
Submitted:
21 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Background: The implementation of tyrosine kinase inhibitors (TKIs) in the treatment of chronic myeloid leukemia (CML) has brought a significant improvement in the prognosis for CML patients and a decrease in the number of patients requiring allogeneic hematopoietic stem cell transplantation (allo-HCT). Nevertheless, the impact of TKIs on allo-HCT outcomes have not been thoroughly explored. Objectives: The main endpoint of our research was to assess the impact of prior TKI treatment on acute graft-versus-host disease (aGvHD) and chronic graft-versus-host disease (cGvHD). Methods: In our retrospective analysis we included 240 patients treated between 1993 and 2013, and divided them into 3 groups according to the therapy administered prior to matched related or matched unrelated donor allo-HCT (imatinib group n=41, dasatinib/nilotinib group n=28, TKI naïve group n=171). Results: Both the cumulative incidence of aGvHD (p=0.044) and cGvHD (p<0.001) in individuals receiving second generation TKIs (2G-TKIs) prior to allo-HCT compared to patients receiving no TKIs or imatinib (IMA) (40.7% vs 61.4% vs 70.7%, p=0.044; 25.0% vs 76.4% vs 51.2%, p<0.001, respectively). In case of the 2G-TKI cohort, the number of low-grade aGvHD and cGvHD was significantly lower compared to the IMA and TKI-naïve groups (p=0.018, p=0.004; p<0.001 versus TKI-naïve, respectively). In terms of 3-year overall survival (OS) there were no important variations between TKI-naïve, IMA and 2G-TKI (55% vs 49.9% vs 69.6%, p=0.740). Conclusions: The results of our study suggest that TKI treatment prior to allo-HCT may have protective impact on immune-mediated outcomes.
Keywords:
allogeneic hematopoietic stem cell transplantation
; chronic myeloid leukaemia
; tyrosine kinase inhibitors
; imatinib
; dasatinib
; nilotinib
1. Introduction
Tyrosine kinase inhibitors (TKIs) have become a widely accepted therapeutic approach for patients diagnosed with chronic myeloid leukaemia (CML) ever since the introduction of the first TKI in the late 1990s, that is imatinib mesylate [1]. The groundbreaking outcomes of the IRIS trial further solidified their pivotal role in revolutionising the management of this hematopoietic malignancy [2]. 2G-TKIs, especially dasatinib and nilotinib, have demonstrated highly promising results in cases of imatinib resistance or intolerance, yielding a long-term OS rate exceeding 70% [3,4]. Moreover, in newly diagnosed CML patients, the 5-year cumulative probability of achieving a major molecular response (MMR) exceeds 75%, markedly surpassing the corresponding rate attained with imatinib [5,6]. Although TKIs have proven to be effective, allo-HCT continues to be a viable and potentially curative alternative for patients who do not achieve long-lasting responses to TKI-based therapies or for those with advanced-stage disease [7,8,9].
The significance of allo-HCT in achieving long-term survival and potential cure for patients diagnosed with chronic phase CML (CML-CP) was well-established before the advent of TKIs [10,11]. The concept of a graft-versus-leukemia effect in CML gained support from studies demonstrating that donor lymphocyte infusion could effectively salvage relapsed disease after allo-HCT [12,13]. However, the number of performed allo-HCTs for CML in the first chronic phase (CP1) has substantially diminished following the introduction of TKIs [14]. Currently, the majority of patients referred to allo-HCT are those considered at high-risk, that is at disease stages beyond CP1, or those that have experienced treatment failure with TKIs [15,16]. According to the latest update on CML management [17], allo-HCT has been suggested to be a viability in CML-CP with resistance to 2G-TKI therapy with no guiding mutations or in cases of a potential T315I mutation after either ponatinib or asciminib treatment on a trial basis [18,19]. The blast phase of CML (CML-BP) is different from the CP, as it rather resembles acute leukaemia, displaying substantial changes in proliferation, differentiation, and apoptosis, leading to pronounced alterations in treatment response [20]. Despite a significant reduction in the incidence of CML-BP with the introduction of TKIs compared to the pre-TKI era [21], responses to TKI treatment in CML-BP patients are of temporary character, and their prognosis remains poor despite advancements in drug development [22]. Hence, allo-HCT remains the sole curative option for this subgroup of patients, and TKIs may offer a therapeutic window that allows for the possibility of allografting [21,22]. Currently individuals with CML accelerated phase (CML-AP) or CML blast phase (CML-BP) might undergo TKI treatment in order to lower the CML burden (preferably with newer generations of TKIs such as ponatinib or dasatinib), and should afterwards be considered for early allo-HCT [23].
According to previous research, the use of imatinib does not negatively impact transplant outcomes including acute and chronic graft-versus-host disease (aGvHD/cGvHD) [24,25,26,27,28]. Similarly, trials designed to evaluate 2G-TKI treatment prior to allo-HCT have not provided any evidence of 2G-TKIs having a harmful effect on the post-transplantation period [29,30,31,32]. Also, prior exposure to TKIs could potentially result in patients having better allo-HCT outcomes if transplantation is performed in a better molecular response status [27,29]. Considering the numerous roles of kinases in the GvHD pathophysiology, it was supposed that the administration of TKIs could represent a potentially effective approach for regulating the activation of B and T cells, resulting effective in the treatment of GvHD [33]. Both first generation TKIs (1G-TKIs) as well as 2G-TKI therapies (dasatinib, nilotinib) have been demonstrated to be effective in the treatment of steroid-refractory cGvHD (SR-cGvHD), including sclerotic cGvHD [34,35,36,37]. Furthermore, inhibitors targeting Janus Associated Kinases (JAK1 and JAK2) hold promise in the management of SR-cGvHD and steroid-refractory aGvHD (SR-aGvHD) with, for instance, ruxolitinib (targeting both JAK1 and JAK2) being approved by the Food and Drug Administration (FDA) and European Medicines Agency (EMA) for cGvHD after failure of one or two lines of systemic therapy and SR-aGvHD [33,38,39]. It should be noted that increased direct drug toxicity [40] or immune dysfunction [41,42] may also limit the success of allo-HCT, considering that each TKI has multiple off-target effects.
This retrospective study on behalf of the Polish Adult Leukaemia Group (PALG) aims to compare GvHD and survival outcomes of allo-HCT of three groups comprising a cohort of patients from the pre-TKI era and individuals underwent either 1G-TKI or 2G-TKI treatment prior to transplantation, all of whom suffered from CML.
2. Materials and Methods
Patients
This analysis is focused on CML patients treated with allo-HCT in different treatment eras. We analysed three groups of patients: TKI naïve, so called historic group, collecting patients transplanted before imatinib era, the second one (IMA) with patients transplanted after imatinib failure before 2G-TKIs became widely available and he last one transplanted after second generation TKIs failure (2G-TKI; dasatinib or nilotinib) used as a second line treatment after imatinib failure. The patients were treated in several PALG associated centres between 1993 and 2013. Into the statistical analysis there were taken variables such as sex, patients’ age, disease duration before transplant, using interferon alfa (IFNα) and TKIs during the treatment and its duration, CML phase at day of transplant, conditioning regimen, application of GvHD prophylaxis, presence and grade of acute and chronic GvHD after the procedure of allo-HCT, evaluation in Karnofsky scale, AB0 mismatch, transplant risk category (using the Grathwohl scale), CMV status. All of the patients underwent matched related or matched unrelated donor (MRD/MUD) allo-HCT with reduced intensity or myeloablative conditioning regimens (RIC/MAC). GvHD prophylaxis followed standard protocols, which comprised cyclosporine A (CsA), methotrexate (MTX), and in cases of a MUD also anti-thymocyte globulin (ATG). Patient-, donor- and transplant-related characteristics can be found in Table 1 and Table 2.
Definitions
CML chronic and advanced phases were diagnosed according to ELN criteria [43,44]. aGvHD diagnosis and grading was based on 1994 consensus [45] with an update of MAGIC consortium [46]. The diagnosis and global scoring of chronic graft versus host disease came from National Institute of Health 2005 criteria [47] but we had to combine cases scored 2 and 3 in one group to standardise the grading in all three groups. The historic group grading was based on traditional Seattle 1980 criteria [48] referring to “limited” and “extensive” chronic GvHD cases. To make the analysis clear we put NIH 2005 score 2 and 3 cases (from ”new era” transplantations) and Seattle “extensive” cases in one advanced group - 2. NIH score 1 and “limited” Seattle cases were put in one group as well - 1.
Study endpoints
The main objective of this retrospective analysis is to assess the impact of 1G-TKI and 2G-TKI treatment on the development of aGvHD and cGvHD in individuals with CML undergoing allo-HCT. The secondary outcomes included 3-year OS.
Statistical Analysis
Statistica v.13.3 (TIBCO Software Inc., Palo Alto, CA, USA) was used for statistical analysis. Verification of normality of quantitative variables was performed using the Shapiro-Wilk test. Due to the absence of normal distribution characteristics or heterogeneity of variance, the statistical significance of differences between the three groups was assessed using the non-parametric Kruskal-Wallis test. The significance of differences in frequencies for qualitative variables was calculated using the chi-square test. The Kaplan-Meier estimator was used to estimate survival probabilities. The significance of differences between survival curves in the three groups was verified by the chi-square test. Statistical test results were deemed statistically significant when the p value was < 0.05. In multivariate analysis, considering that aGvHD and cGvHD are binary variables, logistic regression was employed. The results of multivariate analysis are presented in Table 3.
3. Results
Patient-, disease-, and transplantation-related characteristics
The characteristics for all individuals divided into 3 subgroups - TKI-naïve (n=171), IMA (n=41) and 2G-TKI (n=28) are presented in Table 1 and Table 2. The 2G-TKIs used prior to allo-HCT were either dasatinib or nilotinib while the 1G-TKI was imatinib. The disproportion in the number of individuals in each cohort is a consequence of the introduction of TKIs, which drastically reduced the number of performed allo-HCTs. The characteristics n the three groups were comparable with regard to patient sex and donor sex/age. The individuals in the 2G-TKI group were significantly older (37 vs 35 vs 48 years of age, p<0.001), likely due to the refinement of CML therapy resulting in a longer time-to-transplant period. The ratios of MRD/MUD allo-HCTs were 75.5%/21.6% for TKI-naïve, 34.1%/65.9% for IMA, 35.7%/64.3% for 2G-TKI (p=<0.001), with either BM or PBSC being the source of stem cells (58.5%/41.5%, 46.3%/53.7%, 14.3%/85.7%, p<0.001, respectively). At the day of transplant, most individuals in every cohort were in CP1: 88% vs 37.9% vs 71.4%, p=0.002 for TKI-naïve, IMA and 2G-TKI respectively. Of note, there were significantly more patients in their second or next CP at the moment of allo-HCT in the IMA group (3.6% vs 32.4% vs 0%), which might have influenced survival outcomes. The number of individuals receiving RIC conditioning was significantly higher in 2G-TKI (11.8% vs 17.1 % vs 46.4%, p<0.001). Also, the median CD34+ count was comparable among the three cohorts (4.0x106/kg vs 5.5x106/kg vs 4.0x106/kg, p=0.543, respectively). The median follow-up time was 41 months for TKI-naïve, 19 months for IMA, and 30 months for 2G-TKI (p<0.001).
Acute and chronic graft-versus-host disease
Data about aGvHD and cGvHD can be found in Table 2 and Figure 1 and Figure 2A,B. Out of the 240 patients included in the analysis, GvHD grade assessment was performed in 231 individuals for aGvHD, and 226 for cGvHD. The outcomes of both the cumulative incidence of aGvHD and cGvHD were the least favorable in the TKI-naïve and IMA cohorts compared to 2G-TKI (61.4% vs 70.7% vs 40.7%, p=0.044; 76.4% vs 51.2% vs 25%, p=25.0%, p<0.001 respectively). Also, the 2G-TKI cohort yielded significantly more low-grade aGvHD compared to TKI-naïve and IMA (p=0.004, p=0.018, respectively) and cGvHD in contrast to TKI-naïve (p<0.001). By multivariate analysis, a female donor setting (HR 2.17, 95% CI 1.15-4.08, p=0.017) and ATG-based GvHD prophylaxis (HR 2.80, 95% CI 1.15-6.79, p=0.023) had an adverse impact on aGvHD incidence. Also, CML accelerated phase (HR 3.13, 95% CI 1.05-9.37, p=0.041) and female donor (HR 2.43, 95% CI 1.26-4.69, p=0.009) were a predictor of cGvHD. RIC conditioning lowered the occurrence of cGvHD (HR 0.24, 95% CI 0.11-0.51, p<0.001). The median day of aGvHD and cGvHD onset was comparable among the three groups (36 vs 44 vs 32, p=0.894; 139 vs 131 vs 257, p=0.625, respectively).
Survival outcomes
4. Discussion
The introduction of TKIs had a pivotal role in the changing landscape of CML-CP management [49]. In the frontline treatment of CML-CP, imatinib and the three 2G-TKI formulations (bosutinib, dasatinib, and nilotinib) yield comparable survival outcomes. However, 2G-TKIs can induce deep molecular response (DMR) more rapidly, potentially shortening the time to achieve treatment-free remission (TFR) [50]. With optimal follow-up seeking for signs of treatment resistance and adequate patient compliance all of the available therapeutic options result in near-normal life expectancy and quality of life [51,52,53,54,55,56]. It is believed that the occurrence is 10 % in case of primary and 30% in case of secondary resistance to frontline TKI therapy [57]. Taking into account TKI-related toxicities, there is an ongoing debate about the most appropriate moment for considering the discontinuation of TKI therapy. Most experts currently lean towards sustaining TKI treatment in the absence of adverse effects, as it was proved that ceasing TKIs after 2 years of DMR yields 3-year TFR rates of 40%–50% [58,59,60], while discontinuation after achieving a DMR for at least 5 years results in a 5-year TFR of over 80% [61]. In spite of this promising results, the current recommendations indicate that allo-HCT should be considered in case of treatment failure or intolerance to at least one 2G-TKI, or in case of a T315I mutation - after a trial therapy with ponatinib or asciminib [18,19]. Also, allo-HCT should be considered in CML-AP and CML-BP after lowering the CML burden through a new-generation TKI [27,29]. In our retrospective study, we sought to assess the influence of IMA and 2G-TKI therapy prior to allo-HCT compared to a historic group from the pre-TKI era on transplant-related toxicity, that is the occurrence of aGvHD and cGvHD, as well as analyse survival outcomes.
Our subgroup analysis revealed that individuals from the 2G-TKI cohort experienced aGvHD significantly less frequently and, if it occurred, its grade was lower compared to TKI-naïve and IMA (40.7% vs 61.4% vs 70.7%, p=0.044; p=0.018 vs TKI-naïve, p=0.004 vs IMA, respectively, as shown in Figure 1 and Figure 2A). We demonstrated similar results for cGvHD, with 2G-TKIs guaranteeing more favorable outcomes both with regard to overall cGvHD incidence (25% vs 76.4% vs 51.2%, p<0.001) and cGvHD grade (2G-TKI vs TKI-naïve p<0.001, Figure 2B). No differences were found with regard to the day of onset of aGvHD and cGvHD (day +32 vs day +36 vs day +44, p=0.849; 139 vs 131 vs 257, p=0.625, respectively). According to the results of multivariate analysis, neither MAC nor MUD or the recipient’s age influenced the occurrence of GvHD. Among the retrievable literature, four studies included a comparison of the influence of prior IMA therapy on post-transplant outcomes with historical groups [25,26,62,63], and one perfomed a similar analysis but with 1-, 2- and 3-generation TKIs [64]. In terms of aGvHD incidence, none of the aforementioned papers demonstrated statistically significant differences between the TKI-treated and TKI-naïve cohorts, regardless of the TKI generation [25,26,62,63,64]. Discrepancies have been found concerning cGvHD despite most studies corroborating towards TKI treatment not having an impact on its incidence[62,63,64]. In the research by Oehler et al. [26] analyzing allo-HCT outcomes of 145 individuals administered IMA and 231 from the historical groups, IMA therapy resulted in a significantly lower hazard of cGvHD (HR = 0.33, 95% CI 0.22-0.48, p=<0.001). A similar observation was made in a trial by Deininger et al. [25] which consisted of a comparison of 70 patients with CML and 21 with Ph+ ALL receiving pre-transplant IMA with historical controls identified in the EBMT database. The individuals exposed to IMA prior to allo-HCT yielded a significantly lower incidence of cGvHD in comparison to control (36.7% vs. 58.8%, p=0.03), which was confirmed by multivariate analysis (OR=0.44, p=0.027) [25].
In order to be able to draw more accurate conclusions, besides a thorough analysis of the available literature we sought to include a few considerations for other factors that could have influenced GvHD-related outcomes. PBSC as a source of stem cells has been previously associated with a higher incidence of aGvHD and cGvHD [65] and cGvHD alone [66,67]. In our analysis, the 2G-TKI group had the highest percentage of PBSC vs BM in comparison with TKI-naïve and IMA (85.7% vs 41.5% vs 53.7%, p<0.001; 2G-TKI vs IMA p=0.02, 2G-TKI vs TKI-naïve p=0.001). Furthermore, RIC conditioning was significantly more frequent in 2G-TKI group (11.8% vs 17.1 % vs 46.4%, p<0.001). There are comparative studies confirming reduced overall incidence of aGvHD grades 2-4 in patients conditioned with RIC [68,69,70,71,72] but none of them has been able to show a difference in terms of cGvHD incidence depending of the type of conditioning regimen. Moreover, recent studies surprisingly revealed RIC to be a factor increasing incidence of cGvHD [73] which, however, is in contradiction to the results of our multivariate analysis as it revealed that RIC conditioning lowered the occurrence of cGvHD (HR 0.24, 95% CI 0.11-0.51, p<0.001). Taking into account these results, we could assume that RIC conditioning might have had a positive impact on aGvHD occurrence in the 2G-TKI cohort, but it is not certain whether it should be enrolled into the list of cGvHD protective agents Also, Cox logistic regression demonstrated that a female donor setting (HR 2.17, 95% CI 1.15-4.08, p=0.017) and ATG-based GvHD prophylaxis (HR 2.80, 95% CI 1.15-6.79, p=0.023) negatively influenced aGvHD incidence. As for cGvHD, CML-AP (HR 3.13, 95% CI 1.05-9.37, p=0.041) and female donor (HR 2.43, 95% CI 1.26-4.69, p=0.009) were a predictor of its occurrence. The number of female donors was comparable among the three groups with, however, significant differences in the ratio of CML-AP (8.4% for TKI-naïve vs 21.6 % for IMA vs 14.3% for 2G-TKI, p<0.001).
We did not demonstrate important variations of 3-year OS between TKI-naïve, IMA and 2G-TKI (55% vs 49.9% vs 69.6%, p=0.740), but we found surprising that the IMA group manifested a tendency towards a lower 3-year OS compared to the TKI-naïve one. This observation is most likely the result of a substantial variance in the number of individuals in second or next CP at the moment of allo-HCT (3.6% vs 32.4% vs 0% for TKI-naïve, IMA and 2G-TKI respectively), which might have negatively impacted survival outcomes in the IMA subgroup. In a retrospective study by Shen et al. [63] the use of IMA was also associated with a significantly higher 0.5 year transplant-related mortality (27.8% vs. 5.9%, p=0.001) compared to no prior TKI therapy. It should be noted that like in our study, it is probable that this finding could be related to a relevant difference in disease stage at the moment of allo-HCT between the two groups (total BC+AP+CP2+CP3 in 47.2% for IMA vs. 8.6% TKI-naïve, p=0.001) [63]. The other papers found that long-term survival outcomes were not affected neither by the use of IMA prior to allo-HCT [25,26,62,63] nor 1-, 2-, and 3-generation TKIs [64].
Attempts are known to use TKIs in GvHD treatment, particularly in cGvHD. Experimental therapies for cutaneous cGvHD with imatinib and nilotinib in mouse models have shown promising outcomes, lowering the intensity of the symptoms compared to the group treated with prednisone [48]. A recent study published in 2023 by a group of Canadian researchers aimed to assess the feasibility of numerous therapeutic agents in the treatment of cGvHD, including ruxolitinib, imatinib, and ibrutinib [74]. Over time, 80% of patients achieved clinical benefit, which enabled a decrease in prednisone dosage across all three TKIs. The 12-month failure-free survival (FFS) rate was notably higher in the imatinib (71%) and ruxolitinib groups (67%) compared to the ibrutinib group (46%). However, the 12-month OS rate remained consistent across all three groups, ranging from 96% to 100% among patients [74]. Up to date, ibrutinib, ruxolitinib, and belumosudil are the only drugs approved by the Food and Drug Administration for the treatment of steroid-refractory cGvHD [75].
Our study has some limitations, such as its retrospective design and a relatively short follow-up time. Also, we did not have access to all of the necessary data including hematopoietic recovery, causes of mortality and infections, which could have made our paper more comprehensive. Finally, not all of the patients who developed GvHD could have been assessed utilizing the same tools, hence the need for standardization (as described in the Materials and Methods section).
Despite the aforementioned caveats to our study, the results we obtained confirm that TKI treatment prior to allo-HCT does not negatively impact the post-transplantation outcomes, including aGvHD and cGvHD. Our analyses suggests that 2G-TKI therapy could significantly lower the cumulative incidence of cGvHD and aGvHD as well as their grade in case of their occurrence. Also, we demonstrated no variations in terms of 3-year OS between the three cohorts. In our view, this analysis remains relevant despite the prevalent use TKIs which have drastically changed the landscape of CML therapy in the past decades. Unlike CML-CP patients, who often proceed to allo-HCT following resistance or intolerance to 2-generation TKIs therapy or after a trial therapy with asciminib or ponatinib in case of T315I mutation, allo-HCT in CML-AP or CML-BP should be considered after lowering the CML burden with new-generation TKIs [18,19]. This study offers an analysis of the outcomes of allo-HCT for these subgroups of patients.
5. Conclusions
In conclusion, our study provides valuable insights into the impact of TKI therapy prior to allo-HCT on post-transplantation outcomes, particularly concerning the incidence and severity of aGvHD and cGvHD. Our findings indicate that 2G-TKI therapy may significantly reduce the occurrence and grade of both aGvHD and cGvHD, without negatively affecting overall survival rates. These results are particularly relevant given the transformative role TKIs have played in the management of CML, especially in achieving deep molecular responses and potentially allowing for treatment-free remission in certain cases.
Despite some limitations, including the retrospective nature of our study and the variability in follow-up times and data completeness, our analysis suggests that TKI therapy, especially with 2G-TKIs, does not compromise the success of allo-HCT. Moreover, our study highlights the importance of continued research into optimizing pre-transplant therapies to improve post-transplant outcomes in cases where allo-HCT should be considered. As CML treatment continues to evolve, our findings underscore the need for personalized approaches in selecting pre-transplant therapies to enhance patient outcomes in this challenging setting.
Author Contributions
Conceptualization, U.G., J.D., A.P., W.P., J.Z.; methodology, U.G., J.D.; investigation, U.G.; software K.D.; data curation, A.P., W.P., J.Z., J.K., Z.D.; writing—original draft preparation, U.G.; writing—review and editing, U.G., J.D., A.P.; supervision, J.D., A.P., W.P., J.Z., L.G., S.G.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki; ethical consideration: the Ethics Committee at the Wroclaw Medical University, nr KB 549/2016, date 5 April 2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Druker, B.J.; Talpaz, M.; Resta, D.J.; Peng, B.; Buchdunger, E.; Ford, J.M.; Lydon, N.B.; Kantarjian, H.; Capdeville, R.; Ohno-Jones, S.; et al. Efficacy and Safety of a Specific Inhibitor of the BCR-ABL Tyrosine Kinase in Chronic Myeloid Leukemia. N. Engl. J. Med. 2001, 344, 1031–1037. [Google Scholar] [CrossRef]
- O’Brien, S.G.; Guilhot, F.; Larson, R.A.; Gathmann, I.; Baccarani, M.; Cervantes, F.; Cornelissen, J.J.; Fischer, T.; Hochhaus, A.; Hughes, T.; et al. Imatinib Compared with Interferon and Low-Dose Cytarabine for Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia. N. Engl. J. Med. 2003, 348, 994–1004. [Google Scholar] [CrossRef]
- Shah, N.P.; Guilhot, F.; Cortes, J.E.; Schiffer, C.A.; le Coutre, P.; Brümmendorf, T.H.; Kantarjian, H.M.; Hochhaus, A.; Rousselot, P.; Mohamed, H.; et al. Long-Term Outcome with Dasatinib after Imatinib Failure in Chronic-Phase Chronic Myeloid Leukemia: Follow-up of a Phase 3 Study. Blood 2014, 123, 2317–2324. [Google Scholar] [CrossRef] [PubMed]
- Giles, F.J.; le Coutre, P.D.; Pinilla-Ibarz, J.; Larson, R.A.; Gattermann, N.; Ottmann, O.G.; Hochhaus, A.; Radich, J.P.; Saglio, G.; Hughes, T.P.; et al. Nilotinib in Imatinib-Resistant or Imatinib-Intolerant Patients with Chronic Myeloid Leukemia in Chronic Phase: 48-Month Follow-up Results of a Phase II Study. Leukemia 2013, 27, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Saglio, G.; Hughes, T.P.; Larson, R.A.; Kim, D.-W.; Issaragrisil, S.; le Coutre, P.D.; Etienne, G.; Dorlhiac-Llacer, P.E.; Clark, R.E.; et al. Long-Term Benefits and Risks of Frontline Nilotinib vs Imatinib for Chronic Myeloid Leukemia in Chronic Phase: 5-Year Update of the Randomized ENESTnd Trial. Leukemia 2016, 30, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Saglio, G.; Kantarjian, H.M.; Baccarani, M.; Mayer, J.; Boqué, C.; Shah, N.P.; Chuah, C.; Casanova, L.; Bradley-Garelik, B.; et al. Final 5-Year Study Results of DASISION: The Dasatinib Versus Imatinib Study in Treatment-Naïve Chronic Myeloid Leukemia Patients Trial. J. Clin. Oncol. 2016, 34, 2333–2340. [Google Scholar] [CrossRef]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet Recommendations for the Management of Chronic Myeloid Leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Barrett, A.J.; Ito, S. The Role of Stem Cell Transplantation for Chronic Myelogenous Leukemia in the 21st Century. Blood 2015, 125, 3230–3235. [Google Scholar] [CrossRef]
- Lübking, A.; Dreimane, A.; Sandin, F.; Isaksson, C.; Märkevärn, B.; Brune, M.; Ljungman, P.; Lenhoff, S.; Stenke, L.; Höglund, M.; et al. Allogeneic Stem Cell Transplantation for Chronic Myeloid Leukemia in the TKI Era: Population-Based Data from the Swedish CML Registry. Bone Marrow Transplant. 2019, 54, 1764–1774. [Google Scholar] [CrossRef]
- Mughal, T.I.; Radich, J.P.; Deininger, M.W.; Apperley, J.F.; Hughes, T.P.; Harrison, C.J.; Gambacorti-Passerini, C.; Saglio, G.; Cortes, J.; Daley, G.Q. Chronic Myeloid Leukemia: Reminiscences and Dreams. Haematologica 2016, 101, 541–558. [Google Scholar] [CrossRef]
- Gratwohl, A.; Brand, R.; Apperley, J.; Crawley, C.; Ruutu, T.; Corradini, P.; Carreras, E.; Devergie, A.; Guglielmi, C.; Kolb, H.-J.; et al. Allogeneic Hematopoietic Stem Cell Transplantation for Chronic Myeloid Leukemia in Europe 2006: Transplant Activity, Long-Term Data and Current Results. An Analysis by the Chronic Leukemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Haematologica 2006, 91, 513–521. [Google Scholar] [PubMed]
- Dazzi, F.; Szydlo, R.M.; Craddock, C.; Cross, N.C.; Kaeda, J.; Chase, A.; Olavarria, E.; van Rhee, F.; Kanfer, E.; Apperley, J.F.; et al. Comparison of Single-Dose and Escalating-Dose Regimens of Donor Lymphocyte Infusion for Relapse after Allografting for Chronic Myeloid Leukemia. Blood 2000, 95, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Pavlu, J.; Szydlo, R.M.; Goldman, J.M.; Apperley, J.F. Three Decades of Transplantation for Chronic Myeloid Leukemia: What Have We Learned? Blood 2011, 117, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Innes, A.J.; Milojkovic, D.; Apperley, J.F. Allogeneic Transplantation for CML in the TKI Era: Striking the Right Balance. Nat. Rev. Clin. Oncol. 2016, 13, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Gratwohl, A.; Heim, D. Current Role of Stem Cell Transplantation in Chronic Myeloid Leukaemia. Best Pract. Res. Clin. Haematol. 2009, 22, 431–443. [Google Scholar] [CrossRef]
- Passweg, J.R.; Baldomero, H.; Gratwohl, A.; Bregni, M.; Cesaro, S.; Dreger, P.; de Witte, T.; Farge-Bancel, D.; Gaspar, B.; Marsh, J.; et al. The EBMT Activity Survey: 1990-2010. Bone Marrow Transplant. 2012, 47, 906–923. [Google Scholar] [CrossRef]
- Jabbour, E.; Kantarjian, H. Chronic Myeloid Leukemia: 2025 Update on Diagnosis, Therapy, and Monitoring. Am. J. Hematol. 2024. [CrossRef]
- Jabbour, E.; Cortes, J.; Santos, F.P.S.; Jones, D.; O’Brien, S.; Rondon, G.; Popat, U.; Giralt, S.; Kebriaei, P.; Jones, R.B.; et al. Results of Allogeneic Hematopoietic Stem Cell Transplantation for Chronic Myelogenous Leukemia Patients Who Failed Tyrosine Kinase Inhibitors after Developing BCR-ABL1 Kinase Domain Mutations. Blood 2011, 117, 3641–3647. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, F.E.; Basak, G.W.; Kim, D.-W.; Olavarria, E.; Pinilla-Ibarz, J.; Apperley, J.F.; Hughes, T.; Niederwieser, D.; Mauro, M.J.; Chuah, C.; et al. Overall Survival with Ponatinib versus Allogeneic Stem Cell Transplantation in Philadelphia Chromosome-Positive Leukemias with the T315I Mutation. Cancer 2017, 123, 2875–2880. [Google Scholar] [CrossRef]
- Hughes, T.P.; Kaeda, J.; Branford, S.; Rudzki, Z.; Hochhaus, A.; Hensley, M.L.; Gathmann, I.; Bolton, A.E.; van Hoomissen, I.C.; Goldman, J.M.; et al. Frequency of Major Molecular Responses to Imatinib or Interferon Alfa plus Cytarabine in Newly Diagnosed Chronic Myeloid Leukemia. N. Engl. J. Med. 2003, 349, 1423–1432. [Google Scholar] [CrossRef]
- Kantarjian, H.; Shah, N.P.; Hochhaus, A.; Cortes, J.; Shah, S.; Ayala, M.; Moiraghi, B.; Shen, Z.; Mayer, J.; Pasquini, R.; et al. Dasatinib versus Imatinib in Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia. N. Engl. J. Med. 2010, 362, 2260–2270. [Google Scholar] [CrossRef] [PubMed]
- Saglio, G.; Kim, D.-W.; Issaragrisil, S.; le Coutre, P.; Etienne, G.; Lobo, C.; Pasquini, R.; Clark, R.E.; Hochhaus, A.; Hughes, T.P.; et al. Nilotinib versus Imatinib for Newly Diagnosed Chronic Myeloid Leukemia. N. Engl. J. Med. 2010, 362, 2251–2259. [Google Scholar] [CrossRef]
- Saussele, S.; Richter, J.; Guilhot, J.; Gruber, F.X.; Hjorth-Hansen, H.; Almeida, A.; Janssen, J.J.W.M.; Mayer, J.; Koskenvesa, P.; Panayiotidis, P.; et al. Discontinuation of Tyrosine Kinase Inhibitor Therapy in Chronic Myeloid Leukaemia (EURO-SKI): A Prespecified Interim Analysis of a Prospective, Multicentre, Non-Randomised, Trial. Lancet Oncol. 2018, 19, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Zaucha, J.M.; Prejzner, W.; Giebel, S.; Gooley, T.A.; Szatkowski, D.; Kałwak, K.; Wojnar, J.; Kruzel, T.; Balon, J.; Hołowiecki, J.; et al. Imatinib Therapy prior to Myeloablative Allogeneic Stem Cell Transplantation. Bone Marrow Transplant. 2005, 36, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Deininger, M.; Schleuning, M.; Greinix, H.; Sayer, H.G.; Fischer, T.; Martinez, J.; Maziarz, R.; Olavarria, E.; Verdonck, L.; Schaefer, K.; et al. The Effect of Prior Exposure to Imatinib on Transplant-Related Mortality. Haematologica 2006, 91, 452–459. [Google Scholar]
- Oehler, V.G.; Gooley, T.; Snyder, D.S.; Johnston, L.; Lin, A.; Cummings, C.C.; Chu, S.; Bhatia, R.; Forman, S.J.; Negrin, R.S.; et al. The Effects of Imatinib Mesylate Treatment before Allogeneic Transplantation for Chronic Myeloid Leukemia. Blood 2007, 109, 1782–1789. [Google Scholar] [CrossRef]
- Lee, S.J.; Kukreja, M.; Wang, T.; Giralt, S.A.; Szer, J.; Arora, M.; Woolfrey, A.E.; Cervantes, F.; Champlin, R.E.; Gale, R.P.; et al. Impact of Prior Imatinib Mesylate on the Outcome of Hematopoietic Cell Transplantation for Chronic Myeloid Leukemia. Blood 2008, 112, 3500–3507. [Google Scholar] [CrossRef]
- Saussele, S.; Lauseker, M.; Gratwohl, A.; Beelen, D.W.; Bunjes, D.; Schwerdtfeger, R.; Kolb, H.-J.; Ho, A.D.; Falge, C.; Holler, E.; et al. Allogeneic Hematopoietic Stem Cell Transplantation (allo SCT) for Chronic Myeloid Leukemia in the Imatinib Era: Evaluation of Its Impact within a Subgroup of the Randomized German CML Study IV. Blood 2010, 115, 1880–1885. [Google Scholar] [CrossRef]
- Jabbour, E.; Cortes, J.; Kantarjian, H.; Giralt, S.; Andersson, B.S.; Giles, F.; Shpall, E.; Kebriaei, P.; Champlin, R.; de Lima, M. Novel Tyrosine Kinase Inhibitor Therapy before Allogeneic Stem Cell Transplantation in Patients with Chronic Myeloid Leukemia: No Evidence for Increased Transplant-Related Toxicity. Cancer 2007, 110, 340–344. [Google Scholar] [CrossRef]
- Shimoni, A.; Leiba, M.; Schleuning, M.; Martineau, G.; Renaud, M.; Koren-Michowitz, M.; Ribakovski, E.; le Coutre, P.; Arnold, R.; Guilhot, F.; et al. Prior Treatment with the Tyrosine Kinase Inhibitors Dasatinib and Nilotinib Allows Stem Cell Transplantation (SCT) in a Less Advanced Disease Phase and Does Not Increase SCT Toxicity in Patients with Chronic Myelogenous Leukemia and Philadelphia Positive Acute Lymphoblastic Leukemia. Leukemia 2009, 23, 190–194. [Google Scholar]
- Breccia, M.; Palandri, F.; Iori, A.P.; Colaci, E.; Latagliata, R.; Castagnetti, F.; Torelli, G.F.; Usai, S.; Valle, V.; Martinelli, G.; et al. Second-Generation Tyrosine Kinase Inhibitors before Allogeneic Stem Cell Transplantation in Patients with Chronic Myeloid Leukemia Resistant to Imatinib. Leuk. Res. 2010, 34, 143–147. [Google Scholar] [CrossRef]
- Piekarska, A.; Gil, L.; Prejzner, W.; Wiśniewski, P.; Leszczyńska, A.; Gniot, M.; Komarnicki, M.; Hellmann, A. Pretransplantation Use of the Second-Generation Tyrosine Kinase Inhibitors Has No Negative Impact on the HCT Outcome. Ann. Hematol. 2015, 94, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- Saidu, N.E.B.; Bonini, C.; Dickinson, A.; Grce, M.; Inngjerdingen, M.; Koehl, U.; Toubert, A.; Zeiser, R.; Galimberti, S. New Approaches for the Treatment of Chronic Graft-Versus-Host Disease: Current Status and Future Directions. Front. Immunol. 2020, 11, 578314. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ortega, I.; Parody, R.; Servitje, O.; Muniesa, C.; Arnan, M.; Patino, B.; Sureda, A.; Duarte, R.F. Imatinib and Dasatinib as Salvage Therapy for Sclerotic Chronic Graft-vs-Host Disease. Croat. Med. J. 2016, 57, 247–254. [Google Scholar] [CrossRef]
- Sánchez-Ortega, I.; Servitje, O.; Arnan, M.; Ortí, G.; Peralta, T.; Manresa, F.; Duarte, R.F. Dasatinib as Salvage Therapy for Steroid Refractory and Imatinib Resistant or Intolerant Sclerotic Chronic Graft-versus-Host Disease. Biol. Blood Marrow Transplant. 2012, 18, 318–323. [Google Scholar] [CrossRef]
- Srour, M.; Alsuliman, T.; Labreuche, J.; Bulabois, C.-E.; Chevallier, P.; Daguindau, E.; Forcade, E.; François, S.; Guillerm, G.; Coiteux, V.; et al. Nilotinib Efficacy and Safety as Salvage Treatment Following Imatinib Intolerance And/or Inefficacy in Steroid Refractory Chronic Graft-versus-Host-Disease (SR-cGVHD): A Prospective, Multicenter, Phase II Study on Behalf of the Francophone Society of Bone Marrow Transplantation and Cellular Therapy (SFGM-TC). Bone Marrow Transplant. 2023, 58, 401–406. [Google Scholar] [PubMed]
- Olivieri, A.; Mancini, G.; Olivieri, J.; Marinelli Busilacchi, E.; Cimminiello, M.; Pascale, S.P.; Nuccorini, R.; Patriarca, F.; Corradini, P.; Bacigalupo, A.; et al. Nilotinib in Steroid-Refractory cGVHD: Prospective Parallel Evaluation of Response, according to NIH Criteria and Exploratory Response Criteria (GITMO Criteria). Bone Marrow Transplant. 2020, 55, 2077–2086. [Google Scholar] [CrossRef] [PubMed]
- Drugs@FDA: FDA-Approved Drugs. Available online: http://www.accessdata.fda.gov/scripts/cder/daf (accessed on 7 August 2024).
- Jakavi. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/jakavi (accessed on 7 August 2024).
- Moslehi, J.J.; Deininger, M. Tyrosine Kinase Inhibitor-Associated Cardiovascular Toxicity in Chronic Myeloid Leukemia. J. Clin. Oncol. 2015, 33, 4210–4218. [Google Scholar] [CrossRef]
- de Lavallade, H.; Khoder, A.; Hart, M.; Sarvaria, A.; Sekine, T.; Alsuliman, A.; Mielke, S.; Bazeos, A.; Stringaris, K.; Ali, S.; et al. Tyrosine Kinase Inhibitors Impair B-Cell Immune Responses in CML through off-Target Inhibition of Kinases Important for Cell Signaling. Blood 2013, 122, 227–238. [Google Scholar] [CrossRef]
- Hayashi, Y.; Nakamae, H.; Katayama, T.; Nakane, T.; Koh, H.; Nakamae, M.; Hirose, A.; Hagihara, K.; Terada, Y.; Nakao, Y.; et al. Different Immunoprofiles in Patients with Chronic Myeloid Leukemia Treated with Imatinib, Nilotinib or Dasatinib. Leuk. Lymphoma 2012, 53, 1084–1089. [Google Scholar] [CrossRef]
- Baccarani, M.; Saglio, G.; Goldman, J.; Hochhaus, A.; Simonsson, B.; Appelbaum, F.; Apperley, J.; Cervantes, F.; Cortes, J.; Deininger, M.; et al. Evolving Concepts in the Management of Chronic Myeloid Leukemia: Recommendations from an Expert Panel on Behalf of the European LeukemiaNet. Blood 2006, 108, 1809–1820. [Google Scholar] [CrossRef]
- Baccarani, M.; Cortes, J.; Pane, F.; Niederwieser, D.; Saglio, G.; Apperley, J.; Cervantes, F.; Deininger, M.; Gratwohl, A.; Guilhot, F.; et al. Chronic Myeloid Leukemia: An Update of Concepts and Management Recommendations of European LeukemiaNet. J. Clin. Oncol. 2009, 27, 6041–6051. [Google Scholar] [CrossRef] [PubMed]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Harris, A.C.; Young, R.; Devine, S.; Hogan, W.J.; Ayuk, F.; Bunworasate, U.; Chanswangphuwana, C.; Efebera, Y.A.; Holler, E.; Litzow, M.; et al. International, Multicenter Standardization of Acute Graft-versus-Host Disease Clinical Data Collection: A Report from the Mount Sinai Acute GVHD International Consortium. Biol. Blood Marrow Transplant. 2016, 22, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Filipovich, A.H.; Weisdorf, D.; Pavletic, S.; Socie, G.; Wingard, J.R.; Lee, S.J.; Martin, P.; Chien, J.; Przepiorka, D.; Couriel, D.; et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. Diagnosis and Staging Working Group Report. Biol. Blood Marrow Transplant. 2005, 11, 945–956. [Google Scholar] [CrossRef]
- Shulman, H.M.; Sullivan, K.M.; Weiden, P.L.; McDonald, G.B.; Striker, G.E.; Sale, G.E.; Hackman, R.; Tsoi, M.S.; Storb, R.; Thomas, E.D. Chronic Graft-versus-Host Syndrome in Man. A Long-Term Clinicopathologic Study of 20 Seattle Patients. Am. J. Med. 1980, 69, 204–217. [Google Scholar] [CrossRef]
- Hoffmann, V.S.; Baccarani, M.; Hasford, J.; Castagnetti, F.; Di Raimondo, F.; Casado, L.F.; Turkina, A.; Zackova, D.; Ossenkoppele, G.; Zaritskey, A.; et al. Treatment and Outcome of 2904 CML Patients from the EUTOS Population-Based Registry. Leukemia 2017, 31, 593–601. [Google Scholar] [CrossRef]
- Senapati, J.; Sasaki, K.; Issa, G.C.; Lipton, J.H.; Radich, J.P.; Jabbour, E.; Kantarjian, H.M. Management of Chronic Myeloid Leukemia in 2023 - Common Ground and Common Sense. Blood Cancer J. 2023, 13, 58. [Google Scholar] [CrossRef]
- Jain, P.; Kantarjian, H.; Alattar, M.L.; Jabbour, E.; Sasaki, K.; Nogueras Gonzalez, G.; Dellasala, S.; Pierce, S.; Verstovsek, S.; Wierda, W.; et al. Long-Term Molecular and Cytogenetic Response and Survival Outcomes with Imatinib 400 Mg, Imatinib 800 Mg, Dasatinib, and Nilotinib in Patients with Chronic-Phase Chronic Myeloid Leukaemia: Retrospective Analysis of Patient Data from Five Clinical Trials. Lancet Haematol 2015, 2, e118–e128. [Google Scholar] [CrossRef]
- Bower, H.; Björkholm, M.; Dickman, P.W.; Höglund, M.; Lambert, P.C.; Andersson, T.M.-L. Life Expectancy of Patients With Chronic Myeloid Leukemia Approaches the Life Expectancy of the General Population. J. Clin. Oncol. 2016, 34, 2851–2857. [Google Scholar] [CrossRef]
- Hehlmann, R.; Lauseker, M.; Saußele, S.; Pfirrmann, M.; Krause, S.; Kolb, H.J.; Neubauer, A.; Hossfeld, D.K.; Nerl, C.; Gratwohl, A.; et al. Assessment of Imatinib as First-Line Treatment of Chronic Myeloid Leukemia: 10-Year Survival Results of the Randomized CML Study IV and Impact of Non-CML Determinants. Leukemia 2017, 31, 2398–2406. [Google Scholar] [CrossRef]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Breccia, M. Imatinib Improved the Overall Survival of Chronic Myeloid Leukemia Patients in Low- and Middle-Income Countries: A Therapeutic Goal Has Been Reached. EClinicalMedicine 2020, 19, 100277. [Google Scholar] [CrossRef]
- Maas, C.C.H.M.; van Klaveren, D.; Ector, G.I.C.G.; Posthuma, E.F.M.; Visser, O.; Westerweel, P.E.; Janssen, J.J.W.M.; Blijlevens, N.M.A.; Dinmohamed, A.G. The Evolution of the Loss of Life Expectancy in Patients with Chronic Myeloid Leukaemia: A Population-Based Study in the Netherlands, 1989-2018. Br. J. Haematol. 2022, 196, 1219–1224. [Google Scholar] [CrossRef]
- Molica, M.; Naqvi, K.; Cortes, J.E.; Paul, S.; Kadia, T.M.; Breccia, M.; Kantarjian, H.; Jabbour, E.J. Treatment-Free Remission in Chronic Myeloid Leukemia. Clin. Adv. Hematol. Oncol. 2019, 17, 686–696. [Google Scholar] [PubMed]
- Radich, J.P.; Hochhaus, A.; Masszi, T.; Hellmann, A.; Stentoft, J.; Casares, M.T.G.; García-Gutiérrez, J.V.; Conneally, E.; le Coutre, P.D.; Gattermann, N.; et al. Treatment-Free Remission Following Frontline Nilotinib in Patients with Chronic Phase Chronic Myeloid Leukemia: 5-Year Update of the ENESTfreedom Trial. Leukemia 2021, 35, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.P.; García-Gutiérrez, V.; Jiménez-Velasco, A.; Larson, S.; Saussele, S.; Rea, D.; Mahon, F.-X.; Levy, M.Y.; Gómez-Casares, M.T.; Pane, F.; et al. Dasatinib Discontinuation in Patients with Chronic-Phase Chronic Myeloid Leukemia and Stable Deep Molecular Response: The DASFREE Study. Leuk. Lymphoma 2020, 61, 650–659. [Google Scholar] [CrossRef]
- Gugliotta, G.; Castagnetti, F.; Breccia, M.; Levato, L.; Intermesoli, T.; D’Adda, M.; Salvucci, M.; Stagno, F.; Rege-Cambrin, G.; Tiribelli, M.; et al. Treatment-Free Remission in Chronic Myeloid Leukemia Patients Treated Front-Line with Nilotinib: 10-Year Followup of the GIMEMA CML 0307 Study. Haematologica 2022, 107, 2356–2364. [Google Scholar] [CrossRef]
- Haddad, F.G.; Sasaki, K.; Issa, G.C.; Garcia-Manero, G.; Ravandi, F.; Kadia, T.; Cortes, J.; Konopleva, M.; Pemmaraju, N.; Alvarado, Y.; et al. Treatment-Free Remission in Patients with Chronic Myeloid Leukemia Following the Discontinuation of Tyrosine Kinase Inhibitors. Am. J. Hematol. 2022, 97, 856–864. [Google Scholar] [CrossRef]
- Khoury, H.J.; Kukreja, M.; Goldman, J.M.; Wang, T.; Halter, J.; Arora, M.; Gupta, V.; Rizzieri, D.A.; George, B.; Keating, A.; et al. Prognostic Factors for Outcomes in Allogeneic Transplantation for CML in the Imatinib Era: A CIBMTR Analysis. Bone Marrow Transplant. 2012, 47, 810–816. [Google Scholar] [CrossRef]
- Shen, K.; Liu, Q.; Sun, J.; Jiang, Q.; Ye, Y.; Huang, H.; Meng, F.; Zhou, Y.; Yang, M. Prior Exposure to Imatinib Does Not Impact Outcome of Allogeneic Hematopoietic Transplantation for Chronic Myeloid Leukemia Patients: A Single-Center Experience in China. Int. J. Clin. Exp. Med. 2015, 8, 2495–2505. [Google Scholar] [PubMed]
- Heim, D.; Baldomero, H.; Medinger, M.; Masouridi-Levrat, S.; Schanz, U.; Nair, G.; Güngör, T.; Halter, J.; Passweg, J.R.; Chalandon, Y.; et al. Allogeneic Haematopoietic Cell Transplantation for Chronic Myeloid Leukaemia in Switzerland in the Face of Rapid Development of Effective Drugs. Swiss Med. Wkly 2024, 154, 3754. [Google Scholar] [CrossRef]
- Friedrichs, B.; Tichelli, A.; Bacigalupo, A.; Russell, N.H.; Ruutu, T.; Shapira, M.Y.; Beksac, M.; Hasenclever, D.; Socié, G.; Schmitz, N. Long-Term Outcome and Late Effects in Patients Transplanted with Mobilised Blood or Bone Marrow: A Randomised Trial. Lancet Oncol. 2010, 11, 331–338. [Google Scholar] [CrossRef]
- Blaise, D.; Kuentz, M.; Fortanier, C.; Bourhis, J.H.; Milpied, N.; Sutton, L.; Jouet, J.P.; Attal, M.; Bordigoni, P.; Cahn, J.Y.; et al. Randomized Trial of Bone Marrow versus Lenograstim-Primed Blood Cell Allogeneic Transplantation in Patients with Early-Stage Leukemia: A Report from the Société Française de Greffe de Moelle. J. Clin. Oncol. 2000, 18, 537–546. [Google Scholar] [CrossRef]
- Vigorito, A.C.; Azevedo, W.M.; Marques, J.F.; Azevedo, A.M.; Eid, K.A.; Aranha, F.J.; Lorand-Metze, I.; Oliveira, G.B.; Correa, M.E.; Reis, A.R.; et al. A Randomised, Prospective Comparison of Allogeneic Bone Marrow and Peripheral Blood Progenitor Cell Transplantation in the Treatment of Haematological Malignancies. Bone Marrow Transplant. 1998, 22, 1145–1151. [Google Scholar] [CrossRef]
- Couriel, D.R.; Saliba, R.M.; Giralt, S.; Khouri, I.; Andersson, B.; de Lima, M.; Hosing, C.; Anderlini, P.; Donato, M.; Cleary, K.; et al. Acute and Chronic Graft-versus-Host Disease after Ablative and Nonmyeloablative Conditioning for Allogeneic Hematopoietic Transplantation. Biol. Blood Marrow Transplant. 2004, 10, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Simón, J.A.; Díez-Campelo, M.; Martino, R.; Brunet, S.; Urbano, A.; Caballero, M.D.; de León, A.; Valcárcel, D.; Carreras, E.; del Cañizo, M.C.; et al. Influence of the Intensity of the Conditioning Regimen on the Characteristics of Acute and Chronic Graft-versus-Host Disease after Allogeneic Transplantation. Br. J. Haematol. 2005, 130, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Mielcarek, M.; Martin, P.J.; Leisenring, W.; Flowers, M.E.D.; Maloney, D.G.; Sandmaier, B.M.; Maris, M.B.; Storb, R. Graft-versus-Host Disease after Nonmyeloablative versus Conventional Hematopoietic Stem Cell Transplantation. Blood 2003, 102, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Sohn, S.K.; Baek, J.H.; Kim, J.G.; Lee, J.W.; Min, W.S.; Kim, D.W.; Choi, S.-J.; Lee, J.-H.; Lee, K.-H.; et al. Retrospective Multicenter Study of Allogeneic Peripheral Blood Stem Cell Transplantation Followed by Reduced-Intensity Conditioning or Conventional Myeloablative Regimen. Acta Haematol. 2005, 113, 220–227. [Google Scholar] [CrossRef]
- Aoudjhane, M.; Labopin, M.; Gorin, N.C.; Shimoni, A.; Ruutu, T.; Kolb, H.-J.; Frassoni, F.; Boiron, J.M.; Yin, J.L.; Finke, J.; et al. Comparative Outcome of Reduced Intensity and Myeloablative Conditioning Regimen in HLA Identical Sibling Allogeneic Haematopoietic Stem Cell Transplantation for Patients Older than 50 Years of Age with Acute Myeloblastic Leukaemia: A Retrospective Survey from the Acute Leukemia Working Party (ALWP) of the European Group for Blood and Marrow Transplantation (EBMT). Leukemia 2005, 19, 2304–2312. [Google Scholar]
- Afram, G.; Simón, J.A.P.; Remberger, M.; Caballero-Velázquez, T.; Martino, R.; Piñana, J.L.; Ringden, O.; Esquirol, A.; Lopez-Corral, L.; Garcia, I.; et al. Reduced Intensity Conditioning Increases Risk of Severe cGVHD: Identification of Risk Factors for cGVHD in a Multicenter Setting. Med. Oncol. 2018, 35, 79. [Google Scholar] [CrossRef] [PubMed]
- Linn, S.M.; Novitzky-Basso, I.; Abduljalil, O.; Pasic, I.; Lam, W.; Law, A.; Michelis, F.V.; Gerbitz, A.; Viswabandya, A.; Lipton, J.; et al. A Single-Center, Real-World Experience of Chronic GVHD Treatment Using Ibrutinib, Imatinib, and Ruxolitinib and Its Treatment Outcomes. Hematol. Oncol. Stem Cell Ther. 2023, 17, 60–71. [Google Scholar] [PubMed]
- Zeiser, R. Novel Approaches to the Treatment of Chronic Graft-Versus-Host Disease. J. Clin. Oncol. 2023, 41, 1820–1824. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Impact of 1-generation and 2-generation TKIs on the cumulative HR of aGvHD (12 months) and cGvHD (36 months).
Figure 1.
Impact of 1-generation and 2-generation TKIs on the cumulative HR of aGvHD (12 months) and cGvHD (36 months).
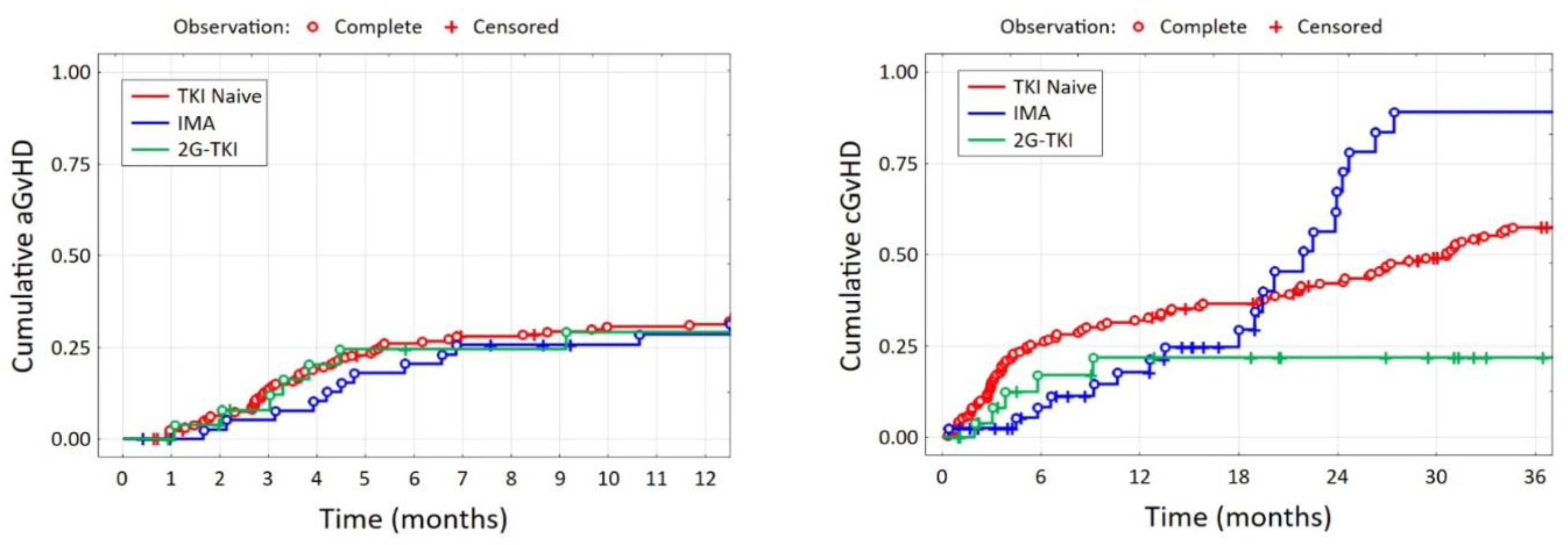
Figure 2.
Impact of 1-generation and 2-generation TKIs on the grade of aGvHD (A) and cGvHD (B).
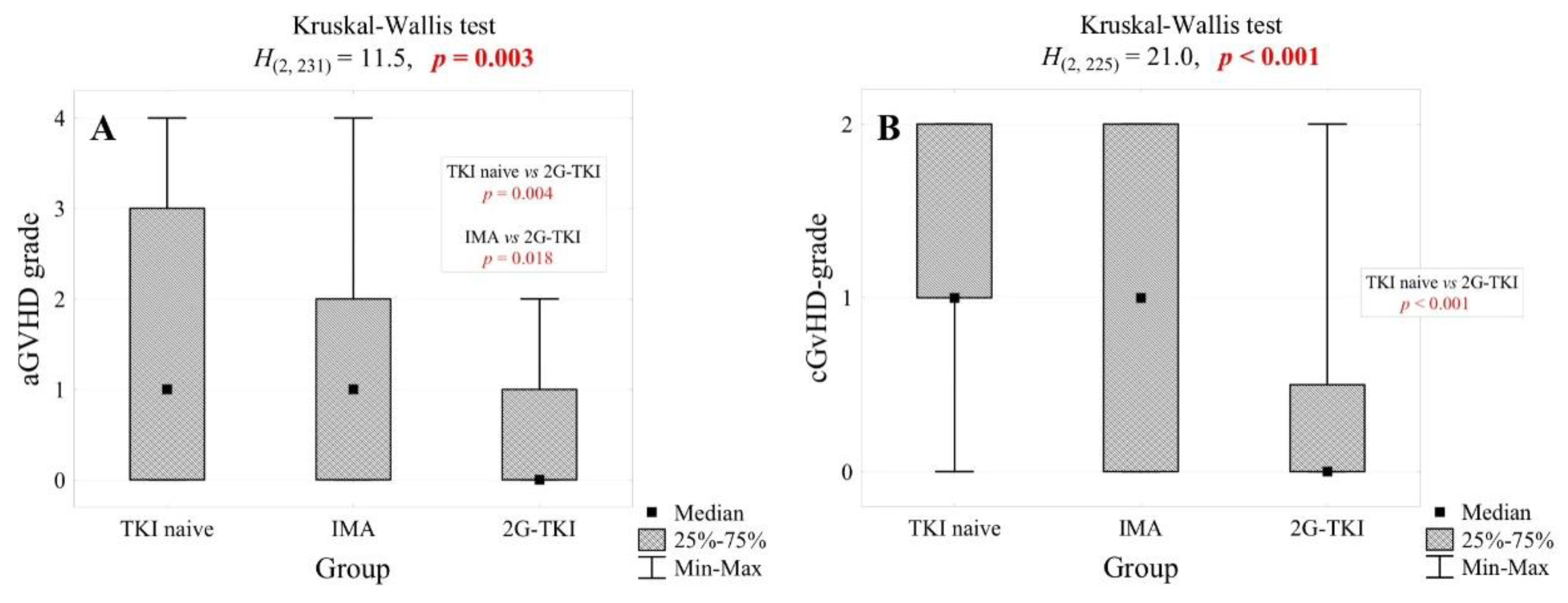
Figure 3.
Impact of 1-generation and 2-generation TKIs on OS probability.
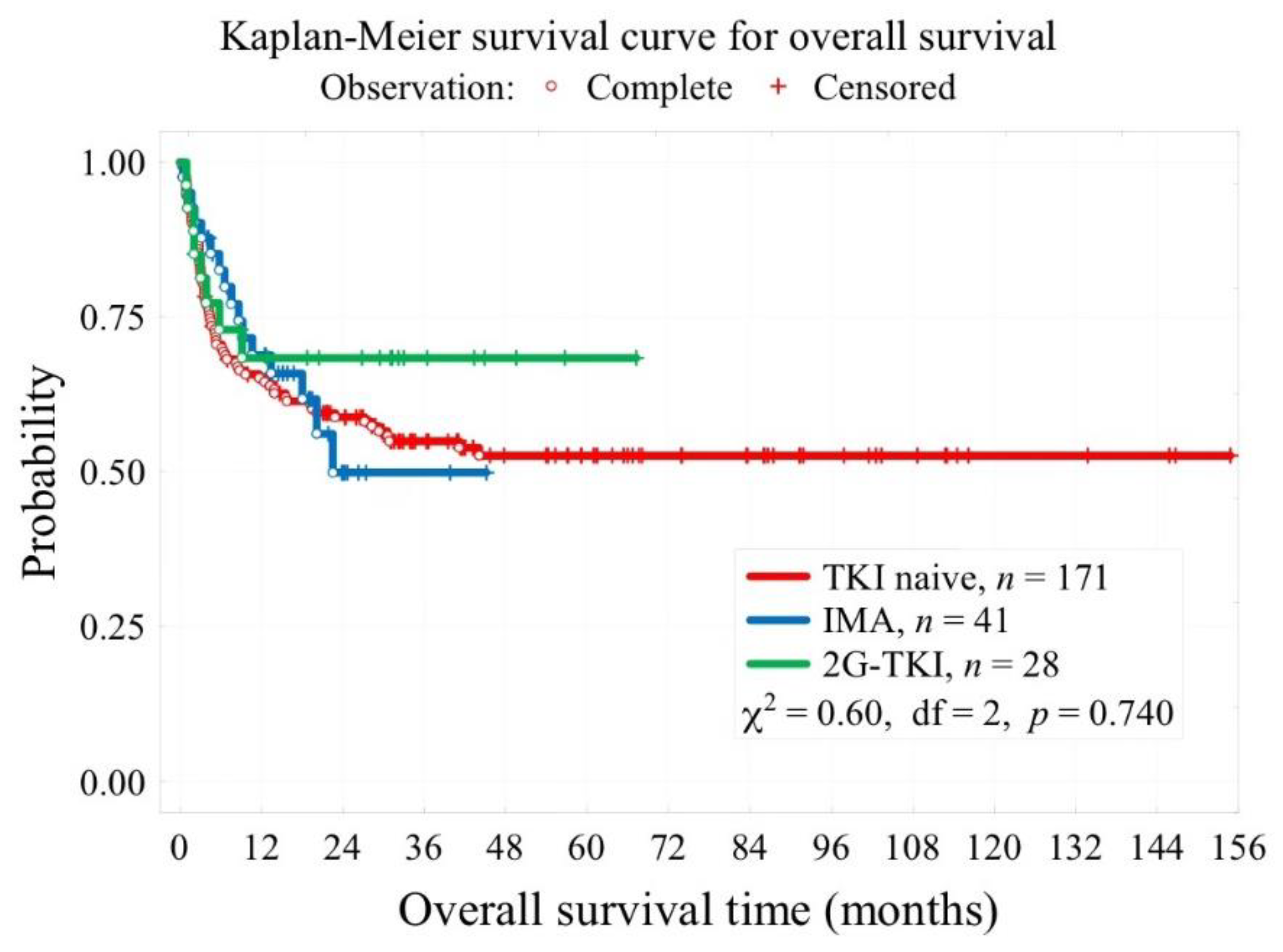

Table 1.
Patient-, donor- and transplant-related characteristics. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, BM - bone marrow, PBSC - peripheral blood stem cells, WBC - white blood cell count, CML - chronic myeloid leukaemia, Ph+ CML - Philadelphia chromosome positive chronic myeloid leukaemia, HU - hydroxyurea, IFNα - interferon-alfa, RIC - reduced intensity conditioning, TBI - total body irradiation, ATG - anti-thymocyte globulin, MTX - methotrexate.
Table 1.
Patient-, donor- and transplant-related characteristics. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, BM - bone marrow, PBSC - peripheral blood stem cells, WBC - white blood cell count, CML - chronic myeloid leukaemia, Ph+ CML - Philadelphia chromosome positive chronic myeloid leukaemia, HU - hydroxyurea, IFNα - interferon-alfa, RIC - reduced intensity conditioning, TBI - total body irradiation, ATG - anti-thymocyte globulin, MTX - methotrexate.
| p-value | |||||||
| TKI naïve N = 171 |
IMA N = 41 |
2G-TKI N = 28 |
|||||
| Patient sex, n (%) | 0.211 | ||||||
| Male | 100 | 58.8% | 26 | 63.4% | 12 | 42.9% | |
| Female | 71 | 41.2% | 15 | 36.6% | 16 | 57.1% | |
| Patient age (years), Me [Q1; Q3] | 37 [28; 44] | 35 [26; 40] | 48 [33; 57] | < 0.001 | |||
| Donor sex, n (%) | 0.766 | ||||||
| Male | 101 | 58.7% | 26 | 63.4% | 0 | 0.0% | |
| Female | 70 | 41.3% | 15 | 36.6% | 28 | 100% | |
| Donor age (years), M ± SD | 37.0 ± 10.4 | 37.6 ± 11.3 | - | 0.769 | |||
| Type of donor, n (%) | <0.001 | ||||||
| Sibling | 129 | 75.5% | 14 | 34.1% | 10 | 35.7% | |
| Unrelated | 37 | 21.6% | 27 | 65.9% | 18 | 64.3% | |
| Other | 5 | 2.9% | 0 | 0.0% | 0 | 0.0% | |
| Source of stem cells, n (%) | <0.001 | ||||||
| BM | 100 | 58,5% | 19 | 46,3% | 4 | 14,3% | |
| PBSC | 71 | 41,5% | 22 | 53,7% | 24 | 85,7% | |
| Transplant risk category, Me [Q1; Q3] | 2 [1; 3] | 3 [3; 4] | - | 1.000 | |||
| Median CD34+ count ×106/kg, Me [Q1; Q3] | 4.0 [2.7; 5.7] | 5.5 [2.2; 7.1] | 4.0 [3.6; 4.7] | 0.543 | |||
| Donor positive CMV status, n (%) | 99 | 77.3% | 21 | 51.2% | NA | 0.006 | |
| CML phase at day of transplant, n (%) | <0.001 | ||||||
| Chronic Phase | 147 | 88.0% | 14 | 37.9% | 20 | 71.4% | |
| Accelerated Phase | 14 | 8.4% | 8 | 21.6% | 4 | 14.3% | |
| Blast Crisis Phase | 0 | 0.0% | 3 | 8.1% | 4 | 14.3% | |
| Second/next Chronic Phase | 6 | 3.6% | 12 | 32.4% | 0 | 0.0% | |
| HU 1 year before transplant | 140 | 98.6% | 14 | 66.7% | NA | <0.001 | |
| IFNa (yes), n (%) | 22 | 14.8% | 16 | 47.1% | 0 | 0.0% | <0.001 |
| RIC (yes), n (%) | 20 | 11.8% | 7 | 17.1% | 13 | 46.4% | <0.001 |
| High dose TBI (yes), n (%) | 6 | 3.5% | 11 | 28.9% | 1 | 3.6% | <0.001 |
| ATG in condtioning regimen | 48 | 28,1% | 27 | 71,1% | NA | <0.001 | |
Table 2.
Patient-, donor- and transplant-related characteristics (continuation). The comment “for (number) pt.” means the number of patients for whom data was available. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, aGvHD - acute graft-versus-host disease, cGvHD - chronic graft-versus-host disease, VOD - veno-occlusive disease, ANC - absolute neutrophil count, PLT - platelet count, Hgb - haemoglobin, HU - hydroxyurea.
Table 2.
Patient-, donor- and transplant-related characteristics (continuation). The comment “for (number) pt.” means the number of patients for whom data was available. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, aGvHD - acute graft-versus-host disease, cGvHD - chronic graft-versus-host disease, VOD - veno-occlusive disease, ANC - absolute neutrophil count, PLT - platelet count, Hgb - haemoglobin, HU - hydroxyurea.
| p-value | |||||||
| TKI naïve N = 171 |
IMA N = 41 |
2G-TKI N = 28 |
|||||
| aGvHD day, Me [Q1; Q3] | 36 [24; 54] | 44 [23; 59] | 32 [24; 49] | 0.894 | |||
| cGvHD day, Me [Q1; Q3] | 139 [103; 250] | 131 [120; 151] | 257 [132; 317] | 0.625 | |||
| aGvHD (yes), n (%) | for 163 pt. | for 27 pt. | 0.044 | ||||
| 100 | 61.4% | 29 | 70.7% | 11 | 40.7% | ||
| aGvHD grade, n (%) | for 163 pt. | for 27 pt. | 0.002 | ||||
| 0 | 63 | 38.7% | 12 | 29.3% | 16 | 59.3% | |
| 1 | 25 | 15.3% | 9 | 22.0% | 9 | 33.3% | |
| 2 | 33 | 20.2% | 13 | 31.7% | 2 | 7.4% | |
| 3 | 18 | 11.0% | 6 | 14.6% | 0 | 0.0% | |
| 4 | 24 | 14.7% | 1 | 2.4% | 0 | 0.0% | |
| cGvHD (yes), n (%) | for 157 pt. | <0.001 | |||||
| 120 | 76.4% | 21 | 51.2% | 7 | 25.0% | ||
| cGvHD grade, n (%) | for 157 pt. | <0.001 | |||||
| 0 | 37 | 23.6% | 20 | 48.8% | 21 | 75.0% | |
| 1 | 49 | 31.2% | 7 | 17.1% | 2 | 7.1% | |
| 2 | 71 | 45.2% | 14 | 34.1% | 5 | 17.9% | |
| Karnofsky scale at the day of last contact, Me [Q1; Q3] | 85 [0; 100] | 90 [80; 100] | NA | 1.000 | |||
| Patient status at the day of last contact, n (%) | |||||||
| Dead | 76 | 44,4% | 16 | 39,0% | 8 | 29,6% | 0.268 |
| Relapse | 73 | 42,7% | 14 | 35,9% | 3 | 11,1% | 0.007 |
Table 3.
Results of multivariate analysis based on patient, disease and transplant characteristics for patients for all cohorts. Note: only statistically significant results were included. The full results of multivariate analysis are included as Supplementary Materials. Abbreviations: GvHD - graft-versus-host disease, ATG - anti-thymocyte globulin, CML - chronic myeloid leukaemia.
Table 3.
Results of multivariate analysis based on patient, disease and transplant characteristics for patients for all cohorts. Note: only statistically significant results were included. The full results of multivariate analysis are included as Supplementary Materials. Abbreviations: GvHD - graft-versus-host disease, ATG - anti-thymocyte globulin, CML - chronic myeloid leukaemia.
| Variable | Risk Factor for | HR | 95% CI | p Value |
|---|---|---|---|---|
| Donor sex: female | Acute GvHD | 2.17 | 1.15-4.08 | 0.017 |
| GvHD prophylaxis: ATG | 2.80 | 1.15-6.79 | 0.023 | |
| Donor sex: female | Chronic GvHD | 2.43 | 1.26-4.69 | 0.009 |
| RIC conditioning | 0.24 | 0.11-0.51 | <0.001 | |
| CML accelerated phase | 3.13 | 1.05-9.36 | 0.041 |
Table 4.
Patient-, donor- and transplant-related characteristics (continuation). The comment “for (number) pt.” means the number of patients for whom data was available. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, OS - overall survival.
Table 4.
Patient-, donor- and transplant-related characteristics (continuation). The comment “for (number) pt.” means the number of patients for whom data was available. Abbreviations: IMA - imatinib, 2G-TKI - 2nd generation tyrosine kinase inhibitor, OS - overall survival.
| p-value | ||||
| TKI naïve N = 171 |
IMA N = 41 |
2G-TKI N = 28 |
||
| Median follow-up time, months | 41 [28; 73] for 163 pt. |
19 [14; 24] | 30 [16; 40] | <0.001 |
| 3-year overall survival OS (t=3 years) | 55% | 49.9% | 69.6% | 0.740 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



