
Submitted:
22 February 2026
Posted:
28 February 2026
You are already at the latest version
Abstract
(1) Background This scoping review aimed to systematically map how non-technical care is conceptualised and practised within sport and exercise medicine (SEM), particularly in elite sport contexts. It explored perspectives of both SEM practitioners and athletes, focusing on relational attributes such as trust, communication, and practitioner characteristics that underpin non-technical care. (2) Methods: A scoping review was conducted following PRISMA-ScR guidelines and registered with the Open Science Framework. Three databases (PubMed, Sport Discus, ScienceDirect) were searched in August 2025, supplemented by hand searching. Eligibility criteria followed the PCC framework, including elite athletes and SEM practitioners, with a focus on non-technical care attributes. Twenty-three articles met the inclusion criteria. (3) Results Three overarching themes emerged: (1) Communication: Active listening, verbal/non-verbal strategies, and multidisciplinary dialogue; (2) Trust: Influenced by confidentiality, competence, and long-term relationships, though inconsistently defined; (3) Desired practitioner characteristics: Professional credibility, collaborative approaches, and personal attributes such as humility and empathy. Only one study referenced non-technical frameworks (therapeutic alliance and shared decision-making). (4) Conclusions: Non-technical care in SEM is primarily understood through trust and communication, yet lacks conceptual clarity and tailored frameworks. Findings highlight the need for models that integrate relational, ethical, and contextual dimensions of elite sport to support consistent, person-centred care.
Keywords:
care
; female athlete
; rugby
; sports medicine practitioners
1. Introduction
Care is a fundamental concept in healthcare, encompassing not only clinical interventions but also the relational, emotional, and ethical dimensions of practitioner-patient interactions. It has been defined in various ways. Donabedian [1] adopts a “humanitarian” perspective, emphasising identifying a fundamental purpose of care to elevate suffering. Krause and Boldt [2] discuss how it is both a descriptive concept and a normative orientation balancing optimal patient care with the demands of the institute and its limitations. In England, there is an independent regulator for health and adult care called the Care Quality Commission (CQC), which aims for everyone to receive “safe, effective and compassionate care” [3]. This view of care possesses two components: the technical focus of treatments and interventions, which must be safe and effective for the relevant patient group, and the non-technical attributes necessary for delivering compassionate care. Although both are essential to providing “high-quality care”, this paper concentrates on the non-technical aspects, exploring the attributes, definitions, and concepts that might exist within the elite sports setting to deliver compassionate care.
Sports and exercise medicine (SEM) practitioners are responsible for caring for the mental and physical health of athletes within a performance sports environment. SEM practitioners, often employed directly by sports organisations, manage athletes’ health to help them regain full fitness and return to competitive play. This involves the wider interdisciplinary team, including coaches who are also decision-makers for team selection [4]. It can leave SEM practitioners trying to balance the conflicting responsibilities of maintaining athlete confidentiality while and reporting to coaching staff any injuries or player performance concerns [5,6]. Consequently, athletes may withhold information due to concerns about selection or breaches of confidentiality [7,8]. In a study by White et al. [7], interviewing elite female rugby players, it was found that athletes questioned the care and trust they placed in the medical team. They reported being excluded from decisions affecting their health and their prospects of a successful return to play after significant injury, which impacted their identity both as athletes and individuals.
Although the current study retains a tight focus on care in SEM, we should be cognisant of the wider literature concerning care, with which SEM has had limited engagement. Significant theorists include Noddings [9] ethics of care which examines the inter-dependent reciprocal relationship between someone who is being cared for (an athlete) and their carer (the practitioner). Whereby there is a trusting relationship with cyclical dialogue and empathy. This level of care requires high concentration levels, and the carer needs to be competent to perform this level of care and have access to the appropriate resources to care [10].
The concept of non-technical care encompasses a wide range of interpersonal and contextual factors such as communication, empathy, trust, and shared decision-making [11], which are likely to be studied using diverse methodologies and across various settings. Given these findings there is a need for research that can further delve into the therapeutic relationship and consider care as part of communication and how it may also contribute to relationship conflict [12] and consider it within an understanding of the concept of trust [13] and be able to give a consideration to this within the area of psychological safety and sports medicine [14]. There is a greater need to reveal how SEM practitioners balance these competing needs and identify future research directions, but also to understand if existing frameworks e.g., the therapeutic alliance [15] do enough to address these issues. To further consider this, a scoping review methodology is well positioned to map the state of the literature.
This scoping review aims to systematically map the existing literature on conceptualisations and practices of care in SEM, with a particular focus on elite sport settings. It explores the perspectives of both SEM practitioners and athletes towards non-technical care, revealing the characteristics they consider necessary for a caring relationship, such as trust, verbal communication, and non-verbal communication and how practitioners might be able to develop these attributes.
2. Materials and Methods
Protocol and Registration
The scoping review was developed based on the PRISMA-ScR guidelines [16]; Protocol registered with the Open Science Framework on the 6th of September 2025, accessed: https://osf.io/
Eligibility Criteria
The eligibility criteria were identified using the recommended acronym PCC [17];
Population
The population included was sports medicine practitioners and/or athletes’ perspectives of their sports medicine practitioners. Sports medicine practitioners included Doctors, Physiotherapists and rehab therapists [18] who have regular contact with the athlete. Articles were included if they referenced other members of the multidisciplinary team, but only results related to the sports medicine team were extracted, and those results had to be a minimum of 2 sentences. There was no restriction on gender or age, including under 18 if they were competing at a national level.
Including the perspectives of the athletes provides an understanding of how they might perceive non-technical care.
Concept
Focus was on non-technical care in sport, which included communication, trust, and rapport between athletes and sports medicine practitioners. It looked if these traits were defined, how they might be developed and the importance for a positive therapeutic relationship.
Context
There was no restriction on geographical location and sports were included, including para sports. The criteria were focused on the participation level of the professional/elite. This was defined as athletes who are competing at the highest level within their sport, such as internationally. Within team sports, influential teams/athletes who are recognised within their respective sports. By focusing on elite sport, the aim was to review how non-technical care might be displayed in a full-time environment, considering the potential influence of the wider multidisciplinary team and performance impact.
Other
Full-text articles in English. Empirical research, whether published or not, such as theses were included. There was no date restriction or geographical location. This is to increase the potential data sources that could be included in the review.
Information Sources and Search
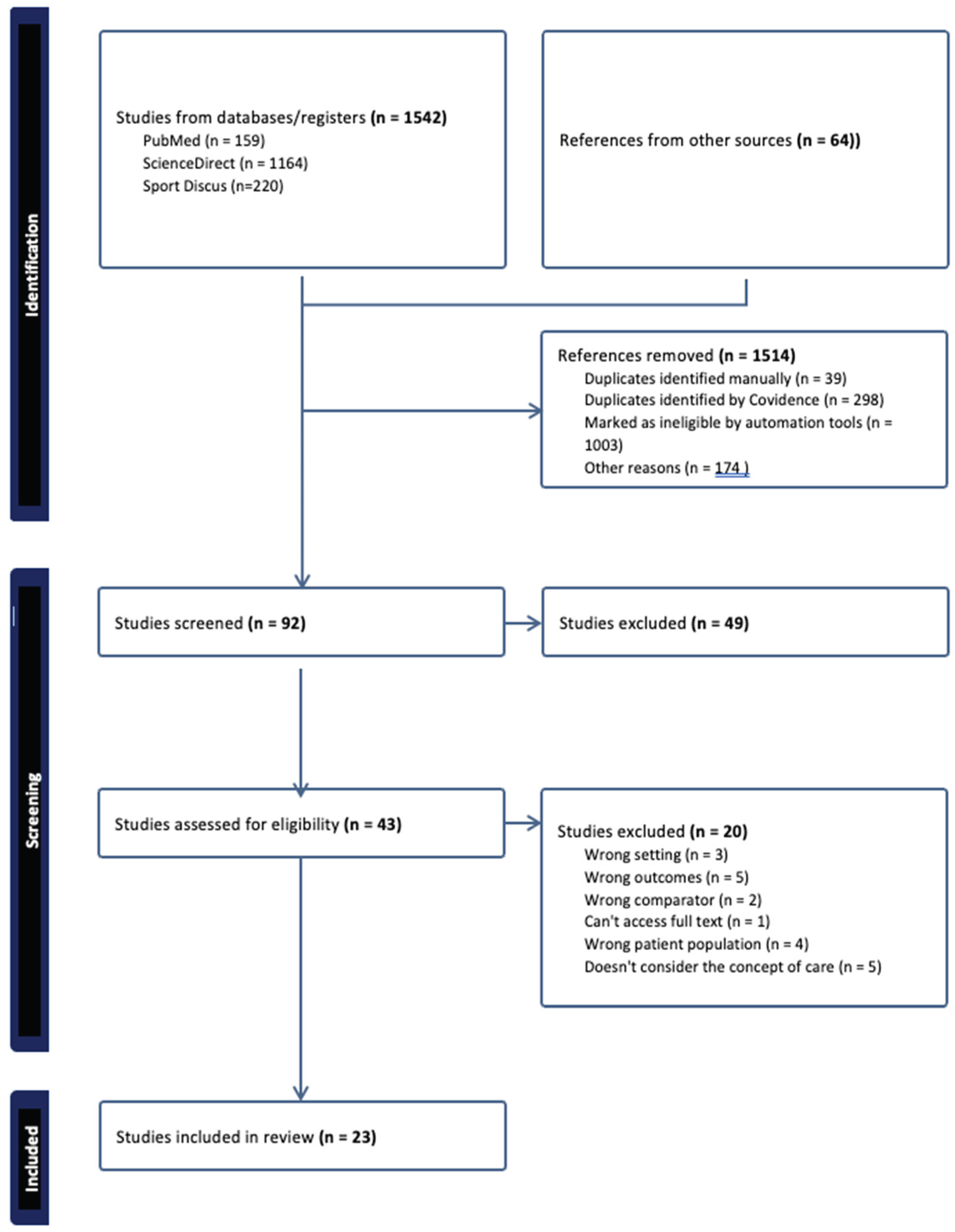
As shown in Figure 1, the following databases were accessed on August 11th, 2025: PubMed, Sport Discus, and ScienceDirect.
Databases were searched using the following key terms: “sports physiotherapy” OR “sports physiotherapist” OR “rehabilitation” OR “sports medicine” OR “athletic therapy” OR “physical therapy”) AND (“elite athlete*” OR “professional athlete*” OR “high-performance sport” OR “Olympic sport” OR “team sport”) AND (“decision-making” OR “shared decision making” OR “therapeutic alliance” OR “communication” OR “interprofessional collaboration” OR “pain” OR “injury” OR “return to play” OR “psychological skills” OR “trust” OR “adherence” OR “experiential learning”) AND (“qualitative” OR “semi-structured interview*” OR “survey” OR “case report” OR “phenomenological” OR “exploratory study”.
Articles were screened and duplicates removed using Covidence [19]. The lead author reviewed all articles, and secondary screening was completed between AS and PG.
Selection of Sources and Evidence
Titles and abstracts were screened first. Once duplicates were removed, screening against the topic area and inclusion criteria using Covidence was carried out. A second reviewer (PG/AS) systematically screened the articles with Covidence and was not aware of the decisions made by the other reviewers. Articles that were screened and where a conflict arose between two of the screeners were discussed and evaluated against the eligibility criteria. If no consensus was reached, the decision was referred to the reviewer not involved, who made the final call.
Data Charting Process and Data Items
Using Microsoft Excel, the main characteristics of the 43 articles were extracted based on their relevance to the study to facilitate in-depth reading of the articles by the lead author. The main characteristics extracted included study type, population, and results related to care. A critical appraisal of the articles was not completed due to the nature of the scoping review.
Synthesis
Due to the heterogeneity of the results, they are synthesised without a meta-analysis, using the amended Arksey and O’Malley scoping review framework by Westphaln et al. [20].
3. Results
Selection of Sources of Evidence
The search strategy identified a total of 1,542 papers: PubMed (n = 159), ScienceDirect (n = 1,164), and Sport Discus (n = 220). An additional 64 papers were included following hand searching and reference list screening (Figure 1). After title and abstract screening, 43 papers met the inclusion criteria. Following full-text review, 23 papers were included in the final synthesis (see Table 1).
Characteristics of Sources of Evidence
The included studies were published between 2000 and 2024, with 13 papers (57%) published between 2020 and 2024 [21,22,23,24,25,26,27,28,29,30,31,32,33]. Seventeen studies employed qualitative methodologies [21,22,23,24,25,26,27,28,29,30,33,34,35,36,37,38,39], primarily using semi-structured interviews. Four studies were quantitative [40,41,42,43] utilizing surveys. One study was a case report [32] and one was a narrative review [31].

Table 1.
Study Characteristics of the twenty-three articles included.
| Authors | Study Type | Location of study | Participants- SEM/Athlete | Gender | Key Findings |
| Aitchison, Rushton, Martin, Soundy and Heneghan (2021) [21] | Qualitative- Interviews | United Kingdom | 8 athletes | 5 Female, 3 Male | 1. Tangible aid- Emotional support, listening caring, information on injury prevention. provided emotional support through listening and caring, and informational support through offering advice on injury prevention. 2. Physiotherapy was also viewed as having the potential to be an educational tool if utilised correctly |
| Arvinen-Barrow, Massey and Hemmings (2014) [34] | Qualitative- Interviews | United Kingdom | 10 athletes | 10 males | 1. Athletes expect SEM to show a real interest in them and 100% effort to get them back fit. 2. Honest and open communication needed. 3. Expect SEM are able to pick up and read the athletes emotional state. 4. Motivate you and friend like behaviour |
| Barrette and Harman (2020) [22] | Qualitative- Interviews | North America | 4 athletes and 3 Rehabilitation specialists | 5 Female, 2 Male | 1. SEM a resource when unsure what is happening with body and trust the physio to guide 2. Supportive when injured but aware there was an element of risk taking due to pressure 3. Having a strong rapport improved rehab as athlete trusted it |
| Charmant, van der Wees, Staal, van Cingel, Sieben and de Bie (2021) [23] | Qualitative- Interviews | Netherlands | 10 physios and 10 athletes | 15 women and 5 males | 1. Relationship is entirely built upon trust 2. Communication- both parties need to see the other one as equals and small talk is an important aspect. 3. Good communication with the wider interdisciplinary team is required. 4. Athletes want to feel listened to, respected, shared-decision making and taken seriously. |
| Ekstrand, Lundqvist, Davison, D’Hooghe and Pensgaard (2018) [40] | Quantitative - Survey | Europe | 77 medical staff | Not stated | 1. Ranking low quality communication with the head coach had a higher injury burden and incidence. 2. High quality communication within the medical team- lower injury rates and better training attendance. 3. Attendance to training was lower if there was a lower quality communication between medics and fitness team. |
| Francis, Andersen and Maley (2000) [41] | Quantitative - Survey | Australia | 57 Physios and 28 athletes | Physios- 21 Female and 36 Male. Athletes 28 Male | 1. Positive communication an important factor. 2. Enthusiastic and knowledgeable physio. 3. Listening skills- interpersonal skills |
| Horan, Kelly, Hägglund, Blake, Roe and Delahunt (2023) [24] | Qualitative- Interviews | Ireland | 17 athletes and 8 medics | Medical- 2 Females and 6 male. Players 17 females | 1. Interpersonal skills and communication were key attributes in injury management. 2. Players believe that medics should put the athletes best interests first but it isn’t always the case. 3. Trust an important aspect- to report an injury and when to push them on through an injury |
| Kerai, Wadey, and Salim (2019) [35] | Qualitative- Interviews | United Kingdom | 10 physios | 5 Female and 5 Male | 1. Stress, burnout and transaction side of relationship. 2. Sport is high pressured and expected to be like that and impacts the culture 3. Relationship with MDT and athletes- Conflict as the organisation pays them when making difficult decisions |
| Knott (2024) [6] | Qualitative- Interviews | United Kingdom | 15 Physios | 7 females and 8 males | 1. A willingness to constantly go above and beyond for the athlete. 2. Often a poor work/life balance as need to sacrifice for the athlete. 2. There can be conflict between performance decision and health decisions. 3. Communication is important and style situational |
| Mann, Grana, Indelicato, O’Neill and George (2007) [42] | Quantitative - Survey | USA | 827 Doctors | Not stated | 1. Discomfort over discussing psychological and sensitive issues |
| Marks, Courtney and Healey (2023) [26] | Qualitative- Interviews | USA | 35 athletes | 15 Female and 20 Male | 1. A trusting relationship is a key factor, managing information not going further than they want to. 2. A previous or established history improves the trust |
| Marshall, Donovan-Hall and Ryall (2012) [36] | Qualitative- Interviews | United Kingdom | 9 athletes | 3 Females and 5 Males | 1. Athlete intrinsic motivation not to let the physio down. 2. Physio should be supportive, sympathetic, attentive, approachable, listens to their views. 3. Trusting the physio. |
| McKenna, Delaney and Phillips (2002) [37] | Qualitative- Interviews | United Kingdom | 10 Physios | 5 Female and 5 Male | 1. Having previous exp as an ex-athlete helped rapport and knowing the athletes world. 2. Knowing the athlete as a person. 3. Respect sometimes lacking from athlete to physio |
| Bonell Monsonís, Verhagen, Kaux and Bolling (2021) [27] | Qualitative- Interviews | Belgium | 8 athletes, 2 physical therapists and 1 medical doctor | Not stated | 1. Constant communication between athletes and SEM creates a trusting relationship. 2. Athlete has confidence in the SEM team |
| Noesgaard and Sæther (2024) [28] | Qualitative- Interviews | Norway | 2 athletes and 1 physio | Not stated | 1. Players and medical staff feel SEM must manage the performance and athlete health risks balance. 2. Players need to trust the SEM to make the right decision for them. 3. Trust, communication and collaboration are fundamental elements |
| Paraskevopoulos, Gioftsos, Georgoudis and Papandreou (2023) [29] | Qualitative- Interviews | Greece | 8 athletes | 5 female and 3 male | 1. Physio provides mental support. 2. Confidence in the physio through their years of experience and level of team |
| Rees and Hardy (2000) [38] | Qualitative- Interviews | United Kingdom | 10 athletes | 5 Female and 5 Male | 1. Reassurance from the physiotherapist 2. Physio experience in the sport themselves as an ex-athlete |
| Scott and Malcolm (2015) [39] | Qualitative- Interviews | United Kingdom | 14 physios and 14 doctors | Not stated | 1. Physios and doctors have a strong rapport and communicate well together, rarely have conflict. 2. Physios feel immersed with their athletes working with them closely. 3. Strong emotional element around managing the athlete and injury. 4. Need to establish trust with the athlete |
| Stewart, Fletcher, Arnold and McEwan (2023) [30] | Qualitative- Interviews | United Kingdom | 4 physios (18 MDT) | 5 female and 13 males | 1. Interpersonal compatibility, role clarity, culture, hierarchy affect the team effectiveness. 2. Shared objectives. 3. Communication a crucial aspect of team effectiveness and performance |
| Stewart, Fletcher, Arnold and McEwan (2024) [31] | Narrative review | N/A | N/A | N/A | 1. Desirable- disciplinary knowledge, technical competency, and interpersonal qualities |
| VanEtten, Briggs, DeWitt, Mansfield and Kaeding (2021) [32] | Case Report | USA | 1 athlete and 1 physio | 1 Therapist male and 1 athlete Male | 1. Communication and goal setting that was achievable and relatable to the athlete. 2. Rapport and trust improved adherence 3. Shared decision making on when to adjust interventions 4. Therapeutic alliance framework |
| Vella, Bolling, Verhagen and Moore (2022) [33] | Qualitative- Interviews | Malta | 7 athletes and 3 medics | 4 females and 9 males | 1. Relationship between physio and athlete can affect how much they are willing to push them |
| Woods and Woods (2012) [43] | Quantitative - Survey | Ireland | 13 athletes | 5 female and 8 males | 1. Good qualities- being accessible, interested in you, patient, persistent, communicator, understand the high emotional and psychological demands of the sport. 2. Communication to the athlete and wider MDT |
Key: SEM- Sports and Exercise Medicine. MDT- Multidisciplinary Team.
Geographically, 17 studies were conducted in Europe [6,21,23,24,27,28,29,30,31,33,34,35,36,37,38,39,40,43] four in North America [22,26,32,42], and one in Australia [41].
Regarding participant demographics, five studies [27,28,39,40,42], did not report participant gender, and one study [31] (a narrative review) deemed it not applicable. Two studies [32,34] included only male participants, while 15 studies [21,22,23,24,26,30,34,35,36,37,38,41,43] included both males and females.
Nine studies [22,23,24,27,28,32,33,39,41] involved both athletes and sports medicine practitioners. Seven studies [21,26,29,34,36,38,43] focused on athletes’ perspectives, while six [6,30,35,37,40,42] explored the views of sports medicine practitioners. One study [32] involved an elite paediatric athlete under the age of 18.
Participants represented a wide range of sports disciplines, with only one study [21] focusing specifically on para-sports. The largest sample size was 827 participants [42]. Three studies [26,40,41] had sample sizes between 30 and 90, while the remaining 18 studies [6,21,22,23,24,27,28,29,31,32,33,34,35,36,37,38,43] included 29 or fewer participants.
Synthesis of Results
Only one study [32] referenced a non-technical model or framework, highlighting the role of the therapeutic alliance in promoting exercise adherence and shared decision-making. Across the 23 included studies, key traits related to non-technical care were grouped into three overarching themes with corresponding subthemes: communication, trust, and non-technical characteristics of the ideal sports medicine practitioner.
- Communication
Communication was the most frequently reported theme, discussed in 17 studies [6,21,22,23,24,28,30,31,32,33,34,39,40,41,42,43] This theme explored the various forms, strategies, and impacts of communication in non-technical care.
1.1 Types of communication
Various forms of communication were identified, including active listening, verbal and non-verbal communication, and communication across the wider multidisciplinary team. Open and honest dialogue was explicitly emphasized in six studies [28,30,31,34,39,43]. Active listening was highlighted in four studies [21, 23, 30. 41] as essential for building rapport. Verbal communication was considered important, with tone, language, and timing significantly influencing effectiveness [6]. Communication across the multidisciplinary team was noted as valuable, as athletes appreciated when coaches and other practitioners were informed about their condition [24,30,31]. Non-verbal communication, such as body language and attentiveness, was recognized for reinforcing verbal messages and fostering rapport [23].
1.2 Strategies to develop successful communication
Strategies to develop successful communication included informal conversations or “small talk,” which were discussed in five studies [23,26,34,36,39]. These interactions helped reduce athlete anxiety and conveyed care and understanding from the practitioner. Athletes particularly valued clear explanations regarding injuries, rehabilitation processes, and expectations, as well as the accessibility of practitioners for ongoing support [32,43]. These factors contributed to athletes feeling involved in decision-making and having a sense of control.
1.3 Impact of successful communication
One quantitative study [40] measured the impact of communication and found that teams with high-quality communication among SEM professionals experienced significantly lower injury incidence and burden, along with improved training attendance. Three studies [23,30,39] reported that effective communication enhanced mutual respect and improved both personal and therapeutic outcomes for practitioners.
- 2.
- Trust
Trust was the second most frequently discussed theme, appearing in 15 studies [6,22,23,24,26,27,30,31,32,33,34,36,39,43]. It was influenced by the environment, the sensitivity of information shared, and the perceived competence of the SEM practitioner.
2.1 Definition of Trust
Despite its importance, a consistent definition of trust was lacking across studies. Only one study [23] provided a formal definition, describing trust as a combination of professional integrity and rapport, including confidentiality and genuine concern for athlete well-being. These elements were echoed across other studies, particularly in relation to injury disclosure [23,24,33,39]. Athletes noted that trust influenced their willingness to report injuries and return to the same practitioner. Some athletes feared that disclosing injuries could affect team selection, while others appreciated when practitioners advocated for appropriate rest or withdrawal from training.
2.2 Strategies to develop trust
Strategies to develop trust included long-term relationships, often developed over multiple seasons [26,39], and perceived credibility, which was influenced by practitioners’ affiliations with high-profile teams [29,36]. Nine studies [6,23,24,28,32,33,34,35,36,43] emphasized the importance of clinical competency in fostering athlete confidence and trust in the practitioner’s ability to facilitate return to competition.
- 3.
- Desired characteristics of a sports medicine practitioner
This theme examined the personal and professional attributes considered desirable SEM practitioners, as identified by both athletes and SEM professionals across the included studies.
3.1 Professional traits
Many of the professional qualities highlighted overlapped with elements discussed under the themes of communication and trust. Athletes consistently valued practitioners who prioritised a timely and safe return to sport, while also incorporating the athlete’s perspective into rehabilitation planning [34,36,37,40]. Collaborative approaches were particularly appreciated, as they empowered athletes to take an active role in their recovery. This sense of involvement was described as humanising and helped athletes feel recognised as individuals rather than simply as physical bodies [6,23,30,36]. Access and consistent presence of the SEM practitioner especially during training and competition were also identified as important from the athlete’s perspective [6,23,35,39]. However, SEM practitioners themselves expressed concern that such expectations could contribute to work-life imbalance and increase the risk of burnout [6,23,35].
3.2 Personal Attributes
A recurring sentiment was the importance of practitioners “just being a good person” [30]. This broad concept encompassed qualities such as humility, open-mindedness, and a willingness to collaborate within the wider multidisciplinary team [31]. These traits were seen as foundational to building rapport and fostering a supportive therapeutic environment. Additionally, prior experience as an athlete was perceived as a valuable asset [36,37]. Practitioners with athletic backgrounds were thought to possess a deeper understanding of the physical and psychological demands faced by athletes, which enhanced their ability to empathise and communicate effectively.
4. Discussion
This scoping review examined how non-technical care is conceptualised and practised within sport and exercise medicine (SEM), particularly in elite sport contexts. The findings reveal that care in SEM is primarily understood through two central themes: trust and communication. These themes are consistently highlighted across the literature in this study, yet there remains limited consensus on their precise definitions or on the strategies required to develop them. Without conceptual clarity, we remain in the dark as to how to improve or develop the relevant capacities in those trying to care, leading to inconsistency in practice.
Trust emerged as a critical but inconsistently defined concept. In broader healthcare literature, trust is often described as confidence in another person’s competence and intentions [13,44]. Aristotle’s triad of intelligence, character, and goodwill provides a useful lens for understanding how athletes initially place trust in practitioners [45]. These qualities can generate initial confidence at the start of a relationship, but deeper trust, which is necessary for athletes to disclose sensitive information, develops over time through repeated authentic interactions. Studies by Marks, Courtney and Healey [26] and Scott and Malcolm [39] emphasise that trust is strengthened across multiple seasons, as athletes and practitioners build a shared history together. Early trust may also be influenced by professional reputation [29,36], but athletes often remain cautious until they are convinced that practitioners act in their best interests. This reflects a symbolic interactionist perspective, where trust evolves through ongoing relational exchanges rather than being established once and for all at the outset.
Communication was equally central, encompassing both verbal and non-verbal dimensions. Noddings’ ethics of care [9,46] provides a valuable theoretical foundation, particularly her concept of engrossment, the deliberate attention to the cared-for person. In SEM practice, engrossment aligns with active listening, open-ended questioning, and the use of athletes’ own words in descriptions [47]. Such practices help alleviate anxiety and foster a sense of being understood. Informal “small talk” also plays a role in building rapport, as several studies have noted [23,26,34,36,39], though practitioners must remain cautious about self-disclosure. Behnia [13] warns that inappropriate or poorly timed self-disclosure can shift focus away from athlete needs and undermine the caring relationship. Effective communication therefore underpins reciprocal relationships, reinforcing trust and therapeutic outcomes.
The findings resonate strongly with the broader healthcare discourse on person-centred care (PCC). PCC emphasises individual values, autonomy, and experiences, moving beyond patient-centred models that risk overlooking the clinician’s role [48]. In SEM, PCC could provide a useful framework for integrating trust and communication while acknowledging the relational complexity of elite sport. Elite sport involves multiple intersecting dyads, athlete–practitioner, coach–athlete, practitioner- practitioner and coach–practitioner, and PCC helps practitioners navigate these dynamics while prioritising athlete wellbeing [10]. This assists with collaboration between the various dyads and a way to balance performance demands with the ethical responsibility to care for athletes as people rather than simply performers. This allows for reciprocity of care between the dyads which aligns with the second of the three core components of Nodding’s [9] care theory. By emphasising reciprocity and collaboration, PCC offers a way to balance performance demands. An example of this can be seen in Sports Coaching, Garner et al. [49] presents the POWA model that foregrounds humility as a central consideration for building trust in the coach-athlete dyad.
Empirical studies illustrate how care manifests in practice. Dohsten [50], for example, found that Swedish coaches demonstrated care by viewing athletes holistically, engaging in two-way dialogue, and fostering trust. They emphasised understanding athletes’ feelings both within and outside the sporting context, thereby creating a reciprocal relationship where feedback could be exchanged in both directions. Similarly, Morris et al. [51] reported that American rugby players valued coaches who prioritised safety and holistic support. Players described how coaches engaged in open conversations about careers and supported them in balancing training with family, education, or additional jobs. These practices demonstrated motivational displacement, where coaches put aside their own needs to prioritise those of the athletes. This is the third component of care in Nodding’s [9] theory. Players felt their voices were heard, and this sense of being valued motivated them to work harder and instilled greater confidence in their performance. Such examples highlight how care extends beyond injury management to encompass identity, autonomy, and wellbeing.
Despite these insights, explicit frameworks for non-technical care in SEM remain scarce. Only one study [32] referenced the shared-decision making model and therapeutic alliance model. Difficulties in applying shared decision-making in elite sport were noted by Nelis et al., [52]. Participants in that study believed that shared decision-making was less feasible in elite sport compared to general healthcare, due to the unique relational dynamics and performance pressures inherent in such environments. This strengthens the need for tailored frameworks that integrate communication, trust, and practitioner characteristics while accounting for the specific demands of elite sport. Such models could guide SEM practitioners in delivering consistent, person-centred care that balances technical expertise with relational and ethical dimensions.
The discussion of trust and communication also highlights the importance of context. Care in SEM is not static but adapts to different environments, such as the medical room, the field of play, or the human factor, emotion, personality, expectations and the team culture [53]. Nodding’s [46] emphasises that caring is an individual and complex process; what might be perceived as caring by one athlete may not be perceived the same way by another.
The relational complexity of elite sport further complicates the delivery of care. Athletes often operate within multidisciplinary teams, where SEM practitioners must balance confidentiality with the need to report injuries or performance concerns to coaches [5,6]. This dual responsibility can create tension, as athletes may withhold information due to concerns about selection or breaches of confidentiality [7,8]. Such dynamics highlight the ethical dimension of care, where practitioners must navigate competing responsibilities while maintaining trust and prioritising athlete wellbeing. Person-centred care provides a useful lens for addressing these challenges, as it emphasises reciprocity and collaboration, helping practitioners balance institutional demands with the needs of individual athletes [54].
Limitations and Future Research
This review has several limitations. The majority of the included studies employed qualitative methodologies, while valuable for exploring perspectives, are dependent on researcher interpretation and may limit generalisability. Only one study focused on para-sports and one on age-group athletes, leaving gaps in understanding how non-technical care is experienced across diverse populations. Moreover, the scarcity of explicit frameworks suggests that some relevant studies may have been missed due to terminology inconsistencies. Finally, while this review focused on non-technical care, it is important to recognise that technical and non-technical dimensions are interdependent; effective care requires both.
Future research should aim to develop and validate frameworks of PCC tailored to SEM. Comparative studies across different sporting contexts, including para-sports and youth athletes, would provide valuable insights into how non-technical care is experienced across diverse populations. Training programmes that explicitly address developing trust, non-verbal communication and relational skills may also enhance practitioner competence in delivering person-centred care. But it is vital that the athletes voice is a part of the future research to gain their perspectives and understanding of how they perceive care.
Clinical Implications
Communication with the athlete through both verbal and non-verbal communication enables SEM practitioners to establish a rapport to develop trust with the athlete. This can be achieved through various means such as “small talk” although being mindful the practitioner does not dominant the conversation. This enables initial trust with the athlete which can develop over time in to a deeper level of trust where the athlete feels comfortable about diverging more sensitive information. The SEM practitioner needs to keep the athlete as a person at the centre of their care and provide them with the space and ability to have a say in how they are cared for.
5. Conclusions
These findings demonstrate that non-technical care in SEM is primarily conceptualised through trust and communication, with desired practitioner characteristics reflecting an orientation towards person-centred care. However, explicit frameworks are scarce, and consensus on definitions and strategies remains limited. Integrating person-centred care into SEM offers a promising avenue for addressing these gaps, providing a structured framework that recognises athletes as individuals and fosters reciprocal relationships. SEM practitioners should approach every interaction with athletes as a dynamic and unique relationship, with the potential to positively or negatively influence both therapeutic outcomes and athletes’ perceptions of care. By embracing person-centred principles, practitioners can enhance the quality of non-technical care in elite sport, balancing performance demands with athlete wellbeing.
Author Contributions
Conceptualization, CW, PG and AS. methodology, CW, PG and AS, formal analysis, CW, PG and AS; writing—original draft preparation, CW writing—review and editing, CW, PG, IH and AS.; supervision, PG, AS and IH.; project administration, CW. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Donabedian, A. (1974). Aspects of Medical Care Administration. Harvard University Press: Cambridge, Mass.
- Krause, F. and Boldt, J. (2018) Care in Healthcare: Reflections on Theory and Practice. Palgrave Macmillan.
- Care Quality Commission. (2025). UK. Available at: https://www.cqc.org.uk.
- Dijkstra HP, Pollock N, Chakraverty R, Alonso JM. Managing the health of the elite athlete: a new integrated performance health management and coaching model. Br J Sports Med. 2014;48(7):523–31.
- Anderson, L. (2009) Writing a new code of ethics for sports physicians: principles and challenges. British Journal of Sports Medicine. 43: 1079-1082. [CrossRef]
- Knott, S. and Phillips, N. (2025) Speaking Up about Athlete Welfare in Sport – A Physio’s Challenge. IJSPT. 20(6):766-769. [CrossRef]
- White C., Garner, P., Horsley, I., Soundy, A. (2025) Experiences of Female Rugby Union Players and Practitioners in Rehabilitation Following a Shoulder Injury. Sports (Basel). May 28;13(6):166. PMID: 40559678; PMCID: PMC12196548. [CrossRef]
- Rees, H., J. Matthews, U. McCarthy Persson, E. Delahunt, C. Boreham and C. Blake (2022). “The knowledge and attitudes of field hockey athletes to injury, injury reporting and injury prevention: A qualitative study.” J Sci Med Sport 25(10): 820-827.
- Noddings, N. (1988). An ethic of caring and its implications for instructional arrangements. American Journal of 581 Education, 96(2), 215- 230. [CrossRef]
- Cronin, C., Z. R. Knowles and K. Enright (2019). “The challenge to care in a Premier League Football Club.” Sports Coaching Review 9(2): 123-146.
- Burns, L., Weissensteiner, J. and Cohen, M. (2019) Supportive interpersonal relationships: a key component to high- performance sport. British Journal of Sports Medicine. 53:22.
- Salcinovic, B., Drew, M., Dijkstra, P., Waddington, G. and Serpell, B. (2022) Factors Influencing Team Performance: What Can Support Teams in High-Performance Sport Learn from Other Industries? A Systematic Scoping Review. Sports Medicine Open. 8:25. [CrossRef]
- Behnia, B. (2008) Trust Development: A Discussion of Three Approaches and a Proposed Alternative. British Journal of Social Work. 38, 1425-1441. [CrossRef]
- Walton, C., Purcell, R., Pilkington, V., Hall, K., Kentta, G., Vella, S. and Rice, S. (2024) Psychological Safety for Mental Health in Elite Sport: A Theoretically Informed Model. Sports Medicine. 54:557-564. [CrossRef]
- Hall A, Ferreira P, Maher C., Latimer, J. and Ferreira, M. (2010) The influence of the therapist- patient relationship on treatment outcome in physical rehabilitation: a systematic review. Physical Therapy. 90:8, 1099 –1110.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. (2018) PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 169:467–73. [CrossRef]
- Peters MD. In no uncertain terms: the importance of a defined objective in scoping reviews. JBI Database System Rev Implement Rep. 2016;14(2):1–4.
- McEwan, I. and Taylor, W. (2010) ‘When do I get to run on with the magic sponge?’ The twin illusions of meritocracy and democracy in the professions of sports medicine and physiotherapy, Qualitative Research in Sport and Exercise, 2:1, 77-91. [CrossRef]
- Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
- Westphaln, K., Regoeczi, W., Masotya, M., Vazquez-Westphaln, B., Lounsbury, K., McDavid, L., Lee, H., Johnson, J. and Ronis, S. (2021) From Arksey and O’Malley and Beyond: Customizations to enhance a team-base d, mixe d approach to scoping review methodology. MethodsX. 8.
- Aitchison, B., Rushton, A., Martin, P., Soundy, A. and Heneghan, N. (2021) The podium illusion: a phenomenological study of the influence of social support on well-being and performance in elite para swimmers. BMC Sports science, medicine and Rehabilitation. 13:42. [CrossRef]
- Barrette, A., & Harman, K. (2020). Athletes Play Through Pain-What Does That Mean for Rehabilitation Specialists? J Sport Rehabil, 29(5), 640-649. [CrossRef]
- Charmant, W. M., van der Wees, P. J., Staal, J. B., van Cingel, R., Sieben, J. M., & de Bie, R. A. (2021). A framework exploring the therapeutic alliance between elite athletes and physiotherapists: a qualitative study. BMC Sports Sci Med Rehabil, 13(1), 122. [CrossRef]
- Horan, D., Kelly, S., Hagglund, M., Blake, C., Roe, M., & Delahunt, E. (2023). Players’, Head Coaches’, And Medical Personnels’ Knowledge, Understandings and Perceptions of Injuries and Injury Prevention in Elite-Level Women’s Football in Ireland. Sports Med Open, 9(1), 64. [CrossRef]
- Knott, S. (2024) Speaking Up in Elite Sport: An exploratory-descriptive qualitative study of UK physiotherapists’ experiences. Thesis. Cardiff University.
- Marks, A., Courtney, C. A., & Healey, W. E. (2023). Perceptions of Physical Therapy and The Role of Physical Therapists In Injury Prevention Among Professional Basketball Players: A Qualitative Study. Int J Sports Phys Ther, 18(5), 1186-1195. [CrossRef]
- Bonell Monsonís O, Verhagen E, Kaux J-F, et al. ‘I always considered I needed injury prevention to become an elite athlete’: the road to the Olympics from the athlete and staff perspective. BMJ Open Sport & Exercise Medicine 2021;7:e001217. [CrossRef]
- Noesgaard, M. and Sæther, S. (2024) Decision-making on injury prevention and rehabilitation in professional football – A coach, medical staff, and player perspective. The Sport Journal.
- Paraskevopoulos, E., Gioftsos, G., Georgoudis, G., & Papandreou, M. (2023). Perceived Barriers and Facilitators of Sports Rehabilitation Adherence in Injured Volleyball Athletes: A Qualitative Study From Greece. Journal of Clinical Sport Psychology, 17(1), 86-105. [CrossRef]
- Stewart, P., Fletcher, D., Arnold, R., & McEwan, D. (2023). Exploring perceptions of performance support team effectiveness in elite sport. Sport Management Review, 27(2), 300-321. [CrossRef]
- Stewart, P., Fletcher, D., Arnold, R., & McEwan, D. (2024). Performance support team effectiveness in elite sport: a narrative review. International Review of Sport and Exercise Psychology, 1-24. [CrossRef]
- VanEtten, L., Briggs, M., DeWitt, J., Mansfield, C., & Kaeding, C. (2021). The Implementation of Therapeutic Alliance in the Rehabilitation of an Elite Pediatric Athlete with Salter-Harris Fracture: A Case Report. Int J Sports Phys Ther, 16(2), 539-551. [CrossRef]
- Vella, S., Bolling, C., Verhagen, E., & Moore, I. S. (2022). Perceiving, reporting and managing an injury - perspectives from national team football players, coaches, and health professionals. Sci Med Footb, 6(4), 421-433. [CrossRef]
- Arvinen-Barrow, M., Massey, W. V., & Hemmings, B. (2014). Role of sport medicine professionals in addressing psychosocial aspects of sport-injury rehabilitation: professional athletes’ views. J Athl Train, 49(6), 764-772. [CrossRef]
- Kerai, S., Wadey, R., & Salim, J. (2019). Stressors experienced in elite sport by physiotherapists. Sport, Exercise, and Performance Psychology, 8(3), 255-272. [CrossRef]
- Marshall, A., Donovan-Hall, M. and Ryall, S. (2012) An exploration of athletes’ views on their adherence to physiotherapy rehabilitation after sport injury. Journal of sport rehabilitation. 21, 18-25.
- McKenna, J., Delaney, H., & Phillips, S. (2002). Physiotherapists’ lived experience of rehabilitating elite athletes. Physical Therapy in Sport, 3(2), 66-78. [CrossRef]
- Rees, T and Hardy, L. (2000) An investigation of the social support experiences of high-level sports performers. The Sports Psychologists. 14, 327-347.
- Scott, A., & Malcolm, D. (2014). ‘Involved in every step’: how working practices shape the influence of physiotherapists in elite sport. Qualitative Research in Sport, Exercise and Health, 7(4), 539-556. [CrossRef]
- Ekstrand, J., Lundqvist, D., Davison, M., D’Hooghe, M., & Pensgaard, A. M. (2019). Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs. Br J Sports Med, 53(5), 304-308. [CrossRef]
- Francis, S., Andersen, M. and Maley, P. (2000) Physiotherapists’ and male professional athletes’ views on psychological skills for rehabilitation. Journal of Science and Medicine in Sport 3 {1):17-29.
- Mann, B. J., Grana, W. A., Indelicato, P. A., O’Neill, D. F., & George, S. Z. (2007). A survey of sports medicine physicians regarding psychological issues in patient-athletes. Am J Sports Med, 35(12), 2140-2147. [CrossRef]
- Woods, A., & Woods, C. B. (2012). An exploration of the perspectives of elite Irish rowers on the role of the sports physiotherapist. Phys Ther Sport, 13(1), 16-21. [CrossRef]
- Rousseau, D. M., Sitkin, S. B., Burt, R. S. and Camerer, C. (1998) ‘Not so different after all: A cross-discipline view of trust’, Academy of Management Review, 23(3), pp. 393–404.
- Giffin, K. (1973) ‘Interaction variables of interpersonal trust’, Humanitias, 9(3), pp. 297–315.
- Noddings, N. (2013). Caring; A relational approach to ethics and moral education. London: University of California Press.
- Kleiner, M., Kinsell, E., Miciak, M., Teachman, G. and Walton, D. (2022) “Passion to do the right thing”: searching for the ‘good’ in physiotherapist practice. Physiotherapy Theory and Practice. 40:2, 288-303. [CrossRef]
- Buetow, S. (2011) Person-centred care: Bridging current models of the clinician- patient relationship. The international Journal of Person Centred Medicine. 1:1. 196-203.
- Garner, P., Roberts, W., Baker, C. and Cote, J. (2022) Characteristics of a person-centred coaching approach. International Journal of Sports Science & Coaching. 17(4) 722–733. [CrossRef]
- Dohsten, J., Barker-Ruchti, N., & Lindgren, E. C. (2020). Caring as sustainable coaching in elite athletics: benefits and challenges. Sports Coaching Review, 9(1), 48–70. [CrossRef]
- Morris, S., Fisher, L., Moore, M., Schools, J., Knust, S. and Christy, Z. (2023) “Make someone love something and share your passion”: Perceptions of coach caring amongst Elite women’s rugby sevens athletes, Sports Coaching Review, 12:1, 87-107. [CrossRef]
- Nelis S, Dijkstra HP, Damman OC, Farooq, A. and Verhagen, E. (2024) Shared decision-making with athletes: a survey study of healthcare professionals’ perspectives. BMJ Open Sport & Exercise Medicine;10:e001913. [CrossRef]
- Armour, K. (2014) Pedagogical cases in physical education and youth sport. (1st edition) Oxon: Routledge.
- Tomaselli G, Buttigieg SC, Rosano A, Cassar M and Grima G (2020) Person-Centered Care From a Relational Ethics Perspective for the Delivery of High Quality and Safe Healthcare: A Scoping Review. Front. Public Health 8:44. [CrossRef]
Figure 1.
PRISMA-SCR flow chart of selection of sources of evidence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



