
Submitted:
28 February 2026
Posted:
04 March 2026
You are already at the latest version
Abstract
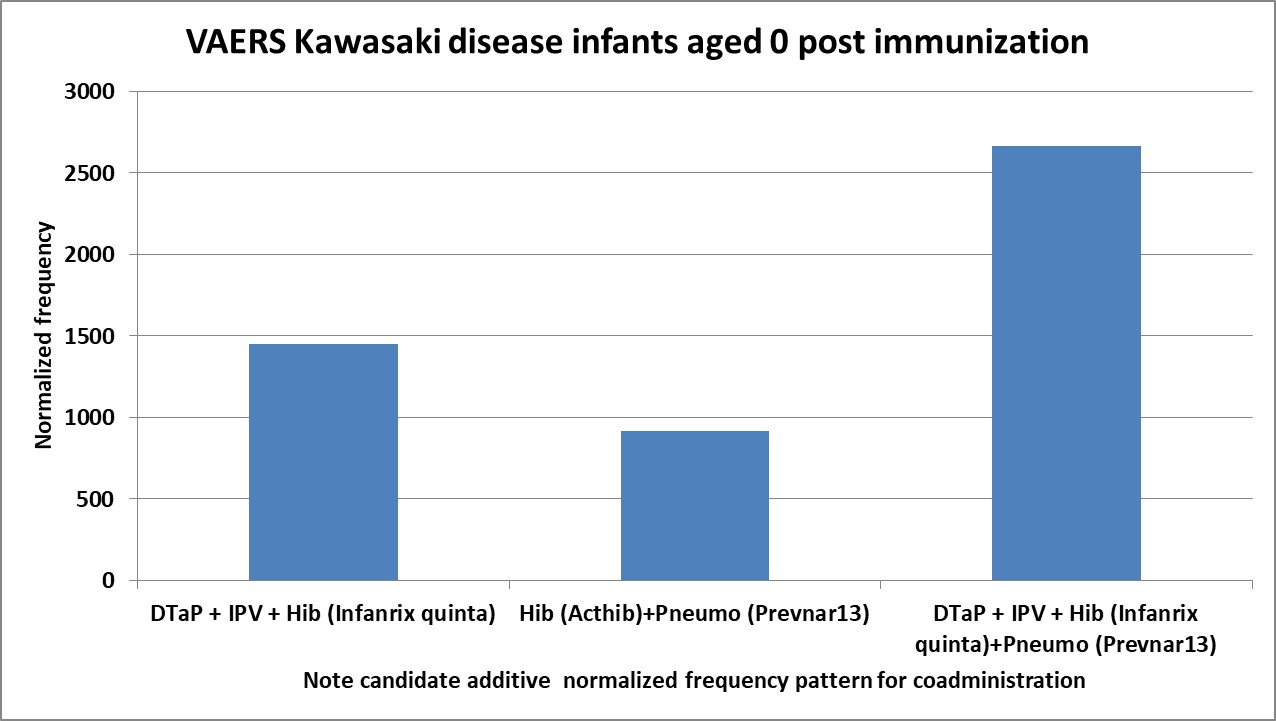
Background/Objectives: Kawasaki’s disease (KD) is a leading cause of heart disease in children. The multisystem inflammatory syndrome (MIS) associated with the SARS-CoV-2 virus is similar to KD. The etiologies of KD and MIS are unknown. Both diseases are associated with pathogens and immunizations. Methods: The Vaccine Adverse Event Reporting System (VAERS) was retrospectively examined for etiology insights into both KD and MIS. Results: Immediate-onset KD-associated safety signals were detected for specific vaccines and coadministered combinations of these vaccines for young infants; a subset of these associations have a male sex bias, whereas others appear to be sex neutral. These specific vaccines may contain manufacturing contaminants (e.g., endotoxins) that are activating mast cells via Toll-like receptors. MIS-V cases were enriched in children of all ages. Conclusions: Both KD and MIS appear to involve two activation pathways. The first pathway involves high titers of immune complexes that activate Fc receptors on mast cells, platelets, and other immune cells. Immune complex titers higher than primary immune response levels are predicted to be required to activate low-affinity IgG FcgR2α receptors on immune cells and platelets. IVIG treatment is predicted to directly compete with immune complex binding to FcgR2α receptors. The second pathway appears to directly activate mast cells and other immune cells without involving immune complexes or Fc receptors. Cardiac adverse events, coronary artery aneurysms (CAAs), myocarditis, transient left ventricular dysfunction, and acquired heart disease are predicted to result from pressure induced lesions indirectly caused by cardiac capillary vasoconstrictions. Second, mast cell activation (e.g., endotoxin contaminants) or persistent infections are likely causes of IVIG nonresponders for KD and MIS. MIS appears to be KD associated with the SARS-CoV-2 virus or the COVID-19 spike protein (MIS-V).
Keywords:
Kawasaki disease
; multisystem inflammatory syndrome
; MIS
; vasculitis disease
; mast cells
; histamine
; vaccines
; immunization
; manufacturing contaminant
; endotoxin
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



