
Submitted:
29 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
Purpose
To analyse diagnostic and therapeutic impact of molecular imaging TNM (miTNM) stage obtained with 18F-DCFPyL versus 18F-Fluorocholine in head to head comparison in biochemical recurrence (BCR) prostate cancer (PCa).
Material and methods
Patients with BCR PCa after radical treatment with previous 18F-Fluorocholine-PET/CT (negative or oligometastatic disease) were derived to 18F-DCFPyL-PET/CT. Patients were classified attending to: grade group, EAU classification, PSA, PSA doubling time (PSAdt) and PSA velocity (PSAvel).
The overall detection rate (DR) and miTNM stage according to PROMISE criteria were assessed for both radiotracers and also correlation (Kappa). The influence of PSA and kinetics on both PET/CT (DR and miTNM) and predictive value of unfavourable kinetics on miTNM were determined.
Cut-off PSA, PSAdt and PSAvel values able to predict PET/CT results were determined. Change in miTNM and treatment derived of 18F-DCFPyL information with respect to 18F-Fluorocholine was also evaluated.
Results
We studied 138 patients. 18F-DCFPyL showed a higher DR than 18F-Fluorocholine (64.5% vs 33.3%). 18F-DCFPyL and 18F-Fluorocholine detected T in 33.3% versus 19.6%, N in 27.5% versus 13.8%, M in 30.4% versus 8.7%. Both tracers DR showed significant associations with PSA and PSAvel. Significant association was only found between miTNM and PSA on 18F-Fluorocholine-PET/CT (p=0.033). For 18F-Fluorocholine and 18F-DCFPyL PET/CT a PSAdt cut-off of 4.09 and 5.59 months, respectively, were able to predict M stage. 18F-DCFPyL changed therapeutic management in 40/138 patients.
Conclusion
18F-DCFPyL provides a higher DR and superior miTNM staging than 18F-Fluorocholine in restaging BCR, especially with high PSA and unfavourable PSA kinetics, showing a fair agreement to 18F-Fluorocholine.
Keywords:
18F-DCFPyL
; 18F-Fluorocholine
; miTNM
; PSA level
; PSA kinetics
; therapeutic impact
1. Introduction
Up to a half of pT2-3 node-negative prostate cancer (PCa) patients experience biochemical recurrence (BCR) after radical prostatectomy (RP) or radiotherapy [1]. Detection of responsible lesions in the context of a BCR constitutes a major challenge for conventional imaging modalities as computed tomography (CT) and bone scan.
Choline-based PET/CT has been the traditional imaging modality of choice in restaging patients following BCR [2]. However, multiple studies have shown low sensitivity and specificity, particularly at low prostate specific antigen (PSA) levels, which can result in delays in salvage therapies [3,4]. For several years, and due to these limitations, the development of radionuclides that recognizes prostate-specific membrane antigen (PSMA) ligands has been proposed as an alternative, with higher sensitivity and specificity in BCR PCa patients [5]. These “top diagnostic” radiotracers have increased the detection rate (DR) of oligometastatic disease (OD) that has driven recent advancements in metastasis-directed treatment strategies of oligometastatic PCa.
18F-DCFPyL [2-(3-(1-carboxy-5-[(6-[18F]fluoro-pyridine-3-carbonyl)-amino]-pentyl)-ureido)-pentanedioic acid] is a radiofluorinated, small molecule high affinity inhibitor of PSMA [6]. The current restrictions in its use in our environment explain the dual-tracer diagnostic approach in some cases of BCR, especially in those with a PSA level >2 ng/mL and a previous negative or doubtful choline-labelled PET/CT. Some studies have addressed utility of 68Ga-labelled PSMA ligands and choline-labelled tracers in head to head comparison [7,8], although no previous reported experience exists using the newest developed 18F-DCFPyL. On the other hand, if we only use DR to compare both radiotracers, the real diagnostic potential of PSMA-ligands with respect to choline-labelled tracers may be limited. In addition, differences in therapeutic impact have been scarcely assessed [9].
The Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE) criteria summarize standards for study design and reporting of prostate cancer molecular imaging. PROMISE criteria propose a molecular imaging TNM (miTNM) for the interpretation of PSMA ligands PET/CT designed to organize findings in comprehensible categories and to promote the exchange of information among physicians and institutions [10].
The aim of our study was multiple: (i) to analyse the concordance between 18F-DCFPyL and 18F-Fluorocholine, in head to head comparison, regarding DR and miTNM stage using PROMISE criteria, (ii) to address the predictive value of unfavourable PSA kinetics on miTNM, and (iii) to assess the therapeutic impact of 18F-DCFPyL with respect to 18F-Fluorocholine-PET/CT in patients with BCR PCa.
2. Material and methods
2.1. Patients
Patients with BCR of PCa after radical treatment (RP, radiotherapy, or both) were derived from different hospitals of our region for re-staging with 18F-Fluorocholine-PET/CT between August 2020 and December 2021. No patient was under androgen deprivation therapy (ADT). Patients with negative or doubtful 18F-Fluorocholine-PET/CT, or with OD, underwent 18F-DCFPyL-PET/CT and were included in a prospective dataset. 18F-DCFPyL-PET/CT was performed within the context of compassionate use under the approval of the Spanish Agency of Medication and Health Care Products and after being approved by a multidisciplinary committee and previous patient informed and signed consent. Database registry analysis of patients was approved by aEthical Committee (internal code of 2022-53).
The inclusion criteria of selected patients for the present analysis were: (i) time window between both PET/CT within 2 months, (ii) minimum clinical follow-up of 6 months. We established as OD the presence of ≤ 3 lesions affecting lymph node (pelvis and/or retroperitoneum) or bone. Patients were classified in groups taking into account: grade group (1 to 5) [11], European Association of Urology (EAU) classification adapted from D’Amico risk category (low/intermediate/high) [1], PSA value closest to PET/CTs (PSA ≤ 1 ng/ml, 1 < PSA ≤ 2 and PSA > 2), PSA doubling time (PSAdt) ≤ or > 6 months and PSA velocity (PSAvel) ≥ or < 0.2 ng/ml/month. The initial radical treatment and subsequent salvage treatment, if previous BCR, were obtained.
Acquisition protocol
18F-Fluorocholine and 18F-DCFPyL PET/CTs were performed in a unique reference hospital and with the same hybrid PET/CT scanner (Discovery 5R/IQ, GE) in 3D acquisition mode for 2 minutes per bed position. Low dose CT (120 kV, 80 mA) without contrast was performed for attenuation correction and as an anatomical map. There was no fasting requirement and only a correct hydration previous to both radiotracer administrations was orally promoted.
The acquisition protocol of 18F-Fluorocholine and 18F-DCFPyL PET/CT included an early standard study from skull to proximal legs 5–15 and 120 minutes, respectively, after the intravenous administration of an activity of 2–4 MBq/Kg, previous administration of diuretic. A delayed study of the pelvis, in cases with significant urinary bladder retention or doubtful evaluation, was performed 60 and 30 min after the standard acquisition, on 18F-Fluorocholine and 18F-DCFPyL scans, respectively.
Image analysis and interpretation
The emission data was corrected for scatter, random coincidence events, and system dead time using the provided software. All 18F-Fluorocholine and 18F-DCFPyL scans were evaluated in the Advantage Workstation software version 4.7 (GE Healthcare) allowing review of PET, CT, and fused imaging data. Two experienced nuclear medicine physicians evaluated both scans, and a third observer reviewed them in case of discordances. Any focal uptake higher than adjacent background, that did not correspond to physiological uptake, urinary excretion or benign conditions, was considered PET-positive and malignant.
Lesions identified with both tracers were classified in local recurrence (T), lymph nodes (N) and metastases (M), using miTNM stage defined by PROMISE criteria [10].
18F-Fluorocholine avid lesions without any correspondence on 18F-DCFPyL-PET/CT, histopathological or imaging confirmation were considered false positive. In the case of 18F-DCFPyL, avid lesions lacking histopathological verification were rated as malignant if there was a corresponding anatomical finding suspicious for malignancy or MRI or if it was considered clinically malignant in the follow-up by multidisciplinary committee. Otherwise, these uptakes were considered false positive.
Therapeutic management and follow-up
All diagnostic procedures and treatments undertaken, including surgery, radiotherapy, duration and type of systemic therapy, and any biopsies obtained, were documented in the follow-up.
Changes in therapeutic management because of 18F-DCFPyL, with respect to 18F-Fluorocholine-PET/CT information, were assessed. Different curative options for BCR are available depending on initial radical treatment. For patients who underwent RP, prostatic fossa radiotherapy is a possibility for either positive or negative prostatic fossa disease detection on PET/CT. Pelvic nodal recurrence could be treated with stereotactic body radiotherapy (SBRT) or surgery. On the other hand, patients who underwent radical prostate radiotherapy have more limitations for a new radiotherapy procedure, in case of prostatic radiotracer uptake on PET/CT, except for brachytherapy, needing a previous histologic confirmation of active disease. Polimetastatic disease (>3) with extension to the retroperitoneal territory and/or bones is treated with systemic therapy (ADT) with/without a combination of androgen receptor-axis-targeted therapies (ARAT) in cases of more extensive disease.
We considered that changes in management happened when 18F-DCFPyL-PET/CT modified treatment decision reached after 18F-Fluorocholine findings. The added therapeutic impact of 18F-DCFPyL-PET/CT over 18F-Fluorocholine-PET/CT (escalation vs. de-escalation) was assessed. Escalation was defined as locorregional radiotherapy/surgery or ARAT (Abiraterone, Apalutamide or Enzalutamide) in cases of regional or metastatic disease, respectively, only detected by 18F-DCFPyL. De-escalation with only follow-up was decided in cases of a negative 18F-DCFPyL and positive 18F-Fluorocholine, considering that the latter was false positive, or when PET/CT results were different and therapeutic decision after 18F-Fluorocholine was not performed, for example, more disease on 18F-DCFPyL PET/CT that allowed the standard treatment (ADT) instead of local treatment. No therapeutic impact was considered if the results of both scans were concordant or whether different, no differences in treatment were reported with respect to the information derived from 18F-Fluorocholine. Cases when no therapeutic impact happened due to patients’ clinical conditions were recorded.
In follow-up, all diagnostic procedures and treatments undertaken were documented. Serial PSA was obtained every 3 months after planned treatment. Initial treatment response was defined as a drop in PSA levels of greater than 50% from pre-treatment levels in the absence of ADT at the time of PSA assessment at least 6 months after treatment administration. For local curative treatments (surgery or radiotherapy) a minimum time window of 2 months with respect to 18F-DCFPyL was considered reliable for assessing efficacy. Men with ADT as part of their treatment were not included in this assessment.
2.2. Statistical analysis
Statistical analysis was performed using SPSS software (v. 28). Quantitative variables were represented by mean and standard deviation and qualitative variables by frequency and percentage. Relation between qualitative variables was studied using Chi-squared Pearson test. Kolmogorov-Smirnov test was used to study normality of the quantitative variables with result of non-normal variables, and the nonparametric tests Kruskal-Wallis and Mann-Whitney were used to compare the means of the quantitative variables. Overall DR for 18F-Fluorocholine and 18F-DCFPyL PET/CTs and concordance (Kappa, k) were assessed, classifying the results as poor (<0.20), weak (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80) and very good (0.81–1.00). We also analysed DR of T, N and M recurrence for both tracers, and concordance.
We statistically analysed the correlation between patients’ characteristics classified in groups (Gleason Score, EAU classification, recurrence PSA and kinetics) and PET/CTs results, both DR and miTNM. In all cases a p value < 0.05 was considered statistically significant. Based on the obtained results a second assessment was focused on the search of strongest cut-off values of PSA, achieved by receiver operating characteristic (ROC) curve, for the prediction of metastatic disease in comparison with exclusively T and/or N disease.
Search strategy and study selection for the review
Two authors (LGZ and AMGV) performed a computer literature search on PubMed/MEDLINE databases to find relevant retrospective or prospective published articles on head-to-head comparison between choline-labelled tracers and PSMA-ligands in BCR PCa. The exclusion criteria were: (i) articles in no English language, (ii) review articles, editorials or letters, comments, conference proceedings, case reports or small case series (<20) and (iii) no head-to-head comparison among these two imaging methods.
The researchers independently reviewed the titles and abstracts of the retrieved articles, applying the inclusion and exclusion criteria. After the selection, the full-text version of the remaining articles, to assess their eligibility for inclusion, were obtained resolving disagreements in a consensus meeting.
3. Results
One hundred and thirty-eight patients were enrolled. All the patients’ characteristics are presented in Table 1.
- Detection rate and TNM staging by 18F-DCFPyL and 18F-Fluorocholine PET/CT
18F-DCFPyL showed a higher DR than 18F-Fluorocholine, 64.5% (89/138) and 33.3% (46/138), respectively (Table 2). Both were negative in 44 patients (31.9%) and positive in 41 (29.7%), however, in 20/41 patients, 18F-DCFPyL visualized additional lesions with respect to 18F-Fluorocholine, which entailed miTNM stage change in 17 patients (Figure 1).
On the other hand, 18F-DCFPyL was positive alone in 48/89 (53.9%) patients, being oligometastatic in 25 (Figure 2). Five patients were exclusively positive with 18F-Fluorocholine-PET/CT, and thus 18F-DCFPyL down-staged 18F-Fluorocholine results from positive to negative (3 follow-up, 1 biopsy (negative) and 1 ADT). 18F-DCFPyL up-staged 5/21 patients with OD on 18F-Fluorocholine-PET/CT to polimetastatic disease after 18F-DCFPyL.
18F-DCFPyL and 18F-Fluorocholine PET/CTs detected T in 33.3% and 19.6%, respectively, with a moderate concordance. N was observed in 27.5% on 18F-DCFPyL scans and 13.8% on 18F-Fluorocholine. However, the most significant difference was found for M detection, 30.4% and 8.7%, for 18F-DCFPyL and 18F-Fluorocholine respectively (Table 3).
- miTNM: molecular imaging TNM, k: kappa.
Regarding first to subsequent BCR, 18F-Choline DR was 35.6% and 27% respectively, and 18F-DCFPyL DR 61.4% and 72.9%. No statistically differences were found in first to subsequent BCR DR neither 18F-Choline or 18F-DCFPyL (p = 0.435 and p = 0.164, respectively). We found weak (k = 0.378, p < 0.001) and poor (k = 0.079, p < 0.467) concordance in first to subsequent BCR DR between 18F-Choline and 18F-DCFPyL.
Correlation between PET/CT results and PSA kinetics
Both 18F-DCFPyL and 18F-Fluorocholine PET/CT DR showed significant associations with PSA groups and PSAvel. No significant association was found with PSAdt. 18F-DCFPyL DR was 81.3% in patients with PSA > 2 ng/ml, higher than patients with 1 < PSA ≤ 2 (58.8%) and PSA ≤ 1 ng/ml (39.1%). It was also higher in patients with PSAvel > 0.2 ng/ml/month (90.5%) compared with those with PSAvel ≤ 0.2 ng/ml/month (53.7%). 18F-Fluorocholine DR was also higher in cases with PSA > 2 ng/ml (46.6%), being 35.3% and 13.04% in patients with 1 < PSA ≤ 2 and PSA ≤ 1 ng/ml respectively, and 52.4% in cases with PSAvel > 0.2 ng/ml/month versus 26.3% with PSAvel ≤ 0.2 ng/ml/month. In addition, mean PSA was statistically different among patients with T and N recurrence on 18F-Fluorocholine-PET/CT (p = 0.028). Also differences in mean PSA and PSAdt were found between N and M (p = 0.034), and T and M (p = 0.031) metabolic disease, respectively, on 18F-DCFPyL-PET/CT (Table 4).
Using predefined cut-off values of PSA and PSA kinetics values significant association was only found between miTNM and PSA groups on 18F-Fluorocholine-PET/CT (p = 0.033) and not for PSAdt or PSAvel. No statistical association was found between miTNM, PSA or PSA kinetics on 18F-DCFPyL PET/CT. In ROC analysis, only a PSAdt cut-off of 4.09 months showed significant association for the prediction of M stage with 18F-Fluorocholine-PET/CT (66.7% sensitivity, 73.8% specificity, 0.720 AUC, p = 0.012). For 18F-DCFPyL PET/CT the obtained cut-offs in the prediction of M stage were: PSA of 2.41 ng/ml (66.7% sensitivity, 64.4% specificity, 0.675 AUC, p = 0.002), PSAdt of 5.59 months (61.1% sensitivity, 60.8% specificity, 0.679 AUC, p = 0.001) and PSAvel of 0.13 ng/ml/month (66.7% sensitivity, 61.4% specificity, 0.723 AUC, p < 0.001).
- Therapeutic impact and follow-up
As a result of 18F-DCFPyL-PET/CT, therapeutic management was changed in 40/138 (29%) patients with respect to 18F-Fluorocholine-PET/CT based planning treatment. Escalation was elected in 34 patients: 6 radiotherapy, 5 radiotherapy plus ADT, 6 surgery, 1 prostate cryoablation and 16 ARAT. De-escalation occurred in 6 patients: follow-up in 4 cases (3 18F-DCFPyL negative and 1 with prostatic uptake with both radiotracers and no malignant disease confirmed by biopsy) and ADT instead local treatment in 2 cases. Nevertheless, a potential change in therapeutic management was not achieved because of patient’s comorbidities in 11 patients.
Derived from positive 18F-DCFPyL-PET/CT, 19 patients underwent additional diagnostic procedures to confirm the results: 8 by imaging (3/8 was confirmed) and 11 by histological analysis (8/11 was confirmed) (Figure 3) (Figure 4).
18F-DCFPyL-PET/CT was negative in 49/138 patients (7 low, 14 intermediate and 28 high risk). Follow-up was adopted in 29 patients (4 positive 18F-Fluorocholine-PET/CT) and 20 intermediate/high risk patients underwent treatment (12 prostatic fossa radiotherapy, 8 ADT, 1/8 choline-positive). Regarding the false positive, six patients with positive 18F-DCFPyL-PET/CT (2 prostate gland, 3 bone and 1 rectum) had a normal MRI (Figure 5) (Figure 6). Ten patients were choline-positive and considered false positive (2 prostate gland, 5 lymph nodes, 2 bone, 1 pelvic mass) due to 18F-DCFPyL PET/CT result, biopsy or clinical follow-up.
For patients who benefited from a treatment change, local treatments were exclusively guided by 18F-DCFPyL in eleven patients. Follow-up showed: PSA decreased in 6 (4 radiotherapy, 1 cryoablation, 1 surgery), PSA increased in 2 surgically treated patients (in one patient an ulterior 18F-DCFPyL-PET/CT revealed an incomplete surgical procedure and in the other one, surgical procedure was performed almost 7 months after 18F-DCFPyL-PET/CT), in 2 patients biochemical progression occurred before treatment decision, and the remaining patient was missed.
- Literature review
Literature search results from PubMed/MEDLINE revealed 17 articles. Reviewing titles and abstracts, 7 articles were excluded: 4 because not in the field of interest of this review and 3 as reviews. Ten articles were selected and retrieved in full-text version [7,8,9,12,13,14,15,16,17,18]. Data of 1868 patients with BCR PCa who underwent choline-labelled tracers and PSMA ligands PET/CT were eligible for the analysis (systematic review). Methodology and results of the selected papers are summarized on Table 5.
4. Discussion
In BCR, diagnostic impact of PSMA-ligands against choline-labelled tracers is significantly higher in patients with low PSA levels and previous negative/doubtful choline-labelled PET/CT in whom the detection of OD might enable metastasis-directed treatments [19,20]. Differences in classification of OD using both tracers exist, with up-staging for the PSMA ligands especially in choline-negative patients [15]. In our study, patients with previous negative/oligometastatic 18F-Fluorocholine-PET/CT were referred to 18F-DCFPyL expecting a benefit by the detection of more metastases. In fact, we found that 5/21 patients with OD in 18F-Fluorocholine-PET/CT were up-staged to polimetastatic after 18F-DCFPyL, similar to previous reported results [15]. The absence of consensus about oligometastatic definition can limit diagnostic impact comparison of different radiotracers. In previous studies, OD was defined as M stage with ≤ 5 lesions [15,16], whereas other authors considered ≤ 3 as we did in this study [7]. Chevalme et al. found, using 68Ga-PSMA, OD (1–3 foci) in 31% of the cases with previous negative/doubtful 18F-Fluorocholine [7]. In our sample, 18F-DCFPyL-PET/CT detected OD in the 52.1% (25/48) of choline-negative cases. In a relevant number of cases, we detected positive lymph nodes and bone lesions which showed divergent findings with both tracers. The majority were only 18F-DCFPyL-positive, probably due to higher lesion/background ratio and sensitivity compared to 18F-Fluorocholine that enables detection of smaller lesions.
Previous authors found a PSMA-ligands DR from 43.8% to 67% in choline-negative cases, greater in those with doubtful findings [7,8,14,16]. Our results are in accordance with previous, with a 18F-DCFPyL DR of 53.9% in patients with negative/equivocal 18F-Fluorocholine although we did not assess differences between negative and equivocal results based on few cases of the latter (5).
Chevalme et al. found that that DR was lower in first BCR versus previous (63 vs. 72%) [7]. In our study, no significant differences were found neither 18F-Fluorocholine nor 18F-DCFPyL. On the other hand, DR shows a great association with PSA kinetics with independence of the radiotracer used on PET/CT. However, despite a PSAdt ≤ 6 months has been reported as a strong predictor of positivity of choline-labelled PET/CT [20], we don’t find a significant association with DR or miTNM for any of the studied radiotracers with their counterparts. This absence of significant association with predefined unfavourable PSA kinetics promotes the interest in exploring other clinical, metabolic and laboratory parameters. In fact, we found that different cut-off values of PSA kinetics were able to predict M stage, especially for 18F-DCFPyL-PET/CT, although with a moderate accuracy.
Regarding disease location on BCR PCa, 18F-DCFPyL-PET/CT detected T in 33.3% of cases, similar to 26% reported by Chevalme et al. [7], but higher than 11% of Barbaud et al. [8] explained by higher rate of patients Barbaud et al. included with RP (76%). We observed higher T detection than 18F-Fluorocholine, although with a moderate concordance (k = 0.403, p < 0.001). Discrimination between benign and malignant intraprostatic tissue is hampered by low specificity of choline-labelled tracers for PCa based on high affinity of this radiotracer by benign hyperplasia [21,22]. Lymph node is the most prevalent disease location in BCR PCa, showing PSMA-ligands a DR from 34% to 39% with choline-negative [7,8,15]. Our N disease detection using 18F-DCFPyL was lower (27.5%), with a weak concordance with 18F-Fluorocholine. Previous authors found that 55% of the detected lymph nodes were identified with both tracers. Thus, using PSMA-ligands, increase in DR affecting both the number and locations of lymph nodes is a fact [15]. However, the most significant difference in our sample was M detection, 30.4% and 8.7%, for 18F-DCFPyL and 18F-Fluorocholine respectively, in accordance with previous studies [7,15].
Usually PSMA-ligands spots all choline-positive lesions and discordances are mainly related to choline-negative/PSMA-positive findings [13,15]. The explanations of these discordances are contradictory and based on: (i) different metastasis environment with a loss of expression of PSMA that can occur in less than 10% of primary or metastatic prostate tumours [23]; (ii) tumour progression between scans in cases of a wide time interval [9]; and (iii) unspecific inflammation can promote choline uptake in lymph nodes, that can explain additionally choline-positive lymph nodes [24]. PSMA-ligands specificity may range from 36% to 100% [25,26], per se as it targets PSMA, a glycoprotein which overexpression seems more characteristic for PCa than up-regulation of choline kinase [26]. Based on that, we considered findings of PSMA ligands as standard, as previous authors [15,17].
Prostatic fossa salvage radiation treatment (SRT) is the current standard of care in men with their first BCR after RP with about half of men achieving a complete biochemical response at 5 years after SRT [27]. In patients with a previous radical radiotherapy, only brachytherapy is indicated if malignancy is histopathologically confirmed. On the other hand, a second BCR, in patients undergone previous radiotherapy of prostatic fossa, with or without pelvic lymph nodes involved, reduces the potential local treatment options. Therefore, ADT becomes a therapeutic option in patients with BCR without located disease or no indication for any local treatment (SRT or surgery).
Therapeutic impact of PSMA-ligands with respect to choline-labelled PET/CT has been scarcely analysed, ranging from 54% to 74% [8,17]. We observed an impact management in 29% of cases although it could be raised to 37% if patients’ comorbidities that limited correct treatment have been included. Escalation was considered when the treatment modification involved changing/adding radiotherapy fields or adding ARAT to the systemic ADT. Thus, men with a previous RP without disease or with disease confined to the prostatic fossa on PET/CT imaging were expected to proceed to SRT or a combination of radiotherapy and ADT if few lesions were defined on 18F-DCFPyL-PET/CT or ADT plus ARAT in case of multiple locations (M stage) in patients with no chemotherapy indication. The therapeutic impact derived from 18F-DCFPyL over 18F-Fluorocholine findings allowed treatment escalation in most of our patients (34/40). However, the assessment of therapeutic impact is controversial, being not only dependent of the accuracy of diagnostic techniques but on other factors as previously received treatments and the comorbidities or physical status of the patients so, although 18F-DCFPyL-PET/CT result could have changed the therapeutic management, this decision was not carried out because of that in some patients of our sample. Diagnostic escalation (additional diagnostic imaging vs. biopsy) to confirm 18F-DCFPyL results is another relevant aspect to be assessed. In our sample, 19 patients were derived to additional diagnostic procedures, only 11 by histological analysis, lower than the 24% reported by Morigi et al. [17]. About half of men who experience BCR after RP and undergo SRT to the prostatic bed, even when there are no significant imaging findings, are currently cured [28] suggesting that SRT should still be considered despite a negative imaging result [29]. On the other hand, focused radiotherapy based on PSMA ligands PET/CT, exhibits higher response rates compared to the conventional procedure without metabolic guide, although can not guarantee undetectable PSA in all the cases, that means that PSMA PET/CT still underestimates the extent of the recurrent disease [8,29]. In the present analysis, 12 out of 49 patients with a negative 18F-DCFPyL-PET/CT underwent prostatic fossa radiotherapy.
Thus, therapeutic implications of PSMA-ligands can be significant can be significant. Target miss in BCR due to insufficient diagnostic work-up may lead to inadequate definition local disease and to untreated microscopic or macroscopic disease distant from prostatic fossa (N1/M1). The expected result, derived from an earlier and more accurate diagnosis of PSMA ligands PET/CT, is the opportunity for focused management using focal treatments, with a reduction of the introduction of ADT. The possibility of an improved disease control as long as possible before ADT introduction, would reduce the resistance to ADT during their disease, which may limit future therapeutic possibilities [30,31].
Regarding limitations, histopathological confirmation of our PET/CT results was not always feasible, although it is a controversial issue and probably neither indicated nor ethical. In addition, 2 months period used between both PET/CT could limit a reliable comparison between both radiotracers in cases of a highly proliferative disease. However, PCa usually presents with slow growth and noticeable changes within this period are very unlikely. With respect to the strengths, this is the first reported experience of 18F-DCFPyL in parallel comparison with 18F-Fluorocholine in a significant sample of patients with BCR PCa.
5. Conclusions
18F-DCFPyL provided a higher DR than 18F-Fluorocholine in restaging of BCR, especially in patients with high PSA and unfavourable PSA kinetics, being superior in miTNM staging and showing a fair agreement to 18F-Fluorocholine-PET/CT. Information derived from 18F-DCFPyL changed therapeutic management in a significant number of patients (29%) with respect to 18F-Fluorocholine-PET/CT.
No disclaimer.
All the authors have participated in the writing and revision of this article and take public responsibility for its content.
The present publication is approved by all authors and by the responsible authorities where the work was carried out.
All the authors confirm the fact that the article is not under consideration for publication elsewhere.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Institutional Review Board Statement
This study was approved by a reference Ethical Committee (internal code of 2022-53).
Informed Consent Statement
Patients signed an informed consent to participate and to use their anonymous data for analysis and publication of results.
Conflicts of Interest
The authors have no relevant financial or non-financial interests to disclose.
References
- Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part II: Treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol 2017, 71, 630–42. [Google Scholar] [CrossRef] [PubMed]
- Fanti S, Minozzi S, Castellucci P, Balduzzi S, Herrmann K, Krause BJ, et al. PET/CT with 11C-choline for evaluation of prostate cancer patients with biochemical recurrence: meta-analysis and critical review of available data. Eur J Nucl Med Mol Imaging 2016, 43, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Castellucci P, Fuccio C, Nanni C, Santi I, Rizzello A, Lodi F, et al. Influence of trigger PSA and PSA kinetics on 11C-Choline PET/CT detection rate in patients with biochemical relapse after radical prostatectomy. J Nucl Med 2009, 50, 1394–400. [Google Scholar] [CrossRef]
- Evangelista L, Briganti A, Fanti S, Joniau S, Reske S, Schiavina R, et al. New clinical indications for 18F/11C-choline, new tracers for positron emission tomography and a promising hybrid device for prostate cancer staging: a systematic review of the literature. Eur Urol 2016, 70, 161–75. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh A, Haberkorn U, Eder M, Eisenhut M, Zechmann CM. [68Ga]gallium-labelled PSMA ligand as superior PET tracer for the diagnosis of prostate cancer: comparison with 18F-FECH. Eur J Nucl Med Mol Imaging 2012, 39, 1085–86. [Google Scholar] [CrossRef] [PubMed]
- Rowe S, Gorin M, Pienta K, Siegel B, Carroll P, Pouliot F, et al. Results from the OSPREY trial: A Prospective Phase 2/3 Multi-Center Study of 18F-DCFPyL PET/CT imaging in patients with prostate cancer—Examination of diagnostic accuracy. J Nucl Med 2019, 60, 586. [Google Scholar]
- Chevalme YM, Boudali L, Gauthé M, Rousseau C, Skanjeti A, Merlin C, et al. Survey by the French Medicine Agency (ANSM) of the imaging protocol, detection rate, and safety of 68Ga-PSMA-11 PET/CT in the biochemical recurrence of prostate cancer in case of negative or equivocal 18F-fluorocholine PET/CT: 1084 examinations. Eur J Nucl Med Mol Imaging 2021, 48, 2935–50. [Google Scholar] [CrossRef]
- Barbaud M, Frindel M, Ferrer L, Thiec ML, Rusu D, Rauscher A, et al. 68Ga-PSMA-11 PET-CT study in prostate cancer patients with biochemical recurrence and non-contributive 18F-Choline PET-CT: Impact on therapeutic decision-making and biomarker changes. The Prostate 2019, 79, 454–61. [Google Scholar] [CrossRef]
- Witkowska-Patena, E, Gizewska A, Dziuk M, Miśko J, Budzyńska A, Walęcka-Mazur A. Head-to-Head Comparison of 18F-Prostate-Specific Membrane Antigen-1007 and 18F-Fluorocholine PET/CT in biochemically relapsed Prostate Cancer. Clin Nucl Med 2019, 44, e629–e633. [Google Scholar] [CrossRef]
- Eiber M, Herrmann K, Calais J, Hadaschik B, Giesel FL, Hartenbach M, et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J Nucl Med 2018, 59, 469–78. [Google Scholar] [CrossRef]
- van Leenders GJLH, van der Kwast TH, Grignon DJ, Evans AJ, Kristiansen G, Kweldam CF, et al. The 2019 International Society of Urological Pathology (ISUP) Consensus Conference on Grading of Prostatic Carcinoma. Am J Surg Pathol 2020, 44, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Alonso O, Dos Santos G, García Fontes M, Balter H, Engler H. 68Ga-PSMA and 11C-choline comparison using a tri-modality PET/CT-MRI (3.0 T) system with a dedicated shuttle. Eur J Hybrid Imaging 2018, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Cantiello F, Crocerossa F, Russo GI, Gangemi V, Ferro M, Vartolomei MD, et al. Comparison between 64Cu-PSMA-617 PET/CT and 18F-Choline PET/CT imaging in early diagnosis of prostate cancer biochemical recurrence. Clin Genitourin Cancer 2018, 16, 385–91. [Google Scholar] [CrossRef] [PubMed]
- Caroli P, Sandler I, Matteucci F, De Giorgi U, Uccelli L, Celli M, et al. 68Ga-PSMA PET/CT in patients with recurrent prostate cancer after radical treatment: prospective results in 314 patients. Eur J Nucl Med Mol Imaging 2018, 45, 2035–44. [Google Scholar] [CrossRef] [PubMed]
- Schwenck J, Rempp H, Reischl G, Kruck S, Stenzl A, Nikolaou K, et al. Comparison of 68Ga-labelled PSMA-11 and 11C-choline in the detection of prostate cancer metastases by PET/CT. Eur J Nucl Med Mol Imaging 2017, 44, 92–101. [Google Scholar] [CrossRef]
- Bluemel C, Krebs M, Polat B, Linke F, Eiber M, Samnick S, et al. 68Ga- PSMA-PET/CT in patients with biochemical prostate cancer recurrence and negative 18F-choline-PET/CT. Clin Nucl Med 2016, 41, 515–21.
- Morigi JJ, Stricker PD, van Leeuwen PJ, Tang R, Ho B, Nguyen Q, et al. Prospective comparison of 18F-fluoromethylcholine versus 68Ga-PSMA PET/CT in prostate cancer patients who have rising PSA after curative treatment and are being considered for targeted therapy. J Nucl Med 2015, 56, 1185–90. [Google Scholar] [CrossRef]
- Afshar-Oromieh A, Zechmann CM, Malcher A, Eder M, Eisenhut M, Linhart HG, et al. Comparison of PET imaging with a 68Ga-labelled PSMA ligand and 18F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging 2014, 41, 11–20. [Google Scholar] [CrossRef]
- Umbehr MH, Müntener M, Hany T, Sulser T, Bachmann LM. The role of 11C-choline and 18F-fluorocholine positron emission tomography (PET) and PET/CT in prostate cancer: a systematic review and meta-analysis. Eur Urol 2013, 64, 106–17. [Google Scholar] [CrossRef]
- Treglia G, Ceriani L, Sadeghi R, Giovacchini G, Giovanella L. Relationship between prostate-specific antigen kinetics and detection rate of radiolabelled choline PET/CT in restaging prostate cancer patients: a meta-analysis. Clin Chem Lab Med 2014, 52, 725–33. [Google Scholar]
- Souvatzoglou M, Weirich G, Schwarzenboeck S, Maurer T, Schuster T, Bundschuh RA, et al. The sensitivity of 11C choline PET/CT to localize prostate cancer depends on the tumor configuration. Clin Cancer Res 2011, 17, 3751–59. [Google Scholar] [CrossRef] [PubMed]
- Farsad M, Schiavina R, Castellucci P, Nanni C, Corti B, Martorana G, et al. Detection and localization of prostate cancer: correlation of 11C-choline PET/CT with histo-pathologic step-section analysis. J Nucl Med 2005, 46, 1642–9. [Google Scholar]
- Mannweiler S, Amersdorfer P, Trajanoski S, Terrett JA, King D, Mehes G. Heterogeneity of prostate-specific membrane antigen (PSMA) expression in prostate carcinoma with distant metastasis. Pathol Oncol Res 2009, 15, 167–72. [Google Scholar] [CrossRef] [PubMed]
- van Waarde A, Jager PL, Ishiwata K, Dierckx RA, Elsinga PH. Comparison of sigma-ligands and metabolic PET tracers for differentiating tumor from inflammation. J Nucl Med 2006, 47, 150–4. [Google Scholar]
- Giesel FL, Hadaschik B, Cardinale J, Radtke J, Vinsensia M, Lehnert W, et al. F-18 labelled PSMA-1007: biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur J Nucl Med Mol Imaging 2017, 44, 678–88. [Google Scholar] [CrossRef]
- Ghosh A, HestonWD. Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J Cell Biochem 2004, 91, 528–39. [Google Scholar] [CrossRef]
- Carrie C, Hasbini A, de Laroche G, Richaud P, Guerif S, Latorzeff I, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): a randomised, multicentre, open-label phase 3 trial. Lancet Oncol 2016, 17, 747–56. [Google Scholar] [CrossRef]
- Stephenson AJ, Scardino PT, Kattan MW, Pisansky TM, Slawin KM, Klein EA, et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J Clin Oncol 2007, 25, 2035–41. [Google Scholar] [CrossRef]
- Fendler WP, Calais J, Eiber M, Flavell RR, Mishoe A, Feng FY, et al. Assessment of 68Ga-PSMA-11 PET accuracy in localizing recurrent prostate cancer: a prospective single-arm clinical trial. JAMA Oncol 2019, 5, 856–63. [Google Scholar] [CrossRef]
- Tosoian JJ, Gorin MA, Ross AE, Pienta KJ, Tran PT, Schaeffer EM. Oligometastatic prostate cancer: definitions, clinical outcomes and treatment considerations. Nat Rev Urol 2017, 14, 15–25. [Google Scholar] [CrossRef]
- Han S, Woo S, Kim YJ, Suh CH. Impact of 68 Ga-PSMA PET on the management of patients with prostate cancer: a systematic review and meta-analysis. Eur Urol 2018, 74, 179–90. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
59-year-old patient. Gleason 7 PCa treated with radiotherapy plus ADT. After ADT withdrawal BCR was detected (PSA 2.44 ng/mL, PSAdt 2.6 mo, PSAvel 0.15 ng/mL/mo). 18F-Fluorocholine (a) demonstrated only prostatic uptake and 18F-DCFPyL-PET/CT (b) showed prostatic tracer uptake and lymph node metastasis (arrows). Time window of sixteen days between both scans. 18F-DCFPyL changed therapeutic management allowing escalation (ADT + Apalutamide).
Figure 1.
59-year-old patient. Gleason 7 PCa treated with radiotherapy plus ADT. After ADT withdrawal BCR was detected (PSA 2.44 ng/mL, PSAdt 2.6 mo, PSAvel 0.15 ng/mL/mo). 18F-Fluorocholine (a) demonstrated only prostatic uptake and 18F-DCFPyL-PET/CT (b) showed prostatic tracer uptake and lymph node metastasis (arrows). Time window of sixteen days between both scans. 18F-DCFPyL changed therapeutic management allowing escalation (ADT + Apalutamide).
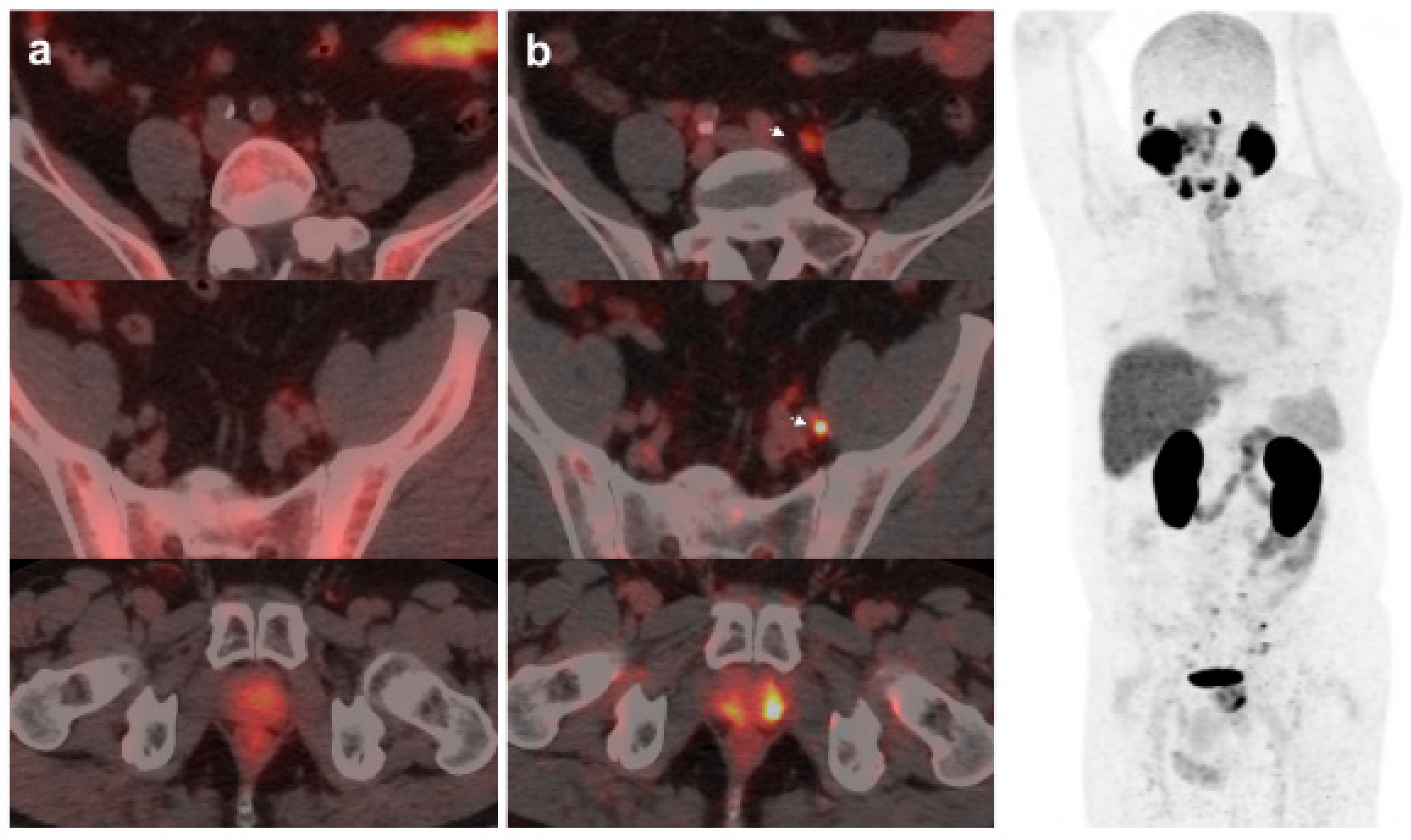
Figure 2.
67-year-old patient. Gleason 7 PCa treated with RP. First BCR treated with prostate fossa radiotherapy. Second BCR (PSA: 0.63 ng/mL, PSAdt 8.6 mo, PSAvel 0.04 ng/mL/mo) scanned with 18F-Fluorocholine (a) and 18F-DCFPyL-PET/CT (b), time window of six days. Lymph nodes metastasis (arrows) were demonstrated only on 18F-DCFPyL scan, changing therapeutic management (escalation). Patient underwent lymph nodes SBRT descending PSA level.
Figure 2.
67-year-old patient. Gleason 7 PCa treated with RP. First BCR treated with prostate fossa radiotherapy. Second BCR (PSA: 0.63 ng/mL, PSAdt 8.6 mo, PSAvel 0.04 ng/mL/mo) scanned with 18F-Fluorocholine (a) and 18F-DCFPyL-PET/CT (b), time window of six days. Lymph nodes metastasis (arrows) were demonstrated only on 18F-DCFPyL scan, changing therapeutic management (escalation). Patient underwent lymph nodes SBRT descending PSA level.
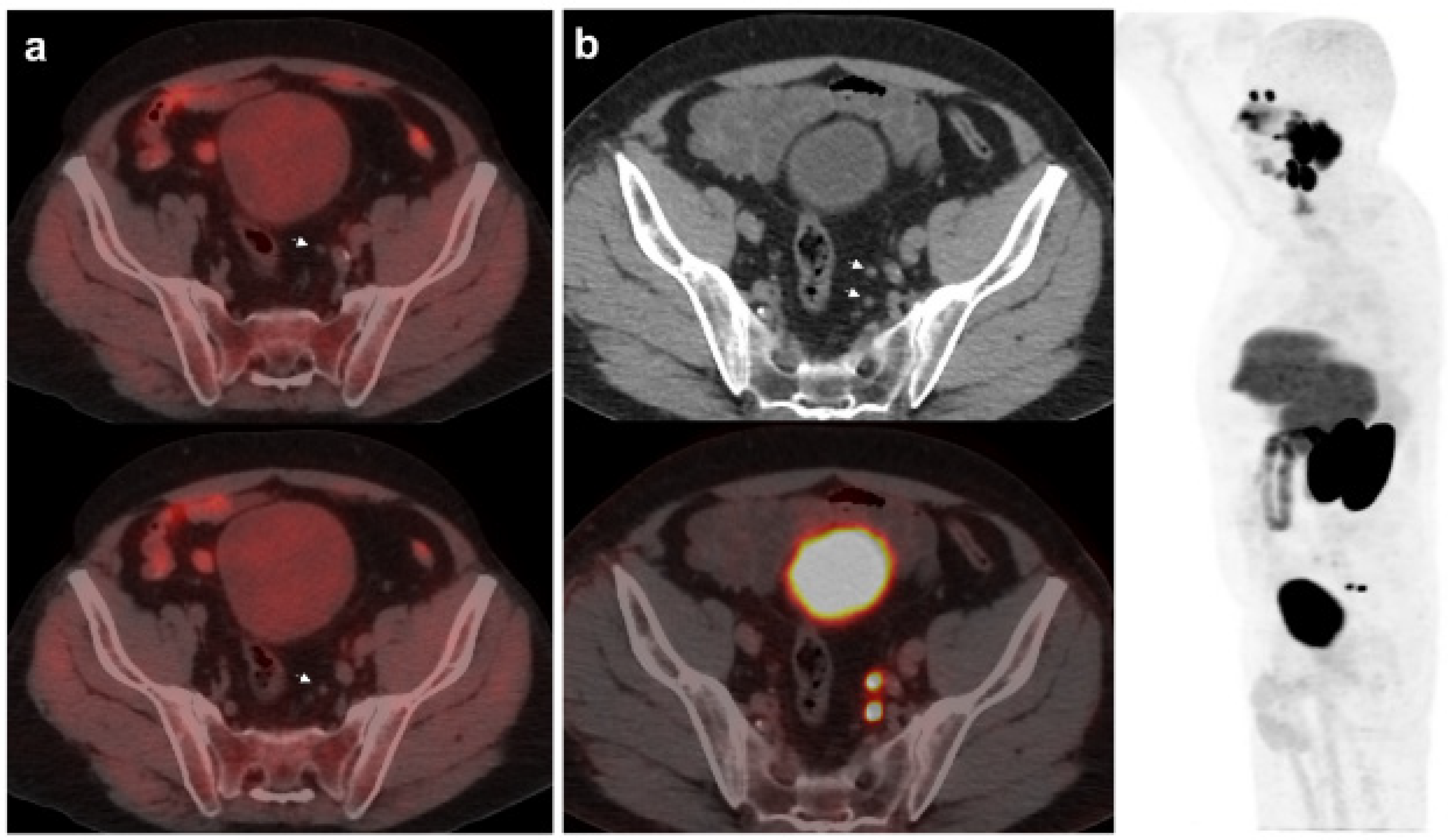
Figure 3.
55-year-old patient. Gleason 8 PCa treated with RP. First BCR treated with prostate fossa radiotherapy. Second BCR (PSA: 0.84 ng/mL, PSAdt 5.99 mo, PSAvel 0.07 ng/mL/mo). 18F-Fluorocholine-PET/CT negative (a). 18F-DCFPyL-PET/CT (b), time window of twenty days, revealed two right external iliac lymph node metastasis (arrows). Lymphadenectomy was decided (escalation), without histopathological confirmation of malignancy. In follow-up PSA progressed (2.07 ng/mL) and an additional 18F-DCFPyL-PET/CT (c) showed exactly same lymph nodes (arrows). SBRT was administered decreasing the PSA level, reclassifying 18F-DCFPyL-PET/CT results as true positive.
Figure 3.
55-year-old patient. Gleason 8 PCa treated with RP. First BCR treated with prostate fossa radiotherapy. Second BCR (PSA: 0.84 ng/mL, PSAdt 5.99 mo, PSAvel 0.07 ng/mL/mo). 18F-Fluorocholine-PET/CT negative (a). 18F-DCFPyL-PET/CT (b), time window of twenty days, revealed two right external iliac lymph node metastasis (arrows). Lymphadenectomy was decided (escalation), without histopathological confirmation of malignancy. In follow-up PSA progressed (2.07 ng/mL) and an additional 18F-DCFPyL-PET/CT (c) showed exactly same lymph nodes (arrows). SBRT was administered decreasing the PSA level, reclassifying 18F-DCFPyL-PET/CT results as true positive.
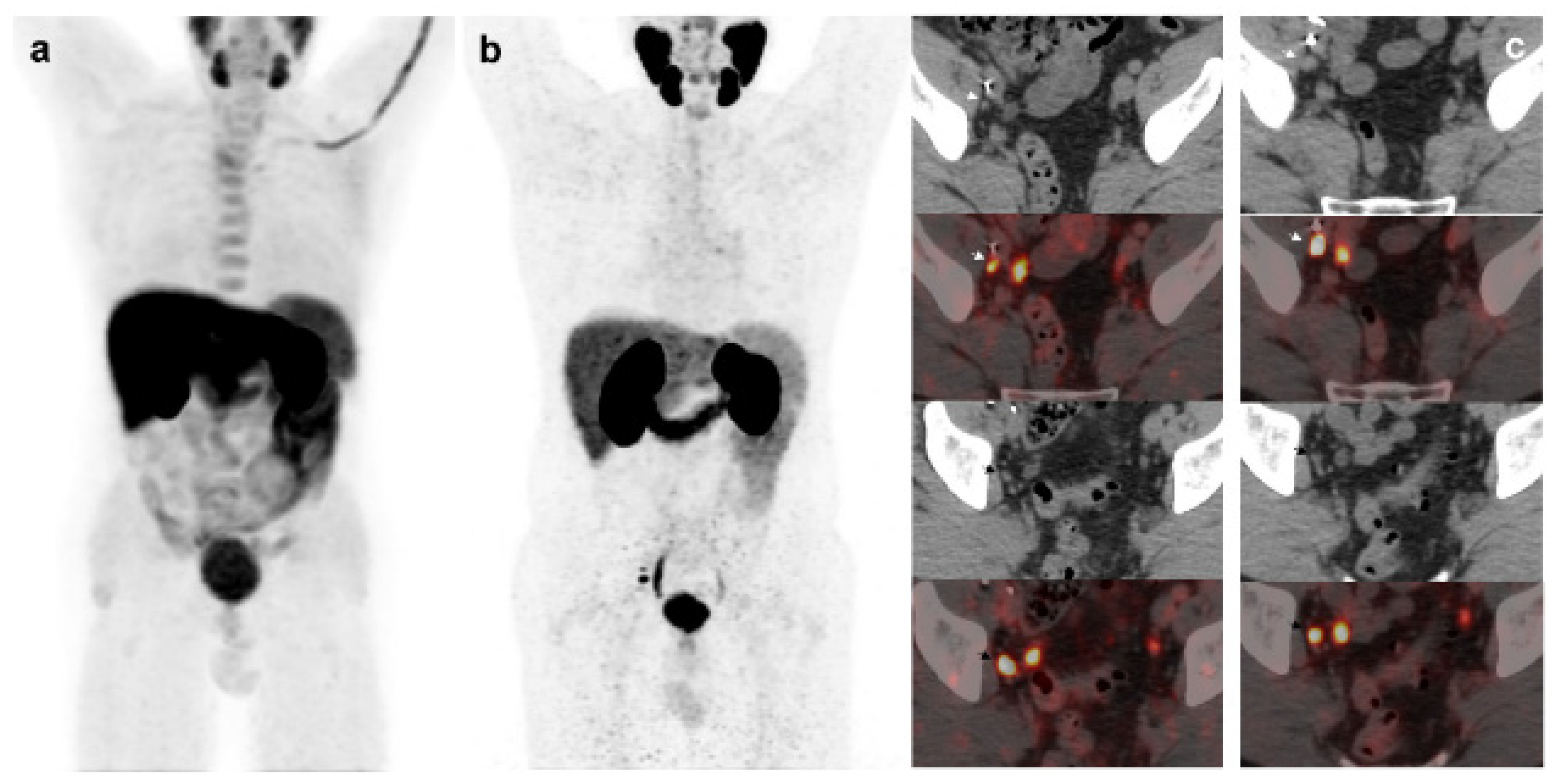
Figure 4.
70-year-old patient. Gleason 9 PCa, treated initially with RP and radiotherapy after his first BCR.Second BCR (PSA: 0.7 ng/mL, PSAdt 5.6 mo, PSAvel 0.05 ng/mL/mo) with 18F-Fluorocholine (a) and 18F-DCFPyL scans showing mediastinal lymph node tracer uptake (b) reported as inflammatory process. Follow-up was decided and PSA level continued increasing. A new 18F-DCFPyL scan (c) was performed 3 months later, showed and increased in size and metabolism of mediastinal lymph node with additional microfoci of radiotracer uptake in lung and bone, suspicious of metastases. An endobronchial ultrasound guided lymph node biopsy confirmed prostatic origin of metastasis. ADT + Apalutamide was initiated (escalation).
Figure 4.
70-year-old patient. Gleason 9 PCa, treated initially with RP and radiotherapy after his first BCR.Second BCR (PSA: 0.7 ng/mL, PSAdt 5.6 mo, PSAvel 0.05 ng/mL/mo) with 18F-Fluorocholine (a) and 18F-DCFPyL scans showing mediastinal lymph node tracer uptake (b) reported as inflammatory process. Follow-up was decided and PSA level continued increasing. A new 18F-DCFPyL scan (c) was performed 3 months later, showed and increased in size and metabolism of mediastinal lymph node with additional microfoci of radiotracer uptake in lung and bone, suspicious of metastases. An endobronchial ultrasound guided lymph node biopsy confirmed prostatic origin of metastasis. ADT + Apalutamide was initiated (escalation).
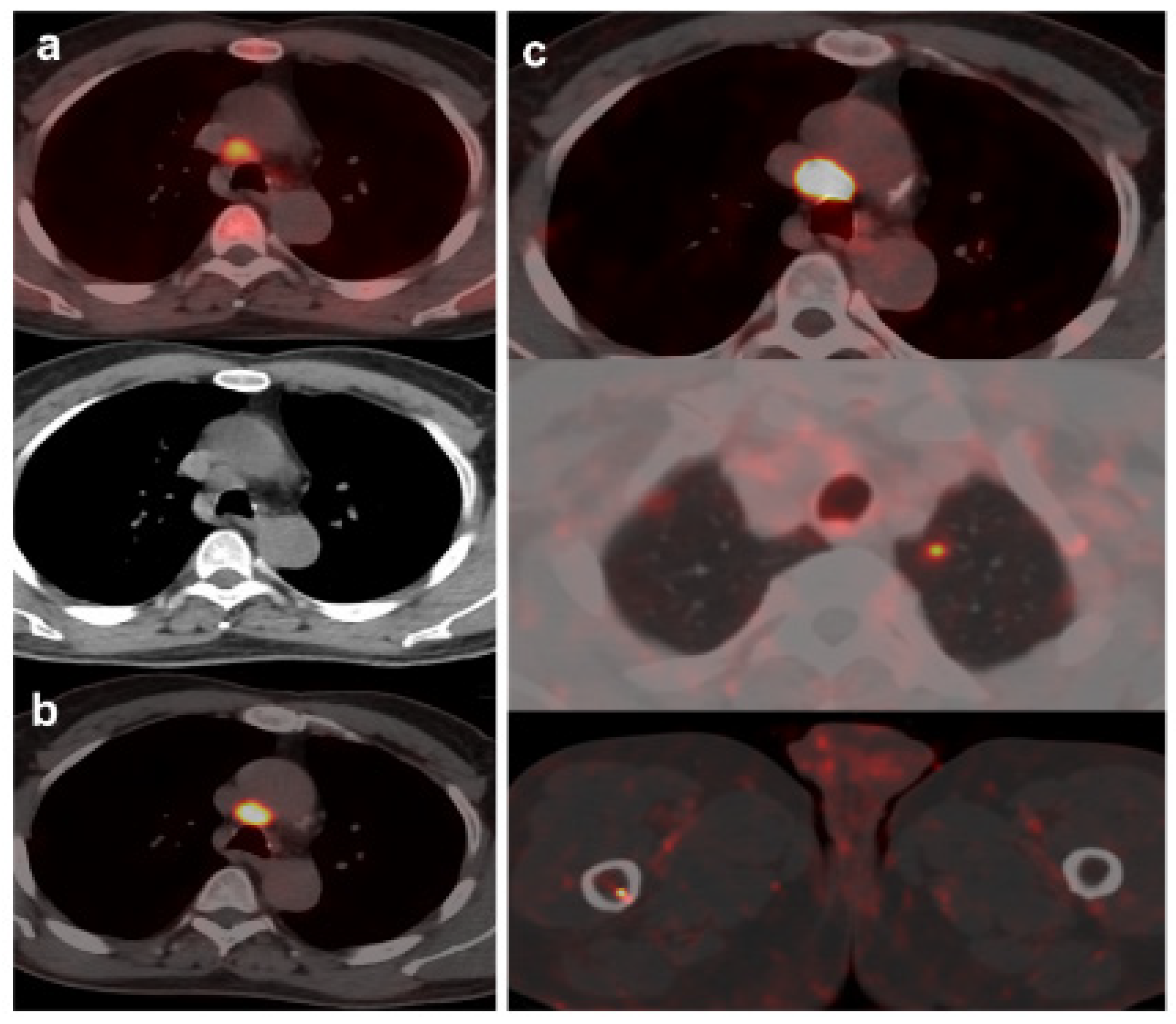
Figure 5.
BCR in a 71-year-old patient (PSA: 0.26 ng/mL, PSAdt: 1.09 mo, PSAvel: 0.2 ng/mL/mo, PSAdt 1.09 mo, PSAvel 0.2 ng/mL/mo) after RP of PCa (Gleason 6, pT2c). 18F-DCFPyL scan showed a slightuptake on left iliac bone with minimal sclerotic changes. Previous negative 18F-Fluorocholine scan (timewindow of one week). MRI did not confirm malignancy of PSMA uptake (false positive). Prostatic bedradiotherapy was given and PSA level decreased.
Figure 5.
BCR in a 71-year-old patient (PSA: 0.26 ng/mL, PSAdt: 1.09 mo, PSAvel: 0.2 ng/mL/mo, PSAdt 1.09 mo, PSAvel 0.2 ng/mL/mo) after RP of PCa (Gleason 6, pT2c). 18F-DCFPyL scan showed a slightuptake on left iliac bone with minimal sclerotic changes. Previous negative 18F-Fluorocholine scan (timewindow of one week). MRI did not confirm malignancy of PSMA uptake (false positive). Prostatic bedradiotherapy was given and PSA level decreased.
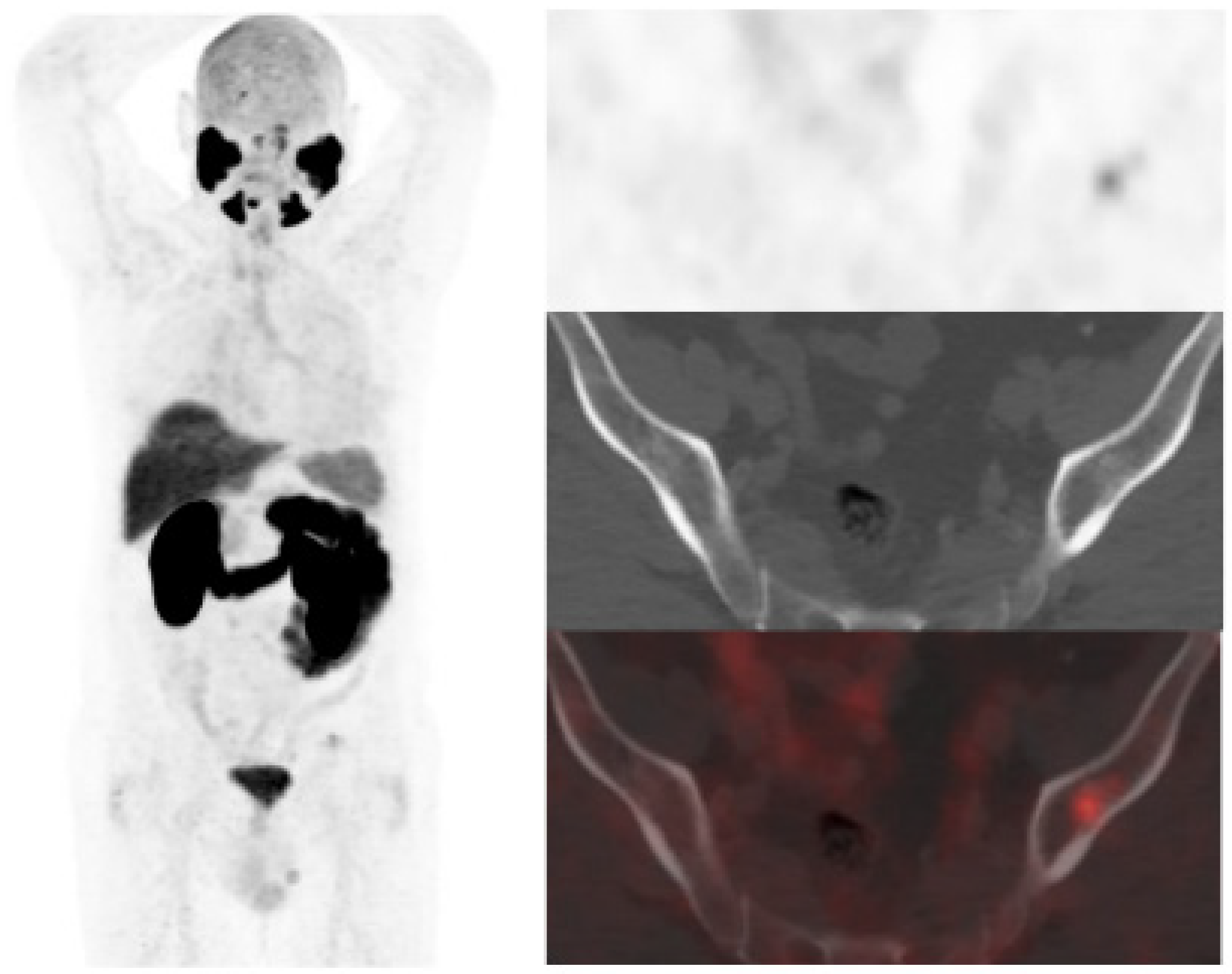
Figure 6.
56-year-old patient. PCa (Gleason 6) treated with braquitherapy. BCR (PSA: 5.4 ng/mL, PSAdt 6.17 mo, PSAvel 0.55 ng/mL/mo). 18F-Fluorocholine (a) showed prostate gland uptake and right external iliac lymph nodes metastasis (arrow). One month later the patient was also scanned with 18F-DCFPyL (b) revealing only prostate gland pathological tracer uptake. Prostate biopsy was negative (false PSMA positive). Follow-up was decided and PSA level keeps oscillating (4–5 ng/mL) with an additional negative 18F-DCFPyL PET/CT one year later.
Figure 6.
56-year-old patient. PCa (Gleason 6) treated with braquitherapy. BCR (PSA: 5.4 ng/mL, PSAdt 6.17 mo, PSAvel 0.55 ng/mL/mo). 18F-Fluorocholine (a) showed prostate gland uptake and right external iliac lymph nodes metastasis (arrow). One month later the patient was also scanned with 18F-DCFPyL (b) revealing only prostate gland pathological tracer uptake. Prostate biopsy was negative (false PSMA positive). Follow-up was decided and PSA level keeps oscillating (4–5 ng/mL) with an additional negative 18F-DCFPyL PET/CT one year later.
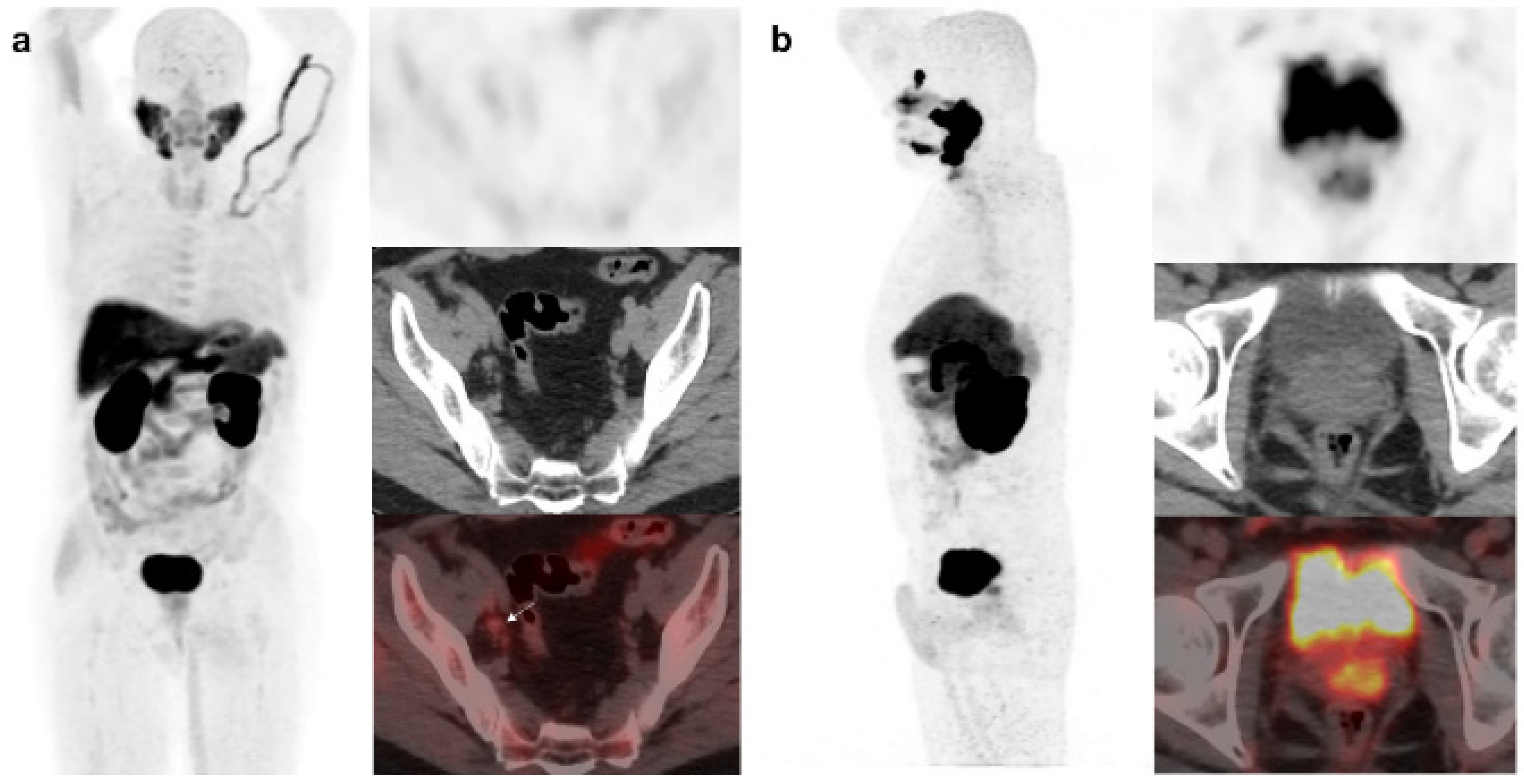

Table 1.
Baseline characteristics of 138 study subjects.
| Characteristic | Value |
|---|---|
| Age (y) | |
| Mean ± SD | 69.77 ± 7.54 |
| Range | 55–87 |
| Grade group | |
| 1 | 46 (33.3%) |
| 2 | 39 (28.3%) |
| 3 | 30 (21.7%) |
| 4 | 12 (8.7%) |
| 5 | 11 (8%) |
| D’Amico risk | |
| Low | 24 (17.4%) |
| Intermediate | 38 (27.5%) |
| High | 76 (55.1%) |
| Primary treatment | |
| Surgery | 48 (34.8%) |
| Radiotherapy | 60 (43.5%) |
| Both | 30 (21.7%) |
| PSA closest to PET/CTs (ng/ml) | |
| Mean ± SD | 2.80 ± 4.83 |
| PSA ≤ 1 | 46 (33.4%) |
| 1 < PSA ≤ 2 | 17 (12.3%) |
| PSA > 2 | 75 (54.3%) |
| PSAdt (month) | |
| Mean ± SD | 7.34 ± 11.74 |
| ≤ 6 | 73 (52.9%) |
| > 6 | 65 (47.1%) |
| PSAvel (ng/ml/month) | |
| Mean ± SD | 0.26 ± 0.68 |
| ≥ 0.2 | 45 (32.6%) |
| < 0.2 | 93 (67.4%) |
| Biochemical relapse | |
| First | 100 (72.5%) |
| Second or further | 38 (27.5%) |
PSA: prostate specific antigen; SD: standard deviation; PSAdt: PSA doubling time, PSAvel: PSA velocity.
Table 2.
Per patient miTNM obtained from 18F-DCFPyL and 18F-Fluorocholine. PET/CT.
| 18F-DCFPyL | |||||
| (+) | (-) | Total | |||
| T | 18F-Fluorocholine | (+) | 20 | 7 | 27 |
| (-) | 26 | 85 | 111 | ||
| Total | 46 | 92 | 138 | ||
| N1 | (+) | 4 | 8 | 12 | |
| (-) | 15 | 111 | 126 | ||
| Total | 19 | 119 | 138 | ||
| N2 | (+) | 4 | 2 | 6 | |
| (-) | 14 | 118 | 132 | ||
| Total | 18 | 120 | 138 | ||
| M1a | (+) | 2 | 1 | 3 | |
| (-) | 14 | 121 | 135 | ||
| Total | 16 | 122 | 138 | ||
| M1b | (+) | 5 | 2 | 7 | |
| (-) | 16 | 115 | 131 | ||
| Total | 21 | 117 | 138 | ||
| M1c | (+) | 2 | 0 | 2 | |
| (-) | 3 | 133 | 136 | ||
| Total | 5 | 133 | 138 | ||
T: local recurrence; N1: single lymph node region; N2: multiple lymph node regions (≥2); M1a: extrapelvic lymph nodes; M1b: bone involvement; M1c: other sites.
Table 3.
Concordance between 18F-DCFPyL and 18F-Fluorocholine miTNM stages.
| miTNM | Kappa (p value) |
|---|---|
| T | k = 0.403 (p < 0.001) |
| N1 | k = 0.143 (p = 0.086) |
| N2 | k = 0.287 (p < 0.001) |
| M1a | k = 0.181 (p = 0.003) |
| M1b | k = 0.304 (p < 0.001) |
| M1c | k = 0.562 (p < 0.001) |
miTNM: molecular imaging TNM, k: kappa.
Table 4.
PSA, PSAdt and PSAvel (mean ± SD) in miTNM comparison of 18F-DCFPyL and 18F-Fluorocholine.
| 18F-Fluorocholine | 18F-DCFPyL | ||
|---|---|---|---|
| PSA (ng/ml) | T | 3.95 ± 1.92 | 3.17 ± 2.16 |
| N | 2.68 ± 2.10 | 2.25 ± 2.14 | |
| M | 2.73 ± 1.86 | 4.63 ± 8.67 | |
| PSAdt (months) | T | 5.07 ± 12.13 | 7.56 ± 10.83 |
| N | 6.13 ± 4.23 | 5.87 ± 3.51 | |
| M | 9.32 ± 18.42 | 7.34 ± 11.20 | |
| PSAvel (ng/ml/month) | T | 0.45 ± 0.79 | 0.23 ± 0.36 |
| N | 0.28 ± 0.23 | 0.18 ± 0.15 | |
| M | 0.34 ± 0.44 | 0.56 ± 1.19 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



