
Submitted:
30 December 2023
Posted:
03 January 2024
You are already at the latest version
Abstract
The kipping handstand push-up (kHSPU) is an exercise performed by many thousands of CrossFit participants. The safety of kHSPUs has been questioned because of vertical impacts upon the head. Here, we measured the axial loads placed upon the head during kHSPUs and sought to identify other factors that may place participants at risk of injury. 16 volunteers from a single gym performed 3 sets of up to 7 kHSPUs with their head and one hand contacting force platforms. Forces were recorded continuously and video recording were made while performing the exercises. The force profiles showed distinct landing and kipping peaks. Participants landed with more force than during their normal headstand, but less than their body weight. The force on the head was greatest during the "kip," and was usually more than body weight. Participants who reported pain following kHSPUs moved their head into extension during the exercises. Forces to the head during kHSPUs were below forces proposed for damage to the young male cervical spine, but overlapped those proposed for female cervical spines. While kipping handstand push-ups may be safe for young and previously uninjured male athletes, they may be unsafe for females and for those with previous injury or other compromising factors.
Keywords:
CrossFit
; coaching
; neck injury
; fitness
; biomechanics
Introduction
The kipping handstand push-up (kHSPU) is an exercise unique to CrossFit, and is hotly debated in terms of usefulness and
safety. Handstand pushups are quite difficult to perform, requiring substantial
strength in primarily the deltoids but also of the supporting muscles of the
shoulder girdle and torso. A variation of the exercise that allows the
participant to perform more repetitions involves “kipping.” After first
performing a back-facing handstand against a wall, the athlete then lowers
their body until their head lands on the floor (typically on a pad). The legs
are flexed into an upside-down squat position, and then forcibly pushed upwards
to gather vertical momentum (this is called the “kip”). The kip is coordinated
with pressing or pushing the body vertically back into the handstand position. Videos
of kHSPUs are readily available on the internet by searching “kipping handstand
push-up.”
Much controversy about the safety of kHSPUs appears
in online discussions, typically from clinically trained coaches. Arguments
include the possibility of neck injury and concussion, usually mentioning the
impact from the descent as the probable mechanism of injury. However, there has
been no study of the forces involved in kHSPUs, or the symptoms, if any,
secondary to performing them. Because the exercises involve the head relatively
slowly impacting the floor or a pad on each repetition, the chief concern is
neck injury. The incidence of neck injuries in CrossFit is reported to be 3-10%
of all injuries,1-4 but there are no published details regarding the
type or severity of the neck injuries that occur secondary to CrossFit
training, and none specifically mentioning kHSPUs.
There are limited data on forces to the head during
headstands and possible short- or long-term effects of this loading. Hector and
Jensen measured the forces on the head during headstands (Sirsasana pose) and
reported that participants placed 40-48% of their body weight on their heads
when stable.5 The only other possibly relevant data come from
studies of people who carried loads on their heads for employment.6-9
Not surprisingly, these studies show that chronic load bearing on the head
leads to premature cervical spinal degeneration, and that it seems independent
of the weight carried (10-100 Kg).7
There are more than 5 million CrossFit participants
worldwide, and kHSPUs are part of their routine programming. It is unknown how
many participants perform these exercises, but even if 25% of the participants
do perform them (estimate from the gym here involved), the safety information
is relevant for a large population. In this paper we provide the first analysis
of the forces exerted on the head during kHSPUs.
A draft of this manuscript was published as a
preprint: https://www.preprints.org/manuscript/202309.0271/v1
Materials and Methods
The primary outcome of this study was to
characterize the axial forces on the head during kHSPUs. These forces were
directly measured using force platforms (described below). To assess factors
that may contribute to neck injury, video recordings were made of the head
during the exercises. The number of final participants was not set until the
variability of the data was known. We stopped recruitment when the data
appeared representative of the population performing kHSPUs, meaning that the
variety of movements seen by both men and women appeared to have been captured
by the study population.
The protocol for this study was approved by the
Bove Consulting Institutional Review Board (#2022-01). We recruited 16
participants from a single CrossFit gym by word of mouth and by notices placed
in the gym. The standard method of performing kipping handstand pushups is
available online on CrossFit and other websites, and participants are
supervised by credentialed coaches. Therefore, a sample from any
well-established gym is likely to be representative of the population
performing kHSPUs. Inclusion criteria included the willingness to participate,
being at least 18 years old, and having the ability to perform at least 2
kHSPUs. Exclusion criteria included the inability to perform the exercises. Participants
included 6 female and 10 male adults, ranging from 23 to 66 years old (Table 1). The investigator explained the
procedures to each participant, and gave each an approved consent form to read
and sign prior to beginning participation.
Each participant was asked questions regarding
their performance of kHSPUs and other similar exercises to qualitatively
establish their relative strength and skill level (Table 1). Each participant was asked if they
experienced neck pain or headaches that were associated with performing kHSPUs.
Two force platforms (PASPORT, PASCO, USA) and one
plywood platform were covered with 5 cm thick foam cushions and covered with
heavy polyester fabric. The density of the foam and the covering were similar
to the exercise mats used by most athletes when performing this exercise. The
platforms were positioned to measure the forces experienced by the head and by
the right hand (only two force platforms were available). Platforms were placed
level and in the same plane, slightly offset so that the head and hands would
land close to their centers. The force platforms were connected to a bridge
amplifier (SPARKlink® Air, PASCO, USA), which was connected to a computer running Capstone software
(PASCO, USA). The accuracy and precision of the measurements were confirmed
using manufacturer’s instructions. Video recordings focused on the head of each
participant were made using the camera of an iPhone 10 to track movement of the
head during the kHSPUs. The device was placed on a tripod 20 cm from the floor
and took 30 frames per second.
Participants were asked to warm up as they felt was
appropriate, before starting. When ready, the participant stood on the middle
platform for at least 5 seconds to measure their weight. Then the participant
went into a handstand for at least 5 seconds to obtain a stable force
measurement. They then to descended into a headstand for at least 5 seconds to
obtain a stable force measurement. The subjects then returned to standing. When
ready, the participants performed 3 sets of up to 7 kHSPUs (maximum 21 repetitions),
with rests between sets as desired. They were specifically instructed to
perform the exercises as they normally do, meaning that their repetition speed
and all other parameters of the exercises were not dictated or controlled other
than by the participant. Data were collected at 1kHz and saved for offline
analysis.

Table 1.
Participant demographics. The participant numbers in this table are matched to those in the figures. *= Body mass as dressed, CF = CrossFit, kHSPU = maximum number of kipping handstand push-ups participant reported they were capable of performing, Strict = number of handstand pushups the participant reported they were capable of performing without kipping.
Table 1.
Participant demographics. The participant numbers in this table are matched to those in the figures. *= Body mass as dressed, CF = CrossFit, kHSPU = maximum number of kipping handstand push-ups participant reported they were capable of performing, Strict = number of handstand pushups the participant reported they were capable of performing without kipping.
| Participant | Age | Sex | Height (M) | Mass (Kg)* | Years of CF | Years kHSPU | # kHSPU | # Strict | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 23 | F | 1.63 | 73.3 | 6 | 4 | 20 | 12 | ||
| 2 | 24 | M | 1.78 | 78.7 | 8 | 7 | 20 | 8 | ||
| 3 | 50 | M | 1.83 | 96.2 | 5 | 5 | 10 | 0 | ||
| 4 | 39 | M | 1.83 | 79.7 | 3 | 2 | 15 | 8 | ||
| 5 | 38 | M | 1.78 | 89.8 | 12 | 8 | 7 | 5 | ||
| 6 | 29 | F | 1.56 | 63.7 | 2 | 2 | 7 | 2 | ||
| 7 | 40 | M | 1.73 | 84.0 | 10 | 10 | 20 | 10 | ||
| 8 | 40 | F | 1.65 | 65.7 | 6 | 5 | 12 | 0 | ||
| 9 | 44 | M | 1.65 | 85.3 | 10 | 9 | 30 | 15 | ||
| 10 | 29 | M | 1.93 | 102.2 | 3 | 2 | 30 | 15 | ||
| 11 | 36 | F | 1.68 | 64.5 | 10 | 2 | 20 | 2 | ||
| 12 | 49 | F | 1.52 | 63.3 | 7 | 6 | 10 | 0 | ||
| 13 | 26 | M | 1.75 | 79.9 | 4 | 3 | 38 | 20 | ||
| 14 | 31 | M | 1.89 | 96.0 | 1 | 1 | 10 | 1 | ||
| 15 | 66 | M | 1.8 | 83.6 | 6 | 4 | 20 | 0 | ||
| 16 | 33 | F | 1.52 | 58.2 | 7 | 5 | 8 | 15 | ||
| Mean | 6.3 | 4.7 | 17.3 | 7.1 | ||||||
| SD | 3.2 | 2.7 | 9.2 | 6.7 | ||||||
We imported data into Spike 2 (CED, UK; this is a waveform analysis tool) for analysis. The peak forces exerted by the head on the force platforms and the event times were collected for individual kHSPUs using the cursors supplied with the program (Figure 1A). Because the more detailed methods of data extraction used were largely developed while analyzing the data, they are considered results and are presented in that section. We imported video recordings into Kinovea 0.9.5 10 for movement analysis. During at least two repetitions, the path of the external acoustic meatus was tracked, paying particular attention to the path during the weight-bearing phase of the exercise.
Statistical analyses and graphing were performed using Prism 9.5. ANOVA was used to compare within-group variability. Because the purpose of this report does not include statistical comparison of participants, post-hoc tests are not reported with the ANOVA analyses. Multiple unpaired t-tests were used to compare kipping forces to landing forces. Spearman r was used to seek correlation between otherwise disparate measures, such as landing force and body weight. Fisher’s exact tests were used to determine if there was a relationship between reported pain symptoms and head movements during the loaded phase of the exercises. A Mann-Whitney U test was performed to compare the report of pain following the exercises to the time of the loaded phase of the exercises. For all comparisons, p ≤ 0.05 was considered statistically significant.
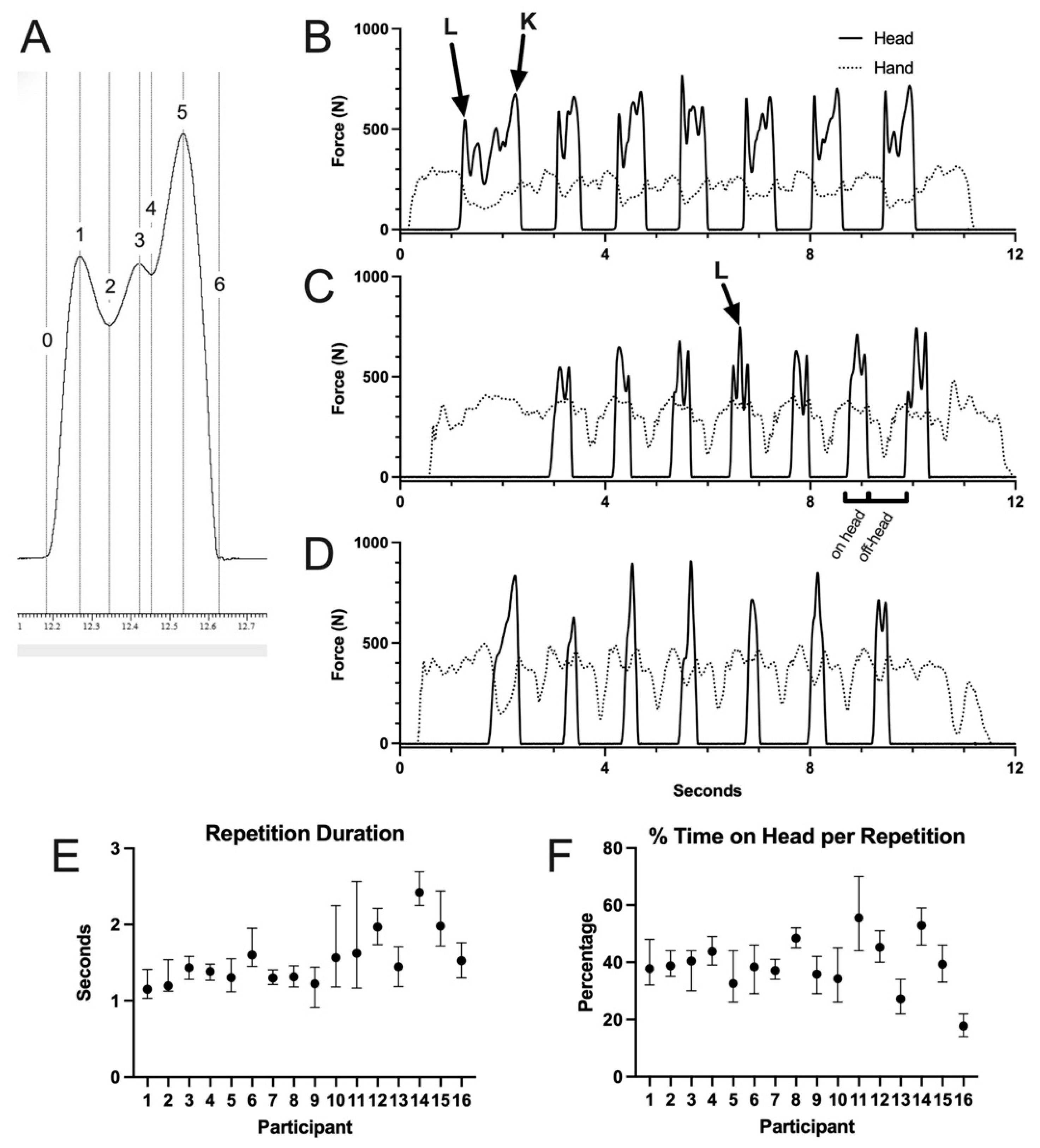
Figure 1.
Representative recordings of forces on head during kipping handstand pushups (kHSPUs). A. Typical force waveform of a single repetition showing points measured. In this waveform, the peaks indicated by 1 and 5 were used for the landing and kipping forces, respectively. The time between 0 and 6 was recorded as the repetition duration. Peaks 2, 3, and 4 were used as required to calculate the landing or kipping force if necessary (such as in 1C, at “L”). Traces B, C, and D reflect the variety of kHSPU performance. All recordings are raw data of single sessions of repetitions. L = landing forces recorded, K = kipping force recorded. In C, the brackets show the time on head and time off-head, which combined were taken as the repetition duration. E. Repetition duration for each participant. F. Percentage of time on head for each repetition.
Figure 1.
Representative recordings of forces on head during kipping handstand pushups (kHSPUs). A. Typical force waveform of a single repetition showing points measured. In this waveform, the peaks indicated by 1 and 5 were used for the landing and kipping forces, respectively. The time between 0 and 6 was recorded as the repetition duration. Peaks 2, 3, and 4 were used as required to calculate the landing or kipping force if necessary (such as in 1C, at “L”). Traces B, C, and D reflect the variety of kHSPU performance. All recordings are raw data of single sessions of repetitions. L = landing forces recorded, K = kipping force recorded. In C, the brackets show the time on head and time off-head, which combined were taken as the repetition duration. E. Repetition duration for each participant. F. Percentage of time on head for each repetition.
Results
Most participants were considered advanced in terms of how long they had been attending any CrossFit gym, how long they had been able to perform kHSPUs, and how many they could perform. Twelve participants completed 21 kHSPU repetitions, with the others completing 15, 17, 18, and 20 repetitions. We recorded the force profiles of 322 kHSPUs. The force profiles were surprisingly complex (Figure 1). The first force peak occurred when the head initially contacted the pad (Figure 1A, arrow “L”), which we called the “landing force.” The last force peak was when the participant “kipped,” the process by which the legs were actively drawn towards the chest (reducing the force on the head) and then forcibly pushed upwards for momentum (increasing the force on the head; Figure 1A, arrow “K”). We called this peak the “kip force.” In 60% of the recordings, more peaks could be seen (Figure 1 A-B). These peaks were more pronounced in participants who were more deliberately bringing their legs into kipping position to ready themselves for the kip (confirmed using other full body video recordings, after the primary data collection and solely for this purpose). When present, the higher of the two was recorded as the landing force (Figure 1B, arrow “L”). Peaks also occurred due to rebound of the entire body or more mobile parts of the body, and if later in the repetition, could occur because of unloading some weight from the wall (while on the head, the posterior pelvis rests against the wall) or because of impact of the heels on the wall before the unloading was complete. These forces were not reported. When only two clear peaks were discernable (30% of recordings), they were recorded as the landing and kip forces. When only one peak was discernable (10% of the recordings), as in Figure 1C for 6 of 7 repetitions, it was recorded as the kip force. Repetition durations were calculated by combining one duration on the head and one adjacent duration off the head (see Figure 1B). Most participants showed consistent total repetition durations and percent of that duration on the head (Figure 1D-E), but there were significant differences between participants (total repetition durations F (15, 69) = 52.8, p < 0.001; % repetition duration on head F (15,100) = 70.1, p < 0.001).
Participants placed 69% (12.5 SD) of their body weight on their head during the headstand performed prior to the kHSPUs. The mean landing forces, with ranges to show the maximum and minimum forces, are shown for each participant in Figure 2A, and are expressed as a percentage of body weight in Figure 2B. The landing forces were more than the measured headstand force, but typically less than their body weight. The mean peak landing force (n = 16, Figure 2A, top of range bars) was 896 N (SD = 232 N). There was a statistically significant difference in mean landing force between participants by non-parametric ANOVA (F (15, 137) = 37.7, p < 0.001). The mean landing forces were positively correlated to body weight (Spearman r = 0.67, p <0.05).
The kipping forces are similarly depicted (Figure 2C-D). The kipping forces were typically higher than the body weight. The mean kipping forces were statistically significantly higher than the landing forces for 10, lower for 2, and not different for 4 participants (multiple unpaired t-tests; Figure 2E). The mean peak kipping force (n = 16, Figure 2C, top of range bars) was 991 N (SD = 189 N). Kipping forces differed between participants (F (15,189) = 81.4, p < 0.001), and were also positively correlated to body weight (r = 0.57, p <0.05).
The peak landing and kipping forces for each participant compared to published failure forces of the cervical spine (also see discussion) can be seen in Figure 2F.
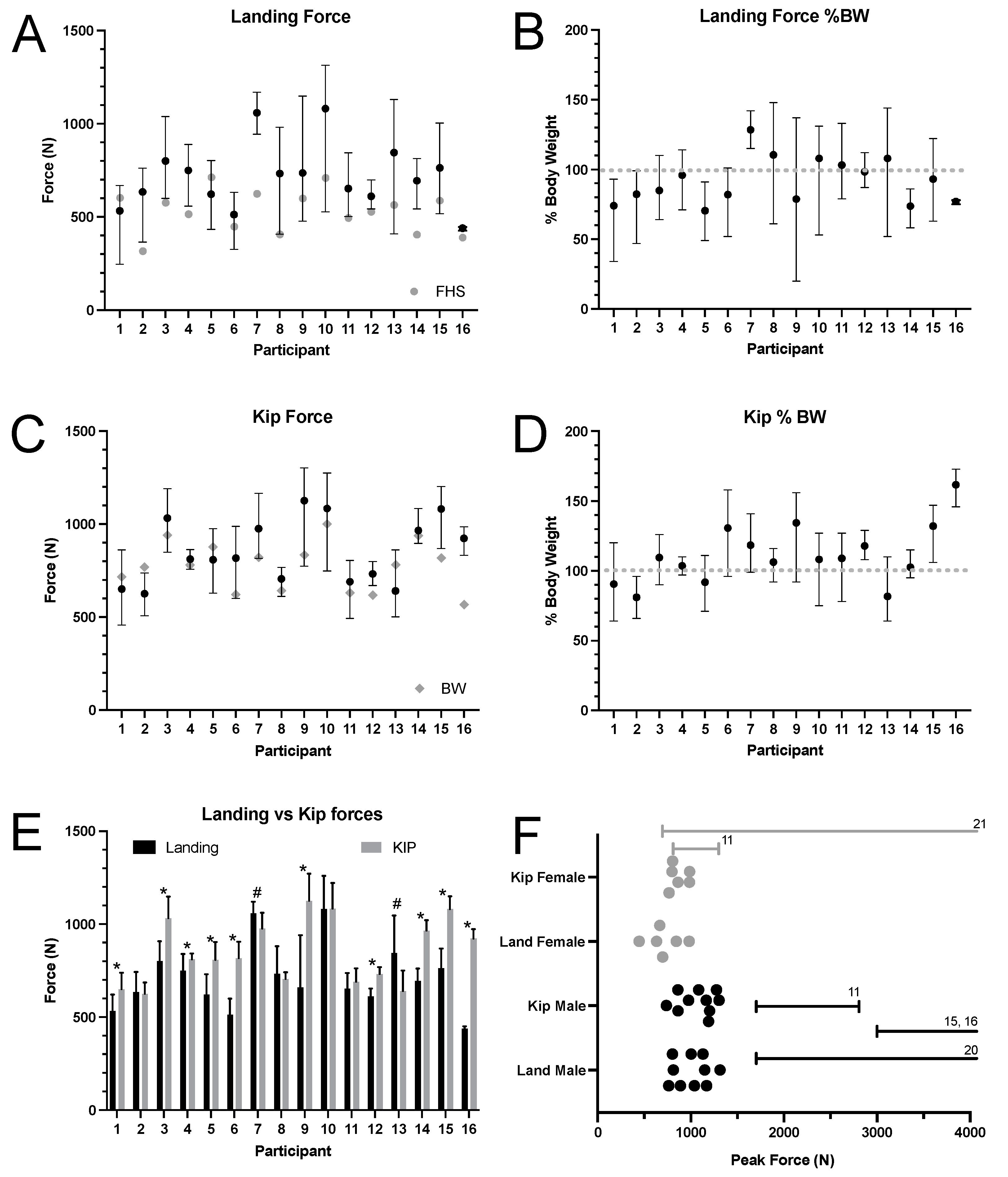
Figure 2.
Forces on head during kHSPUs for each participant. A and C. Landing and kipping forces are depicted (means with ranges). In A, gray circles are the force measured during headstand (FHS). In C, gray diamonds are body weights. B and D. Landing and kipping forces expressed as the percentage of body weight. 100% Body weight shown with interrupted gray line. E. Comparison of landing and kipping forces (means with SDs). * = kipping higher than landing, # = landing higher than kipping (t-tests, p≤0.05). F. Maximum landing and kipping forces for each participant. Bars represent published ranges of forces shown to cause neck injury from axial loads to head (numbers correlate to source references).
Figure 2.
Forces on head during kHSPUs for each participant. A and C. Landing and kipping forces are depicted (means with ranges). In A, gray circles are the force measured during headstand (FHS). In C, gray diamonds are body weights. B and D. Landing and kipping forces expressed as the percentage of body weight. 100% Body weight shown with interrupted gray line. E. Comparison of landing and kipping forces (means with SDs). * = kipping higher than landing, # = landing higher than kipping (t-tests, p≤0.05). F. Maximum landing and kipping forces for each participant. Bars represent published ranges of forces shown to cause neck injury from axial loads to head (numbers correlate to source references).
Most participants (n = 10) had minimal to no head movement in the sagittal plane during the load-bearing part of the kHSPU, displaying an elliptical movement of the head (as indicated by the external acoustic meatus) during each repetition (Figure 3A). Because this was most frequently observed pattern, was observed in the most advanced participants, and because none of these participants reported pain related to kHSPUs, it was adopted as “characteristic.” However, the other 6 participants showed movement into extension during loadbearing (4 during the landing impact (Figure 3B) and 2 during the kip (Figure 3C)). None moved into flexion.
Five of the 16 participants (31%) reported having neck stiffness, pain, and/or headaches following kHSPUs. All 5 showed neck movement during the head load-bearing phase, moving into extension (Figure 3 B-C). A Fisher’s exact test showed a significant association between the report of pain and movement during the loadbearing phase (p = 0.001) with a positive predictive value of 0.83. There was no relationship between the presence or absence of reported pain and mean duration on the head (Mann-Whitney U test, p = 0.712). The participants were separated into groups by the presence (n=5) or absence (n=11) of symptoms after performing kHSPUs, and the force data were compared. There were no statistically significant differences between these groups in landing or kip forces (raw or %BW), or duration on the head.
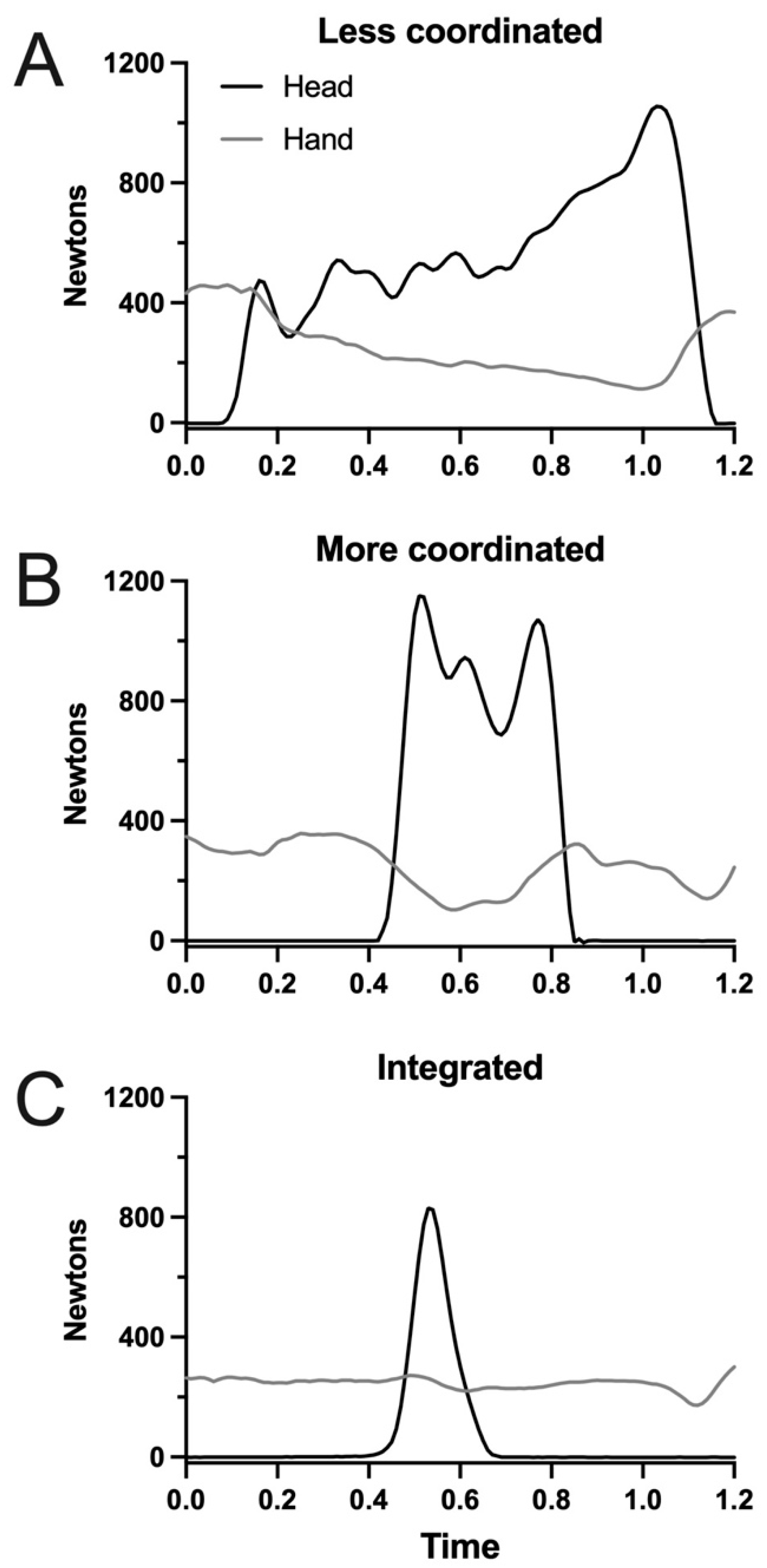
Comparisons were made to quantify and qualify participant skill and fatigue, which may be related to safety. The mean duration on the head was strongly statistically correlated to the sum of the number of peaks per participant (from all repetitions; Spearman r = 0.78, p = 0.001), which seemed to be related to coordination of the movements. Traces were subjectively evaluated for smoothness (Figure 4A-C), with the intent to judge relative coordination. As can be appreciated in Figure 4A, the longer duration on the head also showed a higher variability of the forces on the head. This reflects the gradual lowering of the legs in preparation for the kip. A more coordinated movement is represented in Figure 4B, where the trace is smooth and the force exerted by the hand increased with the head leaving the force platform. The seemingly most coordinated pattern is seen in Figure 4C (participant 16), where there is almost constant force by the hand, a short time on the head, and one peak. This is referred to as “integrated.” For each participant, simple linear regression of the repetition speed, duration on and off the head, and landing and kip forces were performed. None of these changed with the number of repetitions (data not shown), which was interpreted as indicating that the participants did not fatigue enough during the sets to alter their movement patterns.
Discussion
In this report we describe the forces borne by the head during kHSPUs. The forces ranged from 0.5 - 1.300 kN, which are below the reported threshold for catastrophic failure predicted for young males with healthy spines but overlap with published failure levels for females (however, see discussion below). An important observation was that the forces were higher during the kip than during the landing. Head movement during the load-bearing phase of the exercise was strongly correlated with self-reports of post-exercise neck pain and/or headache.
One limitation of this study may be that the sample size was determined subjectively, when the author concluded that the movement patterns observed were representative of the larger population, and that the study was performed at one facility. Studying participants from other gyms may have led to more diverse observations.
The primary limitation of this study is in terms of interpretation since there are no clear published data to allow a conclusion of “safe” versus “unsafe.” It is unethical to prospectively study forces that cause damage in living humans, which is reflected in the relative lack of literature to which direct comparisons can be made to the observations of this study. The published literature taken together support that 3.6 - 4kN is the tolerance of the healthy young male cervical spine to catastrophic injury,11,12 but forces in the range here reported are close to those shown to cause severe injury in some experiments,11,13-17 The population performing this exercise includes males and females of all ages (and nationality). While the difference in the forces for males shown in Figure 2F in comparison to the published forces may seem acceptable for most healthy participants it must be stressed that the tolerance forces were proposed for young male cervical spines without degeneration, and are the limits at which catastrophic injuries occur. Older and female spines can be expected to have a lower tolerance for injury.18 Cervical spinal degeneration occurs secondary to injuries, occurs in most individuals as they age,19 and reduces the strength of the spinal holding elements,20 all of which render individuals more susceptible to compressive injuries.21 Our data support that these exercises should not be considered safe for females.
The observation that the kipping forces were higher than the landing forces is important. Participants should know that they will not avoid high forces to the head by attempts to land relatively gently. As examples, although data on previous injuries were not collected for all participants, two of the participants, both <30 years old, stated that they had suffered multiple concussions during sports, and thus attempted to land relatively gently on their heads (which they did). One of them (participant 2) had among the lowest peak kip forces, but the other (participant 6) had a much higher peak kip force (0.98 kN) compared to their peak landing force (0.63 kN). The alternative is to not land on the head at all, and bear the momentum of the kip using the shoulder muscles. In that case, it becomes easier to perform the “strict” handstand pushup, without kipping. In that form of the exercise, there is minimal to no force on the head.
We observed a high rate of post-kHSPU symptoms (31%), and show that movement of the head into extension during these exercises is a positive predictor for neck pain and/or headaches. While there is no way to strengthen the neck to withstand compression, it is possible to strengthen and train towards greater stability. Modeled as a column, the cervical spine is stiffest and thus more capable of withstanding axial loading when the force vector passes through the occipital condyles and the T1 vertebral body.22,23 Any bending compromises the stiffness of the cervical spine, and renders it more susceptible to injury.20 All who perform these exercises should be taught to keep their neck as stiff and stable as possible, and to position their head so that their vertex contacts the floor (or pad).
There has been no report, including case studies, of injuries following kHSPUs. Some participants in our study had been performing kHSPUs regularly for up to 12 years with no reported negative effect. We cannot explain this apparent disparity, and it presents more difficulty with making a blanket statement about safety. However, since a history of head and neck injury, degenerative changes, and age are known to reduce neck load bearing capability, such athletes should be dissuaded from performing kHSPUs. The motions of the head (and likely the neck) observed in this study, which were associated with post-kHSPU pain, were not readily appreciated, but were apparent using slow motion video. It is recommended that coaches perform this relatively easy analysis on athletes, especially those who suffer post-kHSPU symptoms. Athletes and coaches should also know that more padding will cause more force to be translated to the neck.11,23
Kipping HSPUs are unique, quirky, and fun, and require strength and coordination. However, we show here that they appear unsafe for females to perform, since the forces are overlapping with those published as causing severe neck injury. Age and previous injury are also critical to consider when making the decision to participate in this exercise. As in American football, where concussions occur regularly, kHSPUs will likely remain an exercise performed by many thousands of people worldwide. The participants in this study had all received similar coaching, where proper head posture and neck bracing during these exercises was stressed. These exercises are typically performed while a clock is running, and technique can become secondary to performing the maximum number of repetitions, at the discretion of the athlete. It is hoped that further study into the incidence of post-kSPHU symptoms will be performed to allow better coaching towards kHSPU safety.
Author Contributions
GMB conceptualized and designed the study, collected and analyzed the data, and wrote the manuscript.
Institutional Review Board Statement
This study involved human participants and IRB approval was obtained.
Acknowledgments
The author thanks the owner of CrossFit Rising Tide for allowing the study to be performed within their facility, and thanks each athlete who volunteered to be part of this study. There was no external funding for this study.
Conflicts of Interest
The author declares that there are no financial or other conflicts of interest.
References
- Feito Y, Burrows Ek, Tabb Lp. A 4-Year Analysis Of The Incidence Of Injuries Among Crossfit-Trained Participants. Orthop J Sports Med. 2018, 6, 1–8. [CrossRef]
- Szeles Prq, Da Costa Ts, Da Cunha Ra; et al. Crossfit And The Epidemiology Of Musculoskeletal Injuries: A Prospective 12-Week Cohort Study. Orthop J Sports Med. 2020, 8, 1–9. [CrossRef]
- Mehrab M, De Vos Rj, Kraan Ga, Mathijssen Nmc. Injury Incidence And Patterns Among Dutch Crossfit Athletes. Orthop J Sports Med. 2017, 5, 1–13. [CrossRef]
- Montalvo Am, Shaefer H, Rodriguez B, Li T, Epnere K, Myer Gd. Retrospective Injury Epidemiology And Risk Factors For Injury In Crossfit. J Sports Sci Med. 2017, 16, 53–59.
- Hector R, Jensen Jl. Sirsasana (Headstand) Technique Alters Head/Neck Loading: Considerations For Safety. J Bodyw Mov Ther. 2015, 19, 434–441. [CrossRef]
- Dave Br, Krishnan A, Rai Rr, Degulmadi D, Mayi S. The Effect Of Head Loading On Cervical Spine In Manual Laborers. Asian Spine J. 2021, 15, 17–22. [CrossRef] [PubMed]
- Jäger Hj, Gordon-Harris L, Mehring Um, Goetz Gf, Mathias Kd. Degenerative Change In The Cervical Spine And Load-Carrying On The Head. Skeletal Radiol. 1997, 26, 475–481. [CrossRef]
- Levy, Lf. Porter’s Neck. Br Med J. 1968, 2, 16–19. [Google Scholar] [CrossRef]
- Joosab M, Torode M, Rao Pv. Preliminary Findings On The Effect Of Load-Carrying To The Structural Integrity Of The Cervical Spine. Surg Radiol Anat. 1994, 16, 393–398. [CrossRef]
- Charmont J. Kinovea (0.9.5). 2021.
- Nightingale Rw, Mcelhaney Jh, Camacho Dl, Kleinberger M, Winkelstein Ba, Myers Bs. The Dynamic Responses Of The Cervical Spine: Buckling, End Conditions, And Tolerance In Compressive Impacts. Sae Transactions. 1997, 106, 3968–3988.
- Nightingale Rw, Mcelhaney Jh, Richardson Wj, Myers Bs. Dynamic Responses Of The Head And Cervical Spine To Axial Impact Loading. J Biomech. 1996, 29, 307–318. [CrossRef] [PubMed]
- Nusholtz Gs, Melvin Jw, Huelke Df, Alem Nm, Blank Jg. Response Of The Cervical Spine To Superior—Inferior Head Impact. Sae Transactions. 1981, 90, 3144–3162.
- Alem Nm, Nusholtz Gs, Melvin Jw. Head And Neck Response To Axial Impacts. Sae Transactions. 1984, 93, 927–940.
- Yoganandan N, Sances A, Jr., Maiman Dj, Myklebust Jb, Pech P, Larson Sj. Experimental Spinal Injuries With Vertical Impact. Spine (Phila Pa 1976). 1986, 11, 855–860. [CrossRef]
- Alem Nm, Nusholtz Gs, Melvin Jw. Superior-Inferior Head Impact Tolerance Levels. Ann Arbor, Michigan: University Of Michigan Transportation Research Institute; 1982.
- Yoganandan N, Pintar Fa, Humm Jr, Maiman Dj, Voo L, Merkle A. Cervical Spine Injuries, Mechanisms, Stability And Ais Scores From Vertical Loading Applied To Military Environments. Eur Spine J. 2016, 25, 2193–2201. [CrossRef]
- Pintar Fa, Yoganandan N, Voo L. Effect Of Age And Loading Rate On Human Cervical Spine Injury Threshold. Spine (Phila Pa 1976). 1998, 23, 1957–1962. [CrossRef]
- Tao Y, Galbusera F, Niemeyer F, Samartzis D, Vogele D, Wilke Hj. Radiographic Cervical Spine Degenerative Findings: A Study On A Large Population From Age 18 To 97 Years. Eur Spine J. 2021, 30, 431–443. [CrossRef] [PubMed]
- Maiman Dj, Sances A, Jr., Myklebust Jb; et al. Compression Injuries Of The Cervical Spine: A Biomechanical Analysis. Neurosurgery. 1983, 13, 254–260. [CrossRef] [PubMed]
- Yoganandan N, Chirvi S, Voo L, Pintar Fa, Banerjee A. Role Of Age And Injury Mechanism On Cervical Spine Injury Tolerance From Head Contact Loading. Traffic Inj Prev. 2018, 19, 165–172. [CrossRef]
- Cusick Jf, Yoganandan N. Biomechanics Of The Cervical Spine 4: Major Injuries. Clin Biomech (Bristol, Avon). 2002, 17, 1–20. [CrossRef]
- Pintar Fa, Yoganandan N, Voo L, Cusick Jf, Maiman Dj, Sances A. Dynamic Characteristics Of The Human Cervical Spine. 1995.
Figure 3.
Head movements during kHSPUs. A. The head and neck remained stable during the weight-bearing phase (participant #1). The arrow indicates the direction of the path of the external acoustic meatus (EAM) during one full repetition. This overall pattern of movement was shared by the more experienced participants, and was accepted by this analysis as “good technique.” B. The EAM moved forward during the landing. C. The EAM moved forward just prior to the kip. In both B and C, the arrow indicates the direction of the movement, which is reversed from A. These paths of the EAM indicate neck extension during the kip; both participants reported neck pain and headaches following kHSPUs.
Figure 3.
Head movements during kHSPUs. A. The head and neck remained stable during the weight-bearing phase (participant #1). The arrow indicates the direction of the path of the external acoustic meatus (EAM) during one full repetition. This overall pattern of movement was shared by the more experienced participants, and was accepted by this analysis as “good technique.” B. The EAM moved forward during the landing. C. The EAM moved forward just prior to the kip. In both B and C, the arrow indicates the direction of the movement, which is reversed from A. These paths of the EAM indicate neck extension during the kip; both participants reported neck pain and headaches following kHSPUs.
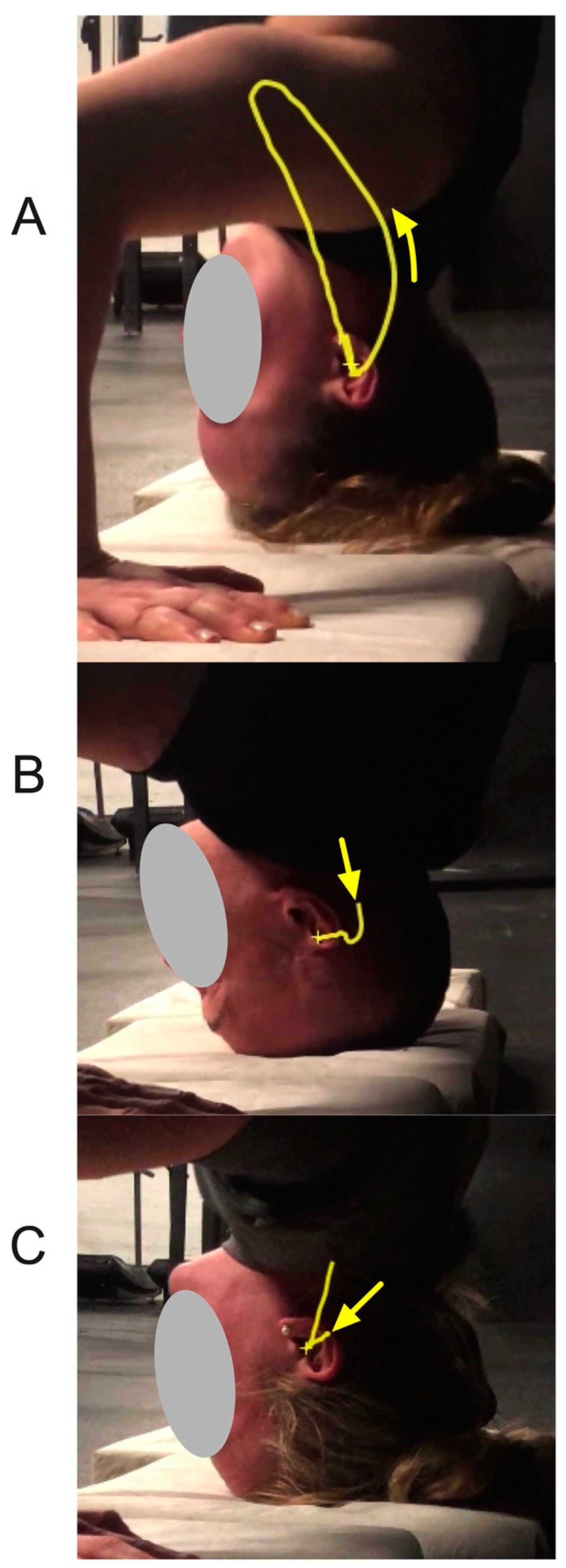
Figure 4.
Sample force profiles suggesting coordination differences among participants. A. The relatively long duration and varying force on the head is consistent with the inexperience of this participant (<1 year). B. This was the most typical force profile, showing the initial landing force, a smaller force when the legs came into kipping position, and the kip force, with smooth transitions. C. This force profile was considered to reflect the most coordinated effort and most efficient exercise, which we have termed “integrated.” Note that the force on the hand remained steady, indicating that the participant (#16) did not rest on their head during the exercises. Yet, this participant (#16) still placed >800N (~1.5X body weight) on their head during the kip (Figure 2 C-D). .
Figure 4.
Sample force profiles suggesting coordination differences among participants. A. The relatively long duration and varying force on the head is consistent with the inexperience of this participant (<1 year). B. This was the most typical force profile, showing the initial landing force, a smaller force when the legs came into kipping position, and the kip force, with smooth transitions. C. This force profile was considered to reflect the most coordinated effort and most efficient exercise, which we have termed “integrated.” Note that the force on the hand remained steady, indicating that the participant (#16) did not rest on their head during the exercises. Yet, this participant (#16) still placed >800N (~1.5X body weight) on their head during the kip (Figure 2 C-D). .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



