
Submitted:
03 October 2023
Posted:
04 October 2023
Read the latest preprint version here
Abstract
Obesity in adolescents combined with the increased exposure time to electronic devices, enhances a sedentary lifestyle and is linked to the risk of developing musculoskeletal injuries. The aim of this study was to identify possible correlations between anthropometric characteristics, body composition, exposure time to electronic devices or screen time (ST) and physical activity (PA) level along with muscle power and dynamic knee valgus (DKV) in young athletes to avoid future injuries. A total of 125 adolescent basketball athletes (66.4% boys), 12 to 17 years old (13.94±1.58 years) participated. Anthropometric and demographic characteristics were recorded. PA level was assessed through IPAQ and ST through a single question from the HELENA study. The Counter Movement Jump test was used for the evaluation of the lower limb muscle power, while the Single Leg Drop Jump test was used for the evaluation of the dynamic knee valgus via two-dimensional (2D) kinematic analysis. The Pearson index showed a statistically significant positive correlation between muscle power and height (r=0.788, p<0.001), while the Spearman index showed a smaller but equally statistically significant positive correlation with BMI (rs =0.651, p<0.001) and age (rs=0.579, p<0.001). The ST (rs= -0.194, p=0.03) showed a weak negative correlation with DKV, while PA (r=0.85, p<0.001) showed a high, statistically significant, positive correlation. The anthropometric characteristics of adolescent athletes can determine their ability to produce muscle power. A high level of physical activity could play a key role in compensating and thus reducing the negative effects of high exposure to screen time on the dynamic knee valgus
Keywords:
Adolescents
; Physical Activity
; Muscle Power
; Handgrip Strength
; Dynamic Knee Val-28 gus
; Screen Time
; Movement Behavior
; BMI
; body mass index
; Single Leg Drop Jump Test
1. Introduction
Adolescents normally dispose of a high variety of body movements that are constantly enriched in time.[1] However, the adopted modern style of living along with the recent COVID-19 quarantine, have significantly affected adolescents’ motor development. The adolescents’ preference for sedentary activities (computer games, cellphone use or watching TV) over physical or sporting activities has resulted in them being more inactive and passive.[1,2]
It needs to be mentioned though that a sedentary lifestyle during adolescence highly predisposes to an inactive life during adulthood, consequently affecting their level of health.[3,4,5] Inactivity is strongly associated with the onset of obesity from an early age. Nowadays obesity is reaching epidemic proportions in children and adolescents.[5,6] Excess body weight and obesity are negatively associated with fitness parameters that are significant indicators of overall health status, such as cardiorespiratory fitness and muscle power.[3,7,8,9,10]
Existing research data also reports that adolescents with low lower limb power are highly predisposed to an increased risk of cardiovascular disease, musculoskeletal injuries, and osteoarthritis in adulthood.[11,12] Additionally, overweight and obese adolescents, particularly those involved in sports, appear to be more prone to musculoskeletal injuries, mainly injuries of the lower extremities and especially the knee.[13,14,15]
Among adolescents, the injuries with the highest incidence are partial or total rupture of the anterior cruciate ligament (ACL), anterior knee pain syndrome (AKPS) and patellar tendinopathy. The main triggering mechanism for the aforementioned injuries appears to be the dynamic knee valgus (DKV).[16,17,18,19,20]
Lack of physical activity (PA) level or an increased sedentary life seem to be associated with the overall health status and the occurrence of knee injuries. Based on the aforementioned fact this study aimed to search for and, further, identify the possible correlations between anthropometric characteristics, obesity, physical activity and exposure time to electronic devices with muscle power and dynamic knee valgus, to adjust them in the future for performance enhancement and knee injury prevention.
2. Materials and Methods
Study Design
The study protocol was approved by the Ethics Committee of the Department of Physiotherapy at the University of Thessaly (1083/21-10-2022). The study was performed following the principles in the Declaration of Helsinki; thus, consistent with the value of respect for the volunteers who would participate. Informed consent was obtained from all subjects involved in the study and written informed consent was obtained from all the participants to publish this paper.
Sample
The sample consisted of 177 adolescent athletes (73% boys, 27% girls) from two basketball academies originating from two cities in Central Greece. Participants’ eligibility criteria were the following a) aged between 12 and 17 years (adolescence phase) [21], b) absence of lower limb injury within the last 3 months or other comorbidity precluding exercise implementation (e.g., neurological, or cognitive conditions), c) parents’ signed consent information sheet. The sample size was calculated using the G*Power 3.1.9.4 program with a 95% confidence level and a significance level of 5% or 0.05. After adjusting for potential dropouts (estimated attrition rate ≤10%), a minimum sample of 112 adolescents was required
Data Collection
All measurements and data recording procedures were performed by 3 l independent physiotherapists. Measurement data were initially recorded on a laptop and then backed up to an external hard drive to be processed and evaluated by the trial investigator after the completion of the assessment period. Equipment
The SOEHNLE 5003 precision electronic ultrasonic stadiometer, which covers a measuring range from 30cm to 240cm, was used to calculate the participants’ height. A precision electronic weighing scale was used to measure weight in kilograms (kg). Recorded height and weight data were further used for the calculation of the BMI.[22,23]
The International Physical Activity Questionnaire (IPAQ) records and assesses daily and weekly PA levels. IPAQ demonstrates high reliability and validity values.[24] In this study, PA was assessed through the Greek short version of the IPAQ (7 questions) that presents adequate reliability and validity scores in adolescents.[25,26]
A single question from the HELENA study was used to record the time of exposure on screen-based electronic devices.[27,28] Its reliability (r > 0.8) is adequate.[28]
In the present study, the program chosen to perform the two-dimensional analysis was the KINOVEA. The KINOVEA software is a valid and reliable instrument, which provides accurate measurements for the assessment of the height of the vertical jump and the kinematic analysis of the dynamic knee valgus.[29,30] The potentiality of Kinovea to thoroughly evaluate an athlete’s sports performance and overall health status is well documented.[31,32]
A tripod, a camera (Go Pro, 4K, 30fps), 5 reflective markers, and a 30cm height box were used as data collector tools for the Counter Movement Jump test and the Single Leg Drop Jump. These tools are affordable and easy to find and use, thus ideal for wide use. Additionally, the reliability and validity of these tools have also been tested in healthy adolescents.[31,32,33,34]
Assessment
For those who consented to participation, both the baseline assessment- including anthropometric (height, weight) and demographic data- and the study measurements were conducted once on the basketball courts of each participating team (Figure 1).
Height was measured with the participants being barefoot with their feet touching each other at the heels and their body in an upright position (Figure 2). Weight measurement was conducted with the adolescent athletes stepping on the scale barefoot. (Figure 2).
The calculation of Body Mass Index (BMI) was based on the international system units (SI) with the formula: Body Mass Index = Weight (kg) / Height2 (m2) and then given as a z-score in three categories: normal/overweight/obese.[22,23,35]
Based on the responses on the IPAQ, a numerical score for weekly PA was generated, representing MET-minutes/week, which was translated into 3 categories, low/moderate/high.[36]
The question used from the HELENA study to record time spent using screen-based electronic devices was: “How much time do you spend on average each day watching television, watching videos, or playing games on a computer, games console, mobile phone or tablet. The following responses were picked as possible answers: 0) none, 1) 0–30 min, 2) 30–60 min, 3) 1–2 hours, 4) 2–4 hours, and 5) > 4 hours. According to their answers, the participants were categorized into: “low” (<2 hours per day), “high” (2-4 hours per day), and ‘very high’ (>4 hours per day) based on the international guidelines for limiting the total time spent on e-use screen-based devices for children and adolescents.[27,28,37,38]
Procedures
After appropriate warming up, a maximum vertical jump and a single leg drop jump test were conducted to evaluate the lower limb power the dynamic knee valgus respectively.
Prior to tests (countermovement jump test and single leg drop jump), reflective markers were placed on each participant as reference points. These points were the anterior superior iliac spine, the medial and lateral femoral condyle, and the medial and lateral malleolus on the dominant leg (Figure 3).[29] Based on each participant’s choice of kick-leg to a ball, the dominant limb was determined [29,37]
Assessment
The two-dimensional (2D) analysis program KINOVEA was used to record the maximum vertical jump (CMJ) and the single-leg drop jump. For the CMJ, each participant was allowed to perform two jumps, with a 1-minute rest between jumps. The best-performing jump was selected for analysis through the 2D analysis with the Kinovea program.[30]
The equation used to predict the power of the lower limbs through the height of the vertical jump and each participant’s weight, was that of Mahar et al. (2022), as it showed the highest accuracy rates and reliability (R=.93, R2=.87) among all the equations that exist so far in the literature. The equation was as follows:
VJ Power (W) = -1354.820 + (VJ Height * 35.455) + (Body mass * 43.942).[33]
For the single-leg drop jump test, each participant jumped off a box and landed on their dominant leg. A single leg jump to the possible maximum height was subsequently performed that ended by re-landing on the same leg and remaining still on it for 2 seconds.[29]
To calculate the knee valgus angle, two axes were considered. The first axis was the line from the anterior superior iliac spine to the midpoint of the distance between the two knee reflective markers, corresponding to the femur. The second axis was from the midpoint of the distance between the two knee reflective markers to the midpoint of the distance between the two ankle reflective markers, corresponding to the tibia (Figure 2).[29] The larger the angle formed by these two aforementioned axes, the smaller the dynamic valgus angle of the knee. This angle is referred below as the knee landing angle (KLA) (Figure 3).
Statistics
Statistical Package for Social Sciences (SPSS) V.29.0 was used for data analyses. Calculations were also performed through Microsoft Office Excel 2013. The significance level was set at p=0.05.
Anthropometric factors (gender, weight, height, BMI), PA, as well as ST, were defined as independent variables. The lower limb muscle power and the dynamic knee valgus were defined as the dependent variables.
Descriptive statistics was performed to obtain the means of the above variables as well as the standard deviation. Data normality was checked via the Kolmogorov-Smirnov and Shapiro-Wilk tests.
Analysis of Variance was performed using the Anova Post-Hoc test, between the three groups of BMI based on z-score and dependent variables, as well as the three groups of ST, and the three groups of PA level. Finally, Multiple Linear Regression was used to assess the ability of the variables selected to predict muscle power.
3. Results
125 adolescents participated in the study (83 boys and 42 girls). Descriptive analysis revealed an average participant age of 13.94±1.58 years, height of 1.66±0.1 m an average weight of 62.77±14.26 kg and an average BMI of 22.53±3.8 kg/m2. Descriptive statistics is presented in Table 1.
The lower limb muscle power data follow a normal distribution for both boys (p=0.2) and girls (p=0.931), while the KLA data follow a normal distribution for boys (p=0.05) but do not follow a normal distribution for girls (p=0.019). There was no statistically significant difference between genders for a) BMI, b) Screen Time and c) DKV[ boys: Mean = 163.8± 8.1 degrees; girls: Mean = 164.3± 7.2 degrees, t = -0.28, p = 0.272]. On the contrary, a significant statistical difference between boys and girls was revealed for height, weight and muscle power [boys: M = 2808.6 ±780.8 Watts, girls: M = 2339.3 ±456 Watts; t = 3.59, p < 0.001 (two-tailed)] variables.
Specifically, in terms of dependent variables, there is a significant statistical difference in muscle power between boys (Mean = 2808.6 ±780.8 Watts) and girls (Mean = 2339.3 ±456 Watts); t = 3.59, p < 0.001 (two-tailed) (Table 4.5). The magnitude of the difference in mean for muscle power (Mean difference = 517.1; -95% CI = 210.7 to 727.8 Watts) was 0.68 (large size effect) In terms of the dynamic knee valgus, there was no statistically significant difference between boys and girls.
The one-way ANOVA-Post Hoc Test showed a statistically significant difference (p<0.001) between adolescents of normal weight and overweight, and those of normal weight and obese: F=14.03, p<0.001 regarding the BMI groups and the muscle power (Table 2). The KLA showed no statistically significant difference between adolescents with normal BMI and both overweight and obese children: F=0.125, p=0.88 (Table 2).
Muscle power showed a statistically significant difference (p=0.037) between adolescents with low (<2 hours per day) ST compared with those with very high (>4 hours per day) ST: F=3.39, p=0.037 (Table 3). The DKV showed a statistically significant difference between adolescents with low ST and those with high ST: F=4.42, p=0.014 (Table 3).
None of the adolescents had a low level of PA. Muscle power showed that there was no statistically significant difference (p=0.456) between adolescents who had moderate PA with those who had a high PA level [F=0.55, p=0.456]. The DKV showed a statistically significant difference between adolescents with high PA and those with moderate PA [F=257.73, p<0.001].
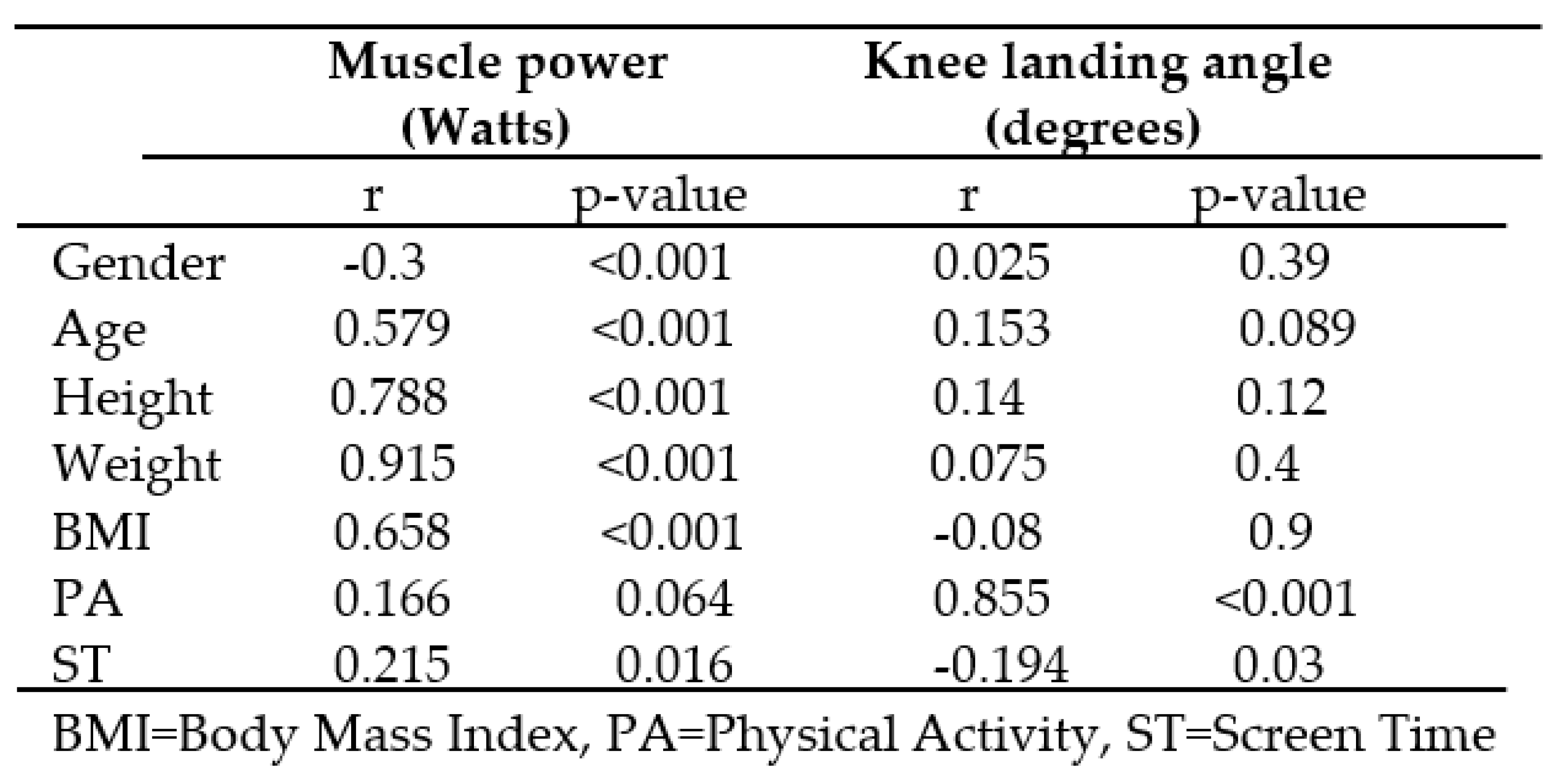
Gender, age, height, weight, BMI, and Screen Time had a statistically significant positive correlation with lower limb muscle power (Table 5). Through the categorization of BMI based on z-score, it appears that there was a statistically significant positive correlation with muscle power.
The regression analysis showed that gender, age, height, and BMI were included in the final model. From that model, 90% of lower limb muscle power can be predicted from the independent variables: gender, age, height and BMI and the predictive equation was:
Muscle Power (Watts) = -6581,45 – (206,7*Gender) + (79,3*Age-years) + (3706,69*Height-m) + (99,47*BMI-kg/m2).
PA level had a statistically significant positive correlation with the KLA, in contrast with the time of exposure to electronic devices with a screen, which showed a statistically significant negative correlation with the KLA.
4. Discussion
The present study aimed to investigate the possible correlations between the anthropometric characteristics, the PA levels and the ST with the lower limb muscle power and dynamic knee valgus in adolescent basketball athletes. The study involved adolescents residing in Greece, which makes it perhaps one of the first studies nationwide that addresses the prevention of musculoskeletal injuries in this country.
Based on the results, it appears that anthropometric characteristics show a high, positive, statistically significant correlation with lower limb muscle power. The data of the existing literature seem to agree with these results, as these variables increase linearly until the age of 16 for both genders.[39,40]
In this study, it appears that anthropometric characteristics show a non-statistically significant correlation with dynamic knee valgus angle. This finding is in contrast to that reported in existing literature, where gender (particularly the female one) is an important factor. More specifically, females, due to their body characteristics, present a higher static and dynamic knee valgus.[16,41,42,43]
However, the sample of the present study consisted of adolescents who were basketball athletes who practiced regularly to a great extent. Many basketball movements include patterns of DKV; thus, basketball players may have become familiarized with them; explaining the lack of correlation between anthropometric characteristics and DKV reported by this study.[14]
The correlation between ST and muscle power is positive but low. The fact that the study sample consisted of adolescent athletes, which predisposes them to a rather higher PA level than non-athlete adolescents, could explain the above low correlation. PA and ST are recognized as lifestyle behaviors, and their impact on different aspects of the health status is –up to now- under-explored.[6,44] Though, it needs to be mentioned that the results of this study indicate that the PA could outweigh the negative consequences of screen time on lower limb muscle power.
Furthermore, screen time appears to have a negative effect, but to a minor extent, on KLA, which means that adolescents with a higher ST also have a greater dynamic knee valgus angle. This means that inactivity and sedentary lifestyle through increased exposure to screen-based electronic devices are even to a small extent a predisposed factor in increased dynamic knee valgus and possible future injury. These results are in agreement with existing research; however, it should be noted that in these studies the sample did not consist of adolescent athletes.[16,45]
On the other hand, PA level shows a very high and positive, statistically significant correlation with knee landing angle. Thus, the higher an adolescent’s PA level is, the greater the landing knee angle in the uni pedal landing after a jump, hence the lower the dynamic knee valgus; thus participants with a high level of PA are less likely to experience an injury due to an increased dynamic knee valgus.
Until now, only two studies have investigated the relationship between PA and DKVA. A study, addressing participants with a reconstructed ACL, reports that the better the PA level of their participants, the lower the DKVA, however, their sample consisted of individuals with a reconstructed ACL.[46] Furthermore, a systematic review evaluating factors associated with ACL injury among the general population (and not only adolescents), reported that the level of PA negatively influences dynamic knee valgus, i.e. the better the PA level, the lower the dynamic knee valgus.[41]
Study Limitation
The heterogeneity between the sexes was the primary limitation of this study since the boys were almost twice as many as the girls, which could affect the generalization of the study results. Subjectively assessed PA and ST results through questionnaires may have led to an over/underestimation of the PA and ST levels. Additionally, the choice of a 2D analysis to a 3D analysis may have prevented the thorough assessment of the testing structures and the landing components.
5. Conclusions
The anthropometric characteristics of adolescent athletes can determine their ability to produce muscle power. A high level of physical activity could play a key role in compensating and thus reducing the negative effects of high exposure to screen time on the dynamic knee valgus. However, further research is needed in larger and more population-representative samples. Furthermore, more longitudinal studies are suggested that would assess the correlation of muscle power and dynamic knee valgus in Greek athletes throughout their careers.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, S.A.., K.E. and P.G..; methodology, S.A., and P.G..; validation, S.A., K.E., and P.G.; formal analysis, S.A., G.P., and A.V.; writing—original draft preparation, S.A.; writing—review and editing, G.P. and A.V.; supervision, P.G.; project administration, P.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Prior to the study, the study protocol was approved by the Ethics Committee of the Department of Physiotherapy at the University of Thessaly (1083/21-10-2022). The study was performed following the principles in the Declaration of Helsinki; thus, consistent with the value of respect for the volunteers who would participate.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from all the participants to publish this paper.
Data Availability Statement
Data will be available upon request.
Conflicts of Interest
The authors declare that there is no conflict of interest.
References
- Carriedo A, Cecchini J, Fernández-Álvarez L, González C. Physical Activity and Physical Fitness in Adolescents after the COVID-19 Lockdown and One Year Afterward. Int J Environ Res Public Health 2022, 19, 14660. [Google Scholar] [CrossRef] [PubMed]
- Dahlgren A, Sjöblom L, Eke H, Bonn SE, Trolle Y, Lagerros. Screen time and physical activity in children and adolescents aged 10–15 years. PLoS One 2021, 16. [Google Scholar] [CrossRef]
- Gaya AR, Dias AF, Lemes VB, Gonçalves JC, Marques PA, Guedes G, et al. Aggregation of risk indicators to cardiometabolic and musculoskeletal health in Brazilian adolescents in the periods 2008/09 and 2013/14. J Pediatr (Rio J) 2018, 94, 177–183. [Google Scholar] [CrossRef]
- Lemes VB, Gaya ACA, Gaya AR. Comparison of 24-h movement behavior, health-related quality of life, and waist to height ratio between adolescents with healthy body mass index (BMI) and adolescents with BMI in the cardiometabolic risk zone. Sport Sci Health 2022. [CrossRef]
- O’brien W, Issartel J, Belton S. Relationship between physical activity, screen time and weight status among young adolescents. Sports 2018, 6, 57. [Google Scholar] [CrossRef]
- Nevill AM, Duncan MJ, Lahart IM, Sandercock G. Cardiorespiratory fitness and activity explains the obesity-deprivation relationship in children. Health Promot Int 2018, 33, 479–487. [Google Scholar] [CrossRef]
- Artero EG, Ruiz JR, Ortega FB, España-Romero V, Vicente-Rodríguez G, Molnar D, et al. Muscular and cardiorespiratory fitness are independently associated with metabolic risk in adolescents: The HELENA study. Pediatr Diabetes 2011, 12, 704–712. [Google Scholar] [CrossRef]
- Górnicka M, Hamulka J, Wadolowska L, Kowalkowska J, Kostyra E, Tomaszewska M, et al. Activity–inactivity patterns, screen time, and physical activity: The association with overweight, central obesity and muscle strength in Polish teenagers. report from the ABC of healthy eating study. Int J Environ Res Public Health 2020, 17, 1–21. [Google Scholar] [CrossRef]
- Janney CA, Jakicic JM. The influence of exercise and BMI on injuries and illnesses in overweight and obese individuals: A randomized control trial. International Journal of Behavioral Nutrition and Physical Activity 2010, 7. [Google Scholar] [CrossRef]
- Pepera G, Hadjiandrea S, Iliadis I, Sandercock GRH, Batalik L. Associations between cardiorespiratory fitness, fatness, hemodynamic characteristics, and sedentary behaviour in primary school-aged children. BMC Sports Sci Med Rehabil 2022, 14. [Google Scholar] [CrossRef]
- Lee HS, Jeong WW, Choi YJ, Seo YG, Noh HM, Song HJ, et al. Association between physical fitness and cardiometabolic risk of children and adolescents in Korea. Korean J Fam Med 2019, 40, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Mintjens S, Menting MD, Daams JG, van Poppel MNM, Roseboom TJ, Gemke RJBJ. Cardiorespiratory Fitness in Childhood and Adolescence Affects Future Cardiovascular Risk Factors: A Systematic Review of Longitudinal Studies. Sports Medicine 2018, 48, 2577–2605. [Google Scholar] [CrossRef] [PubMed]
- Finch CF, Kemp JL, Clapperton AJ. The incidence and burden of hospital-treated sports-related injury in people aged 15+ years in Victoria, Australia, 2004-2010: A future epidemic of osteoarthritis? Osteoarthritis Cartilage 2015, 23, 1138–1143. [CrossRef]
- Leppänen M, Pasanen K, Kujala UM, Vasankari T, Kannus P, Äyrämö S, et al. Stiff Landings Are Associated with Increased ACL Injury Risk in Young Female Basketball and Floorball Players. American Journal of Sports Medicine 2017, 45, 386–393. [Google Scholar] [CrossRef]
- Lopes TJA, Simic M, Myer GD, Ford KR, Hewett TE, Pappas E. The Effects of Injury Prevention Programs on the Biomechanics of Landing Tasks: A Systematic Review With Meta-analysis. American Journal of Sports Medicine 2018, 46, 1492–1499. [Google Scholar] [CrossRef]
- El Gharib MH, El Tohamy AM, Mohamed NE. Determining the relationship between the quadriceps and tibiofemoral angles among adolescents. J Taibah Univ Med Sci 2021, 16, 70–76. [Google Scholar] [CrossRef]
- García-Luna MA, Cortell-Tormo JM, García-Jaén M, Ortega-Navarro M, Tortosa-Martínez J. Acute effects of ACL injury-prevention warm-up and soccer-specific fatigue protocol on dynamic knee valgus in youth male soccer players. Int J Environ Res Public Health 2020, 17, 1–14. [Google Scholar] [CrossRef]
- Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med 2009, 43, 417–422. [Google Scholar] [CrossRef]
- Parikh SN, Shrivastava RK. Evaluation of Children with Injuries Around the Knee. Indian J Pediatr 2016, 83, 844–851. [Google Scholar] [CrossRef]
- Hewett TE, Myer GD, Ford KR, Heidt RS, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. American Journal of Sports Medicine 2005, 33, 492–501. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Prevalence of thinness among children and adolescents, BMI < -2 standard deviations below the median (crude estimate) (%). The Global Health Observatory 2007.
- Barlow, SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007, 120 (Suppl. 4). [Google Scholar] [CrossRef]
- De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. 2011.
- Papathanasiou G, Georgoudis G, Georgakopoulos D, Katsouras C, Kalfakakou V, Evangelou A. Criterion-related validity of the short International Physical Activity Questionnaire against exercise capacity in young adults. Eur J Prev Cardiol 2010, 17, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou G, Georgoudis G, Georgakopoulos D, Kalfakakou V, Katsouras C, Evangelou A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. European Journal of Cardiovascular Prevention and Rehabilitation 2009, 17, 380–386. [Google Scholar]
- Sandercock GRH, Ogunleye AA. Independence of physical activity and screen time as predictors of cardiorespiratory fitness in youth. Pediatr Res 2013, 73, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Sandercock G RH, Ogunleye A, Voss C. Screen time and physical activity in youth: thief of time or lifestyle choice? J Phys Act Health 2012, 9, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Dingenen B, Malfait B, Vanrenterghem J, Robinson MA, Verschueren SMP, Staes FF. Can two-dimensional measured peak sagittal plane excursions during drop vertical jumps help identify three-dimensional measured joint moments? Knee 2015, 22, 73–79. [Google Scholar] [CrossRef]
- Pueo B, Penichet-Tomas A, Jimenez-Olmedo JM. Validity, reliability and usefulness of smartphone and kinovea motion analysis software for direct measurement of vertical jump height. Physiol Behav 2020, 227. [CrossRef]
- Holden S, Boreham C, Doherty C, Delahunt E. Two-dimensional knee valgus displacement as a predictor of patellofemoral pain in adolescent females. Scand J Med Sci Sports 2017, 27, 188–194. [Google Scholar] [CrossRef]
- Numata H, Nakase J, Kitaoka K, Shima Y, Oshima T, Takata Y, et al. Two-dimensional motion analysis of dynamic knee valgus identifies female high school athletes at risk of non-contact anterior cruciate ligament injury. Knee Surgery, Sports Traumatology, Arthroscopy 2018, 26, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Mahar MT, Welk GJ, Janz KF, Laurson K, Zhu W, Baptista F. Estimation of Lower Body Muscle Power from Vertical Jump in Youth. Meas Phys Educ Exerc Sci 2022. [Google Scholar] [CrossRef]
- Dadfar M, Soltani M, Novinzad MB, Raahemifar K. Lower extremity energy absorption strategies at different phases during single and double-leg landings with knee valgus in pubertal female athletes. Sci Rep 2021, 11. [Google Scholar] [CrossRef]
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Papers Establishing a standard definition for child overweight and obesity worldwide: international survey. n.d.
- Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-Country reliability and validity. Med Sci Sports Exerc 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- AMERICAN ACADEMY OF PEDIATRICS Committee on Public Education Children, Adolescents, and Television. 2001.
- Sandercock GRH, Alibrahim M, Bellamy M. Media device ownership and media use: Associations with sedentary time, physical activity and fitness in English youth. Prev Med Rep 2016, 4, 162–168. [Google Scholar] [CrossRef]
- Duncan MJ, Hankey J, Nevill AM. Peak-Power Estimation Equations in 12-to 16-Year-Old Children: Comparing Linear with Allometric Models. vol. 25. 2013.
- Temfemo A, Hugues J, Chardon K, Mandengue SH, Ahmaidi S. Relationship between vertical jumping performance and anthropometric characteristics during growth in boys and girls. Eur J Pediatr 2009, 168, 457–464. [Google Scholar] [CrossRef]
- Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: Moving from risk factor identification to injury pattern recognition - Narrative review and new concept. Br J Sports Med 2016, 50, 1309–1314. [Google Scholar] [CrossRef]
- Hershkovich O, Thein R, Gordon B, Burstein G, Tenenbaum S, Derazne E, et al. Coronal Knee Malalignment in Young Adults and Its Link to Body Measures. Journal of Knee Surgery 2019, 32, 421–426. [Google Scholar] [CrossRef]
- Larwa J, Stoy C, Chafetz RS, Boniello M, Franklin C. Stiff landings, core stability, and dynamic knee valgus: A systematic review on documented anterior cruciate ligament ruptures in male and female athletes. Int J Environ Res Public Health 2021, 18. [Google Scholar] [CrossRef]
- Franceschin MJ, da Veiga GV. Association of cardiorespiratory fitness, physical activity level, and sedentary behaviour with overweight in adolescents. Revista Brasileira de Cineantropometria e Desempenho Humano 2020, 22, 1–12. [Google Scholar] [CrossRef]
- Taylor ED, Theim KR, Mirch MC, Ghorbani S, Tanofsky-Kraff M, Adler-Wailes DC, et al. Orthopedic complications of overweight in children and adolescents. Pediatrics 2006, 117, 2167–2174. [Google Scholar] [CrossRef] [PubMed]
- Asaeda M, Nakamae A, Hirata K, Kono Y, Uenishi H, Adachi N. Factors associated with dynamic knee valgus angle during single-leg forward landing in patients after anterior cruciate ligament reconstruction. Asia Pac J Sports Med Arthrosc Rehabil Technol 2020, 22, 56–61. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the study.

Figure 2.
Measurement of (a) height and (b) weight.
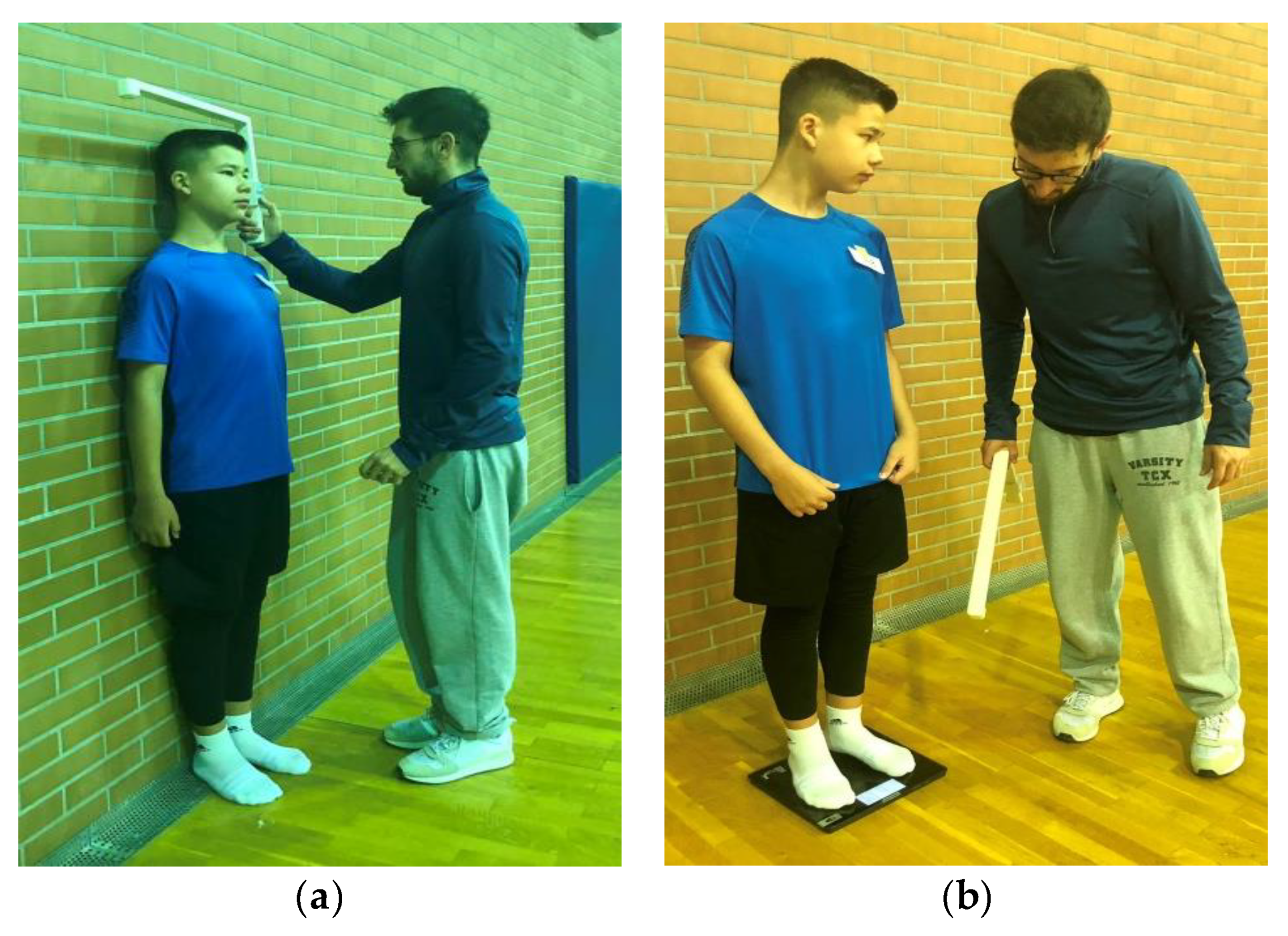
Figure 3.
Guide points for placing the 5 reflective markers and the knee landing angle (KLA): (a) the 5 markers in the standing position, (b) the markers for the calculation of the center of the knee and ankle joints, (c) the measurement of the knee landing angle (KLA).
Figure 3.
Guide points for placing the 5 reflective markers and the knee landing angle (KLA): (a) the 5 markers in the standing position, (b) the markers for the calculation of the center of the knee and ankle joints, (c) the measurement of the knee landing angle (KLA).
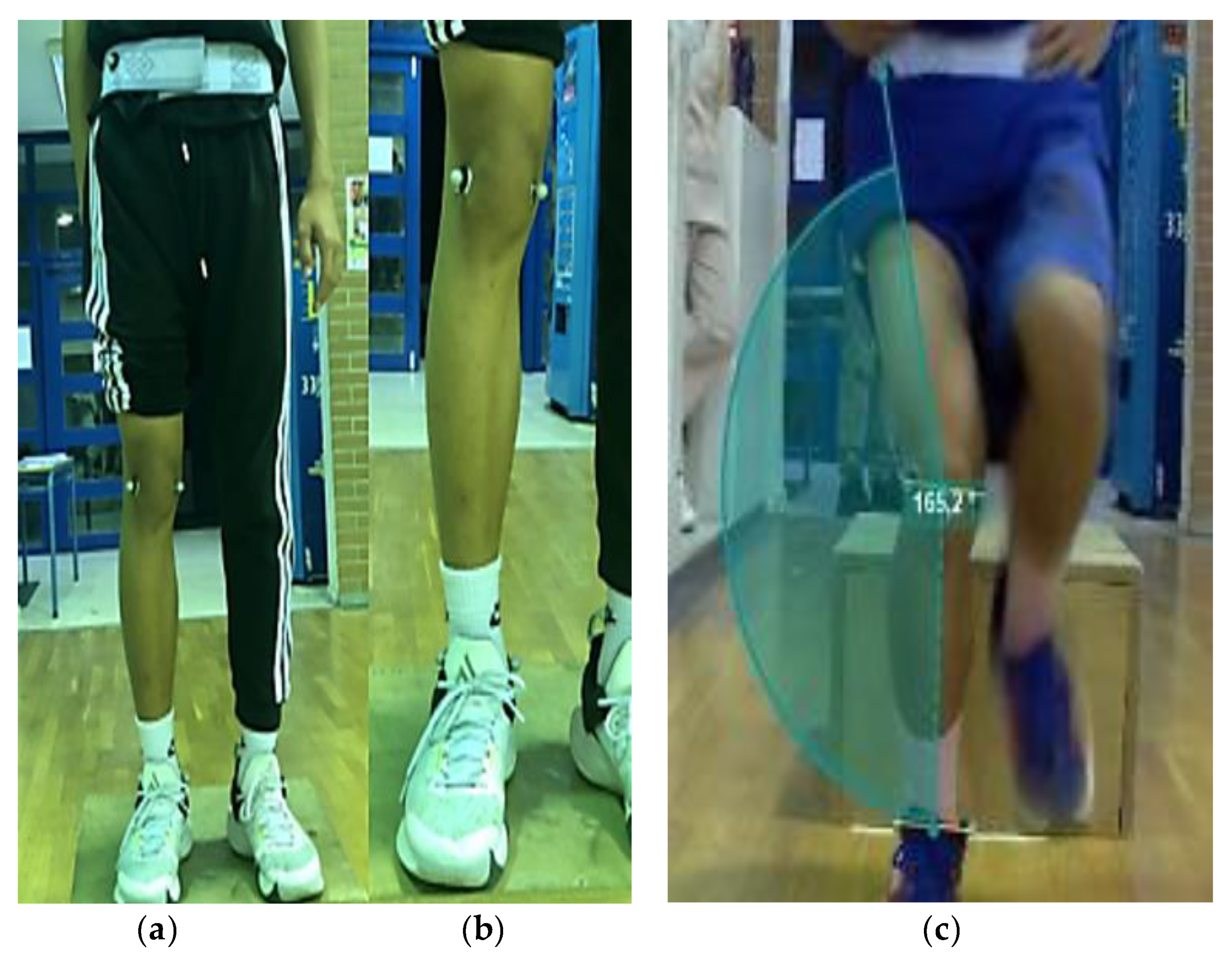

Table 1.
Descriptive statistics.
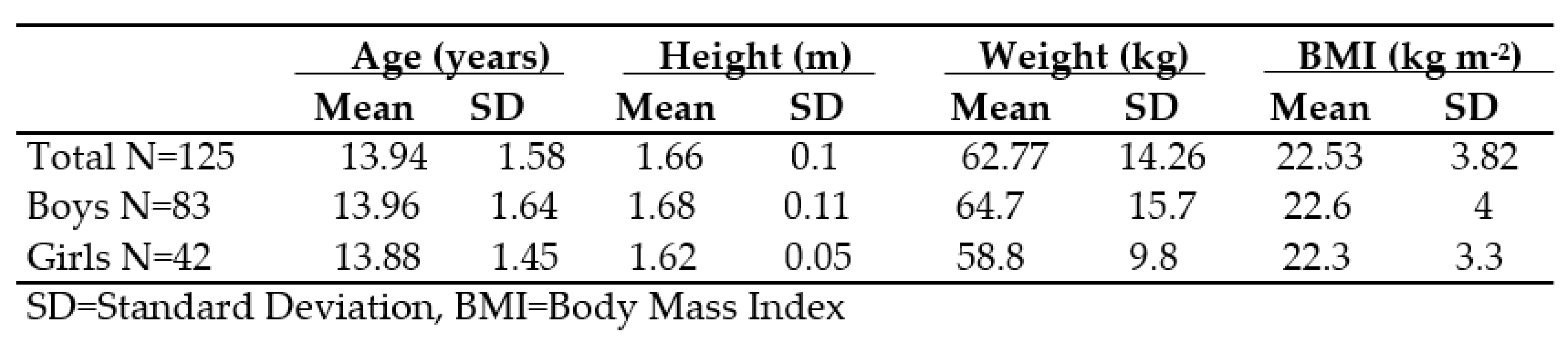
Table 2.
Comparisons between BMI groups for muscle power and knee landing angle.
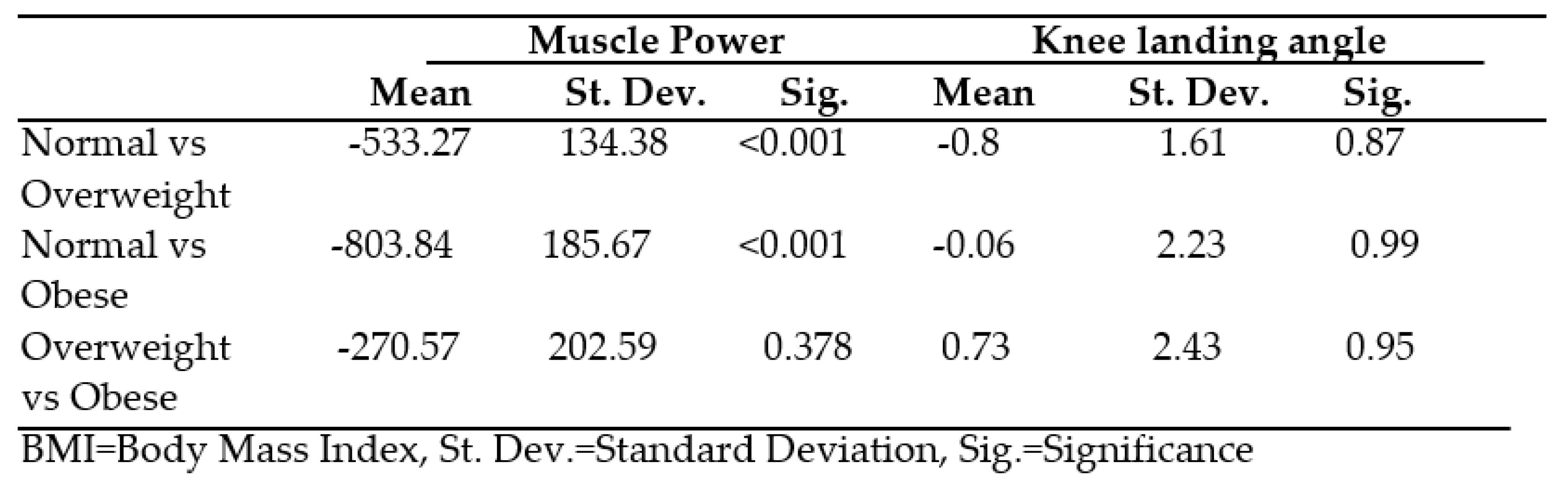
Table 3.
Comparisons between ST groups for muscle power and knee landing angle.
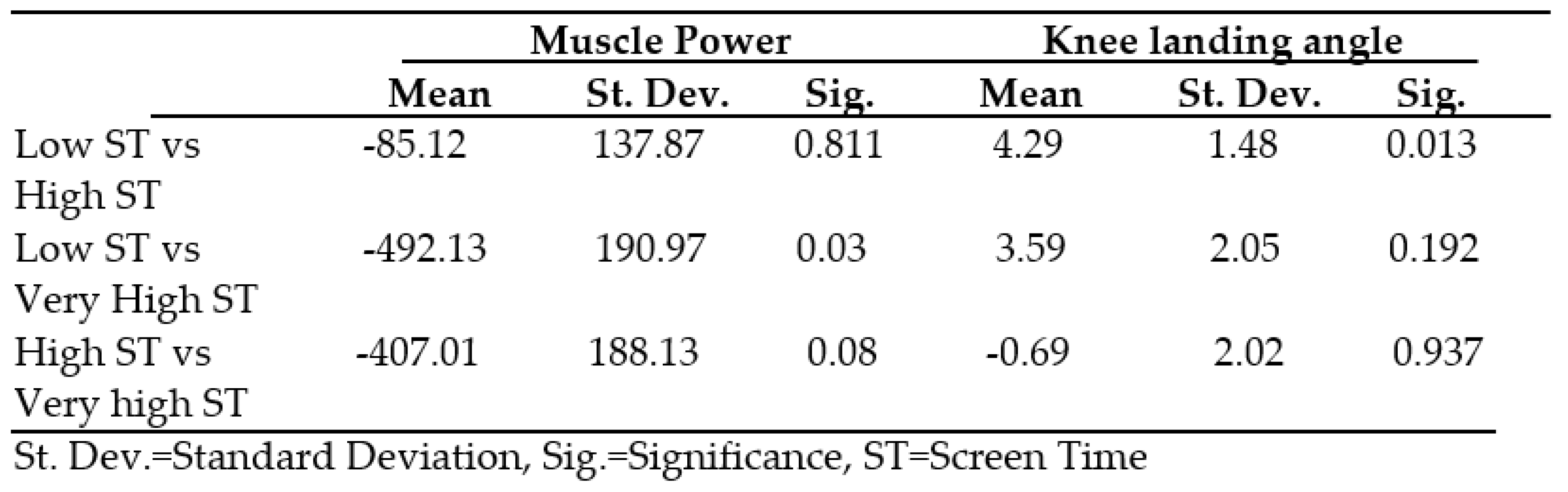
Table 4.
Comparisons between PA groups for muscle power and knee landing angle.
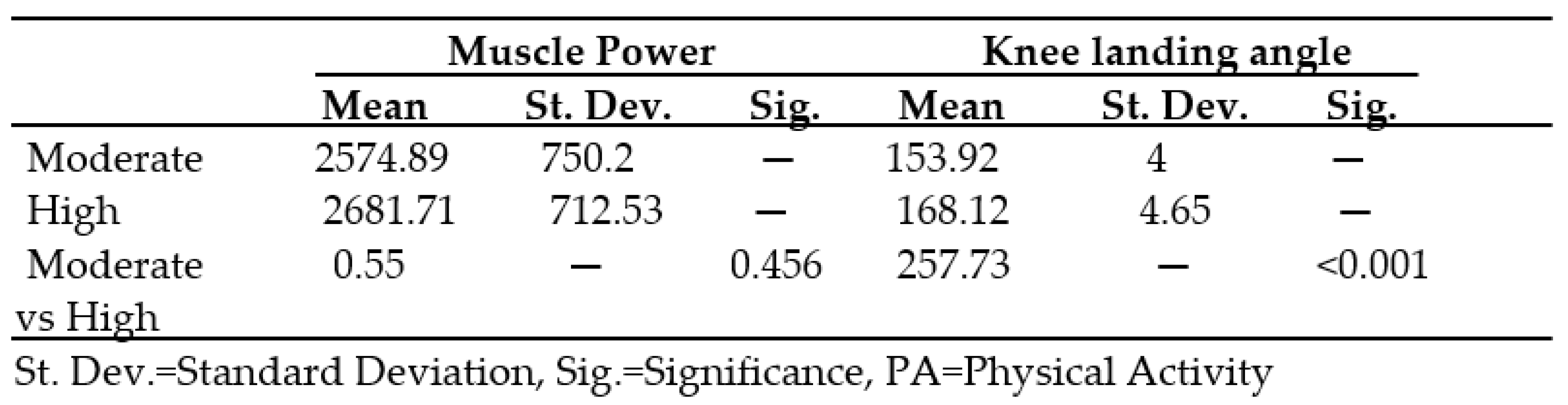
Table 5.
Correlation between the independent and the dependent variables.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



