Submitted:
27 November 2023
Posted:
29 November 2023
You are already at the latest version
Abstract
Breast cancer is the most common cancer among women worldwide, and estrogen receptor-positive (ER+) breast cancer accounts for a significant proportion of cases. While various treatments are available, endocrine therapies are often the first-line treatment for this type of breast cancer. However, the development of drug resistance poses a significant challenge in managing this disease. ESR1 mutations have been identified as a common mechanism of endocrine therapy resistance in ER+ breast cancer. The first-generation selective estrogen receptor degrader (SERD) fulvestrant has shown some activity against ESR1 mutant tumors. However, due to its poor bioavailability and need for intramuscular injection, it may not be the optimal therapy for patients.
Second-generation SERDs have been developed to overcome these limitations. These newer drugs have improved oral bioavailability and pharmacokinetics, making them more convenient and effective for patients. Several oral SERDs are now in phase III trials for early and advanced ER+ breast cancer. This review summarizes the background of oral SERD development, the current status, and future perspectives.
Keywords:
Breast cancer
; Estrogen receptor-positive
; endocrine therapies
; resistance
; selective estrogen degrades
; Oral
Introduction
Breast cancer is a leading cause of cancer-related deaths among women worldwide, with over 2 million new cases diagnosed each year [1]. It is estimated that there were 297,790 new breast cancer cases in 2023, accounting for 15% of new cancer diagnoses with 43,700 deaths [2]. The majority of breast cancers express the estrogen receptor (80%) [3]. Therefore, endocrine therapy (ET) has been a mainstay of breast cancer treatment for many years. ET blocks the estrogen receptor pathway and inhibits the growth and proliferation of estrogen receptor-positive (ER+) breast cancer[3]. Aromatase inhibitors (AI) and a selective ER modulator, tamoxifen, have been used to treat ER+ breast cancers. However, the development of resistance to these ET has limited their effectiveness, driving the exploration of new treatment options [4]. Fulvestrant, a Selective Estrogen Receptor Degrader (SERD), represents a newer class of ET that specifically target and degrade the ER, reducing ER’s activity and inhibiting the growth of ER+ breast cancer [5].
This unique mechanism of action offered the potential for fulvestrant to effectively treat breast cancers that have developed resistance to traditional ET [6]. Fulvestrant has been shown to prolong progression-free survival and possibly overall survival compared to AI among metastatic ER+ HER2 non-amplified (HER2-) breast cancer patients [7,8,9]. In addition, fulvestrant has been well tolerated, with the most common side effects being mild to moderate, including hot flashes, fatigue, and join pain in the clinical trials [9].
Mechanism of Action of SERDs
The activity of the ER is primarily mediated through its interaction with specific DNA sequences known as estrogen response elements (EREs). The estrogen binding to the ER promotes the dimerization of the receptor and its subsequent binding to the EREs located in the promoter regions of estrogen-responsive genes. Once bound to the ERE, the ER acts as a transcription factor, recruiting coactivators or corepressors to initiate the transcription of the target genes [8]. AIs primarily act by reducing estrogen levels available for binding to the ER, thereby decreasing its activity as a transcription factor. In contrast, SERMs bind to the ER and modulate its activity tissue-specific manner. For example, in breast tissue, SERMs such as tamoxifen act as antagonists, competing with estrogen for the ER binding site and preventing the activation of genes involved in cell growth and proliferation. Selective estrogen receptor degraders (SERDs) are a newer class of ET that bind to the ER and induce its degradation, thereby reducing the overall activity of the receptor. Unlike SERMs, which can act as either agonists or antagonists, SERDs act exclusively as antagonists of the ER. This class of drugs includes fulvestrant, the first and, until January 2023, the only FDA-approved SERD. SERDs can block the effects of estrogen on breast cancer cells by binding to the ER and promoting its degradation, leading to a decrease in the expression and activity of ER target genes [10]. (Figure 1) Fulvestrant has been shown to induce the proteasomal degradation of the ER in a dose-dependent manner [11]. This is achieved through its ability to promote the dissociation of chaperone proteins such as heat shock protein 90 (Hsp90) and p23 from the ER, resulting in the exposure of a hydrophobic surface on the receptor recognized by the E3 ubiquitin ligase complex. The E3 ligase then adds ubiquitin molecules to the exposed lysine residues on the ER, targeting it for the degradation by the proteasome [12]. Additionally, fulvestrant has been shown to have a longer duration of action than other ER antagonists due to its ability to induce downregulation and degradation of the receptor, as opposed to simply blocking its activity [10].
Mechanism of action of ORAL SERDS
Overall, the unique molecular mechanism of the fulvestrant as a SERD has led to its successful use in treating advanced ER+ breast cancer, both as a first-line therapy and in patients who have progressed on prior endocrine therapies as a single agent or in combination with other ET or targeted therapies [8,13,14,15,16].
However, fulvestrant has several limitations. Fulvestrant is only available as an injectable formulation. This can be inconvenient for patients who prefer oral medications or have difficulty with injections. Compared to an AI, fulvestrant seems to be superior in treating ER+ metastatic breast cancer with ESR1 mutation. However, fulvestrant’s efficacy against ESR1 mutant metastatic breast cancer in the second line is modest at best with median PFS ranging from 3-4 months [14,17]. Additionally, and most importantly, after adopting CDK4/6 inhibitors in combination with AI as the standard first-line treatment for metastatic ER+ breast cancer a few years ago, newer clinical data have revealed minimal efficacy of fulvestrant monotherapy in the second line among these CDK4/6 inhibitor-treated tumors [18]. Several oral SERDs are in development to address these drawbacks and are currently in clinical trials.
Elacestrant
Elacestrant is a nonsteroidal oral SERD that degrades ER and inhibits gene transcription, induction, and cell proliferation, specifically in ER+ breast cancer cell lines [13]. In January 2023, this drug became the first oral SERD to receive the FDA’s approval in treating ER+ HER2 negative (HER2-) metastatic breast cancer [19].
RAD1901-005 was a phase I study that studied the effects of elacestrant as monotherapy among pretreated postmenopausal patients with ER+ HER2- metastatic breast cancer. Elacestrant was associated with an objective response rate (ORR) of 19.4% among patients who received RP2D, 15% in patients with prior SERD use, 16.7% in patients with prior CDK4/6i use, and 33.3% in patients with ESR1 mutation. The clinical benefit rate was 42.6% overall. No dose limiting toxicity (DLT) was observed. The most common adverse effects (AEs) include nausea (33%), increased blood triglycerides (25%), and decreased blood phosphorus (25%). Lastly, the most AEs were grades 1-2. The recommended phase II dose was 400mg once daily [13]. RAD1901-106 was a phase Ib open-label non-randomized study investigating the effects of elacestrant monotherapy on the ER binding sites in 16 patients with pretreated postmenopausal ER+ metastatic breast cancer. The median reduction in tumor fluoroestradiol (FES) uptake was 89.1%. ORR was 11.1%, and the clinical benefit rate was 30.8%. Common AEs include nausea (68.8%), fatigue (50%), and dyspepsia (43.8%). Most AEs were grade 2 in severity. Findings showed reduced ER availability with elacestrant doses of 200 or 400 mg daily and a modest antitumor activity in this heavily pretreated population [20]. SOLTI-1905 ELIPSE was a phase I study investigating the effect of preoperative elacestrant monotherapy on cancer cell proliferation in postmenopausal women with treatment-naïve ER+ HER2- early-stage breast cancer [21]. The primary endpoint was complete cell cycle arrest (CCCA) defined as Ki67 ≤ 2.7%. After 4 weeks, CCCA was achieved in 27% of patients. A 41% relative reduction in Ki-67 from baseline was also observed. One treatment-related AE required the patient to discontinue treatment. Most AEs were hot flash and constipation, which were all grade 1. These findings showed that elacestrant was associated with good biological response with a tolerable safety profile [22].
The encouraging data from the RAD1901-005 study supported the development of the EMERALD trial, an active phase III trial comparing the efficacy and safety of elacestrant with the standard of care (SOC) ET (fulvestrant or exemestane) in patients with breast cancer who have prior received a CDK4/6 inhibitor [13]. The EMERALD trial showed an increase in progression-free survival (PFS) [6 months PFS 34.3% (95% CI, 27.2 to 41.5) versus 20.4% (95% CI, 14.1 to 26.7), HR 0.70 (0.55 to 0.88)] associated with elacestrant versus SOC. Among the patients with ESR1 mutation, the 6-month PFS was 40.8 vs. 19.1 months [HR 0.55 (0.39 to 0.77)], demonstrating more benefit with elacestrant vs. SOC in this cohort compared to the benefit seen in all patients. Among patients without ESR1 mutant tumors, the 6-month PFS was 28.58 vs 21.85 months [HR 0.866 (0.628 to 1.186)], numerically showing the trend towards favoring elacestrant but not reaching the statistical significance. Twenty-seven percent of patients on the elacestrant arm and 20% on the SOC arm developed grade 3 or 4 AEs. Most common AEs with elacestrant were GI related, including nausea, vomiting, diarrhea, decreased appetite, and arthralgias. In addition, the duration of disease control with a CDK4/6 inhibitor was predictive of the benefit of elacestrant compared to SOC. Patients with at least 6 months, 12 months, and 18 months of prior CDK4/6 inhibitor use had median PFS of 2.79 vs. 1.91 months, 3.78 vs. 1.91 months, and 5.45 vs. 3.29 months, favoring elacestrant in each group [23]. Based on the results from the EMERALD trial, elacestrant was approved by the FDA for treating ER+ HER2- advanced breast cancer with ESR1 mutation and prior treatment with at least one line of ET.
There are a few ongoing studies with elacestrant. The ELEVATE study is a phase 1b/2, open-label, umbrella study where RP2D of elacestrant, combined with other drugs (alpelisib, everolimus, ribociclib, and palbociclib), will be identified and safety and efficacy assessed (NCT05563220)[24]. NCT04791384 is an ongoing phase Ib/II study investigating the combination therapy of elacestrant with abemaciclib in HR+ HER2- metastatic breast cancer with metastasis to the brain [25].
Other Oral SERDs in Development
Camizestrant (AZD9833)
Camizestrant is a pure ER antagonist and next-generational oral SERD. SERENA 1 is a phase I, open-label, dose-dependent exposure trial that analyzed the safety, tolerability, and preliminary clinical efficacy of camizestrant monotherapy [part A (escalation)/ part B (expansion)] and in combination with palbociclib (parts C/D), everolimus (E/F), abemaciclib (G/H) and capivasertib (I/J) in pretreated women with ER+ HER2- advanced breast cancer. In part A/B, treatment-related AEs were visual disturbances, bradycardia, nausea, fatigue, dizziness, and vomiting. Three doses- 75mg QD, 150mg QD and 300mg QD were proposed for a phase II study. One out of 7, 2 out of 11, and 2 out of 10 patients achieved ORR with these doses, respectively, in this study [26]. SERENA-1 parts C/D is an ongoing study with a multi-part open-label trial currently examining camizestrant combined with palbociclib. Data from camizestrant 75mg QD in combination with the standard dose of palbociclib has been presented [27]. Some patients experienced bradycardia, GI disturbances, and visual disturbances likely related to camizestrant; however, most were grade 1, and no patients required dose interruption or reduction for AEs in this study. The clinical benefit rate at 24 weeks for these heavily pretreated patients was 28% with this combination [27]. This combination will be further analyzed in ongoing phase III studies of SERENA-4 and SERENA-6 [27].
SERNA-2 is a randomized, open-label, multicentre phase II trial that analyzed the efficacy and safety of camizestrant with the various dosages of 75mg-300mg administered as a monotherapy in women with ER+, HER2- previously treated advanced breast cancer in comparison with fulvestrant. Camizestrant 300mg QD arm was discontinued after 20 patients were enrolled in that arm. Camizestrant significantly reduced the risk of disease progression by 42% at a 75mg dose [HR] 0.58, 0.41-0.81); p=0.0124, p=0.0124, PFS of 7.2 vs. 3.7 months) and 33% at a 150mg dose [HR 0.67, 0.48-0.92); p=0.0161, PFS of 7.7 vs 3.7 months) compared to fulvestrant [28]. Among the ESR1 mutant tumors, median PFS with camizestrant 75 and 150mg QD and fulvestrant were 6.3, 9.2, and 2.2 months, numerically favoring a benefit with camizestrant compared to fulvestrant but was not statistically significant as this phase II study was not powered to demonstrate benefit in ESR1 mutant subset. Among the ESR1 wild-type tumors, the efficacy seemed similar numerically: 7.2, 5.8, and 7.2 months, respectively. Twelve percent of patients receiving 75mg QD of camizestrant developed grade 3 or higher AEs compared to 13% receiving fulvestrant and 21% receiving camizestrant 150mg QD. The most common AEs were bradycardia, visual disturbances, and fatigue.
Multiple ongoing trials are investigating camizestrant further. SERENA-3 is a randomized, open-label, parallel-group pre-surgical trial looking at different Camizestrant 75-150mg doses in postmenopausal and possible premenopausal women with ER+/HER2- primary breast cancer [29]. SERENA-4 is an ongoing randomized multicenter, double-blind phase III trial comparing the safety and efficacy of camizestrant plus palbociclib vs. anastrzole plus palbociclib in patients with ER+/HER2- previously untreated breast cancer [30].
SERENA-6 is a novel and exciting phase III clinical trial where patients with advanced ER+ HER2- breast cancer who are receiving an AI plus palbociclib or abemaciclib and have developed ESR1 mutation but without overt disease progression will be randomized to continuation of current treatment vs. switching AI to camizestrant with the continuation of same CDK4/6 inhibitor [31]. The primary endpoint is PFS.
Giredestrant
Giredestrant is another nonsteroidal SERD designed to target ER+ breast cancer [32]. GO39932 is an 1a/1b multicenter, open-label, dose-escalation study investigating the safety profile and preliminary antitumor activity of giredestrant alone, giredestrant in combination with palbociclib. Participants have ER+ HER2- advanced or metastatic breast cancer [33].
In GO39932 Cohort A, giredestrant as a single agent was well tolerated at all doses without any DLTs, with low-grade AEs (i.e., nausea, arthralgia, and fatigue), none of which required participants to discontinue treatment in phase 1a. It had encouraging antitumor effects and clinical benefits at all doses [34]. In GO39932 cohort B, giredestrant with palbociclib was assessed. None of the participants had to discontinue treatment due to AEs. Adverse effects in >/= 10% of patients included neutropenia, fatigue, bradycardia, diarrhea/constipation, dizziness/nausea, and so forth. 57% of patients had >/= grade 3 AEs. 50% of patients had >/= grade 3 neutropenia. No drug-drug interactions were observed between giredestrant and palbociclib [32,34]. Clinical activity reported for the 30mg monotherapy arm and the 100mg dose with the palbociclib arm was encouraging, with ORR at 20.0% and 47.7%, respectively. Clinical benefit rates were 55.0% and 81.3%, respectively [35].
acelERA BC is a randomized, open-label, multicenter phase 2 study. It investigated the safety and efficacy of girdestrant compared to physicians’ choice ET (fulvestrant or an AI) for patients with ER+ HER2- locally advanced or metastatic breast cancer who have already been treated with one to two types of systemic therapy [36]. The trial could not meet the primary endopoint of investigator-assessed PFS; nevertheless, the giredestrant did show numerical improvement compared to ET in ORR and clinical benefit rate. Additionally, in patients with the ESR1 mutation, their PFS was numerically higher with the giredestrant. Lastly, it was well tolerated and had a good safety profile consistent with others [37].
CoopERA is a completed randomized, open-label, multicenter phase 2 study investigating the efficacy, safety, and pharmacokinetics of giredestrant versus anastrozole within a 14-day window of opportunity phase followed by 16 weeks of neoadjuvant treatment phase of giredestrant plus palbociclib vs. anastrozole plus plalbociclib. The patient population is postmenopausal with ER+ HER2- untreated early breast cancer [38]. Giredestrant did indeed meet the primary endpoint and had higher Ki-67 suppression after week 2 compared to anastrozole. Note, this higher suppression continued up to surgery with giredestrant with palbociclib (–81% [95% CI: –86%, –75%]) versus anastrozole with palbociclib (–74% [95% CI: –80%, –67%]). Lastly, the safety profile compares to other giredestrant studies. This study shows that giredestrant demonstrates more antiproliferation in ER+ HER- early breast cancer than an aromatase inhibitor, anastrozole. Giredestrant with palbociclib also had a higher complete cell cycle arrest at surgery, defined as Ki67 ≤ 2.7% compared to anastrozole with palbociclib (20% vs. 14%) [39]. There are multiple ongoing studies investigating giredestrant in ER+ breast cancer where results are pending.
evERA is an ongoing randomized, open-label, multicenter phase III study that investigates the efficacy and safety of giredestrant with everolimus versus exemestane with everolimus. Participants are patients with ER+ HER2- locally advanced or metastatic breast cancer [40].
lidERA is an ongoing randomized, open-label, multicenter phase III study investigating the efficacy and safety of giredestrant versus physician's choice endocrine therapy. Participants are patients with medium-risk and high-risk histologically-proven Stage I to Stage III confirmed ER+ HER2- early breast cancer [40,41]. Both pre and postmenopausal women are eligible for this study.
Amcenestrant
Amcenestrant is an orally bioavailable SERD with pure ER antagonism in vivo [42]. AMEERA-1 is an open-label single-arm study that evaluated amcenestrant monotherapy in postmenopausal women with ER+/HER2- advanced breast cancer who were heavily pretreated. In AMEERA-1 arm 1 part A-B, the optimal dosing of 400mg QB of amcenestrant monotherapy was chosen for Phase 2 dose with no grade ≥3 TRAEs like cardiac/eye toxicities reported. The confirmed objective response rate was 5/46 (10.9%), with an overall clinical benefit rate (CBR) of 13/46 (28.3%). The ESR1 wild type and mutated ESR1 showed similar CBR of 34.6% and 21.1%, respectively [43]. The result showed that amcenestrant at RP2D of 400mg QD monotherapy demonstrated antitumor activity regardless of baseline ESR1 mutation status and was well tolerated [43].
AMEERA-3 was a prospective, open-label, randomized phase 2 study to assess safety and efficacy of amcenestrant compared to ET of physician’s choice in patients with ER+/HER2- metastatic or locally advanced breast cancer or metastatic breast cancer that progressed on ET. However, the trial did not meet its primary endpoint. The PFS was similar at 3.6 months for amcenestrant and 3.7 months for endocrine monotherapy [44]. TRAEs mainly were grade 1 or 2. In the I-SPY2 Endocrine Optimization Protocol (EOP) the safety and efficacy of amcenestrant was evaluated with and without abemaciclib or letrozole [45]. The primary objective of the EOP is to assess the feasibility of treating molecularly selected patients with early stage ER+ HER2- molecular low risk breast cancerwith neoadjuvant endocrine therapy.
AMEERA-4 (NCT04191382) was a phase II preoperative window of opportunity that compared the safety and efficacy of two dose levels of amcenestrant and standard dose of letrozole with paired biopsies assessed for biomarkers in 1:1:1 randomization design among early stage ER+ HER2- breast cancer patients [46]. The primary endpoint was the change from baseline in Ki67 after 2 weeks of treatment with amcenestrant or letrozole using paired biopsies. The reduction of Ki67 was 75.9% (67.9, 81.9) for amcenestrant 400 mg, 68.2% (58.4, 75.7) for amcenestrant 200 mg and 77.7% (70.0, 83.4) for letrozole.All TRAEs were grade 1 or 2 and were similar among 3 arms ranging from 20-25%. This trial was prematurely discontinued by the sponsor due to their strategic decision to stop the development of this drug.
AMEERA-5, a phase III, randomized, double-blind, multinational study that analyzed women with ER+HER2- metastatic breast cancer and compared amcenstrant plus palbociclib versus letrozole plus palbociclib failed to reach the prespecified boundary of continuation on interim analysis [47]. Based on this, the global clinical development of amcenestrant was discontinued by the sponsor.
Imlunestrant
Imlunestrant is another oral SERD in development. EMBER is an ongoing phase 1a/1b study with imlunestrant (doses 200-1200 mg) used as a monotherapy and combined with abemaciclib +/- an aromatase inhibitor (anastrozole, exemestane, or letrozole). In phase 1a, patients with ER+ HER2- advanced breast cancer with three or fewer prior therapies were recruited. Patients with ER+ endometrial cancer with prior platinum therapy were also recruited [48]. So far, monotherapy demonstrates no dose-dependent toxicities, TEAEs mostly grade 1 or 2, including nausea, fatigue, and diarrhea. There was one grade 3 TEAE, diarrhea. Additionally, combination therapy (imlunestrant with abemaciclib +/- an aromatase inhibitor) in phase 1b has shown a satisfactory safety profile [49]. New findings presented at the 2022 San Antonio Breast Cancer Symposium regarding the combination therapy shows favorable efficacy with a 12-month PFS compared to existing historical data from MONARCH 2 and 3 [50]. Another monotherapy trial is EMBER-2, an ongoing phase 1 study preoperative window studying the effects of imlunestrant on Stage I-III ER+ HER2- breast cancer in postmenopausal patients. As of yet, no results have been released [51].
EMBER-3 is an open-label, randomized 3-arm phase 3 study which compares safety and efficacy of imlunestrant monotherapy vs. SOC ET (exemestane or fulvestrant) vs. imlunestrant plus abemaciclib among advanced ER+ HER2- breast cancer patients who have prior received an ET for advanced breast cancer [52] . EMBER-4 is another ongoing phase 3 study investigating imlunestrant compared to SOC ET in participants with high risk ER+ HER2- early breast cancer. These participants will have already had two to five years of adjuvant endocrine therapy prior to this [53].
Rintodestrant
Rintodestrant is an oral SERD that competitively binds and degrades the estrogen receptor (ER). The safety and efficacy of rintodestrant were investigated in a phase 1 study NCT03455270 among ER+ HER2- advanced breast cancer patients. Based on the part 1 (dose escalation) and part 2 (dose expansion), optimal dose of rintodestrant was 800mg daily. Overall 63% patients develop TRAEs and most common TRAEs were hot flush, fatigue and nausea [54]. The part 3 of the study assessed safety and efficacy of the combination of rintodestrant with palbociclib in patients with HR+/HER2- metastatic breast cancer already progressed on previous endocrine therapy. The overall CBR with this combination was 61% (61% among ESR1 wild type, 56% ESR1 mutant) [55].
AZD9496
AZD9496 is a preclinical compound that can be taken orally and is nonsteroidal, potent, and selective in the degradation and inhibition of ER activity [56]. Investigations of the effects of AZD9496, tamoxifen, and fulvestrant on estrogen-responsive genes in tumor samples were reported in a study. A human transcriptome array was used to measure mRNA levels in tumors treated with the drugs. Gene expression analysis was performed on tumors treated with the drugs. According to the study results, AZD9496 inhibits the expression of estrogen-responsive genes similarly to fulvestrant and tamoxifen. A dose-dependent inhibitory effect was also observed between fulvestrant and AZD9496 in MCF-7 cells compared to tamoxifen when estrogen-regulated genes were examined. A significant decrease in ESR1 mRNA levels was not observed in vitro, suggesting that the protein downregulation previously described is due to a decrease in protein levels rather than an increase in transcript levels [57].
A preclinical study showed that AZD9496 could antagonize and degrade the estrogen receptor in breast cancer cell lines, xenograft models, and patient-derived xenografts with mutations in the ESR1 gene. AZD9496 was more effective at inhibiting tumor growth when combined with the PI3K pathway inhibitors and a CDK4/6 inhibitor. Clinical trials of AZD9496 in phase I showed good tolerability and safety, and some patients who had been heavily pretreated could stabilize their disease for a prolonged period [57].
As part of a clinical trial conducted by Robertson et al. (NCT03236974), AZD9496 was compared with fulvestrant with regard to the effects on changes in ER, progesterone receptor (PR), and Ki-67 biomarkers in patients who were newly diagnosed with ER+ HER2- breast cancer. A random allocation of patients was conducted between days 5 and 14 for treatment with AZD9496 and day 1 for fulvestrant. Based on the study's results, AZD9496 reduced the expression of ER, PR, and Ki-67, but the reductions were not superior to fulvestrant ones. The plasma concentration of AZD9496 was lower than predicted, whereas the plasma concentration of fulvestrant was consistent with historical data. Both treatments had no significant safety concerns and were well tolerated [56].
Other SERDs in Early Stage of Development
Borestrant
ZB716, also called borestrant, is a modified form of SERD fulvestrant with a boronic acid insertion allowing it to be orally bioavailable. Borestrant has shown superiority in comparison to fulvestrant with better ER antagonism in preclinical data. ENZENO is an ongoing open-label, multicenter phase I/II study investigating borestrant's properties as a monotherapy: safety, pharmacokinetics, pharmacodynamics, tolerability, and preliminary antitumor properties. Additionally, these properties will be investigated with combination therapy: borestrant with palbociclib. Participants are patients with ER+ HER2- locally advanced or metastatic breast cancer. As of yet, no results have been released [58].
D-0502 (Taragarestrant)
This study, with identifier NCT03471663, is an ongoing open-label phase 1 study investigating the safety, pharmacokinetics, preliminary antitumor properties, and tolerability of D-0502 as a monotherapy as well as in conjunction with palbociclib as a combination therapy. Participants are patients with ER+ HER2- advanced or metastatic breast cancer [59]. So far, results have shown good tolerability and preliminary clinical activity with D-0502. Regarding 22 patients that received monotherapy, preliminary efficacy results show an ORR of 5% and CBR of 36%. Among 13 patients that received D-0502 in combination with palbociclib, preliminary results showed an ORR of 15% and CBR of 77%. Additionally, there were no dose-limiting toxicities observed [60].
ZN-c5
ZN-c5 is another oral small molecule antagonist and degrader of estrogen receptors that is being developed [61]. ZN-c5 has shown some activity in estrogen-dependent tumor models and has been well tolerated in clinical trials. In a clinical trial (NCT04514159), ZN-c5 was combined with abemaciclib. Patients may have undergone one previous hormonal-based therapy; however, they have not undergone any prior chemotherapy or received CDK4/6 inhibitors. The study was conducted in continuous 28-day cycles until disease progression or the occurrence of unacceptable toxicity. In the first clinical trial, ZN-c5 demonstrated good tolerance when administered at a dose of 50 mg [62].
Zn-c5 is an effective antagonist of the estrogen receptor in vivo and in vitro, as well as a potent degradative agent, and it is highly bioavailable compared to other SERDs. Oral administration of ZN-c5 at 5 mg/kg and 10 mg/kg resulted in significant inhibition of tumor growth in MCF-7 orthotopic tumor xenograft models, and ZN-c5 combined with CDK4/6 or PI3K inhibitors enhanced antitumor activity. The antitumor activity of ZN-c5 was also improved over that of fulvestrant in ER mutant models [61]. As a single agent and in combination studies, zinc-c5 is currently undergoing clinical trials, and its potency and degradation properties may potentially benefit patients with estrogen receptor-positive breast cancer (NCT03560531, NCT04514159) [62,63].
In addition to testing ZN-c5 on MCF-7 cells, its effects were also tested on patient-derived xenograft models with ER mutations, such as WHIM20, a patient-derived model with the Y537S mutation in ESR1. ZN-c5 at 40 mg/kg reduced tumor growth by 64%, while fulvestrant at 200 mg/kg only reduced tumor growth by 13% (eight times higher than the clinical dose). According to these results, ZN-c5 exhibits superior antitumor properties compared with fulvestrant in xenograft models of human tumors [61].
In a clinical trial (NCT04514159), ZN-c5 was administered in combination with abemaciclib. Patients may have undergone one previous hormonal-based therapy; however, they have not undergone any prior chemotherapy or received CDK4/6 inhibitors. The study was conducted in continuous 28-day cycles until disease progression or the occurrence of unacceptable toxicity In the first clinical trial, ZN-c5 demonstrated good tolerance when administered at a dose of 50 mg [62]. This treatment demonstrates encouraging antitumor properties as an orally bioavailable SERD, thereby holding the potential to offer significant benefits to individuals afflicted with estrogen receptor-positive breast cancer.
Discussion
SERDs are important endocrine therapy used to treat ER positive breast cancer. Parenteral SERD fulvestrant has been approved and been used in the treatment of metastatic ER positive breast cancer for the last 2 decades. However, need for large volume intramuscular injections and poor bioavailability are important limitations of fulvestrant. In addition, in the current era of CDK4/6 inhibitors, the activity of fulvestrant on ER positive breast cancer (both ESR1 wild type and ESR1 mutant) after tumor progression on CDK4/6 inhibitors appears limited.
The current trend of robust clinical studies for the development of oral SERDs may replace fulvestrant and improve outcomes of patients with ER positive metastatic breast cancer. Elacestrant, a novel oral SERD has already received approval from the FDA for the treatment of ESR1 mutant ER positive HER2 negative metastatic breast cancer after at least one line of endocrine therapy. Based on the elacestrant data, ESR1 mutation and longer disease control with a CDK4/6 inhibitor appear to be predictive biomarkers for this oral SERD.
Fulvestrant still has a role in treating ER positive HER2 negative metastatic breast cancer, especially those with ESR1 wild type, often in combination with a targeted therapy. In addition, clinicians may chose fulvestrant in clinical scenario where compliance for oral medication is questionable. Similarly, elacestrant (and future oral SERDs, if approved) are prescription drugs while fulvestrant is generally administered in oncology clinics. There may be insurance coverage and out-of-pocket costs variations between oral SERDs vs. fulvestrant. This should also be explored and discussed with the patients.
From safety standpoint, in general, adverse effects associated with oral SERDs seem to be manageable. As the results of ongoing studies with novel oral SERDs (as single agent or in combination with other targeted therapies), the landscape of endocrine therapy-based treatment for ER positive HER2 negative breast cancer may continue to evolve in the next few years. There is a lack of data of activity of oral SERDs in PIK3CA mutant ER positive HER2 negative metastatic breast cancer. Hopefully, current ongoing studies and planned future studies will address this.
Conclusions
In this paper, we have discussed current preclinical and clinical data on novel oral SERDs. Many oral SERDs demonstrate meaningful efficacy and manageable safety in early-stage clinical trials. As of May 2023, elacestrant remains the only oral SERD to have received FDA’s approval in the treatment of ER positive HER2 negative metastatic breast cancer. Results of ongoing studies may lead to approval of more oral SERDs as a single agent or as a part of combination therapy in this space.

Table 1.
Summary of the clinical trial of SERD with its efficacy and safety features.
| Trial (Identifier) | Status | Study design | Study drug | Number enrolled | Disease setting | Study Population | Results | Safety |
|---|---|---|---|---|---|---|---|---|
| RAD1901-005 (NCT02338349) | Completed | Phase I Single group, open-label | Elascetrant (400 mg daily) | 57 | LABC or mBC | Postmenopausal patients with ER+ HER2- BC | ORR 19.4% in patients with RP2D, 15% in patients with prior SERD use, 16.7% in patients with prior CDK4/6i use, and 33.3% in patients with ESR1 mutation. The clinical benefit rate was 42.6% overall | No DLTs, most common AEs include nausea (33%), increated blood triglycerides (25%) and decreased blood phosphorous (25%), most AEs were grade 1-2 |
| RAD1901-106 (NCT02650817) | Completed | Phase Ib Two-cohort, open-label | Elascetrant (200-400 mg daily) | 16 | LABC or mBC | Postmenopausal patients with ER+ HER2- BC | Median reduction in tumor FES uptake was 89.1%. ORR was 11.1% and clinical benefit rate was 30.8% | Common adverse effects include nausea (68.8%), fatigue (50%), dyspepsia (43.8%). Most AEs were grade 2 in severity |
| SOLTI-1905 ELIPSE (NCT04797728) | Completed | Phase I Single group, open-label | Elascetrant (400 mg daily for 4 weeks) | 23 | Early resectable breast cancer | Treatment naive postmenopausal patients with ER+ HER2- BC | After 4 weeks, CCCA was achieved in 27% of patients. A 41% relative reduction in Ki-67 from baseline was observed | 1 TRAE event requiring patient to discontinue treatment. Most AEs were hot flush (n=6), hot flush (n=6), and constipation (n=2); all of which were grade 1 |
| NCT04791384 | Recruiting | Phase Ib/II Single group, open-label | Elascetrant + Abemaciclib | 44 | mBC | ER+ HER2- BC with brain mets and </= 2 prior lines of treatment | N/A | N/A |
| EMERALD (NCT03778931) | Active, not recruiting | Phase III Randomized, open-label | Elascetrant vs SOC (i.e. fulvestrant, anastrozole, letrozole, exemestane) | 478 | LABC or mBC | Postmenopausal patients with ER+ HER2- BC | The longer the duration of prior CDK4/6i, the increased PFS observed with elacestrant vs SOC. With duration on CDK4/6i of at least 12 months, median PFS was 8.6 months with elacestrant compared to 2.1 months with SOC. | Most AEs were grade 1-2, such as nausea. There were no grade 4 TRAEs reported. 3.4% of patients with elacestrant had to discontinue therapy versus 0,9% of patients with SOC. No deaths were observed in either arms. |
| GO39932 Cohort A (NCT03332797) | Active, not recruiting | Phase I Non-randomized, open-label | Giredestrant (10-250 mg) | 181 | LABC or mBC | ER+ HER2- BC | ORR at 20.0% and 47.7% respectively. Clinical benefit rates were 55.0% and 81.3% respectively. Of the FES-PET avid disease patients, 78% showed complete or near complete suppression of FES uptake. | No DLTs, low grade AEs (i.e. nausea, arthralgia, fatigue). None of the AEs required treatment termination |
| acelERA BC (NCT04576455) | Active, not recruiting | |||||||
| GO39932 Cohort B (NCT03332797) | ||||||||
| MORPHEUS-BREAST CANCER (NCT04802759) | Recruiting | Phase Ib/II Randomized, open-label, umbrella study | Giredestrant (30 mg) +/- abemaciclib/ipatasertib/inavolisib/ribociclib/everolimus/samuraciclib/PH FDC SC/PH FDC SC + abemaciclib/ PH FDC SC + palbociclib | 510 | Inoperable LABC or mBC | Cohort 1: ER+ HER2- BC who have shown disease progression during or after CDK4/6 inhibitor treatment in either 1st or 2nd line setting. Cohort 2: ER+ HER2+ BC who have shown disease progression during or after SOC anti-HER2 therapy (i.e. trastuzumab-and-taxane-based therapy), HER2-targeting ADC (i.e. ado-trastuzumab emtansine or trastuzumab-deruxtecan), or HER2-targeting TKIs (i.e. tucatinib, lapatinib, pyrotinib, or neratinib) | N/A | N/A |
| CoopERA (NCT04436744) | ||||||||
| evERA (NCT05306340) | Recruiting | Phase III, Randomized, open-label | Giredestrant (30 mg) + everolimus (10 mg) for 4 weeks versus Exmestane (25 mg) + everolimus (10 mg) for 4 weeks | 320 | LABC or mBC | ER+ HER2- BC participants with prior treatment of CDK4/6 inhibitors and endocrine therapy | N/A | N/A |
| heredERA (NCT05296798) | Recruiting | Phase III Randomized, open-label | Giredestrant + Phesgo versus ET (investigator's choice) + Phesgo after induction therapy with a taxane + Phesgo | 812 | LABC or mBC | ER+ HER2+ BC that is previously untreated | N/A | N/A |
| persevERA (NCT04546009) | Recruiting | Phase III, Randomized, double-blind | Giredestrant (30 mg daily) + palbociclib (125 mg for 3 weeks in every 4 week cycle) versus letrozole (2.5 mg daily) + palbociclib (125 mg for 3 weeks in every 4 week cycle) | 978 | LABC or mBC | ER+ HER2- recurrent or progressed BC | N/A | N/A |
| lidERA (NCT04961996) | Recruiting | Phase III Randomized, open-label | Giredestrant (30 mg daily) versus physician's choice ET for 5 years (if tolerated) | 4100 | early BC | Medium to high risk Stage I-III histologically confirmed ER+ HER2- BC | N/A | N/A |
| SERENA-1 part A (NCT03616587) | Ongoing | Phase I FIH 1, Open Label | camizestrant (25–450 mg daily) | 403 | LABC or mBC | women with HR+/ HER2- BC | 85% loss of mESR1,ORR 16.3%, CBR 42.3% (50% mESR1), mPFS 5.5 mo | DLT at 300 mg and 450 mg. G1: Visual disturbances, bradycardia, nausea, fatigue, dizziness, vomiting, asthenia |
| SERENA-2 (NCT04214288) | Active, not recruiting | Phase II randomized, open-label | camizestrant (75–300 mg) vs fulvestrant | 240 | LABC or mBC | postmenopausal women with HR+/ HER2- BC | Camizestrant 75mg reduced the risk of disease progression by 42% at a 75mg dose ([HR] 0.58, p=0.0124, median PFS of 7.2 versus 3.7 months 33% at a 150mg dose HR 0.67, PFS of 7.7 versus 3.7 months | TRAE's≥ 3 75ng: BP increase (1.3%)fatigue, nausea, anemia, arthralgia, alanine transaminase increase, extremity pain, hyponatremia, 150mg BP increase 1.3%, 300mg diarrhea (5.0%) and BP Increase (5.0%), Fulvestrant-Anemia (2.7%) |
| SERENA-3 | Recruiting | Phase II randomized, open-label | camizestrant (75-150mg) with 5 day washout before surgery | 132 | LABC or mBC | postmenopausal (possible premenopausal)women with HR+/ HER2- BC | N/A | N/A |
| SERENA-1 parts C/D (NCT03616587) | Ongoing | Phase I Multiple parts, open label | camizestrant + palbociclib | 305 (75 mg parts C/D 25) | LABC or mBC | women with ER+/HER2- BC | ORR 12%, 24 weeksCBR 28% | DLT at 150 mg dose. 75 mg cohorts G ≥ 3: neutropenia (68%). 75 mg cohorts all G: neutropenia (80%), visual disturbances (44%), fatigue (20%), infections (20%), anemia (20%), bradycardia (16%), nausea (16%), decreased appetite (12%), diarrhea (12%), vomiting (12%) |
| SERENA-4 (NCT04711252) | Recruiting | Phase III randomized, double blind | camizestrant (75 mg daily) + palbociclib (125 mg 3w/ 1w) vs anastrozole (1 mg daily) + palbociclib Men and premenopausal patient receive LHRH agonist in addition to study treatment | 1342 | LABC or mBC | De novo or recurrent ER+/HER2- BC. | N/A | N/A |
| SERENA-6 (NCT04964934) | Ongoing | Phase III randomized, double-blind | camizestrant + CDK4/6i (palbociclib or abemaciclib) vs ongoing treatment with AI (anastrozole or letrozole) + CDK4/6 | 300 | LABC or mBC | ER+/HER2- BC on current 1 L SOC. Detectable ESR1 mutation. | N/A | N/A |
| NCT03455270 part 3 | Active, Recruitment Completed | Phase I Single Group, Open Label | rintodestrant (800 mg daily) + palbociclib (125 mg 3w/ 1w) | 107 | LABC or mBC | women with ER+/HER2- BC | Palbociclib w/ Rintodestrnat CBR of 60% compared to Rintodestrant alone of 28%. ORR 5%(4% WTESR1,6%mESR1),CBR 60%(61% WTESR1,56%mESR1),mPFS 7.4mo | G ≥ 3: neutropenia(53%), leukopenia(18%).All G: neutropenia(90%), leukopenia(45%), anemia(15%),thrombocytopenia(10%),asymptomaticbacteriuria (10%) |
| AMEERA-1 arm 1 part A-B | Active, Not Recruiting | Phase I/ II Randomized, Open Label | amcenestrant (200–600 mg daily) | 136 | LABC or mBC | women with ER+/HER2- BC | ORR 5/46 10.9%, (CBR) of 13/46 (28.3%). ESR1 wild type and mutated ESR1 showed similar CBR (34.6% and 21.1% respectively | No Grade ≥3 TRAE's or clinically significant cardiac/eye toxicities were reported. |
| AMEERA-3 (NCT04059484) | Active, Not Recruiting | Phase II Randomized, Open Label | AMC 400mg WD or Single agent TPC (fulvestrant, aromatase inhibitor, or tamoxifen | 367 | LABC or mBC | postmenopausal women, premenopausal, or men taking GnRH agonist with ER+/HER2- aBC who received <2 prior ET and ≤ 1 prior chemotherapy or ≤ 1 targeted therapy for aBC. | Study did not meet primary objective, PFS per ICR numerically similar between AMC and TPC-PFTS 3.6 vs 3.7 months, HR 1.051 | 0.7% Grade ≥ 3 TRAEs; TRAE’s with AMV vs TPC Grade 1/2: Nausea (14.0% vs 4.1%), vomiting (8.4% vs 1.4%), hot flush (8.4% vs 7.5%), asthenia (7.0% vs 1.4%), fatigue (5.6% vs 6.1%), and injection site pain (0% vs 6.8%); 4.9% |
| AMEERA-1 arm 2-5 | ||||||||
| I-SPY1 EOP (NCT01042379 ) | Recruiting | Phase II Randomized, open label | amcenestrant (200 mg daily) ± abemaciclib/ letrozole for 6 mo | 5000 | early stage BC neoadjuvant | clinical highrisk and molecular lowrisk (MammaPrint® low-risk score) ER+/HER2- BC (≥2.5 cm) | N/A | N/A |
| AMEERA-5 (NCT04478266) | Active, Not recruiting | Phase III Randomized, double blind | amcenestrant (200 mg daily) + palbociclib vs letrozole + palbociclib | 1068 | LABC or mBC | ER+/HER2- BC. ECOG 0–2 | Interim analysis showed negative results and an Independent Data Monitoring Committee found that amcenestrat in combination with palbociclibdid not meet the criteria for continuation when compared to the control arm. | No new safety signals were observed |
| AMEERA-6 ( (NCT05128773) | Terminated | Phase III Randomized, double blind | amcenestrant vs tamoxifen 5 years | 3 | early stage BC adjuvant | stage IIB or III ER+/ HER2± BC undergone surgery and adjuvant RT if indicated. | Study Terminated | Study Termianted |
| EMBER (NCT04188548) | Recruiting | Phase Ia/Ib Randomized, open label. multi-cohort | Imlunestrant (200-1200 mg daily) +/- everolimus, abemaciclib, alpelisib, trastuzumab | 500 | LABC or mBC and other select non-breast cancer | HR+ HER2- BC with 3 or less prior lines of treatment and ER+ endometrial cancer previously treated with platinum therapy | Combination therapy also shows positive antitumor properties with a 12 month PFS in comparison to MONARCH 2 and 3 | Monotherapy demonstrates no dose-dependent toxicities, TEAEs were mostly grade 1-2 (i.e. nausea, fatigue, diarrhea). Combination therapy showed adequate safety profile |
| EMBER-2 (NCT04647487) | Active, Not recruiting | Phase I Randomized, open-label | Imlunestrant | 90 | early stage (I-III) BC neoadjuvant | Post-menopausal women with ER+ HER2- BC | N/A | N/A |
| EMBER-3 (NCT04975308) | Recruiting | Phase III Randomized, open-label | Imlunestrant +/- abemaciclib versus ET (investigator's choice) | 860 | LABC or mBC | ER+ HER2- previously treated with ET | N/A | N/A |
| EMBER-4 (NCT05514054) | Recruiting | Phase III Randomized, open-label | Imlunestrant versus ET (investigator's choice) | 6000 | Early BC with increased risk of recurrence | Patients with ER+ HER2- BC who received 2-5 years of adjuvant ET | N/A | N/A |
| ENZENO (NCT04669587) | Recruiting | Phase I/II Non-randomized, open-label | Borestrant +/- palbociclib | 106 | LABC or mBC | ER+ HER2- BC | N/A | N/A |
| NCT03471663 | Active, Not recruiting | Phase I Randomized, open-label, multi-parts | D-0502 +/- palbociclib | 200 | LABC or mBC | ER+ HER2- BC | Radiological tumor response and CBR observed in both monotherapy and combination therapy | No DLTs |
| NCT04514159 | Ongoing | Phase I/II Open-label, multi-center |
ZN-c5 | 181 | mBC | Postmenopausal patients, adenocarcinoma of the breast ER+ HER2- BC |
N/A | N/A |
Author Contributions
Study conception and design: NN and AD; Draft manuscript preparation: NN, SB, SG, EMG, OM, ST, CF, ROR, AD; Edit and review: NN, SB, SG, EMG, OM, ST, CF, ROR, AD.
Funding
No funding.
Conflicts of Interest
NN: SB, SG, EMG, OM, ST, CF: Has no disclosures. ROR: Advisor for Pfizer. AD: Honoraria for OncLive/MJH Science, Gilead Sciences, AstraZeneca, WebMD/Medscape and research funding form celcuity, Puma Biotechnology.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar]
- Society. AC. Cancer Statistics Center 03/22/23. Available online: http://cancerstatisticscenter.cancer.org.
- Lumachi F, Santeufemia DA, Basso SM. Current medical treatment of estrogen receptor-positive breast cancer. World J. Biol. Chem. 2015, 6, 231. [Google Scholar]
- Alataki A, Dowsett M. Human epidermal growth factor receptor-2 and endocrine resistance in hormone-dependent breast cancer. Endocr. -Relat. Cancer 2022, 29, R105. [Google Scholar] [CrossRef] [PubMed]
- Lu Y, Liu W. Selective estrogen receptor degraders (SERDs): a promising strategy for estrogen receptor positive endocrine-resistant breast cancer. J. Med. Chem. 2020, 63, 15094–114. [Google Scholar] [CrossRef]
- Ferraro E, Walsh EM, Tao JJ, Chandarlapaty S, Jhaveri K. Accelerating drug development in breast cancer: New frontiers for ER inhibition. Cancer Treat. Rev. 2022, 102432. [CrossRef]
- Robertson JF, Llombart-Cussac A, Rolski J, Feltl D, Dewar J, Macpherson E, et al. Activity of fulvestrant 500 mg versus anastrozole 1 mg as first-line treatment for advanced breast cancer: results from the FIRST study. J. Clin. Oncol. 2009, 27, 4530–5. [Google Scholar] [CrossRef]
- Robertson JF, Bondarenko IM, Trishkina E, Dvorkin M, Panasci L, Manikhas A, et al. Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): an international, randomised, double-blind, phase 3 trial. Lancet 2016, 388, 2997–3005. [Google Scholar] [CrossRef]
- Ellis MJ, Llombart-Cussac A, Feltl D, Dewar JA, Jasiówka M, Hewson N, et al. Fulvestrant 500 mg versus anastrozole 1 mg for the first-line treatment of advanced breast cancer: overall survival analysis from the phase II FIRST study. J. Clin. Oncol. 2015, 33, 3781. [Google Scholar] [CrossRef]
- Di Leo A, Jerusalem G, Petruzelka L, Torres R, Bondarenko IN, Khasanov R, et al. Results of the CONFIRM phase III trial comparing fulvestrant 250 mg with fulvestrant 500 mg in postmenopausal women with estrogen receptor-positive advanced breast cancer. J Clin Oncol 2010, 28, 4594–600. [Google Scholar] [CrossRef]
- Valachis A, Mauri D, Polyzos NP, Mavroudis D, Georgoulias V, Casazza G. Fulvestrant in the treatment of advanced breast cancer: a systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Oncol. /Hematol. 2010, 73, 220–7. [Google Scholar] [CrossRef]
- Garcia-Fructuoso I, Gomez-Bravo R, Schettini F. Integrating new oral selective oestrogen receptor degraders in the breast cancer treatment. Curr. Opin. Oncol. 2022, 34, 635–42. [Google Scholar] [CrossRef]
- Bardia A, Kaklamani V, Wilks S, Weise A, Richards D, Harb W, et al. Phase I study of elacestrant (RAD1901), a novel selective estrogen receptor degrader, in ER-positive, HER2-negative advanced breast cancer. J. Clin. Oncol. 2021, 39, 1360. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli M, Rugo HS, Im S-A, Slamon DJ, Harbeck N, Bondarenko I, et al. Overall Survival With Palbociclib And Fulvestrant in Women With HR+/HER2-ABC: Updated Exploratory Analyses of PALOMA-3, a Double-Blind, Phase 3 Randomized Study 2022.
- Hamilton E, Cortes J, Ozyilkan O, Chen S-C, Petrakova K, Manikhas A, et al. nextMONARCH: abemaciclib monotherapy or combined with tamoxifen for metastatic breast cancer. Clin. Breast Cancer 2021, 21, 181–90.e2. [Google Scholar] [CrossRef] [PubMed]
- Slamon DJ, Neven P, Chia S, Fasching PA, De Laurentiis M, Im S-A, et al. Overall survival with ribociclib plus fulvestrant in advanced breast cancer. New Engl. J. Med. 2020, 382, 514–24. [Google Scholar] [CrossRef] [PubMed]
- Turner NC, Swift C, Kilburn L, Fribbens C, Beaney M, Garcia-Murillas I, et al. ESR1 mutations and overall survival on fulvestrant versus exemestane in advanced hormone receptor–positive breast cancer: a combined analysis of the phase III SoFEA and EFECT trials. Clin. Cancer Res. 2020, 26, 5172–7. [Google Scholar] [CrossRef] [PubMed]
- Lindeman GJ, Fernando TM, Bowen R, Jerzak KJ, Song X, Decker T, et al. VERONICA: Randomized Phase II Study of Fulvestrant and Venetoclax in ER-Positive Metastatic Breast Cancer Post-CDK4/6 Inhibitors–Efficacy, Safety, and Biomarker Results. Clin. Cancer Res. 2022, 28, 3256–67. [Google Scholar] [CrossRef] [PubMed]
- FDA approves elacestrant for ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-elacestrant-er-positive-her2-negative-esr1-mutated-advanced-or-metastatic-breast-cancer.
- Jager A, de Vries EG, der Houven van Oordt C, Neven P, Venema CM, Glaudemans AW, et al. A phase 1b study evaluating the effect of elacestrant treatment on estrogen receptor availability and estradiol binding to the estrogen receptor in metastatic breast cancer lesions using 18F-FES PET/CT imaging. Breast Cancer Res. 2020, 22, 1–11. [Google Scholar]
- Elacestrant in Preoperative Setting, a Window of Opportunity Study (ELIPSE) - Full Text View - ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04797728.
- Vidal M, Pascual T, Falato C, Sanchez-Bayona R, Muñoz M, Cerbrecos I, et al. Abstract PD13-01: PD13-01 Elacestrant in postmenopausal women with estrogen receptor positive and HER2-negative early breast cancer: primary efficacy and safety analysis of the preoperative, window of opportunity SOLTI-1905-ELIPSE trial. Cancer Res. 2023, 83 (5_Supplement), PD13-01-PD13-01.
- Bardia A, Bidard F, Neven P, Streich G, Montero A, Forget F, et al. EMERALD phase 3 trial of elacestrant versus standard of care endocrine therapy in patients with ER+/HER2-metastatic breast cancer: updated results by duration of prior CDK4/6i in metastatic setting. Proceedings of the SABC 2022.
- Open-Label Umbrella Study to Evaluate Safety and Efficacy of Elacestrant In Various Combination In Patients With Metastatic Breast Cancer (ELEVATE). ClinicalTrials.gov identifier: NCT05563220. Updated May 26, 2023. Available online: https://clinicaltrials.gov/ct2/show/NCT05563220.
- Phase Ib/II Trial of Abemaciclib and Elacestrant in Patients with Brain Metastasis Due to HR+/Her2- Breast Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT04791384.
- Hamilton EP, Oliveira M, Banerji U, Hernando C, Garcia-Corbacho J, Armstrong A, et al. A phase I dose escalation and expansion study of the next generation oral SERD AZD9833 in women with ER-positive, HER2-negative advanced breast cancer. Am. Soc. Clin. Oncol. 2020. [CrossRef]
- Oliveira M, Hamilton EP, Incorvati J, Bermejo de la Heras B, Calvo E, García-Corbacho J, et al. Serena-1: Updated analyses from a phase 1 study (parts C/D) of the next-generation oral SERD camizestrant (AZD9833) in combination with palbociclib, in women with ER-positive, HER2-negative advanced breast cancer. Am. Soc. Clin. Oncol. 2022. [CrossRef]
- Oliveira M, Pominchuk D, Nowecki Z, Hamilton E, Kulyaba Y, Andabekov T, et al., editors. Camizestrant, a next generation oral SERD vs fulvestrant in post-menopausal women with advanced ER-positive HER2-negative breast cancer: results of the randomized, multi-dose phase 2 SERENA-2 trial 2022 San Antonio Breast Cancer Symposium; 2022.
- Robertson JF, Moppett I, Rocha JEB, Dzagnidze G, Harding J, Klinowska T, et al. Abstract OT-09-05: a randomized, pre-surgical study to investigate the biological effects of AZD9833 doses in women with ER-positive HER2-negative primary breast cancer (SERENA-3). Cancer Res. 2021, 81 (4_Supplement), OT-09-5-OT--5.
- André F, Im S-A, Neven P, Baird RD, Ettl J, Goetz MP, et al. Abstract OT2-11-06: SERENA-4: A Phase III comparison of AZD9833 (camizestrant) plus palbociclib, versus anastrozole plus palbociclib, for patients with ER-positive/HER2-negative advanced breast cancer who have not previously received systemic treatment for advanced disease. Cancer Res. 2022, 82 (4_Supplement), OT2-11-06-OT2-11-06. [CrossRef]
- Bidard F-C, Kalinsky K, Cristofanilli M, Bianchini G, Chia SK, Janni W, et al. Abstract OT2-11-05: SERENA-6: A Phase III study to assess the efficacy and safety of AZD9833 (camizestrant) compared with aromatase inhibitors when given in combination with palbociclib or abemaciclib in patients with HR+/HER2-metastatic breast cancer with detectable ESR1 m who have not experienced disease progression on first-line therapy. Cancer Res. 2022, 82 (4_Supplement), OT2-11-05-OT2-11-05. [Google Scholar]
- Lim E, Jhaveri KL, Perez-Fidalgo JA, Bellet M, Boni V, Perez Garcia JM, et al. A phase Ib study to evaluate the oral selective estrogen receptor degrader GDC-9545 alone or combined with palbociclib in metastatic ER-positive HER2-negative breast cancer. Am. Soc. Clin. Oncol. 2020. [CrossRef]
- A Study of GDC-9545 Alone or in Combination with Palbociclib and/or Luteinizing Hormone-Releasing Hormone (LHRH) Agonist in Locally Advanced or Metastatic Estrogen Receptor. Available online: https://clinicaltrials.gov/ct2/show/NCT03332797.
- Jhaveri KL, Boni V, Sohn J, Villanueva-Vásquez R, Bardia A, Schmid P, et al. Safety and activity of single-agent giredestrant (GDC-9545) from a phase Ia/b study in patients (pts) with estrogen receptor-positive (ER+), HER2-negative locally advanced/metastatic breast cancer (LA/mBC). J Clin Oncol 2021, 39 (15_suppl), 1017. [Google Scholar]
- Turner NC, Loi S, Moore HM, Chang C-W, Eng-Wong J, Bardia A, et al. Abstract PD13-07: activity and biomarker analyses from a phase Ia/b study of giredestrant (GDC-9545, G) with or without palbociclib (palbo) in patients with estrogen receptor-positive, HER2-negative locally advanced/metastatic breast cancer (ER+/HER2-LA/mBC). Cancer Res. 2022, 82 (4_Supplement), PD13-07-PD13-07. [Google Scholar] [CrossRef]
- Martin M, Lim E, Chavez Mac Gregor M, Shivhare M, Ross G, Patre M, et al. acelERA Breast Cancer (BC): Phase II study evaluating efficacy and safety of giredestrant (GDC-9545) versus physician’s choice of endocrine monotherapy in patients (pts) with estrogen receptor-positive, HER2-negative (ER+/HER2-) locally advanced or metastatic breast cancer (LA/mBC). Wolters Kluwer Health 2021. [CrossRef]
- Jimenez MM, Lim E, Mac Gregor MC, Bardia A, Wu J, Zhang Q, et al. 211MO Giredestrant (GDC-9545) vs physician choice of endocrine monotherapy (PCET) in patients (pts) with ER+, HER2–locally advanced/metastatic breast cancer (LA/mBC): primary analysis of the phase II, randomised, open-label acelERA BC study. Ann. Oncol. 2022, 33, S633–S4. [Google Scholar] [CrossRef]
- A Study to Evaluate the Efficacy, Safety, and Pharmacokinetics of Giredestrant Plus Palbociclib Compared with Anastrozole Plus Palbociclib for Postmenopausal Women with Estrogen Receptor-Positive and HER2-Negative Untreated Early Breast Cancer (coopERA Breast Cancer).
- Fasching PA, Bardia A, Quiroga V, Park YH, Blancas I, Alonso JL, et al. Neoadjuvant giredestrant (GDC-9545) plus palbociclib (P) versus anastrozole (A) plus P in postmenopausal women with estrogen receptor–positive, HER2-negative, untreated early breast cancer (ER+/HER2–eBC): Final analysis of the randomized, open-label, international phase 2 coopERA BC study. Am. Soc. Clin. Oncol. 2022. [CrossRef]
- A Study Evaluating the Efficacy and Safety of Giredestrant Plus Everolimus Compared with Exemestane Plus Everolimus in Participants with Estrogen Receptor-Positive, HER2-Negative, Locally Advanced or Metastatic Breast Cancer (evERA Breast Cancer).
- A Study Evaluating the Efficacy and Safety of Adjuvant Giredestrant Compared with Physician's Choice of Adjuvant Endocrine Monotherapy in Participants with Estrogen Receptor-Positive, HER2-Negative Early Breast Cancer (lidERA Breast Cancer).
- Shomali M, Cheng J, Sun F, Koundinya M, Guo Z, Hebert AT, et al. SAR439859, a novel selective estrogen receptor degrader (SERD), demonstrates effective and broad antitumor activity in wild-type and mutant ER-positive breast cancer models. Mol. Cancer Ther. 2021, 20, 250–62. [Google Scholar] [CrossRef] [PubMed]
- Bardia A, Chandarlapaty S, Linden HM, Ulaner GA, Gosselin A, Cartot-Cotton S, et al. AMEERA-1 phase 1/2 study of amcenestrant, SAR439859, in postmenopausal women with ER-positive/HER2-negative advanced breast cancer. Nat. Commun. 2022, 13, 4116. [Google Scholar] [CrossRef]
- Tolaney S, Chan A, Petrakova K, Delaloge S, Campone M, Iwata H, et al. 212MO AMEERA-3, a phase II study of amcenestrant (AMC) versus endocrine treatment of physician’s choice (TPC) in patients (pts) with endocrine-resistant ER+/HER2− advanced breast cancer (aBC). Ann. Oncol. 2022, 33, S634–S5. [Google Scholar] [CrossRef]
- Chien AJ, Kalinsky KM, Molina-Vega J, Mukhtar R, Giridhar K, Olopade OI, et al. Abstract OT1-10-02: i-SPY2 endocrine optimization protocol (EOP): a pilot neoadjuvant endocrine therapy study with amcenestrant as monotherapy or in combination with abemacicilib or letrozole in molecularly selected HR+/HER2-clinical stage 2/3 breast cancer. Cancer Res. 2022, 82 (4_Supplement), OT1-10-02-OT1-10-02. [Google Scholar]
- Campone M, Dong Y, Ling B, Wang L, Herold CI. AMEERA-4: A preoperative window-of-opportunity (WOO) study to assess the pharmacodynamic (PD) activity of amcenestrant or letrozole in postmenopausal patients with ER+/HER2− primary breast cancer. Am. Soc. Clin. Oncol. 2022. [CrossRef]
- Bardia A, Cortes J, Hurvitz SA, Delaloge S, Iwata H, Shao Z-M, et al. AMEERA-5: a randomized, double-blind phase 3 study of amcenestrant plus palbociclib versus letrozole plus palbociclib for previously untreated ER+/HER2–advanced breast cancer. Ther. Adv. Med. Oncol. 2022, 14, 17588359221083956. [Google Scholar]
- A Study of LY3484356 in Participants with Advanced or Metastatic Breast Cancer or Endometrial Cancer (EMBER). Available online: https://clinicaltrials.gov/ct2/show/NCT04188548.
- Jhaveri KL, Lim E, Hamilton EP, Saura C, Meniawy T, Jeselsohn R, et al. A first-in-human phase 1a/b trial of LY3484356, an oral selective estrogen receptor (ER) degrader (SERD) in ER+ advanced breast cancer (aBC) and endometrial endometrioid cancer (EEC): Results from the EMBER study. Wolters Kluwer Health; 2021.
- Jhaveri K, Wang H-C, Ma C, Lim E, Tao JJ, Manso L, et al. Abstract PD13-12: PD13-12 Imlunestrant, an oral selective estrogen receptor degrader, in combination with abemaciclib with or without an aromatase inhibitor, in estrogen receptor-positive advanced breast cancer: Results from the phase 1a/b EMBER study. Cancer Res. 2023, 83 (5_Supplement), PD13-2-PD-2. [CrossRef]
- A Study of LY3484356 in Women with Breast Cancer Before Having Surgery (EMBER-2) - Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT04647487.
- A Study of Imlunestrant, Investigator's Choice of Endocrine Therapy, and Imlunestrant Plus Abemaciclib in Participants With ER+, HER2- Advanced Breast Cancer (EMBER-3) - Full Text View.
- A Study of Imlunestrant Versus Standard Endocrine Therapy in Participants with Early Breast Cancer (EMBER-4). Available online: https://clinicaltrials.gov/ct2/show/NCT05514054.
- Aftimos P, Neven P, Pegram M, van Oordt CWM-vdH, Dees EC, Schröder C, et al. Abstract PS12-04: rintodestrant (G1T48), an oral selective estrogen receptor degrader in ER+/HER2-locally advanced or metastatic breast cancer: updated phase 1 results and dose selection. Cancer Res. 2021, 81 (4_Supplement), PS12-04-PS12-04.
- Aftimos P, Maglakelidze M, Glaudemans AW, Hamilton E, Chap L, de Vries E, et al. Abstract PD8-07: Pharmacodynamic analysis from a phase 1 study of rintodestrant (G1T48), an oral selective estrogen receptor degrader, in ER+/HER2-locally advanced or metastatic breast cancer. Cancer Res. 2021, 81 (4_Supplement), PD8-07-PD8-.
- Robertson JF, Evans A, Henschen S, Kirwan C, Jahan A, Kenny L, et al. Abstract P6-04-01: A pre-surgical, window of opportunity study comparing the novel oral SERD AZD9496 with fulvestrant in patients with newly diagnosed ER+ HER2-primary breast cancer. Cancer Res. 2020, 80 (4_Supplement), P6-04-1-P6--1.
- Weir HM, Bradbury RH, Lawson M, Rabow AA, Buttar D, Callis RJ, et al. AZD9496: An Oral Estrogen Receptor Inhibitor That Blocks the Growth of ER-Positive and ESR1-Mutant Breast Tumors in Preclinical ModelsPharmacology of SERD Inhibitor in Breast Cancer Models. Cancer Res. 2016, 76, 3307–18. [Google Scholar] [CrossRef] [PubMed]
- ER+/HER2- Locally Advanced or Metastatic Breast Cancer (ENZENO Study) (ENZENO).
- A First-in-Human Study of D-0502 Alone and in Combination with Palbociclib in Women with Advanced or Metastatic ER-Positive and HER2-Negative Breast Cancer.
- Osborne C, Richards DA, Wilks ST, Diab S, Juric D, Lathrop K, et al. Abstract PS11-26: a phase 1 study of D-0502, an orally bioavailable SERD, for advanced or metastatic HR-positive and HER2-negative breast cancer. Cancer Res. 2021, 81 (4_Supplement), PS11-26-PS11-26. [CrossRef]
- Samatar AA, Li J, Hegde S, Huang P, Ma J, Bunker K, et al. Discovery of ZN-c5, a novel potent and oral selective estrogen receptor degrader. Cancer Res. 2020, 80 (16_Supplement), 4373.
- Keogh G, Papish S, Piskorski W, Ulanska M, Jackson B, Suster M, et al. 564TiP A phase Ib dose-escalation study of ZN-c5, an oral selective estrogen receptor degrader (SERD), in combination with abemaciclib in patients with advanced estrogen receptor (ER)+/HER2-breast cancer. Ann. Oncol. 2021, 32, S618–S9. [Google Scholar] [CrossRef]
- Abramson V, Linden H, Crew K, Mortimer J, Alidzanovic J, Nangia J, et al. 565TiP A phase I/II dose-escalation and expansion study of ZN-c5, an oral selective estrogen receptor degrader (SERD), as monotherapy and in combination with palbociclib in patients with advanced estrogen receptor (ER)+/HER2-breast cancer. Ann. Oncol. 2021, 32, S619. [Google Scholar] [CrossRef]
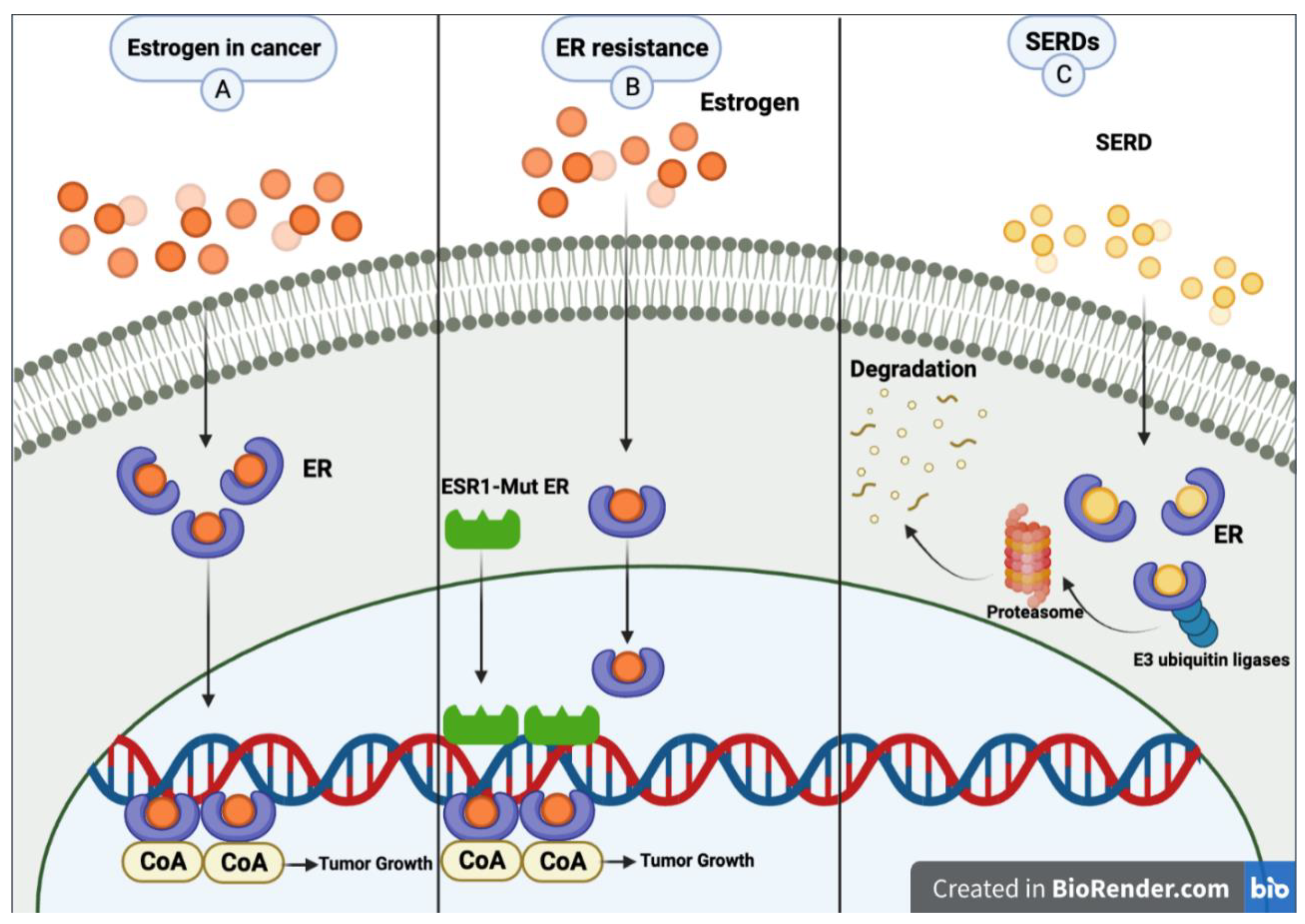
Figure 1.
Common pathway for estrogen in breast cancer. B. Metastatic breast cancer patients may experience resistance mechanisms to endocrine therapy. A mutation of estrogen receptor 1 (ESR1) causes constant ER activity and enhanced transcription of ER-dependent genes without hormones, resulting in resistance to estrogen deprivation and aromatase inhibitor therapy. C. SERDs bind to the estrogen receptor, then E3 ubiquitin ligases and ubiquitinate the ER, marking it for degradation by the proteasome. The proteasome eventually degrades the ubiquitinated ER. Created with BioRender.com.
Figure 1.
Common pathway for estrogen in breast cancer. B. Metastatic breast cancer patients may experience resistance mechanisms to endocrine therapy. A mutation of estrogen receptor 1 (ESR1) causes constant ER activity and enhanced transcription of ER-dependent genes without hormones, resulting in resistance to estrogen deprivation and aromatase inhibitor therapy. C. SERDs bind to the estrogen receptor, then E3 ubiquitin ligases and ubiquitinate the ER, marking it for degradation by the proteasome. The proteasome eventually degrades the ubiquitinated ER. Created with BioRender.com.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



