
Submitted:
08 March 2025
Posted:
10 March 2025
You are already at the latest version
Abstract
Transformative neuropathology is redefining human brain research by integrating foundational descriptive pathology with advanced methodologies to drive discoveries that inform diagnostics, therapeutics, and disease prevention. These approaches, spanning multi-omics studies and machine learning applications, enable the identification of biomarkers, therapeutic targets, and complex disease patterns through comprehensive analyses of postmortem human brain tissue. Yet critical challenges, including sustainability of brain banks, expanding donor participation, strengthening training pipelines, enabling rapid autopsies, and supporting collaborative platforms. Innovations in digital pathology, tissue quality enhancement, harmonized data standards, and machine learning integration offer groundbreaking opportunities to accelerate research in aging and neurodegeneration. Lessons from neuroimaging, regarding progress in establishing common data frameworks and multi-site collaborations, offer a valuable roadmap for streamlining innovations. In this Perspective, we outline actionable solutions to leverage existing resources, envision future opportunities, and advance collaboration to drive translational discoveries and safeguard the sustainability of brain banks underpinning transformative neuropathology.
Keywords:
neuropathology
; spatial biology
; omics
; digital pathology
; machine learning
; biomarkers
Introduction
The integration of advanced multi-omics, digital pathology, and machine learning with traditional neuropathology is transforming our understanding of brain diseases with profound implications for diagnostics, therapeutics, and prevention. What was once the domain of science fiction is now our tangible reality with: large-scale -omics studies of human brain tissue uncovering novel biomarkers and therapeutic targets, high-throughput digital scanning of microscope slides enabling remote viewing and computerized analysis of spatial biology patterns of disease, and greater availability of neuroimaging and fluid biomarkers to unveil diagnostic and prognostic neuropathologic alterations. Moreover, the high computational capacity provided by machine learning is driving unprecedented insights by enabling prediction, discovery, and characterization of subtle patterns across expansive -omics and whole-slide image microscopy datasets. With the goal to explore the significant progress in the study of postmortem human brain tissue, moving from the theoretical potential of applying advanced techniques to the practical reality of modern science in the fields of aging and neurodegenerative diseases, a workshop convened at Banbury Center hosted by Cold Spring Harbor Laboratory. A convergence of expertise in brain banking, neuropathology, high dimensional molecular data (-omics), digital pathology, neuroimaging, computational methods, and machine learning was gathered to discuss approaches to optimize and enhance existing workflows and infrastructure in a rapidly evolving biomedical landscape. We report workshop outcomes to promote new biomedical discoveries and introduce the concept of transformative neuropathology (Figure 1), a term we use to describe the integration of foundational descriptive pathology with advanced technologies and methodologies. By defining this paradigm shift, we aim to inspire a reimagining of neuropathology’s role in driving innovation and addressing critical challenges in brain disease research. We structure this Perspective by identifying key challenges facing the realm of research-based biorepositories of human brain tissue that can be utilized by as a springboard to inspire future investigations and funding.
Prospective Brain Collections & Increasing Representation for Broader Insights
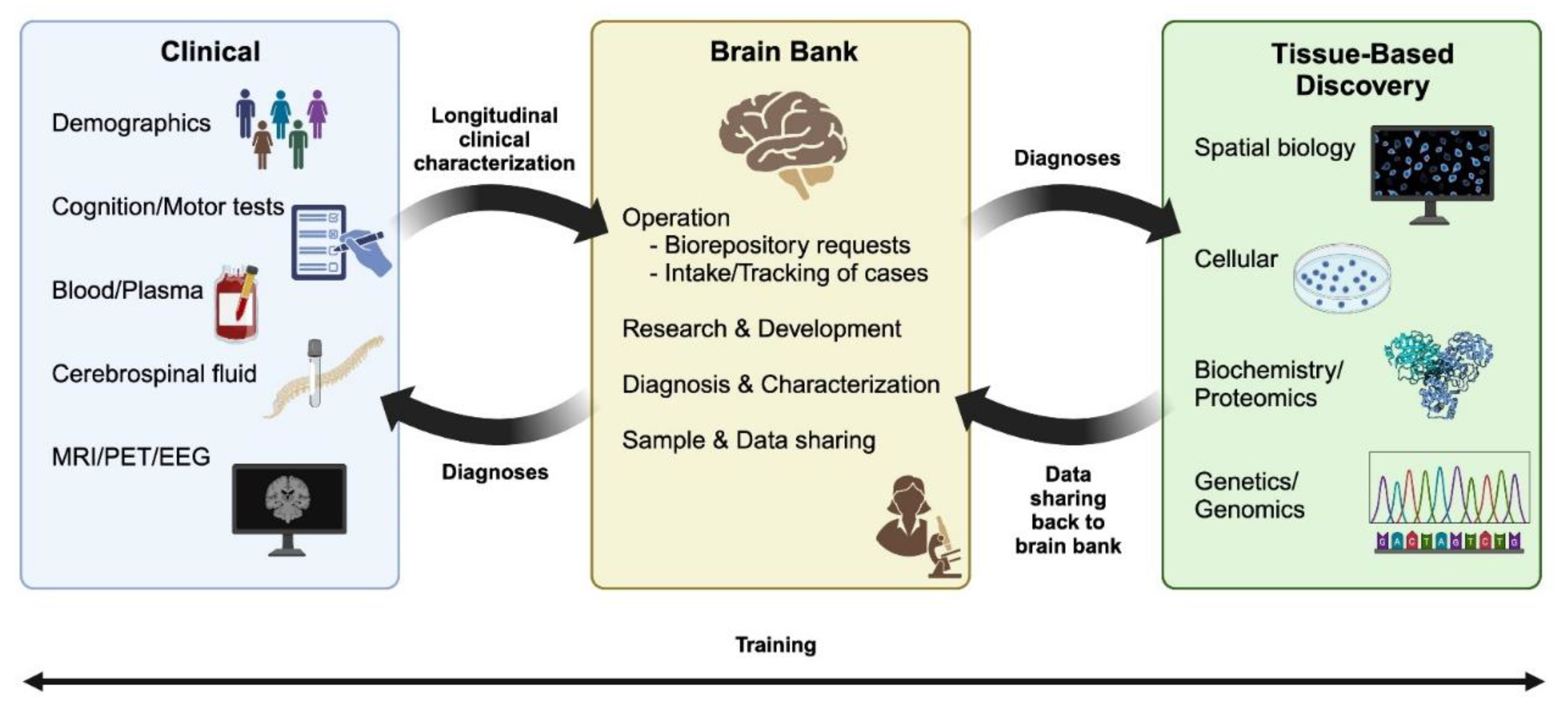
Brain banks, collections, or libraries can serve many functions, such as providing closure to donors’ families through diagnostic evaluation, supporting transformative research, providing educational opportunities, and offering training opportunities in neuropathology (Figure 2) [1]. The careful preservation and archiving of brains from individuals who consented for donation by skilled brain bank staff ensure the availability of high-quality tissue, critical to unraveling the complexities of the human brain [2]. This essential work not only provides the foundation for promoting scientific discovery but also strengthens the collaborative framework needed to tackle critical questions in in aging and neurodegenerative research [1,3]. As the biomedical field continues to move from passive recruitment to active recruitment, expanding brain donor participation across different backgrounds (i.e., economic status, aging across lifespan, cognitive and motor health, geographic ancestry) becomes even more critical (see Box 1 with reference to subsection in line with text).
Future-facing models of long-term research partnerships where engagement spans decades prior to brain donation are exemplified by the Oxford Project to Investigate Memory and Ageing [4], Lothian Birth Cohort 1936 [5], Mayo Clinic Study of Aging [6], Einstein Aging Study [7], Minority Aging Research Study [8], and Brain & Body Donation Program [9]. Recruiting individuals across the aging spectrum may require intentional engagement strategies, such as engaging care partners of study participants already enrolled in longitudinal studies, to ensure a minimum set of consistent antemortem measures (1.1). Healthy aging brains provide baseline understanding of age and sex differences in neuroanatomic structures that are key to the development of tissue-based atlases. Partnership with medical examiners could further expand donor recruitment across populations with limited research participation [1,10-12], especially helping to define the age range of histologic changes and their relevance as a control for young-onset disorders (e.g. frontotemporal dementia, Alzheimer’s in individuals <65 years [13,14]). Partnerships with ambassadors from the lay public and with clinicians through multi-component program projects further provides mutual opportunities to receive and share knowledge to enhance healthy brain aging [15,16] (1.2).
Building Capacity for Expertise in Neuropathology and Informatics
Historically, brain bank leadership required formal medical training. However, with fewer neuropathologists entering the field, in addition to the need to engage junior neuropathology experts in aging and neurodegenerative research, it has become necessary to expand the range of trained professionals who can develop and manage a brain bank (Box 2) [17]. The operations required to facilitate brain donation and tissue provision are complex and involve unique expertise that may take years to acquire/master. Neuropathology expertise requires extensive training as an MD or PhD to enable systematic evaluation of age-related histologic changes and a full range of neurologic conditions including neurodegenerative diseases, cerebrovascular lesions, demyelinating and other neuroinflammatory conditions, central nervous system infections, as well as neoplastic, metabolic and neurodevelopmental disorders depending upon the brain bank’s focus. As diagnosis may be a small fraction of the abundance of tasks involved in operations, it is imperative to have knowledge on research methodologies and the scientific process when leading a brain bank. Emphasis on training pipelines provided across brain bank networks geared toward neuropathology clinical fellows and neuroscience research trainees is recommended (2.1). To further strengthen the future of brain banks with informatics support, data science training with formal training through coursework and hands-on experience is additionally recommended (2.2). Ease of access to human brain tissue for qualified investigators is crucial for supporting translational research. The United Kingdom Brain Bank Network[18], Netherlands Brain Bank[19], Parkinson’s Progression Markers Initiative (PPMI)[20], Rush Alzheimer Disease Center[21], National Alzheimer’s Coordinating Center[22], and National Institute of Health’s NeuroBioBank[23], provide an accessible portal for qualified researchers to identify and request human brain tissue. These portals required significant investment in infrastructure and integration of informaticians, for which funds are rarely available, (e.g., data scientist, bioinformatician, biostatistician) to work continually with neuropathology experts with the goal of sustained improvements based on user feedback.
Broader access to neuropathology training for a more novice audience through conference workshops and publicly available neuropathology-based encyclopedias[24] are also recommended to enhance communication between tissue requestors and tissue providers (2.3). Given the importance of paired phenotypic data with tissue selection (Figure 2), strengthening collaborations with clinicians to enhance translational potential of tissue-based discoveries and consideration of structured clinical training of brain bank support staff to enhance retrospective abstraction of clinical progression is recommended (2.4). Initiatives to enhance sustainability of brain banks amidst ever increasing demand for tissue provision may be found through: infrastructure built into research grants and program projects led by brain bank directors, working with home institutions to create cost recovery mechanisms, partnering with development for philanthropic sponsorship, engaging with leadership for institutional support, collaborating with intramural researchers in field adjacent domains (e.g., cancer research), or applying to government-led opportunities (e.g., National Institute of Health’s NeuroBioBank[23]). The Netherlands Brain Bank[25] and Banner Sun Health’s Brain & Body Program instituted partial support through a cost recovery model to facilitate staffing for tissue provision[9,26]. The United Kingdom Brain Bank Network adopted a similar cost recovery models, along with the development of harmonized protocols, legal guidance, and administrative guidance for a holistic approach to sustainable brain banking[18].
Innovating Tissue Quality Strategies to Unlock Molecular Insights
Maximizing the potential of molecular discoveries in aging and neurodegenerative research requires innovative strategies to overcome the limitations posed by using archival human brain tissue (Box 3). Advances in -omics, including single-cell and spatially resolved methods, enable precise identification of disease signatures[27,28,29,30,31,32,33,34,35]. High-throughput analysis of frozen or formalin-fixed paraffin embedded (FFPE) brain tissue offers unbiased, multimodal insights into brain physiology and disease, supporting breakthroughs like whole-brain mapping [28,31,35,36,37], network modeling to uncover druggable targets[38,39], and identification of key post-translational modifications [40,41]. Omics-based research has emerged as a guiding force in the study of both neuronal and glial biology of aging, highlighting pathway dynamics to discern biologic perturbations as exampled in aging42, Alzheimer’s disease [28,43,44], amyotrophic lateral sclerosis[45], Huntington disease[32], Lewy body disease[46], and progressive supranuclear palsy[47]. Deep, quantitative neuropathologic characterization further enables the reconstruction of antemortem trajectories when combined with high-dimensional -omics data[48]. These types of work, made possible by broad collaboration and integration of various data modalities, delineate a clear path toward identifying critical phenotypic markers of cellular states for broader consideration of molecular diagnostics (3.1). Scientific advances, like those uncovered by cryo-electron microscopy[49,50,51,52,53], are the direct result of innovative approaches to investigate archival brain tissue. A coordinated effort to develop methods for utilizing pre-existing materials (e.g., stored formalin-fixed or frozen tissue) is essential to unlocking the full potential of archival collections. As technology advances, the use of tissue previously considered suboptimal enters into the realm of possibilities (e.g., probe-based technology for FFPE tissue, 3.2).
New imaging techniques, like array tomography combined with super-resolution microscopy requires non-standard autopsy tissue processing[54,55] including immediate use of fresh tissue upon procurement (3.3). This necessitates additional funding to support brain bank staff in performing rapid-response protocols and ensuring timely communication between tissue providers and the research team. Through ongoing collaboration and enhanced tissue innovations, we stand at the precipice of further breakthroughs in understanding pathogenesis holding the promise for alleviating the burden of these devastating diseases on individuals and their families. To future-proof valuable tissue samples for discovery-based -omics methodologies, the continuation of centralized resources is recommended to establish best practices and minimum standards for tissue preparation (e.g., fixation, freezing) and storage (3.4). While it may not be possible to overhaul protocols for the entirety of a brain bank’s collection to support rapidly advancing -omics techniques, it is crucial to understand the quantitative variables that capture tissue quality for each modality and to underscore the importance of a flexible and collaborative framework between neuropathology experts and researchers to allow for innovative use of tissue[1,54,55].
Streamlining Digital Slide Sharing and Analysis to Enhance Translational Potential
The necessity for efficient slide sharing capabilities and neuropathology-centric initiatives are key considerations to realizing the full benefits of digital pathology (Box 4). Digital pathology is a versatile technology that continues to advance our understanding of the spatial biology of age-related changes, neurodegenerative lesions, and cerebrovascular insults[56,57,58]. Whole slide images from diagnostic slides or project-specific slides are scanned at high-resolution to enable the neuropathology expert, clinician, and/or researcher to readily view the entirety of the tissue or focus on specific areas of interest. Digitized slides can be annotated for diagnostic, research, and/or educational purposes. Digitization comes with the added value of integrating computational analytic tools for high-throughput image segmentation of neuroanatomic structures to objectively quantify lesions and histologic changes (4.1). Efforts to compare established semi-quantitative scores with digital pathology measures show a strong correlation between the manual scores and digitized measures offering hope toward automated quantification of disease burden[59,60,61]. Staging systems of neurodegenerative diseases [62,63,64,65,66,67,68] are often inherent to the success of consensus initiatives with clinician and scientific partners [69,70,71,72,73,74,75]. With digital pathology already benefitting efforts like the Rainwater criteria for progressive supranuclear palsy[74] and McKee criteria for chronic traumatic encephalopathy[66]; we embrace a present reality with continued opportunities to apply machine learning and neural networks to systematically analyze whole slide images that compliment diagnostic procedures in a brain bank[76,77,78,79,80].
Neuropathology-centric initiatives to address the need for slide sharing and hosting efforts may play a crucial role in overcoming local implementation barriers[81] (4.2). Notably, the Digital Slide Archive[82], originally designed for cancer research[83], is being adapted for aging and neurodegenerative research, showcasing the potential for global collaboration (4.3). In lieu of a central repository, individual brain banks are drawing upon local resources and philanthropy to make their collections digitally available[84]. The benefits of digital pathology go beyond technical aspects. Its integration into clinical practice offers significant potential for improved diagnostics and treatment planning through systematic analyses of autopsied individuals with antemortem clinical data[85,86]. For example, digital pathology can quantitatively measure histologic changes, enhancing the translational value of postmortem studies that investigate neuroimaging and fluid biomarker changes[87,88,89]. Moreover, large-scale research efforts stand to gain from the ability of digital pathology to capture the heterogeneity of neurodegeneration in the aging brain, paving the way for more targeted and personalized approaches toward understanding and combating these multifaceted disorders[56,68,90,91]. As the aging and neurodegeneration fields advance, continued exploration, collaboration, and support for an alliance of worldwide brain banks are essential to unlocking the full potential of digital pathology in biomedical research and clinical applications (4.4).
Building Collaborative Platforms to Accelerate Tissue-Based Discoveries
Key considerations regarding increased slide digitization and to increasingly linked -omics datasets, are data storage and harmonization of common data elements and file formats (Box 5). There is a critical need for data to be harmonized, comply with international data protection laws, and use common data models to allow access and analysis between research groups without not dependence on proprietary software. Looking to the neuroimaging field for inspiration, notable initiatives demonstrating the aspirational power of unity in scientific exploration, comprise among others PPMI[20] and Alzheimer's Disease Neuroimaging Initiative (ADNI)[92]. Recognizing the importance of a central data repository, universal file formats, and need for collaborative platforms – the Laboratory of NeuroImaging (LONI) was founded[93]. LONI's focus on data sharing enhances transparency and harmonization within the neuroimaging community[94], benefitting multi-site interpretation of data. LONI houses and manages ADNI data, enabling the infrastructure for ADNI's harmonization efforts that continue to accelerate progress in understanding Alzheimer's disease and related dementias. ADNI data is used to both test[95] and validate novel hypotheses[96]. However, applicability of ADNI-based findings across economic backgrounds, as well as those having multiple disease etiologies[97], was recognized as a limitation motivating novel recruitment efforts with focused efforts to strengthen study participation[98]. Qualified researchers seeking to reverse engineer postmortem findings[62,63,99] can download data from initiatives like ADNI[100], PPMI[20], and Longitudinal Early Onset Alzheimer’s Disease Study[101] to more broadly examine heterogenous biomarker patterns through identification of longitudinal trajectories[102] or toward enhanced molecular diagnostics of fluid biomarkers[103,104]. Conversely, open platforms and online repositories for neuroimaging (e.g. OpenNeuro[105], Neurovault[100]) and high-dimensional molecular data (e.g. Alzheimer’ disease knowledge portal[106], Global Parkinson's Genetics Program[107]) enable data deposition from individual groups to enhance reusability of datasets.
As we usher in the next frontiers of neuropathology, harmonizing methodologies and data across research endeavors to promote interoperability standards for common data elements with enough flexibility for local innovation will be critical[108]. However, caution should be applied to mandatory adherence of common data elements to avoid penalization of brain banks who lack funding to update protocols (5.1). By implementing case-level tracking system through a digital object identifier (DOI) (5.2) in collaboration with bioethicists and establishing a codified brain library through an accessible portal, data tracking, sharing, and harmonization will be enhanced, laying a robust foundation for future advancements (5.3). The DOI system will allow brain banks to assess tissue quality through automated feedback from publications and enable researchers to select the highest-quality samples for new studies while integrating findings from earlier analyses. This system could not only increase the value of existing brain tissue repositories but also accelerates biomedical discoveries. A key feature of tissue preservation is systematic neuroanatomic dissection. Looking ahead, the development of a human common coordinate framework[109] emerges as a visionary approach to further enhance harmonization (5.4), offering a unified language for researchers worldwide and firmly establishing the biomedical science community in an era of transformative neuropathologic research. Similar approaches were developed for antemortem neuroimaging, such as the “neuromaps” initiative working across multiple brain maps[110]. Currently, annotation of Brodmann areas against the Allen Brain Atlas[111,112] is an increasingly used neuroanatomic resource that could be leveraged to create the human common coordinate framework. As spatial biology interrogation of the human brain continues to accelerate, brain banks may consider translating local sampling protocols to publicly available tissue atlas for reporting of regions and Brodmann areas toward wider applicability of tissue-based findings.
Harnessing machine learning to revolutionize brain banking
While attention is primarily focused on applying machine learning for research endeavors seeking to automate tedious, repetitive work and diagnostic applications[113,114,115], it is imperative to explore the vast spectrum of potential applications beyond these domains (Box 6). The untapped potential of machine learning could revolutionize processes beyond diagnostic prediction, to instead focus on ‘pain points’ in data acquisition and processing in a brain bank. Consider the prospect of expediting quality control workflows through quality control mechanisms where machine learning serves as an adept assistant in expediting tasks and enhancing overall efficiency of brain banking and digital pathology workflows (6.1). For instance, the integration of machine learning in decision-making could extend to the realm of selecting suitable cases for specific -omics analyses, streamlining research pathways, and optimizing resource allocation. Moreover, image analysis tools from the private sector[116] are already developed from image sharpening, modulating, and transforming, simply awaiting creative application to histologic images. The journey towards fully harnessing machine learning’s potential will entail envisioning and embracing novel use cases that not only enhances outcomes but also fosters a more streamlined and effective ecosystem.
Looking to the future, the power of advancements in computational pipelines could be redirected toward seemingly obsolete techniques. By combining pioneering data processing methods with historic approaches (e.g., Nissl) or routine techniques (e.g., hematoxylin & eosin [H&E] stained tissue), it may be possible to discover intricate markers and insights through simpler and more widely accessible measures. This transformative approach relies on training complex models with high-level data and then distilling that knowledge for application to routine technologies like H&E staining[117]. Computer-driven visualization and data mining from existing slide archives hold immense potential for identifying previously overlooked cellular and subcellular changes[118], as well as enabling integration with genomics[119] and other large-scale data sources. Importantly, adapting machine learning models to basic approaches, such as H&E staining carries little risk. To overcome relative lack of labelled images to inform classification or segmentation models[120], recent vision-language foundation models for pathology have introduced promising solutions. For example, leveraging image-text pairs with descriptions available from medically-oriented social media, Large-scale Artificial Intelligence Open Network[121], educational sources, and images and descriptions from PubMed literature, the OpenPath dataset was developed[120]. These vision-language pathology models enable users to retrieve examples by image-based or natural language searches[120,122]. Moreover, machine learning approaches are already providing an expanded repertoire for -omics studies through integration with light microscopy for isotropic super-resolution of synapses[123], decision-making for gene prioritization[124], and lesion identification[77]. Application of machine learning may play a critical role in facilitating a convergence of data streams (6.2), seeking to propel the biomedical science community forward as researchers continue to push the bounds through integration of complex technologies like spatial transcriptomics and electron microscopy to study brain injury[27]. Ultimately, machine learning approaches are a key additional element in the neuropathology expert’s toolbox, serving to speed up and enhance their ability to derive meaningful insights from tissue in health and disease.
Conclusions
Advancements in brain banking, tissue-based -omics, digital pathology, and machine learning – along with insights from neuroimaging harmonization efforts – mark an unprecedented era in neuropathology. By coining the term transformative neuropathology, we hope to provide a unifying framework that highlights the field’s evolving role in leveraging advanced technologies to accelerate discovery and translational research. The methods and collaborations discussed here illustrate the vast potential of human brain tissue studies to drive molecular breakthroughs that delay disease progression and emphasize the importance for early disease detection. The rapidly evolving field requires striking a balance between supporting large, comprehensive brain banks and small, more specialized ones. While large brain banks facilitate broad-scale studies and initiatives, smaller brain banks excel in focused, targeted research. Supporting both large and small brain banks ensures that a wide range of research priorities – whether broad or specialized – advance our understanding of the human brain. However, both large and small brain banks often experience understaffing. To ensure their sustainability, tissue requestors and providers must proactively work together. This includes directing funds toward brain banks, fostering partnerships with clinical teams, harmonizing data, and cross training the next generation of researchers. Such efforts will ensure that brain banks remain at the forefront biomedical discoveries, advancing our understanding of aging and neurodegeneration to improve outcomes. By incorporating advanced technologies into human brain tissue research, we can unlock new scientific opportunities for scientific discovery. This integrated approach will ultimately enhance diagnostic precision, enable personalized therapy, and significantly reduce the global burden of neurodegenerative diseases on patients, families, and healthcare systems.
Boxes
| Box 1 | Low autopsy rate for healthy aging and groups with limited representation in scientific research |
| 1.1 Enhanced education on brain donation through outreach |
Recommended solutions:
|
| 1.2 Enhanced efforts to recruit healthy aging and broaden age spectrum of brain donors |
Recommended solutions:
|
| Box 2 | Dearth of neuropathology experts and informaticians with brain banking knowledge |
| 2.1 Neuropathologytraining fellowships for MDs and PhDs |
Recommended solutions:
|
| 2.2 Data science training and integration |
Recommended solutions:
|
| 2.3 NeuroPathopedia - Neuropathology-based encyclopedia |
Recommended solutions:
|
| 2.4 Phenotypic data collection and tissue provision |
Recommended solutions:
|
| Box 3 | Tissue quality innovations needed to maximize molecular discoveries |
| 3.1 Molecular and biochemical diagnostics beyond immunohistochemistry |
Recommended solutions:
|
| 3.2 Enhanced efforts for development of methods to utilize existing brain bank materials |
Recommended solutions:
|
| 3.3 Enhancing procurement areas and autopsy response teams for sample collection |
Recommended solutions:
|
| 3.4 Harmonization in tissue preparation (fixative, freezing), storage, and inventory |
Recommended solutions:
|
| Box 4 | Limited capabilities for digital slide sharing to facilitate harmonization of disease staging and capturing phenotypic heterogeneity |
| 4.1 Neuroanatomic segmentation for digitized slides |
Recommended solutions:
|
| 4.2 Slide sharing/hosting efforts |
Recommended solutions:
|
| 4.3 Neuropathology-centric initiatives |
Recommended solutions:
|
| 4.4 Alliance of worldwide brain banks |
Recommended solutions:
|
| Box 5 | Relative lack of common neuropathologic data models and secure storage platforms |
| 5.1 Data harmonization for common data elements |
Recommended solutions:
|
| 5.2 Sample-level tracking through a universal digital object identifier (DOI) |
Recommended solutions:
|
| 5.3 Codified brain library through an accessible portal |
Recommended solutions:
|
| 5.4 Common Coordinate Framework |
Recommended solutions:
|
| Box 6 | Emerging need for machine learning to optimize brain bank workflow |
| 6.1 Quality control for digitized slides |
Recommended solutions:
|
| 6.2 Convergence of diverse data streams |
Recommended solutions:
|
Acknowledgements
Support for the workshop hosted at Cold Spring Harbor Laboratory was provided by Chan Zuckerberg Initiative DAF, an advised fund of Silicon Valley Community Foundation. Preparation for this Perspective was supported in part by the National Institute on Aging (R01-AG075802, R01-AG076040, RF1-AG069052) and National Institute of Neurological Disorders and Stroke (R01-NS127186). We thank Dr. Thomas Beach and Dr. Thomas Montine for their counsel during the preparation of this article; and gratefully acknowledge the work of Dr. Derek Caetano-Anolles for design of Figure 1 and Hsin-Pei Wang for design of Figure 2. We also extend our gratitude to Dr. Lilian Coie for her support in drafting the manuscript.
References
- Danner, B.; Gonzalez, A.D.; Corbett, W.C.; Alhneif, M.; Etemadmoghadam, S.; Parker-Garza, J.; and Flanagan, M.E. Brain banking in the United States and Europe: Importance, challenges, and future trends. Journal of Neuropathology & Experimental Neurology 2024, 83, 219–229. [Google Scholar] [CrossRef]
- Beach, T.G. Alzheimer's disease and the "Valley Of Death": not enough guidance from human brain tissue? J Alzheimers Dis 2013, 33 Suppl 1, S219–233. [Google Scholar] [CrossRef]
- Carlos, A.F.; Poloni, T.E.; Medici, V.; Chikhladze, M.; Guaita, A.; and Ceroni, M. From brain collections to modern brain banks: A historical perspective. Alzheimers Dement (N Y) 2019, 5, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R.; Smith, A.D.; Jobst, K.A.; Refsum, H.; Sutton, L.; and Ueland, P.M. Folate, vitamin B12, and serum total homocysteine levels in confirmed Alzheimer disease. Arch Neurol 1998, 55, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Deary, I.J.; Gow, A.J.; Taylor, M.D.; Corley, J.; Brett, C.; Wilson, V.; Campbell, H.; Whalley, L.J.; Visscher, P.M.; Porteous, D.J.; and Starr, J.M. The Lothian Birth Cohort 1936: a study to examine influences on cognitive ageing from age 11 to age 70 and beyond. BMC Geriatr 2007, 7, 28. [Google Scholar] [CrossRef]
- Roberts, R.O.; Geda, Y.E.; Knopman, D.S.; Cha, R.H.; Pankratz, V.S.; Boeve, B.F.; Ivnik, R.J.; Tangalos, E.G.; Petersen, R.C.; and Rocca, W.A. The Mayo Clinic Study of Aging: design and sampling, participation, baseline measures and sample characteristics. Neuroepidemiology 2008, 30, 58–69. [Google Scholar] [CrossRef]
- Katz, M.J.; Lipton, R.B.; Hall, C.B.; Zimmerman, M.E.; Sanders, A.E.; Verghese, J.; Dickson, D.W.; and Derby, C.A. Age-specific and sex-specific prevalence and incidence of mild cognitive impairment, dementia, and Alzheimer dementia in blacks and whites: a report from the Einstein Aging Study. Alzheimer Dis Assoc Disord 2012, 26, 335–343. [Google Scholar] [CrossRef]
- Barnes, L.L.; Shah, R.C.; Aggarwal, N.T.; Bennett, D.A.; and Schneider, J.A. The Minority Aging Research Study: ongoing efforts to obtain brain donation in African Americans without dementia. Curr Alzheimer Res 2012, 9, 734–745. [Google Scholar] [CrossRef]
- Beach, T.G.; Adler, C.H.; Sue, L.I.; Serrano, G.; Shill, H.A.; Walker, D.G.; Lue, L.; Roher, A.E.; Dugger, B.N.; Maarouf, C.; et al. Arizona Study of Aging and Neurodegenerative Disorders and Brain and Body Donation Program. Neuropathology 2015, 35, 354–389. [Google Scholar] [CrossRef]
- Kok, E.H.; Paetau, A.; Martiskainen, M.; Lyytikainen, L.P.; Lehtimaki, T.; Karhunen, P.; and Myllykangas, L. Accumulation of Lewy-Related Pathology Starts in Middle Age: The Tampere Sudden Death Study. Ann Neurol 2024, 95, 843–848. [Google Scholar] [CrossRef]
- Smith, C.; and Millar, T. Brain donation procedures in the Sudden Death Brain Bank in Edinburgh. Handb Clin Neurol 2018, 150, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Alafuzoff, I.; Arzberger, T.; Al-Sarraj, S.; Bodi, I.; Bogdanovic, N.; Braak, H.; Bugiani, O.; Del-Tredici, K.; Ferrer, I.; Gelpi, E.; et al. Staging of neurofibrillary pathology in Alzheimer's disease: a study of the BrainNet Europe Consortium. Brain Pathol 2008, 18, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Rossor, M.N.; Fox, N.C.; Mummery, C.J.; Schott, J.M.; and Warren, J.D. The diagnosis of young-onset dementia. Lancet Neurol 2010, 9, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Liesinger, A.M.; Graff-Radford, N.R.; Duara, R.; Carter, R.E.; Hanna Al-Shaikh, F.S.; Koga, S.; Hinkle, K.M.; DiLello, S.K.; Johnson, M.F.; Aziz, A.; et al. Sex and age interact to determine clinicopathologic differences in Alzheimer's disease. Acta Neuropathol 2018, 136, 873–885. [Google Scholar] [CrossRef]
- Glover, C.M.; Shah, R.C.; Bennett, D.A.; Wilson, R.S.; and Barnes, L.L. Perceived Impediments to Completed Brain Autopsies Among Diverse Older Adults Who Have Signed a Uniform Anatomical Gift Act for Brain Donation for Clinical Research. Ethn Dis 2020, 30, 709–718. [Google Scholar] [CrossRef]
- Glover, C.M.; Shah, R.C.; Bennett, D.A.; Wilson, R.S.; and Barnes, L.L. The Health Equity Through Aging Research And Discussion (HEARD) Study: A Proposed Two-Phase Sequential Mixed-Methods Research Design To Understand Barriers And Facilitators Of Brain Donation Among Diverse Older Adults. Exp Aging Res 2020, 46, 311–322. [Google Scholar] [CrossRef]
- Metter, D.M.; Colgan, T.J.; Leung, S.T.; Timmons, C.F.; and Park, J.Y. Trends in the US and Canadian Pathologist Workforces From 2007 to 2017. JAMA Netw Open 2019, 2, e194337. [Google Scholar] [CrossRef]
- United Kingdom Brain Bank Network (2024). https://ukbbn.brainsfordementiaresearch.org.
- Netherlands Brain Bank (2024). https://www.brainbank.nl.
- Parkinson's Progression Markers Initiative (2024). https://www.ppmi-info.org/.
- Rush Alzheimer's Disease Center (2024). https://www.radc.rush.edu.
- National Alzheimer's Coordinating Center (2024). https://naccdata.org/.
- National Institute of Health NeuroBioBank (2024). https://neurobiobank.nih.gov/about/.
- Schmidt, R.E. (2024). https://neuropathologyatlas.wustl.edu/.
- Rademaker, S.H.M.; and Huitinga, I. A new viewpoint: running a nonprofit brain bank as a business. Handb Clin Neurol 2018, 150, 93–101. [Google Scholar] [CrossRef]
- Brain & Body Donation Program (2024). https://www.bannerhealth.com/services/research/about-banner-research/research-programs/brain-and-body-donation-program.
- Androvic, P.; Schifferer, M.; Perez Anderson, K.; Cantuti-Castelvetri, L.; Jiang, H.; Ji, H.; Liu, L.; Gouna, G.; Berghoff, S.A.; Besson-Girard, S.; et al. Spatial Transcriptomics-correlated Electron Microscopy maps transcriptional and ultrastructural responses to brain injury. Nat Commun 2023, 14, 4115. [Google Scholar] [CrossRef]
- Gabitto, M.I.; Travaglini, K.J.; Rachleff, V.M.; Kaplan, E.S.; Long, B.; Ariza, J.; Ding, Y.; Mahoney, J.T.; Dee, N.; Goldy, J.; et al. Integrated multimodal cell atlas of Alzheimer’s disease. bioRxiv 2024, 2023.2005.2008.539485. [CrossRef]
- Maniatis, S.; Petrescu, J.; and Phatnani, H. Spatially resolved transcriptomics and its applications in cancer. Curr Opin Genet Dev 2021, 66, 70–77. [Google Scholar] [CrossRef]
- Vickovic, S.; Lötstedt, B.; Klughammer, J.; Mages, S.; Segerstolpe, Å.; Rozenblatt-Rosen, O.; and Regev, A. SM-Omics is an automated platform for high-throughput spatial multi-omics. Nature Communications 2022, 13, 795. [Google Scholar] [CrossRef]
- Jorstad, N.L.; Close, J.; Johansen, N.; Yanny, A.M.; Barkan, E.R.; Travaglini, K.J.; Bertagnolli, D.; Campos, J.; Casper, T.; Crichton, K.; et al. Transcriptomic cytoarchitecture reveals principles of human neocortex organization. Science 2023, 382, eadf6812. [Google Scholar] [CrossRef]
- Paryani, F.; Kwon, J.S.; Ng, C.W.; Madden, N.; Ofori, K.; Tang, A.; Lu, H.; Li, J.; Mahajan, A.; Davidson, S.M.; et al. Multi-OMIC analysis of Huntington disease reveals a neuroprotective astrocyte state. bioRxiv. 2023. [CrossRef]
- Otero-Garcia, M.; Mahajani, S.U.; Wakhloo, D.; Tang, W.; Xue, Y.-Q.; Morabito, S.; Pan, J.; Oberhauser, J.; Madira, A.E.; Shakouri, T.; et al. Molecular signatures underlying neurofibrillary tangle susceptibility in Alzheimer’s disease. Neuron 2022, 110, 2929–2948e2928. [Google Scholar] [CrossRef]
- Leng, K.; Li, E.; Eser, R.; Piergies, A.; Sit, R.; Tan, M.; Neff, N.; Li, S.H.; Rodriguez, R.D.; Suemoto, C.K.; et al. Molecular characterization of selectively vulnerable neurons in Alzheimer's disease. Nat Neurosci 2021, 24, 276–287. [Google Scholar] [CrossRef]
- Colonna, M.; Konopka, G.; Liddelow, S.A.; Nowakowski, T.; Awatramani, R.; Bateup, H.S.; Cadwell, C.R.; Caglayan, E.; Chen, J.L.; Gillis, J.; et al. Implementation and validation of single-cell genomics experiments in neuroscience. Nat Neurosci 2024, 27, 2310–2325. [Google Scholar] [CrossRef]
- Hawrylycz, M.J.; Lein, E.S.; Guillozet-Bongaarts, A.L.; Shen, E.H.; Ng, L.; Miller, J.A.; van de Lagemaat, L.N.; Smith, K.A.; Ebbert, A.; Riley, Z.L.; et al. An anatomically comprehensive atlas of the adult human brain transcriptome. Nature 2012, 489, 391–399. [Google Scholar] [CrossRef]
- Adameyko, I.; Bakken, T.; Bhaduri, A.; Chhatbar, C.; Filbin, M.G.; Gate, D.; Hochgerner, H.; Kim, C.N.; Krull, J.; La Manno, G.; et al. Applying single-cell and single-nucleus genomics to studies of cellular heterogeneity and cell fate transitions in the nervous system. Nat Neurosci 2024, 27, 2278–2291. [Google Scholar] [CrossRef]
- Wang, M.; Li, A.; Sekiya, M.; Beckmann, N.D.; Quan, X.; Schrode, N.; Fernando, M.B.; Yu, A.; Zhu, L.; Cao, J.; et al. Transformative Network Modeling of Multi-omics Data Reveals Detailed Circuits, Key Regulators, and Potential Therapeutics for Alzheimer's Disease. Neuron 2021, 109, 257–272 e214. [Google Scholar] [CrossRef]
- Mostafavi, S.; Gaiteri, C.; Sullivan, S.E.; White, C.C.; Tasaki, S.; Xu, J.; Taga, M.; Klein, H.U.; Patrick, E.; Komashko, V.; et al. A molecular network of the aging human brain provides insights into the pathology and cognitive decline of Alzheimer's disease. Nat Neurosci 2018, 21, 811–819. [Google Scholar] [CrossRef]
- Wesseling, H.; Mair, W.; Kumar, M.; Schlaffner, C.N.; Tang, S.; Beerepoot, P.; Fatou, B.; Guise, A.J.; Cheng, L.; Takeda, S.; et al. Tau PTM Profiles Identify Patient Heterogeneity and Stages of Alzheimer’s Disease. Cell 2020, 183, 1699–1713e1613. [Google Scholar] [CrossRef]
- Dujardin, S.; Commins, C.; Lathuiliere, A.; Beerepoot, P.; Fernandes, A.R.; Kamath, T.V.; De Los Santos, M.B.; Klickstein, N.; Corjuc, D.L.; Corjuc, B.T.; et al. Tau molecular diversity contributes to clinical heterogeneity in Alzheimer's disease. Nat Med 2020, 26, 1256–1263. [Google Scholar] [CrossRef]
- Lopes, K.P.; Snijders, G.J.L.; Humphrey, J.; Allan, A.; Sneeboer, M.A.M.; Navarro, E.; Schilder, B.M.; Vialle, R.A.; Parks, M.; Missall, R.; et al. Genetic analysis of the human microglial transcriptome across brain regions, aging and disease pathologies. Nat Genet 2022, 54, 4–17. [Google Scholar] [CrossRef]
- De Jager, P.L.; Ma, Y.; McCabe, C.; Xu, J.; Vardarajan, B.N.; Felsky, D.; Klein, H.U.; White, C.C.; Peters, M.A.; Lodgson, B.; et al. A multi-omic atlas of the human frontal cortex for aging and Alzheimer's disease research. Sci Data 2018, 5, 180142. [Google Scholar] [CrossRef]
- Brase, L.; You, S.F.; D'Oliveira Albanus, R.; Del-Aguila, J.L.; Dai, Y.; Novotny, B.C.; Soriano-Tarraga, C.; Dykstra, T.; Fernandez, M.V.; Budde, J.P.; et al. Single-nucleus RNA-sequencing of autosomal dominant Alzheimer disease and risk variant carriers. Nat Commun 2023, 14, 2314. [Google Scholar] [CrossRef]
- Maniatis, S.; Aijo, T.; Vickovic, S.; Braine, C.; Kang, K.; Mollbrink, A.; Fagegaltier, D.; Andrusivova, Z.; Saarenpaa, S.; Saiz-Castro, G.; et al. Spatiotemporal dynamics of molecular pathology in amyotrophic lateral sclerosis. Science 2019, 364, 89–93. [Google Scholar] [CrossRef]
- Fiorini, M.R.; Dilliott, A.A.; Thomas, R.A.; and Farhan, S.M.K. Transcriptomics of Human Brain Tissue in Parkinson's Disease: a Comparison of Bulk and Single-cell RNA Sequencing. Mol Neurobiol. 2024. [CrossRef]
- Wang, X.; Allen, M.; Is, O.; Reddy, J.S.; Tutor-New, F.Q.; Castanedes Casey, M.; Carrasquillo, M.M.; Oatman, S.R.; Min, Y.; Asmann, Y.W.; et al. Alzheimer's disease and progressive supranuclear palsy share similar transcriptomic changes in distinct brain regions. J Clin Invest 2022, 132. [Google Scholar] [CrossRef]
- Green, G.S.; Fujita, M.; Yang, H.S.; Taga, M.; Cain, A.; McCabe, C.; Comandante-Lou, N.; White, C.C.; Schmidtner, A.K.; Zeng, L.; et al. Cellular communities reveal trajectories of brain ageing and Alzheimer's disease. Nature 2024, 633, 634–645. [Google Scholar] [CrossRef]
- Fitzpatrick, A.W.P.; Falcon, B.; He, S.; Murzin, A.G.; Murshudov, G.; Garringer, H.J.; Crowther, R.A.; Ghetti, B.; Goedert, M.; and Scheres, S.H.W. Cryo-EM structures of tau filaments from Alzheimer's disease. Nature 2017, 547, 185–190. [Google Scholar] [CrossRef]
- Kollmer, M.; Close, W.; Funk, L.; Rasmussen, J.; Bsoul, A.; Schierhorn, A.; Schmidt, M.; Sigurdson, C.J.; Jucker, M.; and Fandrich, M. Cryo-EM structure and polymorphism of Abeta amyloid fibrils purified from Alzheimer's brain tissue. Nat Commun 2019, 10, 4760. [Google Scholar] [CrossRef]
- Li, B.; Ge, P.; Murray, K.A.; Sheth, P.; Zhang, M.; Nair, G.; Sawaya, M.R.; Shin, W.S.; Boyer, D.R.; Ye, S.; et al. Cryo-EM of full-length alpha-synuclein reveals fibril polymorphs with a common structural kernel. Nat Commun 2018, 9, 3609. [Google Scholar] [CrossRef]
- Cao, Q.; Boyer, D.R.; Sawaya, M.R.; Ge, P.; and Eisenberg, D.S. Cryo-EM structures of four polymorphic TDP-43 amyloid cores. Nat Struct Mol Biol 2019, 26, 619–627. [Google Scholar] [CrossRef]
- Glynn, C.; Sawaya, M.R.; Ge, P.; Gallagher-Jones, M.; Short, C.W.; Bowman, R.; Apostol, M.; Zhou, Z.H.; Eisenberg, D.S.; and Rodriguez, J.A. Cryo-EM structure of a human prion fibril with a hydrophobic, protease-resistant core. Nat Struct Mol Biol 2020, 27, 417–423. [Google Scholar] [CrossRef]
- Colom-Cadena, M.; Davies, C.; Sirisi, S.; Lee, J.E.; Simzer, E.M.; Tzioras, M.; Querol-Vilaseca, M.; Sanchez-Aced, E.; Chang, Y.Y.; Holt, K.; et al. Synaptic oligomeric tau in Alzheimer's disease - A potential culprit in the spread of tau pathology through the brain. Neuron 2023, 111, 2170–2183 e2176. [Google Scholar] [CrossRef]
- Kay, K.R.; Smith, C.; Wright, A.K.; Serrano-Pozo, A.; Pooler, A.M.; Koffie, R.; Bastin, M.E.; Bak, T.H.; Abrahams, S.; Kopeikina, K.J.; et al. Studying synapses in human brain with array tomography and electron microscopy. Nature protocols 2013, 8, 1366–1380. [Google Scholar] [CrossRef]
- Kouri, N.; Frankenhauser, I.; Peng, Z.; Labuzan, S.A.; Boon, B.D.C.; Moloney, C.M.; Pottier, C.; Wickland, D.P.; Caetano-Anolles, K.; Corriveau-Lecavalier, N.; et al. Clinicopathologic Heterogeneity and Glial Activation Patterns in Alzheimer Disease. JAMA Neurol 2024, 81, 619–629. [Google Scholar] [CrossRef]
- Jolink, W.M.T.; van Veluw, S.J.; Zwanenburg, J.J.M.; Rozemuller, A.J.M.; van Hecke, W.; Frosch, M.P.; Bacskai, B.J.; Rinkel, G.J.E.; Greenberg, S.M.; and Klijn, C.J.M. Histopathology of Cerebral Microinfarcts and Microbleeds in Spontaneous Intracerebral Hemorrhage. Transl Stroke Res 2023, 14, 174–184. [Google Scholar] [CrossRef]
- Shakir, M.N.; and Dugger, B.N. Advances in Deep Neuropathological Phenotyping of Alzheimer Disease: Past, Present, and Future. J Neuropathol Exp Neurol 2022, 81, 2–15. [Google Scholar] [CrossRef]
- Kapasi, A.; Poirier, J.; Hedayat, A.; Scherlek, A.; Mondal, S.; Wu, T.; Gibbons, J.; Barnes, L.L.; Bennett, D.A.; Leurgans, S.E.; and Schneider, J.A. High-throughput digital quantification of Alzheimer disease pathology and associated infrastructure in large autopsy studies. Journal of Neuropathology & Experimental Neurology 2023, 82, 976–986. [Google Scholar] [CrossRef]
- Neltner, J.H.; Abner, E.L.; Schmitt, F.A.; Denison, S.K.; Anderson, S.; Patel, E.; and Nelson, P.T. Digital pathology and image analysis for robust high-throughput quantitative assessment of Alzheimer disease neuropathologic changes. J Neuropathol Exp Neurol 2012, 71, 1075–1085. [Google Scholar] [CrossRef]
- Scalco, R.; Oliveira, L.C.; Lai, Z.; Harvey, D.J.; Abujamil, L.; DeCarli, C.; Jin, L.W.; Chuah, C.N.; and Dugger, B.N. Machine learning quantification of Amyloid-beta deposits in the temporal lobe of 131 brain bank cases. Acta Neuropathol Commun 2024, 12, 134. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K.; Rub, U.; de Vos, R.A.; Jansen Steur, E.N.; and Braak, E. Staging of brain pathology related to sporadic Parkinson's disease. Neurobiol Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Braak, H.; and Braak, E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 1991, 82, 239–259. [Google Scholar] [CrossRef]
- Thal, D.R.; Rub, U.; Orantes, M.; and Braak, H. Phases of A beta-deposition in the human brain and its relevance for the development of AD. Neurology 2002, 58, 1791–1800. [Google Scholar] [CrossRef]
- Deramecourt, V.; Slade, J.Y.; Oakley, A.E.; Perry, R.H.; Ince, P.G.; Maurage, C.A.; and Kalaria, R.N. Staging and natural history of cerebrovascular pathology in dementia. Neurology 2012, 78, 1043–1050. [Google Scholar] [CrossRef]
- McKee, A.C.; Stein, T.D.; Huber, B.R.; Crary, J.F.; Bieniek, K.; Dickson, D.; Alvarez, V.E.; Cherry, J.D.; Farrell, K.; Butler, M.; et al. Chronic traumatic encephalopathy (CTE): criteria for neuropathological diagnosis and relationship to repetitive head impacts. Acta Neuropathol 2023, 145, 371–394. [Google Scholar] [CrossRef]
- Brettschneider, J.; Del Tredici, K.; Toledo, J.B.; Robinson, J.L.; Irwin, D.J.; Grossman, M.; Suh, E.; Van Deerlin, V.M.; Wood, E.M.; Baek, Y.; et al. Stages of pTDP-43 pathology in amyotrophic lateral sclerosis. Ann Neurol 2013, 74, 20–38. [Google Scholar] [CrossRef]
- Salvi, M.; Molinari, F.; Ciccarelli, M.; Testi, R.; Taraglio, S.; and Imperiale, D. Quantitative analysis of prion disease using an AI-powered digital pathology framework. Sci Rep 2023, 13, 17759. [Google Scholar] [CrossRef]
- Cairns, N.J.; Bigio, E.H.; Mackenzie, I.R.; Neumann, M.; Lee, V.M.; Hatanpaa, K.J.; White, C.L. ; 3rd, Schneider, J.A.; Grinberg, L.T.; Halliday, G.; et al. Neuropathologic diagnostic and nosologic criteria for frontotemporal lobar degeneration: consensus of the Consortium for Frontotemporal Lobar Degeneration. Acta Neuropathol 2007, 114, 5–22. [Google Scholar] [CrossRef]
- Mackenzie, I.R.; Neumann, M.; Bigio, E.H.; Cairns, N.J.; Alafuzoff, I.; Kril, J.; Kovacs, G.G.; Ghetti, B.; Halliday, G.; Holm, I.E.; et al. Nomenclature for neuropathologic subtypes of frontotemporal lobar degeneration: consensus recommendations. Acta Neuropathol 2009, 117, 15–18. [Google Scholar] [CrossRef] [PubMed]
- McKeith, I.G.; Boeve, B.F.; Dickson, D.W.; Halliday, G.; Taylor, J.P.; Weintraub, D.; Aarsland, D.; Galvin, J.; Attems, J.; Ballard, C.G.; et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology 2017, 89, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Nelson, P.T.; Dickson, D.W.; Trojanowski, J.Q.; Jack, C.R.; Boyle, P.A.; Arfanakis, K.; Rademakers, R.; Alafuzoff, I.; Attems, J.; Brayne, C.; et al. Limbic-predominant age-related TDP-43 encephalopathy (LATE): consensus working group report. Brain 2019, 142, 1503–1527. [Google Scholar] [CrossRef] [PubMed]
- Hauw, J.J.; Daniel, S.E.; Dickson, D.; Horoupian, D.S.; Jellinger, K.; Lantos, P.L.; McKee, A.; Tabaton, M.; and Litvan, I. Preliminary NINDS neuropathologic criteria for Steele-Richardson-Olszewski syndrome (progressive supranuclear palsy). Neurology 1994, 44, 2015–2019. [Google Scholar] [CrossRef]
- Roemer, S.F.; Grinberg, L.T.; Crary, J.F.; Seeley, W.W.; McKee, A.C.; Kovacs, G.G.; Beach, T.G.; Duyckaerts, C.; Ferrer, I.A.; Gelpi, E.; et al. Rainwater Charitable Foundation criteria for the neuropathologic diagnosis of progressive supranuclear palsy. Acta neuropathologica 2022, 144, 603–614. [Google Scholar] [CrossRef]
- Mackenzie, I.R.; Neumann, M.; Baborie, A.; Sampathu, D.M.; Du Plessis, D.; Jaros, E.; Perry, R.H.; Trojanowski, J.Q.; Mann, D.M.; and Lee, V.M. A harmonized classification system for FTLD-TDP pathology. Acta Neuropathol 2011, 122, 111–113. [Google Scholar] [CrossRef]
- Signaevsky, M.; Prastawa, M.; Farrell, K.; Tabish, N.; Baldwin, E.; Han, N.; Iida, M.A.; Koll, J.; Bryce, C.; Purohit, D.; et al. Artificial intelligence in neuropathology: deep learning-based assessment of tauopathy. Laboratory Investigation 2019, 99, 1019–1029. [Google Scholar] [CrossRef]
- Tang, Z.; Chuang, K.V.; DeCarli, C.; Jin, L.-W.; Beckett, L.; Keiser, M.J.; and Dugger, B.N. Interpretable classification of Alzheimer’s disease pathologies with a convolutional neural network pipeline. Nature Communications 2019, 10, 2173. [Google Scholar] [CrossRef]
- Sekiya, H.; Koga, S.; Murakami, A.; Kawazoe, M.; Kim, M.; Martin, N.B.; Uitti, R.J.; Cheshire, W.P.; Wszolek, Z.K.; and Dickson, D.W. Validation Study of the MDS Criteria for the Diagnosis of Multiple System Atrophy in the Mayo Clinic Brain Bank. Neurology 2023, 101, e2460–e2471. [Google Scholar] [CrossRef]
- Koga, S.; Zhou, X.; and Dickson, D.W. Machine learning-based decision tree classifier for the diagnosis of progressive supranuclear palsy and corticobasal degeneration. Neuropathol Appl Neurobiol 2021, 47, 931–941. [Google Scholar] [CrossRef]
- Koga, S.; Ghayal, N.B.; and Dickson, D.W. Deep Learning-Based Image Classification in Differentiating Tufted Astrocytes, Astrocytic Plaques, and Neuritic Plaques. J Neuropathol Exp Neurol 2021, 80, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Scalco, R.; Hamsafar, Y.; White, C.L.; Schneider, J.A.; Reichard, R.R.; Prokop, S.; Perrin, R.J.; Nelson, P.T.; Mooney, S.; Lieberman, A.P.; et al. The status of digital pathology and associated infrastructure within Alzheimer's Disease Centers. J Neuropathol Exp Neurol 2023, 82, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Digital Slide Archive (2024). https://digitalslidearchive.github.io/digital_slide_archive/.
- Gutman, D.A.; Cobb, J.; Somanna, D.; Park, Y.; Wang, F.; Kurc, T.; Saltz, J.H.; Brat, D.J.; Cooper, L.A.D.; and Kong, J. Cancer Digital Slide Archive: an informatics resource to support integrated in silico analysis of TCGA pathology data. Journal of the American Medical Informatics Association 2013, 20, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Mount Sinai Brain Slide (2024). https://www.mountsinaicharcot.org/home.
- Baxi, V.; Edwards, R.; Montalto, M.; and Saha, S. Digital pathology and artificial intelligence in translational medicine and clinical practice. Mod Pathol 2022, 35, 23–32. [Google Scholar] [CrossRef]
- Huang, Z.; Yang, E.; Shen, J.; Gratzinger, D.; Eyerer, F.; Liang, B.; Nirschl, J.; Bingham, D.; Dussaq, A.M.; Kunder, C.; et al. A pathologist-AI collaboration framework for enhancing diagnostic accuracies and efficiencies. Nat Biomed Eng. 2024. [Google Scholar] [CrossRef]
- Murray, M.E.; Moloney, C.M.; Kouri, N.; Syrjanen, J.A.; Matchett, B.J.; Rothberg, D.M.; Tranovich, J.F.; Sirmans, T.N.H.; Wiste, H.J.; Boon, B.D.C.; et al. Global neuropathologic severity of Alzheimer's disease and locus coeruleus vulnerability influences plasma phosphorylated tau levels. Mol Neurodegener 2022, 17, 85. [Google Scholar] [CrossRef]
- Mattsson-Carlgren, N.; Janelidze, S.; Bateman, R.J.; Smith, R.; Stomrud, E.; Serrano, G.E.; Reiman, E.M.; Palmqvist, S.; Dage, J.L.; Beach, T.G.; and Hansson, O. Soluble P-tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau. EMBO Mol Med 2021, 13, e14022. [Google Scholar] [CrossRef]
- Murray, M.E.; Przybelski, S.A.; Lesnick, T.G.; Liesinger, A.M.; Spychalla, A.; Zhang, B.; Gunter, J.L.; Parisi, J.E.; Boeve, B.F.; Knopman, D.S.; et al. Early Alzheimer's disease neuropathology detected by proton MR spectroscopy. J Neurosci 2014, 34, 16247–16255. [Google Scholar] [CrossRef]
- Hanna Al-Shaikh, F.S.; Duara, R.; Crook, J.E.; Lesser, E.R.; Schaeverbeke, J.; Hinkle, K.M.; Ross, O.A.; Ertekin-Taner, N.; Pedraza, O.; Dickson, D.W.; et al. Selective Vulnerability of the Nucleus Basalis of Meynert Among Neuropathologic Subtypes of Alzheimer Disease. JAMA Neurol 2020, 77, 225–233. [Google Scholar] [CrossRef]
- Arezoumandan, S.; Xie, S.X.; Cousins, K.A.Q.; Mechanic-Hamilton, D.J.; Peterson, C.S.; Huang, C.Y.; Ohm, D.T.; Ittyerah, R.; McMillan, C.T.; Wolk, D.A.; et al. Regional distribution and maturation of tau pathology among phenotypic variants of Alzheimer's disease. Acta Neuropathol 2022, 144, 1103–1116. [Google Scholar] [CrossRef]
- Mueller, S.G.; Weiner, M.W.; Thal, L.J.; Petersen, R.C.; Jack, C.; Jagust, W.; Trojanowski, J.Q.; Toga, A.W.; and Beckett, L. The Alzheimer's disease neuroimaging initiative. Neuroimaging Clin N Am 2005, 15, 869–877, xi. [Google Scholar] [CrossRef] [PubMed]
- Van Horn, J.D.; and Toga, A.W. Is it time to re-prioritize neuroimaging databases and digital repositories? Neuroimage 2009, 47, 1720–1734. [Google Scholar] [CrossRef] [PubMed]
- Dinov, I.D.; Van Horn, J.D.; Lozev, K.M.; Magsipoc, R.; Petrosyan, P.; Liu, Z.; Mackenzie-Graham, A.; Eggert, P.; Parker, D.S.; and Toga, A.W. Efficient, Distributed and Interactive Neuroimaging Data Analysis Using the LONI Pipeline. Front Neuroinform 2009, 3, 22. [Google Scholar] [CrossRef]
- Jones, D.T.; Knopman, D.S.; Gunter, J.L.; Graff-Radford, J.; Vemuri, P.; Boeve, B.F.; Petersen, R.C.; Weiner, M.W.; Jack, C.R. ; Jr, and Initiative, o. b.o.t.A.s.D.N. Cascading network failure across the Alzheimer’s disease spectrum. Brain 2015, 139, 547–562. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Lowe, V.; Graff-Radford, J.; Botha, H.; Barnard, L.; Wiepert, D.; Murphy, M.C.; Murray, M.; Senjem, M.; Gunter, J.; et al. A computational model of neurodegeneration in Alzheimer’s disease. Nature Communications 2022, 13, 1643. [Google Scholar] [CrossRef]
- Petersen, R.C.; Aisen, P.S.; Beckett, L.A.; Donohue, M.C.; Gamst, A.C.; Harvey, D.J.; Jack, C.R. ; Jr. , Jagust, W.J.; Shaw, L.M.; Toga, A.W.; et al. Alzheimer's Disease Neuroimaging Initiative (ADNI): clinical characterization. Neurology 2010, 74, 201–209. [Google Scholar] [CrossRef]
- Weiner, M.W.; Veitch, D.P.; Miller, M.J.; Aisen, P.S.; Albala, B.; Beckett, L.A.; Green, R.C.; Harvey, D.; Jack, C.R. ; Jr. , Jagust, W.; et al. Increasing participant diversity in AD research: Plans for digital screening, blood testing, and a community-engaged approach in the Alzheimer's Disease Neuroimaging Initiative 4. Alzheimers Dement 2023, 19, 307–317. [Google Scholar] [CrossRef]
- Murray, M.E.; Graff-Radford, N.R.; Ross, O.A.; Petersen, R.C.; Duara, R.; and Dickson, D.W. Neuropathologically defined subtypes of Alzheimer's disease with distinct clinical characteristics: a retrospective study. Lancet Neurol 2011, 10, 785–796. [Google Scholar] [CrossRef]
- Alzheimer's Disease Neuroimaging Initiative Image and Data Archive (2024). https://ida.loni.usc.edu/login.jsp.
- Longitudinal Early Onset Alzheimer’s Disease Study (2024). https://leads-study.medicine.iu.edu/.
- Vogel, J.W.; Young, A.L.; Oxtoby, N.P.; Smith, R.; Ossenkoppele, R.; Strandberg, O.T.; La Joie, R.; Aksman, L.M.; Grothe, M.J.; Iturria-Medina, Y.; et al. Four distinct trajectories of tau deposition identified in Alzheimer's disease. Nat Med 2021, 27, 871–881. [Google Scholar] [CrossRef]
- Siderowf, A.; Concha-Marambio, L.; Lafontant, D.E.; Farris, C.M.; Ma, Y.; Urenia, P.A.; Nguyen, H.; Alcalay, R.N.; Chahine, L.M.; Foroud, T.; et al. Assessment of heterogeneity among participants in the Parkinson's Progression Markers Initiative cohort using alpha-synuclein seed amplification: a cross-sectional study. Lancet Neurol 2023, 22, 407–417. [Google Scholar] [CrossRef]
- Hansson, O.; Seibyl, J.; Stomrud, E.; Zetterberg, H.; Trojanowski, J.Q.; Bittner, T.; Lifke, V.; Corradini, V.; Eichenlaub, U.; Batrla, R.; et al. CSF biomarkers of Alzheimer's disease concord with amyloid-beta PET and predict clinical progression: A study of fully automated immunoassays in BioFINDER and ADNI cohorts. Alzheimers Dement 2018, 14, 1470–1481. [Google Scholar] [CrossRef] [PubMed]
- OpenNeuro (2024). https://openneuro.org/.
- Alzheimer's Disease Knowledge Portal (2024). https://adknowledgeportal.synapse.org.
- Global Parkinson's Genetics, P. GP2: The Global Parkinson's Genetics Program. Mov Disord 2021, 36, 842–851. [Google Scholar] [CrossRef]
- Long, R.A.; Ballard, S.; Shah, S.; Bianchi, O.; Jones, L.; Koretsky, M.J.; Kuznetsov, N.; Marsan, E.; Jen, B.; Chiang, P.; et al. A new AI-assisted data standard accelerates interoperability in biomedical research. medRxiv. 2024. [CrossRef]
- Wang, Q.; Ding, S.L.; Li, Y.; Royall, J.; Feng, D.; Lesnar, P.; Graddis, N.; Naeemi, M.; Facer, B.; Ho, A.; et al. The Allen Mouse Brain Common Coordinate Framework: A 3D Reference Atlas. Cell 2020, 181, 936–953 e920. [Google Scholar] [CrossRef]
- Markello, R.D.; Hansen, J.Y.; Liu, Z.Q.; Bazinet, V.; Shafiei, G.; Suarez, L.E.; Blostein, N.; Seidlitz, J.; Baillet, S.; Satterthwaite, T.D.; et al. neuromaps: structural and functional interpretation of brain maps. Nat Methods 2022, 19, 1472–1479. [Google Scholar] [CrossRef]
- Allen Brain Atlas (2024). https://atlas.brain-map.org.
- Ding, S.L.; Royall, J.J.; Sunkin, S.M.; Ng, L.; Facer, B.A.; Lesnar, P.; Guillozet-Bongaarts, A.; McMurray, B.; Szafer, A.; Dolbeare, T.A.; et al. Comprehensive cellular-resolution atlas of the adult human brain. J Comp Neurol 2016, 524, 3127–3481. [Google Scholar] [CrossRef]
- Vizcarra, J.C.; Pearce, T.M.; Dugger, B.N.; Keiser, M.J.; Gearing, M.; Crary, J.F.; Kiely, E.J.; Morris, M.; White, B.; Glass, J.D.; et al. Toward a generalizable machine learning workflow for neurodegenerative disease staging with focus on neurofibrillary tangles. Acta Neuropathol Commun 2023, 11, 202. [Google Scholar] [CrossRef]
- Marx, G.A.; Koenigsberg, D.G.; McKenzie, A.T.; Kauffman, J.; Hanson, R.W.; Whitney, K.; Signaevsky, M.; Prastawa, M.; Iida, M.A.; White, C.L. ; 3rd, et al. Artificial intelligence-derived neurofibrillary tangle burden is associated with antemortem cognitive impairment. Acta Neuropathol Commun 2022, 10, 157. [Google Scholar] [CrossRef]
- Ingrassia, L.; Boluda, S.; Potier, M.C.; Haik, S.; Jimenez, G.; Kar, A.; Racoceanu, D.; Delatour, B.; and Stimmer, L. Automated deep learning segmentation of neuritic plaques and neurofibrillary tangles in Alzheimer disease brain sections using a proprietary software. J Neuropathol Exp Neurol 2024, 83, 752–762. [Google Scholar] [CrossRef]
- Meta (2024). https://ai.meta.com/resources/.
- He, B.; Bukhari, S.; Fox, E.; Abid, A.; Shen, J.; Kawas, C.; Corrada, M.; Montine, T.; and Zou, J. AI-enabled in silico immunohistochemical characterization for Alzheimer's disease. Cell Rep Methods 2022, 2, 100191. [Google Scholar] [CrossRef]
- Chang, J.; and Hatfield, B. Advancements in computer vision and pathology: Unraveling the potential of artificial intelligence for precision diagnosis and beyond. Adv Cancer Res 2024, 161, 431–478. [Google Scholar] [CrossRef] [PubMed]
- Unger, M.; and Kather, J.N. Deep learning in cancer genomics and histopathology. Genome Med 2024, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Bianchi, F.; Yuksekgonul, M.; Montine, T.J.; and Zou, J. A visual-language foundation model for pathology image analysis using medical Twitter. Nat Med 2023, 29, 2307–2316. [Google Scholar] [CrossRef] [PubMed]
- Schuhmann, C.; Beaumont, R.; Vencu, R.; Gordon, C.; Wightman, R.; Cherti, M.; Coombes, T.; Katta, A.; Mullis, C.; Wortsman, M.; et al. LAION-5B: An open large-scale dataset for training next generation image-text models. arXiv:2210.08402. 10.48550/arXiv.2210.08402. [CrossRef]
- Lu, M.Y.; Chen, B.; Williamson, D.F.K.; Chen, R.J.; Liang, I.; Ding, T.; Jaume, G.; Odintsov, I.; Le, L.P.; Gerber, G.; et al. A visual-language foundation model for computational pathology. Nat Med 2024, 30, 863–874. [Google Scholar] [CrossRef]
- Velicky, P.; Miguel, E.; Michalska, J.M.; Lyudchik, J.; Wei, D.; Lin, Z.; Watson, J.F.; Troidl, J.; Beyer, J.; Ben-Simon, Y.; et al. Dense 4D nanoscale reconstruction of living brain tissue. Nat Methods 2023, 20, 1256–1265. [Google Scholar] [CrossRef]
- Crist, A.M.; Hinkle, K.M.; Wang, X.; Moloney, C.M.; Matchett, B.J.; Labuzan, S.A.; Frankenhauser, I.; Azu, N.O.; Liesinger, A.M.; Lesser, E.R.; et al. Transcriptomic analysis to identify genes associated with selective hippocampal vulnerability in Alzheimer's disease. Nat Commun 2021, 12, 2311. [Google Scholar] [CrossRef]
- Gutt, J.; Isla, E.; Bertler, A.N.; Bodeker, G.E.; Bracegirdle, T.J.; Cavanagh, R.D.; Comiso, J.C.; Convey, P.; Cummings, V.; De Conto, R.; et al. Cross-disciplinarity in the advance of Antarctic ecosystem research. Mar Genomics 2018, 37, 1–17. [Google Scholar] [CrossRef]
- Morlett Paredes, A.; Guarena, L.A.; Stickel, A.M.; Schairer, C.E.; and Gonzalez, H.M. To donate, or not to donate, that is the question: Latino insights into brain donation. Alzheimers Dement 2023, 19, 1274–1280. [Google Scholar] [CrossRef]
- Fischl, B.; and Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc Natl Acad Sci U S A 2000, 97, 11050–11055. [Google Scholar] [CrossRef]
- Beekly, D.L.; Ramos, E.M.; van Belle, G.; Deitrich, W.; Clark, A.D.; Jacka, M.E.; Kukull, W.A.; and Centers, N.I.-A.s.D. The National Alzheimer's Coordinating Center (NACC) Database: an Alzheimer disease database. Alzheimer Dis Assoc Disord 2004, 18, 270–277. [Google Scholar]
- National Alzheimer's Coordinating Center (2024). https://naccdata.org/adrc-resources/best-practices.
- Fischl, B. FreeSurfer. Neuroimage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- Digital Imaging and Communications in Medicine (2024). https://dicom.nema.org/Dicom/DICOMWSI/.
- Moore, J.; Allan, C.; Besson, S.; Burel, J.M.; Diel, E.; Gault, D.; Kozlowski, K.; Lindner, D.; Linkert, M.; Manz, T.; et al. OME-NGFF: a next-generation file format for expanding bioimaging data-access strategies. Nat Methods 2021, 18, 1496–1498. [Google Scholar] [CrossRef]
Figure 1.
Transformative Neuropathology. Through a convergence of team science collaborations, human tissue-based studies have the unprecedented ability to uncover molecular clues that advance our diagnostic and prognostic understanding of complex brain diseases. The integration of these complementary fields fosters innovative approaches that bridge descriptive pathology with cutting-edge technologies, enabling precise identification of disease mechanisms, predictive diagnostics, and targeted therapeutic strategies. This holistic framework exemplifies the potential of transformative neuropathology in the modern era of advanced biomedical research. (Figure concept adapted from Gutt et al. [125]).
Figure 1.
Transformative Neuropathology. Through a convergence of team science collaborations, human tissue-based studies have the unprecedented ability to uncover molecular clues that advance our diagnostic and prognostic understanding of complex brain diseases. The integration of these complementary fields fosters innovative approaches that bridge descriptive pathology with cutting-edge technologies, enabling precise identification of disease mechanisms, predictive diagnostics, and targeted therapeutic strategies. This holistic framework exemplifies the potential of transformative neuropathology in the modern era of advanced biomedical research. (Figure concept adapted from Gutt et al. [125]).
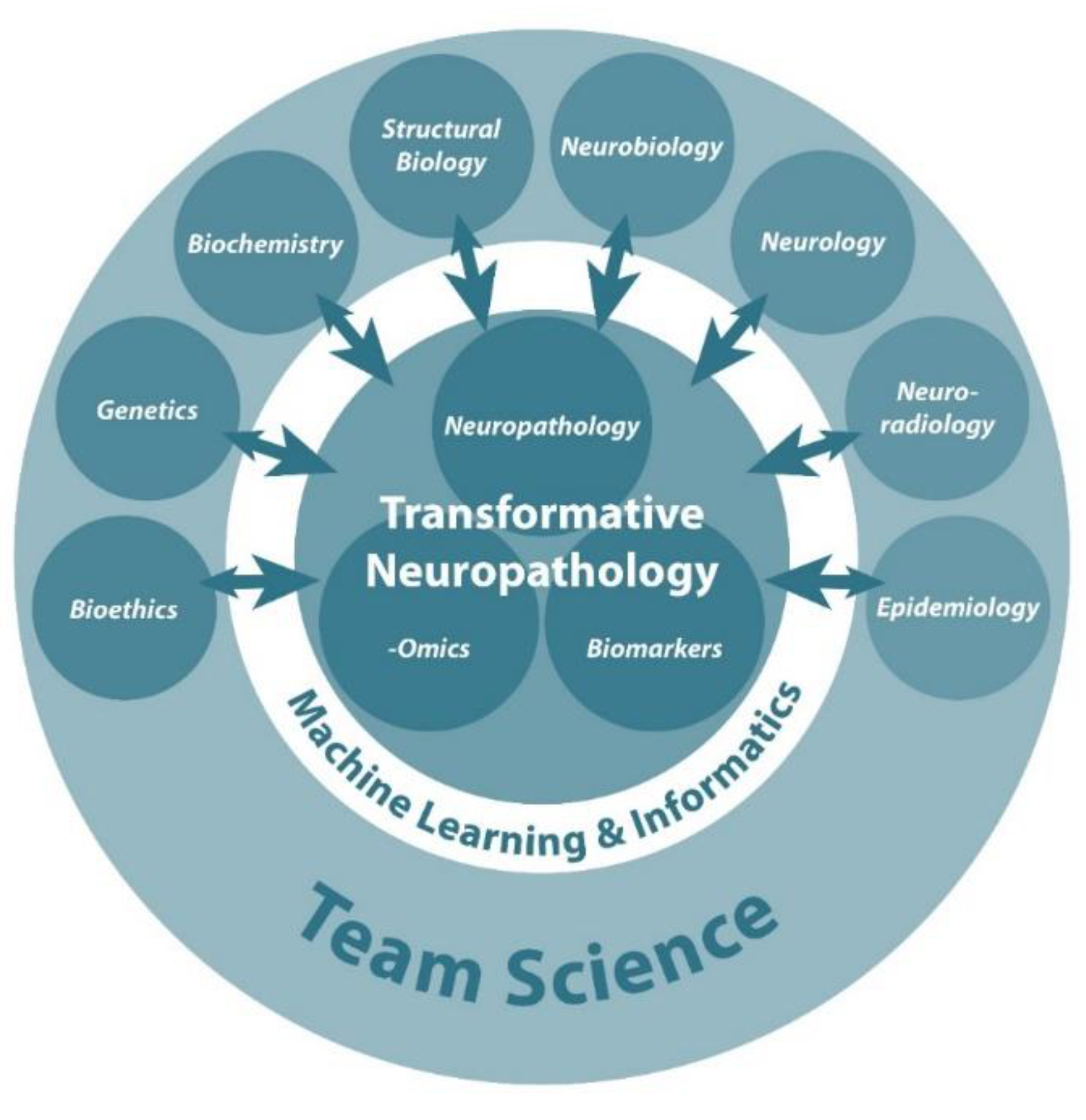
Figure 2.
Conceptual Framework of a Brain Bank. The successful brain bioresource will be closely linked to well-characterized clinical cohorts with detailed sequential clinical assessments, often including neuroimaging, and linked biospecimens such as blood and cerebrospinal fluid samples. This allows postmortem-derived data to be linked to data points across the evolution of the disorder under study. With return of -omics data back to brain banks and clinicopathologic data provision to bioinformaticians, the transformative potential remains endless. Informaticians (e.g., data scientist, bioinformatician, biostatistician) trained in the setting of a brain bank could enable a future where externally facing queryable databases drawing from electronic medical records. To ensure privacy and eliminate security concerns over stored genotype-phenotype data, analytic tools could be designed without the ability to decrypt genetic data. Such bidirectional approaches will result in multimodal tissue phenotyping, with digitally scanned slides being linked to protein immunohistochemistry, genomic data, spatial proteomics, and spatial transcriptomic data. Critical to the successful model, funded efforts would be undertaken to make all data available to the research community. Figure created in BioRender.
Figure 2.
Conceptual Framework of a Brain Bank. The successful brain bioresource will be closely linked to well-characterized clinical cohorts with detailed sequential clinical assessments, often including neuroimaging, and linked biospecimens such as blood and cerebrospinal fluid samples. This allows postmortem-derived data to be linked to data points across the evolution of the disorder under study. With return of -omics data back to brain banks and clinicopathologic data provision to bioinformaticians, the transformative potential remains endless. Informaticians (e.g., data scientist, bioinformatician, biostatistician) trained in the setting of a brain bank could enable a future where externally facing queryable databases drawing from electronic medical records. To ensure privacy and eliminate security concerns over stored genotype-phenotype data, analytic tools could be designed without the ability to decrypt genetic data. Such bidirectional approaches will result in multimodal tissue phenotyping, with digitally scanned slides being linked to protein immunohistochemistry, genomic data, spatial proteomics, and spatial transcriptomic data. Critical to the successful model, funded efforts would be undertaken to make all data available to the research community. Figure created in BioRender.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



