Submitted:
26 May 2026
Posted:
27 May 2026
You are already at the latest version
Abstract
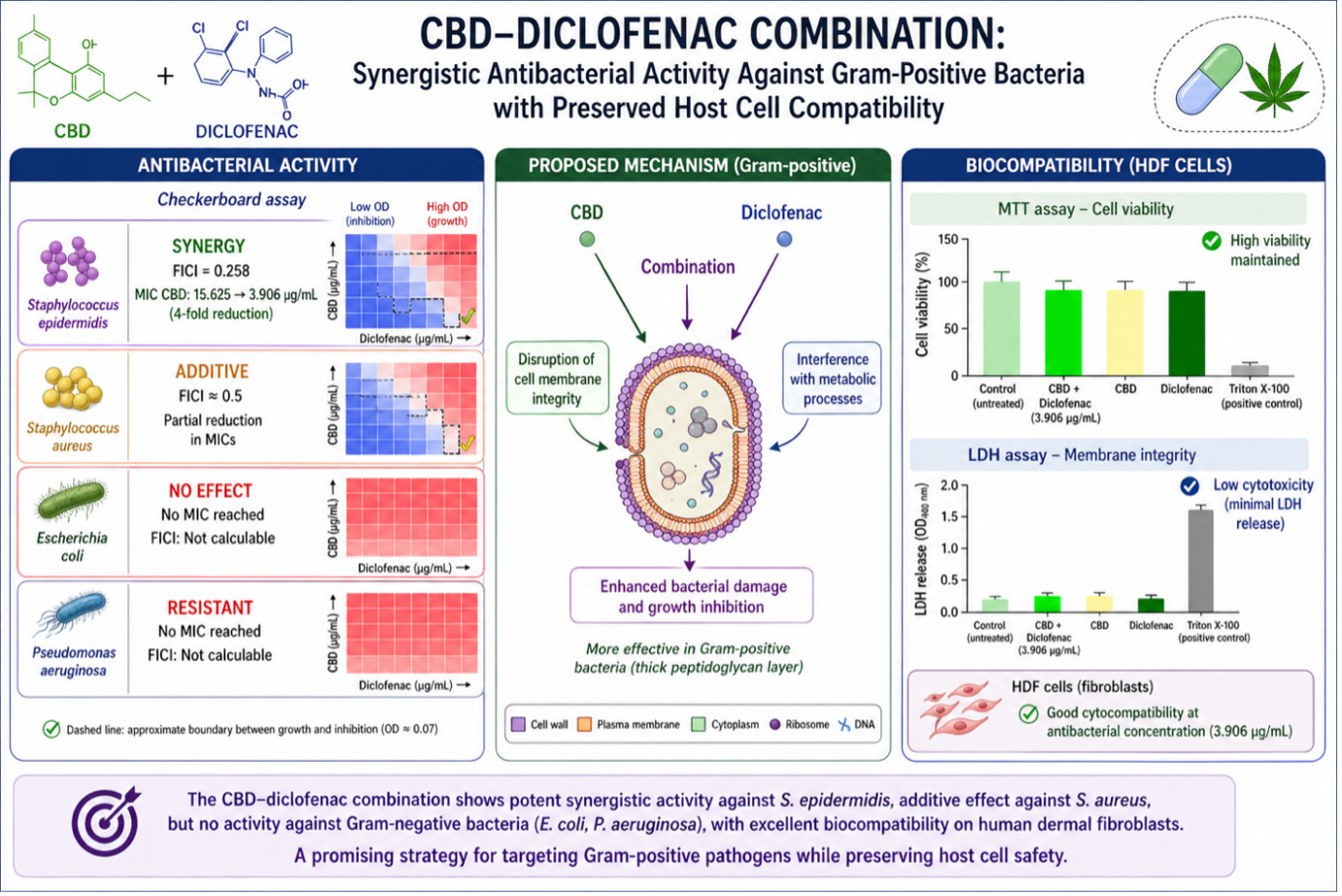
Antimicrobial resistance demands intensive research on new nonantibiotics and drug repurposing to expand the arsenal of antimicrobial agents. The present work analysed the combination of Diclofenac (DFNAC) and Cannabidiol (CBD) and evaluated its potentiation and its biocompatibility. The formulation's potency has been tested against Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa. The DFNAC-CBD formulation showed an evident synergistic effect, a significant decrease in the minimum inhibitory concentration against Staphylococcus epidermidis, and an additive effect against Staphylococcus aureus, indicating the levels of cooperation between the two compounds. The formulation exhibited no antibacterial activity against the Gram-negative strains such as Escherichia coli and Pseudomonas aeruginosa, explicable by their innate resistance and the formulation's ineffectiveness against the bacterial outer membrane. The results suggested that DFNAC may interfere with bacterial metabolic processes and CBD may disrupt bacterial membrane integrity. MTT and LDH assays demonstrated that the antibacterial concentration (3.906 µg/mL) preserves cell viability and membrane integrity. Live/Dead staining confirms cell viability and normal morphology. The results indicate that the DFNAC-CBD combination functions within a therapeutic window, achieving antimicrobial efficacy through complementary MOA and without inducing significant cytotoxicity. Therefore, the proposed combination has significant potential as a nonantibiotic formula to control the use and dosage of common antibiotics.
Keywords:
antimicrobial
; potentiation
; cannabidiol
; Diclofenac
; synergism
; personalised medicine
1. Introduction
Rapidly increasing antimicrobial resistance (AMR) is a significant challenge as bacteria evolve mechanisms to evade therapeutic agents, complicating the management of viral, bacterial, parasitic, and fungal diseases, jeopardising public health systems, exacerbating social inequalities, especially in resource-limited areas, impacting the health of animals and plants, and endangering food security [1]. Since AMR-related mortality is projected to rise to over 39 million between 2025 and 2050, the economic implications are enormous, with additional healthcare costs projected at US$1 trillion by 2050 and GDP losses up to US$3.4 trillion annually by 2030 [2,3]. The 2022 Global Antimicrobial Resistance and Use Surveillance System (GLASS) highlighted alarming levels of resistance among bacterial pathogens, including E. coli and Staphylococcus aureus [4]. Leveraging plants that produce secondary metabolites could provide innovative antibiotics to combat this resistance [5]. Thus, exploring natural products [6] and drug repurposing [7] could support the strategies to tackle the pressing threat of multidrug resistance. In this context, some of the FDA-approved nonantibiotic medication classes, including nonsteroidal anti-inflammatory drugs (NSAIDs), antidepressants, antiplatelets, antipsychotics, and statins, have antibacterial effects [8,9] against both Gram-positive and Gram-negative bacteria [10,11,12] and can play essential parts.
Diclofenac sodium (DFNAC), a potent nonsteroidal anti-inflammatory agent, also exhibits antibacterial activity [13] and has various applications [14]. DFNAC alone exhibited activity against drug-sensitive and drug-resistant clinical isolates of Staphylococcus aureus, Listeria monocytogenes, Escherichia coli, and Mycobacterium spp. [15]. Also, combined with streptomycin [15], curcumin [16], gentamicin or ampicillin [17], streptomycin [18] has potential for the management of problematic antibiotic-resistant Gram-positive and Gram-negative bacterial infections. Furthermore, DFNAC-kanamycin and DFNAC-tetracycline demonstrated additive interactions and promising control of the Escherichia coli and Staphylococcus aureus biofilms [19]. Notably, synergistic effects have been observed between DFNAC and echinocandin anidulafungin on the tested biofilms [20], DFNAC and Pelargonium graveolens against C. parapsilosis [21], and DFNAC and Colistin against Multidrug-Resistant Acinetobacter baumannii [22]. DFNAC, in combination with β-lactams, inhibits MRSA-associated biofilm formation on implants [23] and can be used in combination with antibiotics as an anti-virulence agent against MDR-MRSA [24]. However, no potentiation was observed when DFNAC was tested as an adjuvant to antibiotic therapy (cefuroxime, chloramphenicol) against 10 strains of S. aureus [25].
Meantime, the discovery of phyto-cannabinoids and the identification of their chemical structure, characterised by a lipid structure featuring alkyl-resorcinol and monoterpene moieties, led to the exploration of the endocannabinoid system as the main pharmacological target for cannabinoids [26,27]. Despite ongoing debates about the legal status of Cannabis, there is evidence for its useful therapeutic applications in modern medicine, from nausea [28], pain [29,30] Parkinson’s disease and multiple sclerosis-related symptoms [31,32], to sleep disorders [33] and antibacterial and antifilm activities against a broad spectrum of Gram-positive bacteria and some Gram-negative bacteria, including multidrug-resistant (MDR) strains [27,34]. Therefore, distinct Cannabis-derived molecules expand the repertoire of antibiotic-independent treatment options [35]. For instance, CBD-polymyxin B exerted an antimicrobial effect against E. coli [36], ultrapure CBD-polymyxin B showed potentiated antibacterial activity against Klebsiella pneumoniae, Escherichia coli, and Acinetobacter baumannii, including four antibiotic-resistant K. pneumoniae isolates [37], CBD-ampicillin and CBD-polymyxin B showed potential synergism on S. Typhimurium [38] and CBD-colistin on A. baumannii [27,34], and additive and/or synergistic effect against LOS-expressing Gram-negative diplococci; however, no potential synergism between CBD and kanamycin [27,34]. While some studies recognised CBD as a powerful, low-resistance-inducing antibiotic against Gram-positive bacteria, others expressed caution due to inconsistencies in bacterial sensitivity and limitations in treating Gram-negative infections [27,34,39] Since dosage is crucial when therapeutic windows are narrow, potentiation has been considered, and “drug repurposing” [11] leverages synergism with nonantibiotics to extend the spectrum.
The present work explored the combination of DFNAC and CBD and their potential as an alternative antibiotic-independent treatment and prevention strategy in the combat of bacterial infections caused by Staphylococcus epidermidis, Staphylococcus aureus, Escherichia coli and Pseudomonas aeruginosa. With acceptable biocompatibility and potentiation of antibiotic activity through complementary MOAs, the combination of DFNAC and CBD shows potential for further studies and targeted applications.
2. Results
The proposed formulation combining DFNAC and CBD has been evaluated for its antimicrobial effects against Gram-positive and Gram-negative bacteria representative as well as its biocompatibility.
2.1. The Antibacterial Activity of DFNAC and CBD Formulation
2.1.1. The Antimicrobial Effect Against Gram-Positive Bacteria
The antibacterial activity of CBD, DFNAC, and their combination was evaluated against Staphylococcus aureus and Staphylococcus epidermidis using broth microdilution and checkerboard assays (Figure 1).
For S. aureus, CBD alone exhibited antibacterial activity with a MIC of 3.906 µg/mL (Figure 1A), while DFNAC showed inhibitory effects only at high concentrations (MIC = 500 µg/mL; Figure 1B). The combination of CBD and DFNAC (Figure 1C) resulted in a modest improvement in antibacterial activity, reflected by reduced optical density values at lower concentrations. The checkerboard analysis (Figure 1G) confirmed an additive interaction, with a FICI value of approximately 0.5, indicating partial cooperation between the two compounds without true synergism.
In contrast, S. epidermidis displayed a different susceptibility profile. CBD alone showed a higher MIC (15.625 µg/mL; Figure 1D), while DFNAC again exhibited weak antibacterial activity (Figure 1E). However, the combination (Figure 1F) significantly enhanced bacterial inhibition, reducing the effective concentration required to achieve complete growth suppression. The checkerboard heatmap (Figure 1H) clearly demonstrates a shift toward lower OD values across combined concentrations, with the MIC of the combination identified at 3.906 µg/mL for both compounds. The calculated FICI value of 0.258 indicates a strong synergistic interaction, corresponding to a 4-fold reduction in the CBD MIC. These results highlight a strain-dependent response to the DFNAC – CBD combination. While S. aureus showed only additive effects, S. epidermidis exhibited pronounced synergism, suggesting differences in cell envelope structure, membrane permeability, or metabolic sensitivity between the two species. The enhanced efficacy observed in S. epidermidis may result from complementary mechanisms of action, including CBD-induced membrane disruption combined with DFNAC-mediated interference with bacterial metabolic processes.
Overall, the data demonstrate that the DFNAC– CBD combination is particularly effective against S. epidermidis, with synergistic activity, whereas only additive effects are observed against S. aureus. The result highlights the potential of such combinations for selectively targeting Gram-positive pathogens.
2.1.2. The Antimicrobial Effect Against Gram-Negative Bacteria
Both E. coli and P. aeruginosa exhibited resistance to CBD and the DFNAC–CBD combination, with no MIC reached and no evidence of synergistic interaction (Figure 2). Indeed, markedly different behaviour was observed for Pseudomonas aeruginosa and E. coli, in which neither CBD alone nor the DFNAC–CBD combination achieved a minimum inhibitory concentration within the tested range. Consequently, FICI values could not be determined. These results indicate a lack of antibacterial efficacy and absence of synergistic interaction against this strain. The intrinsic resistance of P. aeruginosa is well documented. It can be attributed to its highly impermeable outer membrane, efficient efflux pump systems, and adaptive resistance mechanisms, which collectively limit the penetration and activity of many antimicrobial compounds.
Overall, these findings demonstrate that the effectiveness of the DFNAC–CBD combination is strongly dependent on bacterial species. The observed synergistic effect against S. epidermidis, combined with additive activity against S. aureus and lack of efficacy against P. aeruginosa, underscores the importance of considering bacterial physiology and resistance mechanisms when evaluating combination therapies. This strain-specific response suggests that such combinations may be particularly valuable against susceptible Gram-positive pathogens, while alternative strategies are required to target inherently resistant Gram-negative bacteria.
2.2. The Biocompatibility of DFNAC-CBD Formulation
The cytotoxic effects of the DFNAC–CBD combination (3.906 µg/mL) on HDF cells were further evaluated using the LDH assay, which reflects cell membrane integrity. As shown in Figure 3, all tested samples exhibited low LDH release than the positive control, indicating minimal membrane damage. The DFNAC–CBD combination induced only a slight increase in LDH release relative to the negative control, suggesting limited cytotoxicity. Importantly, the LDH levels remained significantly lower than those observed for the positive control, confirming that the treatment does not cause substantial cell lysis or membrane disruption.
The overall trend observed in the LDH assay is consistent with the MTT results, supporting the conclusion that the tested concentration maintains high cell viability while inducing only minor cytotoxic effects. The result indicates that the antibacterial MIC concentration does not compromise cell membrane integrity to a biologically significant extent. Taken together, the low LDH release and preserved metabolic activity demonstrate that the DFNAC–CBD combination exhibits good cytocompatibility with HDF cells, reinforcing its potential for biomedical applications that require both antimicrobial efficacy and host cell safety.
3. Discussion
The rise of antibiotic resistance in bacterial pathogens is reducing the effectiveness of essential antibiotics used in invasive surgery and chemotherapy, complicating treatment for normally manageable diseases. To address this, developing new antibacterials and identifying molecules that enhance the efficacy of existing antibiotics are critical priorities.
This study evaluated the antimicrobial responses of various bacterial strains, particularly focusing on the potential synergistic effects of DFNAC and CBD while considering drug repurposing [40] and previous research [41,42]. Some findings suggest that CBD acts as a “potentiator,” improving standard antibiotics’ effectiveness against resistant strains, while others indicate it may be an effective standalone antibacterial agent for topical use [43]. Other studies highlight DFNAC’s notable antibacterial and anti-inflammatory effects [44]. Our results demonstrated the synergistic interaction against Staphylococcus epidermidis, when combining DFNAC and CBD, significantly enhancing antibacterial efficacy and substantially reducing the minimum inhibitory concentration (MIC). Conversely, when tested against Staphylococcus aureus, the combination exhibited an additive effect, indicating partial cooperation between DFNAC and CBD.
Indeed, research has been directed at identifying antimicrobial candidates to combat the rising antibiotic resistance in Gram-positive bacteria. Given the serious infections caused by Staphylococcus aureus, investigating natural products like CBD [36,45,46] is a logical step, and further evidence of in vivo efficacy is warranted [47,48]. However, pharmacodynamic studies are required to assess drug-drug interactions for a continuous evaluation of CBD’s benefits [42,43].
The question revolves around its MOA – whether it disrupts the bacterial membranes or targets specific metabolic pathways – raising issue of whether it is bactericidal or bacteriostatic. The proposed mechanism for DFNAC-CBD combination, particularly against Gram-positive bacteria, suggests complementary mechanisms leading to enhanced bacterial damage and growth inhibition: CBD primarily disrupts bacterial membrane integrity, while DFNAC interferes with intracellular metabolic processes. Previous studies also indicated different mechanisms when NSAIDs are paired with antibiotics against S. epidermidis and S. aureus. DFNAC c sodium against S. epidermidis, indicated a high affinity for S. epidermidis proteins and TcaR enzymes and suggested molecular docking [44]. DFNAC combined with Gentamicin against S. aureus showed a synergistic effect (FIC index 0.38) [15], suggesting efflux pump inhibition. Conversely, Ketorolac combined with Gentamicin against S. aureus biofilms demonstrated synergistic activity against S. aureus biofilms (FIC index 0.31), likely through modulation of the biofilm matrix [49].
Despite showing weak to moderate direct antibacterial activity (MICs ranging from 32 to 512 µg/mL), based on the Checkerboard assays - the primary method for testing synergistic activity – NSAIDs exhibited synergistic effects with various antibiotics like Gentamicin, Ciprofloxacin, Oxacillin, Chloramphenicol, Cefuroxime, and Tetracycline (FIC indices generally < 0.5 to 0.625). Efflux pump inhibition is frequently proposed as MOA [40]. Moving forward, more molecular studies are essential to validate these findings and explore the potential of NSAIDs as modulators or antibacterial adjuvants. However, challenges remain, such as achieving effective concentrations without toxicity and confirming mechanisms to ensure pharmacokinetic and pharmacodynamic compatibility, specificity and avoid off-target effects. Furthermore, our exploratory evidence indicates that the combination of DFNAC and CBD may become a significant antimicrobial pairing, aligning with the ongoing efforts to refine applications [50,51,52] and establish a regulatory framework [53] for future pharmacological products. It also aims to address methodological inconsistencies in standardised testing methods, culture media, and CBD sources.
Notably, we found no antibacterial activity against the Gram-negative strains Escherichia coli and Pseudomonas aeruginosa, which reflects their intrinsic resistance and highlights the combination’s inability to overcome the permeability barrier of their outer membranes. While it is widely accepted that CBD is highly effective against Gram-positive bacteria, including MRSA, there is a debate about its efficacy against Gram-negative bacteria. Many studies support the view that CBD is inactive against Gram-negative bacteria due to their protective outer membrane. However, a conflicting hypothesis suggests that certain Gram-negative bacteria—specifically Neisseria gonorrhoeae, Neisseria meningitidis, and Legionella pneumophila—are highly sensitive to CBD. This observation raises the question of whether CBD is a niche Gram-positive agent or a broad-spectrum candidate with tailored applications [27,34,54,55]. In the meantime, dose–response studies against E. coli and S. aureus indicated that DFNAC reduced metabolic activity without removing biofilm mass at therapeutic concentrations, resulting in significant reductions in colony-forming units within the biofilm as confirmed by Scanning Electron Microscopy [56]. However, the bactericidal effect against Gram-negative and Gram-positive bacteria – evident through inhibition of biofilm formation or reduction of metabolic viability – is limited at clinically relevant concentrations with standardised MBIC or MBEC values missing. The minimum bactericidal concentrations (MBCs) were consistently above 2000 µg/mL, indicating limited bactericidal potential [40]. Therefore, direct and consistent data on membrane disruption as well as in vivo or toxicity study results are still needed for conclusive mapping. To aid in drug formulation profiling, our study provided information on drug-drug interactions and confirmed the biocompatibility of the proposed combination of DFNAC and CBD. We highlighted the biocompatibility profile of the combination on human dermal fibroblasts (HDF). Both MTT and LDH assays demonstrated that the antibacterial concentration (3.906 µg/mL) preserves cell viability and membrane integrity. Live/Dead staining confirmed that most cells remained viable and exhibited normal morphology. The overall results indicate that the combination operates within a therapeutic window, achieving antimicrobial efficacy without inducing significant cytotoxicity. Moreover, the combination shows high biocompatibility. Investigations reported that CBD decreased the overall acidity levels in rats treated with DFNAC, suggesting that cannabidiol effectively treated the condition [57], or provided hepatoprotection against DFNAC sodium-induced hepatotoxicity [58]. However, the increasing interest in cannabis also requires a deeper understanding of the potential interactions between CBD with NSAIDs based on current knowledge and evidence [59,60].
Therefore, further rigorous quantitative biofilm assays, mechanistic membrane studies, and validation through clinical or animal models are essential before NSAIDs [41] and CBD [61] can be considered viable anti-biofilm adjuvants. Although DFNAC was tested in clinical trials involving patients with uncomplicated urinary tract infections and cellulitis [43], additional studies are necessary to complete its antimicrobial profile. Recent developments in plant-derived and synthetic cannabinoids [51] and NSAIDs [62] support the hypothesis that new therapeutic formulations [63,64] can be designed [65] specifically to address the antimicrobial crisis while meeting clinical applications [66] and regulatory requirements. Moreover, addressing antibiotic resistance through drug reprofiling will enhance formulations for personalised medicine.
4. Materials and Methods
The antimicrobial interaction between CBD and DFNAC was evaluated against ATCC bacterial strains cultured in tryptic soy broth (TSB). Bacterial suspensions were prepared from overnight cultures and adjusted to the required inoculum density. Serial two-fold dilutions of CBD, DFNAC, and CBD–DFNAC combinations were prepared in TSB in sterile 96-well microplates. Wells containing bacteria without treatment served as growth controls, while wells containing TSB and tested compounds without bacteria were used as blanks. Plates were incubated at 37 °C for 24 h, after which bacterial growth was evaluated by measuring optical density at 620 nm. The minimum inhibitory concentration (MIC) was defined as the lowest concentration showing no visible bacterial growth and OD values comparable to the blank control. The interaction between CBD and DFNAC was assessed using the fractional inhibitory concentration index (FICI), calculated as follows:
FICI= (MIC CBD in combination/MIC CBD alone) x (MIC CBD in combination / MIC DFNAC alone)
The interaction was interpreted as synergistic when FICI ≤ 0.5, additive when 0.5 < FICI ≤ 1, indifferent when 1 < FICI ≤ 4, and antagonistic when FICI > 4.
Cell viability and metabolic activity were assessed using the MTT Cell Proliferation Assay Kit (Roche Diagnostics) according to the manufacturer’s protocol. Human dermal fibroblasts (HDFs) were seeded in 24-well plates at a density of 1 × 10⁴ cells/well and cultured in Dulbecco’s Modified Eagle Medium (DMEM) supplemented with 10% fetal bovine serum (FBS) under standard conditions (37 °C, 5% CO₂, humidified atmosphere). After 24 h to allow cell attachment, the culture medium was replaced and the cells were exposed to the tested CBD–diclofenac mixtures at the selected concentrations.
Following 24 h incubation, the culture medium was removed and the cells were gently washed with phosphate-buffered saline (PBS). MTT reagent was added to each well at a final concentration of 0.5 mg/mL and incubated for 4 h at 37 °C to permit the formation of formazan crystals by metabolically active cells. Subsequently, the crystals were dissolved using the supplied solubilization solution, and absorbance was measured at 550 nm using a Multiskan FC microplate reader (Thermo Scientific). The obtained absorbance values were considered directly proportional to the number of viable cells and overall metabolic activity.
Cytotoxicity and membrane integrity were further evaluated using the Lactate Dehydrogenase (LDH) Cytotoxicity Detection Kit (Roche Diagnostics), following the manufacturer’s instructions. After 24 h exposure to the CBD–diclofenac formulations, 50 µL of culture supernatant from each well was collected and transferred to a 96-well plate. Subsequently, 100 µL of freshly prepared reaction mixture was added to each sample and incubated for 15–20 min at room temperature in the dark. The assay is based on the quantification of LDH released from damaged cells into the extracellular medium, generating a colored product proportional to membrane disruption and cytotoxicity. Absorbance was measured at 490 nm with a reference wavelength of 600 nm using a Tecan Infinite 200 Pro microplate reader. Results were expressed as optical density (OD) values.
Cell viability and morphology were additionally analyzed using the Live/Dead Viability/Cytotoxicity Kit (Invitrogen, Thermo Fisher Scientific). HDF cells were seeded at a density of 1 × 10⁴ cells/well and incubated with the CBD–diclofenac mixtures for 24–72 h under standard culture conditions (37 °C, 5% CO₂). After treatment, the culture medium was removed and the cells were carefully washed with PBS. A staining solution containing calcein-AM, which labels viable cells with green fluorescence, and ethidium homodimer-1, which stains dead cells red, was prepared according to the manufacturer’s recommendations and added to each well. Samples were incubated for 30–60 min in the dark at room temperature prior to imaging. Fluorescence images were acquired using a Zeiss Axioscope fluorescence microscope equipped with an AxioCam imaging system in order to evaluate cell viability, morphology, and cellular attachment following exposure to the tested formulation.
5. Conclusions
Combining DFNAC, a common potent non-steroidal anti-inflammatory drug, with CBD offers a promising approach to enhance antimicrobial capacity against various bacterial strains. This combination targets both the bacterial membrane and cellular mechanisms, thereby reducing antibiotics resistance. Combining complementary MOAs facilitated a synergistic effect against S. epidermidis and an additive effect against S. aureus. The lack of antibacterial activity detected against the Gram-negative strains Escherichia coli and Pseudomonas aeruginosa reflects the need for new complementary MOAs that can simultaneously disrupt bacterial defence mechanisms and prevent the development of resistance. Using a combination of DFNAC and CBD allows for lower, less toxic doses of both substances and co-treatment reduces the development of resistance compared to single-agent treatment. Moreover, the proposed combination provides both direct bacteria killing and anti-inflammatory properties, helping reduce tissue damages during infection and personalised, targeted therapeutic approaches. DFNAC and CBD are excellent candidates for repurposing as adjuncts to enhance the efficacy of conventional antibiotics.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, F.S.I., G.G.P. and B.M.T; methodology, G.G.P. and F.S.I.; validation, F.S.I., G.G.P., B.M.T, and C.I.; formal analysis, G.G.P. and F.S.I.; investigation, G.G.P. and F.S.I.; resources, G.G.P., F.S.I and C.I.; data curation, G.G.P.; writing—original draft preparation, F.S.I. and G.G.P.; writing—review and editing, F.S.I., G.G.P., B.M.T. and C.I.; visualization, G.G.P., F.S.I.; supervision, F.S.I.; funding acquisition, C.I. All authors have read and agreed to the published version of the manuscript.”
Funding
The authors acknowledge the European Union’s Horizon Europe Research and Innovation framework programme 2021–2027, under the Coordination and Support Actions, HORIZON-WIDERA-2022-TALENTS-01 (grant agreement - 101087007 – eBio-hub). Funded by the European Union. Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or European Research Executive Agency (REA). Neither the European Union nor the granting authority can be held responsible for them.
Data Availability Statement
The datasets generated and/or analyzed during the current study are publicly available in the Mendeley Data repository: Gradisteanu G. “CBD-DCFN testing”, Mendeley Data, V1, 2026. https://doi.org/10.17632/6hv6tzgjg3.1
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AMR | antimicrobial resistance |
| CBD | Canabidiol |
| DFNAC | Diclofenac |
| FICI | fractional inhibitory concentration index |
| HDF | human dermal fibroblasts |
| LDH | Lactate dehydrogenase |
| MIC | minimum inhibitory concentration |
| MBC | minimum bactericidal concentrations |
| MOA | Mechanism of action |
| NSAID | nonsteroidal anti-inflammatory drugs |
| OD | Optical density |
| TSB | tryptic soy broth |
References
- Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 8 May 2026).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Available online: https://documents1.worldbank.org/curated/en/323311493396993758/pdf/final-report.pdf (accessed on 8 May 2026).
- Available online: https://www.who.int/publications/i/item/9789240062702 (accessed on 8 May 2026).
- Kumar, V.; Singh, A.; Sharma, N.; Saini, R.; Kumar, H.; El–Shazly, M.; Dev, K. Combating bacterial antibiotic resistance with phytocompounds: Current trends and future perspectives. Med. Drug Discov. 2025, 100228. [CrossRef]
- Hobson, C.; Chan, A.N.; Wright, G.D. The antibiotic resistome: a guide for the discovery of natural products as antimicrobial agents. Chem. Rev. 2021, 121, 3464–3494. [Google Scholar] [CrossRef]
- Farha, M.A.; Brown, E.D. Drug repurposing for antimicrobial discovery. Nat. Microbiol. 2019, 4, 565–577. [Google Scholar] [CrossRef]
- Boyd, N.K.; Lee, G.C.; Teng, C.; Frei, C.R. In vitro activity of non-antibiotic drugs against Staphylococcus aureus clinical strains. J. Glob. Antimicrob. Resist. 2021, 27, 167–171. [Google Scholar] [CrossRef]
- Dediu, V.; Ghitman, J.; Gradisteanu Pircalabioru, G.; Chan, K.H.; Iliescu, F.S.; Iliescu, C. Trends in photothermal nanostructures for antimicrobial applications. Int. J. Mol. Sci. 2023, 24, 9375. [Google Scholar] [CrossRef]
- Lagadinou, M.; Onisor, M.O.; Rigas, A.; Musetescu, D.-V.; Gkentzi, D.; Assimakopoulos, S.F.; Panos, G.; Marangos, M. Antimicrobial properties on non-antibiotic drugs in the era of increased bacterial resistance. Antibiotics 2020, 9, 107. [Google Scholar] [CrossRef]
- Barbarossa, A.; Rosato, A.; Corbo, F.; Clodoveo, M.L.; Fracchiolla, G.; Carrieri, A.; Carocci, A. Non-antibiotic drug repositioning as an alternative antimicrobial approach. Antibiotics 2022, 11, 816. [Google Scholar] [CrossRef] [PubMed]
- Roibu, A.; Iliescu, F.S.; Zamfirescu, A.-M.; Radu, E.; Andrei, L.-E.; Osi, A.R.; Gheorghiu, G.-L.; Cobianu, C.; Iliescu, C. Core–Shell Plasmonic Nanocomposites with Synergistic Photothermal and Photochemical Activity for Biomedical Applications. Nanomaterials 2026, 16, 174. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.; Silva, P.M. Non-antibiotic compounds: The activity of the NSAID diclofenac on bacteria—A review. Int. J. Curr. Microbiol. Appl. Sci. 2018, 7, 340–351. [Google Scholar] [CrossRef]
- Ferrer-Luque, C.M.; Baca, P.; Solana, C.; Rodríguez-Archilla, A.; Arias-Moliz, M.T.; Ruiz-Linares, M. Antibiofilm activity of diclofenac and antibiotic solutions in endodontic therapy. J. Endod. 2021, 47, 1138–1143. [Google Scholar] [CrossRef]
- Mazumdar, K.; Dastidar, S.; Park, J.; Dutta, N. The anti-inflammatory non-antibiotic helper compound diclofenac: an antibacterial drug target. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 881–891. [Google Scholar] [CrossRef]
- M. Karajeh, A.; N. Alkaraki, R.; Gaber, Y. Novel synergistic antibacterial activity of meloxicam-curcumin and diclofenac-curcumin combinations against methicillin-sensitive S. aureus and E. faecium. Beni-Suef Univ. J. Basic Appl. Sci. 2025, 14, 20. [Google Scholar] [CrossRef]
- Dutta, N.K.; Mazumdar, K.; Park, J.H. In vitro synergistic effect of gentamicin with the anti-inflammatory agent diclofenac against Listeria monocytogenes. Lett. Appl. Microbiol. 2009, 48, 783–785. [Google Scholar] [PubMed]
- Dutta, N.K.; Annadurai, S.; Mazumdar, K.; Dastidar, S.G.; Kristiansen, J.E.; Molnar, J.; Martins, M.; Amaral, L. Potential management of resistant microbial infections with a novel non-antibiotic: the anti-inflammatory drug diclofenac sodium. Int. J. Antimicrob. Agents 2007, 30, 242–249. [Google Scholar] [CrossRef]
- Leão, C.; Borges, A.; Simões, M. NSAIDs as a drug repurposing strategy for biofilm control. Antibiotics 2020, 9, 591. [Google Scholar] [CrossRef]
- Rosato, A.; Catalano, A.; Carocci, A.; Carrieri, A.; Carone, A.; Caggiano, G.; Franchini, C.; Corbo, F.; Montagna, M.T. In vitro interactions between anidulafungin and nonsteroidal anti-inflammatory drugs on biofilms of Candida spp. Bioorganic Med. Chem. 2016, 24, 1002–1005. [Google Scholar] [CrossRef]
- Rosato, A.; Altini, E.; Sblano, S.; Salvagno, L.; Maggi, F.; de Michele, G.; Carocci, A.; Clodoveo, M.L.; Corbo, F.; Fracchiolla, G. Synergistic activity of new diclofenac and essential oils combinations against different Candida spp. Antibiotics 2021, 10, 688. [Google Scholar] [CrossRef]
- Selvam, P.K.; Mohan, S.; Vasudevan, K. Synergistic Interaction of Diclofenac with Colistin Enhances Antimicrobial Efficacy Against Multidrug-Resistant Acinetobacter baumannii. The Microbe 2026, 100706. [Google Scholar] [CrossRef]
- Zhang, S.; Qu, X.; Tang, H.; Wang, Y.; Yang, H.; Yuan, W.; Yue, B. Diclofenac Resensitizes Methicillin-Resistant Staphylococcus aureus to β-Lactams and Prevents Implant Infections. Adv. Sci. 2021, 8, 2100681. [Google Scholar] [CrossRef] [PubMed]
- Abbas, H.A.; Atallah, H.; El-Sayed, M.A.; El-Ganiny, A.M. Diclofenac mitigates virulence of multidrug-resistant Staphylococcus aureus. Arch. Microbiol. 2020, 202, 2751–2760. [Google Scholar] [CrossRef]
- Chan, E.W.L.; Yee, Z.Y.; Raja, I.; Yap, J.K.Y. Synergistic effect of non-steroidal anti-inflammatory drugs (NSAIDs) on antibacterial activity of cefuroxime and chloramphenicol against methicillin-resistant Staphylococcus aureus. J. Glob. Antimicrob. Resist. 2017, 10, 70–74. [Google Scholar] [CrossRef]
- Bonini, S.A.; Premoli, M.; Tambaro, S.; Kumar, A.; Maccarinelli, G.; Memo, M.; Mastinu, A. Cannabis sativa: A comprehensive ethnopharmacological review of a medicinal plant with a long history. J. Ethnopharmacol. 2018, 227, 300–315. [Google Scholar] [CrossRef]
- Tihăuan, B.M.; Onisei, T.; Slootweg, W.; Gună, D.; Iliescu, C.; Chifiriuc, M.C. Cannabidiol—A friend or a foe? Eur. J. Pharm. Sci. 2025, 208, 107036. [Google Scholar] [CrossRef]
- Grimison, P.; Mersiades, A.; Kirby, A.; Lintzeris, N.; Morton, R.; Haber, P.; Olver, I.; Walsh, A.; McGregor, I.; Cheung, Y. Oral THC: CBD cannabis extract for refractory chemotherapy-induced nausea and vomiting: a randomised, placebo-controlled, phase II crossover trial. Ann. Oncol. 2020, 31, 1553–1560. [Google Scholar] [CrossRef]
- Guillouard, M.; Authier, N.; Pereira, B.; Soubrier, M.; Mathieu, S. Cannabis use assessment and its impact on pain in rheumatologic diseases: a systematic review and meta-analysis. Rheumatology 2021, 60, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hong, P.J.; May, C.; Rehman, Y.; Oparin, Y.; Hong, C.J.; Hong, B.Y.; AminiLari, M.; Gallo, L.; Kaushal, A. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomised clinical trials. BMJ 2021, 374. [Google Scholar] [CrossRef] [PubMed]
- Urbi, B.; Corbett, J.; Hughes, I.; Owusu, M.A.; Thorning, S.; Broadley, S.A.; Sabet, A.; Heshmat, S. Effects of cannabis in Parkinson’s disease: a systematic review and meta-analysis. J. Park. Dis. 2022, 12, 495–508. [Google Scholar] [CrossRef]
- Zajicek, J.; Fox, P.; Sanders, H.; Wright, D.; Vickery, J.; Nunn, A.; Thompson, A. Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): multicentre randomised placebo-controlled trial. The lancet 2003, 362, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Ried, K.; Tamanna, T.; Matthews, S.; Sali, A. Medicinal cannabis improves sleep in adults with insomnia: a randomised double-blind placebo-controlled crossover study. J. Sleep Res. 2023, 32, e13793. [Google Scholar] [CrossRef] [PubMed]
- Blaskovich, M.A.; Kavanagh, A.M.; Elliott, A.G.; Zhang, B.; Ramu, S.; Amado, M.; Lowe, G.J.; Hinton, A.O.; Pham, D.M.T.; Zuegg, J. The antimicrobial potential of cannabidiol. Commun. Biol. 2021, 4, 7. [Google Scholar] [CrossRef]
- Werner, M.; Bereswill, S.; Heimesaat, M.M. A recent update on the antibacterial effects of distinct bioactive molecules derived from the Cannabis plant. Eur. J. Microbiol. Immunol. 2024, 14, 333–339. [Google Scholar] [CrossRef]
- Farha, M.A.; El-Halfawy, O.M.; Gale, R.T.; MacNair, C.R.; Carfrae, L.A.; Zhang, X.; Jentsch, N.G.; Magolan, J.; Brown, E.D. Uncovering the hidden antibiotic potential of cannabis. ACS Infect. Dis. 2020, 6, 338–346. [Google Scholar] [CrossRef]
- Abichabki, N.; Zacharias, L.V.; Moreira, N.C.; Bellissimo-Rodrigues, F.; Moreira, F.L.; Benzi, J.R.; Ogasawara, T.M.; Ferreira, J.C.; Ribeiro, C.M.; Pavan, F.R. Potential cannabidiol (CBD) repurposing as antibacterial and promising therapy of CBD plus polymyxin B (PB) against PB-resistant gram-negative bacilli. Sci. Rep. 2022, 12, 6454. [Google Scholar] [CrossRef]
- Gildea, L.; Ayariga, J.A.; Xu, J.; Villafane, R.; Robertson, B.K.; Samuel-Foo, M.; Ajayi, O.S. Cannabis sativa CBD extract exhibits synergy with broad-spectrum antibiotics against Salmonella enterica subsp. Enterica serovar Typhimurium. Microorganisms 2022, 10, 2360. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.; Neira Agonh, D.; Lehmann, C. Antibacterial effects of phytocannabinoids. Life 2022, 12, 1394. [Google Scholar] [CrossRef] [PubMed]
- Tiwana, G.; Cock, I.E.; Taylor, S.M.; Cheesman, M.J. Beyond Antibiotics: Repurposing Non-Antibiotic Drugs as Novel Antibacterial Agents to Combat Resistance. Int. J. Mol. Sci. 2025, 26, 9880. [Google Scholar] [CrossRef]
- Dronik, M.; Stasevych, M. Expanding Horizons: Opportunities for Diclofenac Beyond Traditional Use—A Review. Sci. Pharm. 2025, 93, 31. [Google Scholar] [CrossRef]
- Gałka, S. Cannabis sativa in the fight against drug-resistant bacteria and fungi. Folia Medica Cracoviensia 2025, 65, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Okpala, O.E.; Rondevaldova, J.; Kokoska, L. Anti-inflammatory drugs as potential antimicrobial agents: a review. Front. Pharmacol. 2025, 16, 1557333. [Google Scholar] [CrossRef]
- Abo-Kamar, A.M.; Abdelaziz, A.A.; Ashour, A.E.; Shaldam, M.A.; Elekhnawy, E. Employing diclofenac sodium as a novel therapeutic frontier for Staphylococcus epidermidis infections. Sci. Rep. 2025, 15, 31377. [Google Scholar] [CrossRef]
- Wright, G.D. Solving the antibiotic crisis. ACS Infect. Dis. 2015, 1, 80–84. [Google Scholar] [CrossRef]
- Harvey, A.L.; Edrada-Ebel, R.; Quinn, R.J. The re-emergence of natural products for drug discovery in the genomics era. Nat. Rev. Drug Discov. 2015, 14, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Popescu, A.; Dreanca, A.; Sarpataki, O.; Cernea, M.; Jourdan, A.; Marcus, I. Cannabidiol, from Past to Present: a Review. Vet. Drug/Medicamentul Vet. 2023, 17. [Google Scholar]
- Klahn, P. Cannabinoids-promising antimicrobial drugs or intoxicants with benefits? Antibiotics 2020, 9, 297. [Google Scholar] [CrossRef]
- Sekar, A.; Gil, D.; Tierney, P.; McCanne, M.; Daesety, V.; Trendafilova, D.; Muratoglu, O.K.; Oral, E. Synergistic use of anti-inflammatory ketorolac and gentamicin to target staphylococcal biofilms. J. Transl. Med. 2024, 22, 102. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, P.H.M.P.; Dinelli, R.G.; Garzón, H.S.; Suárez, D.R.; Corral, M.A.T.; Christoff, E.P.; Bueno, M.R.; Sandi, U.M.; Suárez, L.J.; Bueno-Silva, B. Evaluation of the antimicrobial effect of cannabidiol (CBD) in a multispecies subgingival biofilm model. J. Oral. Microbiol. 2026, 18, 2603706. [Google Scholar] [CrossRef] [PubMed]
- Musa, S.; Dayan, L. Recent development of plant-derived and synthetic cannabinoids as novel antimicrobial agents. Future Med. Chem. 2025, 17, 2881–2894. [Google Scholar] [CrossRef] [PubMed]
- Simei, J.L.Q.; Souza, J.D.R.; Pedrazzi, J.F.; Guimarães, F.S.; Campos, A.C.; Zuardi, A.; Hallak, J.E.C.; Crippa, J.A.S. Research and clinical practice involving the use of cannabis products, with emphasis on cannabidiol: A narrative review. Pharmaceuticals 2024, 17, 1644. [Google Scholar] [CrossRef] [PubMed]
- Razouk, L.; Hamdy, R.; Ahmad, A.; Razouk, O.; Mohamed, N.A.; Soliman, S.S. Hemp versus marijuana: Chemistry-and pharmacology-associated regulatory framework. Med. Sci. Law. 2026, 00258024261420541. [Google Scholar] [CrossRef]
- Garzón, H.S.; Loaiza-Oliva, M.; Martínez-Pabón, M.C.; Puerta-Suárez, J.; Téllez Corral, M.A.; Bueno-Silva, B.; Suárez, D.R.; Díaz-Báez, D.; Suárez, L.J. Antibiofilm and immune-modulatory activity of cannabidiol and cannabigerol in oral environments—In vitro study. Antibiotics 2024, 13, 342. [Google Scholar] [CrossRef]
- Fang, S.; Kang, W.-T.; Li, H.; Cai, Q.; Liang, W.; Zeng, M.; Yu, Q.; Zhong, R.; Tao, Y.; Liu, S. Development of cannabidiol derivatives as potent broad-spectrum antibacterial agents with membrane-disruptive mechanism. Eur. J. Med. Chem. 2024, 266, 116149. [Google Scholar] [CrossRef]
- Reśliński, A.; Dąbrowiecki, S.; Głowacka, K. The impact of diclofenac and ibuprofen on biofilm formation on the surface of polypropylene mesh. Hernia 2015, 19, 179–185. [Google Scholar] [CrossRef]
- Sharif, S.J.; Kadhim, H.M.; Ahmed, B.S.; Ridha-Salman, H. Gastroprotective and therapeutic effects of emodin on rat model of diclofenac-induced gastric ulceration. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2026, 399, 4519–4536. [Google Scholar] [CrossRef]
- Shehu, R.; Kabir, I. Therapeutic Potential of Cannabis sativa Extract in Mitigating Diclofenac-Induced Renal Toxicity in Wistar Rats. SJMLS 2024, 9. [Google Scholar]
- Balachandran, P.; Elsohly, M.; Hill, K.P. Cannabidiol interactions with medications, illicit substances, and alcohol: a comprehensive review. J. General. Intern. Med. 2021, 36, 2074–2084. [Google Scholar] [CrossRef]
- Alsherbiny, M.A.; Li, C.G. Medicinal cannabis—potential drug interactions. Medicines 2018, 6, 3. [Google Scholar] [CrossRef]
- Coelho, M.J.; Araújo, M.D.; Carvalho, M.; Cardoso, I.L.; Manso, M.C.; Pina, C. Antimicrobial potential of cannabinoids: a scoping review of the past 5 years. Microorganisms 2025, 13, 325. [Google Scholar] [CrossRef]
- Ghosh, J.; Repon, M.R.; Pranta, A.D.; Rupanty, N.S.; Khan, F.; Noor, T. Bioactive component integrated textiles: A promising source of medicine and healthcare. J. Eng. Fibers Fabr. 2025, 20, 15589250241308561. [Google Scholar] [CrossRef]
- Ilieva, L.; Baev, V.; Marhova, M.; Yahubyan, G.; Apostolova, E.; Gozmanova, M.; Gochev, V.; Paunova-Krasteva, T.; Damyanova, T.; Kostadinova, S. Potential of Fermented Food-Derived Lactiplantibacillus Cell-Free Supernatants to Control Staphylococcus aureus Growth and Biofilm Development. Int. J. Mol. Sci. 2026, 27, 760. [Google Scholar] [CrossRef]
- Laohavisuti, N.; Boonchom, B.; Rungrojchaipon, P.; Boonmee, W.; Seesanong, S.; Punthipayanon, S. A Simple and Rapid Synthesis of Spherical Silver Phosphate (Ag3PO4) and Its Antimicrobial Activity in Plant Tissue Culture. Int. J. Mol. Sci. 2025, 26, 7371. [Google Scholar] [CrossRef]
- Gao, Z.; Liu, M.; Wang, Z.; Zhang, M.; Shen, G.; Gong, Y.; Zheng, K.; Yang, M.; Wang, Q. In vitro antibacterial activity evaluation and mechanism of morphology-controlled synthesis of cerium dioxide nanoparticles. Int. J. Mol. Sci. 2025, 26, 10587. [Google Scholar] [CrossRef]
- Wolfson, G.; Steinberg, D.; Eliassaf, A.; Morshina, A.; Enríquez-Rodríguez, C.J.; Polacheck, I.; Korem, M.; Shalev, O. Anandamide Alters Glycolytic Activity in Streptococcus mutans: Metabolomics and Stable Isotope Labeling Study. Int. J. Mol. Sci. 2025, 26, 8401. [Google Scholar] [CrossRef]
Figure 1.
Antibacterial activity and synergistic interaction of diclofenac (DFNAC) and cannabidiol (CBD) against Staphylococcus aureus and Staphylococcus epidermidis. (A–C) Antibacterial activity against S. aureus: (A) MIC of CBD, (B) MIC of DFNAC, and (C) MIC of the DFNAC –CBD combination. (D–F) Antibacterial activity against S. epidermidis: (D) MIC of CBD, (E) MIC of DFNAC, and (F) MIC of the DFNAC– CBD combination. (G–H) Checkerboard assays illustrating the interaction between CBD and DFNAC: (G) S. aureus and (H) S. epidermidis. Optical density (OD₆₀₀) values are represented as heatmaps, where blue indicates bacterial growth inhibition (low OD) and red indicates bacterial proliferation (high OD). The dashed line represents the approximate boundary between growth and inhibition (OD ≈ 0.07). Green boxes indicate the minimum inhibitory concentration (MIC) of the combination, defined as the lowest concentrations of both compounds that completely inhibit bacterial growth. The fractional inhibitory concentration index (FICI) indicates an additive effect for S. aureus (FICI ≈ 0.5) and a synergistic effect for S. epidermidis (FICI = 0.258). Data are presented as mean ± standard deviation from 3 independent experiments.
Figure 1.
Antibacterial activity and synergistic interaction of diclofenac (DFNAC) and cannabidiol (CBD) against Staphylococcus aureus and Staphylococcus epidermidis. (A–C) Antibacterial activity against S. aureus: (A) MIC of CBD, (B) MIC of DFNAC, and (C) MIC of the DFNAC –CBD combination. (D–F) Antibacterial activity against S. epidermidis: (D) MIC of CBD, (E) MIC of DFNAC, and (F) MIC of the DFNAC– CBD combination. (G–H) Checkerboard assays illustrating the interaction between CBD and DFNAC: (G) S. aureus and (H) S. epidermidis. Optical density (OD₆₀₀) values are represented as heatmaps, where blue indicates bacterial growth inhibition (low OD) and red indicates bacterial proliferation (high OD). The dashed line represents the approximate boundary between growth and inhibition (OD ≈ 0.07). Green boxes indicate the minimum inhibitory concentration (MIC) of the combination, defined as the lowest concentrations of both compounds that completely inhibit bacterial growth. The fractional inhibitory concentration index (FICI) indicates an additive effect for S. aureus (FICI ≈ 0.5) and a synergistic effect for S. epidermidis (FICI = 0.258). Data are presented as mean ± standard deviation from 3 independent experiments.

Figure 2.
Antibacterial activity of diclofenac (DFNAC), cannabidiol (CBD), and their combination against Gram-negative bacteria: Pseudomonas aeruginosa and Escherichia coli. (A–C) Antibacterial activity against E. coli: (A) MIC of CBD, (B) MIC of DFNAC, and (C) MIC of the DFNAC–CBD combination. (D–F) Antibacterial activity against P. aeruginosa: (D) MIC of CBD, (E) MIC of DFNAC, and (F) MIC of the DFNAC–CBD combination.
Figure 2.
Antibacterial activity of diclofenac (DFNAC), cannabidiol (CBD), and their combination against Gram-negative bacteria: Pseudomonas aeruginosa and Escherichia coli. (A–C) Antibacterial activity against E. coli: (A) MIC of CBD, (B) MIC of DFNAC, and (C) MIC of the DFNAC–CBD combination. (D–F) Antibacterial activity against P. aeruginosa: (D) MIC of CBD, (E) MIC of DFNAC, and (F) MIC of the DFNAC–CBD combination.

Figure 3.
Biocompatibility assessment of CBD,DFNAC, and their combination on human dermal fibroblasts (HDF). (A) Lactate dehydrogenase (LDH) assay evaluating cell membrane integrity. LDH release is expressed as optical density (OD₄₉₀ nm), with higher values indicating increased cytotoxicity. The cytotoxic control represents maximum LDH release. (B) MTT assay assessing cellular metabolic activity. Cell viability is expressed as optical density (OD₅₅₀ nm), proportional to the number of metabolically active cells. The cytotoxic control shows a marked reduction in viability. (C) Live/Dead fluorescence imaging of HDF cells after exposure to the tested compounds. Viable cells are stained green (calcein-AM), while dead cells are stained red (ethidium homodimer). Representative images show preserved cell morphology and a predominance of viable cells in all treated groups, comparable to the control. Overall, the results indicate that CBD, DFNAC, and their combination maintain high cell viability with minimal cytotoxic effects at the tested concentration.
Figure 3.
Biocompatibility assessment of CBD,DFNAC, and their combination on human dermal fibroblasts (HDF). (A) Lactate dehydrogenase (LDH) assay evaluating cell membrane integrity. LDH release is expressed as optical density (OD₄₉₀ nm), with higher values indicating increased cytotoxicity. The cytotoxic control represents maximum LDH release. (B) MTT assay assessing cellular metabolic activity. Cell viability is expressed as optical density (OD₅₅₀ nm), proportional to the number of metabolically active cells. The cytotoxic control shows a marked reduction in viability. (C) Live/Dead fluorescence imaging of HDF cells after exposure to the tested compounds. Viable cells are stained green (calcein-AM), while dead cells are stained red (ethidium homodimer). Representative images show preserved cell morphology and a predominance of viable cells in all treated groups, comparable to the control. Overall, the results indicate that CBD, DFNAC, and their combination maintain high cell viability with minimal cytotoxic effects at the tested concentration.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



