts to determine the clinical outcomes conclusively.
1.3. Naural Killer (NK) Cell Therapy for MB
Unlike T cells, NK cells do not require specific tumor antigens to be presented on the surface of the MHC molecules. Instead, to identify target cells, they require “induced self” and “missing self” modes, which represent activating signals or inhibiting signals, respectively [52]. Expression of ligands for the NK group 2 member D activation receptor (NKG2D), including major histocompatibility complex class I-related chains A (MICA), UL16 binding protein (ULPB-2), and CD155, was found in MB patient samples and CD133+ (HTB-185 and 1603-MED) and CD133- (HTB-186) MB cell lines [53,54]. Not surprisingly, NK cells have lysis activity in MB cells, and blocking the inhibitory ligand MHC I potentiates the killing [54]. MB cell lines secrete high levels of TGF-β, which could impair NK cell function. To circumvent this problem, a modified NK cell expressing a dominant negative form of TGF-β receptor was developed and was shown to thwart impairment of cytotoxic activity [55]. NK cell targeting MB in vivo has also been tested in a DAOY cell xenograft model. Two doses of intratumoral administration of NK cells significantly reduced the tumor burden [56]. The results of a phase I clinical trial that used ex vivo expanded autologous NK cells to treat recurrent MB and ependymoma have just been published (NCT02271711) [57]. The study recruited 9 pediatric patients aged from 9 to 18 years. No dose-limiting toxicity was reported. However, after an initial remission, all patients eventually showed progressive disease after 3 cycles of 3 weekly infusions. One patient showed stable disease for one month at the end of follow-up, and one patient showed transient response after five infusions of NK cells before tumor progression. Despite these disappointing results, NK cells showed an increase of more than eleven-fold in the CSF after repetitive infusions. Thus far, the trial has demonstrated the safety and feasibility of ex vivo-produced and infused autologous NK cells while awaiting further modification of the strategy to improve efficacy. Another phase I/II clinical trial is ongoing using 177Lu-DTPA-omburtamab (antibody to B7-H3) to treat recurrent MB (NCT04167618). In a preclinical study, this antibody was shown to engage NK cells to kill cancer cells through antibody-dependent cellular cytotoxicity (ADCC) [58]. In sum, both preclinical and clinical studies showed tumor regression, indicating the feasibility of using NK cells to treat MB and ependymoma. The subsequent tumor recurrence is likely attributed to alterations in activating and inhibitory signals or the development of a suppressive tumor microenvironment (e.g., TGFβ). There is a critical need for further studies and refinement of the existing strategy to address these factors.
1.4. Vaccine Therapy for MB
Cancer vaccine therapies have also been explored to treat MB. One study tested autologous tumor lysate-loaded monocyte-derived DC, recruiting 45 children, including 33 high-grade gliomas (HGG), 5 MBs (MB)/primitive neuro-ectodermal tumor (PNET), 4 ependymoma, and 3 atypical teratoid-rhabdoid tumor (ATRT). The results demonstrated the safety and feasibility of the therapy. However, the authors couldn’t draw any definitive conclusions on whether there is clinical benefit to the patients because the study was limited to determining only the technical and clinical feasibility [59]. Nair et al. (2015) have developed RNA-loaded DCs to use as a vaccine [60]. Using personalized total tumor RNA-loaded DC and ex vivo-expanded autologous lymphocytes to treat MB patients are currently in Phase I and II clinical trials (NCT01326104).
1.5. Oncolytic Virus Therapy for MB
Oncolytic virus therapies have been developed from various viral sources, including Measles virus (MV), herpes simplex virus-1 (HSV-1), Poliovirus, Picornavirus, and Myxoma virus (MYXV), etc. For brain tumors, most of them were initially developed to treat malignant glioma; however, some of them showed promising results also in cell culture models and pre-clinical MB mouse models and entered clinical trials.
MV receptor CD46 has been found to be expressed on the cell surface of MB cell lines as well as tumor tissues from patients. Intratumoral treatment of MV therapy showed increased survival of mice orthotopically transplanted with D283 cells [61]. MV’s oncolytic activity has also been tested in a c-Myc and Gfi1b-overexpressing group 3 mouse model, which showed promising results [62]. A single intertumoral injection of MV resulted in complete tumor regression and prolonged animal survival compared to treatments with PBS or heat-inactivated MV [62]. Encouraged by the results, various modifications have been made to MV to improve its efficacy. For example, MV was modified to express the human thyroidal sodium iodide symporter (NIS) to trace the virus-infected tumor cells and concentrate the delivery of radioiodine to enhance the efficacy of oncolytic viruses. D283-transplanted mice treated with modified virus and radioiodine showed significantly prolonged survival than either virus- or radioiodine-treated group of mice [63]. Currently, a phase I study aiming to determine the safety and dose of MV-NIS in children and young adults is ongoing (NCT02962167). MV has also been engineered to express angiogenesis inhibitor protein endostatin and angiostatin. However, the effect of these modified viruses on D283-transplanted mice was not significantly different from that of non-modified ones [64].
Several strains of HSV-1 have been developed to treat brain tumors, considering their intrinsic neurotropism [65]. The γ134.5 principal virulence gene, necessary for the virus to replicate in normal cells but not tumor cells, is usually deleted in oHSV, allowing tumor cells to be specifically targeted while sparing normal cells [66]. oHSV G207 is generated by deleting both copies of γ34.5 and inserting a lacZ to viral ribonucleotide reductase (ICP6) [66]. A phase I clinical trial is ongoing to determine the safety of inoculating G207 into a recurrent or refractory cerebellar brain tumor (NCT03911388). M002 is also created by deleting the two copies of γ34.5 and, at the same time, expressing murine IL-12 [67]. Both viruses have been shown to infect CD133+ and CD15+ expressing MB cells D283 (Group 4/3, no MYC amplification), D341 (Group 3, MYC amplified), D384 (Group 3, MYC amplified), D425 (Group 3, MYC amplified) in vitro and in vivo. Mice orthotopically transplanted with either D341 or D425 showed superior survival when intratumorally injected with either of these viruses three days after tumor transplantation [68]. Another HSV-based oncolytic virus C134 has been developed, where again both copies of HSV’s γ34.5 have been knocked out and incorporated an IRS1 gene from cytomegalovirus to overcome the protein translation shut down caused by deleting the γ34.5 gene [69]. This virus was previously shown to be safe in both mice and non-human primates in pre-clinical assessments [70]. Human MB cells D283 (peritoneal metastatic MB cells) and D425 (group 3 MB) showed more than 10 times higher sensitivity towards C134 infection in vitro compared to mouse SHH and group 3 MB cells. An orthotopic transplanted mouse model showed advantages in survival in the C134-treated group. Single-cell RNA sequencing data indicated an enriched M1-like response in virus-treated tumor tissue [71]. rRp450 is another clinically available attenuated HSV-1 strain. It is deficient in the ICP6 gene. Unlike the oHSVs, rRp450 contains intact copies of the neurovirulence gene γ34.5 and harbors an insertion of rat CYP2B1 transgene, which encodes an enzyme responsible for activating the chemotherapeutic prodrug cyclophosphamide (CPA) and ifosfamide [72]. rRp450 has been proven to have oncolytic activity tested in D283 and D425 MB cell lines in vitro. When intratumorally injected into orthotopic mouse models of D283 and D425, the virus-treated group showed significantly prolonged survival compared to the control-treated group. Moreover, a study in AT/RT revealed that the addition of CPA significantly enhanced rRp450's in vivo efficacy. This study suggests that oncolytic herpes viruses with the ability to bioactivate the prodrug CPA merit further investigation as a potential therapy for pediatric brain tumors. [73].
PVSRIPO, a chimeric virus combining poliovirus and human rhinovirus type 2, is generated by exchanging the poliovirus internal ribosomal entry site with that of the human rhinovirus type 2, which resulted in deficient propagation in normal neuronal cells but kept its ability to grow in glial neoplasms [74]. Poliovirus receptor CD155 (PVR) has been found to be expressed in MB tissues, and its RNA level is significantly higher in group3γ, WNTα, and WNTβ compared to other subtypes. The expression of PVR in MB cell lines D283 and D341 has also been confirmed. But, PVSRIPO oncolytic activity has only been tested on D341 cells in vitro [75].
Picornavirus Seneca Valley virus-001 (SV-001) has been adapted to kill MB cells. This virus is not a human pathogen and has not been shown to associate with diseases in mice and rats [76], yet it can infect human cells. It is reported that SV-001 showed oncolytic activity towards neuroendocrine cancers and retinoblastoma [76,77]. A panel of 10 primary MB cells was tested for SVV-001 infection, and half of them were permissive to virus infection. Further study showed SVV-001 could infect CD133+ MB cancer stem cells and prevent neutrosphere formation. A single systemically administrated SVV-001 was able to pass BBB and infect orthotopic xenograft tumor cells, resulting in prolonged animal survival [78].
Myxoma virus (MYXV) is another promising oncolytic virus candidate. Like SVV-001, the myxoma virus is not a human pathogen. Normally, it only infects European rabbits and is not associated with any disease in all other vertebrate species tested, including humans [79]. When ten MB cell lines were tested, nine were susceptible to MYXV infection in vitro, and rapamycin enhanced MYXV replication and, thus, its oncolytic activity. Using D341 and DAOY cells orthotopic models, the authors showed that intratumoral injection of MYXV significantly prolonged animal survival, and this effect was further enhanced in the presence of rapamycin. Moreover, an added benefit of including rapamycin in the treatment is that it could reduce or eliminate spinal cord and ventricle metastases of DAOY tumor cells [80].
In summary, the preclinical data conducted thus far show promising results in PDX mouse models; however, only a few clinical trials have been conducted to evaluate the efficacy of oncolytic viruses against MB in patients.
2. Pediatric Glioma
Gliomas are the most common central nervous system (CNS) tumors in pediatric patients. The majority of pediatric gliomas are low-grade gliomas (LGGs) that are benign and slow-growing, and WHO classifies them as grades I and II. The rest are high-grade gliomas (HGGs), and WHO classifies them as grades III and IV because they develop and progress rapidly, and their clinical outcomes are extremely poor.
Pediatric low-grade gliomas (pLGGs) account for one-third of all pediatric CNS tumors [14]. They are a heterogeneous group of tumors, including pilocytic, pilomyxoid, subependymal giant cells, and diffuse astrocytomas [81]. They can arise from anywhere in the CNS, and the cerebellum is the most common location, followed by the cerebral hemispheres, deep midline structures, optic pathways, and brainstem [82]. WHO classifies them as grade I and grade II tumors [19]. The prognosis for these tumors is favorable, with a 10-year overall survival of 85%-96% [83,84]. The standard therapy for pLGG is complete surgical resection [85]. However, for those pLGGs where resection is not possible, chemotherapy is the first-line regimen [86]. Due to severe side effects, radiotherapy is generally saved for older patients or patients on whom surgery, chemotherapy, and targeted therapy have been exhausted [87]. Recent advances in genomic profiling showed that the majority of tumors harbor single identifiable driver alteration, which can be classified as RAS/MAPK pathway-related or non-RAS/MAPK pathway-related alterations. RAS/MAPK pathway alteration consisting of 70% of all sporadic pLGGs includes KIAA1549-BRAF, BRAF p.V600E, NF1 mutations, CRAF Fusions, etc. Non-RAS/MAPK-related alterations consist of MYB alterations, MYBL1 alterations, IDH1 Mutations, etc. [88,89,90,91]
Pediatric high-grade gliomas (pHGGs) are less common in children compared to adults. They account for around 10% of pediatric CNS tumors, yet they cause over 40% of all childhood brain tumor deaths [92,93]. The 5-year survival rate is less than 10% for patients with pHGGs and 1% for diffuse midline glioma (DMG; previously known as DIPG) H3 K27-altered [94]. Unlike their counterpart in adults, where it occurs mainly in the cerebral hemispheres, pHGGs can affect children anywhere in the CNS. Half of the pHGG cases occur in midline locations, particularly in the thalamus and the pons, which makes surgery impossible with poor prognosis [95]. Despite the children’s pHGGs having the same histology characteristics as adults’ HGGs, they harbor essentially different genetic alterations [96]. Three main types of pHGGs have been identified based on their molecular characteristics: histone H3 mutant (~40%), the isocitrate dehydrogenase gene (IDH) mutant, and the H3/IDH wildtype [97,98]. DIPGs, as defined by their name, are a group of aggressive tumors arising from the brainstem and pons and are usually considered separately from non-brainstem HGGs [81,93]. According to WHO classification, pediatric gliomas with a K27M mutation in histone H3 is classified as DMG H3 K27-altered, which includes more than 80% of DMGs [19,99].
2.1. ICI Therapy for Pediatric Glioma
Two retrospective studies evaluated ICI therapy targeting PD-1 or CTLA-4 on recurrent or refractory pediatric CNS tumors. The first study included 11 patients: 2 patients with DIPG, 5 with HGGs, 1 with ependymoma, 1 with craniopharyngioma, 1 with high-grade neuroepithelial tumor, and 1 with nongerminomatous germ cell tumor. All the patients received radiotherapy prior to ICI therapies. Ten of the eleven patients showed toxicity upon treatment, and six of them developed grade 3 or 4 toxicity, including rash, colitis, mucositis, type I diabetes, fatigue, infection/wound dehiscence, and transaminitis/hyperbilirubinemia. Two patients had to be discontinued from treatment due to grade 4 toxicity. During the treatment, three patients showed partial response, 7 showed stable disease, and one showed progressive disease. Due to the enhanced effectiveness observed, the authors determined that additional trials are warranted to assess the advantages of ICI therapy in pediatric CNS tumors, notwithstanding the noted toxicity [100]. The second retrospective study used nivolumab to treat pediatric recurrent or refractory brain tumors and demonstrated the safety of the therapy [101]. This study included 10 pediatric patients: 5 HGGs, 1 LGG, 1 MB, 1 ependymoma, 1 pineoblastoma, and 1 CNS embryonal tumor. No dose-limiting toxicity was reported. Three of the patients showed a partial response at the primary tumor site, and 2 of them eventually developed metastatic disease. The median survival for PD-L1-positive patients (13.7 weeks) was significantly longer than that for PD-L1-negative patients (4.2 weeks). The authors concluded that nivolumab is well tolerated in pediatric brain tumor patients and has a transient partial response in PD-L1-positive patients. Contradicting these findings, one clinical trial reported that NIVO ± IPI did not show significant clinical benefit compared to historical data (NCT03130959) [37]. Moreover, a separate clinical trial utilizing IDO (Indoleamine 2,3-dioxygenase, which helps to generate a tolerogenic milieu to suppress T cells and enhance Treg fuction) pathway inhibitor indoximod to treat newly diagnosed DIPG, enrolled 13 pediatric patients (NCT02502708). The results revealed that indoximod treatment was well tolerated and pharmacodynamic response were observed. Two patients showed an near complete responses for 7.6 and 13.3 months [102]. Taken together, these studies show ICI therapy is fairly tolerated in PBT patients, but the clinical benefit is inconclusive. Currently, a number of large prospective clinical trials are ongoing to evaluate the safety and efficacy of ICI therapy in treating pediatric CNS tumors including HGGs, DIPG, MB, ependymoma, hypermutated brain tumors etc. (NCT04323046, NCT02359565, NCT04049669)
2.2. CAR T Therapy for Pediatric Glioma
Similar to MB, several targets in pediatric glioma have been identified for developing CAR T cell therapy. Epidermal growth factor receptor splice variant III (EGFRvIII), which is the most common mutation of EGFR, is caused by a deletion of exons 2 to 7 of the EGFR gene [103]. Thus, as a neoantigen, EGFRvIII is considered a promising target for targeted cancer treatment since it is not expressed in normal tissues. It is reported that EGFRvIII is expressed in 17% (6/35) of pediatric high glioma samples and 6 out of 11 cases of pediatric DIPG samples [104,105]. A preclinical study showed increased animal survival in an orthotopic xenograft model [106]. The first human clinical trial of EGFRvIII CAR T cells treating recurrent glioblastoma recruited 10 adult patients, and the result showed that infusion of EGFRvIII CAR T cells was feasible and safe (NCT02209376). Of the seven patients evaluated, 5 showed antigen decrease after treatment. However, a robust expression of inhibitory molecules and regulatory T-cell infiltration have also been observed. These results indicate that tumor antigen heterogeneity and/or escape, as well as suppressive tumor microenvironment, may need to be addressed to improve the efficacy [107]. A clinical trial using EGFR806-specific CAR T cells (recognize both EGFRvIII and amplified EGFR [108]) locoregional immunotherapy for EGFR-positive recurrent or refractory pediatric CNS tumors is ongoing (NCT03638167).
HER2 is reported to be highly expressed in pHGG patient samples (~37%) [47]. In order to overcome the on-target off-tumor activity we mentioned above, studies have used HER2 CAR with an FRP5-based scFv. These HER-2 CAR T cells showed promising results in both glioblastoma and DIPG PDX models [109,110,111,112]. Notably, divalent CAR T combining HER2 and IL13Rα2 significantly improved the survival of the animals in the glioblastoma PDX model compared to single CAR T treatment while also mitigating antigen escape [109]. The evidence further suggests that trivalent CAR T combining HER2, IL13Rα2, and EphA2 could overcome interpatient variability and achieve superior efficacy compared to single and bivalent CAR [110]. A phase I clinical trial aimed at testing the safety of FRP5-based HER2-CAR VST cells (virus-specific T cells, redirected for HER2 recognition, proved to increase the persistence of the infused T cells [113]) therapy on 17 HGG patients, including 7 children/adolescent (NCT01109095). The results showed no severe adverse events, suggesting that the infusion of autologous HER2-CAR T cells is safe, and further clinical trials are needed to determine its clinical benefit [114]. Additionally, as mentioned above, intracranial injection of HER2 CAR T cells has also been safe in young patients with recurrent/refractory CNS tumors (NCT03500991) [115]. Currently, there is an ongoing clinical trial (NCT02442297) that employs HER2 CAR T cells for the treatment of recurrent or refractory brain tumors. Moreover, to address the heterogeneity of tumors, multiple CARs are being combined. For instance, a study (NCT05768880) is recruiting subjects with plans to utilize quadruple CAR T cells expressing combinations of B7-H3, EGFR806, HER2, and IL13-zetakine CAR for treating pediatric DIPG, DMG, and recurrent or refractory CNS tumors. Additionally, T cells targeting Tumor Antigen Associated (TAA) (WT1, PRAME and/or Survivin) are being utilized for the treatment of brain tumors in another clinical trial (NCT03652545).
IL13Rα2, as mentioned above, is a high-affinity monomeric receptor for Th2 cytokine interleukin-13. It is upregulated in various brain tumors, including over half of the HGGs, and its expression is associated with poor prognosis [116,117]. Given that IL13Rα2 is a receptor for IL13, a mutated IL13 (E13Y) was used instead of scFv to redirect the T cells for IL13Rα2 recognition, and at the same time reduce cross-activity to IL13Rα1. First-generation CAR T cells (IL13-zetakine) containing IL13(E13Y) and CD3ζ were developed and showed profound efficacy in a glioblastoma orthotopic model [118]. However, reaction to IL13Rα1 has been observed, raising concerns of off-target reactions [119]. A first-in-human clinical trial (NCT00730613) reported the safety and feasibility of using IL13(E13Y)-zetakine CTL for treating recurrent glioblastoma in adults. Intracranial administration of IL13(E13Y)-zetakine CTL to 3 patients was well tolerated, with two patients showing transient anti-glioma responses, which was consistent with short CAR T cell persistence. Of note, a reduced IL13Rα2 expression after CAR T treatment was observed, indicating antigen escaping [120]. A second generation of IL13(E13Y)-based CAR T containing 4-1BB (IL13BBζ) has been shown to improve the persistence and enrichment of the central memory T cells population [121]. A phase I clinical trial on IL13BBζ T cells is ongoing for treating recurrent or refractory malignant glioma (NCT02208362). While the full report is not yet available, one of the patients who received two doses of intracranial delivery of IL13BBζ T cells showed continued response and tumor regression for 7.5 months, suggesting promising outcomes are likely [122]. In order to reduce cross-reaction to IL13Rα1, membrane-bound IL13 was further mutated, generating YYB-103 CAR T cells, which showed higher selectivity for IL13Rα2 than IL13Rα1. Both i.c. and i.v. injection of YYB-103 CAR T cells prolonged animal survival in an orthotopic malignant glioma model [123]. In separate studies, anti-IL13Rα2 scFv-based CAR T cells have also been developed. IL13Rα2 CAR T cells with endodomains of either CD28ζ, 4-1BBζ, or CD28.OX40ζ all increased animal survival in a glioma xenograft model [124,125,126]. Additionally, given the heterogenous characteristic of glioma, bivalent and trivalent CAR containing HER2 and IL13Rα2, and HER2, EphA2, and IL13Rα2 have also been developed, as we discussed above.
Disialoganglioside (GD2) has been found on a wide variety of solid tumors, including neuroblastomas, melanomas, retinoblastomas, Ewing sarcomas, and gliomas [127]. GD2 expression has been found in 80% of glioma cell lines (N=20) and tumor biopsies (N=30) [128]. In addition, samples from DIPG patients express uniformly high levels of GD2 [129]. GD2-CAR T cell showed potent efficacy in 5 different H3-K27M+ DMG orthotopic xenograft models. However, due to some expression in normal cells, some of the GD2-CAR T cell-treated mice showed lethal hydrocephalus, which raised concerns of on-target off-tumor effects [129]. Combining GD2-CAR T with other therapies, including IL-15 or IGF1R/IR inhibitors, has shown superior efficacy in glioblastoma and DIPG mouse models [130,131]. Results of two phase I clinical trials of GD2-CAR T therapy for H3K27M+ DMG and glioblastoma have been published. Differing from the results from the mouse model, GD2-CAR T therapy was well tolerated, and on-target off-tumor toxicity was not observed (NCT04196413, NCT03170141). One study (NCT04196413) recruited 4 patients (3 with H3K27M-mutated DIPG, 1 with spinal cord DMG) aged between 5 and 25 years old. Three of them showed clinical and radiographic improvements. Increased pro-inflammatory cytokines, including IFNγ, TNF, IL-2, and IL-6, were found in the CSF when administrated through i.c.v. route compared to i.v injection, suggesting a local immune activation [132]. Addressing the concerns of safety, the second study (NCT03170141) developed a fourth-generation CAR (4SCAR), which included an inducible suicide caspase 9 gene. A total of 8 GD2+ GBM patients, with 4 under the age of 18, were recruited. Five out of eight patients showed partial response or stable disease [133]. Together, these results demonstrate the safety of i.v. and i.c infusion of GD2-CAR in both adults and pediatric patients. Due to the limited sample size, the clinical benefit awaits to be determined in further expanded trials. Clinical trials are currently underway, recruiting participants for the treatment of GD2-expressing brain tumors using modified GD2 CAR T cells (NCT04099797, NCT05298995).
In a B7H3 study comprising 388 pediatric solid tumors and brain tumors, the authors showed that 84% of HGGs and 100% of DIPG samples expressed B7H3 [48]. B7H3 expression in patients’ samples and cell lines of pHGG and DIPG has also been confirmed by other studies, and its expression level is correlated with WHO grading [134,135,136]. B7H3 CAR T cell treatment in a glioma PDX model, either systematically or intracranially, showed promising results of significantly prolonging survival and completely regressing tumors [47,135,136]. A first-in-human phase I clinical trial is ongoing to investigate the bioactivity and safety of intraventricular infusion of B7H3 CAR T cells for children and young adult DIPGs patients and recurrent or refractory pediatric CNS tumors (NCT04185038). The preliminary data of the first three DIPG patients showed no dose-limiting toxicities and local immune activation and persistence of B7H3 CAR T cells in cerebrospinal fluid (CSF), suggesting the feasibility of further clinical trials [137].
Ephrin type-A receptor 2 (EphA2) is a tyrosine kinase receptor of the ephrin receptor family. It has been reported that EphA2 is highly expressed in pediatric gliomas, and its expression level inversely correlates with the malignancy grade of the tumors [138]. In mouse PDX models, EphA2 CAR T cells showed promising efficacy in treating high-grade gliomas [139,140]. A preliminary report of a first-in-human trial of i.v. administrated EphA2 CAR T cells to 3 recurrent glioblastoma patients has been published (NCT03423992). Two of those patients showed grade 2 cytokine release syndrome, which resolved with dexamethasone medication. CAR T cells were found in both peripheral blood and CSF and persisted for more than four weeks. One patient showed a transient diminishing of the tumor [141]. Although these results support feasibility, all three patients recruited were adults, and further investigations in pediatric patients are necessary.
CD147, also known as extracellular matrix metalloproteinase inducer (EMMPRIN), is a glycoprotein belonging to the immunoglobulin superfamily, which is initially recognized as a regulator of matrix metalloproteinase. It is upregulated in pediatric gliomas compared to normal brain tissues, and its expression correlates with high-grade gliomas [142]. However, normal tissues still express low levels of CD147, such as epithelial and endothelial cells, and brain and heart tissues [143], which may explain why the phase I clinical trial was only available to adult patients with recurrent malignant glioma (NCT04045847).
In summary, many CAR T therapies targeting pediatric glioma are under phase I clinical trial. Among those whose preliminary data have been reported support safety and feasibility for further study. Antigen escape has also been noticed. Due to the limited sample sizes, the clinical benefits of these treatments need to be further determined in expanded clinical trials.
2.3. Vaccines for Pediatric Gliomas
Three types of vaccines are under development to treat pHGG: DC, peptide, and mRNA vaccines. DC vaccine is loaded with either autologous tumor cell lysates/RNA or cell lysates from other patients. One study recruited 45 children with recurrent malignant brain tumors, including 33 HGGs, and treated them with autologous tumor lysate-loaded DCs. Their results showed that HGG patients responded more favorably to vaccination than MB/PNET and ependymoma patients [59]. An additional clinical trial conducted with tumor lysate-pulsed DC and treating 3 newly diagnosed or recurrent pHGGs also showed safe and feasible outcomes. Two patients are alive 51 and 40 months after treatment, and one patient showed partial response, as seen from the MRI result (NCT00107185) [144]. Another study treated 9 newly diagnosed DIPG patients with autologous DCs loaded with allogeneic tumor cell-lines lysate (ATCL) composed of eight cells derived from five H3K27-mutated DIPG patients (NCT02840123). Anti-tumor responses were confirmed in both peripheral blood and CSF, indicating promising outcomes [145]. Currently, a phase I/II clinical trial is ongoing to use WT1 mRNA-loaded autologous monocyte-derived DCs as adjuvant therapy following previous therapies in pediatric patients with HGGs and DIPG (NCT04911621). Clinical trials which also using tumor RNA loaded DC to treat pHGGs and DIPG are ongoing (NCT03334305, NCT03396575). Collectively, all the published DC-based vaccines demonstrated safety and feasibility in pediatric patients. However, the clinical benefits still need to be evaluated in the future.
For developing peptide-based vaccines, three molecules IL13Rα2, EphA2, and survivin (glioma-associated antigens (GAAs)) were identified in the pediatric brain stem glioma and non-brain stem glioma samples, and almost all samples examined had a high-level expression of at least one of these molecules [146]. A phase I clinical trial is underway to evaluate the safety and immune response of using HLA-A2-restricted GGAs combined with poly-ICLC to treat pediatric gliomas (NCT01130077). Three reports have been published for treating newly diagnosed pediatric high-risk gliomas, recurrent low-grade gliomas, and recurrent HGGs. The first report recruited 26 pediatric patients aged from 2.2 to 17.9 years with newly diagnosed high-risk gliomas. No dose-related toxicity was reported following GAAs vaccination. During the first two vaccination courses, 19 patients showed stable disease, 2 patients showed partial response, and one had a minor response. Overall median survival was 13.3 months for brainstem gliomas and 25.5 months for HGG patients. Specific immune responses towards inoculated antigens of 21 patients using ELISPOT showed that 13 patients had positive responses to at least one of the three antigens [147]. A second trial used a peptide vaccine derived from GAAs to treat pediatric recurrent low-grade gliomas, recruiting 14 pediatric patients aged from 1.9 to 19.0 years. Two patients were excluded due to grade 3 urticaria and progressive disease. Except for urticaria, no regimen-limiting toxicity was reported. The overall survival rate was 100% over the average 42-month follow-up, and the median progression-free time was 9.9 months. ELISPOT assay showed all patients responded to at least one of the GAAs [148]. The third and most recent study was designed to evaluate GAAs peptide vaccine to treat pediatric recurrent HGGs. This trial recruited 12 pediatric patients aged from 2.3 to 23.3 years: 6 with glioblastoma, 5 with anaplastic astrocytoma, and one with malignant gliomatosis cerebri. No dose-limiting non-CNS toxicity was reported. The median overall survival was 12.9 months, and the median progression-free survival was 4.1 months. ELISPOT analysis showed that GAAs-specific response was detected in 9 patients [149]. Taking together, these trials demonstrate the safety and feasibility of using GAAs-derived peptide vaccines for pediatric brain tumors. Since these trials were the first trials in children, further evaluation in larger patient cohorts will be needed to determine the clinical benefits of this strategy.
H3.3K27M DIPG contains a K27M mutation in histone 3. Chheda et al. (2018) identified an HLA-A2-restricted epitope containing H3.3K27M mutation and a TCR that specifically recognizes the corresponding H3.3K27M epitope in glioma cells [150]. These data established a foundation for T cell-based therapy as well as H3.3K27M based vaccine therapy for patients with H3.3K27M+ glioma. However, whether the H3.3K27M epitope could be naturally processed in HLA-A*02:01 is still being debated [151]. Nonetheless, a phase I clinical trial is ongoing using H3.3K27M peptide vaccine combined with ICI (nivolumab) for treating pediatric patients with newly diagnosed DIPG and other gliomas (NCT02960230). This study recruited 19 DIPG and 10 nonpontine DMG pediatric patients. No grade 4 treatment-related adverse events were reported. The median overall survival for patients with a specific H3.3K27M CD8+ response (16.1 months) was significantly longer than that of the nonresponders (9.8 months) [152]. These data showed the H3.3K27M vaccine is well tolerated and showed some clinical benefits for H3.3K27M+ pediatric patients. Another clinical trial is recruiting to treat DIPG patients with H3.3-K27M neoantigen vaccine (NCT04749641).
While the HLA-restricted vaccines seem promising, only patients with specific HLA types could benefit from these therapies. The newly emerging RNA-based vaccines, successfully used against SARS-CoV-2 during the recent pandemic, could be available to all patient haplotypes. A phase I clinical trial is ongoing, which adapts autologous total tumor mRNA and pp65-LAMP (human cytomegalovirus phosphoprotein 65 RNA conjugated with lysosomal associated membrane protein RNA) mRNA-loaded DOTAP liposome vaccine to treat pediatric HGGs and adult glioblastoma (NCT04573140). However, this study is only recruiting adult patients now. Safety of RNA vaccine on pediatric patients will need further evaluation.
Collectively, three different types of vaccines are being developed, including DC-based, peptide-based, and mRNA vaccines. Published preliminary results on pediatric patients are available for the first two type of vaccines, which indicate acceptable safety and significant anti-tumor reaction. However, further trials with a larger number of patients will be needed to establish their clinical benefits.
2.4. NK cell Therapy for Pediatric Glioma
There is limited NK cell infiltration in pHGGs (~2% among immune cells), probably due to the immunosuppressive microenvironment containing TGFβ, IL-8, PD-L1, and B7-H3 [153,154]. In preclinical studies, ex vivo expanded NK cells showed promising outcomes in glioblastoma xenograft mouse models [155,156]. Further, retrovirally expressing a TGF-β-dominant-negative receptor II (DNRII) in NK cells was proven to maintain their cytotoxic activity towards glioblastoma cell line U87 in the presence of suppressing TGFβ [157]. Another preclinical study showed that glioblastoma stem cells (GSC) are sensitive to the treatment of allogeneic NK cells in vitro, and treating GSC-engrafted mice with allogeneic NK cells combined with inhibiting αv integrin/TGF-β1 axis prevented GSC-induced NK cell dysfunction and tumor growth [158]. All these preliminary preclinical data support the feasibility of clinical trials in evaluating NK cell therapies in pediatric glioma patients.
2.5. Oncolytic Virus Therapy for Pediatric Glioma
SVV-001, which efficiently kills MB cells, has also been used to treat pHGG. When tested infecting cells from six pediatric malignant glioma patients in vitro, SVV-001 infected and killed four of them. 6 PDX orthotopic xenograft mouse models were further generated, and 3 of them showed significant improvement in survival upon SVV-001 inoculation [159].
Newcastle disease virus (NDV) is a single-stranded virus that belongs to the paramyxovirus family. NDV infects poultry's respiratory, nervous, and digestive systems, but only causes minor flu-like symptoms in humans [160]. NDV has been widely used for targeting various cancers, including neuroblastoma, melanoma, lung, ovarian, stomach, pancreatic, colorectal cancers, etc., and some of them (e.g., melanoma) have already shown favorable results in clinical trials [161]. For pediatric glioma, three pediatric and one adult patients with recurrent glioblastoma were treated with oncolytic NDV (MTH-68/H) when conventional therapies failed. The treatment showed encouraging results with a significantly prolonged survival rate of 5 to 9 years [162]. Another study reported the treatment of a 12-year-old boy with anaplastic astrocytoma using MTH-68/H after conventional therapies failed. The tumor regressed significantly to 15% of its original size but reoccurred 4 months later [163]. Both studies showed safe and exciting clinical outcomes, encouraging further clinical trials with larger pediatric sample sizes.
Oncolytic HSV strain G207 has been shown to be safe with clinical benefits in treating adult recurrent glioblastoma patients [164,165,166]. 8 patient-derived pediatric high-grade tumor xenografts (4 MBs, 2 glioblastomas, 1 supratentorial PNET, and 1 ependymoma) were tested for their permissibility for G207 replication. The result showed that pediatric tumors were more sensitive to G207 treatment than their adult counterparts [167]. This result prompted the phase I clinical trial of using G207 to treat pediatric recurrent supratentorial malignant tumors (NCT02457845). Twelve patients aged from 7 to 18 years with HGG were recruited. Only grade I adverse events were reported. No virus shedding and viremia were detected. The median overall survival was 12.2 months. 18 months after G207 treatment, 4 out of 11 patients were still alive when last followed-up on June 5, 2020. Additionally, tumor-infiltrating lymphocytes were significantly increased upon G207 treatment. Taken together, this trial showed intratumoral G207 infusion was safe and offered clinical benefit to pHGG patients [168]. Two phase I clinical trials are currently in progress, investigating G207 for its efficacy in targeting pediatric recurrent or refractory cerebellar brain tumors, with or without irradiation (NCT03911388, NCT04482933). Another oHSV strain HSV1716, besides its tumor cell lytic activity, was also shown to inhibit the migration and invasion of pHGG and IDPG both in vitro and in vivo [169]. In addition, a phase I clinical trial using HSV1716 targeting refractory or recurrent HGGs after surgery in two pediatric patients has been completed, but the results have not been published yet (NCT02031965).
Delta-24-RGD (clinic name DNX-2401) is an adenovirus engineered to destroy cancer cells specifically. A 24-base pair deletion was introduced in the viral gene E1A, which allows the virus to replicate only in tumor cells with an aberrant RB pathway. It also harbors an additional RGD sequence (peptide sequences with arginine-glycine-aspartic acid (RGD) motif) that allows the virus to bind ανβ3 and ανβ5 integrins that are upregulated in various cancers [170,171]. This virus has a proven safety profile, and when tested in adult gliomas, it had a distinct therapeutic advantage [172]. Preclinical evidence on pHGG and DIPGs showed prolonged animal survival in both immunodeficient and immunocompetent models and, in addition, had powerful synergistic effect with radiotherapy [170,173]. A clinical trial of DNX-2401 for treating DIPG has been completed (NCT03178032) [174]. 12 patients with newly diagnosed DIPG aged from 3 to 18 years received viral particles, and 11 of them received subsequent radiotherapy. Three grade 3 adverse events (hemiparesis and neurologic deterioration) were reported in two patients. 9 patients showed reduced tumor size, 3 showed partial response, and 8 showed stable disease. The median survival was 17.8 months. Collectively, intratumoral infusion of DNX-2401 followed by radiotherapy is safe while reducing or stabilizing DIPG tumors in some patients, albeit with some reported adverse events. Another ongoing clinical trial (NCT04758533) is recruiting participants to explore the use of bone marrow-derived allogenic mesenchymal stem cells for delivering an adenovirus strain ICOVIR-5.
Another novel virus-based gene-mediated cytotoxic immunotherapy (GMCI) approach engineered an adenoviral vector to deliver a herpes virus thymidine-kinase gene (AdV-tk) to tumor cells, followed by killing the tumor cells with anti-herpetic prodrugs, which are the substrates for HSV-tk. In this strategy, AdV-tk is injected into the tumor site, and the tumor-killing effect is expanded to nearby cells through the spreading of activated prodrug [175]. A phase I dose-escalation study evaluated the safety of using GMCI combined with conventional therapies in treating pediatric malignant glioma and recurrent ependymoma (NCT00634231) [176]. The study recruited 8 pediatric patients, 6 with glioblastoma, 1 with anaplastic astrocytoma, and 1 with recurrent ependymoma. No dose-limiting toxicity was reported. Two glioblastoma and recurrent ependymoma patients survived for more than 24 months, with 2 alive without progression for 37.3 and 47.7 months after treatment. In conclusion, GMCI has been proven to be safe in pediatric patients with brain tumors when combined with radiation therapy with or without temozolomide, supporting further investigation to determine its clinical benefit.
Taken together, the reports mostly show promising results, demonstrating the potency in activating anti-tumor immune responses. At the same time, careful attention must be paid to the adverse side effects experienced by some candidates.
3. Ependymoma
Ependymomas are the third most common childhood CNS tumors [177]. They account for 6% of all pediatric brain tumors [178]. Pediatric ependymomas can arise in all compartments of the CNS, and the posterior fossa is the most prevalent location (~54.4%), followed by supratentorial sites (~32.5%) and the spine (~13.1%) [179,180]. The standard treatment for newly diagnosed non-metastatic pediatric ependymoma is complete resection of the tumor followed by local fractionated radiotherapy except for extremely young infants [181]. The 5-year overall survival rate of ependymomas is 50-81% [179]. The previous classification of ependymoma was based on its location and histology. As our understanding of the molecular characteristics of ependymoma has improved, WHO now classifies them into 10 subtypes according to their location, morphology, and molecular signatures. These subtypes can be broadly categorized into three groups based on the location: supratentorial, posterior fossa (PF), and spinal ependymoma (summarized in Table 2) [19,182]. For example, the subtypes of supratentorial ependymoma are based on their molecular signature, which include ZFTA fusion or YAP1 fusion-positive and others. Posterior fossa ependymoma contains group A (PFA), group B (PFB), and others based on their DNA methylation profiling [183]. In spinal ependymomas, a new subtype defined by MYCN amplification has been added [19,184].
3.1. ICI for Pediatric Ependymoma
In a phase I clinical trial (NCT02793466), pediatric patients with solid and CNS tumors were recruited to test the PD-L1 antibody durvalumab. The trial included 5 osteosarcoma, 4 ependymoma and 1 each of glioblastoma, astrocytoma, rhabdomyosarcoma, synovial sarcoma, hepatoblastoma and adrenocortical carcinoma. The results indicated the observation of only one event of dose-limiting toxicity. Notably, 3 out of 5 ependymoma patients exhibited clinical benefits [185]. Another clinical trial enrolled 22 ependymoma patients to assess the safety of NIVO ± IPI treatment, showing no unmanageable adverse events. However, clinical benefits were not observed in this cohort (NCT03130959) [37]. Currently, multiple ongoing clinical trials are assessing the safety and efficacy of ICI therapy for pediatric CNS tumors including HGGs, DIPG, MB, ependymoma, hypermutated brain tumors etc. (NCT04323046, NCT02359565, NCT03130959, NCT04049669)
3.2. CAR T Therapy for Pediatric Ependymoma
EphA2, HER2, and IL13Rα2 have been expressed in almost all pediatric ependymoma patient samples from the three subgroups (83/84, 77/84, 72/84). Mono-CARs and Tri-CAR were investigated for their efficacy in treating three PFA ependymomas in orthotopic PDX mouse models. The results showed that HER2 and TRI-CAR treatment profoundly improved animal survival [49]. Currently, two phase I clinical trials are ongoing to investigate the safety of adopting HER2 CAR T cells in treating pediatric ependymoma and pediatric CNS tumors, including ependymoma (NCT04903080, NCT03500991), and the latter one has published their interim results [115]. Three patients (2 ependymomas and 1 anaplastic astrocytoma) were recruited in this trial and subjected to locoregional delivery of HER2 CAR T therapy. No dose-limiting toxicity was reported. All three patients showed both clinical and laboratory evidence of local CNS immune activation, including high concentrations of CXCL10 and CCL2 in the CSF. This interim report indicated the safety and feasibility of repeated intra-CNS delivery of HER2 CAR T cells in pediatric and young adult patients.
B7H3 expression was also identified in ependymoma tumors, with a study revealing that all ependymoma samples demonstrated either medium or high levels of B7H3 expression. Moreover, elevated B7H3 mRNA levels were found to be associated with a shorter median survival [134]. Currently, a phase I clinical trial is underway to assess the safety of using B7H3 CAR T cells in the treatment of young patients with primary CNS tumors including MB, high grade glioma, glioblastoma, DIPG and ependymoma (NCT05835687).
3.3. Vaccines for Pediatric Ependymoma
Autologous tumor lysate-loaded DC treatment was tested by one study on 4 pediatric ependymoma patients. However, the results proved that the ependymoma patients did not have a favorable response to the vaccination, as seen with the HGG patients [59]. Glioma-associated antigens (GAAs) EphA2, IL13Rα2, and survivin were also found to be upregulated in pediatric ependymoma. Among 19 pediatric ependymoma samples examined, 84% had upregulated IL13Rα2, 95% EphA2, and 95% survivin [186]. Currently, a phase I clinical trial is ongoing to evaluate the safety of using peptide vaccine combined with immunoadjuvant imiquimod in pediatric recurrent ependymoma (NCT01795313). Another phase I clinical trial is also ongoing using SurVaxM (a peptide vaccine against survivin) targeting pediatric progressive or relapsed MB, HGGs, ependymoma, and newly diagnosed DIPG (NCT04978727).
Comparing to MB and pediatric glioma, research on ependymoma is limited, due to its rarity. Additionally, the scarcity of genetic and PDX models has hindered pre-clinical studies as highlighted in the review by Hwang et. al. [187]. Thus, more time and efforts are essential to advance the understanding of ependymoma.
4. Tumor Immune Microenvironment (TIME)
Tumor immune microenvironment (TIME) is a critical determinant in the effectiveness of immunotherapies. In fact, it has been shown that the nature of the TIME could be used to predict the host response and the success of immunotherapies [188,189].
4.1. Medulloblastoma TIME
Compared to other pediatric brain tumors, MB has fewer immune cell infiltration in the tumor microenvironment[35,189]. Also, the fewer infiltrating immune cells are largely heterogeneous among the four subgroups. For example, deconvolution of the sequencing data of large cohorts of patients revealed the immune composition of TIME in the subtypes as follows: (i) SHH tumors have the most numbers of T cells, fibroblast, and monocytic lineage cells, (ii) group 3 tumors have low levels of T cells and macrophages, but the highest number of CD8+ T-cells, and (iii) group 4 tumors have the highest number of cytotoxic lymphocytes [35]. Likewise, another study using DNA methylation data showed that group 3 tumors had more CD8+ T cells than group 4, group 4 tumors had the largest number of NK cell infiltration, and SHH tumors had the greatest infiltration of B cells. Additionally, results from SHH and group 3 MB tumor mouse models showed that SHH tumors had more myeloid-derived suppressor cells (MDSC), tumor-associated macrophages (TAMs), and CD4+ and CD8+ T cells. The group 3 tumor had more PD-1+ CD8+ T cells within the CD3+ population and showed better response to anti-PD-1 treatment [36]. Microglia is one of the major immune cells responsible for the immune surveillance of the brain. TAMs are known for their role in glioblastoma growth [190] and, therefore, TAMs’ role has also been explored, but the results were conflicting. Using an SHH MB mouse model (NeuroD2-SmoA1), Maximov et al. showed that TAMs had anti-tumor activity, as depleting TAMs resulted in promoting tumor growth [191]. Conversely, when Tan et al. decreased the number of TAMs in another SHH MB mouse model (Atoh1-SmoM2) using an inhibitor of colony-stimulating factor 1 receptor (CSF1R), it resulted in tumor regression and prolonged survival [192]. Another study evaluated the influence of depleting TAMs after irradiation in an SHH MB mouse model (Ptch1+/-Tp53-/-). Their results showed that reducing TAMs significantly promoted the CD8+ T cell population, indicating TAMs are immunosuppressive. However, they didn’t find survival benefits in these mice, which they attributed to increased neutrophils [193]. Collectively, medulloblastoma TIME is still inadequately studied, and the evidence thus far is inconsistent, probably due to the use of different datasets/algorithms or mouse models. Nonetheless, several immunotherapies have been tested on MB in preclinical models, and the outcomes are promising. Therefore, the future development of immunotherapies for medulloblastoma should first focus on clarifying the composition of TIME more accurately and designing therapies accordingly.
4.2. Pediatric Glioma TIME
Among gliomas, pLGG tumors exhibit more immune cell infiltration than pHGG tumors, with DIPG showing the least infiltration [194,195]. pLGG and pHGG samples display increased TAMs, CD3+, and CD8+ T cells compared to control tissues, but DIPG samples did not show such increases over normal tissues [195] [194,196,197]. pLGGs tend to have more myeloid cell infiltration than pHGGs, but variations in samples make it unclear [194,196,197]. Studies that used deconvolution analysis of sequencing data of larger cohorts as mentioned above confirmed that pLGGs had more monocytes infiltration (~35% of infiltrated cells) than pHGGs (~26% of non-cancer cells) [189]. This study also confirmed that pHGGs had fewer CD8+ T cell infiltration, which was even lower than that of MBs. Further, Treg cells (15%) and eosinophils (13%) were also among the most infiltrated immune cells in pHGGs. In addition, variations in immune cell types and numbers were also found in subtypes. Based on the classification by MacKay et al. of over 1000 pHGGs and DIPG patient data (WT-A, WT-B, WT-C, IDH, GBM G34, and GBM K27), it is showed that WT-A group had significantly higher infiltration of immune cells and monocytes than other groups, while GBM G34 mutations had lower number of infiltrated immune cells and eosinophils [97,189]. Interestingly, finding from DIPG was inconsistent with the IHC analysis where no changes in macrophages, T cells, and cytokines were seen [195,198]. Using CIBERSORT algorithm, an in silico study showed that DIPG tumors had more CD4+ Treg cells, eosinophils, DCs, and neutrophils, and fewer CD8+ T cells, NK cells, M1 cells, and activated mast cells compared to pediatric hemisphere HGG tumors [199]. Thus, the TIME of DIPG is unclear and further in-depth studies are needed to clarify the immune composition. In summary, pLGGs that have more immune cells infiltration, consistent with their favorable prognosis, are considered immunologically “hot” tumors. pHGGs that have fewer CD8+ T cells infiltration and significant TAMs and Treg cells infiltration are considered as having an immune suppressive environment. DIPG tumors are considered as “cold” tumors, but awaits further confirmation.
4.3. Ependymoma TIME
A study using flow cytometry and analyzing 7 pilocytic astrocytoma (PA, low-grade glioma), 19 ependymoma, 5 glioblastoma (GBM), 6 MB, and 5 nontumor brain control showed that PA and ependymoma tumors contained more activated HLA-DR and CD64-positive myeloid cells and lymphoid cells compared to GBM, MB, and control. This observation indicates ependymoma is relatively immunologically active [200]. An in silico study, using CIBERSORT and xCell, confirmed the infiltration of M2-like macrophages, activated NK cells, T follicular helper cells, CD4+ memory T cells, and B cells [201]. Yet another study analyzed the gene expression changes during recurrence and found that posterior fossa subgroups A (PFA) had an immunosuppressive phenotype associated with tissue remodeling and wound healing, while PFB had an activated adaptive immunity and increased T-cell infiltration [202]. Furthermore, using multi-omics data of PFA ependymoma (represents 70% of all pediatric ependymoma) [182], Griesinger et al. identified a subgroup of hypoxia myeloid cells that had the features of myeloid-derived suppressive cells, which could contribute to the immune suppressive microenvironment [203]. Overall, evidence shows that ependymoma tumors have a significant infiltration of immune cells with an immunosuppressive microenvironment.
5. Future Directions and Prospective
Developing immunotherapies for PBTs is likely to be high-powered in the near future. Beside the common issues we encountered when adopting immunotherapies to treat solid tumors, such as tumor heterogeneity and suppressive TME, the unique location of the tumors and distinct composition of the tumor environment of the developing brain present unique challenges, contributing to unresponsiveness and tumor recurrence and making developing PBT therapies more formidable and challenging. For example, pre-clinical studies showed that CAR T cell treatments were more effective when inoculated intratumorally or intracranially compared to intravenously injection. Moreover, since a lot of the immunotherapies are previously developed for adult brain tumors, the different tumor characteristics and TME between pediatric and adult patients should also be considered when developing immunotherapies for PBTs [204,205,206].
Moreover, while various immunotherapies have been employed across different pediatric brain tumors, each approach has its own role in promoting tumor immune surveillance (Figure 1). However, they also have specific limitations which could eventually lead to the nonresponsiveness and recurrence. ICI therapies, notably effective in tumors with higher mutation rates, may encounter limitations in pediatric brain tumors with lower mutation burdens. CAR T cells, designed to target tumor-specific antigens on the cell surface, face challenges associated with tumor heterogeneity. Despite efforts to enhance target coverage by combining different CARs, comprehensive coverage of all tumor cells is not guaranteed. Cancer vaccines encounter similar challenges tied to tumor heterogeneity, coupled with the risk of inefficient induction of antigen-specific immune responses and limited effector cell infiltration into the tumor site. Oncolytic viruses face issues with a high level of pre-existing neutralizing antibodies and development of adoptive anti-virus responses. Immunotherapies can take lessons from the wildly successful HIV therapy Highly Active Antiretroviral Therapy (HAART). HAART contains a combination of drugs targeting different viral life cycles and has been proven to increase the efficacy and reduce the chance of the virus developing resistance [207]. Thus, combining different anti-tumor therapies may increase the potency and, at the same time, reduce the likelihood of tumor recurrence. For example, combining low-dose irradiation and CAR T therapies was shown to enhance CAR T efficacy and mitigate antigen escape in pancreatic adenocarcinoma [208]. Likewise, combining oncolytic virus and immune checkpoint inhibitors increased the responsiveness compared to ICI treatment alone [209]. Another example showed that CAR T cells recognizing multiple targets could also overcome the heterogeneity in neuroblastoma [210]. Future directions should focus on advancing our knowledge of tumorigenesis and immune surveillance in the unique environment of the developing brain, and future drugs should be designed accordingly for more effective and safe treatment of pediatric brain tumors. At the same time, combining therapeutic approaches appears to be more promising to eradicate brain tumors in children.
Funding
This research received no external funding.
Conflicts of Interest
No conflict of interest.
References
- Heath, J.A., S. Zacharoulis, and M.W. Kieran, Pediatric neuro-oncology: current status and future directions. Asia Pac J Clin Oncol, 2012. 8(3): p. 223-31. [CrossRef]
- Lutz, K., S.T. Jünger, and M. Messing-Jünger, Essential Management of Pediatric Brain Tumors. Children (Basel), 2022. 9(4). [CrossRef]
- Chevignard, M., et al., Core deficits and quality of survival after childhood medulloblastoma: a review. Neurooncol Pract, 2017. 4(2): p. 82-97. [CrossRef]
- Lah, T.T., M. Novak, and B. Breznik, Brain malignancies: Glioblastoma and brain metastases. Semin Cancer Biol, 2020. 60: p. 262-273. [CrossRef]
- Aziz-Bose, R. and M. Monje, Diffuse intrinsic pontine glioma: molecular landscape and emerging therapeutic targets. Curr Opin Oncol, 2019. 31(6): p. 522-530. [CrossRef]
- Liu, C., et al., Clinical cancer immunotherapy: Current progress and prospects. Front Immunol, 2022. 13: p. 961805. [CrossRef]
- Seidel, J.A., A. Otsuka, and K. Kabashima, Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front Oncol, 2018. 8: p. 86. [CrossRef]
- Kalos, M. and C.H. June, Adoptive T cell transfer for cancer immunotherapy in the era of synthetic biology. Immunity, 2013. 39(1): p. 49-60. [CrossRef]
- Lin, M.J., et al., Cancer vaccines: the next immunotherapy frontier. Nat Cancer, 2022. 3(8): p. 911-926. [CrossRef]
- Shalhout, S.Z., et al., Therapy with oncolytic viruses: progress and challenges. Nat Rev Clin Oncol, 2023. 20(3): p. 160-177. [CrossRef]
- Louis, D.N., et al., The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol, 2021. 23(8): p. 1231-1251. [CrossRef]
- Louis, D.N., et al., The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol, 2016. 131(6): p. 803-20. [CrossRef]
- Fangusaro, J. and P. Bandopadhayay, Advances in the classification and treatment of pediatric brain tumors. Curr Opin Pediatr, 2021. 33(1): p. 26-32. [CrossRef]
- Ostrom, Q.T., et al., CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011-2015. Neuro Oncol, 2018. 20(suppl_4): p. iv1-iv86. [CrossRef]
- Rossi, A., et al., Medulloblastoma: from molecular pathology to therapy. Clin Cancer Res, 2008. 14(4): p. 971-6. [CrossRef]
- Northcott, P.A., et al., Medulloblastoma. Nature Reviews Disease Primers, 2019. 5(1): p. 11. [CrossRef]
- Smoll, N.R. and K.J. Drummond, The incidence of medulloblastomas and primitive neurectodermal tumours in adults and children. J Clin Neurosci, 2012. 19(11): p. 1541-4. [CrossRef]
- Gajjar, A., et al., Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol, 2006. 7(10): p. 813-20. [CrossRef]
- Louis, D.N., et al., The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro-Oncology, 2021. 23(8): p. 1231-1251. [CrossRef]
- Taylor, M.D., et al., Molecular subgroups of medulloblastoma: the current consensus. Acta Neuropathol, 2012. 123(4): p. 465-72. [CrossRef]
- Cavalli, F.M.G., et al., Intertumoral Heterogeneity within Medulloblastoma Subgroups. Cancer Cell, 2017. 31(6): p. 737-754 e6. [CrossRef]
- Manoranjan, B., et al., Wnt activation as a therapeutic strategy in medulloblastoma. Nat Commun, 2020. 11(1): p. 4323. [CrossRef]
- Sursal, T., et al., Molecular Stratification of Medulloblastoma: Clinical Outcomes and Therapeutic Interventions. Anticancer Res, 2022. 42(5): p. 2225-2239. [CrossRef]
- Thompson, M.C., et al., Genomics identifies medulloblastoma subgroups that are enriched for specific genetic alterations. J Clin Oncol, 2006. 24(12): p. 1924-31. [CrossRef]
- Kool, M., et al., Genome sequencing of SHH medulloblastoma predicts genotype-related response to smoothened inhibition. Cancer Cell, 2014. 25(3): p. 393-405. [CrossRef]
- Menyhart, O. and B. Gyorffy, Principles of tumorigenesis and emerging molecular drivers of SHH-activated medulloblastomas. Ann Clin Transl Neurol, 2019. 6(5): p. 990-1005. [CrossRef]
- Zhukova, N., et al., Subgroup-specific prognostic implications of TP53 mutation in medulloblastoma. J Clin Oncol, 2013. 31(23): p. 2927-35. [CrossRef]
- Ramaswamy, V., et al., Risk stratification of childhood medulloblastoma in the molecular era: the current consensus. Acta Neuropathol, 2016. 131(6): p. 821-31. [CrossRef]
- Northcott, P.A., et al., The whole-genome landscape of medulloblastoma subtypes. Nature, 2017. 547(7663): p. 311-317. [CrossRef]
- Choi, J.Y., Medulloblastoma: Current Perspectives and Recent Advances. Brain Tumor Res Treat, 2023. 11(1): p. 28-38. [CrossRef]
- Sharma, T., et al., Second-generation molecular subgrouping of medulloblastoma: an international meta-analysis of Group 3 and Group 4 subtypes. Acta Neuropathol, 2019. 138(2): p. 309-326. [CrossRef]
- Kumar, R., A.P.Y. Liu, and P.A. Northcott, Medulloblastoma genomics in the modern molecular era. Brain Pathol, 2020. 30(3): p. 679-690. [CrossRef]
- Vermeulen, J.F., et al., Prognostic relevance of tumor-infiltrating lymphocytes and immune checkpoints in pediatric medulloblastoma. Oncoimmunology, 2018. 7(3): p. e1398877. [CrossRef]
- Martin, A.M., et al., PD-L1 expression in medulloblastoma: an evaluation by subgroup. Oncotarget, 2018. 9(27): p. 19177-19191. [CrossRef]
- Bockmayr, M., et al., Subgroup-specific immune and stromal microenvironment in medulloblastoma. Oncoimmunology, 2018. 7(9): p. e1462430. [CrossRef]
- Pham, C.D., et al., Differential Immune Microenvironments and Response to Immune Checkpoint Blockade among Molecular Subtypes of Murine Medulloblastoma. Clin Cancer Res, 2016. 22(3): p. 582-95. [CrossRef]
- Dunkel, I.J., et al., Nivolumab with or without ipilimumab in pediatric patients with high-grade CNS malignancies: Safety, efficacy, biomarker, and pharmacokinetics-CheckMate 908. Neuro Oncol, 2023. 25(8): p. 1530-1545. [CrossRef]
- Eisemann, T. and R.J. Wechsler-Reya, Coming in from the cold: overcoming the hostile immune microenvironment of medulloblastoma. Genes Dev, 2022. 36(9-10): p. 514-532. [CrossRef]
- Ahmed, N., et al., Regression of experimental medulloblastoma following transfer of HER2-specific T cells. Cancer Res, 2007. 67(12): p. 5957-64. [CrossRef]
- Gajjar, A., et al., Clinical, histopathologic, and molecular markers of prognosis: toward a new disease risk stratification system for medulloblastoma. J Clin Oncol, 2004. 22(6): p. 984-93. [CrossRef]
- Nellan, A., et al., Durable regression of Medulloblastoma after regional and intravenous delivery of anti-HER2 chimeric antigen receptor T cells. J Immunother Cancer, 2018. 6(1): p. 30. [CrossRef]
- Ivanov, D.P., et al., In vitro models of medulloblastoma: Choosing the right tool for the job. J Biotechnol, 2016. 236: p. 10-25. [CrossRef]
- Morgan, R.A., et al., Case report of a serious adverse event following the administration of T cells transduced with a chimeric antigen receptor recognizing ERBB2. Mol Ther, 2010. 18(4): p. 843-51. [CrossRef]
- Epping, M.T. and R. Bernards, A causal role for the human tumor antigen preferentially expressed antigen of melanoma in cancer. Cancer Res, 2006. 66(22): p. 10639-42. [CrossRef]
- Orlando, D., et al., Adoptive Immunotherapy Using PRAME-Specific T Cells in Medulloblastoma. Cancer Res, 2018. 78(12): p. 3337-3349. [CrossRef]
- Li, S., et al., Pediatric medulloblastoma express immune checkpoint B7-H3. Clin Transl Oncol, 2022. 24(6): p. 1204-1208. [CrossRef]
- Haydar, D., et al., Cell-surface antigen profiling of pediatric brain tumors: B7-H3 is consistently expressed and can be targeted via local or systemic CAR T-cell delivery. Neuro Oncol, 2021. 23(6): p. 999-1011. [CrossRef]
- Majzner, R.G., et al., CAR T Cells Targeting B7-H3, a Pan-Cancer Antigen, Demonstrate Potent Preclinical Activity Against Pediatric Solid Tumors and Brain Tumors. Clin Cancer Res, 2019. 25(8): p. 2560-2574. [CrossRef]
- Donovan, L.K., et al., Locoregional delivery of CAR T cells to the cerebrospinal fluid for treatment of metastatic medulloblastoma and ependymoma. Nature Medicine, 2020. 26(5): p. 720-731. [CrossRef]
- Donovan, L.K., et al., Locoregional delivery of CAR T cells to the cerebrospinal fluid for treatment of metastatic medulloblastoma and ependymoma. Nat Med, 2020. 26(5): p. 720-731. [CrossRef]
- Stastny, M.J., et al., Medulloblastomas Expressing IL13Rα2 are Targets for IL13-zetakine+ Cytolytic T Cells. Journal of Pediatric Hematology/Oncology, 2007. 29(10): p. 669-677. [CrossRef]
- Wu, S.Y., et al., Natural killer cells in cancer biology and therapy. Mol Cancer, 2020. 19(1): p. 120. [CrossRef]
- Castriconi, R., et al., Both CD133+ and CD133- medulloblastoma cell lines express ligands for triggering NK receptors and are susceptible to NK-mediated cytotoxicity. Eur J Immunol, 2007. 37(11): p. 3190-6. [CrossRef]
- Fernández, L., et al., In vitro Natural Killer Cell Immunotherapy for Medulloblastoma. Front Oncol, 2013. 3: p. 94. [CrossRef]
- Powell, A.B., et al., Medulloblastoma rendered susceptible to NK-cell attack by TGFβ neutralization. J Transl Med, 2019. 17(1): p. 321. [CrossRef]
- Kennis, B.A., et al., Monitoring of intracerebellarly-administered natural killer cells with fluorine-19 MRI. J Neurooncol, 2019. 142(3): p. 395-407. [CrossRef]
- Khatua, S., et al., Phase I study of intraventricular infusions of autologous ex vivo expanded NK cells in children with recurrent medulloblastoma and ependymoma. Neuro Oncol, 2020. 22(8): p. 1214-1225. [CrossRef]
- Vallera, D.A., et al., NK-Cell-Mediated Targeting of Various Solid Tumors Using a B7-H3 Tri-Specific Killer Engager In Vitro and In Vivo. Cancers (Basel), 2020. 12(9). [CrossRef]
- Ardon, H., et al., Adjuvant dendritic cell-based tumour vaccination for children with malignant brain tumours. Pediatr Blood Cancer, 2010. 54(4): p. 519-25. [CrossRef]
- Nair, S.K., et al., Ex vivo generation of dendritic cells from cryopreserved, post-induction chemotherapy, mobilized leukapheresis from pediatric patients with medulloblastoma. J Neurooncol, 2015. 125(1): p. 65-74. [CrossRef]
- Studebaker, A.W., et al., Treatment of medulloblastoma with a modified measles virus. Neuro Oncol, 2010. 12(10): p. 1034-42. [CrossRef]
- Lal, S., et al., An oncolytic measles virus–sensitive Group 3 medulloblastoma model in immune-competent mice. Neuro-Oncology, 2018. 20(12): p. 1606-1615. [CrossRef]
- Hutzen, B., et al., Treatment of medulloblastoma using an oncolytic measles virus encoding the thyroidal sodium iodide symporter shows enhanced efficacy with radioiodine. BMC Cancer, 2012. 12: p. 508. [CrossRef]
- Hutzen, B., et al., Treatment of medulloblastoma with oncolytic measles viruses expressing the angiogenesis inhibitors endostatin and angiostatin. BMC Cancer, 2014. 14: p. 206. [CrossRef]
- Friedman, G.K., et al., Herpes simplex virus oncolytic therapy for pediatric malignancies. Mol Ther, 2009. 17(7): p. 1125-35. [CrossRef]
- Mineta, T., et al., Attenuated multi-mutated herpes simplex virus-1 for the treatment of malignant gliomas. Nat Med, 1995. 1(9): p. 938-43. [CrossRef]
- Parker, J.N., et al., Engineered herpes simplex virus expressing IL-12 in the treatment of experimental murine brain tumors. Proc Natl Acad Sci U S A, 2000. 97(5): p. 2208-13. [CrossRef]
- Friedman, G.K., et al., Pediatric medulloblastoma xenografts including molecular subgroup 3 and CD133+ and CD15+ cells are sensitive to killing by oncolytic herpes simplex viruses. Neuro Oncol, 2016. 18(2): p. 227-35. [CrossRef]
- Cassady, K.A., Human cytomegalovirus TRS1 and IRS1 gene products block the double-stranded-RNA-activated host protein shutoff response induced by herpes simplex virus type 1 infection. J Virol, 2005. 79(14): p. 8707-15. [CrossRef]
- Cassady, K.A., et al., Pre-clinical Assessment of C134, a Chimeric Oncolytic Herpes Simplex Virus, in Mice and Non-human Primates. Mol Ther Oncolytics, 2017. 5: p. 1-10. [CrossRef]
- Hedberg, J., et al., Oncolytic virus-driven immune remodeling revealed in mouse medulloblastomas at single cell resolution. Mol Ther Oncolytics, 2023. 30: p. 39-55. [CrossRef]
- Chase, M., R.Y. Chung, and E.A. Chiocca, An oncolytic viral mutant that delivers the CYP2B1 transgene and augments cyclophosphamide chemotherapy. Nature Biotechnology, 1998. 16(5): p. 444-448. [CrossRef]
- Studebaker, A.W., et al., Oncolytic Herpes Virus rRp450 Shows Efficacy in Orthotopic Xenograft Group 3/4 Medulloblastomas and Atypical Teratoid/Rhabdoid Tumors. Mol Ther Oncolytics, 2017. 6: p. 22-30. [CrossRef]
- Gromeier, M., et al., Intergeneric poliovirus recombinants for the treatment of malignant glioma. Proc Natl Acad Sci U S A, 2000. 97(12): p. 6803-8. [CrossRef]
- Thompson, E.M., et al., Poliovirus Receptor (CD155) Expression in Pediatric Brain Tumors Mediates Oncolysis of Medulloblastoma and Pleomorphic Xanthoastrocytoma. J Neuropathol Exp Neurol, 2018. 77(8): p. 696-702. [CrossRef]
- Reddy, P.S., et al., Seneca Valley virus, a systemically deliverable oncolytic picornavirus, and the treatment of neuroendocrine cancers. J Natl Cancer Inst, 2007. 99(21): p. 1623-33. [CrossRef]
- Wadhwa, L., et al., Treatment of invasive retinoblastoma in a murine model using an oncolytic picornavirus. Cancer Res, 2007. 67(22): p. 10653-6. [CrossRef]
- Yu, L., et al., A single intravenous injection of oncolytic picornavirus SVV-001 eliminates medulloblastomas in primary tumor-based orthotopic xenograft mouse models. Neuro Oncol, 2011. 13(1): p. 14-27. [CrossRef]
- McFadden, G., Poxvirus tropism. Nat Rev Microbiol, 2005. 3(3): p. 201-13. [CrossRef]
- Lun, X.Q., et al., Targeting human medulloblastoma: oncolytic virotherapy with myxoma virus is enhanced by rapamycin. Cancer Res, 2007. 67(18): p. 8818-27. [CrossRef]
- Pollack, I.F., S. Agnihotri, and A. Broniscer, Childhood brain tumors: current management, biological insights, and future directions. J Neurosurg Pediatr, 2019. 23(3): p. 261-273. [CrossRef]
- Freeman, C.R., J.P. Farmer, and J. Montes, Low-grade astrocytomas in children: evolving management strategies. Int J Radiat Oncol Biol Phys, 1998. 41(5): p. 979-87. [CrossRef]
- Krishnatry, R., et al., Clinical and treatment factors determining long-term outcomes for adult survivors of childhood low-grade glioma: A population-based study. Cancer, 2016. 122(8): p. 1261-9. [CrossRef]
- Bandopadhayay, P., et al., Long-term outcome of 4,040 children diagnosed with pediatric low-grade gliomas: an analysis of the Surveillance Epidemiology and End Results (SEER) database. Pediatr Blood Cancer, 2014. 61(7): p. 1173-9. [CrossRef]
- Shaw, E.G. and J.H. Wisoff, Prospective clinical trials of intracranial low-grade glioma in adults and children. Neuro Oncol, 2003. 5(3): p. 153-60. [CrossRef]
- Ater, J.L., et al., Nonrandomized comparison of neurofibromatosis type 1 and non-neurofibromatosis type 1 children who received carboplatin and vincristine for progressive low-grade glioma: A report from the Children's Oncology Group. Cancer, 2016. 122(12): p. 1928-36. [CrossRef]
- de Blank, P., et al., Management of pediatric low-grade glioma. Curr Opin Pediatr, 2019. 31(1): p. 21-27. [CrossRef]
- Zhang, J., et al., Whole-genome sequencing identifies genetic alterations in pediatric low-grade gliomas. Nat Genet, 2013. 45(6): p. 602-12. [CrossRef]
- Jones, D.T., et al., Oncogenic RAF1 rearrangement and a novel BRAF mutation as alternatives to KIAA1549:BRAF fusion in activating the MAPK pathway in pilocytic astrocytoma. Oncogene, 2009. 28(20): p. 2119-23. [CrossRef]
- Pfister, S., et al., BRAF gene duplication constitutes a mechanism of MAPK pathway activation in low-grade astrocytomas. J Clin Invest, 2008. 118(5): p. 1739-49. [CrossRef]
- Ryall, S., U. Tabori, and C. Hawkins, Pediatric low-grade glioma in the era of molecular diagnostics. Acta Neuropathol Commun, 2020. 8(1): p. 30. [CrossRef]
- Cole, B.L., Neuropathology of Pediatric Brain Tumors: A Concise Review. Neurosurgery, 2022. 90(1): p. 7-15. [CrossRef]
- Ostrom, Q.T., et al., CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014-2018. Neuro Oncol, 2021. 23(12 Suppl 2): p. iii1-iii105. [CrossRef]
- Blionas, A., et al., Paediatric gliomas: diagnosis, molecular biology and management. Ann Transl Med, 2018. 6(12): p. 251. [CrossRef]
- Jones, C. and S.J. Baker, Unique genetic and epigenetic mechanisms driving paediatric diffuse high-grade glioma. Nature Reviews Cancer, 2014. 14(10): p. 651-661. [CrossRef]
- Thorbinson, C. and J.P. Kilday, Childhood Malignant Brain Tumors: Balancing the Bench and Bedside. Cancers (Basel), 2021. 13(23). [CrossRef]
- Mackay, A., et al., Integrated Molecular Meta-Analysis of 1,000 Pediatric High-Grade and Diffuse Intrinsic Pontine Glioma. Cancer Cell, 2017. 32(4): p. 520-537.e5. [CrossRef]
- Thorbinson, C. and J.-P. Kilday, Childhood Malignant Brain Tumors: Balancing the Bench and Bedside. Cancers, 2021. 13(23): p. 6099. [CrossRef]
- Damodharan, S., et al., Diffuse Intrinsic Pontine Glioma: Molecular Landscape, Evolving Treatment Strategies and Emerging Clinical Trials. J Pers Med, 2022. 12(5). [CrossRef]
- Cacciotti, C., et al., Immune checkpoint inhibition for pediatric patients with recurrent/refractory CNS tumors: a single institution experience. J Neurooncol, 2020. 149(1): p. 113-122. [CrossRef]
- Gorsi, H.S., et al., Nivolumab in the Treatment of Recurrent or Refractory Pediatric Brain Tumors: A Single Institutional Experience. J Pediatr Hematol Oncol, 2019. 41(4): p. e235-e241. [CrossRef]
- S. Johnson, T., et al., IMMU-04. FIRST-IN-CHILDREN PHASE 1B STUDY USING THE IDO PATHWAY INHIBITOR INDOXIMOD IN COMBINATION WITH RADIATION AND CHEMOTHERAPY FOR CHILDREN WITH NEWLY DIAGNOSED DIPG (NCT02502708, NLG2105). Neuro-Oncology, 2021. 23(Supplement_1): p. i27-i27. [CrossRef]
- Kim, H.M., et al., The epidermal growth factor receptor variant type III mutation frequently found in gliomas induces astrogenesis in human cerebral organoids. Cell Prolif, 2021. 54(2): p. e12965. [CrossRef]
- Bax, D.A., et al., EGFRvIII deletion mutations in pediatric high-grade glioma and response to targeted therapy in pediatric glioma cell lines. Clin Cancer Res, 2009. 15(18): p. 5753-61. [CrossRef]
- Li, G., et al., Expression of epidermal growth factor variant III (EGFRvIII) in pediatric diffuse intrinsic pontine gliomas. J Neurooncol, 2012. 108(3): p. 395-402. [CrossRef]
- Johnson, L.A., et al., Rational development and characterization of humanized anti-EGFR variant III chimeric antigen receptor T cells for glioblastoma. Sci Transl Med, 2015. 7(275): p. 275ra22. [CrossRef]
- O'Rourke, D.M., et al., A single dose of peripherally infused EGFRvIII-directed CAR T cells mediates antigen loss and induces adaptive resistance in patients with recurrent glioblastoma. Sci Transl Med, 2017. 9(399). [CrossRef]
- Ravanpay, A.C., et al., EGFR806-CAR T cells selectively target a tumor-restricted EGFR epitope in glioblastoma. Oncotarget, 2019. 10(66): p. 7080-7095. [CrossRef]
- Hegde, M., et al., Tandem CAR T cells targeting HER2 and IL13Rα2 mitigate tumor antigen escape. J Clin Invest, 2016. 126(8): p. 3036-52. [CrossRef]
- Bielamowicz, K., et al., Trivalent CAR T cells overcome interpatient antigenic variability in glioblastoma. Neuro Oncol, 2018. 20(4): p. 506-518. [CrossRef]
- Shen, L., et al., The efficacy of third generation anti-HER2 chimeric antigen receptor T cells in combination with PD1 blockade against malignant glioblastoma cells. Oncol Rep, 2019. 42(4): p. 1549-1557. [CrossRef]
- Wang, S.S., et al., HER2 chimeric antigen receptor T cell immunotherapy is an effective treatment for diffuse intrinsic pontine glioma. Neurooncol Adv, 2023. 5(1): p. vdad024. [CrossRef]
- Pule, M.A., et al., Virus-specific T cells engineered to coexpress tumor-specific receptors: persistence and antitumor activity in individuals with neuroblastoma. Nat Med, 2008. 14(11): p. 1264-70. [CrossRef]
- Ahmed, N., et al., HER2-Specific Chimeric Antigen Receptor-Modified Virus-Specific T Cells for Progressive Glioblastoma: A Phase 1 Dose-Escalation Trial. JAMA Oncol, 2017. 3(8): p. 1094-1101. [CrossRef]
- Vitanza, N.A., et al., Locoregional infusion of HER2-specific CAR T cells in children and young adults with recurrent or refractory CNS tumors: an interim analysis. Nat Med, 2021. 27(9): p. 1544-1552. [CrossRef]
- Zeng, J., et al., IL13RA2 is overexpressed in malignant gliomas and related to clinical outcome of patients. Am J Transl Res, 2020. 12(8): p. 4702-4714.
- Knudson, K.M., et al., Recent Advances in IL-13Rα2-Directed Cancer Immunotherapy. Front Immunol, 2022. 13: p. 878365. [CrossRef]
- Kahlon, K.S., et al., Specific recognition and killing of glioblastoma multiforme by interleukin 13-zetakine redirected cytolytic T cells. Cancer Res, 2004. 64(24): p. 9160-6. [CrossRef]
- Krebs, S., et al., T cells redirected to interleukin-13Rα2 with interleukin-13 mutein--chimeric antigen receptors have anti-glioma activity but also recognize interleukin-13Rα1. Cytotherapy, 2014. 16(8): p. 1121-31. [CrossRef]
- Brown, C.E., et al., Bioactivity and Safety of IL13Rα2-Redirected Chimeric Antigen Receptor CD8+ T Cells in Patients with Recurrent Glioblastoma. Clin Cancer Res, 2015. 21(18): p. 4062-72. [CrossRef]
- Brown, C.E., et al., Optimization of IL13Rα2-Targeted Chimeric Antigen Receptor T Cells for Improved Anti-tumor Efficacy against Glioblastoma. Mol Ther, 2018. 26(1): p. 31-44. [CrossRef]
- Brown, C.E., et al., Regression of Glioblastoma after Chimeric Antigen Receptor T-Cell Therapy. N Engl J Med, 2016. 375(26): p. 2561-9. [CrossRef]
- Kim, K., et al., Chimeric Antigen Receptor T Cells With Modified Interleukin-13 Preferentially Recognize IL13Rα2 and Suppress Malignant Glioma: A Preclinical Study. Front Immunol, 2021. 12: p. 715000. [CrossRef]
- Krenciute, G., et al., Characterization and Functional Analysis of scFv-based Chimeric Antigen Receptors to Redirect T Cells to IL13Rα2-positive Glioma. Mol Ther, 2016. 24(2): p. 354-363. [CrossRef]
- Pituch, K.C., et al., Adoptive Transfer of IL13Rα2-Specific Chimeric Antigen Receptor T Cells Creates a Pro-inflammatory Environment in Glioblastoma. Mol Ther, 2018. 26(4): p. 986-995. [CrossRef]
- Gu, A., et al., IL13Rα2-targeted third-generation CAR-T cells with CD28 transmembrane domain mediate the best anti-glioblastoma efficacy. Cancer Immunol Immunother, 2023. 72(7): p. 2393-2403. [CrossRef]
- Nazha, B., C. Inal, and T.K. Owonikoko, Disialoganglioside GD2 Expression in Solid Tumors and Role as a Target for Cancer Therapy. Front Oncol, 2020. 10: p. 1000. [CrossRef]
- Longee, D.C., et al., Disialoganglioside GD2 in human neuroectodermal tumor cell lines and gliomas. Acta Neuropathol, 1991. 82(1): p. 45-54. [CrossRef]
- Mount, C.W., et al., Potent antitumor efficacy of anti-GD2 CAR T cells in H3-K27M(+) diffuse midline gliomas. Nat Med, 2018. 24(5): p. 572-579. [CrossRef]
- de Billy, E., et al., Dual IGF1R/IR inhibitors in combination with GD2-CAR T-cells display a potent anti-tumor activity in diffuse midline glioma H3K27M-mutant. Neuro Oncol, 2022. 24(7): p. 1150-1163. [CrossRef]
- Gargett, T., et al., GD2-targeting CAR-T cells enhanced by transgenic IL-15 expression are an effective and clinically feasible therapy for glioblastoma. J Immunother Cancer, 2022. 10(9). [CrossRef]
- Majzner, R.G., et al., GD2-CAR T cell therapy for H3K27M-mutated diffuse midline gliomas. Nature, 2022. 603(7903): p. 934-941. [CrossRef]
- Liu, Z., et al., Safety and antitumor activity of GD2-Specific 4SCAR-T cells in patients with glioblastoma. Mol Cancer, 2023. 22(1): p. 3. [CrossRef]
- Maachani, U.B., et al., B7-H3 as a Prognostic Biomarker and Therapeutic Target in Pediatric central nervous system Tumors. Transl Oncol, 2020. 13(2): p. 365-371. [CrossRef]
- Tang, X., et al., B7-H3 as a Novel CAR-T Therapeutic Target for Glioblastoma. Mol Ther Oncolytics, 2019. 14: p. 279-287. [CrossRef]
- Nehama, D., et al., B7-H3-redirected chimeric antigen receptor T cells target glioblastoma and neurospheres. EBioMedicine, 2019. 47: p. 33-43. [CrossRef]
- Vitanza, N.A., et al., Intraventricular B7-H3 CAR T Cells for Diffuse Intrinsic Pontine Glioma: Preliminary First-in-Human Bioactivity and Safety. Cancer Discov, 2023. 13(1): p. 114-131. [CrossRef]
- Arnone, C.M., et al., Oncolytic adenovirus and gene therapy with EphA2-BiTE for the treatment of pediatric high-grade gliomas. J Immunother Cancer, 2021. 9(5). [CrossRef]
- Yi, Z., et al., Optimizing EphA2-CAR T Cells for the Adoptive Immunotherapy of Glioma. Mol Ther Methods Clin Dev, 2018. 9: p. 70-80. [CrossRef]
- Chow, K.K., et al., T cells redirected to EphA2 for the immunotherapy of glioblastoma. Mol Ther, 2013. 21(3): p. 629-37. [CrossRef]
- Lin, Q., et al., First-in-Human Trial of EphA2-Redirected CAR T-Cells in Patients With Recurrent Glioblastoma: A Preliminary Report of Three Cases at the Starting Dose. Front Oncol, 2021. 11: p. 694941. [CrossRef]
- Gu, J., et al., Clinical implications and prognostic value of EMMPRIN/CD147 and MMP2 expression in pediatric gliomas. Eur J Pediatr, 2009. 168(6): p. 705-10. [CrossRef]
- Maggs, L., et al., CAR T Cell-Based Immunotherapy for the Treatment of Glioblastoma. Front Neurosci, 2021. 15: p. 662064. [CrossRef]
- Lasky, J.L., 3rd, et al., Autologous tumor lysate-pulsed dendritic cell immunotherapy for pediatric patients with newly diagnosed or recurrent high-grade gliomas. Anticancer Res, 2013. 33(5): p. 2047-56.
- Benitez-Ribas, D., et al., Immune Response Generated With the Administration of Autologous Dendritic Cells Pulsed With an Allogenic Tumoral Cell-Lines Lysate in Patients With Newly Diagnosed Diffuse Intrinsic Pontine Glioma. Front Oncol, 2018. 8: p. 127. [CrossRef]
- Okada, H., et al., Expression of glioma-associated antigens in pediatric brain stem and non-brain stem gliomas. J Neurooncol, 2008. 88(3): p. 245-50. [CrossRef]
- Pollack, I.F., et al., Antigen-specific immune responses and clinical outcome after vaccination with glioma-associated antigen peptides and polyinosinic-polycytidylic acid stabilized by lysine and carboxymethylcellulose in children with newly diagnosed malignant brainstem and nonbrainstem gliomas. J Clin Oncol, 2014. 32(19): p. 2050-8. [CrossRef]
- Pollack, I.F., et al., Immune responses and outcome after vaccination with glioma-associated antigen peptides and poly-ICLC in a pilot study for pediatric recurrent low-grade gliomas. Neuro Oncol, 2016. 18(8): p. 1157-68. [CrossRef]
- Pollack, I.F., et al., Antigen-specific immunoreactivity and clinical outcome following vaccination with glioma-associated antigen peptides in children with recurrent high-grade gliomas: results of a pilot study. J Neurooncol, 2016. 130(3): p. 517-527. [CrossRef]
- Chheda, Z.S., et al., Novel and shared neoantigen derived from histone 3 variant H3.3K27M mutation for glioma T cell therapy. J Exp Med, 2018. 215(1): p. 141-157. [CrossRef]
- Immisch, L., et al., Response to: Correspondence on 'H3.3K27M mutation is not a suitable target for immunotherapy in HLA-A2+ patients with diffuse midline glioma' by Chheda et al. J Immunother Cancer, 2023. 11(3). [CrossRef]
- Mueller, S., et al., Mass cytometry detects H3.3K27M-specific vaccine responses in diffuse midline glioma. J Clin Invest, 2020. 130(12): p. 6325-6337. [CrossRef]
- Kmiecik, J., J. Zimmer, and M. Chekenya, Natural killer cells in intracranial neoplasms: presence and therapeutic efficacy against brain tumours. J Neurooncol, 2014. 116(1): p. 1-9. [CrossRef]
- Fares, J., et al., Advances in NK cell therapy for brain tumors. NPJ Precis Oncol, 2023. 7(1): p. 17. [CrossRef]
- Chu, Y., et al., Combinatorial immunotherapy of N-803 (IL-15 superagonist) and dinutuximab with ex vivo expanded natural killer cells significantly enhances in vitro cytotoxicity against GD2(+) pediatric solid tumors and in vivo survival of xenografted immunodeficient NSG mice. J Immunother Cancer, 2021. 9(7). [CrossRef]
- Shida, Y., et al., Ex Vivo Expanded and Activated Natural Killer Cells Prolong the Overall Survival of Mice with Glioblastoma-like Cell-Derived Tumors. Int J Mol Sci, 2021. 22(18). [CrossRef]
- Yvon, E.S., et al., Cord blood natural killer cells expressing a dominant negative TGF-β receptor: Implications for adoptive immunotherapy for glioblastoma. Cytotherapy, 2017. 19(3): p. 408-418. [CrossRef]
- Shaim, H., et al., Targeting the αv integrin/TGF-β axis improves natural killer cell function against glioblastoma stem cells. J Clin Invest, 2021. 131(14). [CrossRef]
- Liu, Z., et al., Intravenous injection of oncolytic picornavirus SVV-001 prolongs animal survival in a panel of primary tumor-based orthotopic xenograft mouse models of pediatric glioma. Neuro Oncol, 2013. 15(9): p. 1173-85. [CrossRef]
- Tayeb, S., Z. Zakay-Rones, and A. Panet, Therapeutic potential of oncolytic Newcastle disease virus: a critical review. Oncolytic Virother, 2015. 4: p. 49-62. [CrossRef]
- Lam, H.Y., et al., Safety and clinical usage of newcastle disease virus in cancer therapy. J Biomed Biotechnol, 2011. 2011: p. 718710. [CrossRef]
- Csatary, L.K., et al., MTH-68/H oncolytic viral treatment in human high-grade gliomas. J Neurooncol, 2004. 67(1-2): p. 83-93. [CrossRef]
- Wagner, S., et al., Combined treatment of pediatric high-grade glioma with the oncolytic viral strain MTH-68/H and oral valproic acid. Apmis, 2006. 114(10): p. 731-43. [CrossRef]
- Markert, J.M., et al., A phase 1 trial of oncolytic HSV-1, G207, given in combination with radiation for recurrent GBM demonstrates safety and radiographic responses. Mol Ther, 2014. 22(5): p. 1048-55. [CrossRef]
- Markert, J.M., et al., Phase Ib trial of mutant herpes simplex virus G207 inoculated pre-and post-tumor resection for recurrent GBM. Mol Ther, 2009. 17(1): p. 199-207. [CrossRef]
- Markert, J.M., et al., Conditionally replicating herpes simplex virus mutant, G207 for the treatment of malignant glioma: results of a phase I trial. Gene Ther, 2000. 7(10): p. 867-74. [CrossRef]
- Ring, E., et al., PCM-09COMPARISON OF THE SENSITIVITIES OF PEDIATRIC HIGH-GRADE BRAIN TUMOR VERSUS ADULT GLIOBLASTOMA XENOGRAFTS TO ENGINEERED ONCOLYTIC HERPES SIMPLEX VIROTHERAPY. Neuro-Oncology, 2016. 18(suppl_3): p. iii141-iii141. [CrossRef]
- Friedman, G.K., et al., Oncolytic HSV-1 G207 Immunovirotherapy for Pediatric High-Grade Gliomas. N Engl J Med, 2021. 384(17): p. 1613-1622. [CrossRef]
- Cockle, J.V., et al., Oncolytic Herpes Simplex Virus Inhibits Pediatric Brain Tumor Migration and Invasion. Mol Ther Oncolytics, 2017. 5: p. 75-86. [CrossRef]
- Martínez-Vélez, N., et al., The oncolytic virus Delta-24-RGD elicits an antitumor effect in pediatric glioma and DIPG mouse models. Nature Communications, 2019. 10(1): p. 2235. [CrossRef]
- Fueyo, J., et al., Preclinical Characterization of the Antiglioma Activity of a Tropism-Enhanced Adenovirus Targeted to the Retinoblastoma Pathway. JNCI: Journal of the National Cancer Institute, 2003. 95(9): p. 652-660. [CrossRef]
- Lang, F.F., et al., Phase I Study of DNX-2401 (Delta-24-RGD) Oncolytic Adenovirus: Replication and Immunotherapeutic Effects in Recurrent Malignant Glioma. J Clin Oncol, 2018. 36(14): p. 1419-1427. [CrossRef]
- Martinez-Velez, N., et al., Delta-24-RGD combined with radiotherapy exerts a potent antitumor effect in diffuse intrinsic pontine glioma and pediatric high grade glioma models. Acta Neuropathologica Communications, 2019. 7(1): p. 64. [CrossRef]
- Gállego Pérez-Larraya, J., et al., Oncolytic DNX-2401 Virus for Pediatric Diffuse Intrinsic Pontine Glioma. N Engl J Med, 2022. 386(26): p. 2471-2481. [CrossRef]
- Aguilar, L.K., B.W. Guzik, and E. Aguilar-Cordova, Cytotoxic immunotherapy strategies for cancer: mechanisms and clinical development. J Cell Biochem, 2011. 112(8): p. 1969-77. [CrossRef]
- Kieran, M.W., et al., Phase I study of gene-mediated cytotoxic immunotherapy with AdV-tk as adjuvant to surgery and radiation for pediatric malignant glioma and recurrent ependymoma. Neuro Oncol, 2019. 21(4): p. 537-546. [CrossRef]
- Vitanza, N.A. and S. Partap, Pediatric Ependymoma. J Child Neurol, 2016. 31(12): p. 1354-66. [CrossRef]
- Ostrom, Q.T., et al., Alex's Lemonade Stand Foundation Infant and Childhood Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2007-2011. Neuro Oncol, 2015. 16 Suppl 10(Suppl 10): p. x1-x36. [CrossRef]
- McGuire, C.S., K.L. Sainani, and P.G. Fisher, Incidence patterns for ependymoma: a surveillance, epidemiology, and end results study. J Neurosurg, 2009. 110(4): p. 725-9. [CrossRef]
- Elsamadicy, A.A., et al., Comparison of epidemiology, treatments, and outcomes in pediatric versus adult ependymoma. Neurooncol Adv, 2020. 2(1): p. vdaa019. [CrossRef]
- Merchant, T.E., et al., Conformal radiotherapy after surgery for paediatric ependymoma: a prospective study. Lancet Oncol, 2009. 10(3): p. 258-66. [CrossRef]
- Pajtler, K.W., et al., Molecular Classification of Ependymal Tumors across All CNS Compartments, Histopathological Grades, and Age Groups. Cancer Cell, 2015. 27(5): p. 728-43. [CrossRef]
- Witt, H., et al., DNA methylation-based classification of ependymomas in adulthood: implications for diagnosis and treatment. Neuro Oncol, 2018. 20(12): p. 1616-1624. [CrossRef]
- Larrew, T., et al., Molecular Classification and Therapeutic Targets in Ependymoma. Cancers (Basel), 2021. 13(24). [CrossRef]
- Mascarenhas, L., et al., Phase 1 clinical trial of durvalumab in children with solid and central nervous system tumors. Journal of Clinical Oncology, 2022. 40(16_suppl): p. 10029-10029. [CrossRef]
- Yeung, J.T., et al., Increased expression of tumor-associated antigens in pediatric and adult ependymomas: implication for vaccine therapy. J Neurooncol, 2013. 111(2): p. 103-11. [CrossRef]
- Hwang, E.I., et al., Why haven't we solved intracranial pediatric ependymoma? Current questions and barriers to treatment advances. Neoplasia, 2023. 39: p. 100895. [CrossRef]
- Sahu, A., et al., In vivo tumor immune microenvironment phenotypes correlate with inflammation and vasculature to predict immunotherapy response. Nat Commun, 2022. 13(1): p. 5312. [CrossRef]
- Grabovska, Y., et al., Pediatric pan-central nervous system tumor analysis of immune-cell infiltration identifies correlates of antitumor immunity. Nature Communications, 2020. 11(1): p. 4324. [CrossRef]
- Andersen, J.K., H. Miletic, and J.A. Hossain, Tumor-Associated Macrophages in Gliomas-Basic Insights and Treatment Opportunities. Cancers (Basel), 2022. 14(5). [CrossRef]
- Maximov, V., et al., Tumour-associated macrophages exhibit anti-tumoural properties in Sonic Hedgehog medulloblastoma. Nature Communications, 2019. 10(1): p. 2410. [CrossRef]
- Tan, I.L., et al., CSF1R inhibition depletes tumor-associated macrophages and attenuates tumor progression in a mouse sonic Hedgehog-Medulloblastoma model. Oncogene, 2021. 40(2): p. 396-407. [CrossRef]
- Dang, M.T., et al., Macrophages in SHH subgroup medulloblastoma display dynamic heterogeneity that varies with treatment modality. Cell Rep, 2021. 34(13): p. 108917. [CrossRef]
- Plant, A.S., et al., Immunophenotyping of pediatric brain tumors: correlating immune infiltrate with histology, mutational load, and survival and assessing clonal T cell response. J Neurooncol, 2018. 137(2): p. 269-278. [CrossRef]
- Lieberman, N.A.P., et al., Characterization of the immune microenvironment of diffuse intrinsic pontine glioma: implications for development of immunotherapy. Neuro Oncol, 2019. 21(1): p. 83-94. [CrossRef]
- Robinson, M.H., et al., Subtype and grade-dependent spatial heterogeneity of T-cell infiltration in pediatric glioma. J Immunother Cancer, 2020. 8(2). [CrossRef]
- Ross, J.L., et al., Platelet-derived growth factor beta is a potent inflammatory driver in paediatric high-grade glioma. Brain, 2021. 144(1): p. 53-69. [CrossRef]
- Lin, G.L., et al., Non-inflammatory tumor microenvironment of diffuse intrinsic pontine glioma. Acta Neuropathol Commun, 2018. 6(1): p. 51. [CrossRef]
- Bailey, C.P., et al., Computational immune infiltration analysis of pediatric high-grade gliomas (pHGGs) reveals differences in immunosuppression and prognosis by tumor location. Comput Syst Oncol, 2021. 1(3). [CrossRef]
- Griesinger, A.M., et al., Characterization of distinct immunophenotypes across pediatric brain tumor types. J Immunol, 2013. 191(9): p. 4880-8. [CrossRef]
- Ritzmann, T., et al., EPEN-23. A COMPUTATIONAL ANALYSIS OF THE TUMOUR IMMUNE MICROENVIRONMENT IN PAEDIATRIC EPENDYMOMA. Neuro-Oncology, 2020. 22(Supplement_3): p. iii312-iii312. [CrossRef]
- Hoffman, L.M., et al., Molecular sub-group-specific immunophenotypic changes are associated with outcome in recurrent posterior fossa ependymoma. Acta Neuropathol, 2014. 127(5): p. 731-45. [CrossRef]
- Griesinger, A.M., et al., Multi-omic approach identifies hypoxic tumor-associated myeloid cells that drive immunobiology of high-risk pediatric ependymoma. iScience, 2023. 26(9): p. 107585. [CrossRef]
- Budhiraja, S., et al., Immunobiology and Cytokine Modulation of the Pediatric Brain Tumor Microenvironment: A Scoping Review. Cancers, 2023. 15(14): p. 3655. [CrossRef]
- van Bree, N. and M. Wilhelm, The Tumor Microenvironment of Medulloblastoma: An Intricate Multicellular Network with Therapeutic Potential. Cancers (Basel), 2022. 14(20). [CrossRef]
- Wang, S.S., P. Bandopadhayay, and M.R. Jenkins, Towards Immunotherapy for Pediatric Brain Tumors. Trends Immunol, 2019. 40(8): p. 748-761. [CrossRef]
- Lu, D.Y., et al., HAART in HIV/AIDS Treatments: Future Trends. Infect Disord Drug Targets, 2018. 18(1): p. 15-22. [CrossRef]
- DeSelm, C., et al., Low-Dose Radiation Conditioning Enables CAR T Cells to Mitigate Antigen Escape. Mol Ther, 2018. 26(11): p. 2542-2552. [CrossRef]
- Hwang, J.K., J. Hong, and C.O. Yun, Oncolytic Viruses and Immune Checkpoint Inhibitors: Preclinical Developments to Clinical Trials. Int J Mol Sci, 2020. 21(22). [CrossRef]
- Tian, M., et al., An optimized bicistronic chimeric antigen receptor against GPC2 or CD276 overcomes heterogeneous expression in neuroblastoma. J Clin Invest, 2022. 132(16). [CrossRef]
Figure 1.
Immunotherapies in anti-tumor responses. Under physiological conditions, tumor antigens would be taken up by APCs, processed and precented on the MHC molecules. T cells are activated by recognizing antigens presented on MHC complex. Activated T cells then proliferate and migrate to tumor site. In tumor microenvironment, effector T cells recognize the antigen presented on the surface of tumor cells and kill tumor cells. Immunotherapies take places in different steps during anti-tumor responses. Immune checkpoint inhibitors release T cell inhibition at both T cell activation and target killing steps. Adoptive cell therapies provide the immune cells for tumor killing. Cancer vaccines provide peptides or antigen loaded DCs for T cell activation. Oncolytic viruses kill tumor cells to release tumor antigens and are able to turn the cold TME to a hot TME. The conventional therapy including radio- and chemo-therapy are able to kill tumor cells and alter the TME.
Figure 1.
Immunotherapies in anti-tumor responses. Under physiological conditions, tumor antigens would be taken up by APCs, processed and precented on the MHC molecules. T cells are activated by recognizing antigens presented on MHC complex. Activated T cells then proliferate and migrate to tumor site. In tumor microenvironment, effector T cells recognize the antigen presented on the surface of tumor cells and kill tumor cells. Immunotherapies take places in different steps during anti-tumor responses. Immune checkpoint inhibitors release T cell inhibition at both T cell activation and target killing steps. Adoptive cell therapies provide the immune cells for tumor killing. Cancer vaccines provide peptides or antigen loaded DCs for T cell activation. Oncolytic viruses kill tumor cells to release tumor antigens and are able to turn the cold TME to a hot TME. The conventional therapy including radio- and chemo-therapy are able to kill tumor cells and alter the TME.
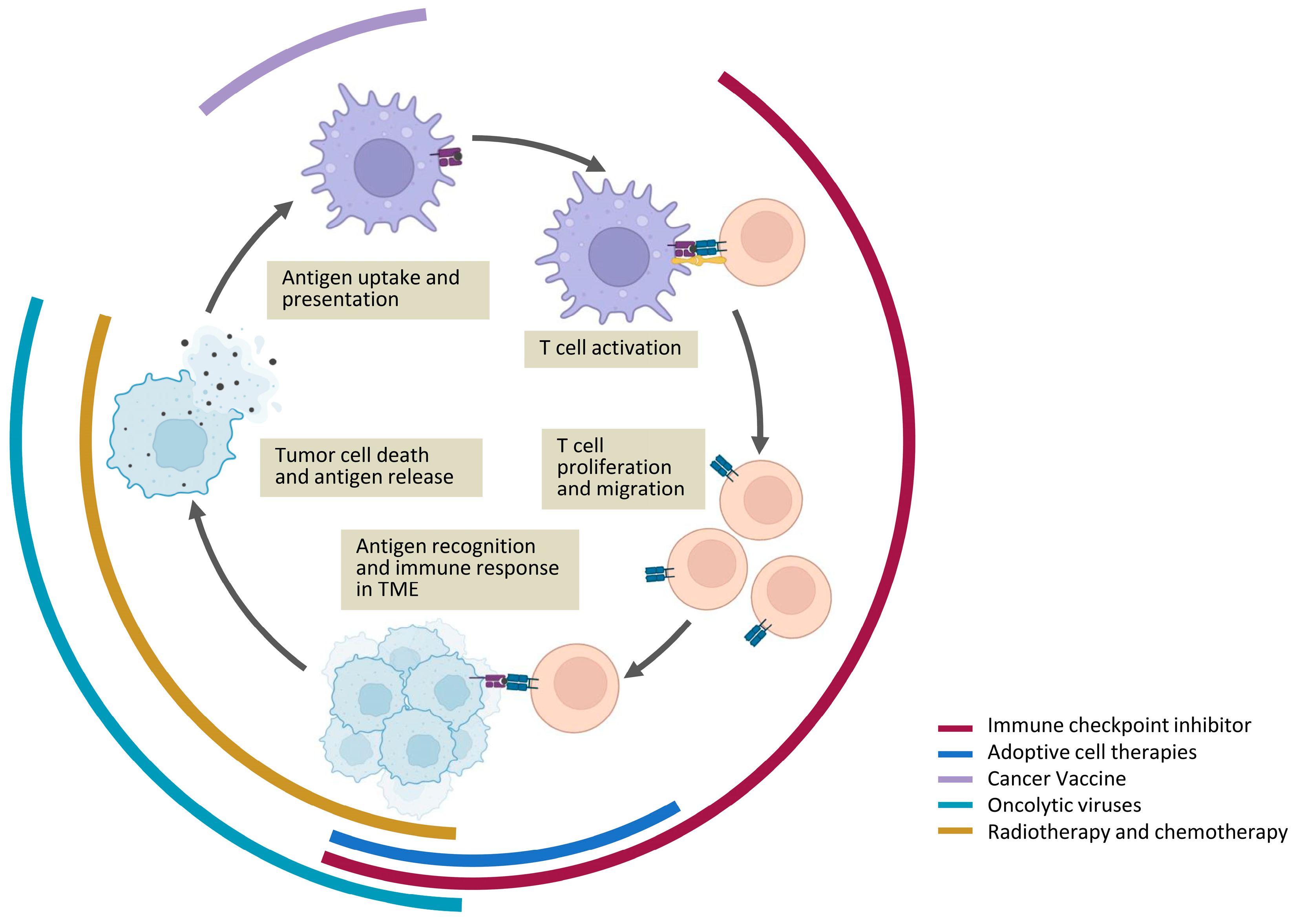

Table 1.
Clinical trials of immunotherapies for PBTs.
| ICI therapies | ||||||||
| NCT number | Tumor | Title | Phase | Treatment | Ages | Status | Time | Results |
| NCT02359565 | Constitutional Mismatch Repair Deficiency Syndrome Lynch Syndrome Malignant Glioma Recurrent Brain Neoplasm Recurrent Childhood Ependymoma Recurrent Diffuse Intrinsic Pontine Glioma Recurrent Medulloblastoma Refractory Brain Neoplasm Refractory Diffuse Intrinsic Pontine Glioma Refractory Ependymoma Refractory Medulloblastoma |
Pembrolizumab in Treating Younger Patients With Recurrent, Progressive, or Refractory High-Grade Gliomas, Diffuse Intrinsic Pontine Gliomas, Hypermutated Brain Tumors, Ependymoma or Medulloblastoma | Phase I | Pembrolizumab | 1 Year to 30 Years | Recruiting | 05/2015-12/2026 | |
| NCT02502708 | Glioblastoma Multiforme Glioma Gliosarcoma Malignant Brain Tumor Ependymoma Medulloblastoma Diffuse Intrinsic Pontine Glioma Primary CNS Tumor |
Study of the IDO Pathway Inhibitor, Indoximod, and Temozolomide for Pediatric Patients With Progressive Primary Malignant Brain Tumors | Phase I | indoximod | 3 Years to 21 Years | Completed | 10/2015-02/2020 | Johnson et. al. 2021 |
| NCT02793466 | Solid Tumor Lymphoma Central Nervous System Tumors |
Durvalumab in Pediatric and Adolescent Patients | Phase I | Durvalumab | 1 Year to 17 Years | Completed | 07/2016-04/2023 | Mascarenhas et. al 2022 |
| NCT03130959 | Various Advanced Cancer Diffuse Intrinsic Pontine Glioma non-brainstem High Grade Glioma medulloblastoma |
A Study to Evaluate the Safety and Efficacy of Nivolumab Monotherapy and Nivolumab in Combination With Ipilimumab in Pediatric Participants With High Grade Primary Central Nervous System (CNS) Malignancies (CheckMate 908) | Phase II | Nivolumab, Ipilimumab | 6 Months to 21 Years | Completed | 06/2017-01-2022 | Dunkel et.al. 2023 |
| NCT04049669 | Glioblastoma Medulloblastoma Ependymoma Diffuse Intrinsic Pontine Glioma |
Pediatric Trial of Indoximod With Chemotherapy and Radiation for Relapsed Brain Tumors or Newly Diagnosed DIPG | Phase I | indoximod | 3 Years to 21 Years | Recruiting | 10/2019-10/2027 | |
| NCT04323046 | Glioblastoma Malignant Glioma Recurrent Glioblastoma Recurrent Malignant Glioma Recurrent Grade III Glioma Grade III Glioma |
Immunotherapy Before and After Surgery for Treatment of Recurrent or Progressive High Grade Glioma in Children and Young Adults | Phase I | nivolumab | 6 Months to 25 Years | Recruiting | 10/2020-03/2029 | |
| NCT04167618 | Medulloblastoma, Childhood | 177Lu-DTPA-Omburtamab Radioimmunotherapy for Recurrent or Refractory Medulloblastoma | Phase I/II | 177Lu-DTPA-omburtamab | 3 Years to 19 Years | Terminated | 09/2021-08/2022 | |
| CAR T cell therapies | ||||||||
| NCT number | Tumor | title | Phase | Treatment | Ages | Status | Time | Results |
| NCT01109095 | Glioblastoma Multiforme (GBM) | CMV-specific Cytotoxic T Lymphocytes Expressing CAR Targeting HER2 in Patients With GBM (HERT-GBM) | Phase I | HER2-CAR CMV-T cell | Child, Adult, Older Adult | Completed | 10/2010-03/2018 | Badhiwala et.al. 2013 |
| NCT02271711 | Recurrent Childhood Medulloblastoma Recurrent Ependymoma Recurrent Medulloblastoma |
Expanded Natural Killer Cell Infusion in Treating Younger Patients With Recurrent/Refractory Brain Tumors | Phase I | Autologous NK cells | up to 21 Years | Completed | 03/2015-08/2020 | Khatua et.al. 2020 |
| NCT02208362 | Recurrent Glioblastoma Recurrent Malignant Glioma Recurrent WHO Grade II Glioma Recurrent WHO Grade III Glioma Refractory Glioblastoma Refractory Malignant Glioma Refractory WHO Grade II Glioma Refractory WHO Grade III Glioma |
Genetically Modified T-cells in Treating Patients With Recurrent or Refractory Malignant Glioma | Phase I | IL13Rα2-Specific CAR T cell | 12 Years to 75 Years | Active, Not recruiting | 05/2015-12/2023 | Brown et.al. 2016 |
| NCT02442297 | Brain Tumor, Recurrent Brain Tumor, Refractory |
T Cells Expressing HER2-specific Chimeric Antigen Receptors(CAR) for Patients With HER2-Positive CNS Tumors (iCAR) | Phase I | HER2 CAR T cell | 3 Years and older | Active, Not recruiting | 04/2016-04/2037 | |
| NCT03500991 | Central Nervous System Tumor, Pediatric Glioma Ependymoma Medulloblastoma Germ Cell Tumor Atypical Teratoid/Rhabdoid Tumor Primitive Neuroectodermal Tumor Choroid Plexus Carcinoma Pineoblastoma |
HER2-specific CAR T Cell Locoregional Immunotherapy for HER2-positive Recurrent/Refractory Pediatric CNS Tumors | Phase I | HER2-Specific CAR T Cell | 1 Year to 26 Years | Active, Not recruiting | 07/2018-07/2039 | Vitanza et.al. 2021 |
| NCT03652545 | Brain Tumor | Multi-antigen T Cell Infusion Against Neuro-oncologic Disease (REMIND) | Phase I | multi-antigen associated specific cytotoxic T lymphocytes (TAA-T) | 6 Months to 80 Years | Recruiting | 12/2018-03/2026 | |
| NCT03638167 | Central Nervous System Tumor, Pediatric Glioma Ependymoma Medulloblastoma Germ Cell Tumor Atypical Teratoid/Rhabdoid Tumor Primitive Neuroectodermal Tumor Choroid Plexus Carcinoma Pineoblastoma |
EGFR806-specific CAR T Cell Locoregional Immunotherapy for EGFR-positive Recurrent or Refractory Pediatric CNS Tumors | Phase I | EGFR806-specific CAR T cell |
1 Year to 26 Years | Active, Not recruiting | 03/2019-03/2040 | |
| NCT04185038 | Central Nervous System Tumor Diffuse Intrinsic Pontine Glioma Diffuse Midline Glioma Ependymoma Medulloblastoma, Childhood Germ Cell Tumor Atypical Teratoid/Rhabdoid Tumor Primitive Neuroectodermal Tumor Choroid Plexus Carcinoma Pineoblastoma, Childhood Glioma |
Study of B7-H3-Specific CAR T Cell Locoregional Immunotherapy for Diffuse Intrinsic Pontine Glioma/Diffuse Midline Glioma and Recurrent or Refractory Pediatric Central Nervous System Tumors | Phase I | B7-H3-Specific CAR T cell | 1 Year to 26 Years | Recruiting | 12/2019-05/2041 | |
| NCT04099797 | Diffuse Intrinsic Pontine Glioma High Grade Glioma Embryonal Tumor Ependymal Tumor |
C7R-GD2.CAR T Cells for Patients With GD2-expressing Brain Tumors (GAIL-B) | Phase I | C7R-GD2.CAR T Cell | 12 Months to 21 Years | Recruiting | 02/2020-02/2039 | |
| NCT03170141 | Glioblastoma Multiforme of Brain Glioblastoma Multiforme |
Immunogene-modified T (IgT) Cells Against Glioblastoma Multiforme | Phase I | GD2-specific 4SCAR T cells | 1 Year to 80 Years | Enrolling by Invitation | 05/2020-12/2023 | Liu et.al. 2023 |
| NCT04196413 | Glioma of Spinal Cord Glioma of Brainstem |
GD2 CAR T Cells in Diffuse Intrinsic Pontine Gliomas(DIPG) & Spinal Diffuse Midline Glioma(DMG) | Phase I | GD2 CAR T cell | 2 Years to 50 Years | Recruiting | 06/2020-07/2043 | |
| NCT04510051 | Malignant Brain Neoplasm Recurrent Malignant Brain Neoplasm Refractory Malignant Brain Neoplasm |
CAR T Cells After Lymphodepletion for the Treatment of IL13Rα2 Positive Recurrent or Refractory Brain Tumors in Children | Phase I | IL13(EQ)BBzeta/CD19t+ T cells | 4 Years to 25 Years | Recruiting | 12/2020-08/2024 | |
| NCT04903080 | Ependymoma | HER2-specific Chimeric Antigen Receptor (CAR) T Cells for Children With Ependymoma | Phase I | HER2 CAR T cell | 1 Year to 22 Years | Active, Not recruiting | 07/2022-02/2043 | |
| NCT05835687 | Central Nervous System Neoplasms Atypical Teratoid/Rhabdoid Tumor Diffuse Midline Glioma, H3 K27M-Mutant Ependymoma High Grade Glioma Glioblastoma Medulloblastoma |
Loc3CAR: Locoregional Delivery of B7-H3-CAR T Cells for Pediatric Patients With Primary CNS Tumors | Phase I | B7-H3-CAR T cell | up to 21 Years | Recruiting | 04/2023-03/2028 | |
| NCT05768880 | Diffuse Intrinsic Pontine Glioma Diffuse Midline Glioma Recurrent CNS Tumor, Adult Recurrent, CNS Tumor, Childhood Refractory Primary Malignant Central Nervous System Neoplas |
Study of B7-H3, EGFR806, HER2, And IL13-Zetakine (Quad) CAR T Cell Locoregional Immunotherapy For Pediatric Diffuse Intrinsic Pontine Glioma, Diffuse Midline Glioma, And Recurrent Or Refractory Central Nervous System Tumors | Phase I | SC-CAR4BRAIN, an autologous CD4+ and CD8+ T cells expressing combinations of B7-H3, EGFR806, HER2, and IL13-zetakine CAR | 1 Year to 26 Years | Recruiting | 05/2023-12/2043 | |
| NCT05298995 | Brain Tumor, Pediatric Medulloblastoma, Childhood Embryonal Tumor High Grade Glioma Diffuse Midline Glioma Diffuse Intrinsic Pontine Glioma Brain Tumor Adult |
GD2-CAR T Cells for Pediatric Brain Tumours | Phase I | iC9-GD2-CAR T-cell | 6 Months to 30 Years | Recruiting | 11/2023-11/2038 | |
| Vaccine therapies | ||||||||
| NCT number | Tumor | title | Phase | Treatment | Ages | Status | Time | Results |
| NCT00107185 | Brain and Central Nervous System Tumors | Vaccine Therapy in Treating Young Patients Who Are Undergoing Surgery for Malignant Glioma | Phase I | autologous tumor lysate-pulsed DC vaccine | 1 Year to 18 Years | Completed | 01/2005-03/2010 | Lasky et.al. 2013 |
| NCT01130077 | Newly Diagnosed Pediatric Pontine Glioma Newly Diagnosed Pediatric High Grade Glioma Recurrent Pediatric High Grade Glioma Recurrent Pediatric Low Grade Glioma |
A Pilot Study of Glioma Associated Antigen Vaccines in Conjunction With Poly-ICLC in Pediatric Gliomas | Phase I | HLA-A2 restricted GGAs combine with poly-ICLC | 12 Months to 21 Years | Active, Not recruiting | 02/2009-12/2025 | Pollack et. al. 2014 |
| NCT01326104 | Medulloblastoma Neuroectodermal Tumor |
Vaccine Immunotherapy for Recurrent Medulloblastoma and Primitive Neuroectodermal Tumor (Re-MATCH) | Phase II | DC vaccine | up to 30 Years | Active, Not recruiting | 09/2010-12/2023 | |
| NCT01795313 | Ependymoma | Immunotherapy for Recurrent Ependymomas in Children Using Tumor Antigen Peptides With Imiquimod | Phase I | IL-13Rα2, EphA2, Survivin | 12 Months to 21 Years | Recruiting | 08/2012-12/2025 | |
| NCT02840123 | Diffuse Intrinsic Pontine Glioma | Safety Study of DIPG Treatment With Autologous Dendritic Cells Pulsed With Lysated Allegenic Tumor Lines | Phase I | autologous DC pulsed with lysated allegenic tumor lines | 3 Years to 18 Years | Unknown | 06/2016-03/2019 | Benitez-Ribas et.al. 2018 |
| NCT02960230 | Diffuse Intrinsic Pontine Glioma Glioma Diffuse Midline Glioma, H3 K27M-Mutant |
H3.3K27M Peptide Vaccine With Nivolumab for Children With Newly Diagnosed DIPG and Other Gliomas | Phase I/II | H3.3K27M Specific Peptide Vaccine Combined With Poly-ICLC With and Without PD-1 Inhibition | 3 Years to 21 Years | Active, Not recruiting | 11/2016-11/2024 | Muller et. al. 2022 |
| NCT03334305 | Malignant Glioma High Grade Glioma |
Adoptive Cellular Therapy in Pediatric Patients With High-grade Gliomas (ACTION) | Phase I | DC vaccine | 3 Years to 21 Years | Active, Not recruiting | 05/2018-05/2026 | |
| NCT03396575 | Diffuse Intrinsic Pontine Glioma (DIPG) Brain Stem Glioma |
Brain Stem Gliomas Treated With Adoptive Cellular Therapy During Focal Radiotherapy Recovery Alone or With Dose-intensified Temozolomide (Phase I) (BRAVO) | Phase I | DC vaccine | 3 Years to 30 Years | Active, Not recruiting | 07/2018-06/2025 | |
| NCT04749641 | Diffuse Intrinsic Pontine Glioma | Neoantigen Vaccine Therapy Against H3.3-K27M Diffuse Intrinsic Pontine Glioma (ENACTING) | Phase I | H3.3-K27M Neoantigen Vaccine | 5 Years and older | Recruiting | 03/2021-12/2024 | |
| NCT04911621 | High Grade Glioma Diffuse Intrinsic Pontine Glioma |
Adjuvant Dendritic Cell Immunotherapy for Pediatric Patients With High-grade Glioma or Diffuse Intrinsic Pontine Glioma (ADDICT-pedGLIO) | Phase I/II | WT1 mRNA-loaded autologous monocyte-derived DCs | 12 Months to 17 Years | Active, Not recruiting | 09/2021-06/2027 | |
| NCT04573140 | Adult Glioblastoma | A Study of RNA-lipid Particle (RNA-LP) Vaccines for Newly Diagnosed Pediatric High-Grade Gliomas (pHGG) and Adult Glioblastoma (GBM) (PNOC020) | Phase I | RNA-LP vaccines | 21 Years and older | Recruiting | 10/2021-07/2027 | |
| NCT04978727 | Medulloblastoma Glioblastoma Multiforme Anaplastic Astrocytoma High-grade Astrocytoma NOS Anaplastic Oligodendroglioma Anaplastic Ependymoma Ependymoma Diffuse Intrinsic Pontine Glioma |
A Pilot Study of SurVaxM in Children Progressive or Relapsed Medulloblastoma, High Grade Glioma, Ependymoma and Newly Diagnosed Diffuse Intrinsic Pontine Glioma | Phase I | SurVaxM | 1 Year to 21 Years | Recruiting | 07/2022-06/2028 | |
| Oncolytic virus therapies | ||||||||
| NCT number | Tumor | title | Phase | Treatment | Ages | Status | Time | Results |
| NCT00634231 | Malignant Glioma Recurrent Ependymoma |
A Phase I Study of AdV-tk + Prodrug Therapy in Combination With Radiation Therapy for Pediatric Brain Tumors | Phase I | AdV-tk followed by valacyclovir | 3 Years to 21 Years | Completed | 10/2010-06/2021 | Kieran et.al. 2019 |
| NCT02457845 | Supratentorial Neoplasms, Malignant Malignant Glioma Glioblastoma Anaplastic Astrocytoma PNET Cerebral Primitive Neuroectodermal Tumor Embryonal Tumor |
HSV G207 Alone or With a Single Radiation Dose in Children With Progressive or Recurrent Supratentorial Brain Tumors | Phase I | HSV G207 | 3 Years to 18 Years | Active, Not recruiting | 05/2016-01/2024 | Friedman et.al. 2021 |
| NCT02962167 | Medulloblastoma, Childhood, Recurrent Atypical Teratoid/Rhabdoid Tumor Medulloblastoma Recurrent |
Modified Measles Virus (MV-NIS) for Children and Young Adults With Recurrent Medulloblastoma or Recurrent ATRT | Phase I | modified measles virus (MV-NIS) | 12 Months to 39 Years | Completed | 02/2017-05/2023 | |
| NCT03178032 | Brainstem Glioma | Oncolytic Adenovirus, DNX-2401, for Naive Diffuse Intrinsic Pontine Gliomas | Phase I | DNX-2401 | 1 Year to 18 Years | Completed | 05/2017-1/2021 | Gállego Pérez-Larraya et.al. 2022 |
| NCT03043391 | Malignant Glioma Anaplastic Astrocytoma Anaplastic Oligoastrocytoma Anaplastic Oligodendroglioma Glioblastoma Gliosarcoma Atypical Teratoid/Rhabdoid Tumor of Brain Medulloblastoma Ependymoma Pleomorphic Xanthoastrocytoma of Brain Embryonal Tumor of Brain |
Phase 1b Study PVSRIPO for Recurrent Malignant Glioma in Children | Phase I | oncolytic poliovirus (PVSRIPO) | 12 Years to 21 Years | Unkown | 12/2017-03/2022 | |
| NCT04482933 | Neoplasms High Grade Glioma Glioblastoma Multiforme Malignant Glioma of Brain Anaplastic Astrocytoma of Brain High-grade Glioma Anaplastic Glioma Giant Cell Glioblastoma |
HSV G207 With a Single Radiation Dose in Children With Recurrent High-Grade Glioma | Phase II | HSV G207 combined with a single 5 Gy dose of radiation | 3 Years to 21 Years | Active, Not recruiting | 12/2023-12/2028 | |
| NCT03911388 | Recurrent or Refractory Cerebellar Brain Tumors | HSV G207 in Children With Recurrent or Refractory Cerebellar Brain Tumors | Phase I | HSV G207 | 3 Years to 21 Years | Recruiting | 09/2019-09/2026 | |
| NCT04758533 | Diffuse Intrinsic Pontine Glioma Medulloblastoma, Childhood, Recurrent |
Clinical Trial to Assess the Safety and Efficacy of AloCELYVIR With Newly Diagnosed Diffuse Intrinsic Pontine Glioma (DIPG) in Combination With Radiotherapy or Medulloblastoma in Monotherapy (AloCELYVIR) | Phase I/II | bone marrow-derived allogenic mesenchymal stem cells loaded with an oncolytic Adenovirus (ICOVIR-5) | 1 Year to 21 Years | Recruiting | 04/2021-04/2026 | |
Table 2.
2021 WHO classification of ependymoma.
| Location | Molecular grouping | WHO grade |
|---|---|---|
| Supratentorial | ZFTA fusion positive | |
| YAP1 fusion positive | ||
| Supratentorial ependymoma (other) | 2, 3 | |
| Posterior fossa | Posterior fossa group A | |
| Posterior fossa group B | ||
| Posterior fossa ependymoma (other) | 2, 3 | |
| Spine | MYCN amplified | |
| Spinal ependymoma | 2, 3 | |
| Spinal cord | Myxopapillary ependymoma | 2 |
| CNS | Subependymoma | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



