
Submitted:
08 September 2023
Posted:
11 September 2023
You are already at the latest version
Abstract
Brain disorders pose a significant global healthcare challenge due to their complexity and profound impact on individuals and society. This review explores recent advancements in brain disease research, deepening our understanding and progress towards treatments. Technological innovations, like high-resolution imaging and optogenetics, play a pivotal role in illuminating cellular structures and dissecting neural circuits. Genetic analysis identifies dis-ease-associated genes and mutations, yet translating findings to clinical applications remains challenging. Epigenomics, transcriptomics, and proteomics provide molecular insights, un-covering disrupted pathways in conditions like Alzheimer's disease. Stem cell models elucidate developmental mechanisms, and immunotherapies, including CAR T cells, emerge as prom-ising strategies for brain cancers like glioblastoma. Genome editing tools, exemplified by CRISPR, enable precise modification of disease genes in models, deepening our understanding of pathogenesis. Multifaceted approaches integrating human studies, animal models, and bi-oinformatics propel the field forward. However, complexities persist, as disease specificity for cell types or brain regions remains an enigma, and genetic factors interact with environmental influences, highlighting disease intricacies. Ultimately, interdisciplinary efforts combining bi-ophysical and psychospiritual perspectives are essential to fully understand brain health and unlock transformative treatments for these debilitating disorders. A comprehensive under-standing of brain disorders is vital to improve the quality of life for millions and alleviate the global burden of neurological afflictions. Continued collaborative research will lead to an era of improved brain health worldwide.
Keywords:
Brain disorders
; Transformative treatments
; Disease specificity
; Stem cell models
; CRISPR
; Immunotherapies.
1. Introduction
James Parkinson's seminal work, "An Essay on the Shaking Palsy," penned more than two centuries ago, marked the inception of our understanding of Parkinson's disease (PD) [3]. Since then, PD has emerged as a focal point of rigorous scientific inquiry and medical exploration, transcending the boundaries of mere motor disturbances to reveal a complex interplay of genetic, environmental, and pathological factors [4].
PD, characterized by the cardinal motor features of tremor, rigidity, bradykinesia, and postural instability, represents but a fraction of its intricate manifestations, which extend beyond these observable parameters [5,6]. Central to the investigation of PD is the unraveling of its genetic underpinnings, a task that has witnessed remarkable advancements in recent years[7]. Genetic analysis has unveiled an array of disease-associated genes, shedding profound light on the origins of PD and even enabling earlier diagnoses in pre-symptomatic stages[8,9,10]. Yet, the translation of these promising genetic discoveries into practical clinical applications remains an enduring challenge[11,12]. Compounding the complexity of PD is its clinical heterogeneity, leading to the classification of various clinical subtypes that reflect biological and pathophysiological differences among individuals with PD[13,14]. This diversity underscores the imperative for personalized and precision treatment approaches, particularly in the quest for disease modification[15].
While numerous pharmacological agents have been designed to modify the disease or alleviate symptoms, their journey through clinical trials has been marked by formidable challenges, often resulting in failure to meet primary endpoints[16,17]. These hurdles encompass the clinical diversity of PD populations, patient selection intricacies, the absence of suitable preclinical models for sporadic PD, the quest for a definitive disease biomarker, and the determination of the optimal time frame for disease-modifying interventions [18,19]. Nevertheless, the relentless pursuit of effective therapies persists, with a growing focus on nondopaminergic approaches that target various facets of the disease[6,15]. These approaches encompass small-molecule inhibitors, calcium channel blockers, iron chelators, anti-inflammatory agents, and immunotherapies, each showing promise in animal studies and paving the way for human clinical trials[11,20,21]. Beyond pharmacological interventions, the PD research landscape also explores non-pharmacological avenues, including gene therapies, neurotrophic factors, cell restoration therapies, and the electrical modulation of neural circuits through deep brain stimulation (DBS)[22]. These offer alternative pathways for intervention and disease modification [23,24].
In this extensive review, we meticulously document the significant milestones in Parkinson's disease (PD) research spanning the past two centuries, while also shedding light on the present challenges. These challenges are intricately intertwined with the multifaceted origins of PD, prompting a compelling need for innovative therapeutic solutions. Within these pages, we explore the emerging developments that hold the potential to shape the future landscape of PD research, with a particular emphasis on the critical roles played by pre-motor symptoms and early diagnosis in the pursuit of more effective treatment strategies. Our journey takes us through the transformative evolution of PD, transcending its origins as a mere clinical description. Instead, it emerges as a complex interplay of genetic, environmental, and molecular factors, underscoring the rapid advancement of critical fields such as genetics, drug discovery, and drug delivery systems. These disciplines now stand as essential pillars in our ongoing quest to unravel the intricacies of this enigmatic neurological disorder. As we navigate the promising horizons of PD research, we acknowledge the path illuminated by the accumulated knowledge and innovations of the past two centuries. The remarkable voyage from James Parkinson's initial observations to our current state of understanding serves as a testament to the steadfast commitment to unveil the mysteries concealed within this challenging neurological condition. Looking ahead, we anticipate exciting new developments on the horizon that will continue to enrich our comprehension of PD, with a heightened focus on the pivotal roles played by pre-motor symptoms and early diagnosis, as we endeavor to forge more effective therapeutic avenues for those affected by PD.
2. Two Centuries of Parkinson's Disease: Insights and Innovations
Two centuries have elapsed since James Parkinson penned his groundbreaking "Essay on the Shaking Palsy," providing the world with the initial glimpse into a condition characterized by tremors at rest, bradykinesia, and akinesia [1]. While this essay marked the first formal description of what would later bear his name, Parkinson's Disease (PD), it wasn't until half a century later that the contributions of Jean-Martin Charcot began to define the clinical and anatomopathological foundations of PD [2]. Subsequent years witnessed further revelations in the understanding of this enigmatic disorder (Figure 1).
In 1893, Blocq and Marinescu observed resting tremors in a patient, reminiscent of parkinsonian symptoms, attributed to a tuberculous granuloma affecting the ipsilateral Substantia nigra pars compacta (SNc)[25]. Building upon this observation, Brissaud speculated that the SNc might be the epicenter of PD pathology [26]. It wasn't until two decades later that Trétiakoff uncovered neuropathological transformations in the SNc of PD patients, including a significant reduction in neuromelanin content and the presence of cytoplasmic inclusions known as Lewy bodies (LB) [27]. These inclusions, previously described by James Lewy, became a focal point of neuropathological investigations[28]. The combined hallmark of dopaminergic neuron loss in the SNc and the presence of LB solidified as the anatomopathological signature and diagnostic criterion for PD [29].
With diagnostic criteria established, the foremost challenge remained effective treatment[18]. The first neurosurgery targeting the basal ganglia (BG) for PD treatment occurred in 1940[30]. Progress accelerated in the late 1950s and mid-1960s with the discovery of dopamine (DA) as a neurotransmitter and its pivotal role in the striatum [31]. Carlsson's revelation of DA's functional significance, supported by experiments demonstrating reserpine's motor activity reduction, reversed by L-3,4-dihydroxyphenylalanine (L-DOPA) administration, marked a significant turning point in our understanding of motor control in the BG [32]. Ehringer and Hornykiewicz further delineated the striatal DA deficiency in PD [10], while subsequent studies revealed dopaminergic nigrostriatal projections and emphasized the significance of the dorsolateral striatum, primarily affected in PD [33]. The L-DOPA era was inaugurated when Cotzias demonstrated the anti-parkinsonian effects of L-DOPA administration [34].
A groundbreaking moment occurred in 1983 when Langston and colleagues unveiled a group of drug users who developed acute parkinsonism after exposure to MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)[35]. MPTP exposure induced an acute syndrome mirroring PD, as MPP+ (MPTP metabolite) wreaked havoc on dopaminergic neurons within the substantia nigra through mitochondrial matrix and electron transport chain disruptions [36]. It was subsequently observed that PD patients exhibited a marked reduction in complex I activity in the SNc [37]. The identification of certain PD patients harboring polymorphisms in genes associated with complex I subunits hinted at a potential vulnerability factor [[38]. MPTP-based models enabled researchers to replicate PD hallmarks both in vitro and in vivo [16]. While pharmacological DA treatments enjoyed success, cell-based DA replacement approaches proved less fruitful [39].
In the late 1990s, genetic analysis advances led to the identification of mutations in the SNCA gene, encoding alpha-synuclein (α-syn), as the first genetic cause of PD [40]. Notably, α-syn was recognized as the primary component of LB, ushering in a new era of understanding [41]. Braak and colleagues proposed a pathological staging of PD based on these findings [42]. Subsequent years saw the identification of numerous other genes implicated in PD pathogenesis [39]. These genetic revelations opened new avenues for potential therapies, underpinned by the development of experimental models utilizing transgenic animals bearing PD-associated mutations[43]. Alongside these advances, neurotoxin-based animal models, such as MPTP or 6-OHDA, contributed valuable insights into potential disease intervention targets [32].
Contemporary research has extended into the intriguing realm of gut microbiota's potential link to PD etiology, opening novel avenues of investigation [44]. The focus now encompasses decoding pre-symptomatic phases and translating scientific progress into disease-modifying therapies for PD [45]. Exciting approaches with less invasive technologies like gamma knife or focused ultrasound have emerged for PD motor symptom treatment [46]. These developments herald a promising future in our quest to understand and combat Parkinson's Disease (PD) comprehensively.
3. Genetic Mysteries of Parkinson's Disease
The elucidation of the genetic underpinnings of familial Parkinson's Disease (PD) began in 1997 when the p.Ala30Thr missense mutation in the alpha-synuclein gene (SNCA) was identified[47]. This mutation was found in a large German family spanning four generations, as well as in three unrelated Greek families, where PD appeared in two to three generations[13,48]. Subsequently, several other pathogenetically significant missense mutations in SNCA were discovered, including p.Ala30Pro, p.Glu46Lys, p.Gly51Asp, p.Ala53Glu, and p.Ala53Thr[49]. It was noted that mutations altering gene dosage through duplications and triplications, without affecting protein structure, could also contribute to PD[50]. The prevalence of SNCA mutations is relatively low, occurring in approximately 0.2% of sporadic PD cases and 1-2% of familial PD cases[51]. However, these mutations link different forms of the disease and underscore the crucial role of alpha-synuclein structural and functional abnormalities in PD pathogenesis[52]. Over time, the list of genes implicated in familial PD has expanded, with more than 10 genes now definitively linked to Mendelian PD[53]. The table provides concise descriptions of these genes and their roles in PD pathogenesis. However, ongoing research continues to explore the contributions of these and other genes to PD's etiopathogenesis[25,54].
One intriguing case is the ubiquitin carboxy-terminal hydrolase UCHL1 (PARK5) gene, which was identified in a German family with late-onset PD[55]. Despite this initial discovery, subsequent familial PD cases with UCHL1 mutations have been rare[50]. Nevertheless, various polymorphic variants of UCHL1, particularly the p.Ser18Tyr missense mutation, have been extensively studied in sporadic PD[56]. Despite conflicting results, comprehensive meta-analyses across different populations failed to establish a significant association between this polymorphism and PD risk[57]. Studies in transgenic mice with UCHL1 mutations have yielded mixed outcomes, adding complexity to the gene's role in PD[58]. While some mice displayed neurodegeneration and altered alpha-synuclein metabolism, others did not[59]. The p.Ser18Tyr variant, in particular, exhibited antioxidant activity and reduced neurodegeneration risk in carriers[60].
Another noteworthy gene, not included in the table, is the GBA gene, responsible for glucocerebrosidase production. Mutations in this gene were originally identified in Gaucher disease patients, characterized by systemic issues and neurological disturbances[61]. Over 300 pathogenetically significant GBA mutations have been described, and they play a definite role in PD development[62]. However, even homozygous carriers of GBA mutations may not all develop parkinsonism[63]. For example, only about 9% of individuals homozygous for the Asn370Ser mutation (associated with mild Gaucher disease without severe neurological symptoms) develop parkinsonism[55]. Additionally, heterozygous carriers of GBA mutations, who comprise about 10% of carriers, have an increased risk of developing PD[64]. The penetrance of these mutations, meaning the likelihood of developing PD, is estimated at 30% by the age of 80[62]. Different mutations predominate in various ethnic groups[65].
Leucine-rich repeat kinase 2 (LRRK2) gene mutations also exhibit reduced penetrance. Despite over 100 known LRRK2 mutations, only six have clear familial associations[66]. For instance, the p.Gly2019Ser mutation, the most common LRRK2 variant, has an 85% penetrance by age 80[67]. However, penetrance can vary among different ethnic groups and is even lower for mutations in codon 1441[68]. In general, it is believed that monogenic forms of PD account for 5-10% of cases, with LRRK2 and PRKN being the major contributors to autosomal dominant and autosomal recessive forms, respectively[21,69]. However, the precise risk assessment based solely on the presence of these mutations remains challenging[70].
Moreover, the frequency of pathogenetically significant mutations in major PD-associated genes varies among populations, emphasizing the need for comprehensive genetic analysis and the search for new PD-related genes[71]. While various commercial genetic testing panels are available, they should be supplemented with detailed familial and phenotypic information for optimal accuracy[72]. Notably, a core panel of five genes, including PRKN, LRRK2, SNCA, PINK1, and PARK7, offers comparable efficiency to extensive gene panels[73,74,75](Table 1).
4. Multifaceted Challenges of Parkinson's Disease: Navigating Motor and Non-Motor Symptoms
Parkinson's disease presents a multifaceted spectrum of symptoms that encompass both motor and non-motor manifestations, and understanding these complexities is vital in providing effective care and management for individuals affected by this progressive neurodegenerative condition[77].
Motor symptoms of Parkinson's often include bradykinesia, characterized by the gradual reduction in movement speed[5]. This can lead to difficulties in performing everyday activities and a noticeable slowing down of tasks. Stiff and rigid muscles can limit one's range of motion, resulting in discomfort and making simple movements challenging[41]. A hallmark symptom of Parkinson's is the resting tremor, typically beginning in a limb, most commonly the hand or fingers[78]. Postural issues may develop, causing a stooped posture, and balance problems can contribute to falls and injuries[79]. Gait problems, such as freezing, shuffling steps, drooped shoulders, and a lack of arm swing, further impact mobility[80]. Facial expressions often become reduced, referred to as "masking," which can affect interpersonal interactions[3] (Figure 2).
On the non-motor side, Parkinson's introduces a host of other challenges[81]. Cognitive impairment varies in severity, ranging from mild memory difficulties and reduced ability to multitask to more severe cognitive decline and dementia[80]. Depression and anxiety are not mere emotional reactions to the diagnosis; they are integral parts of the disease, linked to changes in brain chemistry[5]. Sleep disturbances, including REM Sleep Disorder and Restless Legs Syndrome, disrupt rest and can lead to fatigue[24]. Loss of the sense of smell is often an early indicator of Parkinson's, occurring before other symptoms become apparent[13]. Constipation and speech changes, such as quieter or breathy voices, can also manifest. Swallowing difficulties may affect chewing, tongue movement, and the ability to consume food or liquids comfortably[82]. Vision difficulties can arise due to changes in eye movement, stemming from the loss of dopamine-producing neurons. Lastly, apathy, marked by a general lack of motivation and emotional expression, alongside fatigue, can impact an individual's quality of life[83].
5. Advancing Parkinson's Care: Technology's Transformative Impact
Understanding and effectively managing Parkinson's disease (PD) is a complex and evolving challenge in the realm of healthcare[84]. As this debilitating neurodegenerative disorder progresses, individuals with PD often experience a wide array of motor symptoms, cognitive changes, and fluctuations in their condition[85]. To address these complexities, researchers and healthcare professionals have increasingly turned to innovative technological solutions to monitor and assess various facets of PD[86]. One such technological advancement is Electromyography (EMG), which offers a unique window into the progression of PD[87]. By analyzing muscle activity and tremors, EMG provides valuable insights into the severity and development of motor symptoms in PD patients[88]. It allows for a more objective and precise assessment, facilitating tailored treatment strategies[60].
In parallel, Electroencephalogram (EEG) technology has emerged as a powerful tool for monitoring PD. By tracking changes in brain wave patterns, EEG helps in understanding the cognitive aspects of the disease and its impact on motor control[86]. This information aids in disease monitoring and enables healthcare providers to make informed decisions regarding treatment plans[89]. Brain imaging modalities and 3D motion analysis systems represent another dimension of PD assessment[90]. These technologies offer detailed insights into brain structures and movement patterns, shedding light on how PD affects both the brain and motor function. Such comprehensive assessments contribute to a more holistic understanding of the disease's progression[91].
Wearable sensors have transformed the landscape of PD monitoring by providing continuous, real-time data on movement and posture[92]. These sensors, including accelerometers and gyroscopes, offer objective measurements of gait, balance, and motor fluctuations[87]. They enable early detection of symptoms, personalized treatment adjustments, and improved patient care[93]. Physical activity monitoring for people with PD (PWP) has become increasingly important in assessing disease progression and the effectiveness of interventions[54]. Wearable devices and smartphone applications allow for remote monitoring, encouraging physical activity and enabling healthcare providers to track patient progress more effectively[94].
Levodopa Induced Dyskinesia (LID) is a common challenge in PD treatment. Technology aids in the identification of LID episodes, facilitating medication adjustments to minimize these side effects and enhance the patient's quality of life[95].In the realm of symptom severity estimation, technology assists in quantifying the impact of core PD symptoms such as tremors, bradykinesia, and dyskinesia. These objective assessments provide valuable support for clinical evaluations[5].
Moreover, the integration of web-based applications into PD home monitoring systems enhances convenience and data collection. Patients can self-report symptoms, fostering a more personalized approach to care[80]. Gait impairment is a hallmark of PD, and advanced gait analysis technologies enable a more detailed assessment of this aspect. These assessments inform treatment strategies and help in implementing fall prevention measures[78]. In recent years, technology has extended its reach into uncontrolled home environments, allowing for the monitoring of PD motor symptoms in real-world settings. This approach provides a more accurate depiction of the daily challenges faced by individuals with PD[96].
Lastly, audio sensors have been employed to capture vocal and speech patterns in PD patients[97]. These sensors assist in the assessment of speech impairments, which are common in PD, and provide insights into the disease's progression[98]. Overall, the integration of these various technological approaches represents a significant leap forward in the assessment and management of Parkinson's disease (Figure 3). By offering objective, real-time data and insights, these technologies enhance early diagnosis, enable personalized treatment plans, and ultimately improve the quality of life for individuals living with PD.
6. Revolutionary Advancements: Cutting-Edge Technologies Transforming the Clinical Evaluation, and Therapies for Parkinson's Disease"
Over the past decade, a wave of innovative technology-driven tools and therapeutic approaches has emerged, aimed at revolutionizing the way we diagnose, clinically assess, and treat individuals with movement disorders, particularly Parkinson's Disease[28]. This remarkable progress has been made possible by the ever-evolving landscape of molecular and cellular techniques, coupled with extraordinary advancements in technology. These breakthroughs collectively represent a significant milestone in enhancing our overall comprehension of this complex disease[99].
6.1. Innovative Approaches for Enhanced Parkinson's Disease Therapy: Targeted Drug Delivery Systems
For decades, various therapies have been introduced for the clinical management of Parkinson's Disease (PD) using available medications[100]. However, a significant challenge remains in effectively delivering drugs to the central nervous system (CNS) due to the protective blood-brain barrier (BBB)[101]. Recent advancements in micro- and nanosystems have shown promise in improving drug transport to the brain, circumventing BBB limitations and enhancing the therapeutic properties of both conventional and novel drug molecules[90].
Micro-/nano-drug delivery systems (DDSs) offer versatile options for localized treatment through direct brain administration or systemic delivery to the CNS[102]. These DDSs can be classified as either biodegradable or non-biodegradable, depending on the material and formulation[103]. Numerous preclinical studies have explored different micro-/nano-DDSs for drug and small molecule delivery to the brain, demonstrating varying degrees of success in providing neuroprotection[104]. Beyond the parenteral route, alternative administration methods such as buccal, subcutaneous, and intranasal delivery have gained attention for improving the onset time and bioavailability of dopaminergic drugs[105]. Intranasal administration, in particular, offers a non-invasive way to bypass the BBB through olfactory and trigeminal pathways, enhancing bioavailability and reducing the required drug concentrations[106]. Considering that many PD patients experience dysphagia as their condition progresses, efforts have been directed toward developing novel formulations to facilitate drug delivery at lower concentrations, further improving treatment outcomes[107].
Polymeric nanoparticles have emerged as a promising option for theranostic drug delivery due to their ability to facilitate drug transport across the blood-brain barrier (BBB), enabling the delivery of otherwise impermeable drugs like dopamine (DA)[108]. Surface-modified polymeric nanoparticles have shown successful outcomes, including reduced anxiety and improved motor function upon incorporating DA[109]. Additionally, solid lipid nanoparticles (SLNs) offer advantages such as biocompatibility and high drug-loading capacity[110]. By modifying their surfaces and sizes, SLNs can enhance drug targeting and bioavailability, making them suitable for central nervous system (CNS) drug delivery, as demonstrated in studies involving drugs like apomorphine and rotigotine, which showed enhanced drug uptake and sustained release[111]. Microencapsulation techniques have been employed to create long-acting injection products with controlled drug release, reducing systemic toxicity and achieving therapeutic drug concentrations in specific regions[112]. Liposomes, known for their versatility in encapsulating hydrophilic and lipophilic drugs, have been valuable for targeted drug delivery to the brain through surface modifications[104]. Intranasal and transdermal liposomal formulations have demonstrated potential in improving drug bioavailability while reducing side effects[113] (Figure 4).
6.2. Focused Ultrasound: Pioneering Non-Invasive Solutions for Neurological Disorders
In recent years, focused ultrasound (FUS) therapies have emerged as transformative modalities in the management of neurological disorders[114]. This non-invasive technique involves the precise application of focused acoustic energy (ultrasound) to specific regions of the brain. Guided by magnetic resonance imaging (MR), MR-guided FUS (MRgFUS) has enabled computer-calibrated targeting, ensuring a high degree of accuracy and real-time feedback on treatment effectiveness[115] (Figure 5).
Initial investigations into MRgFUS thalamotomy for essential tremor yielded encouraging results, with a marked reduction in hand tremors observed [116]. In the context of Parkinson's disease (PD), MRgFUS is being explored as a non-invasive means of ablating brain areas responsible for the disease's motor symptoms[117]. Notably, the application of MRgFUS to the pallidothalamic tract in PD patients in 2014 resulted in significant clinical improvements [118]. Subsequent studies targeting the ventral intermediate thalamic nuclei (Vim) reported noteworthy reductions in mean UPDRS scores post-procedure in PD patients [119]. In a recent pilot study, MRgFUS unilateral subthalamotomy was found to be well-tolerated and effective in improving motor symptoms in noticeably asymmetric PD patients [120].
Several critical questions remain unanswered, including the optimal target for treating PD symptoms and the potential need for individualized target selection[121]. Additionally, long-term durability of FUS ablation outcomes and the safety and feasibility of bilateral procedures require further investigation[122]. The non-invasive nature of this approach, coupled with its immediate and seemingly enduring clinical benefits, renders it a compelling option for individuals who may be unsuitable or averse to deep brain stimulation (DBS) therapy[123]. To solidify the preliminary findings and evaluate the potential utility of ablative FUS therapy in treating PD patients, rigorous large-scale randomized controlled trials are imperative[124]. Furthermore, ongoing research explores other FUS applications, such as opening the blood-brain barrier (BBB) and neuromodulation [125].Notably, low-intensity ultrasound has demonstrated the ability to reduce α-synuclein levels in PC12 cells [116]. Recent advancements combining MRgFUS with intravenous microbubbles and a shRNA sequence targeting α-synuclein have resulted in reduced α-synuclein immunoreactivity in various brain regions, offering promise for altering the progression of Lewy body pathology, particularly in conjunction with early disease diagnosis [126]. In summary, FUS technology presents a compelling frontier in the treatment of neurological disorders, with particular promise in the management of Parkinson's disease. Further research and clinical validation are essential to unlock its full potential for improving patient outcomes and altering the course of neurodegenerative diseases.
6.3. Advancements in Deep Brain Stimulation (DBS) for Parkinson's Disease
In recent years, device-aided therapies have evolved to become indispensable tools in the treatment of advanced Parkinson's disease (PD) patients[127]. These therapies, including levodopa–carbidopa infusion gel (LCIG), subcutaneous apomorphine pump infusion, and deep brain stimulation (DBS), have undergone rigorous scrutiny in large prospective clinical studies, establishing their safety, validity, and remarkable efficacy [128].
DBS, in particular, stands out as a transformative surgical approach that entails the precise implantation of one or more electrodes into specific regions of the brain[87]. Over the years, a substantial body of evidence has consistently demonstrated the effectiveness of DBS in addressing motor fluctuations, reducing dyskinesia, and significantly enhancing the overall quality of life in advanced PD patients, whether the target is the subthalamic nucleus (STN) or the globus pallidus internus (GPi) [129]. What is particularly noteworthy is the enduring nature of these benefits, with positive outcomes persisting for more than a decade [130]. Even in patients with a relatively shorter disease duration, DBS has showcased its superiority over best medical treatment regimens in terms of motor improvement and quality of life [131].
The landscape of deep brain stimulation has witnessed a remarkable evolution driven by innovations in neurosurgical techniques, including the advent of asleep surgery[132]. Further, specialized devices such as microelectrodes have enabled more precise and targeted electrode placements[128]. The refinement of programming and stimulation algorithms has also played a pivotal role in optimizing patient outcomes[87]. A milestone achievement in this progress is the introduction of directional electrodes, heralding a new era in DBS[131]. These electrodes allow for segmented stimulation, significantly enhancing precision in therapeutic targeting. Directional electrodes hold the promise of minimizing adverse effects commonly associated with conventional DBS approaches [130] (Figure 6).
To further elevate the management of motor fluctuations and minimize the adverse effects of DBS, researchers and clinicians are increasingly turning to adaptive DBS (aDBS)[128]. This innovative approach aims to personalize stimulation by continuously monitoring local field potentials (LFP) directly from the stimulating electrode. aDBS activates stimulation only when LFP beta power surpasses a customized threshold, providing real-time modulation of stimulation parameters[87]. Preliminary findings are promising, indicating that aDBS surpasses conventional DBS in terms of improving motor scores and effectively controlling levodopa-induced dyskinesias[132]. However, to firmly establish the sustained benefit and efficacy of this groundbreaking strategy, more extensive research encompassing longer timeframes and larger patient cohorts is indispensable [87].
In summary, the remarkable progress in deep brain stimulation represents a beacon of hope for individuals battling Parkinson's disease. As we delve deeper into the realm of personalized and responsive treatment modalities, the future of DBS holds the potential to further enhance the lives of PD patients and transform the landscape of neurological healthcare.
7. Conclusion
In the foreseeable future, the aging population in developed nations will inevitably amplify the burden of neurodegenerative diseases. Parkinson's Disease (PD) poses a unique challenge as its treatment demands a personalized approach, striking a delicate balance between symptom management, drug dosage, side effect mitigation, and patient expectations. This presents clinicians and researchers with an urgent call for a symbiotic relationship between medicine and research. Two centuries have elapsed since the publication of James Parkinson's seminal essay, during which our comprehension of this disease has undergone remarkable progress, continually forging new tools and avenues for exploration. Presently, fields such as functional genetics, novel molecular mechanisms, brain imaging, and biomarker detection stand as the guiding lights in our research strategies. Nevertheless, despite the substantial headway made, the quest for an improved early clinical diagnosis and a definitive cure remains unfulfilled. In this context, research into drug delivery mechanisms emerges as a beacon of hope, potentially offering safer and more efficacious treatments for PD. Years of investigation have underscored the importance of considering environmental factors alongside genetics when scrutinizing the progression of PD. However, there is an imperative need for further research to unravel the intricate mechanisms by which this pathology propagates from cell to cell within the brain and from other organs to the central nervous system. Crucially, studies should also be directed towards the development of early diagnostic tools and a deeper understanding of the distinct susceptibilities of pathogenic factors affecting dopaminergic neurons. PD is entangled with a complex web of pathophysiological processes encompassing α-synuclein aggregation, neuroinflammation, mitochondrial dysfunction, neuronal vulnerability, iron deposition, and neural network alterations. Given the interplay among these multifaceted pathways and the clinical diversity observed, a targeted therapeutic approach becomes imperative.Although current treatment options offer symptomatic relief, advances in high-throughput screening methods for small molecules, improved disease modeling, and progress in analytical technologies promise to usher in novel compounds and repurposed drugs. Immunotherapies hold the potential to stimulate the body's response to α-synuclein, introducing a novel mechanism of action. Within the realm of cell-based therapies, insights gained from research have illuminated the path forward, with some induced pluripotent stem cell (iPSC) therapies offering the prospect of personalized treatment.
Furthermore, the advent of adaptive Deep Brain Stimulation (DBS) and optogenetically inspired DBS opens doors to more precise targeting. Collectively, these advancements underscore a promising future for PD therapies. As we stand at the nexus of innovation and discovery, it is imperative that we harness these breakthroughs to alleviate the suffering caused by Parkinson's Disease and strive toward a future where its treatment and prevention are not just aspirations, but realities.
Author Contributions
AAM contributed to the writing and revision of the manuscript. IH prepared the review, conducting editing tasks, and overseeing the project's progress and KM contributed to the project by assisting with data visualization.
Funding
This research receives no external funding
Conflicts of Interest
The authors affirm that the research was conducted independently, without any commercial or financial affiliations that might pose a potential conflict of interest.
References
- Del Rey, N.L.; Quiroga-Varela, A.; Garbayo, E.; Carballo-Carbajal, I.; Fernandez-Santiago, R.; Monje, M.H.G.; Trigo-Damas, I.; Blanco-Prieto, M.J.; Blesa, J. Advances in Parkinson's Disease: 200 Years Later. Front Neuroanat 2018, 12, 113. [Google Scholar] [CrossRef]
- Elkouzi, A.; Vedam-Mai, V.; Eisinger, R.S.; Okun, M.S. Emerging therapies in Parkinson disease - repurposed drugs and new approaches. Nat Rev Neurol 2019, 15, 204–223. [Google Scholar] [CrossRef]
- Ascherio, A.; Schwarzschild, M.A. The epidemiology of Parkinson's disease: risk factors and prevention. The Lancet Neurology 2016, 15, 1257–1272. [Google Scholar] [CrossRef]
- Tangamornsuksan, W.; Lohitnavy, O.; Sruamsiri, R.; Chaiyakunapruk, N.; Norman Scholfield, C.; Reisfeld, B.; Lohitnavy, M. Paraquat exposure and Parkinson’s disease: A systematic review and meta-analysis. Archives of Environmental and Occupational Health 2019, 74, 225–238. [Google Scholar] [CrossRef]
- Chaudhuri, K.R.; Healy, D.G.; Schapira, A.H.V. Non-motor symptoms of Parkinson's disease: Diagnosis and management. Lancet Neurology 2006, 5, 235–245. [Google Scholar] [CrossRef]
- Angelopoulou, E.; Paudel, Y.N.; Piperi, C. miR-124 and Parkinson's disease: A biomarker with therapeutic potential. Pharmacological Research 2019, 150. [Google Scholar] [CrossRef]
- Batistela, M.S.; Josviak, N.D.; Sulzbach, C.D.; de Souza, R.L.R. An overview of circulating cell-free microRNAs as putative biomarkers in Alzheimer's and Parkinson's Diseases. International Journal of Neuroscience 2017, 127, 547–558. [Google Scholar] [CrossRef]
- Breckenridge, C.B.; Berry, C.; Chang, E.T.; Sielken, R.L., Jr.; Mandel, J.S. Association between Parkinson's disease and cigarette smoking, rural living, well-water consumption, farming and pesticide use: Systematic review and meta-analysis. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Chuang, Y.H.; Paul, K.C.; Bronstein, J.M.; Bordelon, Y.; Horvath, S.; Ritz, B. Parkinson's disease is associated with DNA methylation levels in human blood and saliva. Genome Medicine 2017, 9. [Google Scholar] [CrossRef]
- Kalia, L.V.; Lang, A.E. Parkinson's disease. The Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Caggiu, E.; Paulus, K.; Mameli, G.; Arru, G.; Sechi, G.P.; Sechi, L.A. Differential expression of miRNA 155 and miRNA 146a in Parkinson's disease patients. eNeurologicalSci 2018, 13, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Baghi, M.; Rostamian Delavar, M.; Yadegari, E.; Peymani, M.; Pozo, D.; Hossein Nasr-Esfahani, M.; Ghaedi, K. Modified level of miR-376a is associated with Parkinson's disease. Journal of Cellular and Molecular Medicine 2020, 24, 2622–2634. [Google Scholar] [CrossRef] [PubMed]
- Conway, K.A.; Harper, J.D.; Lansbury, P.T. Accelerated in vitro fibril formation by a mutant α-synuclein linked to early-onset Parkinson disease. Nature Medicine 1998, 4, 1318–1320. [Google Scholar] [CrossRef]
- Borsche, M.; König, I.R.; Delcambre, S.; Petrucci, S.; Balck, A.; Bruggemann, N.; Zimprich, A.; Wasner, K.; Pereira, S.L.; Avenali, M.; et al. Mitochondrial damage-associated inflammation highlights biomarkers in PRKN/PINK1 parkinsonism. Brain 2020, 143, 3041–3051. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, D.J.; Borges, A.F.; Souza, P.O.; De Souza, P.R.; De Barros Cardoso, C.R.; Dorta, M.L.; De Oliveira, M.A.P.; Teixeira, A.L.; Ribeiro-Dias, F. Decreased toll-like receptor 2 and toll-like receptor 7/8-induced cytokines in Parkinson's disease patients. NeuroImmunoModulation 2016, 23, 58–66. [Google Scholar] [CrossRef]
- Masliah, E.; Rockenstein, E.; Adame, A.; Alford, M.; Crews, L.; Hashimoto, M.; Seubert, P.; Lee, M.; Goldstein, J.; Chilcote, T.; et al. Effects of α-synuclein immunization in a mouse model of Parkinson's disease. Neuron 2005, 46, 857–868. [Google Scholar] [CrossRef]
- Sidransky, E.; Nalls, M.A.; Aasly, J.O.; Aharon-Peretz, J.; Annesi, G.; Barbosa, E.R.; Bar-Shira, A.; Berg, D.; Bras, J.; Brice, A.; et al. Multicenter analysis of glucocerebrosidase mutations in Parkinson's disease. New England Journal of Medicine 2009, 361, 1651–1661. [Google Scholar] [CrossRef]
- Abuelezz, N.Z.; Nasr, F.E.; Abdel Aal, W.M.; Molokhia, T.; Zaky, A. Sera miR-34a, miR-29b and miR-181c as potential novel diagnostic biomarker panel for Alzheimers in the Egyptian population. Experimental Gerontology 2022, 169. [Google Scholar] [CrossRef]
- Adamczak, S.; Dale, G.; De Rivero Vaccari, J.P.; Bullock, M.R.; Dietrich, W.D.; Keane, R.W. Inflammasome proteins in cerebrospinal fluid of brain-injured patients as biomarkers of functional outcome: Clinical article. Journal of Neurosurgery 2012, 117, 1119–1125. [Google Scholar] [CrossRef]
- Henderson-Smith, A.; Fisch, K.M.; Hua, J.; Liu, G.; Ricciardelli, E.; Jepsen, K.; Huentelman, M.; Stalberg, G.; Edland, S.D.; Scherzer, C.R.; et al. DNA methylation changes associated with Parkinson’s disease progression: outcomes from the first longitudinal genome-wide methylation analysis in blood. Epigenetics 2019, 14, 365–382. [Google Scholar] [CrossRef]
- Fan, Y.; Howden, A.J.M.; Sarhan, A.R.; Lis, P.; Ito, G.; Martinez, T.N.; Brockmann, K.; Gasser, T.; Alessi, D.R.; Sammler, E.M. Interrogating Parkinson’s disease LRRK2 kinase pathway activity by assessing Rab10 phosphorylation in human neutrophils. Biochemical Journal 2018, 475, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, R.; Elbaz, A.; Sanft, K.R.; Peterson, B.J.; Bower, J.H.; Ahlskog, J.E.; Grossardt, B.R.; De Andrade, M.; Maraganore, D.M.; Rocca, W.A. Education and occupations preceding Parkinson disease: A population-based case-control study. Neurology 2005, 65, 1575–1583. [Google Scholar] [CrossRef] [PubMed]
- Racette, B.A.; Nielsen, S.S.; Criswell, S.R.; Sheppard, L.; Seixas, N.; Warden, M.N.; Checkoway, H. Dose-dependent progression of parkinsonism in manganese-exposed welders. Neurology 2017, 88, 344–351. [Google Scholar] [CrossRef]
- Goldman, J.E.; Yen, S.H.; Chiu, F.C.; Peress, N.S. Lewy bodies of Parkinson's disease contain neurofilament antigens. Science 1983, 221, 1082–1084. [Google Scholar] [CrossRef] [PubMed]
- Doherty, K.M.; Silveira-Moriyama, L.; Parkkinen, L.; Healy, D.G.; Farrell, M.; Mencacci, N.E.; Ahmed, Z.; Brett, F.M.; Hardy, J.; Quinn, N.; et al. Parkin disease: A clinicopathologic entity? JAMA Neurology 2013, 70, 571–579. [Google Scholar] [CrossRef]
- Martin, I.; Kim, J.W.; Dawson, V.L.; Dawson, T.M. LRRK2 pathobiology in Parkinson's disease. Journal of Neurochemistry 2014, 131, 554–565. [Google Scholar] [CrossRef]
- Wong, Y.C.; Krainc, D. α-synuclein toxicity in neurodegeneration: Mechanism and therapeutic strategies. Nature Medicine 2017, 23, 1–13. [Google Scholar] [CrossRef]
- Torra, A.; Parent, A.; Cuadros, T.; Rodríguez-Galván, B.; Ruiz-Bronchal, E.; Ballabio, A.; Bortolozzi, A.; Vila, M.; Bové, J. Overexpression of TFEB Drives a Pleiotropic Neurotrophic Effect and Prevents Parkinson's Disease-Related Neurodegeneration. Molecular Therapy 2018, 26, 1552–1567. [Google Scholar] [CrossRef]
- Kenborg, L.; Funch Lassen, C.; Hansen, J.; Olsen, J.H. Parkinson's disease and other neurodegenerative disorders among welders: A Danish cohort study. Movement Disorders 2012, 27, 1283–1289. [Google Scholar] [CrossRef]
- Cao, F.; Liu, Z.; Sun, G. Diagnostic value of miR-193a-3p in Alzheimer's disease and miR-193a-3p attenuates amyloid-β induced neurotoxicity by targeting PTEN. Experimental Gerontology 2020, 130. [Google Scholar] [CrossRef]
- Andersen, J.V.; Schousboe, A.; Verkhratsky, A. Astrocyte energy and neurotransmitter metabolism in Alzheimer's disease: Integration of the glutamate/GABA-glutamine cycle. Progress in Neurobiology 2022, 217. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Tang, Y.; Yu, M.; Wu, L.; Liu, F.; Ni, J.; Wang, Z.; Wang, J.; Fei, J.; Wang, W.; et al. Downregulation of blood serum microRNA 29 family in patients with Parkinson's disease. Scientific Reports 2017, 7. [Google Scholar] [CrossRef]
- Chinta, S.J.; Mallajosyula, J.K.; Rane, A.; Andersen, J.K. Mitochondrial alpha-synuclein accumulation impairs complex I function in dopaminergic neurons and results in increased mitophagy in vivo. Neuroscience Letters 2010, 486, 235–239. [Google Scholar] [CrossRef]
- Guzman, J.N.; Sanchez-Padilla, J.; Wokosin, D.; Kondapalli, J.; Ilijic, E.; Schumacker, P.T.; Surmeier, D.J. Oxidant stress evoked by pacemaking in dopaminergic neurons is attenuated by DJ-1. Nature 2010, 468, 696–700. [Google Scholar] [CrossRef]
- Ren, L.; Yi, J.; Yang, J.; Li, P.; Cheng, X.; Mao, P. Nonsteroidal anti-inflammatory drugs use and risk of Parkinson disease: A dose–response meta-analysis. Medicine (United States) 2018, 97. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Kang, X.; Lin, B.; Yu, Q.; Song, B.; Gao, G.; Chen, Y.; Sun, X.; Li, X.; et al. One-Step Biallelic and Scarless Correction of a β-Thalassemia Mutation in Patient-Specific iPSCs without Drug Selection. Molecular Therapy - Nucleic Acids 2017, 6, 57–67. [Google Scholar] [CrossRef]
- Lu, G.; Middleton, R.E.; Sun, H.; Naniong, M.; Ott, C.J.; Mitsiades, C.S.; Wong, K.K.; Bradner, J.E.; Kaelin Jr, W.G. The myeloma drug lenalidomide promotes the cereblon-dependent destruction of ikaros proteins. Science 2014, 343, 305–309. [Google Scholar] [CrossRef]
- Goldman, S.M.; Marek, K.; Ottman, R.; Meng, C.; Comyns, K.; Chan, P.; Ma, J.; Marras, C.; Langston, J.W.; Ross, G.W.; et al. Concordance for Parkinson's disease in twins: A 20-year update. Annals of Neurology 2019, 85, 600–605. [Google Scholar] [CrossRef]
- Schwarzschild, M.A.; Chen, J.F.; Ascherio, A. Caffeinated clues and the promise of adenosine A2a antagonists in PD. Neurology 2002, 58, 1154–1160. [Google Scholar] [CrossRef]
- Nalls, M.A.; Pankratz, N.; Lill, C.M.; Do, C.B.; Hernandez, D.G.; Saad, M.; Destefano, A.L.; Kara, E.; Bras, J.; Sharma, M.; et al. Large-scale meta-analysis of genome-wide association data identifies six new risk loci for Parkinson's disease. Nature Genetics 2014, 46, 989–993. [Google Scholar] [CrossRef]
- Chuang, Y.H.; Lu, A.T.; Paul, K.C.; Folle, A.D.; Bronstein, J.M.; Bordelon, Y.; Horvath, S.; Ritz, B. Longitudinal Epigenome-Wide Methylation Study of Cognitive Decline and Motor Progression in Parkinson's Disease. Journal of Parkinson's Disease 2019, 9, 389–400. [Google Scholar] [CrossRef]
- Pagan, F.; Hebron, M.; Valadez, E.H.; Torres-Yaghi, Y.; Huang, X.; Mills, R.R.; Wilmarth, B.M.; Howard, H.; Dunn, C.; Carlson, A.; et al. Nilotinib effects in Parkinson's disease and dementia with lewy bodies. Journal of Parkinson's Disease 2016, 6, 503–517. [Google Scholar] [CrossRef]
- Blanz, J.; Saftig, P. Parkinson's disease: acid-glucocerebrosidase activity and alpha-synuclein clearance. Journal of Neurochemistry 2016, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Guhathakurta, S.; Evangelista, B.A.; Ghosh, S.; Basu, S.; Kim, Y.S. Hypomethylation of intron1 of α-synuclein gene does not correlate with Parkinson’s disease. Molecular Brain 2017, 10, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Jacobs, E.; Schwarzschild, M.A.; McCullough, M.L.; Calle, E.E.; Thun, M.J.; Ascherio, A. Nonsteroidal antiinflammatory drug use and the risk for Parkinson's disease. Annals of Neurology 2005, 58, 963–967. [Google Scholar] [CrossRef]
- Karuppagounder, S.S.; Brahmachari, S.; Lee, Y.; Dawson, V.L.; Dawson, T.M.; Ko, H.S. The c-Abl inhibitor, nilotinib, protects dopaminergic neurons in a preclinical animal model of Parkinson's disease. Scientific Reports 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Stubblefield, B.; Cookson, M.R.; Goldin, E.; Velayati, A.; Tayebi, N.; Sidransky, E. Aggregation of α-synuclein in brain samples from subjects with glucocerebrosidase mutations. Molecular Genetics and Metabolism 2011, 104, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Lindersson, E.; Beedholm, R.; Højrup, P.; Moos, T.; Gai, W.; Hendil, K.B.; Jensen, P.H. Proteasomal Inhibition by α-Synuclein Filaments and Oligomers. Journal of Biological Chemistry 2004, 279, 12924–12934. [Google Scholar] [CrossRef]
- Cuervo, A.M.; Stafanis, L.; Fredenburg, R.; Lansbury, P.T.; Sulzer, D. Impaired degradation of mutant α-synuclein by chaperone-mediated autophagy. Science 2004, 305, 1292–1295. [Google Scholar] [CrossRef]
- Bressan, E.; Reed, X.; Bansal, V.; Hutchins, E.; Cobb, M.M.; Webb, M.G.; Alsop, E.; Grenn, F.P.; Illarionova, A.; Savytska, N.; et al. The foundational data initiative for Parkinsons disease (FOUNDIN-PD): enabling efficient translation from genetic maps to mechanism. bioRxiv 2021. [Google Scholar]
- Cai, M.; Liu, Z.; Li, W.; Wang, Y.; xie, A. Association between rs823128 polymorphism and the risk of Parkinson's disease: A meta-analysis. Neuroscience Letters 2018, 665, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Corces, M.R.; Shcherbina, A.; Kundu, S.; Gloudemans, M.J.; Frésard, L.; Granja, J.M.; Louie, B.H.; Eulalio, T.; Shams, S.; Bagdatli, S.T.; et al. Single-cell epigenomic analyses implicate candidate causal variants at inherited risk loci for Alzheimer’s and Parkinson’s diseases. Nature Genetics 2020, 52, 1158–1168. [Google Scholar] [CrossRef] [PubMed]
- Foo, J.N.; Chew, E.G.Y.; Chung, S.J.; Peng, R.; Blauwendraat, C.; Nalls, M.A.; Mok, K.Y.; Satake, W.; Toda, T.; Chao, Y.; et al. Identification of Risk Loci for Parkinson Disease in Asians and Comparison of Risk between Asians and Europeans: A Genome-Wide Association Study. JAMA Neurology 2020, 77, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.; Han, D.; Cheng, Q.; Zhang, P.; Zhao, C.; Min, J.; Wang, F. Association of Levels of Physical Activity With Risk of Parkinson Disease: A Systematic Review and Meta-analysis. JAMA network open 2018, 1, e182421. [Google Scholar] [CrossRef]
- Riboldi, G.M.; Di Fonzo, A.B. GBA, Gaucher disease, and parkinson’s disease: From genetic to clinic to new therapeutic approaches. Cells 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Bustos, B.I.; Billingsley, K.; Blauwendraat, C.; Raphael Gibbs, J.; Gan-Or, Z.; Krainc, D.; Singleton, A.B.; Lubbe, S.J. For the International Parkinson’s Disease Genomics Consortium (IPDGC). Genome-Wide Contribution of Common Short-Tandem Repeats to Parkinson’s Disease Genetic Risk. 0000.
- Desplats, P.; Spencer, B.; Coffee, E.; Patel, P.; Michael, S.; Patrick, C.; Adame, A.; Rockenstein, E.; Masliah, E. α-synuclein sequesters Dnmt1 from the nucleus: A novel mechanism for epigenetic alterations in Lewy body diseases. Journal of Biological Chemistry 2011, 286, 9031–9037. [Google Scholar] [CrossRef]
- Goldman, J.S. Predictive Genetic Counseling for Neurodegenerative Diseases: Past, Present, and Future. Cold Spring Harb. Perspect. Med 2019, 23, a036525. [Google Scholar] [CrossRef]
- Nativio, R.; Lan, Y.; Donahue, G.; Sidoli, S.; Berson, A.; Srinivasan, A.R.; Shcherbakova, O.; Amlie-Wolf, A.; Nie, J.; Cui, X.; et al. An integrated multi-omics approach identifies epigenetic alterations associated with Alzheimer’s disease. Nature Genetics 2020, 52, 1024–1035. [Google Scholar] [CrossRef]
- Tan, A.H.; Noyce, A.; Carrasco, A.M.; Brice, A.; Reimer, A.; Illarionova, A.; Singleton, A.; Schumacher-Schuh, A.; Stecher, B.; Siddiqi, B.; et al. GP2: The Global Parkinson's Genetics Program. Movement Disorders 2021, 36, 842–851. [Google Scholar] [CrossRef]
- Brockmann, K.; Srulijes, K.; Pflederer, S.; Hauser, A.K.; Schulte, C.; Maetzler, W.; Gasser, T.; Berg, D. GBA-associated Parkinson's disease: Reduced survival and more rapid progression in a prospective longitudinal study. Movement Disorders 2015, 30, 407–411. [Google Scholar] [CrossRef]
- Cilia, R.; Tunesi, S.; Marotta, G.; Cereda, E.; Siri, C.; Tesei, S.; Zecchinelli, A.L.; Canesi, M.; Mariani, C.B.; Meucci, N.; et al. Survival and dementia in GBA-associated Parkinson's disease: The mutation matters. Annals of Neurology 2016, 80, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Hruska, K.S.; LaMarca, M.E.; Scott, C.R.; Sidransky, E. Gaucher disease: Mutation and polymorphism spectrum in the glucocerebrosidase gene (GBA). Human Mutation 2008, 29, 567–583. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Lee, C.Y.; Menozzi, E.; Schapira, A.H.V. Genetic variations in GBA1 and LRRK2 genes: Biochemical and clinical consequences in Parkinson disease. Frontiers in Neurology 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Samocha, K.E.; Robinson, E.B.; Sanders, S.J.; Stevens, C.; Sabo, A.; McGrath, L.M.; Kosmicki, J.A.; Rehnström, K.; Mallick, S.; Kirby, A.; et al. A framework for the interpretation of de novo mutation in human disease. Nature Genetics 2014, 46, 944–950. [Google Scholar] [CrossRef]
- Cornejo-Olivas, M.; Torres, L.; Velit-Salazar, M.R.; Inca-Martinez, M.; Mazzetti, P.; Cosentino, C.; Micheli, F.; Perandones, C.; Dieguez, E.; Raggio, V.; et al. Variable frequency of LRRK2 variants in the Latin American research consortium on the genetics of Parkinson's disease (LARGE-PD), a case of ancestry /692/617/375/1718 /631/208/1516 article. npj Parkinson's Disease 2017, 3. [Google Scholar] [CrossRef]
- Cresto, N.; Gardier, C.; Gubinelli, F.; Gaillard, M.C.; Liot, G.; West, A.B.; Brouillet, E. The unlikely partnership between LRRK2 and α-synuclein in Parkinson's disease. European Journal of Neuroscience 2019, 49, 339–363. [Google Scholar] [CrossRef]
- Esteves, A.R.; Swerdlow, R.H.; Cardoso, S.M. LRRK2, a puzzling protein: Insights into Parkinson's disease pathogenesis. Experimental Neurology 2014, 261, 206–216. [Google Scholar] [CrossRef]
- Herzig, M.C.; Kolly, C.; Persohn, E.; Theil, D.; Schweizer, T.; Hafner, T.; Stemmelen, C.; Troxler, T.J.; Schmid, P.; Danner, S.; et al. LRRK2 protein levels are determined by kinase function and are crucial for kidney and lung homeostasis in mice. Human Molecular Genetics 2011, 20, 4209–4223. [Google Scholar] [CrossRef]
- West, A.B. Achieving neuroprotection with LRRK2 kinase inhibitors in Parkinson disease. Experimental Neurology 2017, 298, 236–245. [Google Scholar] [CrossRef]
- Ozelius, L.J.; Senthil, G.; Saunders-Pullman, R.; Ohmann, E.; Deligtisch, A.; Tagliati, M.; Hunt, A.L.; Klein, C.; Henick, B.; Hailpern, S.M.; et al. LRRK2 G2019S as a cause of Parkinson's disease in Ashkenazi Jews [14]. New England Journal of Medicine 2006, 354, 424–425. [Google Scholar] [CrossRef]
- Ness, D.; Ren, Z.; Gardai, S.; Sharpnack, D.; Johnson, V.J.; Brennan, R.J.; Brigham, E.F.; Olaharski, A.J. Leucine-Rich Repeat Kinase 2 (LRRK2)-Deficient Rats Exhibit Renal Tubule Injury and Perturbations in Metabolic and Immunological Homeostasis. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Crook, A.; Jacobs, C.; Newton-John, T.; O’Shea, R.; McEwen, A. Genetic Counseling and Testing Practices for Late-Onset Neurodegenerative Disease: A Systematic Review. J. Neurol 2021. [Google Scholar] [CrossRef]
- Alcalay, R.N.; Kehoe, C.; Shorr, E.; Battista, R.; Hall, A.; Simuni, T.; Marder, K.; Wills, A.M.; Naito, A.; Beck, J.C.; et al. Genetic testing for Parkinson disease: current practice, knowledge, and attitudes among US and Canadian movement disorders specialists. Genetics in Medicine 2020, 22, 574–580. [Google Scholar] [CrossRef]
- Payne, K.; Walls, B.; Wojcieszek, J. Approach to Assessment of Parkinson Disease with Emphasis on Genetic Testing. Medical Clinics of North America 2019, 103, 1055–1075. [Google Scholar] [CrossRef]
- Blauwendraat, C.; Heilbron, K.; Vallerga, C.L.; Bandres-Ciga, S.; von Coelln, R.; Pihlstrøm, L.; Simón-Sánchez, J.; Schulte, C.; Sharma, M.; Krohn, L.; et al. Parkinson's disease age at onset genome-wide association study: Defining heritability, genetic loci, and α-synuclein mechanisms. Movement Disorders 2019, 34, 866–875. [Google Scholar] [CrossRef] [PubMed]
- Balint, E.; Ashkar, A.A. Remote hyperinflammation drives neurological disease via T-cell-mediated innate-like cytotoxicity. Cellular and Molecular Immunology 2021, 18, 1638–1640. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, P.; Shabbott, B.; Cortés, J.C. Motor control abnormalities in Parkinson's disease. Cold Spring Harbor Perspectives in Medicine 2012, 2. [Google Scholar] [CrossRef] [PubMed]
- Richter, F.; Subramaniam, S.R.; Magen, I.; Lee, P.; Hayes, J.; Attar, A.; Zhu, C.; Franich, N.R.; Bove, N.; De La Rosa, K.; et al. A Molecular Tweezer Ameliorates Motor Deficits in Mice Overexpressing α-Synuclein. Neurotherapeutics 2017, 14, 1107–1119. [Google Scholar] [CrossRef]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-motor features of Parkinson disease. Nature Reviews Neuroscience 2017, 18, 435–450. [Google Scholar] [CrossRef]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson's disease. Parkinsonism and Related Disorders 2016, 22, S119–S122. [Google Scholar] [CrossRef]
- Cruz Hernández, J.C.; Bracko, O.; Kersbergen, C.J.; Muse, V.; Haft-Javaherian, M.; Berg, M.; Park, L.; Vinarcsik, L.K.; Ivasyk, I.; Rivera, D.A.; et al. Neutrophil adhesion in brain capillaries reduces cortical blood flow and impairs memory function in Alzheimer’s disease mouse models. Nature Neuroscience 2019, 22, 413–420. [Google Scholar] [CrossRef] [PubMed]
- De Strooper, B.; Karran, E. The Cellular Phase of Alzheimer's Disease. Cell 2016, 164, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Williams, U.; Bandmann, O.; Walker, R. Parkinson’s disease in sub-Saharan Africa: A review of epidemiology, genetics and access to care. J Mov Disord 2018, 11, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Chiriches, C.; Guillen, N.; Rokicki, M.; Guy, C.; Mian, A.; Ottmann, O.G.; Ruthardt, M. Subtractive Interaction Proteomics Reveal a Network of Signaling Pathways Activated By an Oncogenic Transcription Factor in High Risk AML. Blood 2018, 132, 3917–3917. [Google Scholar] [CrossRef]
- Ghanouni, P.; Pauly, K.B.; Elias, W.J.; Henderson, J.; Sheehan, J.; Monteith, S.; Wintermark, M. Transcranial MRI-guided focused ultrasound: A review of the technologic and neurologic applications. American Journal of Roentgenology 2015, 205, 150–159. [Google Scholar] [CrossRef]
- Lehman, V.T.; Lee, K.H.; Klassen, B.T.; Blezek, D.J.; Goyal, A.; Shah, B.R.; Gorny, K.R.; Huston, J., III; Kaufmann, T.J. MRI and tractography techniques to localize the ventral intermediate nucleus and dentatorubrothalamic tract for deep brain stimulation and MR-guided focused ultrasound: A narrative review and update. Neurosurgical Focus 2020, 49. [Google Scholar] [CrossRef]
- Xu, J.P. Progress in the stereotaxic technics. Chinese Journal of Neurology and Psychiatry 1983, 16, 60–62. [Google Scholar]
- Guilhon, E.; Voisin, P.; de Zwart, J.A.; Quesson, B.; Salomir, R.; Maurange, C.; Bouchaud, V.; Smirnov, P.; de Verneuil, H.; Vekris, A.; et al. Spatial and temporal control of transgene expression in vivo using a heat-sensitive promoter and MRI-guided focused ultrasound. Journal of Gene Medicine 2003, 5, 333–342. [Google Scholar] [CrossRef]
- Long, L.; Cai, X.; Guo, R.; Wang, P.; Wu, L.; Yin, T.; Liao, S.; Lu, Z. Treatment of Parkinson's disease in rats by Nrf2 transfection using MRI-guided focused ultrasound delivery of nanomicrobubbles. Biochemical and Biophysical Research Communications 2017, 482, 75–80. [Google Scholar] [CrossRef]
- Grüll, H.; Langereis, S. Hyperthermia-triggered drug delivery from temperature-sensitive liposomes using MRI-guided high intensity focused ultrasound. Journal of Controlled Release 2012, 161, 317–327. [Google Scholar] [CrossRef]
- Wang, X.; Xiong, Y.; Lin, J.; Lou, X. Target Selection for Magnetic Resonance-Guided Focused Ultrasound in the Treatment of Parkinson's Disease. Journal of Magnetic Resonance Imaging 2022, 56, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Loesch, D.P.; Horimoto, A.R.V.R.; Heilbron, K.; Sarihan, E.I.; Inca-Martinez, M.; Mason, E.; Cornejo-Olivas, M.; Torres, L.; Mazzetti, P.; Cosentino, C.; et al. Characterizing the Genetic Architecture of Parkinson's Disease in Latinos. Annals of Neurology 2021, 90, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Logroscino, G.; Sesso, H.D.; Paffenbarger Jr, R.S.; Lee, I.M. Physical activity and risk of Parkinson's disease: A prospective cohort study. Journal of Neurology, Neurosurgery and Psychiatry 2006, 77, 1318–1322. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vicente, M.; Talloczy, Z.; Kaushik, S.; Massey, A.C.; Mazzulli, J.; Mosharov, E.V.; Hodara, R.; Fredenburg, R.; Wu, D.C.; Follenzi, A.; et al. Dopamine-modified α-synuclein blocks chaperone-mediated autophagy. Journal of Clinical Investigation 2008, 118, 777–778. [Google Scholar] [CrossRef] [PubMed]
- Gallay, M.N.; Moser, D.; Rossi, F.; Magara, A.E.; Strasser, M.; Bühler, R.; Kowalski, M.; Pourtehrani, P.; Dragalina, C.; Federau, C.; et al. MRgFUS Pallidothalamic Tractotomy for Chronic Therapy-Resistant Parkinson's Disease in 51 Consecutive Patients: Single Center Experience. Frontiers in Surgery 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.S.; Woodworth, G.F.; Vujaskovic, Z.; Mishra, M.V. Radiosensitization of high-grade gliomas through induced hyperthermia: Review of clinical experience and the potential role of MR-guided focused ultrasound. Radiotherapy and Oncology 2020, 142, 43–51. [Google Scholar] [CrossRef]
- Legon, W.; Sato, T.F.; Opitz, A.; Mueller, J.; Barbour, A.; Williams, A.; Tyler, W.J. Transcranial focused ultrasound modulates the activity of primary somatosensory cortex in humans. Nature Neuroscience 2014, 17, 322–329. [Google Scholar] [CrossRef]
- Schneeberger, A.; Tierney, L.; Mandler, M. Active immunization therapies for Parkinson's disease and multiple system atrophy. Movement Disorders 2016, 31, 214–224. [Google Scholar] [CrossRef]
- Iwaki, H.; Blauwendraat, C.; Leonard, H.L.; Kim, J.J.; Liu, G.; Maple-Grødem, J.; Corvol, J.C.; Pihlstrøm, L.; van Nimwegen, M.; Hutten, S.J.; et al. Genomewide association study of Parkinson's disease clinical biomarkers in 12 longitudinal patients' cohorts. Movement Disorders 2019, 34, 1839–1850. [Google Scholar] [CrossRef]
- Bracko, O.; Njiru, B.N.; Swallow, M.; Ali, M.; Haft-Javaherian, M.; Schaffer, C.B. Increasing cerebral blood flow improves cognition into late stages in Alzheimer’s disease mice. Journal of Cerebral Blood Flow and Metabolism 2020, 40, 1441–1452. [Google Scholar] [CrossRef]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, preparation, and applications. Nanoscale Research Letters 2013, 8. [Google Scholar] [CrossRef]
- Awasthi, R.; Roseblade, A.; Hansbro, P.M.; Rathbone, M.J.; Dua, K.; Bebawy, M. Nanoparticles in cancer treatment: Opportunities and obstacles. Current Drug Targets 2018, 19, 1696–1709. [Google Scholar] [CrossRef] [PubMed]
- Bozzuto, G.; Molinari, A. Liposomes as nanomedical devices. International Journal of Nanomedicine 2015, 10, 975–999. [Google Scholar] [CrossRef] [PubMed]
- Chandra Bhatt, P.; Srivastava, P.; Pandey, P.; Khan, W.; Panda, B.P. Nose to brain delivery of astaxanthin-loaded solid lipid nanoparticles: Fabrication, radio labeling, optimization and biological studies. RSC Advances 2016, 6, 10001–10010. [Google Scholar] [CrossRef]
- Dilnawaz, F.; Singh, A.; Mewar, S.; Sharma, U.; Jagannathan, N.R.; Sahoo, S.K. The transport of non-surfactant based paclitaxel loaded magnetic nanoparticles across the blood brain barrier in a rat model. Biomaterials 2012, 33, 2936–2951. [Google Scholar] [CrossRef] [PubMed]
- Dudhipala, N.; Gorre, T. Neuroprotective effect of ropinirole lipid nanoparticles enriched hydrogel for parkinson’s disease: In vitro, ex vivo, pharmacokinetic and pharmacodynamic evaluation. Pharmaceutics 2020, 12. [Google Scholar] [CrossRef]
- Gelperina, S.; Maksimenko, O.; Khalansky, A.; Vanchugova, L.; Shipulo, E.; Abbasova, K.; Berdiev, R.; Wohlfart, S.; Chepurnova, N.; Kreuter, J. Drug delivery to the brain using surfactant-coated poly(lactide-co-glycolide) nanoparticles: Influence of the formulation parameters. European Journal of Pharmaceutics and Biopharmaceutics 2010, 74, 157–163. [Google Scholar] [CrossRef]
- Gu, Z.; Chen, H.; Zhao, H.; Yang, W.; Song, Y.; Li, X.; Wang, Y.; Du, D.; Liao, H.; Pan, W.; et al. New insight into brain disease therapy: nanomedicines-crossing blood–brain barrier and extracellular space for drug delivery. Expert Opinion on Drug Delivery 2022, 19, 1618–1635. [Google Scholar] [CrossRef]
- Duan, Y.; Dhar, A.; Patel, C.; Khimani, M.; Neogi, S.; Sharma, P.; Siva Kumar, N.; Vekariya, R.L. A brief review on solid lipid nanoparticles: Part and parcel of contemporary drug delivery systems. RSC Advances 2020, 10, 26777–26791. [Google Scholar] [CrossRef]
- Kundu, P.; Das, M.; Tripathy, K.; Sahoo, S.K. Delivery of Dual Drug Loaded Lipid Based Nanoparticles across the Blood-Brain Barrier Impart Enhanced Neuroprotection in a Rotenone Induced Mouse Model of Parkinson's Disease. ACS Chemical Neuroscience 2016, 7, 1658–1670. [Google Scholar] [CrossRef]
- Fong, C.; Le, T.; Drummond, C.J. Lyotropic liquid crystal engineering–ordered nanostructured small molecule amphiphile self-assembly materials by design. Chemical Society Reviews 2012, 41, 1297–1322. [Google Scholar] [CrossRef] [PubMed]
- Etheridge, M.L.; Campbell, S.A.; Erdman, A.G.; Haynes, C.L.; Wolf, S.M.; McCullough, J. The big picture on nanomedicine: The state of investigational and approved nanomedicine products. Nanomedicine: Nanotechnology, Biology, and Medicine 2013, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Abrahao, A.; Meng, Y.; Llinas, M.; Huang, Y.; Hamani, C.; Mainprize, T.; Aubert, I.; Heyn, C.; Black, S.E.; Hynynen, K.; et al. First-in-human trial of blood–brain barrier opening in amyotrophic lateral sclerosis using MR-guided focused ultrasound. Nature Communications 2019, 10. [Google Scholar] [CrossRef]
- Bond, A.E.; Shah, B.B.; Huss, D.S.; Dallapiazza, R.F.; Warren, A.; Harrison, M.B.; Sperling, S.A.; Wang, X.Q.; Gwinn, R.; Witt, J.; et al. Safety and efficacy of focused ultrasound thalamotomy for patients with medication-refractory, tremor-dominant Parkinson disease a randomized Clinical trial. JAMA Neurology 2017, 74, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Dallapiazza, R.F.; Timbie, K.F.; Holmberg, S.; Gatesman, J.; Lopes, M.B.; Price, R.J.; Miller, G.W.; Elias, W.J. Noninvasive neuromodulation and thalamic mapping with low-intensity focused ultrasound. Journal of Neurosurgery 2018, 128, 875–884. [Google Scholar] [CrossRef]
- Jung, N.Y.; Park, C.K.; Kim, M.; Lee, P.H.; Sohn, Y.H.; Chang, J.W. The efficacy and limits of magnetic resonance–guided focused ultrasound pallidotomy for Parkinson’s disease: A Phase I clinical trial. Journal of Neurosurgery 2019, 1306, 1853–1861. [Google Scholar] [CrossRef]
- Elias, W.J.; Lipsman, N.; Ondo, W.G.; Ghanouni, P.; Kim, Y.G.; Lee, W.; Schwartz, M.; Hynynen, K.; Lozano, A.M.; Shah, B.B.; et al. A randomized trial of focused ultrasound thalamotomy for essential tremor. New England Journal of Medicine 2016, 375, 730–739. [Google Scholar] [CrossRef]
- Gasca-Salas, C.; Fernández-Rodríguez, B.; Pineda-Pardo, J.A.; Rodríguez-Rojas, R.; Obeso, I.; Hernández-Fernández, F.; del Álamo, M.; Mata, D.; Guida, P.; Ordás-Bandera, C.; et al. Blood-brain barrier opening with focused ultrasound in Parkinson’s disease dementia. Nature Communications 2021, 12. [Google Scholar] [CrossRef]
- Xiong, Y.; Lin, J.; Pan, L.; Zong, R.; Bian, X.; Duan, C.; Zhang, D.; Lou, X. Pretherapeutic functional connectivity of tractography-based targeting of the ventral intermediate nucleus for predicting tremor response in patients with Parkinson's disease after thalamotomy with MRI-guided focused ultrasound. Journal of Neurosurgery 2022, 137, 1135–1144. [Google Scholar] [CrossRef]
- Burgess, A.; Dubey, S.; Yeung, S.; Hough, O.; Eterman, N.; Aubert, I.; Hynynen, K. Alzheimer disease in a mouse model: Mr imaging-guided focused ultrasound targeted to the hippocampus opens the blood-brain barrier and improves pathologic abnormalities and behavior. Radiology 2014, 273, 736–745. [Google Scholar] [CrossRef]
- Lee, K.S.; Clennell, B.; Steward, T.G.J.; Gialeli, A.; Cordero-Llana, O.; Whitcomb, D.J. Focused Ultrasound Stimulation as a Neuromodulatory Tool for Parkinson’s Disease: A Scoping Review. Brain Sciences 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- Fry, F.J.; Ades, H.W.; Fry, W.J. Production of reversible changes in the central nervous system by ultrasound. Science 1958, 127, 83–84. [Google Scholar] [CrossRef] [PubMed]
- Krasovitski, B.; Frenkel, V.; Shoham, S.; Kimmel, E. Intramembrane cavitation as a unifying mechanism for ultrasound-induced bioeffects. Proceedings of the National Academy of Sciences of the United States of America 2011, 108, 3258–3263. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Fernández, R.; Rodríguez-Rojas, R.; del Álamo, M.; Hernández-Fernández, F.; Pineda-Pardo, J.A.; Dileone, M.; Alonso-Frech, F.; Foffani, G.; Obeso, I.; Gasca-Salas, C.; et al. Focused ultrasound subthalamotomy in patients with asymmetric Parkinson's disease: a pilot study. The Lancet Neurology 2018, 17, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Moosa, S.; Martínez-Fernández, R.; Elias, W.J.; del Alamo, M.; Eisenberg, H.M.; Fishman, P.S. The role of high-intensity focused ultrasound as a symptomatic treatment for Parkinson's disease. Movement Disorders 2019, 34, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Tyler, W.J.; Tufail, Y.; Finsterwald, M.; Tauchmann, M.L.; Olson, E.J.; Majestic, C. Remote excitation of neuronal circuits using low-intensity, low-frequency ultrasound. PLoS ONE 2008, 3. [Google Scholar] [CrossRef]
- Au, K.L.K.; Wong, J.K.; Tsuboi, T.; Eisinger, R.S.; Moore, K.; Lemos Melo Lobo Jofili Lopes, J. Globus Pallidus Internus (GPi) deep brain stimulation for Parkinson's disease: expert review and commentary. Neurol Ther 2021, 10. [Google Scholar] [CrossRef]
- Ligaard, J.; Sannæs, J.; Pihlstrøm, L. Deep brain stimulation and genetic variability in Parkinson’s disease: a review of the literature. npj Parkinson's Disease 2019, 5. [Google Scholar] [CrossRef]
- Odekerken, V.J.J.; van Laar, T.; Staal, M.J.; Mosch, A.; Hoffmann, C.F.E.; Nijssen, P.C.G.; Beute, G.N.; van Vugt, J.P.P.; Lenders, M.W.P.M.; Contarino, M.F.; et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson's disease (NSTAPS study): A randomised controlled trial. The Lancet Neurology 2013, 12, 37–44. [Google Scholar] [CrossRef]
- Tisch, S.; Zrinzo, L.; Limousin, P.; Bhatia, K.P.; Quinn, N.; Ashkan, K.; Hariz, M. Effect of electrode contact location on clinical efficacy of pallidal deep brain stimulation in primary generalised dystonia. Journal of Neurology, Neurosurgery and Psychiatry 2007, 78, 1314–1319. [Google Scholar] [CrossRef]
- You, Z.; Wu, Y.Y.; Wu, R.; Xu, Z.X.; Wu, X.; Wang, X.P. Efforts of subthalamic nucleus deep brain stimulation on cognitive spectrum: From explicit to implicit changes in the patients with Parkinson's disease for 1 year. CNS Neuroscience and Therapeutics 2020, 26, 972–980. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Charting the Evolution: Milestones in Parkinson's Disease Research from 1800 to Present. Adopted and modified from [1].
Figure 1.
Charting the Evolution: Milestones in Parkinson's Disease Research from 1800 to Present. Adopted and modified from [1].
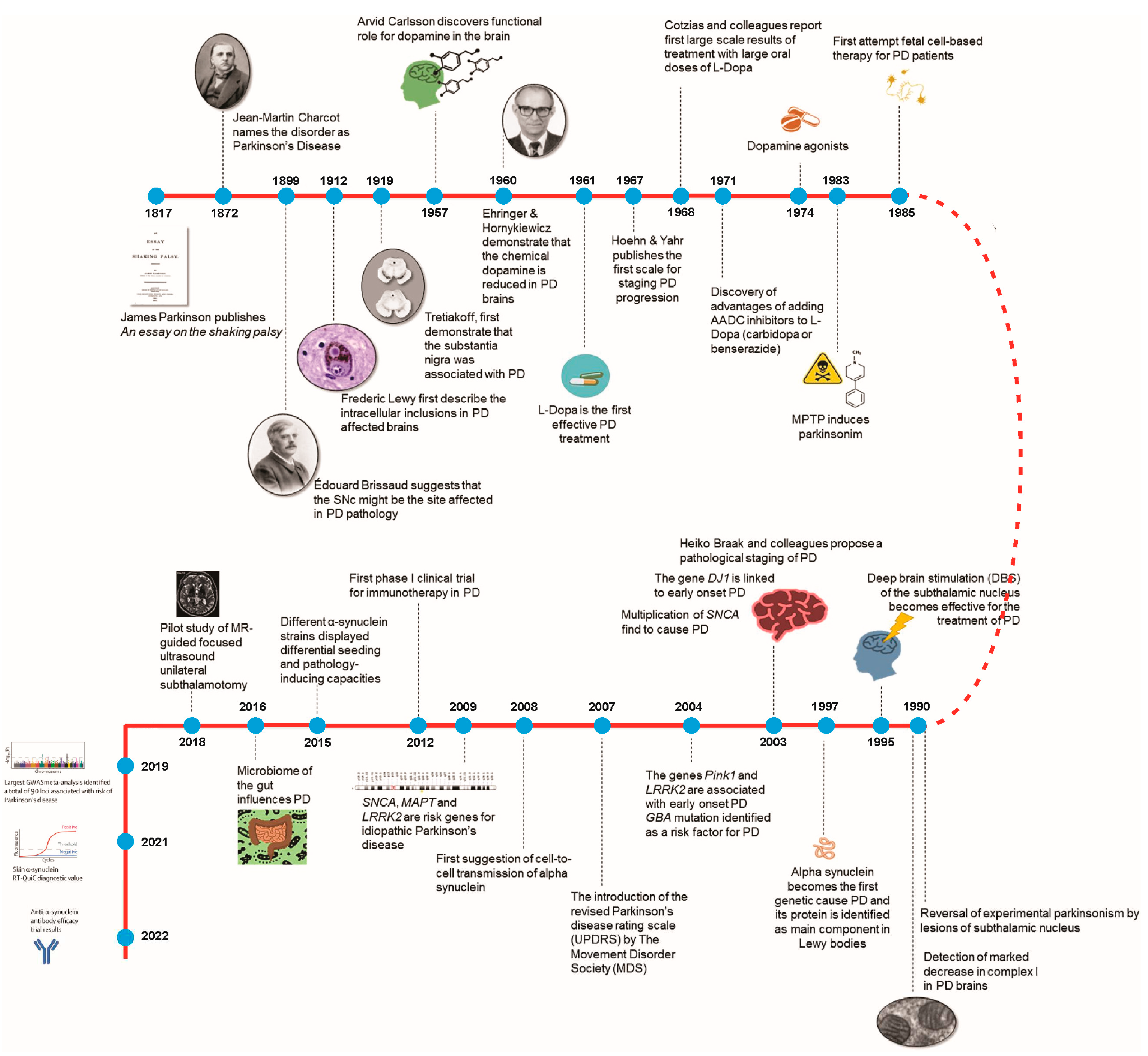
Figure 2.
Navigating the Spectrum: Illustrating Motor and Non-Motor Symptoms of Parkinson's Disease.
Figure 2.
Navigating the Spectrum: Illustrating Motor and Non-Motor Symptoms of Parkinson's Disease.
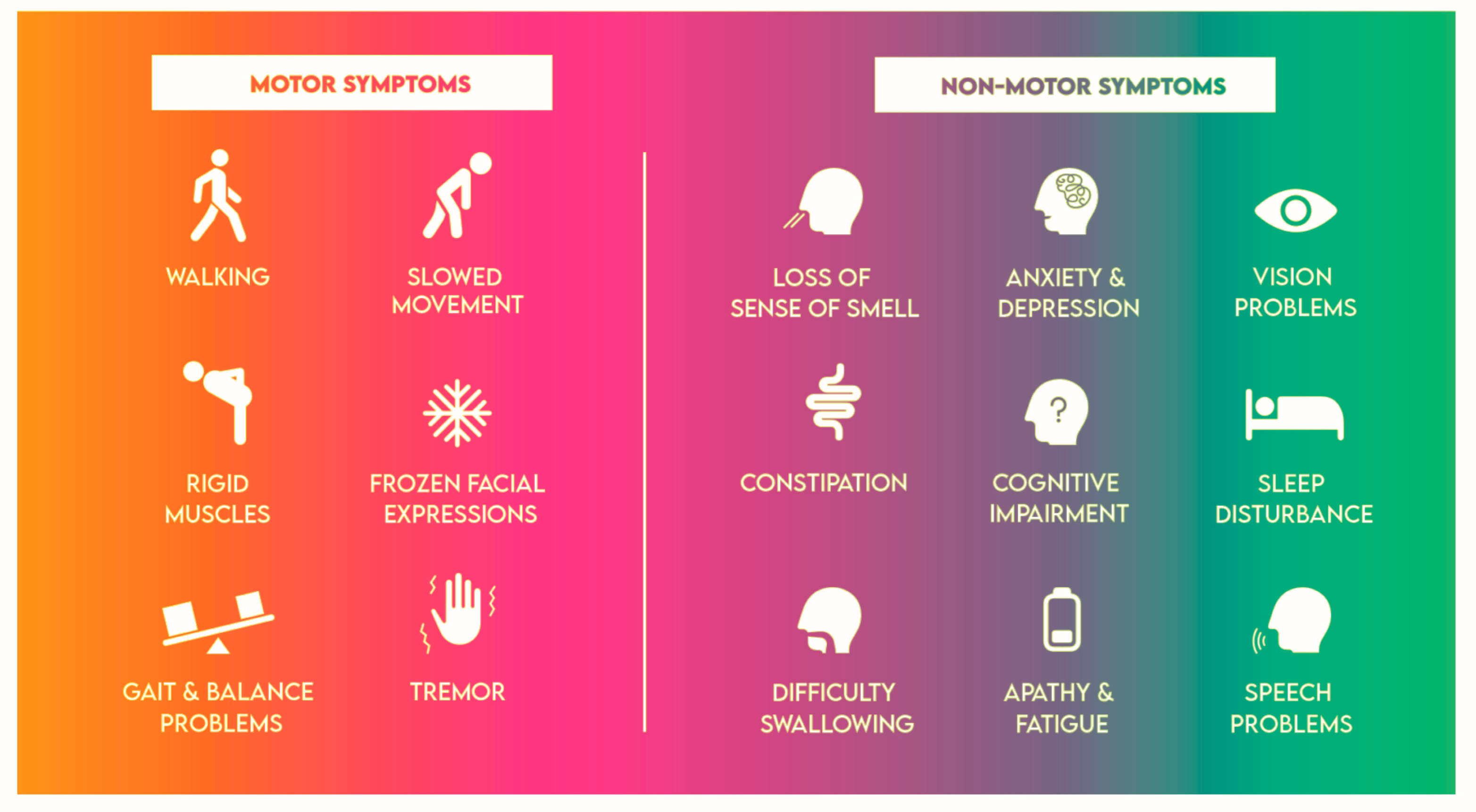
Figure 3.
Comprehensive Overview: Summarizing Assessment Techniques for Parkinson's Disease (PD).
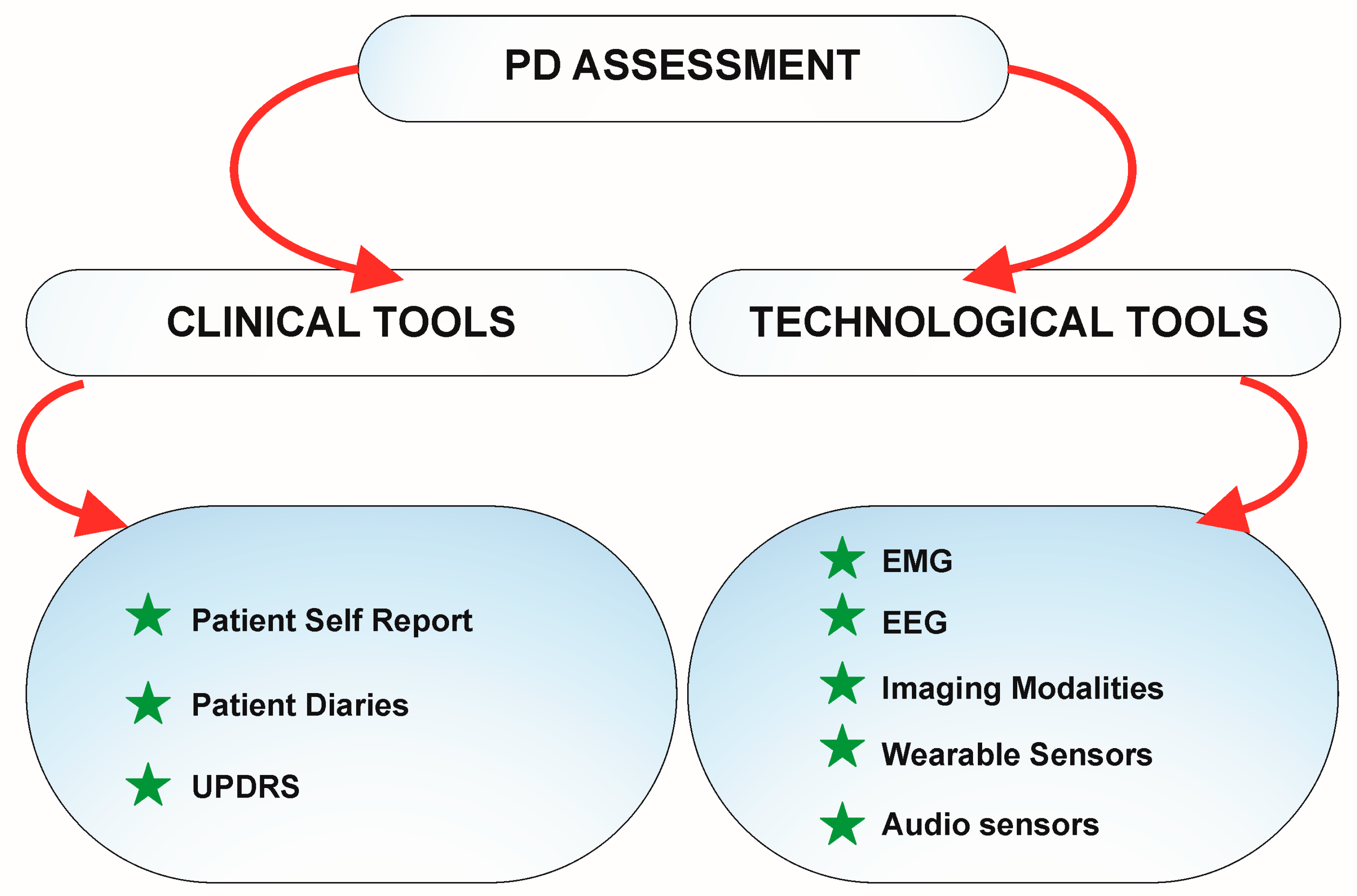
Figure 4.
Exploring the Frontier: Investigating Drug Delivery Systems for Advancing Parkinson's Disease Treatment.
Figure 4.
Exploring the Frontier: Investigating Drug Delivery Systems for Advancing Parkinson's Disease Treatment.
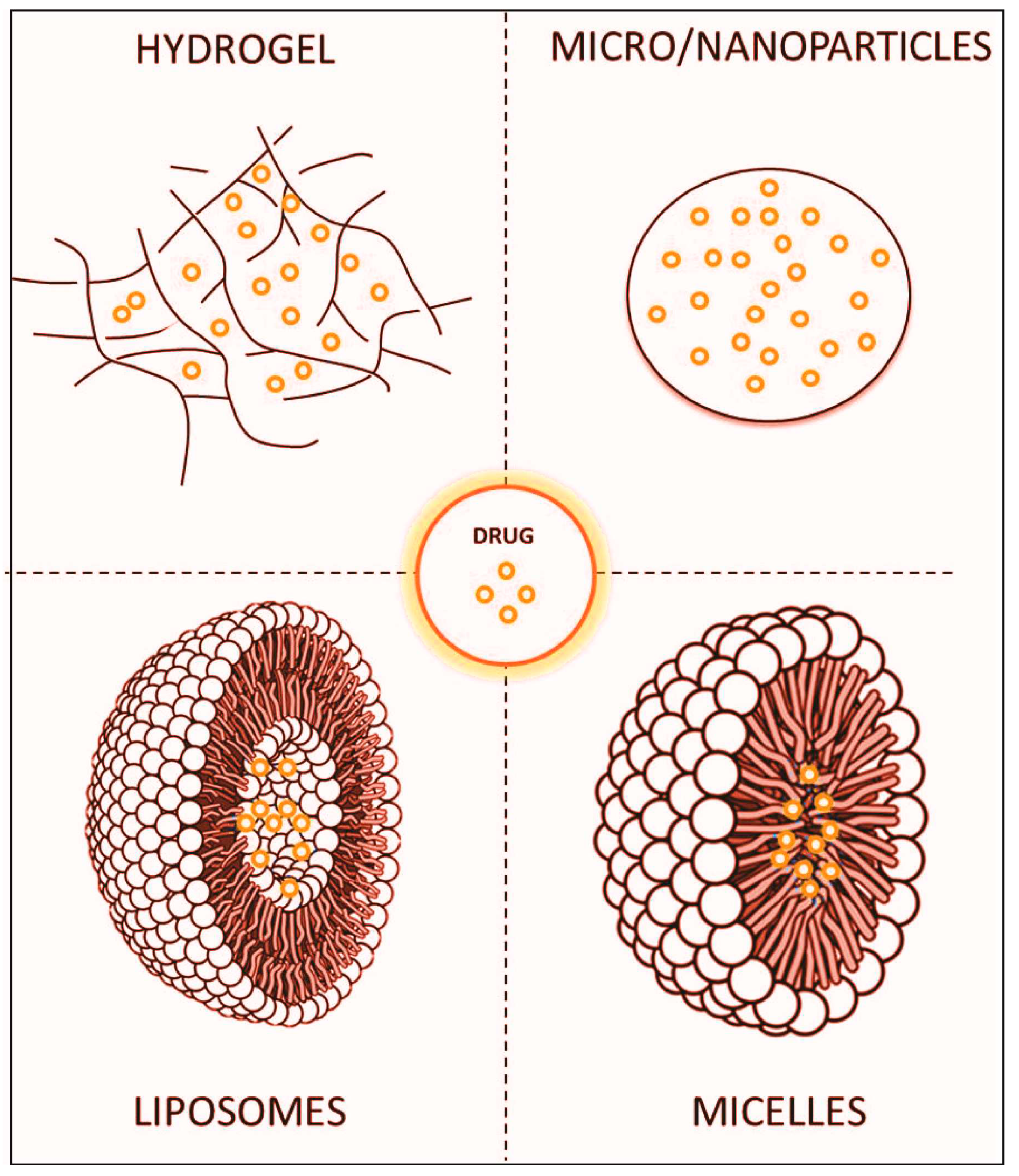
Figure 5.
Comparing Basal Ganglia Circuits: Normal, PD-Affected, and Theoretical Modulation via Focused Ultrasound STN Stimulation. Colors indicate excitatory (green) and inhibitory (red) pathways. Line thickness and style denote signaling strength. Red cross marks SNpc neuron degeneration, while the yellow star highlights STN stimulation. Abbreviations: GPi = globus pallidus internus; GPe = globus pallidus externus; SNpc = substantia nigra pars compacta; SNpr = substantia nigra pars reticulata; STN = subthalamic nucleus.
Figure 5.
Comparing Basal Ganglia Circuits: Normal, PD-Affected, and Theoretical Modulation via Focused Ultrasound STN Stimulation. Colors indicate excitatory (green) and inhibitory (red) pathways. Line thickness and style denote signaling strength. Red cross marks SNpc neuron degeneration, while the yellow star highlights STN stimulation. Abbreviations: GPi = globus pallidus internus; GPe = globus pallidus externus; SNpc = substantia nigra pars compacta; SNpr = substantia nigra pars reticulata; STN = subthalamic nucleus.
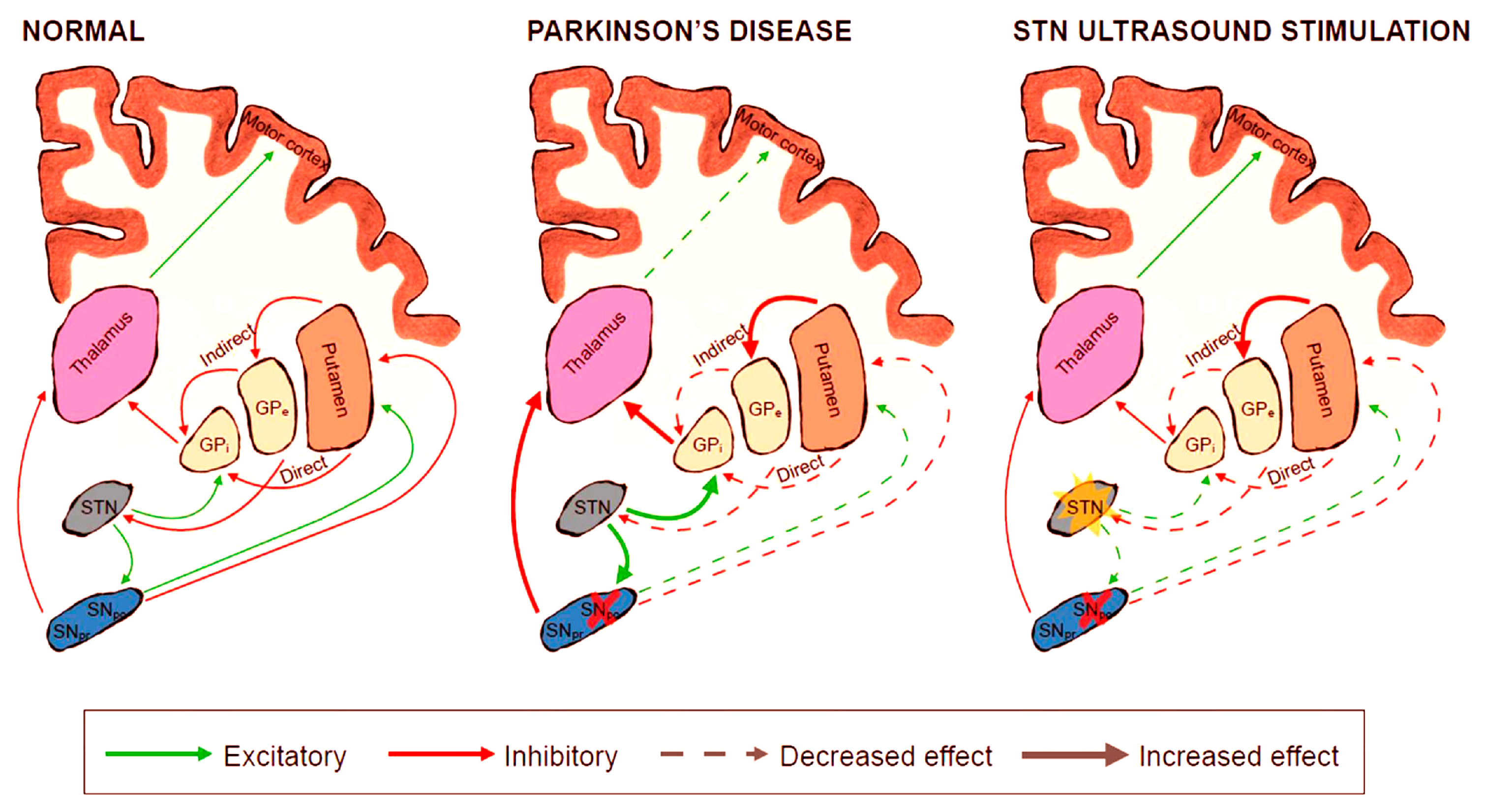
Figure 6.
Beyond Deep Brain Stimulation: Emerging Interest in Non-Invasive and Optogenetic Stimulation Modalities for Parkinson's Disease. Non-invasive electrical stimulation, achieved through temporal interference of electric fields, offers localized stimulation. Optogenetic stimulation involves delivering opsins to specific neurons, enabling light-sensitive channel expression for direct light-based stimulation. Alternatively, certain brain-delivered nanoparticles can convert extracranial infrared light to visible light, facilitating non-invasive optogenetic neuron stimulation. While electrical stimulation tends to be non-specific, optogenetic approaches hold promise for precise neuron targeting. Figure adopted from [2].
Figure 6.
Beyond Deep Brain Stimulation: Emerging Interest in Non-Invasive and Optogenetic Stimulation Modalities for Parkinson's Disease. Non-invasive electrical stimulation, achieved through temporal interference of electric fields, offers localized stimulation. Optogenetic stimulation involves delivering opsins to specific neurons, enabling light-sensitive channel expression for direct light-based stimulation. Alternatively, certain brain-delivered nanoparticles can convert extracranial infrared light to visible light, facilitating non-invasive optogenetic neuron stimulation. While electrical stimulation tends to be non-specific, optogenetic approaches hold promise for precise neuron targeting. Figure adopted from [2].
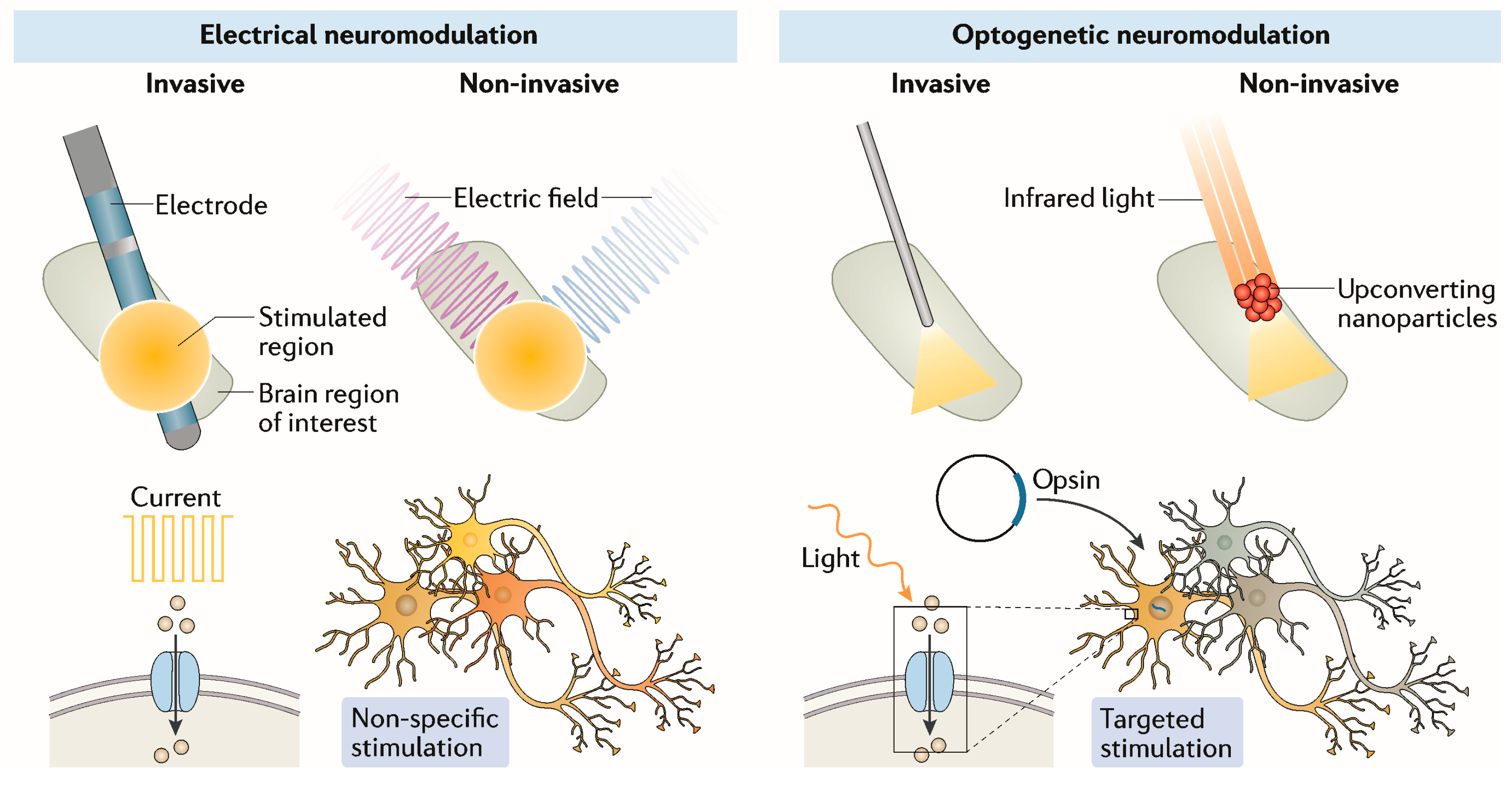

Table 1.
List of genes reported to be linked with Parkinson disease. Data for PD genes adopted from [76].
Table 1.
List of genes reported to be linked with Parkinson disease. Data for PD genes adopted from [76].
| GENE | Year of Discovery | Reported Variants | Frequency | Inheritance | Confidence as a PD Gene |
|---|---|---|---|---|---|
| SNCA * | 1997, 2003 | Missense or multiplication | Very rare | Dominant | Very high |
| PRKN * | 1998 | Missense or loss of function | Rare | Recessive | Very high |
| UCHL1 | 1998 | Missense | Unclear | Dominant | Low |
| PARK7 * | 2003 | Missense | Very rare | Recessive | Very high |
| LRRK2 * | 2004 | Missense | Common | Dominant | Very high |
| PINK1 * | 2004 | Missense or loss of function | Rare | Recessive | Very high |
| POLG | 2004 | Missense or loss of function | Rare | Dominant | High |
| HTRA2 | 2005 | Missense | Unclear | Dominant | Low |
| ATP13A2 * | 2006 | Missense or loss of function | Very rare | Recessive | Very high |
| FBXO7 * | 2008 | Missense | Very rare | Recessive | Very high |
| GIGYF2 | 2008 | Missense | Unclear | Dominant | Low |
| GBA * | 2009 | Missense or loss of function | Common | Dominant (incomplete penetrance) | Very high |
| PLA2G6 * | 2009 | Missense or loss of function | Rare | Recessive | Very high |
| EIF4G1 | 2011 | Missense | Unclear | Dominant | Low |
| VPS35 * | 2011 | Missense | Very rare | Dominant | Very high |
| DNAJC6 | 2012 | Missense or loss of function | Very rare | Recessive | High |
| SYNJ1 | 2013 | Missense or loss of function | Very rare | Recessive | High |
| DNAJC13 | 2014 | Missense | Unclear | Dominant | Low |
| TMEM230 | 2016 | Missense | Unclear | Dominant | Low |
| VPS13C | 2016 | Missense or loss of function | Rare | Recessive | High |
| LRP10 | 2018 | Missense or loss of function | Unclear | Dominant | Low |
| NUS1 | 2018 | Missense | Unclear | Recessive | Low |
| COL6A3 | 2022 | Missense | Rare | Dominant | High |
| TH | 2022 | Missense | Unclear | Dominant | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



