
Submitted:
28 November 2023
Posted:
30 November 2023
You are already at the latest version
Abstract
Up to 50% of patients with high-risk myeloid malignancies die of relapse after allogeneic stem cell transplantation. Current sequential conditioning regimens like the FLAMSA protocol combine intensive induction therapy with TBI or alkylators. Venetoclax has synergistic effects to chemotherapy. In a retrospective survey among German transplant centers, we identified 61 patients with myeloid malignancies that had received FLAMSA based sequential conditioning with Venetoclax between 2018 and 2022 as an individualized treatment approach. Sixty patients (98%) had active disease at transplant and 74% had genetic high-risk features. Patients received allografts from matched unrelated, matched related or mismatched donors. Tumor lysis syndrome occurred in two patients but no significant non-hematologic toxicity related to Venetoclax was observed. At day +30, 55 patients (90%) were in complete remission. Acute GvHD II°-IV° occurred in 17 (28%) and moderate/severe chronic GvHD in 7 patients (12%). Event-free survival and overall survival were 64% and 80% at 1 year as well as 57% and 75% at 2 years, respectively. The combination of sequential FLAMSA-RIC with Venetoclax appears to be safe and highly effective. To further validate these insights and enhance the idea of smart conditioning, a controlled prospective clinical trial has been initiated in 07/2023.
Keywords:
FLAMSA
; allogeneic transplant (aHSCT)
; sequential conditioning
; AML
; MDS
; myeloid malignancies
; reduced-intensity conditioning
; RIC
; Venetoclax
1. Introduction
High-risk myeloid malignancies like (secondary) acute myeloid leukemia (AML), myelodysplastic syndromes (MDS), chronic myelomonocytic leukemia (CMML) and chronic myeloid leukemia (CML) constitute more than 50% of indications for allogeneic hematopoietic stem cell transplantation (aHSCT) in Europe [1,2]. Due to a potent graft-versus-leukemia (GvL) effect [3], aHSCT is the most effective antineoplastic treatment in these diseases and the only potentially curative treatment option. Depending on the individual risk profile, which is defined by underlying genetics, response to induction therapy or a history of preceding neoplasia and/or chemotherapy [4], relapse rates after aHSCT remain high and up to 50% of patients die of relapse [5]. Therefore, further improvement of conditioning regimens especially in elderly patients with a potentially high non-relapse mortality (NRM) [6] is an urgent medical need. Current sequential conditioning regimens combine intensive AML-like induction therapy with either myeloablative (MAC) or reduced intensity conditioning (RIC) using total body irradiation (TBI) or alkylators like Busulfan, Treosulfan and Melphalan [7-10]. The first and currently widely accepted prototype of this treatment strategy, which originally combined cytoreductive chemotherapy with reduced-intensity conditioning and prophylactic infusion of donor lymphocytes (DLIs), is the Fludarabine/Amsacrine/Ara-C (FLAMSA) protocol published by Schmid and Kolb in 2005 [4]. The aim was to balance effective eradication of the leukemic clone with the reduction of regimen-related toxicity. Over the years, this protocol has become one of the most often used conditioning regimens in Europe and has been modified multiple times by changing or adding additional cytotoxic drugs to further improve clinical results [11-15]. Although some protocols were less toxic (e.g. combination of FLAMSA with treosulfan), no study was able to show a higher efficacy [16, 17].
Venetoclax, an inhibitor of B-Cell Lymphoma-2 protein (BCL2), has been shown to selectively target leukemia stem cells (LSCs) due to their overexpression of BCL2. In addition animal studies showed that Venetoclax facilitated engraftment and GVL-effect in mice without higher rates of graft-versus-host-disease (GVHD) by pharmalogically controlling Natural-Killer cells [18, 19]. Knowing that Venetoclax has synergistic effects to chemotherapy without increasing the level of non-hematologic toxicity as it was shown in combination with azacytidine, decitabine or FLAG-Ida [20, 21], it has already been investigated in combination with RIC conditioning using Fludarabine und Busulfan [22]. To reduce relapse rates after aHSCT and improve long-term survival/outcome in patients with high-risk myeloid malignancies, several German transplant centres added Venetoclax to one of the well-known FLAMSA protocol variants as an individualized treatment approach.
2. Patients and Methods
2.1. Patients
Sixty-one patients (median age 58 years, range 20 - 74, 29 female) from six different German transplant centers who received FLAMSA based sequential conditioning in combination with Venetoclax between 2018 and 2022 were identified through questionnaires sent to members of the German Cooperative Transplant Study Group and included in this retrospective analysis. The study was approved by the ethics committee of the Heinrich-Heine University Duesseldorf and all patients gave written informed consent for individualized treatment. Patients suffered from myeloid malignancies (40 AML, 18 MDS, 2 CMML, and 1 CML) and 45 (74%) had high-risk genetic features. Sixty patients had active disease at time of transplant (19 untreated, 41 relapsed/refractory). For 44 patients, a 10/10 HLA matched donor was available (32 unrelated, 12 related) and 17 patients received allografts from mismatched donors (10 haploidentical, 7 with a 9/10 HLA match). Concomitant diseases were registered using the Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI) [23, 24]. At the time of analysis, the median follow-up time was 548 days (range 130-1398) in surviving patients. Detailed patient demographics are shown in Table 1.
2.2. Treatment
Patients received fludarabine 30 mg/m², amsacrine 100 mg/m² and cytarabine 2000 mg/m² on four consecutive days (FLAMSA). In patients > 60 years, cytarabine was age-adjusted to a dose of 1000 mg/m². To reduce the risk of a tumor lysis syndrome (TLS), two patients received low-dose cytarabine in an absolute dose of 100 mg per day on three consecutive days before FLAMSA. FLAMSA was then followed by Treosulfan 10 g/m² on three consecutive days in 22 patients (36%) and 29 patients (47.5%) received Melphalan in an age-adjusted dose of 100 – 200 mg/m² (200 mg/m² for patients < 50 years, 150 mg/m² for patients aged between 50 and 60 years, and 100 mg/m² for patients > 60 years). Within the groups of FLAMSA + Mel and FLAMSA + Treo, three patients and one patient, respectively, received Fludarabin/Cyclophosphamid in addition as published in the original protocol by Luznik et al. for patients with a haploidentical donor [25]. Eight patients (15%) were treated with the original FLAMSA+RIC protocol (4 Gy TBI on one day followed by cyclophosphamide 60 mg/kg body weight (BW) on 2 consecutive days) [4]. One patient received a combination of FLAMSA + cyclophosphamide + 8 Gy TBI while another patient had a combination of FLAMSA + 4 Gy TBI. Five out of ten patients with a haploidentical donor additionally received 2 Gy TBI at the day of transplant. Venetoclax was added one to two days before FLAMSA and continued until the first day after FLAMSA at a dose of 20 – 800 mg daily, with a total dose ranging between 380 – 4700 mg. Two patients were on continuous Venetoclax therapy before conditioning and received a total dose of 6370 mg and 9970 mg. A total of 42 patients (8 related, 34 unrelated donors) received ATG (Grafalon) in 3 daily doses between 5 and 20mg/kg. PtCy was administered to 15 patients (10 haplo, 5 MMUD) on day +3 and +4 after aHSCT in a dose of 50 mg/kg BW per day. Four patients with HLA-identical sibling donors did not receive either ATG or post-transplant cyclophosphamide. Immunosuppressive therapy following allografting consisted of a combination of tacrolimus and mycophenolate mofetil or cyclosporine A and mycophenolate mofetil according to institutional standards. Supportive care, like the application of granulocyte-colony stimulating factor to hasten neutrophil recovery and the administration of antimicrobial prophylaxis also followed institutional standards.
2.3. Monitoring and definitions
After discharge from the hospital, outpatient and subsequent treatment as well as the time of response evaluation followed institutional standards. Complete remission was defined as < 5 % blasts in the bone marrow (BM) by cytomorphology, no evidence of dysplasia and complete count recovery with platelet count > 100.000/µL and absolute neutrophil count > 1000/µl. Time of leukocyte engraftment was defined as the first of 3 consecutive days with a white blood cell count > 1000/µl. Concordantly, time of platelet engraftment was equivalent the first of 3 consecutive days with platelet counts > 20.000/µl. Grading of acute and chronic graft-versus-host disease (aGVHD, cGVHD) was performed according to the established criteria [26, 27].
2.4. Statistics
Event free survival (EFS), Relapse-free survival (RFS), Overall Survival (OS), non-relapse mortality (NRM) as well as treatment response and GVHD-onset were calculated from the day of transplantation to the respective event. Death – independent of its cause – was rated as an event in case of OS. Death and relapse were both separate events with regard to EFS. All time-to-event curves were estimated using the Kaplan-Meier method [28]. Statistical analyses were performed using IBM SPSS statistical software (Version 27).
3. Results
3.1. Hematologic reconstitution and chimerism
All evaluable patients successfully engrafted and hematologic reconstitution of white blood cells (WBC) >1000/µl occurred after a median of 15 days (range 8 – 41 days). Median time to platelet recovery was 19 days (range 2 – 78 days) with four patients (7%) never reaching > 20000 platelets/µl. Analysing hematopoietic reconstitution exclusively for those patients who did not receive ptCy, engraftment of WBC occurred after a median time of 13 days, while median time to platelet recovery was 17 days in these patients. At day +30, 52 patients (87%) had complete donor chimerism, while 4 patients (7%) had a donor chimerism < 90%. Three months after transplant 49 patients (83%) had complete donor chimerism while 5 patients (9%) had a donor chimerism < 90%.
3.2. Toxicity and infections
Tumor lysis syndrome (TLS) as the most dreaded side effect during the combination of FLAMSA and Venetoclax occurred in only two patients (3%). Toxicities and complications during inpatient stay were mainly infections as listed in Table 2. Veno-occlusive disease (VOD), a possibly life-threatening complication in transplant setting, occurred in one patient (1.6%) and was successfully treated with defibrotide. No significant extrahematologic toxicity possibly related to Venetoclax was observed.
3.3. Acute and chronic GVHD
Acute GVHD occurred in 37 patients (61%) with 24 patients (39%) developing grade I to II aGVHD and 13 patients (21%) grade III – IV aGVHD, with only one patient having grade IV GVHD. According to the National Institutes of Health (NIH) criteria, 24 patients (39%) had classic aGVHD and 12 patients (20%) had late-onset aGVHD. According to the NIH criteria for chronic GVHD, 16 patients (26%) had cGVHD, with 11 patients (18%) having mild to moderate and 5 patients (8%) suffering from severe cGVHD. Treatment of GVHD followed institutional standards. Rates of aGVHD and cGvHD are shown in Figure 1.
3.4. Disease response, relapse and survival
At day +30 after aHSCT, 25 patients (41%) achieved a complete hematological remission. Thirty patients (50%) had complete hematological remission with incomplete recovery (CRi), i.e. meaning a platelet count <100 x 109/L and/or an absolute neutrophil count < 1 x 109/L resulting in a CR/CRi rate of 91%. Five patients (8%) had ongoing active disease and one patient was not evaluable due to early death in aplasia on day +15 from septic shock. After a median follow-up of 548 days, 44 patients (72%) were alive (38 patients in ongoing remission, 8 patients after salvage therapy and 6 patients in relapse receiving further treatment). Twenty-three patients (38%) experienced relapse after a median of 172 days (range 62 - 943). Of note, 5 of these patients (22% of relapsed patients) had extramedullary AML manifestations without bone marrow involvement. Of the 5 patients who had active disease at day +30 after aHSCT, 2 patients were alive in complete remission (one after accelerated reduction of immunosuppressive therapy, hereby developing aGVHD and the other one after salvage therapy with hypomethylating agents plus Venetoclax and DLIs). The remaining 3 patients died from their disease. Seven patients (12%) received DLIs in the context of salvage chemotherapy which led to a second, ongoing remission after aHSCT in 3 patients. Another 5 patients (8%) underwent secondary aHSCT after relapse, of whom 3 patients were still alive at the time of analysis. There was a statistically significant difference regarding cumulative incidence of relapse between pre-treated patients and those who underwent upfront aHSCT (p = 0.014) as shown in Figure 2. Relapse occurred less frequent and later in time in patients that had not received any antineoplastic treatment before conditioning. Among all patients overall and event-free survival were 80% and 64% at 1 year as well as 75% and 57% at 2 years, respectively (Figure 3). Classifying patients into two groups regarding the type of donor (10/10 match vs. mismatched donor including haplo and MMUD 9/10), the difference in OS was of borderline significance in favour of 10/10 matched donors (p=0.09). Treatment-related mortality (TRM) was 2% at 3 months and 7% at 1 year. Cumulative incidence of TRM is shown in Figure 4. In total, 17 patients (28%) died. Of these, 12 patients (20%) died because of relapse, 2 patients (3%) had lethal infections and in three patients (5%) death was related to infections in the context of severe GVHD.
4. Discussion
The results of this multi-center, retrospective analysis suggest that the combination of sequential FLAMSA + Venetoclax in a RIC-setting may be a new treatment option for patients with high-risk myeloid malignancies and active disease. In the light of older patient populations, TRM is one of the most critical aspects that needs to be considered when deciding which conditioning regimen might be most suitable for each individual patient. Therefore escalation of dose intensity is not possible in elderly or comorbid patients. The BCL-2 inhibitor Venetoclax recently has become an essential element of AML treatment, especially in elderly patients considered unfit for intensive therapy. Following approval in combination with hypomethylating agents a large amount of data on toxicity and efficacy has been published. Venetoclax has been shown to be highly effective in combination with hypomethylating agents or FLAG-Ida [20, 21]. In addition, Venetoclax demonstrated increased donor engraftment in the setting of RIC while avoiding the toxicity and GVHD-priming effects of MAC in a mouse model [30]. Furthermore, Venetoclax was able to suppress recipient NK cell function via inhibition of BCL2 in mice, thereby avoiding graft rejection without the toxicities associated with more intensive conditioning, including GVHD [19]. The aim of combining FLAMSA with Venetoclax was to increase the efficacy of RIC to the level of MAC regimens without generating MAC-equivalent toxicity.
With a median age of 58 years (range 20 – 74), our patient cohort has been older as compared to most earlier publications on the FLAMSA regimen [7, 9, 29]. Furthermore, with one third of patients having an HCT-CI ≥ 3, our study population had significant underlying health conditions. With this retrospective analysis, we demonstrate good tolerability even in older patients with relatively low TRM (7% at 1 year) compared to prior analyses as for example FLAMSA in combination with melphalan in patients with high-risk myeloid malignancies who underwent upfront aHSCT [13]. There was only one early death from sepsis. Hematopoietic reconstitution occurred after a median of 15 days regarding white blood cell count and 19 days regarding platelets, which is in line with previous studies using FLAMSA-RIC [12, 31, 32]. At day +30 after aHSCT, we observed a cumulative CR rate of 91%, which is again in line with response rates of FLAMSA-based conditioning in the literature [33, 34]. There was no difference compared to previous FLAMSA-RIC studies regarding cumulative incidence of acute and chronic GVHD occurring in 61% and 26%, respectively [8, 35, 36].
Relapse rate remained significant especially in relapsed/refractory disease, with 23 patients (38%) experiencing relapse after a median of 172 days. This is comparable to results of other studies using FLAMSA based conditioning regimens. In the context of active disease (AD) relapse rates in our study are lower than published by Schneidawind et al. or Pfrepper et al. They treated patients with R/R AML in AD with FLAMSA + RIC and documented relapse rates of 52% and 69%, respectively [37, 38]. Patients experiencing relapse could be subdivided into early (<12 months post aHCST) and late relapses (> 12 months after aHSCT) with 14 out of 23 relapses (61%) occurring within the first year. Eighty-seven percent of these patients with early relapse had either a complex karyotype or unfavorable disease risk at diagnosis according to molecular analyses. Regarding those patients who underwent upfront aHSCT, only 3 out of 19 patients (16%) experienced relapse so far. All were late relapses as shown in Figure 2. These observations are in line with the analyses of Platte et al., who found cytogenetics, disease risk stratification at diagnosis and pretransplant strategies to be major determinants for the time of relapse. [39]. Our data regarding timely reconstitution of neutrophils and platelets, rate of acute and chronic GVHD, no additional extra hematologic toxicity as well as early response and relapse are in line with the results of Garcia et al. who added Venetoclax to Fludarabin/Busulfan and evaluated the combination as feasible and safe [22]. There are further plans to investigate the combination of conditioning regimens and Venetoclax in the future. In Melbourne for example, a phase I study in patients with different hematologic malignancies assessing the combination of Venetoclax and Fludarabine/Cyclophosphamide (NCT05005299) is planned while there will be a randomized phase II study assessing the combination of Venetoclax and Sequential Busulfan, Cladribine, and Fludarabine in patients with AML or MRD (NCT 02250937) at the MD Anderson Center [40, 41].
With respect to limitations of our analysis, its retrospective aspect as well as the underlying heterogeneous collective of patients from six different transplant centers in Germany need to be mentioned. Patients received different types of conditioning regimens with different doses of Venetoclax, therefore our analyses are not based on standardized therapies. In addition, supportive care like for example administration of antimicrobial prophylaxis or immunosuppressive therapy followed local institutional standards as well.
To objectify and further validate our insights a controlled prospective trial to evaluate the maximum tolerated dose of Venetoclax in combination with FLAMSA will be the next step. If these early results can be confirmed in a phase I / II study, a randomized controlled trial testing FLAMSA + Venetoclax compared to standard of care is needed.
5. Conclusions
The combination of sequential FLAMSA + RIC with Venetoclax may be a smart way to extend the limited therapy options of patients with high-risk myeloid malignancies as it appears to be safe and highly effective without increasing the rate of non-hematologic toxicity. To further validate these insights and enhance the idea of smart conditioning, a controlled prospective clinical trial should be the next step.
Author Contributions
Conceptualization, G.K and F.S.; methodology, G.K.; formal analysis, F.S.; investigation, G.K. and F.S.; resources, software, SPSS version 27; data curation, G.K., J.T., G.B., J.S., I.H., A.H.; writing—original draft preparation, F.S.; writing—review and editing, G.K. and K.N.; visualization, F.S.; supervision, G.K.; project administration, G.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Heinrich-Heine University in Duesseldorf (protocol code 2022-2203, 23.12.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. The data are not publicly available due to ethical restrictions.
Conflicts of Interest
GK: Advisory Role, Speaker Honoraria and/or travel support: MSD, Pfizer, Amgen, Novartis, Gilead, BMS-Celgene, Abbvie, Medac, Biotest, Takeda, Eurocept; Financing of Scientific Research: BMS-Celgene, Amgen, Abbvie, Eurocept, Medac. GB has received honoraria from Novartis, Jazz, BMS, Gilead and Pfizer and travel grants from Jazz, Gilead and Neovii. JS Advisory Boards organized by Abbvie, AstraZeneca, BeiGene, BMS and JanssenLecture Fees from Astellas, AstraZeneca, BeiGene, BMS, Novartis, Eurocept and Janssen.
References
- Passweg JR, Baldomero H, et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: monitoring of activities and trends over 30 years. Bone Marrow Transplant. 2021, Jul;56(7), 1651-1664. [CrossRef]
- Passweg JR, Baldomero H, et al. Impact of the SARS-CoV-2 pandemic on hematopoietic cell transplantation and cellular therapies in Europe 2020: a report from the EBMT activity survey. Bone Marrow Transplant. 2022, May;57(5), 742-752. [CrossRef]
- Kolb HJ, Schmid C, et al. Graft-versus-leukemia reactions in allogeneic chimeras. Blood. 2004, Feb 1;103(3), 767-76. [CrossRef]
- Schmid C, Schleuning M, et al. Sequential regimen of chemotherapy, reduced-intensity conditioning for allogeneic stem-cell transplantation, and prophylactic donor lymphocyte transfusion in high-risk acute myeloid leukemia and myelodysplastic syndrome. J Clin Oncol., 2005 Aug 20;23(24), 5675-87. [CrossRef]
- Horowitz M, Schreiber H, et al. Epidemiology and biology of relapse after stem cell transplantation. Bone Marrow Transplant, 2018, Nov;53(11), 1379-1389. [CrossRef]
- Weller JF, Lengerke C, et al. Allogeneic hematopoietic stem cell transplantation in patients aged 60-79 years in Germany (1998-2018): a registry study. Haematologica, 2023, Aug 31. [CrossRef]
- Meur GL, Plesa A, et al. Impact on Outcome of Minimal Residual Disease after Hematopoietic Stem Cell Transplantation with Fludarabine, Amsacrine, and Cytosine Arabinoside-Busulfan Conditioning: A Retrospective Monocentric Study. Transplant Cell Ther., 2023, Jan;29(1), 38.e1-38.e9. [CrossRef]
- Jondreville L, Roos-Weil D, et al. FLAMSA-Busulfan-Melphalan as a Sequential Conditioning Regimen in HLA-Matched or Haploidentical Hematopoietic Stem Cell Transplantation for High-Risk Myeloid Diseases. Transplant Cell Ther., 2021, Nov;27(11), 915.e1-915.e8. [CrossRef]
- Holtick U, Herling M, et al. Similar outcome after allogeneic stem cell transplantation with a modified FLAMSA conditioning protocol substituting 4 Gy TBI with treosulfan in an elderly population with high-risk AML. Ann Hematol., 2017, Mar;96(3), 479-487. [CrossRef]
- Malard F, Labopin M, et al. Sequential Intensified Conditioning Regimen Allogeneic Hematopoietic Stem Cell Transplantation in Adult Patients with Intermediate- or High-Risk Acute Myeloid Leukemia in Complete Remission: A Study from the Acute Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Biol Blood Marrow Transplant., 2017, Feb;23(2), 278-284. [CrossRef]
- Zohren F, Czibere A, et al. Fludarabine, amsacrine, high-dose cytarabine and 12 Gy total body irradiation followed by allogeneic hematopoietic stem cell transplantation is effective in patients with relapsed or high-risk acute lymphoblastic leukemia. Bone Marrow Transplant., 2009, Dec;44(12), 785-92. [CrossRef]
- Chemnitz JM, von Lilienfeld-Toal M, et al. Intermediate intensity conditioning regimen containing FLAMSA, treosulfan, cyclophosphamide, and ATG for allogeneic stem cell transplantation in elderly patients with relapsed or high-risk acute myeloid leukemia. Ann Hematol., 2012, Jan;91(1), 47-55. [CrossRef]
- Saure C, Schroeder T, et al. Upfront allogeneic blood stem cell transplantation for patients with high-risk myelodysplastic syndrome or secondary acute myeloid leukemia using a FLAMSA-based high-dose sequential conditioning regimen. Biol Blood Marrow Transplant., 2012, Mar;18(3):, 466-72. [CrossRef]
- Christopeit M, Badbaran A, et al. Correlation of somatic mutations with outcome after FLAMSA-busulfan sequential conditioning and allogeneic stem cell transplantation in patients with myelodysplastic syndromes. Eur J Haematol., 2016, Sep;97(3):, 288-96. [CrossRef]
- Fraccaroli A, Prevalsek D, et al. Sequential HLA-haploidentical transplantation utilizing post-transplantation cyclophosphamide for GvHD prophylaxis in high-risk and relapsed/refractory AML/MDS. Am J Hematol, 2018, Dec;93(12):1524-1531. [CrossRef]
- Gernot Beutel SB, Marie von Lilienfeld, et al. Comparison of sequential conditioning regimens for allogeneic stem cell transplantation in relapsed/refractory AML: A study on behalf of the ALWP of EBMT - The 45th Annual Meeting of the European Society for Blood and Marrow Transplantation: Physicians – Oral Session. Bone Marrow Transplantation, 2019, 54, 55-56.
- Thomas Heinicke, Myriam Labopin, et al. Evaluation of six different types of sequential conditioning regimens for allogeneic stem cell transplantation in relapsed/refractory acute myelogenous leukemia – a study of the Acute Leukemia Working Party of the EBMT, Leukemia & Lymphoma, 2021, 62:2, 399-409. [CrossRef]
- Pollyea DA, Stevens BM, et al. Venetoclax with azacitidine disrupts energy metabolism and targets leukemia stem cells in patients with acute myeloid leukemia. Nat Med., 2018, Dec;24(12), 1859-1866. [CrossRef]
- Jiao Y, Davis JE, et al. Recipient BCL2 inhibition and NK cell ablation form part of a reduced intensity conditioning regime that improves allo-bone marrow transplantation outcomes. Cell Death Differ., 2019, Aug;26(8), 1516-1530. [CrossRef]
- DiNardo CD, Pratz K, et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood, 2019, Jan 3;133(1), 7-17. [CrossRef]
- DiNardo CD, Lachowiez CA, et al. Venetoclax Combined With FLAG-IDA Induction and Consolidation in Newly Diagnosed and Relapsed or Refractory Acute Myeloid Leukemia. J Clin Oncol., 2021, Sep 1;39(25), 2768-2778. [CrossRef]
- Garcia JS, Kim HT, et al. Adding venetoclax to fludarabine/busulfan RIC transplant for high-risk MDS and AML is feasible, safe, and active. Blood Adv., 2021, Dec 28;5(24), 5536-5545. [CrossRef]
- Sorror ML, Sandmaier BM, et al. Comorbidity and disease status based risk stratification of outcomes among patients with acute myeloid leukemia or myelodysplasia receiving allogeneic hematopoietic cell transplantation. J Clin Oncol., 2007, Sep 20;25(27), 4246-54. [CrossRef]
- Sperr WR, Wimazal F, et al. Comorbidity as prognostic variable in MDS: comparative evaluation of the HCT-CI and CCI in a core dataset of 419 patients of the Austrian MDS Study Group. Ann Oncol., 2010, Jan;21(1), 114-9. [CrossRef]
- Luznik L, O'Donnell PV, et al. HLA-haploidentical bone marrow transplantation for hematologic malignancies using nonmyeloablative conditioning and high-dose, posttransplantation cyclophosphamide. Biol Blood Marrow Transplant., 2008, Jun;14(6), 641-50. [CrossRef]
- Glucksberg H, Storb R, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation, 1974, Oct;18(4), 295-304. [CrossRef]
- Filipovich AH, Weisdorf D, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant, 2005, Dec;11(12), 945-56. [CrossRef]
- Kaplan, E. L., and Paul Meier. Nonparametric Estimation from Incomplete Observations. J Am Stat Assoc., 1958, 53, 457–81. [CrossRef]
- Bohl S, von Harsdorf S, et al. Strong impact of extramedullary involvement in high-risk AML patients with active disease receiving the FLAMSA conditioning regimen for HSCT. Bone Marrow Transplant., 2016, Jul;51(7), 994-6. [CrossRef]
- Davis JE, Du K, et al. Venetoclax or Ruxolitinib in Pre-Transplant Conditioning Lowers the Engraftment Barrier by Different Mechanisms in Allogeneic Stem Cell Transplant Recipients. Front Immunol., 2021, Sep 24;12, 749094. [CrossRef]
- Schmid C, Schleuning M, et al. Early allo-SCT for AML with a complex aberrant karyotype--results from a prospective pilot study. Bone Marrow Transplant., 2012, Jan;47(1), 46-53. [CrossRef]
- Krejci M, Doubek M, et al. Combination of fludarabine, amsacrine, and cytarabine followed by reduced-intensity conditioning and allogeneic hematopoietic stem cell transplantation in patients with high-risk acute myeloid leukemia. Ann Hematol., 2013, Oct;92(10), 1397-403. [CrossRef]
- Schmid C, Schleuning M, et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood, 2006, Aug 1;108(3), 1092-9. [CrossRef]
- Pfeiffer T, Schleuning M, et al. Influence of molecular subgroups on outcome of acute myeloid leukemia with normal karyotype in 141 patients undergoing salvage allogeneic stem cell transplantation in primary induction failure or beyond first relapse. Haematologica, 2013, Apr;98(4), 518-25. [CrossRef]
- Holtick U, Shimabukuro-Vornhagen A, et al. FLAMSA reduced-intensity conditioning is equally effective in AML patients with primary induction failure as well as in first or second complete remission. Eur J Haematol., 2016, May;96(5), 475-82. [CrossRef]
- Christopeit M, Badbaran A, et al. Correlation of somatic mutations with outcome after FLAMSA-busulfan sequential conditioning and allogeneic stem cell transplantation in patients with myelodysplastic syndromes. Eur J Haematol., 2016, Sep;97(3), 288-96. [CrossRef]
- Schneidawind D, Federmann B, et al. Allogeneic hematopoietic cell transplantation with reduced-intensity conditioning following FLAMSA for primary refractory or relapsed acute myeloid leukemia. Ann Hematol., 2013, Oct;92(10), 1389-95. [CrossRef]
- Pfrepper C, Klink A, et al. Risk factors for outcome in refractory acute myeloid leukemia patients treated with a combination of fludarabine, cytarabine, and amsacrine followed by a reduced-intensity conditioning and allogeneic stem cell transplantation. J Cancer Res Clin Oncol, 2016, Jan;142(1), 317-24. [CrossRef]
- Platte V, Bergmann A, et al. Clinical and Cytogenetic Characterization of Early and Late Relapses in Patients Allografted for Myeloid Neoplasms with a Myelodysplastic Component. Cancers (Basel), 2022, Dec 18;14(24), 6244. [CrossRef]
- https://clinicaltrials.gov/study/NCT05005299?cond=Venetoclax&term=conditioning&rank=1.
- https://clinicaltrials.gov/study/NCT02250937?cond=Venetoclax&term=conditioning&rank=9.
Figure 1.
Rates of acute and chronic GVHD.
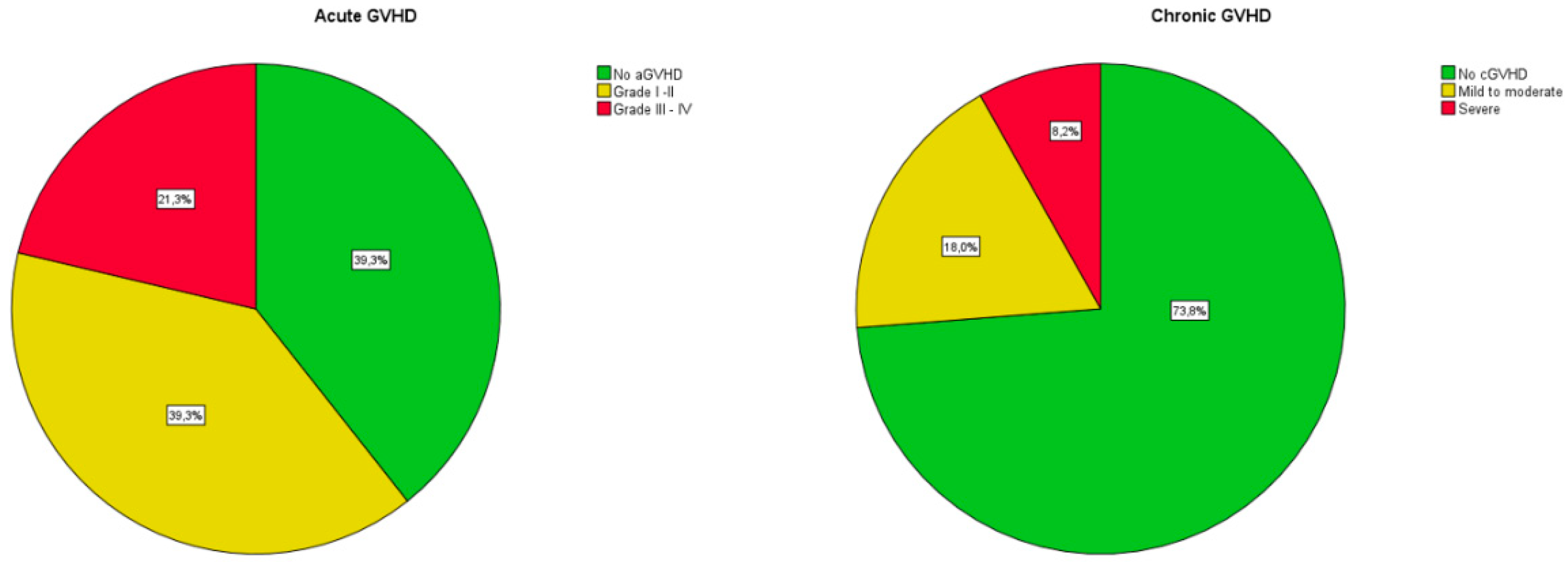
Figure 2.
Cumulative incidence of relapse.
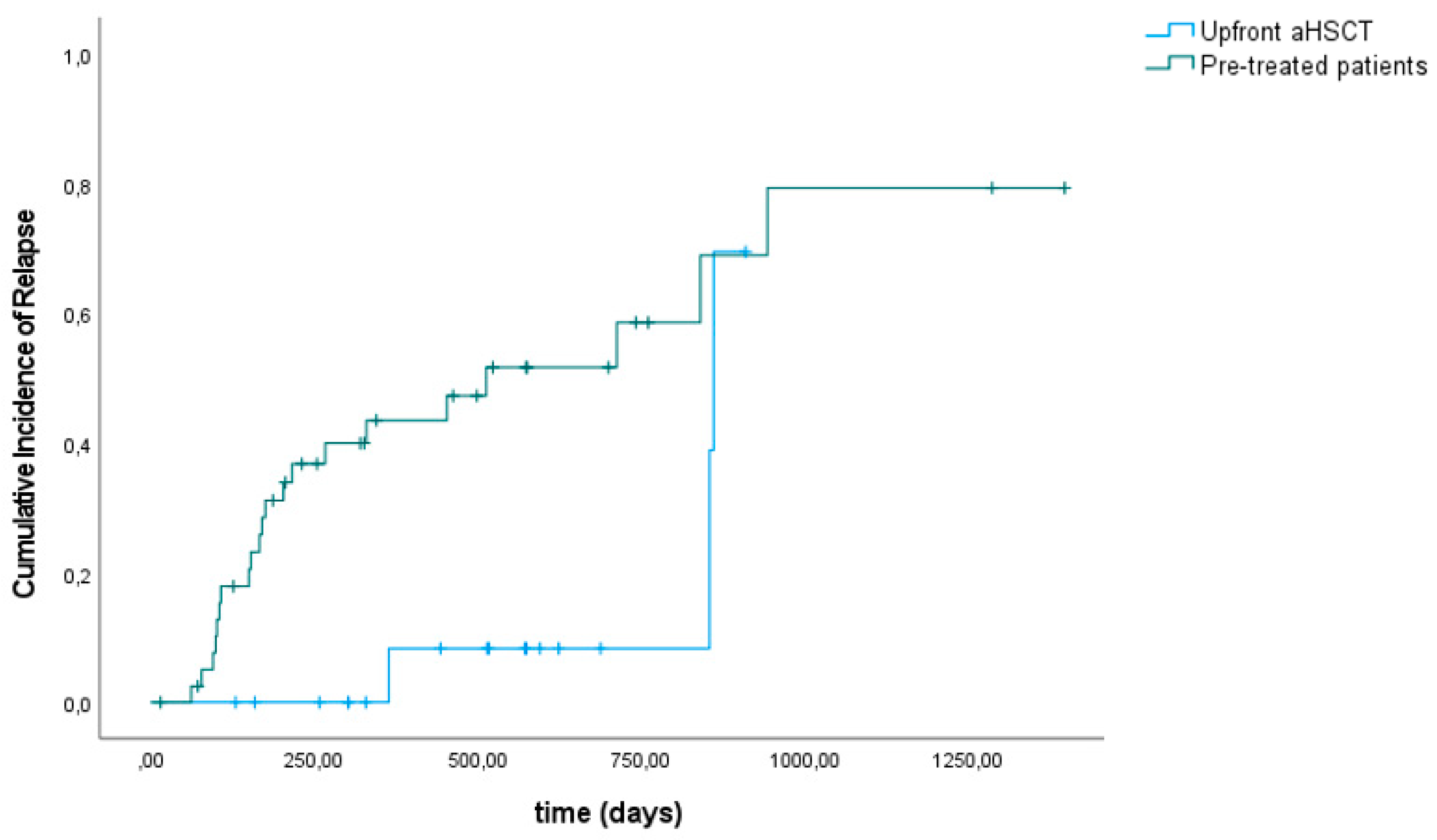
Figure 3.
Overall Survival.
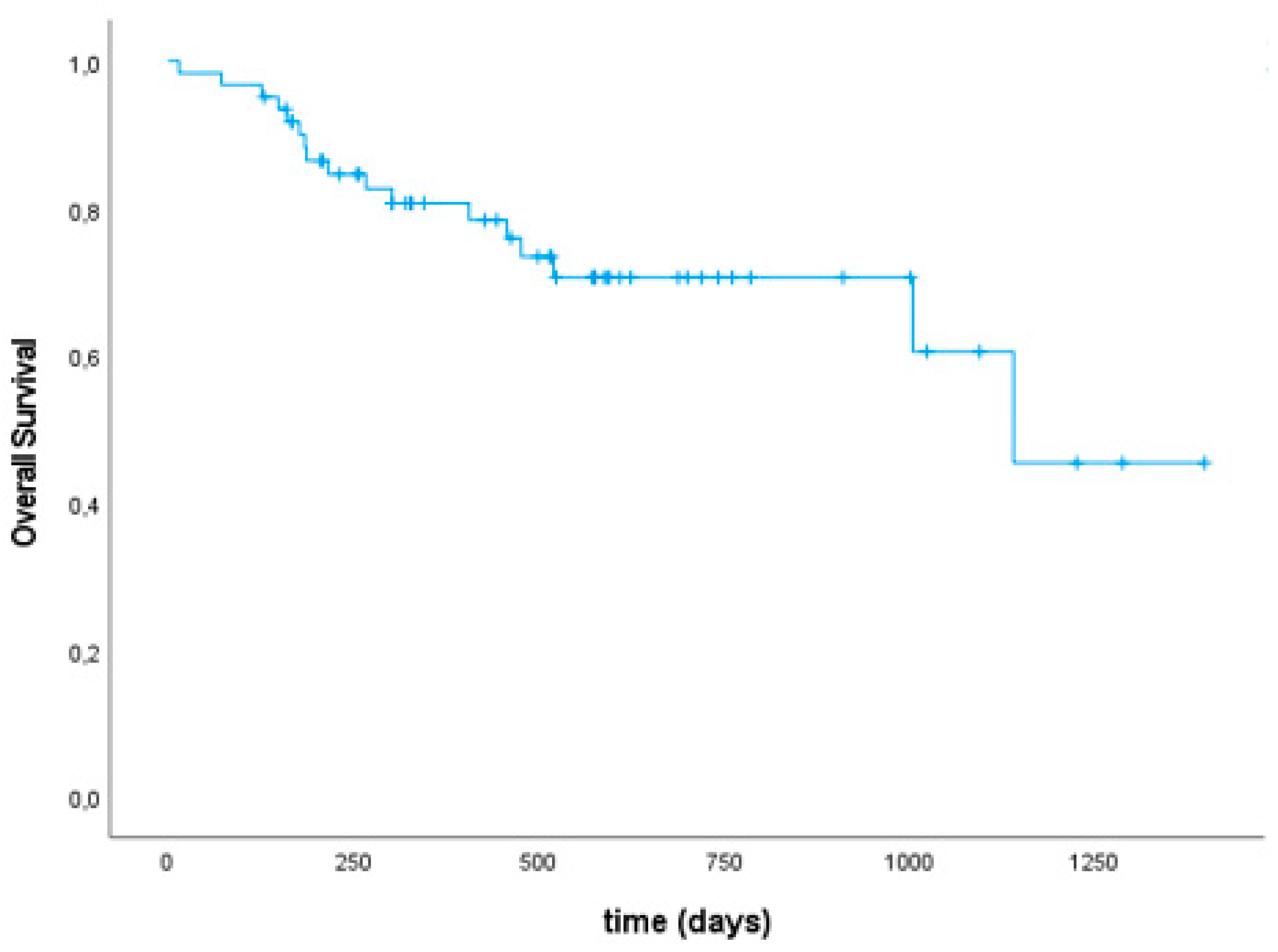
Figure 4.
Cumulative Incidence of NRM.
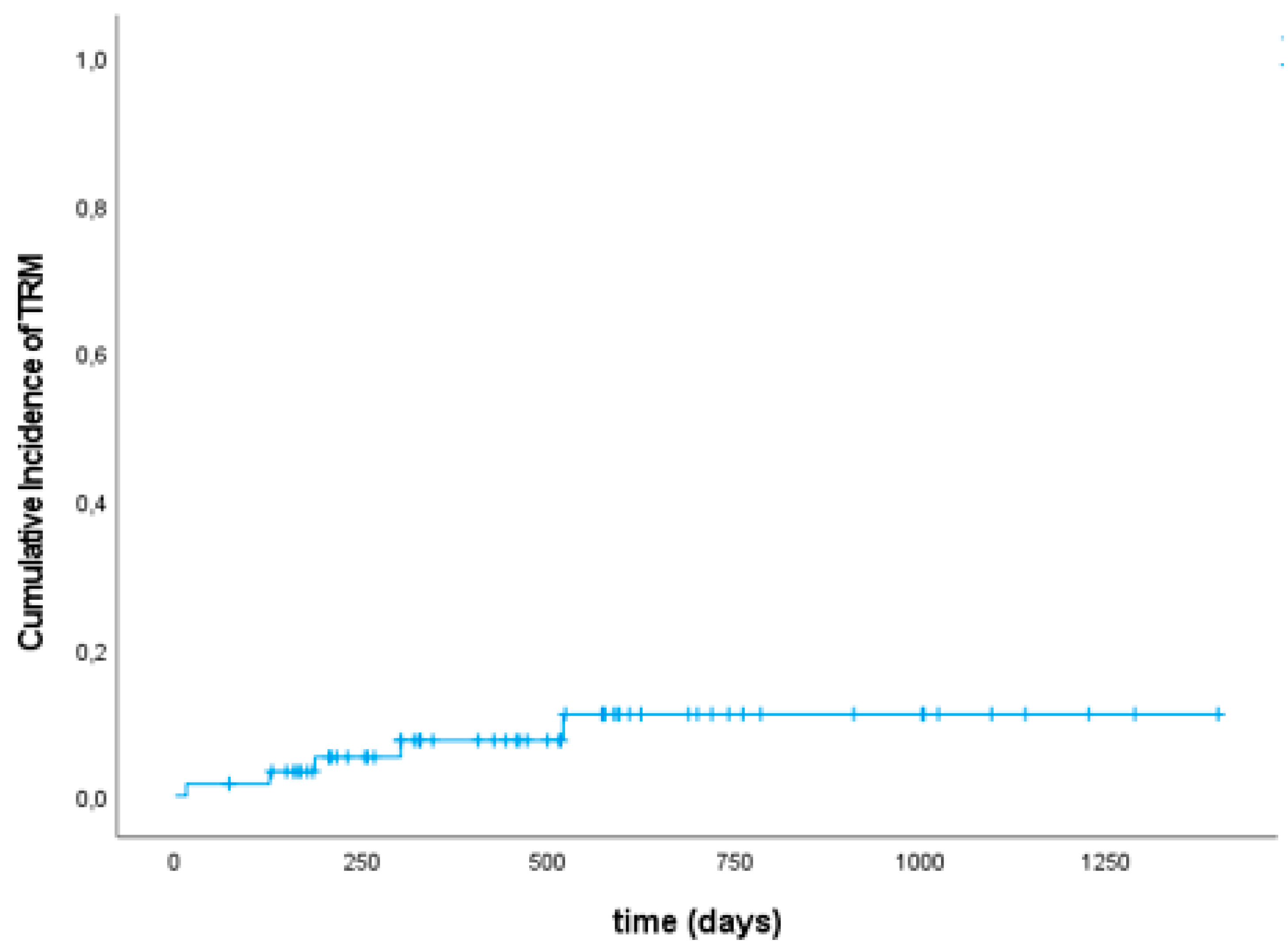

Table 1.
Patient demographics.
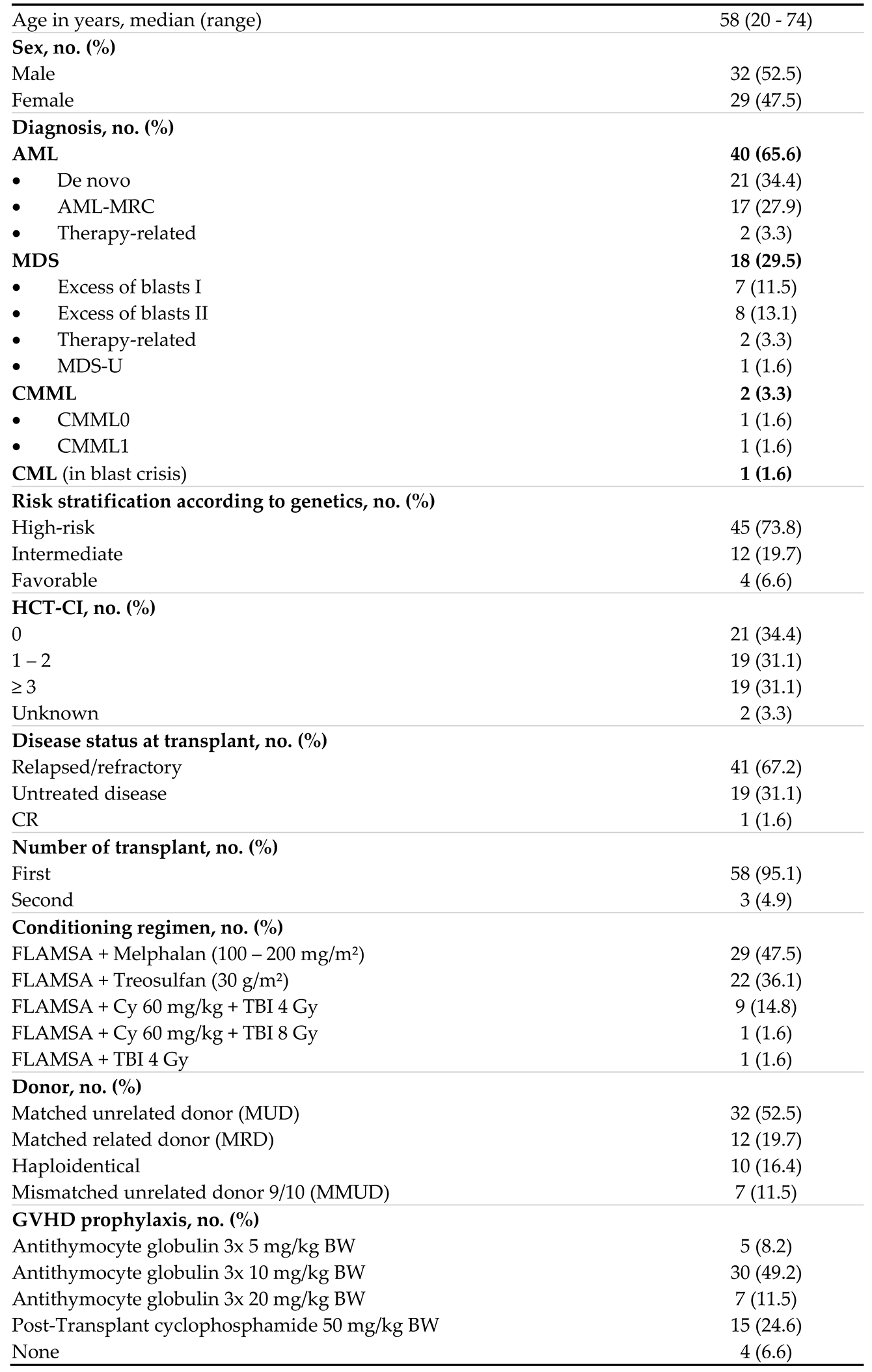 |
Table 2.
Toxicities and complications.
| No. (%) | |
| Infectious | |
|
4 (6.6) 2 (3.3) 1 (1.6) 1 (1.6) 1 (1.6) 1 (1.6) 1 (1.6) |
|
4 (6.6) 3 (4.9) 1 (1.6) 1 (1.6) |
|
5 (8.2) |
|
2 (3.3) 2 (3.3) 1 (1.6) 1 (1.6) 1 (1.6) |
Cardiac
|
3 (4.9) 1 (1.6) 1 (1.6) |
Hemorrhagic
|
1 (1.6) 1 (1.6) |
Other
|
2 (3.3) 1 (1.6) 1 (1.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



