Submitted:
28 May 2026
Posted:
29 May 2026
You are already at the latest version
Abstract
Environmental exposure to persistent and non-persistent endocrine-disrupting chemicals (EDCs), including per- and polyfluoroalkyl substances (PFAS), polychlorinated biphenyls (PCBs), polybrominated diphenyl ethers (PBDEs), polycyclic aromatic hydrocarbons (PAHs), dioxins, phthalates, and bisphenols, has been increasingly associated with elevated cardiovascular disease (CVD) risk.
Emerging evidence suggests the importance of gene–environment interactions in modulating individual susceptibility to EDC-related cardiovascular effects. This review summarizes current knowledge by synthesizing the main classes of EDCs, evaluating the evidence linking them to cardiovascular outcomes, and highlighting how genetic variability may modulate EDC-induced cardiovascular risk.
Across the studies analyzed, the most extensively investigated genetic polymorphisms involve pathways related to oxidative stress regulation, xenobiotic metabolism and detoxification, hormone signaling, and lipid homeostasis. Variants in antioxidant defense genes, such as CAT, eNOS, and PON1, have been associated with increased hypertension risk and vascular dysfunction following exposure to bisphenols and PAHs. Polymorphisms in GSTP1, CYP2C19, ABCB1, and MTHFR may influence susceptibility to cardiometabolic alterations and congenital heart defects, whereas variants in ESR2, FTO, LEPR, and INSIG2 have been linked to obesity, dyslipidemia, and hypertension associated with PFAS, PBDEs, and bisphenols. A deeper understanding of gene–environment interactions is essential to advance preventive cardiology and mitigate the cardiovascular impact of environmental pollutants.
Keywords:
endocrine disrupting chemicals
; PFAS
; PCBs
; PBDEs
; PAHs
; dioxins
; phthalates
; bisphenols
; cardiovascular risk
; genetic polymorphisms
1. Introduction
Endocrine-disrupting chemicals (EDCs), defined as naturally occurring substances or synthetically produced chemicals capable of altering the endocrine system and consequently causing adverse health effects in intact organisms - both wildlife and humans - have progressively become a global public health concern over recent years owing to the rapid expansion of modern industrial activities and the consequent release of these pollutants into the environment [1,2,3]. In addition to EDCs commonly encountered in everyday life through food contact materials, plastic bottles, cosmetics, detergents, and toys (bisphenols, phthalates), other EDCs belong to the class of persistent organic pollutants (POPs) [6]. Compounds such as polychlorobiphenyls (PCBs), polybrominated diphenyl ethers (PBDEs) and per- and polyfluoroalkyl substances (PFAS) are intentionally designed for industrial purposes to exhibit long environmental persistence and are characterized by high lipophilicity, resistance to chemical degradation, and a strong tendency to bioaccumulate in ecosystems and in the adipose tissue of organisms, with persistence extending up to several decades [5,6]. Other POPs including polycyclic aromatic hydrocarbons (PAHs) and dioxins, are not intentionally manufactured but are generated mainly as byproducts of incomplete combustion of organic materials, particularly during industrial processes [3,7]. The list of substances identified as EDCs is continuously evolving, and it has been estimated that close to one thousand compounds have been characterized as EDCs among the tens of thousands of synthetic chemicals currently detected in the environment [4,5].
Importantly, these substances may exert biological effects at low doses, referring to EDC concentrations that are relevant to human exposure levels, and, similar to endogenous hormones, can act through non-monotonic dose–response relationships [8]. Although human exposure to EDCs occurs predominantly via dietary intake and, to a lesser extent, through dermal contact and inhalation, certain classes of EDCs - such as plasticizers and flame retardants - are capable of transplacental transfer, accumulate in placental tissues, and persist in the fetal circulatory system and organs, thereby posing potential risks to fetal development [4,6].
EDCs can adversely affect cardiovascular health by altering hormonal regulation through multiple mechanisms, even as early as fetal life, when EDCs may interfere with developmental processes [9,10]. Within the developmental origins of health and disease (DOHaD) framework, early-life exposure to certain EDCs such as phthalates and bisphenols can “program” long-term cardiovascular risk, increasing susceptibility to perinatal and postnatal cardiometabolic outcomes [11]. This is particularly relevant given that CVD remains the leading cause of global mortality, with rising incidence partly driven by environmental exposures [12,13]. Epidemiological evidence links EDCs such as phthalates, bisphenols, PCBs, PFAS, and PAHs to adverse cardiovascular outcomes and risk markers, including elevated blood pressure, altered blood lipid profile, and atherosclerosis [14,15].
Individual vulnerability to these effects is further modulated by genetic variability, which influences both the magnitude and progression of CVD in response to EDC exposure. Genetic variants in genes involved in xenobiotic metabolism, oxidative stress, lipid and homocysteine metabolism, and hormone signaling - including GSTM1, GSTT1, CYP enzymes, MTHFR, PON1, PPARG, and estrogen receptor genes - may modify susceptibility to the cardiovascular and cardiometabolic effects of EDCs [16,17,18,19,20,21,22]. Although single nucleotide polymorphisms (SNPs) provide important insights into genetic susceptibility, further research is needed to clarify the mechanisms through which they influence responses to EDCs. Establishing SNPs as reliable predictors of disease risk is essential for improving personalized risk assessment and guiding preventive and therapeutic strategies. However, identifying the most relevant genetic determinants in EDC-related disease pathways remains challenging due to the complexity of gene–environment interactions
This review aims to synthesize current evidence on the impact of SNPs on biological responses to EDC exposure, including PCBs, PBDEs, PFAS, PAHs, dioxins, phthalates, and bisphenols. By examining gene-environment interactions in CVD development, the review discusses key underlying biological mechanisms. It also explores how individual genetic profiles may modulate responses to EDC exposure, offering potential targets for personalized prevention and treatment strategies.
2. Human Biomonitoring and Cardiovascular Effects of Endocrine-Disrupting Chemicals
EDCs have been detected in all ecosystems tested, even those located in remote places, with surface waters as the most contaminated media [2]. These contaminants undergo bioaccumulation, bioconcentration, biomagnification, and long-range transport through food webs and water cycles, ultimately reaching humans as final consumers and affecting all life stages [23]. As EDCs are present in a wide range of everyday products, humans are often exposed to multiple chemicals simultaneously [24]. Human biological biomonitoring (HBM) is a key approach for assessing internal exposure, as it reflects the real-life chemical body burden of contaminants and/or their metabolites resulting from total exposure to chemical substances from multiple sources and through different routes [25]. Therefore, HBM can provide essential information not only on total exposure to contaminants, including EDCs, and on how exposure patterns change over time or differ across geographical regions and populations, but also on the effectiveness of policy actions [25].
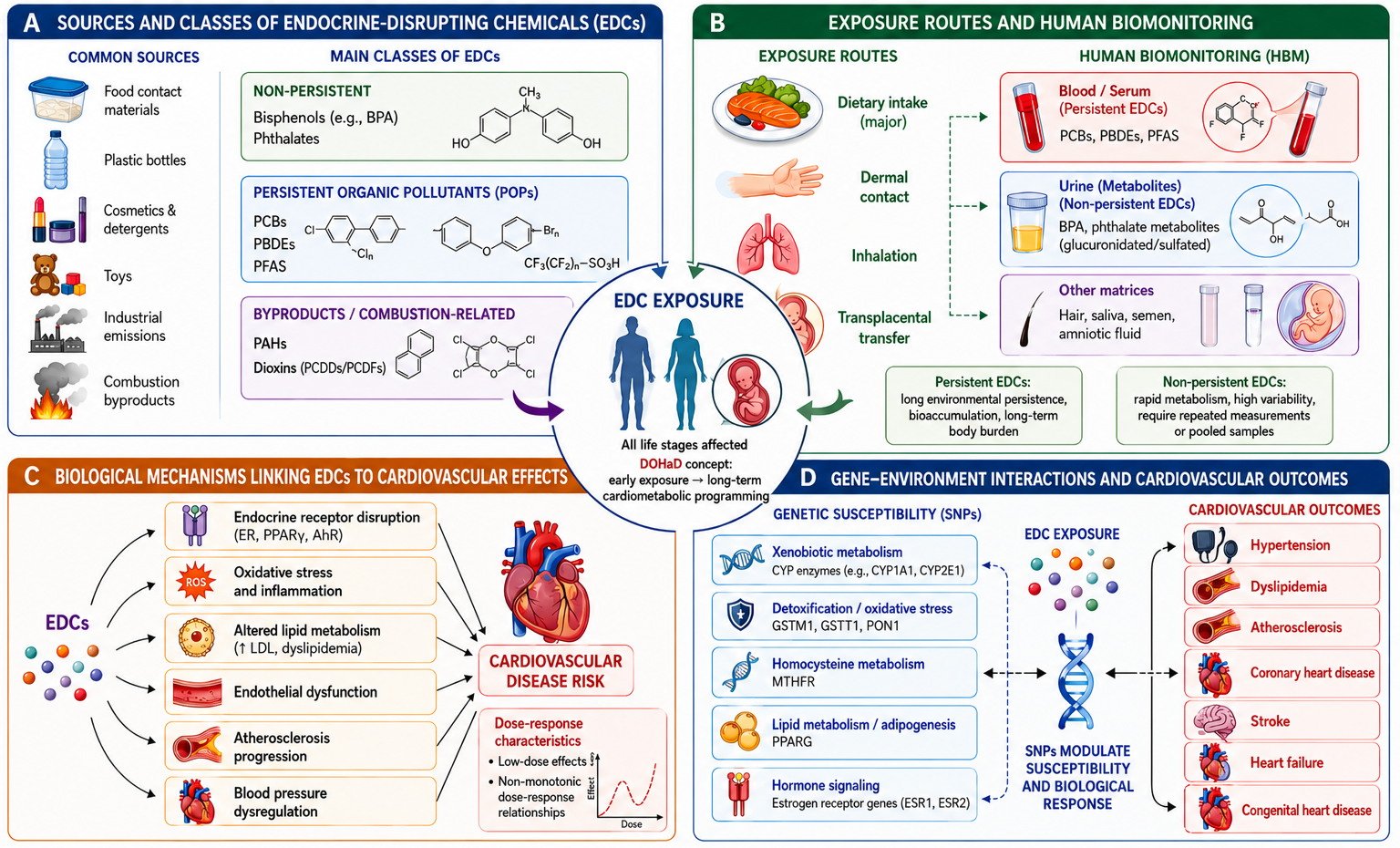
HBM typically assesses the internal concentrations of EDCs and/or their metabolites in blood or urine specimens, although other biological matrices such as amniotic fluid, hair, saliva, and semen can also be used [26]. In general, persistent chemicals (e.g., PCBs, PBDEs, PFAS) are commonly measured in blood or blood derivatives, whereas non-persistent EDCs (e.g., phthalates, bisphenols), due to their hydrophilic nature, undergo extensive metabolism and are conjugated mainly with glucuronide and sulfate groups through human detoxification pathways [24,27]. These reactions generate stable metabolites in varying proportions, which are ultimately excreted via urine [24]. Importantly, while a single concentration of persistent EDCs is a reliable biomarker of exposure over time - regardless of the duration and intensity of exposure - for non-persistent EDCs a single-sample measurement cannot adequately reflect true exposure [27]. Their concentration fluctuates markedly depending on the timing, duration, and intensity of exposure; therefore, multiple measurements or the use of pooled specimens is required to provide a more accurate estimate [27] (Figure 1).
Over the past decade, human biomonitoring of EDCs has gained increasing relevance, also in relation to their potential impact on cardiovascular health. However, despite the growing body of research, the association between EDC exposure and cardiovascular risk remains somewhat inconsistent [28]. Among non-persistent EDCs, bisphenol A (BPA) is a high–production-volume chemical, with approximately ten million tons produced annually worldwide [29]. It is widely used as a monomer in the manufacture of polycarbonate plastics and epoxy resins, which are employed in metal can linings, food containers, baby bottles, dental sealants, medical equipment, thermal paper, toys, and numerous other consumer products [26,30]. Notably, BPA may partially accumulate in adipose tissue, which could account for the relatively slow decline of BPA levels in urine [31]. While one meta-analysis including data from six National Health and Nutrition Examination Survey (NHANES) examination cycles found no significant associations between urinary BPA and five lipid variables related to cardiovascular risk [30], the meta-analysis by Fu et al., which included a total of ten studies, reported a pooled odds ratio (OR) of 1.19 (95% Confidence Interval – 95%CI: 1.03–1.37) for the association between BPA exposure and CVD risk factors [28]. Furthermore, a cross-sectional study based on data from NHANES 2003-2012, demonstrated a significantly positive association between BPA and the risk of CVD (defined as a composite of five self-reported outcomes), with an OR=1.09 (95%CI: 1.01-1.18, p<0.05) per one-unit increment in log-transformed urinary BPA and after adjusting for all covariates [32] These findings support previous results by Yin et al., who reported significant positive associations between urinary BPA levels and both total and individual CVD outcomes, including angina, congestive heart failure, and stroke [33].
Phthalates are the most widely used plasticizers, with a broad range of applications in both industrial and household products [26]. Current global production is estimated at approximately 11 million tons, with continued growth driven by low production costs and the lack of affordable alternatives [34]. In contrast to BPA, phthalates are rapidly metabolized to monoester metabolites and excreted in urine and feces, without accumulating in the human body [26]. Nevertheless, phthalates appear to affect cardiovascular health. In a meta-analysis including five studies that evaluated the association between urinary levels of eight phthalate metabolites and CVD risk, no significant associations were observed for individual metabolites; however, the pooled OR for total phthalate exposure was 1.11 (95%CI: 1.06–1.17) [28]. A recent epidemiological analysis using data from NHANES 2005-2018 reported a significant positive association between phthalate mixtures and CVD prevalence (OR=1.21, 95%CI: 1.07-1.37, p= 0.002) [35]. The study identified several metabolites - mono-(2-ethyl-5-oxohexyl) phthalate (MEOHP), mono-2-ethyl-5-carboxypentyl phthalate (MECPP), monobenzyl phthalate (MBzP), and mono-n-butyl phthalate (MnBP) - as independent and key predictors of CVD (p<0.05) [35].
PFAS are a class of fluorinated synthetic persistent organic chemicals known for their water-resistant, stain-resistant, fire-resistant, and non-stick properties [36,37]. They are produced in high volumes and widely used in numerous industrial and consumer applications, including food-contact materials, personal care products, firefighting foams, and textile protective coatings, resulting in widespread contamination of all environmental matrices [36,38]. Despite the well-established association between PFAS exposure and elevated cholesterol levels in both mechanistic and epidemiological studies, evidence supporting a link with CVD remains insufficient [39,40]. Two recent Swedish longitudinal studies found no significant association between plasma PFAS levels and incident CVD; one assessed perfluorooctanoic acid (PFOA), perfluorooctane sulfonic acid (PFOS,) and perfluorohexanesulfonic acid (PFHxS) in middle-aged individuals, while the other evaluated six PFAS in elderly participants, using a composite endpoint of myocardial infarction, ischemic stroke, and heart failure [36]. Furthermore, a meta-analysis of five independent studies reported a significant inverse association between PFOA levels and incident CVD risk for highest vs lowest exposure (Relative Risk – RR=0.80, 95%CI: 0.66-0.94) [36].
PCBs and PBDEs are two families of POPs in which variation in the number and position of chlorine or bromine atoms gives rise to 209 distinct congeners, resulting in differences in chemical properties and potential toxicity [41,42,43]. Among PCBs, non-coplanar congeners exhibit high reactivity and toxicity, with PCB-77 being one of the most toxic, whereas among PBDEs, PBDE-47 is considered one of the most biologically potent congeners [41]. PCBs have been used as flame retardants and plasticizers [41]; however, their production has been banned in most countries worldwide following ratification of the Stockholm Convention [44]. PBDEs, used since the 1970s in paints, plastics, textiles, building materials, aircraft, and automobiles, were banned in most countries in the early 2000s (penta-BDE and octa-BDE), while deca-BDE production has been subsequently restricted exclusively to vehicle parts until 2036 [41,45]. A meta-analysis of eleven studies demonstrated that PCB-138 and PCB-153 are significant risk factors for CVD (OR=1.35, 95% CI: 1.10–1.66; OR = 1.35, 95% CI: 1.13–1.62, respectively), whereas no association was observed for PCB180 or total PCB exposure [28]. More recently, a large-scale analysis of eleven studies extended these findings by showing robust positive associations between overall PCB exposure (OR=1.56, 95% CI: 1.20–1.75), non-dioxin-like PCBs (OR=1.33, 95% CI: 1.15–1.53), and CVD risk [46]. By contrast, the evidence base linking PBDE exposure to CVD or relevant cardiovascular risk factors is still sparse and inconclusive [47]. However, a recent cross-sectional study using data from NHANES 2005-2016 reported a 23% increased risk of CVD - including coronary heart disease, congestive heart failure, myocardial infarction, angina pectoris, or stroke - in association with higher serum levels of a PBDE mixture (PBDE-28, PBDE-47, PBDE-85, PBDE-99, PBDE-100, PBDE-153, and PBDE-154) (OR=1.23, 95%CI: 1.03–1.47) [48]. Consistently, in U.S. adults, PBDE-209 and PBDE-153 were positively associated with total, remnant, and LDL-cholesterol after adjustment for all covariates, suggesting an increased risk of dyslipidemia and CVD [49].
The term dioxins refers to a heterogeneous group of structurally related, environmentally persistent chemicals generated as by-products of industrial activities, such as metal smelting and the combustion of chlorine-containing organic materials, and exerting toxicity through a common aryl hydrocarbon receptor (AhR)–mediated pathway [50,51]. This group includes polychlorinated dibenzo-p-dioxins (PCDDs), including 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), the most potent congener, together with polychlorinated dibenzofurans (PCDFs). Certain PCBs (dioxin-like PCBs) adopt a coplanar configuration of their biphenyl rings, which allows them to act similarly to dioxins [52]. An early systematic review of twelve longitudinal studies - ten of which were conducted in occupational settings - reported a dose-related increase in mortality from ischemic heart disease and, to a lesser extent, from overall CVD; however, the lack of adjustment for major cardiovascular risk factors limits the consistency and interpretability of these findings [51]. More recently, this evidence has been strengthened by a meta-analysis of ten studies, which found a 31% increased risk of CVD associated with exposure to dioxin-like PCBs (OR=1.31, 95%CI: 1.10–1.57) [46]. Notably, in a representative sample of U.S. adults from NHANES 2003–2004, exposure to dioxins and furans was strongly associated with adverse lipid profiles - including increased LDL and total cholesterol, as well as triglycerides - supporting a link between dioxin exposure and CVD risk [53].
PAHs, generated by incomplete combustion from both natural sources (e.g., wildfires and volcanic activity) and anthropogenic sources (such as vehicle exhaust, residential heating, food grilling, tobacco smoke, and industrial processes), comprise several hundred compounds, although only 16 have been identified as priory pollutants, and seven as probable human carcinogens, by the U.S. Environmental Protection Agency [54,55]. Due to their chemical structure, consisting of two or more fused benzene rings, PAHs are characterized by high stability and hydrophobicity, with hydrophilicity and environmental mobility decreasing as the number of benzene rings increases [55,56]. Despite their environmental persistence, PAHs are extensively metabolized in humans into hydroxylated derivatives that are primarily excreted in urine; nevertheless, parent compounds, with reported half-lives of approximately 6–35 hours, can also be detected in blood [57]. Current evidence links PAH exposure to the pathogenesis of atherosclerosis, cardiometabolic dysfunction, and arterial inflammation [56]. Furthermore, a recent systematic review of twenty studies conducted across diverse geographical regions reported consistent positive associations between PAH exposure and both CVD and established cardiovascular risk factors in occupational settings as well as in the general population [56]. A subsequent systematic review and meta-analysis including a total of nine prospective studies found a significant positive association between all classes of urinary PAH metabolites and both blood pressure (OR=1.32; 95%CI: 1.19-1.48, p < 0.0001) and CVD (OR=1.23; 95%CI: 1.16-1.30, p < 0.0001), while no association was observed with coronary artery disease [54].
In sum, accumulating evidence suggests a potentially important role of EDCs in increasing CVD risk, albeit with substantial heterogeneity in the strength of evidence across different chemical classes. Large, multicenter longitudinal studies with rigorous control of confounding factors, together with a deeper understanding of the underlying biological mechanisms, are warranted to confirm current findings and to inform regulatory strategies aimed at CVD prevention.
3. Gene–Environment Interaction: The Role of Genetic Polymorphisms in Susceptibility to EDC-Induced Cardiovascular Risk
Gene-environment interaction (GxE), whereby genetic background influences the biological response to external exposures, is now widely considered a major determinant shaping interindividual variability in susceptibility to environmental pollutants [58]. Previous evidence has highlighted the relevance of GxE in susceptibility to the effects of toxic elements related to multiple pathological conditions, including CVD [59].
In the context of EDCs, GxE mechanisms are being investigated to explain why comparable levels of exposure may lead to markedly different cardiovascular outcomes across individuals. As discussed in detail below, both genetic variants in candidate genes and polygenic risk profiles may influence key molecular and cellular pathways involved in oxidative stress regulation, xenobiotic metabolism and detoxification, hormone signaling, and lipid homeostasis, thereby modulating the cardiovascular effects of EDCs. Although the available evidence remains limited, emerging studies suggest that genetic variability may contribute to interindividual differences in susceptibility to EDC-induced CVD and related cardiometabolic risk factors.
The following paragraphs and Table 1 summarize the main findings currently available in terms of GxE in cardiovascular field.
3.1. Bisphenols
To date, only one study has directly examined the association between genetic polymorphisms and bisphenol-induced CVD: a case-control study conducted by Jiang et al. in 439 pairs of hypertensive-normotensive subjects showed that polymorphisms in genes involved in oxidative stress pathway, such as CAT rs769214 and rs4755374 (especially AC+CC genotype), eNOS rs1799983, and gene encoding for estrogen receptor 2, ESR2 rs1256049, are associated with increased hypertension risk in relation to BPA exposure [22]. In particular, CAT encodes catalase, a major antioxidant enzyme involved in the maintenance of cellular redox balance, whereas eNOS regulates nitric oxide production and endothelial vascular homeostasis; therefore, alterations in these pathways exacerbate oxidative stress and endothelial dysfunction, two key mechanisms underlying BPA-induced cardiovascular damage.
However, polymorphisms may also indirectly impact cardiovascular risk induced by bisphenols, by promoting intermediate risk factors, such as obesity. Indeed, a polymorphism in the leptin receptor gene (LEPR rs9436303, G allele), which plays a crucial role in satiety regulation, resulted associated with increased body mass index in a population of adolescents and young adults (16-24 years), with a stronger effect in combination with high dietary bisphenol exposure [60]. In children (3-12 years), genetic variability in phase I and II metabolizing enzymes CYP2C19 (rs4244285 G/A) and GSTP1 (rs1695 A/G) has been associated with a twofold increased risk of overweight and obesity under conditions of long-term bisphenol exposure, although these associations showed borderline statistical significance. In the same study, the INSIG2 rs7566605 C/G polymorphism, involved in lipid metabolism, was significantly associated with an almost threefold increased risk of overweight in subjects with short-term bisphenol exposure [61].
3.2. Phthalates
GxE involinh phthalate exposure and cardiovascular risk remains largely unexplored, with the exception of a case-control study conducted by Wang et al. This study is particularly relevant, as sheds light on the association between maternal exposure to these toxicants during the periconceptional period and the risk of congenital heart disease in offspring, particularly septal defects in the presence of genetic variants in the ABCB1 gene. This gene is essential for detoxification, since it encodes for P-glycoprotein (P-gp), the most abundant transporter in the human placenta, which actively effluzes xenobiotics out of cells. Notably, the study found that, although the T allele represents the polymorphic variant of ABCB1 C3435T, increased susceptibility to congenital heart disease associated with maternal exposure to phthalates and alkylphenolic compounds (other EDCs), was observed in C allele carriers. Such effect may be explained by the lower ABCB1/P-gp expression observed in these individuals [62].
3.3. Per- and Polyfluoroalkyl Substances
In the case of PFAS exposure, only one study has reported significant findings in terms of GxE. In a cohort of 504 pregnant women, Kobayashi et al. demonstrated that maternal PFOS exposure significantly interacts with PPARGC1A (rs8192678) and PPARD (rs1053049, rs2267668) polymorphisms to alter circulating fatty acid profiles, particularly by reducing palmitic acid levels, thereby indicating a gene-dependent effect of PFOS on lipid metabolism [63]. Given the central role of PPARGC1A in oxidative stress responses [64] and of PPARD in fatty acid oxidation and lipid homeostasis [65], along with the well-established between circulating fatty acids and CVD risk [66], these interactions may contribute to PFAS-related cardiovascular effects.
3.4. Per- and Polyfluoroalkyl Substances
To date, only two studies have investigated GxE related to PCB exposure and CVD-related conditions. Both studies based their analysis on the definition of polygenic risk scores (PRSs), rather than on individual polymorphisms, and examined their effects in the context of dysglicemia and dyslipidemia, well-established conditions linked to cardiovascular risk [67,68]. The first study, conducted by Tan et al. in 2676 participants from the Wuhan-Zhuhai cohort, applied a PRS constructed from 96 T2D-associated genetic variants. The authors reported a positive interaction between PCB-118 exposure and a high PRS, which was associated with increased fasting plasma glucose and a higher risk of developing T2D over a 6-year follow-up. These findings suggest that genetic predisposition may amplify the adverse effects of PCB exposure on glucose metabolism [69]. Using the same cohort, a PRS for dyslipidemia was subsequently developed. Individuals with a higher genetic predisposition exhibited an increased risk of hypercholesterolemia and hypertriglyceridemia when exposed to PCBs, further supporting the role of genetic background in modulating susceptibility to PCB-related metabolic disturbances [70].
3.5. Polybrominated Diphenyl Ethers
Evidence on G×E involving PBDEs remains scarce, with only one study currently available. In a recent investigation conducted by Hu et al. in a population of 871 participants, 3,571 genetic variants were identified as interacting with PBDE exposure to influence dyslipidemia risk. Among those, the FTO gene rs9869609 G allele showed a stronger correlation with hypercholesterolemia, especially in the context of PBDE-47 exposure. Notably, the authors provided mechanistic insight by demonstrating that this SNP enhances the binding affinity of the BHLHE40 transcription factor, leading to downregulation of SLC6A20 gene expression, a gene encoding a glycine transporter, and, consequently, increased cholesterol accumulation [71].
3.6. Dioxins
To date, no specific SNPs have been identified as genetic modifiers of the cardiovascular effects of dioxins or of dioxin-related cardiovascular risk factors. As a result, the potential contribution of genetic susceptibility to interindividual variability in cardiovascular responses to dioxin exposure remains largely unexplored.
3.7. Polycyclic Aromatic Hydrocarbons
Evidence of GxE involving PAHs and cardiovascular risk factors is currently limited to three studies. In the study of Fernández-Macías et al. in a population of women, the T allele rs1801133 polymorphism of MTHFR gene, encoding an enzyme involved in the metabolism of folates, was found to significantly interact with exposure to PAHs with remarkable effects on cardiovascular risk markers. Specifically, higher levels of asymmetric dimethylarginine (ADMA), a marker of endothelial dysfunction, and an increased atherogenic index of plasma were observed in carriers of this variant, with even greater elevations in the presence of high PAH exposure [19]. Similarly, a significant interaction has been reported between PAH exposure and the PON1 gene rs662 polymorphism (G allele), also associated with increased ADMA levels. PON1 encodes an antioxidant enzyme that prevents low-density lipoprotein (LDL) oxidation and thus protects against atherosclerosis; the coding-region polymorphism leads to an amino acid substitution that reduces enzymatic activity, potentially increasing cardiovascular risk [20]. The third study, based on data from the analysis of Wuhan-Zhuhai cohort employed a lipid-specific PRS. Individuals with a high PRS, when combined with elevated PAH exposure, exhibited increased levels of LDL-cholesterol, further supporting the role of genetic susceptibility in modulating PAH-related cardiometabolic risk [72].
4. Conclusions and Emerging Perspectives
Accumulating evidence suugests that exposure to EDCs may contribute significantly to CVD development through complex biological mechanisms. Human biomonitoring studies have consistently demonstrated widespread exposure to PFAS, PCBs, PBDEs, PAHs, dioxins, phthalates, and bisphenols across populations, supporting growing concerns regarding their long-term cardiovascular consequences.
Importantly, interindividual variability in susceptibility to EDC-related cardiovascular effects cannot be explained solely by differences in exposure levels. Emerging evidence strongly suggests that genetic polymorphisms in pathways involved in oxidative stress responses, metabolism and xenobiotic detoxification, hormone signaling, and lipid homeostasis, may substantially modify cardiovascular responses to EDC exposure. Variants in these genes appear to influence the biological handling of environmental contaminants and the downstream activation of pathogenic pathways associated with cardiometabolic disease.
Specifically, variants in genes involved in antioxidant response, such as CAT, eNOS, and PON1, are associated with higher hypertension risk and enhanced vascular dysfunction under EDC exposure, particularly for bisphenols and PAHs. In parallel, variants in metabolism and detoxification-related genes, such as GSTP1, CYP2C19, ABCB1, and MTHFR appear to modulate susceptibility to cardiometabolic alterations and congenital heart defects under exposure to bisphenols, phthalates, and PAHs. Similarly, polymorphisms affecting lipid and metabolic homeostasis, including ESR2, FTO, LEPR, and INSIG2, are linked to hypertension, obesity, and dyslipidemia following exposure to PFAS, PBDEs, and bisphenols. Multiple genetic variants may affect susceptibility to hyperglycemia and hypercholesterolemia induced by PCBs. Conversely, no evidence has emerged from our analysis related to polymorphisms as modifiers of cardiovascular risk induced by dioxins.
Notably, all the considered studies of gene-environment interaction link EDCs exposure to an adverse cardiovascular outcome, except for the study of Kobayashi et al., where polymorphisms in PPARGC1A and PPARD genes decrease circulating fatty acids under PFAS exposure, effect that may lead to a reduced cardiovascular risk.
Although current findings are promising, the available evidence remains fragmented and is frequently limited by small sample sizes, heterogeneous study designs, differences in exposure assessment, variability in outcome definitions, and insufficient consideration of chemical mixtures. The reproducibility of several reported associations across independent populations also remains limited, while the extensive use of multiple-testing approaches may increase the likelihood of false-positive findings. In addition, potential publication bias toward statistically significant associations should be considered. These methodological limitations are further compounded by the fact that many studies have focused on single EDCs or individual polymorphisms, despite real-world exposure scenarios involving complex mixtures of contaminants interacting simultaneously with multiple genetic variants. Moreover, functional validation is still lacking for several identified susceptibility polymorphisms, limiting the ability to confirm the biological plausibility and mechanistic relevance of the observed associations. Finally, the lack of longitudinal studies integrating exposomic, genomic, and clinical data further weakens causal inference. Importantly, our literature review also identified emerging evidence adopting a broader approach based on polygenic risk scores, in which numerous susceptibility-associated polymorphisms were collectively evaluated in relation to the investigated disorder.
In line with these considerations, further research should prioritize large-scale prospective studies integrating human biomonitoring data with comprehensive genomic, transcriptomic, epigenetic, and metabolomic analyses. Particular attention should be devoted to GxE interactions during vulnerable developmental windows, including prenatal and early-life exposure. In addition, investigating the combined effects of multiple EDCs using mixture-based analytical approaches may better reflect real environmental exposure conditions and improve risk prediction models.
Another important perspective concerns the integration of precision medicine and environmental cardiology. Identifying individual genetic profiles associated with increased vulnerability to EDC exposure could contribute to personalized prevention strategies, early cardiovascular risk stratification, and targeted public health interventions. In this context, induced pluripotent stem cell-derived endothelial cells (iPSC-ECs) represent an innovative and promising experimental model for studying the vascular effects of environmental contaminants. Because iPSC-ECs retain the genetic background of the donor, they offer a unique opportunity to investigate how individual genetic susceptibility influences endothelial responses to EDC exposure [73]. These models may help clarify the molecular mechanisms underlying GxE interactions, including oxidative stress, inflammation, endothelial dysfunction, and altered vascular signaling pathways. Furthermore, iPSC-EC-based platforms could support the identification of early biomarkers of vascular damage and improve the development of personalized preventive and therapeutic strategies in environmental cardiology.
In conclusion, a deeper understanding of the interplay between environmental exposures and genetic susceptibility will be fundamental for advancing preventive cardiology and addressing the growing impact of environmental pollutants on cardiovascular health.
Author Contributions
Conceptualization, F.G. and A.B.; methodology, F.G. and A.B.; writing—original draft preparation, M.P., F.G. and A.B.; writing—review and editing, M.P., F.G., L.S., F.M. and A.B.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Acknowledgments
During the preparation of this manuscript, the authors used Microsoft Copilot 365, GPT 5 for the purposes of English editing. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABCB1 | ATP Binding Cassette Subfamily B Member 1 |
| ADMA | Asymmetric Dimethylarginine |
| AhR | Aryl Hydrocarbon Receptor |
| AIP | Atherogenic Index of Plasma |
| BDE | Brominated Diphenyl Ether |
| BFRs | Brominated Flame Retardants |
| BHLHE40 | Basic Helix-Loop-Helix Family Member E40 |
| BMI | Body Mass Index |
| BPA | Bisphenol A |
| CAT | Catalase |
| CI | Confidence Interval |
| CYP | Cytochrome P450 |
| CVD | Cardiovascular Disease |
| DOHaD | Developmental Origins of Health and Disease |
| EDC | Endocrine-Disrupting Chemical |
| eNOS | Endothelial Nitric Oxide Synthase |
| ESR | Estrogen Receptor |
| GST | Glutathione S-Transferase |
| GxE | Gene–Environment Interaction |
| HBM | Human Biomonitoring |
| INSIG2 | Insulin Induced Gene 2 |
| iPSC-ECs | Induced Pluripotent Stem Cell-Derived Endothelial Cells |
| LDL | Low-Density Lipoprotein |
| LDL-C | Low-Density Lipoprotein Cholesterol |
| LEPR | Leptin Receptor |
| MBzP | Monobenzyl Phthalate |
| MECPP | Mono-2-Ethyl-5-Carboxypentyl Phthalate |
| MEOHP | Mono-(2-Ethyl-5-Oxohexyl) Phthalate |
| MnBP | Mono-n-Butyl Phthalate |
| MTHFR | Methylenetetrahydrofolate Reductase |
| NHANES | National Health and Nutrition Examination Survey |
| OR | Odds Ratio |
| PAH | Polycyclic Aromatic Hydrocarbon |
| PBDE | Polybrominated Diphenyl Ether |
| PCB | Polychlorinated Biphenyl |
| PCDDs | Polychlorinated Dibenzo-p-Dioxins |
| PCDFs | Polychlorinated Dibenzofurans |
| PFAS | Per- and Polyfluoroalkyl Substances |
| PFHxS | Perfluorohexanesulfonic Acid |
| PFOA | Perfluorooctanoic Acid |
| PFOS | Perfluorooctane Sulfonic Acid |
| P-gp | P-Glycoprotein |
| POP | Persistent Organic Pollutant |
| PPARD | Peroxisome Proliferator-Activated Receptor Delta |
| PPARG | Peroxisome Proliferator-Activated Receptor Gamma |
| PPARGC1A | PPARG Coactivator 1 Alpha |
| PRS | Polygenic Risk Score |
| RR | Relative Risk |
| SLC6A20 | Solute Carrier Family 6 Member 20 |
| SNP | Single-Nucleotide Polymorphism |
| T2D | Type 2 Diabetes |
| TCDD | 2,3,7,8-Tetrachlorodibenzo-p-Dioxin |
| TC | Total Cholesterol |
| TG | Triglycerides |
References
- WHO; World Health Organization. Global assessment on the state of the science of endocrine disruptors. 2002. Available online: https://www.who.int/publications/i/item/WHO-PSC-EDC-02.2 (accessed on 12 April 2026).
- Klingelhöfer, D.; Braun, M.; Dröge, J.; Brüggmann, D.; Groneberg, D.A. Global research on endocrine disruptors as emerging hazards for human health and the environment. Front Endocrinol. . 2025, 16, 1561711. [Google Scholar] [CrossRef]
- Chen, J.; Song, P.; Li, C.; Liu, H.; Zhang, L.; Zhou, Y.; Zhou, Z.; Yan, W. Endocrine disrupting chemicals exposure and health: An umbrella review. Ecotoxicol. Env. Saf. 2025, 302, 118574. [Google Scholar] [CrossRef]
- Assenza, M.R.; Gaggi, G.; Di Credico, A.; Ghinassi, B.; Barbagallo, F. The effect of endocrine disruptors on the cardiovascular system: does sex matter? Env. Res. 2025, 277, 121612. [Google Scholar] [CrossRef] [PubMed]
- Macedo, S.; Teixeira, E.; Gaspar, T.B.; Boaventura, P.; Soares, M.A.; Miranda-Alves, L.; Soares, P. Endocrine-disrupting chemicals and endocrine neoplasia: A forty-year systematic review. Env. Res. 2023, 218, 114869. [Google Scholar] [CrossRef]
- Yan, Y.; Guo, F.; Liu, K.; Ding, R.; Wang, Y. The effect of endocrine-disrupting chemicals on placental development. Front Endocrinol. 2023, 14, 1059854. [Google Scholar] [CrossRef] [PubMed]
- Stanmore, B.R. The formation of dioxins in combustion systems. Combust. Flame 2004, 136, 398–427. [Google Scholar] [CrossRef]
- Endocrine Society. Endocrine-Disrupting Chemicals. 2025. Available online: https://www.endocrine.org/advocacy/position-statements/endocrine-disrupting-chemicals (accessed on 12 April 2025).
- WHO; World Health Organization. State of the science of endocrine disrupting chemicals 2012. 2012. Available online: https://www.who.int/publications/i/item/state-of-the-science-of-endocrine-disrupting-chemicals (accessed on 12 April 2025).
- Gore, A.C.; Chappell, V.A.; Fenton, S.E.; Flaws, J.A.; Nadal, A.; Prins, G.S.; Toppari, J.; Zoeller, R.T. EDC-2: The Endocrine Society’s Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocr. Rev. 2015, 36, E1–E150. [Google Scholar] [CrossRef]
- Philips, E.M.; Jaddoe, V.W.V.; Trasande, L. Effects of early exposure to phthalates and bisphenols on cardiometabolic outcomes in pregnancy and childhood. Reprod. Toxicol. 2017, 68, 105–118. [Google Scholar] [CrossRef]
- Chong, B.; Jayabaskaran, J.; Jauhari, S.M.; Chan, S.P.; Goh, R.; Kueh, M.T.W.; Li, H.; Chin, Y.H.; Kong, G.; et al. Global burden of cardiovascular diseases: projections from 2025 to 2050. Eur. J. Prev. Cardiol. 2025, 32, 1001–1015. [Google Scholar] [CrossRef]
- Global Burden of Cardiovascular Diseases and Risks 2023 Collaborators. Global, Regional, and National Burden of Cardiovascular Diseases and Risk Factors in 204 Countries and Territories, 1990-2023. J. Am. Coll. Cardiol. 2025, 86, 2167–2243.
- Ma, C.X.; Ma, X.N.; Li, H.L.; Mauricio, D.; Fu, S.B. Endocrine-disrupting chemicals exposure: cardiometabolic health risk in humans. Cardiovasc Diabetol. 2025, 24, 381. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Bing, S.; Qiu, H.; Wang, S.; Zhang, Y. Association Between Mixed Exposure to Endocrine-Disrupting Chemicals and Cardiovascular Health: Results from the 2003-2016 NHANES. Cardiovasc Toxicol. 2025, 26, 7. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Shan, Z.; Luo, C.; Kang, C.; Yang, Y.; He, P.; Li, S.; Chen, L.; Jiang, X.; Liu, L. Glutathione S-Transferase T1 (GSTT1) Null Polymorphism, Smoking, and Their Interaction in Coronary Heart Disease: A Comprehensive Meta-Analysis. Heart Lung Circ. 2017, 26, 362–370. [Google Scholar] [CrossRef]
- Song, Y.; Shan, Z.; Liu, X.; Chen, X.; Luo, C.; Chen, L.; Wang, Y.; Gong, L.; Liu, L.; Liang, J. An updated meta-analysis showed smoking modify the association of GSTM1 null genotype on the risk of coronary heart disease. Biosci. Rep. 2021, 41, BSR20200490. [Google Scholar] [CrossRef]
- Kobayashi, S.; Sata, F.; Sasaki, S.; Ban, S.; Miyashita, C.; Okada, E.; Limpar, M.; Yoshioka, E.; Kajiwara, J.; Todaka, T.; et al. Genetic association of aromatic hydrocarbon receptor (AHR) and cytochrome P450, family 1, subfamily A, polypeptide 1 (CYP1A1) polymorphisms with dioxin blood concentrations among pregnant Japanese women. Toxicol. Lett. 2013, 219, 269–728. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Macías, J.C.; Ochoa-Martínez, A.C.; Pérez-López, A.A.; Pérez-López, A.L.; Neri-Maldonado, I.; Piña-López, I.G.; Pérez-Maldonado, I.N. The interplay between exposure to PAHs and MTHFR C677T polymorphism on cardiovascular risk biomarkers in Mexican women. Env. Sci. Pollut. Res. Int. 2022, 29, 48466–48476. [Google Scholar] [CrossRef]
- Ochoa-Martínez, Á.C.; Ruíz-Vera, T.; Almendarez-Reyna, C.I.; Orta-García, S.T.; Pérez-Maldonado, I.N. Influence on serum asymmetric dimethylarginine (ADMA) concentrations of human paraoxonase 1 polymorphism (Q192R) and exposure to polycyclic aromatic hydrocarbons (PAHs) in Mexican women, a gene-environment interaction. Chemosphere. 2017, 186, 770–779. [Google Scholar] [CrossRef]
- Yan, C.; Fang, N.; Gong, Y. Evaluation of the causal effects of PFOS on atherosclerosis and its potential toxicological mechanisms: Integrated Mendelian randomization and network toxicology analysis. Ecotoxicol. Env. Saf. 2026, 309, 119618. [Google Scholar] [CrossRef]
- Jiang, S.; Yang, G.; Zhou, S.; Zhang, X.; Peng, C.; Lu, Q. Bisphenol A, S, and F exposure, ESR1/2, CAT, and eNOS genetic polymorphisms, and the risk of hypertension. Ecotoxicol. Env. Saf. 2021, 224, 112684. [Google Scholar] [CrossRef]
- Wee, S.Y.; Aris, A.Z.; Yusoff, F.M.; Praveena, S.M. Public perception on human exposure risk: A case study on endocrine disrupting compounds in the environment. Ecotoxicol. Env. Saf. 2024, 270, 115830. [Google Scholar] [CrossRef]
- Chatziioannou, A.C.; Myridakis, A.; Stephanou, E.G. Biomonitoring of Environmental Phenols, Phthalate Metabolites, Triclosan, and Per- and Polyfluoroalkyl Substances in Humans with Chromatography and Mass Spectrometry. Toxics 2025, 13, 1029. [Google Scholar] [CrossRef] [PubMed]
- Louro, H.; Heinälä, M.; Bessems, J.; Buekers, J.; Vermeire, T.; Woutersen, M.; van Engelen, J.; Borges, T.; Rousselle, C.; Ougier, E.; et al. Human biomonitoring in health risk assessment in Europe: Current practices and recommendations for the future. Int. J. Hyg. Env. Health 2019, 222, 727–737. [Google Scholar] [CrossRef]
- Faniband, M.; Lindh, C.H.; Jönsson, B.A. Human biological monitoring of suspected endocrine-disrupting compounds. Asian J. Androl. 2014, 16, 5–16. [Google Scholar] [CrossRef]
- Calafat, A.M. Contemporary Issues in Exposure Assessment Using Biomonitoring. Curr. Epidemiol. Rep. 2016, 3, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.; Xu, J.; Zhang, R.; Yu, J. The association between environmental endocrine disruptors and cardiovascular diseases: A systematic review and meta-analysis. Env. Res. 2020, 187, 109464. [Google Scholar] [CrossRef]
- Intelligence, Mondor. Bisphenol A (Bpa) Market Size & Share Analysis - Growth Trends And Forecast (2026 - 2031). Available online: https://www.mordorintelligence.com/industry-reports/bisphenol-a-bpa-market (accessed on 16 April 2026).
- Dunder, L.; Lejonklou, M.H.; Lind, P.M.; Lind, L. Urinary bisphenol A and serum lipids: a meta-analysis of six NHANES examination cycles (2003-2014). J. Epidemiol. Community Health 2019, 73, 1012–1019. [Google Scholar] [CrossRef]
- Stahlhut, R.W.; Welshons, W.V.; Swan, S.H. Bisphenol A data in NHANES suggest longer than expected half-life, substantial nonfood exposure, or both. Env. Health Perspect. 2009, 117, 784–789. [Google Scholar] [CrossRef]
- Chen, Z.; He, J.; Shim, W. Association between urinary environmental phenols and the prevalence of cardiovascular diseases in US adults. Env. Sci. Pollut. Res. Int. 2022, 29, 42947–42954. [Google Scholar] [CrossRef]
- Yin, T.; Zhu, X.; Cheang, I.; Zhou, Y.; Liao, S.; Lu, X.; Zhou, Y.; Yao, W.; Li, X.; Zhang, H. Urinary phenols and parabens metabolites associated with cardiovascular disease among adults in the United States. Env. Sci. Pollut. Res. Int. 2023, 30, 25093–25102. [Google Scholar] [CrossRef]
- Gorini, F.; Tonacci, A.; Palazzo, M.; Borghini, A. From Exposure to Atherosclerosis: Mechanistic Insights into Phthalate-Driven Ischemic Heart Disease and Prevention Strategies. Life . 2026, 16, 327. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Zhu, H.; Sun, X.; Zhang, J.; Lin, M.; Sun, P. The association between exposure to phthalates and cardiovascular disease: A comprehensive study utilizing NHANES data from 2005 to 2018 and network toxicology. Chem. Biol. Interact. 2025, 420, 111651. [Google Scholar] [CrossRef] [PubMed]
- Dunder, L.; Salihovic, S.; Varotsis, G.; Lind, P.M.; Elmståhl, S.; Lind, L. Plasma levels of per- and polyfluoroalkyl substances (PFAS) and cardiovascular disease - Results from two independent population-based cohorts and a meta-analysis. Env. Int. 2023, 181, 108250. [Google Scholar] [CrossRef]
- DeLuca, N.M.; Minucci, J.M.; Mullikin, A.; Slover, R.; Cohen Hubal, E.A. Human exposure pathways to poly- and perfluoroalkyl substances (PFAS) from indoor media: A systematic review. Env. Int. 2022, 162, 107149. [Google Scholar] [CrossRef]
- Tokranov, A.K.; Hopkins, Z.R.; Lindsey, B.D.; Jurgens, B.C. PFAS Are Widespread, Not Ubiquitous: Clarifying Misconceptions About the Prevalence of “Forever Chemicals”. Env. Sci. Technol. 2025, 59, 11947–11949. [Google Scholar] [CrossRef] [PubMed]
- Connolly, J.C.; Ishihara, Y.; Sawaya, E.; Whitfield, V.; Garrity, N.; Sohata, R.; Tsymbal, M.; Lundberg, A.; La Merrill, M.A.; DeWitt, J.C.; et al. Per- and Polyfluoroalkyl Substances (PFAS) Enhance Cholesterol Accumulation and Dysregulate Inflammatory Responses in Macrophages. Cardiovasc Toxicol. 2025, 25, 1455–1470. [Google Scholar] [CrossRef]
- Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; Del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.R.; Leblanc, J.C.; et al.; EFSA Panel on Contaminants in the Food Chain (EFSA CONTAM Panel) Risk to human health related to the presence of perfluoroalkyl substances in food. EFSA J. 2020, 18, e06223. [Google Scholar] [CrossRef]
- Martínez, A. Toxicity of persistent organic pollutants: a theoretical study. J. Mol. Model. 2024, 30, 97. [Google Scholar] [CrossRef]
- Herbstman; J, B.; Mall, J.K. Developmental Exposure to Polybrominated Diphenyl Ethers and Neurodevelopment. Curr. Env. Health Rep. 2014, 1, 101–112. [Google Scholar] [CrossRef]
- Weitekamp, C.A.; Phillips, L.J.; Carlson, L.M.; DeLuca, N.M.; Cohen Hubal, E.A.; Lehmann, G.M. A state-of-the-science review of polychlorinated biphenyl exposures at background levels: relative contributions of exposure routes. Sci. Total Environ. 2021, 776, 145912. [Google Scholar] [CrossRef]
- Vorkamp, K. An overlooked environmental issue? A review of the inadvertent formation of PCB-11 and other PCB congeners and their occurrence in consumer products and in the environment. Sci. Total Environ. 2016, 541, 1463–1476. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.; Li, Z.; Jones, K.C.; Zhu, Y. Effects of global treaties on commercial chemicals widely used as additives: a meta-analysis of historical measurements of polybrominated diphenyl ethers. Lancet Planet Health 2025, 9, e538–e552. [Google Scholar] [CrossRef]
- Liu, J.; Shan, Q.; Yang, Y.; He, W. Uncovering the Potential Link Between Polychlorinated Biphenyls and Cardiovascular Diseases: A Comprehensive Analysis. Toxics 2025, 13, 71. [Google Scholar] [CrossRef] [PubMed]
- Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; Del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Ron Hoogenboom, L.; Leblanc, J.C.; et al.; EFSA Panel on Contaminants in the Food Chain (CONTAM) Update of the risk assessment of polybrominated diphenyl ethers (PBDEs) in food. EFSA J. 2024, 22, e8497. [Google Scholar] [CrossRef]
- Yin, W.; Xu, R.; Zou, J.; Wang, Y.; Zhang, Y. Single and combined association between brominated flame retardants and cardiovascular disease: a large-scale cross-sectional study. Front Public Health 2024, 12, 1357052. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Z.; Shen, N.; Qi, X.; Li, H.; Wu, F.; Zhu, Z.; Liu, J.; Xiang, H. Association between exposure to brominated flame retardants (BFRs) and blood lipid profiles in American adults: a cross-sectional study. Lipids Health Dis. 2025, 24, 120. [Google Scholar] [CrossRef]
- Humblet, O.; Birnbaum, L.; Rimm, E.; Mittleman, M.A.; Hauser, R. Dioxins and cardiovascular disease mortality. Env. Health Perspect. 2008, 116, 1443–1448. [Google Scholar] [CrossRef]
- Liang, Y.; Tang, Z.; Jiang, Y.; Ai, C.; Peng, J.; Liu, Y.; Chen, J.; Zhang, J.; Cai, Z. Serum metabolic changes associated with dioxin exposure in a Chinese male cohort. Env. Int. 2020, 143, 105984. [Google Scholar] [CrossRef]
- US EPA; United States Environmental Protection Agency. Learn about dioxin. 2025. Available online: https://www.epa.gov/dioxin/learn-about-dioxin (accessed on 18 April 2026).
- Akinyemi, B.; Obeng-Gyasi, E. Combined Effects of Metals, PCBs, Dioxins, and Furans on Cardiovascular Dysfunction. J. Xenobiot. 2025, 15, 94. [Google Scholar] [CrossRef]
- Mirzababaei, A.; Daneshzad, E.; Moradi, S.; Abaj, F.; Mehranfar, S.; Asbaghi, O.; Clark, C.C.T.; Mirzaei, K. The association between urinary metabolites of polycyclic aromatic hydrocarbons (PAHs) and cardiovascular diseases and blood pressure: a systematic review and meta-analysis of observational studies. Env. Sci. Pollut. Res. Int. 2022, 29, 1712–1728. [Google Scholar] [CrossRef]
- Gao, P.; da Silva, E.; Hou, L.; Denslow, N.D.; Xiang, P.; Ma, L.Q. Human exposure to polycyclic aromatic hydrocarbons: Metabolomics perspective. Env. Int. 2018, 119, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Mallah, M.A.; Mallah, M.A.; Liu, Y.; Xi, H.; Wang, W.; Feng, F.; Zhang, Q. Relationship Between Polycyclic Aromatic Hydrocarbons and Cardiovascular Diseases: A Systematic Review. Front Public Health 2021, 9, 763706. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Guo, C.; Li, Q.; Zhong, Y.; Ma, S.; Zhou, J.; Li, X.; Huang, R.; Yu, Y. Human health risks estimations from polycyclic aromatic hydrocarbons in serum and their hydroxylated metabolites in paired urine samples. Env. Pollut. 2021, 290, 117975. [Google Scholar] [CrossRef]
- Kosnik, M.B.; Enroth, S.; Karlsson, O. Distinct genetic regions are associated with differential population susceptibility to chemical exposures. Environ. Int. 2021, 152, 106488. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, M.; Borghini, A.; Bustaffa, E.; Baldacci, S.; Gorini, F.; Minichilli, F. Genetic polymorphisms as modifiers of health risks from exposure to toxic elements: a traditional literature review. Toxics 2026, 14, 375. [Google Scholar] [CrossRef]
- Ramírez, V.; Robles-Aguilera, V.; Salcedo-Bellido, I.; Gálvez-Ontiveros, Y.; Rodrigo, L.; Martinez-Gonzalez, L.J.; Monteagudo, C.; Álvarez-Cubero, M.J.; Rivas, A. Effects of genetic polymorphisms in body mass index according to dietary exposure to bisphenols and parabens. Chemosphere 2022, 293, 133421. [Google Scholar] [CrossRef]
- Ramírez, V.; Gálvez-Ontiveros, Y.; de Bobadilla, V.A.F.; González-Palacios, P.; Salcedo-Bellido, I.; Samaniego-Sánchez, C.; Álvarez-Cubero, M.J.; Martínez-González, L.J.; Zafra-Gómez, A.; Rivas, A. Exploring the role of genetic variability and exposure to bisphenols and parabens on excess body weight in Spanish children. Ecotoxicol. Environ. Saf. 2024, 286, 117206. [Google Scholar] [CrossRef]
- Wang, C.; Xie, L.; Zhou, K.; Zhan, Y.; Li, Y.; Li, H.; Qiao, L.; Wang, F.; Hua, Y. Increased risk for congenital heart defects in children carrying the ABCB1 gene C3435T polymorphism and maternal periconceptional toxicants exposure. PLoS ONE 2013, 8, e68807. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Sata, F.; Goudarzi, H.; Araki, A.; Miyashita, C.; Sasaki, S.; Okada, E.; Iwasaki, Y.; Nakajima, T.; Kishi, R. Associations among Perfluorooctanesulfonic/Perfluorooctanoic Acid Levels, Nuclear Receptor Gene Polymorphisms, and Lipid Levels in Pregnant Women in the Hokkaido Study. Sci. Rep. 2021, 11, 9994. [Google Scholar] [CrossRef]
- Kadlec, A.O.; Chabowski, D.S.; Ait-Aissa, K.; Gutterman, D.D. Role of PGC-1α in vascular regulation: implications for atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 1467–1474. [Google Scholar] [CrossRef]
- Montaigne, D.; Butruille, L.; Staels, B. PPAR control of metabolism and cardiovascular functions. Nat. Rev. Cardiol. 2021, 18, 809–823. [Google Scholar] [CrossRef]
- Shi, F.; Chowdhury, R.; Sofianopoulou, E.; Koulman, A.; Sun, L.; Steur, M.; Aleksandrova, K.; Dahm, C.C.; Schulze, M.B.; van der Schouw, Y.T.; Agnoli, C.; Amiano, P.; Boer, J.M.A.; Bork, C.S.; Cabrera-Castro, N.; Eichelmann, F.; Elbaz, A.; Farràs, M.; Heath, A.K.; Kaaks, R.; Kaptoge, S.; et al. Association of circulating fatty acids with cardiovascular disease risk: analysis of individual-level data in three large prospective cohorts and updated meta-analysis. Eur. J. Prev. Cardiol. 2025, 32, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Farkouh, M.E.; Newman, J.D.; Garvey, W.T. Cardiometabolic-based chronic disease, adiposity and dysglycemia drivers: JACC state-of-the-art review. J. Am. Coll. Cardiol. 2020, 75, 525–538. [Google Scholar] [CrossRef]
- Ference, B.A.; Graham, I.; Tokgozoglu, L.; Catapano, A.L. Impact of lipids on cardiovascular health: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 1141–1156. [Google Scholar] [CrossRef]
- Tan, Q.; Yang, S.; Wang, B.; Wang, M.; Yu, L.; Liang, R.; Liu, W.; Song, J.; Guo, Y.; Zhou, M.; Chen, W. Gene-environment interaction in long-term effects of polychlorinated biphenyls exposure on glucose homeostasis and type 2 diabetes: the modifying effects of genetic risk and lifestyle. J. Hazard. Mater. 2023, 457, 131757. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zhou, M.; Tan, Q.; Liang, R.; Guo, Y.; Wang, D.; Wang, B.; Xie, Y.; Yin, H.; Yang, S.; Shang, B.; You, X.; Cao, X.; Fan, L.; Ma, J.; Chen, W. Associations of polychlorinated biphenyls exposure, lifestyle, and genetic susceptibility with dyslipidemias: evidence from a general Chinese population. J. Hazard. Mater. 2024, 470, 134073. [Google Scholar] [CrossRef]
- Hu, N.; Li, B.; Lu, Y.; Jiang, Q.; Zhu, Y.; Li, Z.; Qu, Y.; Qiu, T.; Zhang, D.; Wang, Z.; Ma, Y.; Jin, H.; Sun, P.; Song, H.; Zhao, Y.; Zhao, Y.; Zhang, M.; Zhao, F.; Ji, S.; Yuan, B.; Shi, X.; et al. Genetic variations interact with polybrominated diphenyl ether exposure to alter lipid homeostasis. Nat. Commun. 2026, 17, 3529. [Google Scholar] [CrossRef]
- Ma, J.; Hao, X.; Nie, X.; Yang, S.; Zhou, M.; Wang, D.; Wang, B.; Cheng, M.; Ye, Z.; Xie, Y.; Wang, C.; Chen, W. Longitudinal relationships of polycyclic aromatic hydrocarbons exposure and genetic susceptibility with blood lipid profiles. Environ. Int. 2022, 164, 107259. [Google Scholar] [CrossRef]
- Fontanelli, L.; Castronovo, A.; Ferri, C.; Vozzi, F.; Recchia, F.A.; Borghini, A. iPSC-derived endothelial cells as experimental models for predictive and personalized strategies in cardiovascular and cerebrovascular disease. Int. J. Mol. Sci. 2026, 27, 780. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Human biomonitoring strategies for the assessment of major classes of endocrine-disrupting chemicals (EDCs) in biological matrices. The figure summarizes the main chemical classes of EDCs, including bisphenols, phthalates, per- and polyfluoroalkyl substances (PFAS), polychlorinated biphenyls (PCBs), polybrominated diphenyl ethers (PBDEs), dioxins, and polycyclic aromatic hydrocarbons (PAHs), together with their physicochemical properties, metabolic fate, and preferred biological matrices for exposure assessment. Persistent and lipophilic compounds, such as PFAS, PCBs/PBDEs, and dioxins, are primarily measured in blood, serum, or plasma because they bioaccumulate and reflect long-term exposure. In contrast, non-persistent and rapidly metabolized compounds, including bisphenols, phthalates, and PAH metabolites, are preferentially quantified in urine. Alternative matrices such as hair, saliva, semen, breast milk, and amniotic fluid may provide complementary exposure information in selected contexts. The figure also highlights the importance of repeated sampling or pooled specimens for accurately assessing exposure to non-persistent EDCs characterized by high intra-individual variability. Image generated with ChatGPT.
Figure 1.
Human biomonitoring strategies for the assessment of major classes of endocrine-disrupting chemicals (EDCs) in biological matrices. The figure summarizes the main chemical classes of EDCs, including bisphenols, phthalates, per- and polyfluoroalkyl substances (PFAS), polychlorinated biphenyls (PCBs), polybrominated diphenyl ethers (PBDEs), dioxins, and polycyclic aromatic hydrocarbons (PAHs), together with their physicochemical properties, metabolic fate, and preferred biological matrices for exposure assessment. Persistent and lipophilic compounds, such as PFAS, PCBs/PBDEs, and dioxins, are primarily measured in blood, serum, or plasma because they bioaccumulate and reflect long-term exposure. In contrast, non-persistent and rapidly metabolized compounds, including bisphenols, phthalates, and PAH metabolites, are preferentially quantified in urine. Alternative matrices such as hair, saliva, semen, breast milk, and amniotic fluid may provide complementary exposure information in selected contexts. The figure also highlights the importance of repeated sampling or pooled specimens for accurately assessing exposure to non-persistent EDCs characterized by high intra-individual variability. Image generated with ChatGPT.


Table 1.
Genetic polymorphisms modifying cardiovascular risk induced by EDCs. Circles in the “Effect column” are green when SNPs may be correlated with a protective action, red with increased cardiovascular risk.
Table 1.
Genetic polymorphisms modifying cardiovascular risk induced by EDCs. Circles in the “Effect column” are green when SNPs may be correlated with a protective action, red with increased cardiovascular risk.
| Effect | SNP | Gene | Pathway | Reference | EDC | |
|---|---|---|---|---|---|---|
 |
↑ hypertension risk | rs 4755374 C allele | CAT | Oxidative stress/antioxidant defense | [22] | Bisphenols |
|
↑ hypertension risk | rs769214 G/G | ||||
| rs1799983 G/G | eNOS | |||||
| rs1256049 C/C | ESR2 | Hormone signaling and lipid metabolism | ||||
|
↑ BMI | rs9436303 G allele | LEPR | Hormone signaling and lipid metabolism | [60] | |
|
2-fold ↑ risk of overweight and obesity | rs4244285 G/A | CYP2C19 | Metabolism and detoxification | [61] | |
| rs1695 A/G | GSTP1 | |||||
|
~ 3-fold ↑ risk of overweight | rs7566605 C/G | INSIG2 | Hormone signaling and lipid metabolism | ||
|
↑ congenital heart disease risk | rs1045642 C allele | ABCB1 | Metabolism and detoxification | [62] | Phthalates |
 |
↓ circulating fatty acids | rs 8192678 A allele | PPARGC1A | Oxidative stress/antioxidant defense | [63] | PFAS |
| rs1053049 C allele, rs2267668 G allele | PPARD | Hormone signaling and lipid metabolism | ||||
|
↑ fasting plasma glucose and risk of developing T2D | PRS | [69] | PCBs | ||
|
↑ risk of hyperTC, hyperTG, and hyperLDL-C | PRS | [70] | |||
|
↑ hypercholesterolemia risk | rs9869609 G allele | FTO | Hormone signaling and lipid metabolism | [71] | PBDEs |
| Not available | Dioxins | |||||
|
↑ ADMA and AIP | rs1801133 T allele | MTHFR | Metabolism and detoxification | [19] | PAHs |
|
↑ ADMA | rs662 G allele | PON1 | Oxidative stress/antioxidant defense | [20] | |
|
↑ LDL-C | Lipid-specific PRS | [72] | |||
Abbreviations: ↓: decrease of; ↑: increase of; ADMA: asymmetric dimethylarginine; AIP: atherogenic index of plasma; BMI: body mass index; EDC: endocrine-disrupting chemicals; LDL-C: low-density lipoprotein cholesterol; OR: odds ratio; PAHs: polycyclic aromatic hydrocarbons; PBDEs: polybrominated diphenyl ethers; PCBs: polychlorinated biphenyls; PFAS: per- and polyfluoroalkyl substances; PRS: polygenic risk score; SNP: single-nucleotide polymorphism; T2D: type 2 diabetes; TC: total cholesterol; TG: triglycerides.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



