
Submitted:
30 June 2023
Posted:
04 July 2023
You are already at the latest version
Abstract
(1) Background: This study aimed to identify the recurrence and survival rates according to the mismatch repair (MMR), p53, and L1 cell adhesion molecule (L1CAM) states in patients with advanced and recurrent endometrial cancer receiving systemic chemotherapy.; (2) Methods: This single-center retrospective cohort study included chemotherapy-naïve patients (n=156) with advanced-stage (III/IV) or recurrent endometrial cancer who were administered chemotherapy as adjuvant therapy (n=112) or first-line palliative treatment (n=44) between January 2015 and June 2022. MMR and p53 states were assessed using PCR, and L1CAM was tested using immunohistochemistry in the no specific molecular profile (NSMP) group. The primary outcomes were progression-free survival (PFS) and overall survival (OS).; (3) Results: Of the 156 patients, 62 (39.7%), 53 (34.0%), and 41 (26.3%) had NSMP, abnormal p53 (p53abn), and an MMR deficiency (MMR-D), respectively. PFS and OS were longest in MMR-D, followed by NSMP, and were the least in p53abn tumors (PFS: p=0.0006, OS: p=0.0013). After NSMP was classified according to positive or negative L1CAM status, the L1CAM-negative group exhibited significantly lower survival rates than the L1CAM-positive group (PFS: p=0.0001, OS: p=0.0027); p53abn tumors were independent prognostic factors for poor PFS (p=0.039 on the multivariable analysis).; (4) Conclusions: In chemotherapy-naïve patients with advanced and recurrent endometrial cancer, the best prognosis after chemotherapy was obtained using MMR-D, followed by NSMP and p53abn tumors. The L1CAM status is a useful new marker for stratifying NSMP in advanced and recurrent patients.
Keywords:
Endometrial neoplasms
; molecular classification
; Neural cell adhesion molecule L1 (L1CAM)
; Prognosis
; Recurrence
; Survival
1. Introduction
Endometrial cancer (EC) is the sixth most common cancer in women. Approximately 417,000 new patients are identified annually; approximately 97,000 die [1]. An increase in cases from 727 in 1999 to 3287 in 2019 has been observed in Korea. This increase is likely caused by increased exposure to endogenous and exogenous estrogens associated with risk factors such as obesity, diabetes, and increased life expectancy [2,3].
The Cancer Genome Atlas (TCGA) Research Network used whole-genome sequencing to divide EC into four molecular subtypes: DNA polymerase epsilon (POLE)–mutated (ultra-mutated), microsatellite instability-high (MSI-H, hypermutated), copy-number low, and copy-number high. Prognoses differ according to the subtype [4].
The subtypes are more easily classified as mismatch repair (MMR) defective (MMR-D, an MSI-H surrogate), POLE exonuclease domain mutant (a POLE-mutated surrogate), p53 wild type, and p53 null/missense mutant (no specific molecular profile [NSMP] and p53-abnormal [p53abn], surrogates of copy-number low and copy-number high, respectively). Sequencing the DNA of MMR proteins, p53, and the POLE exonuclease domain is a surrogate for immunohistochemistry (IHC) in TCGA classification [5]. Through this subgrouping, the European Society of Gynaecological Oncology has recently suggested new treatment protocols [6]. However, despite these classifications and treatment guidelines, studies on predicting chemotherapy prognoses according to the molecular subtype have not been conducted in patients with advanced and recurrent EC who have not received adjuvant chemotherapy as the primary treatment.
Among many studies on new markers beyond the current classification, the importance of L1CAM, an L1 protein, is emerging. Therefore, evaluating whether a new classification using this marker can be used for determining the prognoses of patients with advanced EC and recurrent EC requiring primary adjuvant therapy is necessary [7]. Therefore, this study examined the prognoses of patients with advanced and recurrent EC who received chemotherapy as adjuvant or palliative therapy. Progression-free survival (PFS) and overall survival (OS) were studied to determine the utility of L1CAM as a prognostic marker for these patients.
2. Materials and Methods
This retrospective cohort study was conducted at the Severance Hospital of the Yonsei University Health System (YUHS, 4-2023-0263).
2.1. Study Population
Patients who met the following inclusion criteria during the period from January 2015 to June 2022 were identified: (1) advanced-stage (III/IV) and recurrent EC with the first recurrence after diagnosis and never treated with chemotherapy, and (2) adjuvant therapy or treatment therapy after recurrence.
2.2. Immunohistochemistry
Formalin-fixed paraffin-embedded slices (4 μm) were deparaffinized and hydrated using xylene and alcohol solutions. Immunostaining was performed using a Ventana Benchmark XT automatic immunostaining instrument (Ventana Medical Systems; Tucson, AZ, USA) according to the manufacturer’s instructions. IHC for MMR proteins (MLH1, MSH2, MSH6, PMS2), p53, and L1CAM were performed using the following antibodies: MutL homolog 1 (MLH1, 1:50; BD Biosciences; San Jose, CA, USA), MutS homolog 2 (MSH2, 1:200; BD Biosciences), MutS homolog 6 (MSH6, 1:100; Cell Marque; Rocklin, CA, USA), PMS1 homolog 2 (PMS2, diluted 1:40, Cell Marque), p53 (clone DO-7, 1:300; Novocastra, Leica Biosystems; Newcastle Upon Tyne, UK), and L1CAM (clone UJ127.11, 1:1000; Sigma; MO, USA).
For MMR proteins, tumors were considered aberrant if tumor cells showed a complete absence of nuclear staining with a positive non-neoplastic internal control and intact if tumor cells exhibited nuclear positivity. The p53 wild-type pattern was defined as weak focal positive staining. Aberrant p53 expression was classified into three patterns: overexpression (diffuse and strong nuclear staining of >70% of tumor cell nuclei), no staining (complete absence of expression), and cytoplasmic expression (cytoplasmic staining of tumor cells). L1CAM evaluation was performed for patients in the NSMP group. For L1CAM evaluation, the percentage of positive membrane staining in tumor cells was scored regardless of staining intensity; tumors with ≥10% positivity were considered L1CAM-positive [8]. Two pathologists (B.A. and E.P.) reviewed all slides, blinded to the patient characteristics and outcomes. If discrepancies occurred, discussion ensued until a consensus was reached.
2.3. Statistical Analysis
Statistical analyses were performed using SPSS statistics version 21.0 (IBM Corp., Armonk, NY, USA) and Prism software (GraphPad; La Jolla, CA, USA). Clinical and demographic characteristics among women were compared using Fisher’s exact test for categorical data and the Wilcoxon rank-sum test for continuous data. The recurrence rate was calculated for each subgroup. PFS and OS were compared among the subgroups using Kaplan–Meier curves and log-rank tests. PFS was defined as the period between surgery and recurrence or death. OS was defined as the period between surgery and death. Both PFS and OS were censored at the last follow-up. Cox proportional hazards regression was used to estimate the effect of molecular subtypes, adjusting for covariates for PFS and OS among the subgroups. The clinical and demographic variables significant in the univariate analysis (p<0.05) were included in the multivariable Cox model.
3. Results
3.1. Flow Diagram (Figure 1)
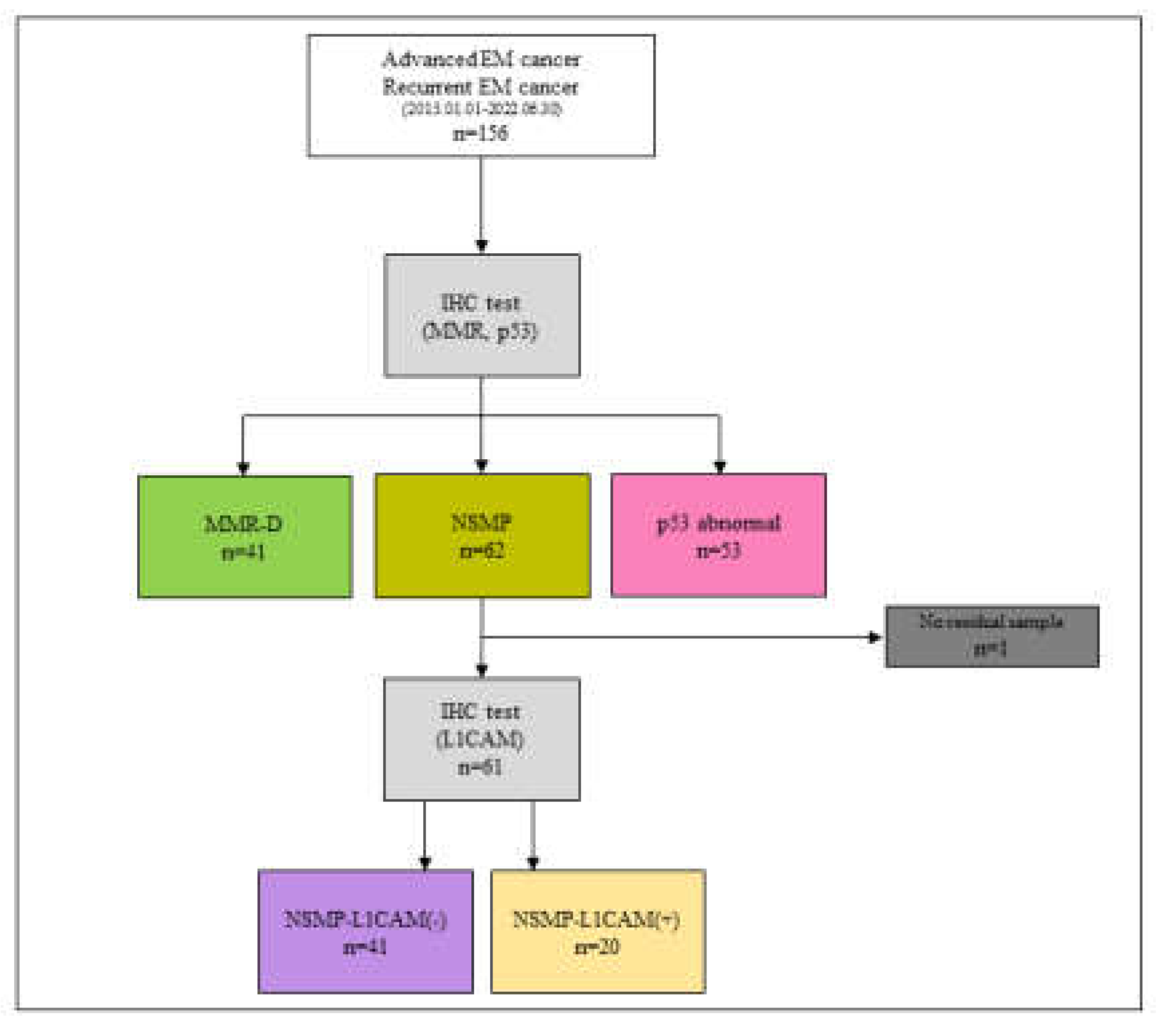
A flow diagram of this study is presented in Figure 1. Between January 2015 and June 2022, 156 patients with advanced-stage/recurrent EC who underwent MMR and p53 tests were identified at the Severance Hospital of YUHS. A total of 41, 62, and 53 patients were identified in the MMR-D, NSMP, and p53abn groups, respectively (Figure 1). L1CAM expression in the NSMP group was confirmed using IHC. Of the 62 patients in the NSMP group, 41 were L1CAM-negative and 20 were L1CAM-positive; one patient did not have a specimen for IHC testing.
Figure 1.
Trial profile.
3.2. Study Demographics(Table 1)
Assessment of the characteristics of the molecular-classification subgroups indicated that women in the MMR-D group were younger; those in the p53abn group were older. Moreover, the tumors in the MMR-D group had a relatively less advanced stage (68.3% stage III) and were predominantly endometrioid (90.2%). The p53abn tumors displayed aggressive pathological features (73.6% grade 3, 49.1% non-endometrioid histology, 64.2% lymph-vascular space invasion [LVSI], and more-advanced stages). Dividing the NSMP group based on L1CAM identified that the L1CAM-positive group had older age, more menopausal states, and aggressive pathologic features (50.0% grade 3, 25.0% non-endometrioid histology, 55.0% LVSI, and more advanced stages) compared with the L1CAM-negative group (Table 1).

Table 1.
Demographic and clinical characteristics overall and by molecular classification and L1CAM status.
Table 1.
Demographic and clinical characteristics overall and by molecular classification and L1CAM status.
| MMR-D (N=41) |
MMR-proficient | Total (N=155) |
p value | ||||
|---|---|---|---|---|---|---|---|
| NSMP-L1CAM(-) (N=41) |
NSMP-L1CAM(+) (N=20) |
p53abn (N=53) |
|||||
| Age(years) | |||||||
| Mean (SD) | 51.7(±9.5) | 55.6(±10.7) | 60.1(±9.4) | 59.6(±10.7) | 56.5(±10.7) | 0.001 | |
| BMI | |||||||
| Mean (SD) | 23.7(±4.5) | 25.4(±4.0) | 23.5(±3.9) | 25.2(±5.3) | 24.6(±4.6) | 0.201 | |
| Parity | |||||||
| 0 | 17(41.5%) | 11(26.8%) | 6(30.0%) | 10(18.9%) | 44(28.4%) | 0.117 | |
| 1 or more | 24(58.5%) | 30(73.2%) | 14(70.0%) | 43(81.1%) | 111(71.6%) | ||
| Diabetes | |||||||
| No | 35(85.4%) | 33(80.5%) | 17(85.0%) | 46(86.8%) | 131(84.5%) | 0.863 | |
| Yes | 6(14.6%) | 8(19.5%) | 3(15.0%) | 7(13.2%) | 24(15.5%) | ||
| Prior malignancies | |||||||
| No | 38(92.7%) | 41(100.0%) | 19(95.0%) | 45(84.9%) | 143(92.3%) | 0.053 | |
| Yes | 3(7.3%) | 0(0.0%) | 1(5.0%) | 8(15.1%) | 12(7.7%) | ||
| CA-125 at diagnosis | |||||||
| Mean (SD) | 130.4(±24.0) | 95.5(±184.3) | 59.1(±67.6) | 154.0(±307.2) | 120.0(±220.1) | 0.338 | |
| Histology | |||||||
| Endometrioid | 37(90.2%) | 34(82.9%) | 15(75.0%) | 27(50.9%) | 113(72.9%) | 0.002 | |
| Serous | 0(0.0%) | 2(4.9%) | 1(5.0%) | 10(18.9%) | 13(8.4%) | ||
| Clear cell | 2(4.9%) | 1(2.4%) | 1(5.0%) | 4(7.5%) | 8(5.2%) | ||
| MMMT | 1(2.4%) | 2(4.9%) | 1(5.0%) | 11(20.8%) | 15(9.7%) | ||
| Adenocarcinoma | 0(0.0%) | 2(4.9%) | 2(10.0%) | 1(1.9%) | 5(3.2%) | ||
| Neuroendocrine | 1(2.4%) | 0(0.0%) | 0(0.0%) | 0(0.0%) | 1(0.6%) | ||
| Stage at diagnosis | |||||||
| III | 28(68.3%) | 27(65.9%) | 12(60.0%) | 28(52.8%) | 95(61.3%) | 0.457 | |
| IV | 7(17.1%) | 4(9.8%) | 5(25.0%) | 13(24.5%) | 29(18.7%) | ||
| Recur | 6(14.6%) | 10(24.4%) | 3(15.0%) | 12(22.6%) | 31(20.0%) | ||
| Staging op pathological grade | |||||||
| 1 | 7(17.1%) | 12(29.3%) | 3(15.0%) | 0(0.0%) | 22(14.2%) | <0.001 | |
| 2 | 24(58.5%) | 19(46.3%) | 6(30.0%) | 14(26.4%) | 63(40.6%) | ||
| 3 | 9(22.0%) | 9(22.0%) | 10(50.0%) | 39(73.6%) | 67(43.2%) | ||
| none | 1(2.4%) | 1(2.4%) | 1(5.0%) | 0(0.0%) | 3(1.9%) | ||
| Staging op LVSI | |||||||
| No | 15(36.6%) | 22(53.7%) | 7(35.0%) | 19(35.8%) | 63(40.6%) | 0.055 | |
| Yes | 25(61.0%) | 19(46.3%) | 11(55.0%) | 34(64.2%) | 89(57.4%) | ||
| Missing | 1(2.4%) | 0(0.0%) | 2(10.0%) | 0(0.0%) | 3(1.9%) | ||
| Radiotherapy | |||||||
| No | 16(39.0%) | 27(65.9%) | 11(55.0%) | 34(64.2%) | 88(56.8%) | 0.049 | |
| Yes | 25(61.0%) | 14(34.1%) | 9(45.0%) | 19(35.8%) | 67(43.2%) | ||
*Abbreviations: Recur, recurrent endometrial cancer; MMR-D, mismatch repair protein deficiency; NSMP, no specific molecular profiled; p53abn, abnormal p53; BMI, body mass index; MMMT, malignant mixed Müllerian tumour; LVSI, lymph-vascular space invasion.
3.3. Survival Result and Multivariable Analysis by Molecular Classification in Advanced Stage and Recurrent Endometrial Cancer
In the overall cohort, PFS and OS were the longest for MMR-D, followed by NSMP and p53abn tumors (Figure 2-A; PFS: p=0.0006, OS: p=0.0013). After NSMP classification according to the L1CAM status, the L1CAM-negative group exhibited longer PFS and OS than the L1CAM-positive group (Figure 2-B; PFS: p=0.0001 and OS: p=0.0030).
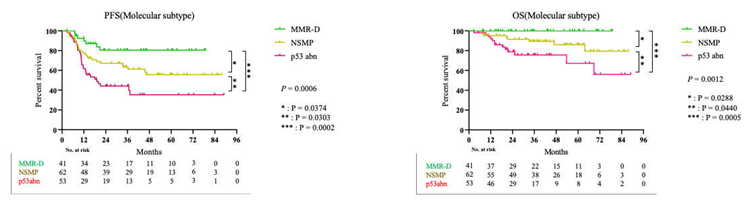
Figure 2-A. Progression free survival(PFS) and overall survival(OS) in molecular classification.
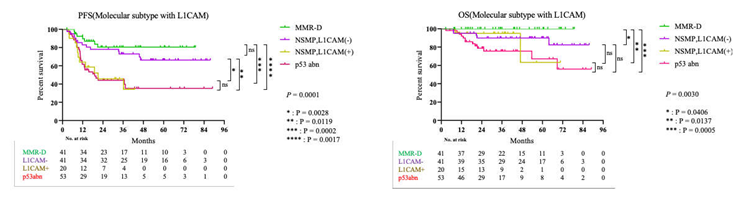
Figure 2-B. Progression free survival(PFS) and overall survival(OS) in molecular classification with L1CAM.
When PFS and OS were compared between patients with stage III disease who received adjuvant therapy and those with stage IV or recurrent disease who received palliative treatment, significant differences in PFS were confirmed based on the molecular subtype and L1CAM status in both groups (Supplement 1-A; PFS: p=0.0205 for molecular subtype and PFS: p=0.0018 for molecular subtype with L1CAM, Supplement 1-B; PFS: p=0.0045 for molecular subtype and PFS: p=0.0097 for molecular subtype with L1CAM). A significant difference in OS was also found, except for the molecular subtypes with L1CAM in the adjuvant therapy group. A difference in the overall tendency was also identified (Supplement 2-A; OS: p=0.0236 for molecular subtype and OS: p=0.0577 for molecular subtype with L1CAM, Supplement 2-B; OS: p=0.0325 for molecular subtype and OS: p=0.1977 for molecular subtype with L1CAM).
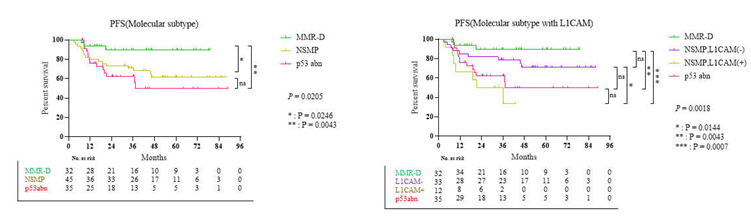
Supplement 1-A. Progression free survival for adjuvant treatment in molecular classification with L1CAM.
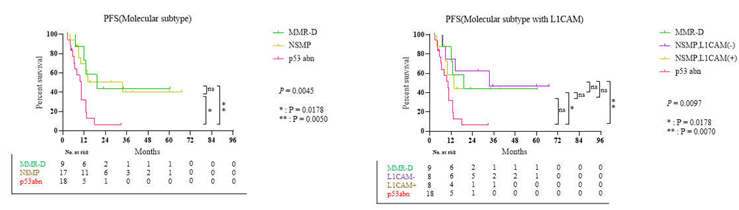
Supplement 1-B. Progression free survival for palliative treatment in molecular classification with L1CAM
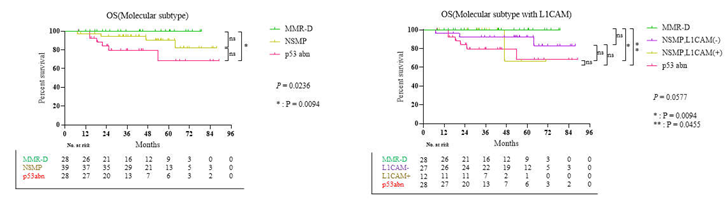
Supplement 2-A. Overall survival for adjuvant treatment in molecular classification with L1CAM.
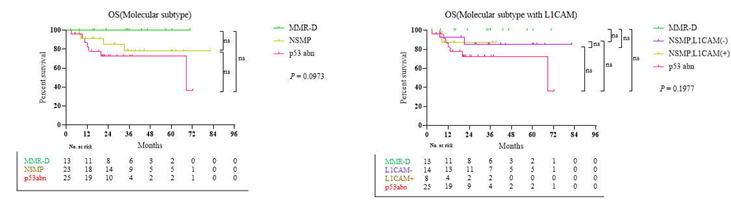
Supplement 2-B. Overall survival for palliative treatment in molecular classification with L1CAM
In the multivariate analysis (Table 2), age, stage, and molecular classification exhibited a trend toward significance for PFS (p=0.010, p=0.009, and p=0.039, respectively). Body mass index (BMI) was significantly associated with OS (p=0.018). For PFS, the hazard ratios (HRs) for stage IV and stage III recurrent EC were 2.137 (CI: 1.098–4.160) and 2.335 (CI: 1.240–4.398), respectively. The HRs for MMR-D and p53abn for NSMP were 0.579 (CI: 0.258–1.300) and 1.599 (CI: 0.911–2.806), respectively. The HR for age was 1.036 (CI: 1.009–1.064), and the HR for BMI was 0.866 (CI: 0.768–0.976) for OS.
4. Discussion
We confirmed that PFS and OS were the worst for the p53abn subtype (p53abn<NSMP<MMR-D) of advanced/recurrent EC after the first chemotherapy. This study compared PFS and OS after chemotherapy in patients with advanced or first recurrent EC and not at all stages of EC. Therefore, it is valuable as a predictor for patients undergoing corresponding treatment. For these differences, in the Ruby Trial, which compared the difference between the platinum-based chemotherapy and chemotherapy with dostarlimab according to the MMR status in advanced/recurrent EC, the MMR-D and MMR-proficient (MMR-P) groups that underwent platinum-based chemotherapy had 24-month PFS rates of 15.7% and 18.8%, respectively [9]. In contrast, in the GY-018 trial comparing the difference between platinum-based chemotherapy and chemotherapy with pembrolizumab according to MMR status in advanced/recurrent EC, the MMR-D with chemotherapy group exhibited a better prognosis than the MMR-P with chemotherapy group [10]. This difference appears to depend on the patients who participated in the studies. In the present study, 43.59% of the 156 patients received radiotherapy, compared to 18.1% in the Ruby Trial.
In addition, in this study, 61.0% of the patients received radiotherapy in the MMR-D group, but only 20% received radiotherapy in the Ruby study, justifying the differences in the results. Also, in the GY-018 trial, 42.7% in the MMR-D group and 39.6% in the MMR-P group received radiotherapy, suggesting that there may be differences depending on radiotherapy treatment [9,10]. In the PORTEC-3 study, the 5-year failure-free survival rates of patients with stage III EC treated with radiotherapy and chemoradiotherapy were reported to be 58.4% and 70.9%, respectively, which appears to indirectly explain the increase in PFS in this study [11].
In the NRG/GOG0210 study and as reported by Kim et al., whereby adjuvant therapy was administered to MMR-D and MMR-P patients in all stages of EC, the difference between both groups was affected by another risk factor that was confirmed in the univariate and multivariate analyses [12,13]. This study’s multivariable analysis revealed that age, stage, and molecular classification were associated with PFS and that BMI was associated with OS.
These risk factors guide treatment decisions, as suggested in various guidelines. In the current ESGO/ESTRO/ESP guidelines published in 2020, the molecular classification, which shows the difference between PFS and OS, was integrated to form a new classification. Risk factors (histopathological type, grade, myometrial invasion, LVSI, etc.) were combined to classify the risk groups as low, intermediate, high-intermediate, high, and advanced metastatic. However, despite the bias of these risk factors, this study confirmed a clear difference in each molecular classification group using chemotherapy. There are implications that molecular classification can be used as a predictor to evaluate the prognosis of patients after chemotherapy [6,14].
Recently, various studies have been conducted on additional markers with characteristics other than those of the four existing molecular classifications [15]. Kommos et al. suggested that L1CAM is a risk factor for stratifying patients with NSMP. L1CAM (CD171) is known to be closely associated with the epithelial-to-mesenchymal transition as a substance related to tumor cell motility and showed a significant difference between specific survival and OS in EC [7]. The subgroup of NSMP-L1CAM-positive tumors associated with high histological grade and high International Federation of Gynecology and Obstetrics stage had as poor an outcome as p53abn tumors [7,15]. Based on the study of L1CAM in EC, the PORTEC-4a study is underway to confirm the results of adjuvant radiotherapy by newly defining favorable, intermediate, and unfavorable groups through molecular classification and additional L1CAM and CTNNB1 results as new markers in patients with early-stage EC [16]. In the present study, L1CAM was used as a new marker to stratify patients in the NSMP group. We found differences in PFS and OS in the NSMP group in patients with advanced-stage/recurrent EC using L1CAM IHC results.
Various studies have demonstrated that the p53abn subtype exhibits a poor prognosis compared with that for other subtypes, and there are no treatment options other than chemotherapy. In this study, the prognosis of this group was poorer than that of the other groups. Samarnthai et al. observed that TP53 mutations are more common in type II EC, which is generally known to progress rapidly and has a poorer prognosis than type 1 EC [17]. Moreover, TP53 mutations can be identified through abnormal p53 IHC results, such as complete absence, overexpression, and cytoplasmic expression of p53 [18]. If proper repair of DNA damage is not achieved, apoptosis proceeds through apoptosis-signaling genes, such as BAX, PUMA, Nox, and PERP. Since carcinogenesis can occur when there is a functional abnormality in p53, the inability of this repair mechanism can be considered the potential underlying mechanism reflecting the poor prognosis of the p53abn subtype [19].
Conversely, in the case of the MMR-D subtype, as a highly immunogenic tumor, it induces the upregulation of tumor-infiltrating lymphocytes by producing high levels of tumor mutant antigen. Through this, the cell-mediated anti-tumor response increases, which appears to be related to prolonged survival [20].
Recently, based on the similar molecular profiles of p53abn and high-grade serous ovarian cancer (HGSOC) using TCGA genomic analysis [4], the development of a treatment protocol using poly (ADP-ribose) polymerase inhibitors has been considered because HGSOC possesses the characteristics of homologous recombination deficiency [20].
Additional classification using new markers, such as L1CAM, is expected to offer various treatment options. Chung et al. demonstrated that using progestin in MMR-D patients yielded a poor response, evident from the lower complete or partial remission rates in terms of the best overall response in early EC compared to that in other molecular classification groups. Therefore, molecular classification could be used as an indicator to determine EC treatment options for women of childbearing age who need fertility preservation [21]. Although L1CAM was useful as a classification marker in the NSMP group in this study, if molecular classification is refined through additional research, it is expected to provide other treatment options, such as fertility preservation in patients with EC.
Since the development of the Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) molecular classification was announced, classification methods using new diagnostic methods besides IHC have garnered attention. One method involves using cervical swab-based genomic DNA (gDNA) of EC through the conventional pap smear technique [22]. The research team verified the loss of MSH2 or MSH6 and aberrant p53 expression using cervical swab-based gDNA and confirmed its value as a tool that can be used to layer ProMisE molecular classification based on tests and stratification. Although only the IHC test technique was used in our study, we expect that rapid treatment of the patient and subsequent treatment plan determination will be possible through the non-invasive early diagnosis and classification of EC.
TCGA Research Network reported that POLE (ultra-mutated) was identified in 7% of all endometrial cancers. Therefore, even in this study, there was a limitation in that it was difficult to exclude the possibility that the corresponding group exists in another molecular subtype [4]. Currently, there is no method for confirming POLE mutations using IHC. However, a technology that can detect POLE mutations using Droplet Digital PCR (ddPCR) developed recently has reached the commercialization stage. This test was designed to detect POLE mutations in exons 9 (P286R, S297F), 13 (V411L), and 14 (A456P, S459F). Mutations can be confirmed using ddPCR, which exhibits higher specificity and sensitivity than real-time PCR [23]. Further, since the expression of the POLE mutation subtype is low in advanced/recurrent EC, it is unlikely to affect the results of this study significantly [24]. In the future, if the prognosis and characteristics of patients by molecular subtype are more clearly confirmed using this technology, it will be useful in guiding treatment protocols.
5. Conclusions
In chemotherapy-naïve patients with advanced and recurrent EC, the most favorable post-chemotherapy PFS and OS were observed for MMR-D, followed by NSMP and p53abn tumors, and the L1CAM status in the NSMP subtype showed a difference in PFS and OS.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
JYL, EP: Conceptualization; JCK, BA: Data curation; JCK: Formal analysis; JYL, EP: Funding acquisition; JCK: Investigation; JYL, EP: Methodology; JYL: Project administration; YL, SK, EJN, SWK, YTK, EP, JYL: Resources; JCK: Software; JYL, EP: Supervision; JCK: Visualization; JCK: Writing – original draft; JYL, EP: Writing – review & editing. All authors read and approved the final manuscript.
Funding
Not applicable.
Institutional Review Board Statement
This retrospective cohort study was conducted at the Severance Hospital of the Yonsei University Health System (YUHS, 4-2023-0263).
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets supporting the study conclusions are included within this manuscript and its additional files.
Acknowledgments
This study was supported by the Severance Hospital Research Fund for Clinical Excellence (C-2022-0013). The funder had no role in the study design; collection, analysis, and interpretation of the data; writing of the report; or decision to submit the article for publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Won, Y.-J.; Lee, J.J.; Jung, K.-W.; Kim, H.-J.; Kong, H.-J.; Im, J.-S.; Seo, H.G. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2019. Cancer Res Treat 2022, 54, 330–344. [Google Scholar] [CrossRef]
- Park, B. Associations between obesity, metabolic syndrome, and endometrial cancer risk in East Asian women. J Gynecol Oncol 2022, 33, e35. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research, N.; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Kommoss, F.K.; Karnezis, A.N.; Kommoss, F.; Talhouk, A.; Taran, F.A.; Staebler, A.; Gilks, C.B.; Huntsman, D.G.; Krämer, B.; Brucker, S.Y.; et al. L1CAM further stratifies endometrial carcinoma patients with no specific molecular risk profile. Br J Cancer 2018, 119, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Zeimet, A.G.; Reimer, D.; Huszar, M.; Winterhoff, B.; Puistola, U.; Azim, S.A.; Müller-Holzner, E.; Ben-Arie, A.; van Kempen, L.C.; Petru, E.; et al. L1CAM in early-stage type I endometrial cancer: results of a large multicenter evaluation. J Natl Cancer Inst 2013, 105, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.R.; Chase, D.M.; Slomovitz, B.M.; dePont Christensen, R.; Novák, Z.; Black, D.; Gilbert, L.; Sharma, S.; Valabrega, G.; Landrum, L.M.; et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. New England Journal of Medicine 2023. [Google Scholar] [CrossRef]
- Eskander, R.N.; Sill, M.W.; Beffa, L.; Moore, R.G.; Hope, J.M.; Musa, F.B.; Mannel, R.; Shahin, M.S.; Cantuaria, G.H.; Girda, E.; et al. Pembrolizumab plus Chemotherapy in Advanced Endometrial Cancer. New England Journal of Medicine 2023. [Google Scholar] [CrossRef]
- de Boer, S.M.; Powell, M.E.; Mileshkin, L.; Katsaros, D.; Bessette, P.; Haie-Meder, C.; Ottevanger, P.B.; Ledermann, J.A.; Khaw, P.; D'Amico, R.; et al. Adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3): patterns of recurrence and post-hoc survival analysis of a randomised phase 3 trial. Lancet Oncol 2019, 20, 1273–1285. [Google Scholar] [CrossRef]
- Kim, S.R.; Pina, A.; Albert, A.; McAlpine, J.; Wolber, R.; Blake Gilks, C.; Kwon, J.S. Does MMR status in endometrial cancer influence response to adjuvant therapy? Gynecol Oncol 2018, 151, 76–81. [Google Scholar] [CrossRef]
- McMeekin, D.S.; Tritchler, D.L.; Cohn, D.E.; Mutch, D.G.; Lankes, H.A.; Geller, M.A.; Powell, M.A.; Backes, F.J.; Landrum, L.M.; Zaino, R.; et al. Clinicopathologic Significance of Mismatch Repair Defects in Endometrial Cancer: An NRG Oncology/Gynecologic Oncology Group Study. J Clin Oncol 2016, 34, 3062–3068. [Google Scholar] [CrossRef]
- Santoro, A.; Angelico, G.; Travaglino, A.; Inzani, F.; Arciuolo, D.; Valente, M.; D'Alessandris, N.; Scaglione, G.; Fiorentino, V.; Raffone, A.; et al. New Pathological and Clinical Insights in Endometrial Cancer in View of the Updated ESGO/ESTRO/ESP Guidelines. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef]
- Alexa, M.; Hasenburg, A.; Battista, M.J. The TCGA Molecular Classification of Endometrial Cancer and Its Possible Impact on Adjuvant Treatment Decisions. Cancers (Basel) 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- van den Heerik, A.; Horeweg, N.; Nout, R.A.; Lutgens, L.; van der Steen-Banasik, E.M.; Westerveld, G.H.; van den Berg, H.A.; Slot, A.; Koppe, F.L.A.; Kommoss, S.; et al. PORTEC-4a: international randomized trial of molecular profile-based adjuvant treatment for women with high-intermediate risk endometrial cancer. Int J Gynecol Cancer 2020, 30, 2002–2007. [Google Scholar] [CrossRef]
- Samarnthai, N.; Hall, K.; Yeh, I.T. Molecular profiling of endometrial malignancies. Obstet Gynecol Int 2010, 2010, 162363. [Google Scholar] [CrossRef]
- Köbel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of P53 Immunohistochemistry in Endometrial Carcinomas: Toward Increased Reproducibility. Int J Gynecol Pathol 2019, 38 Suppl 1, S123–s131. [Google Scholar] [CrossRef]
- Attardi, L.D.; Reczek, E.E.; Cosmas, C.; Demicco, E.G.; McCurrach, M.E.; Lowe, S.W.; Jacks, T. PERP, an apoptosis-associated target of p53, is a novel member of the PMP-22/gas3 family. Genes Dev 2000, 14, 704–718. [Google Scholar] [CrossRef]
- Tabata, J.; Takenaka, M.; Okamoto, A. Molecular typing guiding treatment and prognosis of endometrial cancer. Gynecology and Obstetrics Clinical Medicine 2023. [Google Scholar] [CrossRef]
- Chung, Y.S.; Woo, H.Y.; Lee, J.Y.; Park, E.; Nam, E.J.; Kim, S.; Kim, S.W.; Kim, Y.T. Mismatch repair status influences response to fertility-sparing treatment of endometrial cancer. Am J Obstet Gynecol 2021, 224, 370–e371. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Kim, Y.N.; Lee, K.; Park, E.; Lee, Y.J.; Hwang, S.Y.; Park, J.; Choi, Z.; Kim, S.W.; Kim, S.; et al. Feasibility and clinical applicability of genomic profiling based on cervical smear samples in patients with endometrial cancer. Front Oncol 2022, 12, 942735. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Lee, S.K.; Suh, D.H.; Kim, K.; No, J.H.; Kim, Y.B.; Kim, H. Clinical evaluation of a droplet digital PCR assay for detecting POLE mutations and molecular classification of endometrial cancer. J Gynecol Oncol 2022, 33. [Google Scholar] [CrossRef]
- Jumaah, A.S.; Salim, M.M.; Al-Haddad, H.S.; McAllister, K.A.; Yasseen, A.A. The frequency of POLE-mutation in endometrial carcinoma and prognostic implications: a systemic review and meta-analysis. J Pathol Transl Med 2020, 54, 471–479. [Google Scholar] [CrossRef]
Table 2.
Multivariable Survival Analysis in the Confirmation Cohort (n=156) Using Parameters Available at the Time of Diagnosis.
Table 2.
Multivariable Survival Analysis in the Confirmation Cohort (n=156) Using Parameters Available at the Time of Diagnosis.
| PFS, 61 of 154 Events | OS, 20 of 152 Events | ||||
|---|---|---|---|---|---|
| Variable [Ref] | HR (95% CI) | p value | HR (95% CI) | p value | |
| Age | 1.036(1.009-1.064) | 0.010 | |||
| Stage [III] | 0.009 | ||||
| IV | 2.137(1.098-4.160) | ||||
| Recur | 2.335(1.240-4.398) | ||||
| CA-125 | 1.001(1.000-1.002) | 0.061 | |||
| BMI | 0.866(0.768-0.976) | 0.018 | |||
| Radiotherapy[No] | 0.074 | ||||
| Yes | 0.367(0.122-1.101) | ||||
| Molecular classification [NSMP] | 0.039 | 0.172 | |||
| MMR-D | 0.579(0.258-1.300) | 0.000(0.000-5.407E173) | |||
| p53abn | 1.599(0.911-2.806) | 2.430(0.960-6.151) | |||
*Abbreviations: HR, hazard ratio; Recur, recurrent endometrial cancer; MMR-D, mismatch repair protein deficiency; NSMP, no specific molecular profiled; p53abn, abnormal p53; BMI, body mass index.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



