
Submitted:
15 February 2026
Posted:
27 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Serious adverse events (SAEs) develop following coronavirus disease 2019 (COVID-19) immunization in some vaccine recipients. Adverse events (AEs) after immunization are represented by a combination of background AEs and possibly vaccine-associated AEs. When vaccine-associated events occur, they are related to one or more vaccine components, adjuvants, excipients, potentially manufacturing contaminants, or a combination of these constituents. In a retrospective study of Vaccine Adverse Event Reporting System (VAERS) menstrual AEs following immunization, statistically significant differences were observed for multiple manufacturing lots of the COVID-19 Pfizer-BioNTech and the COVID-19 Moderna vaccines. Manufacturing contaminants are likely causative candidates consistent with the observed data for menstrual AEs. Other manufacturing contaminants associated AEs may be detectable by contrasting the normalized frequency rates between predicted higher contamination lots or vaccines compared to lower contamination lots or vaccines. This retrospective study identified candidate pattern signatures for the most frequently reported AEs to VAERS for identified COVID-19 vaccine lots associated with these menstrual AEs and differences in AE frequencies between three human papillomavirus (HPV) vaccines. Six candidate pattern signatures were identified: hemorrhage (female), gynecologic including hemorrhage pattern, myopericarditis (male-biased), HPV vaccine-associated, neuropathy, and fetus patterns. The hemorrhage pattern was identified in six vaccines, including four influenza vaccines. The gynecologic pattern was identified in seven vaccines, including three COVID-19 and three HPV vaccines. And the myopericarditis pattern was identified in 14 vaccines, including five COVID-19 vaccines with two bivalent COVID-19 vaccines, and three smallpox vaccines. The four MCHPV AEs are elevated primarily in HPV vaccines. One or more of the five MCneuropathy AEs were elevated in 11 vaccines. One or more of the MCfetus AEs were elevated in 11 vaccines. For the identified safety signals for vaccines with more SAE and AE reports in VAERS, the observed differences in normalized frequencies of SAEs and AEs between lots for the same vaccine and comparisons between related vaccines are consistent with predicted differences in manufacturing contamination levels.
Keywords:
menstruation
; menstrual cycle
; endotoxin
; mRNA vaccines
; COVID-19 vaccine
; HPV vaccine
; myocarditis
; pericarditis
1. Introduction
Adverse events (AEs) following immunization (AEFIs) are associated with random background events unassociated with the immunization and possible vaccine-associated AEs. Vaccine-associated AEs are often related to normal immune responses to the vaccine. Other AEs and serious AEs (SAEs) are caused by specific vaccine components, adjuvants, excipients, potentially manufacturing contaminants, or combinations of more than one of these constituents. The Vaccine Adverse Event Reporting System (VAERS) and similar databases are designed to collect population samples of AEs for the detection of associated safety signals. Safety signals can be detected from patterns of AEs associated with specific vaccines and specific vaccine lots connected with higher occurrence frequencies compared to other vaccines and vaccine lots. Closer examinations of AEs, like menstrual disturbances, are warranted for AEs that have higher frequencies for specific vaccines and vaccine lots.
Menstrual disturbances, including heavy menstrual bleeding, were reported following coronavirus disease 2019 (COVID-19) vaccination [1,2,3,4,5,6,7]. Menstrual abnormalities include amenorrhoea/ oligomenorrhoea (33.3%), dysmenorrhea (12.7%), heavy menstrual blood loss (29.4%), intermenstrual blood loss (18.7%), irregular blood loss (22.7%), and less menstrual blood loss (3.5%) [8]. In an online questionnaire study, NCT05083065, varying by specific vaccine, 60-70% of reproductive-age women reported menstrual irregularities after the second COVID-19 vaccine dose, with approximately half of the cases resolving within two months [9]. A study of 14,153 women reported 78% experienced menstrual cycle changes following COVID-19 vaccination [2]. A study of 2,269 women found 66.3% reported menstrual symptoms post-vaccination [10]. A similar online questionnaire study with 338 responses found 63.9% reporting changes to their menstrual cycle [11]. A similar survey of 383 women found increased reporting for women with polycystic ovarian syndrome (23.88% vs. 37.78%, p=0.045), hormonal contraceptive use (OR 2.09, 95%CI, 1.23-3.57, p=0.006), and COVID-19 vaccine skepticism (OR 2.96, 95%CI, 1.79-4.90, p<0.001) [12]. In a study of 24,090 menstrual AEs case reports, increased risks were observed for the Johnson & Johnson vaccine (OR 1.83, 95%CI, 1.33-2.49), the Moderna vaccine (OR 2.44, 95%CI, 1.86-3.20), and the Pfizer BioNTech vaccine (OR 3.04, 95%CI, 2.36-3.93) compared to the AstraZeneca COVID-19 vaccine [8]. For comparison, a retrospective study of reproductive-age women with COVID-19 found 28% had menstrual cycle changes [13]. Unexpected vaginal bleeding also develops in some nonmenstruating women following COVID-19 vaccination [14]. Batch-dependent variability of AEs has been reported for the BNT162b2 mRNA COVID-19 vaccine [15,16]. Menstrual AEs were observed to vary significantly by lot for the COVID-19 Pfizer-BioNTech, COVID-19 Moderna, human papillomavirus (HPV) Cervarix, and HPV Gardasil vaccines [17]. HPV vaccination is associated with elevated risks of autonomic dysfunction and menstrual irregularities, which vary by age [18]. Cases of premature ovarian insufficiency (POI) have been reported post-HPV vaccination [19]; a VAERS retrospective study found a safety signal for POI with HPV4 vaccination [20]. The frequencies of multiple AEs vary by different vaccines and sometimes between lots for the same vaccine.
Discordant differences between vaccines and specific vaccine lots with higher and lower normalized frequencies of AEs can possibly be leveraged to detect other AEs also correlated with these differences. Herein, the VAERS database was retrospectively examined for AEs that vary between selected discordant COVID-19 Pfizer-BioNTech lots, discordant COVID-19 Moderna lots, HPV vaccines with higher menstrual AEs, and COVID-19 lots and HPV vaccines with lower menstrual AEs to identify possible candidate manufacturing contamination signature patterns for future studies. Six candidate manufacturing contamination signature patterns were identified: MChemorrhage, MCgynecologic, MCmyopericarditis, MCHPV, MCneuropathy, and MCfetus patterns.
2. Materials and Methods
2.1. VAERS Retrospective Analysis
The VAERS database [21] was retrospectively examined for the AEs for the COVID-19 Pfizer-BioNTech and the COVID-19 Moderna vaccines for lots with a minimum of 100 AE reports with the Ruby program vaers_tally_lots.rb [22]. The downloaded VAERS data includes all AEs reported from 1990 to May 30, 2025. The VAERS database was retrospectively examined for the AEs for all vaccines with the Ruby programs vaers_tally.rb and vaers_tally_gender.rb [22] for genders male and female. Age group analyses were done with the Ruby program vaers_slice5.rb [22]. These tools calculate the frequencies of reported AEs normalized to 100,000 VAERS reports [23]: AE normalized frequency = (observed AEs/all vaccine AEs)*100,000. These normalized frequencies do not represent true incidence rates but estimated rates of reported AEs with asymptomatic individuals not included. To avoid duplicate data, data is tabulated by the unique “vaers_id” identifier. Normalized frequencies were filtered for a minimum of 200 per 100,000 VAERS reports and a minimum of five AEs for a vaccine or vaccine combination. Vaccines and vaccine combinations including the text “no brand name”, “foreign”, “unknown”, and “vaccine not specified” were excluded to avoid possible reporting biases due to the possibility of underrepresentation of less severe AEs resulting in increased normalized frequency estimates. For reproducibility of results, AE names represent decapitalized VAERS names; note that AEs like “abortion spontaneous” have not been altered to common names like “spontaneous abortion”. Microsoft Excel was used to prepare figures. Note that the figures use the VAERS vaccine names with the brand name within parentheses.
2.2. Adverse Events Following Immunization
Adverse events (X) following immunization can be represented as the sum of immunization-associated AEs and background (B) occurrences of AEs. A background AE is considered an event that develops independently of immunization in the population being examined during the time period examined; background AEs are not considered correlated with immunizations. The reported AEs diminish due to reporting bias as the time since immunization increases, fewer AEs are reported. Vaccine-associated AEs can be modeled for vaccine (V) and adverse events (X) by the risks linked to specific vaccine components (C: 0..r), excipients (E: 0..s), manufacturing contaminants (M: 0..t), and population background (BX) events in equation I.
If AE(V|X) = 0 for multiple vaccines for adverse event X, then each of the components Ci, Ej, and Mk, are all approximately zero for these vaccines, and B is approximately zero for all vaccines. If AE(V|X) = 0 for multiple vaccines and AE(V|X) >> 0 for other vaccines, then there are vaccine-associated AEs for the second set of vaccines. If two different lots for the same vaccine exhibit significant differences, these differences are likely due to intentional changes by the manufacturer to one or more of or .
2.3. Manufacturing Contamination Signature Identification
The VAERS AE reports from 1990 to May 30, 2025, were examined to identify candidate patterns for manufacturing contamination signatures. The approach focused upon previously published COVID-19 Moderna and Pfizer BioNTech lots with high and low normalized frequencies for menstrual AEs frequencies levels [17]. The second approach leveraged differences in normalized frequencies between the three HPV vaccines. The HPV Cervarix bivalent vaccine has the most menstrual AEs. HPV Gardasil, a quadrivalent vaccine, has the second-most menstrual AEs. And HPV Gardasil 9, a nonavalent vaccine, has fewer menstrual AEs. Candidate AEs were identified for patterns from comparisons between HPV Cervarix vs. Gardasil, HPV Cervarix vs. HPV Gardasil 9, and HPV Gardasil vs. HPV Gardasil 9. Identified AEs were characterized across all vaccines, with inclusion for vaccines with normalized frequency at or above 200 per 100,000 VAERS reports.
The COVID-19 Pfizer-BioNTech vaccine lots FG2975, FE3064, and FG7372 were identified with predicted higher levels of manufacturing contamination, and lots EJ6136, EJ6788, and EJ695 were identified with predicted lower levels [17]. The COVID-19 Moderna vaccine lot 3002332 was identified with the highest level of predicted manufacturing contamination, and lots 004M20A, 012L20A, and 013L20A were identified with predicted lower levels [17]. For each VAERS AE, the average of the low lots was subtracted from the high lots. Within the top 100 AEs with the highest differences between the high and low averages, multiple gynecologic AEs were identified. For improved assessments of normalized frequencies, the VAERS AEs were also examined by male and female genders.
Previously, menstrual AEs were identified with candidate manufacturing contamination signatures for three HPV vaccines [17]. The next approach examined differences in normalized frequencies between pairs of HPV vaccines based upon their different patterns of menstrual AEs [17]. First, additional candidate AEs for manufacturing contamination were selected by subtracting normalized frequencies for HPV Gardasil 9 from HPV Gardasil for females; the AEs identified include abortion induced, “caesarean section”, cognitive disorder, fetal disorder, menorrhagia, orthostatic intolerance, postural orthostatic tachycardia syndrome (POTS), and smear cervix abnormal. Second, additional candidate AEs for manufacturing contamination were selected from the sort of HPV Cervarix normalized frequencies: autonomic nervous system imbalance, chronic fatigue syndrome, complex regional pain syndrome (CRPS), mental impairment, “post vaccination syndrome”, and POTS. Given the current female bias in HPV vaccines administered, only the female gender AE normalized frequencies were examined.
3. Results
3.1. COVID-19 Vaccine Candidate Manufacturing Contamination Patterns
For both the COVID-19 Pfizer-BioNTech and the Moderna vaccines, AEs with rankings in the top 100 for females, males, and both genders are illustrated in Figure 1. Candidate vaccine manufacturing contamination pattern signatures were identified for females (MChemorrhage pattern and MCgynecologic pattern including the hemorrhage pattern) and males (MCmyopericarditis pattern) (Figure 2). The candidate hemorrhage pattern was detected for the six vaccines (Figure 2A) that did not include elevated menstrual AEs. The pulmonary embolism AE safety signals were detected for seven of 14 candidate myopericarditis pattern vaccines (anthrax Biothrax, five COVID-19, and smallpox Dryvax).
Examining normalized frequencies by lot can identify candidate safety signals. For the COVID-19 Janssen vaccine, six lots have detected hemorrhage safety signals, including lot 1822809 (5 AEs, 0.7%) (Supplemental Table S1). For the COVID-19 Moderna vaccine, 16 lots have detected hemorrhage safety signals, including lots 3002621 (14 AEs, 1.6%), 3002332 (18 AEs, 1.6%), and 3001659 (7 AEs, 0.9%) (Supplemental Table S2). For the COVID-19 Pfizer-BioNTech vaccine, 124 lots have detectable hemorrhage safety signals, including lots EP6775 (13 AEs, 6.4%), FA9090 (4 AEs, 4.3%), EY5456 (13 AEs, 3.6%), and FE3380 (36 AEs, 3.1%) (Supplemental Table S3). For AE myocarditis, the COVID-19 Janssen vaccine lots ABZ5320 (6 AEs, 2.1%), XD395 (5 AEs, 2.1%), ABZ8354 (4 AEs 3.4%), and 1821286 (4 AEs, 0.8%), and 2 additional lots have detectable safety signals (Supplemental Table S4); the COVID-19 Moderna vaccine lots 052C2A1 (4 AEs, 80.0%), 045D21A (30 AEs, 63.8%), 044D21A (37 AEs, 63.7%), 092D21A (30 AEs, 60.0%), 042D21A (34 AEs, 50.7%), 016E21A (19 AEs, 50.0%), 043D21A (24 AEs, 49.0%), 093D21A (18 AEs, 43.9%), 3002182 (8 AEs, 40.0%), and 179 additional lots have detectable safety signals (Supplemental Table S5); and the COVID-19 Pfizer-BioNTech lots 1E027A (20 AEs, 40.0%), 1E023-1A (12 AEs, 37.5%), FG9984 (13 AEs, 36.1%), FA9099 (56 AEs, 30.9%), ER0866 (15 AEs, 30.6%), FD7206 (44 AEs, 24.4%), and 462 additional lots have detectable safety signals (Supplemental Table S6). For AE pericarditis, the COVID-19 Janssen vaccine lots XD974 (6 AEs, 0.5%), 042A21A (6 AEs, 0.2%), 201A21A (6 AEs, 0.3%), 1805029 (4 AEs, 0.2%), and 205A21A (4 AEs, 0.2%) have detectable safety signals (Supplemental Table S7); the COVID-19 Moderna vaccine lots 019J21A (4 AEs, 30.8%), 042D21A (14 AEs, 20.9%), 3002182 (4 AEs, 20.0%), 3002187 (4 AEs, 19.0%), 044D21A (11 AEs, 19.0%), and 101 additional lots have detectable safety signals (Supplemental Table S8); the COVID-19 Pfizer-BioNTech vaccine lots FL3210 (7 AEs, 23.3%), FA9091 (38 AEs, 22.9%), FA9094 (19 AEs, 21.6%), FA9099 (38 AEs, 21.0%), FD7206 (37 AEs, 20.6%), EY0578 (28 AEs, 20.4%), and 373 additional lots have detectable safety signals (Supplemental Table S9).
3.2. HPV Vaccine Candidate Manufacturing Contamination Patterns
For HPV vaccines, three groups of candidate patterns: HPV, neuropathy, and fetus were identified, see Figure 3. Four candidate MCHPV patterns all appear in HPV Cervarix, two in HPV Gardasil, one in HPV Gardasil 9, and one in DTP Tri-Immunol vaccines, see Figure 3A. The candidate MCneuropathy patterns are illustrated in Figure 3B; the normalized frequency for cognitive disorder for HIB (Tetracoq) of 53,333 per 100,000 (based on 8 AEs of 15 VAERS reports) was not shown due to a high value. In addition to the MChemorrhage and MCgynecologic patterns that include abortion spontaneous, the MCfetus pattern includes “abortion induced”, caesarean section, and fetal disorder (Figure 3C). Note that the MCfetus pattern is not identified in any COVID-19 vaccines. The majority of the HPV Cervarix lots had fewer than 50 total AEs reported; lots AHPVA161BA and AHPVA16AA are examples with multiple reports for multiple AEs identified in Figure 3.
Safety signals can be detected for individual lots for multiple AEs for these HPV patterns. For AE smear cervix abnormal, the HPV Gardasil lots 1448U (5 AEs, 4.95% in females), 1967U (5 AEs, 4.5%), 1448U (5 AEs, 5.0%), 1060U (4 AEs, 2.9%), 1061U (4 AEs, 3.4%), and 1757U (4 AEs, 3.8%) have detectable safety signals. For AE orthostatic intolerance, the HPV Cervarix lots AHPVA149BA (5 AEs, 16.1% in females), AHPVA161BA (5 AEs, 10.6%), AHPVA164BB (4 AEs, 12.5%), and AHPVA143BA (4 AEs, 8.2%) have detectable safety signals. For AE post vaccination syndrome, the HPV Cervarix lots AHPVA162AA (9 AEs, 22.5%), AHPVA149BA (8 AEs, 25.8%), AHPVA161BA (7 AEs, 14.9%), AHPVA164BB (7 AEs, 21.9%), AHPVA149AA (6 AEs, 26.1%), AHPVA156AB (6 AEs, 33.3%), AHPVA123BA (5 AEs, 38.5), AHPVA138BA (4 AEs, 8.7%), AHPVA162DA (4 AEs, 13.3%), AHPVA148BA (4 AEs, 17.4%), and AHPVA143BA (4 AEs, 8.2%) have detectable safety signals. For AE autonomic nervous system imbalance, the HPV Cervarix lots AHPVA164AA (4 AEs, 11.1%) and AHPVA161BA (4 AEs, 8.5%) have detectable safety signals. For AE chronic fatigue syndrome, the HPV Cervarix lot AHPVA161BA (4 AEs, 8.5%) has a detectable safety signal. Note that the HPV Cervarix lot AHPVA161BA was detected for two MCHPV, two MCneuropathy, and mental impairment (4 AEs, 8.5%) patterns for safety signals.
For AE abortion induced, HPV Gardasil lot 0243U (4 AEs, 9.1%) has a detected safety signal. By age bins, abortion induced safety signals are detected for HPV Cervarix for ages 11 to 20 (17 AEs, 0.6%) and ages 21 to 30 (5 AEs, 2.3%), HPV Gardasil for ages 11 to 20 (101 AEs, 0.4%), ages 21 to 30 (49 AEs, 0.9%), and ages 31 to 40 (4 AEs, 0.7%). For AE caesarean section, RSV Abrysvo lot HR4961 (5 AEs, 25.0%), HPV Gardasil lot 0523U (5 AEs, 4.6%), and the Influenza seasonal Flucelvax quadrivalent lots 252664 (13 AEs, 13.0%), 252232 (9 AEs, 30.0%), and 261218 (5 AEs, 31.3%) have detectable safety signals.
3.3. Identified Fetal Adverse Events
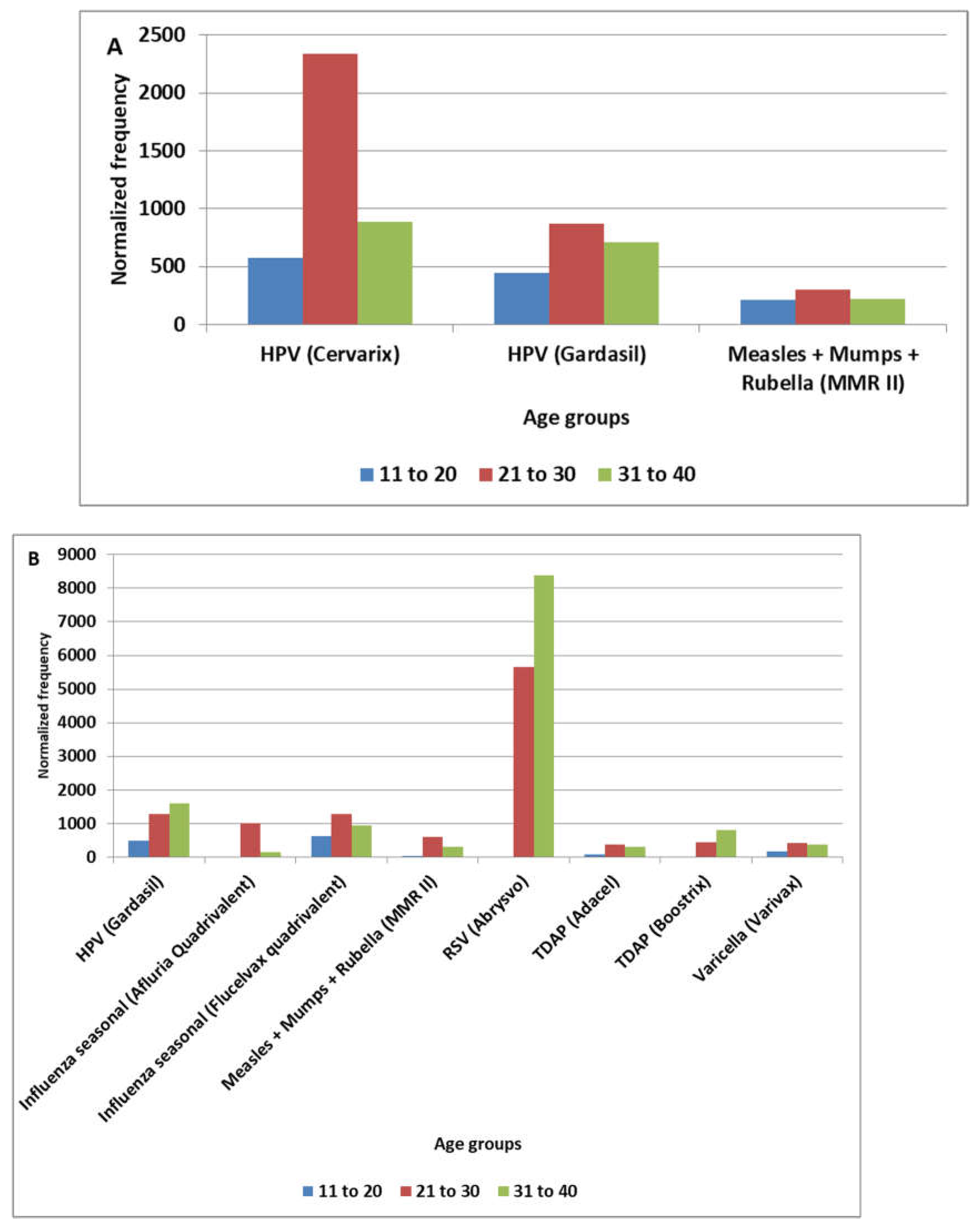
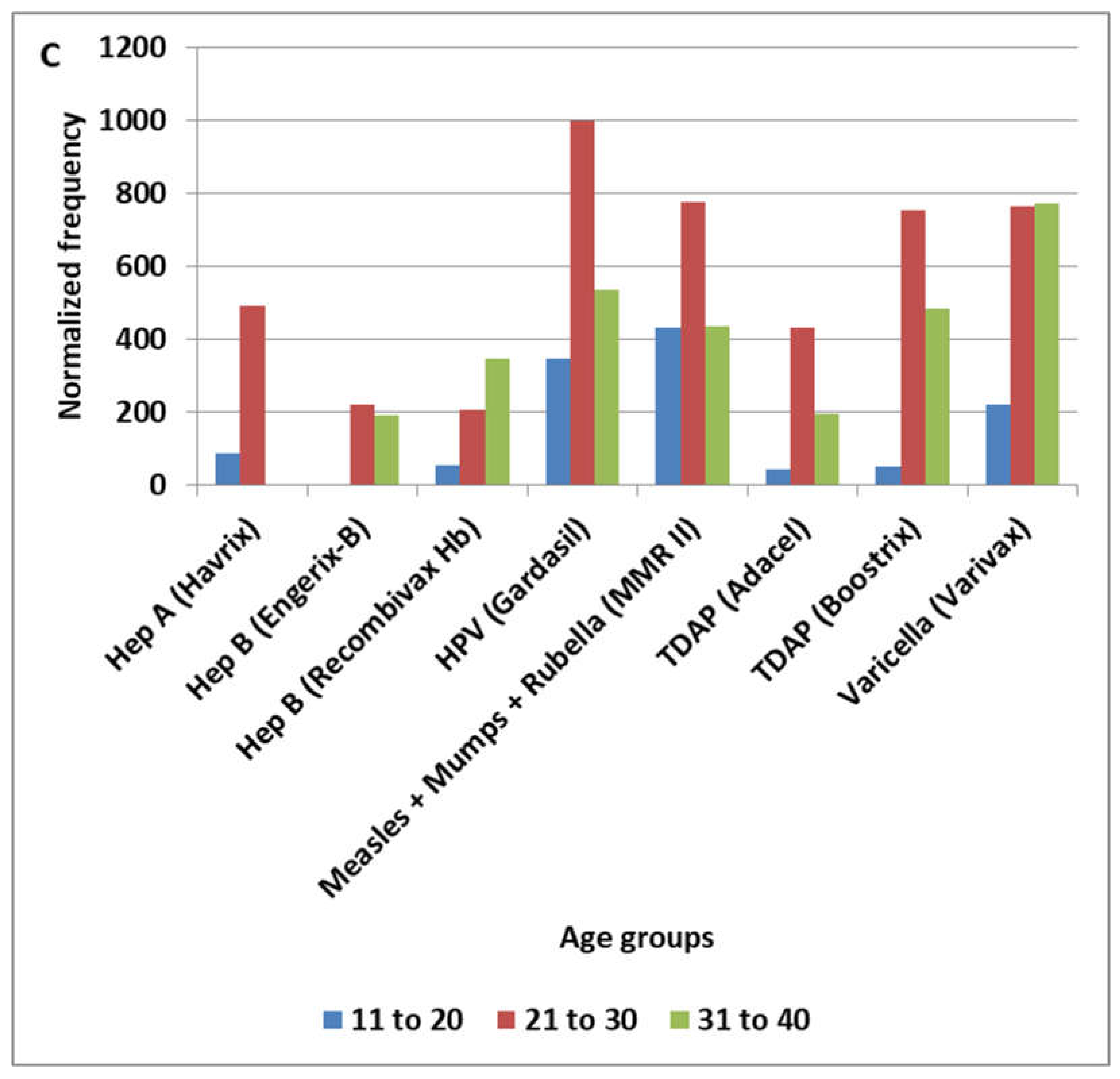
The four adverse events (abortion induced, abortion spontaneous, caesarean section, and fetal disorder) are relevant to females of reproductive age; calculating normalized frequencies including females of non-reproductive age is expected to lower the values calculated. For comparison purposes, AEs are considered by three age groups (11 to 20, 21 to 30, and 31 to 40) for abortion induced (Figure 4A), abortion spontaneous (Supplemental Table S10), caesarean section (Figure 4B), and fetal disorder (Figure 4C). Vaccines with too few adverse events by age group were excluded.
4. Discussion
4.1. Candidate Manufacturing Contamination Patterns
The candidate manufacturing contamination of specific COVID-19 BioNTech and COVID-19 Moderna lots was identified from statistically significant differences in normalized frequencies for COVID-19 and HPV vaccines for menstrual AEs [17]. Batch-dependent variability of AEs has been reported for the BNT162b2 mRNA COVID-19 vaccine [15,16]. Rank ordering AEs for both COVID-19 vaccines and focusing upon AEs shared for females, males, and both genders (Figure 1) identified additional candidate AEs potentially linked to putative manufacturing contaminants in these COVID-19 vaccines. Gender-specific normalized frequencies were calculated for these AEs for all vaccines in VAERS. AE normalized frequency results across all vaccines were consistent with two female-specific and one male-enriched candidate vaccine manufacturing contamination pattern signatures (Figure 2). Three additional candidate manufacturing patterns were identified from HPV Cervarix and HPV Gardasil vaccine data (Figure 3). Endotoxins are one possible manufacturing contaminant. Endotoxin content varying by vaccine batches has been reported for the Haemophilus influenzae type b (Hib) vaccine [24].
A subset of the AEs identified in the MChemorrhage, MCgynecologic, MCmyopericarditis, MCHPV, MCneuropathy, and MCfetus patterns may be linked to specific vaccine components (C) or excipients (E) and not manufacturing contaminants (MC). None of the identified AEs are candidates for population background (B) events based on elevated normalized frequencies not observed for any other vaccines.
4.2. MChemorrhage Pattern
The candidate hemorrhage, MChemorrhage pattern, matches six vaccines (Figure 2A); it includes the AEs abortion spontaneous, contusion, hemorrhage, and vaginal hemorrhage. Note that the RSV Abrysvo only has elevated AEs for contusion and vaginal hemorrhage (caesarean section). Consistent with these results, rare cases of vaccine-induced immune thrombotic thrombocytopenia (VITT) have been reported associated with the Oxford-AstraZeneca adenovirus COVID-19 vaccine [25,26] linked to anti-platelet factor 4 (PF4) antibodies [27,28]. Cases have been reported of hemorrhage associated with the Moderna [29,30,31,32] and the Pfizer-BioNTech [32,33,34,35] vaccines. These mRNA COVID-19 hemorrhage cases are consistent with the reported hemorrhage data in Figure 1A. A case of suspected pulmonary hemorrhage associated with the monovalent H1N1 vaccine has been reported [36]; this case report aligns with the MChemorrhage pattern in Figure 2A. Aside from COVID-19 adenovirus-associated thrombocytopenia, hemorrhage safety signals are detectable for other COVID-19 vaccines in the VAERS database.
4.3. MCgynecologic Pattern
The candidate gynecologic, MCgynecologic pattern, matches eight AEs for seven vaccines (Figure 2B); this study builds upon these previously identified associations [17]. Spontaneous abortion signal has also been detected for HPV bivalent (2vHPV) and nonavalent (9vHPV) HPV vaccines [37]. A study of 638 women receiving HPV quadrivalent (4vHPV) during pregnancy found no adverse pregnancy or birth outcomes [38]. A retrospective study of 2800 women receiving HPV quadrivalent (4vHPV) during pregnancy was not significantly correlated to an increased risk for spontaneous abortion [39]. No association with spontaneous abortion and adverse birth outcomes was identified for the 9-valent HPV vaccine [40]. While these studies did not detect any safety signals associated with HPV vaccines based upon these population samples, this study detected safety signals in the VAERS database data associated with the MCgynecologic pattern.
4.4. MCmyopericarditis Pattern
Myocarditis and pericarditis are well-known COVID-19 mRNA vaccine-associated AEs [41,42,43,44,45,46,47,48,49,50,51,52]. The candidate male-enriched myopericarditis, MCmyopericarditis pattern, matches 14 vaccines (Figure 2C). For the smallpox vaccines, the normalized frequencies were calculated using the total number of all AEs reported to VAERS for males (ACAM2000 n=2,260, Dryvax n=2,280, and Jynneos n=1,722) with observed differences consistent with manufacturing contaminants (Figure 2C). For smallpox ACAM2000 AE reports in VAERS for males, the myocarditis normalized frequency was 13,318 per 100,000 VAERS reports (1 in 7.5), and the pericarditis normalized frequency was 10,265 per 100,000 VAERS reports (1 in 9.7) (Figure 2C).
4.5. MCHPV Pattern
The MCHPV candidate pattern includes complex regional pain syndrome (CRPS), orthostatic intolerance (OI), post vaccination syndrome (PVS), and smear cervix abnormal AEs (Figure 3A). Orthostatic intolerance is an AE where a vaccinee experiences symptoms like dizziness, lightheadedness, or fatigue when standing up, which are relieved by sitting or lying down. A case of PVS has been reported following HPV Cervarix vaccination [53]. Three overlapping reports describe multiple Japanese patients with orthostatic intolerance, chronic regional pain syndrome (CRPS), and/or cognitive dysfunction following HPV Cervarix or HPV Gardasil vaccination [54,55,56]. These four AEs occur with higher frequencies for one or more of the HPV vaccines, all four AEs for HPV Cervarix, and with only PVS also having a detectable signal for DTP Tri-Immunol.
4.6. MCneuropathy Pattern
The MCneuropathy candidate pattern includes autonomic nervous system imbalance, chronic fatigue syndrome, cognitive disorder, mental impairment, and postural orthostatic tachycardia syndrome (POTS) (Figure 3B). POTS AEs are only evident in the HPV Cervarix, HPV Gardasil, HPV Gardasil 9, and COVID-19 Novavax vaccines.
4.7. Abortion Spontaneous AEs and MCfetus Pattern
Since 2021, the United States Centers for Disease Control and Prevention (CDC) states, “COVID-19 vaccination before and during pregnancy is safe, effective, and beneficial to both the pregnant woman and the baby” [57]. The observed normalized frequencies for abortion spontaneous were 455 per 100,000 VAERS reports for COVID-19 Pfizer-BioNTech, 263 per 100,000 for COVID-19 Janssen, and 234 per 100,000 for COVID-19 Moderna vaccines. Lower abortion spontaneous normalized frequencies were observed for the COVID-19 Pfizer-BioNTech bivalent (45 per 100,000 VAERS reports) and the COVID-19 Moderna bivalent (97 per 100,000 VAERS reports) vaccines. A subset of the age group safety signals detected for spontaneous abortion (Supplemental Table S10) may have other causative factors other than manufacturing contaminants. The MCfetus candidate pattern includes abortion induced, caesarean section, and fetal disorder AEs (Figure 3C & 4). The normalized frequencies for these three AEs are calculated based on the total of all AEs reported by females associated with these vaccines – not pregnant females. The normalized frequencies would be higher if the pregnancy status of females were known for these VAERS AE reports and used as the denominator in these normalized frequency calculations; this also applies to the abortion spontaneous AEs included in the MChemorrhage and MCgynecologic patterns (Figure 2). The group of AEs by age groups is shown in Figure 4. While the above CDC claim may be true for COVID-19 vaccines in general, it may be incorrect for lots with predicted higher levels of manufacturing contaminants. Endotoxins are one candidate group of manufacturing contaminants that are worthy of characterization in the identified COVID-19 lots [17].
4.8. Endotoxins – Lipopolysaccharides - Pyrogens
Lipopolysaccharides (LPS), also known as endotoxins or pyrogens, are constituents of the outer membrane of gram-negative bacteria. Endotoxins are a common manufacturing contaminant of vaccines. Detected levels of endotoxins can vary widely by vaccine [58,59]. Endotoxins can disrupt female reproductive function [60]. Reiterating Geier et al., “Selection of vaccine lots with the least endotoxin might reduce some of the adverse effects of vaccinations” [58]. Nanoparticles should be manufactured under endotoxin-free conditions [61]. Endotoxins are possible manufacturing contaminant candidates to confirm or exclude in future studies for the identified lots.
4.9. Study Limitations
This is an exploratory study examining candidate manufacturing contaminants’ safety signatures following immunization. AEFIs can represent background AEs plus possible vaccine-associated AEs and possible manufacturing contaminants AEs. The evidence herein identifies candidate safety signals and does not establish causality for associated AEs. Based on the observed patterns of safety signals, candidate vaccines are identified for future studies of possible vaccine manufacturing contaminants. The predicted manufacturing contaminants have not been identified yet.
5. Conclusions
This study identified six candidate manufacturing contamination signature patterns: MChemorrhage, MCgynecologic, MCmyopericarditis, MCHPV, MCneuropathy, and MCfetus patterns. Future studies could identify the causative agents correlated to these patterns to reduce these causative agents within vaccines, thereby reducing associated AEs and SAEs.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
This research was unfunded.
Data Availability Statement
Ricke, Darrell, 2025, "Candidate vaccine manufacturing contamination adverse events signatures", https://doi.org/10.7910/DVN/3BT4JR, Harvard Dataverse, V1.
Conflicts of Interest
The authors declare they have no competing interests.
References
- Matar SG, Nourelden AZ, Assar A, et al. Effect of COVID-19 vaccine on menstrual experience among females in six Arab countries: A cross sectional study. Influenza Other Respir Viruses. 2023;17(1):e13088. [CrossRef]
- Baena-García L, Aparicio VA, Molina-López A, Aranda P, Cámara-Roca L, Ocón-Hernández O. Premenstrual and menstrual changes reported after COVID-19 vaccination: The EVA project. Womens Health. 2022;18:17455057221112237. [CrossRef]
- Rastegar T, Feryduni L, Fakhraei M. COVID-19 vaccine side effects on menstrual disturbances among Iranian women. New Microbes New Infect. 2023;53:101114. [CrossRef]
- Dabbousi AA, El Masri J, El Ayoubi LM, Ismail O, Zreika B, Salameh P. Menstrual abnormalities post-COVID vaccination: a cross-sectional study on adult Lebanese women. Ir J Med Sci 1971 -. 2023;192(3):1163-1170. [CrossRef]
- Lee KM, Junkins EJ, Luo C, Fatima UA, Cox ML, Clancy KB. Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. medRxiv. 2022. [CrossRef]
- Trogstad L, Laake I, Robertson AH, et al. Heavy bleeding and other menstrual disturbances in young women after COVID-19 vaccination. Vaccine. 2023;41(36):5271-5282. [CrossRef]
- Almomani EY, Hajjo R, Qablan A, Sabbah DA, Al-Momany A. A cross-sectional study confirms temporary post-COVID-19 vaccine menstrual irregularity and the associated physiological changes among vaccinated women in Jordan. Front Med. 2023;10. [CrossRef]
- Duijster JW, Schoep ME, Nieboer TE, Jajou R, Kant A, van Hunsel F. Menstrual abnormalities after COVID-19 vaccination in the Netherlands: A description of spontaneous and longitudinal patient-reported data. Br J Clin Pharmacol. 2023;89(10):3126-3138. [CrossRef]
- Laganà AS, Veronesi G, Ghezzi F, et al. Evaluation of menstrual irregularities after COVID-19 vaccination: Results of the MECOVAC survey. Open Med. 2022;17(1):475-484. [CrossRef]
- Muhaidat N, Alshrouf MA, Azzam MI, Karam AM, Al-Nazer MW, Al-Ani A. Menstrual Symptoms After COVID-19 Vaccine: A Cross-Sectional Investigation in the MENA Region. Int J Womens Health. 2022;14:395-404. [CrossRef]
- Al-Furaydi A, Alrobaish SA, Al-Sowayan N. The COVID-19 vaccines and menstrual disorders. Eur Rev Med Pharmacol Sci. 2023;27(3):1185-11911. [CrossRef]
- Khan GA, Althubaiti A, Alshrif A, Alsayed Z, Jifree H. Dysmenorrhea, intermenstrual bleeding, menstrual flow volume changes, and irregularities following COVID-19 vaccination and the association with vaccine skepticism: A retrospective observational study. Womens Health. 2023;19:17455057231210094. [CrossRef]
- Li K, Chen G, Hou H, et al. Analysis of sex hormones and menstruation in COVID-19 women of child-bearing age. Reprod Biomed Online. 2021;42(1):260-267. [CrossRef]
- Blix K, Laake I, Juvet L, et al. Unexpected vaginal bleeding and COVID-19 vaccination in nonmenstruating women. Sci Adv. 9(38):eadg1391. [CrossRef]
- Schmeling M, Manniche V, Hansen PR. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur J Clin Invest. 2023;53(8):e13998. [CrossRef]
- Manniche V, Schmeling M, Gilthorpe JD, Hansen PR. Reports of Batch-Dependent Suspected Adverse Events of the BNT162b2 mRNA COVID-19 Vaccine: Comparison of Results from Denmark and Sweden. Medicina (Mex). 2024;60(8). [CrossRef]
- Ricke DO. Menstrual adverse events post-COVID-19 and human papillomavirus immunization. Microbes Immun. 2025. [CrossRef]
- Wastila L, Fu YH, Tung CC, Qato DM. Association Between Vaccination for Human Papillomavirus (HPV) and Autonomic Dysfunction and Menstrual Irregularities: A Self-Controlled Case Series Analysis. Drugs Real World Outcomes. 2025;12(3):467-477. [CrossRef]
- Little DT, Ward HRG. Adolescent Premature Ovarian Insufficiency Following Human Papillomavirus Vaccination: A Case Series Seen in General Practice. J Investig Med High Impact Case Rep. 2014;2(4):2324709614556129. [CrossRef]
- Gong L, Ji H huan, Tang X wen, Pan L yun, Chen X, Jia Y tao. Human papillomavirus vaccine-associated premature ovarian insufficiency and related adverse events: data mining of Vaccine Adverse Event Reporting System. Sci Rep. 2020;10(1):10762. [CrossRef]
- VAERS. Vaccine Adverse Event Reporting System. U.S. Department of Health & Human Services; 2025. https://vaers.hhs.gov/data/datasets.html. Accessed June 20, 2025.
- Ricke DO. VAERS-Tools. 2022. https://github.com/doricke/VAERS-Tools. Accessed November 15, 2025.
- Ricke DO. Vaccine-associated Kawasaki disease in children. Microbes Immun. 2025. [CrossRef]
- Ochiai M, Kataoka M, Toyoizumi H, et al. Endotoxin Content in Haemophilus influenzae Type b Vaccine. Jpn J Infect Dis. 2004;57(2):58-59. [CrossRef]
- Wilting FNH, Kotsopoulos AMM, Platteel ACM, van Oers JAH. Intracerebral Hemorrhage and Thrombocytopenia After AstraZeneca COVID-19 Vaccine: Clinical and Diagnostic Challenges of Vaccine-Induced Thrombotic Thrombocytopenia. Cureus. 2021;13(9):e17637. [CrossRef]
- See I, Su JR, Lale A, et al. US Case Reports of Cerebral Venous Sinus Thrombosis With Thrombocytopenia After Ad26.COV2.S Vaccination, March 2 to April 21, 2021. JAMA. 2021;325(24):2448-2456. [CrossRef]
- Greinacher Andreas, Thiele Thomas, Warkentin Theodore E., Weisser Karin, Kyrle Paul A., Eichinger Sabine. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N Engl J Med. 2021;384(22):2092-2101. [CrossRef]
- Muir Kate-Lynn, Kallam Avyakta, Koepsell Scott A., Gundabolu Krishna. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. N Engl J Med. 2021;384(20):1964-1965. [CrossRef]
- Sharma A, Upadhyay B, Banjade R, Poudel B, Luitel P, Kharel B. A Case of Diffuse Alveolar Hemorrhage With COVID-19 Vaccination. Cureus. 2022;14(1):e21665. [CrossRef]
- Syed K, Chaudhary H, Donato A. Central Venous Sinus Thrombosis with Subarachnoid Hemorrhage Following an mRNA COVID-19 Vaccination: Are These Reports Merely Co-Incidental? Am J Case Rep. 2021. [CrossRef]
- Chen QT, Liu Y, Chen YC, et al. Case report: Vaccine-induced immune thrombotic thrombocytopenia complicated by acute cerebral venous thrombosis and hemorrhage after AstraZeneca vaccines followed by Moderna COVID-19 vaccine booster and surgery. Front Neurol. 2022;13. [CrossRef]
- Sugasawa S, Kimura T, Bae Y, Kumasaka T, Ichi S. Two Cases of Rare Intratumoral Hemorrhage Following COVID-19 Vaccination. Cureus. 2022;14(12):e32400. [CrossRef]
- Takeyama R, Fukuda K, Kouzaki Y, et al. Intracerebral hemorrhage due to vasculitis following COVID-19 vaccination: a case report. Acta Neurochir (Wien). 2022;164(2):543-547. [CrossRef]
- Hulscher N, McCullough PA. Delayed Fatal Pulmonary Hemorrhage Following COVID-19 Vaccination: Case Report, Batch Analysis, And Proposed Autopsy Checklist. Preprints. 2024. [CrossRef]
- Yangi K, Demir DD, Uzunkol A. Intracranial Hemorrhage After Pfizer-BioNTech (BNT162b2) mRNA COVID-19 Vaccination: A Case Report. Cureus. 2023;15(4):e37747. [CrossRef]
- Bhurayanontachai R. Possible life-threatening adverse reaction to monovalent H1N1 vaccine. Crit Care. 2010;14(3):422. [CrossRef]
- Zhang J, Lian Z, Xue X, et al. Does HPV vaccination during periconceptional or gestational period increase the risk of adverse pregnancy outcomes?—An updated systematic review and meta-analysis based on timing of vaccination. Acta Obstet Gynecol Scand. 2024;103(10):1943-1954. [CrossRef]
- Lipkind HS, Vazquez-Benitez G, Nordin JD, et al. Maternal and Infant Outcomes After Human Papillomavirus Vaccination in the Periconceptional Period or During Pregnancy. Obstet Gynecol. 2017;130(3). [CrossRef]
- Kharbanda EO, Vazquez-Benitez G, Lipkind HS, et al. Risk of Spontaneous Abortion After Inadvertent Human Papillomavirus Vaccination in Pregnancy. Obstet Gynecol. 2018;132(1). [CrossRef]
- Kharbanda EO, Vazquez-Benitez G, DeSilva MB, et al. Association of Inadvertent 9-Valent Human Papillomavirus Vaccine in Pregnancy With Spontaneous Abortion and Adverse Birth Outcomes. JAMA Netw Open. 2021;4(4):e214340-e214340. [CrossRef]
- Ricke DO. Cardiac adverse events post-vaccination. Brain Heart. 2025;3(2):1-15. [CrossRef]
- Montgomery J, Ryan M, Engler R, et al. Myocarditis Following Immunization With mRNA COVID-19 Vaccines in Members of the US Military. JAMA Cardiol. 2021;6(10):1202. [CrossRef]
- Kim HW, Jenista ER, Wendell DC, et al. Patients With Acute Myocarditis Following mRNA COVID-19 Vaccination. JAMA Cardiol. 2021;6(10):1196. [CrossRef]
- Marshall M, Ferguson ID, Lewis P, et al. Symptomatic Acute Myocarditis in 7 Adolescents After Pfizer-BioNTech COVID-19 Vaccination. Pediatrics. 2021;148(3):e2021052478. [CrossRef]
- Larson KF, Ammirati E, Adler ED, et al. Myocarditis After BNT162b2 and mRNA-1273 Vaccination. Circulation. 2021;144(6):506-508. [CrossRef]
- Rosner CM, Genovese L, Tehrani BN, et al. Myocarditis Temporally Associated With COVID-19 Vaccination. Circulation. 2021;144(6):502-505. [CrossRef]
- Ramírez-García A, Lozano Jiménez S, Darnaude Ximénez I, Gil Cacho A, Aguado-Noya R, Segovia Cubero J. Pericarditis after administration of the BNT162b2 mRNA COVID-19 vaccine. Rev Espanola Cardiol Engl Ed. 2021;74(12):1120-1122. [CrossRef]
- Das BB, Moskowitz WB, Taylor MB, Palmer A. Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination: What Do We Know So Far? Children. 2021;8(7):607. [CrossRef]
- Pepe S, Gregory AT, Denniss AR. Myocarditis, Pericarditis and Cardiomyopathy After COVID-19 Vaccination. Heart Lung Circ. 2021;30(10):1425-1429. [CrossRef]
- Hudson B, Mantooth R, DeLaney M. Myocarditis and pericarditis after vaccination for COVID-19. J Am Coll Emerg Physicians Open. 2021;2(4):e12498. [CrossRef]
- Diaz G, Parsons G, Gering S, Meier A, Hutchinson I, Robicsek A. Myocarditis and Pericarditis After Vaccination for COVID-19. JAMA. 2021;326(12):3.
- Lane S, Yeomans A, Shakir S. Reports of myocarditis and pericarditis following mRNA COVID-19 vaccination: a systematic review of spontaneously reported data from the UK, Europe and the USA and of the scientific literature. BMJ Open. 2022;12(5):e059223. [CrossRef]
- Poddighe D, Castelli L, Marseglia GL, Bruni P. A sudden onset of a pseudo-neurological syndrome after HPV-16/18 AS04-adjuvated vaccine: might it be an autoimmune/inflammatory syndrome induced by adjuvants (ASIA) presenting as a somatoform disorder? Immunol Res. 2014;60(2):236-246. [CrossRef]
- Ozawa K, Hineno A, Kinoshita T, Ishihara S, Ikeda S ichi. Suspected Adverse Effects After Human Papillomavirus Vaccination: A Temporal Relationship Between Vaccine Administration and the Appearance of Symptoms in Japan. Drug Saf. 2017;40(12):1219-1229. [CrossRef]
- Hineno A, Ikeda SI. A Long-Term Observation on the Possible Adverse Effects in Japanese Adolescent Girls after Human Papillomavirus Vaccination. Vaccines. 2021;9(8):856. [CrossRef]
- Kinoshita T, Abe R ta, Hineno A, Tsunekawa K, Nakane S, Ikeda S ichi. Peripheral Sympathetic Nerve Dysfunction in Adolescent Japanese Girls Following Immunization with the Human Papillomavirus Vaccine. Intern Med. 2014;53(19):2185-2200. [CrossRef]
- CDC. COVID-19 Vaccination for Women Who Are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html. Accessed August 1, 2025.
- Geier M R, Stanbro H, Merril C R. Endotoxins in commercial vaccines. Appl Environ Microbiol. 1978;36(3):445-449. [CrossRef]
- Brito LA, Singh M. COMMENTARY: Acceptable Levels of Endotoxin in Vaccine Formulations During Preclinical Research. J Pharm Sci. 2011;100(1):34-37. [CrossRef]
- Bidne KL, Dickson MJ, Ross JW, Baumgard LH, Keating AF. Disruption of female reproductive function by endotoxins. Reproduction. 2018;155(4):R169-R181. [CrossRef]
- Costa JP, Jesus S, Colaço M, Duarte A, Soares E, Borges O. Endotoxin contamination of nanoparticle formulations: A concern in vaccine adjuvant mechanistic studies. Vaccine. 2023;41(23):3481-3485. [CrossRef]
Figure 1.
Common top adverse events for COVID-19 Pfizer-BioNTech and Moderna vaccines for (A) common females adverse events, (B) common males adverse events, and (C) common adverse events for both genders.
Figure 1.
Common top adverse events for COVID-19 Pfizer-BioNTech and Moderna vaccines for (A) common females adverse events, (B) common males adverse events, and (C) common adverse events for both genders.
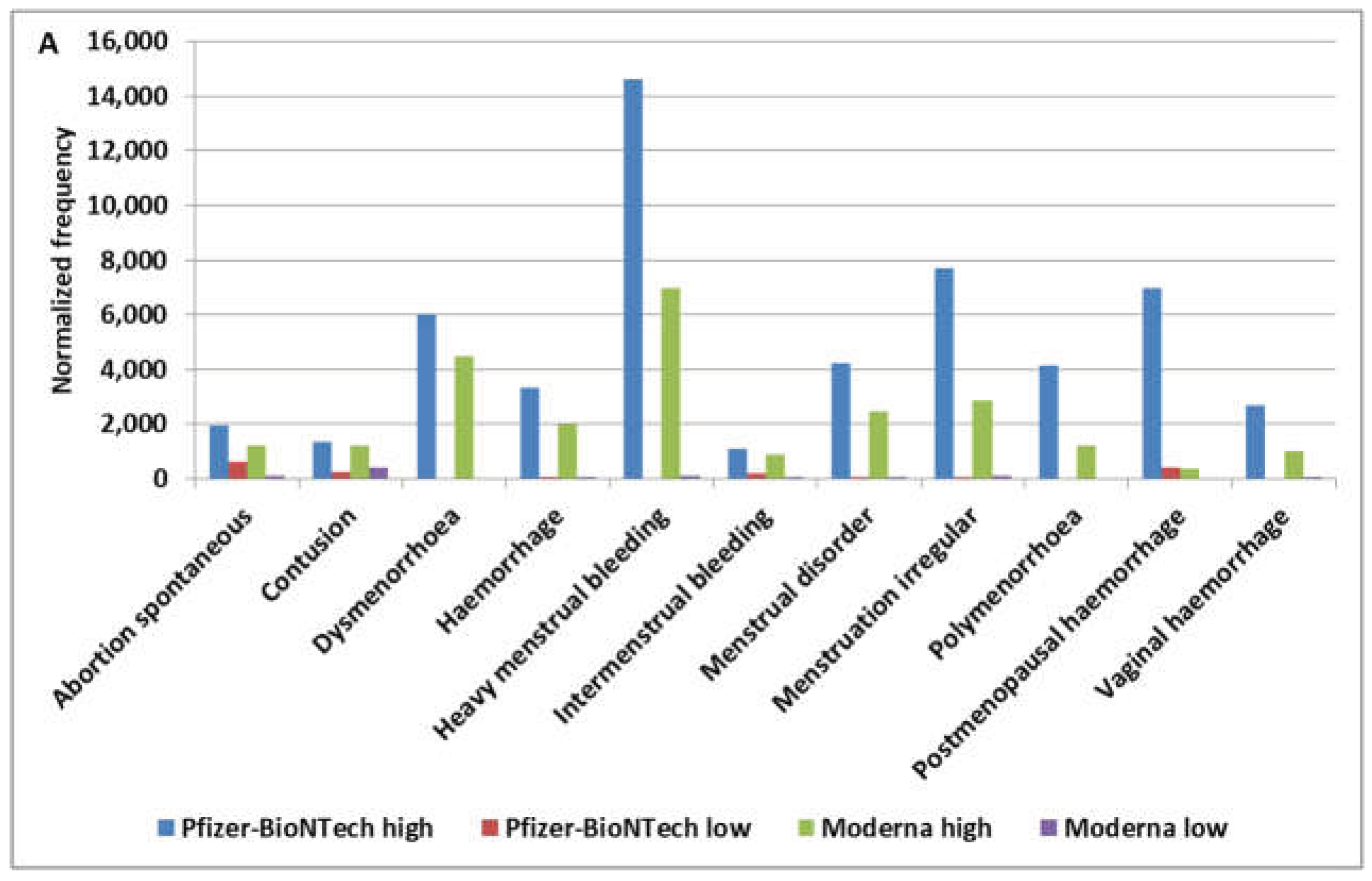
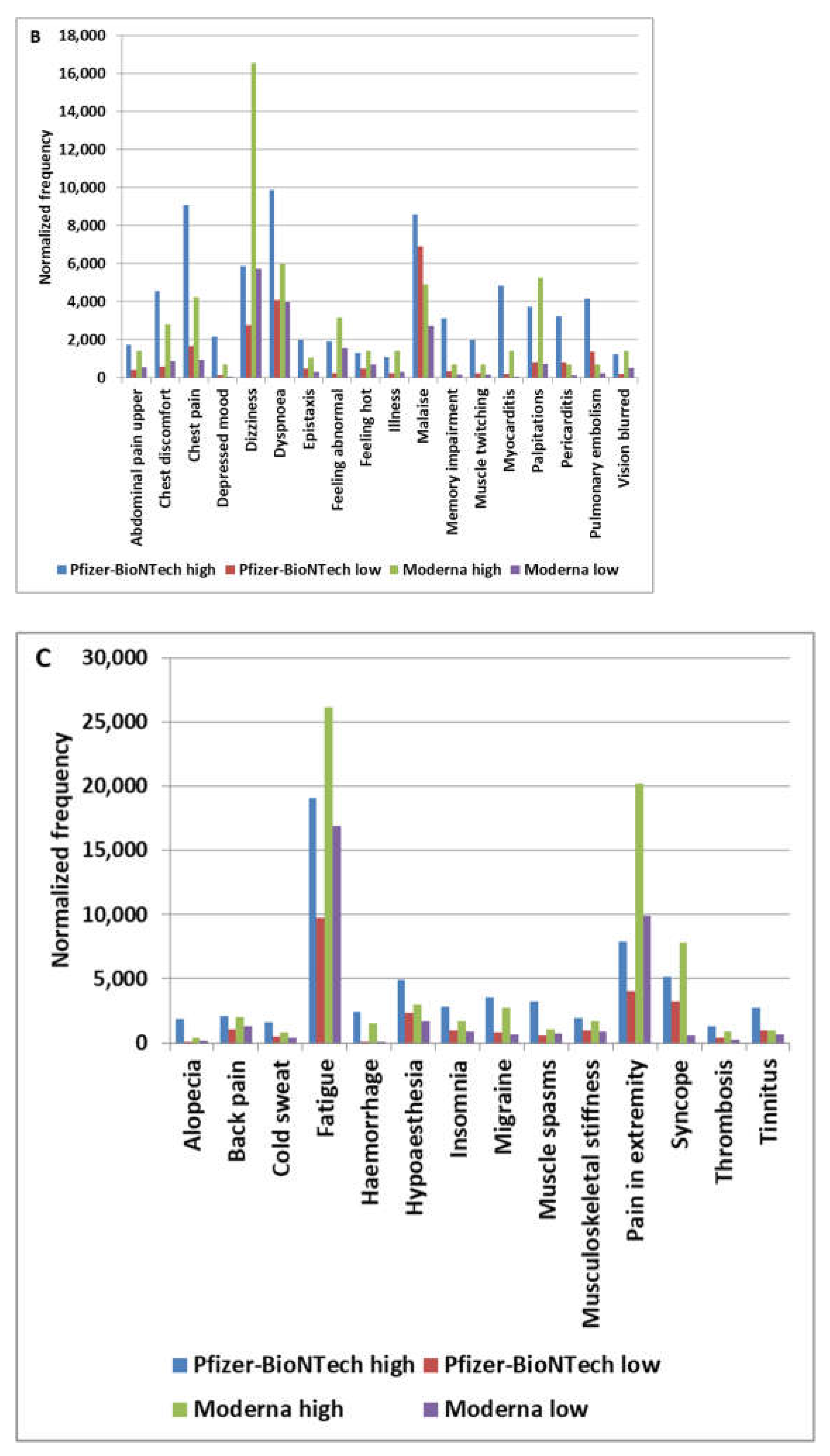
Figure 2.
Candidate vaccine manufacturing contamination candidate pattern signatures associated with (A) hemorrhage (female) manufacturing contamination candidate pattern, (B) gynecologic (including hemorrhage pattern) manufacturing contamination candidate pattern, and (C) male-enrichment adverse events manufacturing contamination candidate pattern.
Figure 2.
Candidate vaccine manufacturing contamination candidate pattern signatures associated with (A) hemorrhage (female) manufacturing contamination candidate pattern, (B) gynecologic (including hemorrhage pattern) manufacturing contamination candidate pattern, and (C) male-enrichment adverse events manufacturing contamination candidate pattern.
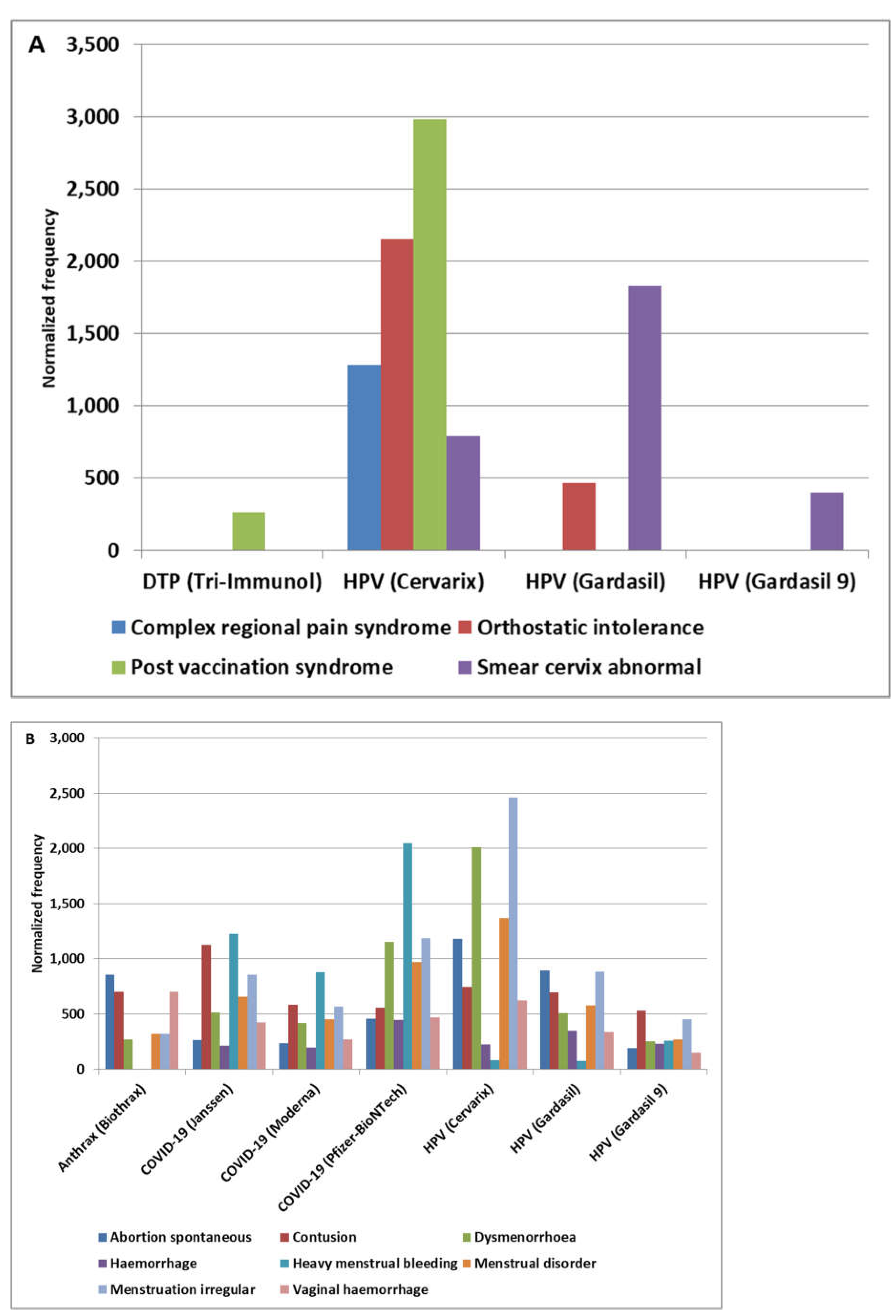
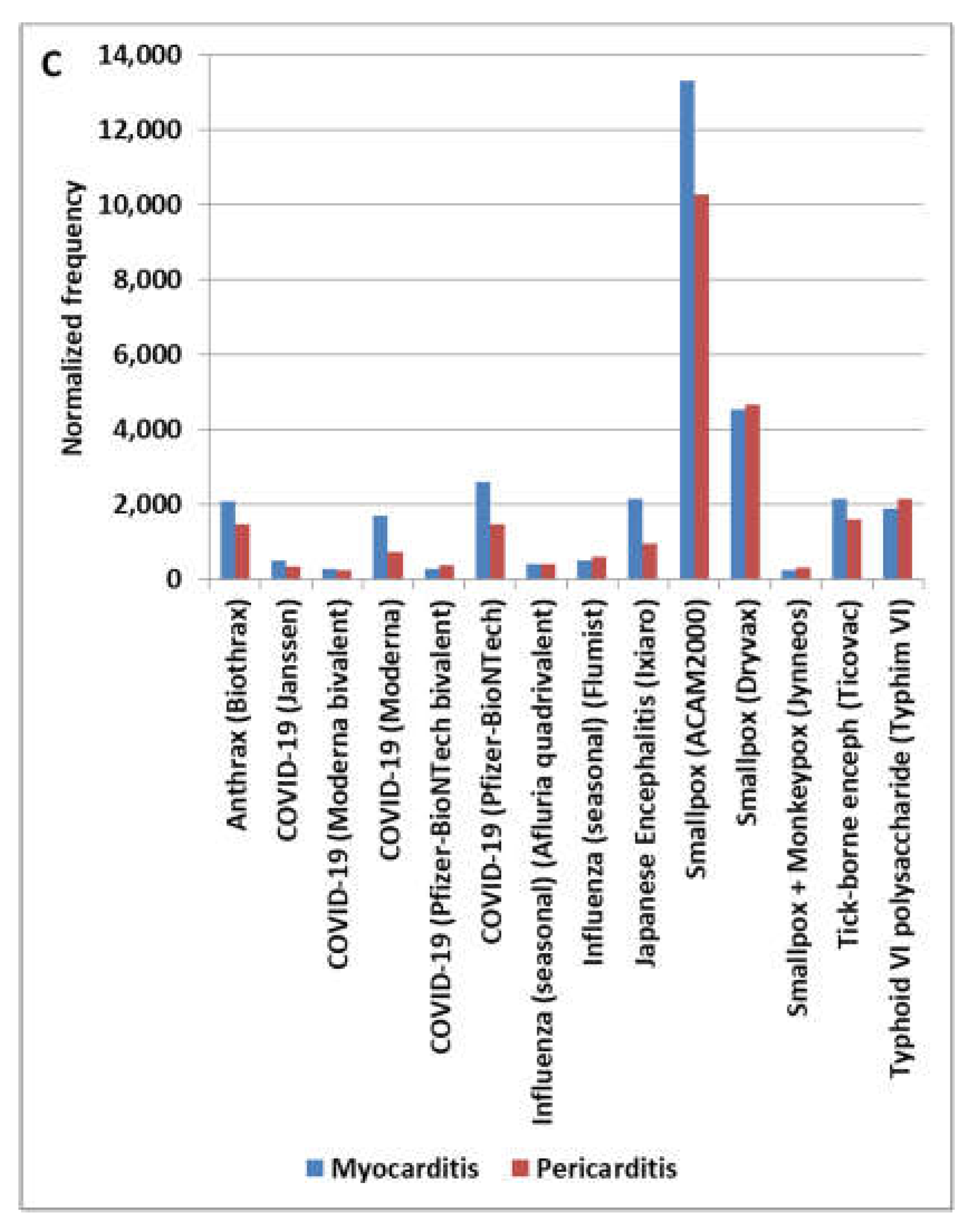
Figure 3.
Candidate vaccine manufacturing contamination pattern signatures associated with HPV Cervarix or HPV Gardasil vaccines in females (A) HPV vaccine manufacturing contamination candidate pattern, (B) neuropathy manufacturing contamination candidate pattern, and (C) fetus manufacturing candidate pattern. The normalized frequency for cognitive disorder for HIB (Tetracoq) of 53,333 per 100,000 (based on 8 AEs of 15 VAERS reports) was not shown due to a high value.
Figure 3.
Candidate vaccine manufacturing contamination pattern signatures associated with HPV Cervarix or HPV Gardasil vaccines in females (A) HPV vaccine manufacturing contamination candidate pattern, (B) neuropathy manufacturing contamination candidate pattern, and (C) fetus manufacturing candidate pattern. The normalized frequency for cognitive disorder for HIB (Tetracoq) of 53,333 per 100,000 (based on 8 AEs of 15 VAERS reports) was not shown due to a high value.
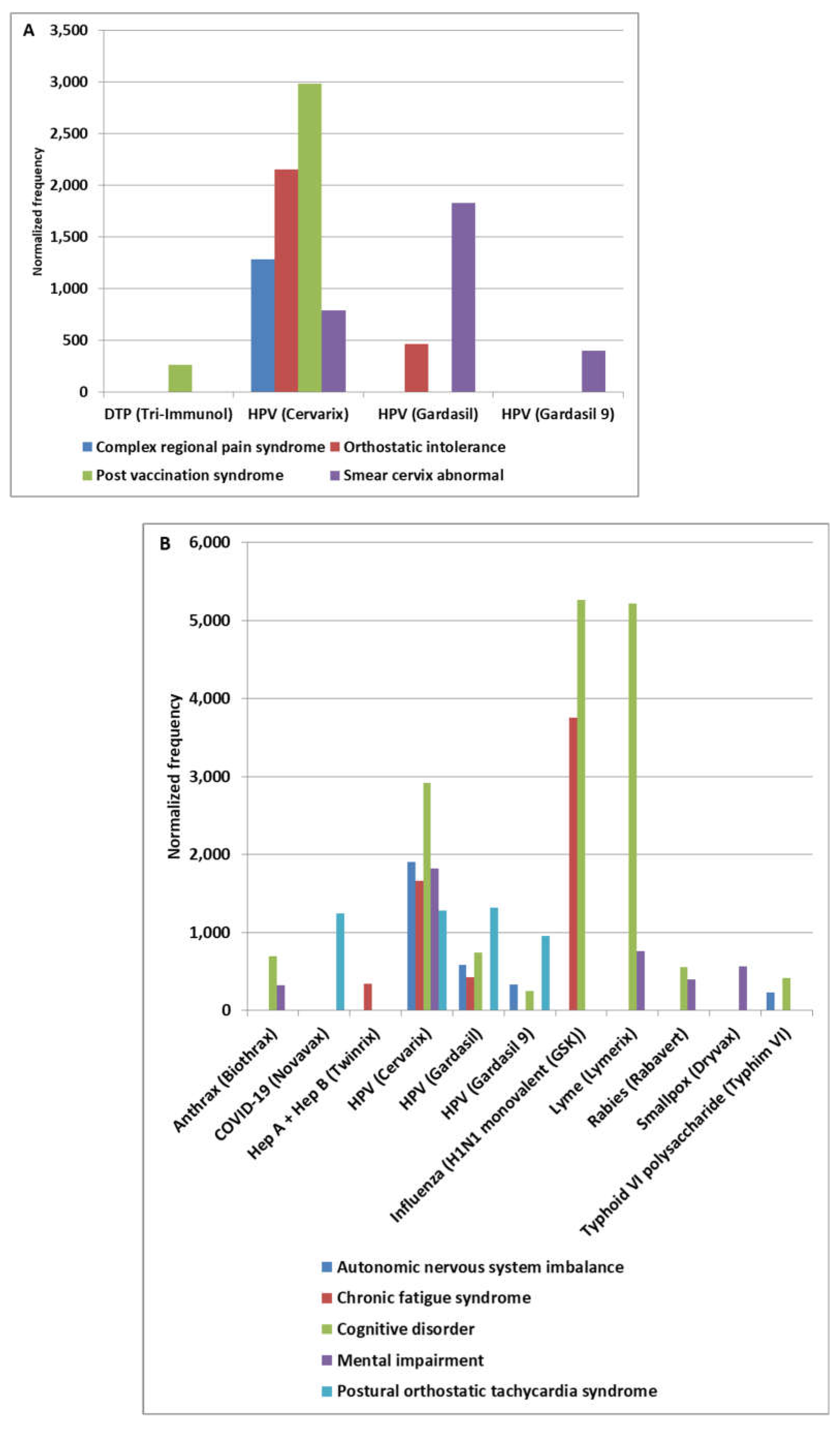
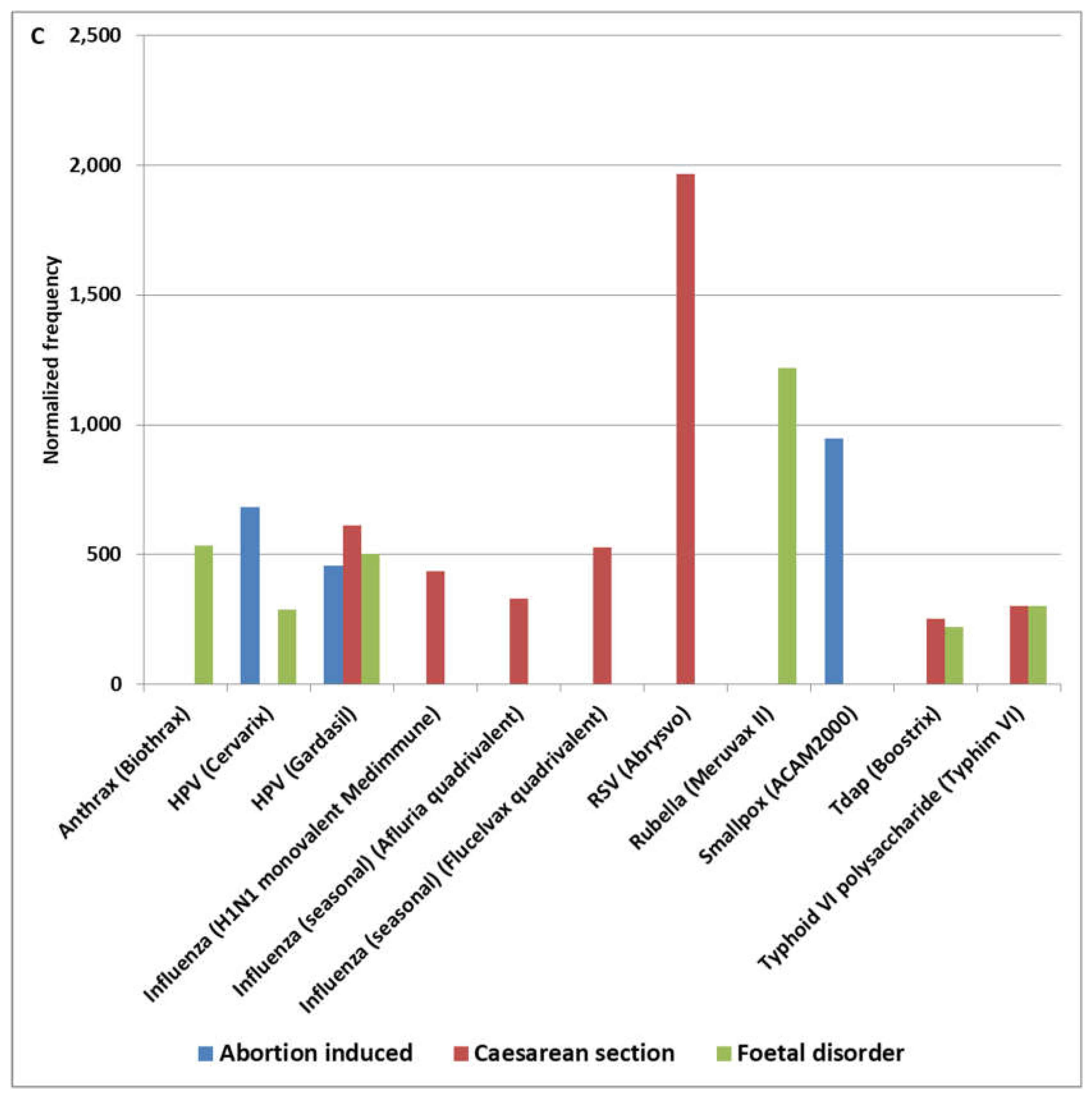
Figure 4.
Adverse events normalized frequencies by age group for (A) abortion induced, (B) caesarean section, and (C) fetal disorder.
Figure 4.
Adverse events normalized frequencies by age group for (A) abortion induced, (B) caesarean section, and (C) fetal disorder.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



