
Submitted:
17 April 2024
Posted:
18 April 2024
You are already at the latest version
Abstract
Despite notable advancements in immunotherapy in the past decades, allogeneic hematopoietic stem cell transplantation (allo-HCT) remains a promising, potentially curative treatment modality. Only a limited number of studies has performed a direct comparison of two prevalent rabbit anti-thymocyte globulin (r-ATG) formulations — specifically, Thymoglobuline (ATG-T, formerly Genzyme) and Grafalon (ATG-G, formerly Fresenius). The primary objective of our retrospective analysis was to compare the outcomes of adult patients undergoing matched or mismatched unrelated donor (MUD/MMUD) allo-HCT, with a graft-versus-host disease (GvHD) prophylaxis based on either ATG-T or ATG-G. A total of 87 patients undergone allo-HCT between 2012 and 2022 were included. We observed no significant differences between ATG-T and ATG-G concerning the occurrence of acute graft-versus-host disease (aGvHD), regardless of its severity. Conversely, chronic graft-versus-host disease (cGvHD) occurred less frequently in the ATG-T group compared to ATG-G (7.5% vs. 38.3%, p=0.001). Patients treated with ATG-T manifested a higher incidence of cytomegalovirus (CMV) reactivations (70% vs. 31.9%, p<0.001), with a shorter time between transplant and CMV (<61 days, 77.8% vs. 33.3%, p=0.008) and a higher median CMV copy number (1000 vs. 0, p=0.004). Notably, despite a higher occurrence of CMV reactivations in the ATG-T cohort, most patients were asymptomatic compared to ATG-G (85.7% vs. 43.8%, p=0.005). Finally, we observed no significant differences in terms of 5-year overall survival (OS) and 3-year probability of relapse while comparing ATG-T and ATG-G (32.0% vs 40.3%, p=0.423; 63.9% vs 55.7%, p=0.438, respectively).
Keywords:
allogeneic hematopoietic stem cell transplantation
; anti-thymocyte globulin
; Thymoglobuline
; Grafalon
; graft-versus-host disease
1. Introduction
Graft-versus-host disease (GvHD) represents a significant complication in the context of allogeneic hematopoietic stem cell transplantation (allo-HCT) [1,2], exerting detrimental effects on both the duration and quality of life of transplant recipients [3]. Factors such as the use of peripheral blood stem cells (PBSC), an increased T cell count, and HLA mismatch currently stand as major risk factors for susceptibility to both acute GvHD (aGvHD) and chronic GvHD (cGvHD) [4,5,6,7].
Historically, before the 1980s, the commonly utilised GvHD prophylaxis regimen was methotrexate (MTX) [8], and the incorporation of cyclosporine A (CsA) in the following years has led to a substantial reduction in the occurrence of aGvHD grade II-IV reaching 20%, that is, from 50% to 30% [9]. In spite of significant advancements in the prevention of GvHD, aGvHD is experienced by over 40% of patients receiving allo-HCT, particularly those of older age [10,11]. Even with the inclusion of mycophenolate mofetil (MMF) alongside MTX and CsA, aGvHD grade II-IV persists up to 30% in MRD allo-HCT recipients aged 40 years or older [12]. Hence, there is a need for developing more effective GvHD prophylactic regimens.
In Europe, the predominant therapeutic strategy for preventing GvHD involves standard prophylaxis consisting of calcineurin inhibitors (CNIs), MTX, or MMF, along with one of the available rabbit anti-thymocyte globulins (r-ATGs) for unrelated donor transplantation. In recent years, this approach has been extended to sibling donor allo-HCT as well [13]. Various countries have access to different formulations of ATGs derived from rabbits, horses, or pigs, produced through the inoculation of human thymocytes or human cell lines. The latter ones, that is porcine ATG (p-ATG) and horse ATG (h-ATG), are less frequently employed medications in the context of European countries.
There are currently two formulations of rabbit anti-thymocyte globulins (rATGs), both composed of polyclonal IgG derived from hyperimmune sera of rabbits. These IgG antibodies are immunized either with human Jurkat leukemia T-cell line in the case of ATG-G (anti-T-lymphocyte globulin, Grafalon; Neovii, Rapperswil, Switzerland; formerly Fresenius) or with human thymocytes in the case of ATG-T (anti-thymocyte globulin, Thymoglobulin; Sanofi, Paris, France; formerly Genzyme) [14]. Additionally, ATG-T and ATG-G differ in the antigens they target. In comparison to ATG-T, the range of antigens recognised by ATG-G is narrower; for instance, ATG-G includes few or no antibodies targeting HLA-DR, CD3, or CD4 [15,16]. Nevertheless, ATG-G possesses more antibodies against CD107 which is expressed on T cells during degranulation, a process resulting from antigenic stimulation [16]. Conversely, ATG-T addresses antigens expressed on T cells (CD2, CD3, CD4, CD6, CD8), natural killer cells, B cells, dendritic cells, and macrophages, as well as HLA-DR and HLA class 1 [12]. ATG-T also consists of antibodies specifically targeting antigens associated with cellular trafficking and adhesion, along with those implicated in inflammation, apoptosis, and cellular proliferation [12]. Competitive binding experiments have indicated that ATG-T demonstrates higher reactivity and a more potent complement-mediated cytotoxic effect toward peripheral blood mononuclear cells than ATG-G. Furthermore, when equal doses of the two formulations are employed, ATG-T more effectively induces apoptosis of dendritic cells than ATG-G. As a result, GvHD prophylaxis typically involves the administration of higher doses of ATG-G than ATG-T.
The immunological consequences of ATG are also influenced by various factors, including timing of administration considering the day of transplantation, the cumulative dosage, and the recipient's lymphocyte count at the time of allo-HCT. Higher doses of rATG, a lower host total lymphocyte count, and closer timing to transplantation can lead to prolonged exposure to ATG after donor T cell infusion [4]. This results in a delayed immune reconstitution [17,18], thereby increasing the potential for vulnerability to infections, relapse, and the development of lymphoproliferative disorders following allo-HCT [19]. Hence, these factors must be taken into consideration when evaluating the outcomes associated with rATG administration [4].
The main aim of our retrospective analysis was to assess the impact of ATG-T and ATG-G on graft-versus-host disease as well as overall survival following allo-HCT in adult patients. Also, considering the molecular differences between these two formulations, we examined the effects on the occurrence of viral reactivations.
2. Materials and Methods
2.1. Patients
Data were obtained upon an in-depth analysis of the patients’ documentation in two Polish Adult Leukaemia Group (PALG) associated centres. The individuals underwent allo-HCT in two PALG-associated centres between 2012 and 2022. Patients included in the analysis are of ≥18 years of age with acute myeloid leukaemia (AML), myelodysplastic syndrome (MDS), acute lymphoblastic leukaemia (ALL), myeloma, lymphoma and other haematological disorders in first, second, third or fourth complete remission. Patients received PBSC allo-HCT from a MUD or MMUD and were administered a myeloablative (MAC), non-myeloablative (NMA) or reduced-instensity (RIC) conditioning regimen. Standard GvHD prophylaxis was employed, based on MTX with tacrolimus (Tac) or CsA with one of the two available rATG formulations - ATG-T or ATG-G. Of note, letermovir CMV prophylaxis, which is currently regarded as a standard, became widely available in Poland only in 2021.
2.2. Outcomes
The primary endpoint of our study was acute and chronic GvHD. Secondary endpoints included CMV related outcomes, OS and probability of relapse. Acute and chronic GvHD were defined following the previously published criteria [20,21]. Relapse was defined as cytogenetic, molecular or morphologic recurrence of the disease. Probability of relapse was defined as the likelihood of disease relapse (which is not the equivalent of relapse-free survival).
2.3. Statistical Methods
Nominal and ordinal variables are presented in the contingency tables as numbers (n) and percentages (%). Quantitative variables are presented as medians and ranges. The chi-square test of independence or Fisher's exact test was used to assess the significance of correlation between two qualitative variables. Survival curves and the Kaplan-Meier procedure were used to assess the effectiveness of treatment. The F-Cox test was used to compare survival curves in the two groups.
All analyses were performed using the statistical software package Statistica v. 13.3 (TIBCO Software Inc., Palo Alto, CA, USA). A p-value of <0.05 was considered to be statistically significant.
3. Results
3.1. Patient-, Disease-, and Transplantation-Related Characteristics
Patient-, disease-, and transplantation-related characteristics are shown in Table 1, Table 2, Table 3, Table 4 and Table 5. A total of 87 patients underwent mismatched- and matched-unrelated allo-HCT, of whom 40 received ATG-T and 47 ATG-G. The characteristics of the patients in the two groups were comparable except for patients’ age (≥55 or <55 years), conditioning regimen (RIC, MAC or NMA), and CMV prophylaxis (aciclovir, valganciclovir, letermovir). The ratios of the applied conditioning regimens (MAC/RIC/NMA) were 82.5%/10%/7.5% for ATG-T, and 53.2%/31.9%/14.9% for ATG-G (p=0.014). There were more patients of ≥55 years of age in the ATG-T group compared to ATG-G (82.5% vs 51.1%, p=0.003), an the median ages were 45 years and 55 years (p=0.065) with female/male ratios of 17/23 and 20/27 (p=0.832), respectively. The median times of follow-up were 27 months (7-42) for the ATG-T group, and 16 months (8-44) for the ATG-G one. The donors were either matched unrelated (MUD) or mismatched unrelated (MMUD) (27.5% vs 72.5%, respectively for ATG-T; 78.7% vs 21.3%, respectively for ATG-G). Also, the median donor ages and CD34+ count were comparable among the two cohorts (30 years vs 33 years, p=0.399; 8.1x106/kg vs 7.4x106/kg, p=0.810, respectively), Most individuals in both the ATG-T and ATG-G group were diagnosed with AML or MDS (37.5% vs 53.2%, respectively), followed by ALL (25% vs 17%, respectively) and lymphoma/myeloma (20% vs 14.9%, respectively). Other diagnoses were classified separately, constituting a mere 17.5% and 14.9%.
3.2. Acute and Chronic GvHD
The results concerning acute and chronic GvHD are presented in Table 3. No statistically significant discrepancies were observed in the occurrence of aGvHD comparing ATG-T and ATG-G. However, there was a tendency for ATG-T to cause more frequently aGvHD, aGvHD grades II-IV with a lower median time of onset of aGvHD in contrast to ATG-G (65% vs 44.7%, p=0.084; 42.5% vs 31.9%, p=0.308; 24 vs 29 days, p=0.366, respectively). Chronic GvHD (cGvHD) was significantly less frequent in the ATG-T group compared to ATG-G (7.5% vs 38.3%, p=0.001).
3.3. Infection-Related Mortality and Viral Infections
The infectious outcomes are shown in Table 4. Patients treated with ATG-T experienced a higher incidence of CMV reactivations (70% vs 31.9%, p<0.001), with a shorter time between transplant and the number of virus copies beyond threshold (<61 days, 77.8% vs 33.3%, p=0.008) and a higher median CMV copy number (1000 vs 0, p=0.004). The number of patients who received letermovir as CMV prophylaxis was similar between the ATG-T and ATG-G groups (7.5% vs 10.9%). Interestingly, despite a higher number of CMV reactivations in the ATG-T cohort, there were more asymptomatic patients than in those who were administered ATG-G (85.7% vs 43.8%, p=0.005). If CMV is not being considered, other viral reactivations were more numerous in the ATG-G group (66% vs 15%, p=0.001), with a statistically significant difference in Epstein-Barr virus (EBV), BK virus (BKV), and JC virus (JCV) reactivations (40.4% vs 10%, p=0.001; 29.8% vs 5%, p=0.004; 21.3% vs 2.5%, p=0.010, respectively).
3.4. Survival Outcomes
4. Discussion
Despite important progress has been made in the area of transplantation procedures, GvHD stands as a major concern limiting allo-HCT’s success, and is one of the most severe complications [1,2]. Also, GvHD negatively impacts the patient’s quality of life and can, in some instances, result fatal [22]. Consequently, endeavours are directed towards identifying the optimal GvHD prophylaxis protocol aimed at GvHD incidence, while maintaining a favourable graft-versus-leukemia (GvL) response and minimising the incidence of potentially lethal viral reactivations. This is of major importance notably in patients undergoing allo-HCT from mismatched related and unrelated donors with PBSC, given their well-established status as predisposing factors for GvHD [4,6]. In this study, we performed a retrospective analysis of patients suffering from various hematological conditions who sustained matched and mismatched unrelated allo-HCT and compared the outcomes of 40 patients who received ATG-T with those of 47 patients who were administered ATG-G.
Our subgroup analysis unveiled no significant difference in the incidence of aGvHD between ATG-T and ATG-G, with a tendency for ATG-T to promote the development of aGvHD, aGvHD grades II-IV with a lower median time of onset of aGvHD (65% vs 44.7%, p=0.084; 42.5% vs 31.9%, p=0.308; 24 vs 29 days, p=0.366, respectively). Our results are in line with most published studies that carried out a comparison of ATG-T and ATG-G [23,24,25,26,27]. Discrepancies concerning aGvHD grades III-IV can be found in the studies by Oosterbrink et al. [24] comparing ATG-T and ATG-G in MUD/MMUD allo-HCT and Liu et al. [25] evaluating the outcomes of allo-HCT with ATG-T and ATG-G in mixed donor settings. Their results are discrepant, as the former study demonstrated favourable results for ATG-G (0% vs 12%, p=0.025) [24], and the latter for ATG-T (2.27% vs 17.39%, p=0.026) [25]. In terms of cGvHD, we found that the employment of ATG-T rather than ATG-G lead to advantageous outcomes (7.5% vs 38.3%, p=0.001). The broad antibody spectrum of ATG-T could be related to its connection with a lower incidence of cGvHD, as it is a polyclonal antibody that targets CD19 and CD20, two molecules present on the surface of B cells [28]. Other trials did not demonstrate any relevant discrepancies [23,24,25,26,27]. In contrast, a network meta-analysis by Gagelmann et al. [29] revealed a higher efficacy of ATG-G in preventing cGvHD and aGvHD compared to ATG-T and standard treatment.
It is commonly acknowledged that the use of r-ATG is correlated with CMV reactivation [30], which may result in significant complications following allo-HCT. The use of both ATG-G and ATG-T may delay immune reconstitution, leading to a heightened susceptibility to infections [31,32]. Nevertheless, both formulations selectively bind to diverse antigens present on immune cell surfaces, with ATG-T’s spectrum being much wider, consequently exhibiting a more potent T-cell depletion effect [16,17,18]. Letermovir has demonstrated efficacy in reducing the morbidity and mortality associated with CMV reactivation [33]; however, it has only become widely available in Poland since 2021. As a consequence, only few patients received it as CMV prophylaxis (7.5% vs 10.9%). With regard to viral infections besides CMV, we found that they occurred more frequently in the ATG-G cohort than in the ATG-T one (66% vs 15%, p=0.001) which, however, has no support from other trials [23,24,25,26,27]. Also, most studies did not find significant differences in CMV reactivations between the two rATG formulations [23,24,25,27]. In contrast, the results of our study suggest that patients treated with ATG-T rather than ATG-G are more likely to develop CMV reactivations (70% vs 31.9%, p<0.001), with a higher median CMV copy number (1000 vs 0, p=0.004) and a shorter time between transplant and CMV reactivation (<61 days, 77.8% vs 33.3%, p=0.008). Additionally, most CMV reactivations in the ATG-T cohort were asymptomatic (85.7% vs 43.8%, p=0.005). A similar outcome, also in an unrelated donor allo-HCT setting, was observed in a trial carried out by Wang et al., where ATG-T was the formulation that prompted CMV reactivations (64.6% vs 29.9%, p<0.001) [26]. The stronger immunosuppressive effect of ATG-T in contrast to ATG-G could be the reason behind this finding. Lastly, neither the 5-year OS and 3-year probability of relapse were influenced by the type of r-ATG (32.0% vs 40.3%, p=0.423; 63.9% vs 55.7%, p=0.438, respectively). These results is in line with the outcomes of other papers [23,24,25,26,27].
This investigation also has limitations due to its retrospective design. Additionally, the group of individuals included in the analysis is relatively small. Owing to the fact that a substantial number of patients was transplanted nearly 10 years ago when the transplantation standards and viral infection prophylactic regimens were not as refined as nowadays, outcomes such as probability of relapse, OS and infection reactivations may be suboptimal.
In conclusion, the results of our study suggest that in case of matched and mismatched unrelated donor allo-HCT the type of administered r-ATG has an important influence on transplantation outcomes. While different formulations of r-ATG do not appear to impact the occurrence of aGvHD, ATG-T seems to lower the incidence of cGvHD compared to ATG-G. Also, CMV reactivations develop more frequently, with a higher CMV copy number and earlier in the post-transplantation period with ATG-T, likely due to its broader antibody spectrum. Of note, in case of ATG-T, there were significantly more asymptomatic infections. With the development of novel, more effective antiviral medications, it seems viable to limit the risk of infectious complications following allo-HCT, despite the employment of GvHD prophylaxis with a stronger T-cell depleting effect.
Author Contributions
Conceptualization, U.G., J.D; methodology, U.G., J.D.; investigation, U.G., M.M-D., M.S.-K., S.G..; software K.D.; data curation, U.G., M.M-D., M.S.-K.; writing—original draft preparation, U.G.; writing—review and editing, U.G., J.D.; supervision, L.G., J.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki; ethical consideration: the Ethics Committee at the Wroclaw Medical University, nr KB 549/2016, date 5 April 2017.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wingard, J.R.; Majhail, N.S.; Brazauskas, R.; Wang, Z.; Sobocinski, K.A.; Jacobsohn, D.; Sorror, M.L.; Horowitz, M.M.; Bolwell, B.; Rizzo, J.D.; et al. Long-Term Survival and Late Deaths after Allogeneic Hematopoietic Cell Transplantation. J Clin Oncol 2011, 29, 2230–2239. [CrossRef]
- Martin, P.J.; Counts, G.W.; Appelbaum, F.R.; Lee, S.J.; Sanders, J.E.; Deeg, H.J.; Flowers, M.E.D.; Syrjala, K.L.; Hansen, J.A.; Storb, R.F.; et al. Life Expectancy in Patients Surviving More than 5 Years after Hematopoietic Cell Transplantation. J Clin Oncol 2010, 28, 1011–1016. [CrossRef]
- Pidala, J.; Kurland, B.; Chai, X.; Majhail, N.; Weisdorf, D.J.; Pavletic, S.; Cutler, C.; Jacobsohn, D.; Palmer, J.; Arai, S.; et al. Patient-Reported Quality of Life Is Associated with Severity of Chronic Graft-versus-Host Disease as Measured by NIH Criteria: Report on Baseline Data from the Chronic GVHD Consortium. Blood 2011, 117, 4651–4657. [CrossRef]
- Watkins, B.; Williams, K.M. Controversies and Expectations for the Prevention of GVHD: A Biological and Clinical Perspective. Front Immunol 2022, 13. [CrossRef]
- Arai, S.; Arora, M.; Wang, T.; Spellman, S.R.; He, W.; Couriel, D.R.; Urbano-Ispizua, A.; Cutler, C.S.; Bacigalupo, A.A.; Battiwalla, M.; et al. Increasing Incidence of Chronic Graft-versus-Host Disease in Allogeneic Transplantation: A Report from the Center for International Blood and Marrow Transplant Research. Biol Blood Marrow Transplant 2015, 21, 266–274. [CrossRef]
- Flowers, M.E.D.; Inamoto, Y.; Carpenter, P.A.; Lee, S.J.; Kiem, H.P.; Petersdorf, E.W.; Pereira, S.E.; Nash, R.A.; Mielcarek, M.; Fero, M.L.; et al. Comparative Analysis of Risk Factors for Acute Graft-versus-Host Disease and for Chronic Graft-versus-Host Disease According to National Institutes of Health Consensus Criteria. Blood 2011, 117, 3214–3219. [CrossRef]
- Anasetti, C.; Logan, B.R.; Lee, S.J.; Waller, E.K.; Weisdorf, D.J.; Wingard, J.R.; Cutler, C.S.; Westervelt, P.; Woolfrey, A.; Couban, S.; et al. Peripheral-Blood Stem Cells versus Bone Marrow from Unrelated Donors. N Engl J Med 2012, 367, 1487–1496. [CrossRef]
- Thomas E.; Storb R.; Clift R.A.; et al: Bone-marrow transplantation (first of two parts). N Engl J Med 292:832-843, 1975.
- Storb R.; Deeg H.J.; Whitehead J.; et al: Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med 314:729-735, 1986.
- Hahn T.; McCarthy P.L. Jr; Zhang M.J.; et al: Risk factors for acute graft-versus-host disease after human leukocyte antigen-identical sibling transplants for adults with leukemia. J Clin Oncol 26:5728-5734, 2008.
- Lai Y.R.; Chen Y.H.; Hu D.M.; et al: Multicenter phase II study of a combination of cyclosporine a, methotrexate and mycophenolate mofetil for GVHD prophylaxis: Results of the Chinese Bone Marrow Transplant Cooperative Group (CBMTCG). J Hematol Oncol 7:59, 2014.
- Mohty M.: Mechanisms of action of antithymocyte globulin: T-cell depletion and beyond. Leukemia 21:1387-1394, 2007 .
- Ruutu, T.; Van Biezen, A.; Hertenstein, B.; Henseler, A.; Garderet, L.; Passweg, J.; Mohty, M.; Sureda, A.; Niederwieser, D.; Gratwohl, A.; et al. Prophylaxis and Treatment of GVHD after Allogeneic Haematopoietic SCT: A Survey of Centre Strategies by the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant 2012, 47, 1459–1464. [CrossRef]
- Baron, F.; Mohty, M.; Blaise, D.; Socié, G.; Labopin, M.; Esteve, J.; Ciceri, F.; Giebel, S.; Gorin, N.C.; Savani, B.N.; et al. Anti-Thymocyte Globulin as Graft-versus-Host Disease Prevention in the Setting of Allogeneic Peripheral Blood Stem Cell Transplantation: A Review from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Haematologica 2017, 102, 224–234. [CrossRef]
- Popow, I.; Leitner, J.; Majdic, O.; J. Kovarik, J.; D. Saemann, M.; Zlabinger, G.J.; Steinberger, P. Assessment of Batch to Batch Variation in Polyclonal Antithymocyte Globulin Preparations. Transplantation 2012, 93, 32–40. [CrossRef]
- Popow, I.; Leitner, J.; Grabmeier-Pfistershammer, K.; Majdic, O.; Zlabinger, G.J.; Kundi, M.; Steinberger, P. A Comprehensive and Quantitative Analysis of the Major Specificities in Rabbit Antithymocyte Globulin Preparations. Am J Transplant 2013, 13, 3103–3113. [CrossRef]
- Servais, S.; Menten-Dedoyart, C.; Beguin, Y.; Seidel, L.; Gothot, A.; Daulne, C.; Willems, E.; Delens, L.; Humblet-Baron, S.; Hannon, M.; et al. Impact of Pre-Transplant Anti-T Cell Globulin (ATG) on Immune Recovery after Myeloablative Allogeneic Peripheral Blood Stem Cell Transplantation. PLoS One 2015, 10. [CrossRef]
- Bosch, M.; Dhadda, M.; Hoegh-Petersen, M.; Liu, Y.; Hagel, L.M.; Podgorny, P.; Ugarte-Torres, A.; Khan, F.M.; Luider, J.; Auer-Grzesiak, I.; et al. Immune Reconstitution after Anti-Thymocyte Globulin-Conditioned Hematopoietic Cell Transplantation. Cytotherapy 2012, 14, 1258–1275. [CrossRef]
- Bonifazi, F.; Rubio, M.T.; Bacigalupo, A.; Boelens, J.J.; Finke, J.; Greinix, H.; Mohty, M.; Nagler, A.; Passweg, J.; Rambaldi, A.; et al. Rabbit ATG/ATLG in Preventing Graft-versus-Host Disease after Allogeneic Stem Cell Transplantation: Consensus-Based Recommendations by an International Expert Panel. Bone Marrow Transplant 2020, 55, 1093–1102. [CrossRef]
- Atkinson K, Horowitz MM, Gale RP, Lee MB, Rimm AA, Bortin MM. Consensus among bone marrow transplanters for diagnosis, grading and treatment of chronic graft-versus-host disease. Committee of the International Bone Marrow Transplant Registry. Bone Marrow Transplant.1989;4:247-254.
- Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15:825-828.
- Lee, S.J.; Logan, B.; Westervelt, P.; Cutler, C.; Woolfrey, A.; Khan, S.P.; Waller, E.K.; Maziarz, R.T.; Wu, J.; Shaw, B.E.; et al. Comparison of Patient-Reported Outcomes in 5-Year Survivors Who Received Bone Marrow vs Peripheral Blood Unrelated Donor Transplantation: Long-Term Follow-up of a Randomized Clinical Trial. JAMA Oncol. 2016, 2, 1583–1589.
- Polverelli, N.; Malagola, M.; Turra, A.; Skert, C.; Perucca, S.; Chiarini, M.; Cattina, F.; Rambaldi, B.; Cancelli, V.; Morello, E.; et al. Comparative Study on ATG-Thymoglobulin versus ATG-Fresenius for the Graft-versus-Host Disease (GVHD) Prophylaxis in Allogeneic Stem Cell Transplantation from Matched Unrelated Donor: A Single-Centre Experience over the Contemporary Years. Leuk. Lymphoma 2018, 59, 2700–2705.
- Oostenbrink, L.V.E.; Jol-Van Der Zijde, C.M.; Kielsen, K.; Jansen-Hoogendijk, A.M.; Ifversen, M.; Müller, K.G.; Lankester, A.C.; Van Halteren, A.G.S.; Bredius, R.G.M.; Schilham, M.W.; et al. Differential Elimination of Anti-Thymocyte Globulin of Fresenius and Genzyme Impacts T-Cell Reconstitution After Hematopoietic Stem Cell Transplantation. Front. Immunol. 2019, 10, 315.
- Liu, L.; Xu, G.; Zhang, Y.; Jiao, W.; Lei, M.; Zhou, H.; Wang, Q.; Qiu, H.; Tang, X.; Han, Y.; et al. Comparison of 2 Different Rabbit Anti-Thymocyte Globulin (r-ATG) Preparations: Thymocyte r-ATG versus T Lymphoblast Cell Line r-ATG in Allogeneic Hematopoietic Stem Cell Transplantation for Acquired Severe Aplastic Anemia: Propensity Score-Matched Analysis. Transplant. Cell. Ther. 2021, 27, 186.e1–186.e3.
- Wang, L.; Kong, P.; Zhang, C.; Gao, L.; Zhu, L.; Liu, J.; Gao, S.; Chen, T.; Liu, H.; Yao, H.; et al. Outcomes of Patients with Hematological Malignancies Who Undergo Unrelated Donor Hematopoietic Stem Cell Transplantation with ATG-Fresenius versus ATG-Genzyme. Ann. Hematol. 2023, 102, 1–11.
- Butera, S.; Cerrano, M.; Brunello, L.; Dellacasa, C.M.; Faraci, D.G.; Vassallo, S.; Mordini, N.; Sorasio, R.; Zallio, F.; Busca, A.; et al. Impact of Anti-Thymocyte Globulin Dose for Graft-versus-Host Disease Prophylaxis in Allogeneic Hematopoietic Cell Transplantation from Matched Unrelated Donors: A Multicenter Experience. Ann. Hematol. 2021, 100, 1837–1847.
- Gaber AO et al (2010) Rabbit antithymocyte globulin (thymoglobulin): 25 years and new frontiers in solid organ transplantation and haematology. Drugs 70(6):691–732.
- Gagelmann, N.; Ayuk, F.; Wolschke, C.; Kröger, N. Comparison of Different Rabbit Anti-Thymocyte Globulin Formulations in Allogeneic Stem Cell Transplantation: Systematic Literature Review and Network Meta-Analysis. Biol. Blood Marrow Transplant. 2017, 23, 2184–2191.
- Luo X-H et al (2021) CMV infection and CMV-specific immune reconstitution following haploidentical stem cell transplantation: an update. Front Immunol 12:732826.
- Marty, F.M.; Ljungman, P.; Chemaly, R.F.; Maertens, J.; Dadwal, S.S.; Duarte, R.F.; Haider, S.; Ullmann, A.J.; Katayama, Y.; Brown, J.; et al. Letermovir Prophylaxis for Cytomegalovirus in Hematopoietic-Cell Transplantation. N. Engl. J. Med. 2017, 377, 2433–2444.
- Schmidt-Hieber, M.; Schwarck, S.; Stroux, A.; Ganepola, S.; Reinke, P.; Thiel, E.; Uharek, L.; Blau, I.W. Immune Reconstitution and Cytomegalovirus Infection after Allogeneic Stem Cell Transplantation: The Important Impact of in Vivo T Cell Depletion. Int. J. Hematol. 2010, 91, 877–885.
- Russo D, Schmitt M, Pilorge S, Stelljes M, Kawakita T, Teal VL, Haber B, Bopp C, Dadwal SS, Badshah C. Efficacy and safety of extended duration letermovir prophylaxis in recipients of haematopoietic stem-cell transplantation at risk of cytomegalovirus infection: a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Haematol. 2024 Feb;11(2):e127-e135.
Figure 1.
Probability of relapse and overall survival with ATG-T (Thymo) and ATG-G (ATG).
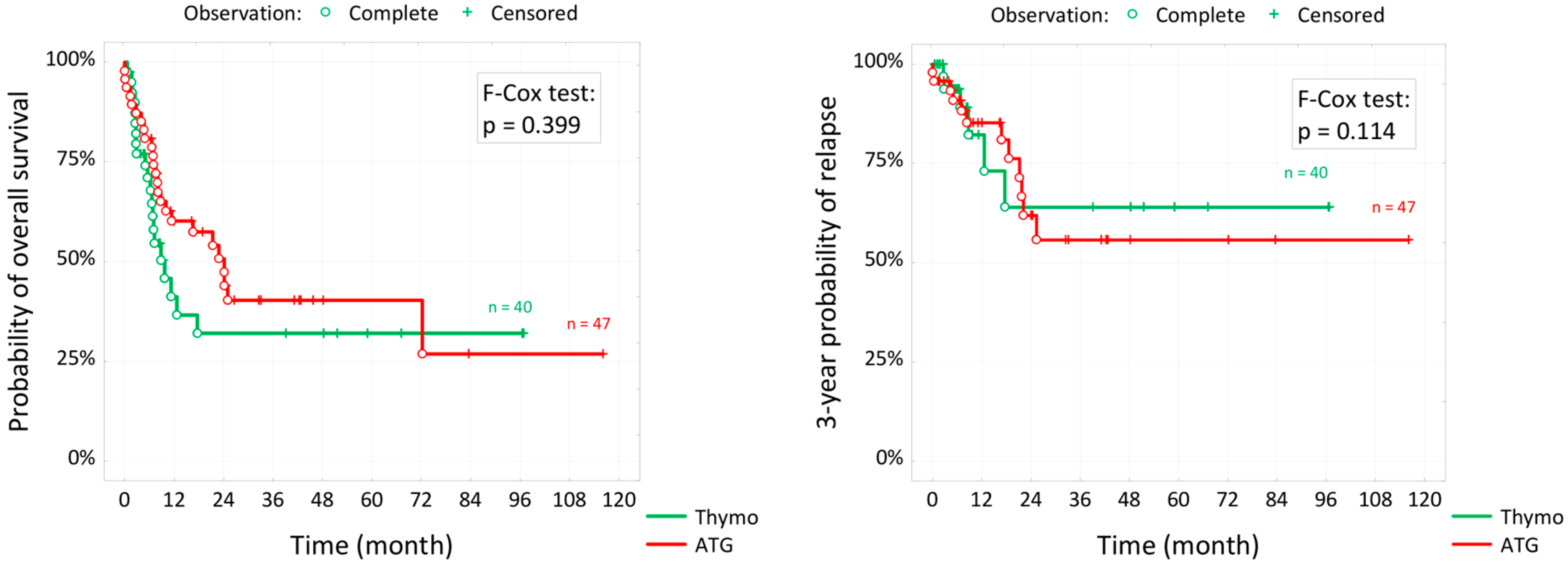

Table 1.
Patient- and disease-related characteristics.
| ATG-T (n = 40) |
ATG-G (n = 47) |
P value | |||
| Median age, y (range) | 45 (35-53) | 55 (39-62) | 0.065 | ||
| Age, n (%) | 0.003 | ||||
| <55 years | 33 | 82.5% | 24 | 51.1% | |
| ≥55 years | 7 | 17.5% | 23 | 48.9% | |
| Sex, n (%) | 0.832 | ||||
| Male | 23 | 57.5% | 27 | 57.4% | |
| Female | 17 | 42.5% | 20 | 42.6% | |
| Diagnosis, n (%) | 0.524 | ||||
| AML+MDS | 15 | 37.5% | 25 | 53.2% | |
| ALL | 10 | 25.0% | 8 | 17.0% | |
| HL+NHL+MM | 8 | 20.0% | 7 | 14.9% | |
| OMF, CML, SAA et al. | 7 | 17.5% | 7 | 14.9% | |
| The advancement of the disease, n (%) | 0.425 | ||||
| Remission | 23 | 57.5% | 32 | 68.1% | |
| Active | 17 | 42.5% | 15 | 39.1% | |
| ELN cytogenetic risk, n (%) | 0.246 | ||||
| Favorable | 3 | 7.5% | 11 | 23.4% | |
| Intermediate | 9 | 22.5% | 9 | 19.2% | |
| Adverse | 5 | 12.5% | 4 | 8.5% | |
| N/A | 23 | 57.5% | 23 | 48.9% | |
| Complete remission number, n (%) | 0.147 | ||||
| 0 | 18 | 45.0% | 14 | 29.8% | |
| 1 | 16 | 40.0% | 27 | 57.4% | |
| 2 | 6 | 15.0% | 3 | 6.4% | |
| 3 | 0 | 0.0% | 2 | 4.3% | |
| 4 | 0 | 2.2% | 1 | 2.1% | |
| CMV IgG, n (%) | 0.936 | ||||
| Negative | 7 | 17.5% | 9 | 19.2% | |
| Positive | 33 | 82.5% | 38 | 80.8% | |
Table 2.
Transplantation-related characteristics.
| ATG-T (n = 40) |
ATG-G (n = 47) |
P value | |||
| Median donor age, years (range) | 30 (24-39) | 33 (25-40) | 0.399 | ||
| Donor age, n (%) | 0.849 | ||||
| <40 years | 30 | 75.0% | 35 | 74.5% | |
| ≥40 years | 10 | 25.0% | 12 | 25.5% | |
| Donor sex, n (%) | 0.145 | ||||
| Male | 11 | 27.5% | 6 | 12.8% | |
| Female | 29 | 72.5% | 41 | 87.2% | |
| Locus with a mismatch, n (%) | 0.221 | ||||
| A | 13 | 44.8% | 1 | 10.0% | |
| B | 2 | 6.9% | 2 | 20.0% | |
| C | 10 | 34.5% | 5 | 50.0% | |
| DQ | 4 | 13.8% | 2 | 20.0% | |
| Donor status CMV IgG , n (%) | 0.954 | ||||
| Negative | 16 | 40.0% | 18 | 38.3% | |
| Positive | 24 | 60.0% | 29 | 61.7% | |
| CMV prophylaxis, n (%) | 0.004 | ||||
| Acyclovir | 36 | 90.0% | 27 | 58.7% | |
| Valgancyclovir | 1 | 2.5% | 4 | 8.7% | |
| Acyclovir+ Valgancyclovir | 0 | 0.0% | 10 | 21.7% | |
| Letermovir | 3 | 7.5% | 5 | 10.9% | |
| Conditioning regimen, n (%) | 0.014 | ||||
| RIC | 4 | 10.0% | 15 | 31.9% | |
| MAC | 33 | 82.5% | 25 | 53.2% | |
| NMA | 3 | 7.5% | 7 | 14.9% | |
| Median CD34+ count, x106/kg (range) | 8.1 [5.1-9.6] | 7.4 [5.5-9.9] | 0.810 | ||
Table 3.
Post-transplantation outcomes - graft-versus-host disease.
| ATG-T (n = 40) |
ATG-G (n = 47) |
P value | |||
| Acute GvHD, n (%) | 0.084 | ||||
| Yes | 26 | 65.0% | 21 | 44.7% | |
| No | 14 | 35.0% | 26 | 55.3% | |
| Degree of acute GvHD, n (%) | 0.103 | ||||
| 0 | 14 | 35.0% | 27 | 57.4% | |
| 1 or 2 | 18 | 45.0% | 15 | 31.9% | |
| 3 or 4 | 8 | 20.0% | 5 | 10.6% | |
| Deegree of acute GvHD, n (%) | 0.308 | ||||
| 0 or 1 | 23 | 57.5% | 32 | 68.1% | |
| 2 or more | 17 | 42.5% | 15 | 31.9% | |
| Median time of onset of acute GVHD, days (range) | 24 [17-36] | 29 [19-49] | 0.366 | ||
| Chronic GvHD, n (%) | 0.001 | ||||
| Yes | 3 | 7.5% | 18 | 38.3% | |
| No | 37 | 92.5% | 29 | 61.7% | |
Table 4.
Post-transplantation outcomes - infections.
| ATG-T (n = 40) |
ATG-G (n = 47) |
P value | |||
| CMV reactivation, n (%) | <0.001 | ||||
| Yes | 28 | 70.0% | 15 | 31.9% | |
| No | 12 | 30.0% | 32 | 68.1% | |
| Median time between transplant and CMV reactivation, days (range) | 35 [26-51] | 69 [33-127] | 0.057 | ||
| Time between transplant and CMV, n (%) | n = 27 | n = 15 | 0.008 | ||
| <61 days | 21 | 77.8% | 5 | 33.3% | |
| ≥61 days | 6 | 22.2% | 10 | 66.7% | |
| Median CMV copy number (PCR), count (range) | 1000 (0-18000) |
0 (0-634) |
0.004 | ||
| CMV copy (CR), n (%) | <0.001 | ||||
| <400 copies | 14 | 35.0% | 35 | 74.5% | |
| ≥400 copies | 26 | 65.0% | 12 | 25.5% | |
| Symptoms of CMV disease, n (%) | n = 35 | n = 16 | 0.005 | ||
| Yes | 5 | 14.3% | 9 | 56.2% | |
| No | 30 | 85.7% | 7 | 43.8% | |
| Disease manifestation, n (%) | 0.367 | ||||
| No | 38 | 96.0% | 37 | 80.4% | |
| Pneumonia CMV | 0 | 0.0% | 2 | 4.3% | |
| Hepatitis | 0 | 0.0% | 1 | 2.2% | |
| Gastrointestinal | 1 | 1.2% | 4 | 8.7% | |
| Pancytopenia | 0 | 0.0% | 1 | 2.2% | |
| Klebsiella | 1 | 1.2% | 1 | 2.2% | |
| Other viral reactivations: | 0.001 | ||||
| Yes | 6 | 15.0% | 31 | 66.0% | |
| No | 34 | 85.0% | 16 | 34.0% | |
| EBV | 4 | 10.0% | 19 | 40.4% | 0.001 |
| BKV | 2 | 5.0% | 14 | 29.8% | 0.004 |
| JCV | 1 | 2.5% | 10 | 21.3% | 0.010 |
| HHV6 | 0 | 0.0% | 1 | 2.1% | 1.000 |
| Others | 1 | 2.5% | 0 | 0.0% | 0.460 |
Table 5.
Post-transplantation outcomes - 3-year probability of relapse and 5-year OS.
| ATG-T (n = 40) |
ATG-G (n = 47) |
P value | |
| Median months of follow-up (interquartile range)* | 8 [5-52] | 22 [12-42] | 0.110 |
| 3-year probability of relapse(t=3) | 63.9% | 55.7% | 0.438 |
| 5-years overall survival OS(t=5) | 32.0% | 40.3% | 0.423 |
| Median survival function** | 8.9 months | 23.1 months |
* Median follow-up time does not include deaths. ** Number of months survived by half the patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



